Athletes both recreational and fully competitive can be impacted by injuries to the muscles and ligaments around the hip.
These injuries interfere with performance levels and sometimes end participation completely.
�Excessive pronation along with shoes with poor shock absorption has been found to be an underlying cause for various leg/hip injuries.
Custom made Orthotics improve the biomechanics of the feet and reduce the extent of pronation helping to prevent sport-related leg/foot injuries.
Over Foot Pronation
Research has determined that athletes with more foot pronation have a higher probability of sustaining a leg injury, including iliotibial band syndrome that comes from excessive tightness of the hip muscles.
People involved in sports or recreational activities lower their likelihood of developing traumatic and overuse hip injuries through chiropractic treatment and using custom foot orthotics.
The amount of pronation during standing and while running at a standard speed is determined by measuring the angles of the footprints.
Athletes with more pronation have a higher likelihood of an overuse injury.
Standing (static) and running (dynamic) prints show the amount of pronation and is a predictor of developing an overuse injury.
Athletic performance and injury prevention involve regularly checking the alignment of patients� feet in the standing position.
Hip Injuries & The Hamstring
Many hip injuries develop from poor biomechanics and improper movement, especially when running.
Smooth muscle coordination provides balance and support for the pelvis and is needed for optimum sports performance.
This includes:
Hamstring muscles
Hip abductor muscles
Tensor fascia lata or the iliotibial band
When there is an issue with the feet and ankles, abnormal motion like over-rotating the entire leg is the perfect set-up for pulls, sprains, and strains.
50% of standing consists of heel strike and maximum pronation.
The hamstring muscles function to control the knee and ankle when the heel strikes and absorb the impact.
The theory behind orthotic support is that orthotics help the hamstrings control the position of the calcaneus and knee, so there is less stress on the hip and pelvis.
Hip Injuries & Over-Pronation
Orthotics can correct excessive pronation and treatment of hip problems. These are some of the problems/pathologies that can develop.
These conditions develop in athletes who push their body’s to the limit going for optimal performances.
Conclusion
Overpronation and poor shock absorption contribute to leg injuries � from:
Foot
Lower leg
Knee
Thigh
Hip
These conditions can be prevented with custom-made orthotics.
Foot biomechanics evaluation is a must
To avoid hip injuries, athletes need regular evaluations of foot alignment and function
Wear well-designed and solid-constructed shoes
Chiropractors can prevent arch breakdown and foot problems with custom orthotics, and also treat numerous injuries to the lower extremities, especially the hips.
Excessive Foot Pronation can Affect *FOOT POSTURE & MOBILITY* | El Paso, TX (2019)
The following video discusses how excessive foot pronation can ultimately affect foot posture and mobility. Several factors can affect foot posture and mobility, such as excessive foot pronation. Excessive foot pronation is most prevalent among the general population, therefore, it is considered to be one of the most common factors for abnormal foot posture and mobility, which can lead to a variety of health issues like overuse injuries. Excessive foot pronation and even supination can ultimately affect overall health and wellness.
Hip Labrum tears in athletes can occur from a single event or recurring trauma. Running may cause labrum tears due to the labrum being utilized more for weight-bearing and taking excess forces while at the end-range motion of the leg. Sporting activities are probable causes, specifically those that require frequent hip rotation or pivoting to a loaded femur as in ballet or hockey. Constant hip rotation places increased strain on the capsular tissue and harm to the iliofemoral ligament. This subsequently causes hip instability putting increased stress on the labrum and causing a hip labrum tear.
What’s Afoot
Chiropractic�seeks to find the cause of the conditions it is used to treat, including pain, instead of just treating symptoms. Because of this, the chiropractor will work to find the cause of the pain, in this case, overpronation and overpronation, and correct it � or the effects of the condition � in addition to treating the back pain.
Overpronation and oversupination can cause a variety of injuries and conditions that affect not only the feet and ankles, but also the knees,�hips, and back as well. Some of the more common injuries and conditions include:
Flat feet or posterior tibial tendon dysfunction
Ankle Sprains
Achilles tendinitis
Arch pain
Plantar fasciitis
Corns
Shin splints
Heel pain
Tight calves
Calluses
Knee pain
Patellar tendonitis
Tight hip flexors
Back pain
Sciatica
Herniated disks
NCBI Resources
Muscle imbalances in the hip, such as tight hip flexors, can cause low back pain � or at least contribute to it. When the hip flexor muscles are too tight, it causes what is known as an anterior pelvic tilt.�Hip flexors�can become too tight if the person sits for extended periods of time or engages in activities like cycling and jogging. A chiropractor can guide you through exercises that will help release the tight muscles and stop the micro spams that occur as a result.
Although hip pain is most often associated with older individuals, in reality, it can affect people from all age groups. The hips are complex joints, which means there are many things that can go wrong in the hips�complications that can lead to pain and discomfort in the hip area. Whatever your age, when hip pain strikes you naturally want to know if there is a way to make it better or eliminate it altogether. Fortunately, chiropractic offers effective methods for addressing hip pain.
Causes of Hip Pain?
There are a surprising number of ways that hip pain can develop. It may show up at one or both sides of your hips, or on the front of your hip. It can also show up on the back of one or both hips. Where the pain develops can serve as an indicator of what is actually causing the pain. Your chiropractor will look closely at your condition to determine the cause, which may be attributed to the following:
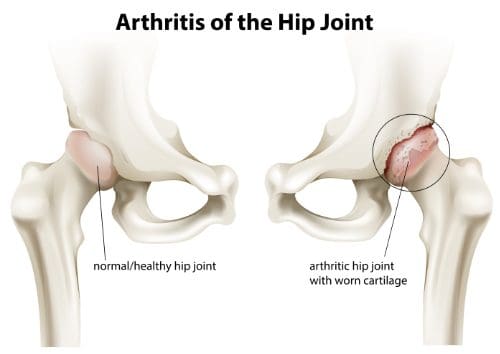
Osteoarthritis
The cartilage that surrounds your joints can begin to wear down over time. The degeneration of cartilage around joints is known as osteoarthritis. Many times, osteoarthritis can develop due to normal wear and tear, which is why the condition is so often associated with aging. However, it is possible for younger individuals to develop osteoarthritis as well.
Transient Osteoarthritis
Both middle-aged men and pregnant women can suffer from transient osteoarthritis. It is a painful condition, but fortunately, it is reversible with proper treatment.
Bursitis
Bursa are sacs filled with fluid found in your joints, including the hips. The bursa are supposed to provide cushioning to your joints and lessen the friction created as your joints move. However, the bursa can become inflamed, which can lead to pain each time the joint is used.
Muscle Strain
There are a multitude of muscles that support the hips and make it possible for them to function. If one or more of those muscles is strained, it can lead to pain. Muscle strain is common in active individuals.
Overuse
Any joint and the soft tissues that support it can be overused. Overuse is common in individuals who perform repetitive motions, such as having to do the same motion hundreds of times a day for particular job activity.
Chiropractic Can Help
Studies have shown that chiropractic can increase mobility and lessen the pain when patients are experiencing hip pain. Treatment can be quite effective for many hip conditions, including all of those listed above. Since chiropractic steers clear of unnecessary medications and surgery, it is non-invasive and can be used regularly with minimal risk of side effects. Even if the condition you suffer from is not completely eliminated by treatment, it can make your symptoms much more tolerable by reducing pain and improving mobility.
Some common treatments for hip pain in chiropractic include:
Adjustments
By realigning your spine, adjustments can reduce or eliminate strain that may be placed on your hips. Regular adjustments can help ensure that your body maintains alignment and minimizes the amount of unnecessary strain might be impacting your hip area.
Exercises
Sometimes the best long-term solution to hip pain is to strengthen the muscles surrounding the hips. Your chiropractor can give you personalized exercises based on your body�s needs to help you get stronger so that your body supports your hips day in and day out.
Stretches
Hip pain can lead to loss of mobility. Appropriate stretches can help you regain some of that mobility.
Contact Us & Schedule An Appointment for Hip Pain Relief
Labrum Tear Hip Treatment El Paso, TX Chiropractor
Andrew Hutchinson turned into chiropractic care and Crossfit rehab after suffering a high ankle sprain and a hip labrum tear for which he moved through with surgery to repair it. After being bedridden for weeks so as to correctly recuperate, Andrew Hutchinson transitioned to chiropractic care and Crossfit rehab to regain his strength, freedom, and flexibility before returning to perform. Although he has suffered other sports accidents, Andrew Hutchinson continues to trust in chiropractic care and Crossfit rehab to keep his spine properly aligned and maintain overall health and wellbeing.
Labrum rips in athletes may occur from a single event or recurring trauma. Running may lead to labrum tears as a result of labrum being used more for weight-bearing and taking excessive forces while at the end-range motion of the leg. Sporting activities are likely causes, especially the ones that require frequent hip rotation or pivoting to some wealthy femur as in ballet or hockey. Continuous hip rotation places increased pressure on the capsular tissue and injury to the iliofemoral ligament. This then causes hip instability placing increased stress on the labrum and resulting in a cool labrum tear.
Hip Weakness
Muscle imbalances in the hip, such as tight hip flexors, can cause low back pain � or at least contribute to it. When the hip flexor muscles are too tight, it causes what is known as an anterior pelvic tilt.�Hip flexors�can become too tight if the person sits for extended periods of time or engages in activities like cycling and jogging. A chiropractor can guide you through exercises that will help release the tight muscles and stop the micro spams that occur as a result.
NCBI Resources
Treating your hip is successful when the focus is on restoring the balance and function of the entire body. This starts from the ground up with the feet along with a chiropractic examination that determines the root cause, which in turn helps in making an informed decision on a treatment plan. This instead of merely reducing the pain and inflammation in the irritated areas.
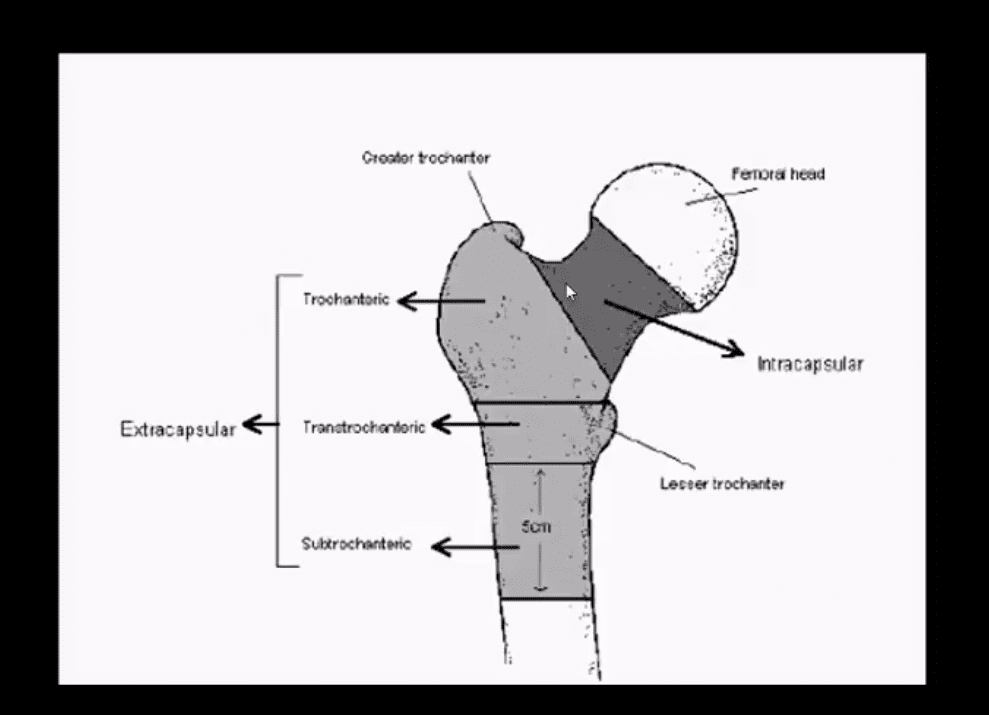
The hip joint is the body�s largest ball-and-socket joint that allows for fluid movement during running, walking, and more.
There is a cushion of cartilage that helps prevent friction when the hip bone moves.
The hip is durable, but with age and use, this cushion can wear down or sustain an injury. So can the muscles, tendons, and bones surrounding the hip, caused by several conditions. These include:
Arthritis, Avascular necrosis (or osteonecrosis)
Certain cancers
Bursitis
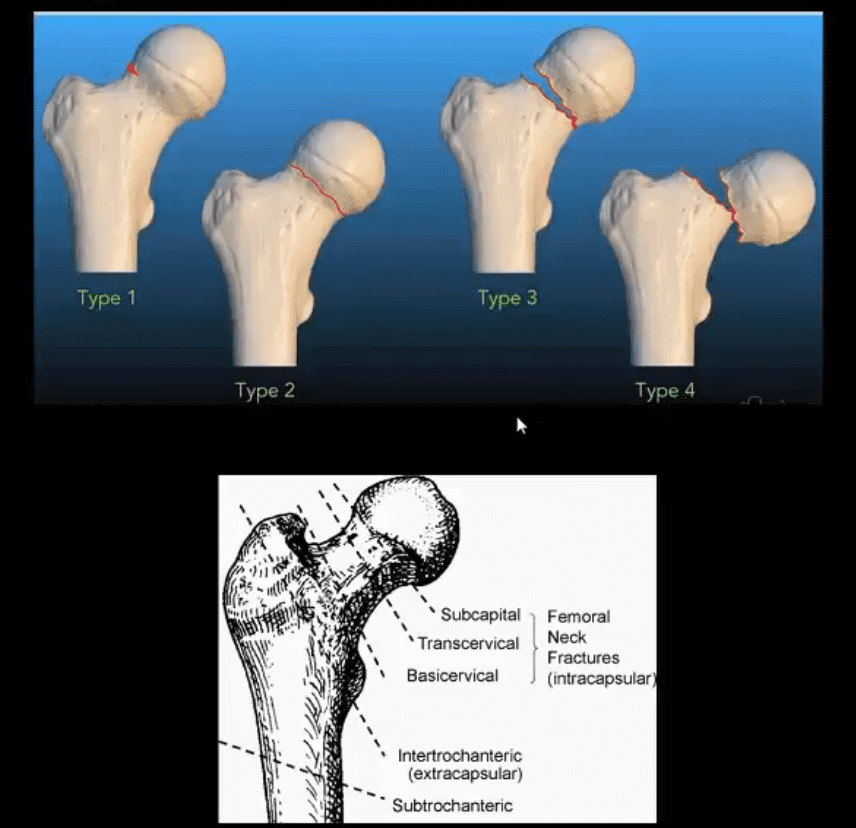
Hip fractures
Hip labral tear
Muscle or tendon strain
Tendinitis
Treating your hip is successful when the focus is on restoring the balance and function of the entire body. This starts from the ground up with the feet along with a chiropractic examination that determines the root cause, which in turn helps in making an informed decision on a treatment plan. This instead of merely reducing the pain and inflammation in the irritated areas.
Symptoms of Hip Pain
Depending on the condition that’s causing your hip pain, you might feel the discomfort in:
Inside of the hip joint
Outside of the hip joint
Groin
Buttocks
Thigh
Treatment
Chiropractic and custom orthotics can help alleviate hip pain with adjustments, icing/heating and resting the affected joint.
Your chiropractor can help you set up a stretching and strengthening exercise regimen that will improve your hip�s function and reduce your pain.
Benefits of Using Custom *Foot Orthotics* | El Paso, TX (2019)
Functional custom foot orthotics understand the anatomy of the foot. By supporting the 3 arches of the foot, functional custom foot orthotics can help promote proper posture to prevent a variety of health issues, including neck pain and back pain. Over the counter, inserts may create more harm than good. Functional custom foot orthotics can also help maintain overall health and wellness. Because every person is unique, functional custom foot orthotics can help balance a person’s unique body structure and function. Dr. Alex Jimenez can help provide functional custom foot orthotics to patients who need to improve their overall health and wellness.
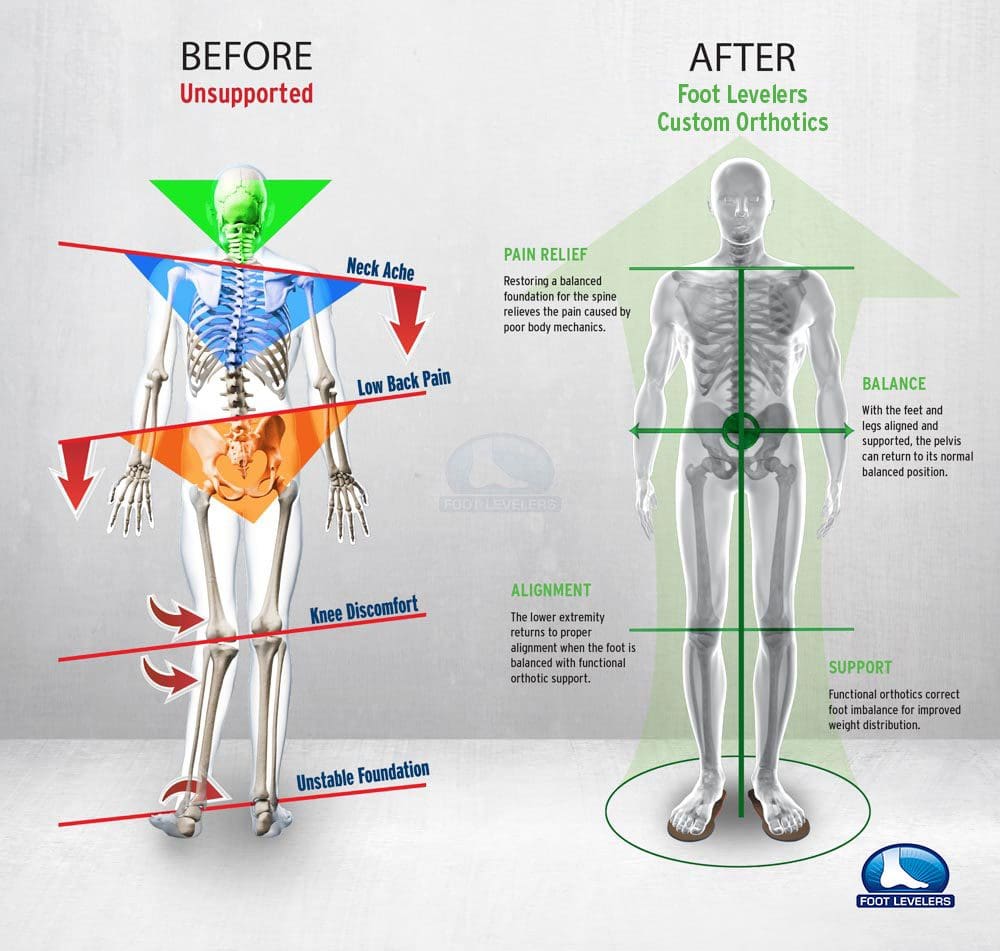
Custom Orthotics
When there are problems with the feet, it can cause problems through the legs and all the way to the spine. This can cause the ankle to pronate, meaning it rolls inward. This alters the way the�bones of the foot line up which extends through the tibia, or shin bone. This can cause a condition called knock knees and it can change the way the entire body is aligned. This puts the body out of balance, destabilizing the spine, and can even cause the pelvis to tilt to one side or the other.
Weak Hip Abduction
Muscle imbalances in the hip, such as tight hip flexors, can cause low back pain � or at least contribute to it. When the hip flexor muscles are too tight, it causes what is known as an anterior pelvic tilt. Hip flexors�can become too tight if the person sits for extended periods of time or engages in activities like cycling and jogging. A chiropractor can guide you through exercises that will help release the tight muscles and stop the micro spams that occur as a result.
NCBI Resources
If the health issue originates in the hip joint itself, common painful symptoms may often include groin pain on the affected side, which can occasionally radiate down the inner region of the thigh into the front of the leg. The painful symptoms can also travel to the knee, making healthcare professionals and patients believe their pain is associated with a knee problem rather than a hip problem
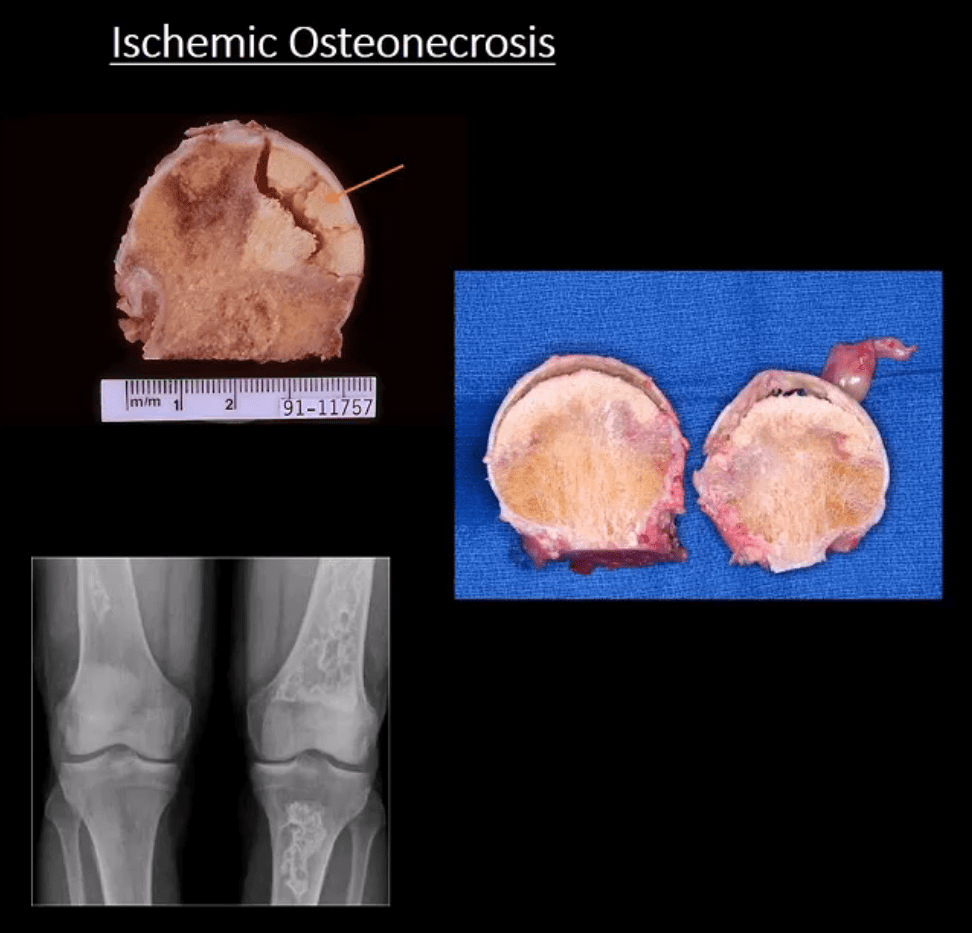
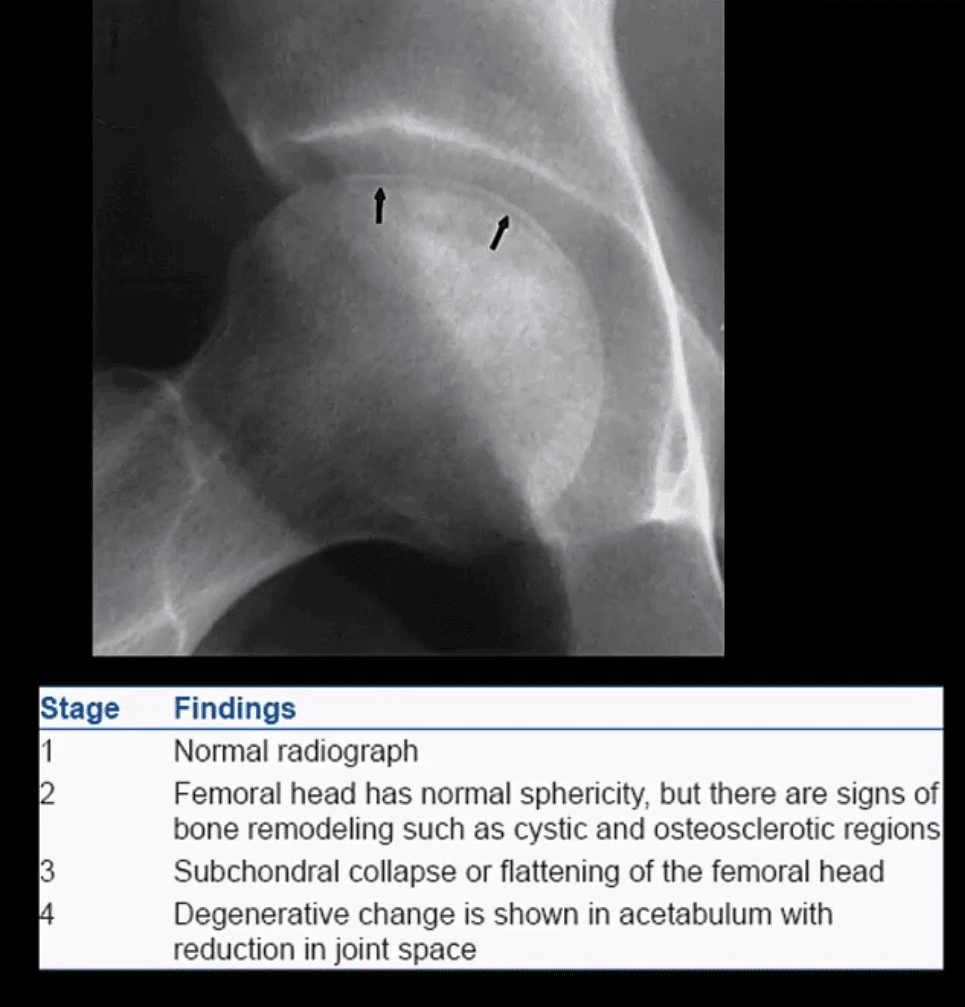
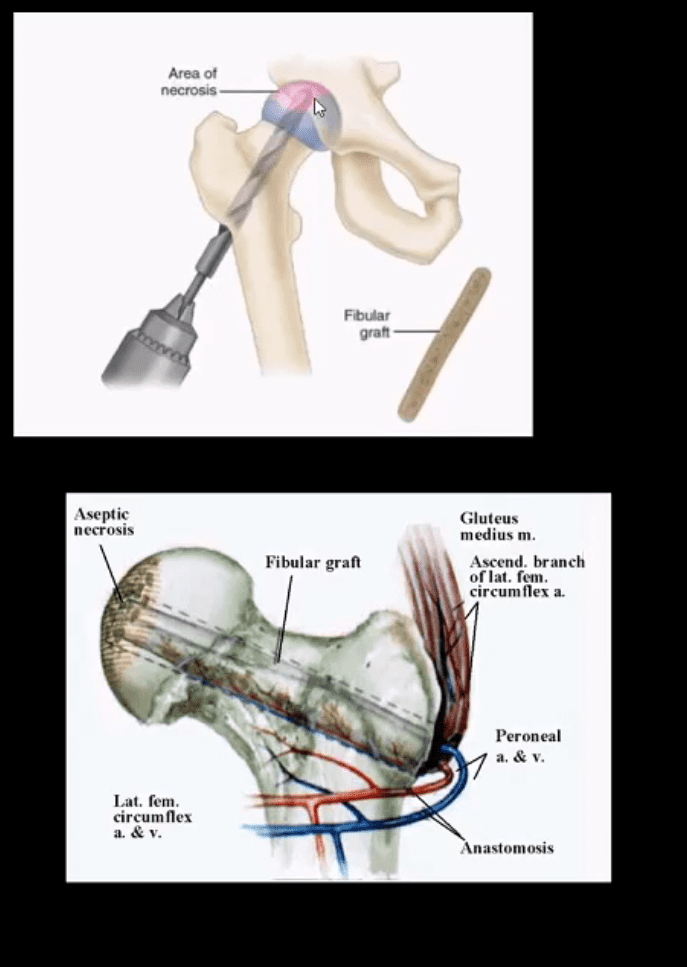
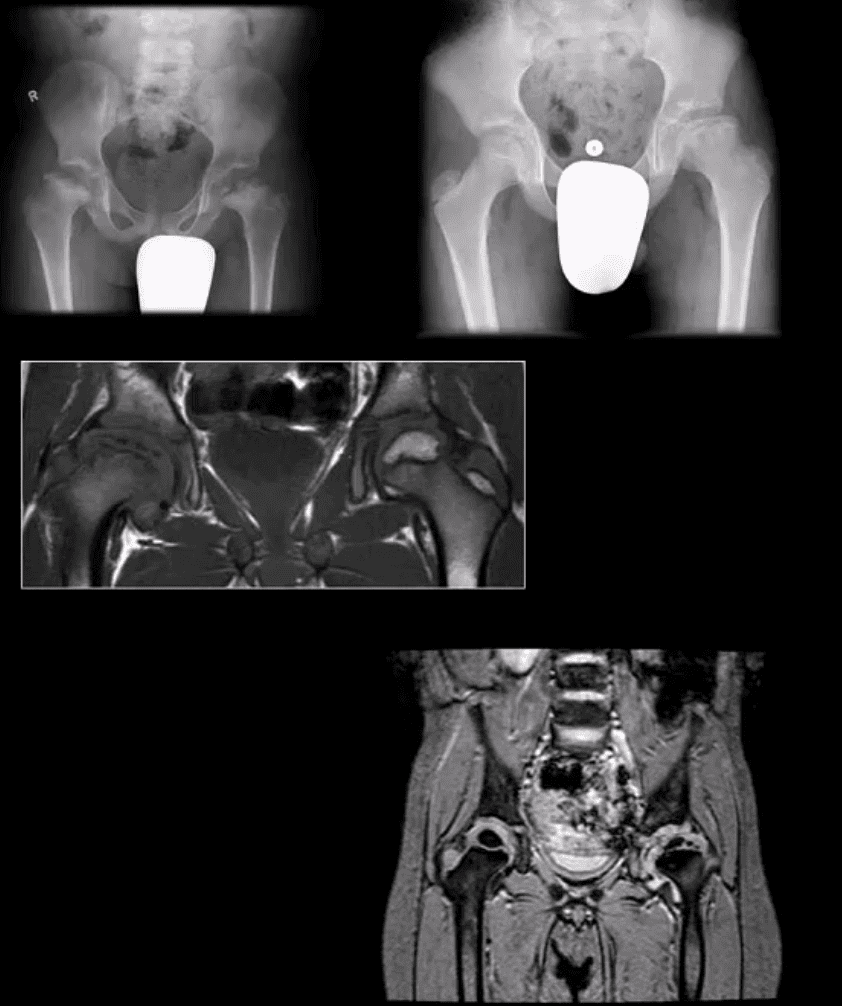
Ischemic Osteonecrosis (More accurate term) aka avascular necrosis AVN: this term describes subarticular (subchondral) bone death
Intramedullary bone infarct: depicts osteonecrosis within the medullary cavity of the bone (above x-ray image)
Causes: m/c: trauma, systemic corticosteroids, diabetes, vasculitis in SLE. The list is long. Other vital causes: Sickle cell disease, Gaucher disease, alcohol, caisson disease, SCFE, LCP, etc.
Pathology: ischemia and bone infarct with resultant devitalized center surrounded by ischemia and edema with normal bone on the outer periphery (MRI double line sign)
Sub-articular necrotic bone eventually collapses and fragments leading to progressive bone and cartilage destruction and rapidly progressing DJD
Early Dx often missed but crucial to prevent severe DJD
M/C Sites
Hips, shoulders, talus, scaphoid bone. Many peripheral idiopathic AVN sites are known by their eponyms (e.g., Kienbock aka AVN of the lunate bone, Preisier aka scaphoid AVN)
Radiography is insensitive to early AVN and may only present as subtle osteopenia
Some of the early appreciable rad features are increased patchy bone sclerosis followed by sub-articular bone collapse or “crescent sign” signifying stage-3 on Ficat classification (above)
Earliest detection and early intervention can be achieved by MRI (most sensitive modality)
If MRI contraindicated or unavailable, 2nd most sensitive modality is radionuclide bone scan (scintigraphy)
X-ray and CT scanning are of equal value
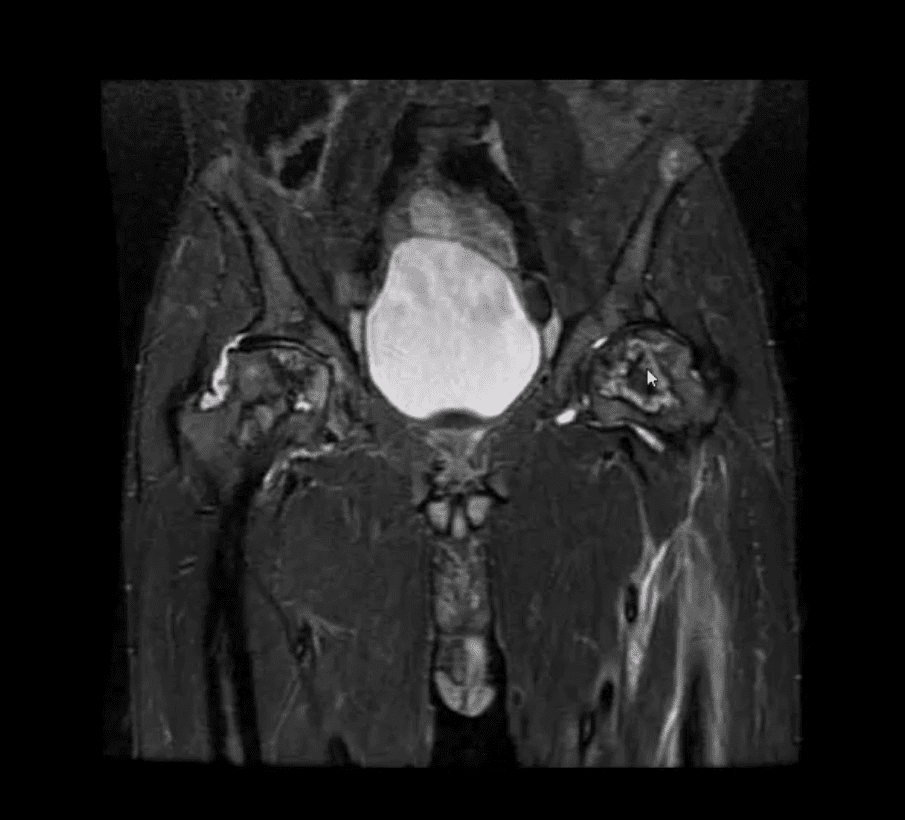
Coronal MRI Slice
Fluid sensitive, sensitive coronal MRI slice revealing bill ischemic osteonecrosis of the femoral head
MRI findings: l
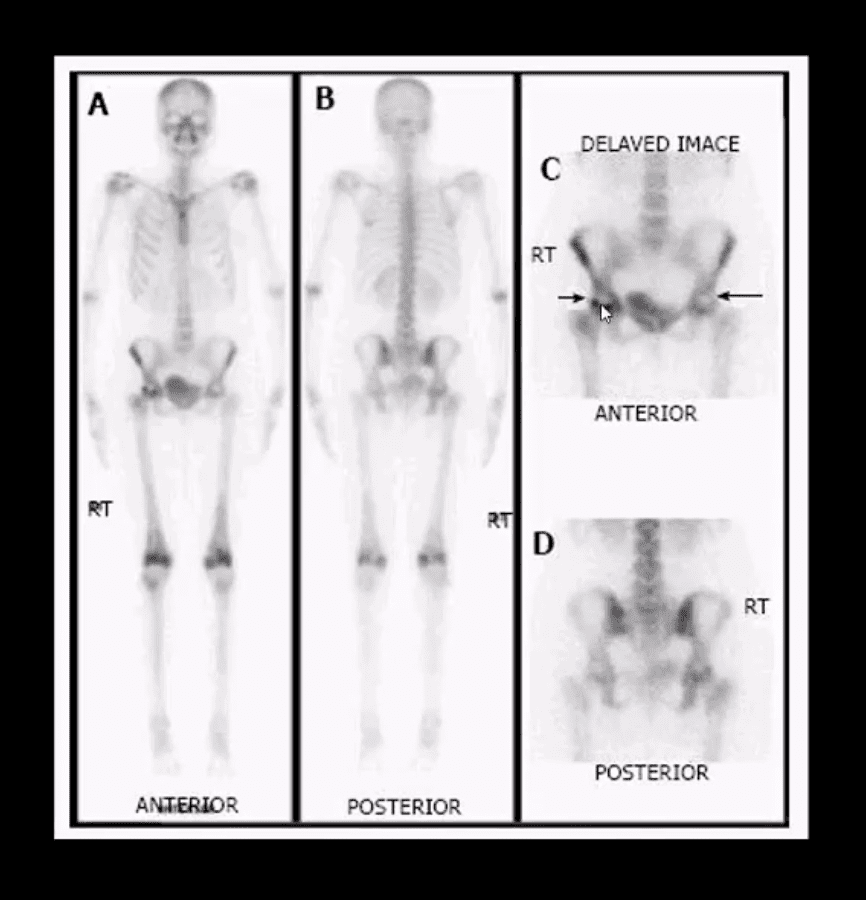
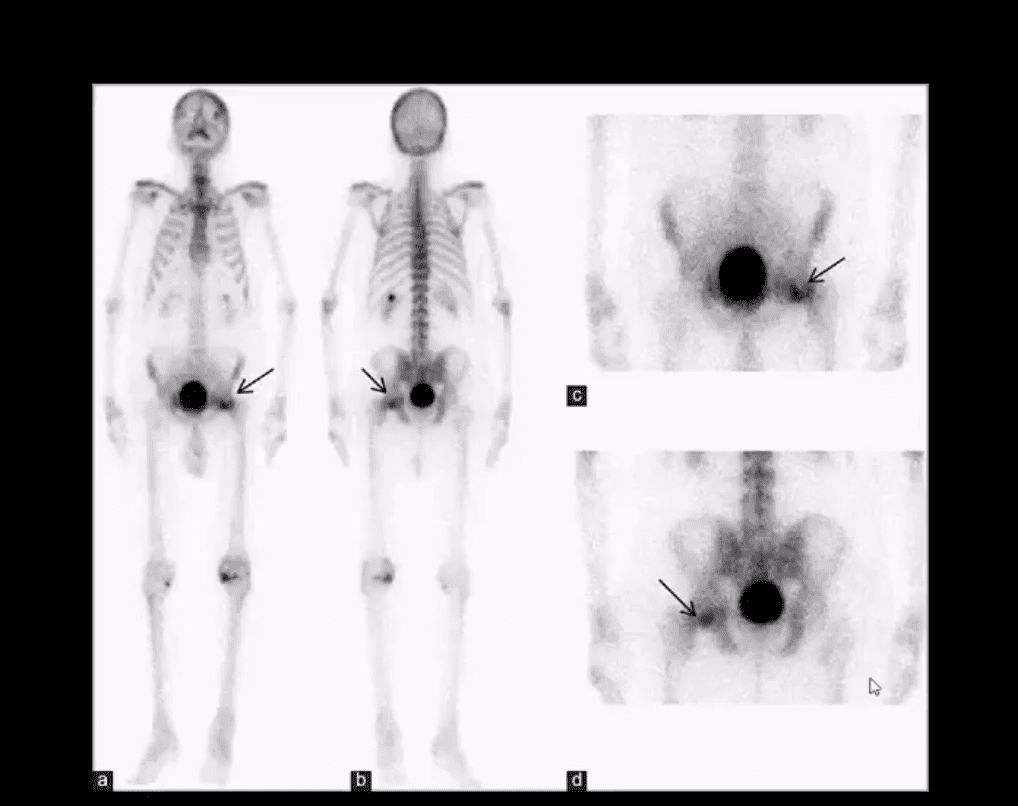
Tc99-MMDP Radionuclide Bone
Bone scan reveals a central area of photopenia (cold spot) d/t necrotic fragment surrounded by increased osteoblastic activity as increased uptake of Tc-99 MDP in the right hip
The patient is a 30-year-old female with breast cancer and chemotherapy treatment who suddenly presented with right hip pain
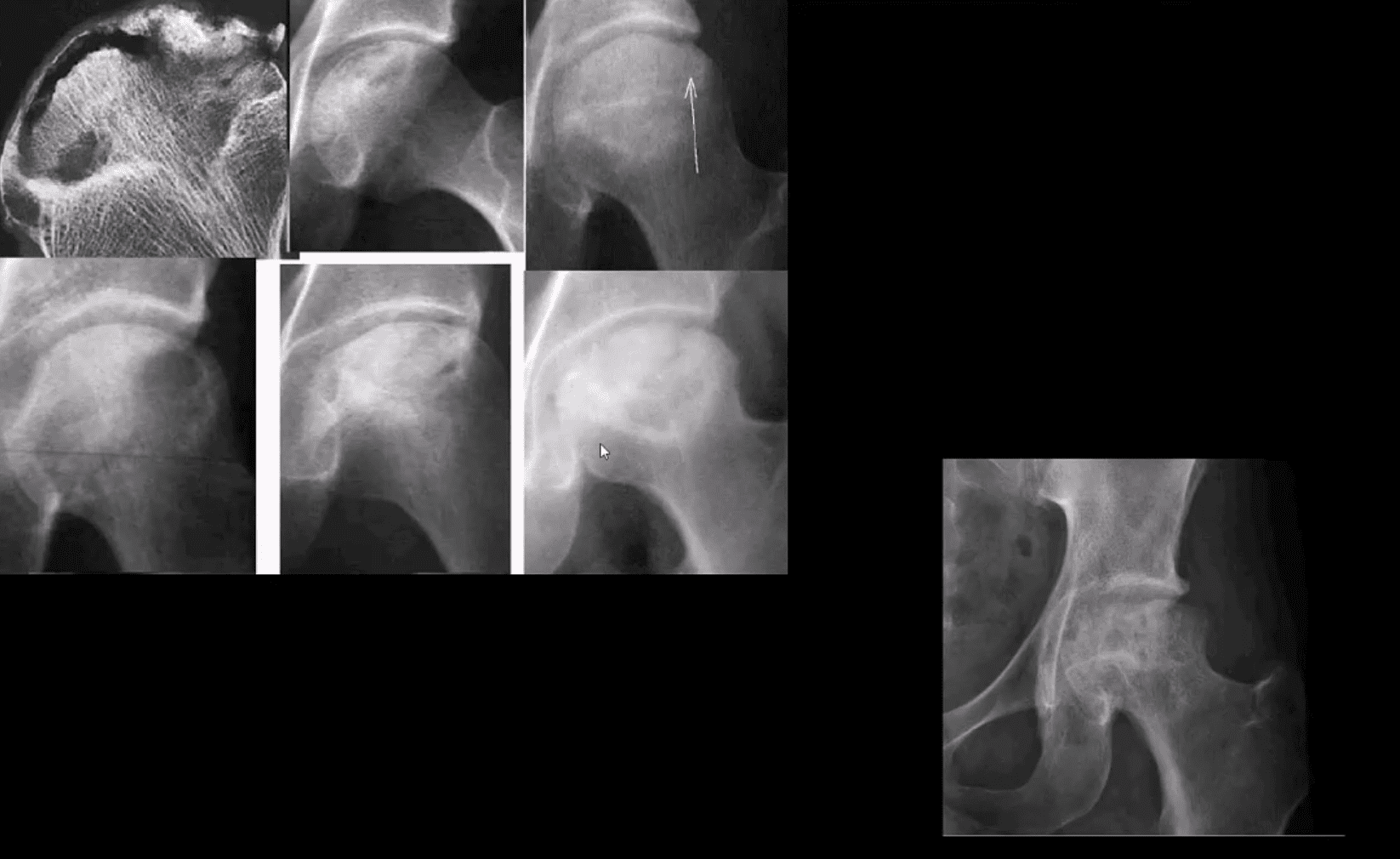
Radiographic Progression of AVN
Later stages present with articular collapse, subarticular cysts, increased patchy sclerosis and complete flattening of the femoral head with resultant severe DJD. Rx: THA
Management
Early imaging Dx with MRI or bone scintigraphy is essential
Referral to the Orthopedic surgeon
Core decompression (above) can be used to revascularize the affected bone during earlier stages but produces mixed results
Delayed changes of AVN: THA as IN severe DJD cases
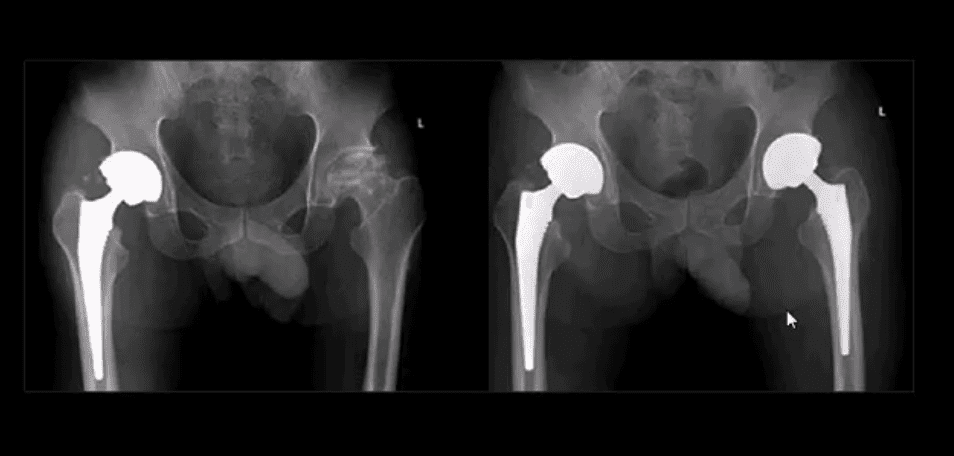
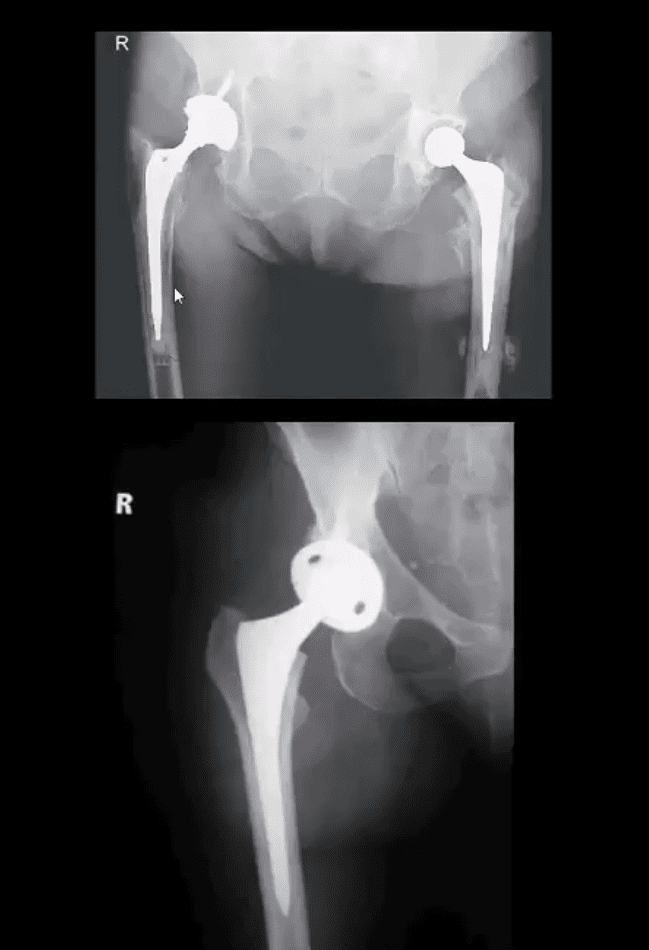
B/L THA
B/L THA in the patient with ischemic osteonecrosis of the right and later left hip
When B/L hip AVN is present, typically consider systemic causes (corticosteroids, diabetes)
Inflammatory Arthritis Affecting the Hip
Consider common systemic inflammatory condition such as RA and AS/EnA
Hip RA may develop in 30% of patients with RA
Key features to DDx inflammatory arthritis vs. DJD is symmetrical/uniform aka concentric joint loss often leading to axial migration and Protrusion Acetabule in advanced cases
Key element between RA vs. AS: the presence of RA bone erosion w/o productive bone changes or enthesitis in AS d/t inflammatory subperiosteal bone proliferation, whiskering/fluffy periostitis (collar-type enthesitis circumferentially affecting head-neck junction)
Dx: Hx, PE, labs: CRP, RH, anti-CCP Ab (RA)
CRP, HLA-B27, RF- (AS)
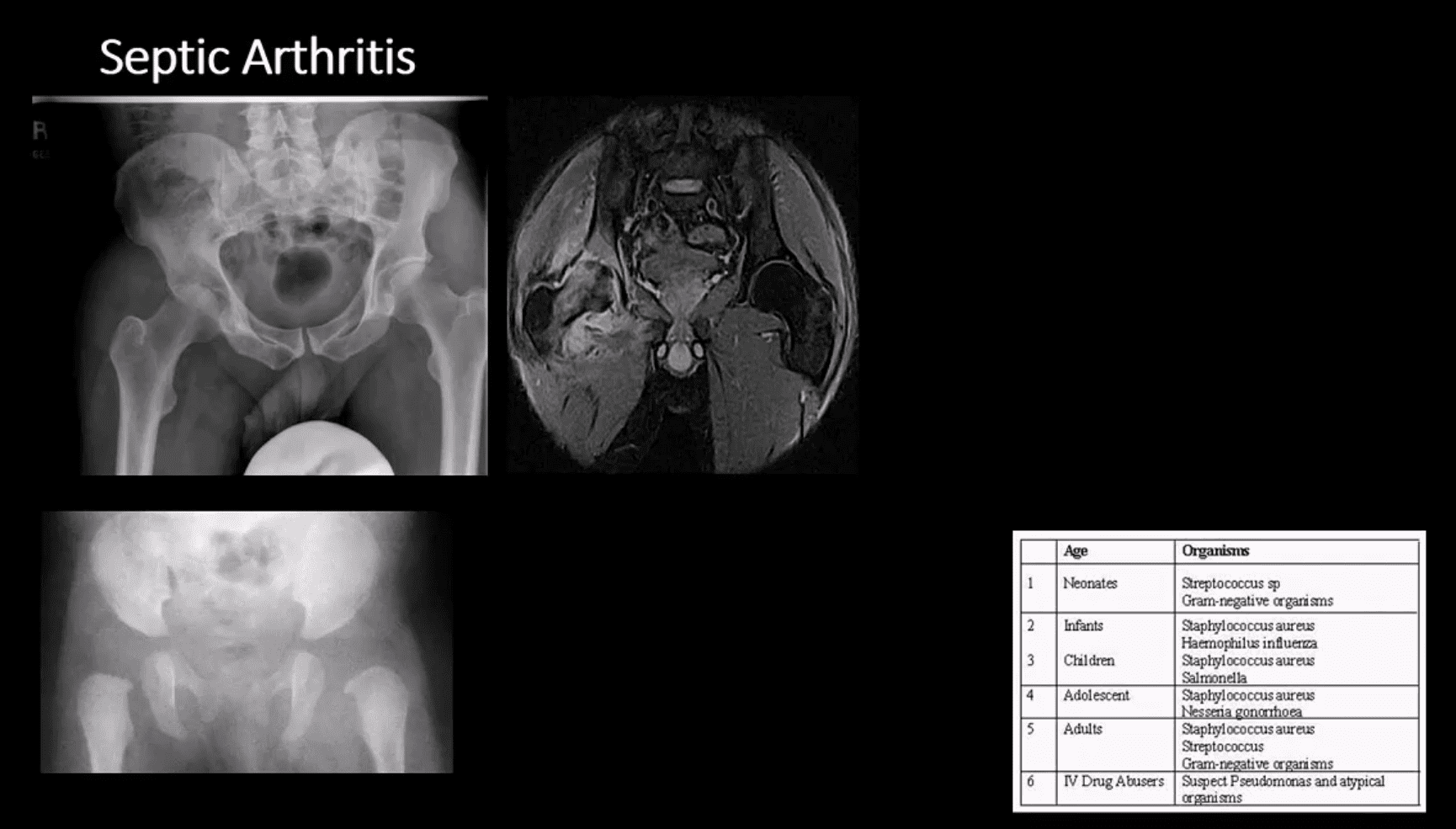
Septic Arthritis
Gonococcal infections, iatrogenic causes, I.V. drug use, and some others
Routes:�hematogenous, adjacent spread, direct inoculation (e.g., iatrogenic)
Clinically: pain and reduced ROM presented as monoarthritis, generalized signs/symptoms. CBC, ESR, CRP changes. ARthrocentesis and culture are crucial
M/C pathogen Staph. Aureus & Neisseria Gonorrhea
1st step: radiography, often unrewarding in the early stage. Later (4-10 days) indistinctness of the white cortical line at the femoral articular epiphysis, loss of joint space, effusion as a widening of the medial joint area (Waldenstrom sign)
MRI – best at early DX: T1, T2, STIR, T1+C may help with early. Early I.V. antibiotics crucial to prevent rapid joint destruction
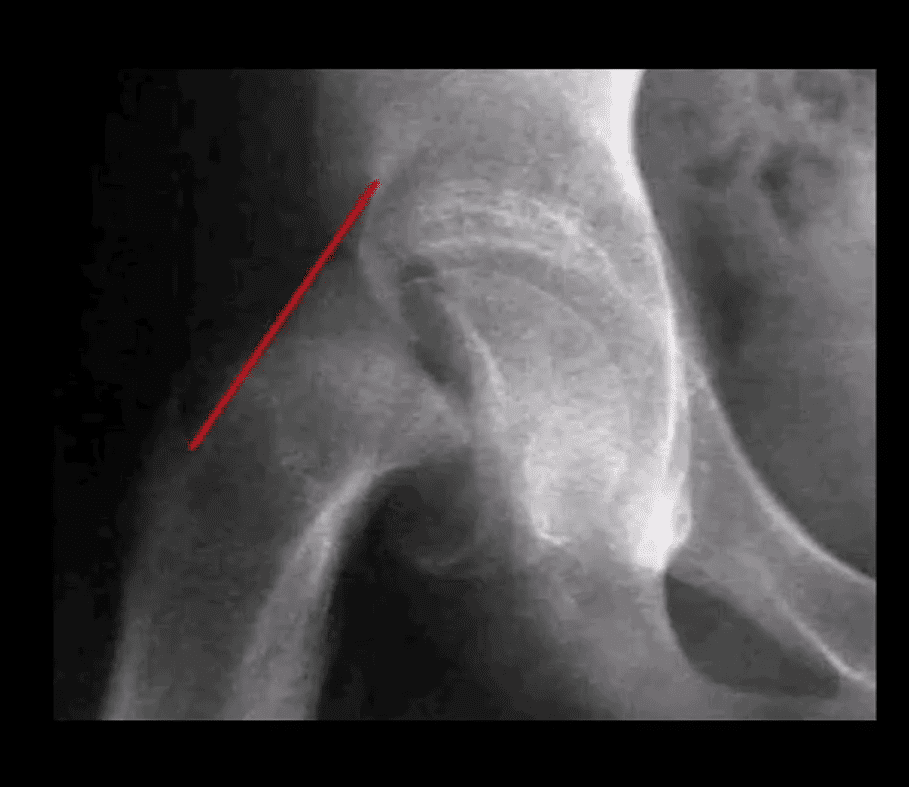
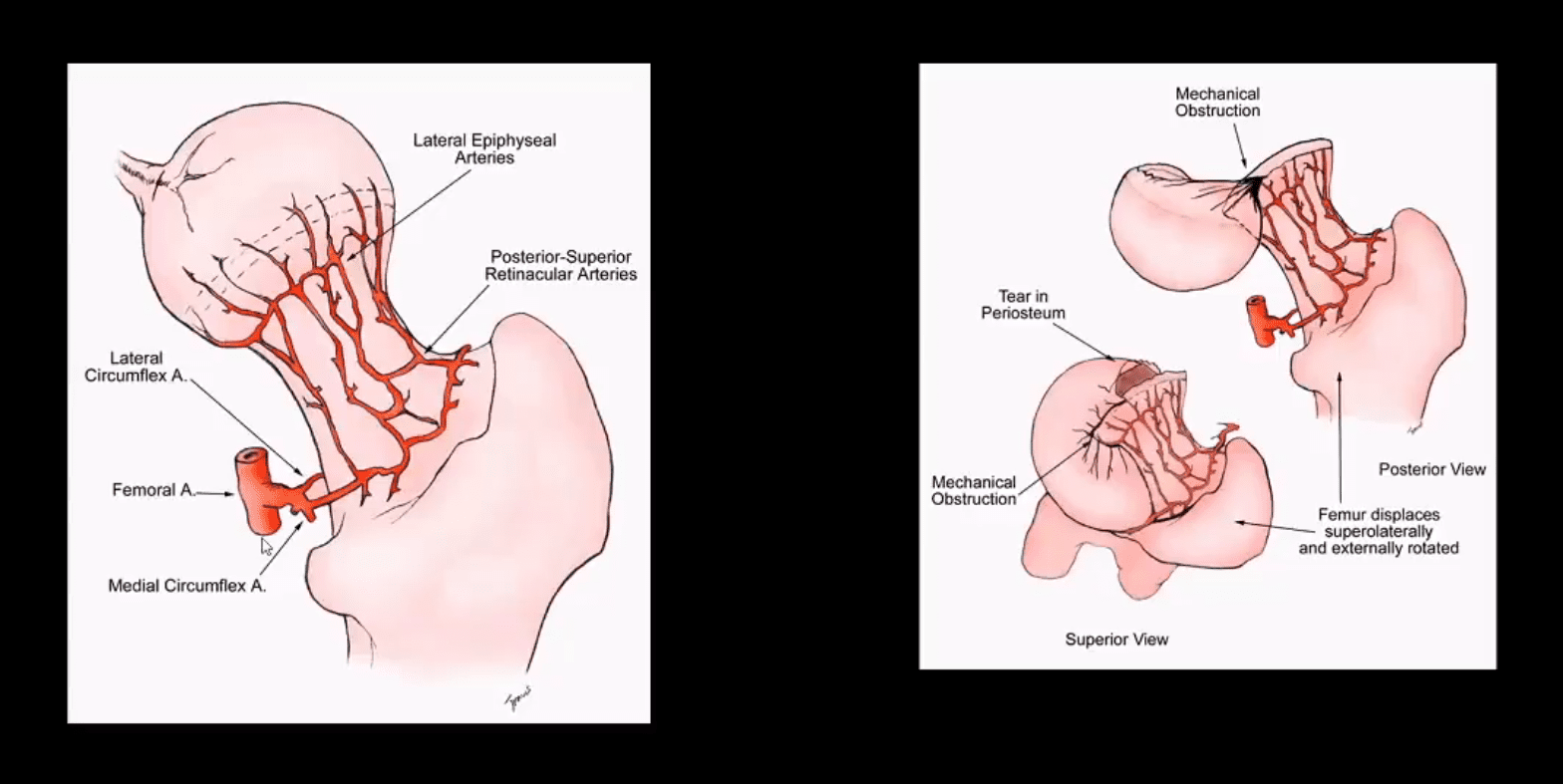
Slipped Capital Femoral Epiphysis (SCFE)
Important to diagnose but easily missed potentially leading to Ischemic Osteonecrosis of the femoral head aka AVN
Presents typically in overweight children (more often boys), age over eight years. Greater incidence in African-American boys
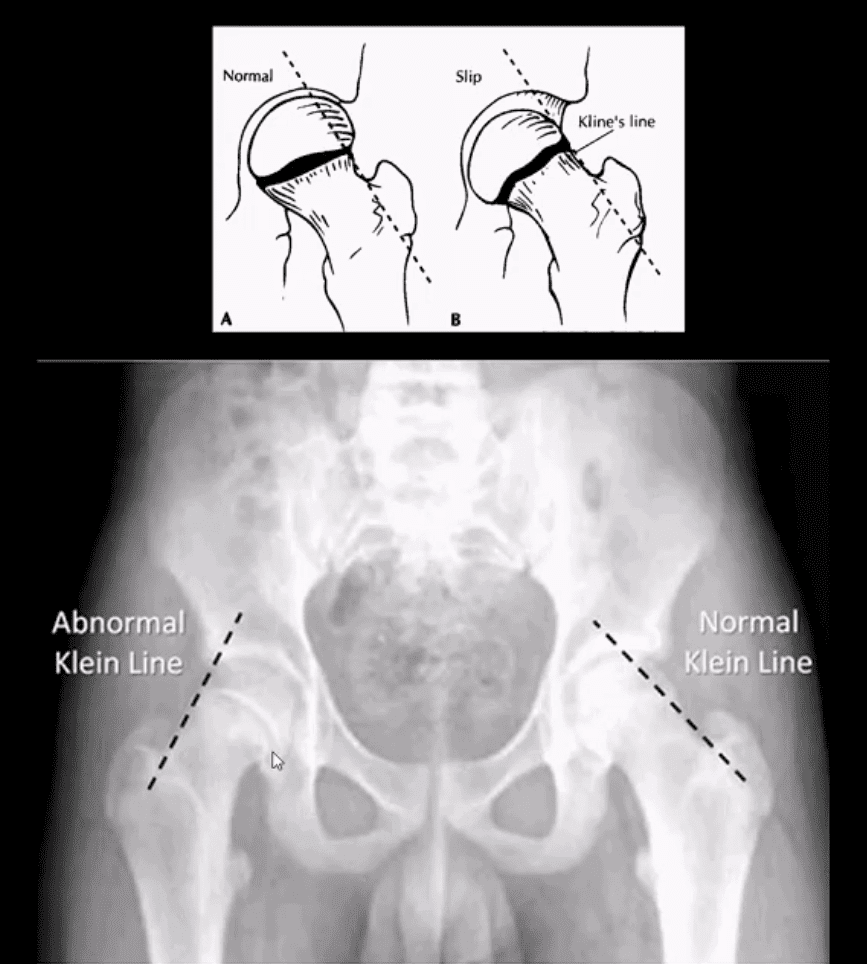
1st step: radiography, especially look for a widened physeal growth plate (so-called pre-slip). Later, slip and disturbed Klein’s line (above image). MRI – best modality for early Dx and early intervention
The frog lateral view often demonstrates the medial slip better than the AP view
Clinically Limping Child or Adolescent
M>F (10-18 years). African-Americans are at greater risk. 20% of cases of SCFE are B/L. Complications: AVN >>DJD
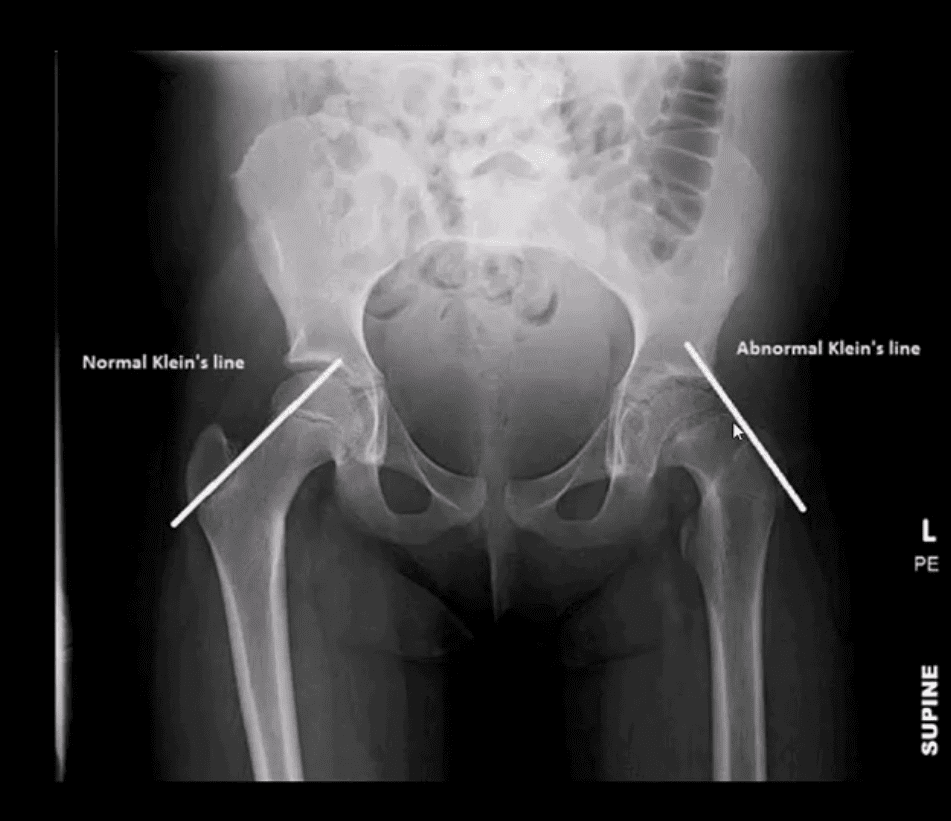
Radiography:�AP pelvis, spot, and frog leg may reveal slippage as Klein line failed to cross through the lateral aspect of the femoral head
Additional features: physis may appear widened
MRI w/o gad, is required for the earliest Dx and prevention of complications (AVN)
Normal and Abnormal Klein Line
Consistent with SCFE. The physis is also widened. Dx: SCFE
Urgent referral to the Pediatric Orthopedic surgeon
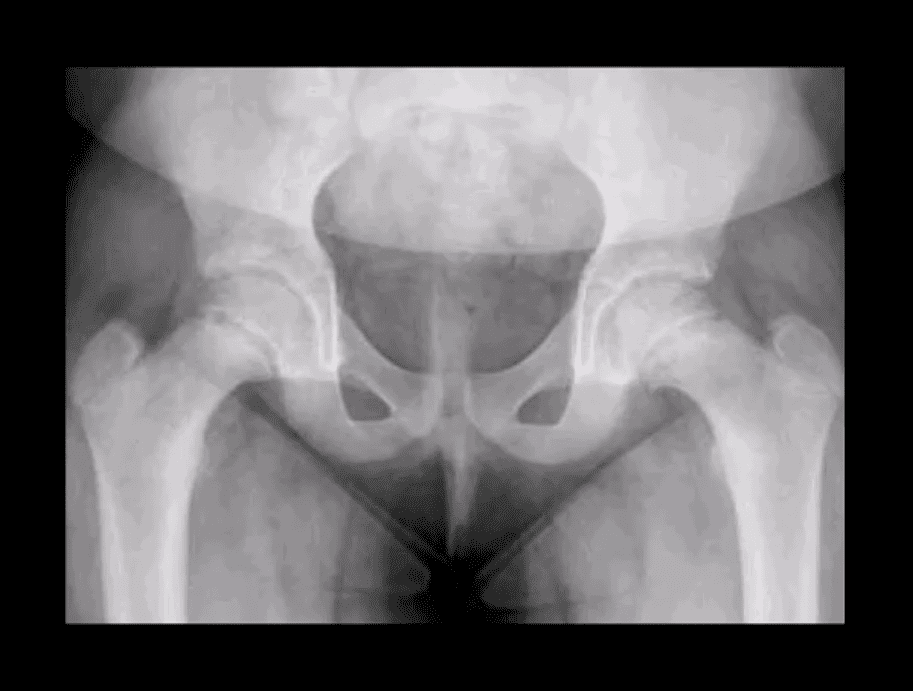
Subtle Changes in Left Hip
Note suspected subtle changes in the left hip that may require MR examination to confirm the Dx
Delay in care may result in major complications
Perthes’ Disease
aka Legg-Calves-Perthes Disease (LCP)
Refers to Osteochondritis of the femoral head with osteonecrosis likely d/t disturbed vascularization of the femoral head
Presents typically in children (more often boys) aged under eight years as atraumatic “limping child.” 15% may have B/L Perthe’s
Imaging steps: 1st step x-radiography, followed by MRI especially in stage 1 (early) w/o x-ray abnormalities
Unspecific signs: joint effusion with Waldenstrome sign+ (>2-mm increase in medial joint space compared to the opposite side). Past approach: Fluoroscopic Arthrography (replaced by MRI)
Pathologic-Radiologic Correlation: in well-established cases, the femoral head characteristically becomes sclerotic, flattened and fragmented due to avascular necrosis (AVN). Later on, an occasional Coxa Magna changes may develop (>10% femoral head enlargement)
Management: symptoms control, bracing. Boys at younger ate show better prognosis d/t more immaturity and better chances of bone/cartilage repair mechanisms. In advanced cases, operative care: osteotomy, hip arthroplasty in adulthood if advanced DJD develops
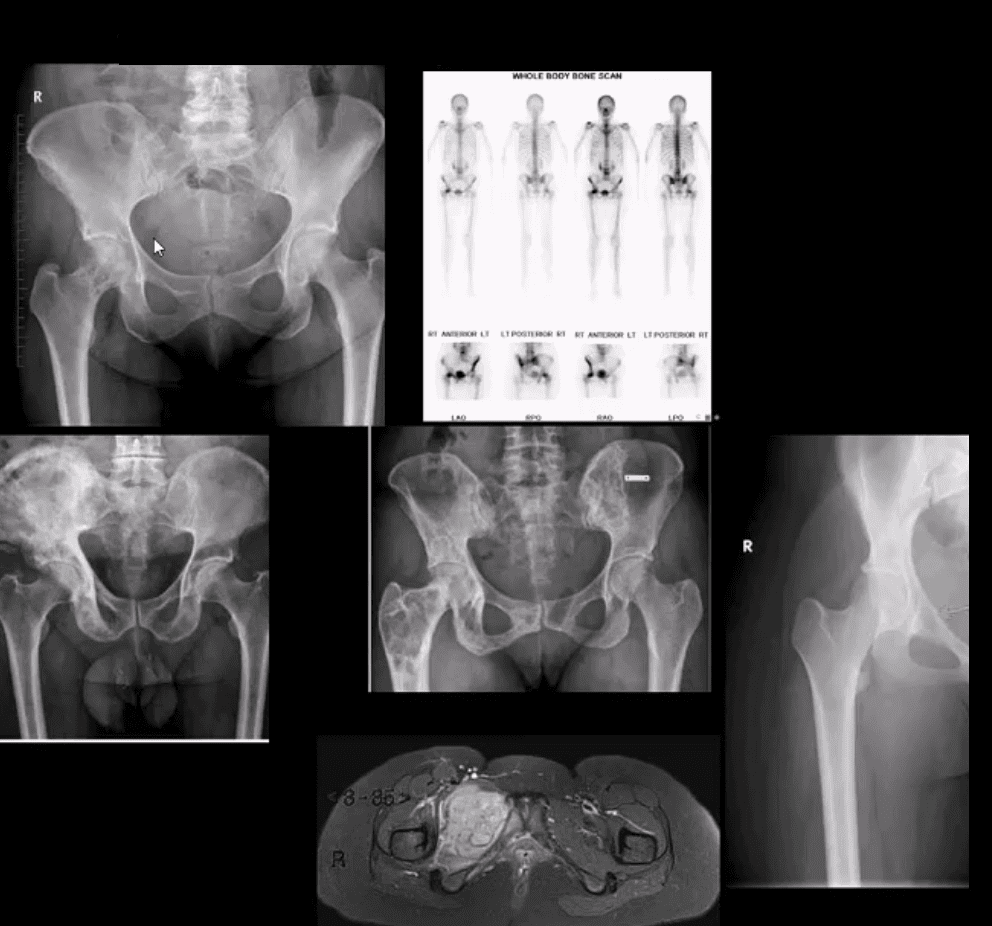
Common Neoplasms & Other Conditions Affecting Hip/Pelvis
M/C hip & pelvis neoplasms in adults: bone metastasis ( above far left), 2nd m/c Multiple Myeloma (M/C primary bone malignancy in adults). Tips: remember Red Marrow distribution. Less frequent: Chondrosarcoma
Paget’s disease of bone (above-bottom left image) is m/c detected in the pelvis and Femurs
Children and young adults ‘limping child’ benign neoplasms: Fibrous Dysplasia (above middle image), Solitary Bone Cyst (21%), Osteoid Osteoma, Chondroblastoma. Malignant pediatric neoplasms: m/c Ewing Sarcoma (above middle right and bottom images) vs. Osteosarcoma. >2y.o-consider Neuroblastoma
Imaging: 1st step: radiography followed by MRI are most appropriate.
If Mets are suspected: Tc99 bone scintigraphy is most sensitive
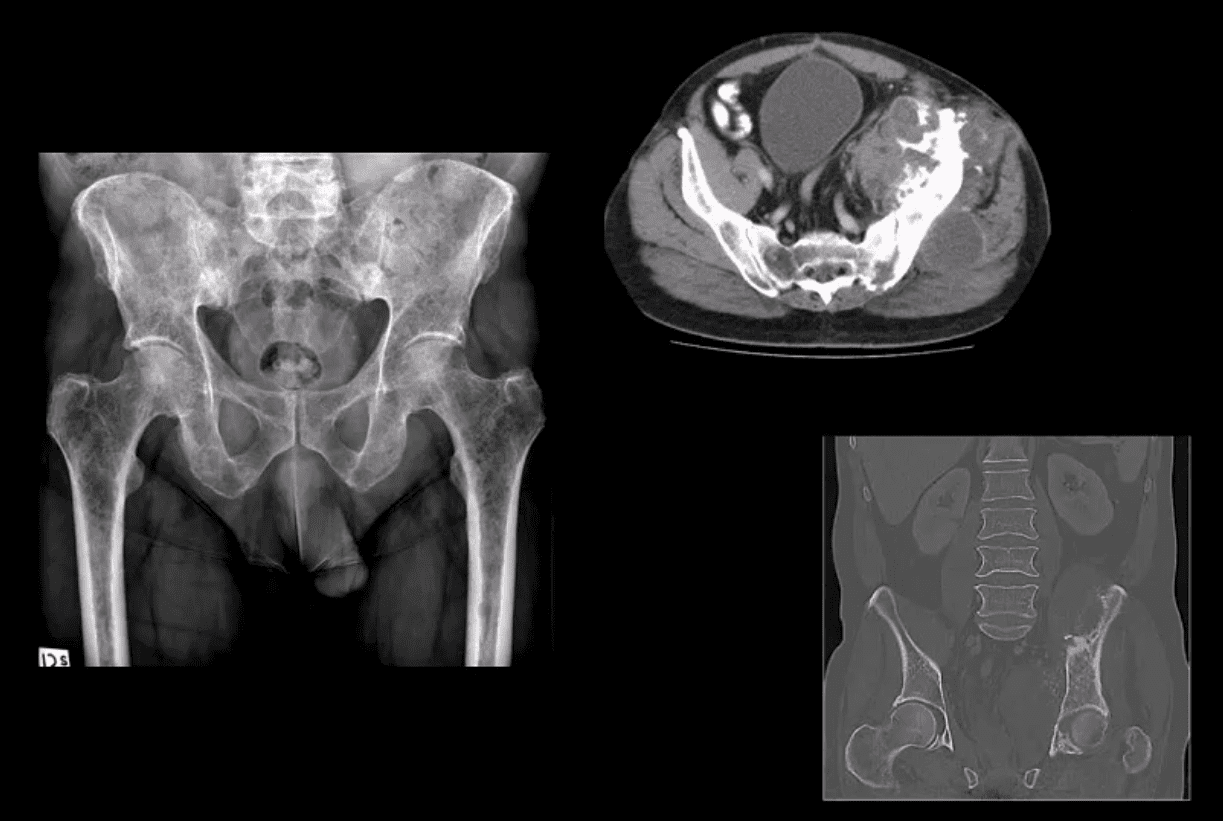
Multiple Myeloma
Multiple Myeloma in a 75-y.o male (AP pelvis view)
Chondrosarcoma in a 60-y.o male (axial and coronal reconstructed CT+C slices in the bone window)
Cancer which develops in specific organs of the human body, including the lungs, breast, or prostate, among others, can sometimes spread into the bone, causing what is known as�metastatic bone disease, or MBD. Approximately more than 1.2 million new cancer cases are diagnosed every year, where about 50 percent can spread,�or metastasize, to the bones.
Through medical advancements, patients diagnosed with several different types of cancers, especially lung, breast, and prostate cancer, can live longer. However, primary cancers in more patients go through bone metastases, where they disperse�to the bone. Meanwhile, other types of cancers do not disperse so easily to the�bone. The most common cancers which develop in the organs and spread to the bones include:
Breast
Lung
Thyroid
Kidney
Prostate
Metastatic bone disease,�or MBD, can damage�and weaken the affected bone, causing pain along the site of spread.�Moreover, patients with MBD are at higher risk of suffering fractures or broken bones. The painful symptoms associated with MBD can make it challenging for the patient to engage in regular physical activities. The main concern of patients with metastatic bone disease is the loss in quality of life.
The extent of the effects of metastatic bone disease on a patient can change and is associated with how cancer has spread, which bones are affected, and how severe the bone harm is. Furthermore, there is a range of treatment choices available to treat MBD. Treatment help patients deal with pain to maintain activity levels and preserve their independence.
Metastatic Bone Disease Explained
The bones are the most common site of spread for cancers which begin in the organs, subsequent to the lung and the liver. Because many patients experience no painful symptoms of metastases to the liver and the lungs, these are often not discovered until the disease is in an advanced stage. In contrast, bone metastases are generally painful when they develop. Cancer most commonly spreads to these sites in the human skeleton:
Skull
Spine
Ribs
Upper arm
Pelvis
Long bones of the leg
Bone Damage
A tumor can completely destroy the bone at the site of spread, a process referred to as osteolytic bone destruction. Damage or weakened bones are most common in cancers which have spread from the lung, thyroid, kidney, and colon. New bone,�called osteoblastic, may also form due to the spread of cancer, more often seen in cancers from the stomach, bladder, and prostate.
Breast cancer often behaves in a combined osteolytic and osteoblastic method. Since the cancer cells secrete factors that interact with all the cells in the human skeleton, causing bone destruction, new bone formation, or both, osteolytic and osteoblastic metastatic bone disease happens. Also, breast cancer may commonly cause MBD in the hip and/or pelvis.
As a result of bone damage and weakness, patients with�metastatic bone disease are prone to fractures. Broken bones caused by MBD are termed “pathological fractures”.�Sometimes, the bone may be so weak that a fracture is imminent, termed “impending pathologic fractures”. Bedrest for lengthy intervals due to broken bones may result in chemical imbalances in the bloodstream, such as raised calcium levels, known as hypercalcemia. Patients with cancer that has spread to the spine can develop nerve damage which can result in paralysis or loss of using their arms and/or legs.
MBD Symptoms
A cancer patient who experiences any pain, especially in the back, arms, and legs should notify their doctor immediately. Pain which manifests without engaging in physical activities is especially concerning. The most common symptoms of�metastatic bone disease include:
Pain: MBD’s most prevalent symptom is pain. Patients may experience pain along their hip and/or pelvis, upper and lower extremities, and spine because the tumor may have damaged or weakened the bone.
Fractures: Broken bones, or fractures, can range from mild to severe and are generally a clear indication of the presence of MBD.
Anemia: The most common sites of spread, skull, spine, ribs, upper and lower extremities, and hip and/or pelvis, correspond to regions of bone marrow which produce high levels of red blood cells, responsible for carrying oxygen to cells. Anemia, or decreased red blood cell production, is a frequent blood abnormality with MBD.
MBD Diagnosis
Before following through with treatment for metastatic bone disease, it’s essential for the healthcare professional to understand the patient’s symptoms as well as their overall health and wellness. The doctor will ask for the patient’s medical history. After the medical history, the healthcare professional will perform a physical examination on the patient. The doctor may also utilize imaging diagnostics to help with the patient’s diagnosis.
Imaging Diagnostics
X-rays:�After the initial diagnosis, they may order x-rays. Because pain may often originate from other regions of the body, the healthcare professional will also order x-rays beyond the regions where the patient is experiencing discomfort. X-rays may tell an oncologist a great deal of information regarding how much bone is affected.
Other imaging tests: The doctor may also order a bone scan. This test can determine if other bones are involved with metastatic bone disease. In select situations, a computerized tomography, or�CT, scan and magnetic resonance imaging, or MRI, may be ordered, especially in scenarios where the spine or hip and/or pelvis are involved.
A variety of cancers can commonly cause metastatic bone disease, or MBD, throughout different regions of the human skeleton. Bone metastases can cause painful symptoms, ultimately affecting an individual’s quality of life. Research studies have demonstrated that metastatic bone disease in the hip and/or pelvis is a prevalent health issue associated with breast cancer. Treatment may vary on the progression of the problem.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
Metastatic Bone Disease Treatment
Advances in surgical techniques, as well as radiation and medical treatment approaches, have significantly improved the quality of life of patients suffering from cancer that has spread to the bone from the site of origin. Treatment options for MBD are based upon how far the cancer has spread, which bones are affected, and how the bone was damaged or weakened.
In many cases of metastatic bone disease, cancer has progressed to multiple bony sites. As a result, treatment is concentrated on managing the symptoms of pain and bone weakness as it is not intended to be curative. The most common treatment option for MBD includes drugs and/or medications, and radiation to control pain and prevent additional spread of metastatic bone disease, and surgery to stabilize weak and broken bones.
Patients with metastatic bone disease require a team approach. A medical oncologist works closely with a radiation oncologist, and an orthopaedic surgeon. Diagnosis is essential in order to follow through with the best treatment approach. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain is the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
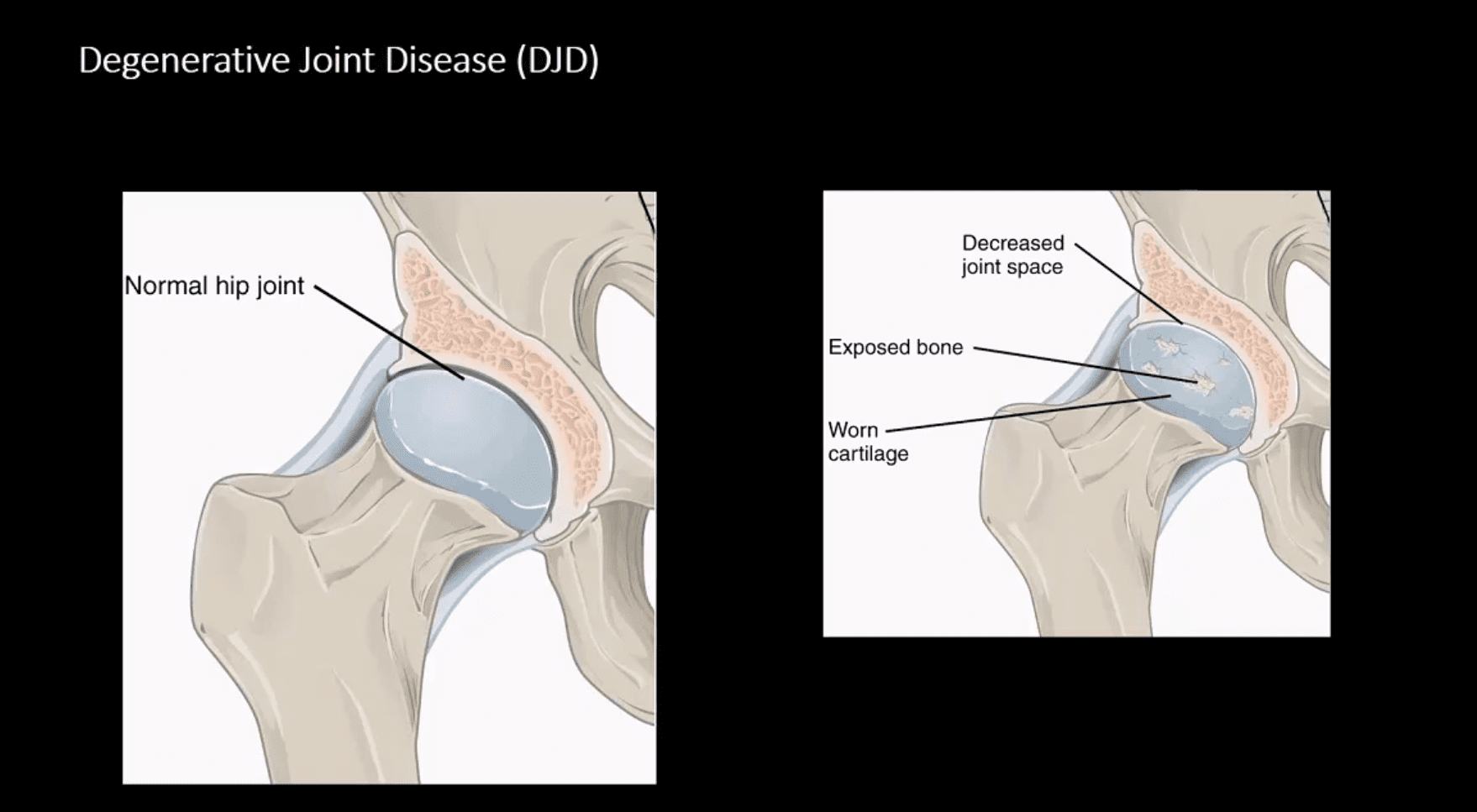
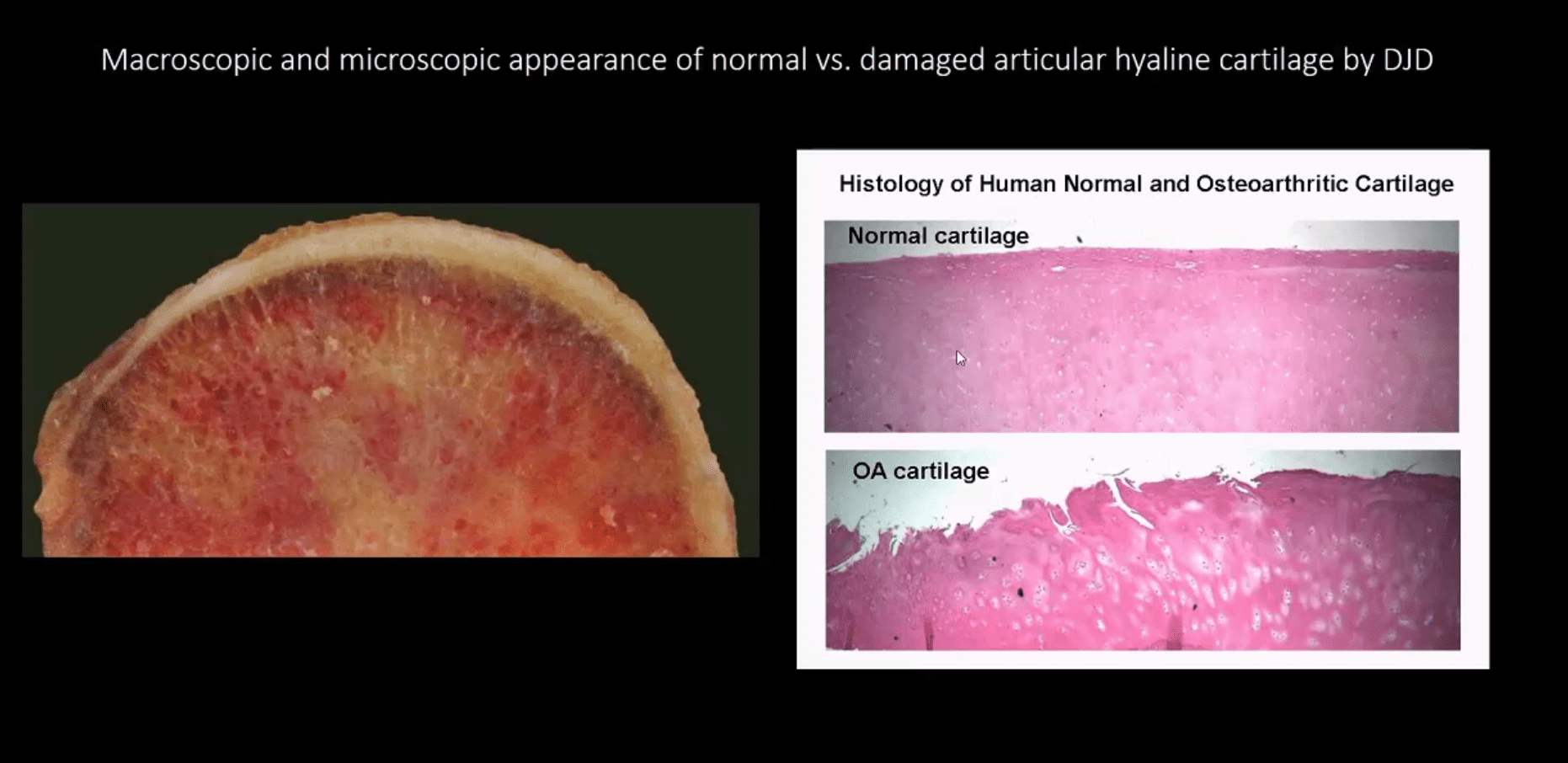
Macroscopic & Microscopic Appearance of Normal vs. Damaged Articular Hyaline Cartilage by DJD
Hip Osteoarthritis (OA) aka Osteoarthrosis
Symptomatic and potentially disabling DJD
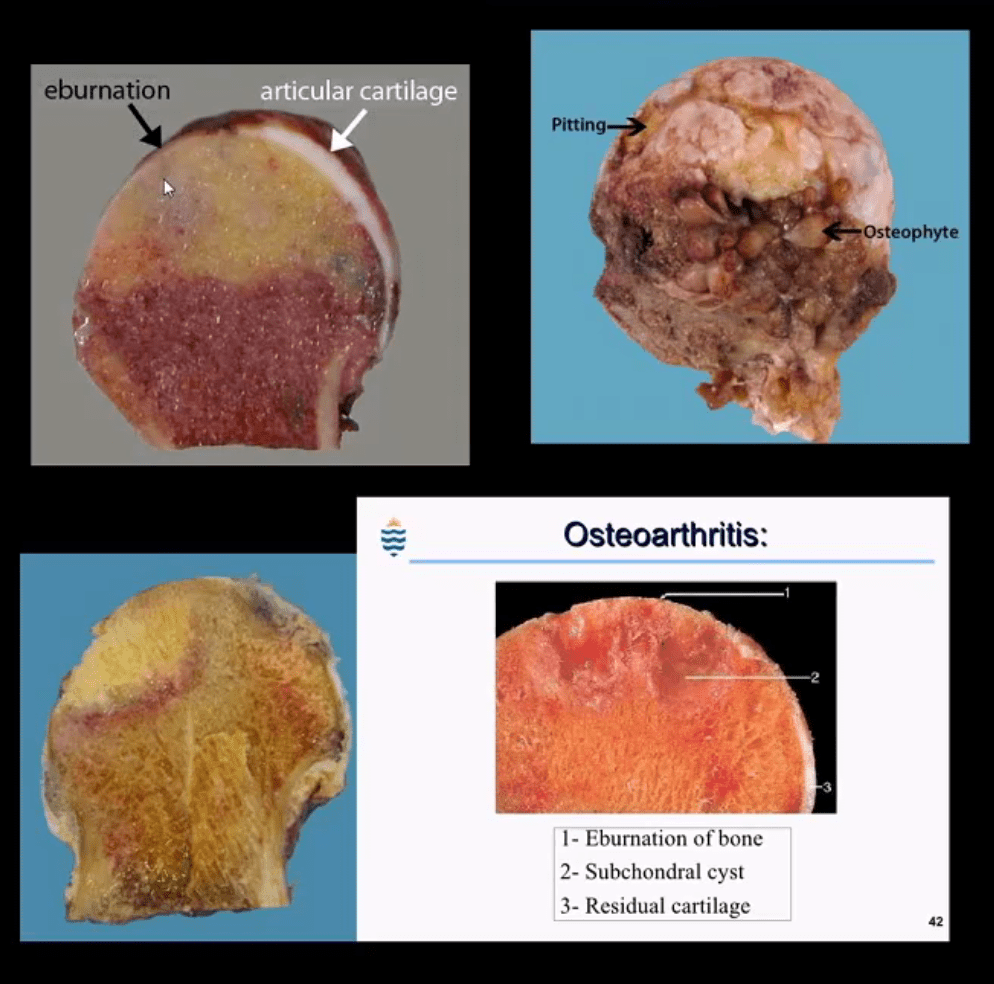
Progressive damage and loss of the articular cartilage causing denudation and eburnation of articular bone
Cystic changes, osteophytes, and gradual joint destruction
Develops d/t repeated joint loading and microtrauma
Obesity, metabolic/genetic factors
Secondary Causes: trauma, FAI syndrome, osteonecrosis, pyrophosphate crystal deposition, previous inflammatory arthritis, Slipped Capital Femoral Epiphysis, Leg-Calves-Perthes disease in children, etc.
Hip OA, 2nd m/c after knee OA. Women>men
88-100 symptomatic cases per 100000
Radiography is the Modality of Choice for the Dx and Grading of DJD
Special imaging is not required unless other complicating factors exist
The acetabular-femoral joint is divided into superior, axial and medial compartments/spaces
Normal joint space at the superior compartment should be 3-4-mm on the AP hip/pelvis view
Understanding the pattern of hip joint narrowing/migration helps with the DDx of DJD vs. Inflammatory arthritis
In DJD, m/c hip narrowing is superior-lateral (non-uniform) vs. inflammatory axial (uniform)
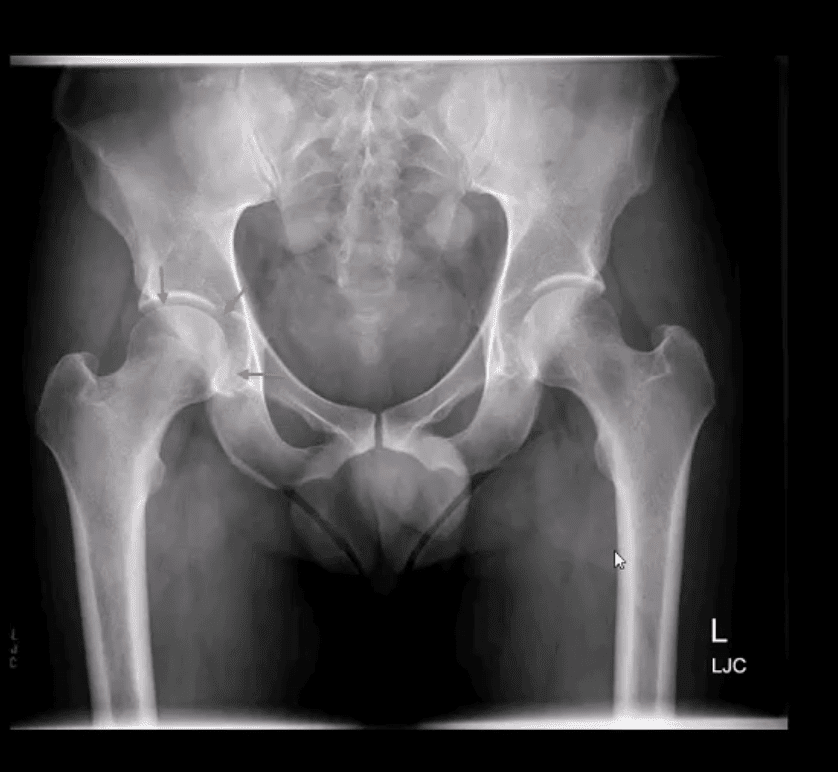
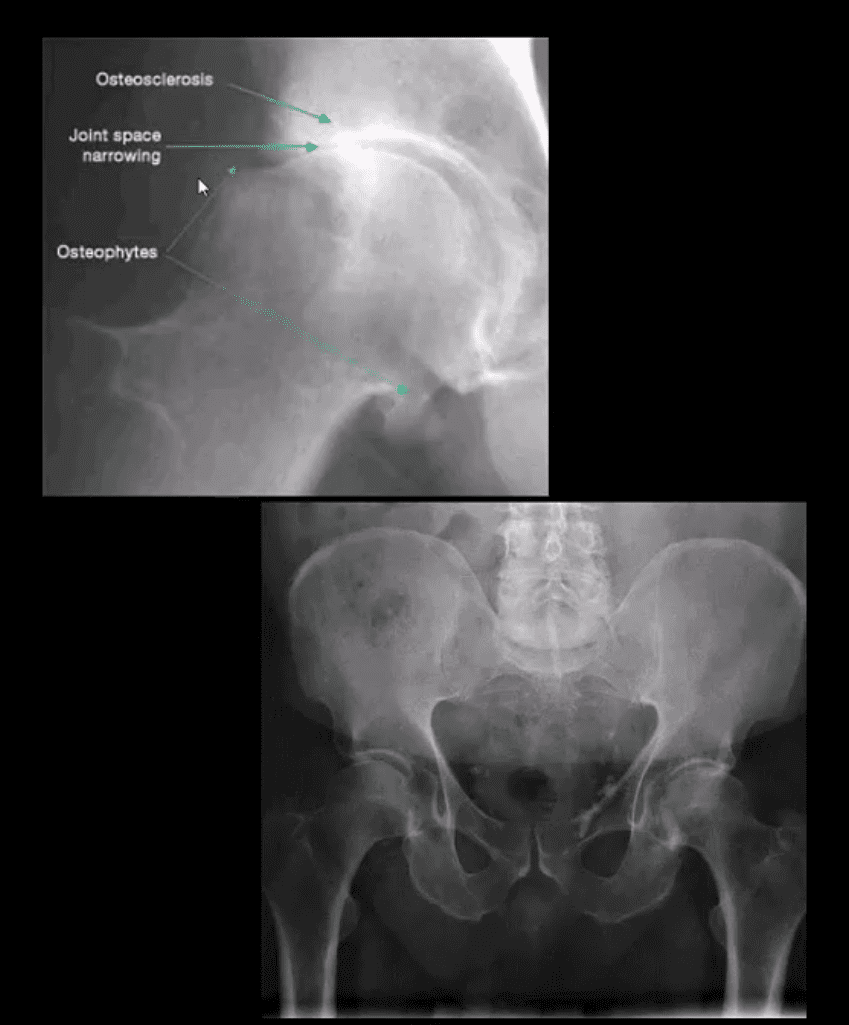
AP Hip Radiograph Demonstrates DJD
With a non-uniform loss of joint space (superior migration), large subcortical cysts and subchondral sclerosis
Radiographic features:
Like with any DJD changes: radiography will reveal L.O.S.S.
L: loss of joint space (non-uniform or asymmetrical)
O: osteophytes aka bony proliferation/spurs
S: Subchondral sclerosis/thickening
S: Subcortical aka subchondral cysts “geodes.”
Hip migration is m/c superior resulting in a “tilt deformity.”
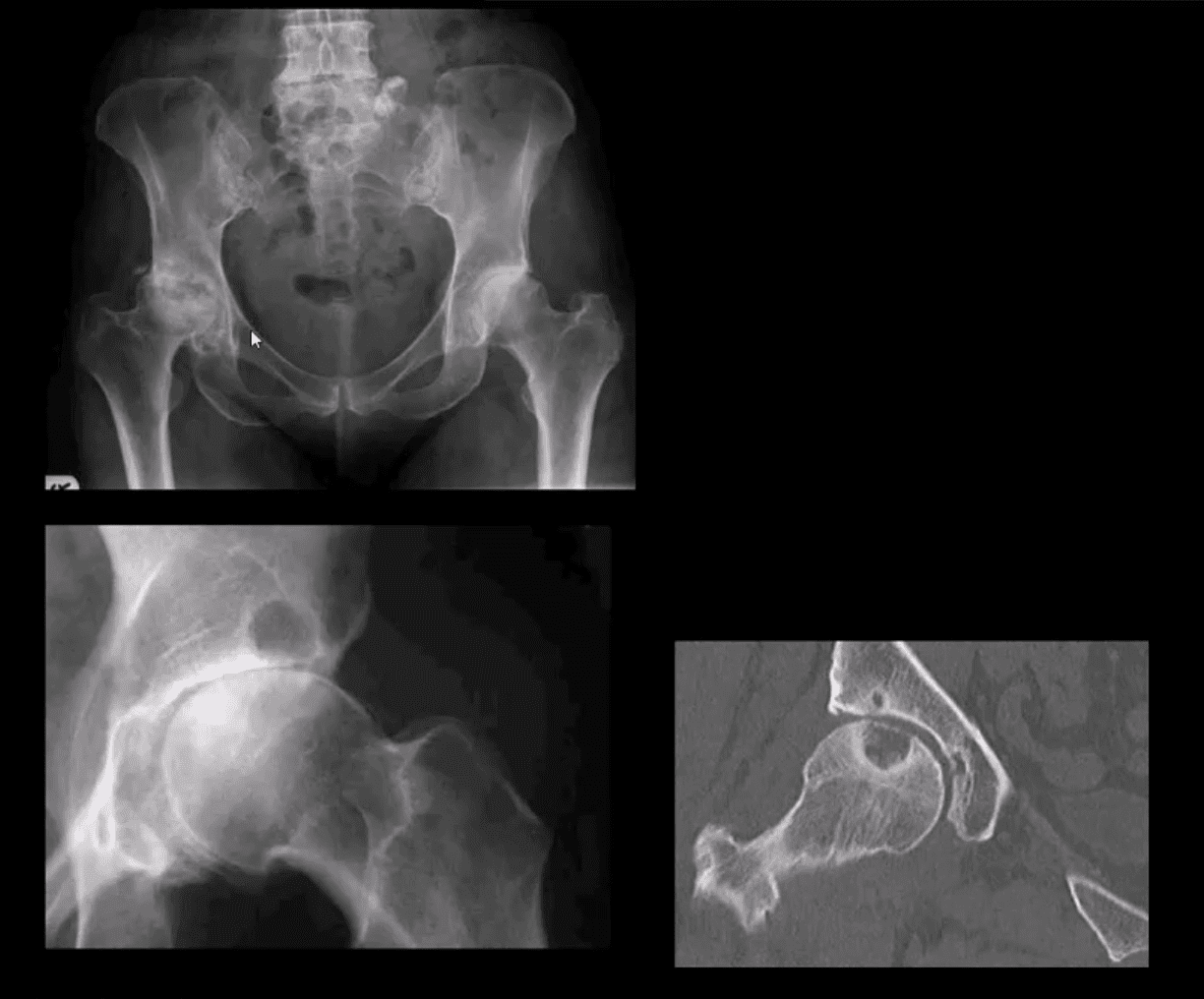
Radiographic Presentation of Hip OA May Vary Depending On Severity
Mild OA: mild reduction of joint space often w/o marked osteophytes and cystic changes
During further changes, collar osteophytes may affect femoral head-neck junction with more significant joint space loss and subchondral bone sclerosis (eburnation)
Cyst formation will often occur along the acetabular and femoral head subarticular/subchondral bone “geodes” and usually filled with joint fluid and some intra-articular gas
Subchondral cysts may occasionally be very large and DDx from neoplasms or infection or other pathology
Coronal Reconstructed CT Slices in Bone Window
Note moderate joint narrowing that appears non-uniform
Sub-chondral cysts formation (geodes) are noted along the acetabular and femoral head subchondral bone
Other features include collar osteophytes along head-neck junction
Dx: DJD of moderate intensity
Referral to the Orthopedic surgeon will be helpful for this patient
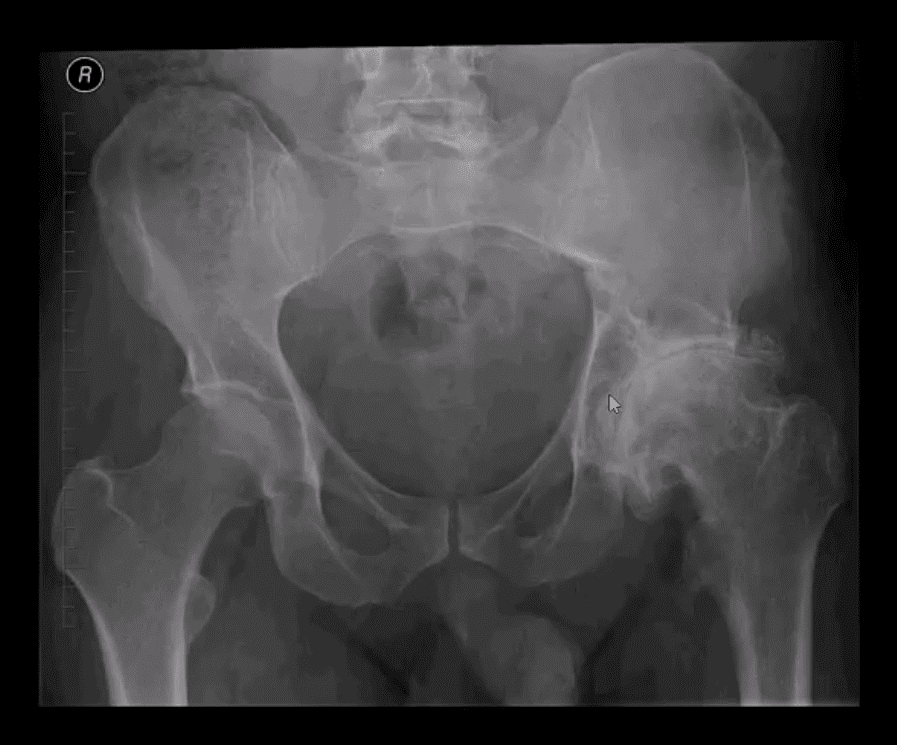
AP Pelvis (below the first image), AP Hip Spot (below the second image) CT Coronal Slice
Note multiple subchondral cysts, severe non-uniform joint narrowing (superior-lateral) and subchondral sclerosis with osteophytes
Advanced hip arthrosis
Severe DJD, Left Hip
When reading radiological reports pay particular attention to the grading of hip OA
Most severe (advanced) OA cases require total hip arthroplasty (THA)
Refer your patients to the Orthopedic surgeon for a consultation
Most mild cases are a good candidate for conservative care
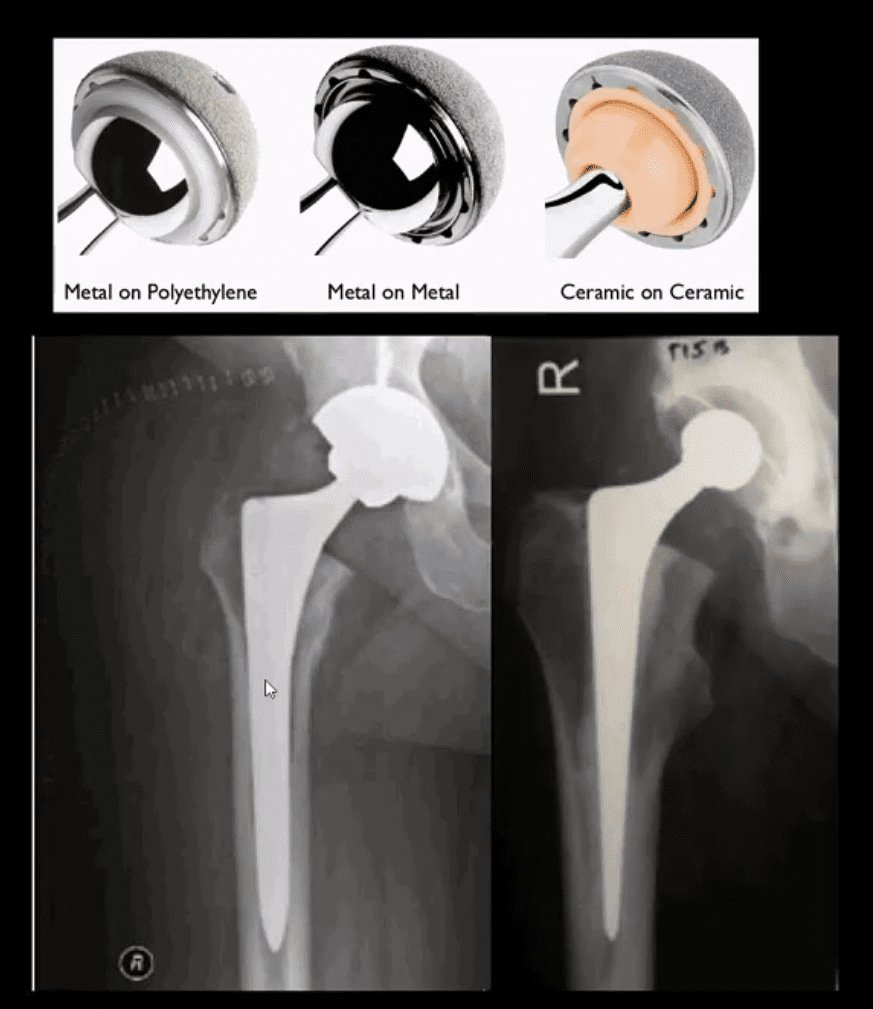
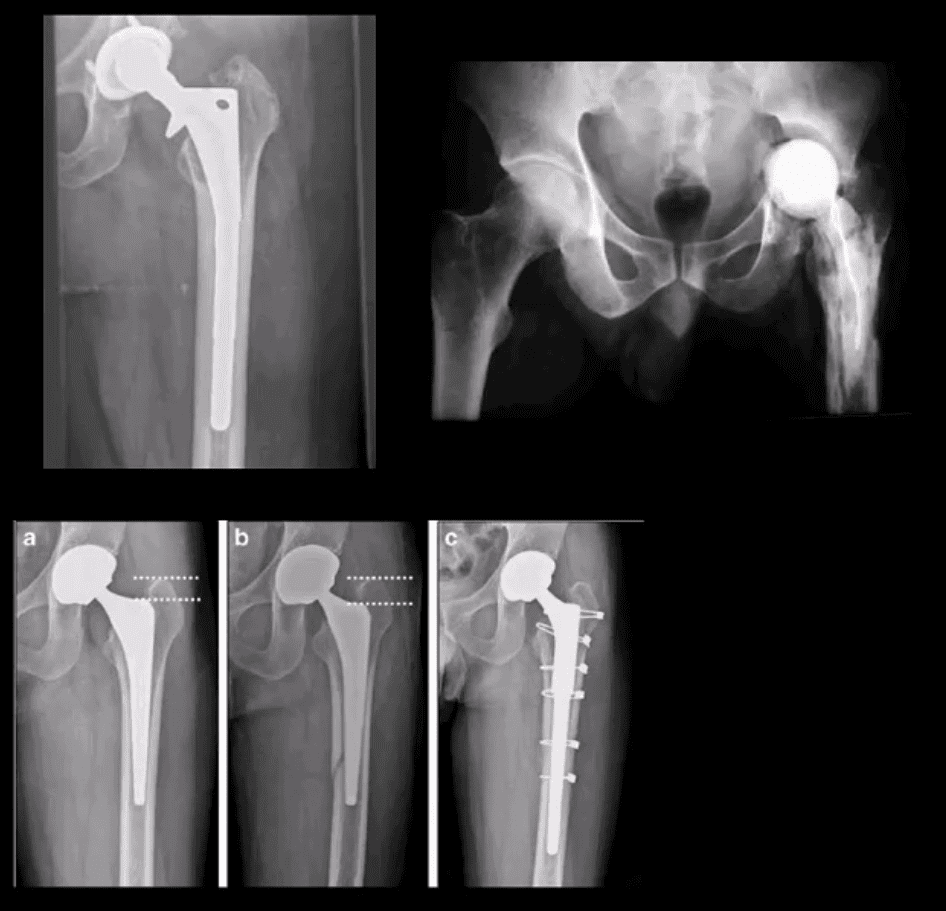
Hip Arthroplasty aka Hip Replacement
Can be total or hemiarthroplasty
THA can be metal on metal, metal on polyethylene and ceramic on ceramic
A hybrid acetabular component with polyethylene and metal backing is also used (above right image)
THA can be cemented (above right image) and non-cemented (above-left image)
Non-cemented arthroplasty is used on younger patients utilizing porous metallic parts allowing good fusion and bone ingrowth into the prosthesis
Failed THA May Develop
Most develop within the first year and require revision
Femoral stem may fracture (above left)
Postsurgical infection (above right)
Fracture adjacent to the prosthesis (stress riser)
Particle disease
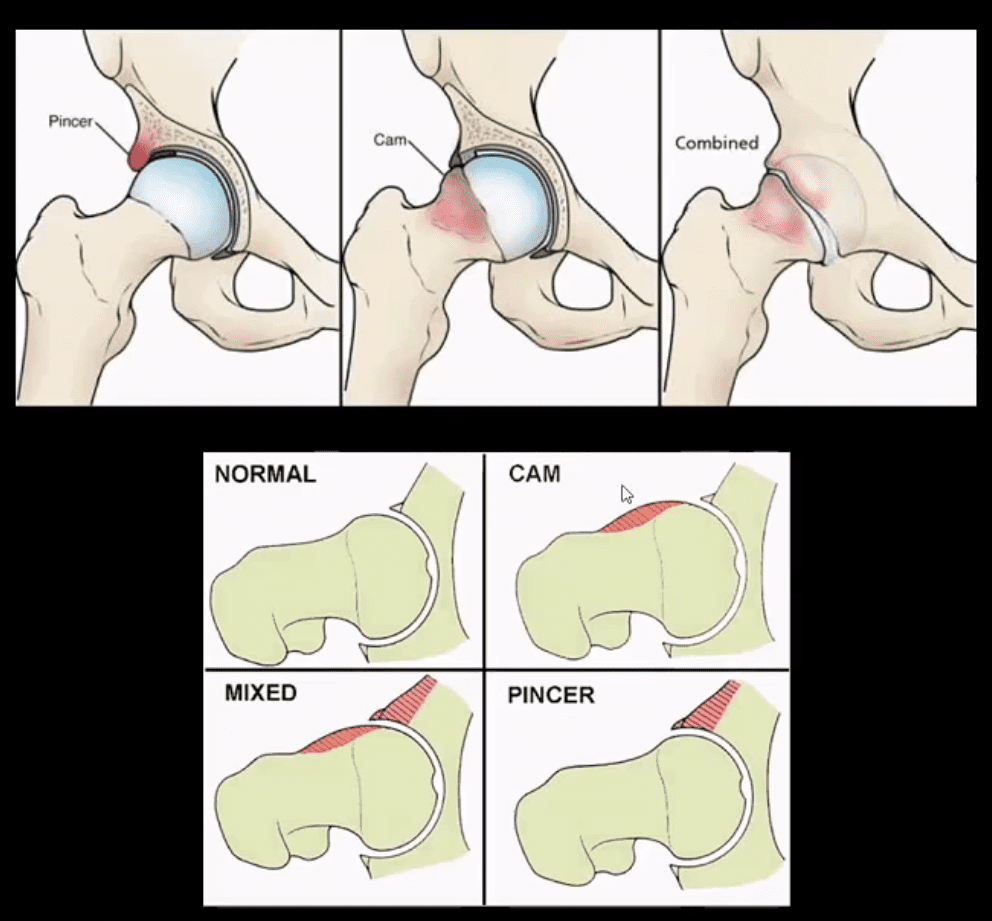
Femoroacetabular Impingement Syndrome
(FAI): abnormality of normal morphology of the hip leading to eventual� cartilage damage and premature DJD
Clinically:�hip/groin pain aggravated by sitting (e.g., hip flexed & externally rotated). Activity related pain on axial loading esp. with hip flexion (e.g., walking uphill)
Pincer-type�acetabulum: > in middle age women potentially� many causes
CAM-type deformity:�> in men in 20-50 m/c 30s
Mixed type (pincer-CAM) is most frequent
Up until the 90s, FAI was not well-recognized
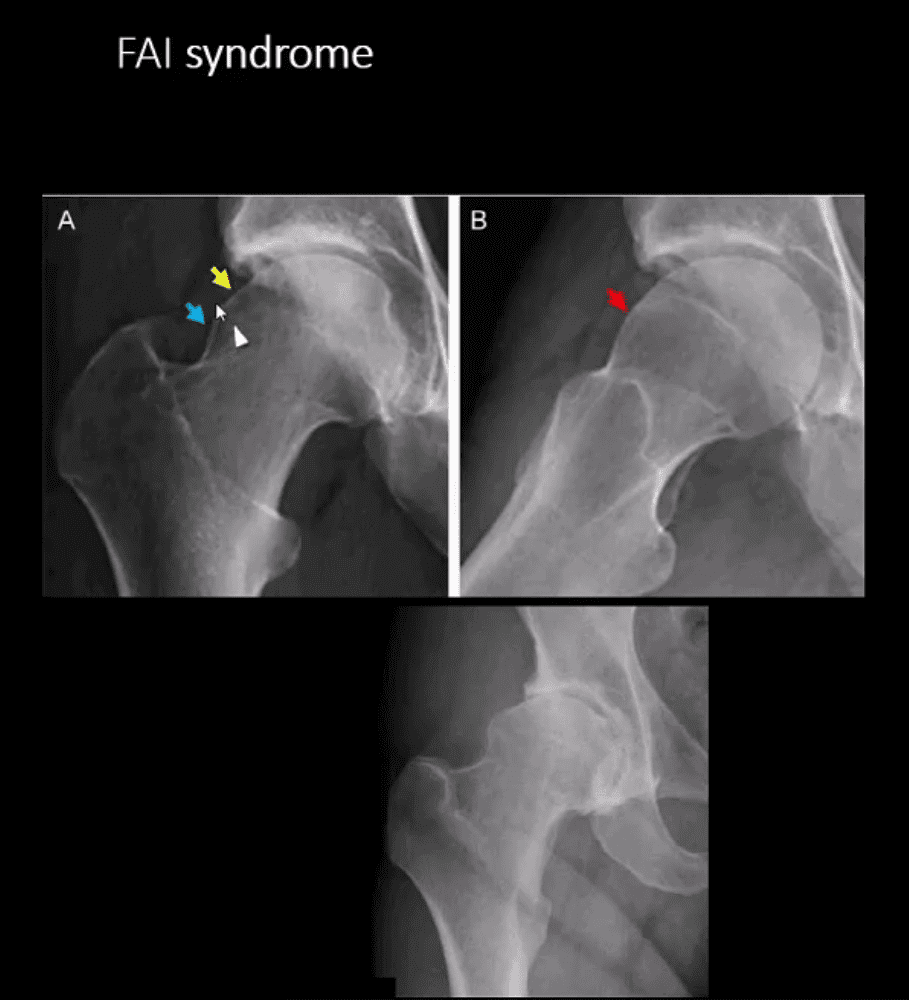
FAI Syndrome
CAM-type FAI syndrome
Radiography can be a reliable Dx tool
X-radiography findings:�osseous bump on the lateral aspect of femoral head-neck junction. Pistol-grip deformity. Loss of normal head sphericity. Associated features: os acetabule, synovial herniation pit (Pit’s pit). Evidence of DJD in advanced cases
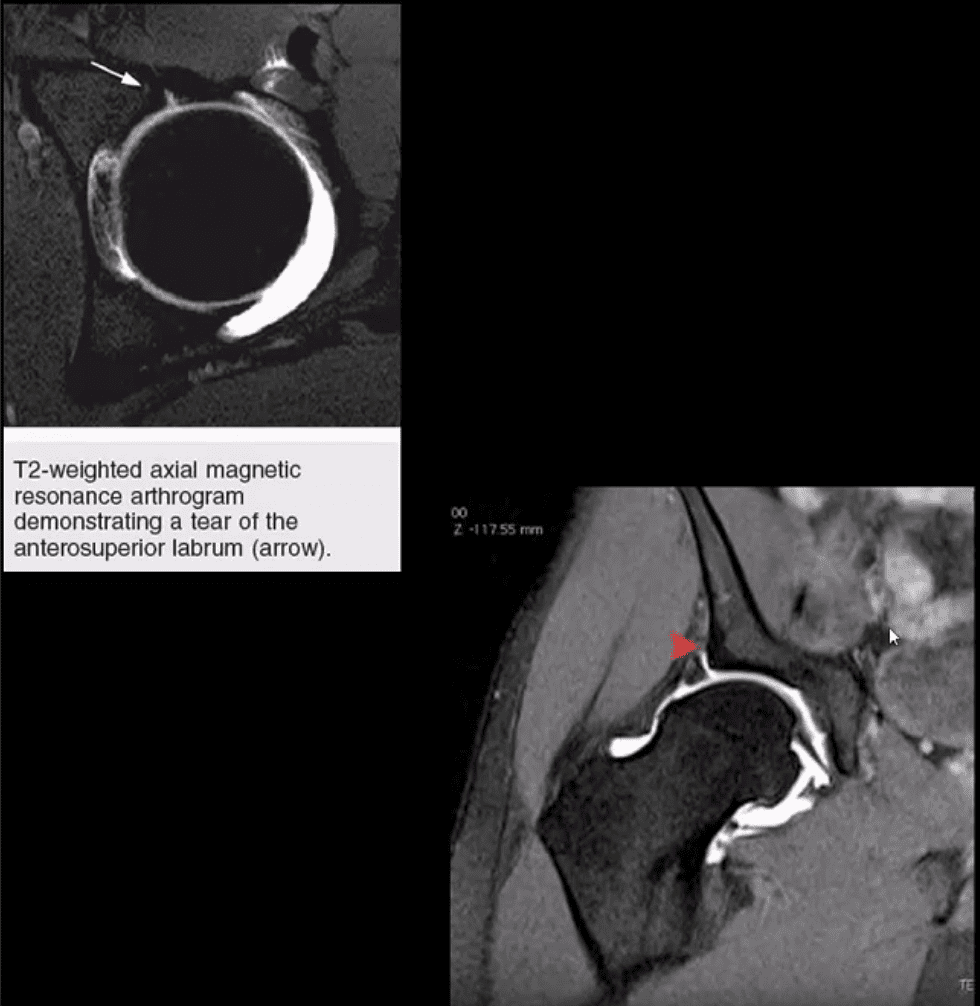
MRI and MR arthrography (most accurate Dx of labral tear) can aid the diagnosis of labral tear and other changes of FAI
Referral to the Orthopedic surgeon is necessary to prevent DJD progression and repair labral abnormalities. Late Dx may lead to irreversible changes of DJD
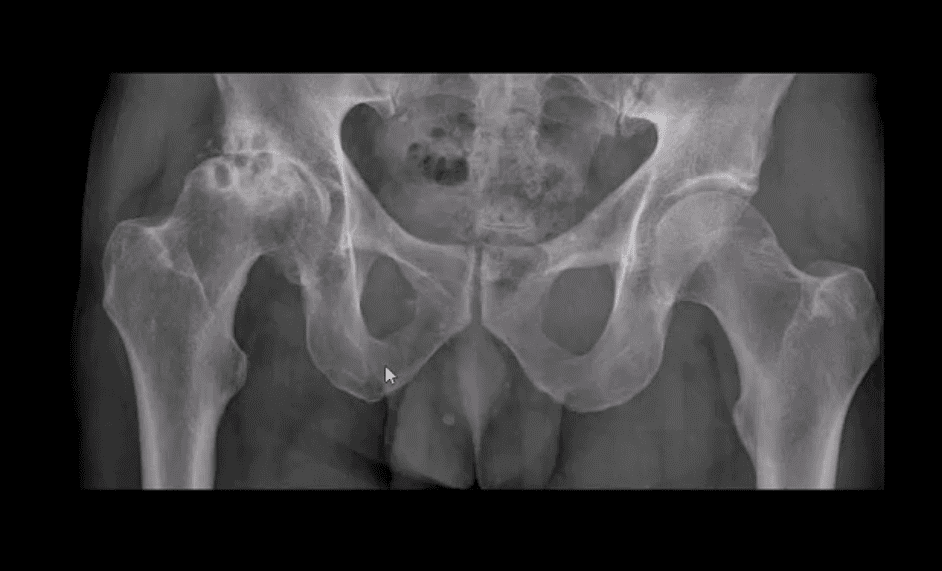
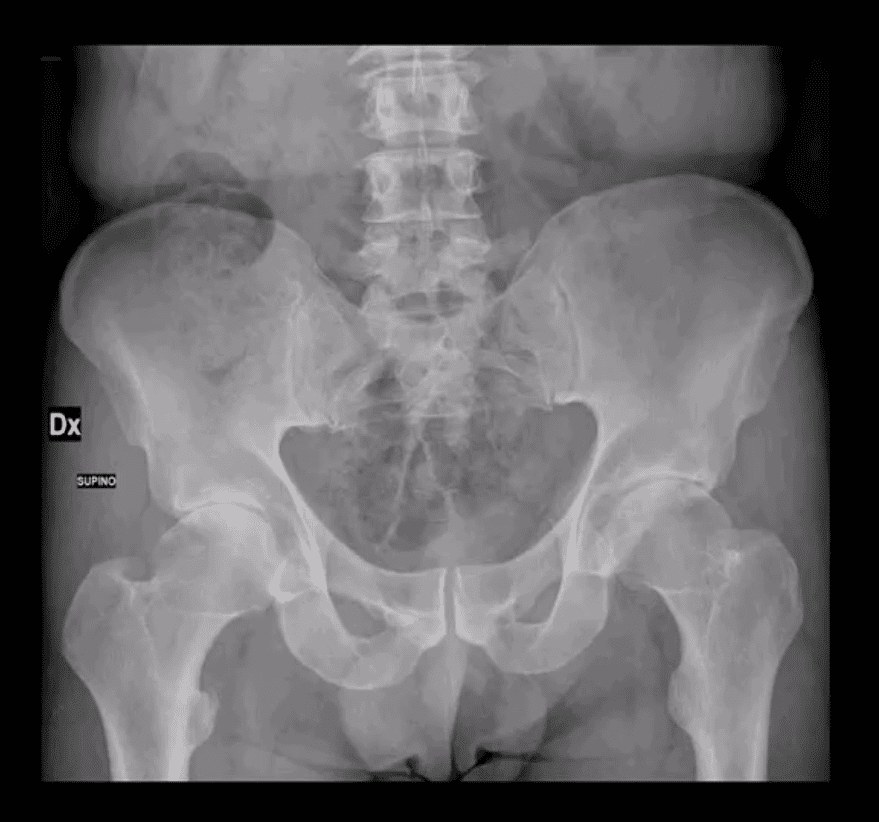
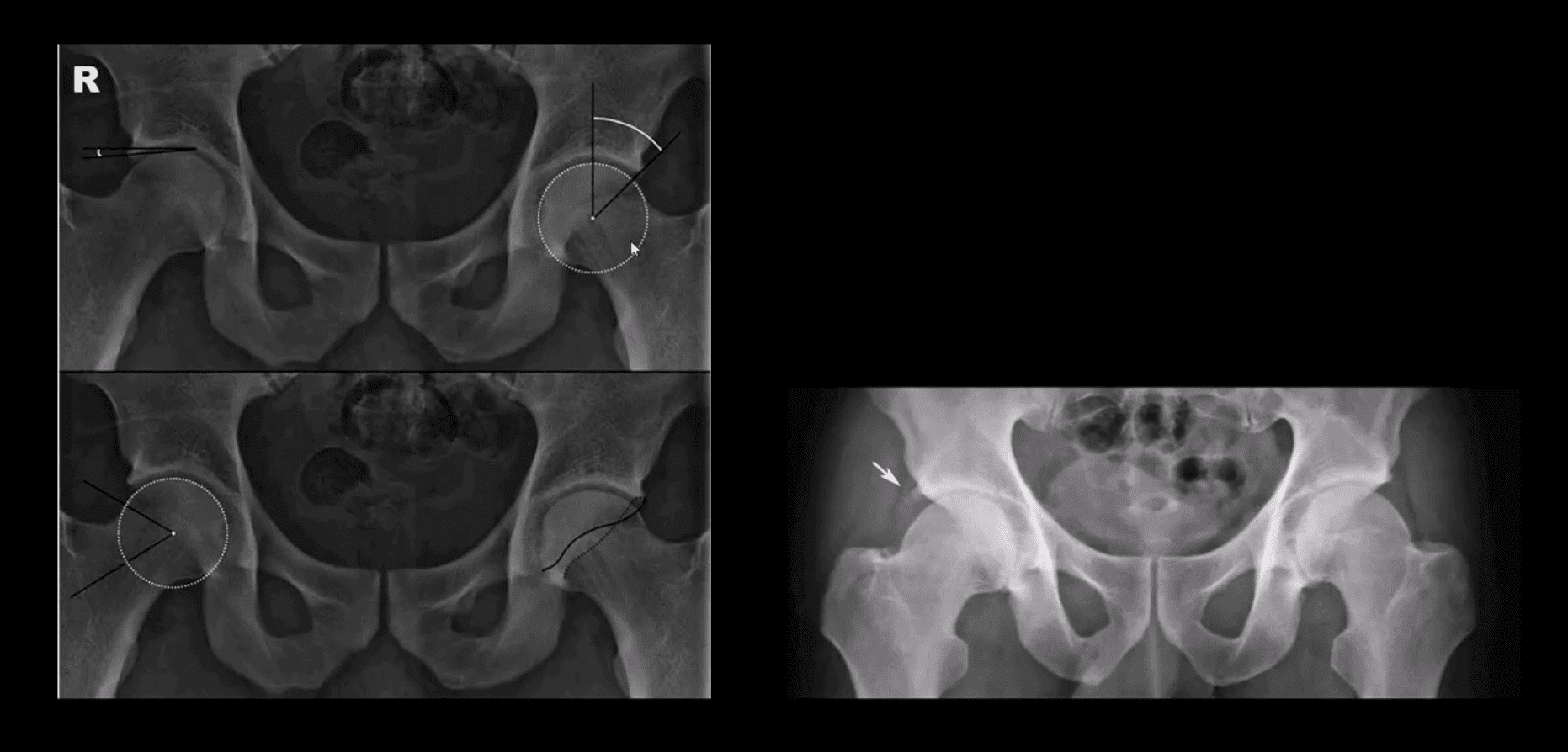
AP Pelvis: B/L CAM-type FAI syndrome
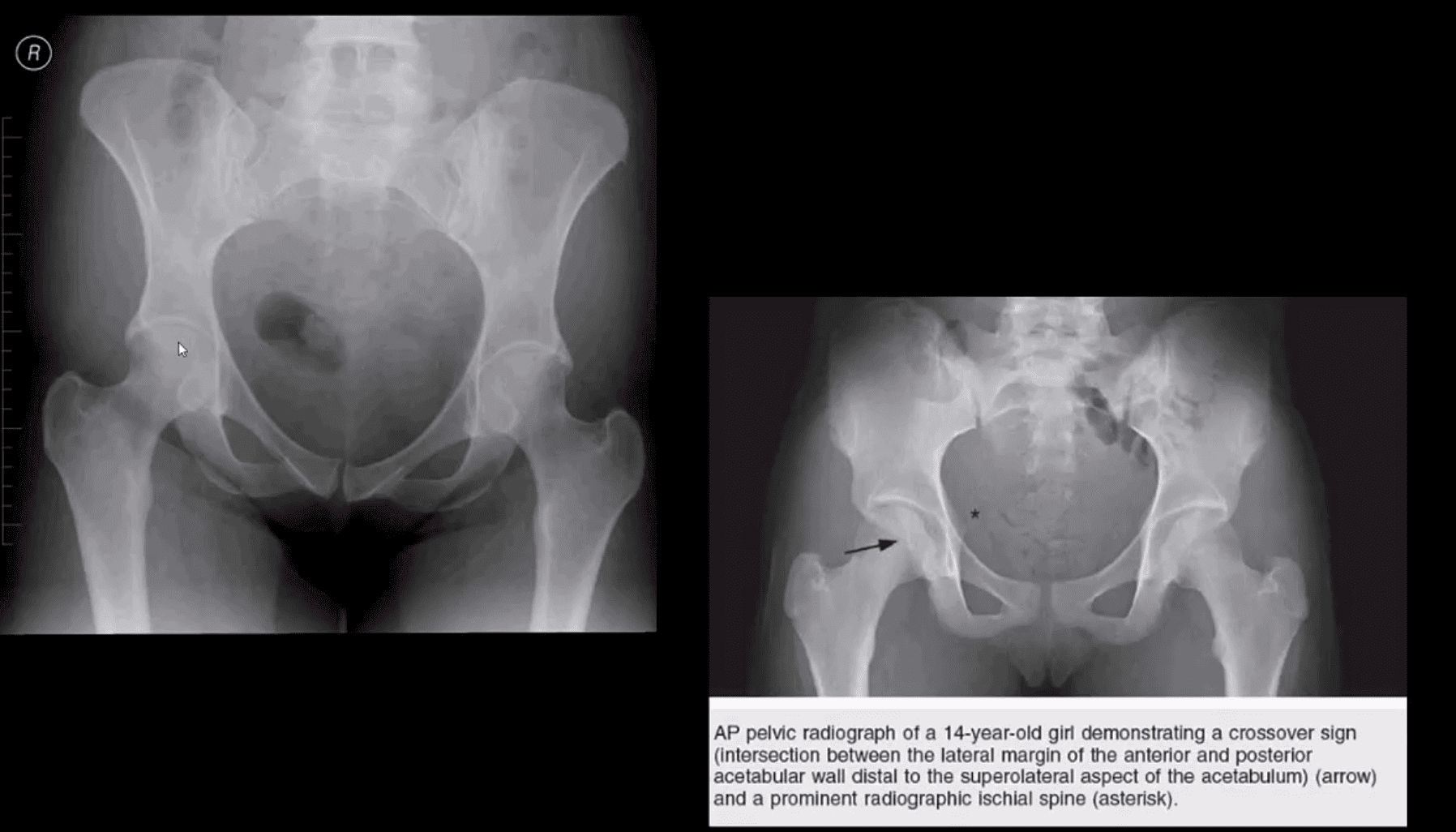
Pincer-Type FAI with Acetabula Over-Coverage
Key radiographic signs: “Cross-over sign” and abnormal center-edge and Alfa-angle evaluation methods
Dx of FAI
Center-edge angle (above the first image) and Alfa-angle (above the second image)
B/L CAM-type FAI with os acetabule�(above right image)
MR Arthrography
Labral tear and CAM-type FAI syndrome on axial (above left) and coronal T2 W (above right) MR arthrography
Note acetabula labral tear. Referral to an orthopedic surgeon is required. For more information:
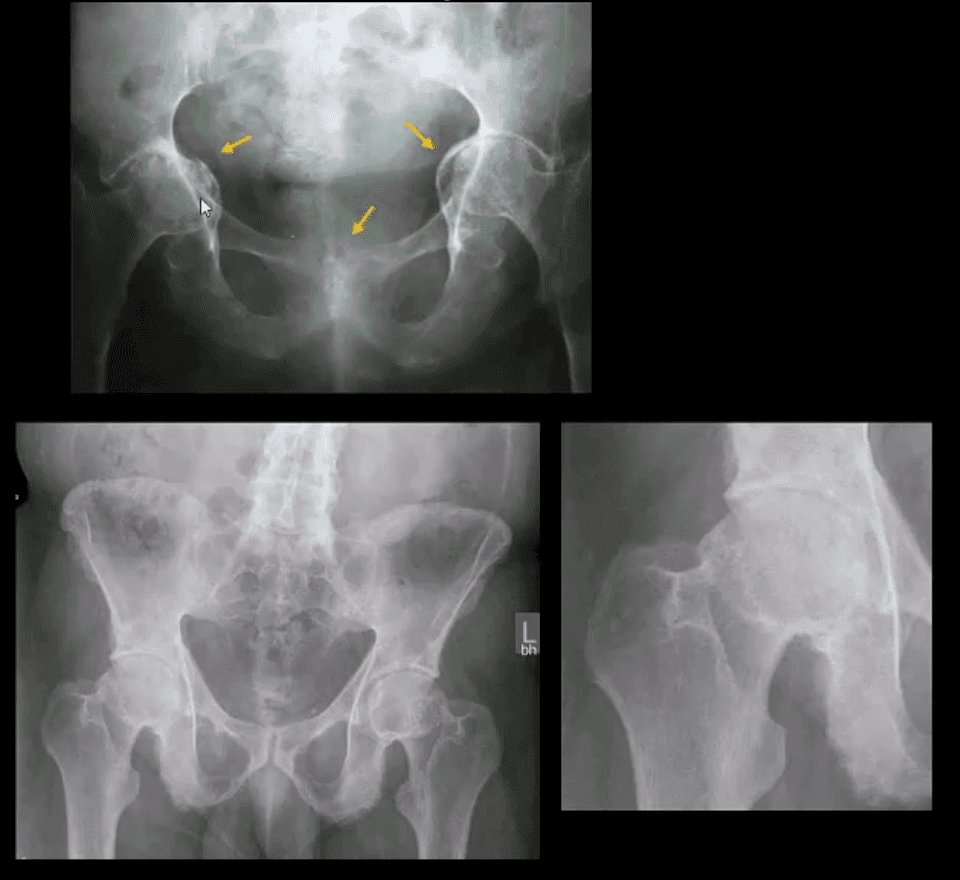
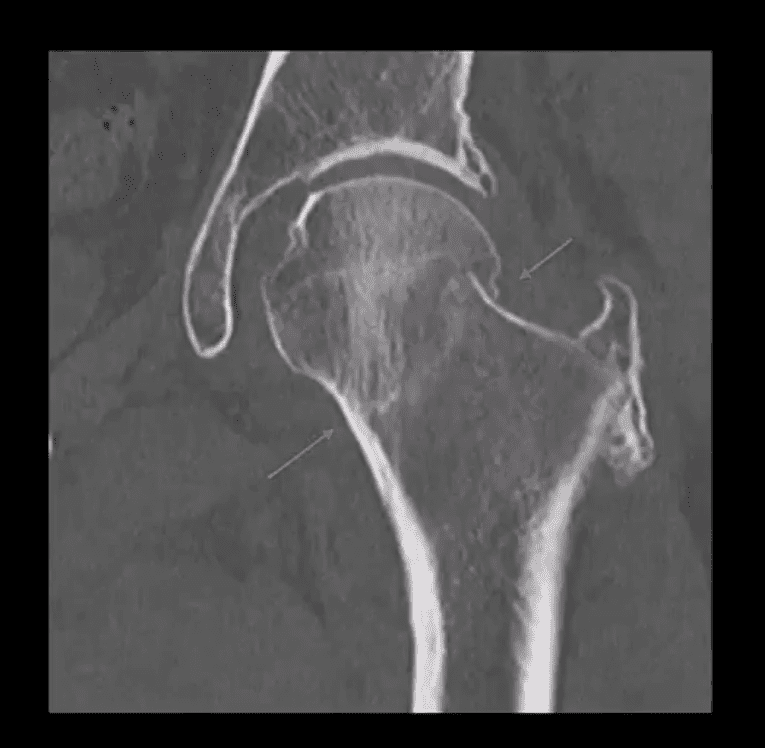
X-radiography pitfalls: some undisplaced Garden 1 & 2 Fxs may be missed d/t pre-existing DJD and osteophytes along the femoral head-neck junction that may overly the Fx line
Fx line is incomplete and too small/subtle especially if the study is read by non-radiologists
Incomplete Fxs if left untreated will not heal and likely to progress to complete Fxs
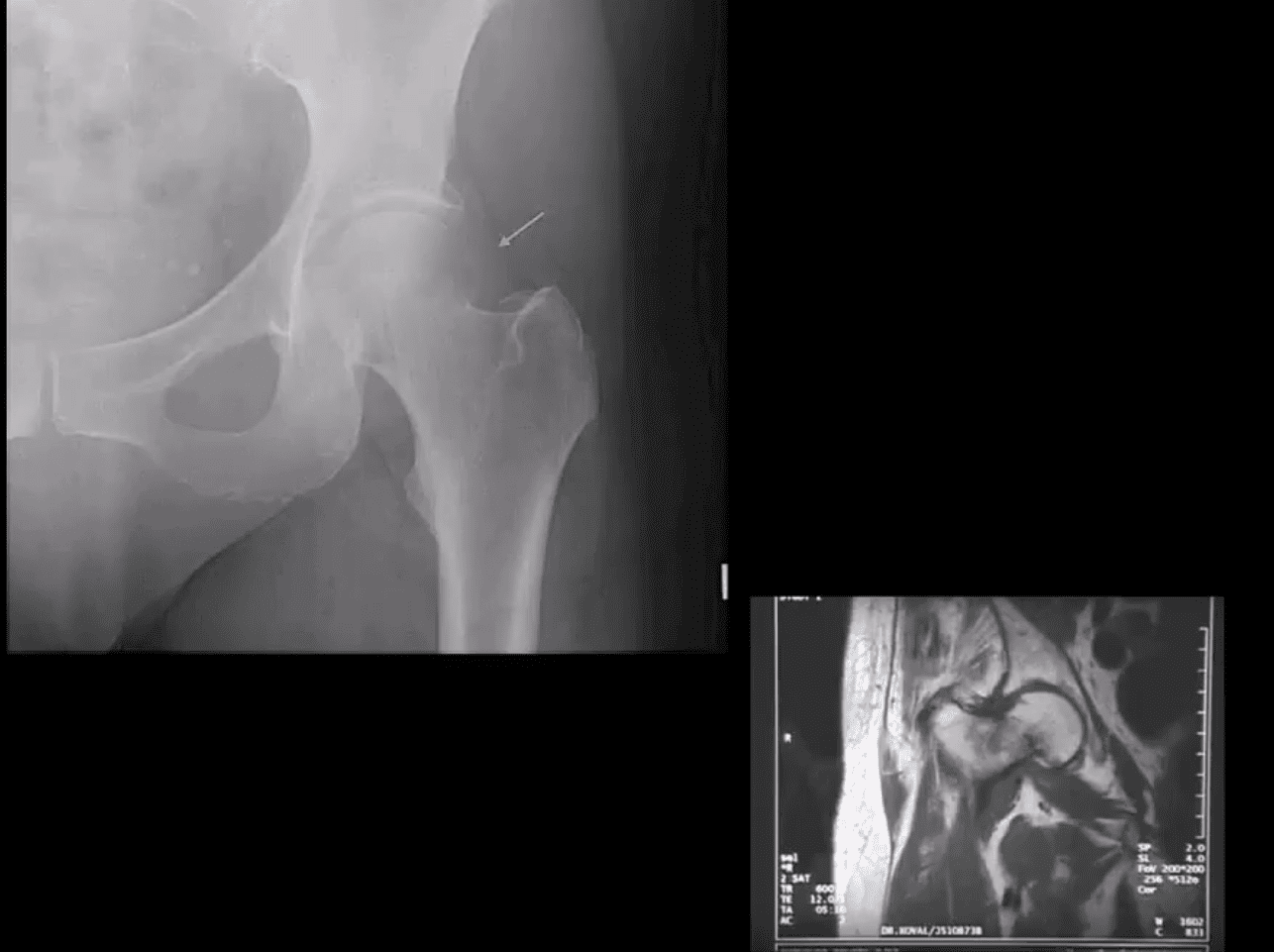
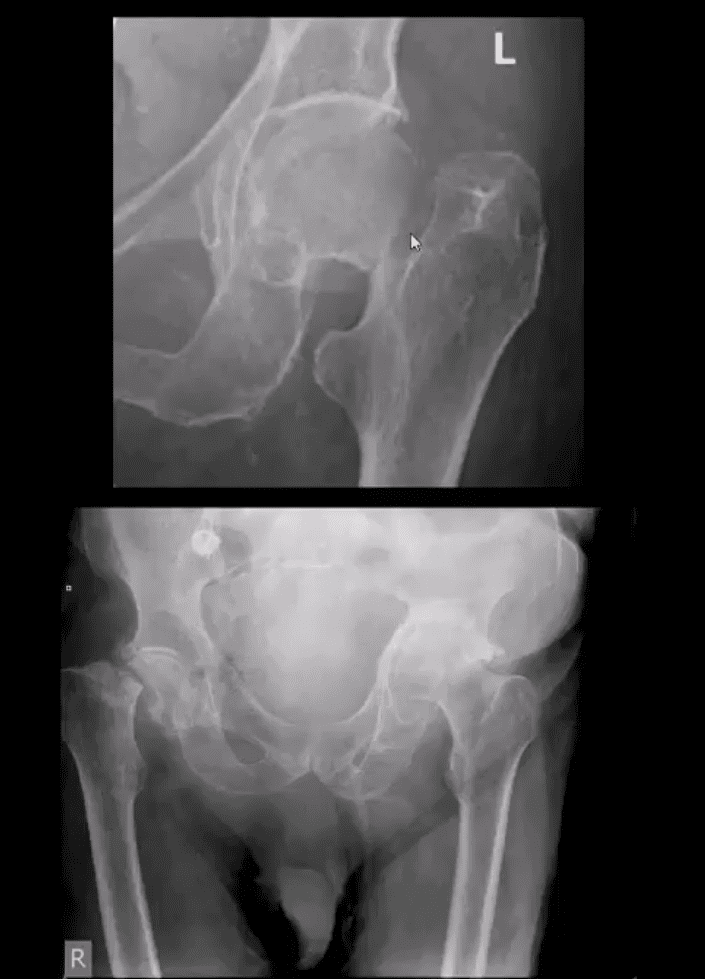
AP hip spot view: note valgus deformity of the head (above yellow arrow) with a small/subtle line of sclerosis in the sub-capital region representing Garden 1 Fx. MRI may help with Dx of subtle radiographic Fxs. If MRI contraindicated, Tc 99 radionuclide bone scan may help demonstrate high uptake of the radiopharmaceutical in Fx (below image)
Above – Tc99 Radionuclide Bone Scan Reveals Left Subcapital Femoral Neck Fx
Garden 2 complete undisplaced (above green arrows) Fx
AP hip: Garden 3 complete partially displaced Fx (above the first image)
AP pelvis: complete displaced Garden 4 Fx (above the second image)
Clinical pearls: in some cases of Garden 4 Fx, DDx may be difficult to differentiate from OSP vs. pathologic fx d/t to bone Mets of Multiple myeloma (MM)
Management: depends on patients age and activity level
Garden 3 & 4� require total hip arthroplasty in patients <85-y.o.
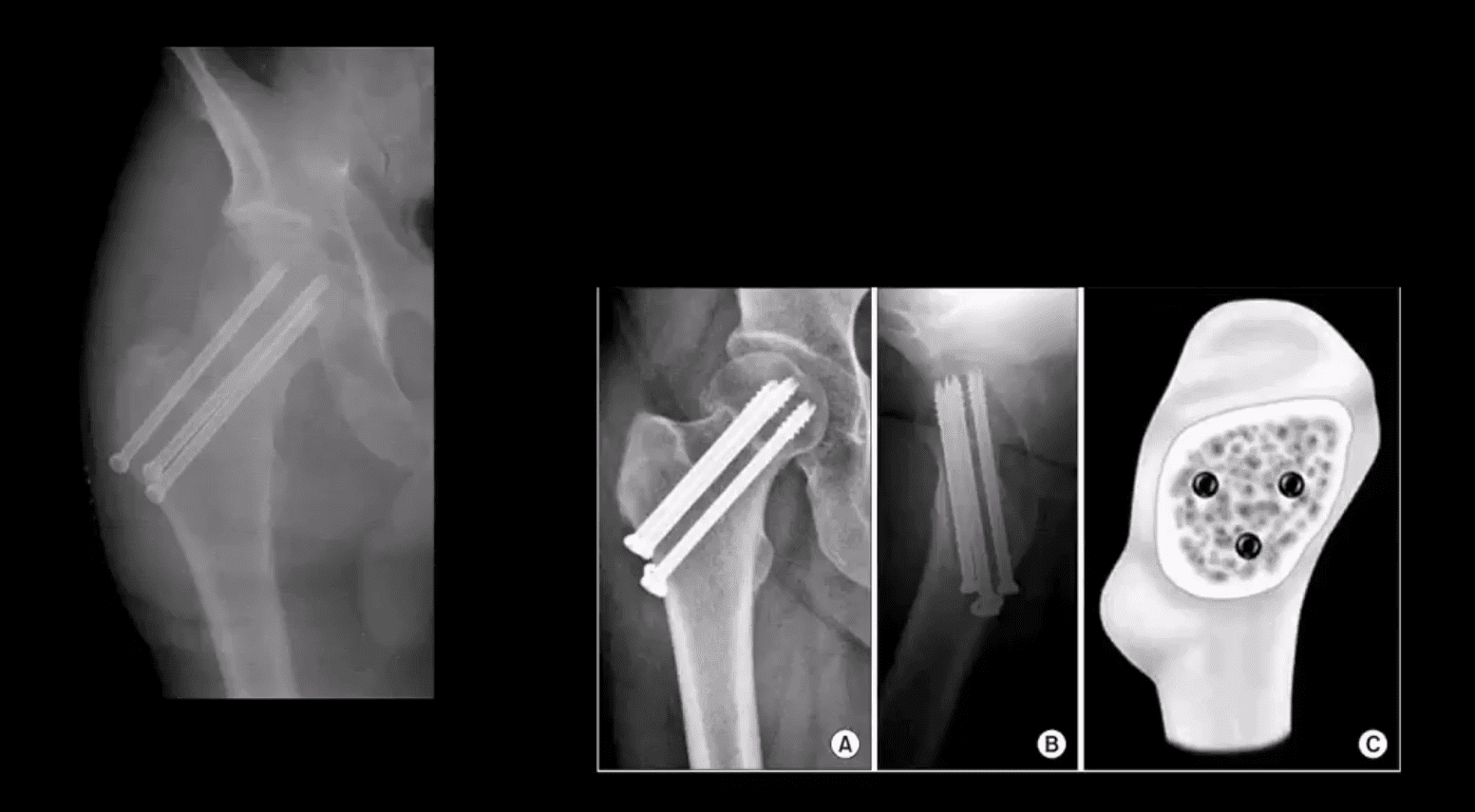
Garden 1 & 2 may be treated with closed reduction of fx and open capsule and 3-cannulated fixating screws
Pre-existing DJD may require total arthroplasty
Occasionally observation may be performed on patients who are not active and significant risks of surgery and depends on surgical centers
m/c Rx of Garden 1 & 2 undisplaced Fx with 3-screws. Screws proximity depends on the bone quality and Fx type
THA aka hip replacement: cemented THA with bone cement (above the first image) vs. non-cemented (biologic) that is used mostly in younger patients
2-types: metal on metal vs. metal on polyethylene
The femoral angle of the prosthesis should have slight valgus but never >140 degrees
The non-cemented component uses porous metal allowing the bone to integrate sometimes coating in bone cement from osteoconduction
THA has good outcome and prognosis
Occasionally cement failure, fractures, and infections may complicate this procedure
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine