The thighs in the lower half of the body work together with the hips to stabilize the legs when the body is in motion. The thighs and the hips also support the weight of the upper half of the body and are surrounded by muscles, ligaments, and nerve roots to supply blood and sensory-motor function to the legs. One of the thigh muscles that work with the hips is the tensor fasciae latae (TFL) muscle. When the thigh muscles are being overused or suffer from injuries, tiny nodules known as trigger points (myofascial pain syndrome) can affect a person’s ability to function worldwide. Today’s article examines what the tensor fasciae latae muscles do, how myofascial pain syndrome affects the thighs, and various stretches/techniques for the thighs. We refer patients to certified providers who incorporate multiple methods in the lower body extremities, like thigh pain treatments correlating to trigger points, to aid individuals dealing with pain symptoms along the tensor fasciae latae muscle. We encourage and appreciate patients by referring them to associated medical providers based on their diagnosis, especially when it is appropriate. We understand that education is an excellent solution to asking our providers complex questions at the patient’s request. Dr. Jimenez, D.C., utilizes this information as an educational service only. Disclaimer
What Does The Tensor Fasciae Latae Muscle Do?
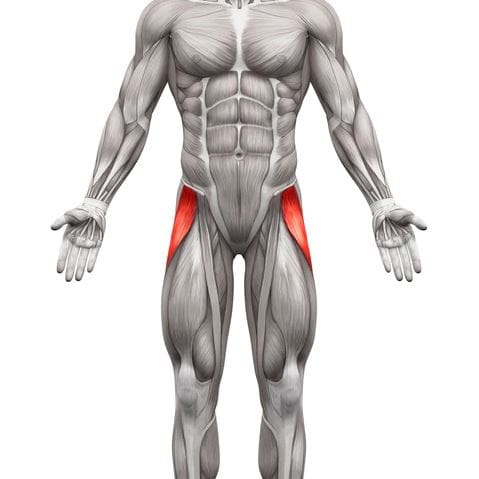
Do you have difficulty walking for a long period? So you feel that your hips feel unstable when you move? Or do you feel radiating pain down from your thighs to your knees? Thigh pain associated with these symptoms can affect a person’s ability to move around from one location to another due to trigger points affecting the tensor fasciae latae muscle. The tensor fasciae latae (TFL) muscles are located at the proximal anterolateral thigh and originate from the anterior superior iliac spine. The TFL muscle is between the superficial and deep muscle fibers of the iliotibial (IT) band, as its attachment assists with knee flexion and lateral rotation. The TFL muscles also work together with the gluteus muscles in various hip movements. Studies reveal that the primary function of the TFL muscles is providing balance to the body’s weight and the non-weight-bearing leg to walk. The TFL muscles allow the individual to walk, run, and assist with movement and stabilization to the hips and knees without pain inflicted on the joints and muscles.
Myofascial Pain Syndrome Affecting The Thighs
Since the TFL muscles allow the person to walk and run, this muscle can become overused and strained through repetitive motions causing many issues to the hips, knees, and thighs. When these issues affect the TFL muscles, they can develop nodules along the muscle fibers known as trigger points or myofascial pain syndrome. Myofascial pain syndrome is a musculoskeletal disorder that can invoke referred pain in one location of the body while affecting the surrounding muscles in a different body location. Myofascial pain syndrome associated with the TFL muscles can cause issues to the hips, thighs, and knees while affecting a person’s ability to walk. Studies reveal that the prevalence of myofascial pain syndrome on the TFL muscles correlates to pain and disability in the thighs. When myofascial pain syndrome affects the TFL muscles, it can mimic chronic knee osteoarthritis.
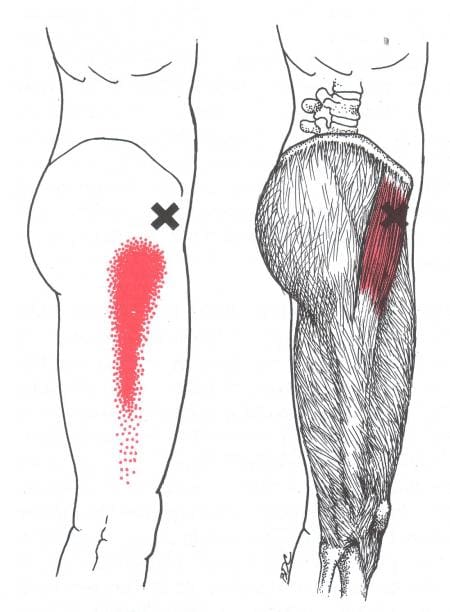
Even though myofascial pain syndrome is challenging to diagnose, it is treatable through various stretches and techniques. In Dr. Janet G. Travell, M.D.’s book, “Myofascial Pain and Dysfunction,” it mentioned that when patients have active trigger points in their TFL muscles, they become aware of the referred pain affecting their hip joints and are unable to lie comfortably on their sides due to the body-weight pressure pressing on the affected TFL muscle. The book also points out that when pain is referred to from trigger points associated with the TFL muscles, it can be mistaken for pain in the glutes.
Trigger Point Of The Week: Tensor Fasciae Latae- Video
Have you been experiencing difficulty walking from one location to another? Do you feel pain in your thighs or knees? Or do you have a problem lying down on your side that is causing you pain? If you have been dealing with walking issues, it could be due to myofascial trigger pain in your tensor fasciae latae (TFL) muscles affecting your ability to walk. The TFL muscles help provide stability to the hips and thighs and assist with knee flexion and lateral rotation. This muscle also allows people to walk and run without any pain inflicted on the joints and muscles. When repetitive motions start to cause the TFL muscles to become overused and strained, it can lead to myofascial pain syndrome or trigger points developing, causing referred pain to the thighs. The video above explains where the TFL muscles are located and where the trigger points on the TFL muscles are causing pain to the thighs. Myofascial pain syndrome can mimic other chronic conditions like knee osteoarthritis, which causes pain and disability to the lower half of the body.
Various Stretches & Techniques For The Thighs
Now myofascial pain syndrome is challenging to diagnose in an examination due to the referred pain affecting one location of the body than the actual source of where the pain is coming. However, it is treatable through various techniques and stretches for the thighs to restore leg mobility. Studies reveal that direct stretching of the TFL (tensor fasciae latae) muscles can reduce long-term pain effects on the hips, thighs, and lower back and improve hip and thigh mobility. Various stretches like hip extensions and laterally rotating the hips can break the myofascial trigger points in the TFL muscle. Using a foam roller on the hips can gently stretch and loosen the muscle fibers on the TFL and help warm up the muscle before working out. Sitting down correctly in a chair can help the hips from causing more muscle strain to the thighs and prevent the TFL muscles from being shortened. Incorporating these stretches and techniques can improve hip and thigh mobility in the legs, allowing the individual to walk or run without pain.
Conclusion
The TFL (tensor fasciae latae) muscles are located on the proximal anterolateral thigh between the IT (iliotibial) band, which assists with knee flexion and lateral rotation. The TFL muscle also works with the gluteal muscles and allows the person to walk, run, and help with stability movement to the hips and knees with inflicted pain on the joints and surrounding muscles. When the TFL muscles become overused, they can develop myofascial trigger pain on the TFL, causing referred hip, knee, and thigh pain. This can cause the individual not to be able to walk for long periods and think they might have osteoarthritis in the knees. Fortunately, people can incorporate various stretches and techniques to reduce the pain in the thighs and hips while managing myofascial trigger pain along the TFL muscles. These various stretches and techniques allow mobility back to the hips and thighs so the individual can walk without pain.
References
Gottschalk, F, et al. “The Functional Anatomy of Tensor Fasciae Latae and Gluteus Medius and Minimus.” Journal of Anatomy, U.S. National Library of Medicine, Oct. 1989, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1256751/.
Ohtsuki, Keisuke. “A 3-Month Follow-up Study of the Long-Term Effects of Direct Stretching of the Tensor Fasciae Latae Muscle in Patients with Acute Lumbago Using a Single-Case Design.” Journal of Physical Therapy Science, The Society of Physical Therapy Science, May 2014, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4047246/.
Simons, D. G., and L. S. Simons. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 2:the Lower Extremities. Williams & Wilkins, 1999.
Sánchez Romero, Eleuterio A, et al. “Prevalence of Myofascial Trigger Points in Patients with Mild to Moderate Painful Knee Osteoarthritis: A Secondary Analysis.” Journal of Clinical Medicine, MDPI, 7 Aug. 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7464556/.
Trammell, Amy P, et al. “Anatomy, Bony Pelvis and Lower Limb, Tensor Fasciae Muscle – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 8 Aug. 2022, https://www.ncbi.nlm.nih.gov/books/NBK499870/.
The body’s lower extremities have a very important role as it helps support the upper body’s weight and provide stability to the lower body. The lower half of the body consists of the lower abdominals, hips, pelvic, and buttock regions, which have various muscles surrounding the lumbar and pelvic areas of the spine. These muscles help protect the lower vital organs and work with the central nervous system to utilize the sensory-motor function of the legs and feet. When normal factors like prolonged sitting or standing begin to affect the lower body, it can cause referred pain to travel down to the legs and push the lower extremities to develop symptoms associated with trigger points on the lower torso. Today’s article looks at the lower torso, how trigger points affect the lower torso, and therapeutic ways to manage trigger points in the lower torso. We refer patients to certified providers who incorporate various techniques in more inadequate body pain treatments related to trigger points to aid people suffering from pain-like symptoms along the lower torso muscles along the body’s lower extremities. We encourage and appreciate patients by referring them to our associated medical providers based on their diagnosis, especially when it is appropriate. We understand that education is an excellent solution to asking our providers complex questions at the patient’s request. Dr. Jimenez, D.C., utilizes this information as an educational service only. Disclaimer
What Is The Lower Torso?
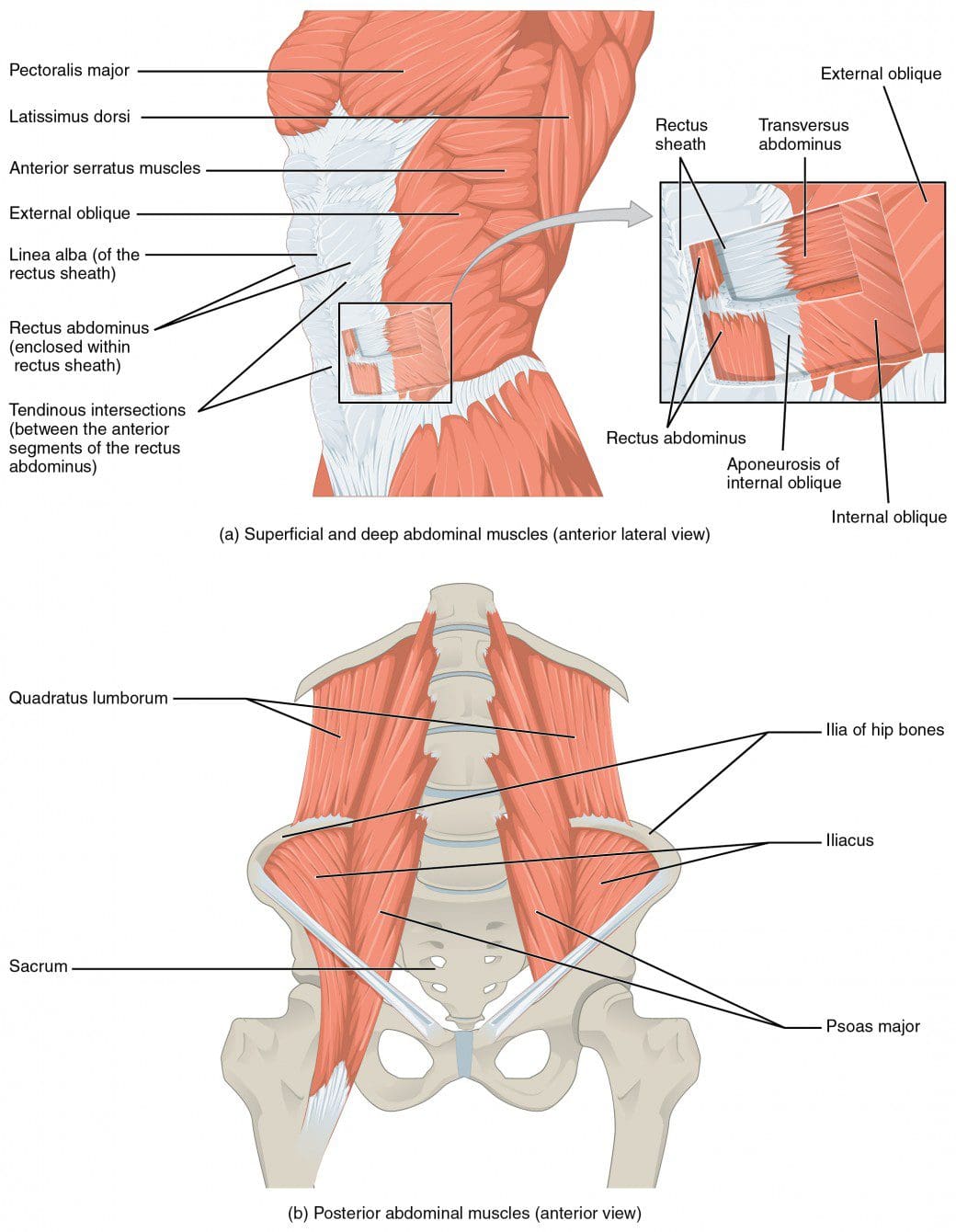
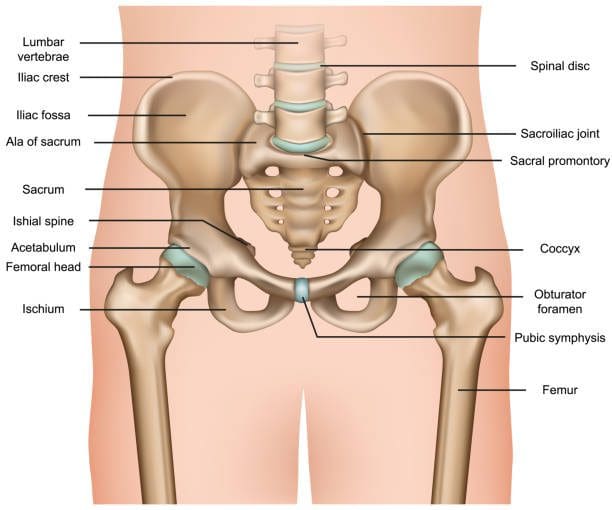
Have you been feeling stiffness around your hips lately? Have you noticed that you are leaning forward constantly, causing strain on your lower back? Or have you been experiencing pain in one location in your lower half? When dealing with these issues in the lower half of the body, it could correlate with somato-visceral symptoms associated with trigger points in the lower torso. The lower torso of the human body, or the lower abdominals, is defined as the anterior region of the trunk between the thoracic diaphragm and serves as the cavity to house the digestive, urinary, endocrine, and parts of the reproductive system. The lower torso has various muscles and nerves that surround the lower back, the hips, the pelvis, and the buttock region of the body that stabilizes the legs when in motion and supports the upper body. The muscles in the lower torso also surround the lumbar and pelvic areas of the spine to protect the joints and vertebrae from becoming dysfunctional. When issues begin to rise and affect the lower torso, it can lead to overlapping problems affecting the body’s lower extremities.
How Do Trigger Points Affect The Lower Torso?
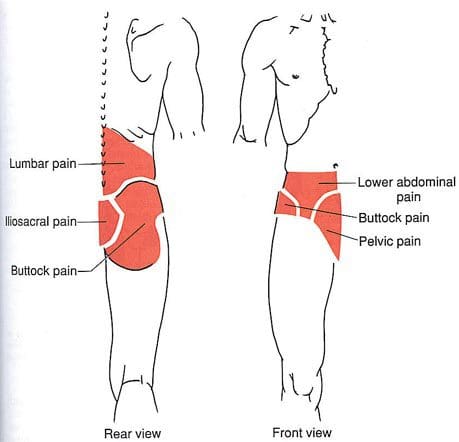
Some of the issues affecting the lower torso that most people don’t realize are that prolonged sitting or standing can cause problems to the legs, hips, pelvis, and feet. This causes the blood supply to pool into the legs and feet, thus causing swelling and muscle weakness in the lower torso muscles. Another issue is when the lower torso has been through a traumatic event that can cause the affected muscles to develop tiny nodules known as trigger points to cause problems in the lower back, hips, pelvis, and buttock region of the body. Studies reveal that trigger points are often characterized by pain causing a limited range of motion in the joints while causing muscular contracture and mimicking other chronic conditions affecting the muscles. When trigger points affect the muscles in the lower torso, “Myofascial Pain and Dysfunction,” written by Dr. Janet Travell, M.D., pain associated with movement can cause tingling or electric sensations down to the lower extremities causing somato-visceral referred pain to the lower torso. Since the nerve roots from the spinal cord branch out to the various muscles and become irritated, causing referred pain to different areas of the lower extremities.
Trigger Point Therapy For The Abs- Video
Have you been dealing with hip mobility issues? What about experiencing low back pain after being in a hunch position for an extended period? Or have you been experiencing problems in your pelvic region? Many of these issues are correlated with trigger points associated with the lower torso. Trigger points or myofascial pain syndrome are caused when the affected muscles have been overused or been through a traumatic event that causes referred pain to different body locations. The video explains where trigger points are located in the lower torso, especially in the abdomen and how to release them through palpations and massage. These techniques can help reduce the pain symptoms that affect the lower torso and manage myofascial pain from developing in the future.
Therapeutic Ways To Manage Trigger Points In The Lower Torso
Pain specialists like chiropractors and massage therapists will use various techniques to reduce the pain and alleviate the trigger points from the affected muscles. Many often go to a pain specialist who deals with trigger points through recommendations by their primary doctor. They will go through an examination process and explain to the pain specialist where the pain is located. Afterward, they will devise a treatment plan with the patient’s primary doctor, allowing them to follow a routine to prevent the pain from returning. Various techniques like stretching the abdominals, exercising, and resting can manage trigger points from returning to the affected muscles and even help bring muscle strength back to the body.
Conclusion
The lower torso consists of the hips, lower back, pelvis, and buttock region while protecting the body’s vital organs. The lower torso helps stabilize, the lower body extremities and supports the upper body’s weight. When normal issues like prolonged sitting or standing start to cause muscle strain to the lower torso region, it can develop trigger points to cause various problems to that region and cause mobility issues in the lower abdominal area. When the pain becomes unbearable, many individuals go to a pain specialist to help manage the trigger points from affecting the lower torso region and bring back mobility function to the lower extremities.
References
Akamatsu, Flavia Emi, et al. “Anatomical Basis of the Myofascial Trigger Points of the Gluteus Maximus Muscle.” BioMed Research International, Hindawi, 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5733974/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 2:the Lower Extremities. Williams & Wilkins, 1999.
Wade, Christian I, and Matthew J Streitz. “Anatomy, Abdomen and Pelvis, Abdomen – Statpearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 25 July 2022, https://www.ncbi.nlm.nih.gov/books/NBK553104/.
The skeletal joints can keep the body upright and stabilized while protecting the internal organs. The skeletal joints also are at risk of factors (normal and traumatic) that can impact the body, thus potentially causing painful symptoms to affect different body areas. Hip pain is among the most common complaints for many individuals, especially the elderly. To that point, when the body suffers from hip pain, it may involve pelvic pain and associated symptoms that mimic other issues within the body. Today’s article examines the causes of hip and pelvic pain, the symptoms related to hip and pelvic pain, and how chiropractic care may relieve hip and pelvic pain. We refer patients to certified providers specializing in osteopathic treatments to help many individuals with hip and pelvic pain. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
The Causes Of Hip & Pelvic Pain
Do you experience stiffness located on your low back or hips? What about sciatic nerve pain that travels down your legs? Or have you been experiencing cramping around the pelvic regions of your body? Experiencing these symptoms may be the potential cause that you might be dealing with hip and pelvic pain. Even though hip pain is often associated with older individuals, it can affect many individuals of different ages. Studies reveal that the pathologies outside the hips may be the cause and referred pain, making diagnosing hip pain difficult. Hip pain causes could be overused joints and soft tissues that support the hips due to repetitive motions, strain from the multiple muscles that support the hips, or arthritic symptoms. Studies reveal that individuals who work in a desk job will potentially develop low back pain due to prolonged sitting, thus becoming associated with excessive mobility of the lumbar spine and decreased hip joint mobility.
Individuals with hip pain could risk developing pelvic pain associated with the overuse of joints and soft tissues. Now how pelvic pain correlates with hip pain, and what’s the causation? Studies reveal that the stabilizing muscles (iliopsoas, pectineus, obturator externus, gluteus minimus, and piriformis muscles) are overworked and become consequent hip and joint destabilization. This causes the affected muscles to become tired and weak and triggers sciatic nerve compression along the piriformis muscle. Pelvic pain associated with hip pain may cause dysfunctional musculoskeletal symptoms along the lower abdominals, hips, and lumbosacral back.
The Associated Symptoms Of Hip & Pelvic Pain
The factors involved with hip and pelvic pain could potentially have associated symptoms that might affect the body’s lower extremities. One of the most prominent symptoms of hip pain is groin pain, which could possibly be involved with pelvic pain since the ligaments and muscles that encompass the hips and groin may be weak and overused. Sometimes various underlying causes do contribute to hip and pelvic pain, causing associated symptoms that may confuse the individual in pain. Hip and pelvic pain may refer to low back and sciatic nerve pain since the lower spine and hips are close together; thus, pinpointing where the true source of pain is in the body’s lower half makes it confusing. Some of the symptoms associated with hip and pelvic pain include:
Low back pain
Muscle weakness
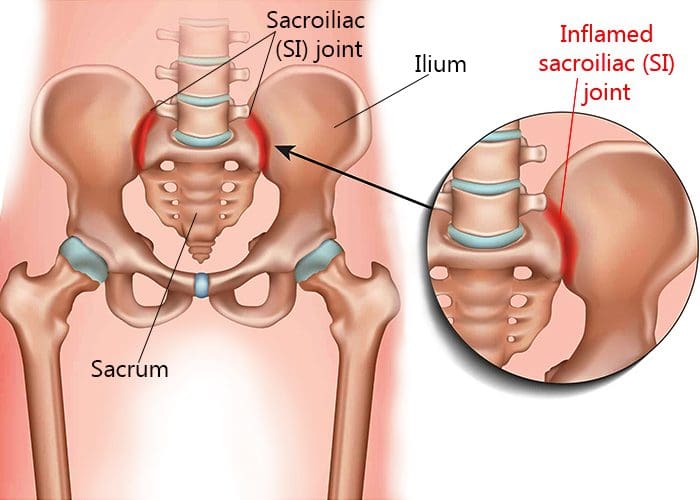
Sacroiliac joint dysfunction
Bladder issues
Sciatic nerve pain
Piriformis syndrome
The 3 Common Causes Of Hip Pain-Video
Have you been dealing with muscle stiffness around or along your hips and lower back? Do you have bladder issues? Or have you experienced muscle weakness in the lower extremities of your body? Some of these symptoms could be associated with hip and pelvic pain. The video above explains the three common causes of hip pain, and interestingly, one of the causes of hip pain could potentially involve the lower back. Studies reveal that since the low back and hips are close to each other, alterations in the lumbopelvic region could potentially be involved with low back pain. Some of the issues associated with the alterations in the lumbopelvic area include:
Limited range of motion on hip rotation
Tissue injury
Stiff joint capsules
Micro/macro trauma
Fortunately, hip and pelvic pain management may help alleviate referred pain issues through chiropractic care.
Chiropractic Relief For Hip & Pelvic Pain
Individuals dealing with hip and pelvic pain may find relief through chiropractic care. The pelvis is a direct continuation of the spine as the sacrum (the five lowest fused vertebrae) and the pelvic girdle complex interact with the joints from the lower skeletal system. If there is pain in the lower body and the individual is unsure whether it is their back or hips, their first course of action is to visit their primary doctor or a chiropractor. Afterward, they will review the individual’s medical history while performing a series of physical exams like various movements to make an accurate diagnosis. Once the pain diagnosis is identified, chiropractors utilize total body alignment by restoring balance in the pelvis and the spine through manipulation. When the spine and hips suffer from a subluxation, it can cause unnecessary strain on the surrounding muscles around the spine and hips. To that point, realigning the spine from a chiropractic adjustment could reduce or eliminate the excessive stress affecting the surrounding muscles. Chiropractic care can also promote various therapies that increase balance along the hips and pelvic region, which include:
Stretching
Therapeutic massage
Physical activities/Exercise therapy
Nutrition
Whether the pain is located in the hips, low back, or pelvic regions, chiropractic care can help restore, address, and alleviate the pain while maintaining optimal long-lasting results.
Conclusion
The skeletal joints can help keep the body upright and stabilized while protecting the internal organs from normal and traumatic factors. When these factors begin to cause an impact on the body, the skeletal joints are at risk of developing pain along the musculoskeletal structure. Hip and pelvic pain have an overlapping relationship as they are amongst the most common complaints for many individuals. To that point, pain from the hips or the pelvic may mimic other issues associated with chronic disorders. Incorporating treatments like chiropractic care can help alleviate, address, and restore the body through spinal manipulation. This allows individuals to be pain-free and help restore balance in their joints.
References
Harris-Hayes, Marcie, et al. “Relationship between the Hip and Low Back Pain in Athletes Who Participate in Rotation-Related Sports.” Journal of Sport Rehabilitation, U.S. National Library of Medicine, Feb. 2009, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2699456/.
Lee, Dae Wook, et al. “Chronic Pelvic Pain Arising from Dysfunctional Stabilizing Muscles of the Hip Joint and Pelvis.” The Korean Journal of Pain, The Korean Pain Society, Oct. 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5061646/.
Luthra, Jatinder Singh, et al. “Understanding Painful Hip in Young Adults: A Review Article.” Hip & Pelvis, Korean Hip Society, Sept. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6726866/.
Nishimura, Takaaki, and Ryo Miyachi. “Relationship between Low Back Pain and Lumbar and Hip Joint Movement in Desk Workers.” Journal of Physical Therapy Science, The Society of Physical Therapy Science, Oct. 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7590845/.
The hips in the lower extremities of the body help stabilize the weight of the upper half while providing movement to the lower half. The hips also allow the body to twist, turn, and bend back and forth. The hip joints connect to the inside of the pelvic bone, while the pelvic bone is connected to the sacroiliac joint, which connects to the spine. When natural wear and tear affects the joints as the body ages, issues like hip pain and osteoarthritis associated with low back pain occur, causing various symptoms to arise in the body. Today’s article looks at osteoarthritis, how it impacts the hips, and how to manage hip osteoarthritis. We refer patients to certified providers specializing in musculoskeletal therapies to help those with hip pain and osteoarthritis. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
What Is Osteoarthritis?
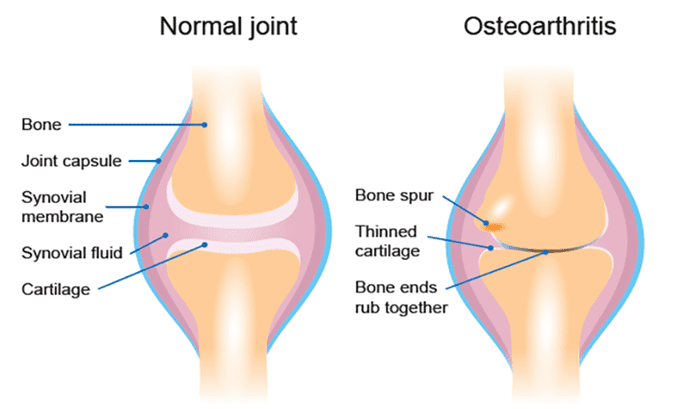
Have you been experiencing pain in your hips or lower back? How about muscle stiffness near the groin? Do symptoms associated with sciatica seem to flare up near your hips and the back of your leg? Many of these symptoms are signs that you could be at risk of developing osteoarthritis near your hips. While arthritis refers to inflammation of the body’s joints, osteoarthritis is a type of arthritis that causes degeneration of the joint cartilage, triggering joint pain and functionality loss. Even though there are several hundred types of arthritis, osteoarthritis is one of the most common types that many people, especially older adults, are affected by. As the body becomes older naturally through age, the repairs from an injury begin to slow down, and the cartilage (the connective tissue that protects the bones from each other) will start to thin out, triggering bone rubbing together, causing inflammation to occur, bone spurs, and inevitable pain. Osteoarthritis is often associated with old age and is multifactorial as factors that can increase the risk of developing osteoarthritis include:
Sex
Age
Obesity
Joint injuries
Genetics
Bone deformities
How Does It Impact The Hips?
Since osteoarthritis affects the joints, how does it cause an impact on the hips? When health issues affect the body, it can cause painful symptoms to gradually worsen and become a risk of developing hip pain. Studies reveal that hip pain is common in all adults and activity levels in the anterior, lateral, or posterior regions near the hips.
Anterior hip pain: Causes referred pain (pain felt in one part of the body but is actually in a different location) associated with internal organ systems.
Lateral hip pain: Causes wear-and-tear pain on the soft muscle tissues on the sides of the hips.
Posterior hip pain: Causes referred pain associated with the lumbar spinal pathology like sciatic nerve entrapment correlating with a deep gluteal syndrome.
All these issues affecting the hips overlap with various issues associated with osteoarthritis. When hip pain originates from osteoarthritis, factors like minimal physical activity or slight movements while resting in bed can worsen due to the hip joints having limited or restricted movement. Studies reveal that hip pain is associated with simple movement impairments that make it difficult to diagnose due to referred pain from the spine, knees, or even the groin area.
How does hip osteoarthritis correlate with groin pain? Studies reveal that when a person is dealing with hip osteoarthritis, groin and buttock pain are slightly more common. The hip joint is behind the groin muscle, which is why groin pain overlaps with hip pain as the root. Hip and groin pain could also be involved with radiating pain down toward the knees in the body.
Exercises For Hip Osteoarthritis- Video
Are you experiencing bladder issues? How about stiffness near or around your hips and groin area? Do issues like low back and sciatica pain? Experiencing these issues could be signs of hip osteoarthritis affecting your lower body. Studies reveal that hip osteoarthritis is a significant source of morbidity, pain, gait abnormalities, and functional impairments potentially involved with other issues. Fortunately, there are ways to manage hip osteoarthritis, as the video above shows eight great exercises for hip osteoarthritis. Certain exercise moves for individuals with hip osteoarthritis can help strengthen the surrounding muscles around the joints while increasing joint mobility to reduce pain and stiffness. Exercising can also be beneficial to the individual as it can provide:
Increase blood circulation
Maintain weight
Provides energy boost
Improves sleep
Promotes muscle endurance
Other available therapies help manage hip osteoarthritis while alleviating associated symptoms affecting the body.
Managing Hip Osteoarthritis Pain
Many individuals suffering from hip osteoarthritis try to find ways to relieve the pain. While they can’t do anything to prevent wear and tear on the joints completely, there are ways to slow down the process and manage hip osteoarthritis in the body. Small changes like incorporating food can dampen inflammatory effects on the joints while providing nutrients to the body. An exercise regime can help strengthen the weak muscles supporting the joints while increasing mobility and range of motion. Treatments like spinal traction and chiropractic care relieve pain and stiffness from joint disorders like osteoarthritis. Chiropractic care provides spinal manipulation on the back and joints to be adjusted. While spinal traction helps the compressed discs lay off the pressure on the surrounding nerves associated with hip pain. Incorporating any of these can help slow the progression of hip osteoarthritis and bring back mobility to the hips.
Conclusion
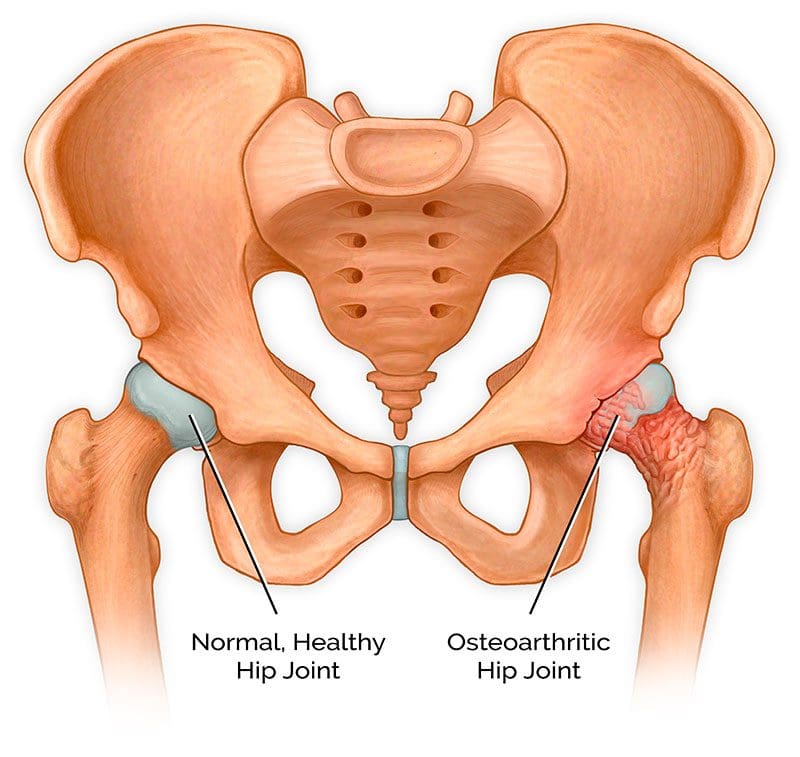
The hips provide stability to the upper and lower parts of the body. While supporting the weight of the upper half and movement to the lower half, the hips can succumb to wear and tear in the body. When the hip joints begin to wear and tear slowly, it can lead to the progression of hip osteoarthritis, where the cartilage of the joints begins to cause the bones to rub against each other, triggering inflammation. Hip osteoarthritis makes diagnosing difficult because the referred pain from the spine, knees, or groin area overlaps the symptoms. All is not lost, as there are available treatments to manage hip osteoarthritis that can help slow the progress of this disorder and bring back the mobility of the lower half of the body.
References
Ahuja, Vanita, et al. “Chronic Hip Pain in Adults: Current Knowledge and Future Prospective.” Journal of Anaesthesiology, Clinical Pharmacology, Wolters Kluwer – Medknow, 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8022067/.
Chamberlain, Rachel. “Hip Pain in Adults: Evaluation and Differential Diagnosis.” American Family Physician, 15 Jan. 2021, https://www.aafp.org/pubs/afp/issues/2021/0115/p81.html.
Khan, A M, et al. “Hip Osteoarthritis: Where Is the Pain?” Annals of the Royal College of Surgeons of England, U.S. National Library of Medicine, Mar. 2004, https://pubmed.ncbi.nlm.nih.gov/15005931/.
Kim, Chan, et al. “Association of Hip Pain with Radiographic Evidence of Hip Osteoarthritis: Diagnostic Test Study.” BMJ (Clinical Research Ed.), BMJ Publishing Group Ltd., 2 Dec. 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4667842/.
Sen, Rouhin, and John A Hurley. “Osteoarthritis – Statpearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 1 May 2022, https://www.ncbi.nlm.nih.gov/books/NBK482326/.
Maintaining healthy joints is crucial to preventing injuries from affecting the body. Incorporating physical activities, eating healthy foods, staying hydrated, and getting a routine check-up are ways to ensure that the body is functional, including the joints. The joints in the body act like shock absorbers that soften the impact of any injuries that the body has sustained. However, as the body ages, so do the joints, causing them to become hardened and cause problems in the body. In today’s article, we will look at sacroiliac dysfunction, what issues it affects besides back pain, and how chiropractic care manages sacroiliac dysfunction. We refer patients to certified providers specializing in musculoskeletal therapies to help those with sacroiliac dysfunction. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
What Is Sacroiliac Dysfunction?
Are you experiencing pain in the pelvis? Do your hips seem tighter than usual? Do you feel muscle stiffness when you twist from side to side? Some of these issues are signs that you might be experiencing sacroiliac dysfunction. Around the pelvic region lies the sacroiliac joint, a weight-bearing solid joint connecting the pelvis to the sacrum. It is surrounded by tough ligaments that support the body as it distributes the weight from the upper body to the lower body. However, like all the other joints in the body, any injury or condition can cause this joint to be unstable and succumb to the pain, causing sacroiliac dysfunction. Sacroiliac dysfunction or sacroiliac joint pain is defined as one of the potential causes of axial low back pain. When there are issues affecting the sacroiliac joints, it’s associated with about a quarter of most low back pain cases. This is due to the problems that overlap with pain associated with the low back. Studies reveal that dysfunction in the sacroiliac joint can relate to leg or back pain, making diagnosing the problem difficult. Back pain associated with sacroiliac dysfunction causes the pelvis to be hypermobile, causing the risk of developing radiating groin pain. Leg pain associated with sacroiliac dysfunction causes muscle tension and stiffness to the low back, legs, or buttock region, mimicking sciatica-like symptoms.
What Other Issues Does It Affect?
Many individuals may not realize that when they are experiencing sacroiliac dysfunction, symptoms show that they overlap with lumbar spine pathologies. However, sacroiliac dysfunction can also affect the pelvic region of the body. Studies reveal that when the muscles around the body’s pelvic area become inflamed or irritated, it can cause stiffness in the sacroiliac joints, thus developing the risk of pelvic pain. Pelvic pain is usually defined as non-menstrual pain that causes functional disability to the lower extremities. Around the pelvic region, the lower sacral nerves provide extensive neurologic connections to the structures throughout the pelvic area that maintain normal pelvic organ function. When issues like sacroiliac dysfunction become the risk of pelvic pain, it may potentially involve pelvic symptoms like constipation. Studies reveal that constipation is significantly associated with a high prevalence of pelvic organ prolapse and low urinary tract symptoms. Other issues that sacroiliac dysfunction correlates with are:
Ankylosing spondylitis
Rheumatoid arthritis
Inflammatory issues
Hip pain
Pelvic pain
Low back pain
Piriformis syndrome
An Overview Of Sacroiliac Joint Pain- Video
Are you experiencing radiating from your lower back down to your leg? How about stiffness in your hips? Are you feeling constipated or have a sense of fullness in your bladder? You may suffer from sacroiliac dysfunction in your pelvic region if you notice these symptoms. The video above explains how to understand sacroiliac joint pain. The sacroiliac joint connects the pelvis and sacrum, surrounded by tough ligaments and muscles that help support the body by distributing weight from the upper body to the lower body. When issues affect the sacroiliac joints can overlap other risk profiles like low back pain, leg pain, and pelvic pain. This can make diagnosing sacroiliac dysfunction difficult because the symptoms are similar to other issues. For example, hip pain is associated with piriformis syndrome while potentially being involved with sciatica. How would hip pain be correlated with piriformis syndrome? The piriformis muscle can become overused and injured and can entrap the sciatic nerve (which runs from the lumbar spine, through the hips, and down to the leg), causing radiating, throbbing pain. Other times referred pain in the low back can affect different areas in the body due to sacroiliac dysfunction. Luckily, there are treatments available to manage sacroiliac dysfunction.
How Chiropractic Care Manages Sacroiliac Dysfunction
When issues of sacroiliac dysfunction become associated with leg or back pain, physicians often misdiagnose it as a soft tissue issue rather than a joint issue. Many doctors might rule out various medical conditions before including sacroiliac dysfunction as part of the diagnosis. Some treatments like massage therapy can help loosen up the tight muscles surrounding the joints relieving the pain and discomfort. At the same time, chiropractic care utilizes spinal manipulation and mobilization to the affected spinal area. Since the sacroiliac joint is an essential part of the musculoskeletal system, chiropractors specialize in this area. Through practical, non-invasive methods, chiropractic care has proven to not only relieve pain in the spine but can also help rehabilitate the spine. Chiropractors are specially trained to guide the individual through several phases of care that help loosen the stiff muscles and strengthen the joints. Chiropractic care will help decrease the pain from returning to the body and let the individual return to their health and wellness journey.
Conclusion
Maintaining healthy joints is crucial to prevent injuries from affecting the body. The sacroiliac joints are part of the musculoskeletal system that connects the pelvic bone to the sacrum. This joint is surrounded by tough ligaments and muscles that support the upper and lower half of the body through weight distribution. When the sacroiliac joint becomes unstable, it can succumb to pain, thus becoming sacroiliac dysfunction. Sacroiliac dysfunction sometimes mimics low back and leg pain, making it difficult to diagnose. Co-morbidities like pelvic pain correlate to sacroiliac dysfunction, causing somato-visceral pain in different body areas. Treatments like chiropractic care can help strengthen the stiff muscles and joints in the body through spinal manipulation and mobilization in practical, non-invasive treatment. Chiropractic care can help rehabilitate the spine while decreasing the pain from returning to the body.
References
Jonely, Holly, et al. “Chronic Sacroiliac Joint and Pelvic Girdle Dysfunction in a 35-Year-Old Nulliparous Woman Successfully Managed with Multimodal and Multidisciplinary Approach.” The Journal of Manual & Manipulative Therapy, Maney Publishing, Feb. 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4459139/.
Raj, Marc A, et al. “Sacroiliac Joint Pain.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 12 Feb. 2022, https://www.ncbi.nlm.nih.gov/books/NBK470299/.
Singh, Prashant, et al. “Pelvic Floor Symptom Related Distress in Chronic Constipation Correlates with a Diagnosis of Irritable Bowel Syndrome with Constipation and Constipation Severity but Not Pelvic Floor Dyssynergia.” Journal of Neurogastroenterology and Motility, Korean Society of Neurogastroenterology and Motility, 31 Jan. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6326213/.
The muscles in our body help us be active when we want to be, rest and repair after activities, and continue to provide everyday movements that help keep the body functioning correctly. For athletes and the general population, physical training and eating healthy foods help deliver fuel to not only the internal organs but also help support the muscles, ligaments, and skeletal joints from injuries. As many individuals start to think about their health and wellness, many factors tend to pop up that can cause them to halt their health and wellness journey. Issues like stress, accidents, traumatic events, and lifestyle habits can affect the body and, over time, can become the risk of developing into chronic problems. An example would be where a person is experiencing hip pain associated with piriformis syndrome. Today’s article looks at piriformis syndrome, how it can cause more than hip pain, and how there are available treatments for piriformis syndrome. We refer patients to certified providers specializing in musculoskeletal therapies to help those with piriformis syndrome. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
What Is Piriformis Syndrome?
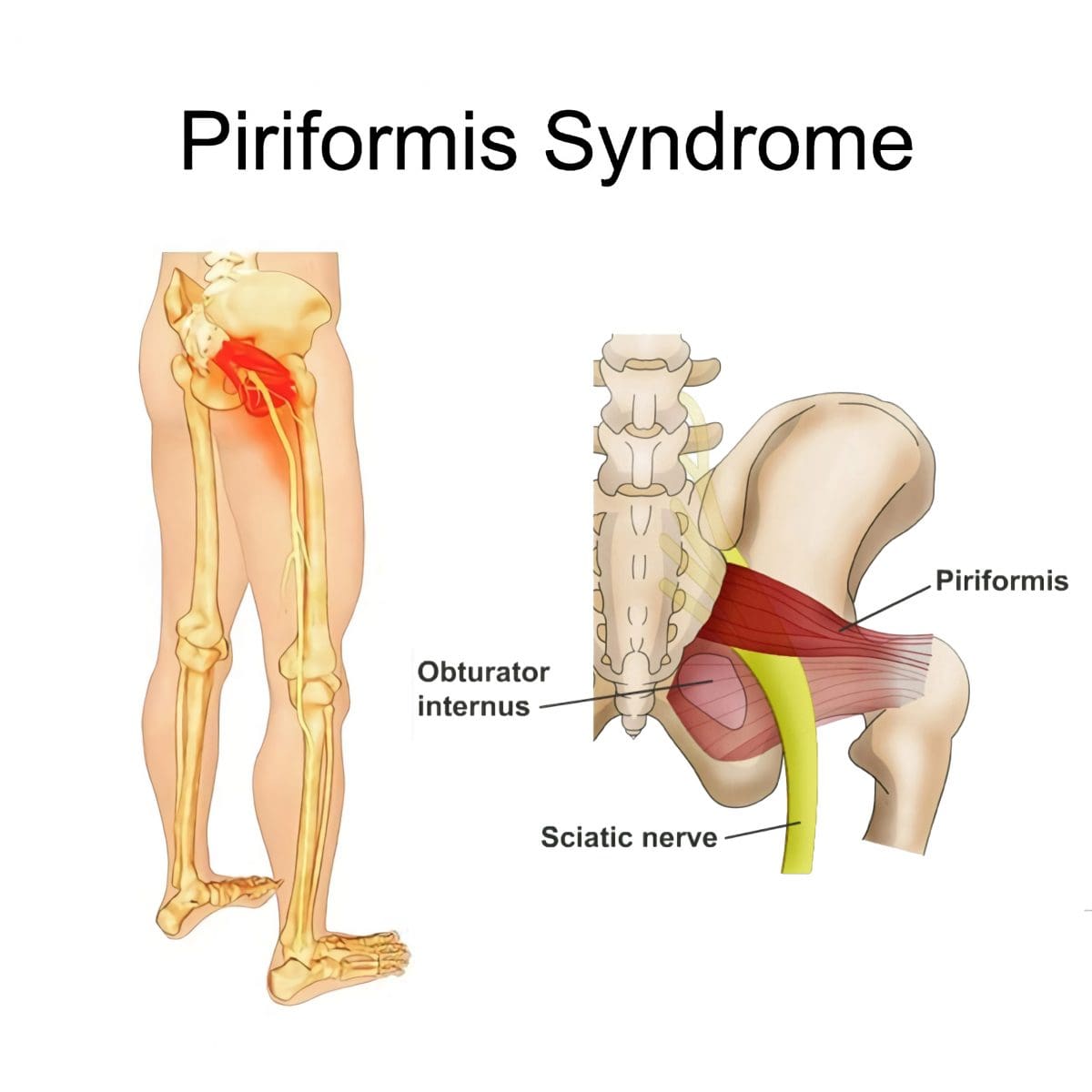
Have you been experiencing pain radiating from the buttock down to your legs? Does it hurt when you are sitting down? Or are you feeling tingling sensations and numbness on your butt and thighs? Some of these symptoms might be signs that you might be experiencing piriformis syndrome. Research studies have defined piriformis syndrome as a clinical condition where everyday stress affecting the body causes the piriformis muscle (the small muscle deep in the buttock region) to become tight and irritates the sciatic nerve. When that sciatic nerve becomes aggravated, it can become the risk of developing into sciatica. Many individuals don’t realize that the sciatic nerve also gets affected when their piriformis muscles in the buttock region become overused and tight through strenuous activities. This is due to the belief that any unusual traumatic abnormality in the piriformis muscle will be associated with sciatica symptoms. However, when a person is experiencing buttock pain that travels down the leg caused by the affected piriformis muscle, many will rule out some of the more common causes of sciatica like nerve root impingement triggered by disc herniation.
Surprisingly, three primary causing factors can be associated with piriformis syndrome. The first causing factor is myofascial trigger points may be the results of referred pain (pain or discomfort from another body location). The second causing factor is nerve entrapment against the greater sciatic foramen passing through the various piriformis muscles. And finally, the third causing factor is sacroiliac joint dysfunction due to piriformis muscle spasm. Studies reveal that the piriformis muscle helps stabilize the sacroiliac joint; when the small muscle starts to become irritated, it causes pain in the buttock region. But how does sacroiliac dysfunction relates to piriformis syndrome? Well, since low back pain is associated with sacroiliac dysfunction, the pain will often radiate down to the knee and the groin muscles while becoming a risk of developing piriformis syndrome.
Piriformis Syndrome Causes More Than Hip Pain?
Due to its broad size in the greater sciatic foramen, the piriformis muscle can become overused and tight, thus becoming piriformis syndrome. Piriformis syndrome can also become a risk to the numerous vessels and nerves that exit out in the pelvis region and may become compressed, causing more than just hip pain. Studies reveal that piriformis syndrome may be masquerading as ischiofemoral impingement triggering extra-articular hip pain by entrapping the quadratus femoris muscle causing groin pain. Another cause that piriformis syndrome is associated with is chronic pelvic pain. How does chronic pelvic pain correlate with piriformis syndrome? Chronic pelvic pain is a non-cyclic pain localized in the pelvis, potentially involving the surrounding muscles like the piriformis muscle supporting the irritated hip joint and pelvis region. Piriformis syndrome could also be an overlapping condition risk of developing other health issues like fibromyalgia in many people. Some conditions have common symptoms associated with piriformis syndrome, including:
Tingling sensations
Numbness
Muscle tenderness
Pain while sitting
Discomfort while exercising
The Difference Between Sciatica & Piriformis Syndrome-Video
Have you found it challenging to be comfortable while sitting down doing leisure activities? How about radiating pain that travels down your leg? Or do your hips feel tight and stiff? Experiencing these symptoms means that you might suffer from piriformis syndrome. The video above explains the difference between piriformis syndrome and sciatica. Studies reveal that piriformis syndrome is classically defined as sciatic pain; however, it is not sciatica. Sciatica is caused by compressed sciatic nerve due to herniated disc in the lumbar spine. In contrast, piriformis syndrome is caused when a traumatic injury or an underlying condition causes the piriformis muscle to spasm and aggravate the sciatic nerve. Various factors like prolonged sitting, repetitive movements that involve the legs, and even extensive stair climbing can cause the piriformis muscle to be easily damaged or injured, causing piriformis syndrome. Fortunately, there are ways to alleviate sciatic nerve pain and improve piriformis syndrome.
Treatments Available For Piriformis Syndrome
Many treatments are accessible to manage the pain and discomfort caused by piriformis syndrome for suffering individuals. Some people take over-the-counter medicine to decrease the pain, while others utilize a hot/cold pack on the affected area to relieve discomfort. The symptoms associated with piriformis syndrome usually go away without any additional treatment; however, if the pain or discomfort is still there, many people might benefit from alternative options for treatment, like chiropractic care, physical therapy, or even spinal decompression. Whether it is through gentle stretching, spinal manipulation, or decompression, these treatments are for anyone dealing with piriformis syndrome and its associated symptoms. Physical therapy can help decrease the painful symptoms associated with piriformis syndrome through gentle stretches that help return a person’s range of motion. Chiropractic care incorporates spinal adjustments and manual manipulations to treat various injuries or conditions. Spinal decompression uses traction to gently pull on the spine to release the aggravated nerve from causing pain. The relief can gradually restore a person’s natural health while managing its associated symptoms with various treatments available for individuals with piriformis syndrome.
Conclusion
Piriformis syndrome is a condition where everyday stress affects the piriformis muscle in the buttock region to become irritated and tight while aggravating the sciatic nerve. Many think traumatic abnormalities affecting their piriformis muscle will be associated with sciatica symptoms. However, sciatica is due to nerve root compression triggered by disc herniation. Piriformis syndrome is where that small muscle is overused from various factors that cause more than hip and butt pain. Some overlapping conditions associated with piriformis syndrome can become mediators for groin and pelvic pain. Fortunately, chiropractic care, physical therapy, and decompression can help restore the body gradually by managing piriformis syndrome and its associated symptoms.
References
Hicks, Brandon L., et al. “Piriformis Syndrome.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 21 Apr. 2022, https://www.ncbi.nlm.nih.gov/books/NBK448172/.
Newman, David P, and Liang Zhou. “Piriformis Syndrome Masquerading as an Ischiofemoral Impingement.” Cureus, Cureus, 16 Sept. 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8520408/.
Professionals, Northwest Medical. “Piriformis Syndrome/Sacroiliac Dysfunction.” Northwest Medical Center, 2021, https://nw-mc.com/piriformis-syndromesacroiliac-dysfunction/.
Ro, Tae Hoon, and Lance Edmonds. “Diagnosis and Management of Piriformis Syndrome: A Rare Anatomic Variant Analyzed by Magnetic Resonance Imaging.” Journal of Clinical Imaging Science, Medknow Publications & Media Pvt Ltd, 21 Feb. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5843966/.
The body is a marvelous functional machine that requires constantly moving worldwide. The body can do everyday movements from the head to the feet and be in weird positions without feeling pain. However, ordinary factors like natural aging, wear and tear, and issues affect the body over time. When these factors start to affect the body, they can cause unwanted symptoms that can inflict pain on specific areas around the body. Some areas that suffer pain include the hips, lower back, neck, the body’s internal systems, and the spine, causing the individual to be miserable. Luckily many treatments do relieve pain in the body and help dampen the effects of the unwanted symptoms that are hindering the individual. Today’s article focuses on hip pain, its symptoms, and how decompression therapy can help many individuals suffering from hip pain. By referring patients to qualified and skilled providers specializing in spinal decompression therapy. To that end, and when appropriate, we advise our patients to refer to our associated medical providers based on their examination. We find that education is the key to asking valuable questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions, please call Dr. Jimenez at 915-850-0900.
What Is Hip Pain?
Are you feeling stiffness from your lower back and hips? Do your hips hurt after falling due to playing sports? How about pain from the lower back to the hips down to the feet? You might be experiencing hip pain. Research studies have stated that hip pain can be associated with many factors that can cause many individuals to be in distress, impair their daily activities, and affect their quality of life. Hip pain can be associated with simple movements that are damaged, like sitting and standing, which can be hard after a while. Other associations that hip pain can occur can be lower back pain, neuropathies, herniation, or chronic pain. According to research studies, hip pain is considered a musculoskeletal disorder. It shows that posterior hip pain in adults is caused by osteoarthritis or traumatic causes like sacral stress fractures that can affect the hips. This musculoskeletal disorder can become a problem for many older adults suffering from hip issues.
The Symptoms
Research studies have found that hip pain is a musculoskeletal complaint affecting young and old adults. Since hip pain is associated with various chronic issues, it can cause many individuals to be miserable and be in constant pain. For adults, hip pain can be one of the issues for those suffering from osteoarthritis in the anterior hip region. As research shows, in the posterior hip region, hip pain can be associated with chronic conditions like piriformis syndrome and lumbar radiculopathy that are centralized in the lower back. Other symptoms that hip pain cause on its own do associate with other chronic conditions, including:
Are you experiencing discomfort from your hips while sitting or standing? How about sharp, throbbing pain coming from your lower back and affecting your hips and legs? Do you feel tenderness and swelling on your joints? These symptoms are various forms of hip pain, and lumbar traction can help lower hip pain symptoms. The video above mentions how to prepare for lumbar traction therapy and how it can alleviate symptoms caused by hip pain. Lumbar traction helps compressed disc in the lumbar region of the spine to be restored to its original state and even takes the pressure off the sciatic nerve and other nerve roots that are causing hip pain to the body. Utilizing traction therapy increases the disc height and allows the lumbar spinal discs to be rehydrated again. Suppose you want to learn more about lumbar traction or decompression and how it can benefit you? In that case, this link will explain what decompression does for the lumbar area in the spine and provide relief from hip pain and its associates.
How Decompression Therapy Helps With Hip Pain
Since hip pain is associated with various other conditions that can affect the body, the most common condition that the body has suffered from is low back pain. There are ways to treat hip and low back pain; some individuals utilize heat and ice to neutralize the pain to go away, and others use chiropractic therapy to get the joints to realign themselves. One of the treatments used to relieve hip and low back pain is decompression therapy. Research studies have found that decompression therapy is safe and effective in helping to improve the blood circulation to the hips to provide relief to the hips. Since hip pain is associated with low back pain, decompression allows the herniated discs to be taken off the nerves surrounding the hips and provide pain relief. Other research studies show that traction is used to create negative gravity pressure to help reduce the pressure that is causing pain to the soft tissues and the nerve roots. This negative gravity allows the spine to separate and create more height for the disc to rehydrate while relieving the individual.
Conclusion
Overall the body is a marvelous machine that has the ability to move without pain. When issues start to affect the body, like the hips and lower back, it can cause the individual to suffer from various forms of pain. Since hip pain is associated with low back pain, it can lead to other chronic issues like sciatica or osteoarthritis, affecting the joints and causing them to swell. Treatments like decompression or traction therapy are used to alleviate the pain caused by the hips or lower back. When people incorporate decompression or traction into their wellness journey, they relax a bit as they are laid down and have their spine stretched slowly. This will cause them relief and take the pressure off the nerve roots that are sending pain signals to the brain. This ensures them that they can take back their lives pain-free.
References
Ahuja, Vanita, et al. “Chronic Hip Pain in Adults: Current Knowledge and Future Prospective.” Journal of Anaesthesiology, Clinical Pharmacology, Wolters Kluwer – Medknow, 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8022067/.
Battaglia, Patrick J, et al. “Posterior, Lateral, and Anterior Hip Pain Due to Musculoskeletal Origin: A Narrative Literature Review of History, Physical Examination, and Diagnostic Imaging.” Journal of Chiropractic Medicine, Elsevier, Dec. 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5106442/.
Choi, Jioun, et al. “Influences of Spinal Decompression Therapy and General Traction Therapy on the Pain, Disability, and Straight Leg Raising of Patients with Intervertebral Disc Herniation.” Journal of Physical Therapy Science, The Society of Physical Therapy Science, Feb. 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4339166/.
Lee, Yun Jong, et al. “Causes of Chronic Hip Pain Undiagnosed or Misdiagnosed by Primary Physicians in Young Adult Patients: A Retrospective Descriptive Study.” Journal of Korean Medical Science, The Korean Academy of Medical Sciences, 11 Dec. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6300658/.
Wilson, John J, and Masaru Furukawa. “Evaluation of the Patient with Hip Pain.” American Family Physician, U.S. National Library of Medicine, 1 Jan. 2014, https://pubmed.ncbi.nlm.nih.gov/24444505/.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine