Healthy Diet: It’s hard to turn on the television or cruise the internet without being bombarded with headlines about “Americans don’t sleep enough” or “one third of adults are obese.”
While stress, heredity, and smoking are all factors that play into a person’s well being, one of the biggest is a healthy diet. Choosing to eat healthy benefits the body in a number of key areas. Still gobbling up the pizza and slurping down the diet soda, unconvinced? See if these eight points about a healthy diet change your mind.
1. Healthy Diet Strengthens & Improves Muscle Function
Healthy muscles carry us where we want to go. The right foods, along with proper exercise, build and maintain muscle mass, maintaining strength and mobility.
2. Promotes A Longer Life
Feeding your body what it needs can add years to your life. Reducing stress is one way to promote health, and a healthy diet is another. Foods rich in minerals and vitamins build up every cell in your body, preparing it to fight illness and stay alive longer.
3. Enables Richer Years
An individual who is healthy maintains a higher level of physical activity and brain function than their less healthy peers. A stronger body provides a richer life with more unique experiences.
4. Makes You Prettier
If you won’t eat healthy for your insides, maybe a better outside will motivate some dietary changes. We all want to be physically attractive. Healthy foods contribute to clear skin and shiny hair that no amount of high priced beauty products provides. Fueling the body with rich omega fatty and other healthy foods nourishes skin, hair, and nails.
5. Makes You Smarter
Research shows certain dietary choices power up your brain to function at a higher level, and help everyday brain function. Introducing “brain foods” into your diet aid with memory retention and problem solving skills.
This is one of the best reasons to commit to a healthy diet of vitamin-rich foods, as a healthy brain allows a much more active and independent lifestyle, from working longer to being able to drive.
6. Decreases Your Injury Risk
A high-functioning body with strong bones and muscles maintains balance, handles heavy loads, and holds up under stress better than its weaker counterparts. Muscles and bones lacking calcium and protein over time grow weaker.
This, unfortunately, causes the body to be less stable and more prone to injury. Falls, slips, and twists end up with more serious injuries if a person’s body isn’t strong and healthy.
7. Fights Bad Genes
If you are already worried about the cancer that runs on mom’s side or the heart attack risk that runs on dad’s side, take heart. While you can’t change your DNA, you can use a healthy diet to combat some of your genetic disposition to disease.
Ingraining a healthy diet into your life, as well as exercise and regular doctor checkups, helps minimize the risk of falling victim to your family’s predisposed illnesses.
If you end up with an illness, whether or not from heredity, a healthy diet….
8. Prepares You To Fight Illness
A nutrient-rich diet boosts a person’s immune system to be able to fight off infection and illness. When a person falls victim to a disease or other medical condition, their diet helps them fight it off so it hopefully doesn’t get worse and is cured quickly.
A healthy diet is integral to a long, happy life. Deciding to eat healthy and maintain that commitment consistently may seem like a big change in lifestyle at first, but it will benefit you and your loved ones in ways that are practically immeasurable.
Tips For Preventing Dehydration
This article is copyrighted by Blogging Chiros LLC for its Doctor of Chiropractic members and may not be copied or duplicated in any manner including printed or electronic media, regardless of whether for a fee or gratis without the prior written permission of Blogging Chiros, LLC.
Wellness Chiropractor, Dr. Alexander Jimenez takes a look at discussing nutrition with patients in a clinical setting.
How Clinicians Can Do Better
Despite overwhelming evidence that relatively small dietary changes can significantly improve health, clinicians seldom discuss nutrition with their patients. Poor nutritional intake and nutrition-related health conditions, such as cardiovascular disease (CVD), diabetes, obesity, hypertension, and many cancers, are highly prevalent in the United States,1 yet only 12% of office visits include counseling about diet.2 Even among high- risk patients with CVD, diabetes, or hyperlipidemia, only 1 in 5 receive nutrition counseling.2 It is likely that many patients receive most of their nutrition information from other, and often unreliable, sources.
These data may reflect the minimal training, time, and reimbursement allocated to nutrition counseling (and preventive services in general) in clinical practice.3 Most physicians and other health care professionals receive limited education on nutrition in medical school (or other professional schools) or in postgraduate training. Just 25% of medical schools offer a dedicated nutrition course, a decline since the status of nutrition education in US medical schools was first assessed in 1985, and few medical schools achieve the 30 hours of nutrition education recommended by the National Academy of Sciences.4 As a result, physicians report inadequate nutrition knowledge and low self-efficacy for counseling patients about diet.3 In addition, time pressures, especially in primary care, limit opportunities to counsel on nutrition or address preventive issues beyond patients� acute complaints. Lack of time is frequently cited as the greatest barrier to counseling on nutrition and obesity.3
Moreover, nutrition and behavioral counseling have traditionally been non-reimbursed services. Few state Medicaid programs cover nutrition or obesity counseling, and before 2012, Medicare explicitly excluded coverage for obesity counseling; although now a reimbursed service for Medicare beneficiaries, just 1% of eligible Medicare beneficiaries receive this counseling.5 Dietitian counseling is also excluded by Medicare, unless patients have diabetes or renal disease. Although the Affordable Care Act mandates coverage for services graded A or B by the US Preventive Services Task Force, including nutrition counseling for patients with CVD risk factors and obesity counseling for patients with a body mass index of 30 or greater, existing private health insurance benefits are in- consistent, and the covered services are often unclear to both clinicians and patients, thereby limiting use.
Furthermore, health behavior change counseling is often frustrating given the current food environment, in which less nutritious foods tend to be less expensive, larger portioned, more easily accessible, and more heavily marketed than healthier options, making patient adherence 6 to nutrition advice challenging. Conflicting and confusing nutrition messages from popular books, blogs, and other media further complicate patient decision making.
Despite these unfavorable trends, there has been progress in this area. The evidence base supporting the benefits of nutrition intervention and behavioral counseling is expanding. Renewed focus on nutrition education in health care professional training is being driven by both student demand and the health care system. Although time pressures and reimbursement remain impediments, incentives and reimbursement options for nutrition and behavioral counseling are growing, and value-based care and health care team approaches hold promise to better align time demands and incentives for long-term care management. Initiatives to integrate clinical care and community resources offer opportunities to leverage resources that alleviate the clinician�s time commitment. There is evidence of some success; for instance, the amount of sugar-sweetened beverages consumed by individuals in the United States has declined substantially over the past 10 years.7
Clinicians can take the following reasonable steps to include nutrition counseling into the flow of daily practice:
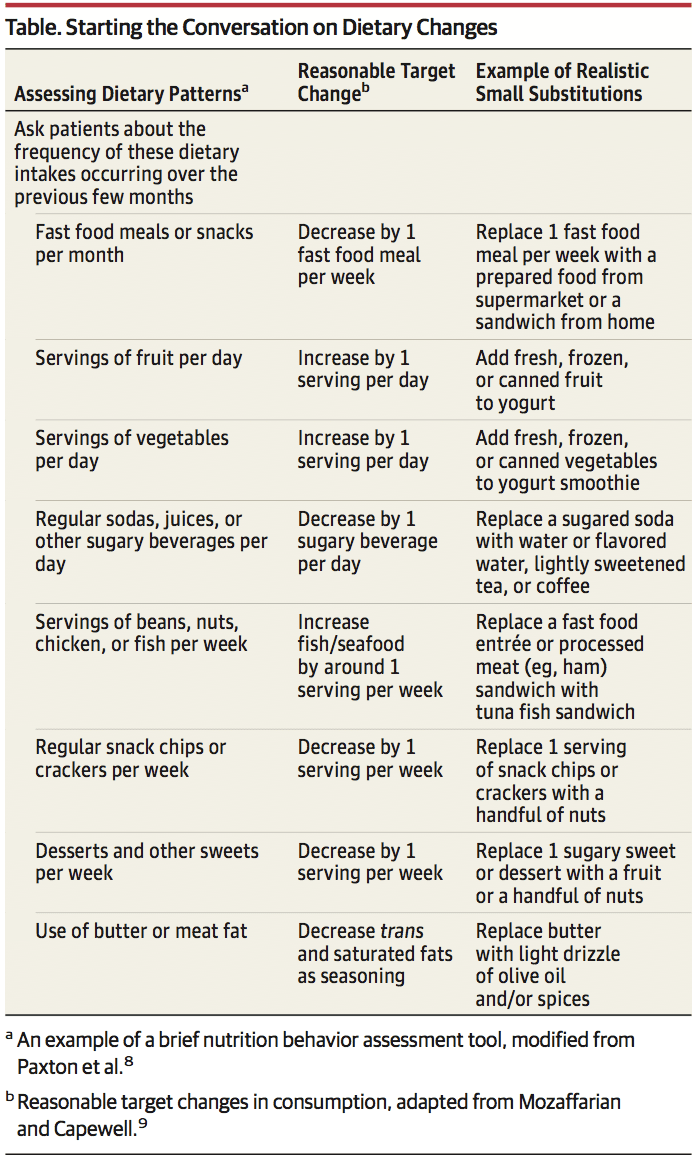
1. Start the conversation. Several short, validated screen- ing questionnaires are available to quickly assess need for nutrition counseling, such as the Starting the Conversation tool8 (Table). This approach can be efficiently used prior to seeing the patient at an appointment, either delivered by medical assistants as part of vital sign assessment or as prescreening paperwork for patients to complete online or in the waiting room.
2. Structure the encounter.�Using methods such as the �5 A�s� (assess, advise, agree, assist, arrange), which has been adapted from tobacco counseling. Motivational interviewing, which has documented efficacy in numerous behavior change settings, is particularly helpful to engage patients who are not yet committed or are hesitant to consider behavioral change.
3. Focus on small steps. Changing lifelong nutrition behaviors can seem overwhelming, but even exceedingly small shifts can have an effect (Table). For example, increasing fruit intake by just 1 serving per day has the estimated potential to reduce cardiovascular mortality risk by 8%, the equivalent of 60 000 fewer deaths annually in the United States and 1.6 million deaths globally.9 Other examples include reducing intake of sugar-sweetened beverages, fast food meals, processed meats, and sweets, while increasing vegetables, legumes, nuts, and whole grains. Emphasize to patients that every food choice is an opportunity to accrue benefits, and even small ones add up. Small substitutions still allow for �treats,� such as replacing potato chips and cheese dip with tortilla chips and salsa, the latter lowering trans fats and saturated fat and increasing whole grain and vegetable intake (Table).
4. Use available resources. Numerous extracurricular resources are readily available for clinicians. The Nutrition in Medicine program offers online, evidence-based nutrition education and tutorials for clinicians and an online, core nutrition curriculum for medical students. The Dietary Guidelines for Americans offers evidence- based and freely available nutrition guidance, tutorials, and tools for clinicians and patients alike. A companion website, Choose My Plate, offers nutrition and counseling advice for clinicians and handy resources for patients, including recently added videos with useful examples of small substitutions that patients will appreciate.
5. Do not do it all at once. Expecting to create long-term behavioral change during a single episode of care is a recipe for frustration and failure, for both the patient and clinician. Empowering and sup- porting patients is an ongoing process, not a 1-time curative event. Use a few minutes at the close of a patient visit to identify opportunities for future counseling, offer to serve as a resource, and be- gin a discussion and support that can be reinforced over time. Take solace in knowing that small initial steps can quickly improve health; for example, reducing trans fats at a single meal (eg, replacing baked goods with fruit or nuts or fried foods with non-fried alternatives) promptly improves endothelial function.10
6. Do not do it all alone.�The primary care physician need not be the sole clinician who provides nutrition counseling. Proactive use of physician extenders (eg, physician assistants, nurses, medical assistants, and health coaches) and referrals can alleviate much of the burden for the busy clinician. Receptionists can distribute assessment and screening questionnaires for patients to complete in the waiting room; medical assistants can document behavioral change progress while assessing vital signs; administrative staff can identify and con- tact patients who are overdue for interaction. Large practices may benefit from including nutrition or health coaches on staff. Referring to clinical specialists and community-based support programs can significantly extend the clinician�s reach.7 In addition to registered dietitians, numerous clinical and community resources are available and often covered by insurance plans. Board-certified obesity medicine specialists, certified diabetes educators, and physician nutrition specialists are available as referrals in many areas. Diabetes Prevention Program group counseling sessions are now covered by Medicare and available throughout communities, such as in many YMCA sites, and electronically.
Summary
Although there is no conclusive evidence that these steps will improve diet and health outcomes for patients, there is virtually no harm in counseling and the potential gains, especially at the population level, are substantial. Nutrition and health behavior change must become a core competency for virtually all physicians and any other health professionals working with patients who have or are at risk for nutrition-related chronic disease.
A Healthier You
Scott Kahan, MD, MPH Department of Health Policy and Management, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland; and George Washington University School of Medicine, Washington, DC.
JoAnn E. Manson, MD, DrPH Department of Medicine, Brigham and Women’s Hospital and Harvard Medical School, Boston, Massachusetts; and Department of Epidemiology, Harvard T. H. Chan School of Public Health, Boston, Massachusetts.
ARTICLE INFORMATION
Published Online: September 7, 2017. doi:10.1001/jama.2017.10434 Conflict of Interest Disclosures: All authors have
completed and submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest and none were reported.
REFERENCES
1. Ward BW, Schiller JS, Goodman RA. Multiple chronic conditions among US adults: a 2012 update. Prev Chronic Dis. 2014;11:E62.
2. Office of Disease Prevention and Health Promotion. Healthy People 2020. https://www.healthypeople.gov/2020/data-search/Search-the-Data#srch=nutrition. Accessed January 23, 2017.
3. Kolasa KM, Rickett K. Barriers to providing nutrition counseling cited by physicians. Nutr Clin Pract. 2010;25(5):502-509.
4. Adams KM, Kohlmeier M, Zeisel SH. Nutrition education in U.S. medical schools: latest update of a national survey. Acad Med. 2010;85(9):1537-1542.
5. Batsis JA, Bynum JPW. Uptake of the Centers for Medicare and Medicaid obesity benefit: 2012-2013. Obesity (Silver Spring). 2016;24(9):1983-1988.
6. Kahan S, Cheskin LJ. Obesity and eating behaviors and behavior change. In: Kahan S, Gielen AC, Fagan PJ, Green LW, eds. Health Behavior Change in Populations. Baltimore, MD: Johns Hopkins University Press; 2014:chap 13.
7. Rehm CD, Pe�alvo JL, Afshin A, Mozaffarian D. Dietary intake among US adults, 1999-2012.JAMA. 2016;315(23):2542-2553.
8. Paxton AE, Strycker LA, Toobert DJ, Ammerman AS, Glasgow RE. Starting the conversation performance of a brief dietary assessment and intervention tool for health professionals. Am J Prev Med. 2011;40(1):67-71.
9. Mozaffarian D, Capewell S. United Nations� dietary policies to prevent cardiovascular disease. BMJ. 2011;343:d5747.
10. Williams MJA, Sutherland WHF, McCormick MP, de Jong SA, Walker RJ, Wilkins GT. Impaired endothelial function following a meal rich in used cooking fat.J Am Coll Cardiol. 1999;33(4):1050-1055
Food writer and author of The Goodness of Nuts & Seeds, Natalie Seldon has this advice for refreshing your diet this spring�
EAT THE RAINBOW
Sweep away the dull winter with spring�s colourful fruits and vegetables; a great way to load up on fibre, vitamins and other disease-fighting compounds. The pigments that give fruits and vegetables their colour are vital antioxidants. Include three or more colours in each meal; scramble eggs with spinach and red pepper, add strawberries and apricots to green salads, brighten up sandwiches with shredded carrot and rocket, and blend blueberries, peaches and banana into smoothies.
SLOW EATING
Make a commitment to regularly preparing fresh food and eating it at the table � cute placemats and all. Firstly, you�re worth it. Secondly, your body will thank you. Eating in front of the TV significantly increases your calorie intake, plus nutritional research evidence shows that eating out, or relying on ready-meals are almost always more likely to provide higher mounts of salt, unhealthy fats and calories than a meal you prepare yourself. Plus, once you have the store cupboard essentials, you�ll actually save money prepping at home. Bonus!
GET YOUR CRUNCH ON
Nourish yourself by including one of the hottest health trends of 2017, nuts and seeds to your diet. These versatile little guys pack a powerful nutritional punch, being high in healthy fats, fi bre and calcium, whilst providing an abundance of antioxidants and minerals. And just to help matters, their gratifying versatility and moreish richness lend themselves to a myriad of both�savoury and sweet dishes, allowing us to conjure up all kinds of culinary magic on any given day. My new book The Goodness of Nuts & Seeds is full of simple and delicious recipe ideas. (Available now via Amazon, most book stockists and Chic et Tralala, Hollybush, Sevenoaks).
VEG FOCUS
It�s official, the healthiest diets in the world have one very important thing in common � they�re all based on plant foods rather than meat. Overwhelming evidence from studies around the world proves that plant foods are your most powerful allies in protecting against several lifestyle-related diseases such as diabetes, obesity and heart disease. Veganism has surged by 35% and is gaining serious momentum. Eating a diet high in veggies, beans, fruits and healthy oils, as well as fish and whole grains � aka the Mediterranean diet � is good for your brain as well as your bod. Shift towards a plant based diet by swapping legumes, meaty veg and tofu for animal products a few meals per week, or try meat-free Monday.
GO GREEN
Using fresh herbs is a great way to add extra flavour to your meals along with getting plenty of health benefits. For example coriander helps remove heavy metals from the body, parsley is rich in immune boosting vitamin C, and rosemary and sage are excellent memory enhancers. Fill your cupboards with healthy alternatives and buy seasonal produce as they are more likely to be even more nutrient dense, as well as more affordable.
FRESH START
Start your day off right with a glass of water and a freshly squeezed lemon or lime. This is a fantastic way to improve your digestion, alkalize your body, and boost your vitamin C levels to support healthy immune function and radiant skin.
EAT YOUR WORDS
To change the way you think about food and bring the joy back into eating, you need to rethink the way you talk about it. Referring to any food as �good� or �bad� has no place in a healthy, balanced approach to eating. As a food writer, I know many people struggle to make peace with eating certain foods as we are programmed by the world around us to use powerful language to describe a range of food we eat. Indeed, an interesting change happens when you remove these negative connotations � you don�t feel the need to hastily shovel food in, or go back for seconds before your conscience catches up with you. You actually enjoy these foods even more, and therefore require them less. Win win!
A Natural Cholesterol-Lowering Supplement Red Yeast Rice Poses Same Health Risks As Statin Drugs
a new study contends.
Red yeast rice could increase risk of muscle injury or liver damage, Italian researchers reported after reviewing 13 years of patient data.
“These findings raise the hypothesis that the safety profile of red yeast rice is highly similar to that of synthetic statins and warrants further investigations to finally characterize the safety profile of red yeast rice,” the researchers concluded.
American heart experts said it’s not surprising that the researchers discovered adverse reactions to red yeast rice that are similar to those produced by statins.
That’s because one of the compounds in red yeast rice — monacolin K — has the same chemical structure as the statin drug lovastatin, said Dr. Paul Thompson.
“Statins actually exist in nature, in fungi and molds and stuff like that,” said Thompson, an American College of Cardiology fellow. “Patients need to know there is lovastatin in this product.” (Brand names for lovastatin are Mevacor and Altoprev.)
However, the new report only details 55 reports of adverse reactions during the entire study period. To Thompson, this indicates they are “a very rare problem.”
“It’s a tempest in a teapot,” Thompson said of the new study.
Red Yeast Rice Is Concocted From Yeast Grown On Rice
U.S. sales of red yeast rice dietary supplements totaled about $20 million a year in both 2008 and 2009, the most recent years for which data are available, according to the U.S. National Center for Complementary and Integrative Health (NCCIH).
The U.S. Food and Drug Administration views red yeast rice products containing more than trace amounts of monacolin K as unapproved new drugs, since they are chemically identical to lovastatin, and cannot be sold legally as dietary supplements.
But dozens of red yeast rice products remain on the market. And products tested as recently as 2011 have been found to contain monacolin K in substantial amounts, the NCCIH says.
For the new study, the Italian researchers reviewed government data collected on natural health products between April 2002 and September 2015.
Reports of muscle pain came from 19 patients, including some who experienced an increase in levels of creatine phosphokinase, an enzyme released when muscle tissue is damaged, the researchers said.
Thirteen of 14 “serious” cases required hospitalization. Ten patients suffered liver damage, the researchers found.
In addition, 12 patients reported gastrointestinal reactions that included upset stomach, nausea, vomiting and diarrhea.
The researchers noted that muscle pain and liver damage are common side effects of statins, which countless people take to lower their cholesterol and their risk of heart attack and stroke.
Study Doesn’t Directly Tie Red Yeast Rice To Any Of These Health Problems
“There’s no way to be absolutely guaranteed certain that most of these cases were related to the red yeast rice,” he said. Thompson is chief of cardiology at Hartford Hospital in Connecticut.
Patients with high cholesterol often buy red yeast rice over the counter when they’re concerned about the side effects of prescription statins, said Dr. Robert Eckel, a spokesman for the American Heart Association.
“You have to let them know that, well, you’re actually taking a statin,” said Eckel, who’s also a professor at the University of Colorado School of Medicine.
The Council for Responsible Nutrition, a supplement manufacturer trade group, recommends that people talk with their doctor before taking red yeast rice to lower cholesterol.
“For the small percentage of people who may have an adverse response to red yeast rice, a doctor can help to determine whether it can be tolerated, and if not, to seek other alternatives,” said Duffy MacKay. He’s the council’s senior vice president of scientific and regulatory affairs.
Some clinical trials have shown that people with a history of statin intolerance seem to tolerate red yeast rice, Eckel said.
Thompson said he prescribes a fair amount of red yeast rice in his clinic as a way to ease reluctant patients into statin treatment.
But because it’s a supplement, the amount of active ingredient in red yeast rice can vary widely from brand to brand and even batch to batch, Thompson and Eckel said.
“The products are not as well-controlled and the dosages are variable,” Eckel said.
Red yeast rice also can prove expensive if taken regularly, because it isn’t covered by insurance, Thompson said.
“My advice is people should take regular statins, even if they have to take it at very low doses,” Thompson said.
The new study appears in the British Journal of Clinical Pharmacology.
SOURCES: Paul D. Thompson, M.D., chief, cardiology, Hartford Hospital, Hartford, Conn., and fellow, American College of Cardiology; Robert Eckel, M.D., professor, University of Colorado School of Medicine, and spokesman, American Heart Association; Duffy MacKay, senior vice president, scientific and regulatory affairs, Council for Responsible Nutrition; Jan. 19, 2017, British Journal of Clinical Pharmacology, online
News stories are written and provided by HealthDay and do not reflect federal policy, the views of MedlinePlus, the National Library of Medicine, the National Institutes of Health, or the U.S. Department of Health and Human Services.
Have you ever wondered why the endless diet plans never work? Find out whether it is a fact or fiction before you follow them religiously!
Hear it straight from the horse’s mouth. Rounding up the view shared by weight loss experts, we zeroed on the top 5 dieting myths, that have been making a fool out of you for a very long time.
1. Gluten Free is The Way to Go:
Whoever got you believing gluten-free products are all you need to lose weight- fooled you big. The products almost always use rice flour that has a tendency to increase the sugar content of the food. The result is altering blood sugar level that leaves you with hunger pangs, reported Women’s Health.
2. Dairy is Not For Diet:
Here’s research that will leave you happy. Full-fat dairy products have shown better weight loss benefits than that glass of skimmed milk you hold. Dairy products are high in protein and are your best bet for weight loss diet. So, next time somebody asks you to ditch the glass of full-fat milk, ditch them instead.
3. Cut Fat to Lose Fat:
Suddenly cutting down on your fat intake will do you no good. There is a good fat and a bad fat. Natural fat and dairy fats are healthy. Avoid processed foods these come with the bad fat.
4. Consuming Food After 8 PM is Bad:
According to The Health Site, this is another dieting myth, which apparently makes no sense. If you are with your friends gorging on oily food, it is bad irrespective of the time. If you can keep your midnight hunger pangs satiated with a healthy snack then, by all means, go for it.
5. Green Tea is Mandatory For Losing Weight:
Have to agree that green tea is good for health but mind you, it is no superfood for your weight loss program. The amount of green tea you have to consume to lose a proper weight is just way too much. Buying expensive green tea weight loss supplements was a marketing technique that got you good.
Here�s to a different kind of body transformation. On Instagram yesterday, fitness influencer Anna Victoria shared a�follower�s photos that document her inspiring recovery from an extreme exercise habit.
In the “before” pic, @barbellkell_fbg is flexing her biceps in a bikini that shows off her chiseled six-pack.
What It Took To Get That Sculpted Bod Was Anything But Healthy
The photo on the left was taken a year and a half ago, when @barbellkell_fbg was committed to a 10-week plan that involved working out�five times a week, sometimes twice a day, and counting macros (down to chewing gum, vitamins, and cough drops), she explains in the caption. “[Z]ero balance, zero living, zero sustainability,” she wrote. “I had my full time job and this, which was another full time job basically.”
The strict dieting and intense workouts�took a serious toll. By the end of the plan, @barbellkell_fbg had a flat belly, and no trace of cellulite�but her energy levels had plummeted. “I could barely lift my feet to run on the treadmill,” she wrote. A blood test showed her white blood cell count was severely depressed. It was so low her doctor wanted to test her for cancer, she says.
After convincing him to do another blood test in a month, @barbellkell_fbg�committed to getting back to “normal.” She ate “to survive,” she said;�and in time, she gained fat and her white blood cell count recovered.
OD’ing on exercise�is a real thing, and it can�cause everything from fatigue to chronic achiness�even an elevated heart rate, which puts more demand on your ticker. “Overexercising�often contributes to pain,�dehydration, or electrolyte imbalances, all of which can lead to an increase in heart rate,” Kathryn Berlacher, MD, a cardiologist at the University of Pittsburgh School of Medicine, explained to�Health in a prior interview.
As for�@barbellkell_fbg, she’s�come a long way in the last 18 months.�She now follows Anna Victoria�s Fit Body Guides, and eats what she wants in moderation. “I feel good. I am strong. I am happy,” she says�and�she loves the body she has now.
Chiropractors who provide care for children � and families � can attest to the many benefits of a healthy spine to a growing child. However, this relatively new area of focus for chiropractic is susceptible to many misconceptions, among the public and the health-care community.
Many of the public perceptions about chiropractic care for children, however, are far from the truth. We explore these misconceptions and spoke to the experts to get the real facts about this thriving chiropractic focus area.
Myth #1 Chiropractic care of children is new.
When some individuals first learn that DCs treat children as well as adults, they may get the wrong idea that chiropractic for kids is new � which is to say untested, experimental and dangerous.
That isn�t the case. Sure, the modern era of this field dates only as far back as the 1980s. But the fact is, the practice actually has much older and stronger roots. �If you go back to 1910, [founder of chiropractic] D.D. Palmer indicated how important it is to check a child�s spine from birth and throughout life,� notes Jeanne Ohm, CEO of the International Chiropractic Pediatrics Association (ICPA), a non-profit organization in Philadelphia.�
By the 1980s, many DCs had developed their practices to treat adults specifically. In 1986, Dr. Larry Webster in the U.S. helped re-establish chiropractic care for children as a legitimate area of focus. He started teaching his child-friendly techniques, and he created the ICPA to further help chiropractors treat children.
Webster passed away in 1997, but his legacy continues. The ICPA now has more than 4,000 members and hundreds of DCs are studying to become chiropractors with a special focus on kids.
Myth #2 Children don�t need chiropractic care.
DCs who treat kids often hear questions along these lines: Why in the world would a child need to see a chiropractor? What good does chiropractic do for a toddler, or even a newborn?
Chiropractors have a few good answers.
�We may see a one-week-old child who is already showing signs of favoring, turning her head to one side versus the other,� says Dr. Judy Forrester, owner of Synergea Family Health Centre, a multidisciplinary clinic in Calgary, Alta. �That may seem minimal� but if we can determine any imbalances or asymmetry with the muscular function or the joint alignment, and we address it early, it�s better. Once those postural patterns and habits develop as they grow, they can be much more difficult to change.�
Dr. Liz Anderson-Peacock is a Barrie, Ont., chiropractor who focuses on care for children. She notes the link between the central nervous systems and various childhood afflictions.
�Children may have symptoms like ear infections, difficulty breathing, colic, attention deficit. We do not treat those things per se. We see those as expressions of the body not interpreting the world properly,� explains Anderson-Peacock, who also serves in the editorial board for the Journal of Maternal, Pediatric and Family Health.
�The organizing system for us to respond to the world is the nervous system. The questions we ask are: if there is something going on with the nervous system, what is it, and can chiropractic care help?�
Anderson-Peacock now spends most of her time travelling around the world doing lectures and other speaking engagements. She also conducts seminars for the ICPA about chiropractic care for children and families.
Ohm from the ICPA links chiropractic to the very moment a child emerges from the womb. �Birth can be traumatic,� she says. The event could cause physical damage that leads to difficulties later. So if a baby develops breathing trouble, �the real cause may simply be a misalignment to the spine from the birth process. Parents who get that will stop at the clinic on the way home from the birth centre to make sure everything is OK.�
Chiropractic & Children
Myth #3 Chiropractors use the same techniques on children as adults.
�That�s what terrifies a lot of chiropractors about adjusting children, as well as parents,� Anderson-Peacock says. �They think we�re going to adjust them like an adult.�
But DCs who treat children do not apply heavy pressure. �Often, it�s a matter of moving the child into a position of ease, holding that position and things will reset quite nicely on their own,� Anderson-Peacock says. Care, she points out, is nowhere near as forceful as it may be for adults.
�That�s why extra training is so crucial. These children are not like miniature adults. For example, spines are primarily cartilaginous until the age of six, and we know cartilage will deform when we have abnormal function. So we want to make sure that function is restored normally. And since the bones are immature, the alignment issues are different. We want to minimize rotations and traction, because children have different needs, due to the immaturity of their musculoskeletal and ligamentous structures.�
The ICPA aims to validate techniques for chiropractic care for children, particularly to help dispel the idea that DCs use the same pressure on kids as they do on adults, Ohm notes. The organization is working with Walter Herzog, co-director of the Human Performance Laboratory at the University of Calgary, to study the pressure required when caring for children. The report should be out by the end of 2015.
Chiropractic & Children with Chronic Conditions
Myth #4 There are no real experts in chiropractic care for children.
In Canada, chiropractic care for children is not a recognized area of specialty, which leads some people to think there are no genuine experts in the field. But that isn�t true.
Many DCs follow accredited courses to develop child-specific skills. Anderson-Peacock spent three years studying at the International Chiropractors Association�s Council on Chiropractic Education (CCE)-accredited program in pediatric chiropractic. She achieved her Diplomate in Clinical Chiropractic Pediatrics (DICCP) in 1996.
Dr. Stacey Hornick is owner of Market Mall Family Chiropractic in Saskatoon, Sask. She attended McTimoney College of Chiropractic, operated by BPP University � a post-secondary institution in London, England. Over three years, she took courses by correspondence and traveled to Thailand, Hong Kong and Australia to complete the residency portion of the program. Having succeeded in her studies last year, she was granted a master�s degree in Chiropractic Paediatrics.
Hundreds of DCs have taken the ICPA�s programs. The ICPA Diplomate Program involves a total of 400 hours of learning and achieved through the successful completion of two levels of study.
The first part � a 200-hour certification program � involves 14 classroom modules, participation in two ICPA Practice Based Research Network projects, and successful completion of the comprehensive certification� final exam.
The second part is a 200-hour advanced competency program. It requires 200 hours of work with more emphasis on research, including either a published research case study or a publishable thesis, as well as clinic work. Enrollment in the first level (200-hour certification program) is a prerequisite to enroll in part two.
Chiropractic care for kids may not be a recognized specialty in Canada, but chiropractic associations recognize it as a legitimate area of focus.
In a statement, the Alberta College and Association of Chiropractors (ACAC) has acknowledged, �chiropractic treatment is as beneficial to children as it is to adults and that the efficacy and benefits of the delivery of chiropractic care to individuals 18 years of age and under are well supported by a body of ongoing research and documented case histories.�
Chiropractic & Teens with Back Pain
Myth #5 Chiropractors don�t collaborate with pediatricians and medical doctors.
Hornick says this simply isn�t the case.
�I often refer pediatric patients to their medical doctors and to medical specialists, and we communicate clearly in the best interests of the child. I see our roles as complementary.�
Forrester also says she has good ties with medical doctors. �The majority of them are very much in favor of working together. Every once in a while you run into someone who thinks we�re all a bunch of quacks and they�re not up to date with the sorts of things we do. But by far the relationship with pediatricians is healthy and puts the patients� best interests first.�
Reality recap
Chiropractic care for kids is not new. Children benefit from chiropractic care. Techniques for children are safe and nowhere near as forceful as they may be for adults. Many DCs are qualified experts, and many child-focused chiropractors establish strong connections with medical doctors. The truth is, DCs can and do share the benefits of their profession with patients across the entire age spectrum.
Mastering pediatrics
Late last year, Dr. Stacey Hornick, a Saskatoon, Sask.-based DC focused on chiropractic care for children became one of the first Canadians to attain a Master�s of Science in Chiropractic Paediatrics.She studied at McTimoney College of Chiropractic, operated by BPP University, a post-secondary institution in London, England. The McTimoney program is the only pediatric chiropractic program that meets the academic requirements for entry into doctoral studies (PhD) in the specific content area of chiropractic pediatrics, an opportunity never before afforded the chiropractic profession, she says.
�For me, it was important to seek out a highly respected qualification in pediatric care,� Hornick says. �There were no university-accredited courses in pediatrics in North America that I was aware of at the time. I liked the idea of studying abroad and at the same time becoming an expert in pediatric-specific assessment, and adjusting techniques that were gentle yet neurologically precise.�
It takes stamina and smarts to get into and complete this tough three-year course. Read on for the requirements. Do you have what it takes?
To enter the program, a candidate must have: a professional qualification in chiropractic and registration with a relevant chiropractic governing body
In each of the first two years of the program, the student must complete:
Work at two residential schools � Hornick explains that usually, students complete their residencies at U.K. chiropractic facilities, but McTimoney also gives students the chance to practice outside of the U.K. For her part, Hornick completed her first-year residency in Thailand, which was memorable. �We stayed at the Children of the Golden Triangle Training Center. It�s a safe haven when kids can go to school and avoid the whole child-trafficking danger, which is a heart-wrenching reality in that part of the world. Many of the children at the facility were orphans � 450 of them. We got to stay with them, and between five chiropractors, we adjusted all of them in three days.�
Online course work � Subjects range from the fundamentals of chiropractic pediatrics to specific requisite topics. Hornick says first-year courses include substrates of chiropractic pediatrics, physical assessment in chiropractic skills and pediatric neurology. �The second year is more application of knowledge.� Courses include normal and variant radiology anatomy in pediatrics, clinical research methodology, and four clinical pediatrics programs.
Structured clinical education, directed and self-directed
Objective structured clinical exam
In the third year of the program, students must complete a research project, including project design, implementation and report at a publishable standard. Hornick�s dissertation: The Effect of Chiropractic on Cortisol Levels in Infants with Colic. The investigation aimed to help doctors understand why chiropractic adjustment has a positive influence on colicky infants. Hornick found that infants with colic who receive chiropractic care demonstrate salivary cortisol release patterns similar to those seen in infants with no colic.
Public�Perceptions about chiropractic care for children are far from the truth. Let’s�explore these misconceptions and speak to experts in order to get the real facts about chiropractic care for children.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine

 5. Makes You Smarter
5. Makes You Smarter
















 �We may see a one-week-old child who is already showing signs of favoring, turning her head to one side versus the other,� says Dr. Judy Forrester, owner of Synergea Family Health Centre, a multidisciplinary clinic in Calgary, Alta. �That may seem minimal� but if we can determine any imbalances or asymmetry with the muscular function or the joint alignment, and we address it early, it�s better. Once those postural patterns and habits develop as they grow, they can be much more difficult to change.�
�We may see a one-week-old child who is already showing signs of favoring, turning her head to one side versus the other,� says Dr. Judy Forrester, owner of Synergea Family Health Centre, a multidisciplinary clinic in Calgary, Alta. �That may seem minimal� but if we can determine any imbalances or asymmetry with the muscular function or the joint alignment, and we address it early, it�s better. Once those postural patterns and habits develop as they grow, they can be much more difficult to change.�