According to research studies, understanding possible nutraceutical interactions for methylation support with the utilization of long-term supraphysiological supplementation of niacin, selenium, and phosphatidylethanolamine can ultimately help promote overall health and wellness. Doctors and functional medicine practitioners must be aware of the nutraceutical interactions for methylation through supplementation.
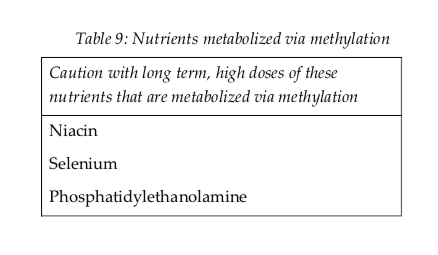
Nutraceutical supplements utilized in integrative functional medicine as well as in nutrition practice can have tremendously powerful effects on physiology. Nutraceutical supplements are one of the primary tools which healthcare professionals utilize to help their patients achieve optimal well-being. However, as mentioned above, healthcare professionals must be aware of possible nutraceutical interactions, especially those which may negatively affect methylation. These are listed in Table 9 below.
Nutrients are metabolized in the human body through methylation, such as niacin, selenium, and phosphatidylethanolamine. Therefore, high dose supplemental regimens of these nutrients can ultimately decrease available methyl donors and cause a methylation deficit. Niacin can also prevent the production of pyridoxal kinase, which is generally known to trigger vitamin B6. High doses of this nutrient may affect overall vitamin B6 status.
Medication Interactions
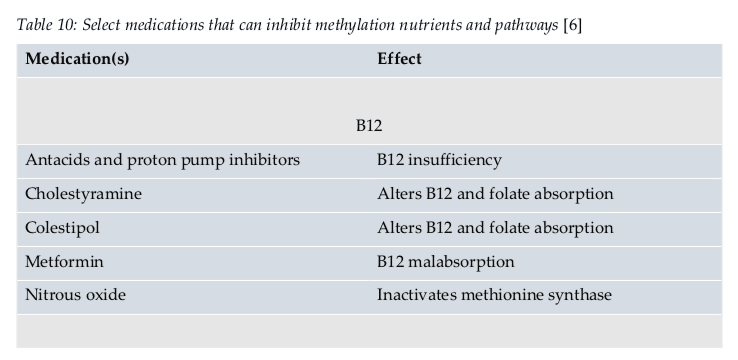
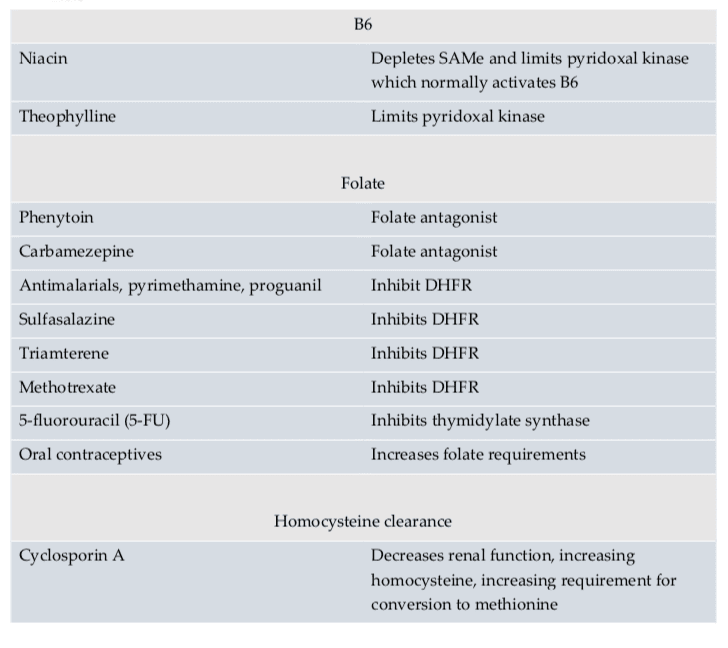
According to research studies, doctors and functional medicine practitioners must also understand possible medication interactions for methylation support. Moreover, healthcare professionals must be aware that medication interactions can ultimately affect methylation status. Several medications have been demonstrated to affect methylation status in a variety of ways. Several medications may even prevent proper nutrient absorption, while several others may restrict enzyme function, and several others still may decrease SAMe. An understanding of these medication interactions is essential to promote optimal methylation support.
Doctors and functional medicine practitioners can recommend a variety of supplements and/or medications to promote methylation support, however, these can also cause a variety of side-effects on every individual. Healthcare professionals must be aware of these nutraceutical and medication interactions and their use must be carefully considered for each patient. Nutrition and lifestyle habits are safe and effective treatment options which can help promote methylation support without the chance of developing side effects.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
Smoothies and Juices for Methylation Support
While many healthcare professionals can recommend nutritional guidelines and lifestyle modifications to improve methylation support, there are several options you can try yourself at home. As described above, methylation support supplementation should be determined by a healthcare professional. Smoothies and juices are a fast and easy way to include all the necessary nutrients you need for methylation support without any side-effects. The smoothies and juices below are part of the Methylation Diet Food Plan.
Sea Green Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup cantaloupe, cubed � 1/2 banana � 1 handful of kale or spinach � 1 handful of Swiss chard � 1/4 avocado � 2 teaspoons spirulina powder � 1 cup water � 3 or more ice cubes Blend all ingredients in a high-speed blender until completely smooth and enjoy!
Berry Bliss Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup blueberries (fresh or frozen, preferably wild) � 1 medium carrot, roughly chopped � 1 tablespoon ground flaxseed or chia seed � 1 tablespoons almonds � Water (to desired consistency) � Ice cubes (optional, may omit if using frozen blueberries) Blend all ingredients in a high-speed blender until smooth and creamy. Best served immediately!
Sweet and Spicy Juice Servings: 1 Cook time: 5-10 minutes � 1 cup honeydew melons � 3 cups spinach, rinsed � 3 cups Swiss chard, rinsed � 1 bunch cilantro (leaves and stems), rinsed � 1-inch knob of ginger, rinsed, peeled and chopped � 2-3 knobs whole turmeric root (optional), rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Ginger Greens Juice Servings: 1 Cook time: 5-10 minutes � 1 cup pineapple cubes � 1 apple, sliced � 1-inch knob of ginger, rinsed, peeled and chopped � 3 cups kale, rinsed and roughly chopped or ripped � 5 cups Swiss chard, rinsed and roughly chopped or ripped Juice all ingredients in a high-quality juicer. Best served immediately!
Zesty Beet Juice Servings: 1 Cook time: 5-10 minutes � 1 grapefruit, peeled and sliced � 1 apple, washed and sliced � 1 whole beet, and leaves if you have them, washed and sliced � 1-inch knob of ginger, rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Protein Power Smoothie Serving: 1 Cook time: 5 minutes � 1 scoop protein powder � 1 tablespoon ground flaxseed � 1/2 banana � 1 kiwi, peeled � 1/2 teaspoon cinnamon � Pinch of cardamom � Non-dairy milk or water, enough to achieve desired consistency Blend all ingredients in a high-powered blender until completely smooth. Best served immediately!
ProLon� Fasting Mimicking Diet
Balanced methylation support can be achieved through proper nutrition. The ProLon� fasting mimicking diet offers a 5-day meal program which has been individually packed and labeled to serve the foods you need for the FMD in precise quantities and combinations. The meal program is made up of ready-to-eat or easy-to-prepare, plant-based foods, including bars, soups, snacks, supplements, a drink concentrate, and teas. The products are scientifically formulated and great tasting. Before starting the ProLon� fasting mimicking diet, 5-day meal program, please make sure to talk to a healthcare professional to find out if the FMD is right for you. The ProLon� fasting mimicking diet can help promote methylation support, among a variety of other healthy benefits.
Many healthcare professionals can recommend a variety of nutraceutical and medication interactions to help improve DNA methylation. Proper nutrition and lifestyle habits can ultimately help improve DNA methylation. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Acute Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly, Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
Dr. Alex Jimenez Discusses Exercise and Methylation
A personalized, moderate exercise plan can promote methylation support. According to research studies, exercise can affect metabolic methylation-related activity and biomarkers. According to a 2014 systematic review, exercise is associated with lower homocysteine levels. In animal models, exercise has been demonstrated to prevent folate deficiency-induced hyperhomocysteinemia through increased BHMT expression in the kidney.
However, several research studies have also demonstrated that exercise can cause a temporary increase in plasma homocysteine, especially in untrained people, which is believed to be due to the increased proteins during exercise to make amino acids available for gluconeogenesis in the liver. This effect can also be triggered by low folate and vitamin B12 status, which is why nutrient repletion is essential for overall health and wellness.
Regular and moderate exercise is an effective treatment for factors which can decrease methyl donors or affect methylation activity, such as psychological stress, oxidative stress, and inflammation. Aerobic exercise and resistance training have also been associated with increased cellular glucose uptake and reduced blood glucose, which can also reduce oxidative stress caused by higher AGE-promoting glucose levels, among other factors.
How Exercise Improves DNA Methylation
The increased production of reactive oxygen species and free radicals during exercise as well as the increased levels of pro-inflammatory cytokines has been demonstrated in a variety of research studies. However, the effects of these changes can depend on a person’s nutrition and lifestyle habits. High-intensity or anaerobic exercise may have pro-oxidative effects, especially in untrained individuals. Endurance exercise, by way of instance, may produce circulating levels of IL-6, up to 120 times that of baseline, as well as increases in other predominantly pro-inflammatory cytokines.
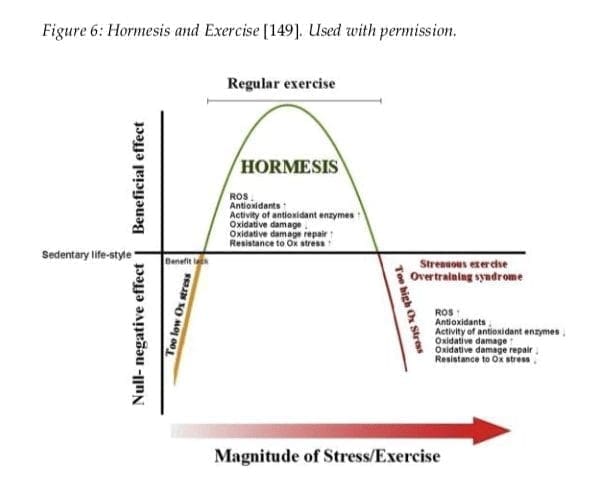
A 2013 systematic review demonstrated the effect of exercise on oxidative stress in the brain. The outcome measures determined that regular, moderate, aerobic exercise increase the brain�s antioxidant capacity, however, high-intensity, anaerobic exercise decreased the antioxidant response. The results can be explained by a hormesis model of exercise (Figure 6), which discusses that low or high levels of exercise can produce negative effects. The gradual build-up of exercise, through regular practice or training, can change the hormesis curve to the right, meaning that exercise tolerance and benefits are highly personalized for each person.
Recent research studies have discussed that antioxidants provided by a diet rich in natural plant phytochemicals, such as vegetables, fruits, whole grains, legumes and beans, sprouts and seeds, are also an effective way to meet the antioxidant needs of the general population and athletes who participate in exercise, physical activities, and/or sports. As a matter of fact, dietary intervention is a much safer and effective treatment than antioxidant supplementation because research studies utilizing supplementation demonstrated insufficient and mixed results. Several researchers even believe that antioxidant supplementation can affect the beneficial hormetic effects of exercise, ultimately affecting well-being.
Exercise can ultimately affect DNA methylation, according to a recent review of literature. By way of instance, in a retrospective research study of 647 women, regular exercise throughout their lifetimes helped preserve the age-related depletion of global methylation status, where exercise and physical activity like sports and daily movement, such as climbing stairs, housework, and yardwork, which was greater than or equal to the average in childhood, adolescence, and adulthood, did have a small yet considerable increase in global DNA methylation compared with participants who did not meet that level of exercise or physical activity in all three life stages.
Women who engaged in exercise or physical activity at or above the average in only one or two of those life stages also demonstrated increased DNA methylation, however, statistical importance was lost. The average level of exercise was determined at 9.8 hours per week in childhood, 5.9 hours per week in teenage years, and 12.5 hours per week in adulthood. Further research studies may be used to gather further outcome measures.
In a separate case-control research study of 500 females, long-term, tai-chi participants of at least one hour per week for 3 years or more, demonstrated a slowing of age-related DNA methylation losses, from 5 to 70 percent, compared with controls. During their research study, the researchers determined a considerable difference in methylation between the two groups at a number of specific sites which only occurred after 50 to 55 years of age, leading them to believe that tai-chi may be of particular benefit in this age-group. Further research studies are still required.
Although the effects of exercise on DNA methylation are not well understood, research studies have demonstrated that this may actually be true due to the inflammation-lowering effects of exercise and physical activity through changes in sex hormone levels that can affect DNA methylation. Mind-body exercises, such as tai-chi, may also be beneficial due to their effects on stress hormone levels and stress responsiveness.
Nutrition and lifestyle habits, such as exercise and physical activity, can help improve DNA methylation. Regardless of your age, research studies have demonstrated that participating in exercise, sports, or any other physical activity can enhance your overall health and wellness. Recent research studies have also determined that proper nutrition and lifestyle habits can improve methylation, a fundamental process of the human body involved in a variety of functions.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
Smoothies and Juices for Methylation Support
While many healthcare professionals can recommend nutritional guidelines and lifestyle modifications to improve methylation support, there are several options you can try yourself at home. As described above, methylation support supplementation should be determined by a healthcare professional. Smoothies and juices are a fast and easy way to include all the necessary nutrients you need for methylation support without any side-effects. The smoothies and juices below are part of the Methylation Diet Food Plan.
Sea Green Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup cantaloupe, cubed � 1/2 banana � 1 handful of kale or spinach � 1 handful of Swiss chard � 1/4 avocado � 2 teaspoons spirulina powder � 1 cup water � 3 or more ice cubes Blend all ingredients in a high-speed blender until completely smooth and enjoy!
Berry Bliss Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup blueberries (fresh or frozen, preferably wild) � 1 medium carrot, roughly chopped � 1 tablespoon ground flaxseed or chia seed � 1 tablespoons almonds � Water (to desired consistency) � Ice cubes (optional, may omit if using frozen blueberries) Blend all ingredients in a high-speed blender until smooth and creamy. Best served immediately!
Sweet and Spicy Juice Servings: 1 Cook time: 5-10 minutes � 1 cup honeydew melons � 3 cups spinach, rinsed � 3 cups Swiss chard, rinsed � 1 bunch cilantro (leaves and stems), rinsed � 1-inch knob of ginger, rinsed, peeled and chopped � 2-3 knobs whole turmeric root (optional), rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Ginger Greens Juice Servings: 1 Cook time: 5-10 minutes � 1 cup pineapple cubes � 1 apple, sliced � 1-inch knob of ginger, rinsed, peeled and chopped � 3 cups kale, rinsed and roughly chopped or ripped � 5 cups Swiss chard, rinsed and roughly chopped or ripped Juice all ingredients in a high-quality juicer. Best served immediately!
Zesty Beet Juice Servings: 1 Cook time: 5-10 minutes � 1 grapefruit, peeled and sliced � 1 apple, washed and sliced � 1 whole beet, and leaves if you have them, washed and sliced � 1-inch knob of ginger, rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Protein Power Smoothie Serving: 1 Cook time: 5 minutes � 1 scoop protein powder � 1 tablespoon ground flaxseed � 1/2 banana � 1 kiwi, peeled � 1/2 teaspoon cinnamon � Pinch of cardamom � Non-dairy milk or water, enough to achieve desired consistency Blend all ingredients in a high-powered blender until completely smooth. Best served immediately!
ProLon� Fasting Mimicking Diet
Balanced methylation support can be achieved through proper nutrition. The ProLon� fasting mimicking diet offers a 5-day meal program which has been individually packed and labeled to serve the foods you need for the FMD in precise quantities and combinations. The meal program is made up of ready-to-eat or easy-to-prepare, plant-based foods, including bars, soups, snacks, supplements, a drink concentrate, and teas. The products are scientifically formulated and great tasting. Before starting the ProLon� fasting mimicking diet, 5-day meal program, please make sure to talk to a healthcare professional to find out if the FMD is right for you. The ProLon� fasting mimicking diet can help promote methylation support, among a variety of other healthy benefits.
Many healthcare professionals can recommend a variety of treatment options to help improve DNA methylation. Proper nutrition and lifestyle habits, such as exercise and physical activity, can ultimately help improve DNA methylation. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Acute Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly, Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
Dr. Alex Jimenez Discusses How Detox Helps Methylation
Reducing our exposure to environmental toxins and promoting biotransformation and elimination are several guidelines recommended by healthcare professionals to improve the human body’s detoxification process. However, proper nutrition and lifestyle habits can also help improve detoxification. In addition, improving methylation can help improve the detoxification process.
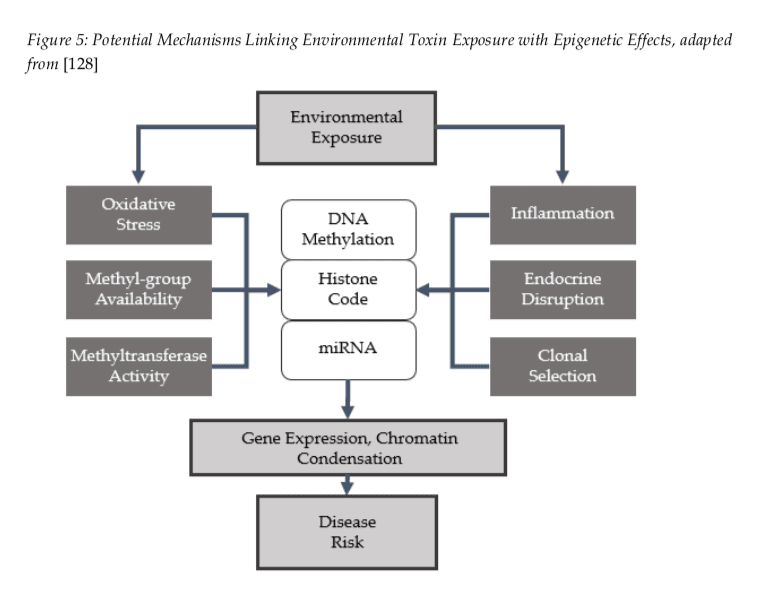
Methylation is an essential detoxification pathway. Our increased exposure to environmental toxins, such as heavy metals and chemicals, can ultimately affect DNA methylation and prevent their safe and effective use. Environmental toxins may also affect DNA methylation through other structures and functions, including endocrine disruption, inflammation, and oxidative stress, among others.
According to research studies, the list of environmental toxins below has been demonstrated to affect DNA methylation, including:
Pesticides
Fertilizer
Automobile fumes
Bisphenol A
Phthalates
Persistent Organic Pollutants (POPs)
Jet fuel
Benzene
Mold toxins (aflatoxin, fumonisin)
Arsenic
Mercury
Lead
Cadmium
Nickel
Increased exposure to heavy metals can cause a variety of health issues. Specific DNMT restriction and decreased DNMT gene expression have also been demonstrated to occur with increased lead exposure. Cadmium also seems to cause DNA hypomethylation through DNMT restriction, however, it may actually have the opposite effect of hypermethylation with increased exposure.
How Detoxification Can Help Improve DNA Methylation
In vitro research studies suggests that one process involved in abnormal DNA hypermethylation occurs through the induction of toxin or inflammation-mediated methyl radicals from oxidized methionine which trigger the development of DNA hypermethylation tumor-suppressing genes that promote gene silencing and oncogenesis. The development of oxidized methionine occurs in smokers, often due to inflammation and aging. Furthermore, inorganic arsenic is detoxified in the human body through methylation, which ultimately leads researchers to believe that increased exposure to arsenic may drain the endogenous pool of methylation donors available.
Total exposure to toxins, such as persistent organic pollutants (POPs) and heavy metals, may also have cumulative and long-lasting effects, according to research studies. Manikkam et al. (2012), evaluated the effects of bisphenol A, phthalates, digoxin and jet fuel (as listed above) on DNA methylation. It was also demonstrated that the epigenetic changes continued throughout multiple generations while it appeared to cause early onset puberty four generations later in rodents. Further research studies are being conducted.
Exposure to environmental toxins may also restrict healthy methylation by affecting other folate processes. Fumonisins, a type of mold toxin, by way of instance, has been demonstrated to restrict the proper function of folate binding proteins, such as human folate receptor alpha. By understanding how toxin exposure affects methylation, reducing these where possible is extremely important.
This may include the evaluation and treatment of exposures to mold, lead, and mercury amalgams, by way of instance, decreasing the utilization of plastic food containers, avoiding high-mercury fish, and switching to non-toxic household and personal care products. The Environmental Working Group (www.ewg.org) provides an excellent resource to further understand sources of toxin exposure.
Supporting endogenous biotransformation through Phase I and Phase II detoxification pathways and well-functioning elimination is also essential to improve DNA methylation through detoxification. Short term use of supplement protocols for detoxification is generally utilized in functional medicine, where an excessive toxic burden has been found. Nutrition and lifestyle habits can also help promote detoxification for methylation support. The list below are basic principles to follow for everyday detoxification support:
Proper hydration
Adequate fiber sources
Low-toxin foods including organic, and antibiotic and hormone-free High intake of colorful plant foods, especially deep greens and berries Regular intake of cruciferous vegetables
Adequate protein intake
Maintain micronutrient intake
Detoxification, or “detox”, refers to the removal of toxins from the human body. Many doctors and functional medicine practitioners utilize a series of alternative treatment methods to help people detox from harmful toxic substance exposure. According to research studies, increased exposure to toxins can also affect DNA methylation. Moreover, healthy methylation is fundamental to help promote the human body’s natural detoxification process. Proper nutrition and lifestyle habits which can help improve DNA methylation can ultimately help promote detoxification and improve overall health and wellness.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
Smoothies and Juices for Methylation Support
While many healthcare professionals can recommend nutritional guidelines and lifestyle modifications to improve methylation support, there are several options you can try yourself at home. As described above, methylation support supplementation should be determined by a healthcare professional. Smoothies and juices are a fast and easy way to include all the necessary nutrients you need for methylation support without any side-effects. The smoothies and juices below are part of the Methylation Diet Food Plan.
Sea Green Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup cantaloupe, cubed � 1/2 banana � 1 handful of kale or spinach � 1 handful of Swiss chard � 1/4 avocado � 2 teaspoons spirulina powder � 1 cup water � 3 or more ice cubes Blend all ingredients in a high-speed blender until completely smooth and enjoy!
Berry Bliss Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup blueberries (fresh or frozen, preferably wild) � 1 medium carrot, roughly chopped � 1 tablespoon ground flaxseed or chia seed � 1 tablespoons almonds � Water (to desired consistency) � Ice cubes (optional, may omit if using frozen blueberries) Blend all ingredients in a high-speed blender until smooth and creamy. Best served immediately!
Sweet and Spicy Juice Servings: 1 Cook time: 5-10 minutes � 1 cup honeydew melons � 3 cups spinach, rinsed � 3 cups Swiss chard, rinsed � 1 bunch cilantro (leaves and stems), rinsed � 1-inch knob of ginger, rinsed, peeled and chopped � 2-3 knobs whole turmeric root (optional), rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Ginger Greens Juice Servings: 1 Cook time: 5-10 minutes � 1 cup pineapple cubes � 1 apple, sliced � 1-inch knob of ginger, rinsed, peeled and chopped � 3 cups kale, rinsed and roughly chopped or ripped � 5 cups Swiss chard, rinsed and roughly chopped or ripped Juice all ingredients in a high-quality juicer. Best served immediately!
Zesty Beet Juice Servings: 1 Cook time: 5-10 minutes � 1 grapefruit, peeled and sliced � 1 apple, washed and sliced � 1 whole beet, and leaves if you have them, washed and sliced � 1-inch knob of ginger, rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Protein Power Smoothie Serving: 1 Cook time: 5 minutes � 1 scoop protein powder � 1 tablespoon ground flaxseed � 1/2 banana � 1 kiwi, peeled � 1/2 teaspoon cinnamon � Pinch of cardamom � Non-dairy milk or water, enough to achieve desired consistency Blend all ingredients in a high-powered blender until completely smooth. Best served immediately!
ProLon� Fasting Mimicking Diet
Balanced methylation support can be achieved through proper nutrition. The ProLon� fasting mimicking diet offers a 5-day meal program which has been individually packed and labeled to serve the foods you need for the FMD in precise quantities and combinations. The meal program is made up of ready-to-eat or easy-to-prepare, plant-based foods, including bars, soups, snacks, supplements, a drink concentrate, and teas. The products are scientifically formulated and great tasting. Before starting the ProLon� fasting mimicking diet, 5-day meal program, please make sure to talk to a healthcare professional to find out if the FMD is right for you. The ProLon� fasting mimicking diet can help promote methylation support, among a variety of other healthy benefits.
Many healthcare professionals recommend a variety of treatment options to help improve detoxification and help prevent health issues associated with DNA methylation. Proper nutrition and lifestyle habits, can improve methylation. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Acute Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly, Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
Dr. Alex Jimenez Explains Methylation Status, Inflammation and Oxidative Stress
As previously mentioned in the past series of articles, doctors can use a variety of clinical assessments to evaluate the methylation status of their patients. Although no assessment method or technique can accurately determine a patient’s methylation activity, current assessments can provide a better understanding of methylation-related genetic polymorphisms, nutrient status, methylation-related neurotransmitters and neurotransmitter metabolites, amino acids, hormones and metabolites, oxidative stress, and detoxification load. Each of these processes and substances can help doctors and patients understand their methylation status.
Understanding Methylation Status
Various assessment methods and techniques, including measures utilized to determine DNA methylation status, are usually exclusive to research studies and are not yet readily available to doctors. Until methylation status assessments become more widely available, further diagnosis is still required to understand diseases, especially since conflicting outcome measures have been found in research studies on the various methodologies. Although methods and techniques from research studies have rapidly started to evolve, patterns of DNA methylation status in humans across cells, tissues, age, populations, environmental factors like nutrition and lifestyle modifications, as well as disease, have only just started to become more widely recognized by researchers and doctors.
It is fundamental that we focus on a variety of these indicators and that we become aware of the restrictions of our interpretations and their misunderstood factors. Plasma homocysteine, by way of instance, can decrease as methylation activity increases, but, it can also decrease when oxidative stress levels increase, regardless if methylation activity increases. However, as we�ve previously mentioned, only several SNPs have known, quantifiable alterations in enzymatic function and their overall outcome measures on methylation remain unknown. Doctors must rely on a variety of clinical assessments to evaluate the methylation status of their patients. In the following articles, we will continue to discuss methylation status assessment options available to doctors for patients.
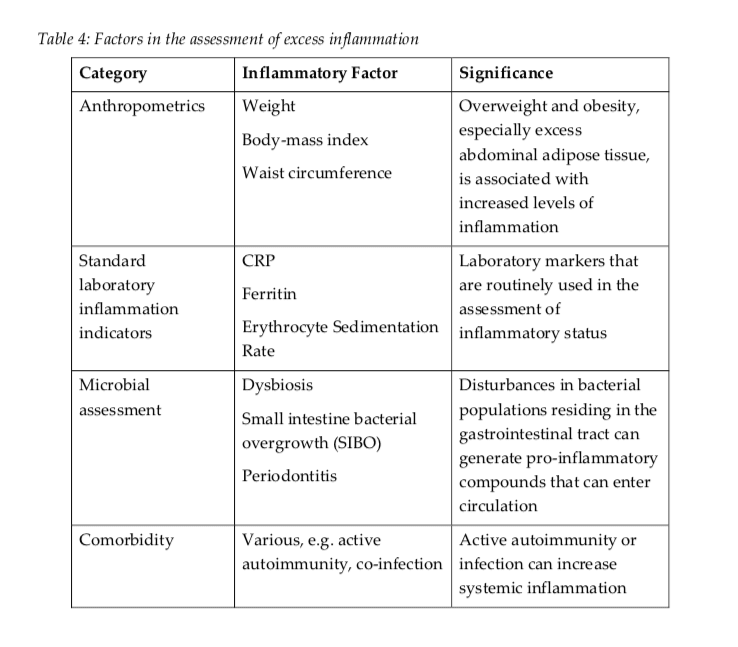
Understanding Inflammation
Inflammation increases the production of cytokine which can alter a patient’s methylation status in a variety of ways. DNA methylation activity is also tremendously affected by inflammation-related signaling molecules. Cytokines, chemokines, free radicals, prostaglandins, growth factors, and matrix metalloproteinases, are produced during inflammation, altering epigenetic changes in DNA methylation activity. IL-1?, by way of instance, suppresses p53 expression, creating a more favorable environment for tumorigenesis. NF?B is a central transcription factor triggered by inflammation which also regulates the expression of more than 400 genes.
Moreover, it directly regulates NK?B-dependent histone demethylase which in turn regulates the fate and transdifferentiation of tumor cells. IL-6, another inflammatory signaling molecule, regulates the activity of DNMTs, microRNAs and histone methyltransferases which affect the epigenetics of p53 tumor suppressor genes by reducing expression. TNF-alpha increases in mitotically-preserved and region-specific DNA methylation activity in a way that seems to include impaired cellular differentiation and renewal. In vitro outcome measures suggest that inflammation may also promote the production of methyl radicals which trigger DNA methylation activity in normal, unmethylated tumor suppressor genes, causing gene silencing and carcinogenesis.
Inflammation can also cause a metabolic milieu that drains methylation resources, by way of instance, through the dysregulation of glucose homeostasis. Pro-inflammatory molecules can also alter insulin signaling in peripheral tissues, reducing inflammatory mediators that promote insulin signaling. Insulin dysfunction and hyperglycemia promote elevated levels of oxidative stress which triggers increased utilization of glutathione and depleted homocysteine, methionine and SAMe. Furthermore, DNA methylation patterns affecting metabolism and inflammation were identified in adipose tissue from subjects with type 2 diabetes.
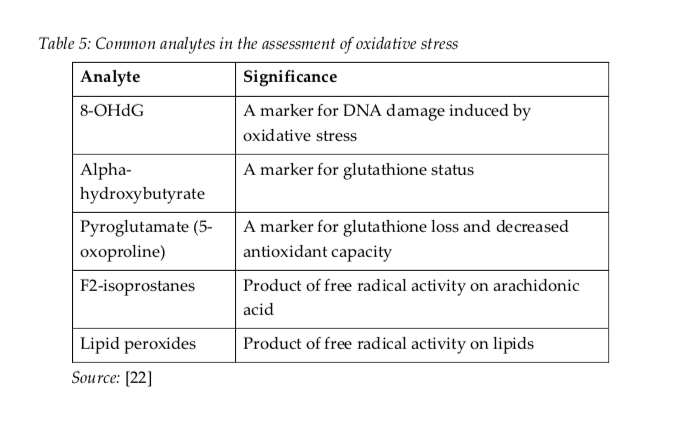
Understanding Oxidative Stress
Oxidative stress is closely associated with inflammation. States of elevated, or chronic, oxidative stress can negatively alter DNA methylation through two mechanisms. First, oxidative stress increases the demand for glutathione synthesis, which pulls homocysteine towards transulfuration pathways, at the expense of methylation pathways and SAMe formation. Second, oxidative stress and increased hydroxyl radical formation can damage DNA and change the ability of DNA methyltransferase enzymes to appropriately methylate DNA. This is one of the most common causes of global DNA hypomethylation and specific areas of hypermethylation.
DNA guanine nucleotides are main regions of DNA damage caused by oxidative stress, which is why they are frequently utilized as a biomarker for DNA-level oxidative stress, or 8OHdG. Generally, guanine functions as a hydrogen bond acceptor to promote the creation of methyl binding protein, or MBP, DNA complexes. However, oxidation of guanine considerably decreases MBP binding when combined to the 5- methylcytosine nucleotide. Additionally, 5-methylcytosine, or 5-mC, may also experience oxidation or hydroxylation, forming 5-hydroxymethylcytosine, or 5-hmC, through oxidative stress. This can tremendously affect interactions with DNA-proteins that can prevent their binding affinity to MBPs, leading to potentially heritable epigenetic alterations.
The methods and techniques commonly utilized to determine DNA methylation can’t distinguish between 5-mC and 5-hmC, which may prove to be an essential distinction, especially in the brain, where most DNA hydroxymethylation can be found. There is outcome measures which demonstrate that acute psychological stress can increase DNA hydroxymethylation in the hippocampal glucocorticoid receptor gene. This epigenetic alteration can lead to the development of neuropsychiatric and neurodegenerative disorders. Aging is also associated with increases in 5-hmC in the brain which may be prevented by caloric restriction and antioxidant upregulation.
A variety of research studies have found that DNA methylation can be affected by inflammation, most commonly caused due to oxidative stress. Increasing outcome measures have also demonstrated that methylation activity may become affected in response to both nutritional and environmental influences. Alterations in DNA methylation caused by inflammation and oxidative stress can lead to problems in gene expression, increasing the potential risk of disease. Understanding the effects of inflammation due to oxidative stress is fundamental when investigating epigenetic mechanisms. DNA methylation assessments based on inflammation and oxidative stress can help patients regulate their overall health and wellness.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
Smoothies and Juices for Methylation Support
While many healthcare professionals can recommend nutritional guidelines and lifestyle modifications to improve methylation support, there are several options you can try yourself at home. As described above, methylation support supplementation should be determined by a healthcare professional. Smoothies and juices are a fast and easy way to include all the necessary nutrients you need for methylation support without any side-effects. The smoothies and juices below are part of the Methylation Diet Food Plan.
Sea Green Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup cantaloupe, cubed � 1/2 banana � 1 handful of kale or spinach � 1 handful of Swiss chard � 1/4 avocado � 2 teaspoons spirulina powder � 1 cup water � 3 or more ice cubes Blend all ingredients in a high-speed blender until completely smooth and enjoy!
Berry Bliss Smoothie Servings: 1 Cook time: 5-10 minutes � 1/2 cup blueberries (fresh or frozen, preferably wild) � 1 medium carrot, roughly chopped � 1 tablespoon ground flaxseed or chia seed � 1 tablespoons almonds � Water (to desired consistency) � Ice cubes (optional, may omit if using frozen blueberries) Blend all ingredients in a high-speed blender until smooth and creamy. Best served immediately!
Sweet and Spicy Juice Servings: 1 Cook time: 5-10 minutes � 1 cup honeydew melons � 3 cups spinach, rinsed � 3 cups Swiss chard, rinsed � 1 bunch cilantro (leaves and stems), rinsed � 1-inch knob of ginger, rinsed, peeled and chopped � 2-3 knobs whole turmeric root (optional), rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Ginger Greens Juice Servings: 1 Cook time: 5-10 minutes � 1 cup pineapple cubes � 1 apple, sliced � 1-inch knob of ginger, rinsed, peeled and chopped � 3 cups kale, rinsed and roughly chopped or ripped � 5 cups Swiss chard, rinsed and roughly chopped or ripped Juice all ingredients in a high-quality juicer. Best served immediately!
Zesty Beet Juice Servings: 1 Cook time: 5-10 minutes � 1 grapefruit, peeled and sliced � 1 apple, washed and sliced � 1 whole beet, and leaves if you have them, washed and sliced � 1-inch knob of ginger, rinsed, peeled and chopped Juice all ingredients in a high-quality juicer. Best served immediately!
Protein Power Smoothie Serving: 1 Cook time: 5 minutes � 1 scoop protein powder � 1 tablespoon ground flaxseed � 1/2 banana � 1 kiwi, peeled � 1/2 teaspoon cinnamon � Pinch of cardamom � Non-dairy milk or water, enough to achieve desired consistency Blend all ingredients in a high-powered blender until completely smooth. Best served immediately!
ProLon� Fasting Mimicking Diet
Balanced methylation support can be achieved through proper nutrition. The ProLon� fasting mimicking diet offers a 5-day meal program which has been individually packed and labeled to serve the foods you need for the FMD in precise quantities and combinations. The meal program is made up of ready-to-eat or easy-to-prepare, plant-based foods, including bars, soups, snacks, supplements, a drink concentrate, and teas. The products are scientifically formulated and great tasting. Before starting the ProLon� fasting mimicking diet, 5-day meal program, please make sure to talk to a healthcare professional to find out if the FMD is right for you. The ProLon� fasting mimicking diet can help promote methylation support, among a variety of other healthy benefits.
Many doctors and functional medicine practitioners may recommend higher doses of methyl donors in several patients, however, further research studies are needed to determine the proper amount of methylation supplementation. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Acute Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly, Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
Functional Medicine Doctor Explains Women’s Hormones
We discussed the basics for men�s hormones. Now let�s discuss the basics for women�s hormones. Unfortunately, the effects of our diet and our environment become more obvious in the anatomy and biochemistry of women. These may frequently manifest as hormone imbalances and they can greatly affect their quality of life. Mood disorders have become an epidemic.
By way of instance, depression affects 20 percent of women, about twice as much in women than in men. And premenstrual syndrome, or PMS, affects between 60 and 75 percent of women in the United States. Infertility is also an epidemic which affects more than one in seven couples and it is generally managed by reproductive endocrinologists through invasive procedures, hormone treatments, and in vitro fertilization, or IVF, often without even evaluating what is the cause of the reproductive health issues. I�ve helped many women improve their hormone imbalances through the basic principles of functional medicine.
Now, these are only several of the reasons why we need to determine the source of hormonal imbalances in women. And I believe this knowledge can help women find the answers they need to improve their overall health and wellness. Most importantly, you need to learn to listen to what your body is telling you. After all, the human body is one of the best doctors.
Taking Control of Women’s Hormones
Women�s hormones are much more complex than men�s hormones because they�re constantly changing based on their cycle as well as on their stage of life. If you�re experiencing mood swings, irregular cycles, menstrual pain, heavy bleeding, infertility, weight gain, and brain fog, functional medicine can help improve your symptoms by balancing your hormones.
So, let�s discuss the differences between pre-menopausal women and post-menopausal women. Pre-menopausal women should experience regular cycles every 28 days that last two or three days without a lot of pain, not too heavy bleeding, and no PMS. However, most women don�t experience regular cycles. A proper nutrition consisting of low sugar and starch, high fat, and more fiber can help correct abnormal cycles. A plant-rich diet can also help improve abnormal cycles. Caffeine and alcohol consumption can even cause hormone imbalances in women. Proper nutrition, including taking supplements like magnesium, B vitamins and fish oil, exercise, sleep, and stress management can help regulate your hormones. This is generally enough to help most women.
A doctor or functional medicine practitioner can also help balance your hormones. Because women�s hormones fluctuate throughout their cycle, progesterone and estrogen levels may be different for each woman. Also, depending on the hormonal health issues, patients may need to run their hormone lab panel tests on either day three or day 21 of their cycle for best results.
Furthermore, we will also need to evaluate your ratio of hormones, like that of estrogen to progesterone, because these can be the cause of numerous symptoms for many women. Estrogen dominance is one of the most common problems associated with a woman�s hormone ratio. Progesterone levels in women should be at their highest during the last half of their cycle. The hormone ratio between progesterone and estrogen should be 10 to one. However, if the human body is not producing the required amounts of progesterone, symptoms of estrogen dominance may begin to manifest, regardless if the human body�s estrogen levels themselves are low. Symptoms of estrogen dominance can include: anxiety, heavy bleeding, PMS, breast tenderness, shorter cycles or spotting between cycles, infertility, fluid retention, weight gain, and sleeping problems.
FSH is produced by the brain to help the follicles and the ovaries prepare to release an egg. LH is another hormone produced by the brain which triggers the release of an egg into the uterus so that conception can occur. LH also helps produce progesterone during the second half of your cycle, which may be another reason why many women have low progesterone levels.
These hormones are fundamental to look at if you�re trying to have a baby. The elevated hormone ratio between LH and FSH can demonstrate the presence of a common health issue known as PCOS or polycystic ovarian syndrome. PCOS is actually not an ovarian health issue. As a matter of fact, it�s a common problem associated with a poor diet and insulin resistance. An increased consumption of sugar and starch can cause irregular cycles, heavy bleeding, acne, hair loss, and infertility.
As for post-menopausal women, hormone blood panel tests are just as important and we generally don�t need to worry about having to evaluate them on a specific day of the month. Also, when we test a woman who�s in their perimenopause, their hormones may be tremendously unstable. Therefore, it�s ultimately essential to diagnose a woman�s symptoms to help treat the source of the health issue.
We previously discussed the importance of testosterone in men. However, testosterone is also important in women. Many women visit numerous doctors after experiencing low energy levels as well as a decreased sex drive. Most doctors will associate these symptoms with aging or they may even tell them it�s all in their head and simply prescribe them some Prozac. But if we were to run a blood panel test on them, their testosterone levels would often come back undetectable. It�s no wonder why women don�t feel like themselves after they�ve lost their libido and their vitality.
Total testosterone levels in women should be between 60 and 80 while free testosterone levels should be over 0.5. Testosterone is fundamental towards maintaining lean muscle mass and optimizing energy. Testosterone is also important for clear brain function.
Now women, if you have low testosterone levels, this may be causing you to experience a reduced sex drive or it may even be making you feel fatigue. However, this isn�t always the cause of these symptoms. That�s why it�s so essential for women to test their sex hormone levels. Testosterone is what is known as an androgen, or a male hormone, but it�s also found in women. Other androgens that help contribute to male characteristics include androstenedione, dihydrotestosterone, or DHT, and DHEA. In polycystic ovarian syndrome, or PCOS, women will commonly develop elevated levels of any of these hormones. Women who consume a lot of sugar and starch may also develop acne, hair loss or they may even grow facial hair. All of these are symptoms of too much testosterone in women.
PCOS affects approximately 8 to 12 percent of women. As previously mentioned, this health issue is a metabolic problem caused by poor nutrition which ultimately affects the human body�s insulin levels. It can also affect other hormones, such as the androgens we previously discussed. When women develop insulin resistance, the production of male sex hormones can increase. Other tests are important when PCOS is caused by FSH and LH hormones.
FSH generally triggers ovulation. However, if a woman�s FSH is too low due to PCOS, ovulation, and therefore, conception can�t occur. This is why women with PCOS are also commonly diagnosed with infertility. And the key is in a woman�s LH to FSH ratio. Increased levels of LH can stimulate androgens, such as testosterone, and decreased levels of FSH can stimulate the follicles and estrogen. Furthermore, facial hair or thinning of the head hair, irregular menstrual cycles, heavy bleeding, and weight gain in women can be symptoms of PCOS. Although PCOS is believed to be a health issue which exclusively affects overweight women, we�re starting to see an increase of women with healthy weights develop PCOS.
Because functional medicine focuses on finding the source of the health issue, if we see cysts on your ovaries or if any other lab tests indicate the presence of PCOS, we won�t simply stop there. And most often, we just have to look back at the patient�s diet. The high consumption of sugar and starch causes a tremendous metabolic disturbance which can cause a variety of other health issues. We will discuss these various metabolic conditions in another article.
Hormones are fundamental to women’s health. Female sex hormones, including estrogen and progesterone, influence a woman’s mood, menstruation, pregnancy, menopause, and more. A variety of other hormones can also affect other aspects of a woman’s health. One of the most common health issues associated with hormonal imbalances in women is known as polycystic ovarian syndrome or PCOS. Women can be tremendously affected by hormone fluctuations. It’s essential for women to seek help from a doctor to find out if their symptoms are caused by hormone imbalances. Functional medicine can also help regulate hormones. Dr. Alex Jimenez D.C., C.C.S.T. Insight
Understanding Women’s Hormones
We measure hormonal imbalances through simple blood tests and we can also measure hormones through urine tests. Tests known as the �DUTCH� and the �Essential Estrogens� are provided by Genova to determine hormone metabolites. These can also determine the downstream breakdown products of hormones in order to help demonstrate what�s happening with your hormone metabolism.
Now, let me explain what are some of the most important things doctors or functional medicine practitioners look at when ordering a DUTCH test or an Essential Estrogens test. Hormone metabolism tests demonstrate your absolute hormone levels as well as which types of metabolites are being triggered. And this is what we utilize to look at your estrogen levels, androgen levels, and progesterone levels, as well as your cortisol levels, which we will discuss later. These are essential metabolites that can be found through our saliva, blood, and urine. We even look at all the different varieties of estrogens which get broken down by the liver.
So, it�s fundamental that we look carefully at our hormone levels. Testing for hormonal imbalances in both men and women can tell us a lot about what�s causing our symptoms as well as what we can do to treat them. We can recommend a series of lifestyle modifications, including guidance and advice in nutrition and exercise. At least that�s what a good functional medicine doctor would do.
The scope of our information is limited to chiropractic and spinal health issues as well as functional medicine topics and discussions. To further discuss the subject matter, please feel free to ask Dr. Alex Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion:�Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief. �
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
Functional Medicine Doctor Explains Men’s Hormones
Hello there, it�s Dr. Alex Jimenez again and welcome to part four of �Taking Control of your Healthcare�. Today, we�re going to discuss hormones. Hormones regulate most of the human body�s systems as they are recognized as the messenger molecules of the endocrine system. Hormone imbalances can cause subtle changes, however, their effects can tremendously impact an individual�s overall health and wellness. And what�s worse, most healthcare professionals don�t treat hormonal imbalances unless they�ve already been considered extreme.
The sex hormones, the thyroid hormones, and the adrenal hormones are the most important hormones we have to keep in balance. There�s a variety of other hormones, of course, but health issues associated with those are often more rare. Many doctors generally won�t test a person for hormone imbalances unless they�ve been trying to conceive a baby or they have sexual dysfunction or any other health issue of this type. And frequently, many doctors miss other problems by performing a screening test rather than a complete test.
What are Hormones?
Hormones are essential towards mental health, gut health, and reproductive health. In functional medicine, we even believe that hormones are vital towards maintaining a healthy immune system. Even if you�re not trying to conceive a baby or if you don�t have sexual dysfunction, it�s important for both men and women to known what their hormone levels look like.
Now, let�s discuss hormonal imbalances in sex hormones. First of all, How does a hormone imbalance manifest itself? Do you experience mood swings and fluctuations in your energy levels? Or if you�re a female, do you experience symptoms of PMS? Or perhaps you need coffee to wake up in the morning and wine to sleep at night? Has your sex drive, or libido, decreased? Do you have brain fog? Or is it difficult for you to focus on tasks?
If you�ve experienced any of these symptoms, you might have a hormonal imbalance in your sex hormones. Hormones are small molecules in charge of transmitting signals from one body system to another. But, if these molecules aren�t functioning accordingly, our energy levels and our mood can be tremendously affected. If you feel that something is off within your own body, talk to your doctor and seek proper testing. Don�t simply guess.
Let�s begin by discussing how you test your hormones. In functional medicine, we can test through saliva, blood, urine, and even stool. But, which is best for testing hormones? The truth is, knowing how and when to test your hormones is important because testing can depend on the marker that you want to look at. By way of instance, blood testing is one of the best and most affordable if you�re simply looking for a preliminary screening. A functional medicine doctor can also determine when a urine test will be more helpful than a blood test or a saliva test.
Taking Control of Men’s Hormones
So, now that you know how to test your hormones, we�ll discuss the different health issues caused by hormonal imbalances in the sex hormones of both men and women. First, let�s talk about men. As for the women, this is still an essential topic for you to learn about because the men in your lives are much less likely to schedule a doctor�s appointment for themselves.
Approximately 39 percent of men over the age of 45 have low levels of testosterone, or what�s known as low T. Elevated insulin levels associated with diabetes and obesity can lower your testosterone levels, which in turn, can increase estrogen levels. When testosterone goes down, your sex drive, or libido, and other functions can be tremendously affected. Excess consumption of sugar and starch can have different impacts for both men and women. Additionally, the utilization of certain drugs and/or medications, lack of exercise and physical activity, as well as inflammation, can also contribute to lower testosterone levels. While the majority of doctors won�t test testosterone levels in a man unless they have sexual dysfunction, I always want to make sure to test the sex hormones if a man has belly fat.
I would also like to discuss the serious side effects of a drug/medication which is commonly prescribed for sexual dysfunction. Statins can help lower cholesterol, however, did you know that your testosterone is made from cholesterol? That�s right. And when you start taking a drug/medication which was designed to decrease your cholesterol, you may also potentially be decreasing your sex hormones. It�s well-known that statins can decrease testosterone, leading to sexual dysfunction and even sometimes causing men to grow breasts, a condition known as gynecomastia. Side effects like these occur when we don�t treat the source of a health issue.
What you eat, including mainly sugar and starch, can be associated with your low testosterone levels and your abnormal cholesterol levels. Treatments like these where you take a drug for one thing but then end up taking another medication for the side effects of the fist medicine is unfortunately something that happens a lot in the medical field, and it can be a real nightmare.
Male testosterone levels are decreasing so much with each generation that normal reference ranges for testosterone levels in males are changing. But, that�s not something we want to happen. We don�t want these abnormal changes to become normal. Therefore, shouldn�t we be trying to find out why the overall health and wellness of our population is decreasing at such an alarming rate rather than lowering our normal standards of well-being?
Before we do that, however, we first have to understand why this problem is happening. From our increased exposure to toxins and our elevated levels of stress to our higher consumption of processed foods, these are only several of the more obvious reasons why our hormones are being affected.
In conventional medicine, the reference ranges for testosterone are between 264 and 916.
When you think about it, however, this is a tremendous range. Does a man with a testosterone level of 265 have the same sexual function as a man with a testosterone level of 916? Most definitely not. Yet these two people are classified under the same category. And with that in mind, what are the optimal reference ranges for testosterone? Men under the age of 30 should have a testosterone level of over 700, and men over the age of 30 should have a testosterone level of at least 500.
Evaluating men�s total testosterone levels is essential but we also need to evaluate their active hormone levels, or their free testosterone levels. Testosterone is carried around on what is known as a sex hormone binding globulin, which then releases it as the human body needs it. This carrier protein is found in the blood and when there�s too much of it, it becomes difficult for the human body to release testosterone when it�s needed.
In men, free testosterone levels should be of at least 10 but, they should optimally be closer to 15 or 20. Additionally, your doctor should check the sex hormone binding globulin or SHBG. As we discussed before, this carrier protein for testosterone and other hormones, can decrease your free testosterone levels. If you don�t check your SHBG, your total testosterone levels might be normal but your free testosterone levels might be too low.
By way of instance, SHBG is similar to a bus filled with many workers. In this case, the workers are testosterone. When we have too many buses, the majority of the workers will stay on the bus while only a few will be out doing their job. A man can have a total testosterone level of 700, however, if they have a free testosterone level of only 5, they�re bound to still feel like they have a total testosterone level of 300.
In summary, we want to make sure that our total testosterone level is over 500 or better, over 600 and we also want to make sure that our free testosterone level is between 15 and 20.
Another hormone you might want to make sure you get tested for is known as dehydroepiandrosterone, or DHEA. DHEA is a precursor hormone for testosterone. It�s also an adrenal hormone, however, we will discuss this later in another article. If an individual�s DHEA is too low, it can indicate that the adrenal glands, which are in charge of the human body�s stress response, may not be functioning appropriately. DHEA levels should be between two to 400.
DHEA, or dehydroepiandrosterone, can be supplemented directly. Many doctors and functional medicine practitioners may also implement stress-relieving methods and techniques into your life, such as mindfulness meditation and yoga, to treat the source of the health issue. Herbal supplements can also help regulate DHEA as well as testosterone levels.
Now, we will discuss a fundamental hormone that is generally only considered to be important in female health, however, this hormone also plays an essential role in men; estrogen. Estrogen helps maintain a healthy sex function as it promotes your libido. It is also protective for the brain. In men�s health, estrogen is often demonized because it can cause health issues like breast development if estrogen levels are too high in men. But, normal estrogen levels are fundamental towards maintaining hormone balance as well as mental health.
Estrogen can increase in men with diabetes and obesity. Elevated insulin exchanges more testosterone into estrogen which may cause additional symptoms like fatigue. This can also create more problems alongside sexual dysfunction, including hair loss. So, if you have less than optimal testosterone levels, you should seek help from a doctor or functional medicine practitioner to find out why. And looking at your estrogen levels is a great place to start.
There are two types of estrogen tests which can help demonstrate your estradiol and estrone levels. These are important markers to look at because one can be elevated while the other can be in the normal range. The brain is the other place you can look at to determine your estrogen levels. Your brain produces hormones which can stimulate sex hormones, such as the follicle stimulating hormone, or FSH, and the luteinizing hormone, or LH, which helps produce testosterone and sperm within the testicles. If your LH is low, then your low testosterone levels may be caused by a brain health issue. However, it�s much more likely that sugar and starch consumption may be causing hormonal imbalances in your sex hormones.
Approximately 70 percent of the testosterone deficiencies in the United States are associated with insulin resistance due to diabetes and obesity. So, if your diet is filled with sugar and starch or if you have belly fat, you may already have decreased testosterone levels.
Hormones are secreted directly into the blood stream in order to control a variety of bodily functions. These can affect growth and development, mood, sexual function, reproduction, and metabolism. As a fundamental part of the endocrine system, hormone imbalances can have a tremendous effect on our overall health and wellness. Men’s hormones, by way of instance, can significantly impact a man’s quality of life. Research studies have demonstrated that decreased testosterone in men can cause a variety of health issues. Evaluating sex hormones in both men and women is essential towards overall health and wellness. Dr. Alex Jimenez D.C., C.C.S.T. Insight
Understanding Men’s Hormones
While we keep discussing the importance of lab tests, we also need to keep asking ourselves why these health issues are happening in the first place. The answers trace back to the basics of health and wellness. What are you eating? Do you participate in exercise or physical activities? Do you sleep properly? Do you have stress? What are your nutrient levels? Of course, several of these answers require more evaluations. That�s why I highly recommend you find a functional medicine doctor who can help get you on the right path towards optimal health and wellness. Most of the time, basic lifestyle modifications including diet, exercise, stress management, sleep and supplements can help. Other times you may need hormone replacement therapy.
The scope of our information is limited to chiropractic and spinal health issues as well as functional medicine topics and discussions. To further discuss the subject matter, please feel free to ask Dr. Alex Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion:�Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
Each chemical reaction which occurs in the human body requires enzymes and each one of these processes needs a coenzyme. But what are coenzymes? They are vitamins and minerals. Approximately 37 billion, billion chemical reactions occur in the human body every second.
That is why proper nutrition and a balanced diet rich in whole foods with vitamins and minerals is fundamental towards overall health and wellness. The majority of people in the United States are vitamin and/or mineral deficient. But, how do you know if you�re a part of the 90 percent of individuals with enough deficiencies to develop disease? We will discuss the tests you can utilize to find out if you�re vitamin and/or mineral deficient and what you can do about it.
What�is�Nutrition?
Hello, welcome to part three of �Taking Control of your Healthcare�. Today, we will discuss one of the fun topics of functional medicine: nutrition. Unfortunately, nutrition is one of the most essential conversations that many doctors aren�t willing to have with their patients. The average medical doctor learns about disease and malnutrition rather than learning how to use nutrition as treatment or even how to use nutritional therapies to achieve optimal health and wellness.
I personally believe that food can be utilized as a form of medicine. That it should be the foundation of medical practice, not an afterthought in medicine. There is no better treatment than proper nutrition. Approximately 90 percent of individuals in the United States aren�t getting the essential nutrients they require for healthy bodily functions. And more than that probably aren�t getting enough nutrients to prevent diseases associated with nutritional deficiencies. However, what is ultimately needed to achieve optimal well-being? More than 98 percent of Americans are deficient in omega-3, 80 percent in vitamin D, 50 percent in magnesium, and 10 percent in vitamin C. Nutrient deficiencies can also continue to cause health issues for years.
Acute diseases, such as rickets, scurvy, beriberi, or iron deficiency anemia, are often the most talked about health issues associated with nutrient deficiency, however, there�s also something known as long latency deficiency diseases. So, how much vitamin D do we need to not get rickets? Not a lot, only 30 units really. And how much do we need to not get osteoporosis? Perhaps about 3,000 to 4,000 units per day. Now, how much folate do we need to not get anemia? Also not very much. But, how much do we need to prevent heart disease, cancer, and dementia? You definitely need a lot more units per day.
Each chemical reaction which occurs in the human body requires enzymes and each one of these processes needs a coenzyme. But what are coenzymes? They are vitamins and minerals. Approximately 37 billion, billion chemical reactions occur in the human body every second.
That is why proper nutrition and a balanced diet rich in whole foods with vitamins and minerals is fundamental towards overall health and wellness. The majority of people in the United States are vitamin and/or mineral deficient. But, how do you know if you�re a part of the 90 percent of individuals with enough deficiencies to develop disease? There are only several nutrients which we are generally tested for. And for a majority of these, doctors aren�t aware of what the optimal values should be which can make correcting the nutrient deficiency so much difficult to do.
Taking Control of Your Nutrition
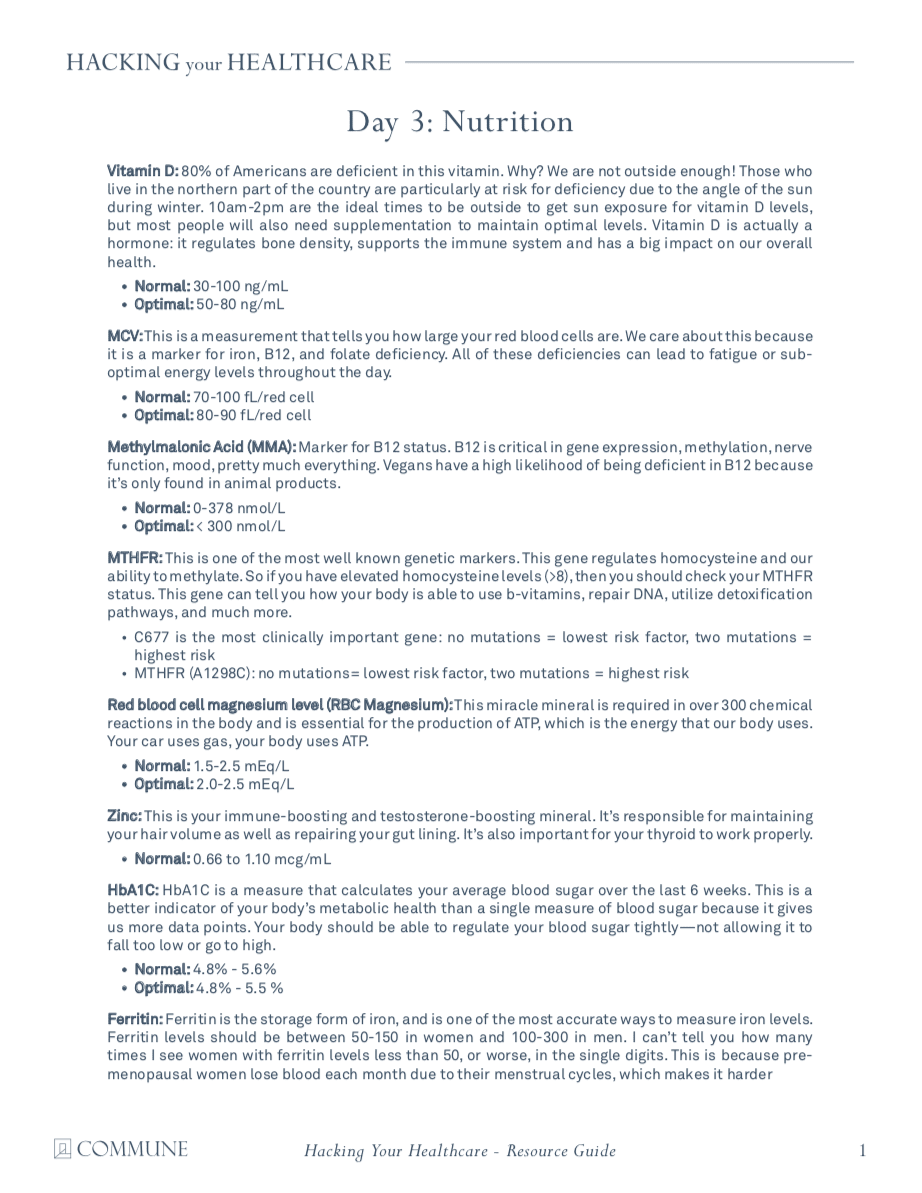
One of the most fundamental nutrients you need to measure is vitamin D. Although it�s referred to as a vitamin, it�s actually more like a hormone and it�s produced from cholesterol. This is yet another reason why cholesterol is essential. Approximately 80 percent of the population is deficient in vitamin D. Unless you�re in the sun 20 minutes every day between 10:00am and 2:00pm, you might need to take vitamin D supplements. In order to supplement properly, however, we need to know from what level you are starting at first. By way of instance, optimal vitamin D levels should be anywhere between 50 and 80 nanograms per milliliter of blood. The recommended amount of vitamin D we can supplement is about 2,000 to 4,000 units.
If you have lower vitamin D levels or if you have genetic problems, you may actually need to supplement with up to 10,000 units of vitamin D. That�s why it�s fundamental to work with a doctor or functional medicine practitioner who can measure and test your nutrient levels as well as help you optimize them. Most supplements contain about 400 units which is 10 times less than the amount most of us need. The optimal levels are generally just over 20. This is way too low. In one research study, women with vitamin D levels between 45 and 60 experienced reduced preterm labors by up to 60 percent. Vitamin D is also essential to help build strong bones and muscles, to improve immune system function, to prevent cancer, and ultimately, to help you live longer. It�s incredible.
Another measurement or test that�s performed by most doctors but is not always interpreted correctly is referred to as the MCV or mean corpuscular volume. The MCV measurement evaluates the size of your red blood cells in a test called CBC, or complete blood count, which is one of the most common blood panels ordered by healthcare professionals. So, if you are deficient in nutrients, your cells can either become smaller or larger. By way of instance, if your cells are too big, it could be a signs of a folate or vitamin B12 deficiency.
B vitamins are essential in numerous chemical reactions within the human body. They help us produce energy as well as help us regulate gene expression in order to create proteins that will ensure our overall health and wellness. If our B vitamins are too low, we could eventually develop an iron deficiency, anemia, or it could even cause a genetic disorder.
Optimal levels of B vitamins should be between 80 to 90. B complex vitamin supplements can help easily optimize levels of B vitamins. But, why would anyone be deficient in B vitamins? Is their diet not providing them with enough nutrients? Are they vegan? Are they taking any drugs and/or medications that prevent vitamin B12 absorption? Moreover, B vitamins are depleted during times of high stress which, as a practicing chiropractor, I can say it happens frequently to a majority of the population in the United States alone.
MCV is not the only measurement or test which evaluates a patient�s levels of B vitamins. Homocysteine is an alternative marker we will discuss in future articles which demonstrates B6, folate, and B12 levels. However, both the MCV and the homocysteine measurement or test only demonstrates that one or more of these nutrients may be deficient. It doesn�t necessarily tell us which one. Therefore, some additional, follow up evaluations may be required.
The MMA, or methylmalonic acid, measurement or test also shows vitamin B12 levels. Ultimately, vitamin B12 is essential for many processes in the human body, including energy production, gene expression, methylation, nerve function, and mood, among many other processes. Vegans have a higher chance of developing a B12 deficiency because it�s only found in animal products. Folate is another fundamental B vitamin. It can be determined directly in the blood, but, homocysteine is a more precise marker for folate levels.
In this section, we�re also going to discuss genetics because there is a measurement or test which can demonstrate a lot more regarding the status of your B vitamins and your ability to utilize them. Our genes are capable of making proteins. We have approximately 20,000 genes which are designed to create proteins. And one third of all the proteins they make are for our enzymes. Enzymes convert molecules into other molecules. These enzymes are also largely dependent on specific nutrients. One of the most fundamental genes which can be affected is known as MTHFR, or methylenetetrahydrofolate reductase. But you can just call it MTHFR.
MTHFR is essential because it helps regulate methylation, homocysteine, and folate, which are vital towards our overall health and wellness. When you have elevated levels of homocysteine, you should check your methylation status by looking for the MTHFR gene through a simple blood test.
Methylation is a key biochemical process which is fundamental towards the proper function of most of the human body�s systems. It triggers billions of times each second. And it ultimately helps control homocysteine, a substance which can damage blood vessels and has been associated with dementia, heart disease, and cancer, among other health issues. Methylation also helps repair your DNA on a regular basis as it helps recycle molecules necessary for detoxification, or getting rid of toxins. It also helps control your mood and it helps manage inflammation. Methylation is critical.
But, to make sure that methylation is active, the human body needs optimal levels of B vitamins. Without enough B vitamins, the methylation process can break down and the effects can be destructive. This is where we start seeing an increase in birth defects, such as spina bifida, down syndrome, and more miscarriages.
MTHFR is frequently abnormal in approximately 35 percent of the population. Methylation breakdown can also increase the risk of developing health issues like osteoporosis and diabetes, cervical dysplasia or cancer, including colon cancer and lung cancer, and even depression, pediatric cognitive dysfunction as well as mood and behavioral disorders, dementia, and stroke. Methylation is truly a key biochemical process.
When we discuss genetics, we have to understand that our environment can alter our genes. So, what if you have an MTHFR variation in your genes? First of all, not all mutations cause health issues. One mutation, by way of instance, known as C677T, is one version of the gene which is more significant than another version of the gene, known as A1298C. Now there�s no need to worry about these gene variations. They serve as examples to demonstrate you the quality of these mutations and how they function. People with these variations of the gene, by way of instance, might only need more folate or they might need a particular type of folate known as methylfolate. This is where a functional medicine practitioner can help their patients.
A genetic test can let you known if you have one of these gene variations. But, don�t get stressed. There�s a lot you can do to optimize your overall health and wellness. Many patients have visited my office after they find out they have these variations in their genes. And they quickly learn that they do have the option to take control of their well-being. However, what you do control is not your genes, you control your gene expression.
If you alter your healthy eating habits, you alter your nutrients. If you alter your environment, you alter which genes become active and which genes become inactive. And with these mutations, you can do just about the same thing by simply following the proper nutrition. When you find a doctor or functional medicine practitioner that�s willing to work with you, they�re going to tell you what lifestyle modifications you should follow to prevent health issues.
So, we�ve only just discussed the B vitamins. Next, we will discuss another fundamental nutrient in the human body: magnesium. Magnesium is a super essential mineral. Approximately 48 percent of people in the United States consume less than the required amount of magnesium from food. Magnesium is necessary in over 300 chemical reactions in the human body. It is also fundamental in the production of ATP, or the energy the human body utilizes as fuel.
A magnesium level blood measurement or test can help determine if you have a deficiency. Magnesium can also help reduce anxiety, calm the nervous system, and improve sleep. It is also an essential nutrient in the management of blood sugar levels. If you�ve been told by a healthcare professional that you have an average blood sugar level of over five and a half in something known as A1c, then magnesium can help.
Also, it�s very easy to know if you have a magnesium deficiency by looking at your current diet and symptoms. Do you eat enough magnesium rich foods like dark, leafy greens, beans, nuts and seeds? Or do you eat a lot of processed foods? Perhaps you also have symptoms such as anxiety, insomnia, constipation, muscle twitching, muscle cramps, PMS, and/or palpitations. If you have one or more of the symptoms I just mentioned, you may have a magnesium deficiency.
Next, we will talk about zinc, the immune-boosting and testosterone-boosting mineral in the human body. This important nutrient is in charge of maintaining your hair volume as well as repairing your gut lining. It�s also responsible for making sure your thyroid is functioning properly. Zinc can be easily measured or tested in the blood and unfortunately, it�s another nutrient we are highly deficient in, in the United States. Additionally, you can also look at your alkaline phosphatase levels, which can be calculated through a liver function evaluation on a regular blood panel. High levels of alkaline phosphatase may indicate the presence of cancer or bone problems, among other health issues, however, low levels of alkaline phosphatase may indicate a zinc deficiency, because it�s a zinc-dependent enzyme.
Finally, the last fundamental nutrient we are going to discuss is iron. Iron is frequently deficient in vegans and vegetarians, or in women in general due to menstruation. Iron is necessary for transporting oxygen throughout the human body and it�s ultimately essential for brain health and wellness. Iron is also important for hair and nails, sleep, and so many other things.
Ferritin is a stored type of iron and it�s this nutrient which helps you see your iron levels. Optimal ferritin levels should be between 50 to 150 in women and 100 to 300 in men. And many times I�ve seen women visit my office who have ferritin levels of less than 50, or worse, in the single digits. This is because pre-menopausal women lose blood every month due to their menstrual cycles and it becomes so much harder for them to maintain proper ferritin levels. Many women also eat way less than what they�re supposed to be eating every day. High levels of ferritin, on the other hand, could be a sign of inflammation, generally caused by insulin resistance to sugar, or it could be a sign of hemochromatosis or iron storage disease, a very dangerous genetic disorder.
Having decreased levels of ferritin can also make you feel tired, and it can cause hair loss, it can cause insomnia. So, even if your blood count is normal, if your ferritin levels are low or your iron levels are low, it can also cause these symptoms. That�s why if you experience symptoms of fatigue, it�s essential to measure or test your ferritin levels. And it can be easily supplemented.
Aside from ferritin, a low MCV can also determine if you have an iron deficiency. Iron deficiencies can cause red blood cells to become very small and that can be demonstrated in low MCV levels, which evaluate the size of your red blood cells. Additionally, transference saturation, serum iron, TIBC, or total iron binding capacity, and hemoglobin, can provide us with a more in depth look at your iron status to distinguish different causes of anemia. These are included on a regular iron blood panel in a lab test.
We�ve discussed several nutrients which can be ordered by a majority of healthcare professinals with access to conventional lab testing. Furthermore, there�s another test which can tell us more about which type of nutrients we need based on our genes. It�s called the DNA health test and it�s provided by a company called DNAlife. This test evaluates a variety of genetic markers associated with detoxification, lipid metabolism, and inflammation, including the MTHFR gene and other B vitamin markers. Now, DNA Health demonstrates the different genes we evaluate. And most of these are common genes, they�re those we can do something about. We analyze the genes we can change based on your nutrition and other lifestyle factors.
It shows us the MTHFR gene, other B vitamin markers, genes that control B6, folate, and B12 as well as demonstrating how they function and whether you have nutrient deficiencies. Then it tells us which nutrients you will need to supplement and how much we will need to give to you. It�s tremendously helpful.
There was an individual who had two variables of the MTHFR gene. This woman had miscarriage after miscarriage after miscarriage. She visited her doctor for an evaluation and it turns out that she had a folate-regulating mutation. So her doctor then started giving her the proper amount of folate she needed and she started having healthy babies. Sometimes, nutrition can be that powerful towards improving a patient�s overall health and wellness.
The DNA health test can help personalize your approach when optimizing your well-being based on your genetics. What we measure utilizing the DNA health test provide well-established insights about your genes as well as what you can do about them.
A micronutrient test known as the individualized optimized nutrition profile or the ION panel, are alternative test options which can also provide information about your current nutritional status. This test is by Genova. This is a robust test which measures all the essential vitamins and minerals, fatty acids, organic acids, and antioxidants you currently have. Ultimately, this test looks for imbalances, insufficiencies, or deficiencies, rather than looking for a specific disease. It looks for things that a majority of doctors never look at.
Functional medicine practitioners or doctors look at patient�s amino acid levels, mineral levels, and even toxin levels from heavy metals like mercury, lead, arsenic, and many more. We also look at your antioxidant levels, vitamin A and vitamin E levels, as well as your CoQ10 antioxidant and beta carotene status. We can determine if a person eats vegetables or not if, by way of instance, they have low levels of beta carotene. We also look at vitamin D levels, essential fatty acids, including your omega-3 fats and your omega-6 fats. We can tell if a person eats junk food. We can tell if a person is eating fish. And We can tell if a person is eating too much olive oil or saturated fats. It�s all demonstrated in these measurements and tests.
An OAT test, or organic acids test, also looks at what is known as organic acids. This test demonstrates a wide array of parameters associated with your mitochondria, which we will discuss in the next article, your B vitamins, your neurotransmitters, your gut flora, and your detoxification. It�s ultimately a comprehensive test which shows me if a patient is well or sick. It shows me where the imbalances are and where I need to recommend lifestyle modifications. It also helps provide clues about other health issues.
By way of instance, if your mitochondria aren�t functioning correctly because you have decreased levels of essential amino acids or you have increased oxidative stress or if you simply have low levels of selenium and zinc, there�s a possibility that you might have some form of toxic overload due to heavy metals. And that�s precisely what I would go looking for. Signs like these provide a lot of information about what we can do to treat a patient. And an experienced functional medicine practitioner or doctor can determine what�s really going on with a patient or they can help patients discover how to optimize their overall health and wellness.
Nutrition is the study of nutrients in food and how the human body utilizes nutrients as well as the relationship between diet, disease and overall health and wellness. Nutrients are a source of nourishment, including carbohydrates, proteins, fats, vitamins, minerals, fiber and water. Functional medicine focuses on the use of food as a form of medicine. A balanced nutrition can help prevent as well as treat a variety of health issues. Similarly, nutrition in functional medicine involves how certain diseases and conditions may be associated with dietary factors, such as poor diet or malnutrition, food allergies and food intolerances. Dr. Alex Jimenez D.C., C.C.S.T.
Understanding Your Nutrition
As good functional medicine doctors we�re often left asking ourselves, why is it that so many people in the United States are overfed but undernourished? Or, why is it that Americans eat too many calories and too few nutrients? The leading causes for the widespread nutritional deficiencies are the following: First, humans evolved from eating wild foods which contained tremendously higher levels of nutrients. Second, the soil we currently utilize to grow our crops in has become greatly depleted of nutrients. Hybridization techniques from industrial farming are yielding animals and vegetables to have decreased levels of nutrients. Third, processed foods have absolutely no nutrients, which is why they frequently have to be fortified. And last but not least, exposure to environmental toxins, lack of sunlight, chronic stress, and poor diet, including increased alcohol, caffeine, and sugar consumption, can increase our nutritional needs, much of which we�re already not getting enough from our current nutrition.
Well you might not need any vitamins, however, if you can meet certain conditions. Perhaps if you only hunted and gathered wild food and if you weren�t exposed to environmental toxins. Or maybe if you went to sleep with the sun and woke up with the sun, sleeping nine hours a night. And if you experienced absolutely no amount of chronic stress. Ultimately if you only drank pure, clean water and breathed pure, clean air. Then, you probably wouldn�t need any vitamins. But the rest of us that don�t follow these conditions, we do need them.
And with that thought, we wrap up this article. In the next article, we will talk about hormones. Hormones can affect almost every aspect of our well-being, and many healthcare professionals don�t understand what our optimal hormone levels should be or even when to test them and what to do about it once they do. Measuring and testing hormone levels should be standard practice, and many patients have never had a blood panel to look at their hormones. It�s fundamental to know as well as understand what�s going on inside your own body. And that�s why this next article is so important. You won�t want to miss our next update. See you soon.
The scope of our information is limited to chiropractic and spinal health issues as well as functional medicine topics and discussions. To further discuss the subject matter, please feel free to ask Dr. Alex Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion:�Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief. �
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine