All sports differ in the relative importance of various physical skills contributing to the game and individual performance. Baseball is a precision sport with fast, explosive movements and full-body activity. The ability to repeatedly perform near maximum level with little rest is necessary for baseball players. Baseball training involves a multidimensional approach that focuses on speed, agility, and strength in a way that is relative to the motions and requirements of the sport.
Baseball Training
Trainers have to assess the unique needs of the sport and determine the time needed to improve each quality within the athlete. They should focus on the following:
Baseball training workouts are targeted at increasing running speed, bat speed, pitching, and throwing velocity that breaks down the muscle groups for improving performance while decreasing the risk of injury. Training consists of combined conditioning that includes:
Throwing a baseball at high velocity is a full-body movement that requires total body development.
Strong leg, hip, and core muscles are necessary to transfer power from the ground, up through the lower body, to the torso, and then the arm and hand to generate a fast, whipping ball release.
This will improve generating power in the throwing muscles.
The objective is to build power utilizing a heavy and then a light load to build arm speed, and using proper form will improve throwing velocity safely.
Proper trunk rotation during arm cocking and strength and flexibility training should involve trunk rotational exercises to develop the obliques so that maximum arm speed can be generated.
Players have to deal with consistent failure and remain confident.
Hitting Mistakes
References
Ellenbecker, Todd S, and Ryoki Aoki. “Step-by-Step Guide to Understanding the Kinetic Chain Concept in the Overhead Athlete.” Current reviews in musculoskeletal medicine vol. 13,2 (2020): 155-163. doi:10.1007/s12178-020-09615-1
Fleisig, Glenn S et al. “Biomechanical Analysis of Weighted-Ball Exercises for Baseball Pitchers.” Sports health vol. 9,3 (2017): 210-215. doi:10.1177/1941738116679816
Rhea, Matthew R, and Derek Bunker. “Baseball-specific conditioning.” International journal of sports physiology and performance vol. 4,3 (2009): 402-7. doi:10.1123/ijspp.4.3.402
Seroyer, Shane T et al. “The kinetic chain in overhand pitching: its potential role for performance enhancement and injury prevention.” Sports health vol. 2,2 (2010): 135-46. doi:10.1177/1941738110362656
Long-distance running, also known as endurance running, is a great way to improve fitness and relieve stress. Health experts say long-distance runners’ benefits include strong cardiovascular health, low cholesterol, healthy blood pressure levels, and improved metabolism. However, it is not easy and requires specific training, but it is not impossible even for beginners. Here is a beginner long-distance running training guide that goes over the fundamental areas needed to develop.
Long Distance Running Training
Running is a great form of cardio that offers several health benefits that, includes:
Weight loss
Stronger muscles
Stronger bones
Improved cardiovascular functionality
One of the main prerequisites is building up the body’s ability to handle the exercise. To reach the full potential as a distance runner, key areas that need developing include:
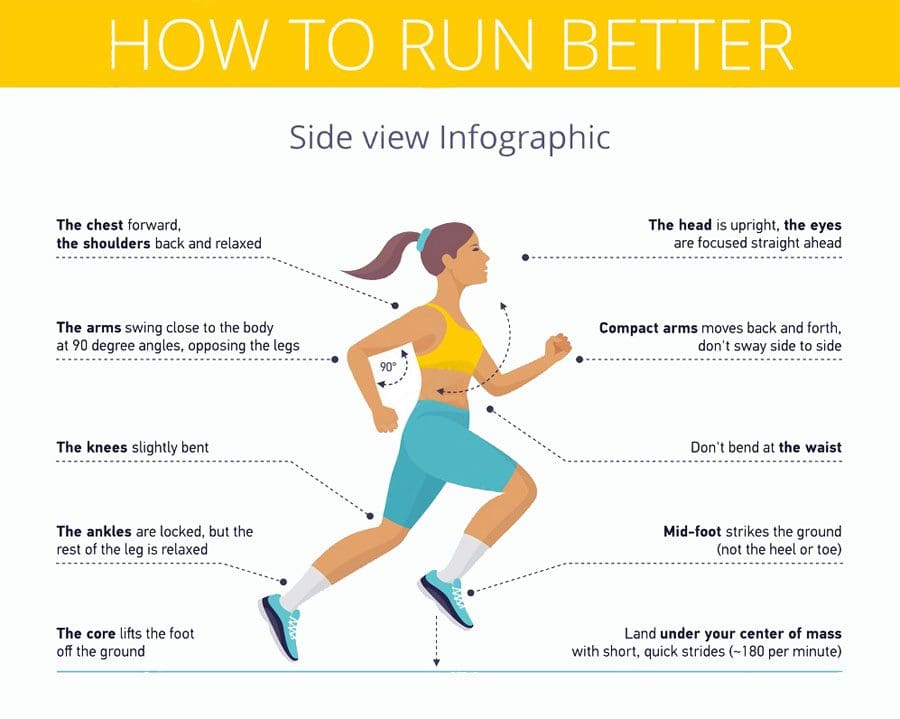
Running technique is essential for gaining the most speed and endurance. Using the correct form, the body is not expending unnecessary energy. The proper running form includes:
Maintaining an upright spine with the head, shoulders, and hips aligned.
Focus on maintaining a steady breathing rhythm.
Follow through on strides.
Do not cut the movements short.
Find your natural stride, which could be leading with the heel or running toe to heel.
Consult an experienced running coach or exercise physiologist for assistance in finding your running form.
Long-Term Goal
The body adapts to the stress of training slowly and over time.
Physiological adaptations cannot be rushed; however, the training program can be optimized to individual needs.
The minimum time before seeing an improvement from training is around six weeks.
Gradual Increase
Training load is a combination of distance, intensity, and the number of runs each week.
The body can only develop with moderate increases over a short time.
Increasing the load too much and too fast leads to injury, illness, and exhaustion.
Limiting distance, intensity, or frequency changes is recommended no more than once a week.
Recovery
Training provides the stimulus to improved fitness, but the body needs recovery time to grow and adapt.
Often beginners want to train hard every day, trying to cover all the elements at once.
This common mistake slows progress and can cause various injuries, fatigue, and loss of motivation.
Rest days are essential to allow the body to recover, develop, adapt, and continue to progress healthily.
The classic training program alternates a hard training day with an easy day or a rest day.
Two consecutive hard training days can be done as long as they are followed by two full recovery days.
Beginner Tips
References
Berryman, Nicolas, et al. “Strength Training for Middle- and Long-Distance Performance: A Meta-Analysis.” International journal of sports physiology and performance vol. 13,1 (2018): 57-63. doi:10.1123/ijspp.2017-0032
Blagrove, Richard C et al. “Effects of Strength Training on the Physiological Determinants of Middle- and Long-Distance Running Performance: A Systematic Review.” Sports medicine (Auckland, N.Z.) vol. 48,5 (2018): 1117-1149. doi:10.1007/s40279-017-0835-7
Kenneally, Mark, et al. “The Effect of Periodization and Training Intensity Distribution on Middle- and Long-Distance Running Performance: A Systematic Review.” International journal of sports physiology and performance vol. 13,9 (2018): 1114-1121. doi:10.1123/ijspp.2017-0327
Tschopp, M, and F Brunner. “Erkrankungen und Überlastungsschäden an der unteren Extremität bei Langstreckenläufern” [Diseases and overuse injuries of the lower extremities in long distance runners]. Zeitschrift fur Rheumatologie vol. 76,5 (2017): 443-450. doi:10.1007/s00393-017-0276-6
van Poppel, Dennis, et al. “Risk factors for overuse injuries in short- and long-distance running: A systematic review.” Journal of sport and health science vol. 10,1 (2021): 14-28. doi:10.1016/j.jshs.2020.06.006
For many athletes following any major endurance event they will return to their houses, to recover, celebrate, reflect and rebuild to their next career step. Some, like the athlete in this case study will need to now focus attention on delayed decisions concerning whether to go under the knife to sort out a chronic injury.�El Paso, TX’s Injury scientist, Dr. Alexander Jimenez takes a look at the study.
My client has been competing in triathlon for 10 or more years, although his career has included a range of serious injuries which have kept him from races for months on end. In the previous two to three decades, however, he’s enjoyed a sustained period of injury-free training and racing, and has climbed to the peak of the world rankings. But the emergence of hip pain has seen him once more return to the physio’s table.
The triathlete’s accident history highlights a common pattern among sportspeople: 2 tibial stress fractures, a femoral neck stress fracture and a serious ankle sprain — every one of these on his right side. The significant contributing element to the bone stress injuries is a 1.5cm leg-length gap (his right leg is shorter).
He’d first experienced comparable hip pain in 2004; it kept him from running for three months. At that time, nothing was detected on a bone scan or MRI, or so the pain went paralyzed. An intra-articular cortisone injection (CSI) elicited no improvement. The athlete remembers that he chose to train on his painful hip, never allowing the symptoms to settle. The nearest he ever came into an investigation was a hypothesis that he could have a little, undetected, labral lesion.
The present episode of hip pain began initially at night after a hard three-hour bicycle ride. Earlier this, however, he hadn’t cycled for five times. He described his initial symptom as a profound hip tightness (lateral and lateral), together with slight pain in his groin. He was able to continue to train however, was feeling that the hip tightness and pain following both cycling and running (swimming was symptom-free).
A week later his symptoms dramatically worsened when he flew from Australia to Singapore, on his way to a French high- altitude camp. As he got off the airplane, he felt deep hip pain as well as the tightness. As elite athletes tend to do, he coached anyway, running a tricky track session, which made the hip much worse: he was unable to ride or run without pain. He instantly started a course of anti- inflammatories.
I met him in Singapore and evaluated him in the airport, initially ruling out any prospect of a disease or systemic matter. He explained he had been feeling an ache during the night, lying in bed; on waking, the hip would be OK, but got worse the longer he walked.
On assessment, he had the following physical signs:
� walking with obvious limp
� pain on hopping (6/10)
�painful right hip quadrant/impingement test (full hip flexion/adduction)
� reduced right hip flexion (-10 degrees compared to left)
� reduced right hip internal rotation (-10 degrees compared to left)
� increased tone on palpation of TFL, adductors, hip flexors, gluteal, piriformis and deep rotators
� lumbar spine and SIJ were OK
� femoral shaft bone stress test was OK � leg length discrepancy (right side 1.5cm shorter)
� right innominate (pelvis) anteriorly rotated
� weakness in right hip abductors/extensors
� reduced calf endurance on right side (-5 reps)
� ankle dorsiflexion range of movement was OK
� reduced proprioception on right (single leg stance, eyes closed).
I thought the differential diagnoses were:
� femoral neck stress fracture
� labral tear, possibly with hip synovitis
� FAI (femoro-acetabular impingement), possibly with hip synovitis.
I initially treated the triathlete with soft- tissue techniques to reduce the tone around the hip joint. Trigger-point releases were performed on his TFL, adductors, gluteals, piriformis, deep rotators and iliopsoas.�This reduced his jump pain into 3/10. Manual long-leg grip further decreased the strain on hopping (2/10). He still had pain and stiffness on walking but it sensed “simpler. As he prepared to embark on his long run flight to Europe, I counseled him to not sit for too long and maintain his stylish as straight as possible to decrease any potential impingement from hip flexion.
Luckily, the hip didn’t get worse throughout the flight. On arrival at the French high-altitude training centre, we initiated a strategy of two swims and two intensive treatments a day, aiming at reducing muscle tone, restoring his range of hip movement and normal muscle control and stamina. We had been expecting that the problem was not a stress fracture, but just minor hip synovitis that could settle quickly. Following a week of conservative treatment, though, we were just able to keep his hop pain in 2/10, and that he still could not run 20 meters without any pain and limping.
In collaboration with medics, we flew to London to see a sports doctor and get MRI scans. The scans revealed no bone stress reaction, fracture or labral ripping — which was a big relief; however, it did show signs consistent with FAI (femoro-acetabular impingement). He had hip synovitis with a rectal lesion on his femur.
Hip injuries aren’t much reported among triathletes — in fact they are notably absent from reports on Olympic and Ironman triathlons, which mention knee, back, H/ Achilles, lower leg, ankle and shoulder as the most common accidents (1-3).
In this state, when the hip is in maximum flexion and internal rotation, the labrum and cartilage abut and impinge; damage to the articular cartilage and acetabular labrum results from this pathologic bony contact. The contact generally results in a structural abnormality of the femur (“camera impingement”) along with the acetabulum (“pincer impingement”) or a combination of both (“mixed impingement”). Over time, via repetitive micro-trauma, the aggravating motion hurts the hip cartilage or labrum (or both) during normal joint motion. This happens along the anterior femoral neck and the anterior–superior acetabular rim. FAI is a possible trigger of early hip joint degeneration (4).
Arthroscopic surgery is the direction of choice for FAI if symptoms do not settle; however as his next Competition was only three and a half a year off, surgery was not an option. Instead, over a five-day interval, the athlete had two cortisone (CSI) and local anesthetic injections into the hip joint (under ultrasound guidance) to settle the indicators.
Our aim was to grow the hip range of motion and extend the capsule to reduce any additional impingement, slowly returning to regular training. Following the competition, the athlete would then should see a hip arthroscopic surgeon to acquire a surgical opinion to the best option for long-term direction.
Injection Relief
After both shots my customer felt sore for five days. The initial CSI settled his pain on hopping to 1/10 and after seven days he managed to operate without symptoms. But minor hip stiffness and aching at the end of the day prevented him from progressing to optimal training, so that he then underwent a second steroid injection. This settled the hop pain into 0/10 and decreased the aching; so after five times he returned to mild cycling and after seven days he started running again, also.
The athlete admitted that, following the first shot, he had done more and gone tougher in training than directed, as he had felt “good. This mistake of “too much too soon — all too common in elite athletes — had led to excessive inflammation and aching in the hip nightly after training. After the next injection he returned to normal intensity slower and more gradually.
My client built his training up to regular levels by four months following the final injection (swimming five times per week, cycling four days and running six to seven days). He began with very easy cycling on a wind trainer for 30 minutes, building slowly to 90 minutes before cycling on the street. He cycled two days on and one day away and avoided hills to the first two weeks. He started jogging on the apartment for 15 minutes and slowly built up to 90 minutes after three weeks. He did not run hills or about the track; and as he ran only on every single day, he would diligently concentrate on technique.
From week six to week 11, my client remained on anti inflammatory medication and underwent two treatments a day.
The hands-on treatment continued to:
� increase hip range of movement
� stretch the hip capsule
� normalise pelvic symmetry and hip muscle tone
� improve muscle control and strength � improve proprioception
� ensure optimal biomechanics via video assessment (cycling and running).
Eleven weeks after he first felt his hip pain, the triathlete returned to racing; however he failed to finish the first race, partially because of minor hip stiffness but mainly due to “fitness. Fortunately there were not any prolonged symptoms after the race and a week after he successfully returned to competition, coming second in a really strong field. His very minor ongoing symptoms were handled with anti-inflammatory drugs and hands-on treatments.
If this athlete wants to pursue a long- term triathlon career up to the London Olympics, then he will now require surgery. The arthroscopic surgical technique initially assesses the cartilage and labral surfaces, debrides any abnormalities of the hip joint cartilage and hip labrum, removes the non-spherical segments of the femoral head�and any prominent sections of the anterior femoral neck and bony growths on the acetabular rim that may continue to contribute to hip joint impingement.�The alternative is early joint degeneration and onset of osteoarthritis.
References:
1. Wilk B et al: �The incidence of musculoskeletal injuries in an amateur triathlete racing club�. J Orthop Sports Phys
Ther 1995 Sep;22(3):108-12.
2. Collins K et al: �Overuse injuries in triathletes. A study of the 1986 Seafair Triathlon�. Am J Sports Med 1989 SepOct;17(5):675-80.
3. Korkia PK et al: �An epidemiological investigation of training and injury patterns in British triathletes�. Br J Sports Med 1994 Sep;28(3):191-6.
4. Ganz R. et al (2003): �Femoroacetabular impingement: a cause for osteoarthritis of the hip�. Clin Orthop Relat Res. 417:112�120. For more information see: www.hipfai.com
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine

 Baseball Training
Baseball Training