Question: I’ve had back pain for awhile and I was able to function through it for a time. But now it’s taking its toll on me, as well as my family. I never believed in chiropractors, but now I’ll try anything. What should I ask my physician about chiropractic?
El Paso, TX. Chiropractor, Dr. Alexander Jimenez has seen this scenario all too often and is happy to inform anyone about chiropractic care and it’s benefits.
About two out of every three people will likely experience significant low back pain at some point. A doctor might suggest any range of potential treatments and therapies. But one that almost is never considered is a referral for spinal manipulation.
It seems doctors have been mistaken for initial treatment of lower back pain.�It may be time for doctors to rethink their chiropractic biases.
Spinal Manipulation:
Along with other less traditional therapies like heat, acupuncture and meditation, chiropractic appears to be as powerful as any other medical treatments doctors prescribe and as safe, if not safer.
Physicians are traditionally wary of spinal manipulation (applying pressure on bones and joints), in part because the practitioners are often not doctors. Patients with back pain don’t seem as skeptical. A survey from 2002 through 2008 found that over 30 percent sought chiropractic care, significantly more than those who sought massage, acupuncture or homeopathy.
Researchers have been looking at the evidence supporting spinal manipulation for a while. Nearly 35 years ago, a systematic review assessed the available research found that there may be some short-term benefits from the process. Two reviews from 2003 agreed for the most part, finding that spinal manipulation worked better than a “sham procedure”, or placebo, but no better or worse than other options.
Recently, in The Journal of the American Medical Association, researchers looked for new studies since 2011, in addition to those that had been performed before.
Evidence from 15 randomized controlled trials, which included more than 1,700 patients, revealed that spinal manipulation minimized their back pain of about 10 points on a 100-point scale. The evidence from 12 randomized controlled trials that overlapped of almost 1,400 patients showed that spinal manipulation also resulted in improved mobility and function.
In February, in Annals of Internal Medicine, another systematic review of non-pharmacologic therapies generally agreed with the recent trials. Based on this review, and other evidence, the American College of Physicians released new clinical practice guidelines for the noninvasive treatment of back pain. They recommended that patients should try spinal manipulation, heat, massage and acupuncture as first-line therapies.
What If The Spinal Adjustment Causes Other Injuries:
Because of the fear of those injuries, physicians are hesitant to refer patients to chiropractors or physical therapists for care. However, in the studies outlined above, there were no serious adverse events reported. It is possible to find stories of injury to the spine from improper adjustments, but these are rare, and almost never involve the lower spine.
What About The Cost:
Some doctors are concerned about the cost of chiropractic, especially since many insurance carriers don’t cover chiropractic. Seeing a chiropractor costs more than taking many non-narcotic pain medications. However, more invasive interventions cost a lot of money. In addition, studies have proven that, in general, users of complementary and alternative medicine spend less for back pain compared to users of only traditional medicine.
Medication and surgery may also result in injuries and prescription pain medicines, like opioids, may result in huge costs, particularly when they’re misused.
Some physicians are uncomfortable that they do not have a clear picture of how spinal manipulation actually works. The reality is that doctors don’t understand why a number of other therapies work either.
Back pain is still the issue and no matter what you do, chiropractic is definitely an option to consider.
Chiropractic: Alternative Approach To Treating Chronic Pain
Question: My car was rear-ended. Since then, my neck hurts, feels rigid, and I have upper back pain. My wife says it’s whiplash and that I should see a physician. Is there anything that I can do to accelerate my recovery? Should I see my physician and/or chiropractor? How long will my pain last?
El Paso, TX
Answer: Your symptoms are typical of a whiplash injury caused by a vehicle accident. Whiplash is cervical spine strain caused when the head and neck are thrust quickly forward and backward. To fully grasp how whiplash can lead to neck pain, you want to recognize the head, which weighs 8-13 pounds and is supported and moved by the neck. Because of this, it’s easy to understand how soft neck muscles and ligaments are stretched during a whiplash accident!
The seriousness of whiplash is dependent on the force of the impact, the way you were seated in your vehicle, and if you were properly restrained with a shoulder and seat belt. By way of instance, if your head was turned, your neck injury may be more painful.
Whiplash Home Treatment Tips
1. Even though your neck injury occurred last week, you may try ice and heat. Ice will help to reduce swollen overstretched muscles and ligaments. Heat increases circulation and eases tight stiff muscles.
Ice: Apply an ice pack for 15 minutes as often as once each hour.
Heat: Apply warmth (moist is greatest!) For 15 minutes every 2 or 3 hours.
Skin Safety:
Never sleep with a ice or heat pack!
Wrap heat or ice in a towel to protect your skin.
Discard punctured store-bought ice or heat products.
2. If your doctor agrees, try an over-the-counter anti-inflammatory medication.
3. Move your neck softly to assist in preventing additional stiffness.
4. Should you work in a computer or desk, take regular breaks to relax your neck muscles.
5. Avoid cradling the phone between your shoulder and head.
6. Avoid carrying heavy packages, especially things such as a pocket book or backpack slung over only one shoulder.
Check With Your Doctor & Chiropractor
Neck pain is common either immediately after or several days following a whiplash injury. Other symptoms can develop too. Fortunately, most symptoms go away in two to four weeks. If your symptoms worsen, or you develop headache, dizziness, blurred vision, difficulty swallowing, arm or hand numbness, check-in with your physician or chiropractor. If necessary, you’ll be referred to a spine specialist.
Your physician or chiropractor will carry out a physical and neurological examination, and acquire a neck X-ray. After they produce a diagnosis, treatment is coordinated for your recovery! Treatment may include prescription pain medication, anti inflammatory drugs, muscle relaxants, a cervical collar, massage and physical therapy.
Other�Symptoms Associated With Whiplash Or Neck Strain:
Headache
Dizziness
Ringing in your ears
Blurred vision
Difficulty concentrating
Difficulty chewing or swallowing
Hoarse voice
Upper back, shoulder, and/ or arm pain
Back pain
Abnormal sensations such as numbness, burning or prickling
Fatigue and sleep problems
Keep in Mind
Most individuals with whiplash improve quickly within a matter of weeks. When you have concerns, we recommend you to speak to a doctor or chiropractor.
For many athletes following any major endurance event they will return to their houses, to recover, celebrate, reflect and rebuild to their next career step. Some, like the athlete in this case study will need to now focus attention on delayed decisions concerning whether to go under the knife to sort out a chronic injury.�El Paso, TX’s Injury scientist, Dr. Alexander Jimenez takes a look at the study.
My client has been competing in triathlon for 10 or more years, although his career has included a range of serious injuries which have kept him from races for months on end. In the previous two to three decades, however, he’s enjoyed a sustained period of injury-free training and racing, and has climbed to the peak of the world rankings. But the emergence of hip pain has seen him once more return to the physio’s table.
The triathlete’s accident history highlights a common pattern among sportspeople: 2 tibial stress fractures, a femoral neck stress fracture and a serious ankle sprain — every one of these on his right side. The significant contributing element to the bone stress injuries is a 1.5cm leg-length gap (his right leg is shorter).
He’d first experienced comparable hip pain in 2004; it kept him from running for three months. At that time, nothing was detected on a bone scan or MRI, or so the pain went paralyzed. An intra-articular cortisone injection (CSI) elicited no improvement. The athlete remembers that he chose to train on his painful hip, never allowing the symptoms to settle. The nearest he ever came into an investigation was a hypothesis that he could have a little, undetected, labral lesion.
The present episode of hip pain began initially at night after a hard three-hour bicycle ride. Earlier this, however, he hadn’t cycled for five times. He described his initial symptom as a profound hip tightness (lateral and lateral), together with slight pain in his groin. He was able to continue to train however, was feeling that the hip tightness and pain following both cycling and running (swimming was symptom-free).
A week later his symptoms dramatically worsened when he flew from Australia to Singapore, on his way to a French high- altitude camp. As he got off the airplane, he felt deep hip pain as well as the tightness. As elite athletes tend to do, he coached anyway, running a tricky track session, which made the hip much worse: he was unable to ride or run without pain. He instantly started a course of anti- inflammatories.
I met him in Singapore and evaluated him in the airport, initially ruling out any prospect of a disease or systemic matter. He explained he had been feeling an ache during the night, lying in bed; on waking, the hip would be OK, but got worse the longer he walked.
On assessment, he had the following physical signs:
� walking with obvious limp
� pain on hopping (6/10)
�painful right hip quadrant/impingement test (full hip flexion/adduction)
� reduced right hip flexion (-10 degrees compared to left)
� reduced right hip internal rotation (-10 degrees compared to left)
� increased tone on palpation of TFL, adductors, hip flexors, gluteal, piriformis and deep rotators
� lumbar spine and SIJ were OK
� femoral shaft bone stress test was OK � leg length discrepancy (right side 1.5cm shorter)
� right innominate (pelvis) anteriorly rotated
� weakness in right hip abductors/extensors
� reduced calf endurance on right side (-5 reps)
� ankle dorsiflexion range of movement was OK
� reduced proprioception on right (single leg stance, eyes closed).
I thought the differential diagnoses were:
� femoral neck stress fracture
� labral tear, possibly with hip synovitis
� FAI (femoro-acetabular impingement), possibly with hip synovitis.
I initially treated the triathlete with soft- tissue techniques to reduce the tone around the hip joint. Trigger-point releases were performed on his TFL, adductors, gluteals, piriformis, deep rotators and iliopsoas.�This reduced his jump pain into 3/10. Manual long-leg grip further decreased the strain on hopping (2/10). He still had pain and stiffness on walking but it sensed “simpler. As he prepared to embark on his long run flight to Europe, I counseled him to not sit for too long and maintain his stylish as straight as possible to decrease any potential impingement from hip flexion.
Luckily, the hip didn’t get worse throughout the flight. On arrival at the French high-altitude training centre, we initiated a strategy of two swims and two intensive treatments a day, aiming at reducing muscle tone, restoring his range of hip movement and normal muscle control and stamina. We had been expecting that the problem was not a stress fracture, but just minor hip synovitis that could settle quickly. Following a week of conservative treatment, though, we were just able to keep his hop pain in 2/10, and that he still could not run 20 meters without any pain and limping.
In collaboration with medics, we flew to London to see a sports doctor and get MRI scans. The scans revealed no bone stress reaction, fracture or labral ripping — which was a big relief; however, it did show signs consistent with FAI (femoro-acetabular impingement). He had hip synovitis with a rectal lesion on his femur.
Hip injuries aren’t much reported among triathletes — in fact they are notably absent from reports on Olympic and Ironman triathlons, which mention knee, back, H/ Achilles, lower leg, ankle and shoulder as the most common accidents (1-3).
In this state, when the hip is in maximum flexion and internal rotation, the labrum and cartilage abut and impinge; damage to the articular cartilage and acetabular labrum results from this pathologic bony contact. The contact generally results in a structural abnormality of the femur (“camera impingement”) along with the acetabulum (“pincer impingement”) or a combination of both (“mixed impingement”). Over time, via repetitive micro-trauma, the aggravating motion hurts the hip cartilage or labrum (or both) during normal joint motion. This happens along the anterior femoral neck and the anterior–superior acetabular rim. FAI is a possible trigger of early hip joint degeneration (4).
Arthroscopic surgery is the direction of choice for FAI if symptoms do not settle; however as his next Competition was only three and a half a year off, surgery was not an option. Instead, over a five-day interval, the athlete had two cortisone (CSI) and local anesthetic injections into the hip joint (under ultrasound guidance) to settle the indicators.
Our aim was to grow the hip range of motion and extend the capsule to reduce any additional impingement, slowly returning to regular training. Following the competition, the athlete would then should see a hip arthroscopic surgeon to acquire a surgical opinion to the best option for long-term direction.
Injection Relief
After both shots my customer felt sore for five days. The initial CSI settled his pain on hopping to 1/10 and after seven days he managed to operate without symptoms. But minor hip stiffness and aching at the end of the day prevented him from progressing to optimal training, so that he then underwent a second steroid injection. This settled the hop pain into 0/10 and decreased the aching; so after five times he returned to mild cycling and after seven days he started running again, also.
The athlete admitted that, following the first shot, he had done more and gone tougher in training than directed, as he had felt “good. This mistake of “too much too soon — all too common in elite athletes — had led to excessive inflammation and aching in the hip nightly after training. After the next injection he returned to normal intensity slower and more gradually.
My client built his training up to regular levels by four months following the final injection (swimming five times per week, cycling four days and running six to seven days). He began with very easy cycling on a wind trainer for 30 minutes, building slowly to 90 minutes before cycling on the street. He cycled two days on and one day away and avoided hills to the first two weeks. He started jogging on the apartment for 15 minutes and slowly built up to 90 minutes after three weeks. He did not run hills or about the track; and as he ran only on every single day, he would diligently concentrate on technique.
From week six to week 11, my client remained on anti inflammatory medication and underwent two treatments a day.
The hands-on treatment continued to:
� increase hip range of movement
� stretch the hip capsule
� normalise pelvic symmetry and hip muscle tone
� improve muscle control and strength � improve proprioception
� ensure optimal biomechanics via video assessment (cycling and running).
Eleven weeks after he first felt his hip pain, the triathlete returned to racing; however he failed to finish the first race, partially because of minor hip stiffness but mainly due to “fitness. Fortunately there were not any prolonged symptoms after the race and a week after he successfully returned to competition, coming second in a really strong field. His very minor ongoing symptoms were handled with anti-inflammatory drugs and hands-on treatments.
If this athlete wants to pursue a long- term triathlon career up to the London Olympics, then he will now require surgery. The arthroscopic surgical technique initially assesses the cartilage and labral surfaces, debrides any abnormalities of the hip joint cartilage and hip labrum, removes the non-spherical segments of the femoral head�and any prominent sections of the anterior femoral neck and bony growths on the acetabular rim that may continue to contribute to hip joint impingement.�The alternative is early joint degeneration and onset of osteoarthritis.
References:
1. Wilk B et al: �The incidence of musculoskeletal injuries in an amateur triathlete racing club�. J Orthop Sports Phys
Ther 1995 Sep;22(3):108-12.
2. Collins K et al: �Overuse injuries in triathletes. A study of the 1986 Seafair Triathlon�. Am J Sports Med 1989 SepOct;17(5):675-80.
3. Korkia PK et al: �An epidemiological investigation of training and injury patterns in British triathletes�. Br J Sports Med 1994 Sep;28(3):191-6.
4. Ganz R. et al (2003): �Femoroacetabular impingement: a cause for osteoarthritis of the hip�. Clin Orthop Relat Res. 417:112�120. For more information see: www.hipfai.com
Exactly how effective are injury-prevention programs in soccer? El Paso, TX.s Scientific chiropractor Dr. Alexander Jimenez looks at the very latest evidence…
Football is the world’s most popular team sport. Injuries are a significant issue for both amateur and professional players. Indeed, previous research has estimated that soccer players are among the most injury-prone athletes having an estimated injury rate of 17-24 accidents per 1000 playing hours(1). Nineteen per cent of all sports injuries which exist in the Netherlands are because of soccer(two) and in Britain alone, the expense of therapy and time lost from work owing to football injuries is estimated to be approximately #1billion annually(1)!
In a landmark study, researchers followed two Champions League teams and gathered data on 2,229 players over seven seasons to examine the injury profile of muscular injuries in soccer players(3). They also analyzed the gamers’ training schedules and data out of their games to construct a detailed picture of the injury risks that were associated. The findings were as follows:
2,908 muscle injuries have been enrolled;
Normally, a player sustained 0.6 muscle injuries each season (equating to around 15 muscle injuries per season at a squad of 25 players);
Muscle injuries constituted 31 percent of all injuries and caused 27% of the total injury lack;
Ninety-two per cent of muscle injuries affected the four Big muscle groups of the lower limbs: hamstrings (37 percent), adductors (23 percent), quadriceps (19%), and calf muscles (13%);
Sixteen per cent of the muscular injuries were re-injuries; nonetheless, these re-injuries caused significantly longer absences than did the first injuries.
The prevalence of muscular injury increased with age.
The exact same group of researchers also carried out a follow-up study (published in 2013) in which they sought to establish the consequences of fixture congestion on injury rates among the gamers(4). Time-loss and exposure injuries were enrolled prospectively from 27 teams over 11 seasons. Matches were grouped based on the amount of recovery days before each match and the accident rates were compared between classes. The results showed that compared to a recovery interval of more or six days, muscular injury rates and overall injury rates were raised in league matches where players had had four or less recovery days.
Given the high levels of trauma among football players (a risk that is increased during periods of match congestion) and the financial pressure of the modern game, it’s perhaps unsurprising that medical team caring for players find that treatment of injuries in players is quite a frustrating and also a never-ending struggle. In addition, it clarifies why some players end up returning to contest prior to the injury has healed completely, setting the stage for injury recurrence, together with protracted absence of this participant from competition and training.
Injury Treatment
Treating injuries in football is both time- consuming and expensive, particularly at the elite level. And while there’s a large literature on the epidemiology of sports injuries, established protocols for treating muscular injuries and assessment criteria for imaging, and a number of clinical and functional tests that could assist the health staff in deciding the optimal point where an athlete can be safely returned to full participation(5,6), the current guidelines haven’t translated into a significant reduction in muscle injury levels in professional sports such as soccer.
To simplify things further, the evidence indicates a new injury often occurs within a couple of weeks after return to contest, and typically costs the player more lost playing time than the key injury(7). The most probable reasons for this observation are likely associated with bodily alterations following the first injury, such as muscle stiffness and/or fatigue, scar tissue formation, biomechanical alterations, neuromuscular inhibition, as well as inadequate treatment — for instance, overly aggressive or incomplete rehabilitation(8-10).
Injury-Prevention Programs
Even armed with knowledge that is up-to-date and the best technology is fraught with difficulty. Remembering the old adage that ‘an ounce of prevention is worth a pound of cure’, a alternative that is far better to attempt to prevent injuries from happening in the first place with an injury-prevention program. This is easier said than done. It is correct that there is an abundance of literature on the effectiveness of methods to avoid harm recurrence and muscle injury, such as enhancing flexibility eccentric and concentric exercises and drills. Despite this and apps like FIFA’s ‘The II’ (see Box 1), the incidence of muscle injuries generally, and the recurrence rate particularly, remains stubbornly high(11-16).
More recent studies indicate that in higher levels of functionality, there might not be much in the way of significant added benefits, while some early study appeared to give evidence for the efficacy of programs in football, as described in box 1. At a follow up to the study described above(18) and that was published this past year, the same group of investigators looked to see if an injury prevention program comprising 10 exercises designed to enhance stability, muscle strength, co-ordination, and versatility of the back, hip and leg muscles (FIFA’s ‘The II’) was effective concerning reducing injury levels and whether it offered any advantages in terms of reducing the related costs of following treatment for injuries that did occur(19).
From the analysis, 479 adult male amateur gamers aged 18-40 years have been split into two classes: the intervention group had been taught to do exercises focusing on core stability, bizarre training of thigh muscles, proprioceptive training, dynamic stabilization, and plyometrics with straight-leg orientation at every training session (2-3 sessions per week) through one season. The management team, meanwhile, continued their usual warm up.
As in the previous study, there were no significant differences in the percentage of players that are injured and injury rates between the two groups. What was intriguing was that in the intervention group, the price of injury treatment was 256 per participant. In the control group nonetheless treatment costs were twice at $606 per participant. The investigators commented that the cost savings in the intervention group may be the result of a rate of knee injuries, which have costs because of more lengthy rehabilitation periods and much more time lost at work compared to a number of different injuries.
Meanwhile, another study on an injury- prevention program (based on The II) in male amateur players had been printed in the end of last year(20). It discovered that (like the previous studies), an intervention program did not decrease the incidence of harm throughout the course of a season. However, such as the study, the players in the intervention group did incur less health care costs, although a justification for this finding wasn’t given. As if to validate the confusion surrounding the value of injury-prevention programs for football players, then a recently published systematic overview of all of the previous studies released thus far fought to achieve a definitive conclusion(21). Six studies involving a total of 6,099 participants met the inclusion criteria and the results of these were conflicting two of the six studies (among large and one of moderate quality) reported a decrease in injury rates that were actual. Four of the six research an ‘preventive effect’, even though the effect of a single study wasn’t statistically significant. Possible reasons for these contradictory findings might be subject choice (sex and level of ability), differences between the intervention programs implemented (content, training frequency and duration) and compliance with this application. What’s clear, however, is that studies investigating the type and seriousness of exercises within an injury-prevention program are still required to reduce the incidence of accidents in soccer efficiently.
Good News On Prevention
Since the review study cited previously(21) was printed, two quite newly published studies on injury-prevention apps in soccer seem to provide more encouraging news — for muscle injuries at least. In one, researchers studied elite players competing over two consecutive seasons, where the first (2008-2009) function as intervention period and the second, the management period (2009-2010)(22). In total, 26 (08/09) and 23 (09/10) elite male pro football players competing within the Scottish Premier League and European competition participated. The accident prevention training program was conducted twice weekly to the entirety of this season (58 avoidance sessions) and the results were compared with the control (no injury-prevention program) year.
On first inspection, the results were disappointing, showing an increase in the complete number of accidents within the intervention period (88 vs 72). But this was largely because of the greater quantity of contusion injuries sustained inside the intervention season (44) compared with control season (23). Assessing like for muscular injuries that were significantly fewer were observed during the intervention season, which had been even more impressive given the larger squad size at the intervention season.
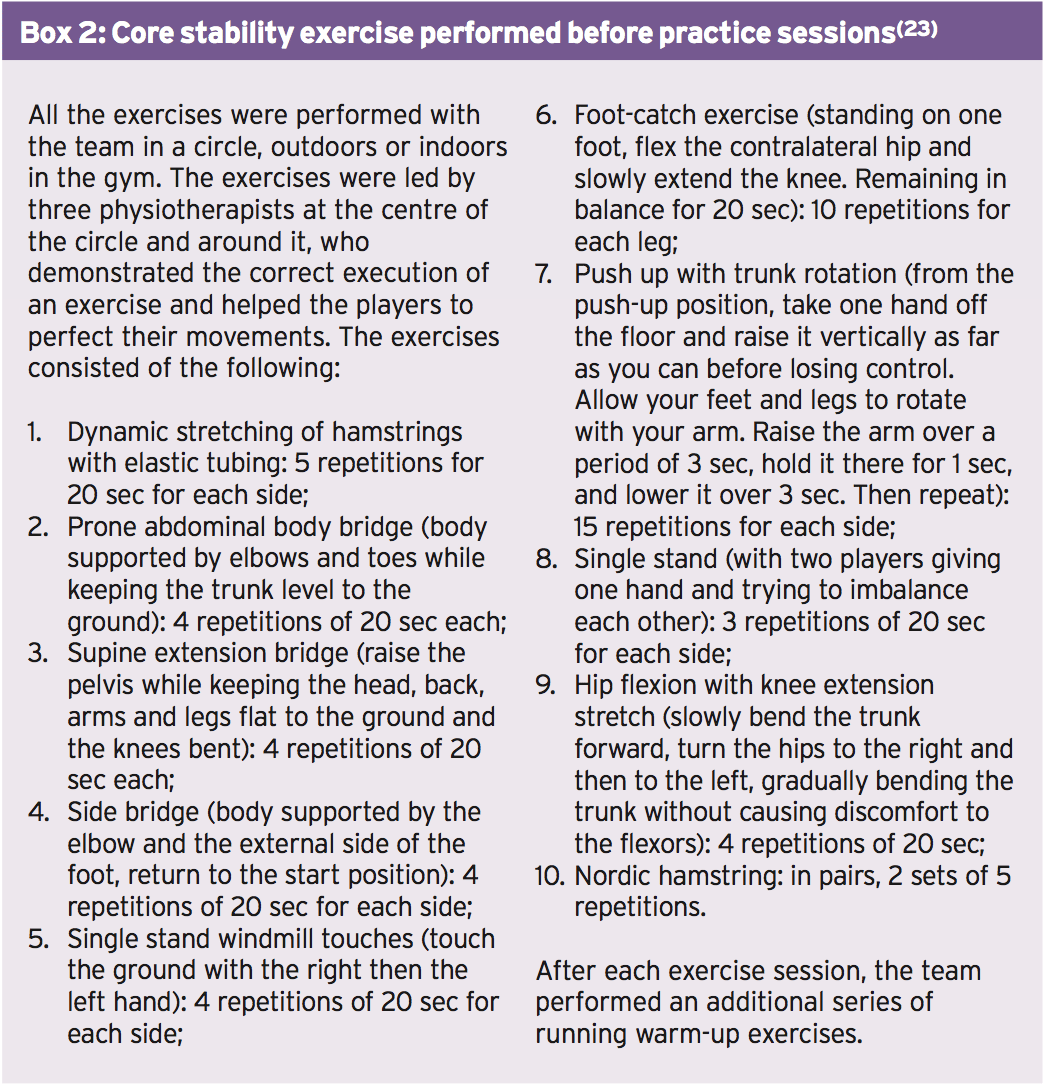
Another newly published study by Italian scientists who researched the effect of a two-tiered injury-prevention program on initial injury and re-injury prevalence in 36 elite male football players also causes encouraging reading(23). During the season prior to that examined in the study, there had been 27 muscle injuries in the group, which accounted for 58.7 percent of the total injuries: 13 of these had occurred throughout practice and 14 during matches. The general incidence of muscular injuries was 5.6 injuries/1000 hours of training/playing exposure and the effect was 106.4 times absence/1000 hours exposure.
To try and decrease the speed of injury through the following season, the team doctor (also among the study’s authors) found an injury-prevention program, conducted 2-3 times per week. This consisted of two elements: a collection of core stability exercises conducted by the whole group prior to each practice session (see Box 2) along with an individualized injury prevention program, which has been started after assessment with kinesiologic and diagnostic tests. At the start of the year, every athlete underwent testing of leg flexibility using the Ober evaluation, Thomas evaluation and straight-leg-raising [SLR] test(24-26). The prone instability test(27) was completed to show spinal instability along with the stork test (28,29) to assess sacroiliac dysfunction. Quadriceps and hamstring strength were measured isokinetically and attention was directed in evaluation of immunity of gluteus medius’ power.
The injuries that happened based on MRI and clinical imaging findings were diagnosed by the medical team. An injury was defined as though it caused the participant to miss the next training session or match, and happened during a scheduled training session or match. An injured player was defined injured before the club medical staff cleared him for participation. Re-injuries were described as those that occurred as those that occurred at the same website no longer than three months following the player had returned to full involvement at early re-injuries and exactly the exact same site.
Results
Throughout the intervention season, a total of 64 injuries occurred — 36 (56 percent) during practice and 28 (44%) during matches. Of them, 20 were muscle injuries, accounting for 31.3 percent of the total injuries; 14 of which occurred during practice and 6 during games. In all, three re-injuries happened and (15 percent of overall muscle injuries) and there were not any premature re-injuries. In comparison with the preceding season with no intervention-program set up, there was a reduction in the number of times and muscle injuries . Specifically, whereas muscle injuries accounted for 31 percent of harms they accounted for 59% of all injuries. Significantly, the number of injuries per 1000 hours of training and playing time was reduced by over half of 5.6 to 2.5. Meanwhile, the number of days fell by nearly two-thirds 106 into 37. The investigators put the success of this intervention down to three key aspects:
An injury prevention program that comprised of core stability exercises similar to those in ‘The II’ program but which differed in its two-tiered arrangement (group and individual sessions), allowing for intense and special training. In contrast, the combined results in research into The II app are probably because of the non- special content and ineffective intensity.
The program’s continuity of commitment by the players to both the group and individual areas.
The addition of bizarre hamstring training in the group program (2 sets of 5 repetitions per week) combined with all the personalized application for players with a history of injury.
Using ice baths in the conclusion of every training session
The investigators cautioned that their study would have included a larger number of topics, but the data still showed a critical progress by the prior year over that. They also argued that by increasing the number of group and individual prevention training sessions, the outcomes could be enhanced.
Summary & Recommendations
Injury treatment in aggressive soccer is equally costly and time-consuming also given the pressures of the game, injury avoidance is more important than ever. But, despite extensive published literature on harm prevention strategies and initiatives such as FIFA’s ‘The II’, the injury rates in soccer remain high, especially in the higher levels.
The latest research indicates that while overall injury prevention programs such as The II might reduce the incidence of trauma in amateur gamers, especially by reducing the incidence of knee injury. However, they will probably not benefit professional players or level. Instead, combining a more individualized approach (using a far greater emphasis on particular exercises determined by kinesiologic and diagnostic testing) with team sessions seems to be desirable. Additionally, it is important that gamers are ‘on-board’ with almost any program and take part regularly (at least twice weekly) to achieve all the potential advantages.
References
1.Br J Sports Med. 2002;36:354-9.
2.Injury Prevention. 2011;17(2):1-5.
3.Am J Sports Med. 2011 Jun;39(6):1226-32
4.Br J Sports Med. 2013 Aug;47(12):743-7.
5. Knee Surg Sports Traumatol Arthrosc 2010; 18:1798-1803.
6.J Orthop Sports Phys Ther 2010; 40:67-81
7.Br J Sports Med 2005; 39:542-546
8. Sports Med 2004; 34:681-695
9. Am J Sports Med 2002; 30:199-203.
10. Sports Med 2012;42:209-226
11. Br J Sports Med 2012; 46:112-117.
12.Am J Sports Med 2004; 32(suppl 1):S5-S16.
13. Am J Sports Med 2010; 38:2051-2057.
14. Am J Sports Med 2010; 38:1147-1153.
15. Br J Sports Med 2006; 40:767-772
16. Am J Sports Med 2013; 41:327-335
17. Am J Sports Med 2002; 30(5):652-9
18.Br J Sports Med 2012 Dec;46(16):1114-8
19. J Physiother 2013 Mar; 59(1):15-23
20. Clin J Sport Med 2013 Nov; 23(6):500-1
21. Sports Med 2013 Apr; 43(4):257-65
22.J Strength Cond Res 2013 Dec; 27(12):3275-85
23. J Muscles, Ligaments and Tendons Journal 2013; 324 3 (4): 324-330
24. J Bone & Joint Surgery 1936; 18:105-110.
25. Phys Ther Sport 2007; 8:14-21.
26.J Orthopaedic and Sports Physical Therapy 1981; 2:117-133
27. Magee DJ. Orthopedic Physical Assessment. 3rd ed. Philadelphia, PA: W.B. Sauders Company; 1997.
28. Spine 2003; 28: 1593-1600
29. Clinical Biomechanics 2004; 19:456-464
The previous rehab masterclass on Lisfrancs injuries highlighted the pathogenesis of injuries, the midfoot joint’s relevant factors, and typical injury mechanisms were presented along with diagnostic findings. In this masterclass scientific specialist Dr. Alexander Jimenez discusses the management of Lisfranc injuries…
Management
After the initial injury, it may not be clear exactly what harm the foot has been done to by the athlete. Both athlete and sports medicine staff may confuse. The athlete with subtle stage 1-type injuries will try to ‘run off’ the pain. As they continue and fail to reevaluate they will stop training/competition.
When an injury into the Lisfranc is suspected, the first MTP joint ought to be assessed to exclude a ‘toe’ injury and the ankle checked to exclude an ankle injury. They crutches till they could be properly analyzed and remain non-weightbearing ideally with an Aircast boot and need to ice the foot aggressively.
Non-operative�Treatment of Lisfranc Injuries
A stage 1 accident that’s functionally secure could be handled with a non-weight posture boot or cast for a first two weeks. They can be analyzed for tenderness on palpation over the TMT joint at this time and follow-up x-rays will be required to exclude any latent diastasis of the second and first metatarsal space. If pain-free on palpation and x ray is normal, they could have the weight bearing status assessed using complete weight bearing foot flat and position is raised by a toe. If that is normal they can stay out of the boot using a custom made orthotic and rehabilitation and return to conditioning may begin.
Then the boot is reapplied, if the foot stays painful to palpate or if they neglect raise test and they stay non weight bearing to partial weight bearing for a further four weeks.
For pain along with weightbearing status they’re reassessed in the stage. If these are uneventful then the rehabilitation and reconditioning stream is moved to by the athlete. If problematic they need to be assessed for postponed stabilisation.
The time period to get a injury that is secure could be a month recovery until return to play.
Operative Treatment Lisfranc Injuries
Stage 2 and stage 3 accidents need to have the midfoot surgically stabilized since they’re generally unstable injuries. Interestingly, Hummell et al (2010) recently clarified a successful result in a point 3 football player with non-operative treatment. The objective of surgery is to acquire a fantastic reduction to optimize functional results. Virtually all expert opinions relating to Lisfranc injuries emphasize the importance of gaining as to avoid long- term morbidity from the midfoot.
Myerson et al (1986) identified some things that result in poor outcome for example residual angulation between the metatarsals, diastasis greater than 2mm between the first and second metatarsals. Correcting these defects is essential to avoid long-term complications like chronic functional disability , post-injury arthritis and instability with walking.
To obtain reduction of the TMT joints reduction is usually necessary to remove any tissue for example little bone fragments or ligaments. Reduction is supported with fluoroscopy. Nevertheless, in instances percutaneous fixation can be accomplished if the dislocation can be reduced by the surgeon under fluoroscopy and stabilize the joints together with wires and screws. However, most will require an open reduction to properly visualize and access of the joints that are tarsometarsal.
The choice of hardware for surgery is debatable surgeons the choices are:
1. Cannulated screws;
2. Solid, Non-cannulated screws;
3. K wires;
4. Bridge plates for tarsometatarsal joints.
At a thorough literature review, Stavlas et al (2010) found that injuries to the first few metatarsals (lateral and middle column) react well with screw fixation, whereas harms to the fourth and fifth metatarsals (lateral column) may respond well with K wire fixation.
Post-Operative Rehabilitation
This will often involve a non-weight- bearing cast or boot to get the first 3 weeks with a CAM/Aircast boot used for the subsequent three to five weeks so that the athlete is complete weight. Weight is slowly built around the eight to twelve months post-operative interval so that in a custom-made orthotic the athlete can weight bear by 3 months that.
The hardware is often removed at 12-16 weeks post-op in lighter athletes and in heavier athletes (>200 lbs) it’s been suggested to take out the hardware in 24 weeks (Nunley and Verullo 2002).
Post-surgery the results are generally favourable. Nunley and Vertullo (2002) discovered that in stable stage 1 harms, great outcome was found with conservative treatment with athletes back to game at 11-18 weeks post-injury. Athletes with stage 2 injuries had good outcomes with ORIF and returned to play 12-20 weeks. Period 3 accidents were not described.
Physiotherapy
The athlete will see that the physiotherapist athletic coach weekly to regain mobility. Interventions will be necessary in addition to direct mobilizations to restore the accessory movements.
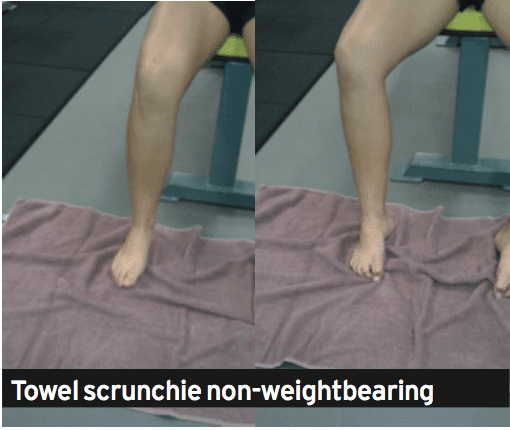
The therapist can also start intrinsic foot muscle exercises at approximately 8-10 weeks post-operative using the weight bearing exercises being postponed until week 12 post-operative. These exercises are designed to retrain the arch to be controlled by the foot muscles. Exercises that will satisfy this are towel scrunchies, cup drop, matt equilibrium and lunge exercises (see below).
The movement can be measured by the therapist regularly with knee.
1. Towel scrunchies. These have been used by therapists to strengthen the muscles that support the foot’s arch.
A. Place a towel onto a tiled or wooden floor (carpet will not work.
B. set the foot relaxed on the towel with all the foot in line with the knee and hip. The feet should be pointing directly ahead.
C. Initiate the movement by attempting to firstly raise the arch. Think about drawing the ball of the foot to the heel. You will see that the arch is going to lift.
D. Next use all the feet to loosen the towel under the foot.
E. Relax the foot and start again.
F. This exercise doesn’t cause any soreness the next day; the muscles should start to fatigue.
G. The development is seated, to standing on one leg and standing on two legs.
2. The cup drop. This can be an interesting and innovative way to integrate inherent arch muscle function and anti- pronator muscle function that is extrinsic using hip muscles that are hip, in particular the gluteus maximus and medius. During weight bearing, the hip is prevented by the gluteus medius muscle from rotating and adducting, and this action works well with the arch muscles preventing excess pronation.
A. Place a few small objects like marbles about one foot in front of your body.
B. Reach forward with the foot and also pick up the masonry with the feet. Of clawing at the masonry this activity will trigger the muscles.
C. Whilst holding the marble in the feet, circle the hip outwards into both sides of the body then behind the body and set the marble at a cup placed at 45 degrees to the cool.
D. It is necessary that the foot stays turned outwards as this retains the gluteus active.
3. The mat balance. This exercise incorporates these together with the arch muscles and adds contraction of the calf muscles both the gastrocnemius and soleus. The drill is done on a gentle matt, to create the exercise challenging. The mat surface generates an unstable situation, and there is mounting evidence that indicates that by incorporating a component of balance control to a rehab exercise may be necessary since the perturbations in movement excite all of the position feedback nerve endings which control proprioception. The nerve endings feedback to the muscle control system and also this potentiates the stimulation of their control muscles.
A.Place a soft mat in addition to a 6mm piece of timber or hard rubber mat. The thicker the mat that the harder the exercise.
B. Stand on the mat but just with the third, fourth and fifth feet connected with the matt. The first and second feet should be hanging unsupported from the mat.
C. This position of the foot makes a scenario whereby the foot wishes to turn in under gravity’s effect. The long pronation muscles in the shin and the muscles need to control the interior of the foot to keep it up and of the floor.
D. Attempting to keep equilibrium (and this will be hard when the matt is too soft), marginally boost the heel to participate the calf muscles.
E. Hold this position for 1-2 seconds and then slowly lower down to the beginning position.
F. Perform 3 sets of 10 repetitions.
4. Lunge with towel scrunchie. This workout is a high-level integration workout which combines gluteals and arch muscles whilst performing a exercise such as the lunge. This sort of exercise is done in late phase rehab prior to running as the muscle activation patterns more resemble what should happen in conducting concerning limb assistance — that is, the arch muscles control pronation, the quads control the knee and patella and the gluteus medius affirms the hip throughout foot strike.
A. Stand on a towel, very similar to Exercise 1 above.
B. Put some theratubing around a post and also wrapped round the upper tibia. The ring has to be guided to pull the tibia inwards, not outwards. This pulling in of the tibia can cause the top leg to follow along with this is imitating hip adduction and internal rotation. The goal of the exercise is to prevent it by maintaining the kneecap aligned with the next toes. The gluteals finally have to work to permit this to occur. Inwards and way would fall from the third toe, if they did not.
C. Gradually lower down into a lunge whilst keeping the monitoring of the kneecap over the next toe and also keeping the towel scrunched up under the foot.
D. Lift up to full knee extension. Rest. Start again.
Strength
The athlete will initially load throughout the foot with the foot impartial. Exercises such as split squat, high- foot leg press and posterior string movements such as deadlifts and stand pulls may start in the weight bearing phase. Exercises requiring more ankle dorsiflexion and so midfoot pronation will be delayed for a couple of weeks until strength and confidence improve (traditional one-leg squats, deadlifts and leg press).
Rehabilitation
The graded progressions for your athlete have been well summarized by Lorenz and Beauchamp (2013). The progression is a staged progression to gradually regain strength and confidence from landing and push-off positions. If the stage is pain free, the progressions could be made, the athlete could do selection and without compensations to the movement.
1. Bilateral heel raises
2. Heel raise,�single-leg eccentric lower
3. Single leg-heel raise from standing
4. Bilateral leaning heel raises
5.�Bilateral leaning heel raises, single leg�eccentric lower
6. Single-leg leaning heel raises
7. Single-leg triple extension heel raises
8. Mini-tramp low Impact exercises
A. Bilateral jumps in position
B. turns in place (two legs).
C. turns in place (two legs).
D. Jog in place
E. Three hops uninvolved, one hop involved
F. Two hops uninvolved, two hops involved
G. One hop uninvolved three hops involved
9. Agility ladder
A. Different frontal transverse plane designs
B. Hopscotch to involved negative (two to one)
10. Single-leg A/P jumps in place
11. Single leg M/L jumps in place
12. Single leg transverse jumps in position
13. Single leg hops in agility ladder
Return To Running
The choice as to when to remove the hardware will influences the choice. As a general rule, when the screws and wires are eliminated, the athlete will be permitted to attend and walk gym sessions to the elimination but running will probably be delayed.
The athlete is encouraged to walk a treadmill using a incline to promote the push. This can start at 12 weeks . The athlete may quickly advance into backward and forward running on grass and it’s expected they are doing so by week 14 depending on when the hardware was taken away. As they progress through running they could slowly begin to construct speed they reach sprint speed.
Gentle off-line running drills such as weaving, easy bypassing, stepping and caricoca drills would normally be started in around 16 weeks post-op and progressed into tougher single-leg and hard-cutting plyometrics as pain allowed. It would be expected that by 20 weeks post-op, the foot has sufficient strength, range of movement and confidence to start team- based ability function. Prior to this, the athlete can experience some frequent field hop tests like tests and single-leg triple jump to assess differences in abilities.
Functional Tests
A evaluation that is practical sports-specific is a test or field test that aims to mimic the movements. The use of practical tests aims to recognize imbalances and will boost confidence in both patient and the clinician the injured patient can return to play. It is effectively a way of reducing the hazard. The evaluation ought to be an objective, measurable and quantifiable test that includes a component of:
Strength
Agility
Power
Balance Neuromuscular status.
The aspects can be incorporated into practical tests such as agility and jumps/ movement evaluations.
The hop tests comprise:
1. Single jump
2. Triple hops
3. Crossover jump
4. 6m timed jump.
Single limb evaluations are necessary as study proves that dual limb and modified double limb tests don’t demonstrate any differences between groups since the uninvolved limb can mask deficits of the thoracic (Myer et al 2011). Single-leg hopping evaluations are sensitive enough to discover asymmetry, and specifically the crossover hop test at six months post-op is the most sensitive of these tests at predicting future function of the knee along with the 6m timed test is the most vulnerable and sensitive of under normal function at six months . (Logerstedt et al 2012).
Therefore isolated single-limb performance tests may provide a critical element to field-based operational performance testing to identify deficits in reduced limb performance, including deficits in force attenuation functional power and postural stability. The capability to maintain isolated single limb electricity is significant in sports that require significant control in stepping edge and cutting manoeuvres. This may require and ability to regenerate and divert and then to absorb force on one limb the motion.
Conclusion
Injuries are uncommon in athletes on account of the severe consequences they could have on athletic role, the sports medicine specialist has to be well versed in evaluation and initial management. They can be challenging injuries manage and to diagnose for the clinician.
Stable Lisfranc injuries with no instability can be handled conservatively stage 2 and 3 accidents involving diastasis of their second and first metatarsals requires consideration. This can be done usually using the open reduction and fixation with screws, K cables and/or plates
Rehabilitation after surgery will take no less than 12-16 weeks it’s typical for the return to sport to take in contact sport athletes. Successful return to competition time frames extend to the 20-24 week stage post-surgery and rehab will involve reduction of the entire limb kinetic chain but also not only the foot muscles.
References
1. Castro et al (2010) Lisfranc joint ligamentous complex: MRI with anatomic correlation in cadavers. AJR. 195; W447-455.
2. Chiodo CP and Myerson MS (2001) Developments and advances in the diagnosis and treatment of injuries to the
tarsometatarsal joint. Orthop Clin North America. 32(11); 11-20.
3. Garrick JG and Requa RK (1988) The epidemiology of foot and ankle injuries in sports. Clinical Sports Medicine. 7: 29-36.
4. Hummell et al (2010) Management of a stage 3 Lisfranc ligament injury in a collegiate football player. Athletic Training and Sports Health Care. 10(10); 1-5.
5. Logerstedt et al (2012) Single-legged hop tests as predictors of self reported knee function after ACL reconstruction. The Delaware-Oslo ACL cohort study. American Journal of Sports Med. 40(10); 2348-2356.
6. Lorenz and Beauchamp (2013) Case report. The functional progression and return to sport criteria for a high school football player following surgery for a Lisfranc injury. The International Journal of Sports Physical Therapy. 8(2); 162-171.
7. Myer GD, Schmitt LC, Brent JL, Ford KR, Barber KD, Scherer BJ, Heidt RS, Divine JG and Hewett TE (2011) Utilization of modified NFL combine testing to identify functional deficits in athletes following ACL reconstruction.
Journal of Sports Physical Therapy. 41(6); 377- 387.
8. Myers et al (1994) Midfoot sprains in collegiate football. American Journal of Sports Medicine. 21; 392-401.
9. Myerson et al (1986) Fracture dislocations of the tarsometatarsal joints: end results correlated with pathology and treatment. Foot and Ankle. 6(5); 225-242.
10. Nunley JA and Vertullo CJ (2002) Classification, investigation and management of midfoot sprains: Lisfranc injuries in the athlete. American Journal of Sports Medicine. 30(6); 871-878.
11. Ouzounian TJ and Sheriff MJ (1989) In vitro determination of midfoot motion. Foot and Ankle. 10; 140-146.
12. Rankine et al (2012) The diagnostic accuracy of radiographs in Lisfranc injury and the potential value of a craniocaudal projection. AJR. 198; W365-369.
13. Shapiro et al (1994) Rupture of the LisFranc�s ligament in athletes. American Journal of Sports Medicine. 22(5); 687-691.
14. Stavlas et al (2010) The role of reduction and internal fixation of Lisfranc fracturedislocation: a systematic review. International Orthopaedics. 34; 1083-1091.
Chiropractor, Dr. Alexander Jimenez summarizes some fascinating injury stories in the combat game…
I was recently on a holiday in Koh Lanta in Thailand and throughout my holiday I visited a Muay Thai training gym for two reasons. Firstly, as I’ve had a fascination with the sport for some time having formerly handled some injuries in some fighters in Australia it was to have a private Muay Thai training session with a few of the boxers. I was that I could use as material. I clarified the purpose of my visit and approached the head coach and discover a few of the interesting injury stories they’d out and he was pleased for me to talk to a few fighters. The following are just two case studies from this fact-finding mission.
The Biker’s Elbow
The initial fighter was a seeing K1 fighter out of Holland who spends six weeks a year in Thailand. He had been a fit and healthy 25-year-old man with a history of prior knee and back injuries; nonetheless, his complaint at this stage was pain on the inside of the right elbow that made grappling through fighting and also lifting weights at the gym hard.
The pain had started only a few days to his recent trip to Thailand and had been present for about five days. It had been focused around the medial epicondyle of the elbow. Any powerful gripping moves whilst flexing the elbow was shown to be debilitating. It had been affecting his coaching as some other work that was grappling was too painful and he was unable to perform any type gym movements such as chin ups and rowing motions. All pushing type movements were asymptomatic.
He whined no preceding elbow pain and refused any trauma to the elbow such as a arm lock-type situation or a hyperextension type injury during training or fighting.
He had been tender to palpate the source of the wrist flexor muscles which start on the elbow along, as well as any forceful wrist extension was uneasy. His elbow felt secure and using a stress test. Strong grip of the hands was painless until he was put to a position of wrist extension that is complete.
With no history of injury and without any changes to his coaching regimen I quizzed him. We exercised that whilst in Thailand he traveled on a scooter — a pastime for thieves to tackle when. He’d spent plenty of time around the sightseeing on the bicycle when he came.
The type of scooter he used was a automatic without equipment shifting the accelerator is on the right side of the bars. The reasoning was because of the continuous wrist extension used to accelerate the scooter at a pronated position, the wrist flexor muscles were put in a position of stretch with constant tension due to the co-contraction of this wrist flexor/extensor group required to do this particular movement. Coupled with this was that the vibration that is constant on the bicycle caused by the movement of the scooter in addition to the frequent pot holes and undulating road typical of Thai roads. The diagnosis was an inflammatory response in the wrist flexor origin.
I made the following suggestions:
1. Regularly extend by putting the hand flat on a table with the wrist turned to supination, the wrist flexors. He was to hold this for 30-second efforts.
2. Soft tissue massage to the wrist flexor muscle group, something he could do in Thailand using the massages on offer.
3. Moderate outrageous wrist flexor exercise working with a 5kg dumbbell using the forearm put on a desk (palm upward) and also to slowly lower the weight into wrist extension and use the flip side to help the concentric lifting. He was to do this
4. Change the hand place on the accelerator. It was suggested he can do three distinct things to achieve this. Primarily he can flare the elbow out broad whilst riding to decrease the amount. He up to this point kept the elbow close in to the body to perform this. Secondly he could occasionally hold the accelerator handle on the end so that he could keep his forearm supination position as this requires radial deviation to quicken the bike. Finally, on stretches of street I invited him undo the grip so he utilized wrist flexion to accelerate the bicycle and to actually supinate his forearm.
5. Rub some topical gel.
Two weeks later, I saw him and he maintained that the elbow pain had entirely subsided.
The Buzzing Thigh
A 30-year-old Thai local fighter had whined a six- month history of a ‘buzzing’ kind pain on the outside of the thigh and in the calf that was ideal region. It’d started after he obtained a hard kick to the back of his right hip. The kick was so strong that he lost function of his right leg at the time and needed a sensation down the thigh into the foot and calf. As this occurred in training, he rested on the leg and stopped and used the Thai concoction of heat and ointments to manage this harm. He returned to coaching a couple of days later and had been involved in a couple of fights after. He felt he had been still practical, but still felt a buzzing sensation every time. He claimed that he managed to perform everything and even blows to the thigh and hip were no longer painful than normal.
On examination he had movement in both hips his internal rotation when lying prone was decreased compared to another side. He was able to squat and perform a single leg pain free. All knee motions and ligament testing demonstrated unremarkable.
What was painful was a slump test on the ideal side and this reproduced the proper- sided throat sensations he experienced with kicking. The pain was made worse with dorsiflexion of the ankle whilst at a slump position.
It was concluded that when he had sustained the blow to the posterior hip, he had bruised the subsequent hematoma and the right piriformis muscle had created fibrosis around the sciatic nerve. Each time he had to stretch into full hip flexion with the knee extended and the foot dorsiflexed to complete a roundhouse kick, he had been effectively stretching the nerve against the port made by the scarring and fibrosis around the guts by the preceding injury to the soft tissues. This would be sufficient to give him a neuropathic-type pain down the leg across the course of the nerve and in the superficial peroneal nerve.
I explained that the way to remove this was to frequently ‘extend’ or move the guts from the vents to try to release the nerve out of any fibrosis. I showed him how to run his own gentle nerve mobilizations as a slide and slide method (neurological wracking) and also how to hold the place on stretch to make a sustained elongation.
He did so sitting on the conclusion of the fighting ring at a full slump position (neck flexed, spine arched into flexion) and he had been to straighten the ideal knee with the foot dorsiflexed until he felt a gentle uncomfortable tug onto the guts (felt like a buzzing down the ideal leg). This was to be achieved to this point of discomfort but not pain. I explained that if he overdid motion and this stretch he could make the issue worse, so I invited him to underdo this and not over do this. He had been to spend five minutes after a warm-up finishing a string of knee extension and release the stretch. After a pause continue this on/off movement for five minutes per day and he was to stretch again.
I didn’t figure out how this solved as this movement would take a few weeks to make a noticeable shiftI can expect that he would have discovered a relief from his signs at some stage in the future.
Chiropractor, Dr. Alexander Jimenez looks at the way this common injury shows itself.
Introduction
Iliotibial band syndrome (ITBS) between the knee is frequently diagnosed in sport injury clinics. ITBS presents having an incidence rate of around 22% in most lower extremity running-related injuries (1) also has been said to be the second most common complaint amongst distance runners (2). ITBS has been given the expression ‘runner’s knee’.
Trainers like endurance runners who perform flexion and extension combined with loading are subjected to this illness. ITBS presents during the first two or three miles in running with no mechanism of injury, which can make identifying the cause more interesting. With plenty of factors having been considered within the literature, changes are often purported to be a cause of ITBS. But some biomechanical factors have been researched and have been found to have little or no effect in the start of ITBS. Therefore this text’s point would be to examine the biomechanical changes which may induce an individual to the beginning of ITBS. The research published reviewed is largely based on a current systematic review that was published in Physical Therapy in Sport in 2014 (3).
Anatomy & Function
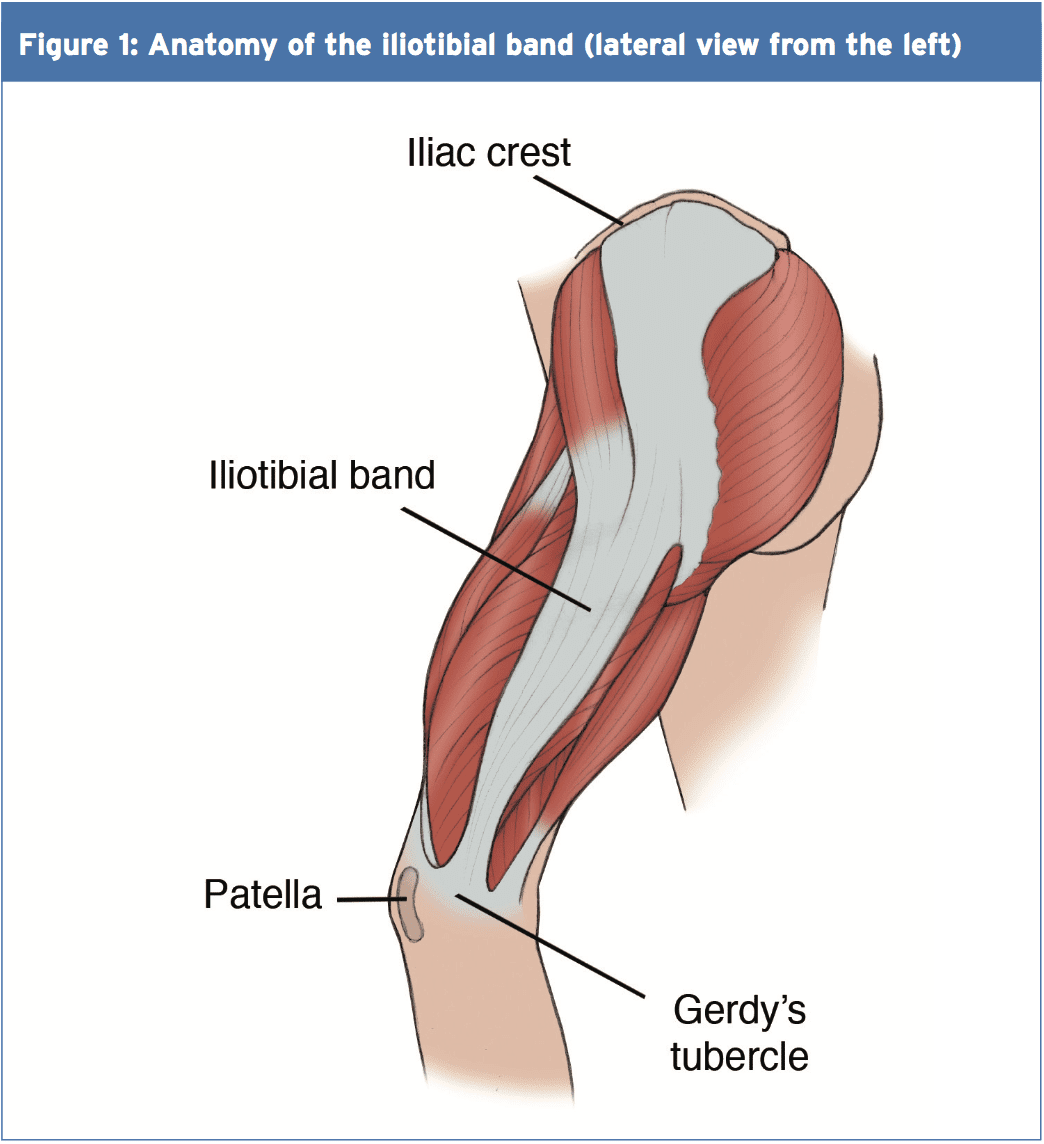
The iliotibial band (ITB) encapsulates the tensor fascia latae (TFL) presenting with both deep and superficial fibre attachments at the pelvis (4). In addition to attaching to the TFL, approximately three-quarters of the gluteus maximus tendon also conjoins with the ITB (4). The ITB courses along the lateral aspect of the hip and passes the greater trochanter. The ITB maintains an attachment on the posterior ridge of the femur whilst attaching itself to the fascia. The ITB has a fixed attachment at the lateral femoral condyle where it then divides into three segments with the first being the lateral patella (3). The remaining two segments cross the knee joint to insert at the head of fibula and most distally at the infrapatellar tubercle also known as Gerdy’s tubercle on the tibia (3). Figure 1 illustrates the location of the ITB.
The ITB passively functions to resist hip adduction, hip internal rotation and internal rotation of the knee in accordance with its attachments at the pelvis, femur and tibia(3). The gluteus maximus functions, through its attachment, to increase stability through the hip and knee complex by increasing the tension of the ITB(4). It is possible to see, based on its attachments at both the knee and hip, how changes could bring about the onset of ITBS.
Studies have proposed that as the knee flexes and extends the ITB ‘slides or flicks’ over the lateral femoral condyle of the knee causing an irritation beneath. This notion was debated by Falvey and colleagues (5), who stated that it was highly unlikely that the ITB would flick or slide over the bone during knee flexion due to it not being a loose structure. But the authors did agree that the impact of compression on the richly innervated fat pad was pain’s cause but by strain of the ITB where pain presents crossing the lateral femoral condyle. Strain rate and strain magnitude were measured in a prospective study involving female runners (6). The results indicated that frequency of strain of the ITB at the lateral femoral condyle was greater that the strain magnitude. This implies that a runner might have the ability to run for a short period but then incur lateral knee pain because of the strain to the ITB.
MRI scans have ascertained the knee flexion angle of 30� elicited the greatest compression of the ITB at the point of heel strike, whereas others have said that maximal compression occurs between 20-30�(2,6). A knee flexion angle at the point of heel strike has been found to be significantly different with 20.6� in ITBS patients compared to 15.3� in the control(7). Downhill running produces a greater knee flexion angle at the point of heel strike eliciting a larger strain load to the ITB and therefore this is often a main precursor to ITBS (6). Although an elevated knee flexion angle at the point of heel strike has been considered to contribute to ITBS, it is essential to examine the lower extremity from the frontal and transverse planes too and not solely from the sagittal plane (2).
Rearfoot Eversion
It’s possible to envisage how rear foot eversion could contribute to ITBS causing internal rotation of the tibia resulting at the distal attachment in greater strain of the ITB. In contrast Ferber and colleagues (2) indicated that there was no significant difference in the peak eversion angle of the female subjects, who were previously diagnosed with ITBS but were now symptom free, compared to controls. In a similar study non-significant differences were found between the currently symptomatic ITBS patients and controls for rear foot eversion (8).
Louw & Deary(3) found that ITBS patients sometimes demonstrated decreased eversion angles, accompanied by decreased internal rotation of the knee, at the point of heel strike. Ferber and colleagues (2) noted an increased inversion moment in the ITBS group which was suggested to control and limit the eversion moment. By comparison, currently symptomatic ITBS patients demonstrated a substantial difference compared to a control group with twice the rear foot motion during running (9).
Knee Internal Rotation
Peak internal rotation angle of the knee was found to be significantly greater in the ITBS patients when compared with controls at the point of heel strike (2). This research was supported by other studies who also found a significant effect for increased internal rotation of the knee following a run of moderate intensity to physical exhaustion(7). With excessive rotation comes compression due to increased strain of the ITB at the attachment.
An explanation of increased internal rotation of the knee was attributed to excessive external rotation of the femur perhaps due to shortening of the piriformis, gemellus inferior and superior and the obutrator externus (8). The authors added that excessive rotation at the hip might result from muscular activity of the rotators that were hip being the medius, minimus and the tensor fascia latae. These studies(2,7) were retrospective in design in that they tested healthy runners with a history of ITB pain, whereas(8) was a prospective study of patients with ITBS at the point of testing.
Hip Adduction Angle & Hip Abductor Strength
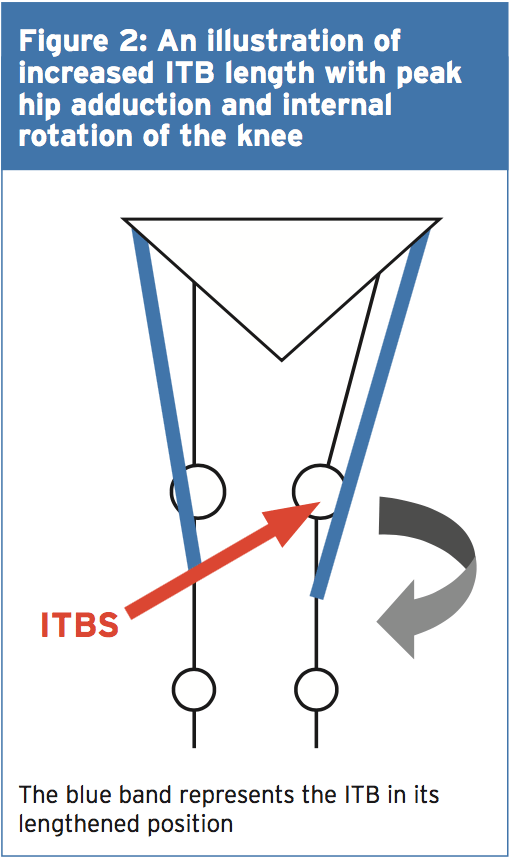
The hip adduction angle during the stance phase has been suggested to be greater. Ferber and colleagues(2) found that the peak hip adduction angle was significantly greater in the ITBS cohort and stated that with 95% confidence. Increased angle results in increased stress to the ITB and consequently increased compression at the lateral femoral condyle when combined with increased internal rotation of the tibia.
Figure 2 illustrates, when peak hip adduction and internal rotation combine, how this may result in increased the compression of the ITB at the lateral femoral condyle. Louw and Deary(3), however, stated that it remained inconclusive whether the peak hip adduction angle was a substantial element. Additional research is therefore required to support Ferber and colleagues'(2) initial findings as this study was a retrospective study carried out on healthy female runners with a history of ITBS.
Hip Abductor Strength
It’s been proposed that an increased peak hip adduction angle may coincide with hip abductor activity involving the gluteus medius in this group. During the stance phase of gait the gluteus medius functions to keep stability. Research has indicated that during stance the adduction forces can exceed three times an individual’s body weight(3). What’s more, it was stated that these forces were beyond the metabolic capacity of the gluteus medius to main pelvic stability during the stance phase using just this muscle alone(3).
Louw and Deary (3) were not able to identify a heightened hip abductor moment in the ITBS patients with increased peak hip adductor angles and suggested that it was more of an issue of timing as opposed to the size of the hip abductors. Louw and Deary (3) stated that the research is yet to examine trunk and pelvic movements in ITBS patients and it is plausible to suggest that biomechanical changes from higher up the kinetic chain has the potential to be a contributing element in ITBS etiology.
A research study of 24 (14 female, 10 male) patients with ITBS undertook a six-week rehabilitation programme to increase the strength of the hip abductors(10). Following six weeks of hip abductor strengthening to running 22 patients reported being pain-free and had returned. The female patients reported an average hip abductor torque increase of 34.9% and the male patients found 51.4% increase. However this study used a hand held dynamometer to measure isometric strength and therefore Fedricson (10) findings should be viewed with caution.
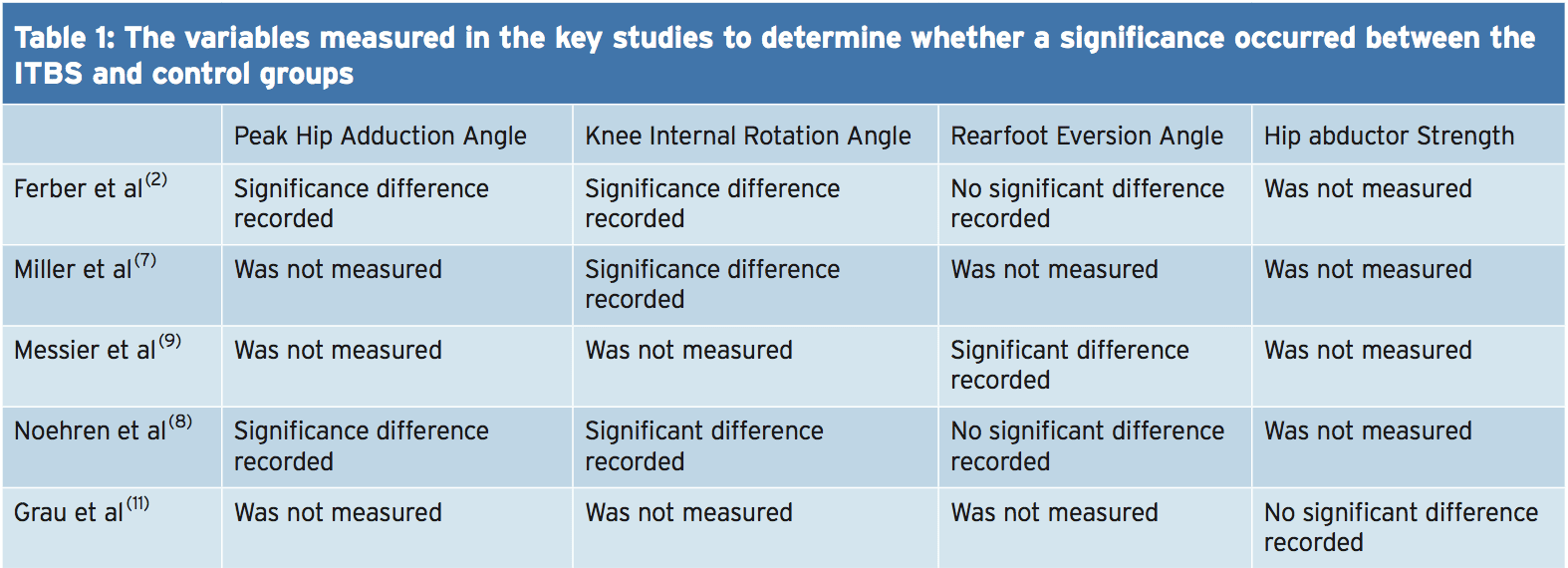
A more recent study assessed the hip abductor strength of currently symptomatic patients with healthy controls in a fixed position(11). The results indicated that no substantial differences occurred for static and dynamic hip abductor strength between the groups. Further research should look into the EMG and strength of the hip abductors in the role of managing ITBS. Table 1 shows of significance in the some of the variables of the studies used in this text.
Rehabilitation programs, following periods of immobilization and during, should include gluteal exercises to provide stability to the leg that is involved. If active exercises for the gluteal muscles are provided in a manner that is secure and effective then this can influence the period of transition from non weight. It’s prudent based on the research provided to date to develop function although research is lacking in terms of quality and volume as to the biomechanical influences on the etiology of ITBS. This guarantees that once load bearing commences that the leg that is involved has the stability and control that is active to keep the beginning of load of the ITB.
Summary
The recent review published by Louw and Deary(3) indicates that much of the research published within the literature depending on the etiology of ITBS is inconclusive. The level of research is relatively low and is based on retrospective trials. The research does indicate that knee biomechanics and abnormal hip is involved in the occurrence of ITBS. The authors ascertain that muscle strength is involved as is foot biomechanics that are abnormal. It is recommended that future research should measure kinematic movements of the hip and knee during downhill running as this is a complaint of ITBS onset.
References
1.Clini J of Sports Med, May 2006,16, (3), 261-268
2.J of Sports Phys Therap, Feb, 2010, 40, 2, 52-58.
3.Phys Therap in Sport, 2014, 15, 64 e75.
4.Surgic and Radiologic Anatomy (Dec) 2004; 26, (6), 433 – 446
5.Scand J of Med & Sci in Sports, Aug 2010, 20 (4), 580-587.
6.Clini Biomech, 2008, 23, 1018-1025.
7.Gait Posture. 2007 Sep, 26 (3), 407-13
8.Clini Biomech, Nov 2007, 22 (9), 951-956.
9.Med Sci in Sport & Ex, 1995, 27, 951-960.
10.Clini J of Sports Med, 2000, 10:169�175.
11. Int J of Sports Med, Jul, 2008, 29 (7), 579-583.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine