Spinal stimulation is a treatment option that could help bring relief from pain and improve the quality of life for individuals dealing with chronic pain, like low back, and leg pain. Spinal stimulation can help reduce and manage chronic pain that does not alleviate or reduce with physical therapy, pain medications, injections, and other non-surgical treatments/therapies. �
It is a form of neuromodulation that works by blocking pain signals that the nerves send out from reaching the brain. A spinal stimulator is a tiny device that is implanted underneath the skin. The device delivers a very low electrical impulse that masks/changes pain signals before they reach the brain.
�
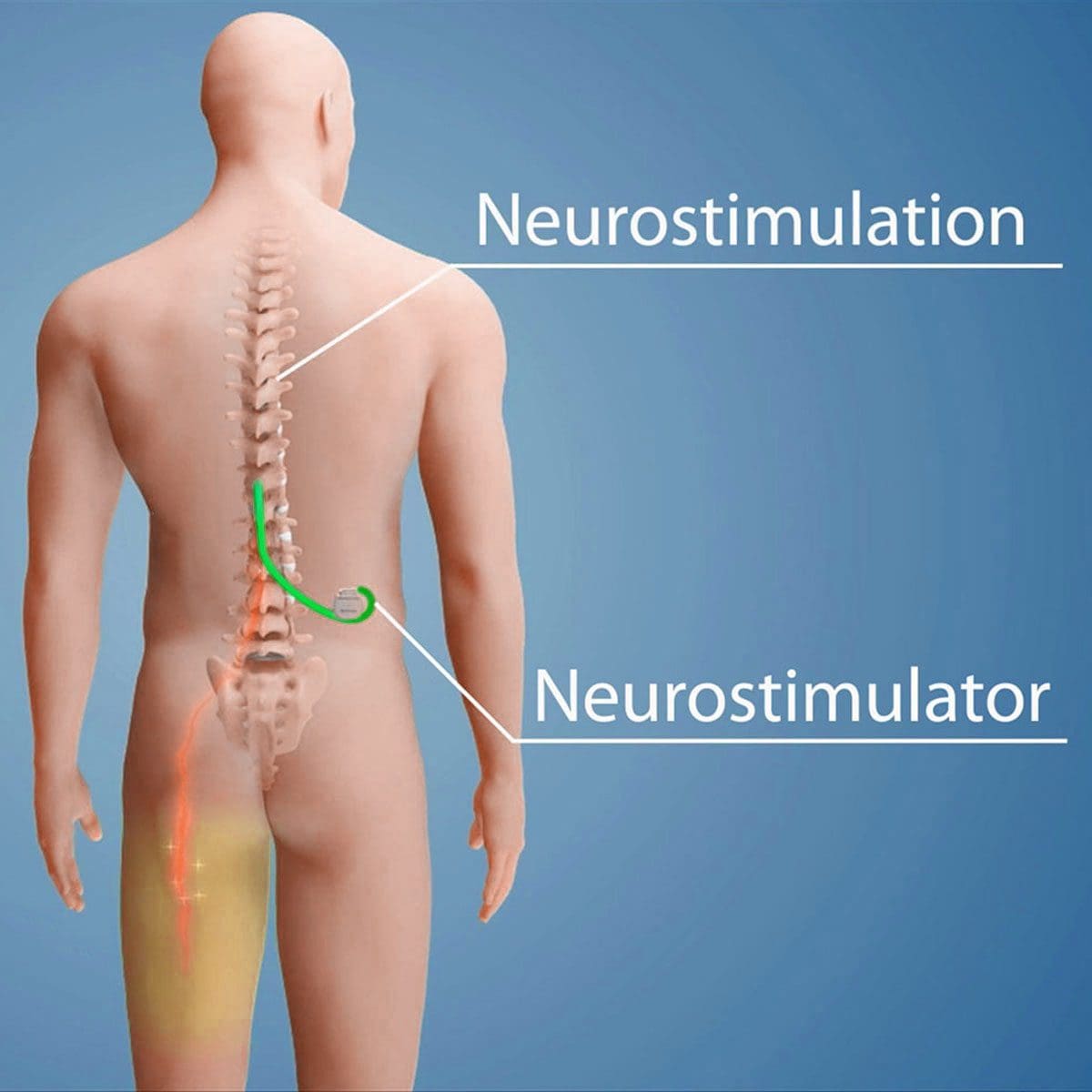
A Spinal Stimulation System
�
Neurostimulator:
This is the entire device that is implanted and sends out electrical impulses through a lead wire to the nerves in the spine.
Lead:
The thin wire that delivers the electrical impulses from the neurostimulator.
Remote control:
This turns on/off the stimulator and increases or decreases the amount of stimulation.
Charger:
Stimulators are rechargeable and normally require recharging about one hour every two weeks.
�
Spinal Stimulator Types:
�
Traditional stimulators
These produce a gentle ringing/tingling sensation that masks the pain.
Burst stimulators
These send out random interval bursts of electrical impulses designed to copy the way the body sends out nerve impulses.
High-frequency stimulators
These reduce pain without generating tingling sensations. �
�
Types of Pain Spinal Stimulation Treats
Spinal stimulation is approved by the U.S. FDA to treat chronic back and leg pain, including pain that doesn’t go away after back surgery known as failed back surgery syndrome. Chronic neuropathic back and leg pain are the most common types that stimulation treats. This means back or leg pain caused by nerve damage from:
Auto accident
Injury – personal, sports, work
Disease
Acute pain is like stepping on a sharp piece of glass, where the pain serves as protection letting you know something is wrong and not to continue. Whereas chronic neuropathic pain lasts for 3 months or more and does not help protect the body. �
�
Spinal stimulation is also used to treat complex regional pain syndrome or CRPS. This is a rare condition that affects the arms/hands or legs/feet and is believed to be caused by damage or malfunction of the nervous system. It is also used in treating peripheral neuropathic pain. This is damage to the nerves outside of the spinal cord often in the hands/feet that is caused by an:
Infection
Trauma
Surgery
Diabetes
Other unknown causes
�
Appropriate Treatment
Spinal cord stimulation should not be used in patients that are pregnant, unable to operate the stimulation system, went through a failed trial of spinal stimulation, and are at risk for surgical complications. The decision to use spinal stimulation is based on an individual’s needs and risks. Talk to a doctor, spine specialist, chiropractor to see if spinal stimulation could be an option.
�
Benefits and Risks
The effects of stimulation are different for everyone. Therefore, it is important to understand that spinal stimulation can help reduce pain, but not completely eliminate it. �
�
The Benefits of Spinal Cord Stimulation
In addition to reducing pain, other benefits of spinal stimulation include:
Better sleep
Improved body function
Increased activity
Improved mobility
Reduced opioid medication/s use
Less need for other types of pain meds
Reduced dependence on braces/bracing
�
Risks
During the implantation, there is a risk for:
Bleeding
Infection
Pain at the site of incision
Nerve damage
Rarely paralysis
� For some individuals, scar tissue can build up over the electrode, which can block the stimulator’s electrical impulse. The lead wire could move or shift out of position. This could lead to impulses being sent to the wrong location. The device itself could shift under the skin causing pain, making it hard to re-charge or communicate with the remote.
There is a risk that the lead wire could detach or break off causing a malfunction and require a replacement. Also, individuals could respond well to the stimulation at first, but later on, they develop a tolerance, and so the therapy no longer has the same impact and the pain could get worse because the nerves stop responding.
�
Take Precautions
Discuss with a doctor, spine specialist, or chiropractor what you can and can’t do after the stimulator is implanted and activated. Here are a few precautions:
Do not drive or operate heavy equipment when the stimulator is active.
Stimulation systems could set off metal detectors, which could require manual screening.
MRIs, electrocautery, diathermy, defibrillators, and cardiac pacemakers could have a negative interaction with certain types of stimulators. This could result in injury or damage to the spinal stimulator. Talk to your doctor to determine if a spinal stimulator is a treatment option that will work for you.
�
Weight Loss Techniques – Push Fitness Center
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at�915-850-0900. The provider(s) Licensed in Texas& New Mexico
With so much at stake, our bodies have developed a complex self-defense system to protect the spinal cord and its critical two-way�sensory information flow. As the body�s nerve center the spinal cord controls almost all voluntary and involuntary movements throughout the torso, arms, and legs.�It also receives sensory input from the torso and limbs. The�spinal cord plays a critical role and needs to be defended. The most prominent protection for the brain is the skull, for the spinal cord, it is more complicated.
Self Defense
The spinal cord consists of a bunch of nerves. One of the self-defenses is the cerebrospinal fluid (CSF) that cushions and nourishes them. On the outside, the spinal cord is protected by the tube structure known as the meninges. Three-layered membranes make up the meninges, each with its own protective role:
Pia mater
Arachnoid mater
Dura mater
Self-defenses do not stop there. Another self-defense includes the vertebrae or the backbones themselves, intervertebral discs, and various muscles and ligaments.
Meninges
The meninges are three layers of membranes that encapsulate the spinal cord at the brainstem from the top to the bottom of the spine. The innermost layer is the pia mater and is attached directly to the spinal cord. It is made up of mostly collagen that has an elasticity that allows the cord to maintain its shape. Next comes the arachnoid mater and is the middle layer.
Its primary role is to maintain the cerebrospinal fluid that fills the subarachnoid space between the pia and the arachnoid. A common condition known as arachnoiditis involves the arachnoid mater. It is a painful inflammation of the membrane that requires medical treatment. It can lead to disability if it is progressive.
Dura Mater
The outer layer is the dura mater and is the toughest. The dura rests on the arachnoid with a small amount of fluid in-between. The epidural space separates this membrane from the wall of the vertebral canal. Although it is tough, tears can occur. Tears can result from:
Injury
Epidural injections
Lumbar punctures
Complications from spine surgery
Some individuals can even develop tears spontaneously, sometimes as a result of a connective tissue disorder. When the dura tears cerebrospinal fluid leaks out of the space, leaving the brain and spine with less cushion and support.
Postural headaches are worse standing than sitting or laying down and can be severe are the most common symptom of spinal fluid leaks. But these tears typically heal quickly with bed rest.
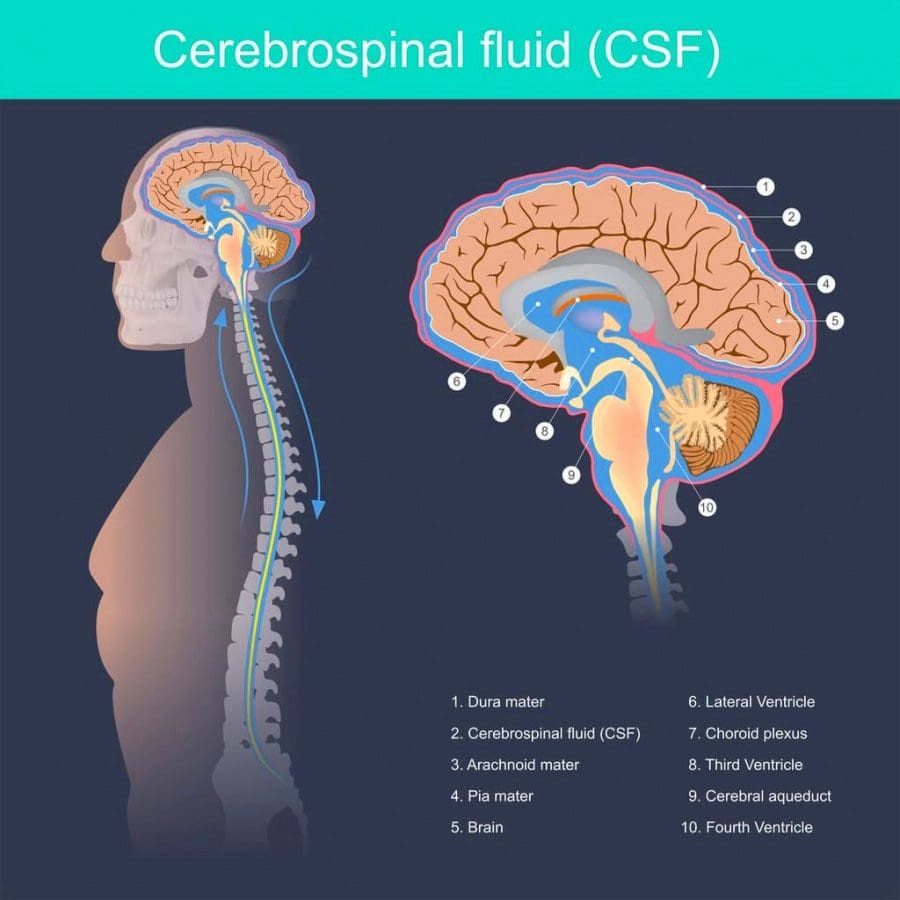
Cerebrospinal Fluid
Cerebrospinal fluid is the clear liquid that fills the space between the pia and the arachnoid. It is made in the brain�s ventricles with its primary function to protect and nourish the spinal cord and brain. The fluid also removes waste products from the brain. The fluid also plays a role in helping doctors diagnose disease/s.
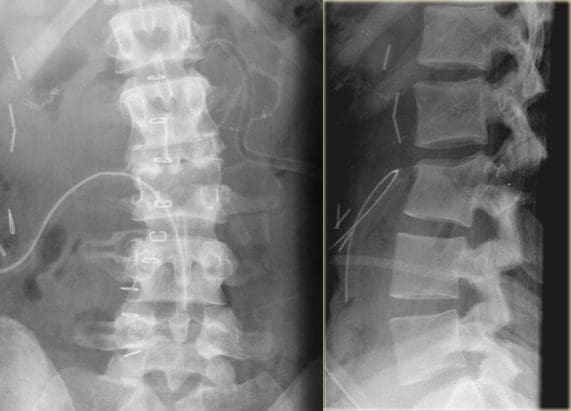
If a doctor suspects a severe infection or disorder of the central nervous system, they perform a lumbar puncture or spinal tap. The fluid can also contain evidence of inflammation or infection from waste products that the central nervous system discarded into the fluid. A doctor inserts a needle between two vertebrae in the lower back to remove a small amount of cerebrospinal fluid. The fluid is sent to the lab and analyzed. Lumbar punctures can be used to diagnose conditions like:
Infectious brain and spinal diseases like meningitis and encephalitis
To see how the fluid is moving diagnostic images are done by injecting dye know as myelography or radioactive substances known as cisternography into the subarachnoid space before imaging. Lumbar punctures can also be used to measure the pressure of the cerebrospinal fluid.
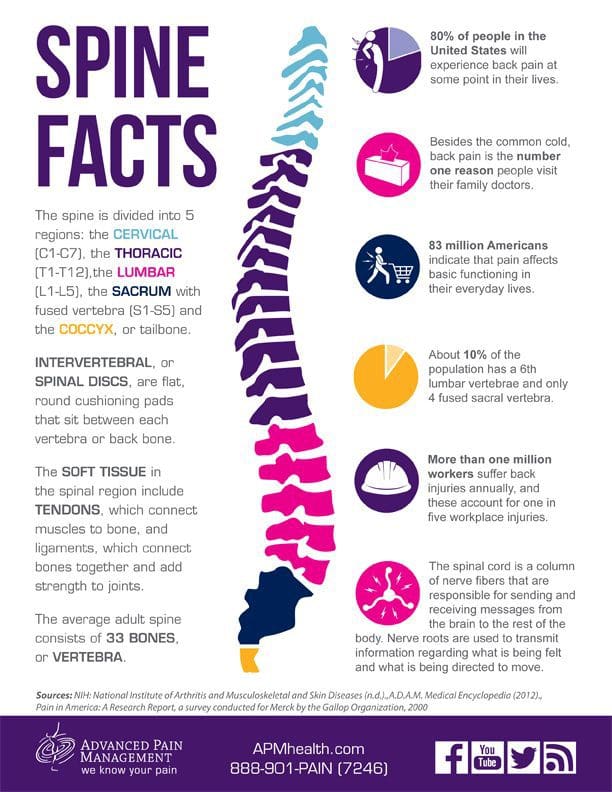
Vertebrae
There are 33 bones that make up the spine that forms a framework shaping the body and protecting the spine.�In a healthy spine, the neck vertebrae curve slightly inward called lordosis, while the middle vertebrae curves outward called kyphosis before meeting the low vertebrae curved inward. This makes the spinal cord flexible and balanced.
Each vertebra has a complex shape with a precise configuration determined by the location in the spine. Many conditions of the vertebrae involve nerves that get pinched/compressed as they exit the spine. Pinched nerves usually result from bone spurs on the vertebrae that crowd the canal and from herniated discs.
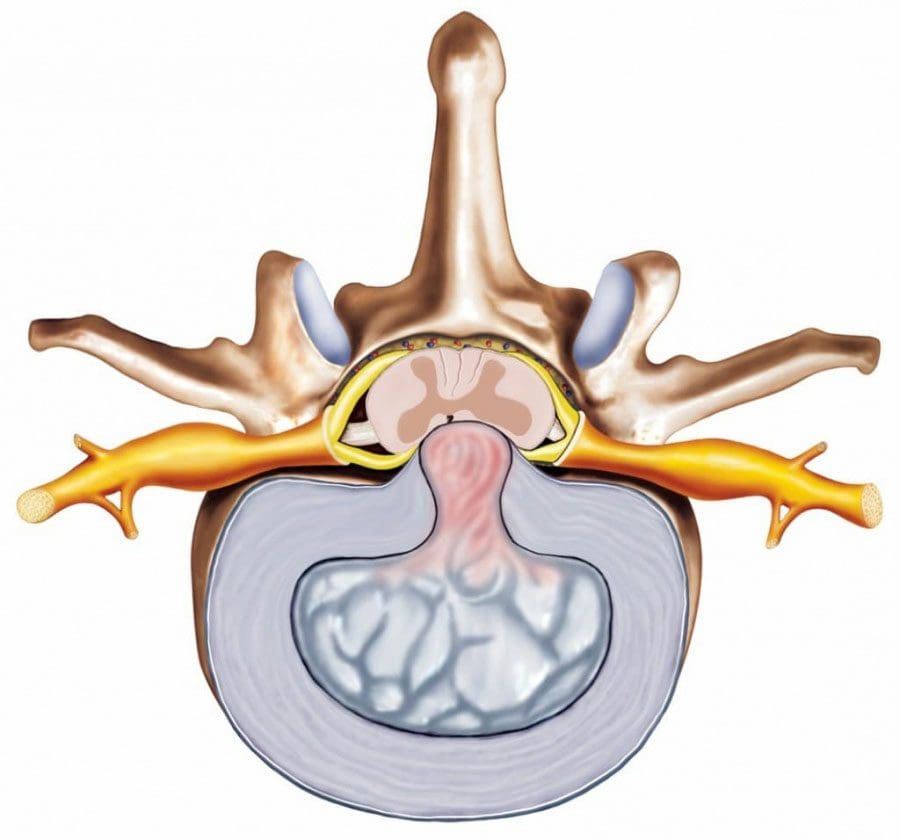
Intervertebral Discs
The intervertebral discs are the spine�s shock absorbers. They fill the space between two vertebrae with no direct contact. The endplates of each are coated with protective cartilage which anchors the discs in place. The gel substance part of each disc is called the nucleus pulposus. The tough cover known as the annulus fibrosus wraps around each disc to protect and shape it. There are no blood vessels in the discs and are nourished by the endplates of the vertebrae.
Herniated discs are the most common disc-related condition. When a disc herniates, the annulus fibrosus tears. The tear leaks out the protective gel to bulge out into the spinal canal. With no room in the canal for anything but the spinal cord and spinal fluid, the gel puts pressure on the surrounding nerve/s and the spinal cord itself. This is called myelopathy when the spinal cord gets compressed. Non-surgical treatments are quite successful in healing herniated disc/s.
The spine�s self-defense is elaborate, effective, and complicated. Consult an experienced spine specialist/chiropractor who can produce the best results and benefits.
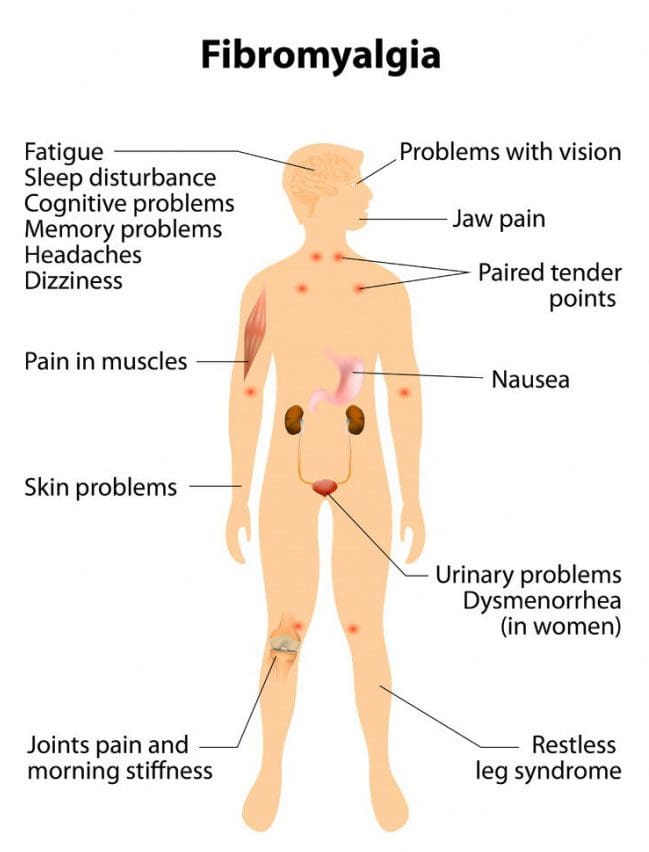
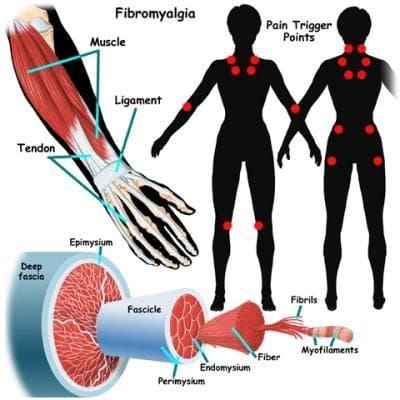
Fibromyalgia is a chronic pain disorder affecting millions and mostly women. It is physically and emotionally distressing. Those with the condition experience widespread chronic muscle pain. Research has shown that individuals with fibromyalgia could have a lower threshold for pain. This can come from injury, emotional distress, or abnormal levels of substances/chemicals in the brain and spine linked to pain sensitivity. One of the most common treatments is chiropractic medicine.
Common symptoms/conditions individuals report:
Chronic fatigue syndrome
Irritable bladder
Irritable bowel syndrome
Migraines
Sleep disorders
Restless legs syndrome
TMJ or Temporomandibular joint disorder
Raynaud’s Syndrome�-�a�rare blood vessel disorder causing the toes and hands to feel cold or numb.
Doctors are still trying to figure out the relationship between these conditions and fibromyalgia.
Causes
Doctors have yet to determine the exact cause, however, research is ongoing and beginning to shed light on the condition. Some possible causes include:
Abnormalities in the endocrine system
Abnormalities in the autonomic nervous system
Genetics
Muscle tissue abnormalities
Abnormal blood flow
As research has discovered many conditions/disorders do not have one cause but rather, several factors that impact the probability of developing the condition.
Questions
It has become one of the most common chronic pain conditions. 1 in 50 Americans are dealing with fibromyalgia. The condition can be difficult to diagnose, and, because of its chronic nature, it can linger for months and even years. Typically it causes pain throughout the body and creates areas that become tender to the slightest touch. There are both traditional and alternative treatments available.
Traditional approaches to manage the pain:
Anti-inflammatory’s
Over-the-counter pain relievers
Sleep medications
Muscle relaxants
Fibromyalgia medications include:
Lyrica – pregabalin, which is a nerve pain medication
Cymbalta – duloxetine hydrochloride, which is an antidepressant that can also help manage pain
Savella – milnacipran HCI, which is an antidepressant and nerve pain medicine
The type of treatment depends on the symptoms. For example, a doctor could prescribe an antidepressant to reduce pain and depression. If stress, anxiety, and trouble sleeping are presenting,�a therapeutic exercise program could be the answer. Individuals prefer natural remedies/therapies instead of more medications like vitamin therapy, acupuncture, and meditation.
Other treatment options include alternative treatments like:
The most common issue is constant and consistent pain, which can affect the entire body for weeks and even months. Individuals realize that chiropractic helps restore overall health and aids the body to heal itself. Adjustments to the spine bring alignment and balance back to the body. Also incorporated is soft tissue work that can relieve and reduce painful pressure/trigger points and decrease pain in tender spots.
Range of motion is increased
Chiropractic medicine also adjusts the body’s joints and helps loosen them up. This increases the range of motion and allows the individual to move more freely and easily. Depending on how long the individual has been dealing with the condition, it can take a few treatments to achieve optimal results, so it does take a commitment from the individual patient. However, in the long run, it is well worth the time.
Sleep is improved
The pain associated with fibromyalgia often affects an individual’s ability to sleep well. Being unable to sleep normally will leave you exhausted, foggy, unable to accomplish things and irritable to downright angry. A chiropractor’s ability to loosen the body’s joints, massage tender points, and kickstart the body’s self-healing mechanisms means individuals with this condition can enjoy deep sleep, and stay asleep.
Complements other therapies
Medicines/treatments/therapies can counteract with each other, or get mixed up and cause side effects. Chiropractic medicine can be utilized in combination with medications/treatments, either traditional or natural. Individuals diagnosed with this condition should speak to their chiropractor about the different treatments available. Customized treatment programs are created case-by-case and are tailored to the specific needs of that individual. Remember there is not a one-stop solution.
Empowers the individual
Individuals that have to deal with painful, chronic conditions can exhaust themselves with the varying treatment options and can feel as if they have no control over the situation. This causes stress, anxiety, and depression, which works against achieving overall wellness. With chiropractic, individuals are more in charge of their treatment plan, which leads to an optimistic outlook in their recovery.�
Chiropractic medicine treats not only the symptoms of fibromyalgia but attempts to get to the root cause to alleviate the condition or to activate the body’s self-healing response. Patients that commit will see the benefits along with reduced pain, better mobility, and sound sleep.
The best benefit is being able to take control of the circumstances and playing a vital role in the managing of an individual’s well-being. Understand that there are options available for fibromyalgia pain management. If you or a loved one has been diagnosed with fibromyalgia, don�t go it alone. Dr. Alex Jimenez is passionate about helping those who are injured or struggling with a condition get relief. Contact us today to schedule an appointment.
Spinal cord injury/s are separated into two phases: There is the primary injury and the secondary injury.
The primary injury refers to the physical trauma to the spine. This could be a:
Car accident
Sports accident
Severe fall
Other traumatic events
When the primary injury happens, neurological injury to the nerves and spinal cord can take place in the form of:
Compression
The compressing of the spinal cord/nerves can cause an impact of bone, disc, and ligaments against the tissues. This is because the spinal canal becomes narrowed and shifts out of proper alignment. This causes the nerves to get pinched during the injury.
Stretching
Tissues get stretched beyond what they’re capable of so the spinal cord can suffer serious damage with the slightest trauma directly to it. Complete cutting or severing of the cord is rare.
Blood supply inadequacy
The injury can cut off or significantly reduce blood supply to the cord and nerves. If the microscopic blood vessels get damaged almost instantaneous hemorrhage or bleeding into the spinal cord.
Spinal cord damage can be seen on an MRI immediately after trauma.
Secondary injury is a cascade of events that occur after the initial trauma, which is the body’s attempt to heal the injury.
This could be seconds, hours, days, and weeks afterward. Several factors play a role in how severe secondary injury will be.
The body releases chemicals in response to trauma. These chemicals cause inflammation, decreased blood flow, and cell death.
Treatments/therapies for spinal cord injuries usually directed at one or more steps during this cascade. Goals of treatment:
Decrease inflammation
Increase blood flow
Reduce scar formation
Slow degradation and cell death
The overall treatment of a spine injury is focused on stabilizing the injury. Once that has been accomplished, there are two following goals:
Treatment priority is to reduce the effects of primary and secondary injuries. One is to immobilize the spine to prevent further injury. This typically happens at the scene of the accident and can be done with a hard collar or brace. IV fluids and medications to maintain blood pressure and possible administration of oxygen may be used. These techniques are fairly standard to deal with primary injury/s.
Surgery could be needed to remove physical impingement/compression on the nerves, restore blood flow, and provide room for subsequent inflammation to help the body heal itself.
Sometimes surgery takes place later to restore the alignment of the bone and correct any deformities that may have occurred. This is as important as decompression for maximizing a patient’s rehabilitation. Stabilization from surgery can help patients sit upright, walk, and maintain proper weight on the trunk. It also helps to avoid developing posture problems in the future.
Methylprednisolone is a steroid that’s considered a neuroprotective agent. This is the only drug treatment supported by the medical community to be used immediately following the primary injury. There is still debate among the medical community as to the effectiveness of this steroid. To date, it has not been defined as a standard of care by any major medical associations.
Treatment Research
Other treatments have been proposed and proven successful in animal trials. These treatments first go through animal trials before human trials. Replicating the benefits in humans is still quite difficult to achieve. There were 100 different treatments that do work in animals, however, methylprednisolone is the only treatment that has demonstrated consistent results.
Reasons why research for spinal cord injuries is tough:
Anatomical differences in animal’s spinal cords: While rodents are typically used for most research, their spinal cords have the ability to create stepping patterns without signals from the brain. That means that after a spinal cord injury with no treatment they can learn to walk again. The human spinal cord cannot do this.
The differences between actual injury and a simulated one: Actual injuries that result in trauma to the spine usually have neurological compression that exceeds that seen in the animal models during the simulated injury. This means that treatments that are effective in animal trials where there is less trauma to the bones and nerves than�when the same treatments are tried for actual injuries, could be less effective because the injury/s are more severe.
During spinal cord treatment tests, researchers typically use mild/moderate spinal cord injuries. Human injuries can vary from one extreme to another that they are either too severe for therapy or too mild that they recover without treatment.
Doing the same experiments and research on animals and humans is complicated: There are all kinds of variables in animal research that can’t be controlled in human studies. There are different models of injury, that happen at different times and are treated with different medications, and all contribute to inconsistencies. The results significantly change the accounts of how useful any given treatment is, especially when comparing the animal studies and human studies.
Example –� Treatments in a laboratory are begun within one hour after injury simulation. This doesn’t happen in clinical settings, because typically, first responders at accident sites work to stabilize the patient’s airway, and spine before they are transported to an emergency room. Replicating that procedure with actual first responders can be quite difficult to do in clinical studies.
Promising Treatments
There are promising treatments in spinal cord injury:
Hypothermia
Naloxone
Corticosteroids
All three have shown positive results in animal trials. But there have been varying results in human trials. While these are positive results, further research from scientists and physicians is needed to develop a highly effective treatment for spinal cord injury.
Hypothermia treatment has piqued a great deal of interest based on a case of its use on a professional football player, that suffered a spinal cord injury. It was a success, but unfortunately, other human studies utilizing this treatment failed to demonstrate the same benefits and some believe the risks outweigh the benefits. Physicians believe that the player’s positive outcome was the result of a less severe injury and early decompression, and not necessarily from the hypothermia treatment.
Researchers debate that freezing reduces blood flow in the injured spinal cord but that it could worsen the secondary injury/s.
Conclusion
Treating spinal cord injury research is still a major focus in the medical community. With progress taking place there is still not yet the major breakthrough. Continued investigation into treatments for spinal cord injuries will go on until spinal injuries are no more.
Severe *Sciatica”* Pain Relief | El Paso, Tx (2020)
NCBI Resources
Spinal injury or trauma can result in myofascial pain syndrome, but lifestyle factors usually have a hand in the condition. Poor posture over a long period,�for example,�sleeping in an awkward position can cause physical muscular stress on the spinal muscles.�Mental and emotional stress can present itself through muscle tension�that helps the development of trigger points.
The�trapezius muscle, that extends from the back of the neck down the shoulders and upper back, is the most common site of spinal trigger points and myofascial pain because of the significant amount of pressure that the muscle has to bear and its susceptibility to whiplash.
Spinal Cord Injuries Are Not Only Caused by Trauma
When people think of spinal cord injury/s or SCI’s, traumatic events like a major auto accident, hard fall, severe sports injury or intense work injury come to mind. It is true that auto accidents are the leading cause, however, non-traumatic accidents and diseases like a spinal tumor can also cause spinal cord injuries.
These types of injuries involve damage to the spinal cord that can temporarily or permanently affect its functionality. Spinal cord injuries are divided into 2 categories: traumatic and non-traumatic. Even with non-traumatic injuries the impact or severity is not lessened and the aftermath can have a devastating effect on a person�s life.
Spinal Cord Injury Trauma
Vehicle crashes: Motor vehicle accidents are the leading cause of traumatic spinal cord injuries, and they account for 40% of all SCI’s.
Falls: Falls are the second cause of traumatic spinal cord injuries, and they account for 32% of injuries.
Violence: Violent acts, like gunshot wounds or a stabbing cause around 14% of spinal cord injuries.
Spinal cord injuries occur more in men than women with 80% of cases affecting men.
Although people of all ages can experience SCI, there are activities/events that increase the risk that affects different age groups more than others. An example is high-impact actions like motor vehicle accidents and sports injuries occur more in young adults. Conversely, spinal cord injuries caused by a fall happens more in adults over age 60.
Regardless, SCI occurs more in the neck or cervical spine. Around 60% of cases involve the neck, followed by the mid-back or thoracic spine that averages to around 32% of injuries. Although most people experience low-back pain, only 9% of spinal injuries occur in the low back and tailbone or lumbosacral spine.
Understanding SCI Trauma
Damage to the spinal cord not only affects the area where the point of impact occurred. The primary injury can also damage cells, dislocate the vertebrae and cause spinal compression. It can also trigger secondary injuries, that cause a series of biological changes. This can happen within weeks or months after the injury.
The secondary injury cascade processes:
Glial cells along with the nerve cells in the spinal cord begin to die. These cells provide nutrients and other support to the nerve cells in the central nervous system. This consists of the brain and spinal cord.
The blood vessels in the spinal cord lose their ability to function, and this reduces the blood supply to the cord. When the blood supply becomes inadequate it is called ischemia. Blood vessel injuries expose the cord to inflammatory cells that in turn cause swelling. When the spinal cord becomes inflamed the spinal cord gets more and more compressed. If this happens�the initial injury progressively worsens.
This changes the cord�s structure and its normal operation. The secondary injury cascade can interfere with the cord�s ability to heal itself. This means an individual could experience permanent nerve pain and dysfunction.
Non-traumatic SCI
Spinal cord damage does not only happen with traumatic events. An SCI can also be caused by non-traumatic diseases in the spine. Tumors are the leading cause, but infections and degenerative disc disease can also cause serious damage.
Non-traumatic SCI’s happen more than traumatic based ones. �The incidence of traumatic SCI in North America comes to around 54 cases per one million people. With the incidence of non-traumatic SCI is around 1,227 cases per million people.
Healthy Spinal Cord Injury Outcomes
Spine researchers are making great strides in developing optimal protective and regenerative treatments to improve spinal cord health after these injuries occur.
Currently, innovative medical, surgical, cell-based and alternative treatments are furthering the medical community�s understanding of SCI’s. This is dramatically improving the quality of life and creating positive futures for individuals who experience these injuries.
Car Accident Injury Rehabilitation | El Paso, Tx (2020)
NCBI Resources
The muscles in the back keep the spine moving and functioning properly.�When the spine or�abdominal muscles are�weak this creates a higher probability of a back strain or injury. Having strong, healthy spine muscles are important because they function in maintaining correct posture, which in some cases, causes chronic back pain because of poor posture.
If�only one part of the body is�strengthened like the back is not enough. Therefore strengthening the rest of the body is a must. These include the body�s core and leg muscles. Total body strength will reduce back pain and can help perform regular activities, like�lifting heavy objects much easier, with more confidence and with a lesser probability of injury.
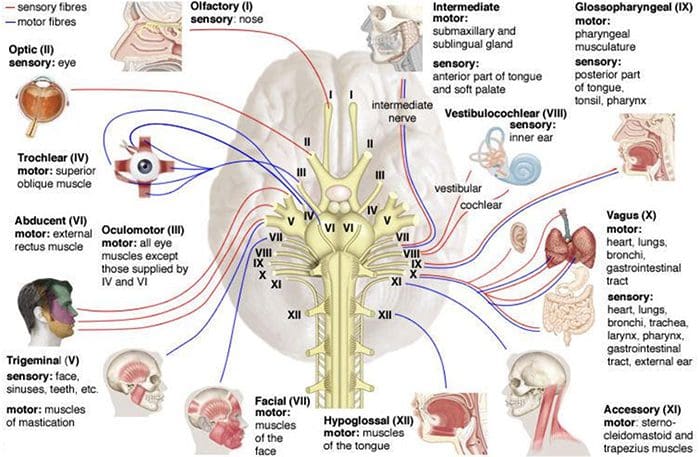
The spinal cord and brain make up the central nervous system while the spinal nerves that branch to the spinal cord and cranial nerves that branch to the brain makes up the peripheral nervous system.
There are thirty-one sets of nerves that extend out of the spinal cord and are connected to it by the nerve root. Each nerve branches out about a half inch from the spinal cord before dividing into smaller branches. The dorsal rami are on the posterior side of the branch while the larger ventral rami are on the anterior side.
The dorsal rami provide nerve function for the skin of the trunk and posterior muscles. The ventral rami from T1 to T12 provide nerve function to the skin of the trunk as well as the lateral and anterior muscles. The anterior divisions that remain for plexuses, networks that provide nerve function to the body. Each plexus has specific areas on the body for skin sensitivity as well as certain muscles. Their point where they exit the spine determines how they are numbered. The four primary plexuses are:
Cervical plexus, C1 � C4, innervates the diaphragm, shoulder, and neck
Brachial plexus, C5 � T1, innervates the upper limbs
Lumbar plexus, T12/L1 � L4, innervates the thigh
Sacral plexus, L4 � S4, innervates the leg and foot.
These spinal nerves have two sets of fibers: motor and sensory. Motor fibers facilitate movement and provide nerve function to the muscles. Sensory fibers facilitate sensitivities to touch, temperature and other stimuli. They provide nerve function to the skin.
What are Myotomes and Dermatomes?
A group of muscles that are innervated by the motor fibers that stem from a specific nerve root is called a myotome. An area of the skin that is innervated by the sensory fibers that stem from a specific nerve root is called a dermatome. These patterns of myotome and dermatome are almost always identical from person to person. There are occasionally variances, but that is rare.
This consistency allows doctors to treat nerve pain in patients. If a specific area is hurting, they know that it is attributed to a certain myotome or dermatome, whichever the case may be, and its corresponding nerve root. Problems with nerve damage are often the result of stretching the nerve or compressing it.
When the nerves are injured in specific areas like the lumbosacral or brachial plexus, it presents as sensory and motor deficits in the limbs that correspond to them. Myotomes and dermatomes are used to assess the extent of the damage.
How are Myotomes and Dermatomes used to Assess Nerve Damage?
When a doctor tests for nerve root damage in a patient, he or she will often test the myotomes or dermatomes for the nerves assigned to that location. A dermatome is examined for abnormal sensation, such as hypersensitivity or lack of sensitivity.
This is done by using stimulus inducing tools such as a pen, paper clip, pinwheel, fingernails, cotton ball, or pads of the fingers. The patient is instructed to provide feedback regarding their response. Some of the abnormal sensation responses include:
A myotome is tested for nerve damage in the muscles which presents as muscle weakness. This grading scale, which assigns a rating to the degree of muscle weakness, is often used:
5 � Normal � Complete range of motion against gravity with full resistance
4 � Good � Complete range of motion against gravity with some resistance
3 � Fair � Complete range of motion against gravity with no resistance, active ROM
2 � Poor � Complete range of motion with some assistance and gravity eliminated
1 � Trace � Evidence of slight muscular contraction, no joint motion evident
0 � Zero � No evidence of muscle contraction
During a typical chiropractic exam, your chiropractor will assess both dermatomes and myotomes for potential neurological problems. This gives them additional insight on how to treat your condition, whether it’s related to a subluxation of vertebral bodies or other, other disease processes.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine