Belly fat is a gateway to back pain/spinal issues that can lead to various health problems. The bulging belly population has grown a bit since the beginning of the COVID-19 pandemic. 37% of individuals have gained weight since it began, according to a global Ipsos survey. If back pain is presenting and there is excess weight around the abdomen known as abdominal obesity, this could be a contributing factor.
Belly fat and posture
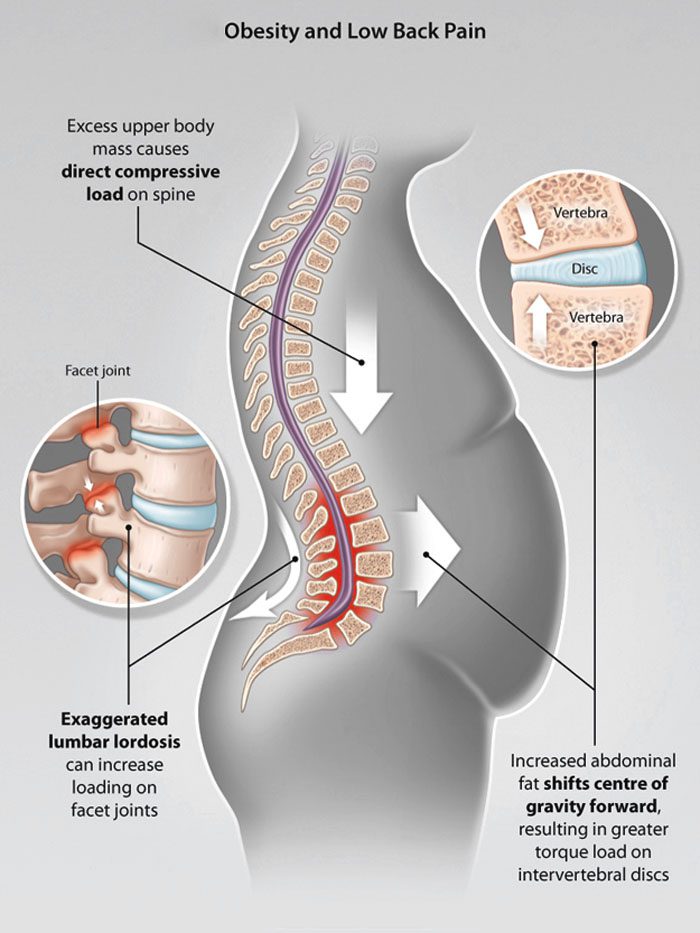
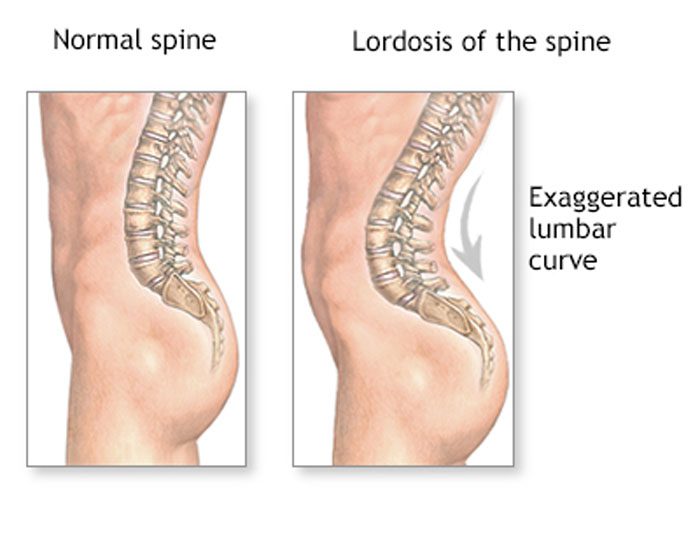
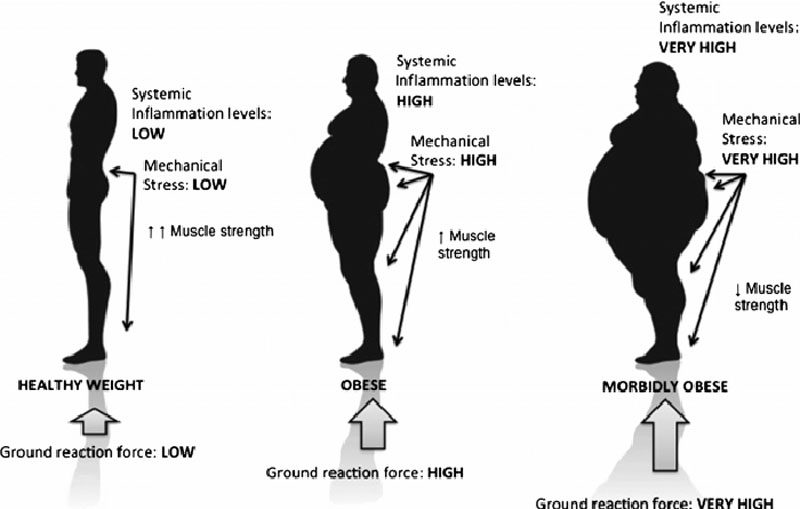
When the natural curves of the spine are normal, the core is stable and well-supported. Excessive weight, including a large abdomen, shifts these curves out of correct alignment. Excessive abdominal fat has been associated with lordosis, which is an excessive inward curve of the spine toward the lower back. One study found that severely obese individuals had pain and changes in posture. This was especially visible in the spine, knees, and feet.
Front-loading shift
The back pain felt from a bulging belly can be caused by a shift in posture and body mechanics. Studies show these can have a negative impact on back pain and body positioning. All or most of the weight is placed on the lower back.
Overloaded discs
Abdominal obesity can damage/injure the discs/shock absorbers of the spine. This leads to:
And a bulging belly can flatten the height of the intervertebral discs.
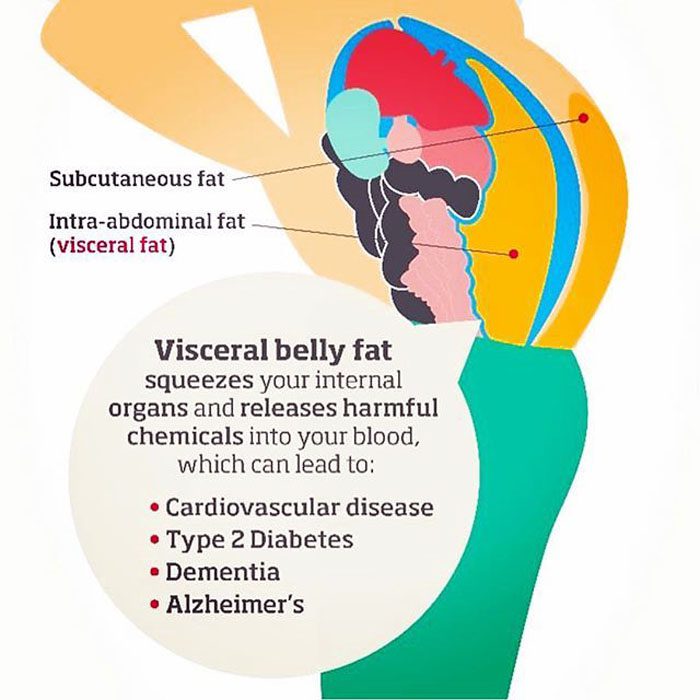
Fat pollutants in the blood
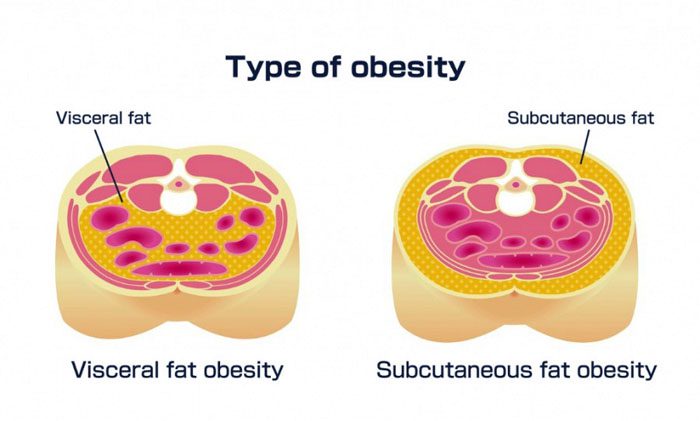
Fat can accumulate and secrete toxins that contribute to swelling and inflammation that can be painful. Over time, these toxins wear down components of the skeletal system.A study found potential links between obesity and degenerative disc disease. Scientists found a connection in obese men, but not obese women. This is believed to be because men tend to store fat in their bellies, and women tend to store fat in the buttocks and thighs.
Damage to the musculoskeletal system
The bones constantly renew themselves, but when there is excess body fat it can interfere with the process. This has the potential to turn into osteoporosis over time. Studies associate visceral fat with lower bone mineral density, and an increase in the risk of fractures.
Ankylosing spondylitis treatment and fat interference
Ankylosing spondylitis is an inflammatory disease that causes chronic back pain and can cause the vertebrae to fuse. The back can be extremely stiff, and the condition can lead to a permanently hunched posture. There are medications to improve symptoms and slow the disease. However, being overweight reduces the drugs’ effectiveness. This is because belly fat can cause medication absorption problems.
Rare spinal condition linked to obesity
Obesity along with a high Body Mass Index increases the risk of a rare condition called spinal epidural lipomatosis or SEL. This is an overgrowth of body fat in the spinal canal. Spinal epidural lipomatosis can cause various types of back pain. This is why it is recommended to have a doctor examine and evaluate any aches or pains.
Body Composition
Kombucha beneficial for gut bacteria
Kombucha contains a wide variety of bacteria and fungi that helps ferment the sugar in kombucha drinks. It is able to affect the existing microbes in the gut by inhibiting the growth of various gut-dwelling pathogens. These include:
It is a probiotic drink made from fermenting green or black tea
It is made up of healthy bacteria that produce acetic acid that is beneficial for blood sugar, insulin levels, and body composition
It helps the body process food by lowering insulin levels after a meal
It contains polyphenols that reduce oxidative stress, to help fight disease risks
It destroys unhealthy bacteria in the gut
It helps increase healthy bacteria
Kombucha can be thought of as a natural antibiotic. However, it does not come with the weight-gain side effect. Improving the health of the gut through fermented foods like kombucha help reduce the risk for weight gain/obesity, as well as restore gut health for those trying to lose weight by creating a healthy gut environment.
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP, CIFM, CTG* email: [email protected] phone: 915-850-0900 Licensed in Texas & New Mexico
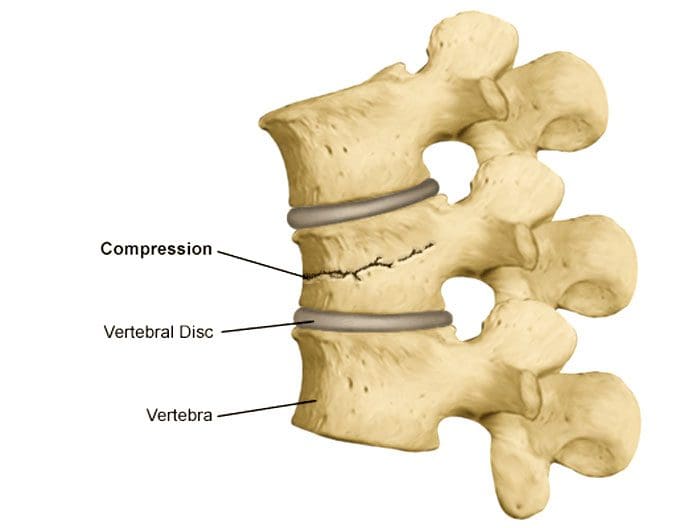
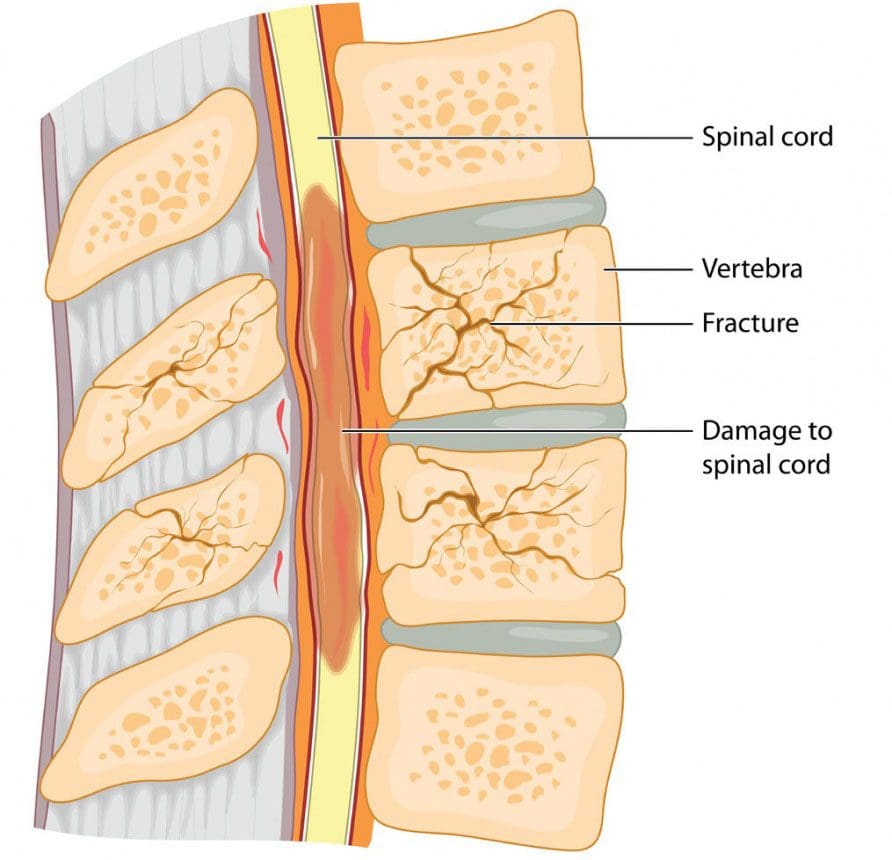
Spinal vertebral compression fractures are a common injury in older individuals brought on from a lowered bone density. Hip and wrist fractures get most of the attention when it comes to osteoporosis. However, spinal fractures happen almost twice as often and affect around 700,000 individuals yearly. This is according to the American Academy of Orthopaedic Surgeons or the AAOS. These types of fractures are also known as:
Fragility fractures
Vertebral compression fractures
Osteoporotic compression fractures. These usually happen as a result of thinning and weakening bones caused by osteoporosis.
The Academy of Orthopedic Surgeons notes that changes in the body’s musculoskeletal bone structure can go unnoticed for years. This leads to the vertebrae narrowing and flattening, rounding the spine as a result, creating compression. Because of the weakened bone, the pressure, even from everyday low-impact movements like reaching, bending or twisting. There are strategies that can help prevent osteoporosis and osteoporotic compression fractures.
More Movement and Physical Activity
One prevention strategy that is highly recommended is more movement and physical activity. This does not include occasional gentle movements like taking a break from sitting. Improving the spine’s health means using the full range of motion and loading the bones so they can get build strength. This could be walking more, which creates spinal resistance. Also using light weights with high repetitions with five to ten pounds of a load is enough to challenge the spine without generating muscle stress.
Individuals think they need to rest more as they get older, but to build and maintain bone density to prevent osteoporotic compression fractures more physical activity is needed. Moving around for 10 to 15 minutes every hour is a good way to start. Incorporating more activity, and focusing on healthy diet changes will help shed excess weight. This will decrease pressure on the spine, reducing the risk of fractures. For individuals with osteoporosis of the spine, it is important to review any exercise plans with a physician or doctor of chiropractic to ensure that they are safe. The wrong types of movement or too much stress on a fragile spine can definitely cause a fracture.
Medications and Other Conditions
There are medications that can help build bone density, but there are also medications for conditions that can actually cause faster bone density loss. Individuals could be taking a medication that’s good for one issue/condition, but not realize it may be associated with a reduction in bone density. This is why it is important to review prescriptions with a doctor with bone density loss side effects in mind. Medications that can cause bone loss include:
Anti-seizure drugs like carbamazepine and phenytoin
Diuretics like furosemide
Also, review any underlying conditions that could affect osteoporosis. As an example, the National Institutes of Health or NIH note that individuals with diabetes, specifically type 1, can have poor bone quality increasing their risk of fractures.
Adding Calcium To The Diet
An adequate intake of calcium is essential for osteoporosis prevention and helps lower the risk of fragility fractures. A low calcium intake contributes significantly to lower bone density and faster bone loss with age. Vitamin D also helps in bone injury prevention.
Treatment
Compression fracture/s diagnosis are confirmed through imaging tests like:
X-rays
Magnetic resonance imaging MRI scan
Bone scan
Computed tomography CT scan
Bone density testing with dual-energy x-ray absorptiometry DEXA will determine bone mineral density. If a scan reveals there is a vertebral compression fracture, the most common approach is no treatment. According to the Academy of Orthopedic Surgeons, most individuals with this type of injury improve within three months with a combined rest period and limited pain medication use.
Some individuals are recommended to wear braces to restrict movement so the fracture can heal without any added compression or stress. For those that do not respond to non-surgical treatment, minimally invasive surgery could become an option. In both cases, a doctor will suggest similar aforementioned strategies to help strengthen the bones and prevent worsening or creating new issues.
More flab on the middle that gets harder to burn off
Performance at work, the gym, or on the road slows down or begins to reverse
Workouts, sporting events, physical activity that the body was able to bounce back from quite easily now take twice as long to recover from
Things start to change when the body enters its 30’s. Whether light exercise, playing weekend games, local sports, etc, the key is to just stay active. By paying close attention to nutrition and making minor adjustments, individuals can maintain and improve body composition, stay strong and healthy in their 30s and be ready for the future.
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP, CIFM, CTG* email: [email protected] phone: 915-850-0900 Licensed in Texas & New Mexico
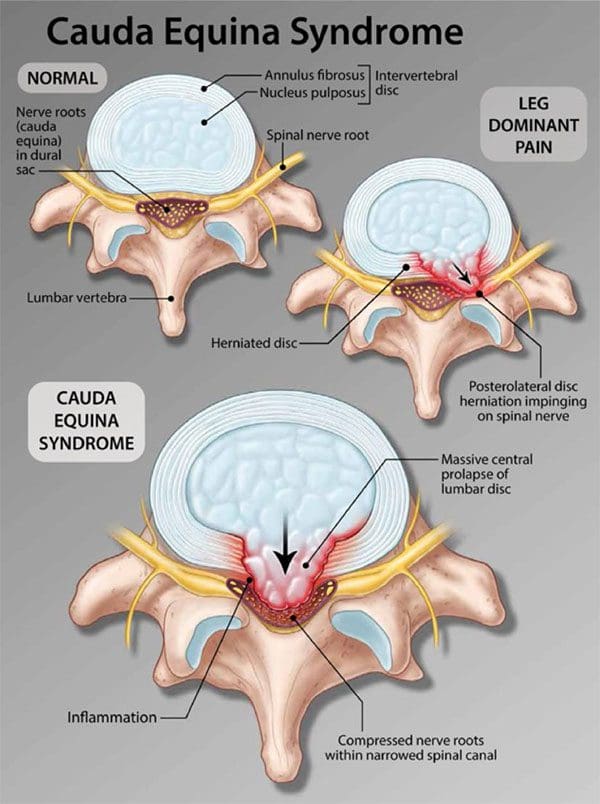
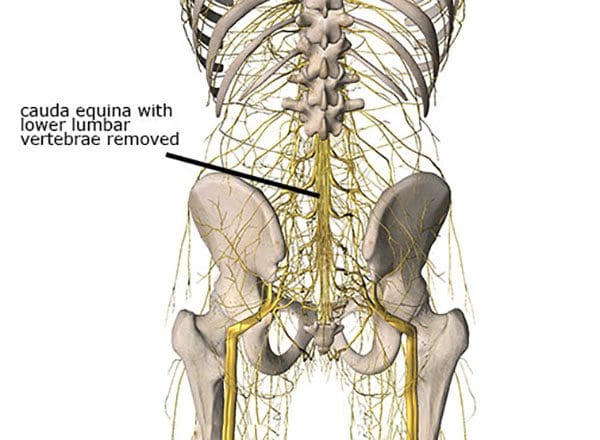
Cauda equina syndrome is an emergency that needs to be treated as soon as possible. It is a form of spinal nerve compression, but if left untreated, it can lead to permanent paralysis of one or both legs and permanent loss of bowel/bladder control. Lower back pain after sitting for too long or improperly lifting something heavy happens to most if not all of us.
However, sometimes pain in the lower back can be an indicator of something more serious. Especially, for individuals that are dealing with or managing back pain. One condition is cauda equina syndrome. It�s not like sciatica or arthritis, but it does have specific symptoms that individuals should be aware of.
Cauda Equina Syndrome
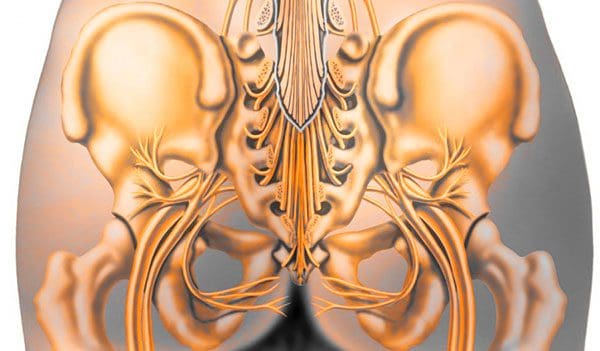
The term comes from Latin that means horse�s tail. The cauda equina forms the group of nerves that run through the lumbar spinal canal. Generally, the condition means two things:
There is nerve compression of most of the lumbar spinal canal
Compression symptoms like numbness or weakness in the leg/s
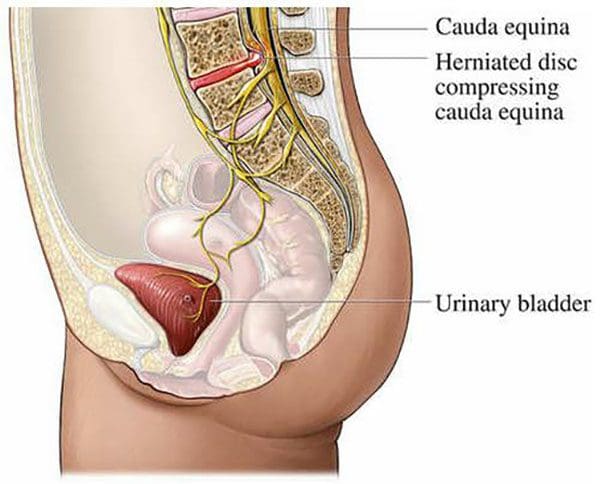
How cauda equina syndrome differs from typical compression of the lumbar spinal canal is that it can be caused by different issues, from fractures, tumors, and infections. More commonly, it is disc herniations that cause the problems. The key difference is the degree of nerve compression, and the number of nerves compressed.
For example, compression of a single nerve will not cause loss of bladder function. But compression of multiple nerves, especially the sacral nerves can cause loss of function. Nerve compression that leads to pain or numbness can be treated differently. Surgery is reserved for severe cases and for individuals that are not improving with non-invasive treatment.
Sneaky Presentation
One of the major factors is long-term compression that individuals do not realize they have. Individuals are more likely to be aware of symptoms from another spinal condition before cauda equina syndrome presents. However, the condition presents quickly but often other overlapping back problems mask cauda equina syndrome.
Causes
The syndrome can be brought on from anything that compresses the nerves. Most commonly, it is a root compression from degenerative processes, specifically lumbar disc herniations. Other causes include:
A doctor will examine any significant changes in bladder, bowel, or leg function that are considered red flags prompting an early and complete assessment. A physician will ask for a complete/detailed history of the onset and progression of symptoms.
The second is a close physical examination which includes testing sensation and strength along with a rectal exam to assess voluntary contraction. Also checking the body’s reflexes, assess walking gait and alignment. If most or all of the symptoms are presenting this will set in motion spinal imaging or an MRI. If the symptoms, exam, and imaging match, it will lead to an emergency admission to the hospital.
Body Composition Spotlight
Obesity and Osteoarthritis Connection
A variety of factors contribute to the development of osteoarthritis, including genetic factors and lifestyle choices. Research supports obesity is a significant risk factor in the development of osteoarthritis. It is pretty straightforward as body weight increases this equals increased load on the spine, and joints, especially the weight-bearing ones like the hips and knees. Increased pressure leads to early wearing, tearing, and eventual development of osteoarthritis. Added weight affects the body’s biomechanics and gait patterns.
However, obesity has also been shown to be a risk factor even on the non-weight-bearing joints. This is based on adipose tissue, which is more than just insulation. Adipose tissue is metabolically active and is involved in the secreting adipokines and cytokines which promote an inflammatory response. Pro-inflammatory adipokines and cytokines can have detrimental effects on joint tissue including damage to cartilage, synovial joints, and subchondral bone. The effect of inflammation on the joints in the body can contribute to the development of osteoarthritis.
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at�915-850-0900. The provider(s) Licensed in Texas& New Mexico*
Minimally invasive surgical procedures can be used to treat spinal compression fractures. These procedures are utilized to reduce severe pain, stabilize the fracture itself, and restore lost height or shape of the broken vertebral body. These procedures are known as:
Balloon kyphoplasty
Vertebroplasty
Vertebral body augmentation
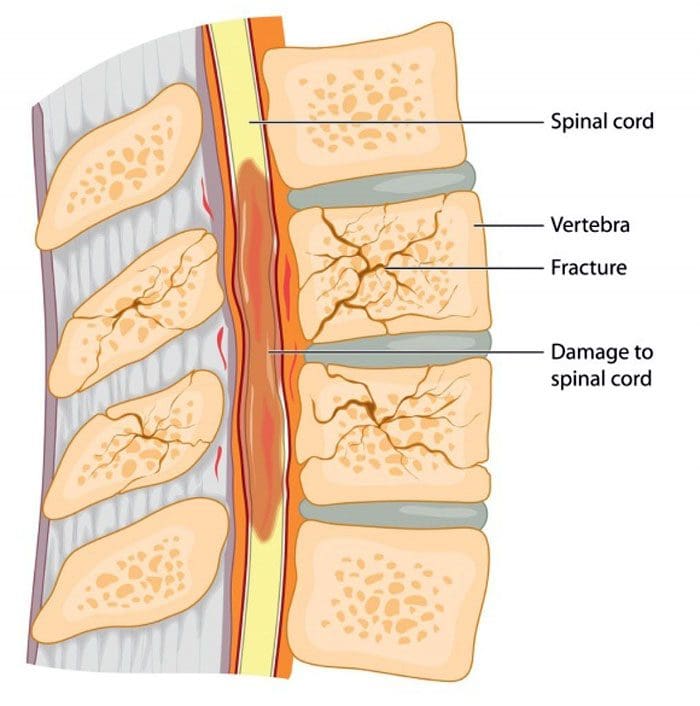
A vertebral compression fracture is a type of spinal fracture that can be caused by osteoporosis. This is a metabolic disease that weakens bone density and increases the risk of fracture/s in the spine, wrist, and hip. Osteopenia and osteoporosis affect millions, according to the National Osteoporosis Foundation. If left untreated, it can progress without an individual knowing and painlessly until the bone/s fracture. A vertebral compression fracture is more frequent than hip fractures and can lead to extended disability.
Vertebroplasty
Vertebroplasty is a minimally invasive treatment done through the skin for painful vertebral compression fractures. It also helps with strengthening the surrounding vertebral bodies also at risk of fracturing. Orthopedic bone cement is injected into the fractured vertebral body.
How is it performed?
Under general anesthesia, a specialized needle for bone is slowly inserted through the soft tissues of the back towards the vertebral compression fracture. The surgeon sees the position of the needle at all times through a real-time x-ray. Once reached a small amount of orthopedic bone cement, called polymethylmethacrylate, is injected into the vertebral body. Polymethylmethacrylate is a medical-grade bone cement that’ss been used for years for various orthopedic procedures.
The cement can sometimes be combined with an antibiotic to reduce the risk of infection along with a powder that has barium or tantalum. This allows it to be seen on the x-ray. The cement is a thick paste that hardens quickly. The fractured body is injected on the right and left sides, the midline of the back. After a few hours, the patient is up and moving. Most go home on the same day.
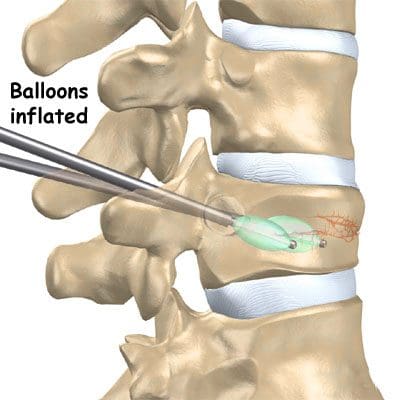
Balloon kyphoplasty
Balloon Kyphoplasty is another newer minimally invasive surgery for vertebral compression fractures that can be associated with osteoporosis. Kyphoplasty utilizes a balloon that expands the compressed bone to help restore lost vertebral height while creating a space where bone cement is injected. Kyphoplasty stabilizes fractures, restores lost vertebral height, and reduces deformities.
How it is performed?
Balloon kyphoplasty is performed under local or general anesthesia. Using real-time x-ray two small incisions are made, and a probe is inserted into the vertebral body space. The bone is drilled and balloon/s, called a bone tamp is a pump that is inserted on each side.
These balloons are inflated with contrast medium so the surgeon can see on the real-time x-ray until each balloon expands to the correct height, and then are taken out. The balloon is used to create a space for the bone cement and helps expand the compressed vertebral body bone. The cement binds and stabilizes the fracture. The cement provides:
Strength
Stability
Hardens rapidly
Restores height
Relieves pain
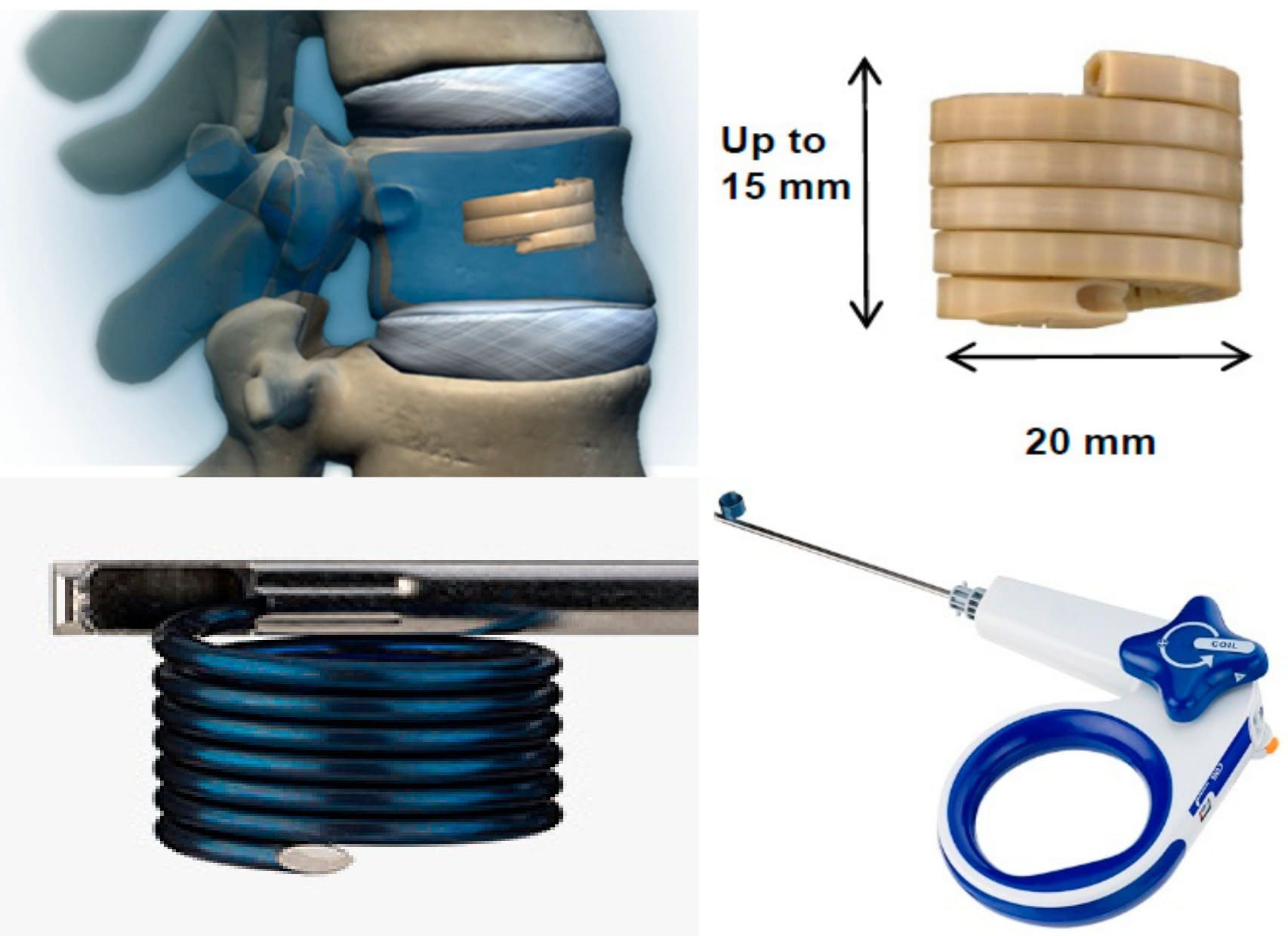
Vertebral augmentation implant
A vertebral augmentation implant is different from vertebroplasty and kyphoplasty. This minimally invasive procedure for middle and lower back spinal compression fractures utilizes a flexible loop spring style spinal implant. It is performed under local or general anesthesia. A real-time x-ray is used to visualize the spinal anatomy and guide the placement of the device. The implant is delivered through a small incision. Once the implant is in place, the bone cement is injected, and the implant is removed.
Potential benefits include:
Reduction of new fractures above or below the existing fracture
Improves the spine’s angle
Reduced spinal deformity
Reduces bone cement leakage
Reduces the amount of bone cement
Benefits of all
Vertebral compression fractures and the limited abilities of traditional surgical options led to the refinement of these surgical systems. Each procedure provides options, as to how the treatment helpsrelieve pain, reduce and stabilize fractures, reduce spinal deformity, and stop the progressive worsening of untreated osteoporosis.
Added benefits:
Surgical time is minimal
Local or general anesthesia is all that is needed
Hospital stay is a day or only a few hours
Patients can quickly return to normal activities
No bracing required
A spine surgeon will explain the purpose and aims of the recommended procedure, including the benefits and risks to help make an informed decision.
Foot Levelers Orthotics Reduce Low Back Pain
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
The importance of Magnetic Resonance Imaging to evaluate the integrity of the lumbar posterior ligament complex post trauma.
Abstract: Posterior ligamentous complex(PLC), consisting of the supraspinous ligament, interspinous ligament, ligamentum flavum, and the facet joint capsules is thought to contribute significantly to the stability of the lumbar spine. There has been much debate on whether Magnetic Resonance Imaging(MRI) is specific and sensitive in diagnosing pathology to the PLC. The objective is to determine the necessity of MRI imaging for evaluating the integrity of the lumbar posterior ligament complex post trauma.
Key Words: Magnetic Resonance Imaging(MRI), interspinous ligament, posterior ligament complex, low back pain, ligament laxity, electromyography, impairment rating
A 41-year-old male, presented to my office for an examination with complaints of low back pain with numbness, tingling and weakness into the left lower extremity after he was the restraint driver in a motor vehicle collision approximately three and a half months� post trauma.�He�rated the pain as a�3/10 on a visual analog scale with 10/10 being the worst and the pain and noted the pain as being�present most of the time.� He stated that he was on pain killers daily and this helped manage his daily activities. Without pain killers his pain levels are rated 8/10 being present most of the time. The pain killers stated by the patient are Oxycodone and Naproxen. He�reported that the pain would be aggravated by activities which required excessive standing, repetitive bending, and lifting. He further noted that in the morning the pain was increased and his left leg would be numb and weak for about the first hour.
The patient stated that his care to date had been managed by a pain management clinic and that he had minimal improvement with treatment which has included physical therapy and massage therapy. He reported the pain clinic next recommended steroid injections which he refused. He states there has been was no imaging ordered and that an Electromyography(EMG) had been performed. He was told the test was negative for pathology.
Prior History: No significant medical history was reported. Clinical Findings:�The patient is 6�0� and weighs 210 lbs.
Physical Exam Findings:
Cervical Spine:
Cervical spine range of motion is full and unrestricted. Maximum cervical compression is negative. Motor and other regional sensory exam are unremarkable at this time.
Thoracic Spine:
Palpation of the thoracic spine region reveals taught and tender fibers in the area of the bilateral upper and mid thoracic musculature. Thoracic spine range of motion is restricted in flexion, extension, bilateral lateral flexion, and bilateral rotation. Regional motor and sensory exam are unremarkable at this time.
Lumbar Spine:
Palpation of the lumbosacral spine region reveals taught and tender fibers in the area of the lumbar paraspinal musculature. Lumbar spine range of motion is limited in flexion, extension, bilateral lateral flexion and bilateral rotation. Extension restriction is due to pain and spasm. Straight leg raise causes pain at approximately 50 degrees when testing either side in the left low back. There is no radicular symptomatology down the leg. Kemp�s maneuver recreates pain in the L4 region on the left. No radicular symptoms are noted. The patient is able to heel and toe walk. Regional motor and sensory exam is unremarkable at this time other than L4, L5 and S1 dermatomes having decreased sensation with light touch.
Muscle testing of the upper and lower extremities was tested at a 5/5 with the exception of the left quadricep tested at a 4/5.� The patient�s deep tendon reflexes of the upper and lower extremities were tested including triceps, biceps, brachioradialis, patella, and Achilles and all were tested at 2+ bilaterally except the left patellar reflex was 1+.
RANGES OF MOTION EVALUATION
All range of motions are based on the�American Medical Association�s Guides to the Evaluation of Permanent Impairment, 5th�Edition1�and performed by a dual inclinometer for the lumbar spine.
�� Range of Motion������Normal�������� Examination�������� % Deficit
Flexion
60
48
20
Extension
25
12
52
Left Lateral Flexion
25
16
36
Right Lateral Flexion
25
18
28
An MRI was ordered to rule out gross pathology.
Imaging:
�
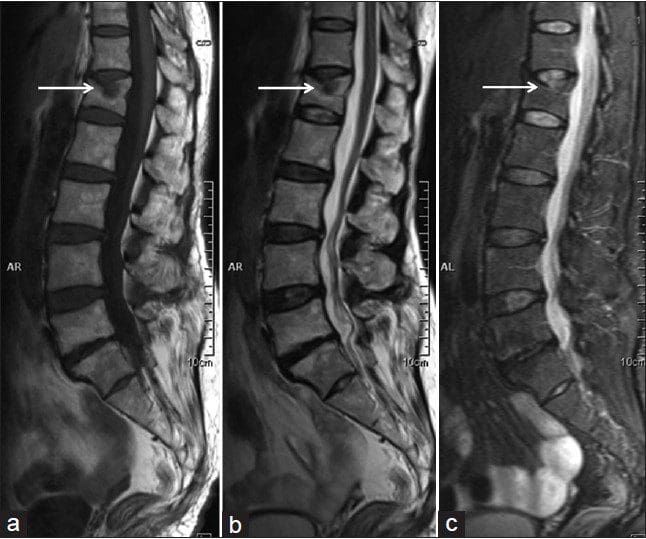
A lumbar MRI reveals;
1)��� Mild disc bulges at T11-T12, T12-L1, L1-L2 and L5-S1
2)��� Low disc signals indicative of disc desiccation at T11-T12, T12-L1, L1-L2, L2-L3, L3-L4 and L4-L5
3)��� Retrolisthesis of 2mm at L3-L4
4)��� Mild ligamentous hypertrophy at L1-L2, L2-L3, L3-L4, L4-L5 and L5-S1
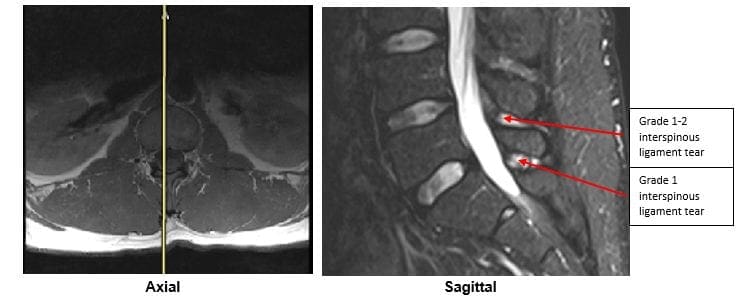
5)��� L4-L5 has a Grade 1-2 tear of the interspinous ligament with mild inflammation
6)��� L5-S1 has a Grade 1 interspinous ligament tear with mild inflammation
After reviewing the MRI I ordered lumbar x-rays to rule out ligament laxity.
X-RAY STUDIES
Lumbar x-rays reveal the following:
1)��� Left lateral tilt
2)��� Retrolisthesis at L1 of 3mm
3)��� Retrolisthesis at L2 of 3mm
4)��� Combined excessive translation of 4mm of L1 during flexion-extension
5)��� Combined excessive translation of 4mm of L2 during flexion-extension
6)��� Excessive translation of L3 in extension posteriorly of 2.5mm
7)��� Decreased disc space at L5-S1
Chiropractic care was initiated. The patient was placed on an initial care plan of 2-3x/week for 3 months and then a recommended break in care for one month so the patient could be evaluated for permanency while he was not care dependent.
At maximum medical improvement, he had continued low back pain rated 4/10, continued numbness and tingling into his left leg and left quadricep weakness rated 4/5. He does not need pain killers for pain management anymore. He continues chiropractic care every two weeks to manage his symptoms.
Conclusion:
In this specific case, pathology to the posterior ligament complex diagnosed on MRI lead to the x-ray finding of excessive translation at L1-L2 and L2-L3. The patient was given a permanent impairment rating of 22% based on my interpretation of the American Medical Association�s Guides to the Evaluation of Permanent Impairment, 5th�Edition1. The interspinous ligament tears at the L4-L5 and L5-S1 level would not have been diagnosed without the MRI.
There has been much debate on whether MRI imaging has a role in evaluating lumbar PLC. MRI is a powerful diagnostic tool that can provide important clinical information regarding the condition of the PLC. Useful sequences for spinal MRI in trauma include sagittal and axial T1-weighted images, T2-weighted FSE, fat-saturated T2-weighted FSE, and STIR sequences to highlight bone edema.2�Ligamentous injuries are best identified on T2-weighted images with fat saturation because the ligaments are thin and bonded on either side by fat, which can appear as hyperintense on both T1 and T2 images.3�T1-weighted images are inadequate in isolation for identifying ligamentous injuries.4�
The diagnostic accuracy for MRI was reported for both supraspinous ligament and interspinous ligament injury with a sensitivity of 89.4% and 98.5%, respectively, and a specificity of 92.3% and 87.2% in 35 patients.5
For patients with persistent symptoms after trauma an MRI may be indicated to evaluate posterior ligamentous complex integrity.
Competing Interests:� There are no competing interests in the writing of this case report.
De-Identification: All of the patient�s data has been removed from this case.
References:
1. Cocchiarella L., Anderson G. Guides to the Evaluation of Permanent Impairment, 5th Edition, Chicago IL, 2001 AMA Press.
2. Cohen, W.A., Giauque, A.P., Hallam, D.K., Linnau, K.F. and Mann, F.A., 2003. Evidence-based approach to use of MR imaging in acute spinal trauma.�European journal of radiology,�48(1), pp.49-60.
3. Terk, M.R., Hume-Neal, M., Fraipont, M., Ahmadi, J. and Colletti, P.M., 1997. Injury of the posterior ligament complex in patients with acute spinal trauma: evaluation by MR imaging.�AJR. American journal of roentgenology,�168(6), pp.1481-1486.
4. Saifuddin, A., Green, R. and White, J., 2003. Magnetic resonance imaging of the cervical ligaments in the absence of trauma.�Spine,�28(15), pp.1686-1691.
5. Haba H, Taneichi H, Kotani Y, et al. Diagnostic accuracy of magnetic resonance imaging for detecting posterior ligamentous complex injury associated with thoracic and lumbar fractures.�J Neurosurg. 2003; 99(1 Suppl):20-26.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine