Chiropractor, Dr. Alexander Jimenez examines the role of biomechanics in medial tibial stress syndrome…
Medial tibial stress syndrome (MTSS � commonly known as shin splints) is not medically serious, yet can suddenly side- line an otherwise healthy athlete. Roughly five percent of all athletic injuries are diagnosed as MTSS(1).
The incidence increases in specific populations, accounting for 13-20% of injuries in runners and up to 35% in military recruits(1,2). MTSS is defined as pain along the posterior-medial border of the lower half of the tibia, which is present during exercise and (usually) diminishes during rest. Athletes identify the lower front half of the leg or shin as the location of discomfort. Palpation along the medial tibia usually reproduces the pain.
Causes Of MTSS
There are two main hypothesized causes for MTSS. The first is that contracting leg�muscles place a repeated strain upon the medial portion of the tibia, inducing periostitis � inflammation of the periosteal outer layer of bone. While the pain of a shin splint is felt along the anterior leg, the muscles that arise from this area are the posterior calf muscles (see figure 1). The tibialis posterior, flexor digitorum longus, and the soleus all arise from the posterior- medial aspect of the proximal half of the tibia. Therefore, the traction force from these muscles on the tibia is unlikely to be the cause of the pain typically felt on the distal portion of the leg.
A variation of this tension theory is that the deep crural fascia (DCF) � the though- connective tissue that surrounds the deep posterior compartment muscles of the leg � pulls excessively on the tibia, again causing trauma to the bone. Researchers at�the University of Honolulu examined a single leg from five male and 11 female adult cadavers. They confirmed that in these specimens, the muscles of the posterior compartment originated above the portion of the leg that is typically painful in MTSS, and the DCF indeed attached along the entire length of the medial tibia(3).
Doctors at the Swedish Medical Centre in Seattle, Washington wondered if, given the anatomy, could the tension from the posterior calf muscles produce a related strain on the tibia at the insertion of the DCF, and thus be the mechanism of injury(4)?
In a descriptive laboratory pilot study of three fresh cadaver specimens, they found that strain at the insertion site of the DCF along the medial tibia progressed linearly as tension increased in the posterior leg muscles. This confirmed that a mechanism for a tension-induced injury at the medial tibia is plausible. However, studies of bone periosteum in MTSS patients have yet to find inflammatory markers consistently enough to confirm the periostitis theory(5).
Tibial Bowing
The second causation theory for MTSS is that repetitive or excessive loading causes a bone-stress reaction in the tibia. The tibia, unable to adequately bear the load, bends during weight bearing. The overload results in micro damage within the bone, and not just along the outer layer. When the repetitive loading outpaces the bone�s ability to repair, localized osteopenia can result. Thus, some consider a tibial stress fracture to be the result of a continuum of bone stress reactions that include MTSS(1).
Magnetic resonance imaging (MRI) of the symptomatic leg often shows bone�marrow edema, periosteal lifting, and areas of increased bony resorption in patients with MTSS(1,5). This supports the bone- stress reaction theory. Magnetic resonance imaging of an athlete with a clinical presentation of MTSS can also help rule out other causes of lower leg pain such as tibial stress fracture, deep posterior compartment syndrome, and popliteal artery entrapment syndrome.
Risk Factors For MTSS
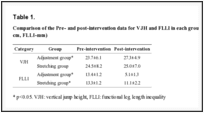
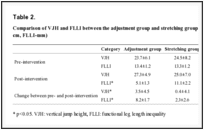
While the aetiology of MTSS is still theoretical, the risk factors for athletes developing it are well determined. A large navicular drop, as determined by the navicular drop test (NDT), significantly correlates with a diagnosis of MTSS(2,5). The NDT measures the difference in height position of the navicular bone, from a neutral subtalar joint position in supported non-weight bearing, to full weight bearing (see figures 2 and 3). The NDT is an indication of the degree of arch collapse during weight bearing. An excursion of more than 10 mm is considered excessive and a significant risk factor for the development of MTSS(5).
Research suggests that athletes with MTSS are found more likely to be female, have a higher BMI, less running experience, and a previous history of MTSS(2,5). Running kinematics for females can differ from males and fit a pattern that is known to leave them vulnerable to anterior cruciate ligament tears and patellofemoral pain syndrome(5). This same biomechanical pattern may also predispose females to MTSS. Hormonal considerations and low bone density are possibly contributing factors in increasing the risk of MTSS in the female athlete as well.
A higher BMI in an athlete likely indicates they have more muscle mass rather than they are overweight. The end result, however, is the same in that the legs bear a significantly heavy load. It is thought that in these instances, the bone growth�stimulated by the tibial bowing may not progress rapidly enough, and injury to the bone occurs. Therefore, those with a higher BMI may need to progress their training programs more slowly, to allow for adaptation.
Those with less running experience are more likely to make training errors (often identified by the athlete) as the catalyst for MTSS. These include increasing distance�too rapidly, changing terrain, overtraining, poor equipment (shoes), etc. Inexperience may also lead the athlete to return to activity too soon, thus accounting for the higher prevalence of MTSS in those who had suffered MTSS previously. Full recovery from MTSS can take anywhere from six to ten months, and if the cause of injury was not rectified or the athlete returns to training too soon, the chances are good the pain will return(5).
Biomechanical Considerations
The NDT is used as a measurable indication of foot pronation. Pronation is a tri-planar movement comprised of eversion at the hind foot, abduction of the forefoot, and dorsiflexion of the ankle. Pronation is a normal movement, and essential in walking and running. When the foot strikes the ground at the initial contact phase of running, the foot begins to pronate and the joints of the foot assume a loose-packed position. This flexibility helps the foot absorb ground reaction forces (see figure 4).
During the loading response phase, the foot further pronates, reaching peak pronation by around 40% of stance phase(6). In mid stance, the foot moves out of pronation and back to a neutral position. During terminal stance, the foot supinates, moving the joints into a closed packed position and creating a rigid lever arm from which to generate the forces for toe off.
Beginning with the loading response phase and throughout the remainder of the single leg stance phase of running, the hip is stabilized, extended, abducted and externally rotated by the concentric contraction of the hip muscles of the stance�leg (the gluteals, piriformis, obturator internus, superior gemellus and inferior gemellus). Weakness or fatigue in any of these muscles can result in internal rotation of the femur, adduction of the knee, internal rotation of the tibia, and over-pronation (see figure 5). Overpronation therefore, can be a result of muscle weakness or fatigue. If this is the case, the athlete may have a quite normal NDT, and yet when the hip muscles don�t function as needed, can overpronate.
In a runner who has significant over pronation, the foot may continue to pronate into mid stance, resulting in a�delayed supination response, and thus less power generation at toe off. The athlete may attempt two biomechanical fixes here that could contribute to the development of MTSS. Firstly, the tibialis posterior will strain to prevent the over pronation. This can add tension to the DCF and strain the medial tibia. Secondly, the gastroc-soleus complex will contract more forcefully at toe off to improve the power generation. Again, the increased force within these muscle groups can theoretically add tension to the medial tibia through the DCF and possibly irritate the periosteum.
Evaluating The Injured Athlete
Knowing that over pronation is one of the leading risk factors for MTSS, start your evaluation at the ground and work your way up. First, perform the NDT, noting if the difference is more than 10mm. Analyze the athlete�s running gait on a treadmill, preferably when the muscles are fatigued, as at the end of a training run. Even with a normal NDT, you may see evidence of over pronation in running (see figure 6).
Next evaluate the knee. Is it adducted? Notice if the hip is level or if either hip is more than 5 degrees from level. These are indications that there is likely weakness at the hip. Traditional muscle testing may not reveal the weakness; therefore, functional muscle testing is required.
Observe the athlete perform a one-legged squat with arms in and arms overhead. Does the hip drop, the knee adduct and the foot pronate? Test the strength of hip abductors in side lying, with hip in neutral, extended, and flexed, keeping the knee straight (see figure 7). Test all three positions with hip rotated in neutral, and at end ranges of external and internal rotation. Test hip extension in prone with the knee straight and bent, in all three positions of hip rotation: external, neutral and internal. The position where you find the weakness is where you should begin strengthening activities.
Treat The kinetic Chain
If there is weakness in the hip, begin by having the athlete perform isometric exercises in the position of weakness. For instance, if you find weakness in hip abduction with extension, then begin isolated isometrics in this position. Not until the muscles consistently fire isometrically in this position for three to five sets of 10 to 20 seconds should you add movement. Once the athlete achieves this level, begin concentric contractions, in that same position, against gravity. Some examples are unilateral bridging and side lying abduction. Eccentric contractions should follow, and then sport specific drills.
Keep in mind if there are other biomechanical compensations, they must also be addressed. If the tibialis posterior is also weak, begin strengthening there. If the calf muscles are tight, initiate a stretching program. Utilise whatever modalities might be helpful. Lastly, consider a stabilising shoe if the ligaments in the foot are over stretched. Using a stabilising shoe for a short time during rehabilitation can�be helpful in cuing the athlete to adopt new movement patterns.
Conclusion
The best way to prevent shin pain from MTSS is to decrease the athlete�s risk factors. Ideally, each athlete should have a basic running gait analysis and proper shoe fitting. Include hip strengthening in functional positions such as unilateral stance as part of the strengthening program. Pair inexperienced athletes with a more experienced mentor to ensure proper training, use of equipment, and investigation of pain at onset. They may be more likely to tell a teammate they are feeling pain than a coach or trainer. Progress the running schedule of heavier athletes more slowly to allow adaptation of the bone. Ensure that athletes fully rehabilitate before returning to play because the chances of recurrence of MTSS are high.
References
1. Am J Sports Med. 2015 Jun;43(6):1538-47
2. Br J Sports Med. 2015 Mar;49(6):362-9
3. Med Sci Sports Exerc. 2009;41(11):1991-1996
4. J Am Podiatr Med Assoc. 2007 Jan;97(1):31-6
5. J Sports Med. 2013;4:229-41
6. Gait and Posture. 1998;7:77�95
Chiropractor, Dr. Alexander Jimenez gives insight into the relevant anatomy and functional biomechanics of the piriformis muscle, highlights the role it plays in musculoskeletal dysfunction and looks at management options in cases of muscle dysfunction.
The piriformis muscle (PM) is well-known in the fraternity of sports medicine as a significant muscle in the posterior hip. It is a muscle that has a role in controlling hip joint rotation and abduction, and it is also a muscle made famous due to its �inversion of action� in rotation. Furthermore, the PM also grabs attention due to its role in the contentious �piriformis syndrome�, a condition implicated as a potential source of pain and dysfunction, not only in the general population but in athletes as well.
Relevant Anatomy
The name piriformis was first coined by Belgian Anatomist Adrian Spigelius in the early 17th century. Its name is derived from the Latin word �pirum� meaning �pear� and �forma� meaning �shape� � ie a pear shaped muscle (see Figure 1)(1).
The PM originates on the anterior surface of the sacrum and is anchored to it by three fleshy attachments between the first, second, third and fourth anterior sacral foramina(2). Occasionally its origin may be so broad that it joins the capsule of the sacroiliac joint above and with the sacrotuberous and/or sacrospinous�ligament below(3,4).
PM is a thick and bulky muscle, and as it passes out of the pelvis through the greater sciatic foramen, it divides the foramen into the suprapiriform and infra-piriform foramina(5). As it courses antero-laterally through the greater sciatic foramen, it tapers out to form a tendon that is attached to the superior-medial surface of the greater trochanter, commonly blending with the common tendon of the obturator internus and gemelli muscles(6).
The nerves and blood vessels in the suprapiriform foramen are the superior gluteal nerve and vessels, and in the infra- piriforma fossa are the inferior gluteal nerves and vessels and the sciatic nerve (SN)(5). Due to its large volume in the greater sciatic foramen, it has the potential to compress the numerous vessels and nerves that exit the pelvis.
PM is closely associated with the other short hip rotators that lie inferior such as the superior gemellus, obturator internus, inferior gemellus and obturator externus(2). The primary difference between the PM and other short rotators is the relationship to the SN. The PM passes posterior to the�nerve whereas the other otators pass anterior (see figure 2).
Variants
A few anatomical variants have been found with the PM:
1. Additional medial attachments to the first and fifth sacral vertebrae and to the coccyx(7).
2. The tendon may fuse with the gluteus medius or minimus above, or superior gemellus below(7).
3. In less than 20% of cases it is divided into two distinct portions through which part or all of the sciatic nerve may pass(7).
4. It may blend with the posterior hip joint capsule as a conjoined tendon with the obturator internus(8).
5. The distal attachment of the PM has shown to vary in dimensions and position on the supero-medial surface of the greater trochanter. It can span a distance of between 25-64% of the anterior-posterior length on the greater trochanter, with 57% attaching more anterior and 43% more posterior(9).
6. Pine et al (2011) studied the insertion point extensively and found that four types of insertion existed and these were classified based on the relationship to the obturator internus(10). The variability in position and breadth of the distal attachment of the PM muscle may influence the validity of the concept known as �inversion of action� (see below).
The other hotly debated issue is the relationship between the PM and the SN. The conclusion is that there are several anatomical variations of the PM and its SN relationship. The sub-types of this variation include(11-13):
Type 1 (A below). Typical pear shape muscle with the nerve running anteriorly and inferiorly to this (in 70%-85% of cases).
Type 2 (B below). The PM is divided into two parts with the common peroneal nerve running between the two parts and the tibial nerve running anterior and below (found in 10-20% of cases).
Type 3 (C below). The peroneal portion loops over the top of the muscle and the tibial portion is below (found in 2-3% of cases).
Type 4 (D below). Undivided nerve passing through the PM (occurs in about 1% of cases).
It is also believed that two other very uncommon variations occur (see E and F below).
Type A is the most common variation, showing the SN passing below the PM
Functional Considerations
The primary functional roles of the PM are;
1. Hip external rotation(15).
2. Abductor at 90 degrees of hip flexion(15).
3. In weight-bearing, the PM restrains the femoral internal rotation during stance phase of walking and running(2).
4. Assists the short hip rotators in compressing the hip joint and stabilising the joint(6).
5. As it can exert an oblique force on the sacrum, it may produce a strong rotary shearing force on the sacroiliac joint (SIJ). This would displace the ipsilateral base of the sacrum anteriorly (forward) and the apex of the sacrum posteriorly(16).
As the PM is the most posterior of the hip external rotators due to its attachment on the anterior surface of the sacrum, it has the greatest leverage to exert a rotation effect on the hip joint. It is often seen clinically that the PM appears to be tight and hypertonic, while the other short hip�rotators that are closer to the axis of rotation become inhibited and hypotonic.
Inversion Of Action
The most contentious issue related to the function of the PM is its �reversal-of- function role� or �inversion of action� role. Many authors have suggested that as the hip approaches angles of 60-90 degrees and greater, the tendon of the PM shifts superiorly on the greater trochanter. As a result, its line of pull renders it ineffective as a hip external rotator; however it does contribute to internal hip rotation. Therefore it reverses its rotation role at high hip flexion angles(15,17,18).
The function of the PM at varying joint angles is an important consideration for the clinician who is evaluating and treating �piriformis syndrome�. Often it has been advocated to stretch the hip into flexion, adduction and external rotation to stretch the PM over the glutes by utilising the �reversal of function� concept.
However, more recent anatomical dissection studies have shown that the attachment of the PM onto the greater trochanter can be variable and in some instances it may insert in a position whereby it is unable to reverse its function, for example in a more posteriorly placed attachment(19). Therefore, stretching the PM into external rotation when the hip is flexed beyond 90 degrees � based upon reversal of function � would be ineffective as a treatment or misleading as an examination technique(19)
MSK Dysfunction & PM Syndrome
Many decades ago, the role that the PM played in creating sciatic-like symptoms was first suggested by Yeoman (1928) when it was considered that some cases of sciatica may originate outside the spine(20). This was supported soon after when Freiberg and Vinkle (1934) successfully cured sciatica by surgically dividing the PM(21). Based on cadaver dissections Beaton and Anson (1938) gave the hypothesis that the spasm of the PM could be responsible for the irritation of the SN(12).
The term �piriformis syndrome� was first coined by Robinson in 1947(22) and was applied to sciatica thought to be caused by an abnormality in the PM (usually traumatic in origin) with emphasis on ruling out more common causes of sciatica such as nerve root impingement from a disc protrusion. It soon became an accepted clinical entity � but with no consensus about the exact clinical signs and diagnostic tests to differentiate it from other sources of sciatica(23,24).
Piriformis syndrome can be defined as a clinical entity whereby the interaction�between the PM and SN may irritate the SN and produce posterior hip pain with distal referral down the posterior thigh, imitating �true sciatica�. Isolating the dysfunction to this region usually follows exclusion of the more common causes of buttock pain and sciatica.
More specifically, complaints of buttock pain with distal referral of symptoms are not unique to the PM. Similar symptoms are prevalent with the more clinically evident lower back pain syndromes and pelvic dysfunctions. Thus, a thorough evaluation of these regions must be performed to exclude underlying pathology(4). It has been suggested that piriformis syndrome� is responsible for 5-6% of cases of sciatica(25,26). In the majority of cases, it occurs in middle-aged patients (mean age 38 yr)(27) and is more prevalent in women(28).
Pathogenesis Of Piriformis Syndrome (PS)
PS may be caused by or relate to three primary causative factors;
1. Referred pain due to myofascial trigger points (see Figure 4)(2,28-30). Examples include tight and shortened muscle fibres precipitated by muscle overuse such as squat and lunge movements in external rotation, or�direct trauma(16). This increases the girth of the PM during contraction, and this may the source of the compression/entrapment.
2. Entrapment of the nerve against the greater sciatic foramen as it passes through the infrapiriform fossa, or within a variant PM(29,31).
3. SIJ dysfunction causing PM spasm(29,32).
Janvokic (2013) has presented a number of causative factors in PS(29);
1. Gluteal trauma in the sacroiliac or gluteal areas.
2. Anatomical variations.
3. Myofascial trigger points.
4. Hypertrophy of the PM or spasm of the PM.
5. Secondary to spinal surgery such as laminectomy.
6. Space occupying lesions such as neoplasm, bursitis, abscess, myositis. 7. Intragluteal injections.
8. Femoral nailing.
Symptoms
Typical symptoms reported in piriformis syndrome include:
A tight or cramping sensation in the buttock and/or hamstring(33).
Gluteal pain (in 98% of cases)(34).
Calf pain (in 59% of cases)(34).
Aggravation through sitting and squatting(35), especially if the trunk is inclined forward or the leg is crossed over the unaffected leg(36).
Possible peripheral nerve signs such as pain and paraesthesia in the back, groin, buttocks, perineum, back of the thigh (in 82% of cases)(34).
Physical Findings & Examinations
Palpable spasm in and around the PM and obturator internus and external tenderness over the greater sciatic notch (in 59-92% of cases)(34,35). The patient is placed in the Sims position. The piriformis line overlies the superior border of the PM and extends from immediately above the greater trochanter to the cephalic border of the greater sciatic foramen at the sacrum. The line is divided into equal thirds. The fully rendered thumb presses on the point of maximum trigger-point tenderness, which is usually found just lateral to the junction of the middle and last thirds of the line.
Hip flexion with active external rotation or passive internal rotation may exacerbate the symptoms(36).
Positive SLR that is less than 15 degrees the normal side(37).
Positive Freiberg�s sign (in 32-63% of cases)(34,35). This test involves reproducing pain on passive forced internal rotation of the hip in the supine position � thought to result from passive stretching of the PM and pressure on the sciatic nerve at the sacrospinous ligament.
Pacers sign (in 30-74% of cases)(34,35). This test involves reproducing pain and weakness on resisted abduction and external rotation of the thigh in a sitting position.
Pain in a FAIR position(34). This involves the reproduction of pain when the leg is held in flexion, adduction and internal rotation.
An accentuated lumbar lordosis and hip flexor tightness predisposes one to increased compression of the sciatic nerve against the sciatic notch by a shortened piriformis(38).
Electro-diagnostic tests may prove useful (see below).
Investigations
Conventional imaging such as X-ray, CT scan and MRI tend to be ineffective in diagnosing piriformis syndrome.
However, some value may exist in electro- diagnostic testing.
It is beyond the scope of this paper to discuss in detail the process of electro- diagnostic testing; the reader is directed to references for more a more detailed description of how these tests are administered(35,36,39). However the purpose of these tests is to find conduction faults in the SN. Findings such as long-latency potentials (for example the H reflex of the tibial nerve and/or peroneal nerve) may be normal at rest but become delayed in positions where the hip external rotators are tightened(27,36,39).
It is accepted that the tibial division of the SN is usually spared, the inferior gluteal nerve that supplies the gluteus maximus may be affected and the muscle becomes atrophied(40). However testing of the peroneal nerve may provide more conclusive results as is more likely to be the�impinged portion of the SN. The H-wave may become extinct during the painful position of forced adduction-internal rotation of the affected leg(36).
The �Myth� Of Piriformis Syndrome
Stewart 2003 argues that piriformis syndrome is an often over-used term to describe any non-specific gluteal tenderness with radiating leg pain(41). He argues that only in rare cases is the PM implicated in nerve compression of the SN to truly qualify as a piriformis syndrome. He cites only limited evidence and cases where the diagnosis of piriformis syndrome can be made.
1. Compressive damage to the SN by the PM. Stewart cites studies whereby in few isolated studies, the SN was seen to be compressed by the PM in instances such as hypertrophy of the muscle,�usual anatomical anomalies such as a bifid PM, and due to compression by fibrous bands.
2. Trauma and scarring to the PM leading to SN involvement; it is possible that rare cases of true Piriformis Syndrome have been caused by direct heavy trauma to the PM due to a blunt trauma to the muscle. This is termed �post- traumatic PS�.
McCory (2001) supports this argument by stating that it is more likely that (given the anatomical relationship of the PM to the various nerves in the deep gluteal region) the buttock pain represents entrapment of the gluteal nerves, and the hamstring pain entrapment of the posterior cutaneous nerve of the thigh, rather than the SN alone(33). This would explain the clinically observed phenomenon in the absence of distal sciatic neurological signs. Whether the PM is the cause of the compression has not been clearly established. It is possible that the obturator internus/gemelli complex is an alternative cause of neural compression. He suggests using the term �deep gluteal syndrome� rather than piriformis syndrome.
Treatment
When it is believed that a piriformis syndrome exists and the clinician feels that a diagnosis has been made, the treatment will usually depend on the suspected cause. If the PM is tight and in spasm then initially conservative treatment will focus on stretching and massaging the tight muscle to remove the PM as being the source of the pain. If this fails, then the following have been suggested and may be attempted(23,36):
Local anaesthetic block � usually performed by anaesthesiologists who have expertise in pain management and in performing nerve blocks.
Steroid injections into the PM.
Botulinum toxin injections into the PM.
Surgical Neurolysis.
Here, we will focus on therapist-directed interventions such as stretching of the PM and direct trigger point massage. It has always been advocated that PM stretches are done in positions of hip flexion greater than 90 degrees, adduction and external rotation to utilize the �inversion of action� effect of the PM to isolate the stretch to this muscle independent of the other hip external rotators.
However, recent evidence from Waldner (2015) using ultrasound investigation discovered that there was no interaction between hip flexion angle and the thickness of the PM tendon in both internal and lateral hip rotation stretching � suggesting that the PM does not invert its action(19). Furthermore, Pine et al (2011)(9) and Fabrizio et al (2011)(10) in their cadaveric studies found that the PM insertion is a lot more complex and varied than first thought. It is possible that the PM may invert its action only in some subjects but not others.
Therefore, due to the disagreements and confusions over the �inversion of action� concept, it is recommended that the clinician �covers all bases� and performs two variations of a PM stretch � stretches in flexion, adduction and external rotation and stretches in flexion, adduction and internal rotation. Examples of these stretches are given in figures 5-7 below.
Trigger Points & Massage
(see Figure 8)
The best approach to palpate the PM trigger points is in the position suggested by Travel and Simons(2) and this is shown below. In this position, the clinician can feel for the deep PM trigger points and apply a sustained pressure to alleviate the trigger�points � and also apply a flush massage to the muscle in this position.�In this position the large gluteus maximus is relaxed and it is easier to feel the deeper PM.
Summary
The PM is a deep posterior hip muscle that is closely related anatomically to both the sacroiliac joint and the sciatic nerve. It is a hip external rotator at hip flexion angles of neutral to 60 degrees of hip flexion, an abductor when in flexion and also contributes to hip extension.
It has been previously accepted that the PM will �invert its action� or �reverse its function� after 60 degrees of flexion to become a hip internal rotator. However, recent ultrasound and cadaveric studies has found conflicting evidence that this �inversion of action� may in fact not exist.
PM is a muscle that is a dominant hip rotator and stabiliser, and thus has a tendency to shorten and become hypertonic. Therefore, stretching and massage techniques are best utilised to reduce the tone through the muscle. Furthermore, it has also been implicated in compression and irritation of the sciatic nerve � often referred to as piriformis syndrome�.
References
1. Contemp Orthop 6:92-96, 1983.
2. Simons et al (1999) Travell and Simons� Myofascial Pain and Dysfunction. Volume 1 Upper Half of the Body (2nd edition). Williams and Wilkins. Baltimore.
3. Anesthesiology; 98: 1442-8, 2003.
4. Joumal of Athletic Training 27(2); 102-110, 1996.
5. Journal of Clinical and Diagnostic Research. Mar, Vol-8(3): 96-97, 2014.
6. Clemente CD: Gray�s Anatomy of the Human Body, American Ed. 30. Lea & Febiger, Philadelphia, 1985 (pp. 568-571).
7. Med J Malaysia 36:227-229, 1981.
8. J Bone Joint Surg;92-B(9):1317-1324, 2010.
9. J Ortho Sports Phys Ther. 2011;41(1):A84, 2011.
10. Clin Anat;24:70-76, 2011.
11. Med Sci Monit, 2015; 21: 3760-3768, 2015.
12. J Bone Joint Surg Am 1938, 20:686-688,1938.
13. Journal of Clinical and Diagnostic Research. 2014 Aug, Vol-8(8): 7-9, 2014.
14. Peng PH. Piriformis syndrome. In: Peng PH, editor. Ultrasound for Pain Medicine Intervention: A Practical Guide. Volume 2. Pelvic Pain. Philip Peng Educational Series. 1st ed. iBook, CA: Apple Inc.; 2013 .
15. Kapandji IA. The Physiology of Joints. 2nd ed. London: Churchill Livingstone; 1970: 68.
16. J Am Osteopath Assoc 73:799-80 7,1974.
17. J Biomechanics. 1999;32:493-50, 1999.
18. Phys Therap. 66(3):351-361, 1986.
19. Journal of Student Physical Therapy Research. 8(4), Article 2 110-122, 2015.
20. Lancet. 212: 1119-23, 1928.
21. J Bone Joint Surg Am 16:126�136, 1934.
22. Am J Surg 1947, 73:356-358, 1947.
23. J Neurol Sci; 39: 577�83, 2012.
24. Orthop Clin North Am; 35: 65-71, 2004
25. Arch Phys Med Rehabil; 83: 295-301,2002.
26. Arch Neurol. 63: 1469�72, 2006.
27. J Bone Joint Surg Am; 81: 941-9,1999.
28. Postgrad Med 58:107-113, 1975.
29. Can J Anesth/J Can Anesth;60:1003�1012, 2013.
30. Arch Phys Med Rehabil 69:784, 1988.
31. Muscle Nerve; 40: 10-8, 2009.
32. J Orthop Sports Phys Ther;40(2):103-111, 2010.
33. Br J Sports Med;35:209�211, 2001.
34. Man Ther 2006; 10: 159-69, 2006.
35. Eur Spine J. 19:2095�2109, 2010.
36. Journal of Orthopaedic Surgery and Research, 5:3, 2010.
37. Muscle & Nerve. November. 646-649, 2003.
38. Kopell H, Thomnpson W. Peripheral Entrapment Neuropathies. Huntington, NY: Krieger, 1975:66.
39. Arch Phys Med Rehabil;73:359�64, 1992.
40. J Bone and Joint Surg, 74-A:1553-1559, 1992.
41. Muscle & Nerve. November. 644-646, 2003
With the competitive season looming, chiropractor Dr. Alexander Jimenez�gives insights & examines the current best thinking on vaccination for athletes, and makes recommendations for sports clinicians.
Without doubt, vaccination is one of the greatest triumphs of modern medicine. Many serious diseases that used to routinely maim or kill large numbers of people are no longer a threat. More than that, vaccination can prevent outbreaks of less serious illness, which although not life threatening, are still unpleasant, leading to missed time from work and school.
Anyone with young children or who has travelled extensively abroad will (hopefully) understand that a programme of vaccination is either required or recommended. When it comes to the travelling athlete however, the situation is rather more complex. While the basic vaccinations (eg typhoid, hepatitis etc when travelling to certain regions of the tropics) are of course still required, clinicians will also want to ensure that their athletes stay as well as possible to compete at their full potential. A mild illness that is an inconvenience to a tourist may be a disaster for an athlete focusing on the peak of his/her season!
Sports clinicians may therefore wish to consider extra vaccinations to minimise the risk of more minor conditions. However, this approach raises a whole new set of issues. For example, which additional vaccinations may be use for athletes who regularly travel abroad? What are the possible side effects of these extra vaccinations and how should vaccines be timed to maximise immunity during the competition, while minimising disruption to training in the run up to competition?
Athletes Are Different
There exists some uncertainty about the most appropriate vaccination regimens in athletes among team doctors and other physicians because general public health vaccination guidelines cannot be easily transferred to elite athletes. Complicating factors include the typical circumstances of athletes� daily life, such as frequent travelling to foreign countries or close contact with teammates and opponents, which might indicate the need for a modification of recommended vaccination schedules. In addition, intense physical activity of training and competition with its possible effects on the immune function can affect decisions about execution and timing of vaccination.
Other complicating factors are that vaccination recommendations are formulated around a public health policy rather than for specific individuals and are likely to change over time(1-3). Also, there�s the issue of cost effectiveness; the majority of vaccines that are not generally recommended are not recommended because the medical benefit is not regarded sufficiently balanced with the costs if implemented across the whole population. This is despite the fact that they may be potentially beneficial in specific individuals(4,5). It�s also important to understand that generalised recommendations take no account of the implications of the effects of illness in athletes, which can be far more profound and far reaching than in the general public (see Box 1).
Further reasons as to why athletes are different when it comes to vaccination include the following:
Athletes are often in close contact with opponents and teammates, which increases the risk of transmission of many diseases, particularly respiratory- transmitted diseases(9,10). Typically, a contact of less than 1-2 metres distance is necessary to transmit diseases such as influenza or other respiratory- transmissible agents such as varicella(11,12).
For blood-borne diseases, the transmission risk due to sport is less pronounced but athletes are still at higher risk than the general population(13,14).
Even healthy non-vaccinated athletes being exposed to an infectious agent (eg contact with a diseased individual) may have to be excluded from training and competition for medical reasons. Usually, such an exclusion has to last for the complete incubation period of a disease, which may be up to three weeks.
Putting all these factors together, the recommendation is that elite, competitive athletes should be vaccinated more aggressively than the general public(15).
Which Vaccinations?
The decision as to which vaccinations are given prior to foreign travel will depend on a number of factors, including the travel�destination(s), the nature of the sport and the health/vaccination history of the individual involved. Regardless of these factors however, it is recommended that ALL adult athletes are routinely vaccinated against the following:
4. Influenza
5. Hepatitis A and B
6. Measles, mumps and varicella (if immunity is not already proven by a natural infection)
Of these, numbers 1-5 should be given as inactivated vaccines while measles, mumps and varicella (chickenpox) should be given as live vaccines(15). A full discussion on the detailed considerations regarding each and every possible vaccination is beyond the scope of this article (readers are directed to a full and recent review of this topic by Luke and D�Hemecourt(15)). However, Table 1 summarises most of the key recommendations.
Vaccination Timing
Timing of vaccinations should be chosen in order to minimise interference with training and competition, and to ensure the immune reaction is not temporarily impaired. Inactivated vaccines generally cause side effects within two days following vaccination. This is in contrast to live vaccinations where the peak of side effects is most likely to occur after 10-14 days when replication of the vaccines is at a maximum. Unless a vaccination needs to be administered urgently, the best time therefore for vaccination is at the onset of resting periods � for example at the beginning of the winter off season.
When a vaccination has to be carried out within a training and/or competition period (eg influenza), there is no major medical problem with training undertaken shortly before or after vaccination. However, it is recommended to vaccinate shortly after a competition in order to make the period of time to the next competition as long as possible. Many vaccinations given via injection can cause local pain and inflammation at the injection site. Clinicians may therefore wish to time vaccine administration so as to not coincide with delayed onset muscle soreness (DOMS) following strenuous exercise.
Vaccination Techniques
Dependent on the injection site, some sport- specific impairments may result (for example buttock pain in runners following a gluteal injection). Obviously, it is advisable to use the non-dominant side for injections in unilateral disciplines such as racquet sports. For vaccines that can be administered using either the intramuscular or the subcutaneous route, the intramuscular option seems to be preferable as it yields higher titer rate (more antibody production) and a lower risk of granuloma.
Injection into the deltoid muscle is preferred if possible, although other muscle sites are possible. Regardless, it is important that the athlete is sitting or lying, and the muscle is completely relaxed. Studies indicate that the use of longer needles (25 mm) and a fast speed of injection/ withdrawal of the needle (1-2 seconds) are associated with less pain(37). Also, an angle of injection of 90 degrees may also help reduce pain in intramuscular injections.
Syncopes or collapses following vaccination are uncommon but may occur; some studies on influenza vaccination suggest the frequency of syncope in younger athletes to be around 1%(38). However, the syncope itself may be less important than secondary injuries caused by the collapse such as skull fracture and cerebral haemorrhage. Given that the majority of syncopes (80 %) occur within 15 min of vaccine administration, it is recommended that athletes are observed for a period of 15-30 minutes following vaccination. This recommendation may be particularly important for endurance athletes because there are indications that, in these athletes, vasovagally-induced syncopes are more frequent(39).
Vaccination Schedule
The recommended vaccination schedules for disease prevention will be dependent on the previous vaccination record and disease history of the athlete in question. Also, some schedules are dependent of the type/brand of vaccines used and recommendations may also differ according to public health policy in each country. Readers are directed to the summary given by Luke and D�Hemecour(15); there are also some excellent downloadable resources on the US Centre for Disease Control and Prevention (CDC) � https://www.cdc.gov/vaccines/ schedules/hcp/adult.html.
Summary
The vaccination requirements for elite athletes are not the same as that for the general public. Not only are these athletes�potentially exposed to more disease pathogens as a result of international travel, even the mildest episode of illness that would be barely noticeable to most of us can be devastating for elite athletic performance. For these reasons, sports clinicians and doctors should take a much more aggressive approach to vaccination of their athletes. Together with steps to reduce exposure and the correct vaccination techniques and timing, clinicians can maximise the potential of their athletes to perform at all times of year across all regions of the globe.
References
1. World Health Organization. WHO vaccinepreventable
diseases: monitoring system. 2012
global summary 2013. http://www.who.int/
immunization_monitoring/data/data_subject/
en/index.html accessed 5th Feb 2017
2. Sta�ndige Impfkommission (STIKO).
Empfehlungen der Sta�ndigen Impfkommission
(STIKO) am Robert Koch-Institut. Epi Bull.
2012;283�10
3. Centers for Disease Control and Prevention.
General recommendations on immunization�
recommendations of the Advisory Committee
on Immunization Practices (ACIP). MMWR
Recomm Rep. 2011;60:1�64
4. Vaccine. 2013;31:6046�9
5. Pharmacoeconomics. 2005;23:855�74
6. J Exp Med. 1970;131:1121�36
7. Am Heart J. 1989;117:1298�302
8. Eur J Epidemiol. 1989;5:348�50
9. Clin J Sport Med. 2011;21:67�70
10. Sports Med. 1997;24:1�7
11. J Infect Dis. 2013;207:1037�46
12. Lancet. 1990;336:1315
13. Br J Sports Med. 2004;38:678�84
14. Clin Sports Med. 2007;26:425�31.
15. Sports Med 2014; 44:1361�1376
16. Vector Borne Zoonotic Dis 2004;4(1):61�70
17. http://www.nhs.uk/Conditions/Lymedisease/Pages/Introduction.aspx#symptoms accessed Feb 2017
18. J Infect Dis 1999;180(3):900�3
19. Ann N Y Acad Sci 2003;990: 295�30
20. J Infect Dis 1984;150(4):480�8
21. N Engl J Med 2001;345(2):79�84
22. Pediatrics. 2013;131:e1716�22.
23. Euro Surveill. 2005;10(6):E050609.2
24. Euro Surveill. 2013;18(7):20467
25. Centers for Disease Control and
Prevention. Epidemiology and prevention of
vaccine-preventable diseases. The pink
book:course textbook. 12th ed.; 2012.
26. World Health Organisation. Poliomyelitis;
2014. http://www.who.int/topics/poliomyelitis/en/
27. Clin Exp Rheumatol. 2001;19:724�6
28. JAMA. 1997;278:551�6
29. Clin Infect Dis. 2004;38:771�9
30. Travel Med. 1998;5:14�7
31. Cochrane Database Syst Rev.
2014;1:CD001261
32. Curr Opin Infect Dis. 2012;25:489�99
33. Drugs. 2013;73:1147�55
34. Hum Vaccin Immunother. 2014;10:995�1007
35. Popul Health Metr. 2013;11:17.
36. Vaccine. 2009;27(Suppl 2):B51�63
37. Arch Dis Child. 2007;92:1105�8
38. Vaccine. 2013;31:6107�12
39. Prog Cardiovasc Dis. 2012;54:438�44
El Paso, TX. Chiropractor Dr. Alex Jimenez discusses student-athletes and injuries.
Most injuries to student-athletes occur during routine practices, but only about a third of public high schools have a full-time trainer, according to the U.S.-based National Athletic Trainers’ Association (NATA).
“It’s important to have the right sports safety protocols in place to ensure the health and welfare of student athletes,” said Larry Cooper, chairman of NATA’s secondary school committee. “By properly preparing for practices and competitions, young athletes can excel on the field and stay off the sidelines with potential injuries.”
As Spring Season Approaches NATA Recommends Parents & Students Review Their Schools Policies On Sports Injuries
Here’s what to consider:
Who handles sports-related injuries? Know who will care for athletes who are hurt during practice. Consider that person’s experience and credentials, including first aid and medical training. Determine who makes medical decisions. Coaches and athletes may not make objective decisions about injuries and safety if they are concerned about winning.
What’s the emergency action plan? Every team should have a written plan detailing what to do if a serious injury occurs. An athletic trainer or first responder should review this plan.
Is all equipment in good working condition? Sports equipment such as field goals, turf, basketball flooring and gymnastics apparatus should be examined to make sure it’s safe. Medical equipment such as splints and spine boards should be checked routinely. Schools should have an automated external defibrillator (AED) and staff trained in its use.
Are high school coaches qualified? All coaches, assistant coaches and team volunteers should undergo a background check. They should have knowledge in the sport they are coaching and all credentials required by the state and athletic conference or league. Coaches should be trained to administer CPR, use an AED and provide first aid.
Are locker rooms and gyms sanitary? These areas should be cleaned routinely to prevent the spread of bacterial, viral and fungal skin infections. Athletes should never share towels, athletic gear, water bottles, razors and hair clippers.
NATA says parents should also help ensure their teens are both mentally and physically prepared to play sports. This includes a preseason physical to identify any health conditions that could limit their participation. Young athletes shouldn’t be pushed or forced to participate. Parents should make sure their child’s school, coaches and other staff have a copy of his or her medical history as well as a completed emergency medical authorization form.
NATA recommends parents, student-athletes and coaches keep these safety tips in mind when spring training begins:
Acclimate gradually. Athletes playing in hot weather should build up their endurance over one to two weeks. During this time, they should stay well hydrated and adjust their exercises according to weather. Athletes who must wear heavy protective equipment should gradually get used to playing in their gear. For example: wear only helmets on days one and two; then helmets and shoulder pads on days three and four, then full gear by day five.
Be aware of concussions. Student-athletes, coaches and school medical staff must be well educated on concussion prevention and management. Students with head injuries should speak up if they experience symptoms such as dizziness, loss of memory, lightheadedness, fatigue or trouble with balance.
Screen for sickle cell. All newborns are tested for this inherited trait that can lead to blockage of blood vessels during intense exertion. Athletes with sickle cell trait should take precautions. Warning signs include fatigue or shortness of breath.
Allow for recovery time. The body needs to rest between seasons. Incorporating recovery time into the year can help prevent injuries. Repetitive motions can put excessive stress on joints, muscles or ligaments, resulting in injuries from overuse.
“It’s critical that all members of a school’s sports medicine team (athletic trainers, physicians and school nurses) work together to help prevent, manage and treat injuries or illnesses should one occur,” Cooper said in a NATA news release. “With a team approach we can reduce acute, chronic or catastrophic injury and ensure a successful season all around.”
News stories are written and provided by HealthDay and do not reflect federal policy, the views of MedlinePlus, the National Library of Medicine, the National Institutes of Health, or the U.S. Department of Health and Human Services.
Do you have a muscle imbalance? Muscle imbalances occur when one side of opposing muscles is stronger than the other. Many exercise enthusiasts may be getting chronic injuries because of muscle imbalances they don�t know they have. According to renowned physical therapist Dr. Kareem Samhouri, locating and correcting muscle imbalances is essential to good health, and can help cure many of the ailments people encounter daily.
Dr. Kareem is a doctor of Physical Therapy & Kinesiology and owner of Dr. Kareem F Samhouri Fitness LLC. In his practice, Dr. Kareem has rehabilitated and trained a wide variety of patients seeking help for an assortment health issues:
Improved athletic performance in Olympic and professional athletes
Joint pain in baby boomers
Balance issues in older patients
Coma victims
Spinal cord injuries
Rare diseases
Heart issues
Lung disease
Pregnancy
Stroke victims
Health issues among children and infants
How To Fix Muscle Imbalance
Dr. Kareem has had many amazing success stories throughout his medical career. One of his favorite patients is a 112 year old women who was wheelchair bound:
�She had very little strength or coordination, but had a great spirit and was willing to work hard. The mission was to reactivate her muscles and nervous system, so we started with simple exercises such as simply lifting one foot and putting it back down.
�Once she was able to do that, we focused on squeezing her knees together and moving them apart. In the beginning she needed assistance, but over time, she was lifting her knees, rotating her shoulders and pulling herself out of her chair with little assistance.
�When she was finally able to lift herself out of the chair without help, she asked me �is there any way I can dance?� The music was turned up and after a little help, she was able to dance for the first time in years!�
Another highlight of Dr. Kareem�s career was helping save the life of a four-day old baby who was born 18 weeks prematurely. This baby was the youngest baby ever born at that hospital and doctors didn�t think this baby was going to survive.
What Dr. Kareem did was to put the baby in different positions:
�Instead of it cringing into fetal position because of all the noises, and sirens, and bells, and whistles going off in the hospital, we opened him up and let his chest breathe a little bit. We moved the baby�s arms in diagonal patterns so he could actually get more breath. We also put a little pressure on the diaphragm so the baby could take deeper breaths, then took the pressure off as the belly would expand and contract.
�All of these factors led towards the baby really just developing a little bit more easily and a little bit faster. Of course, in an infant that�s that young, you really just have to be as gentle as can be. Oftentimes, instead of a hand, it�s just barely a fingertip touch that you�re going to do. When it came to actually moving the baby�s muscles, light, little taps in the areas where the nerve ties into the muscle to say, �Hey, right here.�
�Sure enough, baby got better, grew up totally healthy, and ended up living a healthy life.�
When Dr. Kareem consults with his clients, he shares his philosophy on health: �Your body is designed to heal or decay. From now on, decide on your own health momentum. Regain control while you begin to look and feel years younger.�
Dr. Kareem started on his health journey by simply wanting to help his mother with her health issues, but soon discovered he had health issues of his own. After close scrutiny, he was able to determine that his ailments were due to a muscle imbalance, and they were all alleviated by simply straightening out his posture. He eventually graduated from Pennsylvania State University College of Medicine and became a physical therapist. Shortly thereafter, he added personal training to his resume, opening the world�s first clinic where these practices were taught all under one roof. Dr. Kareem believes the body is meant to move, and the key to good health is getting it to move correctly.
This is the basis of muscle balance therapy, and it is designed to assist the body with the following health issues:
Alleviating pain
Faster healing
Improved mood
Improved posture
Increased athleticism
Greater quality of life
� Causes of Common Muscle Imbalance
There are many causes of muscle imbalance, following are the most common:
Improper Exercise When it comes to traditional exercise, many of us tend to exercise in a one or two-dimensional way, which is primarily comprised of movements that are either forwards and/or backwards. For example, the bench press and running are two exercises that are extremely popular, but they can cause muscle imbalances if other complementary exercises are not included in the workout regimen.
In many cases, muscle imbalances mean that the larger muscles are becoming stronger at a faster rate than the smaller muscles. According to Dr. Kareem, the issues caused by muscle imbalance affects more than the disturbed area and may cause a domino effect. For example, if a person has a rotator cuff imbalance, the nerve signal that shuts down the muscle is turned on. When a muscle gets shut down, not only does it stop a person from being able to move the way they want, but it slows down their metabolism as well. This can make a person less effective at many other things, which could eventually affect their mood.
Even as adults, we are meant to play. Our bodies are designed to move in every possible direction. That�s how you would naturally hit all the different muscles. Unfortunately, many of us don�t play. We go to a gym and try to simulate the movements, yet we�re missing different diagonals, rotations, and areas that would be balanced by real life dynamic movement. Repetitive workout routines can create muscle imbalances that wreck our bodies over time.
Moreover, imbalances can lead to injury. For some exercise enthusiasts who are getting chronic injuries, it may be from an underlying muscle imbalance. A person can be big and strong in certain areas, but his smaller stabilizer muscles are not being used. As a result, the body is thrown out of balance, oftentimes creating a functional problem.
Muscle imbalances can affect people of all ages. Kids can experience overuse injuries very quickly, making them less capable of excelling in a sport. In adults of all fitness levels, muscle imbalances can have a negative impact on performance; they�ll be slower, less coordinated, and unable to learn new movements quickly. In older individuals, muscle imbalances can result in decreased coordination, decreased strength and joint pain. Many times, the pain seems to have come out of nowhere or flares up suddenly, but in reality, it was based on a long history of improper movement.
Sedentary Lifestyle
The human body was made to move, not sit at a desk or in front of the television for an extended period of time. Excess sitting can cause muscles to become tight and eventually shorter than they are designed to be. The dangers associated with the sedentary lifestyle are well documented. According to data from the National Center on Health, Physical Activity and Disability (NCHPAD)1
Sedentary people have the highest rate of heart attacks.
For every 2 hours a person watches television, their risk of Type 2 diabetes�increases 14%
Sedentary individuals have an increased risk of breast and colon cancer.
The risk of stroke is reduced by two-thirds in physically active men and women by 50%.
Bone loss�increases in physically inactive individuals.
Walking for sixty minutes daily can reduce a person�s risk of obesity by 24%.
A Weak Core
A strong core helps keeps the muscles and internal organs properly aligned. A weak core can cause slouching, which can lead to poor posture, which could lead to muscle imbalances. These imbalances in the core can lead to health issues such as constipation, acid reflux, and other issues.
Common Muscle Imbalance Areas
Muscle imbalances can happen throughout the body. Some of the most common imbalances include the following:
Neck flexors.�A person�s neck flexors actually end up quite stretched, while their neck extensors become compressed. This often occurs if a person is right handed and they�re always writing with their right hand, typing in a specific way, reaching for a mouse or a stapler, or just rotating their spine in a very specific pattern and shoulder in the same manner over and over again.
Tight hip flexors. Tight hip flexors are caused by sitting for extended periods of time. The human body was not designed to sit as long and as often as we do, and the result is the hip flexors become shortened. This in turn causes the pelvis to rotate or tilt downward, causing the glutes to become lengthened and weak. This will put more pressure on the hamstrings, increasing the risk of hamstring tears, strains and pulls.
Weak upper back. Another common problem is forward shoulder posture, or �upper crossed syndrome.� This is common among individuals who spend long hours in front of a computer. The head goes forward, and as people make that adjustment, chin comes up, which causes an additional strain. Another cause of the upper back imbalance is performing �pushing� exercises such as pushups and bench presses, but not doing any �pulling� exercises for the back such as bent over rows or pulldowns.
As a result of these imbalances, the trapezius and rhomboid muscles become lengthened and weak, while the pectoral muscles and anterior deltoids become tight.
Tight calves. Women who wear high heels increase their probability of having tight calves. The soleus, gastrocnemius, peroneal, and other muscles in the lower leg become tight. This muscle imbalance can lead to different foot, heel, and ankle problems such as plantar fasciitis and fallen arches.
Tight Piriformis. The piriformis is muscle in the glutes which is also part of the external rotator in the hip. A tight piriformis occurs more often in men than women because men tend to sit with their legs open more often than women. Individuals with a tight piriformis often have knee problems, while others may experience problems with sciatica, which is shooting pain from the glutes to the back of the legs.
Tight abductors. Tight abductors usually occur in women because they tend to sit with their legs crossed. If a person has tight abductors, the femur may become internally rotated, which increases the probability of knee pain.
Muscle imbalance can occur in many different ways. Not only is It important to be aware of their causes, but it�s also important to know the various ways they can harm the body.
Call Today!
Dangers of Muscle Imbalance
Many people are unaware how muscle imbalances can affect their overall health. Oftentimes, I would explain to my clients how �structure affects function.� I would show them an x-ray so they can see how an imbalance could erode their discs early and cause injury. However, it was a challenge for me to get them to understand how that affects their immune system.
Dr. Kareem explains the dangers of muscle imbalance by looking at the problem from both an Eastern medicine philosophy and Western medicine philosophy. He feels both viewpoints are valid, even though they are based on different rationales.
For example, in Western medicine, it�s understood that if we don�t take care of our bodies and keep them in proper alignment, they will begin to deteriorate and become weak very quickly. Pain signals will take over instead of muscle signals and contractions. We�ll begin to lose coordination, which ultimately, means we�ll lose our mobility and become less active. We�ll be less motivated to eat right and begin to feel helpless and assume the fetal position.
When we�re stressed, we curl up in the fetal position, and that�s a position of self-defeat. This position is a sign of anxiety, depression, and tension throughout the entire body. As we begin to look at illness from this perspective, we start to branch over to the Eastern medicine philosophy: how does this affect quality of life?
As we delve deeper into the Eastern medicine philosophy, we must consider the importance of the central nervous system and cerebral spinal fluid (CSF) and how it relates to muscle balancing: If you have a block in CSF flow, and it gets disrupted (through your brain, through your spinal cord, and back up,) it will change the way your entire body communicates.
Dr. Kareem elaborates further: �If there�s something more critical going on in your body right now, like for example, your nervous system�s compromised because CSF flow is blocked, then it doesn�t care if you want to lose weight. It doesn�t care if you have a cut or a laceration on your skin. It�s not going to heal it as well. It certainly doesn�t care if you have wrinkles that you want to get rid of or if your energy level isn�t what you want it to be. You got to fix the root cause, the number one priority in your body, and a domino effect takes place.
�That, perhaps, linked with oral health are two of the most important foundational things you can do to improve your health, period. If you�re not taking good care of your mouth, and you�re not taking good care of the messaging system for your entire body, those are primitive areas of your body that change everything else. The body�s organized in a way where it�s going to work from the highest priority backwards.�
When it comes to health, many people are focused on the wrong things. People are concerned more about the wrinkles� and the weight loss so energy and focus goes there. They don�t realize that root canals, cavitation, and amalgam fillings�in their mouths are making them toxic. It�s important for people to understand these things can cause inflammation, accelerated aging, and other issues. Toxins do this by getting into the cells the nervous system, and ultimately the anterior head. They�re not aware how their spinal cord is stretched and interfering with their nervous system. Instead of focusing on issues like the skin and weight loss, it�s more important to look upstream�and get to the root cause of our health issues.
Dr. Kareem believes that it is important to work on the number one system first, which is the endocrine system. When the endocrine system is under stress, hormones are more important than going on a particular diet. For example, if your pelvis is out of position and it�s properly realigned, you might uncover a six-pack you didn�t know you had:
�This is one of my biggest lessons and one of my earliest personal training finds. This was an introduction for me to muscle balancing. You see, there was this girl named Lindsey, and she worked as hard as anybody could work. She wasn�t anorexic, but she was borderline at that point where she was just doing everything she possibly could in the gym. She was eating correctly, so she wasn�t really skimming off food, but she just couldn�t get that final six-pack. She just wanted a little bit of definition. She always had the four at the top of the abs, but nothing at the bottom.
�Finally, I ended up doing a postural assessment on her. I took a peek. You know what? We just needed to tip her pelvis backwards a little bit. When we tipped her pelvis backwards a little bit, lo and behold, all those folds went away. Her love handles weren�t actually there. There was no extra body fat on her body preventing her from having the body she wanted. She just needed to be in a slightly different position.
�Now, the coolest thing is not only did she end up getting the body that she wanted, but she starting moving so quickly, all her results accelerated. It was months of work to get to this point, where then all of a sudden, in the next 30 days, she hit every single one of her goals. Truth was, it only took two weeks to tip her pelvis back into position and a few simple exercises that anybody can do at home with just their body weight alone.�
Do You Have Muscle Imbalances?
Our subconscious mind knows when the body�s out of position. If we turned the lights off in the room, you know your arms are behind you. You don�t have to look over to see that. That�s because there�s these little mechanoreceptors in every muscle telling your brain, �We�re over here.�
Same with when the head is forward. The mechanoreceptors are firing, letting the brain knows it�s out of position. When something is out of position, it sucks the energy right out of the cell. This �energy drain� is disruptive to your central nervous system and, if uncorrected, your entire body over time.
The subconscious mind knows this, but the average person is unaware the imbalance is occurring. They don�t know their head is tilted forward or their hips are slightly misaligned. They look in the mirror and think they are ok. I remember when I did this type of work saying, �Look at your low shoulder,� and they would look at themselves and say, �What low shoulder?� The point is this imbalance is the norm, but it�s can be a huge performance zapper.
If a person has had muscle imbalance for a period of time, one or both of these things can happen:
Our bodies are going to balance themselves out. If your head is tilted one way, you�ll subconsciously raise your shoulder a little bit to balance.
A person may opt to take medication to try relieve symptoms of discomfort. However, medication doesn�t get to the root cause of the issue, which is the muscle imbalance. In reality, a slight adjustment may be all that is needed.
Checking for Muscle Imbalances
You can check for muscle imbalances in the comfort of your own home:
Take a string and hang it from the ceiling, or have someone hold it for you. With the string, divide your body between right and left sides. Take a picture of yourself and compare your two sides.
1. When you look closely at the picture, look for the following signs of muscle imbalance:
Is one shoulder is up a little bit more than the other?
Is your side bent a little bit?
Is your head slightly tilted?
Is one hip raised little higher than the other?
Do you have a little bit more of a love handle on one side?
Is one hip is tighter than the other?
2. Take a second picture with the string dividing the body from front to back by taking it with the string at your side.
Is your head forward?
Is your chin tipped up?
Is one shoulder a little bit higher or rounder than the other one?
Is your pelvis tipped so that your lower back is arched a bit, and your belly is sticking out?
These imbalances can affect a person in many different ways. For example, if you�re a runner or athlete you may ask yourself �why can�t I get my hamstrings stronger?� or �why can�t I get faster?� This may be a case where you�re not getting the signal because your back�s arched, and you�re tipped out of position. Identifying the imbalances with a concrete image you can reference is an excellent place to begin looking for clues.
Call Today!
Correcting Muscle Imbalances
Once the muscle imbalance is found, steps can be taken to correct it. While many people have the same types of muscle imbalances, Dr. Kareem stresses that it�s also important to focus on personalized health. This simply means to tailor muscle balancing techniques based on your symmetry.
�A lot of people say, �My right bicep is stronger than my left. Should I just lift heavier on my left and try and make up for it?� No. You actually want to back down. You want to cater to the more limited side of your body. Symmetry comes first. The fastest results come from slowing down to balance your body�s strength, and then everything accelerates from there. You want to back off from your weights on both arms to match the strength of your left, and then you would increase.�
�The same thing reflects ability and mobility in tissue release. If you can raise both arms up into the air, but one of your shoulders is hiking up a little bit, don�t go quite as far. Cater to the more limited side just before your shoulder hikes up, and come back. Work on your mobility just here, opening up your chest, increasing your ability to take a deep breath through your diaphragm. Then what happens is before you know it, even just a few reps in oftentimes, you�ll start to get a little bit further. If you just keep pushing past that point of resistance, sure, the left can keep going as far as it wants, but the right�s never going to get any better. That just results in more twisting through your body.�
Dr. Kareem has devised a short, five-minute program that uses a diagonal pattern that brings the body back into alignment naturally:
1. Free Squat
Stand hip width apart or slightly wider
Exhale and slowly lower, looking straight ahead
Inhale and rise back to starting position
Repeat for 50 seconds
Notes: Keep feet firmly planted. Arms can be crossed in front of body, fingertips at your ears, or held out (as shown.)
2. Superset pushup
Start with hands close together
Exhale and lower
Inhale and rise to starting position
Move hands out to shoulder width apart
Exhale and lower
Inhale and rise to starting position
Move arms out passed shoulder width apart
Exhale and lower
Inhale and rise to start position
This is one rep.
Repeat for 50 seconds
Notes: Pushups can be modified by doing them on your knees.
3. Fast Bridges
Lay on back with your feet planted onto the ground
Keep arms on your sides for stability
Raise hips toward the ceiling and lower quickly
Repeat for 50 seconds
Notes: Keep upper back planted on floor. Make sure to raise both hips evenly. Do not tilt the body.
4. Middle Trap (Bird Exercise)
Lower body into squat position
Feet shoulder width apart
Dig heels into floor
Tuck your chin
Extend arms out to sides
Lower arms to floor
Raise arms parallel to sides
Lower
Repeat for 50 seconds
Notes: Move shoulder, not the arms.
5. Rotational Plank
Start in pushup position
Keep core tight
Exhale and slowly roll body upwards on your left side
Inhale and slowly lower body back to pushup starting position
Repeat for 50 seconds
Notes: Keep core tight at all times. Body should be rolling back and forward in one fluid motion. Keep arms in plank positions at all times. Exercise can also be done on forearms.
For more information on these exercises, go to Dr. Kareem�s website.
This exercise program is designed to stimulate the front of body, the back of body, the lower body, and the upper body. This excites all of the nerves in the body and involves the smaller muscles. As a person performs these exercises, his body will quickly learn how to challenge the smaller muscles as well.
The body will begin to balance itself out by recruiting the big muscles to send the signal to the smaller ones. The idea here is to �train a nerve, not a muscle,� and that nerve starts in your head.
Dr. Kareem recommends performing these exercises every day or every other day. 50 seconds of work and 10 seconds of rest before you transition to the next exercise. Everything is one minute, and it�s a total of five minutes every other day.
A popular misconception is we must do a certain amount of weight or reps for an exercise to be effective. Popular opinion is we are to do three sets of 10, three sets of 15, five sets, etc. In actuality, there is no solid evidence saying that that has to be the number instead of three reps or instead of six. The reality is your body just wants the cue in the right direction and let it take over. Instead of overanalyzing, we should just let nature take its course. We can self-optimize and trigger our small cues to say, �hey, body, I want to do this now.� When we send that signal for the first time, the body will understand, and it�ll start to superimpose it onto our lives and our body.
The Power of Visualization
An important part of this exercise is visualization. When a person thinks about a movement, the body begins to respond to that movement. Elite athletes use this method to prepare for a race or athletic event. They visualize the entire race before it happens.
It�s important to watch somebody else demonstrate properly first, then picture yourself doing the same move identically. This is the fastest way to learn a movement, and your body will begin to subconsciously learn how to perform the movement as well. Visualization techniques are very effective, and have shown to increase contractile strength by 30%.
On average, it takes about six weeks for a new exercise or activity to become second nature. A good example is getting out of a chair: the average person just gets up and walks without thinking about it, but in the beginning it may have taken effort. This is often the case with babies first learning to walk or people who are going through rehabilitation. They have to learn certain things all over again until they can do them without thinking about them.
Dealing with Chronic Injuries
When dealing with chronic injuries, Dr. Kareem suggests a person back off from their current activities or lower the intensity to ensure they�re not overtraining. It�s time to allow the body to learn something new, and that can be accomplished by performing the five muscle balance exercises described above. Here are a few tips from Dr. Kareem:
Weekend warrior.�If you�re not moving at all during the week, it may be helpful to decrease the intensity on the weekend warrior activities. If you�ve been playing two hours of basketball a day, cut it down to one just for a few weeks until you get the postural piece right.�
Elite athlete.�If you�re an elite athlete, maybe you�ll cut out a little bit of the time that you�re spending in the gym weight training. What you want to do is just use these five exercises initially, and then replace them over time. Use these five exercises. Do your workout, so you�re still playing basketball, or you�ll still play your sport. Within a few weeks, you�ll notice that your posture�s improved. Do that plumb line test, and you�ll see, �Where do I stand?�
Older individuals.�If you�re an older adult, avoiding falls is going to be the number one predictor of your longevity and quality of life. Take the same five minutes and use it as your five-minute mini circuit, or five-minute circuit in anything that you�re doing to enhance your health.�
�Once you know your body�s moving the way you envisioned, you can replace the five exercises with something different and something more powerful for you. It can be coordination training, speed training, balance reaction training, etc.�
In addition to athletics, doing muscle balancing exercises can help alleviate many other health conditions as well.
Additional Benefits of Muscle Balancing
Muscle balancing therapy has shown to help many conditions including the following:
Arthritis
Speed
Chronic pain
Chronic Fatigue Syndrome
Muscle balancing exercises are designed to improve health on a cellular level, giving attention to cells in the body that need them most.
Improved circulation. Muscle balancing helps the circulatory system become more efficient. This is important because red blood cells carry oxygen and the oxygen mitochondria needed to create energy production for every cell in the body.
Strengthened nervous system. Muscle balancing teaches the body to contract a muscle at the right time and in the right sequence by targeting our nerves instead of our muscles. The body then creates a �pump effect� that allows the deoxygenated blood stuck in your ankles and fingertips to find its way back to your heart efficiently and easily. This allows the heart to focus on getting rich, oxygenated blood back to the rest of your body.
Muscle Balancing with Massage
Dr. Kareem believes in myofascial release, which is a method of applying gentle pressure to eliminate pain and restore motion. When a person gets a massage and they experience a �good hurt,� that can indicate they either have a muscle imbalance or a knot in the muscle.
In addition to the five exercises, a tennis ball, foam roller, or massage are all effective ways to help remove knots and eliminate muscle imbalance. By using these methods, you�re taking something that functions almost like scar tissue, and giving it more slack. When you give your body more slack, you give it more forgiveness. Ultimately, that leads to a more effective, younger-feeling body.
Muscle imbalances can affect a person in many different ways. By eliminating imbalances, a person can see quality of life improve physically, mentally and spiritually. However, fixing muscle imbalance is one piece of the puzzle to realizing optimal health. I encourage you to address any imbalance, but to get real and lasting results a Multi-Therapeutic Approach must be implemented. My MTA involves diet change and variation, proper exercise, fasting, True Cellular Detox�, emotional detox, and more. Combining multiple proven health strategies is the most surefire way I know to fix cellular dysfunction and enjoy your best life.
As a team physician for the St Louis Cardinals during their 2011 World Series Championship season, I learned a lot about the importance of players taking care of themselves firsthand. I would see players preparing themselves both mentally and physically for the game ahead. Kids look up to these players and emulate them. Major League Baseball (MLB) recognizes this and wants their youth players to be healthy and play as safely as possible. This is why MLB took time, energy, and resources, to determine what would be best for today�s young pitchers. Below is a snapshot of what the MLB and the American Sports Medicine Institute (ASMI) found as risk factors for the young pitcher. It�s recommended that these guidelines be followed by coaches, parents, and players.
The MLB Pitch Smart guidelines provide practical, age-appropriate parameters to help parents, players, and coaches avoid overuse injuries and encourage longevity in the careers of young pitchers.
It was found that specific risk factors were seen as creating a higher incidence of injuries. According to the ASMI, youth pitchers that had elbow or shoulder surgery were 36 times more likely to regularly have pitched with arm fatigue. Coaches and parents are encouraged to watch for signs of pitching while fatigued during their game, in the overall season, and during the course of the entire year.
The ASMI also found that players that pitched more than 100 innings over the course of a year were 3.5 times more likely to be injured than those who did not exceed the 100 innings pitched mark. It�s important to note that every inning counts. Games and showcase events should count toward that total number of 100.
Rest is key. Overuse on a daily, weekly, and annual basis is the greatest risk to a young pitcher�s health. Numerous studies have shown that pitchers that throw a greater number of pitches per game, as well as those who don�t get enough rest between outings, are at a greater risk of injury. In fact, in little league baseball, pitch count programs have shown a reduction in shoulder injuries by as much as 50% (Little League, 2011). Setting limits for pitchers throughout the season is vitally important to their health and longevity in the game.
Pitching with injuries to other areas of the body will also affect a player�s biomechanics and change the way he delivers his pitch. An ankle, knee, hip, or spinal injury can cause changes in the biomechanics of how a player throws and will put more stress on his arm. Be cautious with these injuries, because at times the changes in the mechanics of the player can be very subtle; however, they can cause a significant amount of strain on a player�s pitching arm.
For best results for your youth baseball player�s longevity in the sport and keeping a healthy arm for seasons to come follow the MLB�s pitch count and required rest guide.
Call Today!
3 Common Shoulder Sports Injuries
The shoulder is the most mobile joint in the body, which also makes it prone to injury. If you�re an athlete, taxing your shoulder over time with repetitive, overhead movements or participating in contact sports may put your shoulder at risk for injury.
There are several nonsurgical and surgical options available to treat labrum tears in the shoulder.
These are three common shoulder injuries caused by sports participation:
1. SLAP Tear
This is a tear to the ring of cartilage (labrum) that surrounds your shoulder’s socket. A SLAP tear tends to develop over time from repetitive, overhead motions, such as throwing a baseball, playing tennis or volleyball, or swimming.
Athletic performance decreases. You have less power in your shoulder, and your shoulder feels like it could �pop out.�
Certain movements cause pain. You notice that pain occurs with certain movements, like throwing a baseball or lifting an object overhead.
Range of motion decreases. You may not throw or lift an object overhead like you used to, as your range of motion decreases. You may also find reaching movements difficult.
Shoulder pain you can�t pinpoint. You have deep, achy pain in your shoulder, but you can’t pinpoint the exact location.
It�s common to experience shoulder instability if you�re an athlete. This injury can occur if you�re participating in contact sports, including football or hockey, or ones that require repetitive movements, like baseball.
Shoulder instability happens when your ligaments, muscles, and tendons no longer secure your shoulder joint. As a result, the round, top part of your upper arm bone (humeral head) dislocates (the bone pops out of the shoulder socket completely), or subluxates (the bone partially comes out of the socket).
Dislocation is characterized by severe, sudden onset of pain; subluxation (partial dislocation) may be accompanied by short bursts of pain. Other symptoms include arm weakness and lack of movement. Swelling and bruising on your arm are visible changes you may also notice.
This is another injury commonly seen in athletes participating in repetitive, overhead sports, including swimming and tennis. Rotator cuff injuries are typically characterized by weakness in the shoulder, reduced range of motion, and stiffness.
Being aware of these injuries and knowing their symptoms may encourage you to seek medical treatment sooner; early treatment intervention could result in a better outcome and earlier return to sports.
There�s nothing more frustrating for an athlete than sitting injured on the sidelines watching others compete. Although there�s not one foolproof way to stop shoulder pain from occurring, there are several tips that may help prevent it from starting or getting worse.
If you notice shoulder pain during certain activities, say while throwing a baseball or swimming, stop that activity for a period of time and find an alternative exercise, such as riding a stationary bike. Doing so can give your shoulder some time to rest and heal, while maintaining your cardiovascular fitness.
At the same time, don�t eliminate all shoulder movement. This is because you don�t want to develop a stiff shoulder from infrequent use. Consider doing some mild stretches to keep your arm moving.
2. Change Your Sleeping Position
If you notice pain in your right shoulder, don�t sleep on your right side. Try sleeping on your left side or back instead. If sleeping on your back irritates your shoulder, try propping your arm up with a pillow.
3. Warm Up
Exercising cold muscles is never a good idea. Before practicing your volleyball serve or baseball pitch, warm up your body with mild exercise. For example, start walking for a few minutes and gradually build up to a jog. Doing so raises your heart rate and body temperature and activates the synovial fluid (lubricant) in your joints.1 In other words, a mild warm up gets your body ready for the intense workout that follows.
4. Build Up Your Endurance
It�s a good idea to increase your endurance over time. If it�s been a few weeks or months since you�ve hit the tennis court, consider playing for a short period of time�maybe just 20 minutes to start�and build up to a longer period of playing time. Don�t fall into the trap of doing too much too soon, especially when your body is not used to it.
Strengthening your shoulder muscles can help provide support and stabilization to your shoulder joint. This, in turn, may prevent painful injuries like a shoulder dislocation, which is when the ball of your shoulder comes out of its socket.
Speak to your doctor before starting a strengthening program. They can suggest exercises to perform or may recommend working with a physical therapist.
6. Cross-Train
Some sports are particularly taxing on the shoulder due to repetitive, overhead movements. So you may want think about cross-training. If you�re a swimmer, for example, alternate some of your swimming workouts with a running or biking workout to reduce the stress on your shoulder, while still staying physically fit.
Alternatively, if you�re a painter or construction worker�two occupations commonly associated with repetitive, overhead movements�talk to your boss and ask if there are other non-repetitive tasks you can take on.
Above all, listen to your body and be proactive. You may need to make some adjustments to workout or daily routine to help prevent further damage down the road. It may also be worth getting your doctor�s input, even if you think you�ve got a minor injury. Catching injuries or discomfort early may help keep you in the game and prevent painful injuries down the road.
Being aware of sports�injuries and knowing their symptoms may encourage you to seek medical treatment sooner as early treatment intervention could result in a better outcome and earlier return to sports.�For Answers to any questions you may have please call Dr. Jimenez at
Proven�research is now indicating that receiving Chiropractic adjustments to the pelvis can�increase vertical jump height. �This new research further solidifies the stance of many professional and collegiate teams with providing Chiropractic care for their athletes. In addition to injury prevention this research proves that chiropractic care results in an increase in sports performance.
[Purpose] This study aimed to investigate the effect of pelvic adjustment on vertical jump height (VJH) in female university students with functional leg length inequality (FLLI). [Subjects] Thirty female university students with FLLI were divided into a pelvic adjustment group (n = 15) and a stretching (control) group (n = 15). [Methods] VJH was measured using an OptoGait. [Results] After the intervention, jump height improved significantly compared with the pre-intervention height only in the pelvic adjustment group, while FLLI showed statistically significant improvement in both groups. [Conclusion] Pelvic adjustment as per the Gonstead method can be applied as a method of reducing FLLI and increasing VJH.
Key words:�Pelvic adjustment, Functional leg length inequality, Vertical jump height
INTRODUCTION
The pelvis, a structure located between the hip joint and the lumbosacral spine and attached to several muscles, regulates the movement of the hip joint and lumbosacral spine. The position of the pelvis is the most critical factor determining the sagittal alignment and posture of the human body). Only when the pelvis is in the neutral position can be in the right posture, move the upper and lower body in the dynamic posture, and improve daily movements and ambulatory ability).
Functional leg length inequality (FLLI) worsens due to pelvic tilt in the medial plane and pelvic rotation in the sagittal plane). Therefore, FLLI might be improved by pelvic adjustment. High-velocity and low-amplitude (HVLA) adjustment has been widely utilized as a general chiropractic adjustment method). Many studies have indicated that leg length inequality (LLI) causes posture alteration), limiting exercise and causing tension of the muscles and other soft tissues5). LLI is accompanied by several clinical symptoms6)�such as lumbar pain)�and hip pain). Correcting leg length inequality reportedly reduces pain, increases mobility, and improves posture).
Vertical jumping is practiced to enhance the muscular strength and endurance of the leg and serves as a barometer of muscular strength). There have been studies in which plyometric training was undertaken to improve leg muscle strength), dynamic stretching was applied after jogging for 5 minutes to improve vertical jump height (VJH), or HVLA manipulation was performed for talocrural joint dysfunction). However, there has been no study in which FLLI was corrected and VJH was measured as a barometer for leg muscle strength. Many studies have assessed the effect of pelvic adjustment on FLLI), posture), pressure on the foot, and balance). However, no study has investigated the changes in FLLI and VJH resulting from just a single adjustment. Therefore, this study aimed to assess the immediate effects of a single pelvic adjustment on FLLI and VJH in female university students with FLLI.
SUBJECTS AND METHODS
A total of 30 female university students with an FLLI of more than 10?mm between the left and right legs were selected and randomly assigned to one of two groups: the pelvic adjustment group (adjustment group, n = 15) and control group (stretching group, n = 15). The exclusion criteria were as follows: anatomical LLI; degenerative osteoarthritis; muscle, bone, or nervous system problems; ankle joint, knee joint, hip joint, or lumbar pain; limited range of motion due to burn or postsurgical scarring; and regular leg exercise. This study was approved by Korea Nazarene University�s Institutional Review Board, and the safety of all subjects was protected during all parts of the experiment. All subjects understood the purpose of this study and provided written informed consent prior to participation in accordance with the ethical standards of the Declaration of Helsinki.
The age, height, and weight of the subjects in the adjustment group were 23.5�4.7?years, 163.0�5?cm, and 54.1�5?kg, while those in the stretching group were 22.2�6.3?years, 162.7�6?cm, and 53.1�6?kg, respectively. Gender was analyzed using the ?2�test, while age, height, and weight were analyzed using the independent t-test. As these analyses detected no statistically significant differences (p>0.05), the two groups were deemed identical.
The pelvic adjustment performed in the adjustment group consisted of an HVLA technique administered in the prone posture in accordance with Gonstead�s theory. Subjects were instructed to lie prone, their pelvic height was checked, and the posterior-inferior innominate bone was given an anterior-superior impact while the anterior-superior pelvis was given a posterior-inferior impact. When making these impacts, the therapist put one of his hands on top of the other, placed them on the posterior-superior iliac spine or the ischial spine, and then gave the impact using his own weight, gravity, and acceleration). This adjustment was performed 3�5 times by one skilled physical therapist with more than 10?years of clinical experience. The control group stretched the backbone erector, rectus abdominis, iliac muscle, psoas major, quadriceps muscle, leg adductor, and quadratus lumborum adjacent to the pelvis in order to resolve muscular imbalance that could further the pelvic imbalance. In the process, the therapist assisted the subjects in performing additional height training for each muscle and maintaining each posture at the maximum height for 10�15 seconds. The subjects then resumed the initial posture, rested for 5 seconds, and repeated the stretching one more time. Stretching was done three times per posture for a total of 15 minutes).
For leg length measurement, subjects lay straight on a bed, and the tape measure method (TMM) was used to measure the leg from the anterior superior iliac spine (ASIS) to the medial malleolus. Beattie et al. reported that LLI as measured by the TMM did not show a significant difference from radiological findings. We were therefore confident in the reliability of using the TMM for measuring leg length). The measurement started from the ASIS so that pelvic bone-related problems such as pelvic tilt and pelvic asymmetry could be included.
We used an OptoGait (Microgate Srl, Bolzano, Italy), a system for optical detection, to analyze ambulation and measure VJH. On its signal-sending bar, there are 96 LEDs that communicate via an infrared frequency. The signal-receiving bar has an identical number of LEDs. We installed the signal-sending and signal-receiving bars of the OptoGait one meter apart on a flat surface. When a subject performs a vertical jump between the bars, the bars calculate the time at which the subject touches the floor or stays in the air and communicates this information by sending and receiving 1,000 signals per second, generating accurate data. Based on this basic data, the OptoGait software calculates the precise VJH.
Leg length and VJH were measured before and after the intervention. The measured data were analyzed using the statistics program SPSS 12.0 KO (SPSS, Chicago, IL, USA), and the collected data are presented as averages and standard deviations. The significance of pre- and post-intervention differences was tested using the paired t-test, and the significance of between-group differences was tested using the independent t-test. The p-value ? was set at 0.05.
RESULTS
In the pre- and post-intervention comparison, VJH improved significantly only in the adjustment group, while FLLI improved significantly in both the adjustment group and the stretching group (p<0.05) (Table 1). When comparing the pre-intervention data, post-intervention data, and changes between the pre- and post-intervention data, VJH showed statistical significance only for the changes between the pre-and post-intervention data, while FLLI showed statistical significance for post-intervention data and changes between the pre- and post-intervention data (p<0.05) (Table 2).
Table 1.
Comparison of the Pre- and post-intervention data for VJH and FLLI in each group (mean�SD) (Unit: VJH-cm, FLLI-mm)
Table 2.
Comparison of VJH and FLLI between the adjustment group and stretching group (mean�SD) (Unit: VJH-cm, FLLI-mm)
DISCUSSION
The pelvis supports the abdomen, connects the spine and legs, and is involved in transferring weight from the spine to the legs when a person stands up, maintaining a straight posture and enabling smooth arm movements). Due to their erect ambulation, human beings are exposed to gravity and can thus be subject to a malalignment of the pelvis and legs affecting posture, ambulatory pattern, and balance. LLI is easily observed clinically and causes functional disturbance of normal biomechanics).
Winter and Pinto reported that pelvic obliquity is caused by LLI), and Mccaw and Bates explained the relation between biomechanics and spinal deformity due to LLI). Defrin et al. reported that when a shoe insert was used in 22 chronic back pain patients with LLI of 10?mm and less, pain intensity and muscular weakening were reduced), which appears to be due to reduced pain and muscular weakening attributed to decreased pelvic tilt resulting from LLI adjustment. On the basis of previous studies on pelvic adjustment, Alcantara et al. reported that following adjustments using fast and slow speed amplitudes in patients with sacroiliac joint obliquity, pain was reduced, and patients could resume daily life and work). Park et al. reported that balance in 20 elderly men was improved through pelvic adjustment according to the Gonstead method). In this study, FLLI was reduced after pelvic adjustment, a finding similar to a previous study in which pelvic adjustment helped reduce FLLI and the pressure difference between soles).
In this study, stretching was not associated with increased VJH, while pelvic adjustment was. In a previous study by Ryan et al. in which subjects jogged for 5 minutes in order to improve VJH, a barometer for leg strength, and then performed dynamic stretching, VJH was increased as compared with a control group that only jogged for 5 minutes). In the present study, it is suspected that VJH did not increase because only static stretching was applied. Hedlund et al. reported that VJH showed a statistically significant increase following 3 weeks of chiropractic HVLA manipulation in 22 female handball players with talocrural joint dysfunction, which is similar to the findings of the present study).
Pelvic adjustment balances the left and right pelvic height and left and right anterior and posterior rotation of the hip bones, which, in turn, leads to FLLI improvement. It also balances the left and right muscle lengths of the rectus femoris and sartorius, which are involved in the hip bone�s anterior rotation, and the hamstring and gluteus maximus, which are involved in posterior rotation. This seems to explain the improvement in vertical jump ability. We recommend that pelvic adjustment be applied for decreasing FLLI and increasing VJH, a barometer for leg muscle strength, in the future.
Research now indicates that receiving Chiropractic Adjustments to the pelvis can�increase vertical jump height. �This research solidifies many professional and collegiate teams that�provide chiropractic care for their athletes. In addition to injury prevention this research proves that chiropractic care results in greater athletic performance.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine

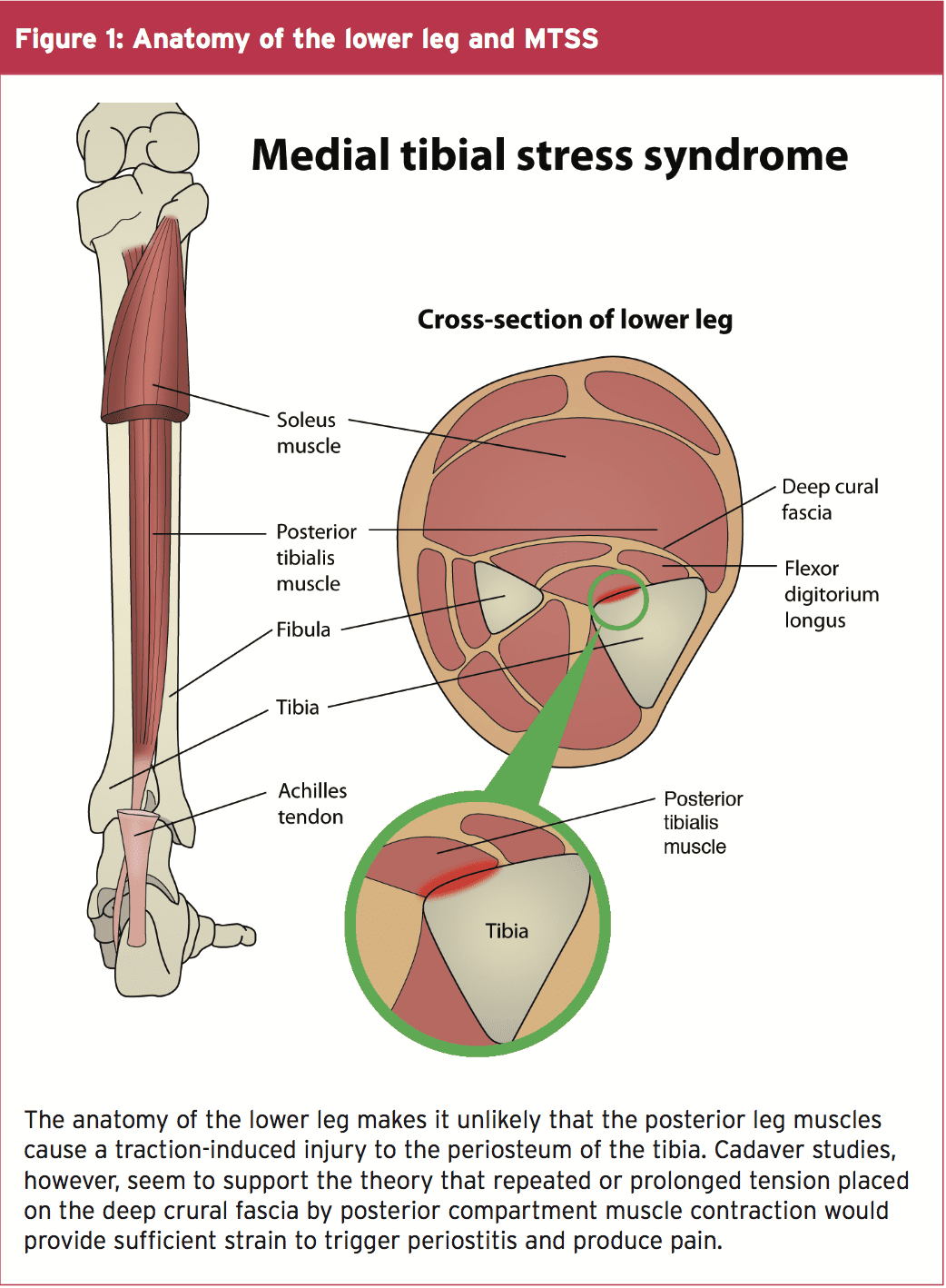
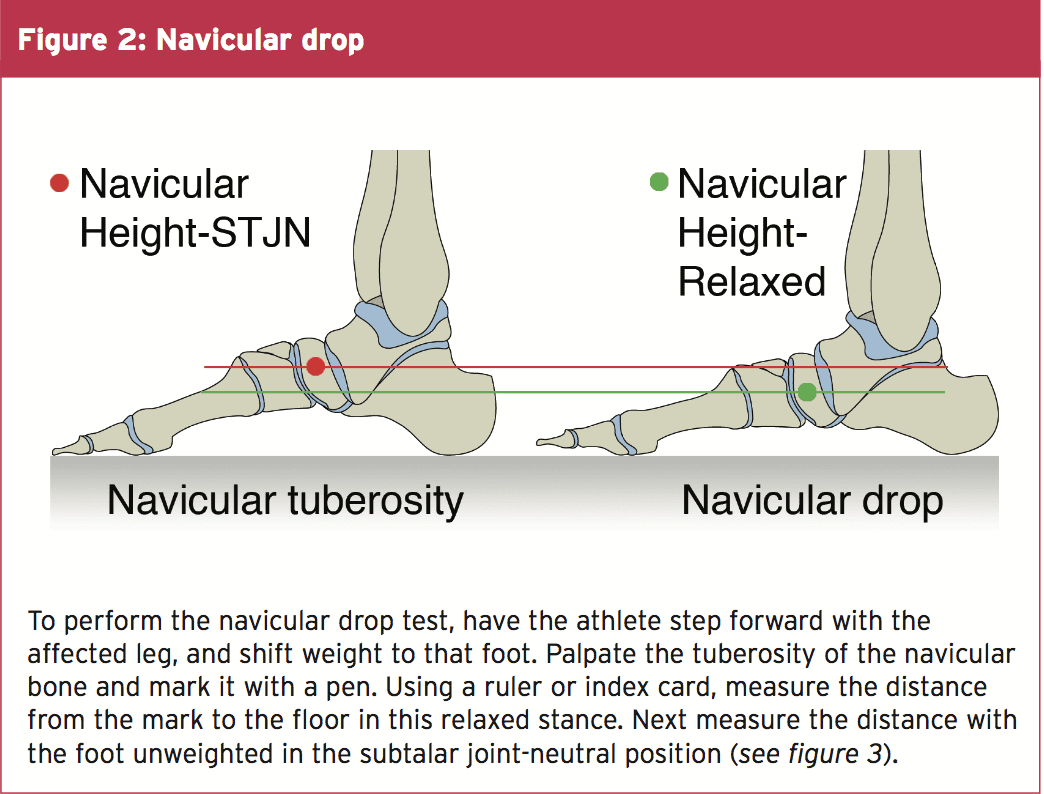
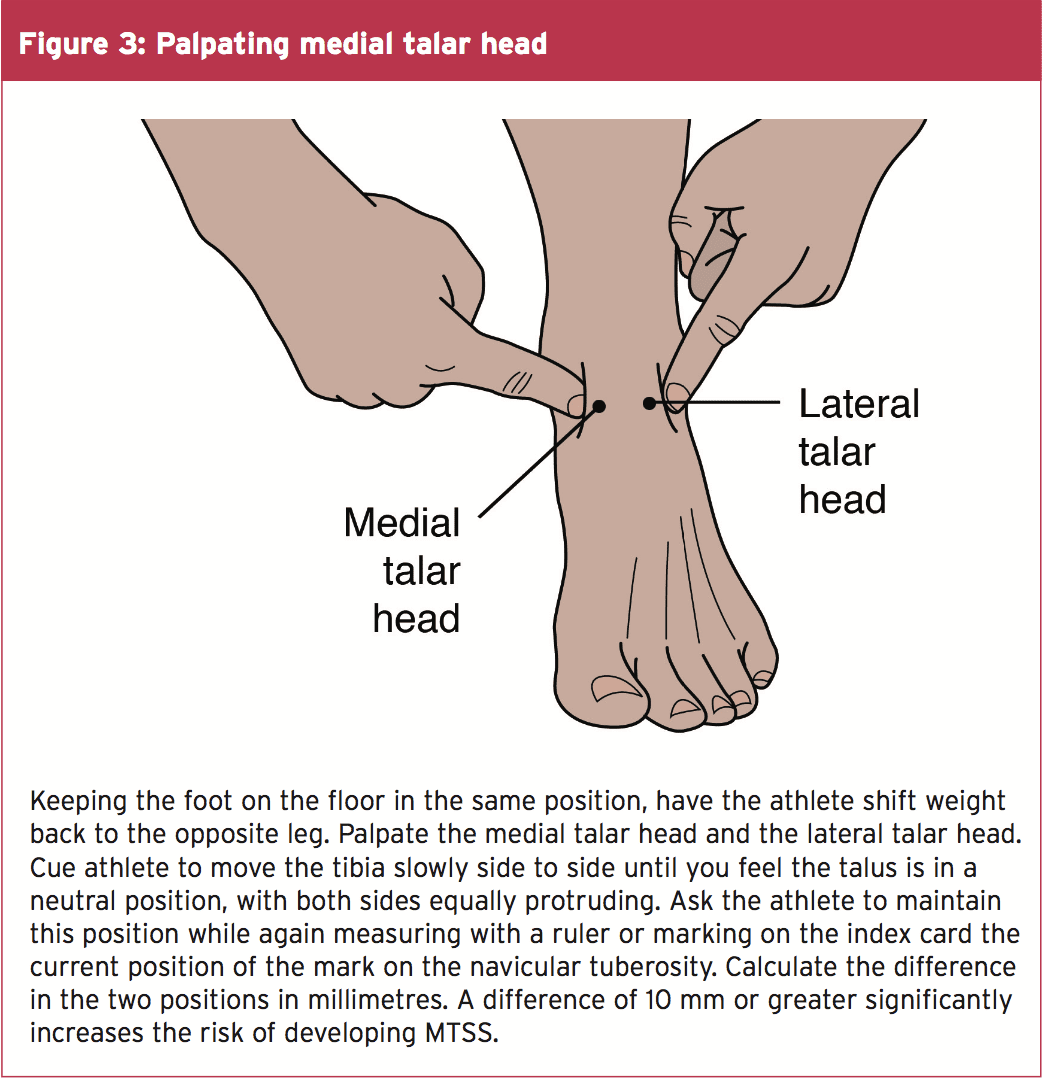
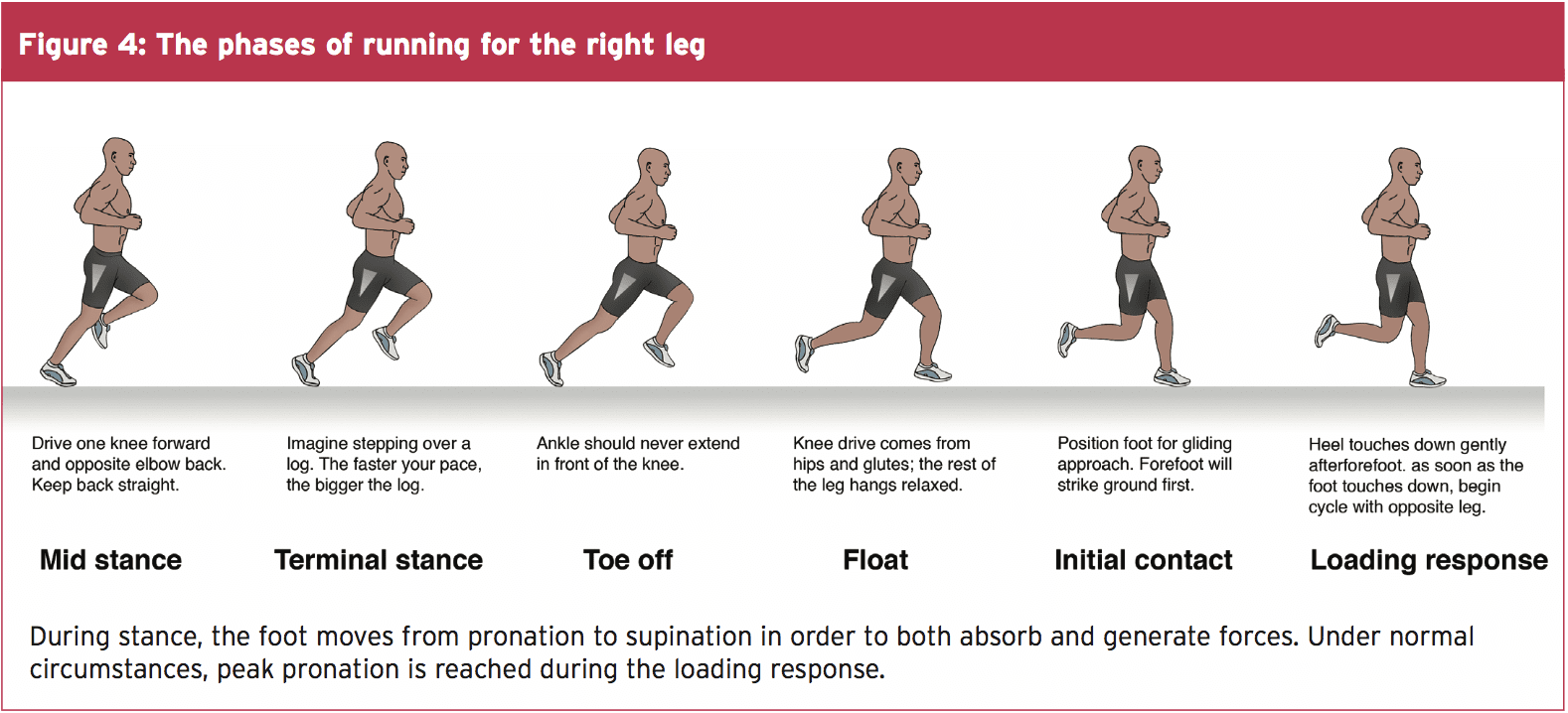
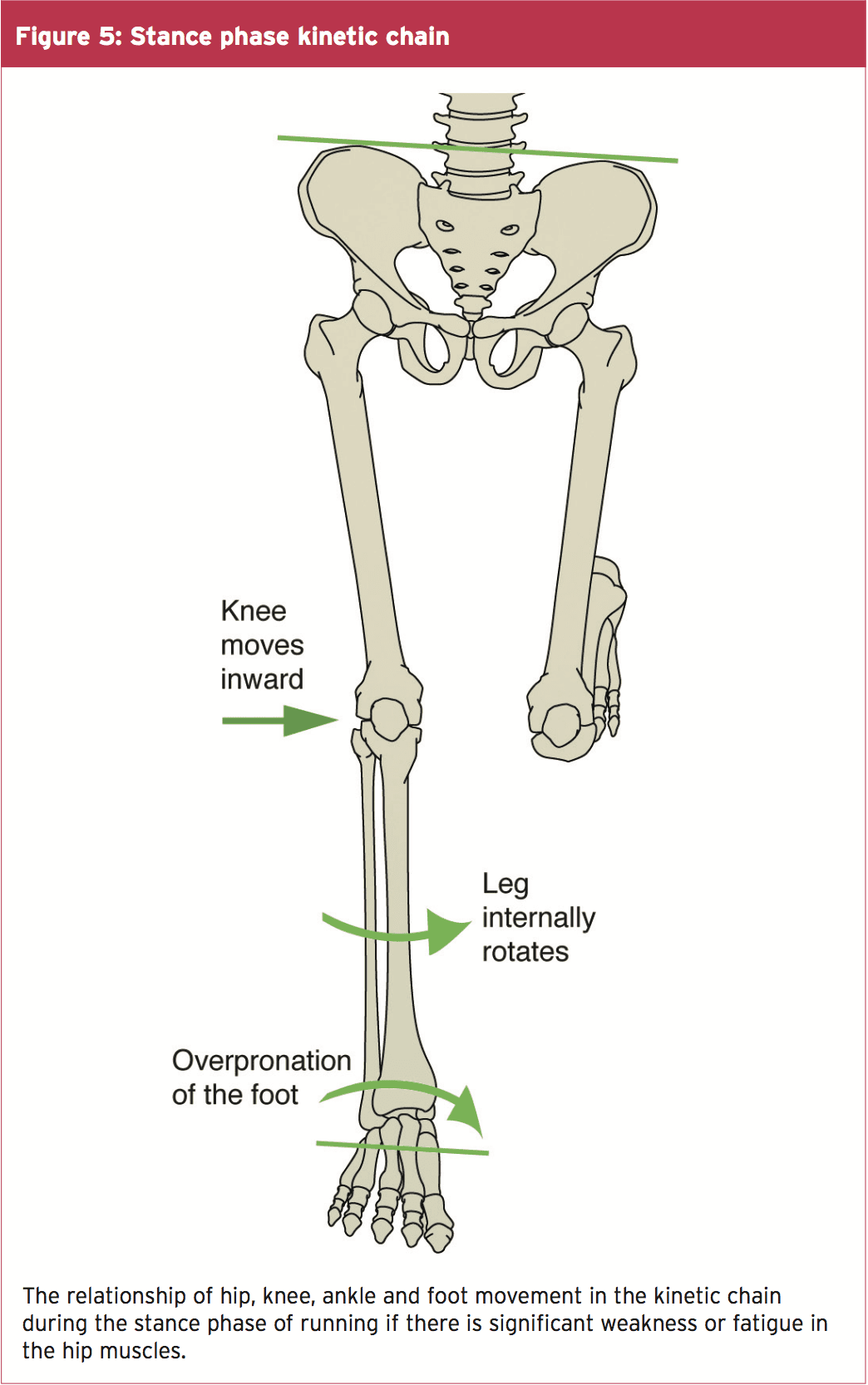
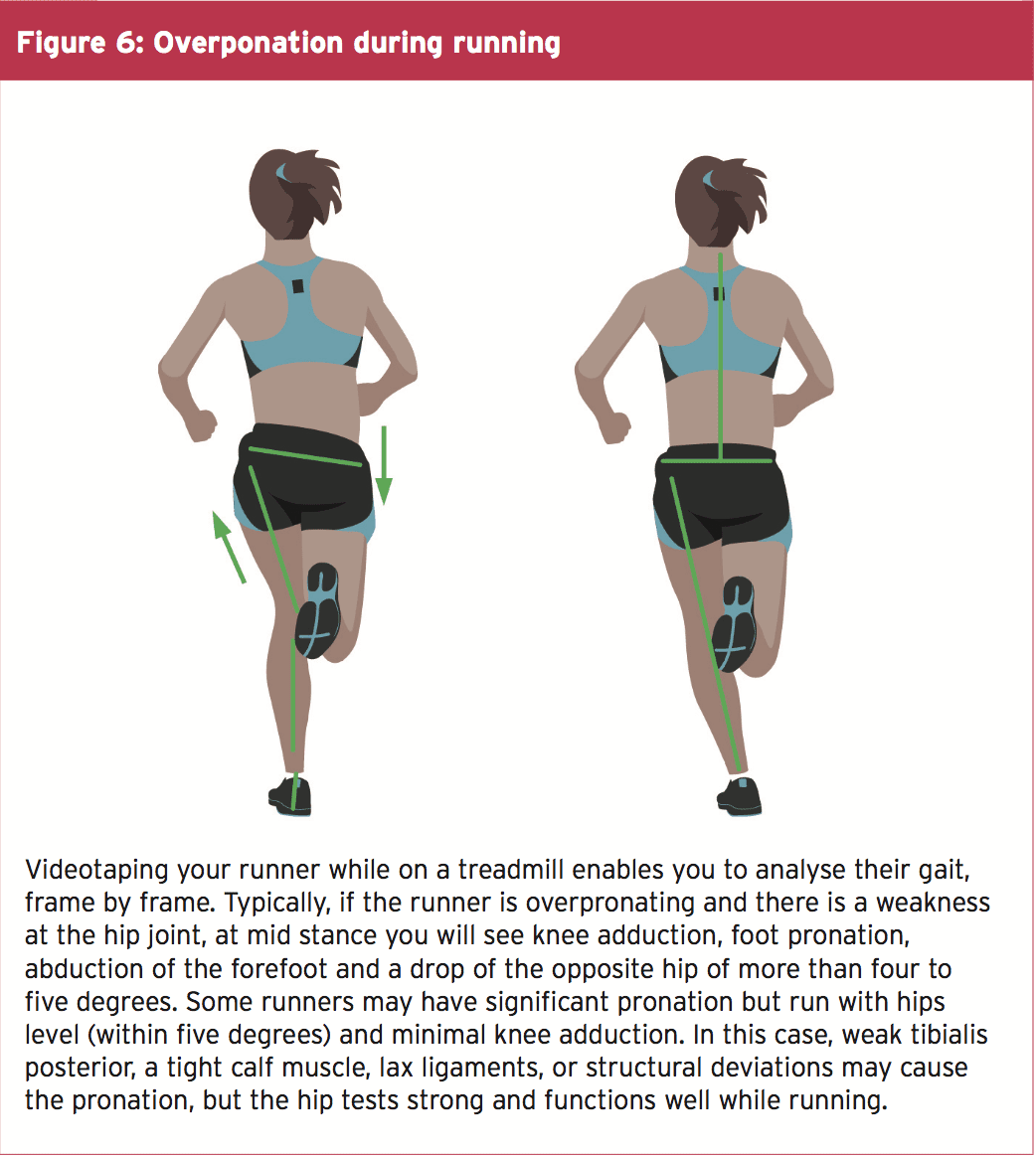
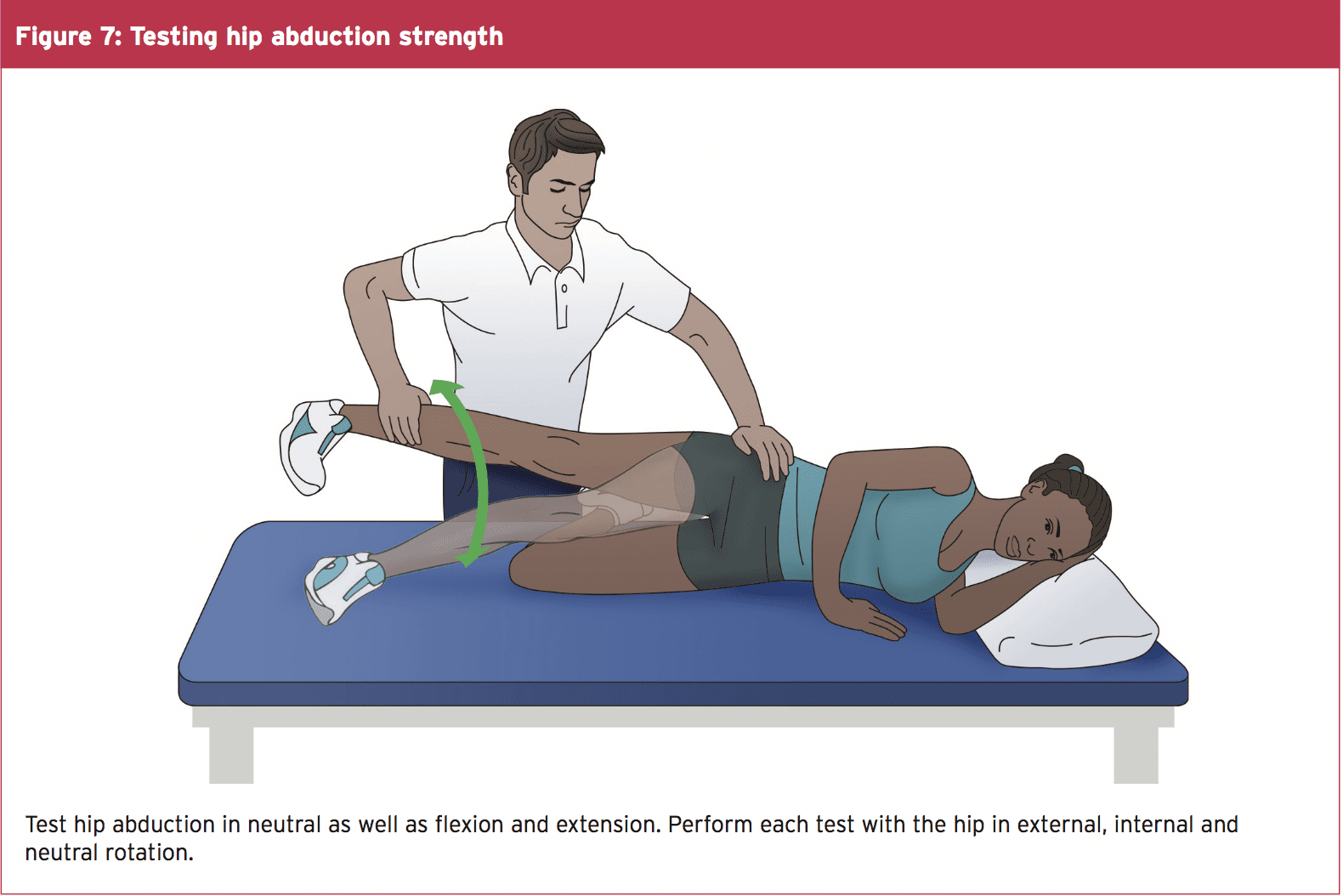

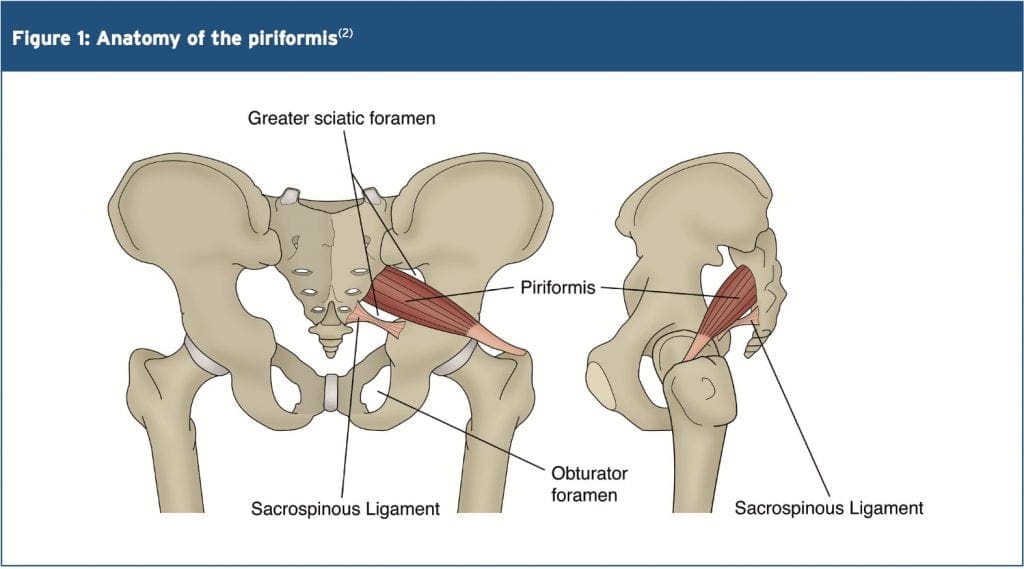
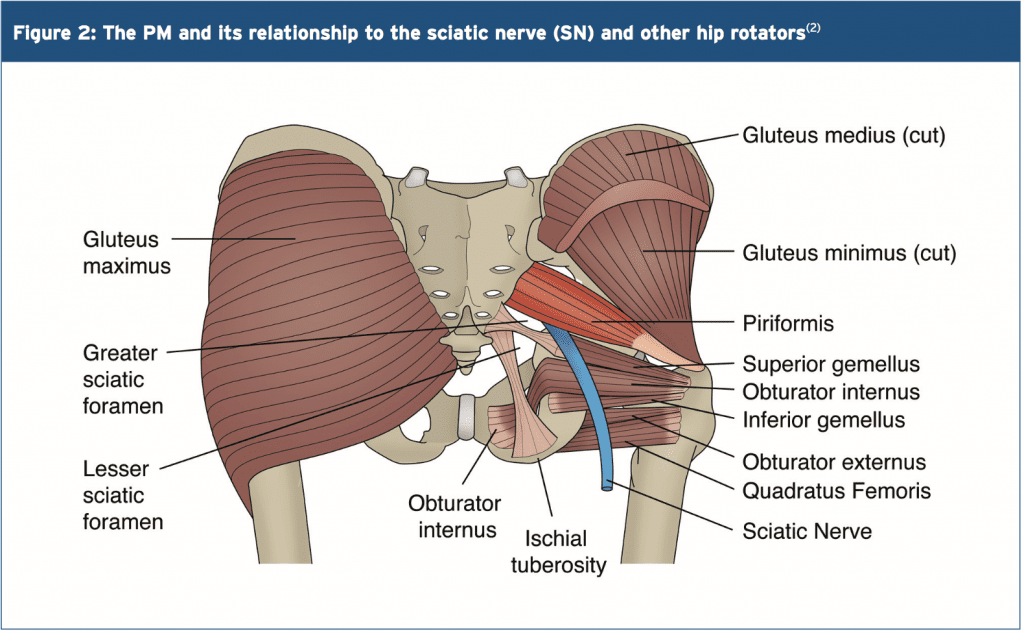 Variants
Variants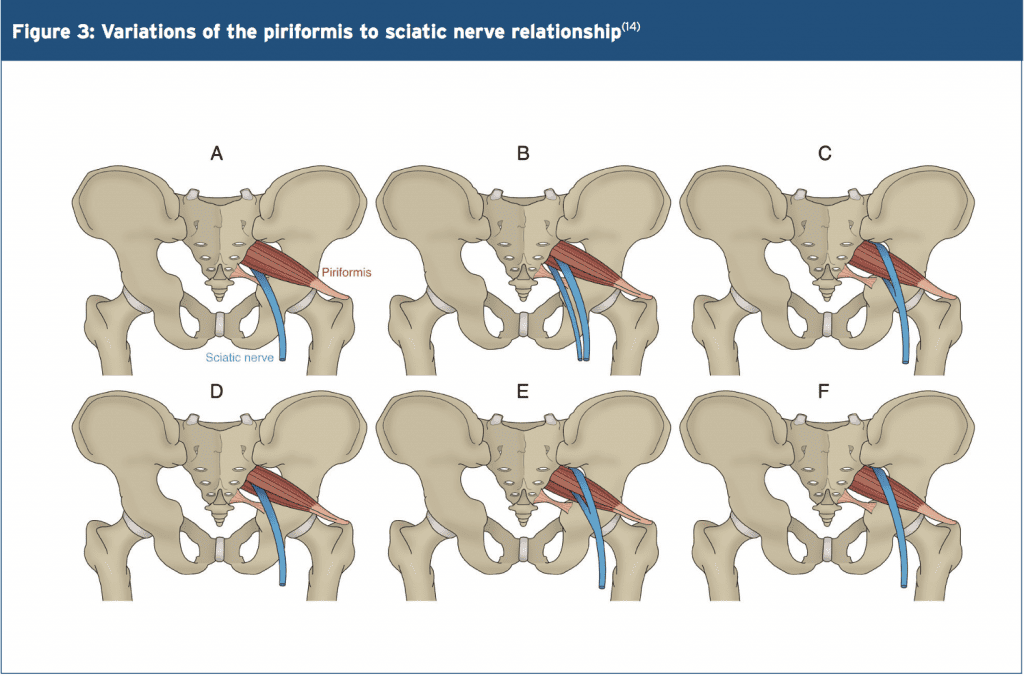
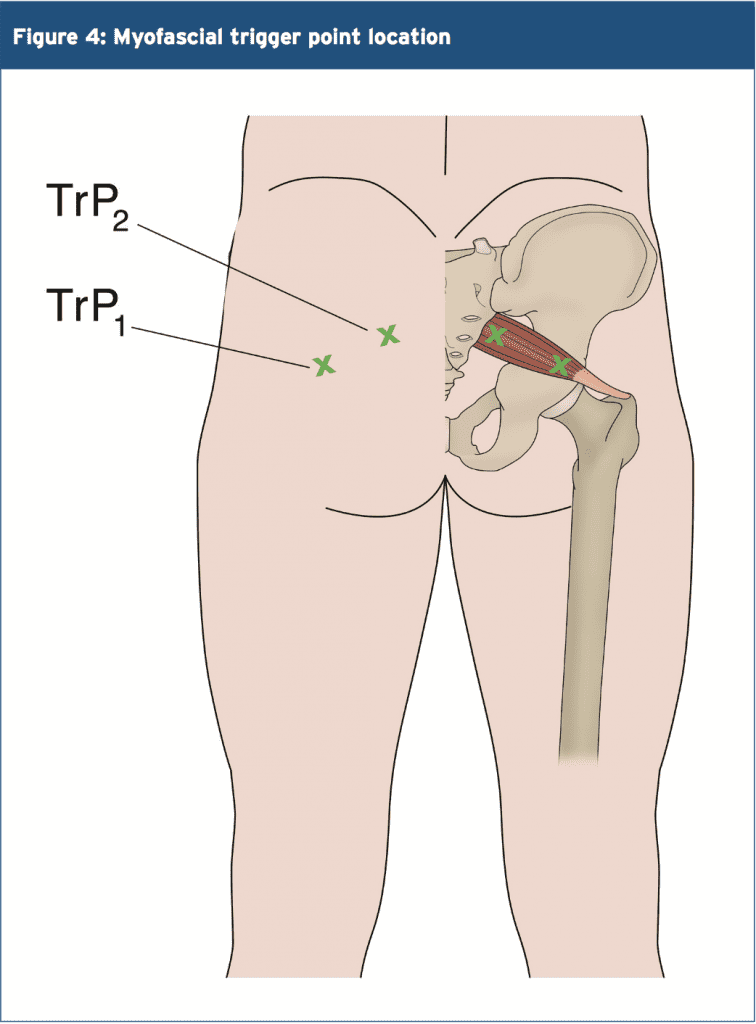
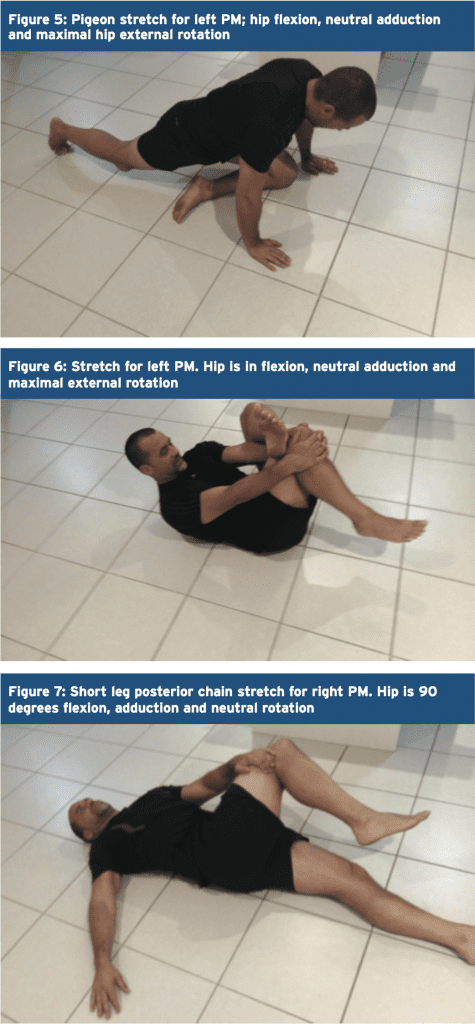 Trigger Points & Massage
Trigger Points & Massage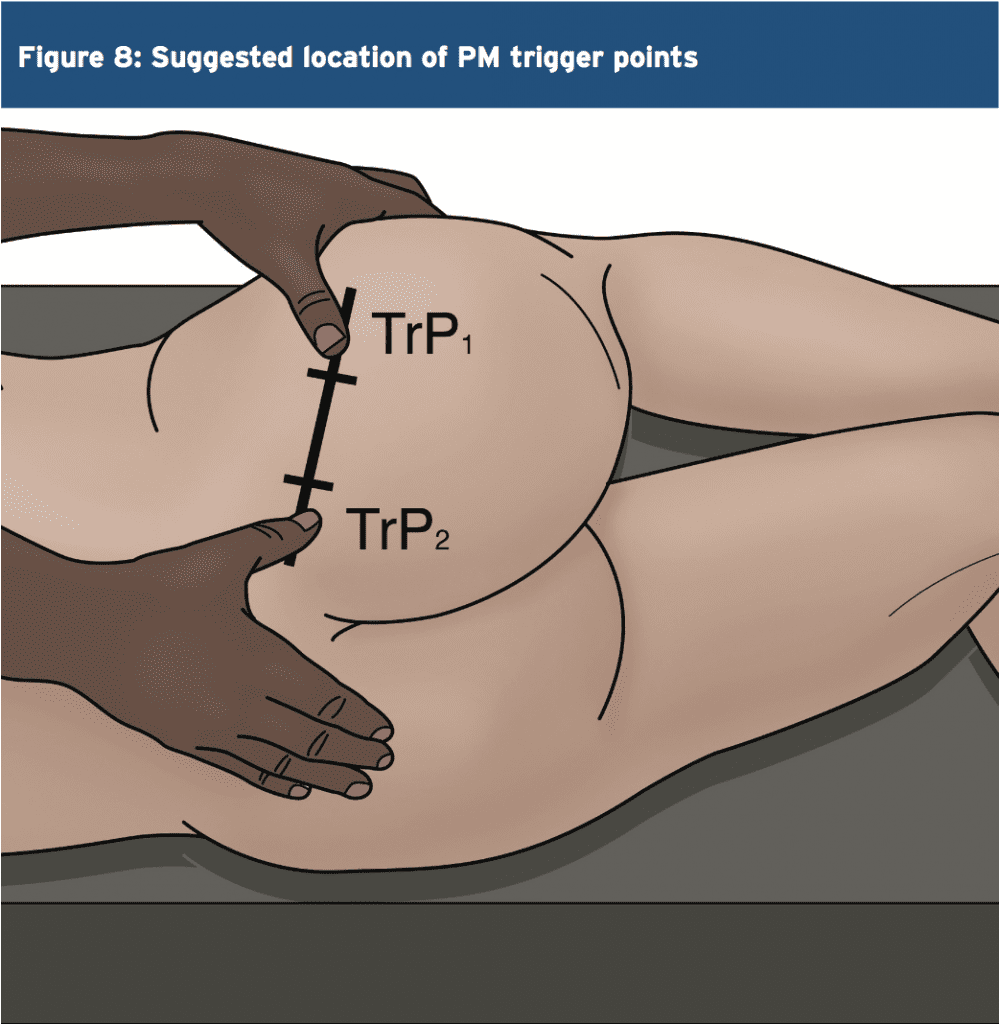

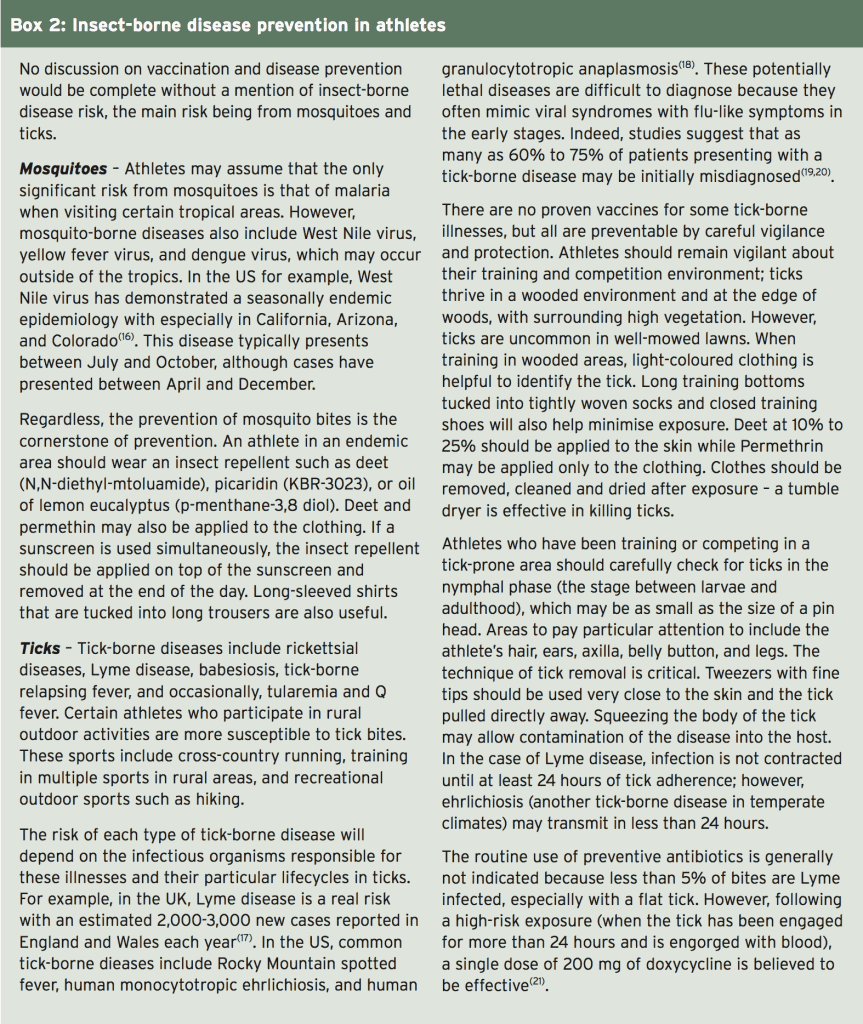
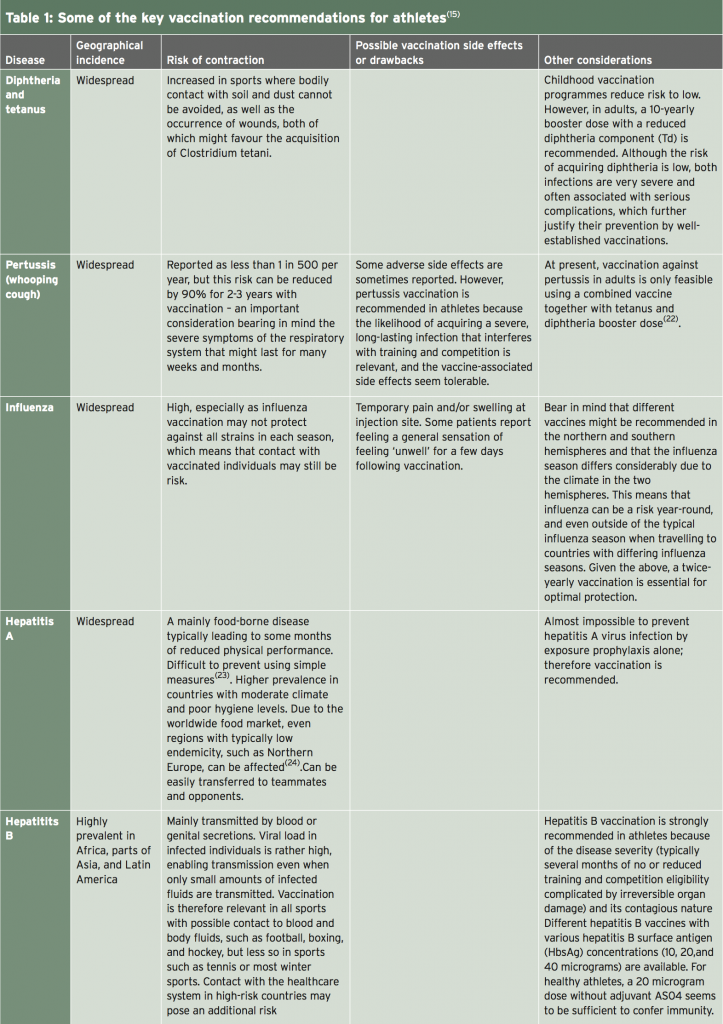
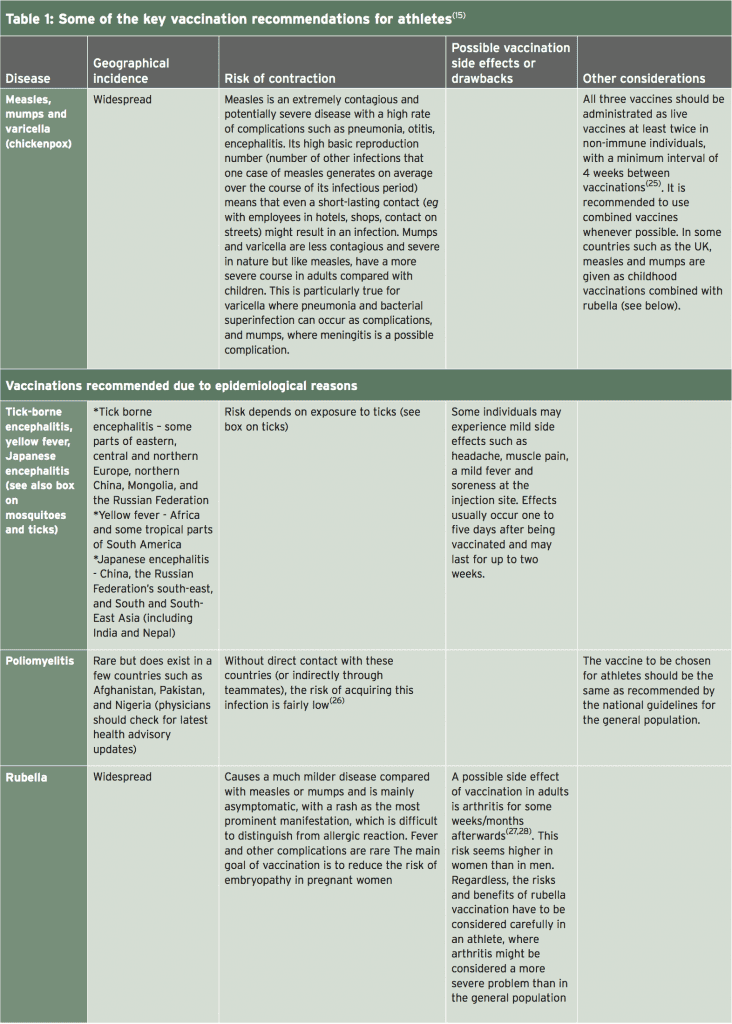
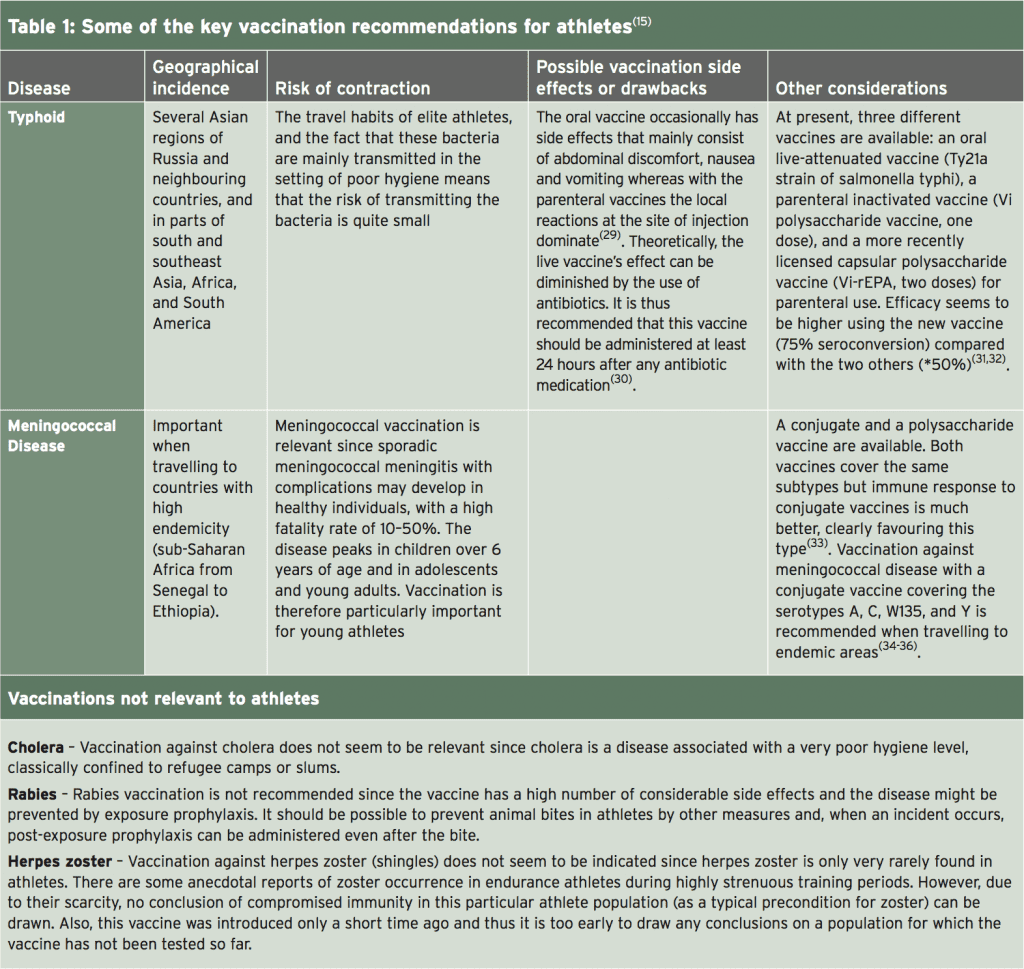















 Muscle balancing therapy has shown to help many conditions including the following:
Muscle balancing therapy has shown to help many conditions including the following:










 A total of 30 female university students with an FLLI of more than 10?mm between the left and right legs were selected and randomly assigned to one of two groups: the pelvic adjustment group (adjustment group, n = 15) and control group (stretching group, n = 15). The exclusion criteria were as follows: anatomical LLI; degenerative osteoarthritis; muscle, bone, or nervous system problems; ankle joint, knee joint, hip joint, or lumbar pain; limited range of motion due to burn or postsurgical scarring; and regular leg exercise. This study was approved by Korea Nazarene University�s Institutional Review Board, and the safety of all subjects was protected during all parts of the experiment. All subjects understood the purpose of this study and provided written informed consent prior to participation in accordance with the ethical standards of the Declaration of Helsinki.
A total of 30 female university students with an FLLI of more than 10?mm between the left and right legs were selected and randomly assigned to one of two groups: the pelvic adjustment group (adjustment group, n = 15) and control group (stretching group, n = 15). The exclusion criteria were as follows: anatomical LLI; degenerative osteoarthritis; muscle, bone, or nervous system problems; ankle joint, knee joint, hip joint, or lumbar pain; limited range of motion due to burn or postsurgical scarring; and regular leg exercise. This study was approved by Korea Nazarene University�s Institutional Review Board, and the safety of all subjects was protected during all parts of the experiment. All subjects understood the purpose of this study and provided written informed consent prior to participation in accordance with the ethical standards of the Declaration of Helsinki.