Chiropractic care is a respected, effective treatment for a variety of conditions as well as for promoting overall wellness. Every day patients seek it out to manage their pain, find relief from health issues, and recover from injuries. But did you know that pro athletes also utilize chiropractic for injuries, soreness, and to keep them playing at optimal levels?
What many may not realize is that an estimated 90 percent of top athletes use chiropractic to step up their game. You don�t have to be an athlete to step up your own game with chiropractic care. Here are three benefits that the pros enjoy � and so can you!
Chiropractic is an effective treatment for pain management.
Chiropractic has long been regarded as a natural, non-invasive, drug-free approach to pain management. Numerous studies have proven its effectiveness in treating pain for some conditions and injuries. Many pro athletes utilize this option to manage their pain from overtaxed muscles and ligaments to activity related injuries.
When the spine not correctly aligned it can put pressure or stress on other areas of the body. Spinal adjustments can help relieve pain in ligaments, joints, discs, and muscles. However, chiropractic techniques can be used for all parts of the body, including arms, hands, fingers, feet, hips, and knees.
Chiropractic helps in preventing injury and enhancing performance.
Doctors of Chiropractic understand that when it comes to treatment, there is not a one size fits all option. Every patient is different, and they will tailor a custom plan that benefits the entire body based on lifestyle, activity level, age, health conditions, and other factors.
The first appointment will include a variety of evaluations that help the doctor determine the best course of treatment for you, including the activities you engage in and the frequency. This way he or she can get an idea of your risk of injury and the areas to concentrate on in your treatment. So, whether you are a pro football player or a weekend warrior, chiropractic can improve your performance and help protect you from injury.
Chiropractic helps in treating many types of injuries.
For pro athletes, injuries are just part of the game. High impact sports like hockey, football, and wrestling tend to result in injuries, but even non-contact sports like baseball, cycling, and golf can lead to injuries as well.
Low impact, as well as low impact athletes, find great value in routine adjustments and spinal alignments. This alone helps to lower their risk of injury as well as improve flexibility and enhance performance. It can help reduce the stress and strain that all types of physical activity place on the body, whether you are a pro golfer or football player, or if you enjoy working in your garden or are a stay at home mom running after kids all day.
Sports equipment with a football, basketball, baseball, soccer, tennis and golf ball and badminton hockey puck as recreation and leisure fun activities for team and individual playing.
Some of the top names in pro sports rely on chiropractic to treat injuries, manage pain, and enhance athletic performance. You might recognize some of the names: Barry Bonds, Arnold Schwarzenegger, Lance Armstrong, Evander Holyfield, Tiger Woods, Joe Montana, and Martina Navratilova are just a few. You don�t have to be an athlete, though, to reap the same benefits that the pros do. You can get them by scheduling an appointment with a chiropractor.
Chiropractic care is a safe, useful healthcare option that is appropriate for all ages and activity levels. Your Doctor of Chiropractic will sit down with you and work with you to create a treatment plan that is tailored to meet your unique needs.
Because this type of treatment focuses on the root of the problem instead of just managing symptoms, your treatment plan will usually involve not only adjustments and chiropractic techniques, but dietary recommendations, exercises, and lifestyle modifications as well so that you enjoy whole body wellness.
Sports Performance is everything! Regardless of whether you�re a pro football player or a weekend warrior, your level of performance in your chosen athletic activity is what takes you to competitive heights.
There are certain things that every athlete knows will make them stronger, faster, more flexible, and have more stamina. Chiropractic care is becoming increasingly popular as a way for the sportsman in all of us to have that competitive edge.
You may know that chiropractic is great for people with back pain or even headaches, but you may be wondering how it can help an athlete. Solid research, along with a proven track record show that chiropractic helps sports performance in several key areas.
Sports Performance & Chiropractic
Increased Flexibility
Flexibility is important for nearly every sport and chiropractic care helps to increase flexibility throughout the body. As the spine is aligned, the body is better able to perform as it should and flexibility is a big part of that.
Better Mobility
When a person has better flexibility they are able to move around better. Chiropractic loosens the joints and spine, releasing energy to flow through the body. Blood flow is increased which means that nutrients and oxygen are carries much more efficiently to the vital organs and brain. This whole body wellness encourages better mobility.
More Resistant To Injury
Because chiropractic keeps the body flexible, there is a much lower risk of injury. Tight muscles can lead to injuries, sometimes serious injury. When the body well aligned and flexible the chances of a pulled or torn muscle or torn ligament are greatly decreased.
Helps Relieve Sports Hernias
Groin pain is a component of around 20 percent of all sports injuries. The thing is, it is often not due to sudden movements that result in injury like a torn muscle. Most of the time is it due to a condition called athletic pubalgia, or sports hernia.
Sports like hockey and football are full contact sports and injuries are not uncommon. However, even milder sports like horseback riding or cycling can also result in injuries or pain from over exertion. One study showed how chiropractic helped relieve the pain of shoulder instability in hockey players.
Chiropractic aligns the spine and body while increasing blood flow, but endorphins are also released through the treatment. This helps the body combat pain in a natural, less invasive way without the use of medications.
Increases Strength
While chiropractic care is typically regarded as a method for relieving pain and alleviating skeletal and muscular issues, it has also been found to improve physical strength. A study on judo athletes who received just three chiropractic care sessions showed that their grip strength improved by 16 percent.
Helps Sports Related Injuries Heal Faster
Chiropractic care has long been a standard practice for aiding in the healing of many sports related injuries including tennis elbow, hamstring pulls, rotator cuff injuries, back strains, and neck pain. While it does help prevent these injuries, in the event that they do occur, chiropractic care helps the athlete recover faster and get back in the game quicker.
So whether you enjoy the occasional game of touch football with the guys or you are a college basketball star, chances are you too can benefit from chiropractic care. Each of these benefits are exceptional in their own right and athletes rely on their chiropractor to keep them in the game, but all these little benefits add up to one significant plus: it improves sports performance. If you want to be stronger, faster, and more agile, the research shows that chiropractic care can certainly help.
Feeling back pain, being unable to perform daily tasks, workout and play sports can be frustrating for anyone. The debilitating symptoms can drive individuals to seek fast relief. But, while a person�s only concern maybe only to fix the day�s pain, fixing the root/cause of the problem is far better in the long run and�can be easily achieved from chiropractic treatment. After receiving a single adjustment, many people especially athletes can expect an increase in their range of motion and less pain. Regardless of the reasons for seeking chiropractic treatment, one question always crosses people�s minds, how often should one see a chiropractor?
The answer to that question depends on the individual�s goals. Generally, spinal complications are not the result of a single day�s activities but tend to occur gradually over a period of time. Many spine conditions and injuries result in symptoms that may intermittently increase and decrease over several years, causing constant, nagging pain or sharp, extreme pain due to wear and tear type of injuries that the body is no longer able to heal on its own.
Chiropractic Treatment Sports Injury
Healing requires time and patience, a person also needs to be aware of what caused the complications in the first place. Suddenly stopping strict exercise routines or gaining weight in a certain amount of time can create an accelerated aging process on the joints.
If an individual�s goals are solely focused on alleviating the pain resulting from one time, then it won�t take much time to heal. Generally, receiving adjustments 2-3 times per week for several weeks can ease pain and decrease other symptoms. But, if a person is seeking to relieve the symptoms associated with an underlying condition or injury, or if a person is seeking to correct an improper posture or a mechanical dysfunction, the process could be much longer. This healing process often may require about 2-3 months of regular adjustments.
Despite completing treatment and successfully alleviating any symptoms, it is recommended to continue chiropractic adjustments on a regular basis. What is considered a regular basis for adjustments? Getting adjusted at least once a week by a chiropractor can help maintain a person�s overall health and can prevent small problems from becoming greater issues. For a greater majority of individuals, especially those who sit most of the day, it�s recommended to maintain an adjustment schedule every week or two. A chiropractor will explain what is the right schedule.
By Dr. Alex Jimenez
Chiropractic Clinic Extra: Sport Injury Treatments
Shin Splint: Whether you are an avid exerciser, an exuberant shopper, or a small child chaser, you have probably felt tightening and burning in your shin at one point in your life. Sometimes, the pain stops when the activity ceases, but other times the pain remains. If shin pain continues bothering you, it may be time to face the fact you have shin splints.
The shin is a bone located in the front part of your lower leg. Shin splints commonly occur in athletes who have intensified or changed their training routines. They also show up in regular people who have changed or added activity to their routine.
The shin has a lot of responsibility during exercise, as it absorbs the shock of the steps, raises the toes, and support the arch of the foot.
A few main culprits play a part in shin splints:
failing to stretch properly before exercising
walking or running on hard surfaces, like pavement
wearing the wrong type of shoes during activity
over-exerting the body with strenuous activity
skipping periods of rest between exercise
Individuals who perform any type of exercise should take appropriate measures to alleviate the above risk factors of shin splints. If you notice pain and soreness in the front part of your lower leg, know how to treat this injury properly.
If rest and ice aren�t doing the job and you’re still suffering pain, it’s time to see a doctor. A thorough exam and possibly an x-ray will diagnose the problem.
Chiropractic care is a powerful choice for treating shin splints and reducing their recurrence.
Chiropractic Treatment Benefits Those Suffering From Shin Splint/s:
Reduction In Pain
Chiropractic is proven to relieve the pain associated with bodily injuries and medical conditions, including shin splints. Sometimes one visit is enough to relieve the pain, other times the pain decreases over a series of appointments. Being able to diminish a high degree of pain down to a manageable level is possible for shin splint patients through chiropractic.
Full Body Alignment
The premise behind chiropractic is that it treats the body as a whole, and, in doing so, promotes healing and health to the injured or diseased areas. A chiropractor may work on your neck to help your calf. With shin splints, he or she may align your spine and joints to lessen the impact of activity on your shins. Again, the entire body is treated in order to create the best environment for health restoration.
Healing Through Adjustments
Treating shin splints is a common procedure for chiropractors. Common practice is to adjust the calf, ankle, and foot to stretch and increase blood flow to the area.
Drug Free Treatment Option
A primary benefit of chiropractic care is it requires no over-the-counter or prescription drugs. Individuals who suffer from stomach issues, or simply prefer to avoid drugs, find chiropractic visits a productive alternative to manage pain and promote healing.
It’s routine for chiropractic treatment of shin splints to include a series of stretching and strengthening exercises the individual performs at home between visits. These exercises further expand on the positive effects of the chiropractic therapy.
If you are one of the many people dealing with shin splints, don’t despair! Consider chiropractic care as your main treatment option or in conjunction with other modes of treatment. Within a few visits, you will experience pain reduction, and enjoy a decreased risk of ever dealing with painful shin splints again.
Soccer is one of the most popular team sports in the United States, and offers an excellent form of exercise to children and adults alike. Unfortunately, the nature of the sport, the repeated movement and the chance of collision, add up to quite a few opportunities for injury.
Lower and upper extremity injuries, overuse injuries, and head, neck, and face injuries are commonplace. According to Stanford Children’s Health, “88,000 children 8-14 were treated in an emergency room for soccer-related injuries.”
Soccer players who take certain precautionary measures decrease their chances of injury. Let�s look at three ways you can avoid injury as a soccer player:
#1: Soccer: Use Proper Equipment
Donning proper fitting cleats, uniforms, and shin guards decrease the risk of being hurt in the first place. Make adjustments often, especially if the player is growing rapidly or fluctuates in weight.
#2: Get Checked Out By A Chiropractor Pre-Season
Soccer players who allow their fitness less to lapse increase the chance of injury. Visit a Doctor of Chiropractic to ensure there are no underlying issues with participating in strenuous activity. A chiropractor is also able to make sure the spine is aligned and muscles and joints are strong and functioning properly.
#3: Pay Attention To The Surroundings
A field that is not kept up well offers a greater chance of turning an ankle or falling. It’s vital to check out the playing area beforehand and note any uneven areas that could cause a player to trip.
In addition, consider the weather. Muddy, slick fields create extra issues, and particularly hot temperatures make players run the risk of dehydration or heat stroke. Prepare for weather issues in advance of the game.
If, even though you take all of these precautions, you still end up injured, there are several options for treatment. The injury is hopefully mild and heals on its own after a few days of rest. More serious injuries require a doctor visit, and one of these three treatments.
First, ice and elevate it: Keep weight off the injured area as much as possible, and elevate it with pillows. Use an ice bag wrapped in a towel to keep down swelling and inflammation. If the injury is painful, over the counter medication helps reduce discomfort.
Then, take a break: The last decision you want to make is to begin playing too soon and re-injure yourself. With more serious injuries, sitting out of a few games, or even an entire season, is a choice that promotes healing and health. Talk to your chiropractor about the timeframe the injury needs to be able to recover correctly, and follow his or her advice.
Finally, keep your chiropractic adjustments: Chiropractors are trained in treating the neuromusculoskeletal system as a whole. Many of the injuries suffered from soccer show an improvement after a few chiropractic visits.
Spinal and joint alignment, muscle healing, and tendon relaxation are all techniques chiropractors employ to promote and hasten healing. Additionally, chiropractors give insight on valuable ways to use nutrition and exercise to keep the body functioning at optimum capacity, to avoid re-injury.
Enjoying physical activity is essential to maintain a routine that provides a healthy, active lifestyle, and joining a soccer team is a great choice for children as well as adults. Knowing the advance precautions to put in place to avoid injury will help keep you strong and safe.
If, however, you or your child end up hurt, these forms of treatment will lessen healing time and get you back in the game at full speed. So give us a call to schedule your next appointment before you get back out on the pitch.
Chiropractic Treatment For Concussions
This article is copyrighted by Blogging Chiros LLC for its Doctor of Chiropractic members and may not be copied or duplicated in any manner including printed or electronic media, regardless of whether for a fee or gratis without the prior written permission of Blogging Chiros, LLC.
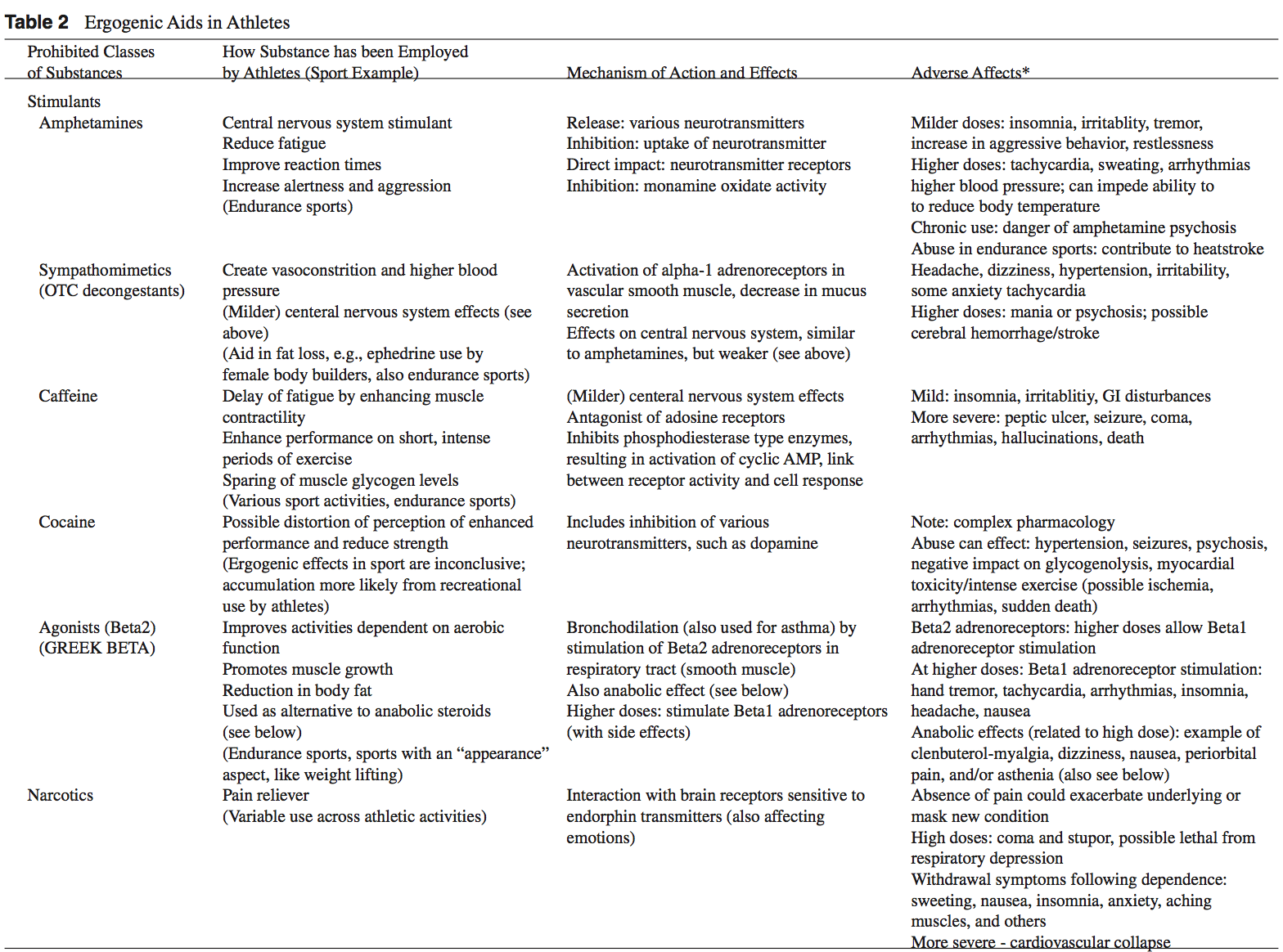
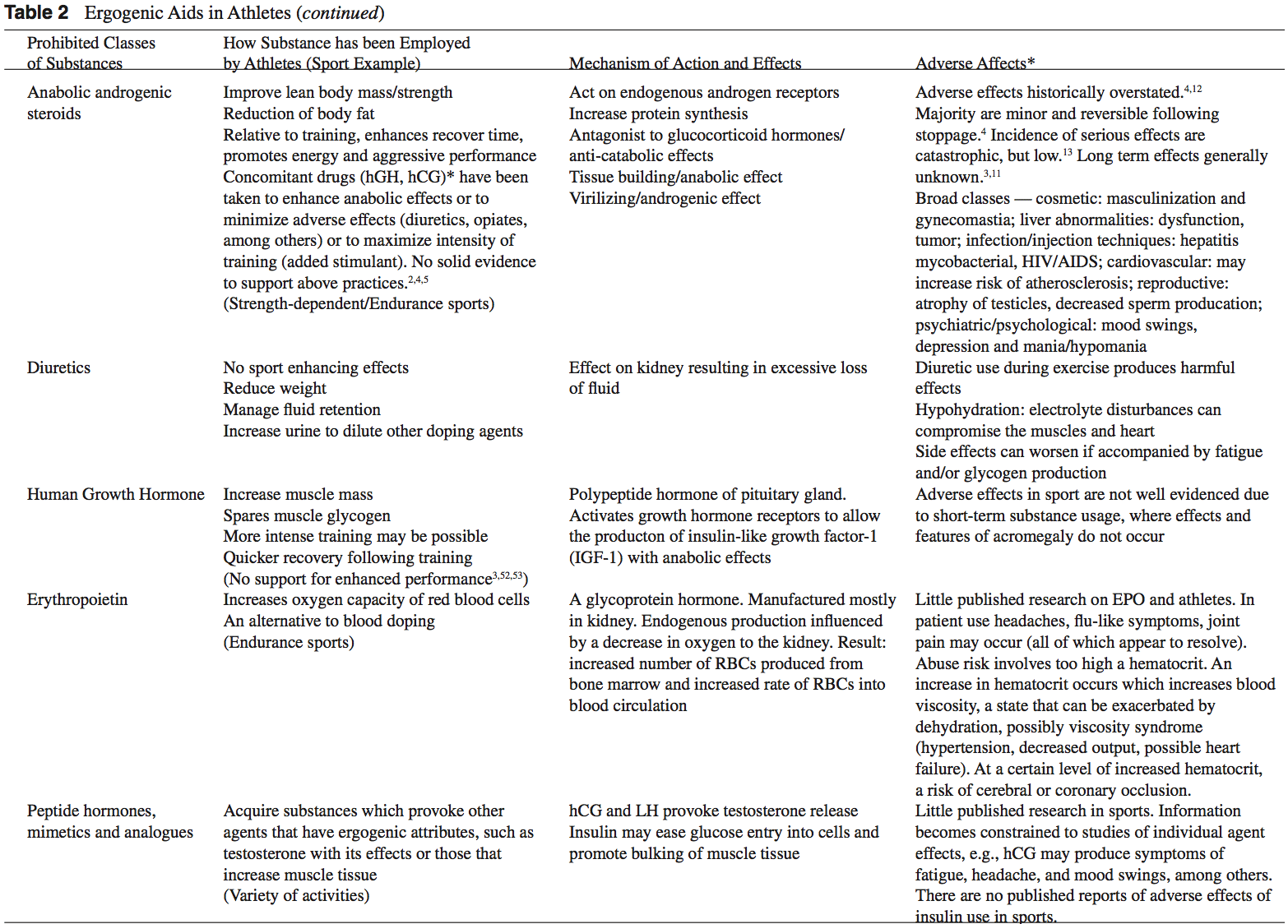
The term �ergogenic� stems from the Greek roots � �Ergon� and �genes,� meaning �work� and �born,� respectively. Any means of enhancing energy production or utilization may be described as an ergogenic aid.1 Ergogenic aids have classically been classified into five categories: mechanical, psychological, physiologic, pharmacologic, and nutritional.2 The present use of the term �ergogenic aid� usually revolves around the physiologic, pharmacologic, and nutritional categories.
While ergogenic aids have been linked to athletic �doping,� the terms are not synonymous. Doping is a term used by the International Olympic Committee (IOC) to describe the administration or use of a substance by a competing athlete with the sole intention of increasing in an artificial and unfair manner his or her performance in competition.3 Not all ergogenic aids are banned by the IOC. A partial listing of substances banned by the United States Olympic Committee is found in Table 1.2,3 Table 2 provides a list of commonly used athletic ergogenic aids.
Ergogenic Aids:
Anabolic-Androgenic Steroids
Anabolic-androgenic steroids (AAS) are testosterone derivatives that exert anabolic (tissue building) and androgenic (masculinizing) influences on the body.3 Since the discovery of the chemical structure of testosterone in 1935, attempts to separate the anabolic and androgenic effects of AAS�have been unsuccessful.3 Athletes have been using AAS since the 1940s in efforts to improve their performance.2 Concerned with widespread abuse of AAS among athletes, the IOC banned AAS use in the early 1960s.2 The Anabolic Steroids Control Act was legalized in 1990, making it a felony to possess or distribute AAS for non-medical purposes in the United States.3,4 Oral, parenteral, transdermal, and intra-nasal forms of AAS are available. The vast majority of AAS used by athletes is thought to be obtained on the �black market,� as only an estimated 10% to 15% of AAS used by athletes for performance enhancement are obtained by prescription.3
AAS are believed to exert their main effect by increasing anabolic processes and inhibiting catabolic processes via specific receptor mediated responses within the target cells.5 Effects of AAS include: the anabolic build-up of muscle mass, the androgenic development of secondary male sexual characteristics, an anti-catabolic reversal of cortisol�s action, and a direct psychological effect thought to allow a more intense and sustained workout.2,5-8 Early studies of AAS and athletes produced mixed results.5,6 More recent reviews support the notions that AAS can provide significant increases in muscle mass and strength in athletes.2,5,6 In order to maximize the effects of AAS on strength and power athletes, an adequate diet and exercise regimen is needed.5 There seems to be little advantage gained while using AAS in the untrained individual.5,9 Benefits obtained from AAS are more established in strength-dependent sports. Data supporting increased aerobic capacity and improved endurance with AAS use is limited and inconclusive.4 AAS effect on endurance sports is currently an area of great interest given the large number of endurance athletes who still use AAS.4,10
An intricate terminology describing the dosing practices of athletes has evolved. Athletes will commonly use AAS over 6 to 12 week �cycles.�4 �Pyramiding� describes a�gradual escalation in the dose of AAS taken over a cycle.2,11 �Stacking� involves the use of more than one AAS, usually with staggered cycles of the individual drugs.2-4 An �array� describes the practice of using other drugs to counteract side effects or enhance the effects of AAS.3 The practices of cycling, pyramiding, and stacking are used by athletes in an attempt to minimize the negative effects of AAS while maximizing the desired enhancements.2,4 At the current time, no solid scientific support exists for these practices.2,4,5
The adverse effects attributed to AAS abuse have been historically overstated.4,12 The majority of AAS side effects are considered minor and reversible following the cessation of use.4 While the incidence of serious side effects from AAS use has been low, devastating consequences have been reported.13 Documented fatalities from myocardial infarc- tion, stroke, and hepatocarcinoma have been attributed to AAS use.2,3 The long-term effects of AAS use are generally unknown.3,11
Dehydroepiandrosterone (DHEA)
Dehydroepiandrosterone (DHEA) is a precursor to testos- terone produced primarily in the adrenal glands.4,14 Natural sources of DHEA include wild yams. The FDA banned sale of DHEA in 1996 due to insuf cient evidence of safety and value; however, DHEA remains a legal and popular item sold as a nutritional supplement.14,15
The mechanism of action of DHEA is poorly understood but most likely revolves around the conversion of DHEA to testosterone in peripheral tissues.4,14 Preliminary studies suggest that DHEA may have a broad range of clinical uses including anti-Alzheimer and anti-Parkinson capabilities, however randomized, double-blinded clinical studies are�lacking.5
DHEA is a pre-cursor to testosterone and theoretically may enhance athletic performance in a manner similar to AAS. Investigations of DHEA use and athletic performance are scarce.14 Existing studies do not support a significant increase in lean body mass, strength, or testosterone levels with the use of DHEA in athletes.14,16-18
Long-term side effects of DHEA use are currently un- known but are probably similar to those associated with AAS use.6,14
Androstenedione
Androstenedione is a testosterone pre-cursor produced in the adrenal glands and gonads. Several professional athletes have used this substance, bringing it to national attention.2 Androstenedione is found naturally in the pollen of Scottish pine trees.19
Similar to DHEA, the mechanism of action and side ef- fects attributed to androstenedione are poorly understood and thought to be related to the conversion of androstenedione to testosterone in the peripheral tissues.5
Despite manufacturers� claims to the contrary, there is little scientific evidence of the purported ergogenic aid effects of androstenedione.2,5,16,20 Recently concerns have grown over the unfavorable alterations in blood lipid and coronary heart disease profiles seen in men using androstenedione as an ergogenic aid.2,20,21
Dietary Supplements
The increased visibility of ergogenic aids in the last de- cade has occurred primarily because of the passage of the United States Dietary Supplement Health and Education Act (DSHEA) of 1994.22 Certain vitamins, minerals, amino acids, herbs, and other botanical preparations can be classified as a �dietary supplement� under the DSHEA guidelines. Dietary supplements, as a result of DSHEA, are no longer under the direct regulatory control of the FDA. In fact, substances sold as a dietary supplement do not require FDA evaluation for safety or efficacy, and do not have to meet quality control standards expected of approved drugs.5 The content and purity of dietary supplements are not regulated and can vary widely.5,23 Since androstenedione and DHEA have been found to occur naturally in plant sources, these testosterone precursors can be labeled as �dietary supplements� and sold legally over-the-counter.
Ephedra
Dietary supplements containing Chinese ephedra, also known as Mahaung, are marketed as performance enhancers and weight-loss aids.24 Ephedra species of herb have been used for over 5,000 years for respiratory ailments.25 Currently, ephedrine alkaloids are found in hundreds of prescriptions and over-the-counter products, such as antihistamines, decongestants, and appetite suppressants.24-26 Ephedra and related ephedrine alkaloids are sympathomimetic agents that�mimic epinephrine effects.
Multiple studies of isolated ephedrine alkaloids have shown no significant enhancement of power or endurance at dosages considered to be safe.24,27-31 In contrast, the combination of caffeine with ephedrine has been associated with improvements in performance and may promote metabolic effects that are conducive to body fat loss.26,32
The actual content of ephedra alkaloids in 20 ephedra- containing dietary supplements was studied using high- performance liquid chromatography.33 Ten of the twenty supplements exhibited marked discrepancies between the label claim for ephedra content and the actual alkaloid content. Between 1995 and 1997, 926 cases of possible Mahuang toxicity were reported to the Food and Drug Ad- ministration.34 A temporal relationship between Mahuang use and severe complications including stroke, myocardial infarction, and sudden death was established in 37 of the 926 cases. In 36 of these 37 cases, the Mahuang use was reported to be within the manufacturers� dosing guidelines.
Ephedra and related ephedrine alkaloids are currently banned by the U.S.O.C. and cannot be recommended for general use given their association with potentially life- threatening side effects.2,34
Creatine
Creatine use in athletes has grown as a result of a 1992 study that showed that creatine supplementation produced a 20% increase in skeletal muscle creatine concentration.2,35 In the phosphorylated form, creatine serves as an energy substrate that contributes to adenosine triphosphate (ATP) re-synthesis during high-intensity exercise.36 Creatine re- mains popular with power and resistance athletes as it is thought to produce increases in strength, muscle mass, and to delay fatigue.2,14,36
Creatine is synthesized from amino acids primarily in the liver, pancreas, and kidney and is excreted by the kidneys. Creatine is found in skeletal muscle, cardiac muscle, brain, retinal, and testicular tissues.2,37 The interest in creatine as an ergogenic aid revolves around its ability to participate as an energy substrate for muscle contraction.14 Creatine, which easily binds phosphorus, can act as a substrate to donate phosphorus for the formation of ATP. Furthermore, creatine-phosphate (PCr) can help buffer lactic acid because hydrogen ions are used when ATP is regenerated.14,36,38 This role of creatine in exercise is governed by the following reaction:
Normally PCr stores deplete within 10 seconds of short, high-intensity exercise.14,39 Increasing the level of PCr in skeletal muscle, in theory, should result in the ability to sustain high-power output longer and lead to a greater re-synthesis of PCr after exercise.14 The beneficial effects of creatine in response to resistance training are most likely mediated by the following sequence: increased muscle creatine concentration, increased training intensity, which lead to an enhanced physiologic adaptation to training with increased muscle mass and strength.36
Studies evaluating the effectiveness of creatine as an er- gogenic aid are mixed.2,36,40 Multiple reports do conclude that short-term creatine supplementation signi cantly enhances the ability to maintain muscular force and power output dur- ing high-intensity exercise.2,36,41,42 Data on results of creatine supplementation with highly trained athletes is inconclusive. While some papers report improvements with creatine use in highly trained individuals with regards to high-intensity exercise, many show no improvements.2,36,43
Most investigators agree that creatine supplementation does not seem to enhance aerobic-oriented activities.2,36,44
Human muscle is thought to have a maximum concen- tration of creatine that it can hold.14,45 There appears to be no additional bene ts of increasing creatine supplementa- tion above this storage capacity of muscle as the excess is simply excreted by the kidneys.2,46 Humans have differing baseline levels of muscle creatine.14 Accordingly, athletes with lower baseline levels of creatine may be more sensi- tive to creatine supplementation than those with a relatively higher baseline creatine level.14,36 The terms �responder� and �nonresponder� have been used to describe two groups of athletes: those with relatively low baseline creatine levels that may show signi cant performance enhancement with creatine supplementation, and those with high baseline creatine levels that do not show marked improvements with creatine supplementation.14,36,47 These differences in creatine concentrations are thought to play a signi cant role in the varied results on performance found in the literature examin- ing creatine supplementation.14
Reported side effects from creatine use have been scarce.2,14 The major reported side effect associated with creatine use is weight gain, which is thought to be primarily a result of water retention.2,14,48 Some reported longer-term side effects include dehydration, muscle cramping, nausea, and seizures.2,49 Given the relative lack of studies, caution still remains about the long-term effects of creatine usage.14 As creatine use among younger athletes continues to increase, concern is growing over the lack of studies that examine the possible side effects speci c to this age group.14,38
Human Growth Hormone
Human growth hormone (hGH) is a polypeptide produced in the anterior pituitary gland. After its release from the pituitary, hGH can exert its effect in all cells of the body via tissue specific receptors. Human growth hormone is shown to promote protein anabolism, carbohydrate tolerance, lipolysis, natriuresis, and bone and connective tissue turnover.4,50
Potential benefits of hGH abuse in athletes revolve around�its anabolic effect on the body.4 Human growth hormone is thought to increase muscle mass, and spare muscle glycogen by stimulating lipolysis during exercise.2,3 The popularity of hGH among athletes is furthered by the fact that hGH re- mains extremely difficult to detect by current drug screening processes.3,51 Human growth hormone may be particularly attractive to female athletes as the virilization side effects associated with AAS use are not thought to occur with hGH.4
There are no studies that demonstrate signi cant increases in athletic performance with the use of hGH.3,52,53 Neither human or animal studies show any signi cant strength gains with supplemental hGH use in non-de cient individuals.4 The abuse of hGH is thought to be increasing despite the lack of scienti c evidence linking hGH to improved athlete performance.3,52 A survey of high school males revealed that as many as 5% reported past or present use of hGH.54 The purity of hGH abused by athletes may be poor as Drug Enforcement Agency estimates project that up to 30% to 50% of the hGH products sold are phony.4,55
Adverse effects of exogenous hGH use are extrapolated from the ndings seen in patients with endogenous over- secretion of hGH.2 Adults with high levels of hGH are at risk for the clinical syndrome of acromegaly. Medical complications associated with acromegaly include: diabetes, hypertension, coronary heart disease, cardiomyopathy, men- strual irregularities, and osteoporosis.2,4 High levels of hGH in individuals with open physis may lead to gigantism.2
Erythropoietin (EPO)
Recombinant EPO (r-EPO) was approved by the FDA for manufacture in 1989 after the EPO gene was cloned in 1985.14 Since its approval, r-EPO has been abused for athletic personal gain as an alternative to blood doping.3,14 Recombinant EPO has largely replaced the practice of blood doping, as r-EPO produces a dose-dependent increase in hematocrit.2 In theory, r-EPO should provide all of the benefits of blood doping without the risks involved in blood transfusion.3
There are few studies evaluating the use of r-EPO in healthy athletes; however, numerous studies have shown a signi cant increase in work capacity due to r-EPO use in patients with renal disease.14 Berglund and Ekblom reported an increased maximal oxygen consumption and increased time to exhaustion in male athletes after a 6 week trial of r-EPO.56
The risks associated with r-EPO abuse involve the potential for dangerously high hematocrit levels.14 A resulting hyperviscosity syndrome may lead to a decreased cardiac output, hypertension, and potential heart failure.3 Further- more, thrombosis could be manifest as myocardial infarction, pulmonary embolism, or cerebrovascular accidents.2,3 Although the use of r-EPO has been banned by the IOC since 1990, its use is extremely difficult to detect with current drug screening measures.2,14
Antioxidants
The antioxidant capabilities of certain vitamins are believed by many to counter-act the production of free-radials that occurs during exercise.14 Most of the research to date involves vitamin E, vitamin C, and beta carotene.2 The existing literature does not support the notion that antioxidants have significant ergogenic capabilities.2,14,57 There are currently no recommendations for antioxidant use in athletes that exceeds the normal adult recommended daily allowance (RDA).
Beta-Hydroxy-Beta-Methylbutyrate
Beta-hydroxy-beta-methylbutyrate (HMB) is a metabolite of the branched-chain amino acid leucine. HMB is theorized to inhibit muscle breakdown during strenuous exercise but its exact mechanism of action remains unknown.14,58 Studies show that HMB supplementation may significantly lower serum lactate dehydrogenase (LDH), lower serum creatine phosphokinase (CPK) levels and delay blood lactate accumulation after endurance training compared to placebo.59,60 Furthermore, short-term HMB use has been shown to significantly increase strength gains with resistance-exercised training over placebo in one double-blinded study.61
HMB is a relatively new ergogenic aid and published results are considered preliminary.14,58 Although there is evidence for a potential ergogenic aid advantage with HMB use in resistance and endurance training, its use can not be recommended until more studies are performed and potential side effects are elicited.
Caffeine
Caffeine is a methylxanthine occurring naturally in many species of plants. Caffeine is thought to work through a variety of mechanisms. The central nervous system effect of caffeine is probably the result of adrenergic receptor antagonism.3 Its use by athletes stems from the theory that caffeine may delay fatigue by enhancing skeletal muscle contractility and spare muscle glycogen levels by enhancing fat metabolism.6 Multiple studies have reported an improved endurance time with caffeine use.6,62,63 There is evidence that caffeine use may enhance performance with more intense short-duration exercise as well.2 The caffeine dosages most associated with an ergogenic effect range in the literature from 3 to 9 mg per kilogram of body weight.2,6
Side effects associated with caffeine use include anxiety, diuresis, insomnia, irritability and gastrointestinal discom- fort.2,6 Higher doses of caffeine ingestion can lead to more serious consequences such as cardiac arrhythmia, hallucina- tions, and even death.2,3
The legal urine level of caffeine for athletes is 12 ?g/ml (IOC standards) and 15 ?g/ml (National Collegiate Athletics Association standards).6 An athlete would need to drink six to eight cups of coffee in one sitting and be tested within 2 to 3 hours to reach urine levels over the IOC legal limit.3 The amount of caffeine needed to produce ergogenic benefits is potentially far less than that required to exceed the athletic�legal limit.3
Ergogenic Aids: Summary
Claims championing exotic substances that produce healing or ergogenic powers have been around for centuries. The�competitive, peer-pressured environment enveloping today�s athletes and adolescences makes these groups particularly susceptible to the uproar surrounding the current ergogenic aid market. Presently, it seems that rumor and anecdotal information overwhelms the available scientific data. While there is evidence that some touted ergogenic aids do indeed enhance performance, there are many unanswered questions about product safety, efficacy, and long-term consequences. A working knowledge of specific ergogenic aids is essential for the treating physician in order to best advise patients and athletes as to the possible benefits and risks of any substance they may be using.
By Adam Bernstein, M.D., Jordan Safirstein, M.D., and Jeffrey E. Rosen, M.D.
Americans’ Perception Of Chiropractic
Blank
References
1. Williams MH: Ergogenic and ergolytic substances. Med Sci
Sports Exerc 24(9 Suppl):S344-S348, 1992.
2. Silver MD: Use of ergogenic aids by athletes. J Am Acad
Orthop Surg 9(1):61-70, 2001.
3. KnoppWD,WangTW,Bach JrBR: Ergogenic drugsin sports.
Clin Sports Med 16(3):375-392, 1997.
4. Sturmi JE, Diorio DJ: Anabolic agents. Clin Sports Med
17(2):261-282, 1998.
5. Blue JG, Lombardo JA: Steroids and steroid-like compounds.
Clin Sports Med 18(3):667-689, 1999.
6. Ahrendt DM: Ergogenic aids: counseling the athlete.Am Fam
Physician 63(5):913-922, 2001.
7. Adolescents and anabolic steroids:A subjectreview.American
Academy of Pediatrics. Committee on Sports Medicine and
Fitness. Pediatrics 99(6):904-908, 1997.
8. Haupt HA: Anabolic steroids and growth hormone. Am J
Sports Med 21(3):468-474, 1993.
9. Kuipers H, et al: Influence of anabolic steroids on body composition,
blood pressure, lipid profile and liver functions in
body builders. Int J Sports Med 12(4):413-418, 1991.
10. Lombardo JA: Medical and performance-enhancing effects
of anabolic steroids. Psychiatr Ann 22:19-23, 1992.
11. YesalisCE,Bahrke MS:Anabolic-androgenic steroids: current
issues. Sports Med 19(5):326-340, 1995.
12. Friedl KE: Effects of anabolic steroids on physical health.
In:Yesalis CE (ed): Anabolic Steroids in Sports and Exercise
(2nd ed). Champaign, IL: Human Kinetics Publishers, Inc.,
2000, pp. 35-48.
13. Bahrke MS, Yesalis CE, Brower KJ: Anabolic-androgenic
steroid abuse and performance-enhancing drugs among adolescents.
Child Adolesc Psychiatr Clin N Am 7(4):821-838,
1998.
14. Stricker PR: Other ergogenic agents. Clin Sports Med
17(2):283-297, 1998.
15. Dehydroepiandrosterone (DHEA). Med Lett Drugs Ther
38(985):91-92, 1996.
16. Wallace MB, et al: Effects of dehydroepiandrosterone vs
androstenedione supplementation in men. Med Sci Sports
Exerc 31(12):1788-1792, 1999.
17. Nestler JE, et al: Dehydroepiandrosterone reduces serum
low density lipoprotein levels and body fat but does not alter
insulin sensitivity in normal men. J Clin Endocrinol Metab
66(1):57-61, 1988.
18. Welle S,Jozefowicz R, Statt M: Failure of dehydroepiandrosterone
to influence energy and protein metabolism in humans.
J Clin Endocrinol Metab 71(5):1259-1264, 1990.
19. Saden-Krehula M, Tajic M, Kolbah D: Testosterone, epitestosterone
and androstenedione in the pollen of Scotch pine
P. silvestris L. Experientia 27(1):108-109, 1971.
20. King DS, et al: Effect of oral androstenedione on serum testosterone
and adaptationsto resistance training in young men:
a randomized controlled trial.JAm MedAssoc 281(21):2020-
2028, 1999.
21. Broeder CE, et al: The Andro Project: physiological and
hormonal influences of androstenedione supplementation in
men 35 to 65 years old participating in a high-intensity resistance
training program.Arch Intern Med 160(20):3093-3104,
2000.
22. Benning JR: Nutrition for exercise and sports performance. In:
Mahan LK (ed): Krause�s Food, Nutrition and Diet Therapy.
Philadephia: W.B. Saunders Co., 2000, pp. 534-557.
23. SkolnickAA: Scientific verdictstill out on DHEA.JAm Med
Assoc 276(17):1365-1367, 1996.
24. Bucci LR: Selected herbals and human exercise performance.
Am J Clin Nutr 72(2 Suppl):624S-636S, 2000.
25. Anonymous: The Ephedras. Lawrence Rev Nat Prod, 1989.
26. DiPasquale M: Stimulants and adaptogens: Part I. Drug Sports
1:2-6, 1992.
27. Sidney KH, Lefcoe NM: The effects of ephedrine on the
physiological and psychological responsesto submaximal and
maximal exercise in man. Med Sci Sports 9(2):95-99, 1977.
28. Bright TP, Sandage Jr BW, Fletcher HP: Selected cardiac and
metabolic responsesto pseudoephedrine with exercise.J Clin
Pharmacol 21(11-12):488-492, 1981.
29. DeMeersman R, Getty D, Schaefer DC: Sympathomimetics
and exercise enhancement: all in the mind? Pharmacol Biochem
Behav 28(3):361-365, 1987.
30. SwainRA, et al: Do pseudoephedrine or phenylpropanolamine
improve maximum oxygen uptake and time to exhaustion?
Clin J Sport Med 7(3):168-173, 1997.
31. Gillies H, et al: Pseudoephedrine is without ergogenic effects
during prolonged exercise. J Appl Physiol 81(6):2611-2617,
1996.
32. Bell DG, Jacobs I, Zamecnik J: Effects of caffeine, ephedrine
and their combination on time to exhaustion during
high-intensity exercise. Eur J Appl Physiol Occup Physiol
77(5):427-433, 1998.
33. Gurley BJ, Gardner SF, Hubbard MA: Content versus label
claims in ephedra-containing dietary supplements. Am J
Health Syst Pharm 57(10):963-969, 2000.
34. Samenuk D, et al: Adverse cardiovascular events temporally
associated with ma huang, an herbal source of ephedrine.
Mayo Clin Proc 77(1):12-16, 2002.
35. Juhn MS: Orla creatine supplementation: Separating fact from
hype. Phys Sportsmed 27:47-56, 1999.
36. Kraemer WJ, Volek JS: Creatine supplementation: Its role in
human performance. Clin Sports Med 18(3):651-666, 1999.
37. Williams MH: The use of nutritional ergogenic aidsin sports:
is it an ethical issue? Int J Sport Nutr 4(2):120-131, 1994.
38. MetzlJD, et al: Creatine use among young athletes. Pediatrics
108(2):421-425, 2001.
39. Spriet LL: Ergogenic aids: recent advances and retreats. In:
Lamb DR, Murray R (eds): Perspectives in Exercise Science
and Sports Medicine. Indianapolis, IN: Benchmark Press,
1998, pp. 185-238.
40. Johnson WA, Landry GL: Nutritional supplements: fact vs.
fiction. Adolesc Med 9(3):501-513, 1998.
41. Williams MH, Branch JD: Creatine supplementation and
exercise performance: an update. J Am Coll Nutr 17(3):216-
234, 1998.
42. Mujika I, Padilla S: Creatine supplementation as an ergogenic
aid forsports performance in highly trained athletes: a critical
review. Int J Sports Med 18(7):491-496, 1997.
43. Kreider RB, et al: Effects of creatine supplementation on body
composition,strength, and sprint performance. Med Sci Sports
Exerc 30(1):73-82, 1998.
44. Balsom PD, et al: Creatine supplementation per se does not
enhance endurance exercise performance.Acta Physiol Scand
149(4):521-523, 1993.
45. Harris RC, Soderlund K, Hultman E: Elevation of creatine in
resting and exercised muscle of normal subjects by creatine
supplementation. Clin Sci (Lond) 83(3):367-374, 1992.
46. Clark JF: Creatine: A review of its nutritional applications in
sport. Nutrition 14(3):322-324, 1998.
47. Casey A, et al: Creatine ingestion favorably affects performance
and muscle metabolism during maximal exercise in
humans. Am J Physiol 271(1):E31-E37, 1996.
48. Volek JS: Creatine supplementation: its effect on human
muscular performance and body composition.J Strength Cond
Res 10:200-210, 1996.
49. Feldman EB: Creatine: a dietary supplement and ergogenic
aid. Nutr Rev 57(2):45-50, 1999.
50. Yarasheski KE: Growth hormone effects on metabolism, body
composition, muscle mass, and strength. Exerc Sport Sci Rev
22:285-312. 1994.
51. Risser WL: Sports medicine. Pediatr Rev 14(11):424-431,
1993.
52. Bidlingmaier M, Wu Z, Strasburger CJ: Doping with growth
hormone. J Pediatr Endocrinol Metab 14(8):1077-1083,
2001.
53. Jenkins PJ: Growth hormone and exercise: physiology, use and
abuse. Growth Horm IGF Res 11(Suppl A):S71-S77, 2001.
54. Rickert VI, et al: Human growth hormone: a new substance
of abuse among adolescents? Clin Pediatr (Phila) 31(12):723-
726, 1992.
55. Council Report: Drug abuse in athletes, anabolic steroids and
human growth hormone. J Am Med Assoc 259:1703-1705,
1988.
56. Berglund B, Ekblom B: Effect of recombinant human erythropoietin
treatment on blood pressure and some haematological
parameters in healthy men. J Intern Med 229(2):125-130,
1991.
57. Williams MH: Nutritional supplements for strength trained
athletes. Sports Sci Exchange 6:1-6, 1993.
58. Williams MH: Facts and fallacies of purported ergogenic
amino acid supplements. Clin Sports Med 18(3):633-649,
1999.
59. Vukovich MD, Dreifort GD: Effect of beta-hydroxy betamethylbutyrate
on the onset of blood lactate accumulation
and VO2 peak in endurance-trained cyclists. J Strength Cond
Res 15(4):491-497, 2001.
60. Knitter AE, et al: Effects of beta-hydroxy-beta-methylbutyrate
on muscle damage after a prolonged run. J Appl Physiol
89(4):1340-1344, 2000.
61. Jowko E, et al: Creatine and beta-hydroxy-beta-methylbutyrate
(HMB) additively increase lean body mass and muscle
strength during a weight-training program. Nutrition 17(7-
8):558-566, 2001.
62. Graham TE, Spriet LL: Performance and metabolic responses
to a high caffeine dose during prolonged exercise. J Appl
Physiol 71(6):2292-2298, 1991.
63. KalmarJM, Cafarelli E: Effects of caffeine on neuromuscular
function. J Appl Physiol 87(2):801-808, 1999.
Chiropractor, Dr. Alex Jimenez looks at lumbar spine disc herniation. What are the Likely signs and symptoms associated with disc herniation, and what would be the selection criteria for micro-discectomy operation in athletes? Complaint in the young college age athlete and professional athlete, and it’s been estimated that over 30% of athletes complain of back pain at least once in the profession(1).
Lumbar spinal disc herniation is one kind Of lumbar injury that can’t just cause painful low back pain, but can also compress nerve roots and create radicular referral of pain into the lower leg with related sensation changes and muscle contraction. This injury will not only influence the short-term opponent ability of the athlete, but might also reoccur and eventually become persistent possibly causing a career ending injury.
Managing disc herniation from the athlete Usually begins with conservative therapy and if this fails, surgical solutions are considered. But often elite athletes will request a quicker resolution to their symptoms to minimize time away from competitors. Therefore, providing the criteria for lumbar spine surgery are suggested, the conservative period will often be compressed, and surgery will be sought earlier. The favored surgical process for the athlete with a disc herniation is that the lumbar disc micro-discectomy.
Anatomy & Biomechanics
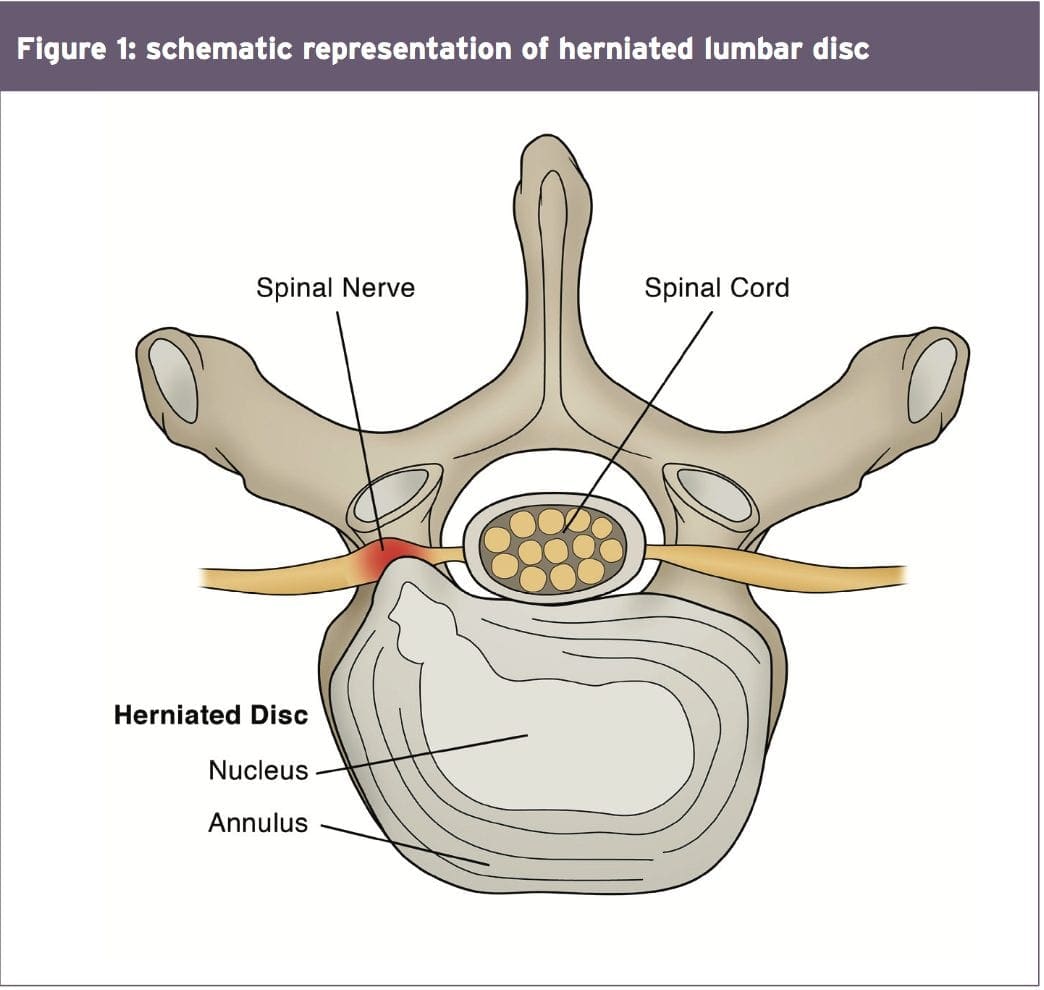
A significant biomechanical role in the spine, allowing for motion between the spinal segments while spreading compressive, shear, and torsional forces(2). These discs include a thick outer ring of fibrous cartilage termed the annulus fibrosis (akin to the onion rings enclosing the center of the onion), which encompasses a more gelatinous core called the nucleus pulposus, which is included within the cartilage end plates inferiorly and superiorly.
The intervertebral disc consists of Cells and substances such as collagen, proteoglycans, and thin fibrochondrocytic tissues, which enable transmission and absorption of forces arising from body weight and muscle activity. To do so, the disc depends mainly on the structural condition of the nucleus pulposus, annulus fibrosis and the vertebra lend plate. If the disc is normal and is functioning optimally, then forces are spread across the disc evenly(3).
But disc degeneration (mobile Degradation, lack of hydration( disc failure) may decrease the capacity of the disc to withstand extrinsic forces, as forces are no longer distributed and spread evenly. Tears and fissures from the annulus can lead, and with adequate external forces, the disc material may herniate. Alternatively, a sizable biomechanical force set on a healthy, ordinary disc may cause extrusion of disc material as a result of crushing failure of this annular fibers — illustrations include a hefty compression type mechanism because of a fall on the tailbone, or strong muscle contraction such as heavy weight lifting(4).
Herniations represent protrusions of Disc material beyond the confines of this annular lining and in the spinal canal (see Figure 1)(5). If the protrusion does not invade the canal or undermine nerve roots then back pain may be the only symptom.
Endoscopic Discectomy 3D Simulation
The pain associated with lumbar Radiculopathy happens due to a mix of nerve root ischemia (due to compression) and inflammation (because of neurochemical inflammatory mediators released from the disc). Throughout a herniation, the nucleus pulposus puts pressure on weakened regions of the annulus, and proceeds through the diminished websites in the annulus in which it ultimately forms a herniation(6 ft). It follows from this that some kind of disc degeneration may exist prior to the disc may really herniated(7).
In contrast to other respiratory Tissues, discs have a inclination to degenerate earlier in life, with some studies demonstrating adolescents presenting signs of degeneration between the ages of 11 to 16(8). With increasing age, there’s further degeneration of the intervertebral discs.
While the disc might be in danger of harm in All fundamental planes of motion, it’s particularly susceptible during repetitive flexion, or hyper-flexion, combined with lateral bending or rotation(10). Traumatic events such as excessive axial compression may also damage the inner structure of the disc. This can occur as a result of a fall or powerful muscular forces developed during tasks such as heavy lifting.
Athletes are generally exposed to high loading conditions. Examples of this include:
1. World-class power lifters, in which the calculated compressive loads on the backbone are involving 18800 Newtons (N) and also 36400N acting in the L3-4 motion segment(11).
2. Elite level football linesmen who have Been proven to present time-related hypertrophy of this disc and changes in vertebrae endplate in response to this repetitive high loading and axial pressure(12).
3. Long distance runners have been Shown to undergo significant strain into the intervertebral disc, indicated by a reduction in disc height(13).
Herniations could be classified depending on Ultimately, herniations are also identified based on level, with most herniations happening at the L4/5 and L5/S1 intervertebral disc level; these can then in turn affect the L5 and S1 nerve roots resulting in clinical sciatica(15). Upper level herniations are less common, and when they do occur with radiculopathy, they will affect the femoral nerve. Finally, the prevalence of disc injury rises increasingly caudally, with the best numbers at the L5/S1 degrees(16).
Herniation In Athletes
The offending movements implicated in The 20-35 age group are the most common group to herniate a disc, most likely because of the fluid nature of the nucleus pulposis and due to behavior(18). This age group are more likely to participate in sports which need high lots of flexion and spinning or are reckless with their positions and positions during loading.
The sports most at risk of disc herniation are:
Hockey
Wrestling
Soccer
Swimming
Basketball
Golf
Tennis
Weightlifting
Rowing
Throwing events
These are the sports that involve either significant Furthermore, those who take part in more and more severe training regimes seem to be at higher risk of spinal pathologies, as do people involved in sports.
Signs & Symptoms Indicating Discectomy
The efficacy of management programs for lumbar spine disc herniation — in terms of the decision to operate or treat conservatively — will be discussed in greater depth in part 2 of this series. However, the decision to operate within an athlete is generally driven by the motivation and approaching goals the athlete has put themselves. They may in fact favor a comparatively simple micro-discectomy instead of waiting for symptoms to abate through an extended period of rehabilitation.
This conservative period of Management may involve medicine therapy, epidural injections, relative back and back muscle recovery, acupuncture, osteo/chiropractic interventions. On the other hand, the normal presenting symptoms and signs that suggest a substantial disc herniation that will require surgical intervention in the athlete comprise:
Low back pain with pain radiating down one or both legs
Positive straight leg raise test
Radicular pain and neurological signs consistent with the nerve root level affected
Mild weakness of distal muscles such as extensor hallucis longus, peroneals, tibialis anterior and soleus. These would fit with the myotome relevant for the disc level
MRI confirming a disc herniation
Possible bladder and bowel symptoms
Failed conservative rehabilitation
Time span in which to enable conservative rehabilitation to be effective. In the overall population, medical practitioners will most likely prescribe a minimal 6-week traditional period of treatment with an overview at 6 weeks as to whether to expand the rehabilitation a further 6 weeks or to seek a specialist opinion. The expert may then attempt more medically orientated interventions such as epidural injections.
The athlete nevertheless will have these They might be more inclined to experience an epidural very early in the conservative period to assess the effectiveness of this procedure. If no signs of progress are evident in a couple of weeks then they may choose to get an immediate lumbar spine micro- discectomy.
Endoscopic Lumbar Discectomy
Local Doctor performs lumbar discectomy using minimally invasive techniques. From the El Paso, TX. Spine Center.
Imaging
MRI remains the favored system of Identifying lumbar spine disc herniation, since it’s also very sensitive to detecting nerve root impingements(23). However, abnormal MRI scans can occur in otherwise asymptomatic patients(25); hence, clinical correlation is always essential before any surgical thought. What’s more, patients can present with clinical signs and symptoms which suggest the diagnosis of acute herniated disc, and yet lack evidence of sufficient pathology on MRI to warrant operation.
Therefore it has been proposed that a Volumetric analysis of a herniated disc on MRI may be potentially beneficial in checking the suitability for operation. Several writers have previously mentioned the possible value of volumetric evaluation of herniated disc on MRI as part of their selection criteria for lumbar surgery(26).
In a survey conducted in Michigan State University, it was found that the size and positioning of the herniated disc determined that the likelihood for operation with what researchers called ‘types 2-B’ and ‘types 2-AB’ being the most likely candidates for surgery(27).
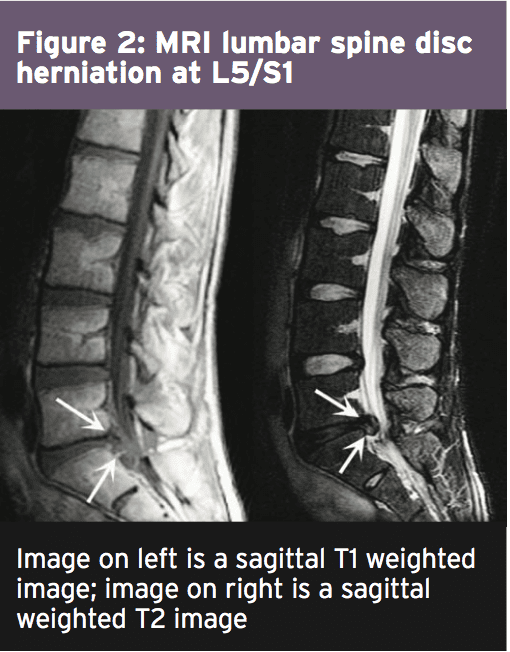
The MRI protocol to your lumbar spine consists of (see Figure 2)
1.Sagittal plane echo T1- weighted sequence
2. Sagittal fast spin echo proton density sequence
3. Sagittal fast spin echo inversion recovery sequence
4.Axial spin echo T1- weighted sequence
Summary
Disc herniations are not a common Complaint in athletes, but they do happen in sports which involve high loads or repetitive flexion and rotation movements. Sufferers of a disc herniation will normally feel focused low-back pain, maybe with referral in the lower limb with associated neurological symptoms if the nerve root was compressed.
Managing a disc herniation within an General population as frequently the risk of a Protracted failed rehabilitation period is Bypassed for the protected and low risk Micro-discectomy procedure. In the Discuss the exact surgical alternatives involved Observing a lumbar spine micro-discectomy.
References
1. Sports Med. 1996;21(4):313�20
2. Radiology. Oct 2007;245(1):62-77
3. Arthritis Research & Therapy. 2003;5(3):120-30
4. The Journal of Bone and Joint Surgery. American volume. Feb 2004;86-A(2):382 � 96
5. Radiology. Oct 2007;245(1):43-61
6. Spine. Sep 15 1996;21(18):2149-55
7. Spine. May-Jun 1982;7(3):184-91
8. Spine. Dec 1 2002;27(23):2631-44
9. Lancet 1986;2:1366�7
10. Disease-A-Month:DM. Dec 2004;50(12):636-69
11. Spine. Mar 1987;12(2):146-9
12. The American Journal of Sports Medicine. Sep 2004;32(6):1434-9
13. The Journal of International Medical Research. 2011;39(2):569-79
14. Spine. 2001;26:E93-113
15. Spine. 1990;15:679-82
16. British Journal of Sports Medicine. Jun 2003;37(3):263-6
17. Prim Care. 2005;32(1):201�29
18. McGill, S.M. Low back disorders: Evidence based prevention and rehabilitation, Human Kinetics Publishers, Champaign, IL, U.S.A., 2002. Second Edition, 2007
19. Spine. Apr 1991;16(4):437-43
20. Skeletal radiology. Jul 2006;35(7):503-9
21. British Journal of Sports Medicine. Nov 2007;41(11):836-41
22. The American Journal of Sports Medicine. Jun 2009;37(6):1208-13
23. Spine. Mar 15 1995;20(6):699-709
24. Phys Sportsmed. 2005;33(4):21�7
25. J Bone Joint Surg Am 1990 . 2:403�408
26. J Orthop Surg (Hong Kong) 2001. 9:1�7
27. Eur Spine J (2010) 19:1087�1093
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine














 Anabolic-Androgenic Steroids
Anabolic-Androgenic Steroids Anabolic-androgenic steroids (AAS) are testosterone derivatives that exert anabolic (tissue building) and androgenic (masculinizing) influences on the body.3 Since the discovery of the chemical structure of testosterone in 1935, attempts to separate the anabolic and androgenic effects of AAS�have been unsuccessful.3
Anabolic-androgenic steroids (AAS) are testosterone derivatives that exert anabolic (tissue building) and androgenic (masculinizing) influences on the body.3 Since the discovery of the chemical structure of testosterone in 1935, attempts to separate the anabolic and androgenic effects of AAS�have been unsuccessful.3  Dehydroepiandrosterone (DHEA) is a precursor to testos- terone produced primarily in the adrenal glands.4,14 Natural sources of DHEA include wild yams. The FDA banned sale of DHEA in 1996 due to insuf cient evidence of safety and value; however, DHEA remains a legal and popular item sold as a nutritional supplement.14,15
Dehydroepiandrosterone (DHEA) is a precursor to testos- terone produced primarily in the adrenal glands.4,14 Natural sources of DHEA include wild yams. The FDA banned sale of DHEA in 1996 due to insuf cient evidence of safety and value; however, DHEA remains a legal and popular item sold as a nutritional supplement.14,15 Androstenedione is a testosterone pre-cursor produced in the adrenal glands and gonads. Several professional athletes have used this substance, bringing it to national attention.2 Androstenedione is found naturally in the pollen of Scottish pine trees.19
Androstenedione is a testosterone pre-cursor produced in the adrenal glands and gonads. Several professional athletes have used this substance, bringing it to national attention.2 Androstenedione is found naturally in the pollen of Scottish pine trees.19 The increased visibility of ergogenic aids in the last de- cade has occurred primarily because of the passage of the United States Dietary Supplement Health and Education Act (DSHEA) of 1994.22 Certain vitamins, minerals, amino acids, herbs, and other botanical preparations can be classified as a �dietary supplement� under the DSHEA guidelines. Dietary supplements, as a result of DSHEA, are no longer under the direct regulatory control of the FDA. In fact, substances sold as a dietary supplement do not require FDA evaluation for safety or efficacy, and do not have to meet quality control standards expected of approved drugs.5 The content and purity of dietary supplements are not regulated and can vary widely.5,23 Since androstenedione and DHEA have been found to occur naturally in plant sources, these testosterone precursors can be labeled as �dietary supplements� and sold legally over-the-counter.
The increased visibility of ergogenic aids in the last de- cade has occurred primarily because of the passage of the United States Dietary Supplement Health and Education Act (DSHEA) of 1994.22 Certain vitamins, minerals, amino acids, herbs, and other botanical preparations can be classified as a �dietary supplement� under the DSHEA guidelines. Dietary supplements, as a result of DSHEA, are no longer under the direct regulatory control of the FDA. In fact, substances sold as a dietary supplement do not require FDA evaluation for safety or efficacy, and do not have to meet quality control standards expected of approved drugs.5 The content and purity of dietary supplements are not regulated and can vary widely.5,23 Since androstenedione and DHEA have been found to occur naturally in plant sources, these testosterone precursors can be labeled as �dietary supplements� and sold legally over-the-counter. Dietary supplements containing Chinese ephedra, also known as Mahaung, are marketed as performance enhancers and weight-loss aids.24 Ephedra species of herb have been used for over 5,000 years for respiratory ailments.25 Currently, ephedrine alkaloids are found in hundreds of prescriptions and over-the-counter products, such as antihistamines, decongestants, and appetite suppressants.24-26 Ephedra and related ephedrine alkaloids are sympathomimetic agents that�mimic epinephrine effects.
Dietary supplements containing Chinese ephedra, also known as Mahaung, are marketed as performance enhancers and weight-loss aids.24 Ephedra species of herb have been used for over 5,000 years for respiratory ailments.25 Currently, ephedrine alkaloids are found in hundreds of prescriptions and over-the-counter products, such as antihistamines, decongestants, and appetite suppressants.24-26 Ephedra and related ephedrine alkaloids are sympathomimetic agents that�mimic epinephrine effects. Creatine use in athletes has grown as a result of a 1992 study that showed that creatine supplementation produced a 20% increase in skeletal muscle creatine concentration.2,35 In the phosphorylated form, creatine serves as an energy substrate that contributes to adenosine triphosphate (ATP) re-synthesis during high-intensity exercise.36 Creatine re- mains popular with power and resistance athletes as it is thought to produce increases in strength, muscle mass, and to delay fatigue.2,14,36
Creatine use in athletes has grown as a result of a 1992 study that showed that creatine supplementation produced a 20% increase in skeletal muscle creatine concentration.2,35 In the phosphorylated form, creatine serves as an energy substrate that contributes to adenosine triphosphate (ATP) re-synthesis during high-intensity exercise.36 Creatine re- mains popular with power and resistance athletes as it is thought to produce increases in strength, muscle mass, and to delay fatigue.2,14,36 Human growth hormone (hGH) is a polypeptide produced in the anterior pituitary gland. After its release from the pituitary, hGH can exert its effect in all cells of the body via tissue specific receptors. Human growth hormone is shown to promote protein anabolism, carbohydrate tolerance, lipolysis, natriuresis, and bone and connective tissue turnover.4,50
Human growth hormone (hGH) is a polypeptide produced in the anterior pituitary gland. After its release from the pituitary, hGH can exert its effect in all cells of the body via tissue specific receptors. Human growth hormone is shown to promote protein anabolism, carbohydrate tolerance, lipolysis, natriuresis, and bone and connective tissue turnover.4,50 Recombinant EPO (r-EPO) was approved by the FDA for manufacture in 1989 after the EPO gene was cloned in 1985.14 Since its approval, r-EPO has been abused for athletic personal gain as an alternative to blood doping.3,14 Recombinant EPO has largely replaced the practice of blood doping, as r-EPO produces a dose-dependent increase in hematocrit.2 In theory, r-EPO should provide all of the benefits of blood doping without the risks involved in blood transfusion.3
Recombinant EPO (r-EPO) was approved by the FDA for manufacture in 1989 after the EPO gene was cloned in 1985.14 Since its approval, r-EPO has been abused for athletic personal gain as an alternative to blood doping.3,14 Recombinant EPO has largely replaced the practice of blood doping, as r-EPO produces a dose-dependent increase in hematocrit.2 In theory, r-EPO should provide all of the benefits of blood doping without the risks involved in blood transfusion.3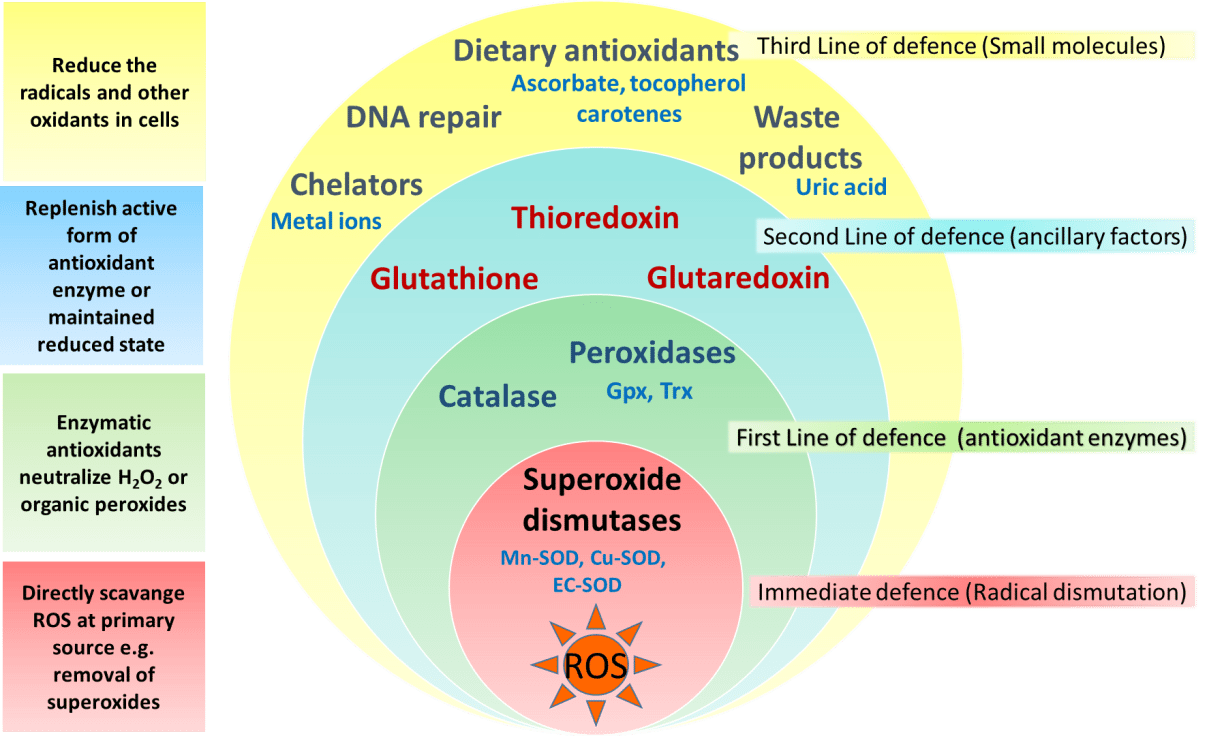 The antioxidant capabilities of certain vitamins are believed by many to counter-act the production of free-radials that occurs during exercise.14 Most of the research to date involves vitamin E, vitamin C, and beta carotene.2 The existing literature does not support the notion that antioxidants have significant ergogenic capabilities.2,14,57 There are currently no recommendations for antioxidant use in athletes that exceeds the normal adult recommended daily allowance (RDA).
The antioxidant capabilities of certain vitamins are believed by many to counter-act the production of free-radials that occurs during exercise.14 Most of the research to date involves vitamin E, vitamin C, and beta carotene.2 The existing literature does not support the notion that antioxidants have significant ergogenic capabilities.2,14,57 There are currently no recommendations for antioxidant use in athletes that exceeds the normal adult recommended daily allowance (RDA). Beta-hydroxy-beta-methylbutyrate (HMB) is a metabolite of the branched-chain amino acid leucine. HMB is theorized to inhibit muscle breakdown during strenuous exercise but its exact mechanism of action remains unknown.14,58 Studies show that HMB supplementation may significantly lower serum lactate dehydrogenase (LDH), lower serum creatine phosphokinase (CPK) levels and delay blood lactate accumulation after endurance training compared to placebo.59,60 Furthermore, short-term HMB use has been shown to significantly increase strength gains with resistance-exercised training over placebo in one double-blinded study.61
Beta-hydroxy-beta-methylbutyrate (HMB) is a metabolite of the branched-chain amino acid leucine. HMB is theorized to inhibit muscle breakdown during strenuous exercise but its exact mechanism of action remains unknown.14,58 Studies show that HMB supplementation may significantly lower serum lactate dehydrogenase (LDH), lower serum creatine phosphokinase (CPK) levels and delay blood lactate accumulation after endurance training compared to placebo.59,60 Furthermore, short-term HMB use has been shown to significantly increase strength gains with resistance-exercised training over placebo in one double-blinded study.61 Caffeine is a methylxanthine occurring naturally in many species of plants. Caffeine is thought to work through a variety of mechanisms. The central nervous system effect of caffeine is probably the result of adrenergic receptor antagonism.3 Its use by athletes stems from the theory that caffeine may delay fatigue by enhancing skeletal muscle contractility and spare muscle glycogen levels by enhancing fat metabolism.6 Multiple studies have reported an improved endurance time with caffeine use.6,62,63 There is evidence that caffeine use may enhance performance with more intense short-duration exercise as well.2 The caffeine dosages most associated with an ergogenic effect range in the literature from 3 to 9 mg per kilogram of body weight.2,6
Caffeine is a methylxanthine occurring naturally in many species of plants. Caffeine is thought to work through a variety of mechanisms. The central nervous system effect of caffeine is probably the result of adrenergic receptor antagonism.3 Its use by athletes stems from the theory that caffeine may delay fatigue by enhancing skeletal muscle contractility and spare muscle glycogen levels by enhancing fat metabolism.6 Multiple studies have reported an improved endurance time with caffeine use.6,62,63 There is evidence that caffeine use may enhance performance with more intense short-duration exercise as well.2 The caffeine dosages most associated with an ergogenic effect range in the literature from 3 to 9 mg per kilogram of body weight.2,6