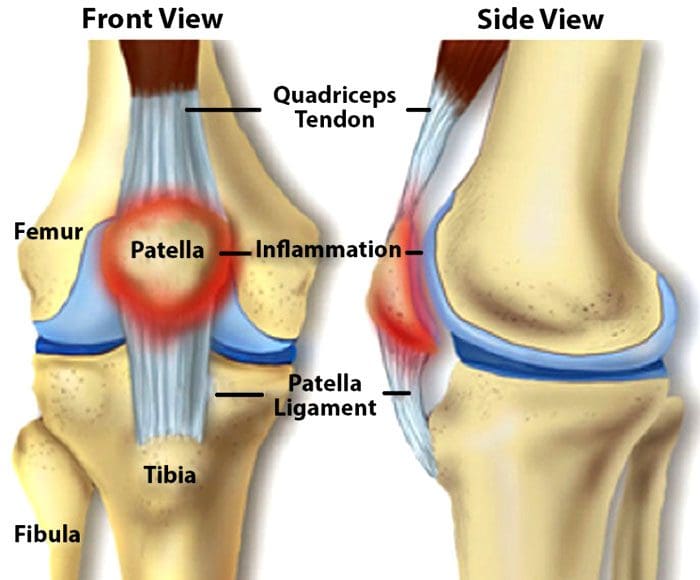
Knee Injuries, Surgeries, and Vitamin D Status. The knee joint is one of the largest and complex joints. It connects the thigh bone to the shinbone, which has a very important role in:
Supporting the body’s weight
Facilitating movement
Allowing the ability to bend the knee
Because of the complexity of the knee joint, it is highly susceptible to injuries. The most common injuries include tears in the:
Ligaments
Tendons
Cartilage
The kneecap itself can be fractured and/or dislocated.
Tears
Meniscal Tears
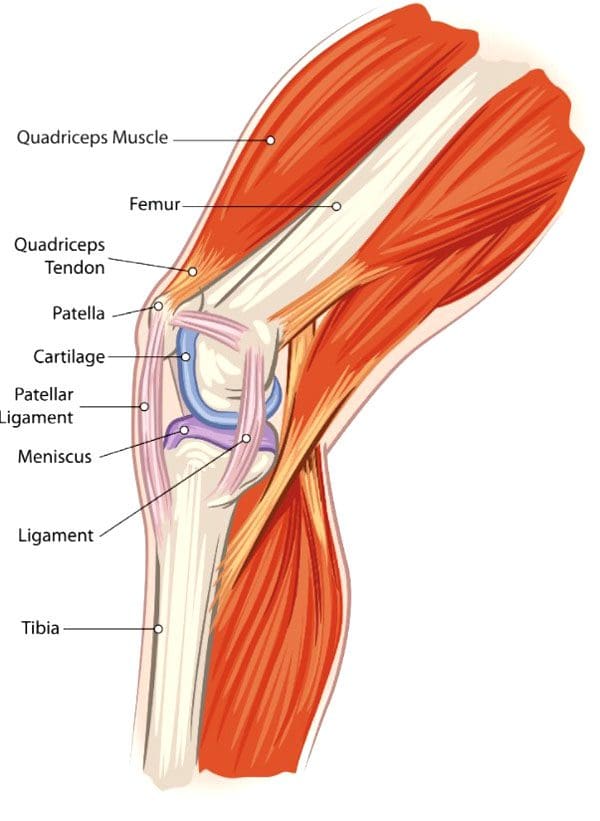
The meniscus is the cartilage between the knee joint that absorbs the impact/shock when running, playing sports, yard work, hiking, bicycling, etc. It cushions the joint and maintains stability.
Meniscus tears are common in sports that have a lot of jumping, starting/stopping quickly, changing direction suddenly, like volleyball, basketball, tennis, soccer, football. This is when the meniscus tears. Surgery can be required, depending on the severity/extent of the injury and tear.
Tendon Tears
The patellar tendon works with the knee muscles in the front of the thigh to straighten the leg. Tears in the patellar tendon are common among middle-aged individuals and those that participate in running or jumping sports.
A complete tear is considered a disabling injury that requires surgery for full functional recovery.
Fortunately, most tears are partial and require rest and chiropractic/physical therapy to heal.
Dislocation
Knee dislocations happen when the knee bones shift out of position. This can happen after a fall, car crash, or high-speed impact. It can also be caused by twisting the knee while the foot stays planted. Dislocations require relocation. However, sometimes a dislocated kneecap corrects itself and returns to the proper position. Other cases can require a mild sedative to allow a doctor to relocate the knee. Dislocations generally take around six weeks to fully heal.
Anterior Cruciate Ligament – ACL Injury
The anterior cruciate ligament or ACL is knee tissue that joins the upper and lower leg bones and maintains the knees’ stability. The ACL can be torn if the lower leg over-extends forward or if the leg gets twisted. ACL injuries are common knee injuries and account for around 40% of sports-related injuries. These injuries can range from a small tear in the ligament to a severe injury where the ligament tears completely or gets separated from the bone. Treatment depends on the severity of the injury. Depending on various factors including the severity of the tear, surgery could be required.
Knee Surgery
For most cases, surgery is done using arthroscopytechnology. This procedure uses small incisions to insert a camera and surgical instruments into the joint. Usually, two or three incisions are needed with recovery time being quicker than large incision surgery where the whole knee is opened. Minimally invasive arthroscopic surgery is preferred by sports medicine experts. With this procedure:
There is no need to cut the tendons or muscles
Bleeding is reduced
Small incisions decrease scarring
Recovery time is shorter
However, sometimes a large incision is required for complex surgical techniques. Common knee surgery procedures include:
Arthroscopy Surgery
This method allows the ability to see inside the knee joint. The procedure is often recommended for:
Diagnosis
Minor repairs to ligaments and/or tendons
Cartilage or bone that needs to be removed
Total Knee Replacement
A full knee replacement is known as arthroplasty. When the joint is damaged beyond repair from injury or disease, an implant is placed in the knee joint restoring function. A small amount of cartilage and bone from the shinbone and thigh bone gets removed for perfect placement of the new knee joint.
Revision Knee Replacement
Most knee replacements last around 15 – 20 years. For individuals that have knee replacement early, then a new operation for new implants could be required. Here, the surgeon removes the original prosthesis and replaces it with a new one.
Partial Knee Replacement
Some knee injuries do not require complete replacement. Here, only the worn-out portion of the joint is replaced. As an example, the cartilage that has been lost in an area of the knee can be repaired with a partial replacement.
Vitamin D Status
A study on athletes that underwent ACL surgery looked at their vitamin d status and how it affected their recovery.
The research concluded that vitamin D status had no effect on surgery outcomes.
However, those with the lowest vitamin D status had three times the failure rate than those with higher vitamin D
The average age of the individuals was around twenty-four and were healthy athletes.
Each of the patients in this study had their vitamin levels measured before the operation and were grouped based on their vitamin D status:
Group 1 vitamin D below 20 ng/mL – considered deficient
Group 2 vitamin D between 20-30 ng/mL – considered low but in a technical range
Group 3 vitamin D above 30 ng/mL – considered sufficient, but not optimal
All were followed for two years with their surgery recovery being measured with two systems.
The Lysholm score, which is a 100 point scoring system that looks at an individual’s knee functions that include:
Mechanical locking
Instability
Pain
Swelling
Stair climbing
Squatting
The WOMAC score is a scoring system that measures:
After 2 years, the Lysholm score and the WOMAC scores were similar.
However, there was a difference in the graft failure rate which was about 6% in group 1 with the lowest vitamin D and around 2% in groups 2 and 3. This shows that the lowest vitamin D status has three times the failure rate compared with those that had increased vitamin D levels. Vitamin D is a known anti-inflammatory with metabolic functions that are documented. Therefore, vitamin D does improve surgical success and recovery in healthy athletes.
Body Composition
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP*, CIFM*, CTG*
email: [email protected]
phone: 915-850-0900
Licensed in Texas & New Mexico
References
Brambilla, Lorenzo, et al. “Outcome of total hip and total knee arthroplasty and vitamin D homeostasis.” British medical bulletin vol. 135,1 (2020): 50-61. doi:10.1093/bmb/ldaa018
European Journal of Orthopedic Surgery and Traumatology, January 2021
Zhang, Hao et al. “Vitamin D Status and Patient Outcomes after Knee or Hip Surgery: A Meta-Analysis.” Annals of nutrition & metabolism vol. 73,2 (2018): 121-130. doi:10.1159/000490670
Athletes both recreational and fully competitive can be impacted by injuries to the muscles and ligaments around the hip.
These injuries interfere with performance levels and sometimes end participation completely.
�Excessive pronation along with shoes with poor shock absorption has been found to be an underlying cause for various leg/hip injuries.
Custom made Orthotics improve the biomechanics of the feet and reduce the extent of pronation helping to prevent sport-related leg/foot injuries.
Over Foot Pronation
Research has determined that athletes with more foot pronation have a higher probability of sustaining a leg injury, including iliotibial band syndrome that comes from excessive tightness of the hip muscles.
People involved in sports or recreational activities lower their likelihood of developing traumatic and overuse hip injuries through chiropractic treatment and using custom foot orthotics.
The amount of pronation during standing and while running at a standard speed is determined by measuring the angles of the footprints.
Athletes with more pronation have a higher likelihood of an overuse injury.
Standing (static) and running (dynamic) prints show the amount of pronation and is a predictor of developing an overuse injury.
Athletic performance and injury prevention involve regularly checking the alignment of patients� feet in the standing position.
Hip Injuries & The Hamstring
Many hip injuries develop from poor biomechanics and improper movement, especially when running.
Smooth muscle coordination provides balance and support for the pelvis and is needed for optimum sports performance.
This includes:
Hamstring muscles
Hip abductor muscles
Tensor fascia lata or the iliotibial band
When there is an issue with the feet and ankles, abnormal motion like over-rotating the entire leg is the perfect set-up for pulls, sprains, and strains.
50% of standing consists of heel strike and maximum pronation.
The hamstring muscles function to control the knee and ankle when the heel strikes and absorb the impact.
The theory behind orthotic support is that orthotics help the hamstrings control the position of the calcaneus and knee, so there is less stress on the hip and pelvis.
Hip Injuries & Over-Pronation
Orthotics can correct excessive pronation and treatment of hip problems. These are some of the problems/pathologies that can develop.
These conditions develop in athletes who push their body’s to the limit going for optimal performances.
Conclusion
Overpronation and poor shock absorption contribute to leg injuries � from:
Foot
Lower leg
Knee
Thigh
Hip
These conditions can be prevented with custom-made orthotics.
Foot biomechanics evaluation is a must
To avoid hip injuries, athletes need regular evaluations of foot alignment and function
Wear well-designed and solid-constructed shoes
Chiropractors can prevent arch breakdown and foot problems with custom orthotics, and also treat numerous injuries to the lower extremities, especially the hips.
Excessive Foot Pronation can Affect *FOOT POSTURE & MOBILITY* | El Paso, TX (2019)
The following video discusses how excessive foot pronation can ultimately affect foot posture and mobility. Several factors can affect foot posture and mobility, such as excessive foot pronation. Excessive foot pronation is most prevalent among the general population, therefore, it is considered to be one of the most common factors for abnormal foot posture and mobility, which can lead to a variety of health issues like overuse injuries. Excessive foot pronation and even supination can ultimately affect overall health and wellness.
Hip Labrum tears in athletes can occur from a single event or recurring trauma. Running may cause labrum tears due to the labrum being utilized more for weight-bearing and taking excess forces while at the end-range motion of the leg. Sporting activities are probable causes, specifically those that require frequent hip rotation or pivoting to a loaded femur as in ballet or hockey. Constant hip rotation places increased strain on the capsular tissue and harm to the iliofemoral ligament. This subsequently causes hip instability putting increased stress on the labrum and causing a hip labrum tear.
What’s Afoot
Chiropractic�seeks to find the cause of the conditions it is used to treat, including pain, instead of just treating symptoms. Because of this, the chiropractor will work to find the cause of the pain, in this case, overpronation and overpronation, and correct it � or the effects of the condition � in addition to treating the back pain.
Overpronation and oversupination can cause a variety of injuries and conditions that affect not only the feet and ankles, but also the knees,�hips, and back as well. Some of the more common injuries and conditions include:
Flat feet or posterior tibial tendon dysfunction
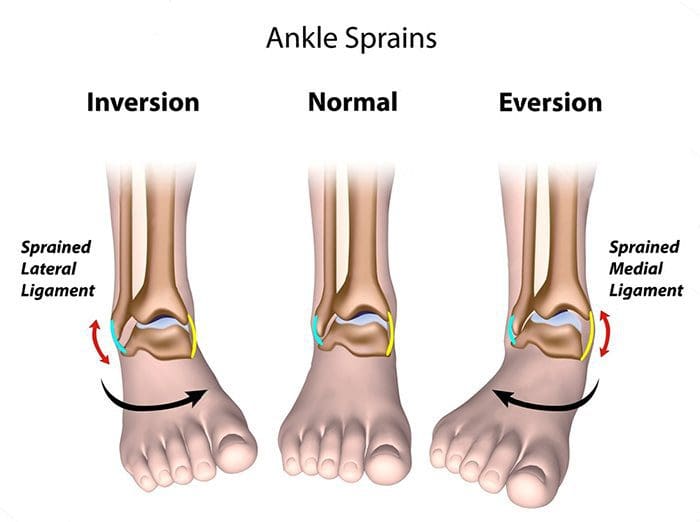
Ankle Sprains
Achilles tendinitis
Arch pain
Plantar fasciitis
Corns
Shin splints
Heel pain
Tight calves
Calluses
Knee pain
Patellar tendonitis
Tight hip flexors
Back pain
Sciatica
Herniated disks
NCBI Resources
Muscle imbalances in the hip, such as tight hip flexors, can cause low back pain � or at least contribute to it. When the hip flexor muscles are too tight, it causes what is known as an anterior pelvic tilt.�Hip flexors�can become too tight if the person sits for extended periods of time or engages in activities like cycling and jogging. A chiropractor can guide you through exercises that will help release the tight muscles and stop the micro spams that occur as a result.
There has been an increasing number of professional athletes and athletic teams in recent years that have chosen to use chiropractors to treat their injuries, help manage their pain, and help keep them at the top of their game concerning performance and stamina. Top athletes like Jordan Spieth, Phil Mickelson, Vernon Davis, and Aaron Rodgers recognize that value in good chiropractic care and have incorporated it into their overall health and wellness programs.
One of the biggest draws is chiropractic�s whole-body approach to health care. A chiropractor will not just treat the symptoms of a problem (such as pain), he or she will work to uncover the cause of the problem and recommend lifestyle changes that will help the athlete not only eliminate their pain, but resolve the issue causing the pain, and take steps to help prevent the problem from recurring.
The NFL Chooses Chiropractic
The National Football League (NFL) has long kept chiropractic care as a standard treatment for its players. The Professional Football Chiropractic Association estimates that the average team chiropractor for the NFL will perform anywhere from 30 to 50 chiropractic adjustments or treatments a week during the football season.
When you consider that the NFL teams employ around 35 chiropractors, that adds up to about 27,000 adjustments in that short 16-week span, but it�s worth it to keep the players in tip-top shape, and many continue chiropractic care even after they retire.
The PGA Chooses Chiropractic
Many top golfers in the Professional Golfers� Association (PGA), such as Arnold Palmer, Jack Nicklaus, and Phil Mickelson see chiropractic care not only as a necessary element in their wellness routines but also as a playing a vital role in their success.
Many use it to enhance their athletic performance, help prevent injuries, help heal from injuries, manage pain, and improve their overall health. Some golfers, like Masters Tournament winner Jordan Spieth, have a chiropractor who travels with him on a full-time basis and provides treatments several times a day.
Olympic Teams and Chiropractic
At the Olympics, the best of the best compete � and put their bodies through a lot of stress and punishment in the process. Most Olympic teams have two chiropractors who travel with them in an official capacity.
After practice or competition, they will get treatments to keep their bodies at optimal performance level. If any of the athletes sustain injuries, the chiropractors can help to manage pain and help heal the injury. Studies show that most injuries that are treated with chiropractic care heal faster and more complete.
The MLB, NBA, and NHL Choose Chiropractic
Most of the teams in the NHL, NBA, and MLB either have a chiropractor they refer to that is outside, or their organization or they have one on staff. This means that not only are chiropractors treating athletes, but they are also treating some of the best athletes in the world.
These people make a living based on how well their bodies perform so it stands to reason they would not turn to just any type of treatment or trend. They choose to reap the benefits of the tried and true chiropractic care.
Chiropractic for Athletes
Athletes know the many benefits that they can get from regular chiropractic care. Some of the top include:
It is drug-free and non-invasive.
It is very effective in pain management.
It can reverse the punishment that the body undergoes while participating in sports.
If you play sports, even if you enjoy a game of touch football on the weekends, you might benefit from chiropractic care. If it�s good enough for the pros, it�s good enough for you!
James Hill, father and teacher to two older sons and a younger daughter called Madison Hill, belong to an athletic family. Madison began participating in several sports because she had been a young woman, but she consequently experienced numerous sports injuries. Luckily, James Hill and his daughter Madison Hill went to go to Dr. Alex Jimenez and he has tremendously helped her recover after every injury she experiences. Collectively, they’ve learned to trust in chiropractic care, particularly following Dr. Alex Jimenez’s innovative treatment techniques and procedures. Mr. Hill expresses his gratitude in addition to how far Dr. Alex Jimenez’s understanding in sports injury therapy has greatly enlarged his general comprehension of the human body’s healing process. After Madison suffered a recent ankle sprain, she was instantly reassured by Dr. Alex Jimenez regarding how much faster she’d return-to-play during chiropractic care. James Hill and Madison Hill highly recommend Dr. Alex Jimenez as the non-surgical selection for volleyball sports injuries, among others..
Chiropractor Ankle Sprain Treatment
Every year, millions of young athletes engage in high school sports. However, once an injury occurs, it might develop into an issue that might result in them having to discontinue their particular sport or physical activity if not treated properly. The pressure to continue participating in the sport or physical activity may cause young athletes not to follow proper recovery guidelines, which might subsequently result in more injury with long-term consequences. Sports injuries among young athletes fall into two key categories: overuse injuries and acute injuries. Both kinds include injuries to the soft tissues and bones. Whether an injury is acute or due to overuse, a young athlete who develops a symptom which impacts their athletic performance should be diagnosed appropriately by a health care professional. Sports accidents which are untreated can lead to permanent disability. Many high school sports injuries can be avoided through appropriate instruction and conditioning.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and recommend�us.
Lower Back Injury: Isaiah Delgado, wrestler, began participating in a fitness and nutrition program at Push-as-RX in order to improve his performance in his physical activities. When he suffered a lower back sports injury, Isaiah Delgado once again came to Push for assistance, except this time, the trainers enrolled him in a rehabilitation program to help him return-to-play as soon as possible. Isaiah Delgado describes Push-as-Rx as a lifestyle and he recommends Push to anyone looking for the right type of support when it comes to recovery and increased performance.
Lower Back Injury And Chiropractic Care
Sports Therapy is an element of healthcare that’s specifically concerned with the prevention of injury and the rehabilitation of the individual back to optimum levels of practical, occupational and sports specific fitness, regardless of age and capacity. It utilizes the fundamentals of sport and exercise sciences incorporating behavioral and physiological processes to prepare the player for training, competition and where applicable, work. A variety of healthcare professionals are able to provide this type of treatment method.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
For many athletes following any major endurance event they will return to their houses, to recover, celebrate, reflect and rebuild to their next career step. Some, like the athlete in this case study will need to now focus attention on delayed decisions concerning whether to go under the knife to sort out a chronic injury.�El Paso, TX’s Injury scientist, Dr. Alexander Jimenez takes a look at the study.
My client has been competing in triathlon for 10 or more years, although his career has included a range of serious injuries which have kept him from races for months on end. In the previous two to three decades, however, he’s enjoyed a sustained period of injury-free training and racing, and has climbed to the peak of the world rankings. But the emergence of hip pain has seen him once more return to the physio’s table.
The triathlete’s accident history highlights a common pattern among sportspeople: 2 tibial stress fractures, a femoral neck stress fracture and a serious ankle sprain — every one of these on his right side. The significant contributing element to the bone stress injuries is a 1.5cm leg-length gap (his right leg is shorter).
He’d first experienced comparable hip pain in 2004; it kept him from running for three months. At that time, nothing was detected on a bone scan or MRI, or so the pain went paralyzed. An intra-articular cortisone injection (CSI) elicited no improvement. The athlete remembers that he chose to train on his painful hip, never allowing the symptoms to settle. The nearest he ever came into an investigation was a hypothesis that he could have a little, undetected, labral lesion.
The present episode of hip pain began initially at night after a hard three-hour bicycle ride. Earlier this, however, he hadn’t cycled for five times. He described his initial symptom as a profound hip tightness (lateral and lateral), together with slight pain in his groin. He was able to continue to train however, was feeling that the hip tightness and pain following both cycling and running (swimming was symptom-free).
A week later his symptoms dramatically worsened when he flew from Australia to Singapore, on his way to a French high- altitude camp. As he got off the airplane, he felt deep hip pain as well as the tightness. As elite athletes tend to do, he coached anyway, running a tricky track session, which made the hip much worse: he was unable to ride or run without pain. He instantly started a course of anti- inflammatories.
I met him in Singapore and evaluated him in the airport, initially ruling out any prospect of a disease or systemic matter. He explained he had been feeling an ache during the night, lying in bed; on waking, the hip would be OK, but got worse the longer he walked.
On assessment, he had the following physical signs:
� walking with obvious limp
� pain on hopping (6/10)
�painful right hip quadrant/impingement test (full hip flexion/adduction)
� reduced right hip flexion (-10 degrees compared to left)
� reduced right hip internal rotation (-10 degrees compared to left)
� increased tone on palpation of TFL, adductors, hip flexors, gluteal, piriformis and deep rotators
� lumbar spine and SIJ were OK
� femoral shaft bone stress test was OK � leg length discrepancy (right side 1.5cm shorter)
� right innominate (pelvis) anteriorly rotated
� weakness in right hip abductors/extensors
� reduced calf endurance on right side (-5 reps)
� ankle dorsiflexion range of movement was OK
� reduced proprioception on right (single leg stance, eyes closed).
I thought the differential diagnoses were:
� femoral neck stress fracture
� labral tear, possibly with hip synovitis
� FAI (femoro-acetabular impingement), possibly with hip synovitis.
I initially treated the triathlete with soft- tissue techniques to reduce the tone around the hip joint. Trigger-point releases were performed on his TFL, adductors, gluteals, piriformis, deep rotators and iliopsoas.�This reduced his jump pain into 3/10. Manual long-leg grip further decreased the strain on hopping (2/10). He still had pain and stiffness on walking but it sensed “simpler. As he prepared to embark on his long run flight to Europe, I counseled him to not sit for too long and maintain his stylish as straight as possible to decrease any potential impingement from hip flexion.
Luckily, the hip didn’t get worse throughout the flight. On arrival at the French high-altitude training centre, we initiated a strategy of two swims and two intensive treatments a day, aiming at reducing muscle tone, restoring his range of hip movement and normal muscle control and stamina. We had been expecting that the problem was not a stress fracture, but just minor hip synovitis that could settle quickly. Following a week of conservative treatment, though, we were just able to keep his hop pain in 2/10, and that he still could not run 20 meters without any pain and limping.
In collaboration with medics, we flew to London to see a sports doctor and get MRI scans. The scans revealed no bone stress reaction, fracture or labral ripping — which was a big relief; however, it did show signs consistent with FAI (femoro-acetabular impingement). He had hip synovitis with a rectal lesion on his femur.
Hip injuries aren’t much reported among triathletes — in fact they are notably absent from reports on Olympic and Ironman triathlons, which mention knee, back, H/ Achilles, lower leg, ankle and shoulder as the most common accidents (1-3).
In this state, when the hip is in maximum flexion and internal rotation, the labrum and cartilage abut and impinge; damage to the articular cartilage and acetabular labrum results from this pathologic bony contact. The contact generally results in a structural abnormality of the femur (“camera impingement”) along with the acetabulum (“pincer impingement”) or a combination of both (“mixed impingement”). Over time, via repetitive micro-trauma, the aggravating motion hurts the hip cartilage or labrum (or both) during normal joint motion. This happens along the anterior femoral neck and the anterior–superior acetabular rim. FAI is a possible trigger of early hip joint degeneration (4).
Arthroscopic surgery is the direction of choice for FAI if symptoms do not settle; however as his next Competition was only three and a half a year off, surgery was not an option. Instead, over a five-day interval, the athlete had two cortisone (CSI) and local anesthetic injections into the hip joint (under ultrasound guidance) to settle the indicators.
Our aim was to grow the hip range of motion and extend the capsule to reduce any additional impingement, slowly returning to regular training. Following the competition, the athlete would then should see a hip arthroscopic surgeon to acquire a surgical opinion to the best option for long-term direction.
Injection Relief
After both shots my customer felt sore for five days. The initial CSI settled his pain on hopping to 1/10 and after seven days he managed to operate without symptoms. But minor hip stiffness and aching at the end of the day prevented him from progressing to optimal training, so that he then underwent a second steroid injection. This settled the hop pain into 0/10 and decreased the aching; so after five times he returned to mild cycling and after seven days he started running again, also.
The athlete admitted that, following the first shot, he had done more and gone tougher in training than directed, as he had felt “good. This mistake of “too much too soon — all too common in elite athletes — had led to excessive inflammation and aching in the hip nightly after training. After the next injection he returned to normal intensity slower and more gradually.
My client built his training up to regular levels by four months following the final injection (swimming five times per week, cycling four days and running six to seven days). He began with very easy cycling on a wind trainer for 30 minutes, building slowly to 90 minutes before cycling on the street. He cycled two days on and one day away and avoided hills to the first two weeks. He started jogging on the apartment for 15 minutes and slowly built up to 90 minutes after three weeks. He did not run hills or about the track; and as he ran only on every single day, he would diligently concentrate on technique.
From week six to week 11, my client remained on anti inflammatory medication and underwent two treatments a day.
The hands-on treatment continued to:
� increase hip range of movement
� stretch the hip capsule
� normalise pelvic symmetry and hip muscle tone
� improve muscle control and strength � improve proprioception
� ensure optimal biomechanics via video assessment (cycling and running).
Eleven weeks after he first felt his hip pain, the triathlete returned to racing; however he failed to finish the first race, partially because of minor hip stiffness but mainly due to “fitness. Fortunately there were not any prolonged symptoms after the race and a week after he successfully returned to competition, coming second in a really strong field. His very minor ongoing symptoms were handled with anti-inflammatory drugs and hands-on treatments.
If this athlete wants to pursue a long- term triathlon career up to the London Olympics, then he will now require surgery. The arthroscopic surgical technique initially assesses the cartilage and labral surfaces, debrides any abnormalities of the hip joint cartilage and hip labrum, removes the non-spherical segments of the femoral head�and any prominent sections of the anterior femoral neck and bony growths on the acetabular rim that may continue to contribute to hip joint impingement.�The alternative is early joint degeneration and onset of osteoarthritis.
References:
1. Wilk B et al: �The incidence of musculoskeletal injuries in an amateur triathlete racing club�. J Orthop Sports Phys
Ther 1995 Sep;22(3):108-12.
2. Collins K et al: �Overuse injuries in triathletes. A study of the 1986 Seafair Triathlon�. Am J Sports Med 1989 SepOct;17(5):675-80.
3. Korkia PK et al: �An epidemiological investigation of training and injury patterns in British triathletes�. Br J Sports Med 1994 Sep;28(3):191-6.
4. Ganz R. et al (2003): �Femoroacetabular impingement: a cause for osteoarthritis of the hip�. Clin Orthop Relat Res. 417:112�120. For more information see: www.hipfai.com
Any marathoner will tell you that the grueling 26-mile races can do a number on the hips, knees, ankles and feet.
Now, a small study suggests that these tests of endurance are also tough on the kidneys.
“Marathon runners demonstrate transient or reverse short-term kidney injury,” said Dr. Chirag Parikh, professor of medicine at Yale University.
In his study of 22 participants in the 2015 Hartford, Conn. Marathon, Parikh found that 82 percent showed acute kidney injury after the race. In this condition, the kidneys fail to filter waste from the blood. The good news is that the kidney injury seems to clear up within two days of the race, he said.
“On day 2, they are all fine,” Parikh said.
Runners likely don’t even know they’ve had this transient injury, Parikh said. “For the short term, I don’t think they would notice anything,” he said. Parikh isn’t certain why the strenuous event is linked with kidney injury. But some potential causes include the sustained rise in core body temperature, dehydration, or the decreased blood flow to the kidneys that occurs during a marathon, he explained. When the blood is pumped to the skin and muscles while running, he said, the kidneys may not get as much blood as they normally do.
Nor can Parikh say whether the effect might be cumulative, getting worse with more marathons run. It may be that the kidney adapts over time instead, he noted.
To evaluate this type of kidney injury, his team looked at blood and urine samples collected before and after the marathon. These tests included measuring blood creatinine levels and proteins in the urine, along with looking at kidney cells on a microscope. Creatinine is a waste product excreted by the kidneys; measuring it in the blood helps assess kidney health.
In a previous study, published in 2011, Dr. Peter McCullough, vice chief of medicine at Baylor University Medical Center in Dallas, and colleagues evaluated 25 men and women marathoners. They found 40 percent of the runners met the definition of acute kidney injury based on their blood creatinine levels.
In the new study, Parikh’s team also “performed an in depth evaluation of the urine and found evidence of injury,” McCullough said.
“The larger question looming is: do these repeated bouts of injury in endurance athletes lead to chronic kidney disease years later? Can anything be done about the injury at the time including hydration strategy?” McCullough said. More study is crucial, he added.
Parikh said additional research is also needed to assess whether certain people may not recover as quickly. For now, those with a family history of kidney disease should let their physician know they run marathons, he suggested.
Dr. Cathy Fieseler said marathoners who want to reduce their risk of kidney injury should avoid anti-inflammatory drugs before the race. Those drugs include over-the-counter ibuprofen (Advil, Motrin IB) and naproxen (Aleve), Fieseler said. Acetaminophen (Tylenol) is cleared through the liver.
Fieseler is a primary care sports medicine doctor at Christus Trinity Mother Frances Health System in Tyler, Texas. She’s also medical director of the American Running Association.
The study was published March 28 in the American Journal of Kidney Diseases.
SOURCES: Chirag Parikh, M.D., Ph.D., professor of medicine, and director of applied translational research, Yale University, New Haven, Conn.; Cathy Fieseler, M.D., primary care sports medicine physician, Christus Trinity Mother Frances Health System, Tyler, Texas; Peter McCullough, M.D., vice chief of medicine, Baylor University Medical Center, Dallas; March 28, 2017, American Journal of Kidney Diseases
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Chiropractic and Athletic Performance
Many athletes who are injured performing their specific sport or physical activity, frequently seek treatment from chiropractors. Chiropractic care focuses on the prevention, diagnosis and treatment of injuries and conditions affecting the musculoskeletal and nervous system. While chiropractic is a safe and effective form of conservative care for a variety of ailments, chiropractic can also be utilized to enhance athletic performance.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine







 We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.










