Reducing stress is important for emotional well being and physical health. Rheumatoid arthritis is a complex condition with no cure and can cause intense chronic pain. Stress only exacerbates the symptoms, affects pain perception, and weakens the body. Stress management is highly important for reducing pain. In a weakened state, an individual is more vulnerable to arthritis symptoms, like flare-ups, weakness, and fatigue.�Chiropractic can help.
There are non-surgical treatments for arthritis, like medications, physical, and massage therapy that address the physical nature of the condition. By eliminating stressful triggers and making healthy behavioral/lifestyle changes a better sense of well being can be achieved.
Different emotions can run rampant:
Confusion
Frustration
Anger
Sadness
Helplessness
And all of these feelings can generate intense stress on an individual. Chiropractic excels in wellness and is becoming more common for individuals to visit chiropractic clinics for treating a variety of different kinds of pain symptoms and conditions. Chiropractic adjustments provide countless benefits to those with arthritis. We�ll explore how chiropractic can help those with arthritis and give additional information along with suggestions on how to alleviate the pain.
What Chiropractic Does
A doctor of chiropractic is a health professional that focuses on wellness and optimal health instead of ailment/sickness symptoms. Their specialty aims at adjusting the spine to correct misalignments that could be pressing down on nerves and causing major disruption in the body. Regular chiropractic not only restores health throughout the body but helps alleviate back pain and any other symptoms associated with an out of alignment spine.
They also work in setting up exercise programs specific to the condition being treated along with the proper diet to utilize in assisting with the management of inflammation and pain.
Arthritis
Arthritis is inflammation in the body’s joints which results in pain, stiffness and limited range of movement. There are over 200 different varieties of arthritis. Generally associated with age, it can affect young people. It can strike pretty much any area of the body. Arthritis can cause damage to soft tissues and muscles.
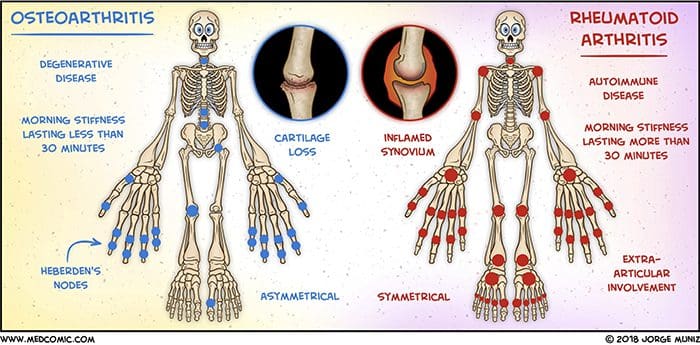
Osteoarthritis also known as degenerative joint disease, is the most common type. It comes from repeated trauma to the joints and occurs more often in the elderly.
Other forms include:
Rheumatoid arthritis is the second common type in which the body�s immune system attacks the joint/s.
Psoriatic arthritis, an autoimmune form of arthritis.
Ankylosing spondylitis is a type of arthritis where the body attacks itself.
Septic arthritis is caused by a viral or bacterial infection of the joint/s.
Diagnosis
Diagnosing arthritis involves a thorough physical examination. Rheumatologists often need help with these cases, and so a medical work-up can be done and a chiropractor could be recommended. This includes X-rays or MRIs, urine, blood analysis, and physical examinations. Having the condition properly diagnosed will help to more effectively treat the symptoms.
Chiropractic
The most common treatment is medication, which takes down the inflammation, the swelling and reduces pain. Chiropractors can be of great help in managing arthritis. Medications work but as we’ve seen they can have long-term health risks like impaired healing, damage to the stomach lining and internal bleeding.
A chiropractor can reduce stress, and reliance on medications, all the while managing the pain and symptoms in a natural way. Chiropractic can:
Improve range of motion
Keeps the spine properly aligned
Improve endurance
Improve flexibility
Increase strength
Increase muscle tone
Develop a dietary and nutritional plan to reduce inflammation
Recommend an exercise regimen conducive to arthritis symptoms
According to the American Chiropractic Association, this is vital in managing arthritis symptoms.
Treatment
Understand that chiropractic cannot cure arthritis. They can help alleviate symptoms, slow the progression and help to reduce stress levels. They will use adjustments in combination with other treatments. This can include:
Hot and cold treatments
Ultrasound treatments
Massage
Electronic muscle stimulation
Physical rehabilitation
Magnet therapy
Reduce Stress
Exercise
Water aerobics or make walking around the park/neighborhood part of a daily routine, as it promotes a healthy mind by reducing stress and anxiety. Gentle exercises like aerobic exercise are perfect because it improves mobility and helps shed a few pounds taking pressure off the joints. Exercise creates endorphins, which reduces pain and uplifts the mood.
Support groups
With any type of painful condition, it’s easy to feel alone. Joining a support group can connect you with people who understand what’s going on and the emotions you’re experiencing. The community helps diminish the sense of isolation.
Relaxation therapy
This focuses on calming the body and mind by making a conscious effort to relax. Even for only a few moments, you might find this technique effective at controlling the stress response. Begin by focusing on one part of the body like the hands, feet, etc.
Concentrate until the area you’re focusing on is completely free of stress or tension. Then imagine weightlessness flow through the body. Close your eyes, lie down, turn off the lights, and think of something soothing. There are no strict guidelines for relaxation. Whatever puts you in a relaxed frame of mind is the way to do it.
Warm bath
Warm moist heat from a shower, bath, or steam room can decrease the secretion of stress hormones and raise levels of endorphins, as aforementioned the body’s natural pain killers.
Take time for yourself
When it comes to reducing stress, balance is key. Staying active, and regular rest/sleep is vital to successful treatment. A balance needs to be in everything you do. Therefore, make time for the things you want to do.
Results
Inflammatory diseases like arthritis have shown the best results are achieved from combating it from all angles. Working with a chiropractor and rheumatologist to combine treatments can make all the difference. A healthy diet and active exercise program will get you in the right direction toward a healthy active lifestyle. If you or a loved one are suffering from arthritis, don�t hesitate to call. We�re here to help in any way possible!
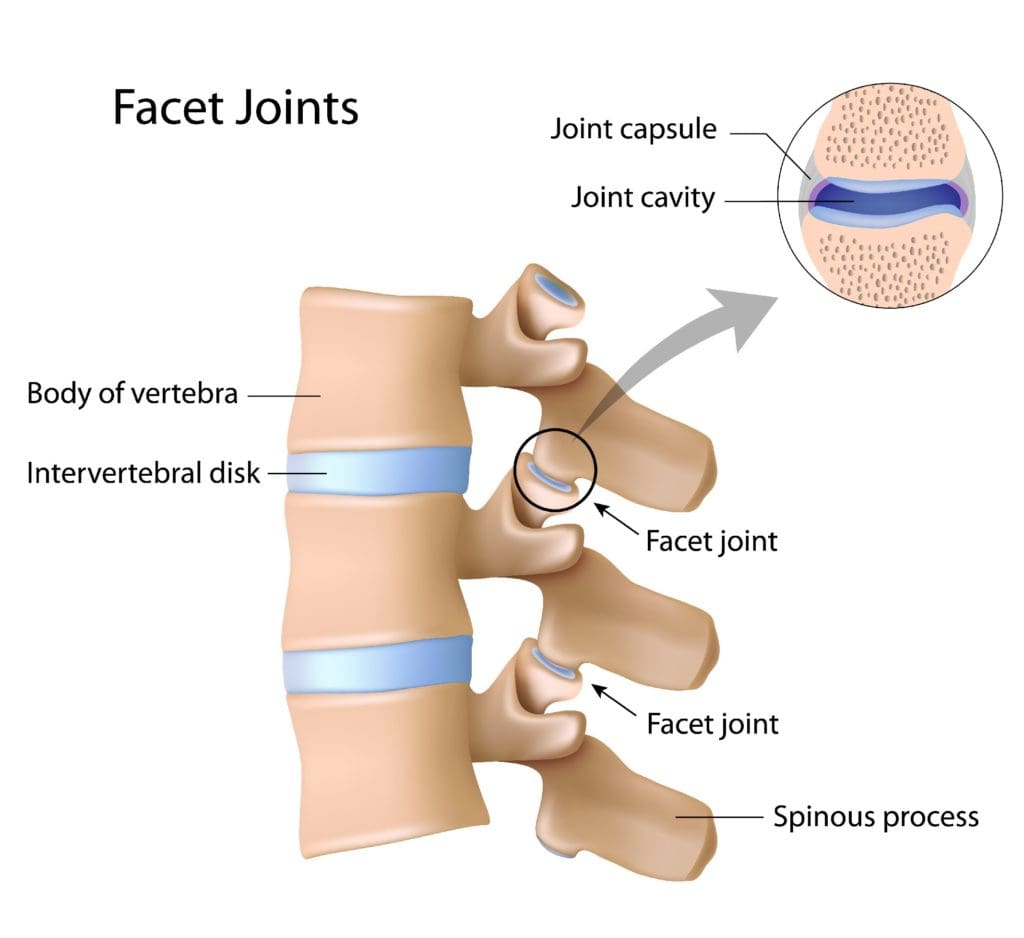
The most�common type of arthritis in children and adolescents is Juvenile idiopathic arthritis aka (JIA) a type of inflammatory arthritis that affects kids 16 years and younger. It is a rare condition, that affects around 1 in every 1,000 children. It can cause�joint�pain and stiffness throughout the body, especially the facet joints/spinal joints.
Types of Arthritis that Fall Under JIA
Juvenile Idiopathic arthritis was known as juvenile rheumatoid arthritis, but it is not a child/teenage version of adult rheumatoid arthritis. Juvenile Idiopathic arthritis falls into a group of several types of arthritis. When a doctor diagnoses JIA, they will determine the type.
To better understand how this arthritis affects the spine, it helps to know some of the terminology.
Enthesitis: Inflammation of the entheses is the area where tendons and ligaments connect to bone/s.
Spondyloarthritis: Arthritis that attacks the entheses of the spine. Ankylosing spondylitis is an example of spondyloarthritis.
The neck joints are the most common to be attacked by JIA. Whereas, spondyloarthritis causes pain and stiffness in the low back.
Typical Symptoms
Juvenile idiopathic arthritis happens in children aged 16 years and younger. Symptoms include:
Joint pain
Swelling
Stiffness
Tenderness
Mild heat or a warmness that has been present for at least 6 weeks.
Other symptoms can include muscles and soft tissues becoming tight, erosion of the bone,�joint misalignment, and abnormal growth patterns.
Diagnosis Can Be A Challenge
Diagnosis is not always straightforward, and there are criteria for diagnosing juvenile idiopathic arthritis. The doctor will perform a physical exam and order tests. They will monitor the child�s symptoms for at least 6 weeks initially, and then for 6 months after the onset of the disease. During this time, figuring the number of joints involved helps determine the diagnosis. As joint involvement can vary by the type of arthritis, and symptoms can and do change regularly.
This arthritis attacks the joints of the spine, specifically in the neck. However, with certain types of spondyloarthropathy, the lower back can become the target.
Diagnosing arthritis involves a complete and thorough examination. If a chiropractor has been brought in to help with the case, a medical work-up by a rheumatologist could be recommended. This includes radiology/X-rays or an MRI, urine, blood analysis and physical examinations.
Treatment
A doctor may recommend a multi-disciplinary approach to treat JIA. They may prescribe various types of therapies/treatments focused on stopping the disease’s progression. The treatment plan will include teaching healthy habits to prevent future back pain.
Medication/s
Treatment usually starts with nonsteroidal anti-inflammatory’s. A doctor can also prescribe a corticosteroid to control the inflammation. Most respond well to anti-inflammatory medication, however, these medicines do not treat the underlying disease or the root cause.
Inflammatory arthritis and its progression can be controlled with certain medications. There are disease-modifying antirheumatic medications that can slow the disease�s progression. There are also TNF-blocking medications that can help block a specific protein known as tumor necrosis factor that causes inflammation. Etanercept known on the market as Enbrel and adalimumab aka Humira are examples of TNF-blockers that can prevent the disease from progressing.
Chiropractic
Understand that chiropractic medicine cannot cure arthritis, but it can help alleviate the symptoms and slow the progression. They will use spinal adjustments in conjunction with other treatments. These can include:
Hot and cold treatments
Ultrasound
Massage
Electronic muscle stimulation
Magnet therapy
Physical rehabilitation
Physical Therapy Exercise
Focuses on:
Proper posture
Joint mobility
Deep breathing
Exercises
Healthy lifestyle education
Patients can develop a forward posture that can lead to a hunched back and neck pain. Postural training and back extension exercises are helpful. Stretching and range of motion exercises keep the facet and rib joints functioning and mobile. Deep breathing expands the chest which expands the rib joints and aids lung function. Depending on the type and severity, a doctor might try other approaches like spine surgery.
Optimal Results
If you or someone has been diagnosed with juvenile idiopathic arthritis in the spine,�learn as much as possible about the disease and the ways to combat it. Being informed about this or any disease encourages empowerment and engagement throughout the treatment process.
The best results are achieved by attacking it from all angles. Working with a chiropractor and rheumatologist in combination. A chiropractor will train the individual on how to maintain a healthy diet and maintain an active exercise program to help with movement. This is geared toward a healthy outcome.
In the same ways that it helps human patients, it also helps animals. It offers a less invasive, medication-free way to manage pain and correct many health issues, including arthritis and joint injuries. A number of pet owners claim chiropractic is not only great for their pets but that their pets are excited to go to appointments and see their chiropractors.
Which animals benefit from veterinary chiropractic care?
Any species of animal can benefit from chiropractic. The most common animals to receive this specialized type of care are dogs, cats, and horses. However, any vertebrate species, including birds, can reap the benefits.
Chiropractic for animals has long been a standard form of treatment with many show horses, race horses, and barrel racers. It is considered a viable, beneficial treatment to help the animals combat the stress their bodies are put under due to their jobs. It is also very good for injuries, speeding healing while managing pain.
It is often used on dogs and cats to help with injuries, arthritis, and aging. Sometimes an animal can hurt but they are unable to communicate that to their owners. If you notice behavioral changes or grumpiness, you may want to check your pet out. He or she may be hurt and can�t tell you � and chiropractic could be the answer.
Most often treated conditions
Veterinary chiropractic helps pets with many conditions that are biomechanical or neurological in origin � much like it helps humans. Some of these conditions include spondylosis, hip dysplasia, and other types of degenerative joint diseases, intervertebral disk disease, neck pain, back pain, and cervical instability. It can also address problems of the autonomic nervous system like musculoskeletal weakness, fecal and urinary incontinence, chronic neck and back pain, and other pain that don�t respond to conventional treatments.
Serious injuries like ligament tears or fractures may require surgical intervention, but chiropractic can help post-surgery. It can help relieve the pain as well as correct secondary problems that could occur due to the animal overcompensating in response to the injury. In performance animals, regular chiropractic care can help prevent injury by maintaining flexibility and a good range of motion.
How does it work?
Chiropractic is designed to help keep the joints and spine in their natural, healthy alignment. The nerves that surround the joints and run along the spine communicate with the central nervous system. This connects to all of the organs in the body, including the brain.
When the spine is out of alignment, even just a little, it can cause disruptions in how the messages are relayed through the central nervous system and to the organs and brain. A misaligned spine can affect the entire body, causing pain in muscles and joints, affecting organ function, and impact the animal�s overall health and wellbeing. When the spine is not aligned, the body will not function as it should.
Give the best possible chiropractic experience.
When you meet with the veterinary chiropractor, make sure that you have all of your pet�s information available, including vaccinations, health care history, any conditions they have, their diet (including supplements), medications they are taking, and their daily activities. If the doctor is treating an injury, explain how the injury occurred if you know.
When the adjustment is over, make sure that you understand any therapy or exercises to do at home, post adjustment. If there is something you don�t understand, ask. The doctor may also provide recommendations regarding lifestyle changes including saddle fit, collar fit, exercise, conditioning, or shoeing. Make sure you follow these as well. Your pet can�t make those decisions for his or her own health, that is up to you. Don�t let them down.
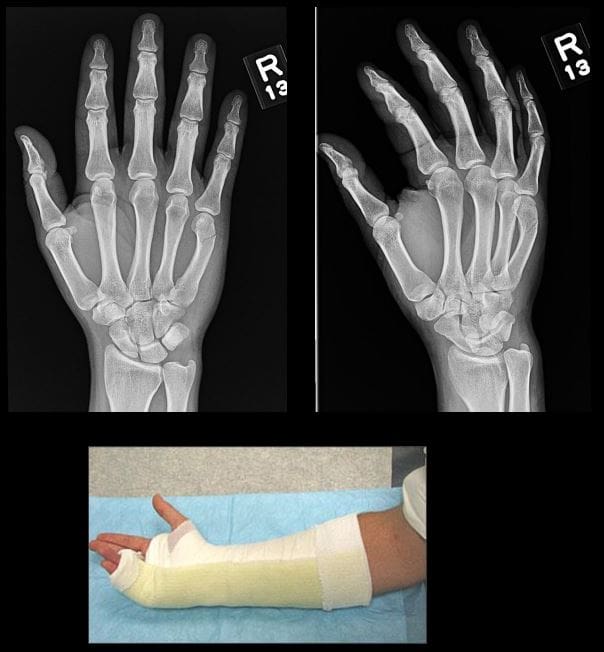
In all cases, Orthopedic hand surgical referral is required
Colles fx: m/c d/t FOOSH+pronation. m/c inOSP/elder women. Rare in men and if occurs need DEXA to avoid hip Fx etc. Young pts: high-energy trauma. Typically extra-articular.50%-cases show Ulna styloid (US) Fx.
Imaging: x-rad is sufficient, CT in complex Fx, MRI helps with ligament tears and TFC.
Rx: if extra-articular and <5-mm distal radius shortening and <5-degree dorsal angulation closed reduction+casting is sufficient. ORIF in complex cases.
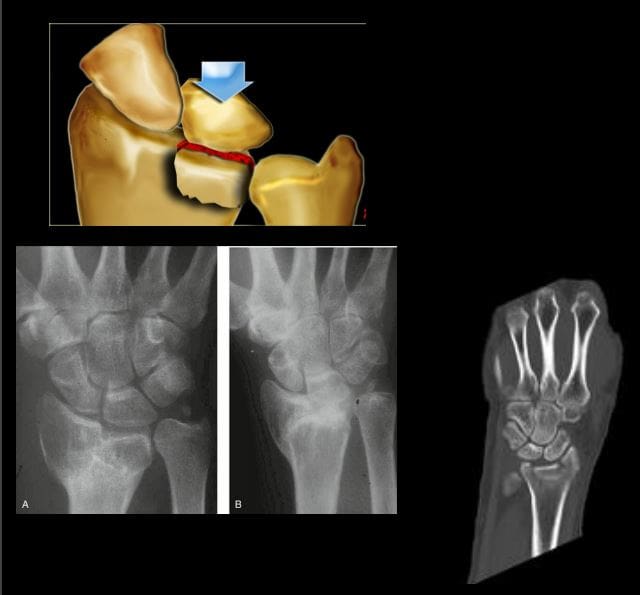
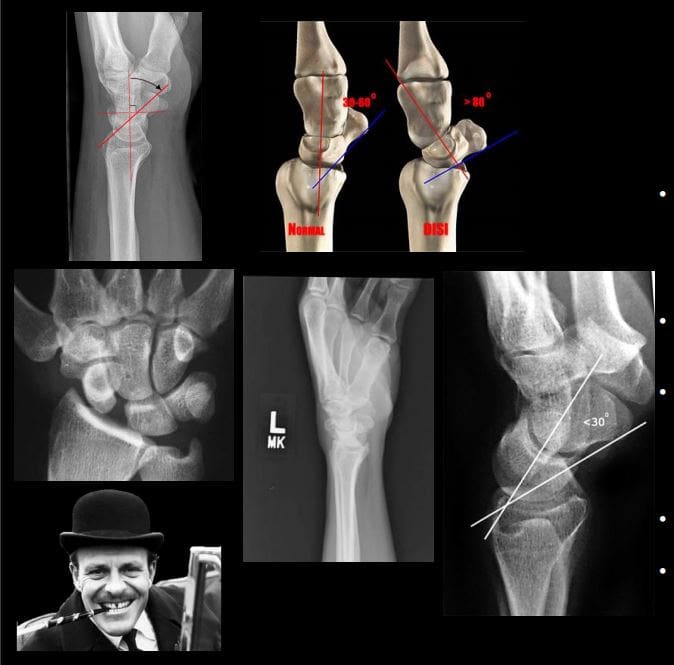
�Image Dx: distal rad impaction/shortening,dorsal angulation of distal fragment, carefully examine if intra-articular extension, 50% US Fx
Smith Fx: Goyrand in French literature. Considered as reversed Colles, otherwise almost identical, I.e., 85% extra-articular, 50%US Fx, OSP/elderly women, young pts-high-energy trauma. Differences: mechanismFOOSHwith flexed wrist thus m. Less frequent.
Imaging steps: (see Colles Fx) C
Complications: similar to Colles Fx
Rad Dx: 85% extra-articular with volar(anterior) angulation of the distal fragment,radial shortening. Carefully examine cortical breach suspecting intra-articular extension that can be named as Smith type 2 or Reversed Barton Fx (next)
Rx: similar approach as in Colles.
Barton fx: FOOSH, impaction of distal radius similar to Colles but the Fx line extends from the dorsal radial aspect into radiocarpal joint resulting with dorsal slip/dislocation of the carpus.
Imaging: 1st sept x-radiography often with CTto examine intra-articular Fx extension and operative planning
Rad Dx: distal radius Fx extending from dorsal into the radiocarpal joint with a variable degree of displacement, the proximal slip of the carpus
If Fx line extends from the volar aspect into the wrist joint named Reversed Barton aka Smith type 2 (above bottom image)
Complications: similar to all distal radius Fx
Rx: operative with ORIF
Chauffeur’s/backfire Fx aka Hutchinson Fx: intra-articular Fx of Radial styloid. The name derives from the time when the car had to be started with a hand crank that could backfire inducing wrist dorsiflexion and radial deviation.
Imaging: x-radiography is sufficient. CT may be helpful if Fx not readily shown by x-rays.
Rx: operative with percutaneous lagscrewin all cases d/t intra-articularnature
Die-Punch Fx: impaction Fx by the Lunate bone into distal articularLunate fossa of the Radius. IntraarticularFx. Derives its name from a technique to shape (impress) a hole in industrial machining “die-punch.”FOOSH injury.
Imaging: 1st step x-rays, may be equivocal d/t subtle depression of the Lunate fossa then CT scanning is most informative.
Rad Dx: impacted lunate fossa region with intra-articular Fx extension. This can present as a comminuted Fxarticular Fx of the Distal Radius.
Rx: operative d/t intra-articular Fx
Construct arcs of Gilula when evaluating carpal injuries. An Important step required to avoid missing subtle changes in carpal alignment and cortical continuity
Scaphoid bone Fx: m/c Fx carpal bone. D/tFOOSH wrist extended radially deviated. Location of Fx is most important to prognosis: Waist-m/c location (70%). May have 70-100%chance of AVN. Proximal pole Fx: 20-30% with a high risk of non-union. Distal pole-10%shows better prognosis. Distal pole Fx is m/c in children. Key clinical sign; pain in the snuffbox.
Imaging: 1st step-x-radiography but 15-20%missed d/t occult Fx. Special views required. Thus MRI is the most sensitive and specific for early occult Fx. Bone scintigraphy has98/100% specificity & sensitivity esp. 2-3 days after the onset. Key rad. Dx: Fx line if evident, displacement and obscuration of scaphoid(navicular) fat pad, examine for scapholunate dissociation. If proximal bone appears sclerotic-AVN occurred. MRI: low on T1 & high on T2/STIR/FSPD d/t bone edema, a�low signalFx line can be noted.
Rx: Spica cast should be applied if clinically suspected even w/o x-ray findings. For waistFx-cast for 3-mo for prox pole 5-mo immobilization. ORIF or percutaneous pinning with a Herbert screw.
Scapholunate Ligaments Dissociation
SNAC wrist: scaphoid non-union advanced collapse. Often d/t non-union and dissociation of scapholunate ligaments (SLL)with progressive radiocarpal and intercarpalDJD. The Proximal scaphoid fragment is attached to Lunate with distal dissociating and rotating�signet ring� sign on x-rays.
SNAC wrist may often result in DISI
Rx: progressive DJD may lead to four-corner arthrodesis
Scapholunate advanced collapse (SLAC wrist): SLLdissociation with progressive intercarpal and radiocarpal DJD and volar or dorsal carpal displacement (DISI & VISI). Causes: trauma, CPPD, DJD, Kienboch disease (AVN of Lunate), Preiserdisease (AVN of Scaphoid).
SLL dissociation will lead to Dorsal or VolarIntercarlate aka Intercarpal Segmental Instability (DISIor VISI).
Rad Dx: Dx underlying cause. X-rays demonstrate dorsal or volar angulation of the Lunate with increased or decreased scapholunate angle on the lateral view. On frontal view: Terry Thomas sign or widening of scapholunate distance 3-4-mm as the upper limit of normal.
�MRI may help with ligament evaluation and pre-surgical planning
Rx: often operative with late DJD. Four-corner arthrodesis
Triquetrum Fx: 2nd m/c carpal bone Fx. M/C dorsal aspect is avulsed by the�tough Dorsal radiocarpal ligament. Cause: FOOSH.
Imaging: x-radiography wrist series is sufficient. Best revealed on the lateral view as an avulsed bone fragment adjacent to the dorsum of the Triquetrum. CT may help if radiographically equivocal.
Rx: conservative care
Complications: rare, may persist as pain on the dorsum of the wrist
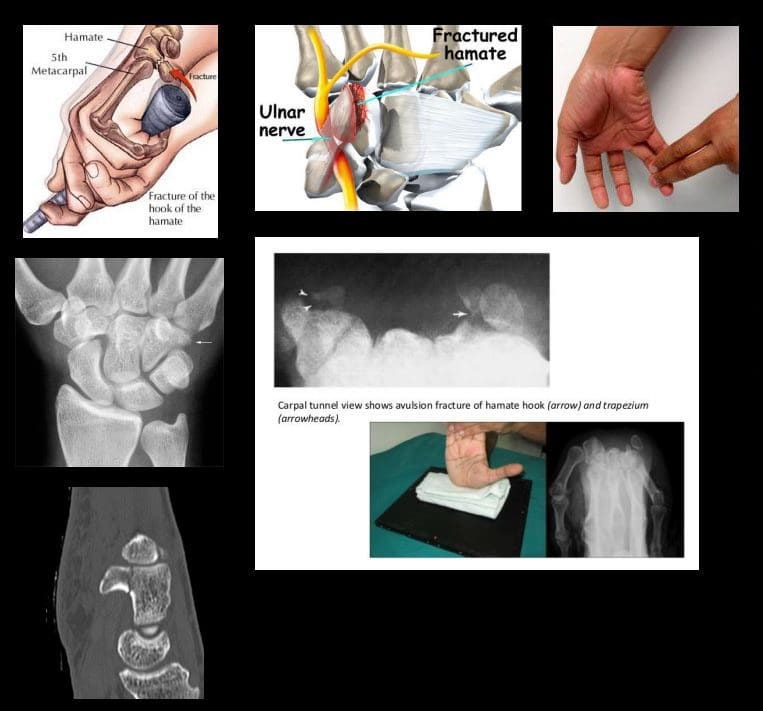
Hook of the Hamate Fx: m/c occurs in batting sports (cricket, baseball, hockey, impact by a golf club, etc.) 2% of carpusFx.
Imaging: x-radiography may fail to detect an Fx unless “carpal tunnel view” is used. CT may help if x-rays unrewarding.
Clinically: pain, positive pull test, weak, painful grip. Deep ulnar n. Branch may be affected within the�Guyon canal.
Rx: usually non-operative, but chronic non-union may require excision.
DDx: bipartite hamate
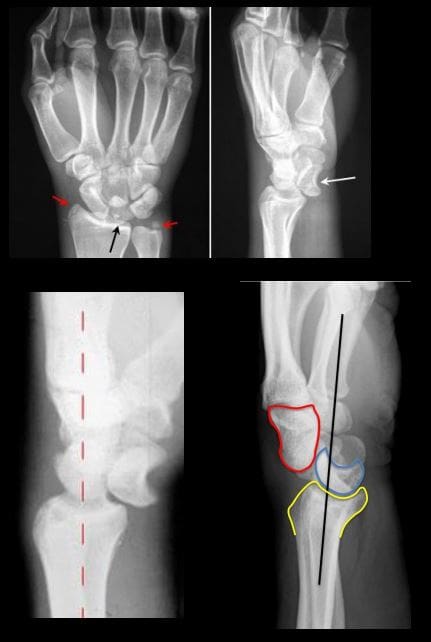
�Lunate vs. Perilunate dislocation: Lunate is m/c dislocated carpal bone. Overall infrequent carpal injury. However, often missed!
Occurs with FOOSH and wrist extended and ulnar deviated. Imaging: 1st step x-rays. Ifunrewarding or require more complex injury evaluation CT scanning.
Key Rad DDx: DDx Lunate from perilunate dislocation. Lunate dislocation: lunate lost its contact with distal radius �spilled teacup� on the lateral. Perilunate dislocation: Lunate maintains its contact with distal radius despite the Capitatedorsally dislocated. Lunate dislocation is additionally helped to identify a �pie sign� d/t Lunate overlapping the Capitate
Rx: emergency reduction and operative repair of torn ligaments
Metacarpal & Phalangeal Injuries
Bennett Fx: intra-articular but noncomminuted impact-type Fx of the base of 1st MC bone of the thumb. X-radiography is sufficient.
Rad Dx: characteristic triangular fragment of bone on the ulnar aspect of the 1st MCbase, often with radial subluxation of the remaining radial aspect of the 1st MC
Complications: DJD, non-union, etc.
Rx: prone to instability/non-union requiring an operative care
Rolando Fx: aka comminuted Bennett with Y or T-configuration. More complex injury. It is unstable requiring operative care
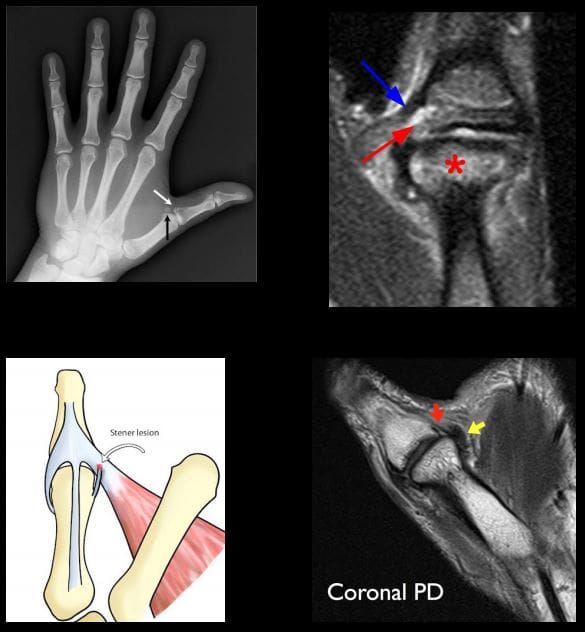
Gamekeeper thumb: traditionally described as a chronic tear of the�ulnar (medial) collateral ligament at 1stMCP in English Gamekeepers’ who performed neck twisting/killing of small game. An acute injury may also be named as Skier’s thumb. This injury can be ligamentous w/o a fracture and an avulsion injury at the 1st proximal phalanx base.
Complication: Stener lesion or displacement of torn ligament over Adductor pollicis muscle that cannot heal w/o surgical repair. MRI Dx is required.
Avoid thumb stress views that can induce a Stenerlesion
Imaging: x-radiography followed by MRI to Dx Stenerlesion. MSK US can be used if MRI is unavailable.
�Stener lesion on MRI & MSUS: ulnar collateral stump is more superficial to Adductor pollicis aponeurosis and appears like a low signal mass-like stump forming so-called “yo-yo on the string sign” reported both on MRI and MSK US.
Rx: often operative
Boxer Fx: m/c MC Fx. An extra-articular usually non-comminuted or minimal comminuted Fx through m/c the 5th and sometimes the 4th MCneck-head junction (occasionally through the shaft) resulting in volar head angulation. Mechanism: direct impact as in clenched fist punching hard surface (e.g., facial bones/wall punching) hence 95% in young males.
Imaging: x-radiography hand series is sufficient
Rad Dx: Fx line transverse or oblique through MCneck with volar head angulation. Evaluate the degree of displacement, critical to report.
N.B. If the same mechanism fractures the 2ndand 3d MC in the same anatomic area, it may require operative care.
Phalangeal hand Fx: m/c skeleton Fx (10% of all Fx). Sports and industrial injuries dominate
Imaging: x-radiography with hand series or PA/lateral finger views will suffice
Rad Dx: if prox phalanx Fx, distal fragment is angled volarly with prox fragment dorsally. Distal phalanx may be angled dorsally. Key observation: nail bed injury, which considered an open Fx with a�risk of infection.
Rx: if <10-degree angulation-buddy-taping with motion rehab. CRPP vs. ORIF can be considered in complex cases-Orthopedic hand surgeon referral
Complication: loss of motion, necrosis, infection.May result with amputation
For additional common injuries: PIP is m/c dislocated joint. Mullet (Baseball) finger, Jersey finger and other injury refer to:
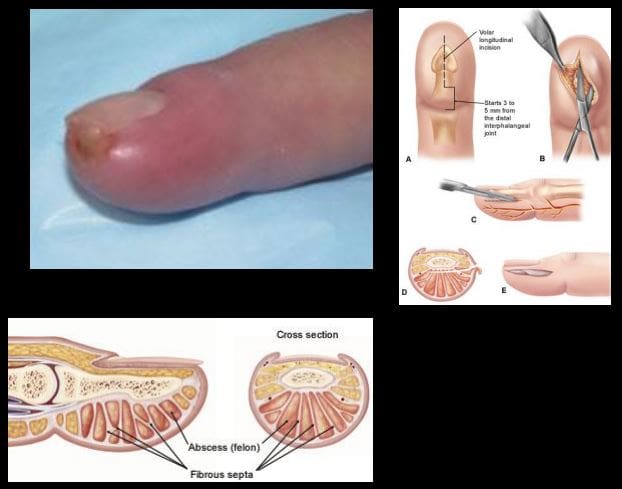
Felon: septic infection of the fingertip pulp typically with Staph.Aureus. Causes: needle prick(diabetics), paronychia, nail splinters, etc. m/c in index and thumb, presenting with pain, swelling, etc.
D/t specific pulp anatomy theinfection>swelling leads to pulp compartment syndrome-pressure and necrosis.
Rx: operative with incision distal to DIP, irrigation/debridement
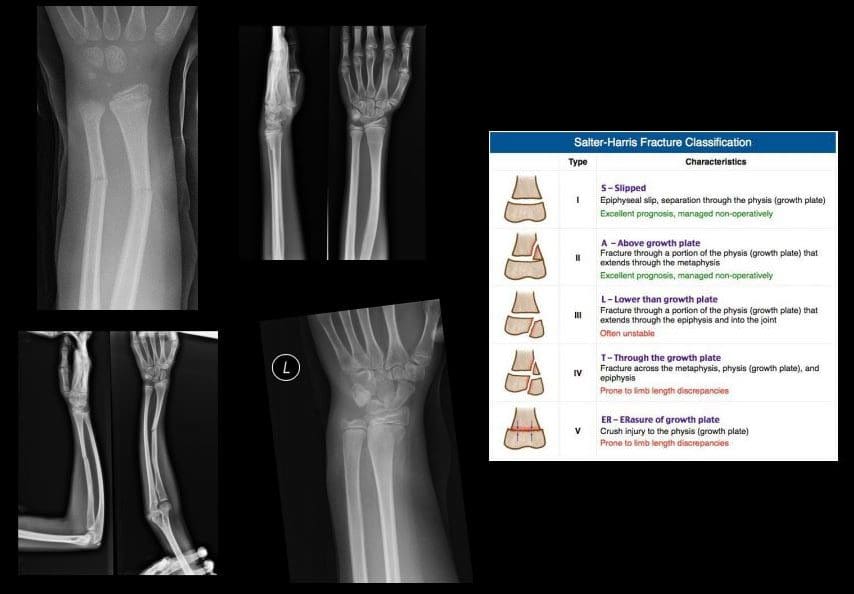
Pediatric Wrist Injury
Incomplete Fx: Greenstick Fx, Torus (Buckle)Fx, Bowing (Plastic) deformity/Fx. D/t FOSHe.g. fell off the monkey bar. m/c affects <10-years-old.
Rx: usually non-operative (closed reduction and casting)
Distal Radioulnar Joint (DRUJ) Instability-common injury following trauma as in FOOSHwith wrist hyperextension and rotation and disruption of DRUJ ligaments and TFCcomplex. Avulsion of ulnar styloid with the�dorsal or volar displacement of distal ulnar should be noted.
Imaging steps: x-rays initially, MRI may identify ligaments and TFC damage, MSKUScan help with ligaments tearing.
Wrist DJD-typically is secondary to trauma, scapholunate dissociation, SLAC, SNAC wrist, CPPD, Keinboch or Preiser Disease and others.
May lead to major functional loss
Imaging: typically presents as radiocarpal JSL, subchondral sclerosis,osteophytosis, subcortical cysts, and loose bodies. Typically additional induces intercarpal degeneration and particularly Tri-scaphe joint.
MRI may be helpful with early recognition of scapholunate dissociation, Lunate/Navicular AVN.
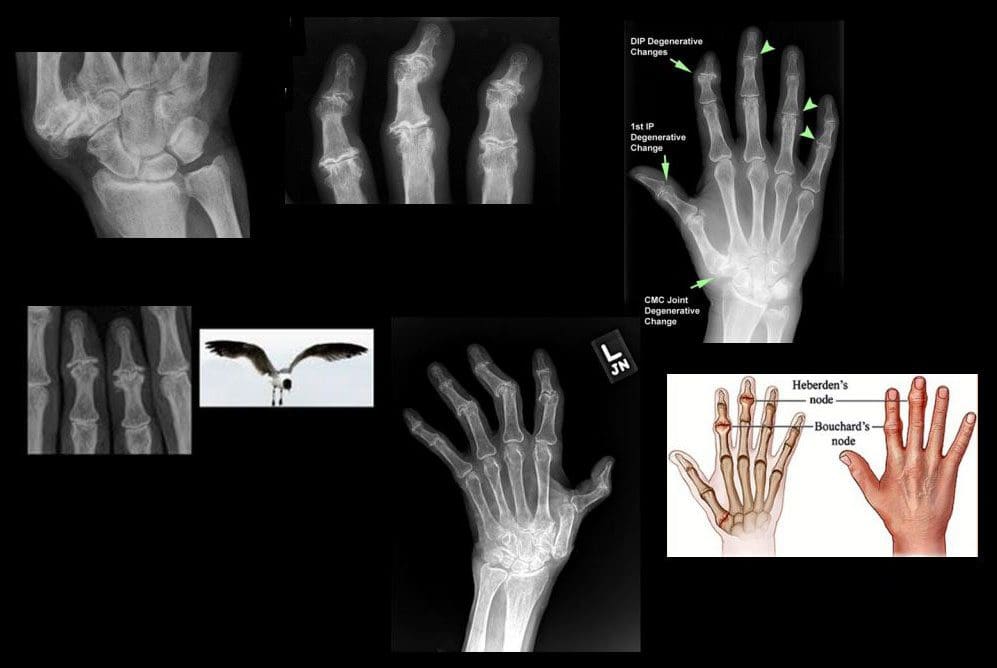
If isolated MCP OA noted considerCPPD & Hemochromatosis (Hook-like osteophytes)
Clinically:
Mid-age females
Typically painless except 1st CMC OA
DIPs-Heberden nodes, PIPs-Bouchard nodes
Erosive OA (occasionally called�inflammatory OA�)
A Spectrum of OA but producing central proximal erosions at DIPs and PIPsresulting with very characteristic �gullwing� appearance. No systemic inflammation (no CRP, RF, Anti-CCP Ab)typically in middle-aged/elderly females, like Hand OA, often seen in families
Rheumatoid Arthritis
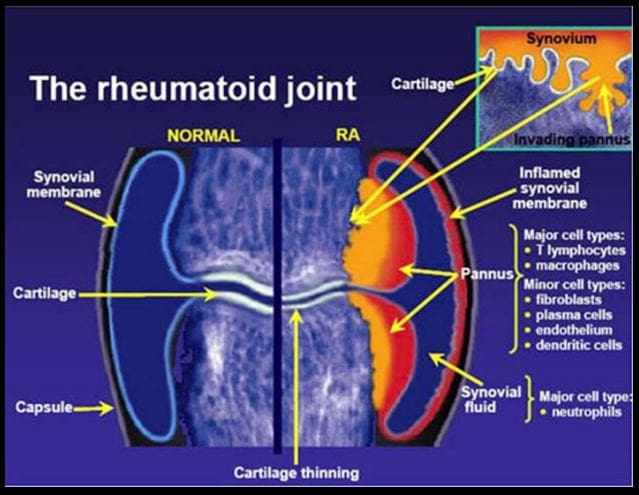
Rheumatoid Arthritis (RA)-chronic systemic inflammatory disease of unknown etiology, targeting synovial joints, tendons with multiple systemic involvement (lung, CVS, Ocular, Skin, etc.) Pathology: Tcell>Macrophage/APC>mediatedautoimmune process resulting in pannus formation and gradual destruction of ST, cartilage, bone,�and other tissues. 3% FemalesVS.1% Males. Environmental triggers: infection, trauma, smoking,�and others in a genetically susceptible individual. 20-30%may be disabled after 10-years.
Arthritis is characterized as the inflammation of one or multiple joints. The most common symptoms of arthritis include pain and discomfort, swelling, inflammation, and stiffness, among others. Arthritis may affect�any joint in the human body, however, it commonly develops in the knee. � Knee arthritis can make everyday�physical activities difficult. The most prevalent types of arthritis are osteoarthritis and rheumatoid arthritis, although there are well over 100 distinct forms of arthritis, affecting children and adults alike. While there is no cure for arthritis, many treatment approaches can help treat the symptoms of knee arthritis.
Anatomy of the Knee
� The knee is the largest and strongest joint in the human body. It is made up of the lower end of the thigh bone,�or femur, the top end of the shin bone, or tibia, and the kneecap, or patella. The ends of the three bones are covered with articular cartilage, a smooth, slippery structure which protects and cushions the bones when bending and straightening the knee.
� Two wedge-shaped parts of cartilage, known as the meniscus, function as shock absorbers between the bones of the knee to help cushion the joint and provide stability. The knee joint is also surrounded by a thin lining known as the synovial membrane. This membrane releases a fluid which lubricates the cartilage and also helps reduce friction in the knee. The significant kinds of arthritis that affect the knee�include osteoarthritis, rheumatoid arthritis, and post-traumatic arthritis.
Osteoarthritis
� Osteoarthritis is the most common type of arthritis which affects the knee joint. This form of arthritis is a degenerative, wear-and-tear health issue which occurs most commonly in people 50 years of age and older, however, it may also develop in younger people.
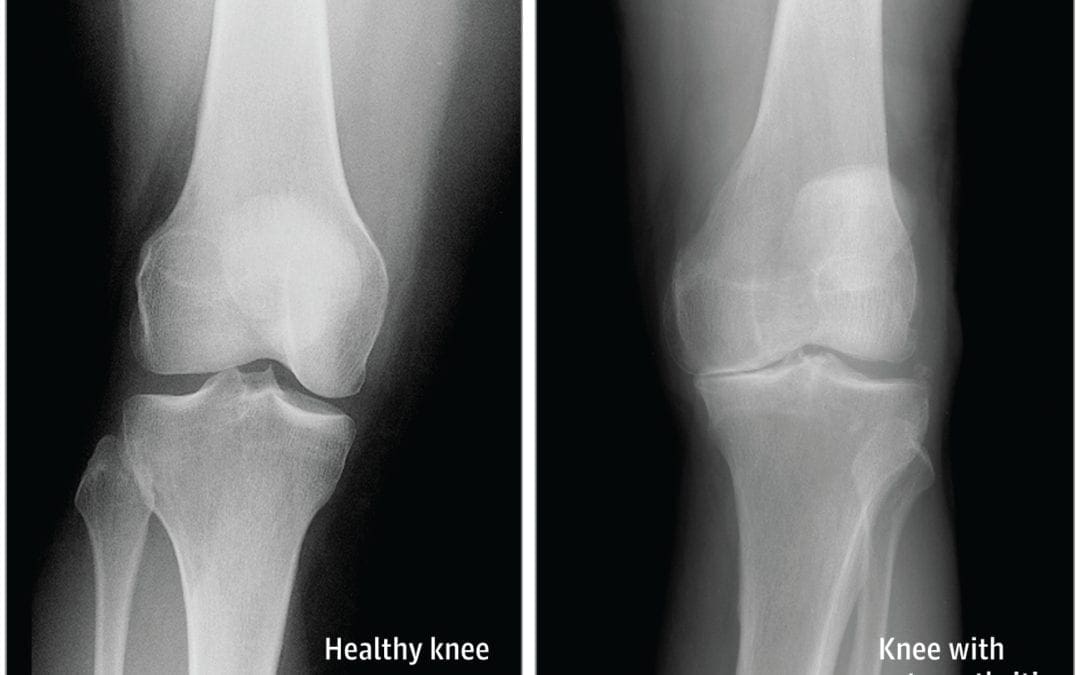
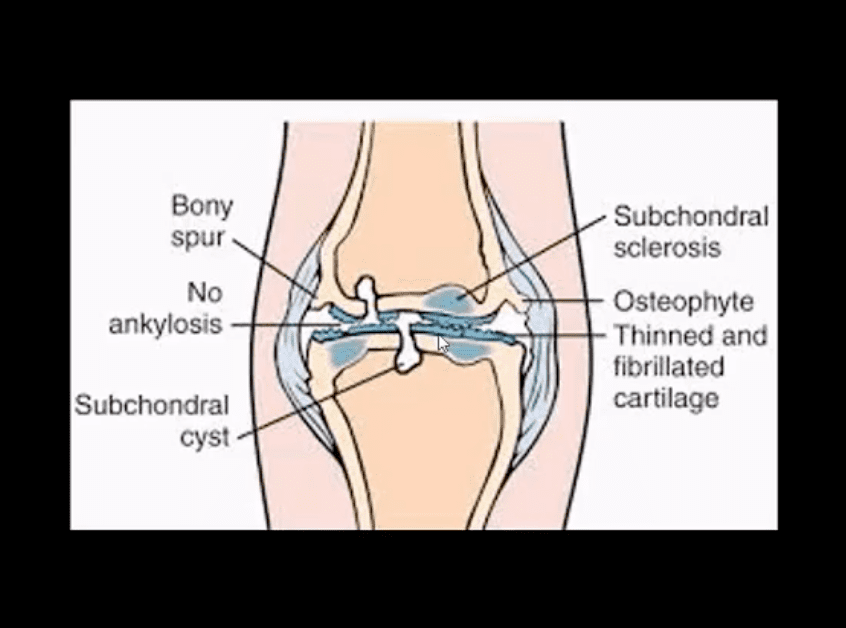
� In osteoarthritis, the cartilage in the knee joint gradually wears away. As the cartilage wears away, the distance between the bones decreases. This can result in bone rubbing and it can�create painful bone spurs. Osteoarthritis generally develops slowly but the pain may worsen over time.
Rheumatoid Arthritis
� Rheumatoid arthritis is a chronic health issue which affects multiple joints throughout the body, especially the knee joint. RA is also symmetrical, meaning it often affects the same joint on each side of the human body.
� In rheumatoid arthritis, the synovial membrane that covers the knee joint becomes inflamed and swollen, causing knee pain, discomfort, and stiffness. RA is an autoimmune disease, which means that the immune system attacks its own soft tissues. The immune system attacks healthy tissue,�including tendons, ligaments and cartilage, as well as softens the bone.
Post-traumatic Arthritis
� Posttraumatic arthritis is a form of arthritis that develops after damage or injury to the knee. By way of instance, the knee joint may be harmed by a broken bone, or fracture, and result in post-traumatic arthritis years after the initial injury. Meniscal tears and ligament injuries can cause additional wear-and-tear on the knee joint, which over time can lead to arthritis and other problems.
Symptoms of Knee Arthritis
� The most common symptoms of knee arthritis include pain and discomfort, inflammation, swelling, and stiffness. Although sudden onset is probable, the painful symptoms generally�develop gradually over time. Additional symptoms of knee arthritis can be recognized as follows:
The joint may become stiff and swollen, making it difficult to bend and straighten the knee.
Swelling and inflammation may be worse in the morning, or when sitting or resting.
Vigorous activity might cause the pain to flare up.
Loose fragments of cartilage and other soft tissue may interfere with the smooth motion of the joints, causing the knee to lock or stick through motion. It could also creak, click, snap or make a grinding sound, known as crepitus.
Pain can cause a sense of fatigue or buckling from the knee.
Many individuals with arthritis may also describe increased joint pain with rainy weather and climate changes.
Diagnosis for Knee Arthritis
� During the patient’s appointment for diagnosis of knee arthritis, the healthcare professional will talk about the symptoms and medical history, as well as conduct a physical examination. The doctor may also order imaging diagnostic tests, such as X-rays, MRI or blood tests for further diagnosis. During the physical examination, the doctor will search for:
Joint inflammation, swelling, warmth, or redness
Tenderness around the knee joint
Assortment of passive and active movement
Instability of the knee joint
Crepitus, the grating sensation inside the joint, with motion
Pain when weight is placed on the knee
Issues with gait, or manner of walking
Any signs of damage or injury to the muscles, tendons, and ligaments surrounding the knee joint
Involvement of additional joints (an indicator of rheumatoid arthritis)
Imaging Diagnostic Tests
X-rays. These imaging diagnostic tests produce images of compact structures, such as bones. They can help distinguish among various forms of arthritis. X-rays for knee arthritis may demonstrate a portion of the joint distance, changes in the bone as well as the formation of bone spurs, known as osteophytes.
Additional tests. Sometimes, magnetic resonance imaging, or MRI, scans, computed tomography, or CT,�scans, or bone scans are required to ascertain the condition of the bone and soft tissues of the knee.
Blood Tests
� Your doctor may also recommend blood tests to determine which type of arthritis you have. With some kinds of arthritis, such as rheumatoid arthritis, blood tests can help with the proper identification of the disease.
Although the knee joint is one of the strongest and largest joints in the human body, it is often prone to suffering damage or injury, resulting in a variety of conditions. In addition, however, other health issues, such as arthritis, can affect the knee joint. In network for most insurances of El Paso, TX, chiropractic care can help ease painful symptoms associated with knee arthritis, among other health issues. Dr. Alex Jimenez D.C., C.C.S.T. Insight
�
Treatment for Knee Arthritis
Non-surgical Treatment
� Non-surgical treatment approaches are often recommended before considering surgical treatment for knee arthritis. Healthcare professionals may recommend a variety of treatment options, including chiropractic care, physical therapy, and lifestyle modifications, among others.
� Lifestyle modifications. Some lifestyle modifications can help protect the knee joint and impede the progress of arthritis. Minimizing physical activities which aggravate the condition, will put less strain on the knee. Losing weight may also help lessen stress and pressure on the knee joint, resulting in less painful symptoms and increased function.
� Chiropractic care and physical therapy.�Chiropractic care utilizes full body chiropractic adjustments to carefully restore any spinal misalignments, or subluxations, which may�be causing symptoms, including arthritis. The doctor may also recommend physical therapy to create an individualized exercise and physical activity program for each patient’s needs.�Specific exercises will help increase range of motion and endurance, as well as help strengthen the muscles in the lower extremities.
� Assistive devices. Using assistive devices, such as a cane, shock-absorbing shoes or inserts, or a brace or knee sleeve, can decrease painful symptoms. A brace helps with function and stability, and may be particularly useful if the arthritis is based on one side of the knee. There are two types of braces that are often used for knee arthritis: A “unloader” brace shifts weight from the affected section of the knee, while a “support” brace helps support the entire knee load.
� Drugs and/or medications. Several types of medications are useful in treating arthritis of the knee. Since individuals respond differently to medications, your doctor will work closely with you to determine the medications and dosages which are safe and effective for you.
Surgical Treatment
� The healthcare professional may recommend surgical treatment if the patient’s knee arthritis causes severe disability and only if the problem isn’t relieved with non-surgical treatment. Like all surgeries, there are a few risks and complications with surgical treatment for knee arthritis. The�doctor will discuss the possible problems with the patient.
� Arthroscopy. During arthroscopy, physicians use instruments and small incisions to diagnose and treat knee joint problems. Arthroscopic surgery isn’t frequently used in the treatment of arthritis of the knee. In cases where osteoarthritis is accompanied with a degenerative meniscal tear, arthroscopic surgery may be wise to treat the torn meniscus.
� Cartilage grafting. Normal cartilage tissue may be taken from a tissue bank or through a different part of the knee to fill out a hole in the articular cartilage. This process is typically considered only for younger patients.
� Synovectomy. The lining damaged by rheumatoid arthritis is eliminated to reduce swelling and pain.
� Osteotomy. In a knee osteotomy, either the tibia (shinbone) or femur (thighbone) is cut then reshaped to relieve stress and pressure on the knee joint. Knee�osteotomy is utilized when early-stage osteoarthritis has damaged one facet of the knee joint. By changing the weight distribution, this can relieve and enhance the function of the knee.
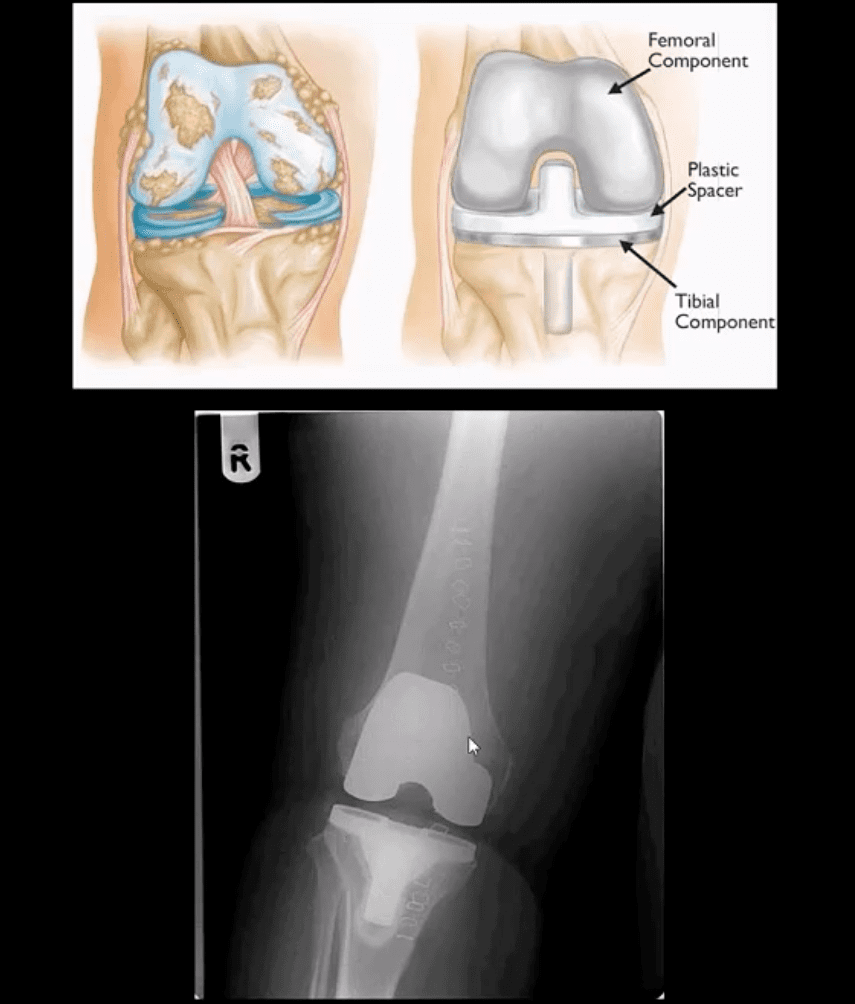
� Total or partial knee replacement (arthroplasty).�The�doctor will remove the damaged bone and cartilage, then place new plastic or metal surfaces to restore the function of the knee�and its surrounding structures.
� Following any type of surgery for knee�arthritis will involve a period of recovery. Recovery time and rehabilitation will depend on the type of surgery performed. It’s essential to talk with your healthcare professional to determine the best treatment option for your�knee arthritis. The scope of our information is limited to chiropractic and spinal health issues. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
� Curated by Dr. Alex Jimenez �
�
Additional Topic Discussion: Relieving Knee Pain without Surgery
� Knee pain is a well-known symptom which can occur due to a variety of knee injuries and/or conditions, including�sports injuries. The knee is one of the most complex joints in the human body as it is made-up of the intersection of four bones, four ligaments, various tendons, two menisci, and cartilage. According to the American Academy of Family Physicians, the most common causes of knee pain include patellar subluxation, patellar tendinitis or jumper’s knee, and Osgood-Schlatter disease. Although knee pain is most likely to occur in people over 60 years old, knee pain can also occur in children and adolescents. Knee pain can be treated at home following the RICE methods, however, severe knee injuries may require immediate medical attention, including chiropractic care.
Sagittal Fluid Sensitive MR slice showing large synovial popliteal (Baker’s) cyst (above top image) and sizeable synovial effusion (above bottom image)
Note multiple patchy dark signal areas on both images, representing fibrinoid inflammatory deposits aka “rice bodies” a characteristic MRI feature of RA
Management Rheumatological Referral & DRM
Conservative management followed by operative care in complicated cases of tendon ruptures and joints dislocations
Supplemental reading:
Diagnosis and Management of Rheumatoid Arthritis – AAFP
Septic arthritis – d/t bacterial or fungal contamination of the joint. SA may cause rapid joint destruction and requires prompt Dx and antibiotic administration
Joints affected: large joints with rich blood supply (knee 50%>hips>shoulders).
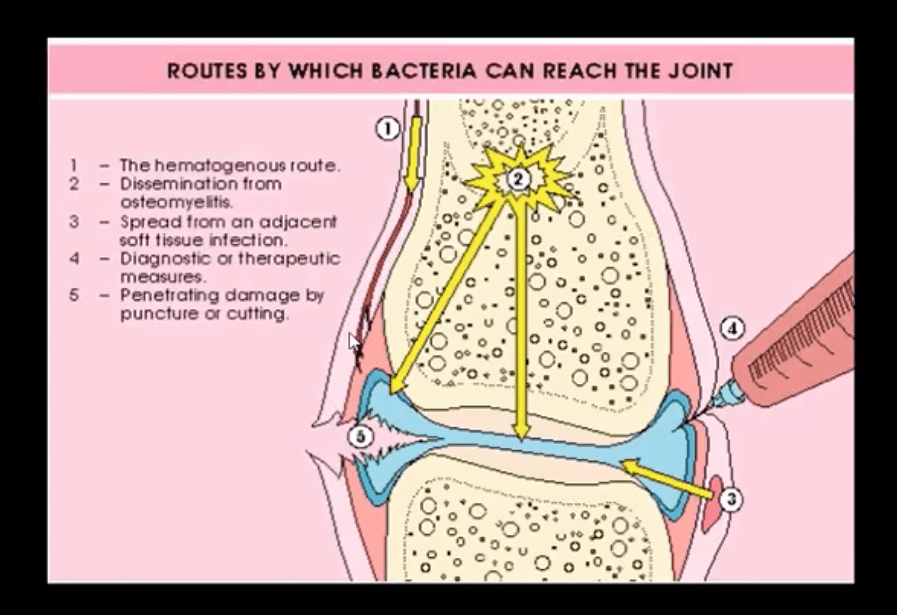
Routs of Infection:
1) Hematogenous is m/c
2) Spread from an adjacent site
3) Direct implantation (e.g., trauma, iatrogenically)
Patients at risk: children, diabetics, immunocompromised, pre-existing joint damage/inflammation, e.g., RA, etc.
I.V. drug users are particularly at risk and also may contaminate atypical joints “the S joints” SIJ, SCJ, Symphysis pubis, ACJ, etc.
Clinically: may vary and depends on host immune response and bacterial virulence. May present with rapid onset or exacerbation of pre-existing joint pain, swelling, limitation of ROM. General signs of malaise, fever, fatigue and elevated ESR, CRP, Leucocytosis may be present.
N.B. Diabetics and immunocompromised may present with fewer manifestations and lack of fever d/t declining immune response
Dx: clinical, radiological and laboratory. Arthrocentesis may be necessary for culture, cell count and purulent synovial examination
Management: I.V. antibiotics
Imaging Dx: begins with radiography but in the early stage most likely will be unremarkable. MRI can be sensitive and help with early identification of joint effusion, bone edema, etc. US may be helpful in the superficial joints and children. US helps with needle guidance. Bone scintigraphy may be used occaisonally if MRI is contraindicated
Routes of Joint Contamination
1. Hematogenous (M/C)
2. Spread from the adjacent site
3. Direct inoculation
M/C organism-Staph aureus
N.B Gonococcal infection may be a top differential in some cases
IV drug users: Pseudomonas, candida
Sickle cell: Salmonella
Animal (cats/dogs) bites: Pasteurella
Occasionally fungal contamination may occur
Radiography
Initially non-specific ST/joint effusion, obscuration/distortion of fat planes. Because it takes 30% of compact and 50-75% trabecular bone to be destroyed before seen on x-rays, radiography is insensitive to some of the early changes. MR imaging is the preferred modality
If MRI is not available or contraindicated. Bone scintigraphy with Tc-99 MDT can help
In children, US preferred to avoid ionizing radiation. In children, US can be more sensitive than in adults due to lack of bone maturation
Radiographic Dx
Early findings are unrewarding. Early features may include joint widening d/t effusion. Soft tissue swelling and obscuration/displacement of fat planes
1-2 weeks: periarticular and adjacent osseous changes are manifesting as patchy demineralization, moth-eaten, permeating bone destruction, loss, and indistinctness of the epiphyseal “white cortical line” with an increase in soft tissue swelling. MRI may be helpful with early Dx.
Late features: complete joint destruction and ankyloses
N.B. Septic arthritis may progress rapidly within days and requires early I.V. antibiotic to prevent major joint destruction
T1 & T2 Knee MRI
T1 (above left) and T2 fat-sat sagittal knee MRI slices reveal loss of normal marrow signal on T1 and increase on T2 due to septic edema. Bone sequestrum d/t osteomyelitis progressing into septic arthritis is noted. Marked joint effusion with adjacent soft tissue edema is seen. Dx: OSM and septic arthritis
Imaging may help the Dx of the septic joint. However, the final Dx is based on Hx, physical examination, blood tests and most importantly synovial aspiration (arthrocentesis)
Synovial fluid should be sent for Gram staining, culture, glucose testing, leukocyte count, and differential determination
ESR/CRP may be elevated
Synovial fluid: WBC can be 50,000-60,000/ul, with 80% neutrophils with depleted glucose levels Gram stain: in 75% gram-positive cocci. Gram staining is less sensitive in gonococcal infection with only 25% of cultures +
In 9% of cases, blood cultures are the only source of pathogen identification and should be obtained before antibiotic treatment
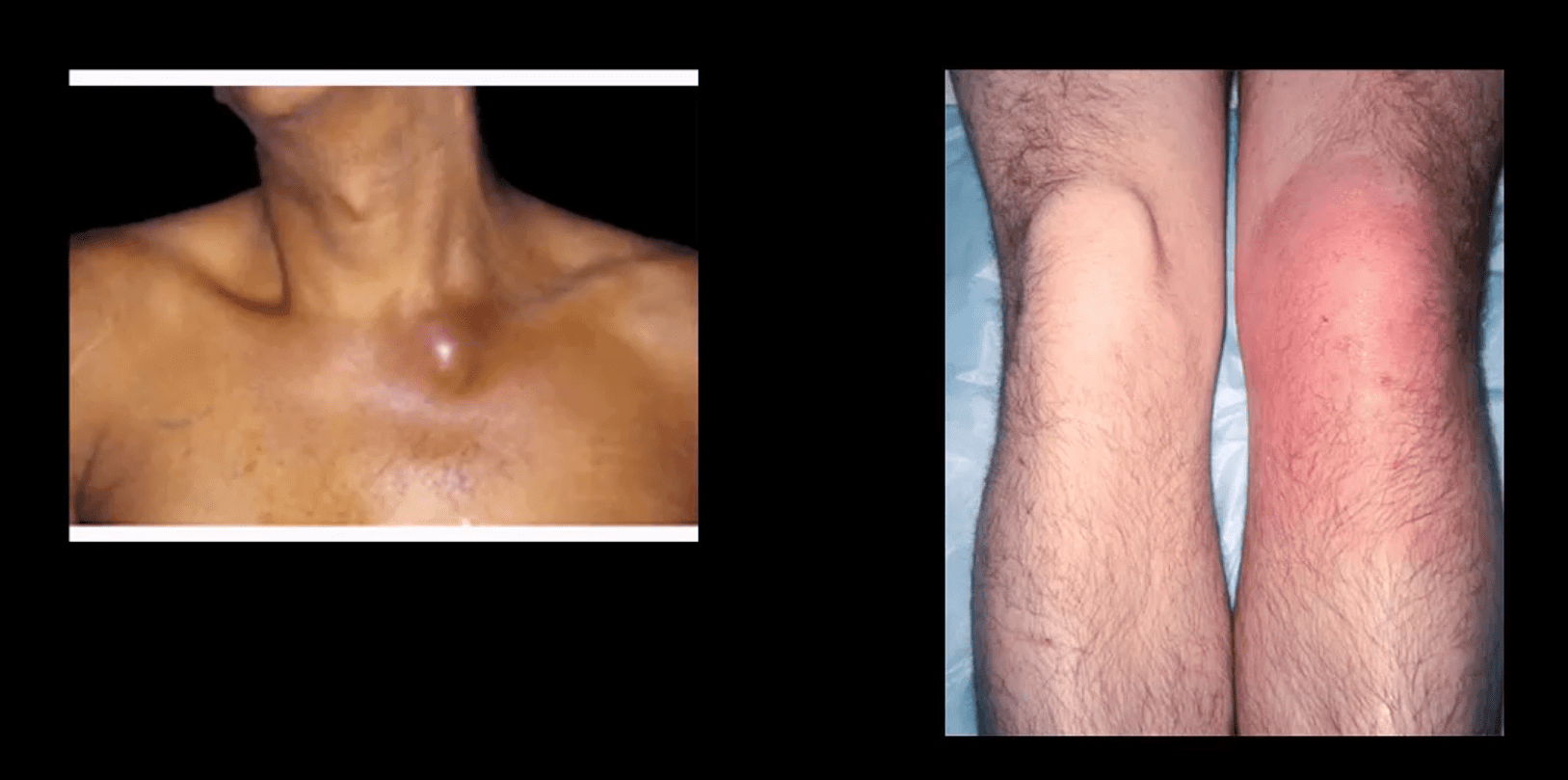
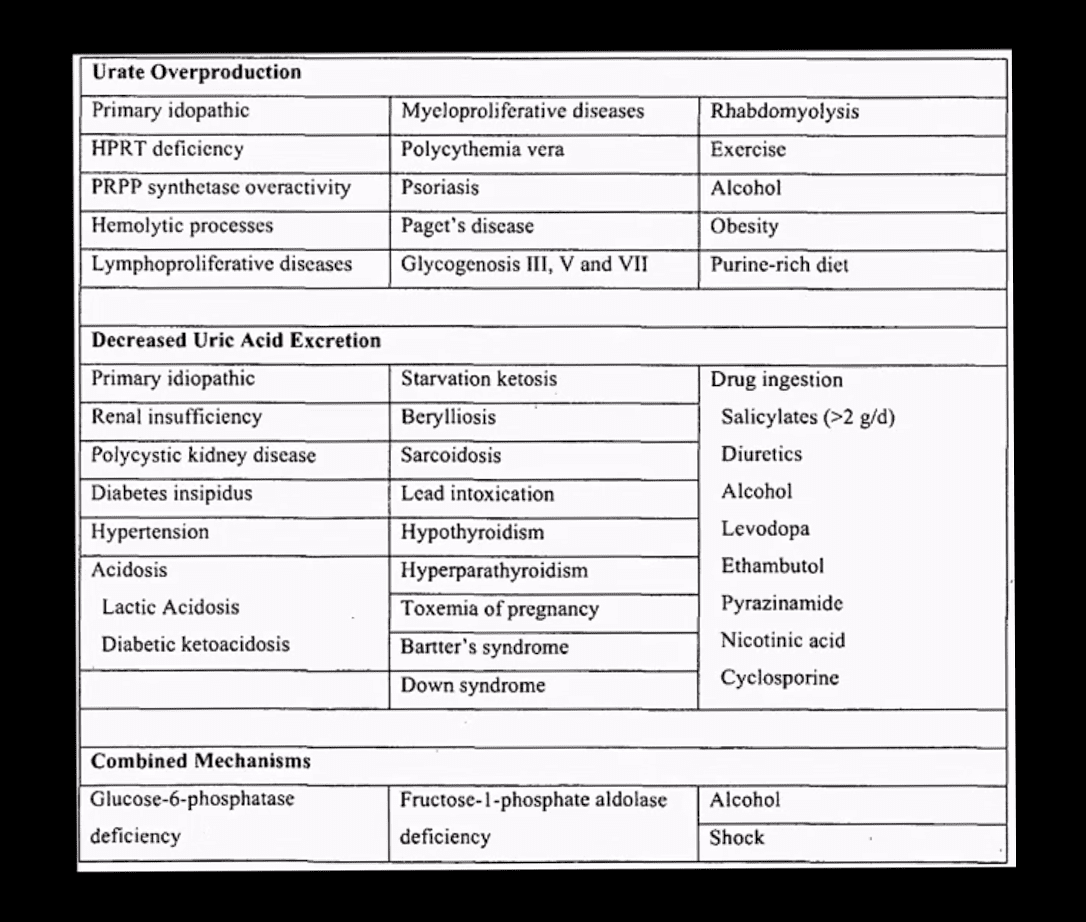
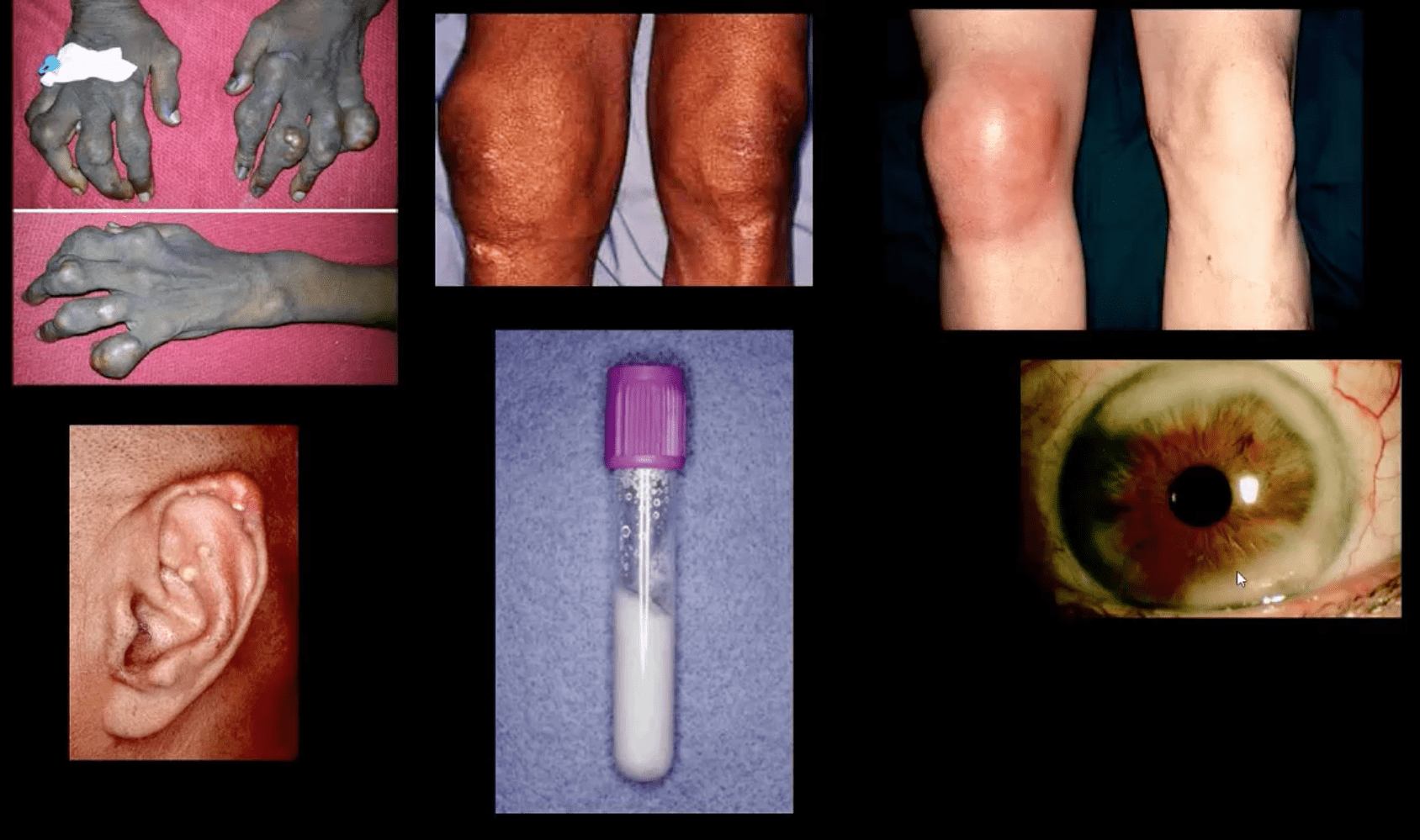
Gout: MSU deposition in and around joints and soft tissues. Elevated levels of serum uric acid (UA) (>7mg/dL) caused by overproduction or under-excretion of uric acid
Once UA reached/exceeded 7mg/dL, it will deposit in the peripheral tissues. Primary gout: disturbed metabolism of nucleic acids and purines break down. Secondary gout: increased cell turnover: Psoriasis, leukemia, multiple myeloma, hemolysis, chemotherapy, etc.
Gout presents with 5-characteristic stages:
1)asymptomatic hyperuricemia (years/decades)
acute attacks of gouty arthritis (waxes and wanes and lasts for several years)
Interval phase between attacks
Chronic tophaceous gout
Gouty nephropathy
Clinical Presentation
Depends� on stages
Acute attacks: acute joint pain “first and the worst” even painful to light touch
DDx: septic joint (both may co-exist) bursitis etc.
Gouty arthritis typically presents as monoarthropathy
Chronic tophaceous stage: deposits in joints, ear pinna, ocular structures, and other regions. Nephrolithiasis etc. Men>women. Obesity, diet, and age >50-60.
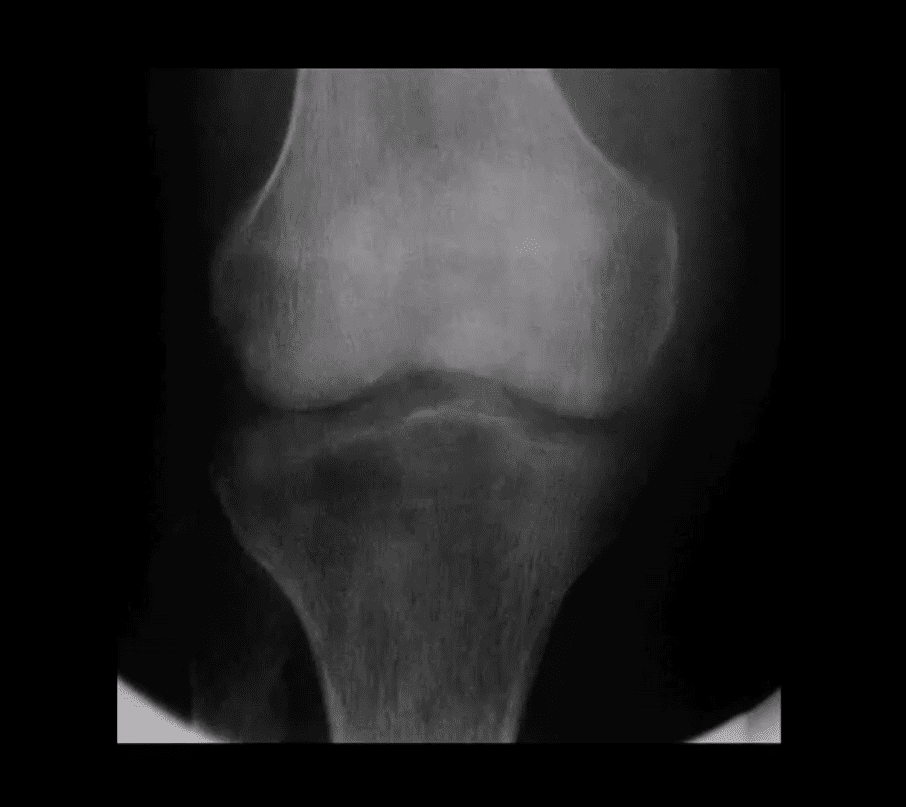
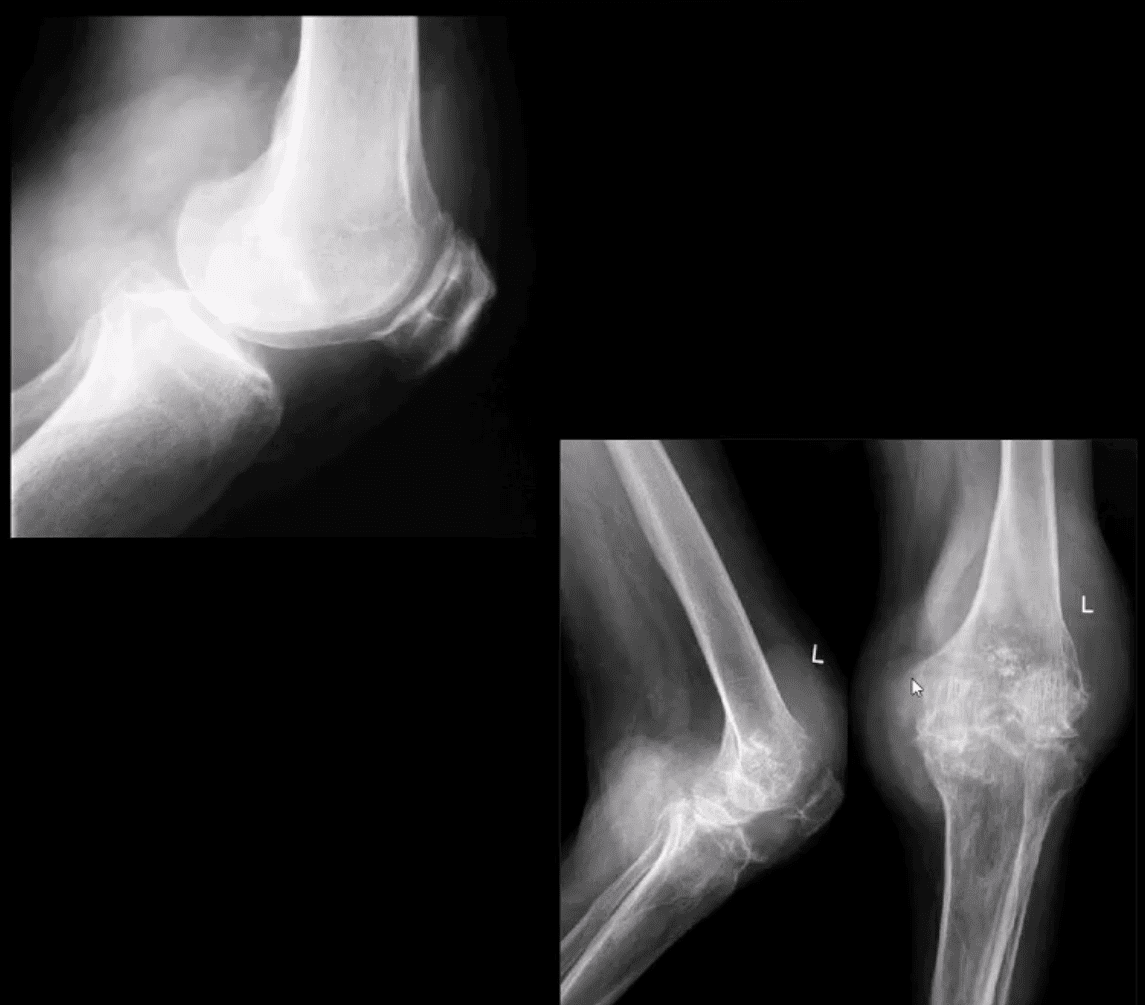
Radiography: early attacks are unremarkable and may present as non-specific joint effusion
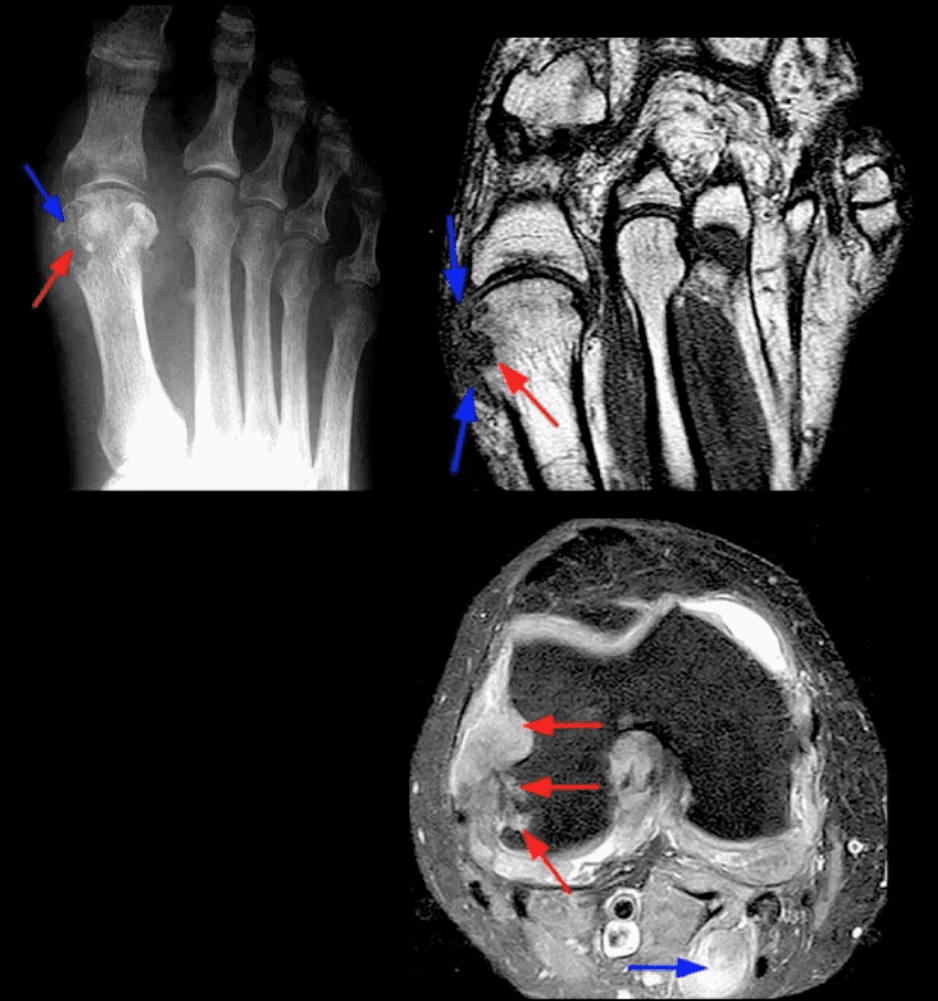
Chronic tophaceous gout radiography: punched out peri-articular, para-articular and intraosseous erosions with overhanging edges. A characteristic rim of sclerosis and internal calcification, soft tissue tophi. Target sites: lower extremity m/c
Rx: allopurinol, colchicine (esp. preventing acute episodes and maintenance)
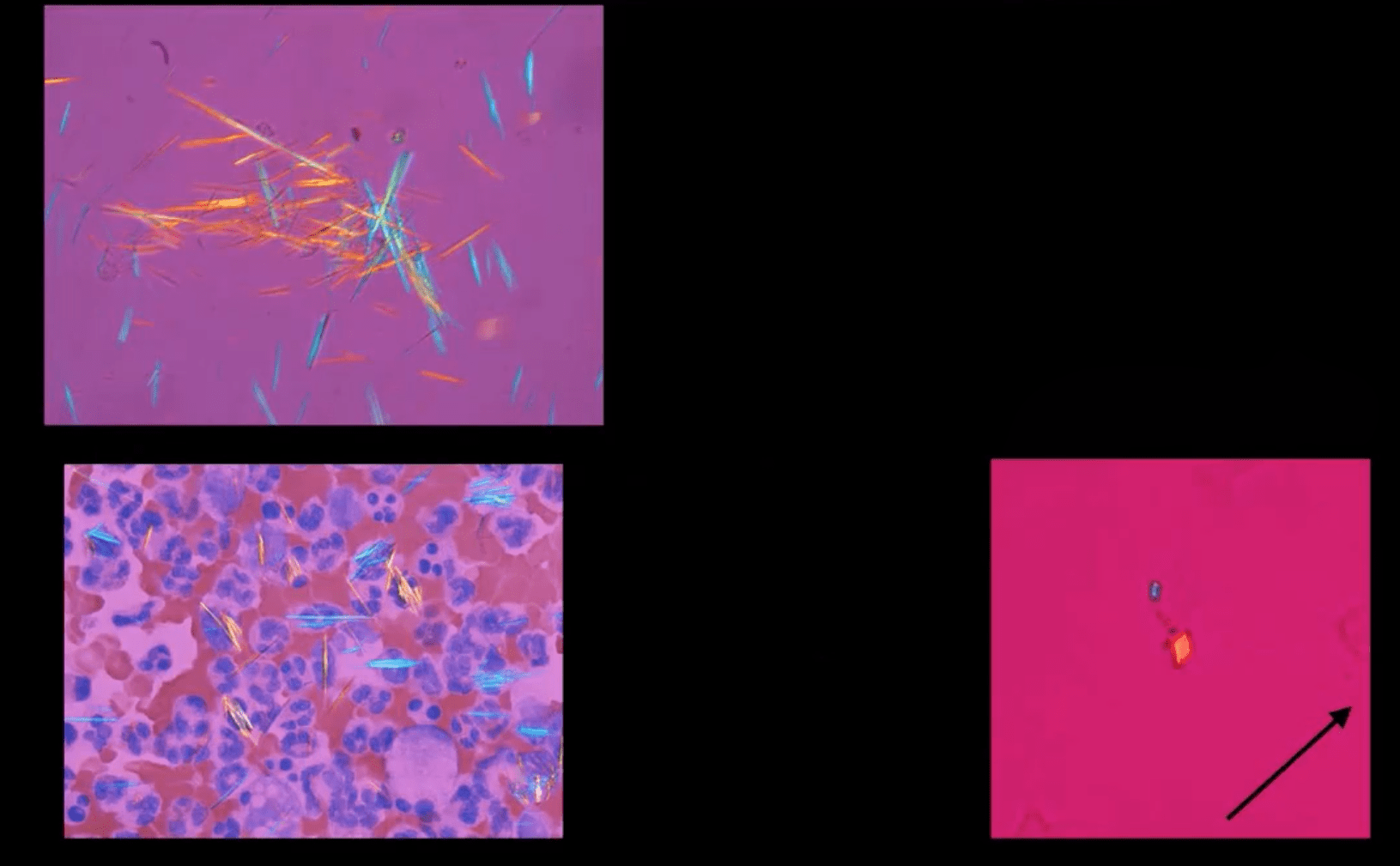
Synovial Aspiration
Synovial aspiration with polarized microscopy reveal negatively birefringent needle-shaped MSU crystals with large inflammatory PMN presence. DDx: positively birefringent rhomboid-shaped CPPD crystals (above bottom right) seen in Pseudogout and CPPD
Large S.T.
Density and joint effusion punched out osseous erosion with overhanging margins, overall preservation of bone density, internal calcifications Dx: chronic tophaceous gout
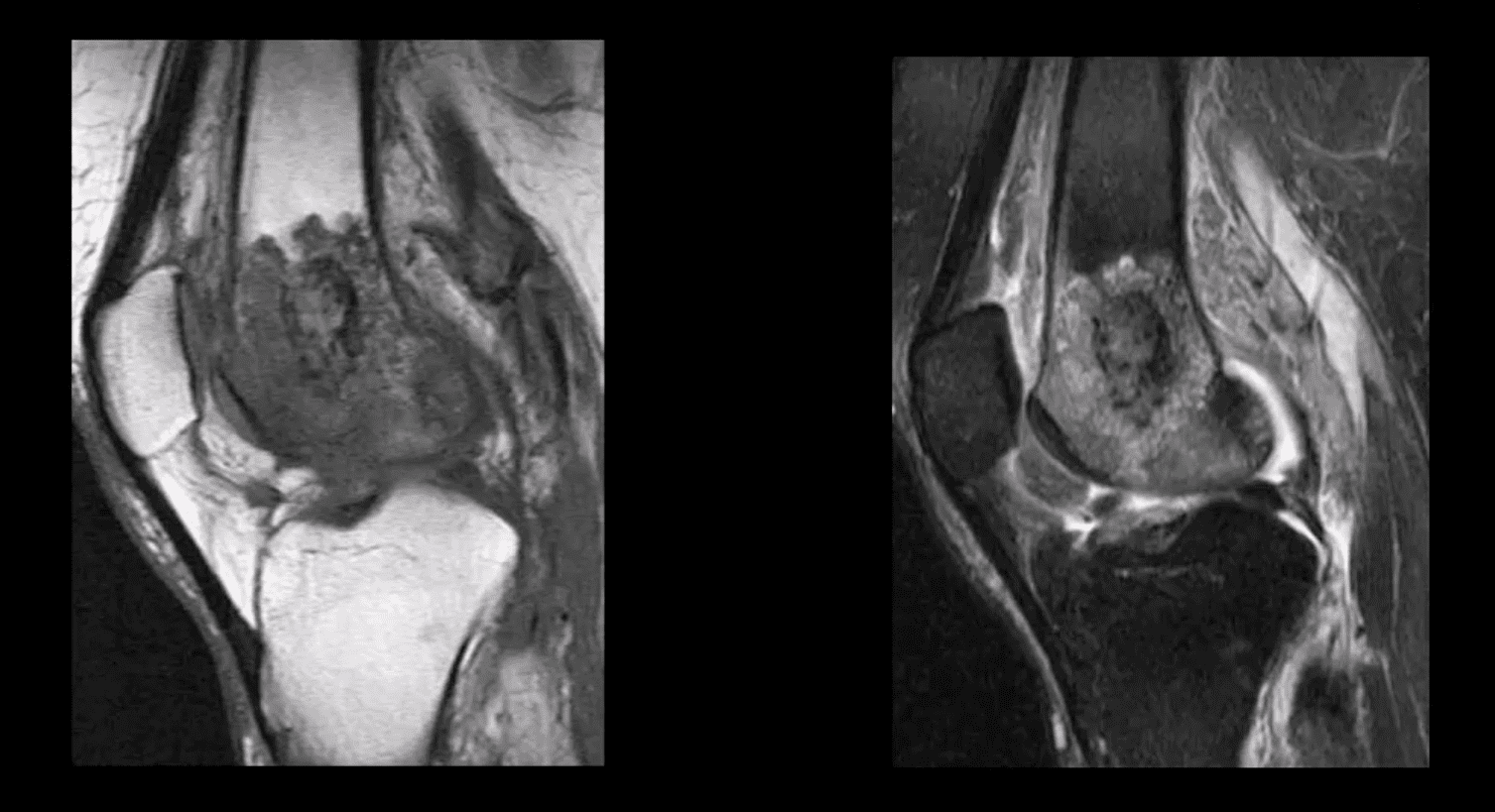
MRI Gout Features
Erosions with overhanging margins, a low signal on T1 and high on T2 and fat-suppressed images. Peripheral contrast enhancement of tophaceous deposits d/t granulation tissue
Dx: final Dx; synovial aspiration and polarized microscopy
Pathology: da disease of the articular cartilage. Continuing mechanical stimulation follows by an initial increase in water and cartilage thickness. Gradual loss of proteoglycans and ground substance. Fissuring/splitting. Chondrocytes are damaged and release enzymes into the joint. Cystic progression and further cartilage loss. Subchondral bone is denuded and exposed to mechanical stresses. It becomes hypervascular forming osteophytes. Subchondral cysts and bone thickening/sclerosis develop.
Imaging plays a crucial role in Dx/grading and management
Clinically: pain on walking/rest, crepitus, swelling d/t synovitis, locking/catching d/t osseocartilaginous fragments and gradual functional loss. Knee OA typically presents as mono and oligoarthritis. DDx: morning pain/stiffness is >30-min DDx from inflammatory arthritis
Treatment: in mild to moderate cases-conservative care. Severe OA-total knee arthroplasty
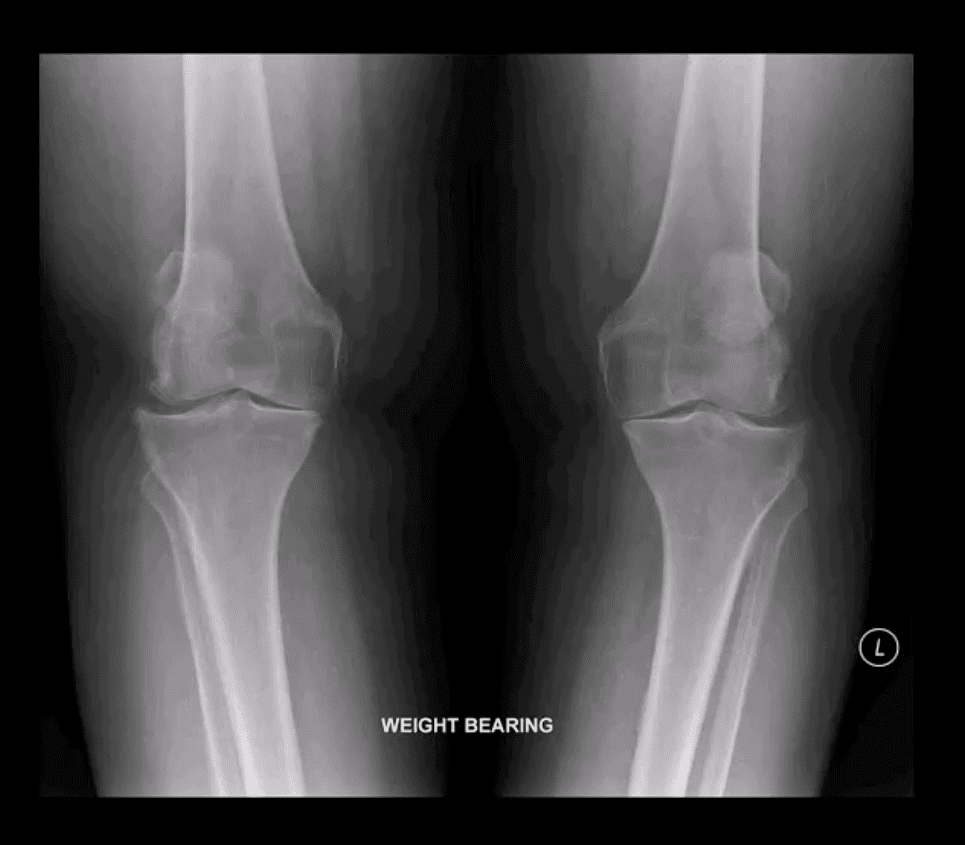
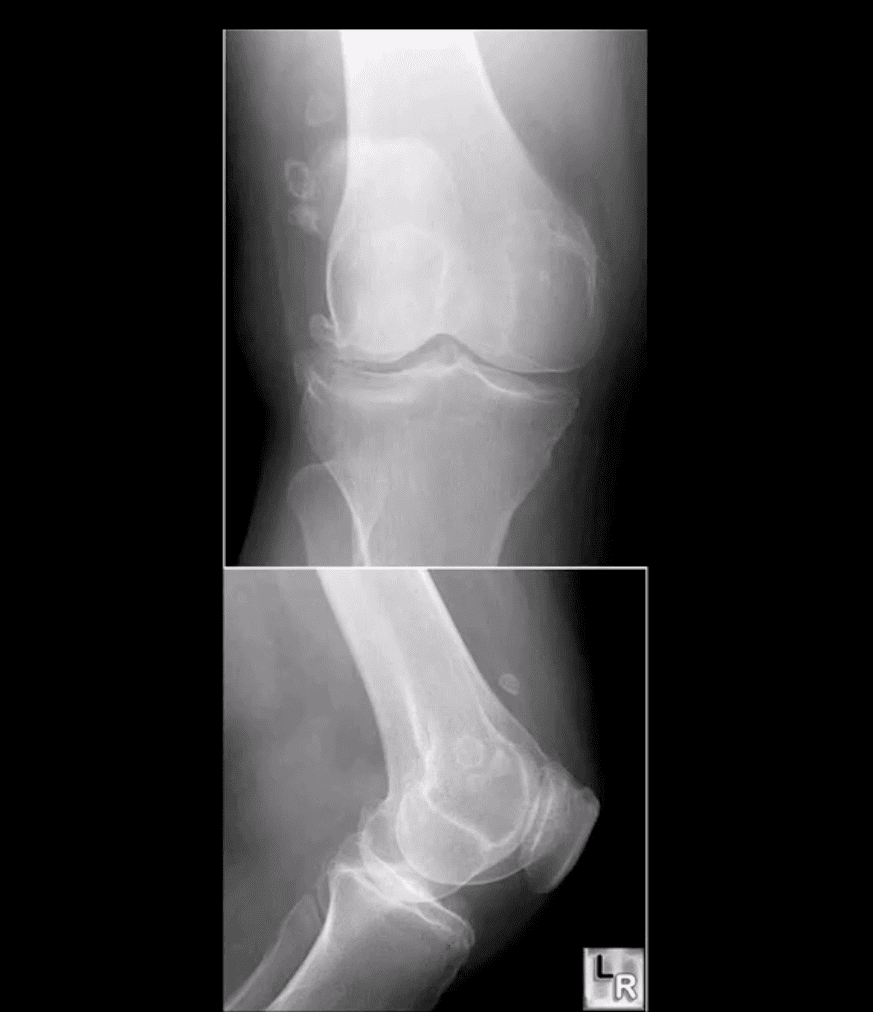
Grade 4: severe JSN, large osteophytes, marked subchondral sclerosis and definite bony deformity
Typical report language will state:
Minor, mild, moderate or severe aka advanced arthrosis
Technique
Radiography: AP weight-bearing knees: note severe JSN of the medial compartment more severely with lateral knee compartment. Osteophytes and marked genu varum deformity and bone deformation
Typically medial femorotibial compartment is affected early and more severely
The patellofemoral compartment is also affected and best visualized on the lateral and Sunrise views
Impressions: severe tri-compartmental knee arthrosis
Recommendations: referral to the orthopedic surgeon
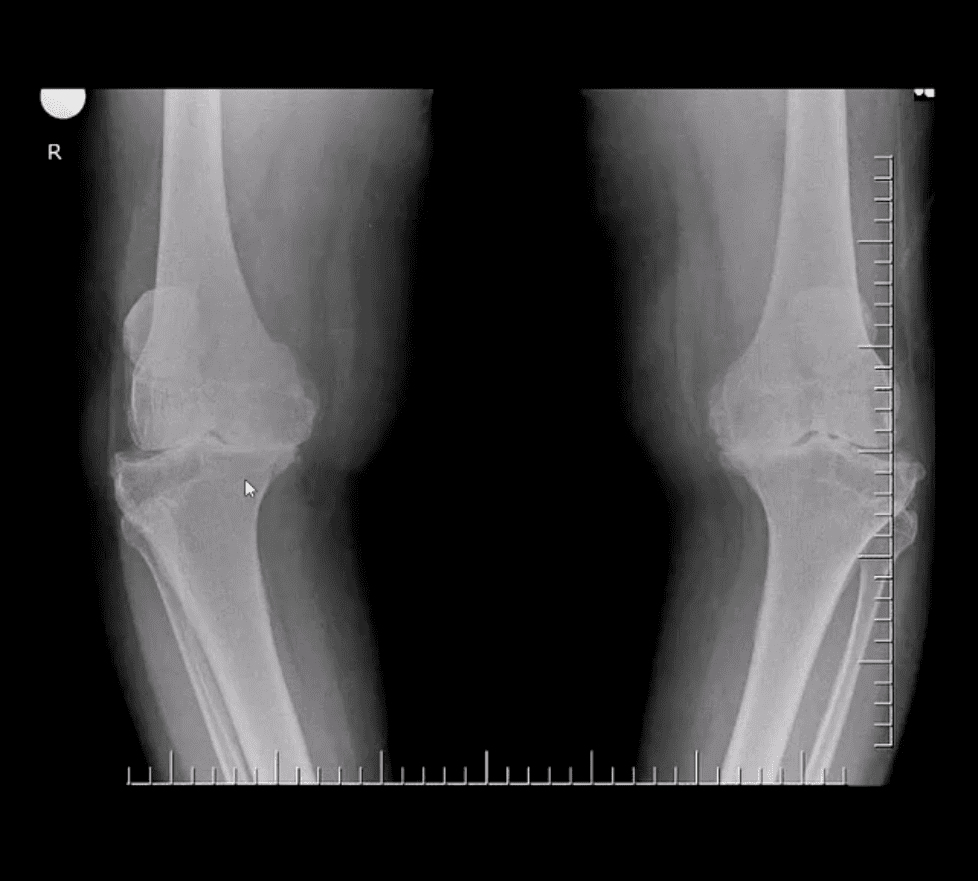
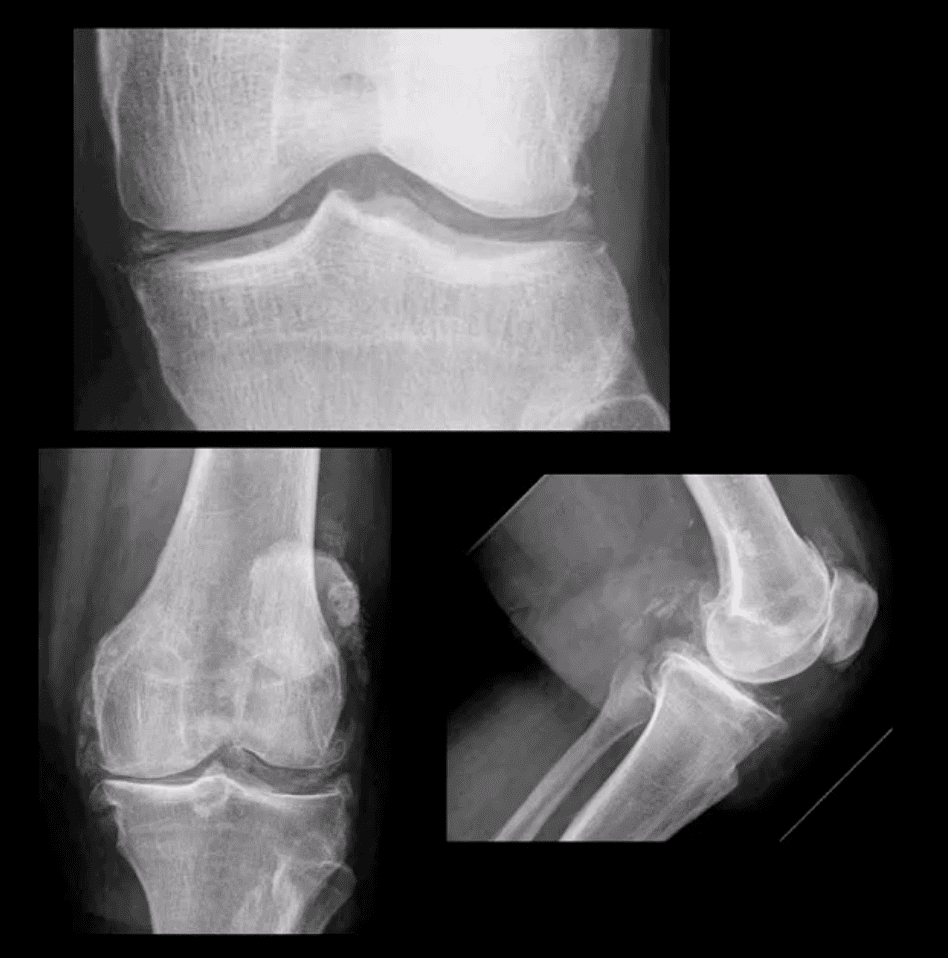
Moderate JSN
B/L AP weight-bearing view (above top image): Moderate JSN primarily of the medial femorotibial compartment. Osteophytosis, subchondral sclerosis and mild bone deformation (genu varum)
May present as asymptomatic chondrocalcinosis, CPPD arthropathy resembling DJD with pan predominance of large subchondral cysts. Often found as isolated PFJ DJD
Pseudogout with an acute attack of knee pain resembling gouty arthritis
Radiography is the 1st step and often reveals the Dx
Arthrocentesis with polarized microscopy may be helpful to DDx between CPPD and Gouty arthritis
Rheumatoid Arthritis
RA: an autoimmune systemic inflammatory disease that targets soft tissues of joints synovium, tendons/ligaments, bursae and extra-articular sites (e.g., eyes, lungs, cardiovascular system)
RA is the m/c inflammatory arthritis, 3% of women and 1% of men. Age: 30-50 F>M 3:1, but may develop at any age. True RA is uncommon in children and should not be confused with Juvenile Idiopathic Arthritis
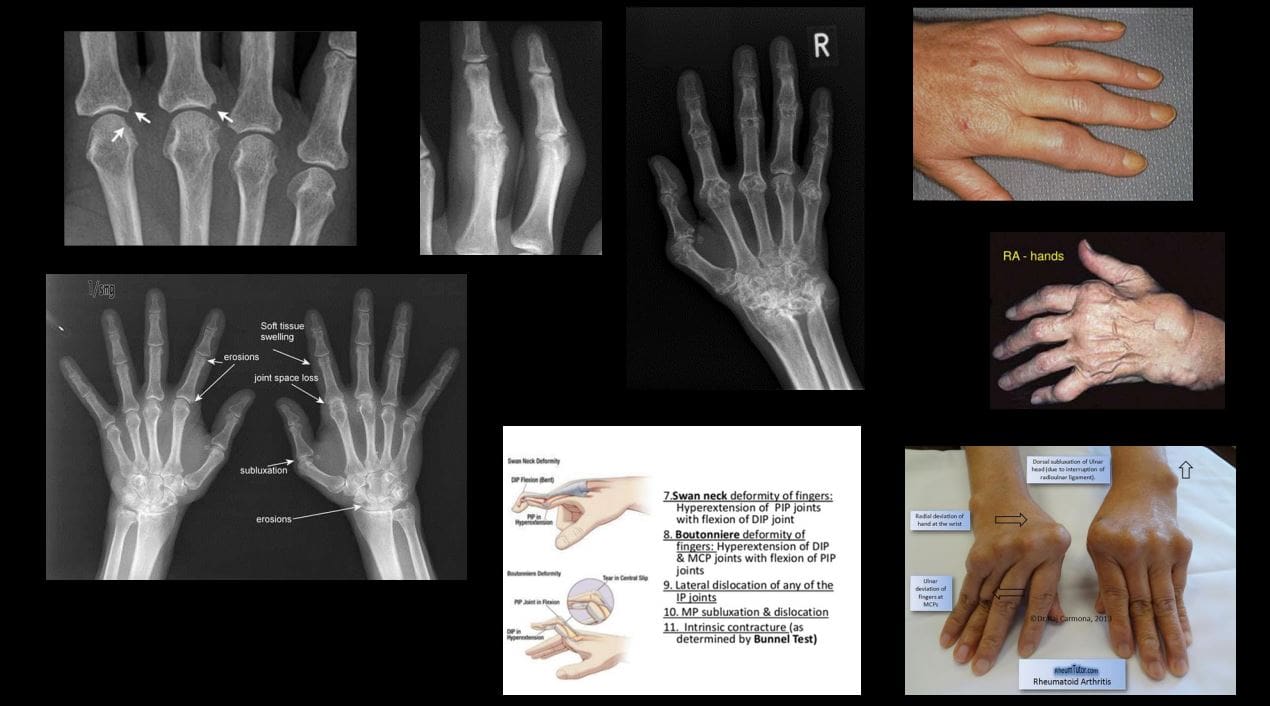
RA most often affects small joints of the hands and feet as symmetrical arthritis (2nd 3rd MCP, 3rd PIPs, wrists & MTPs, sparing DIPs of fingers and toes)
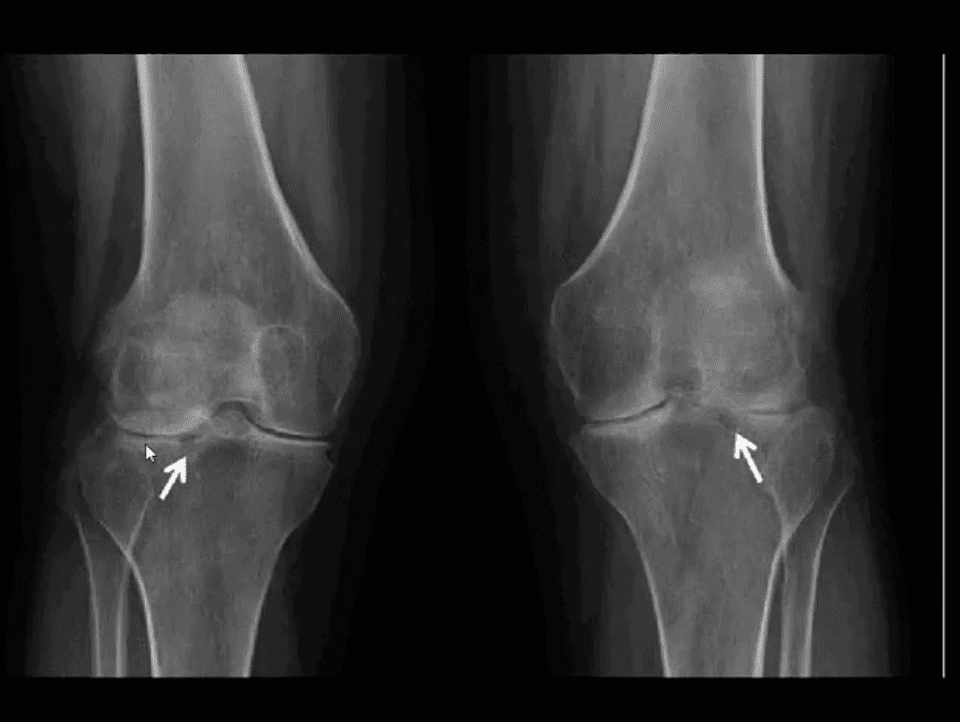
Radiographically: RA presents with joint effusion leading to hyperemia and marginal erosions and periarticular osteoporosis. In the knee, the lateral compartment is affected more frequently leading to valgus deformity. Uniform aka concentric/symmetrical JSN affects all compartments and remains a key Dx clue
An absence of subchondral sclerosis and osteophytes. Popliteal cyst�(Baker’s cyst) may represent synovial pannus and inflammatory synovitis extending into the popliteal region that may rapture and extend into posterior leg compartment
N.B. Following initial RA joint destruction, it is not unusual to note superimposed 2nd OA
Radiography is the 1st step but early joint involvement may be undetectable by x-rays and can be helped by US and/or MRI.
Final Dx is based on Hx, clinical exam, labs, and radiology
Clinical pearls: patients with RA may present with a single knee being affected
Most patients are likely to have bilateral symmetrical hands/feet RA.
Cervical spine, particularly C1-2 is affected in 75-90% of cases throughout the course of the disease
N.B. Sudden exacerbation of joint pain in RA should not underestimate septic arthritis because patients with pre-existing RA are at higher risk of infectious arthritis. Joint aspiration may help with Dx.
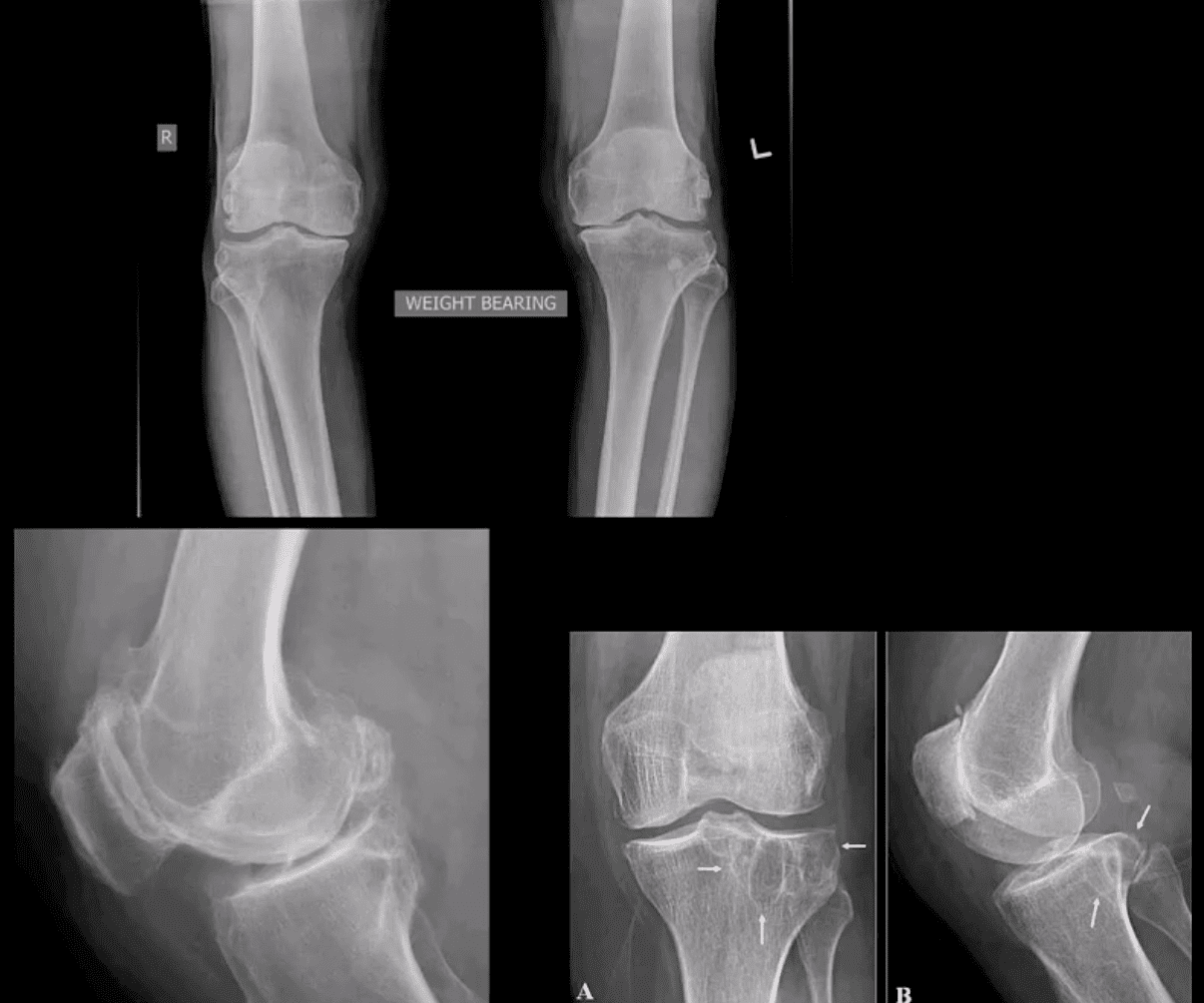
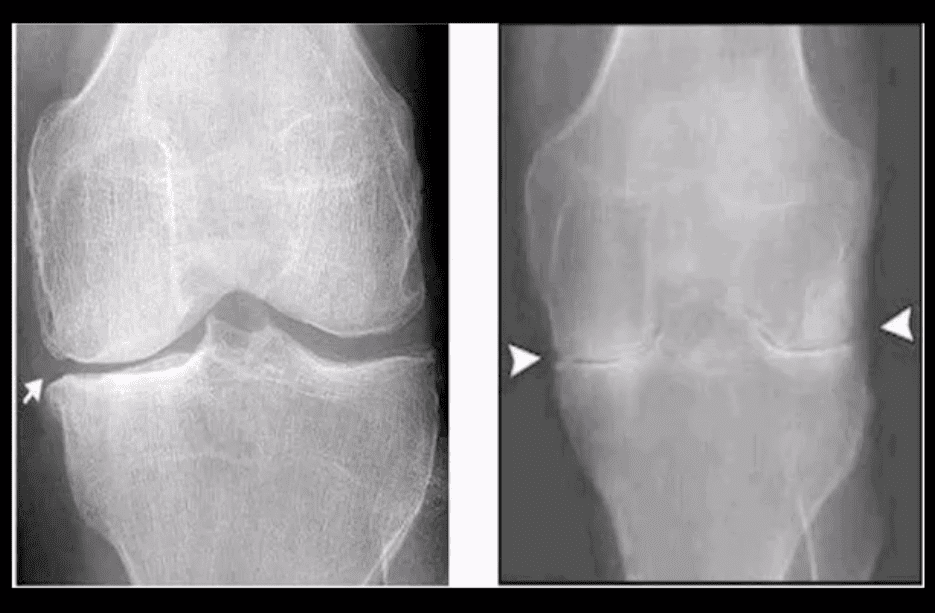
Radiographic DDx
RA (above left) vs. OA (above right)
RA: concentric (uniform) joint space loss, lack of osteophytes and juxta-articular osteopenia.
Clinical Pearls: patients with RA may present radiographically with subchondral sclerosis d/t superimposed DJD. The latter feature should not be interpreted as OA but instead considered as secondary OA
AP Knee Radiograph
Note marked uniform JSN, juxta-articular osteopenia and subchondral cystic changes
Clinical Pearls: subcortical cysts in RA will characteristically lack sclerotic rim noted in OA-associated subcortical cysts.
MRI Sensitivity
MRI is very sensitive and may aid during early Dx of RA.
T2 fat-sat or STIR and T1 + C gad contrast fat-suppressed sequences may be included
MRI Dx of RA: synovial inflammation/effusion, synovial hyperplasia, and pannus formation decreased cartilage thickness, subchondral cysts, and bone erosions
MRI is very sensitive to reveal juxt-articular bone marrow edema, a precursor to erosions
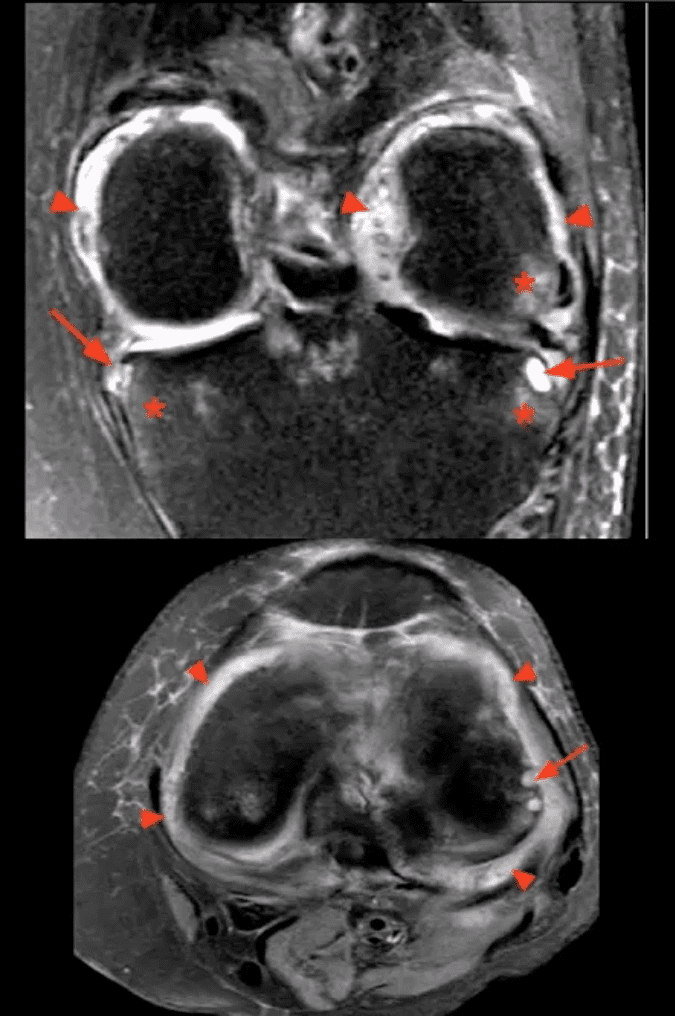
Intra-articular fibrinoid fragments known as “Rice bodies” are characteristic MR sign of RA
Note: T2 fat-sat sagittal MRI revealing large inflammatory joint effusion and pannus synovial proliferation (above arrowheads). No evidence of radiographic or MRI bone erosions present. Dx: RA
STIR MR Slices
Note: STIR MR slices in the axial (above bottom image) and coronal planes (above top image) demonstrate extensive synovitis/effusion (above arrowheads) and multiple erosions in the medial and lateral tibial plateau (above arrows)
Additionally, scattered patchy areas of bone marrow edema are noted (above asterisks) such marrow edema changes are indicative and predictive of future osseous erosions.
Additional features: note thinning and destruction of joint cartilage
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine