Arthritis can be a debilitating disease that interferes with everyday life. There are over 20% of adults aged 65 and older that have arthritis along with all the symptoms like pain, stiffness, swelling, and decreased range of motion. The most commonly affected joints include the shoulders, hands, spine, hips, and knees. Arthritis results from damage to joint cartilage from various factors such as age, wear and tear, injury, being overweight, and disease. While medication and surgery are the most common treatment options, an arthritis chiropractor can offer a conservative, natural, non-invasive option to manage symptoms.
Arthritis Chiropractor Helps By
While arthritis, either caused by wear and tear – Osteoarthritis or disease – Rheumatoid Arthritis cannot be cured. An arthritis chiropractor can help manage symptoms and prevent progression. Chiropractors are trained to use various techniques to help alleviate pain and tension, including arthritis. Chiropractic treatment aims to alleviate pain by adjusting, massaging, and realigning the musculoskeletal system to relieve stress, stretch the muscles, ligaments, tendons, and restore balance within the body. They open the body to allow proper/optimal nerve energy and blood circulation. This is beneficial for arthritic joints to reduce unnecessary strain, translating to reduced wear on the joints and keeping the body active.
Benefits
There are significant benefits that regular chiropractic treatment can offer. These include:
Restored range of motion
Joint pain relief
Inflammation alleviation
Improved nerve function for optimal tissue healing
Regular adjustments will keep the body optimally aligned and functioning smoothly.
Arthritis chiropractors can recognize the most subtle changes.
Lifestyle Adjustments
Healthy lifestyle adjustments help manage arthritis.
Guidance on healthy habits that include:
Anti-inflammatory foods
Weight loss
Proper sleep habits
Exercise training
Stress management
The sooner chiropractic care is sought out, the better to prevent symptoms from worsening. Chiropractic can generate great results with less need for medication/s or surgery.
Body Composition
Identifying The Risk of Sarcopenia and Decreased Mobility
As the body ages, it begins to lose muscle mass, and as more sedentary behavior is adopted, the rate of loss increases along with age-related injury. Identifying these age-related changes in muscle and how they relate to frailty risk can be challenging to identify and track. By accurately measuring fat-free mass in each region of the body, Skeletal Muscle Index – SMI quickly specifies muscle mass and frailty risk. Sarcopenia and frailty specifically affect the elderly population, affecting mortality, cognitive function, and quality of life. Loss of muscle in the arms and legs is associated with:
Reductions in mobility
Increased risk of falls
Frailty
Extended hospital stays
Falls and fractures frequently result in a cycle of muscle deterioration. Analysis tools can help track body composition changes to minimize muscle wasting and the risk of impaired mobility. Assessing skeletal muscle mass in outpatient and hospital settings can decrease debilitating outcomes before they happen. The InBody analysis is quick and easy, providing a calculation for skeletal muscle index and the sum of the lean mass in the arms and legs. The ease of performing the InBody test provides physicians more time to work with and educate individuals on adopting lifestyle changes to help prevent sarcopenia.
References
Aletaha, Daniel. “Precision medicine and management of rheumatoid arthritis.” Journal of autoimmunity vol. 110 (2020): 102405. doi:10.1016/j.jaut.2020.102405
Beasley, Jeanine. “Osteoarthritis and rheumatoid arthritis: conservative therapeutic management.” Journal of hand therapy: official journal of the American Society of Hand Therapists vol. 25,2 (2012): 163-71; quiz 172. doi:10.1016/j.jht.2011.11.001
Demoruelle, M Kristen, and Kevin D Deane. “Treatment strategies in early rheumatoid arthritis and prevention of rheumatoid arthritis.” Current rheumatology reports vol. 14,5 (2012): 472-80. doi:10.1007/s11926-012-0275-1
Kavuncu, Vural, and Deniz Evcik. “Physiotherapy in rheumatoid arthritis.” MedGenMed: Medscape general medicine vol. 6,2 3. 17 May. 2004
Moon, Jeong Jae et al. “New Skeletal Muscle Mass Index in Diagnosis of Sarcopenia.” Journal of bone metabolism vol. 25,1 (2018): 15-21. doi:10.11005/jbm.2018.25.1.15
Sciatica Causes: The sciatic nerve forms by the union of Lumbar4 to Sacral31 nerve roots and exits the pelvis through the greater sciatic foramen, below the piriformis muscle located deep in the buttocks. The nerve runs down the back of the thigh, into the leg, and ends in the foot. The sciatic nerve becomes inflamed, irritated, and/or mechanically compressed. Any type of pain and/or neurological symptom/s from the sciatic nerve is referred to as sciatica. Sciatica is a type of lumbar radiculopathy, which means that the pain originates from the low back and/or sacral nerve roots.
Sciatica Causes
Physical forces on the nerve can cause mechanical compression due to the following conditions:
Herniated Discs
A disc in the lower back can bulge or herniate, causing irritation and/or compression of a sciatic nerve root.
Foraminal Stenosis
Stenosis, the intervertebral opening through which the nerve roots travel, begins to narrow/close in, can compress or irritate the sciatic nerve.
Degeneration
Degenerative changes in the spine like the thickening of facet joint capsules and/or ligaments can compress the sciatic nerve.
Segmental Instability
Instability of a spinal vertebral segment that happens if one vertebra slips over the one beneath it – spondylolisthesis
Complete dislocation of one or more vertebrae can compress the nerve root/s of the nerve.
Other Sciatica Causes
Tumors, cysts, infections, or abscesses in the lower spine or pelvic region can also cause sciatic nerve compression.
Chemical Inflammation
Chemical irritants can include hyaluronic acid and/or fibronectin/protein fragments that leak out of degenerated or herniated discs. These irritants can cause inflammation and/or irritation of the sciatic nerve.
Degenerated discs can cause nerve tissues to grow into the disc, penetrating the outer and inner layers of the disc, causing sciatica. Immune system responses can contribute to pain when exposed to disc fluid.
Substances such as glycosphingolipids/fats and neurofilaments /protein polymers secreted by the immune system are increased in individuals with sciatica. These substances are released from the reaction between nerve roots and exposed disc material, causing inflammation.
Job Occupation
Individuals with specific jobs have an increased risk of developing sciatica. Examples include:
Truck drivers
Desk workers
Teachers
Warehouse workers
Machine workers
Plumbers
Electricians
Carpenters
Fitness trainers
Sitting and standing for long periods, using improper posture, constantly bending, twisting, reaching, and regularly lifting are risk factors for sciatica.
Piriformis Syndrome
Piriformis syndrome is a condition where the piriformis muscle swells and spasms from overuse or inflammation irritating the sciatic nerve that is right underneath. The nerve can get trapped in the muscle causing sciatica-like symptoms that include:
Pain follows the same pattern in the leg as a compressed sciatic nerve root.
Tingling
Numbness
Discomfort from piriformis syndrome feels similar to sciatica, but it is not caused by compressed sciatic nerve root. Piriformis pain comes from compression of the sciatic nerve near the piriformis muscle.
Genetic Sciatica Causes
Sciatica caused by degenerated and/or herniated discs can be genetic. Research has shown that certain genetic factors are more prevalent in individuals with back and spinal problems. These congenital disabilities can cause the discs to become weak and susceptible to external stress. With time the proteins in the disc break down, compromising the integrity and function.
Arthritis and Joint Issues
Arthritis or other inflammatory conditions around the hip joint can cause pain down the leg, similar to sciatica. This is referred pain that spreads out from the source and is not radicular nerve pain that originates in the nerve roots.
Conditions like sacroiliac joint dysfunction or sacroiliitiscan cause sciatica-like pain that runs down the back of the thigh but usually ends before or at the knee.
The pain can be acute and debilitating, like sciatica but is caused by an abnormal motion or malalignment of the sacroiliac joint.
Body Composition
Normal Cholesterol Ranges
High cholesterol can lead to severe consequences when left untreated, but it can be difficult to spot with no noticeable warning signs. This is why it’s essential to monitor cholesterol levels with blood tests, especially if there is an increased risk. Example of normal cholesterol levels for adults 20 years of age or older:
Total cholesterol 125-200 mg/dL
LDL <100 mg/dL
HDL >40 mg/dL men, >50 mg/dL women
Lifestyle
Lack of physical activity contributes to high cholesterol levels.
Diets that mainly consist of processed foods and saturated fats increase the risk of high LDL levels.
Smoking can lower HDL levels.
Aging
Individual risk for developing high cholesterol tends to increase as the body advances in age. This is why it is recommended to have regular physicals and blood tests.
Genetics
Some individuals are more genetically predisposed to developing high cholesterol and heart disease.
Knowing family medical history can help predict whether it may become a problem.
References
Davis D, Maini K, Vasudevan A. Sciatica. [Updated 2021 Sep 2]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507908/
Giuffre BA, Jeanmonod R. Anatomy, Sciatic Nerve. [Updated 2021 Jul 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482431/
Hicks BL, Lam JC, Varacallo M. Piriformis Syndrome. [Updated 2021 Jul 18]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448172/
Raj MA, Ampat G, Varacallo M. Sacroiliac Joint Pain. [Updated 2021 Aug 30]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470299/
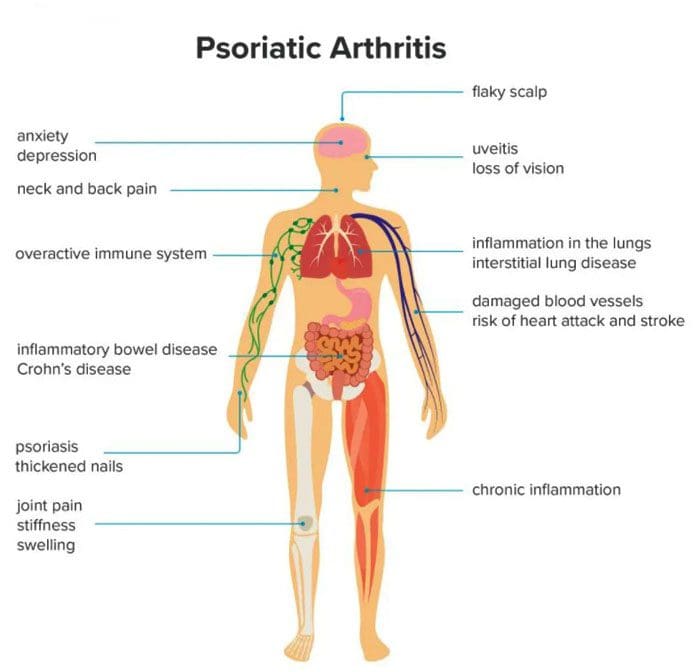
Psoriatic arthritis can develop in individuals who have psoriasis, affecting various joints, especially the knees. Psoriasis is a skin condition that causes skin cells to build up and form patches of itchy, dry skin known as plaques. Psoriatic arthritis is a long-term inflammatory disease that can cause inflammation, stiffness, and pain. Symptoms can progressively worsen over time without treatment. Early diagnosis is vital to minimize damage to the joints and slow the condition’s progress with treatment.
Psoriatic Arthritis
Psoriatic arthritis symptoms like stiffness and swelling can present differently from person to person. For example, some individuals with psoriatic knee arthritis will experience stiffness or pain in one knee, while others experience symptoms in both knees. Psoriatic arthritis in the knee can also cause swelling in the surrounding:
Ligaments
Tendons
Synovial membranes
Symptoms can also present in the:
Elbows
Feet
Hands
Symptoms
Symptoms usually begin between the ages of 30 and 50. Common symptoms include:
Stiffness after resting or sleeping.
Swelling.
Inflammation in the knee and surrounding area.
Warm or hot skin on the knee from the inflammation.
Pain in and around the joints, tendons, or ligaments.
Joint sticking, difficulty moving, or reduced range of motion.
Other symptoms include:
Back pain
Fatigue
Pain and redness in the eyes
Swollen fingers or toes
Difficulty walking from pain in the feet or Achilles tendon.
The severity of psoriasis does not determine psoriatic arthritis symptoms. Symptoms can go through a pattern of relapses and remissions. Individuals can have a sudden attack where symptoms get worse over a short time. After the flare-up, symptoms can improve as the condition goes into remission. Symptoms may not present for a long time until another flare-up. For example, an individual may have severe psoriasis but only mild psoriatic arthritis.
Causes
Psoriatic arthritis develops when the body’s immune system mistakenly attacks healthy cells and tissues. The faulty immune response causes the body to quickly generate new skin cells that stack on top of each other forming plaques. When the condition affects the joints, it leads to inflammation. While there is no apparent cause for psoriatic arthritis, researchers have found connections to genetics and the environment, as well as, individuals with close relatives that have psoriatic arthritis could be more likely to develop the condition. Other factors that could influence the development include:
Severe psoriasis
Traumatic injury/s
Obesity
Nail disease
Smoking
The condition can happen at any age, but according to the National Psoriasis Foundation, most individuals first notice symptoms about ten years after their psoriasis begins. However, only 30% of individuals with psoriasis develop psoriatic arthritis.
Diagnosis
Doctors use imaging tools to diagnose psoriatic arthritis in the knee. They will use:
MRI
X-rays
Ultrasound
To help them check for irregularities or signs of inflammation in the joint and surrounding tissues.
Additional tests are used to rule out other common forms of arthritis like rheumatoid and osteoarthritis.
Blood tests check for inflammation and specific antibodies.
In some cases, a small amount of fluid from the joint is taken to help eliminate the possibility of other underlying conditions like an infection.
Treatment
There is currently no cure for psoriatic arthritis, but treatments are being developed and show promise for long-term management. Current treatments focus on managing symptoms and improving the quality of life for the individual.
Biologics
Biologic medications like tumor necrosis factor or TNF inhibitors are recommended as the first-line therapy for most individuals with a new diagnosis of psoriatic arthritis. These meds help block TNF, which plays a crucial role in inflammation. They have shown to be effective at reducing the severity of symptoms and the frequency of flare-ups. Biologics can cause unwanted side effects, especially in individuals that experience frequent infections and need routine monitoring.
Small Molecule Medications
Individuals that cannot use biologic medications may be recommended a new class of medication called oral small molecules or OSMs. Examples include apremilast – Otezla and tofacitinib – Xeljanz.
Disease-modifying Antirheumatic Drugs
Disease-modifying antirheumatic drugs – DMARDs are a long-term option. They are used to slow the progression of psoriatic arthritis, and examples include methotrexate and cyclosporine. DMARDs work best when an individual begins taking them as early as they can take time to work. However, individuals are encouraged to continue taking them, even if symptoms do not improve right away.
Easing Inflammation
A doctor may prescribe nonsteroidal anti-inflammatory drugs – NSAIDs and corticosteroid injections when knee symptoms flare-up. These are short-term treatments that provide immediate relief, as long-term use can lead to side effects. Individuals can find relief with combined self-care that includes:
Taking over-the-counter NSAIDs like ibuprofen/Advil or naproxen/Aleve.
Applying ice and heat packs.
Gentle exercise to promote a full range of motion.
Gentle stretching or yoga can help relax tight muscles.
However, chiropractic is not the primary treatment for arthritis but is intended to be used in combination to relieve pain, loosen and stretch the muscles and balance the body.
InBody
Strength, Balance, and Improved Body Composition
Functional fitness is the ability to move comfortably every day. The benefits of physical activity also contribute to improved body composition. Working to reach a certain level of functional fitness can help the aging process that has been shown to reduce metabolic rate. Inactivity is why individuals lose Lean Body Mass as they age, leading to increased body fat. Lean Body Mass contributes to the body’s overall Basal Metabolic Rate or BMR, also known as metabolism. This is the number of calories the body needs to support essential functions. Everyone is encouraged to engage in strength training or resistance exercises, but specifically older adults. This can help regain muscle loss which can lead to an increase in lean body mass. The increase in Lean Body Mass increases BMR, which helps prevent fat gain.
References
Chang, K. L., et al. (2015). Chronic pain management: Nonpharmacological therapies for chronic pain [Abstract]. https://www.ncbi.nlm.nih.gov/pubmed/25970869
Chiropractic care for arthritis. (n.d.). arthritis.org/health-wellness/treatment/complementary-therapies/physical-therapies/chiropractic-care-for-arthritis
Managing rheumatoid arthritis is an ongoing balancing act. Flare-ups can still present despite following the rheumatologist’s lifestyle instructions, proper medication use, and a well-maintained RA plan. Monitoring daily activities can help minimize the chances of experiencing episodes.
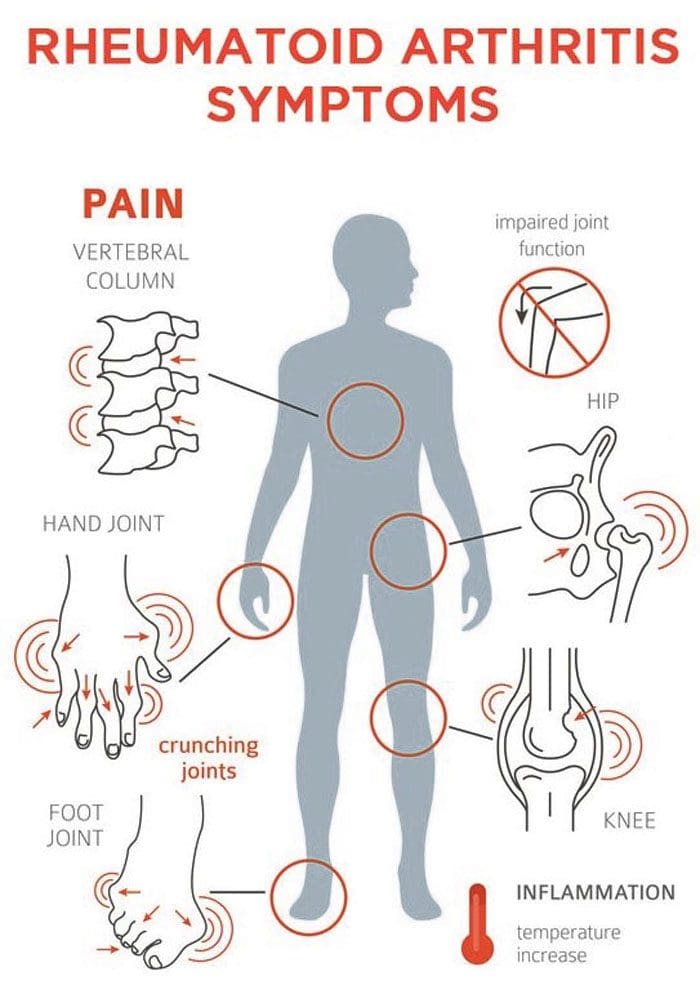
Rheumatoid Arthritis Flare-Ups
A rheumatoid arthritis flare-up is a short-term escalation of arthritis symptoms. A flare-up can go away within a day or can persist for several weeks or months. A flare-up usually involves joint stiffness and pain but can also present as any symptoms worsening. If the flare-up is severe, it can affect the ability to perform regular everyday activities.
Symptoms
Symptoms can vary, and not every person experiences the same. Most individuals describe flare-ups with a sudden increase in:
Pain
Stiffness
Swelling
Limited joint mobility
Fatigue
Symptoms that feel like the flu.
Frequency and severity can also vary.
Back Pain Symptoms
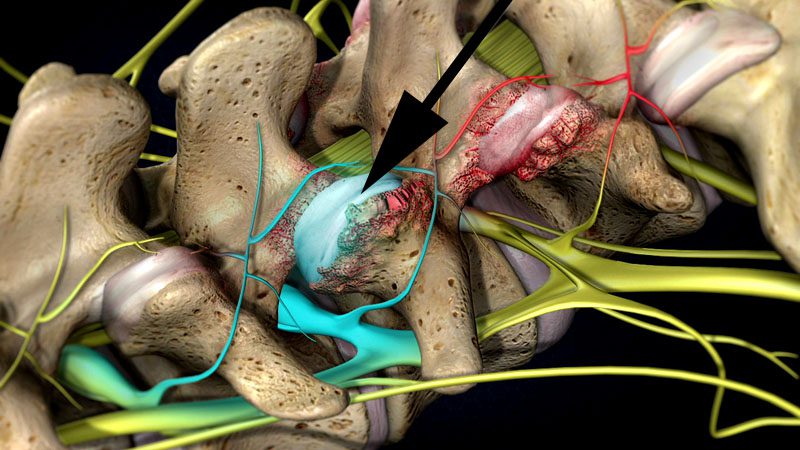
Rheumatoid arthritis can affect many joints. It is the inflammation of a joint’s synovial membrane. These include the facet joints in the spine. The most commonplace in the spine affected by rheumatoid arthritis is the upper neck, around the base of the skull. The joints at the top of the neck get inflamed and can become unstable or form abnormal tissue that sticks out and compress the spinal cord.
Triggers
Several potential flare-up triggers include:
Stress
Not getting enough sleep
Medication changes
Injury
Excessive physical activity and/or exercise
Repetitive overuse injury
Smoking
Spinal infections
Airborne toxins can also be a trigger to a flare-up. Substances include chemicals like household cleaners. Switching to organic and environmentally safe cleaners can help. Airborne toxins are a concern in densely populated cities and areas that experience air pollution and smog. To minimize risks, staying indoors during times of poor air quality is recommended.
However, flare-ups can happen without an identifiable trigger. Certain foods can increase inflammation and could contribute to a flare-up, including:
Avoiding these foods and following a diet that has been developed to prevent symptoms will help significantly. The objective is to learn to identify an RA flare-up to moderate activities accordingly.
Prevention
Managing any chronic medical condition is challenging, especially when trying to predict when a flare-up will happen. There is not a foolproof strategy for prevention, but advice that can help minimize the risks of an RA flare-up.
Understand that the disease can change over time. This means changes in medications and the need for multi-approach treatment. Learning healthy self-care techniques will go a long way in managing symptoms.
Body Composition
Antioxidants protection
Metabolic processes, like energy production, and environmental pollution, can result in free radical production. These are highly reactive molecules that can damage the body’s cells and lead to oxidative stress. This can develop into a disease, including heart disease. The body has natural protective mechanisms to neutralize free radical molecules, including glutathione, which is the body’s top antioxidant. If glutathione becomes depleted because of increased free radicals, the body switches to dietary antioxidants from food as a secondary defense.
Pham-Huy, Lien Ai et al. “Free radicals, antioxidants in disease and health.” International Journal of biomedical science: IJBS vol. 4,2 (2008): 89-96.
Rheumatoid arthritis is said to affect around 1.5 million individuals. Recognized as an autoimmune condition that presents with chronic pain in the body’s joints. It commonly affects regularly used joints like the shoulders, hands, and feet. The condition can begin to present in individuals in their 30s. Concerns that come with a rheumatoid arthritis diagnosis are the condition’s effect on the spinal facet joints. These joints are susceptible to attack from a dysfunctional immune system, leaving them prone to weakness, inflammation, and nerve compression. Chiropractors understand the manifestation of rheumatoid arthritis. They can pinpoint at-risk facet joints and provide corrective relief before more dangerous symptoms begin to present.
Facet joint risks
There are two facet joints that connect each vertebra to the one above and below. Their objective is to stabilize the spine, whether in a neutral position or engaged in flexion/extension movement. When targeted by the body’s immune system, the joints begin to weaken. The body attacks the synovial fluid that lubricates the joints. This creates friction that generates inflammation. Over time the joints break down leading to everything from loss of mobility to bone spurs. When left untreated the facet joints begin to deteriorate, causing nerve compression that can lead to permanent nerve damage. When the joints are not working properly the spine has to work around them.
Subluxations
Disc herniation
Ruptured discs
Sciatica all are possible with facet joint dysfunction.
Treatment
Currently, rheumatoid arthritis cannot be cured but symptoms can go into remission when treatment begins early.Chiropractic is an effective treatment at disrupting the symptoms of joint deterioration that stops the progression.
It has the ability to increase and maintain an individual’s range of motion, from a condition that causes loss of mobility.
It helps to bring rapid pain relief and helps with postural improvements.
It maintains positive spinal health and homeostasis.
Prevents problems with compression and subluxations.
Stretching and strengthening exercises are incorporated to preserve an individual’s spinal integrity.
Diet and nutrition are also adjusted to mitigate the effects, helping with inflammation prevention.
The spinal focus
As rheumatoid arthritis affects the body’s joints, it is vital to protect the facet joints. These joints can experience degenerative damage that can cause long-term problems. Injury Medical Chiropractic and Functional Medicine Clinic provide individuals with the tools necessary to combat rheumatoid arthritis that medications by themselves might not be able to.
Body Composition
Muscle Mass Fitness for Long-Term Health
Muscle building is not just for bodybuilders and athletes. Everyone benefits from building muscle for long-term health. Monitoring the changes in Lean Body Mass can be accomplished by having body composition measured. Body composition analysis can divide an individual’s weight into various components. These include:
Fat Mass
Lean Body Mass
Basal Metabolic Rate will give a clearer picture of overall fitness and health.
Building Lean Body Mass is an investment for maintaining health long-term. The more Lean Body Mass that is built the more is in storage/reserve when the body really needs it. Before adding protein shakes and resistance workouts to the daily regimen, a plan needs to be developed. The first step to building a healthy level of lean body mass is to measure how much there is with a body composition analysis.
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP, CIFM, CTG* email: [email protected] phone: 915-850-0900 Licensed in Texas & New Mexico
References
Pope JE, Cheng J. Facet (Zygapophyseal) Intraarticular Joint Injections: Cervical, Lumbar, and Thoracic. Injections for Back Pain. 129-135. ClinicalKey.com. Accessed July 16, 2019.
Brummett CM, Cohen SP. Pathogenesis, Diagnosis, and Treatment of Zygapophyseal (Facet) Joint Pain. 816-844. ClinicalKey.com. Accessed July 16, 2019.
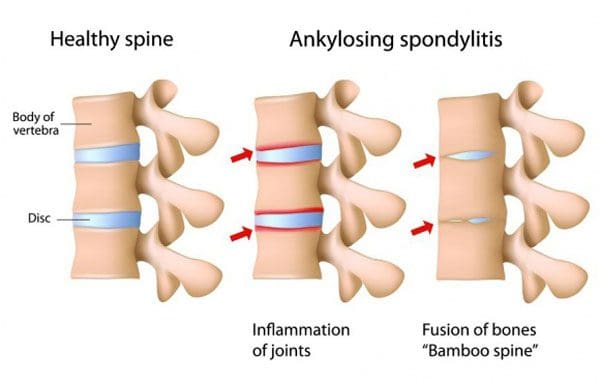
Individuals with ankylosing spondylitis have a new treatment option that was previously used for rheumatoid arthritis. It is a medication that belongs to a class known as JAK inhibitors. Ankylosing spondylitis combines joint pain with reduced mobility. Ankylosing spondylitis is different because in severe cases, the bones in the spine can fuse together, literally reducing mobility.
The disease typically begins with pain and stiffness in the back. This is usually after some time of inactivity. Symptoms start before the age of 45 and develop gradually. There is no cure for ankylosing spondylitis but there are treatments that can improve symptoms and put the condition into remission. Ankylosing spondylitis treatment is the most successful when addressed early before irreversible damage to the joints begins.
Janus Kinase Inhibitors
Janus kinase inhibitors have traditionally been used to treat:
Rheumatoid arthritis
Psoriatic arthritis
Ulcerative colitis
The medication works by decreasing the immune system�s activity. Janus kinase inhibitor drugs affect several cellular compounds that are important in the development and progression of ankylosing spondylitis. Currently, there are only three Janus kinase inhibitor medications available in the United States and FDA-approved to treat rheumatoid arthritis:
Xeljanz
Rinvoq
Olumiant
Each of the approved inhibitors targets specific enzymes
Current Ankylosing Spondylitis Treatments
Janus kinase inhibitors are not given to individuals right away. However, it could be an option if first and second-line treatments are not working. Treatments usually consist of:
First-Line Treatments
NSAIDs
Nonsteroidal anti-inflammatory medications are the most commonly used to treat ankylosing inflammation, pain, and stiffness.
Chiropractic
Chiropractic physical therapy is a major part of ankylosing spondylitis treatment keeping the spine flexible and as healthy as possible. A chiropractic/physical therapy team design and develop specific exercises to fit individual needs, which include:
Stretching and Range-of-motion exercises help maintain flexibility in the joints
Sleeping and walking posture adjustment exercises
Abdominal and spinal exercises to maintain a healthy posture
If nonsteroidal anti-inflammatory medications do not relieve symptoms, then biological medications could be prescribed. This class of medications includes:
Tumor necrosis factor blockers work by targeting cell protein that is part of the immune system, known as tumor necrosis alpha. This protein causes inflammation in the body, and the blockers suppress it.
Interleukin 17 Inhibitors
Interleukin 17 in the body’s immune system defends against infection. It uses an inflammatory response to fight infections. The IL-17 inhibitors suppress the inflammatory response and help reduce symptoms.
Other Treatment Options
Lifestyle Adjustments
Following a medical treatment plan is often combined with diet and lifestyle adjustments that are recommended to help with the condition, these include:
Most individuals with ankylosing spondylitis do not require surgery. However, a doctor could recommend surgery if there is joint damage, the hip-joint needs to be replaced, or if the pain is severe.
Inhibitor Potential
Studies are ongoing in the treatment of ankylosing spondylitis. The drug is currently in Phase 3 trials for the treatment of adults. The trial results have shown patients with active ankylosing spondylitis showed improvement in:
Fatigue
Inflammation
Back pain
The study enrolled adults with active ankylosing spondylitis who took at least two NSAIDs that were ineffective at treating symptoms. Most of the participants were men, average age of 41, and no prior usage of biologic disease-modifying antirheumatic drugs.
Janus kinase could become a standard treatment
There is still not enough research to make a prediction, but the data is promising. The inhibitors seem to be a safe option when used in a properly screened, well-matched setting that includes regular monitoring. The inhibitors appear to be effective and have the advantages of being taken orally and working fast.
Body Composition
Osteoarthritis and weight loss
Being obese has shown to be a high-risk factor for the development of osteoarthritis. This is not only from the effects of extra weight on the body’s joints but also as a result of the inflammatory effects of adipose tissue. The lower back, hips, and knees, bear the majority of the body’s weight.
An excess amount of adipose tissue on the body’s midsection and legs has been shown to negatively impact the weight-bearing joints. Promoting Lean Body Mass and encouraging weight loss lowers the risk of osteoarthritis and improves an individual’s quality of life. Exercise is regarded safe for individuals with osteoarthritis and should be incorporated to improve body composition, reduce Body Fat Mass, improve Lean Body Mass and maintain a healthy weight.
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Hammitzsch A, Lorenz G, Moog P. Impact of Janus Kinase Inhibition on the Treatment of Axial Spondyloarthropathies. Frontiers in Immunology 11:2488, Oct 2020; doi 10.3389/fimmu.2020.591176.�https://www.frontiersin.org/article/10.3389/fimmu.2020.591176, accessed Jan 21, 2021.
van der Heijde D, Baraliakos X, Gensler LS, et al. Efficacy and safety of filgotinib, a selective Janus kinase 1 inhibitor, in patients with active ankylosing spondylitis (TORTUGA): results from a randomized, placebo-controlled, phase 2 trial.�Lancet.�2018 Dec 1;392(10162):2378-2387. doi: 10.1016/S0140-6736(18)32463-2. Epub 2018 Oct 22. PMID: 30360970.�https://pubmed.ncbi.nlm.nih.gov/30360970/�accessed Jan 19, 2021.
Inflammatory spinal arthritis can cause significant joint pain and severely damage sleep quality. Any of the following conditions can cause individuals to experience sleep problems:
Spondylosis (osteoarthritis)
Rheumatoid arthritis
Ankylosing spondylosis
Juvenile idiopathic arthritis
Dr. Jimenez from Injury Medical Chiropractic and Functional Medicine Clinic gives insight into how inflammatory spinal arthritis can disrupt healthy sleep, along with some tips to help individuals with joint pain restore healthy sleep.
Inflammatory Spinal Arthritis and Sleep
First, it is not just the joint pain of arthritis that is causing sleep problems. Research is discovering that more factors could be at play. A study in the journal SLEEP examined how individuals with chronic pain, including osteoarthritis slept. What was revealed was a strong connection between chronic pain and insomnia.
Insomnia can lead to added joint pain because poor sleep can trigger inflammatory pathways that worsen arthritis pain. Plus a poor night of sleep can heighten an individual’s perception of pain the next day. Arthritis pain does not just impact the sleep of adults, but young individuals with juvenile idiopathic arthritis can also struggle with getting healthy sleep. Sleep, pain levels, and mood are strongly related.
Sleep Tips
Achieving quality sleep and a well-rested body can be done. Things to consider to help secure a healthy sleep.
Medication interference/side effects
Corticosteroids could be part of the sleep problem, as corticosteroid treatment has been linked to insomnia. If struggling to fall asleep, talk with a doctor about altering any prescribed medication regimen before sleep like taking aspirin or a nonsteroidal anti-inflammatory NSAID medication in its place.
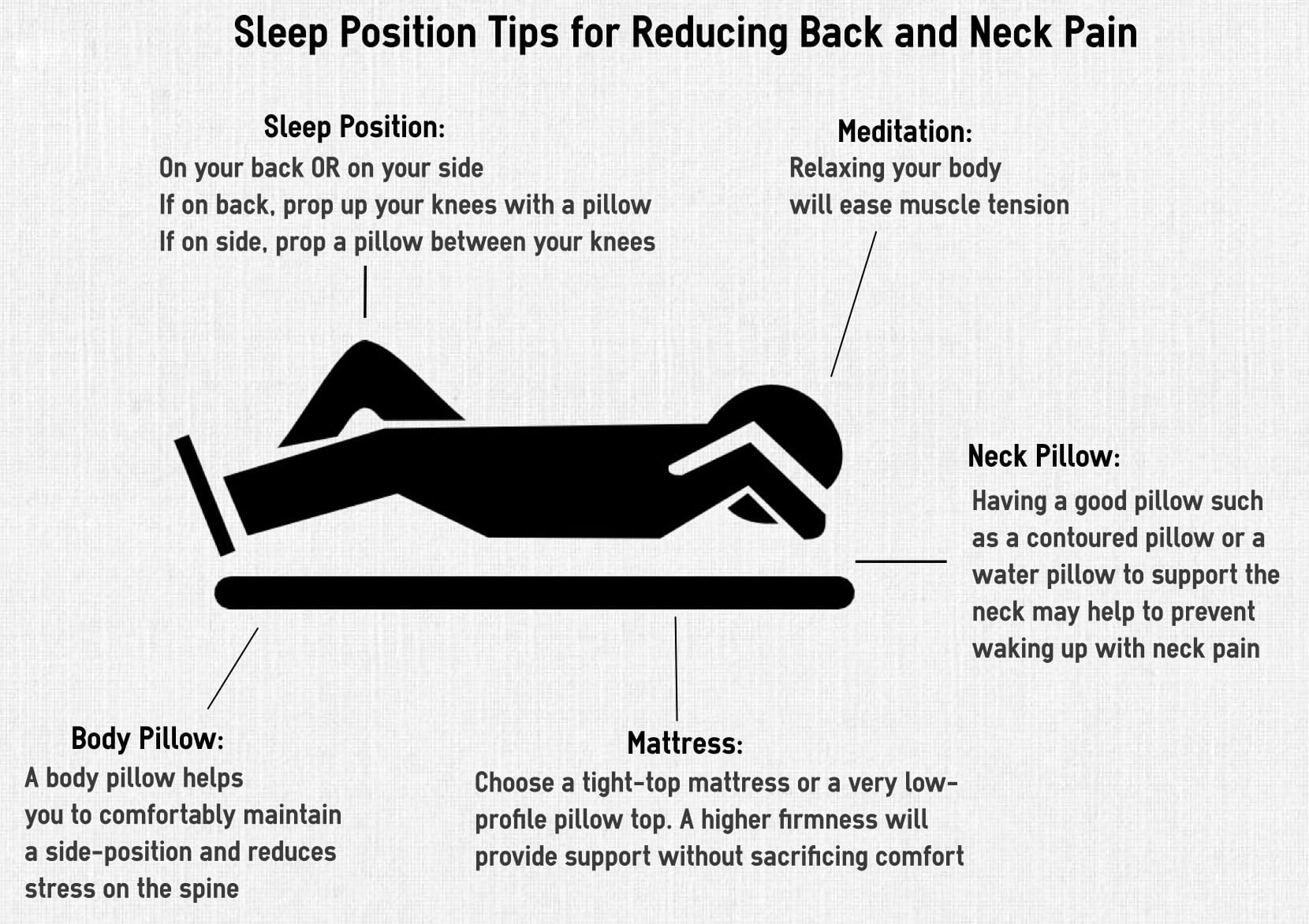
Adjust sleep position to joint pain
If the neck is sore/aching rest the head on a flat pillow so the cervical spine is in a neutral position. For low back joint pain, individuals might find relief by sleeping on their back or side with the knees and hips flexed at a 90-degree angle. For hip joint stiffness, sleeping on the side with a pillow between the legs is recommended.
A firm mattress and support pillow
A firm mattress will support the body and help reduce pain. The right pillow/s are also important for healthy sleep. A lumbar and cervical pillow can help cushion tender areas.
Readjust chores
Joint pain first thing in the morning needs time to adjust. For morning physical chores try to reschedule for later on in the day or if possible the night before. This could be fixing lunches, picking out clothes, preparing breakfast, or packing the work case, tools, etc. The extra time will reduce morning stress and allow the body to gently adjust.
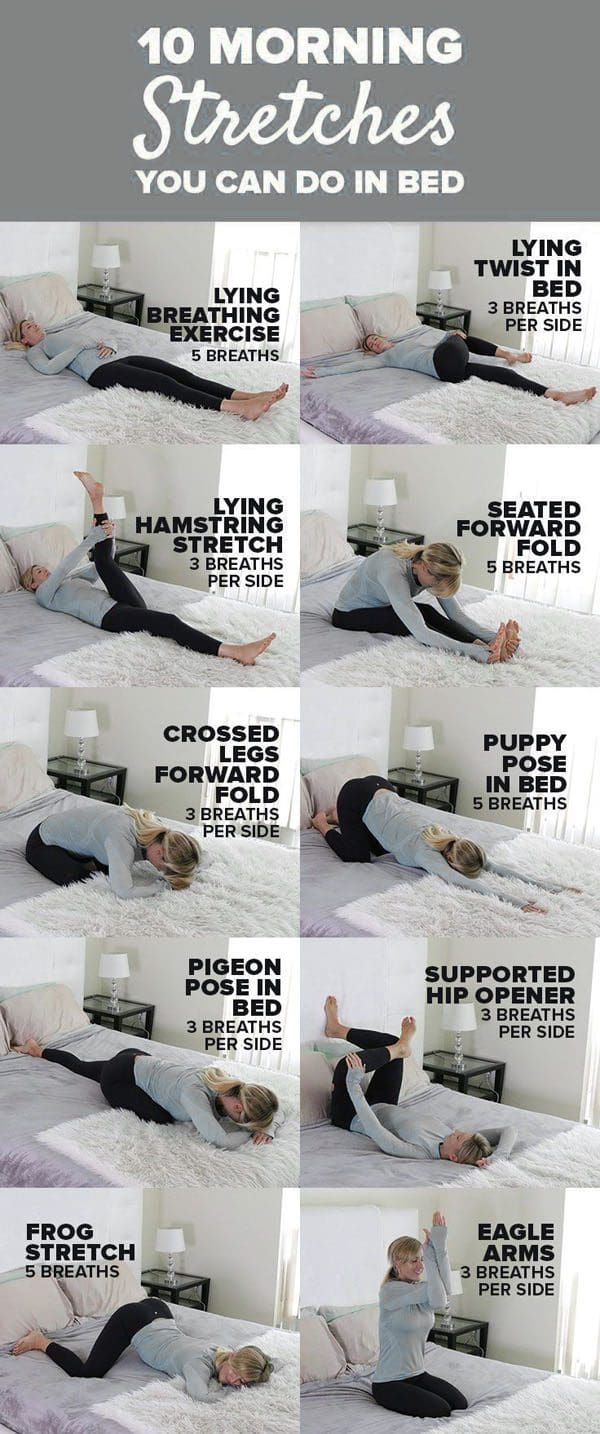
Wake up and stretch
With joint pain in the morning, some gentle stretching can help. Doing some stretches before even getting out of bed will help minimize pain and allow the body to gradually prepare for movement. Follow the stretch session up with a hot shower to loosen stiff joints.
Increase Sleep Quality
Sleep problems can affect anyone even those that don’t have inflammatory spinal arthritis/joint pain. There could be other issues causing sleep problems unrelated to joint pain. If still not getting quality sleep, talk to a rheumatologist about available options.
Body Composition
Osteoarthritis and Exercise
Obesity is a significant risk factor in the development of osteoarthritis. This is not only from the effects of extra weight on the body’s joints but also as a result of the pro-inflammatory effects of adipose tissue. The hips and knees are the weight-bearing joints. Excessive adipose tissue on the midsection and legs have been shown to negatively impact these weight-bearing joints.
Promoting Lean Body Mass and encouraging weight loss can potentially lower the risk of osteoarthritis and improve the quality of life. Gentle exercise is regarded as safe for individuals with osteoarthritis and is a key component to improve body composition, reduce body fat mass, improve lean body mass and maintain a healthy weight. Improving body composition and utilizing exercise in weight management can have a direct and positive effect on joint health.
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Myers W. 9 Ways to Rise and Shine With Osteoarthritis. Everyday Health.�http://www.everydayhealth.com/osteoarthritis/ways-to-rise-and-shine-with-osteoarthritis.aspx. Last updated September 25, 2014. Accessed April 18, 2017.
Watson S. Why Osteoarthritis Could Disrupt Your Sleep�and Your Partner�s. Arthritis Foundation. http://www.arthritis.org/living-with-arthritis/comorbidities/sleep-insomnia/osteoarthritis-and-sleep.php. Accessed April 18, 2017.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine