How do healthcare professionals provide a clinical approach to recognizing trafficking to individuals seeking a safe environment?
Introduction
Around the world, there is a phenomenon that local media and organizations are paying more attention to and that many people should be aware of. This is known as trafficking, and it can encompass a wide range of activities, from forced labor in various industries to sex work. While most individuals of trafficking are usually young women or children, it can affect many individuals of all ages and backgrounds. Many survivors of trafficking are compelled to live with the psychological and physical injuries they sustained from the mistreatment they endured at the hands of their traffickers. This course aims to give medical professionals and others in allied fields an understanding of the realities of human trafficking, as well as the kinds of resources and interventions that can be used to help many individuals trafficking in this two-part series. Today’s article overviews trafficking and how it can impact the individual. In part two, we will discuss the roles and protocols of how healthcare professionals can identify trafficking while providing a safe and positive space for the individual. We discuss with certified associated medical providers who consolidate our patients’ information to assess and identify trafficking in the clinic. We also inform and guide patients while asking their associated medical provider intricate questions to integrate a customized treatment plan for their pain and provide them with a safe and positive space. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
The Definition of Trafficking
It can be challenging to define trafficking since it frequently coexists with other problems like forced marriage, sexual assault, domestic abuse, and forced labor. (Hume & Sidun, 2017) As the United Nations stated, trafficking encompasses the following activities: “as recruitment, transportation, transfer, harboring, or receipt of many individuals using the threat or use of force to achieve the consent of a person having control over another person, for exploitation.” (United Nations Human Rights Office of the High Commissioner, n.d.) The following components of this definition include:
Act: This is a reference to the different forms of human trafficking, including the hiring, transferring, receiving, and harboring of individuals.
Means: Coercion, force, fraud, kidnapping, deception, abuse of power or weakness, or providing cash or other rewards to someone in a position of authority over the victim are typically used to carry out trafficking.
Purpose: Traffickers engage in forced labor, prostitution, sexual exploitation, forced servitude, slavery, and even organ harvesting to further their financial interests.
While the terms are occasionally used synonymously, human trafficking and people smuggling are not the same. Human smuggling is the transportation of a person into the nation by illicit means; it is voluntary, as the person smuggled usually offers compensation to another individual or party to achieve this purpose (Lusk & Lucas, 2009).
The broad term of human trafficking in the Trafficking Victims Protection Act includes both labor trafficking and sex trafficking. Sex trafficking is when someone is under the age of 18 and is obtained, patronized, or solicited for a commercial sex act by deception, force, or compulsion. The forced, coerced, or fraudulent submission of an individual to slavery, debt bondage, involuntary servitude, or peonage is considered labor trafficking. According to the U.S. Congress, the TVPA does not require that trafficking take place if a person is physically moved from one location to another.
The Statistics Of Trafficking
Determining the actual extent of the problem is challenging due to the complexity of the human trafficking issue and the fact that both the offenders and the victims frequently go unnoticed. A few published estimates from academics, researchers, and organizations and agencies responsible for recording and monitoring occurrences of human trafficking are as follows:
According to estimates from the International Labour Organization, there are over 40 million victims of human trafficking worldwide. (International Labour Organization, n.d.)
Over 51,000 complaints of cases of human trafficking have been received by the National Human Trafficking Hotline since 2007 (National Human Trafficking Hotline, n.d.).
The number of persons thought to be trafficked in the United States varies greatly from year to year, with estimates ranging from 40,000 to 50,000. (Weizter, 2007)
In 2017, the United States Department of Justice obtained 1,045 convictions for offenses related to human trafficking, a 78% increase from 2015. (International Labour Organization, n.d.).
According to the International Labour Organization, over 15 million people are in forced marriages, 4.8 million people are victimized by sex trafficking, and forced labor trafficking claims the lives of almost 25 million people globally. (International Labour Organization, 2017)
In the US, Florida is the third-most popular destination for victims of human trafficking. In 2018, there were 767 reports of human trafficking incidents in Florida and close to 1,900 contacts with the National Human Trafficking Hotline. There was almost 70% of sex trafficking, 16.5% of labor trafficking, and 7.5% of both sex and labor trafficking combined. Of the victims, 56% were adults, and 69% were female (National Human Trafficking Hotline, n.d.).
Data Collection Challenges
The current ICD-10-CM abuse codes could not adequately distinguish victims of human trafficking from other abuse victims, even though an increasing number of caregivers are trained to recognize and record individuals of different forms of human trafficking. Clinicians couldn’t properly identify a condition or arrange the resources needed to administer treatment without the right codes. Additionally, this made it impossible to critically monitor the existence and recurrence of human labor or sexual exploitation.
June 2018 saw the publication of the first ICD-10-CM codes for categorizing abuse related to human trafficking, as requested by the American Heart Association’s Hospitals Against Violence program. The proposal for the modification came from the AHA’s Central Office on ICD-10, which collaborated with Catholic Health Initiatives, the Human Trafficking Initiative at Massachusetts General Hospital, and the Freedom Clinic. With effect from FY 2019, certain ICD-10-CM codes can be used to collect data on adult or child forced labor or sexual exploitation, whether it is proven or suspected. These new codes may be issued in addition to other current ICD-10-CM codes for abuse, neglect, and other maltreatment. These codes received support from different hospitals and health systems. Furthermore, there exist novel codes that can be utilized to record an individual’s past labor or sexual exploitation history, examine, rule out, and observe instances of exploitation, and identify multiple, repeating perpetrators of maltreatment and neglect through an external cause of code (Macias-Konstantopoulos, 2018).
The ICD-10-CM provides specific abuse codes for a range of abuse experiences, such as physical abuse of an older adult, sexual abuse of a child, and violence against a spouse or partner. Similar to how disease diagnosis codes are used, tracking the frequency and trends of particular abuse types, their relationships to other injuries and illnesses, and the kinds of resources that might be needed to stop the abuse are all made feasible by recording abuse using the relevant ICD-10-CM code. Adopting prevention strategies, creating best practices for treatment, introducing new services and payment methods, and establishing new financing and research fields are all made possible by using these codes as the primary diagnosis (Macias-Konstantopoulos, 2018).
Documenting particular types of violence and abuse alone does not give a full picture of the abuse experience. Every abuse experience is a result of a complex interaction between several variables, including the physical surroundings, social and familial dynamics, and personal risks and vulnerabilities. Healthcare professionals can respond to illnesses and injuries connected to abuse as well as underlying health-related social and mental requirements more effectively when these aspects are assessed, documented, and coded using ICD-10-CM Z codes. Similarly, applying ICD-10-CM S, T, V, W, X, and Y codes to record and classify external causes of morbidity as well as the nature, purpose, and mechanism of injury can help shed light on how abuse and violence are committed and pave the way for further preventative measures (Macias-Konstantopoulos, 2018).
Required Actions
Coders should be aware of and start using the ICD-10-CM codes for forced labor and sexual exploitation as they examine a patient’s medical records to determine which ICD-10-CM codes to include.
Hospitals and health systems should inform those who need to know—doctors, nurses, other medical professionals, and coding specialists, among others—about the significance of gathering data on forced labor and sexual exploitation of people.
By keeping track of verified and suspected cases within the healthcare system, hospitals, and health systems can better monitor victim requirements and find ways to enhance community health.This practice also offers an additional means of gathering data to help the systemic creation of a service and resource infrastructure, as well as attempts to prevent harm and inform public policy.
The accompanying chart illustrates the distinction between focused and comprehensive assessment, documentation, and coding of abuse. It also highlights how these differences may affect medical professionals’ reactions to cases and their comprehension of the kinds of resources that may be required to help victims of human trafficking (Macias-Konstantopoulos, 2018).
Beyond the Surface: Understanding the Effects of Personal Injury- Video
Common Misconceptions of Trafficking
There is a misconception that trafficking entails the kidnapping and crossing of national or international borders for various activities to individuals. This misconception fails to acknowledge that individual trafficking can be of any ethnicity, gender, or country and that it can happen almost anywhere and in any sector of the economy. A handful of the widespread myths about human trafficking are as follows:
Myth: Physical violence is a common part of trafficking. Traffickers frequently employ nonviolent tactics, such as deception, manipulation, intimidation, and deceit, to coerce their victims into exploitative circumstances, even while physical violence plays a role in many of their crimes.
Myth: Sexual exploitation is a necessary component of trafficking. It’s likely the most well-known type of trafficking, but commercial sexual exploitation of victims is also a frequent practice. However, experts think that labor trafficking is more commonplace throughout the world.
Myth: Only undocumented foreign nationals are victims of trafficking.The Polaris Project operates the National Human Trafficking Hotline, which has handled thousands of cases of trafficking involving foreign nationals who are lawfully employed or residing in the United States.
Myth: Only illicit or covert sectors are involved in trafficking. Trafficking has been documented concerning several legitimate industries, including manufacturing, restaurants, cleaning services, and construction.
Myth: Transporting a person across state or national borders is a part of trafficking. Human smuggling is the illicit movement of persons across state or national borders. There can be trafficking even when there is no cross-border travel. A person may even become a victim of trafficking in their own house or hometown.
Myth: Trafficking is always a part of the commercial sex trade. Any commercial sex with kids is invariably seen as human trafficking. Adult commercial sex is only classified as trafficking when the victim is coerced, compelled, or deceived into doing it against their will.
Common Forms of Trafficking
There are many forms of trafficking as many individuals that were trafficked are categorized into the following:
Sex Trafficking
Bonded Labor/Forced Labor
Child Labor
Child Conscription
The Impact & Consequences of Trafficking on Individuals
For someone who has never experienced human trafficking, it might be challenging to understand why so many victims choose to remain silent or show such a strong willingness to cooperate with their traffickers (Johnson, 2012). According to Baldwin, Fehrenbacher, and Eisenman (2015), the victim’s compliance and quiet are influenced by the following elements, which the quiet Compliance Model explains:
Coercion: Traffickers use violence, intimidation, and depriving the individual of basic needs to force them into obedience. Traffickers may employ psychological strategies, including isolation, degrading treatment, and induced tiredness in addition to physical force. As a result, the individual experiences a distorted sense of reality and feels helpless.
Collusion: The victim’s cooperation with their traffickers in trafficking or other illicit activities may result from a combination of factors, including fear, loneliness, total dependence, and even a sense of identification with the trafficker.
Contrition: The victims’ guilt and regret for their acts, despite the coerced collaboration, only serve to guarantee their quiet (Johnson, 2013).
Trafficking individuals are susceptible to a wide range of health issues, including chronic illnesses brought on by inadequate working conditions or malnourishment, unwanted pregnancies, severe injuries, and STDs. It’s crucial to remember that emotional issues are often experienced as physical illnesses or sensations in certain cultures. For instance, depression, stress, or anxiety may manifest as symptoms of exhaustion, headaches, or gastrointestinal issues (Greenbaum, 2018; Zimmerman, Hossain, & Fun, 2008).
Conclusion
It is important to recognize the signs of trafficking in individuals who have been dealing with these issues. In part 2 of this series, we will look at how healthcare workers are identified and what procedures to take when a patient is trafficked. This allows the individual to know they are in a safe and positive environment to get the help they deserve.
References
Baldwin, S. B., Fehrenbacher, A. E., & Eisenman, D. P. (2015). Psychological Coercion in Human Trafficking. Qualitative Health Research, 25(9), 1171-1181. https://doi.org/10.1177/1049732314557087
Greenbaum, V. J. (2017). Child sex trafficking in the United States: Challenges for the healthcare provider. PLoS Med, 14(11), e1002439. https://doi.org/10.1371/journal.pmed.1002439
Hume, D. L., & Sidun, N. M. (2017). Human Trafficking of Women and Girls: Characteristics, Commonalities, and Complexities. Women & Therapy, 40(1-2), 7-11. https://doi.org/10.1080/02703149.2016.1205904
Lusk, M., & Lucas, F. (2008). The challenge of human trafficking and contemporary slavery. Journal of Comparative Social Welfare, 25(1), 49–57. https://doi.org/10.1080/17486830802514049
Macias-Konstantopoulos, W. L. (2018). Diagnosis Codes for Human Trafficking Can Help Assess Incidence, Risk Factors, and Comorbid Illness and Injury. AMA J Ethics, 20(12), E1143-1151. https://doi.org/10.1001/amajethics.2018.1143
Parreñas, R. S., Hwang, M. C., & Lee, H. R. (2012). What Is Human Trafficking? A Review Essay. Signs: Journal of Women in Culture and Society, 37(4), 1015–1029. https://doi.org/10.1086/664472
Saiz Echezarreta, V., Alvarado, C., & Gómez-Lorenzini, P. (2018). Advocacy of trafficking campaigns: A controversy story. Comunicar, 26(55), 29–38. https://doi.org/10.3916/c55-2018-03
Weitzer, R. (2007). The Social Construction of Sex Trafficking: Ideology and Institutionalization of a Moral Crusade. Politics & Society, 35(3), 447-475. https://doi.org/10.1177/0032329207304319
Zimmerman, C., Hossain, M., Yun, K., Gajdadziev, V., Guzun, N., Tchomarova, M., Ciarrocchi, R. A., Johansson, A., Kefurtova, A., Scodanibbio, S., Motus, M. N., Roche, B., Morison, L., & Watts, C. (2008). The health of trafficked women: a survey of women entering posttrafficking services in Europe. Am J Public Health, 98(1), 55-59. https://doi.org/10.2105/AJPH.2006.108357
A dislocated elbow is a common injury in adults and children and often happens in tandem with bone fractures and nerve and tissue damage. Can physical therapy help to support recovery and ensure range of motion?
Dislocated Elbow Injury
Elbow dislocations are generally caused by trauma when the elbow bones no longer connect. Individuals falling onto an outstretched hand is the most common cause of the injury. (James Layson, Ben J. Best 2023) Healthcare providers will try to relocate the elbow using a closed reduction. Individuals may require surgery if they cannot relocate the elbow using closed reduction.
The hinge function allows the bending and straightening of the arm.
Ball-and-socket joint
The ball-and-socket function allows you to rotate the palm of your hand to face up or face down.
A dislocated elbow injury can damage bones, muscles, ligaments, and tissues. (American Academy of Orthopaedic Surgeons. 2021) The longer the elbow remains out of the joint, the more damage can occur. Elbow dislocations rarely reset into their joints on their own and are recommended to be evaluated by a qualified healthcare provider to prevent permanent damage to nerves or function.
It is not recommended to try to reset the elbow on your own.
A healthcare provider will work to restore the joint and ensure proper alignment.
Before the reset, they will perform a physical examination to assess blood circulation and any nerve damage.
A closed reduction means that the elbow can be relocated without surgery.
Before the closed reduction, a healthcare provider will administer medications to help relax the individual and address the pain. (Medline Plus. 2022)
Once relocated into the correct position, a healthcare provider applies a splint (usually at a 90-degree angle of flexion) to keep the elbow in place. (James Layson, Ben J. Best 2023)
The objective is to prevent elbow extension, which can cause re-dislocation.
For individuals dealing with chronic pain conditions can having a better understanding of pain management specialists help in developing effective multidisciplinary treatment plans?
Pain Management Specialists
Pain management is a growing medical specialty that takes a multi-disciplinary approach to treating all types of pain. It is a branch of medicine that applies scientifically proven techniques and methods to relieve, reduce, and manage pain symptoms and sensations. Pain management specialists evaluate, rehabilitate, and treat a spectrum of conditions, including neuropathic pain, sciatica, postoperative pain, chronic pain conditions, and more. Many primary healthcare providers refer their patients to pain management specialists if pain symptoms are ongoing or significant in their manifestation.
Specialists
Healthcare providers specializing in pain management recognize the complex nature of pain and approach the problem from all directions. Treatment at a pain clinic is patient-centric but depends on the clinic’s available resources. Currently, there are no set standards for the types of disciplines needed, another reason treatment options vary from clinic to clinic. Experts say that a facility should offer patients:
A coordinating practitioner specializing in pain management and consulting specialists on the patient’s behalf.
Other specialties represented in pain management are anesthesiology, neurosurgery, and internal medicine. A coordinating healthcare provider may refer an individual for services from:
A healthcare provider should have completed additional training and credentialing in pain medicine and be an MD with board certification in at least one of the following (American Board of Medical Specialties. 2023)
Anesthesiology
Physical rehabilitation
Psychiatry
Neurology
A pain management physician should also have their practice limited to the specialty they hold the certification.
Management Goals
The field of pain management treats all types of pain as a disease. Chronic, such as headaches; acute, from surgery, and more. This allows for applying science and the latest medical advances to pain relief. There are now many modalities, including:
Medication
Interventional pain management techniques – nerve blocks, spinal cord stimulators, and similar treatments.
Physical therapy
Alternative medicine
The objective is to minimize and make symptoms manageable.
Individuals determined that surgery does not benefit their condition.
A better understanding of pain syndromes by communities and insurance companies and increased pain studies will help increase insurance coverage for treatments and technology to improve interventional outcomes.
Nalamachu S. (2013). An overview of pain management: the clinical efficacy and value of treatment. The American journal of managed care, 19(14 Suppl), s261–s266.
American Society of Interventional Pain Physicians. (2023). Pain Physician.
Individuals dealing with various conditions and diseases and ongoing research to find treatments, where do human regenerative cells come from?
Regenerative Cells
Regenerative cells are stem cells that are specialized to potentially develop into many different types of cells. They are unlike any other cell because:
Being unspecialized they have no specific function in the body.
They can become specialized cells like – brain, muscle, and blood cells.
They can divide and renew continually for a long period.
Blood stem cells are currently the only type that is regularly used in treatment.
For leukemia or lymphoma, only adult cells are used in a procedure known as a bone marrow transplant. (Cleveland Clinic. 2023)
For regenerative cell research, the cells can come from different sources, including adult donors, genetically altered human cells, or embryos.
Bone Marrow Transplants
Bone marrow cells produce all of the body’s blood cells, including red and white blood, and platelets.
Hematopoietic stem cells are those found in bone marrow that is the parent for the different types of cells.
Hematopoietic cells are transplanted in individuals with cancer to replenish bone marrow.
The procedure is often used during high-dose chemotherapy that destroys the existing cells in the bone marrow.
Donated stem cells are injected into a vein and settle in the bone marrow where they begin to produce new healthy blood cells. (Cleveland Clinic. 2023)
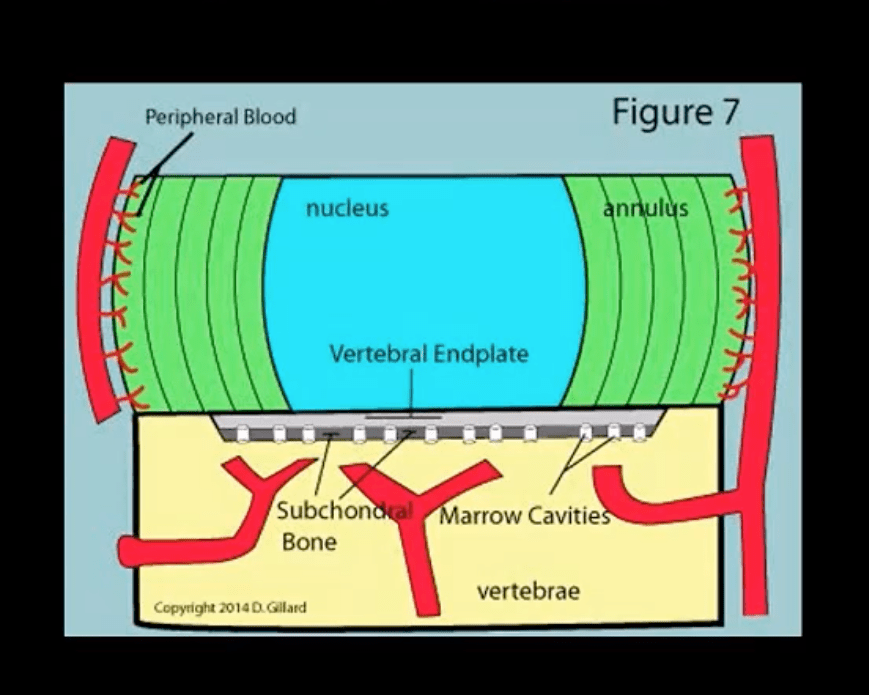
Peripheral Blood Transplants
For some time the only source to extract hematopoietic cells was from bone marrow.
Researchers found that many of these cells were freely circulating in the blood.
Scientists learned how to extract the cells from the blood and transplant them directly.
This type of transplant is a peripheral blood stem cell transplant/PBSCT and has become the more common procedure, however, both methods are still used. (Cleveland Clinic. 2023)
PBSCT is less invasive and does not require the removal of marrow from the hip bone.
Somatic Cells
Adult stem cells are called somatic and are acquired from a donor.
Embryonic stem cells were first grown in a laboratory in 1998 for reproductive research, which created controversy because they were extracted from human embryos that were destroyed or harvested for science. Today their primary use is for research into treatments and potential cures for:
Embryonic cells are pluripotent, which means they can grow into the three types of germ cell layers – ectoderm, mesoderm, and endoderm – that make up the human body and can develop into each of the more than 200 types of cells. (National Institutes of Health. 2016)
Induced Pluripotent Cells
Induced pluripotent stem cells/iPSCs are somatic cells that have been genetically reprogrammed to behave like embryonic cells.
Simara, P., Motl, J. A., & Kaufman, D. S. (2013). Pluripotent stem cells and gene therapy. Translational research : the journal of laboratory and clinical medicine, 161(4), 284–292. https://doi.org/10.1016/j.trsl.2013.01.001
Finkbeiner, S. R., & Spence, J. R. (2013). A gutsy task: generating intestinal tissue from human pluripotent stem cells. Digestive diseases and sciences, 58(5), 1176–1184. https://doi.org/10.1007/s10620-013-2620-2
Al-Shamekh, S., & Goldberg, J. L. (2014). Retinal repair with induced pluripotent stem cells. Translational research : the journal of laboratory and clinical medicine, 163(4), 377–386. https://doi.org/10.1016/j.trsl.2013.11.002
Improving posture can be challenging. Poor posture is often the source of various musculoskeletal issues like chronic pain throughout the body. Poor posture can be so ingrained in the brain that it becomes an unconscious positioning reflex that feels right but could be worsening spinal, hip, and leg problems. The Alexander Technique could be a treatment option that could help long-term.
Alexander Technique
The approach focuses on learning mind-body awareness. It is an educational process to teach individuals to become aware of their body positioning and change unhealthy posture/movement habits into healthy ones. The objective is learning to utilize sufficient levels of muscle tension for everyday activities, like sitting, standing up, and walking in a healthy way to maintain optimal health of the musculoskeletal system.
The theory is that less tension minimizes wear and tear on the muscles and structures of the spine vulnerable to compression.
The fundamental goal of the Alexander Technique is to undo all the unhealthy tension habits to decompress the spine and retrain the mind and body to approach movement and body positioning in a new and healthy way.
Teachings
The technique can be done in a class setting or one-on-one teaching because everyone’s postural and movement habits are unique. A teacher helps identify the tension-inducing postures and educates the individual on how to correct them. Human touch is an integral part of the Alexander Technique. Using their hands gently to adjust the individual to a proper upright position, a teacher helps release pressure from the head, neck, shoulders, and upper back. The individual learns to release the tension throughout their body. The Alexander Technique is a type of hands-on therapy; it is not manipulation or massage. It uses a light touch with no risk of injury to the spine, allowing anyone to participate. However, individuals must be willing to participate/engage in the process to get the benefits. Most individuals can tell if it’s right for them during the first lesson.A typical program teaches:
Staying alert to the body’s warning of tension and compression.
Tension Build Up
Individuals usually don’t even realize they’re constantly placing pressure on their spine from unhealthy postural habits, building up muscular tension they never knew they created. For example, unhealthy neck position habits include:
Pushing the head forward
Slumping over
Pinning the shoulders back
These postures generate/build pressure and tension that radiates outward and down to the large muscles of the spine.
Habitual downward pressure can pull and change the spine’s shape, leading to degenerative forms of spinal deformity in severe cases.
When the tension is released, the neck and body begin to stand upright comfortably, without pulling down or pulling back.
Frederick Matthias Alexander
Developed the technique in the 1890s to help his muscle tension problems affecting his acting career. When performing, he would stiffen his neck and pull his head back and up, building tension that caused him to tighten his throat and lose his voice. He did not know he was doing this until he performed in front of a mirror and saw his awkward positioning. He realized this and retrained himself to pose naturally, stay relaxed, and be aware of any tension building in the muscles to release it immediately. Alexander Technique educators/practitioners practice all over the world. The American Society for the Alexander Technique or AmSAT website has a Find A Teacher Tool that connects individuals to AmSAT-approved teachers.
Body Composition
Practicing Mindfulness
Developing a mindfulness practice can help identify triggers of negative behavior or thoughts. Just like diet and exercise, practicing mindfulness is unique to everyone. It is recommended to try different things like:
Journaling is another way to tune into oneself. Grab a pen and paper, a computer, tablet, or phone, and take a few minutes to write every day.
Write one thing that makes you happy.
One thing you want to improve.
One goal you want to accomplish that day or that week.
Mindful music listening can help reduce stress by allowing the individual to focus their attention when their mind is going in all directions.
Instead of turning to the news or email when waking up, grab a cup of coffee or tea and listen to a favorite podcast or music.
Put the phone away and listen to your mind and self.
Try to meditate in the morning when waking up. This helps set the day’s goals/plans. Goal-setting mindfulness has been shown to reduce stress levels and anxiety. However, if the morning is not possible then at night before bed can be used to reflect on the day’s activities, what went well, what didn’t, how to improve something, whatever the case, the point is to make time for yourself to reflect, set goals, and develop a plan to achieve those goals.
References
Becker, Jordan J et al. “Preliminary evidence for feasibility, efficacy, and mechanisms of Alexander technique group classes for chronic neck pain.” Complementary therapies in medicine vol. 39 (2018): 80-86. doi:10.1016/j.ctim.2018.05.012
Cacciatore et al., Improvement in automatic postural coordination following Alexander technique lessons in a person with low back pain. Physical Therapy Journal, 2005; 85:565-578. Accessed January 5, 2011
Chin, Brian et al. “Psychological mechanisms driving stress resilience in mindfulness training: A randomized controlled trial.” Health psychology: official journal of the Division of Health Psychology, American Psychological Association vol. 38,8 (2019): 759-768. doi:10.1037/hea0000763
Little P, Lewith G, Webley F, et al. Randomised controlled trial of Alexander technique lessons, exercise, and massage (ATEAM) for chronic and recurrent back pain. The BMJ. 2008;337:a884. doi: https://doi.org/10.1136/bmj.a884.
Paolucci, Teresa et al. “Chronic low back pain and postural rehabilitation exercise: a literature review.” Journal of pain research vol. 12 95-107. December 20 2018, doi:10.2147/JPR.S171729
aka Spondylodiscitis and vertebral osteomyelitis overall are relatively infrequent and may present with bimodal distribution: children and adults >50’s
Occasionally considered as two separate entities due to variations in the blood supply of pediatric vs. adult spines
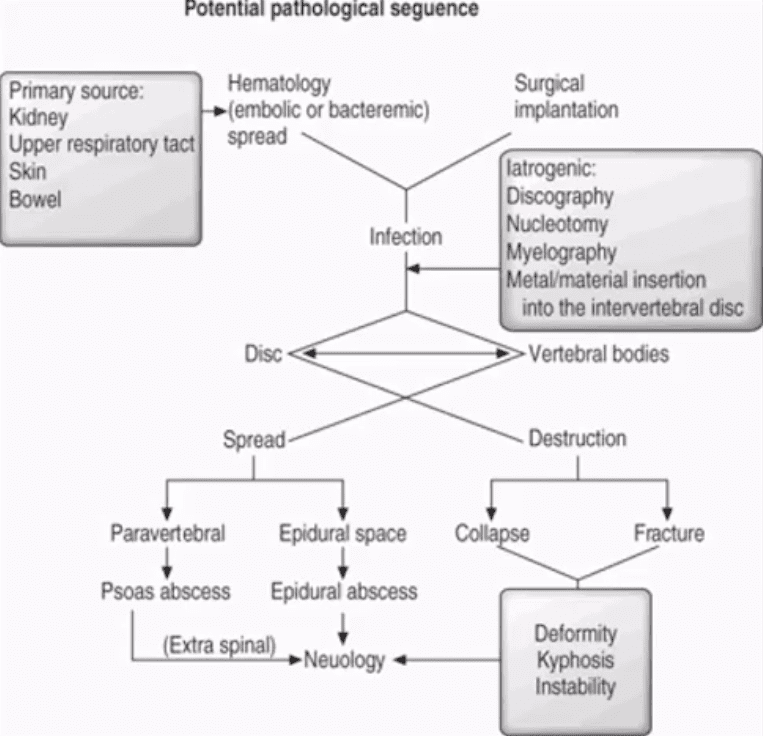
Risk factors/causes: distant site of infection in the body (25-35%), e.g., oropharynx, urogenital infections, bacterial endocarditis, indwelling catheters, florid skin infections furunculosis/abscess, etc.
Iatrogenic:�operative (e.g., discectomy) interventional or diagnostic/therapeutic procedures
Penetrating trauma
Immunocompromised patients
Diabetics
Malnourished patients or patients with low protein
IV drug users
Chronic disease patients, cancer patients etc.
Potential Pathological Sequence
Clinical Presentation
Back pain with or w/o high fever and other “septic” signs. Fever may only present in 50% of children
Exacerbation of pre-existing back pain in post-surgical cases
Neurological complications in advanced cases of vertebral destruction and epidural abscess
Meningitis, septicemia etc.
Labs: Blood tests are unspecific, may or may not indicate elevated ESR/CRP, WBC
Diagnostic imaging is important but
If clinical suspicion is strong, prompt I.V. antibiotics are needed to prevent serious complications
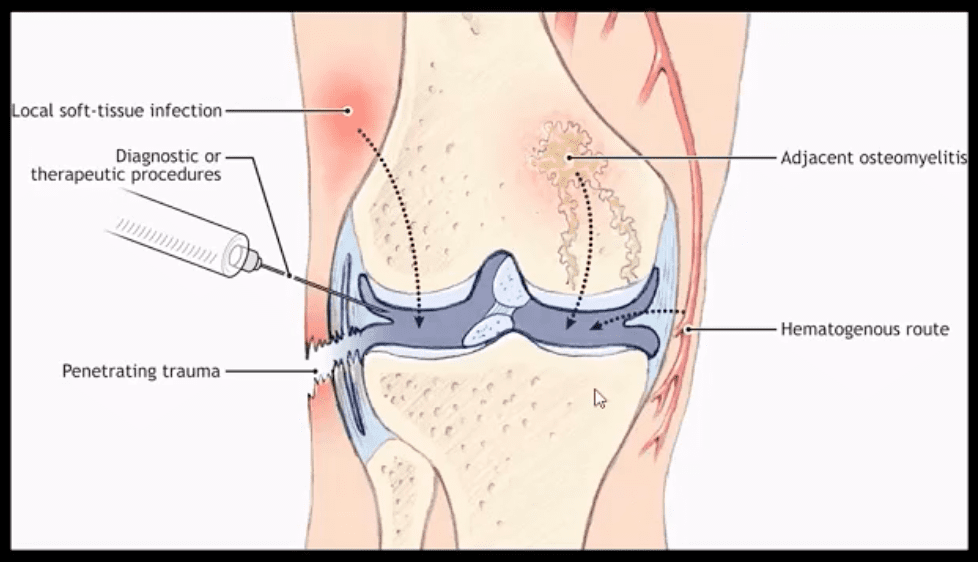
Routes of Infection
Infection routes to the spine are similar to bone in general
3-distinct routes:
1) Hematogenous spread as bacteremia (most common)
2) Adjacent site of infection (e.g., soft tissue abscess)
3)Direct inoculation (e.g., iatrogenic or traumatic)
M/C organism Staph. Aureus
Mycobacterium TB (tuberculous spinal osteomyelitis) aka Pott’s disease can be presented in cases of re-activated or disseminated pulmonary TB
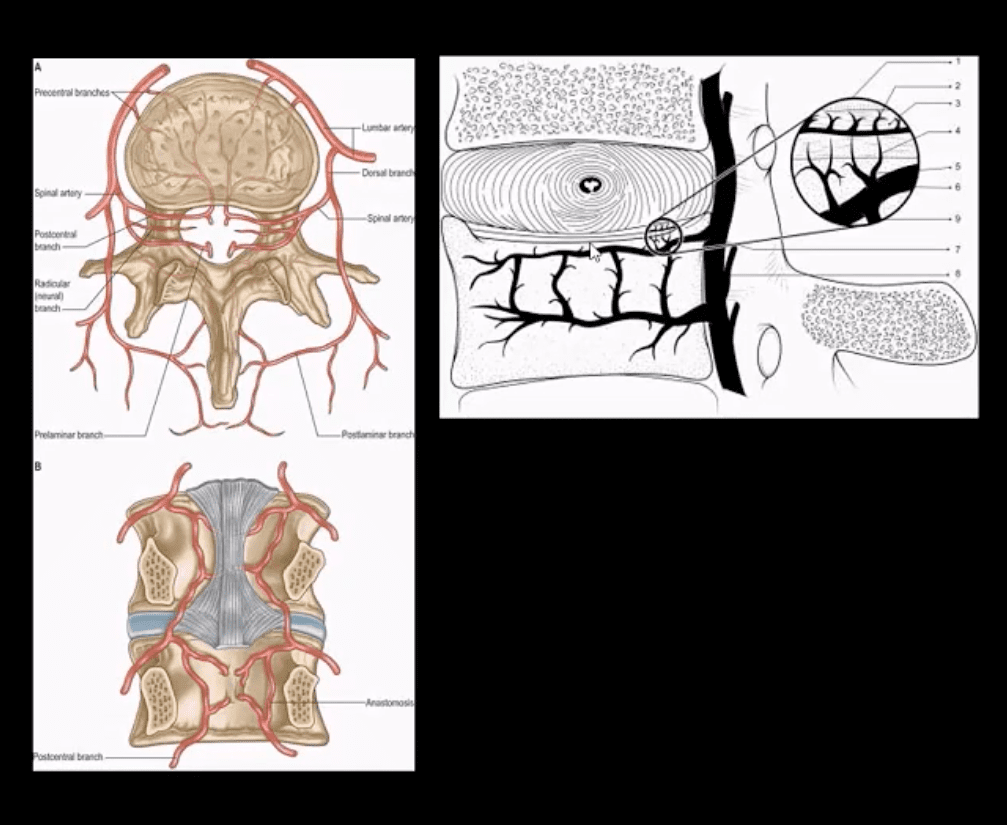
Mechanisms of Spinal Infection
May vary depending on the patients’ age
In children, the IVD receives direct blood supply and can be infected directly spreading to adjacent bone and causing spondylodiscitis
In Adults
The disc is avascular
Pathogens invade adjacent vertebral end-plates via end-arterial supply of the vertebral body that may facilitate infection due to slow, turbulent flow
Organisms may then quickly gain access to disc substance rich in nutrients (discitis) often w/o significant initially visible destruction to the bone
Thus, one of the earliest rad. findings of spinal infection or sudden reduction of disc height
Later end-plate irregularity/sclerosis may develop, subsequently affecting the entire adjacent vertebral bodies
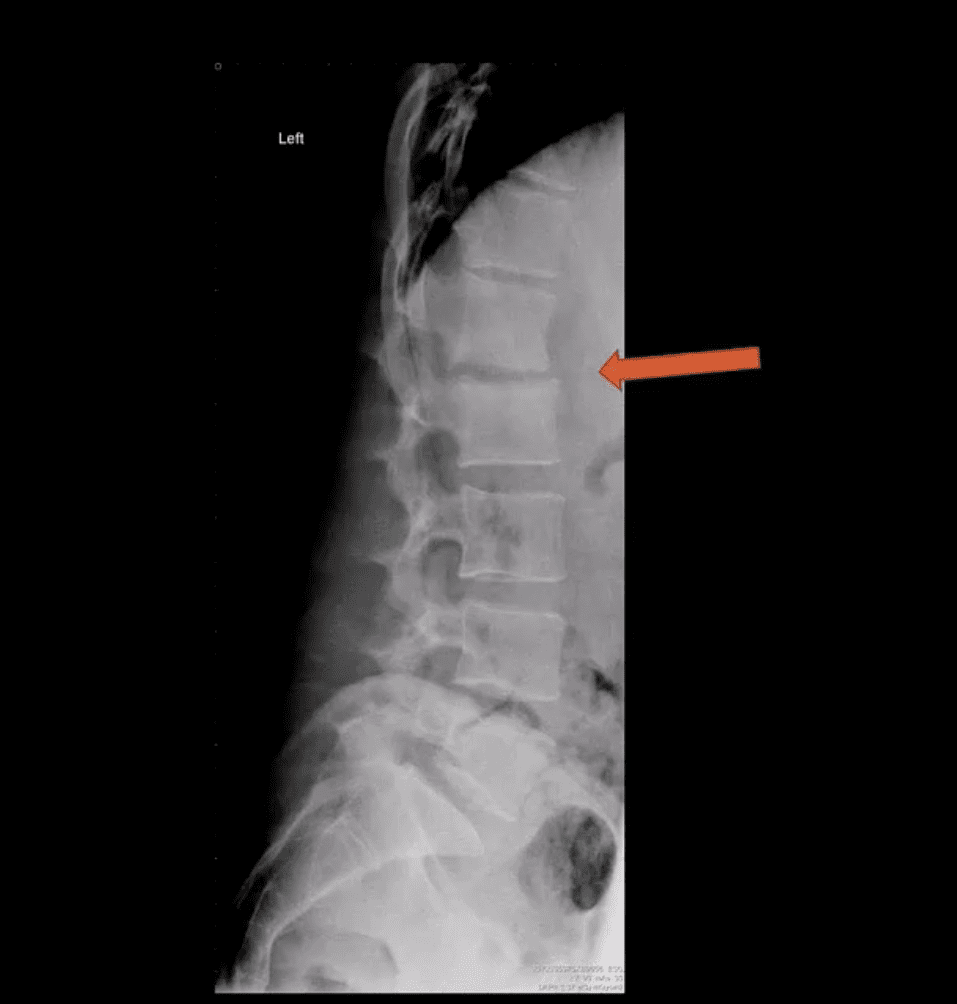
Diagnostic Imaging
Initially, in most cases of MSK complaints, radiography is the 1st imaging step
Initially, X-radiography is often unrewarding and may appear unremarkable for 7-10 days or presents with some subtle soft tissue changes (e.g., obscuration of Psoas shadows etc.)
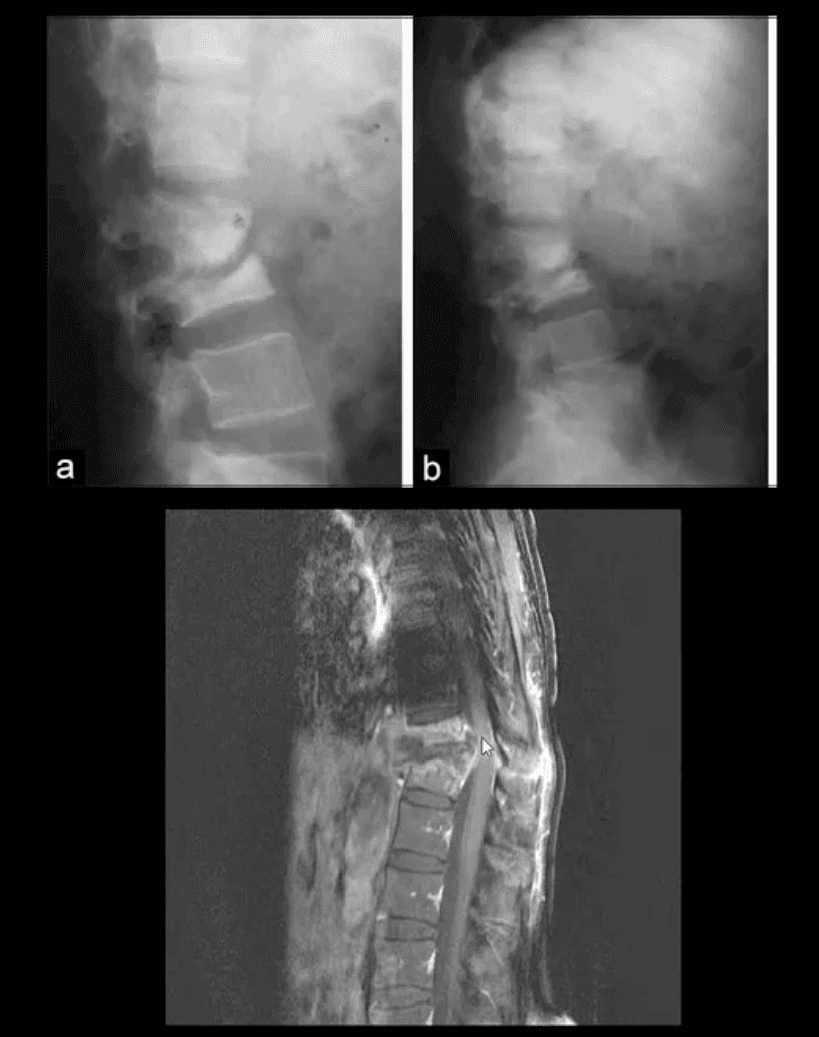
Some of the earliest x-ray signs of pyogenic spondylodiscitis: sudden reduction of disc height (above arrow) during initial 7-10 days
Subsequently (10-20 days) some end-plate irregularity and adjacent sclerosis may be noted
In more advanced cases, subsequent vertebral destruction and collapse may occur
N.B. Reliable feature to DDx between spinal infection and metastasis is the preservation of disc height in the latter
Note:�sudden disc narrowing with no appreciable spondylosis (above the first image) is suspicious for infection (discitis)
MRI +C is required to evaluate suspected infection
N.B. 50-60% of pyogenic spondylodiscitis occur in the lumbar region
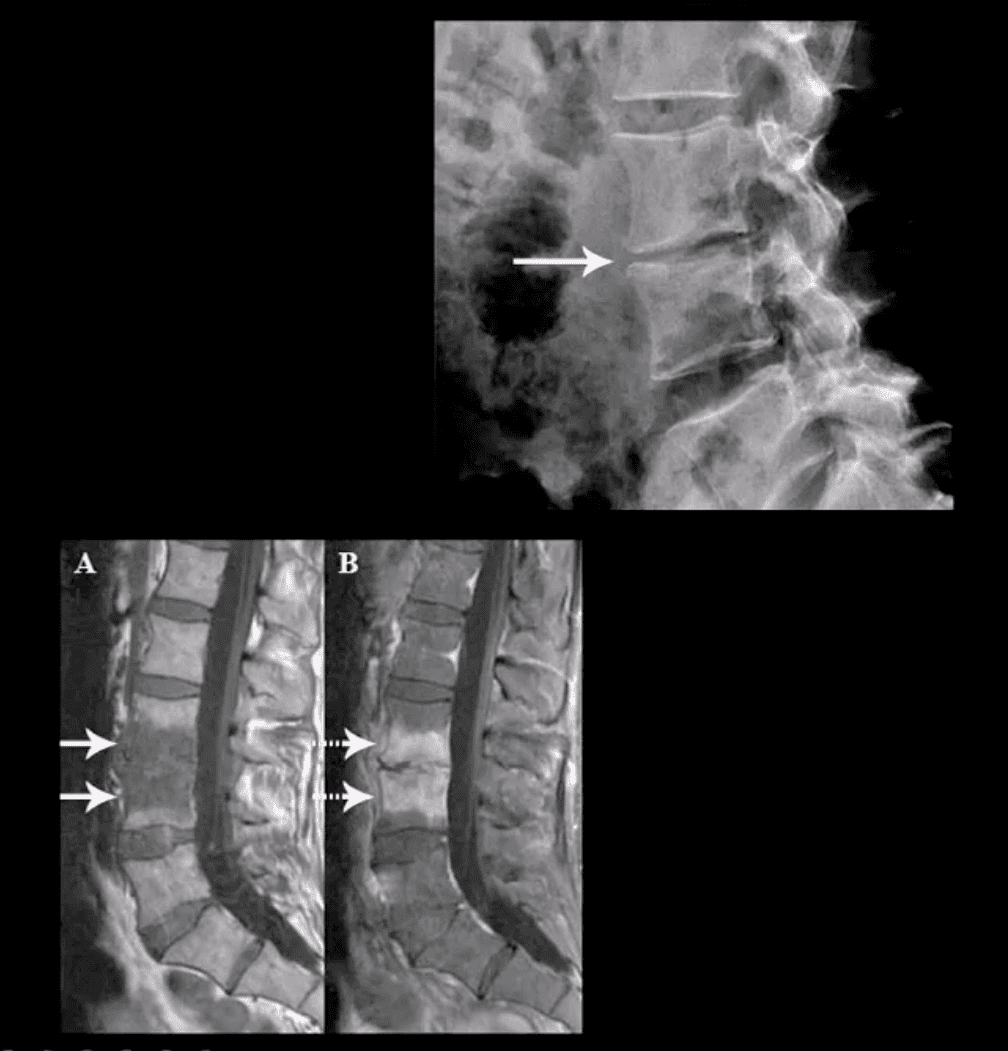
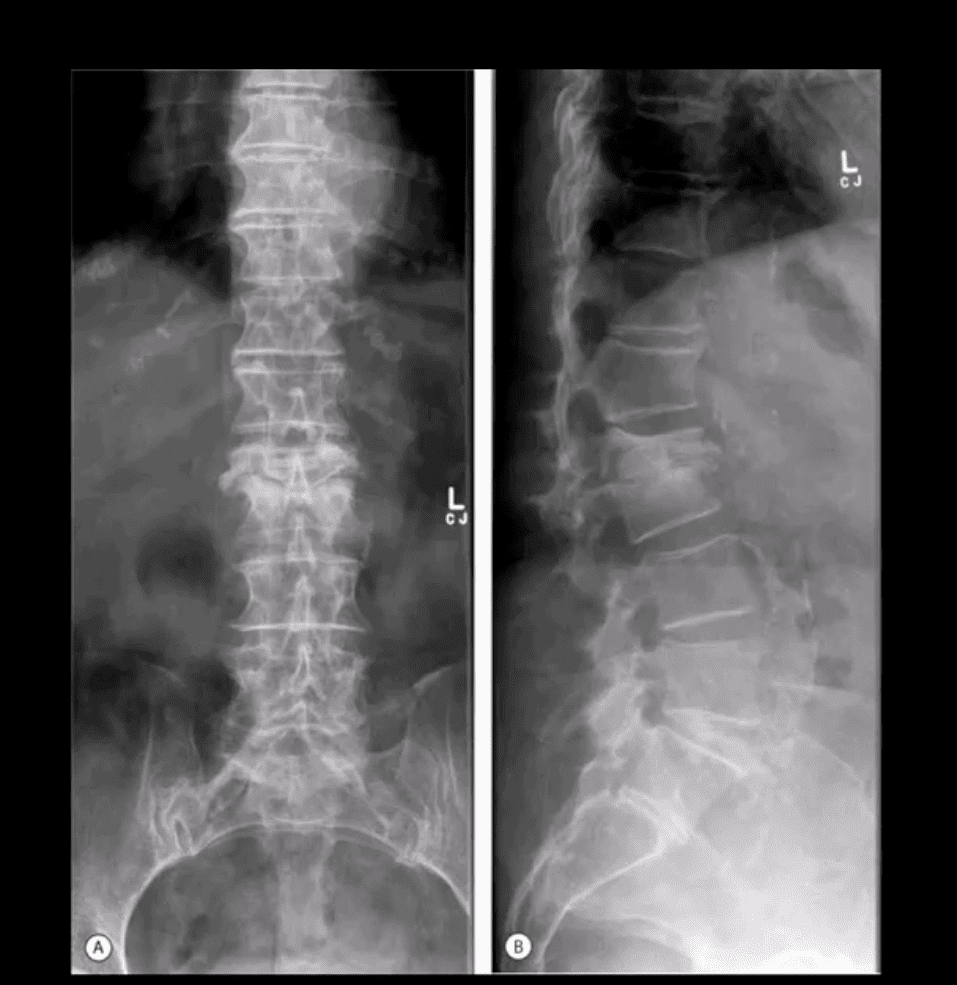
AP & Lateral Lumbar Radiographs
Note severe disc narrowing and adjacent vertebral body destruction at L1-L2 in a 68 -y.o.-female with a known Hx of type 2 DM
Additional imaging modalities should be used to support the Dx
Final Dx: Pyogenic Spondylodiscitis
Sagittal T1 & T2 MRI
Weighted MRI slices of a patient who had laminectomy at L4
MR imaging with gad contrast is the modality of choice for Dx of spinal infection
Early septic changes affecting the disc and adjacent vertebral end-plates are readily demonstrated as a low signal on T1 and high T2/STIR d/t edema and inflammation
T1 FS +C gad images show avid enhancement of the lesion due to granulation tissue around the phlegmon. Peripheral enhancement is also characteristic of an abscess.
Epidural extension/abscess can also be successfully detected my MRI
N.B. 50% of epidural abscess cases present with neurological signs
STIR & T1 FS +C Gad Sagittal MRI
Marked septic collection and edema affecting L4-5 disc and vertebral body with some epidural extension and paraspinal soft tissue edema. Avid contrast enhancement is noted surrounding low signal foci within the bone and disc tissue, some gad. Enhancement is noted in posterior paraspinal muscles and dural spaces
Management: Dx of spondylodiscitis requires prompt I.V antibiotics. If instability and neurological complications develop referral to a Neurosurgeon is required
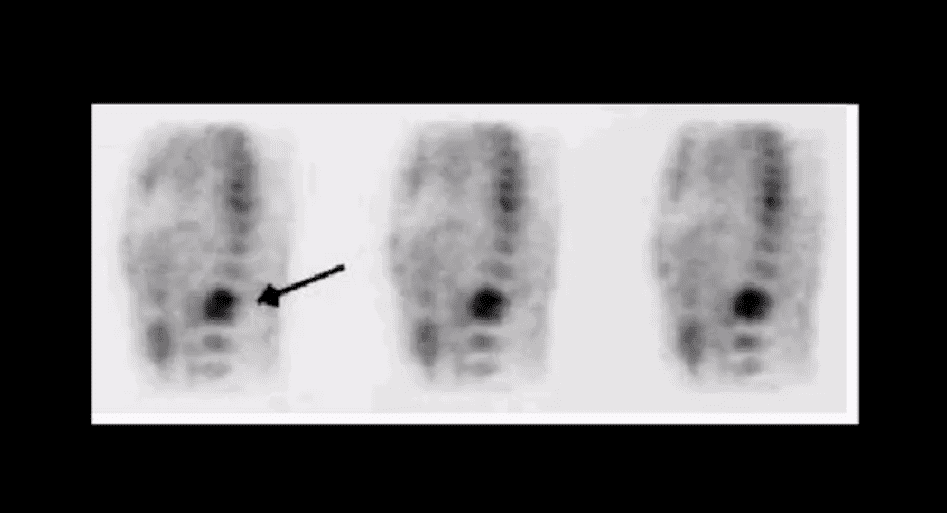
MRI Unavailable or Contraindicated
Bone scintigraphy is very sensitive but non-specific for spinal infection but overall is of great value d/t higher sensitivity than x-rays and relatively low cost.
An area of increased flow with radiopharmaceutical uptake is characteristic but not specific sign of spondylodiscitis
If neurological signs are present and MRI is contraindicated than CT myelography may be used
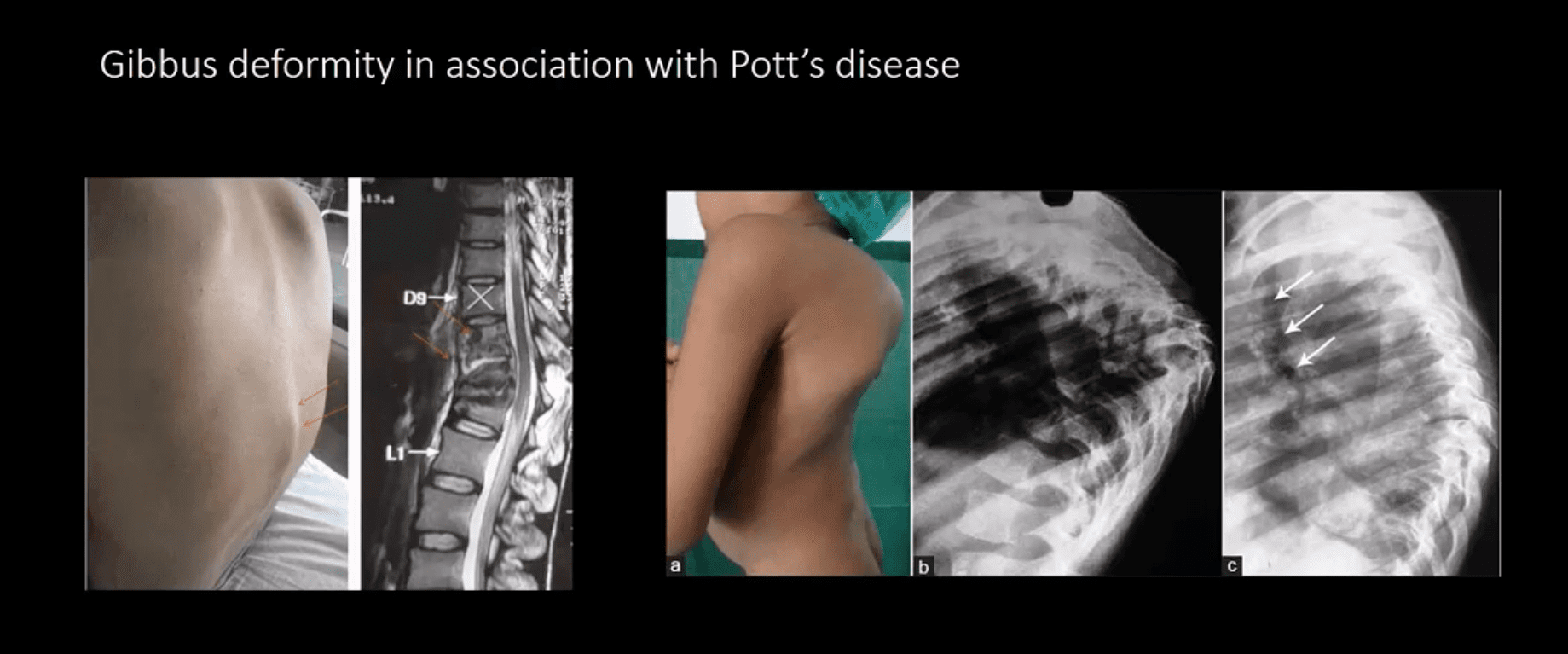
TB Osteomyelitis aka Pott’s Disease
TB osteomyelitis is increasing d/t HIV and other immunocompromised states. Extrapulmonary TB m/c affects the spine and especially the thoracic spine (60%)
Radiographic Pathology:�TB bacillus infects the vertebral body and often spreads subligamentously. “Cold” paraspinal abscess collection may develop and spreads along fascial planes, e.g., Psoas abscess. Disc spaces are preserved until v. late and skip areas are noted helping to DDx TB from pyogenic infection. Severe vertebral destruction aka Gibbus deformity may develop (>60-degree sometimes) and may become permanent. Neurologic and many regional complications may develop
Imagingapproach:�CXR with spinal x-rays 1st step that may be unrewarding but may potentially reveal VB destruction w/o disc narrowing. CT scanning is more superior than x-rays. MRI with gad C is a modality of choice
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine