Diagnosing ankylosing spondylitis usually involves multiple tests. When doctors order blood tests to diagnose ankylosing spondylitis, an individual is experiencing worsening symptoms in their back and joints. Often, a blood test diagnosis means the doctor is looking for evidence of anything else that could be causing the symptoms. However, blood tests by themselves cannot definitively diagnose ankylosing spondylitis, but when combined with imaging and assessment, they can provide important clues that point to the answers.
Ankylosing Spondylitis Blood Test Diagnosis
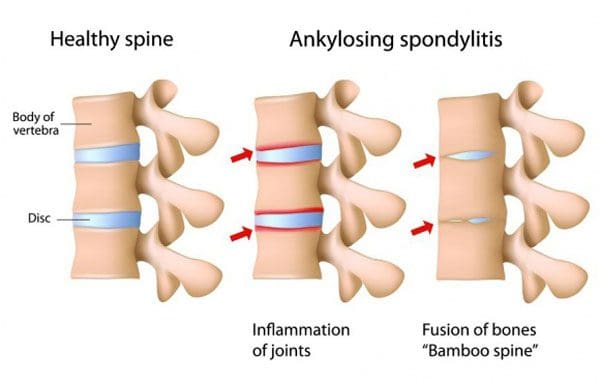
Ankylosing spondylitis is arthritis that primarily affects the spine and hips. It can be difficult to diagnose as no single test can provide thorough information for a definitive diagnosis. A combination of diagnostic tests are utilized, including a physical exam, imaging, and blood tests. Doctors are not only looking for results that will point to ankylosing spondylitis, but they are looking for any results that might point away from the spondylitis results that might provide a different explanation for symptoms.
Physical Exam
The diagnostic process will begin with the individual’s medical history, family history, and physical exam. During the exam, the doctor will ask questions to help rule out other conditions:
How long have symptoms been presenting?
Do symptoms get better with rest or exercise?
Are the symptoms getting worse or staying the same?
Are the symptoms worse at a particular time of day?
The doctor will check for limitations in mobility and palpate tender areas. Many conditions can cause similar symptoms, so the doctor will check to see if the pain or lack of mobility is consistent with ankylosing spondylitis. The feature sign of ankylosing spondylitis is pain and stiffness in the sacroiliac joints. The sacroiliac joints are located in the lower back, where the base of the spine and pelvis meet. The doctor will look at other spinal conditions and symptoms:
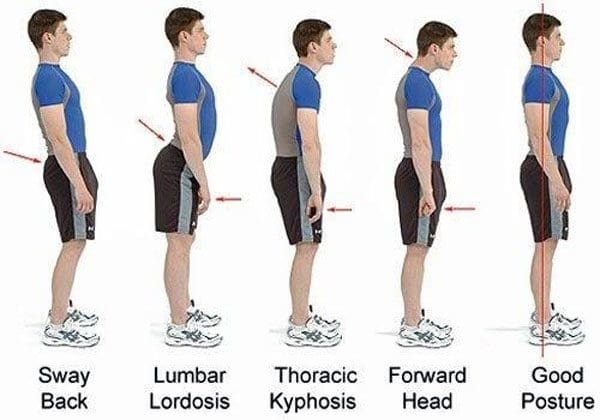
Back pain symptoms caused by – injuries, posture patterns, and/or sleeping positions.
The HLA-B27 gene corresponds with ankylosing spondylitis; if an individual has it, one of their parents has it.
Imaging
X-rays often serve as the first step to a diagnosis.
As the disease progresses, new small bones form between the vertebrae, eventually fusing them.
X-rays work best at mapping the disease progression than the initial diagnosis.
An MRI provides clearer images in the early stages as smaller details are visible.
Blood Tests
Blood tests can help rule out other conditions and check for signs of inflammation, providing supportive evidence along with the results of imaging tests. It typically only takes about a day or two to get the results. The doctor may order one of the following blood tests:
Antinuclear antibodies, or ANA, go after the proteins in the cell’s nucleus, telling the body its cells are the enemy.
This activates an immune response that the body fights to eliminate.
A study determined that ANA is found in 19% of individuals suffering from ankylosing spondylitis and is higher in women than men.
Combined with other tests, the presence of ANA provides another clue to a diagnosis.
Gut Health
The gut microbiome plays an important role in triggering the development of ankylosing spondylitis and its treatment.
Tests to determine the gut’s health can give a doctor a complete picture of what is happening inside the body.
Blood test diagnoses for ankylosing spondylitis and other inflammatory conditions rely heavily on piecing together different tests alongside clinical exams and imaging.
Causes, Symptoms, Diagnosis, and Treatment
References
Cardoneanu, Anca, et al. “Characteristics of the intestinal microbiome in ankylosing spondylitis.” Experimental and therapeutic medicine vol. 22,1 (2021): 676. doi:10.3892/etm.2021.10108
Prohaska, E et al. “Antinukleäre Antikörper bei Spondylitis ankylosans (Morbus Bechterew)” [Antinuclear antibodies in ankylosing spondylitis (author’s transl)]. Wiener klinische Wochenschrift vol. 92,24 (1980): 876-9.
Sheehan, Nicholas J. “The ramifications of HLA-B27.” Journal of the Royal Society of Medicine vol. 97,1 (2004): 10-4. doi:10.1177/014107680409700102
Wenker KJ, Quint JM. Ankylosing Spondylitis. [Updated 2022 Apr 9]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470173/
Xu, Yong-Yue, et al. “Role of the gut microbiome in ankylosing spondylitis: an analysis of studies in the literature.” Discovery medicine vol. 22,123 (2016): 361-370.
Individuals with ankylosing spondylitis have a new treatment option that was previously used for rheumatoid arthritis. It is a medication that belongs to a class known as JAK inhibitors. Ankylosing spondylitis combines joint pain with reduced mobility. Ankylosing spondylitis is different because in severe cases, the bones in the spine can fuse together, literally reducing mobility.
The disease typically begins with pain and stiffness in the back. This is usually after some time of inactivity. Symptoms start before the age of 45 and develop gradually. There is no cure for ankylosing spondylitis but there are treatments that can improve symptoms and put the condition into remission. Ankylosing spondylitis treatment is the most successful when addressed early before irreversible damage to the joints begins.
Janus Kinase Inhibitors
Janus kinase inhibitors have traditionally been used to treat:
Rheumatoid arthritis
Psoriatic arthritis
Ulcerative colitis
The medication works by decreasing the immune system�s activity. Janus kinase inhibitor drugs affect several cellular compounds that are important in the development and progression of ankylosing spondylitis. Currently, there are only three Janus kinase inhibitor medications available in the United States and FDA-approved to treat rheumatoid arthritis:
Xeljanz
Rinvoq
Olumiant
Each of the approved inhibitors targets specific enzymes
Current Ankylosing Spondylitis Treatments
Janus kinase inhibitors are not given to individuals right away. However, it could be an option if first and second-line treatments are not working. Treatments usually consist of:
First-Line Treatments
NSAIDs
Nonsteroidal anti-inflammatory medications are the most commonly used to treat ankylosing inflammation, pain, and stiffness.
Chiropractic
Chiropractic physical therapy is a major part of ankylosing spondylitis treatment keeping the spine flexible and as healthy as possible. A chiropractic/physical therapy team design and develop specific exercises to fit individual needs, which include:
Stretching and Range-of-motion exercises help maintain flexibility in the joints
Sleeping and walking posture adjustment exercises
Abdominal and spinal exercises to maintain a healthy posture
If nonsteroidal anti-inflammatory medications do not relieve symptoms, then biological medications could be prescribed. This class of medications includes:
Tumor necrosis factor blockers work by targeting cell protein that is part of the immune system, known as tumor necrosis alpha. This protein causes inflammation in the body, and the blockers suppress it.
Interleukin 17 Inhibitors
Interleukin 17 in the body’s immune system defends against infection. It uses an inflammatory response to fight infections. The IL-17 inhibitors suppress the inflammatory response and help reduce symptoms.
Other Treatment Options
Lifestyle Adjustments
Following a medical treatment plan is often combined with diet and lifestyle adjustments that are recommended to help with the condition, these include:
Most individuals with ankylosing spondylitis do not require surgery. However, a doctor could recommend surgery if there is joint damage, the hip-joint needs to be replaced, or if the pain is severe.
Inhibitor Potential
Studies are ongoing in the treatment of ankylosing spondylitis. The drug is currently in Phase 3 trials for the treatment of adults. The trial results have shown patients with active ankylosing spondylitis showed improvement in:
Fatigue
Inflammation
Back pain
The study enrolled adults with active ankylosing spondylitis who took at least two NSAIDs that were ineffective at treating symptoms. Most of the participants were men, average age of 41, and no prior usage of biologic disease-modifying antirheumatic drugs.
Janus kinase could become a standard treatment
There is still not enough research to make a prediction, but the data is promising. The inhibitors seem to be a safe option when used in a properly screened, well-matched setting that includes regular monitoring. The inhibitors appear to be effective and have the advantages of being taken orally and working fast.
Body Composition
Osteoarthritis and weight loss
Being obese has shown to be a high-risk factor for the development of osteoarthritis. This is not only from the effects of extra weight on the body’s joints but also as a result of the inflammatory effects of adipose tissue. The lower back, hips, and knees, bear the majority of the body’s weight.
An excess amount of adipose tissue on the body’s midsection and legs has been shown to negatively impact the weight-bearing joints. Promoting Lean Body Mass and encouraging weight loss lowers the risk of osteoarthritis and improves an individual’s quality of life. Exercise is regarded safe for individuals with osteoarthritis and should be incorporated to improve body composition, reduce Body Fat Mass, improve Lean Body Mass and maintain a healthy weight.
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Hammitzsch A, Lorenz G, Moog P. Impact of Janus Kinase Inhibition on the Treatment of Axial Spondyloarthropathies. Frontiers in Immunology 11:2488, Oct 2020; doi 10.3389/fimmu.2020.591176.�https://www.frontiersin.org/article/10.3389/fimmu.2020.591176, accessed Jan 21, 2021.
van der Heijde D, Baraliakos X, Gensler LS, et al. Efficacy and safety of filgotinib, a selective Janus kinase 1 inhibitor, in patients with active ankylosing spondylitis (TORTUGA): results from a randomized, placebo-controlled, phase 2 trial.�Lancet.�2018 Dec 1;392(10162):2378-2387. doi: 10.1016/S0140-6736(18)32463-2. Epub 2018 Oct 22. PMID: 30360970.�https://pubmed.ncbi.nlm.nih.gov/30360970/�accessed Jan 19, 2021.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine