Approximately 5 million people in the United States have been diagnosed with Alzheimer’s disease (AD), one of the most common types of dementia, worldwide. A variety of factors can increase the risk of developing other types of dementia and AD, including poor diet and lifestyle habits. Research studies have also shown that treating the body as a whole may help prevent and, in several cases, even reverse cognitive decline. The goal is to start treatment immediately. In the following article, we will ultimately discuss how a functional medicine approach can help improve AD and other types of dementia.
Dementia and Alzheimer�s Disease Overview
Our brain is a complex organ made-up of about 100 billion neurons that are constantly communicating with each other. Also known as brain cells or nerve cells, neurons play a fundamental role in our cognitive function, including memory, thinking, and learning. Neurons are constantly repairing themselves, especially during sleep, but when brain cells or nerve cells can’t repair themselves, due to a variety of factors, it can ultimately affect cognition. Alzheimer’s disease is associated with a build-up of compounds, such as active microglial cells, tau proteins, and beta-amyloid plaques, among several others.
Because the body can’t break down these compounds, they can start to block the synapses where brain cells or nerve cells communicate with each other. This is believed to be one of the most common causes of AD and other types of dementia. Dr. Dale Bredesen, a renowned expert and neurologist, developed a breakthrough, alternative treatment option for dementia and AD that focuses on reducing glial cells, protein, and plaque build-up in the brain. According to Dr. Bredesen’s research studies, a build-up of these compounds can occur due to toxins, infections, inflammatory biomarkers, and genetics.
Bredesen RECODE Protocol� for Dementia and AD
A variety of factors can increase the risk of developing other types of dementia and Alzheimer’s disease because these can affect the neuron’s ability to repair themselves, ultimately causing brain cell or nerve cell death. As previously mentioned above, they may also cause an excessive build-up of compounds, including microglial cells, tau protein, and beta-amyloid plaque in the brain. Cognitive decline plays a critical role in changing the way the brain creates synapses and preserves memory. Fortunately, a functional medicine approach can help improve Alzheimer’s disease and other types of dementia.
Dr. Bredesen’s RECODE Protocol� is an alternative treatment option that can help prevent and, in several cases, even reverse cognitive decline in people with other types of dementia and Alzheimer’s disease. According to the research studies, Dr. Bredesen’s RECODE Protocol� returned many participants to pre-diagnosis levels of cognition. In other participants, the volume of the hippocampus, the main region of the brain which shrinks in AD and dementia, returned to normal on MRI. By following diet and lifestyle modifications with the RECODE Protocol�, the research study participants recovered their quality of life.
Dr. Bredesen�s RECODE Protocol � is an organized, multifactorial approach which shows that prevention and reversal of cognitive decline are possible by:
Addressing several underlying sources simultaneously
Optimizing essential lifestyle factors like diet, exercise, and sleep
Designing treatment based on each patient’s personal needs
Dr. Bredesen�s RECODE Protocol � follows a functional medicine treatment approach for AD and other types of dementia. Healthcare practitioners trained through the Institute for Functional Medicine (IFM) are seeing positive results in people with dementia and Alzheimer�s disease. IFM healthcare practitioners use functional medicine treatment approaches to identify and address the underlying source of a variety of health issues. IFM healthcare practitioners may be properly suited to apply, and even expand, Dr. Bredesen�s RECODE Protocol � for AD and other types of dementia, among other health issues.
Furthermore, several diet and lifestyle modifications may ultimately help prevent and, in several cases, even reverse dementia and AD, including:
Eating a whole-food low glycemic diet, made-up of predominately plant-based foods with 10-15 servings of non-starchy vegetables per day. Moreover, eat lean proteins, such as legumes and cold-water, low-mercury fish. Eat healthy fats, such as nuts, seeds, and olive oil.
Getting plenty of sleep. When you sleep at night, your body can also heal damaged cells and ultimately boost your immune system.
Getting plenty of exercise and physical activity boosts your metabolism, improves mood, promotes better sleep and much more.
Limiting exposure to toxins. Toxins, such as heavy metals, chemicals, mycotoxins, and even some medications, can cause cognitive decline.
Avoiding stress. Chronic stress can cause hormonal and neurotransmitter changes in the body, causing brain degeneration and atrophy.
Avoiding alcohol. Alcohol is a toxin that affects the liver�s ability to metabolize toxins and it is also commonly associated with brain atrophy.
Approximately 5 million people in the United States have been diagnosed with Alzheimer’s disease (AD), one of the most common types of dementia, worldwide. A variety of factors can increase the risk of developing other types of dementia and AD, including poor diet and lifestyle habits. Research studies have also shown that treating the body as a whole may help prevent and, in several cases, even reverse cognitive decline. The goal is to start treatment immediately. In the following article, we will ultimately discuss how a functional medicine approach can help improve AD and other types of dementia. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Approximately 5 million people in the United States have been diagnosed with Alzheimer’s disease (AD) or one of the most common types of dementia. According to researchers, a variety of factors can ultimately increase the risk of developing AD and other types of dementia, including poor diet and lifestyle habits. Research studies demonstrated that treating the body as a whole may prevent and, in several cases, even reverse cognitive decline. The goal is to start treatment early. In the article above, we discussed how a functional medicine approach can help with dementia and Alzheimer’s disease (AD).
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.�
Curated by Dr. Alex Jimenez
References:
Parke, Emily. �The Functional Medicine Approach to Cognitive Decline.� Dr. Emily Parke – Arizona Wellness Medicine, LLC, 6 Dec. 2018, www.dremilyparke.com/2018/12/06/functional-medicine-cognitive-decline/.
Litwin, Ken A., et al. �The Bredesen Protocol� & Functional Medicine � A Powerful Combination to Prevent & Treat Cognitive Decline.� Kara Fitzgerald ND Naturopathic Doctor, 29 Mar. 2019, www.drkarafitzgerald.com/2018/06/20/the-bredesen-protocol-functional-medicine-a-powerful-combination-to-prevent-treat-cognitive-decline/.
Carpathia Collaborative Staff. �Preventing and Reversing Cognitive Decline.� Carpathia Collaborative, 29 July 2019, carpathiacollaborative.com/blogposts/cognitivedecline.
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention.
Food Sensitivity for the IgG & IgA Immune Response
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with a variety of food sensitivities and intolerances. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs.
Gut Zoomer for Small Intestinal Bacterial Overgrowth (SIBO)
Dr. Alex Jimenez utilizes a series of tests to help evaluate gut health associated with small intestinal bacterial overgrowth (SIBO). The Vibrant Gut ZoomerTM offers a report that includes dietary recommendations and other natural supplementation like prebiotics, probiotics, and polyphenols. The gut microbiome is mainly found in the large intestine and it has more than 1000 species of bacteria that play a fundamental role in the human body, from shaping the immune system and affecting the metabolism of nutrients to strengthening the intestinal mucosal barrier (gut-barrier). It is essential to understand how the number of bacteria that symbiotically live in the human gastrointestinal (GI) tract influences gut health because imbalances in the gut microbiome may ultimately lead to gastrointestinal (GI) tract symptoms, skin conditions, autoimmune disorders, immune system imbalances, and multiple inflammatory disorders.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download
* All of the above XYMOGEN policies remain strictly in force.
Modern Integrated Medicine
The National University of Health Sciences is an institution that offers a variety of rewarding professions to attendees. Students can practice their passion for helping other people achieve overall health and wellness through the institution’s mission. The National University of Health Sciences prepares students to become leaders in the forefront of modern integrated medicine, including chiropractic care. Students have an opportunity to gain unparalleled experience at the National University of Health Sciences to help restore the natural integrity of the patient and define the future of modern integrated medicine.
How often do you have a hard time remembering your appointments? Has it become harder for you to learn new things? How often do you feel you have something that must be done? Or even, how often do you feel more susceptible to pain?�Research studies have demonstrated that brain fog may be associated with Alzheimer’s disease. In the following article, we will discuss how midlife systemic inflammatory markers have ultimately been associated with late-life brain volume. �
Midlife Systemic Inflammatory Markers are Associated with Late-life Brain Volume
Abstract
Objective: To clarify the temporal relationship between systemic inflammation and neurodegeneration, we examined whether a higher level of circulating inflammatory markers during midlife was associated with smaller brain volumes in late-life using a large biracial prospective cohort study.
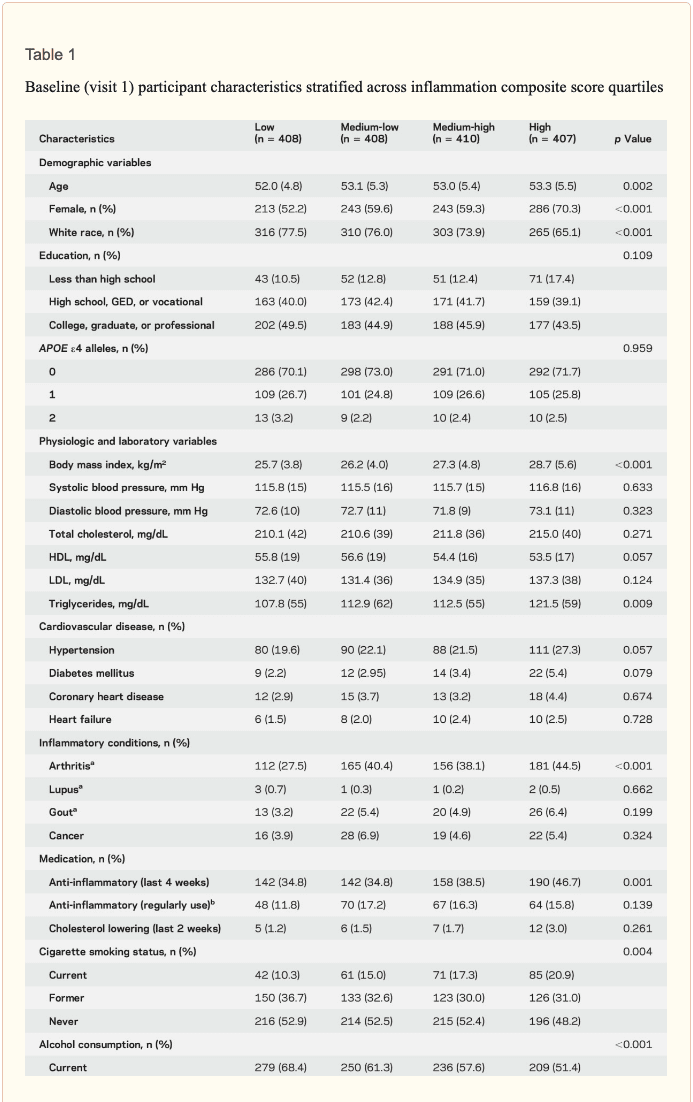
Methods: Plasma levels of systemic inflammatory markers (fibrinogen, albumin, white blood cell count, von Willebrand factor, and Factor VIII) were assessed at baseline in 1,633 participants (mean age 53 [5] years, 60% female, 27% African American) enrolled in the Atherosclerosis Risk in Communities Study. Using all 5 inflammatory markers, an inflammation composite score was created for each participant. We assessed episodic memory and regional brain volumes, using 3T MRI, 24 years later.
Results: Each SD increase in midlife inflammation composite score was associated with 1,788 mm3 greater ventricular (p = 0.013), 110 mm3 smaller hippocampal (p = 0.013), 519 mm3 smaller occipital (p = 0.009), and 532 mm3 smaller Alzheimer disease signature region (p = 0.008) volumes, and reduced episodic memory (p = 0.046) 24 years later. Compared to participants with no elevated (4th quartile) midlife inflammatory markers, participants with elevations in 3 or more markers had, on average, 5% smaller hippocampal and Alzheimer disease signature region volumes. The association between midlife inflammation and late-life brain volume was modified by age and race, whereby younger participants and white participants with higher levels of systemic inflammation during midlife were more likely to show reduced brain volumes subsequently.
Conclusions: Our prospective findings provide evidence for what may be an early contributory role of systemic inflammation in neurodegeneration and cognitive aging.
Introduction
� Although elevated levels of inflammatory markers have been found in the blood,1 CSF,2 and brain parenchyma3 of individuals with cognitive impairment and Alzheimer disease (AD), it remains unclear whether this heightened inflammatory state is driving neurodegenerative changes. If low-grade systemic inflammation does play a causal role in AD and other neurodegenerative diseases, a heightened inflammatory response during midlife would be expected to increase one’s risk for pathologic brain changes much later. Although cross-sectional studies have demonstrated a link between elevated inflammatory markers and reduced brain volume in older adults,4,�7 it remains unclear whether systemic inflammation during midlife, before the onset of significant age- and disease-related neurologic changes, is associated with brain volume loss later in life. � The goal of the current study was to examine how midlife plasma markers of inflammation relate to late-life brain volume among a biracial community sample of older adults. To this end, we examined the relationship between 5 markers of systemic inflammation measured during midlife and MRI measures of regional brain volume 24 years later in the Atherosclerosis Risk in Communities (ARIC) Study cohort. We tested the hypothesis that greater midlife systemic inflammation is associated with smaller brain volumes in regions most susceptible to AD-related atrophy and reduced episodic memory in older adulthood. Based on cross-sectional evidence suggesting that race, sex, and age may modify the association between inflammatory markers and brain volume,5,8,9 the current study also examined the modifying effects of each of these demographic characteristics. �
Methods
� Study population. The ARIC study, an ongoing community-based prospective study, enrolled 15,792 middle-aged adults (45�65 years of age at baseline).10 Participants were selected by probability sampling in 4 US communities: Washington County, Maryland; Forsyth County, North Carolina; northwestern suburbs of Minneapolis, Minnesota; and Jackson, Mississippi. Following the baseline visit in 1987�1989 (visit 1), participants were seen at 3 more visits, approximately 3 years apart until 1996�1998 (visit 4), and at the fifth visit in 2011�2013 (visit 5). � At visit 5, a subset of 1,978 participants was selected to undergo brain MRI scans.11 Participants were selected to undergo a brain MRI based on previous participation in the ARIC Brain MRI Ancillary Study and standard safety exclusion criteria. In addition, all participants with evidence of cognitive impairment at visit 5 and an age-stratified random sample of participants without evidence of cognitive impairment were recruited. The participation rate among eligible individuals selected to undergo brain MRI was approximately 81%. A detailed description of the MRI sampling strategy is provided in the e-Methods at Neurology.org. We excluded participants with poor imaging quality (n = 6), neurologic disease (i.e., stroke, multiple sclerosis) (n = 80), missing inflammatory biomarker data (n = 38), missing covariates (n = 215), and race other than white or African American (n = 6). Participants who met criteria for dementia (5%, n = 83) were excluded from the primary analyses. � Standard protocol approvals, registrations, and patient consents. The ARIC study protocol has been approved by the institutional review boards at each participating center. All participants gave written informed consent at each study visit. � Inflammatory markers. Plasma levels of 4 acute-phase reactants�fibrinogen, albumin, von Willebrand factor (VWF), and Factor VIII (FVIII)�and white blood cell (WBC) count were used to measure systemic inflammation.12 Using standard protocols, study technicians drew fasting blood, centrifuged samples, and froze plasma blood samples at ?70�C until the samples were analyzed.13 Fibrinogen (mg/dL), albumin (g/dL), VWF (% of standard), and FVIII activity (% of standard) measured at visit 1 were analyzed in an ARIC research laboratory in accordance with a standardized protocol.13,14 WBC count was determined from whole anticoagulated blood using an automated particle Coulter Counter within 24 hours of venipuncture. Repeated testing revealed interassay coefficients of variation below 8% for fibrinogen, albumin, FVIII, and WBC, and 17%�19% for VWF.15,16 � Brain MRI. MRI scans were conducted using a 3T MRI scanner.11 Magnetization-prepared rapid gradient echo (MPRAGE), axial T2* gradient recalled echo, axial T2 fluid-attenuated inversion recovery, and axial diffusion tensor imaging sequences were obtained. Freesurfer (surfer.nmr.mgh.harvard.edu) was used to measure brain volume from MPRAGE sequences.17 Total brain and ventricular volume, lobar volume (frontal, temporal, parietal, occipital), AD signature region volume (i.e., the combined volume of the parahippocampal, entorhinal, inferior parietal lobules, hippocampus, and precuneus),18 hippocampal volume, and total intracranial volume were evaluated for the current study. � Episodic memory. Episodic memory was assessed at visit 5, concurrent with the brain MRI, using the delayed word recall test (DWR). DWR is a test that requires participants to learn and recall a list of 10 words following a delay period.19 Participants were scored based on the total number of words correctly recalled. � Covariates. Race, sex, years of education attained (less than high school, high school/General Equivalency Development/vocational school, or any college), cigarette smoking status (current/former/never), average weekly alcohol consumption (grams), and previous cancer diagnosis were self-reported. A random zero sphygmomanometer was used to calculate sitting diastolic and systolic blood pressure. Second and third blood pressure measurements were averaged for the current analyses. Hypertension was defined as systolic blood pressure >140 mm Hg, diastolic blood pressure >90 mm Hg or use of hypertensive medication. Body mass index was calculated using recorded height and weight (kg/m2). Coronary heart disease was defined as self-reported coronary bypass, balloon angioplasty, angioplasty of one or more coronary artery, or myocardial infarction. Medications used in the previous 2 weeks were recorded. The presence of chronic inflammatory conditions (e.g., arthritis, lupus, gout) was assessed by patient self-report of physician diagnosis at visit 4. History of regular anti-inflammatory medication use (e.g., nonsteroidal anti-inflammatory drug, arthritis medication) was assessed at visit 5. All other variables were assessed at visit 1. Dementia diagnosis was adjudicated at visit 5 by an expert committee using cognitive, imaging, and functional data.20 � Total cholesterol and triglycerides were measured using enzymatic methods,21,22 and low-density lipoprotein using the Friedewald equation.23 Serum glucose was measured using the hexokinase method. Diabetes was defined as a fasting glucose ?126 mg/dL or a nonfasting glucose ?200 mg/dL, current use of diabetes medication or insulin, or participant report of physician-diagnosed diabetes. APOE genotype (0, 1, or 2 ?4 alleles) was assessed using the TaqMan assay (Applied Biosystems, Foster City, CA). � Statistical analysis. We examined systemic inflammation as both a continuous and categorical exposure measure. A continuous inflammation composite Z score was created using the 5 inflammatory markers. WBC count was log-transformed to correct for skewness. Each inflammatory biomarker was converted to a standardized Z score such that the group mean was zero with an SD of 1. The mean of the 5 Z scores was calculated to generate an inflammation composite Z score. Because albumin decreases in response to inflammation, albumin values were multiplied by ?1 before being included in the composite Z score. With few exceptions, the intercorrelations between inflammatory markers were within an optimal range, between 0.2 and 0.4; composite score item�test correlations, principal component factor loadings, and Cronbach ? (0.61) were satisfactory for our purposes (table e-1). For each participant, we also created a categorical measure of systemic inflammation by computing the number of inflammatory marker Z scores in the highest quartile (?75%tile) and trichotomizing this number (0, 1�2, or 3�5). � Participant characteristics were compared using an analysis of variance or ?2 tests. Multivariable linear regression was used to assess the association between continuous and categorical inflammation variables and measures of brain volume and episodic memory. Brain volume analyses were adjusted for total intracranial volume, and all analyses included the covariates described in the previous section. Interaction terms or stratification were used to evaluate the modifying effects of age, race, and sex. � Sensitivity analyses were performed excluding participants who reported regular anti-inflammatory medication use during follow-up and including participants who met criteria for dementia. For all analyses, sampling weights were incorporated to account for the ARIC brain MRI sampling strategy. Thus, all results represent estimates for the entire ARIC visit 5 study population. Because the associations between inflammation markers and specific regions of interest (ROIs) are correlated, we did not adjust for multiple comparisons. A 2-sided p-value <0.05 designated statistical significance. All analyses were conducted using Stata Version 14 (StataCorp, College Station, TX). �
Results
� Study population characteristics. A total of 1,633 participants (baseline mean age 52.8 [5.3] years, 27% African American, 60% women, 46% college or professional degree) were included in the study sample. The time between baseline assessment and follow-up MRI scan was 24 (1) years; the average age at follow-up was 76.5 (5.4) years. As shown in table 1, a higher inflammation composite score at baseline was associated with older age, female sex, African American race, and increased levels of a number of cardiovascular risk factors. � Inflammatory markers and brain volume. Each SD increase in inflammation composite score at baseline was associated with a 532 mm3 smaller AD signature region volume (95% confidence interval [CI] ?922 to ?141), a 519 mm3 smaller occipital lobe volume (CI ?906 to ?132), a 110 mm3 smaller hippocampal volume (CI ?196 to ?24), and a 1,788 mm3 larger ventricular volume (CI 371 to 3,205) at follow-up (table 2). We found the estimated effect of a 1 SD increase in inflammation composite score during midlife on occipital lobe, ventricular, and hippocampal volume to be similar to the effect associated with possession of a single APOE ?4 allele in our multivariable regression analyses. No association was found for the total brain, frontal lobe, temporal lobe, or parietal lobe volume (ps > 0.071). Our findings did not change meaningfully after excluding participants who regularly used anti-inflammatory medication during the follow-up period (table e-2) and after including participants who met the criteria for dementia at visit 5 (table e-3). For descriptive purposes, associations between individual inflammatory markers and AD signature region volume are provided in a table e-4. � An assessment of linear trend revealed that compared to individuals with 0 elevated (?75th %tile) inflammatory biomarkers at baseline (reference), those with 1�2 and 3�5 elevated biomarkers had lower AD signature region (p trend = 0.001), occipital lobe (p trend = 0.007), and hippocampal volume (p trend = 0.041) 24 years later (figure 1). Compared to the reference group, participants with 3 or more elevated markers demonstrated 5.3% smaller AD signature region volumes, 5.7% smaller occipital lobe volumes, and 4.6% smaller hippocampal volumes, on average. However, this pattern was not statistically supported for the total brain, ventricular, frontal lobe, temporal lobe, and parietal lobe volume (p trends >0.072). The modifying effects of age, race, and sex. A significant age-by-inflammation composite score interaction was found for the AD signature region, occipital lobe, and hippocampal volume (table 2). Because a reversal of association was observed at age 60 (figures 2, e-1, and e-2), we stratified the sample into young-midlife and old-midlife subgroups (<60/? 60). As displayed in table 2, the associations between higher midlife inflammation composite score and lower AD signature region, occipital lobe, and hippocampal volume at follow-up were significantly stronger among participants who were 60 or younger at baseline compared to those who were older than 60. A marginal race-by-inflammation composite score interaction was found for occipital lobe volume, whereby a higher midlife inflammation composite score was associated with lower occipital lobe volume among white, but not African American, participants (table 3). No interactions with sex were found (table e-5). � Inflammatory markers and episodic memory. Late-life episodic memory, which was associated with hippocampal and AD signature region volume after controlling for age (partial rs > 0.21, ps < 0.001), was reduced among participants with higher levels of the inflammation composite score. Each SD increase in inflammation composite score was associated with a ?0.08 SD performance decrement on the DWR after adjusting for covariates (CI ?0.15 to 0.00; p = 0.046). Similarly, a higher number of elevated inflammatory biomarkers at baseline was associated with reduced DWR performance (p trend = 0.009; figure 1). �
Discussion
� Using a large community sample, we demonstrated that a higher level of systemic inflammatory markers measured during midlife is independently associated with lower regional brain volume and reduced episodic memory 24 years later among older adults without dementia. Similarly, participants who had elevations in a larger number of 5 inflammatory markers during midlife were found to have lower regional brain volumes and reduced episodic memory in late-life in a dose-response manner. For several brain regions, including the hippocampus, the effect of a 1 SD increase in midlife inflammation composite score was comparable to that of possessing a single APOE ?4 allele during late life. Whereas age and race were found to modestly modify the relationship between midlife inflammation and late-life regional brain volume, the previously reported modifying effect of sex was supported. � Although cross-sectional evidence from the Framingham5 study and several other population-based8,9 studies suggests an association between brain volume and inflammation in older adults, the temporal relationship between inflammation and brain volume loss is still not well-understood. As a result, whether heightened systemic inflammation constitutes a potential cause or consequence of neurodegeneration and brain atrophy remains unclear. Because the pathophysiologic processes driving neurodegeneration and brain volume loss begin decades before the onset of frank cognitive decline,24 it is essential to determine how biological processes that take place during middle adulthood relate to neurologic outcomes later in life. By demonstrating that an elevation in plasma inflammatory markers during midlife is independently associated with smaller regional brain volumes, larger ventricular volume, and reduced episodic memory in late life, the current findings provide support for a potential causal, rather than associative, role of systemic inflammation in late-life neurodegeneration (i.e., atrophy) and resulting cognitive decline. The current findings align closely with those from the neurocardiovascular literature, which have found associations between midlife blood pressure,25 cholesterol,26 and diabetes27 and adverse neurologic and cognitive outcomes in older adulthood. The contributing role of systemic inflammation to subsequent neurodegenerative processes has been demonstrated previously by animal studies,28 but had not yet been supported by a large prospective MRI study. � The current results suggest that several demographic factors modify the relationship between midlife inflammation and late-life brain volume. Younger individuals with elevated levels of inflammation (particularly participants in their 40s) were more likely to display lower brain volumes decades later, supporting the idea that elevated systemic inflammation earlier in life may make individuals especially vulnerable to neurodegenerative brain changes as they age. Although we expected stronger effects would emerge within the African American group, given the greater burden of systemic disease29 and dementia,30 the associations between inflammation and brain volume were generally weaker among African Americans. A previous study that examined the moderating effects of race found similar results in a cross-sectional analysis of older adults without dementia.8 � Circulating levels of acute-phase reactants, such as those used in the current study, change in parallel with an inflammatory response as a result of signaling from inflammatory cytokines such as interleukin-6 and tumor necrosis factor-?.12 Cytokines in the periphery have the potential to induce a pro-inflammatory neurotoxic state within the CNS through multiple routes, including activation of endothelial cells of the blood-brain barrier,31 activation of macrophage in circumventricular organs,32 and signaling of the afferent vagus nerve.33 In addition to providing support for a pathogenic role of systemic inflammation in neurodegenerative disease, the present findings indicate that elevations in commonly assayed inflammatory proteins may serve as markers of risk for future neurodegenerative changes and cognitive decline. Although we did not examine all brain regions in our analysis, our assessment of 7 representative ROIs suggests that brain regions vulnerable to atrophy, amyloid deposition, and metabolic abnormalities in the earliest phases of AD may be more vulnerable to volume loss associated with heightened midlife inflammation. This pattern of neuroanatomic specificity has been supported by previous cross-sectional studies of older adults without dementia.4,7,�9,34 � In the context of the current findings, several alternative explanations should be considered. First, it remains possible that elevated systemic inflammation may simply serve as a marker of another pathologic process linked to neurodegeneration (e.g., oxidative stress). Second, it is possible that the biological processes causing brain atrophy to trigger a protective neuroimmune response, which increases peripheral inflammation. Third, the associations found here may be an effect of residual or unmeasured confounding. Despite these caveats, the contributory role of systemic inflammation has been supported by a sizable body of literature implicating peripheral inflammatory signaling in neurodegenerative processes such as neural apoptosis,35 ?-amyloid formation,36 and neuronal tau phosphorylation.37 � Strengths of the current study include the prospective study design, length of follow-up, detailed assessment of potentially confounding variables, large sample size, and the inclusion of a large African American sample. However, the current findings should be interpreted within the context of several limitations. Although the acute-phase reactants used in the present study represent components of the innate immune system, several of these proteins are implicated in another closely related physiologic process, such as hemostasis, which may also influence brain volume. Evaluating inflammatory biomarkers that have greater biological specificity in future prospective studies will allow for stronger inferences about the contributing role of systemic inflammation. Interpretation of the current findings is also limited by the measurement of inflammatory markers at a single time point, as it is unclear whether a single measurement can adequately capture inflammation chronicity. The relatively high interassay variability of VWF also increases the likelihood of exposure misclassification; however, this possibility is mitigated by the use of the inflammation composite score. We found that participants who dropped out and participants who died before visit 5 had significantly higher levels of midlife inflammation, were older, had greater levels of medical comorbidity at baseline, and were more likely to be African American38 (table e-6). As a result, selective attrition may have biased results in the direction of the null hypothesis, particularly for African American and older participants. Finally, our interpretation of the contributory role of inflammation in neurodegeneration rests on the assumption that brain volume loss occurred after inflammatory markers were assessed. Although evidence suggests that this is likely the case (brain volume loss accelerates after age 60 years39), this cannot be confirmed without the assessment of change over time. � Despite these limitations, the current study provides insights into the connection between midlife systemic inflammation and late-life brain volume loss. These findings provide support for inflammation’s early pathogenic role in the development of neurodegenerative brain changes associated with late-life cognitive decline, AD, and other forms of dementia. �
Is inflammation the final trip wire for Alzheimer’s disease?� Research studies have demonstrated that neuroinflammation is considered to be the main epigenetic trip wire for the genetic predisposition of Alzheimer’s disease or AD. Moreover, patients with inflammation can also develop a variety of symptoms, including brain fog which can make thinking, understanding, and remembering basic information challenging. Neuroinflammation can cause brain fog and other other well-known health issues, including Alzheimer’s disease and other neurological diseases. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Neurotransmitter Assessment Form
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. Symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
� In honor of Governor Abbott’s proclamation, October is Chiropractic Health Month. Learn more about the proposal. � Have you been experiencing noticeable variations in your mental speed? Do you suffer from pain, discomfort, and inflammation? Have you been experiencing fatigue, especially after meals or exposure to chemicals, scents, or pollutants?�Brain fog can cause a variety of symptoms, including memory and concentration as well as vision problems. According to the research study above, midlife inflammation and brain fog may be associated with Alzheimer’s disease. � The following article has been referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
� Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
� Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
�
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
� For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
The most common causes of TBI which result in ER visits include slip-and-fall accidents, blows to the head, and automobile accidents. Abrupt forces which jolt the brain violently within the skull, such as shock waves from explosions, which can also cause TBI. Traumatic brain injury can also result from bullet wounds or other injuries which penetrate the skull and brain. �
Doctors characterize traumatic brain injury as mild, moderate, or severe depending on whether the injury causes unconsciousness, how long it lasts, and other symptoms. Although most traumatic brain injuries are characterized as mild because they’re not considered life-threatening, even a mild TBI can have serious and long-lasting effects if left untreated. � Resulting from an impact to the head which interrupts brain function, TBI is a threat to cognitive health in two ways: �
The effects of traumatic brain injury, which may be long-lasting or even permanent, can include unconsciousness, inability to recall the event, confusion, difficulty learning new information, trouble speaking, unsteadiness, lack of coordination, and health issues associated with vision or hearing, among other common symptoms.
TBI may increase the risk of developing Alzheimer’s disease or dementia, years after the injury takes place.
According to the Centers for Disease Control and Prevention (CDC), approximately 2.8 million TBI-associated ER visits, hospitalizations, and deaths occurred in 2013, the latest year for which information is available. The purpose of the following article is to discuss traumatic brain injury (TBI) and its connection with Alzheimer’s disease and other health issues. �
Traumatic Brain Injury Causes
Slip-and-fall accidents are the most common cause of traumatic brain injury, where falls pose a potentially serious risk factor for older adults. According to a CDC special report evaluating data from several federal agencies, approximately 56,000 seniors are hospitalized every year as a result of head injuries sustained in falls. A serious TBI from a slip-and-fall accident may ultimately result in long-term cognitive changes and reduced ability to function as well as overall mood changes. �
About 775,000 older adults have traumatic brain injury-related disability. Measures to reduce the risk of falls include: �
Using a walker or other assistive device to compensate for mobility problems, muscle weakness or poor balance.
Having your vision checked regularly and using glasses or contact lenses that correct for changes.
Working with your doctor to watch for medication side effects or interactions among drugs you�re taking.
Avoiding household hazards, such as clutter, loose rugs or poor lighting.
Automobile accidents are another common cause of traumatic brain injury (TBI). People can reduce the risk of being involved in an auto accident by keeping their vehicle in good condition, following the rules of the road, and buckling their seat belt. Wearing a helmet and when biking, inline skating, or playing contact sports can also help protect the head from TBI. �
TBI Symptoms
The severity of symptoms for traumatic brain injuries largely depends on whether the injury is mild, moderate, or severe. Mild traumatic brain injury (TBI), also known as a concussion, can either not cause unconsciousness or can cause unconsciousness which lasts for 30 minutes or less. Mild traumatic brain injury (TBI) symptoms may include: �
Inability to remember the traumatic event immediately before or up to 24 hours after
Confusion and disorientation
Difficulty learning new information
Headache
Dizziness
Blurry vision
Nausea and vomiting
Ringing in the ears
Trouble speaking coherently
Mood changes or changes in sleeping patterns
These symptoms will commonly manifest at the time of the TBI or soon after, however, these may sometimes not develop till several days or even weeks following the traumatic event. Mild TBI symptoms are generally temporary and these will clear up within hours, days, or weeks following the traumatic even, however, they can occasionally last several months or longer. �
Moderate traumatic brain injury can cause unconsciousness which lasts more than 30 minutes but less than 24 hours and severe traumatic brain injury can cause unconsciousness for more than 24 hours. Symptoms of moderate and severe traumatic brain injury are similar to those of mild traumatic brain injury but these are more serious and longer-lasting. �
In all types of TBI, cognitive changes are the most common symptoms. The ability to learn and remember new information is also frequently affected. Other commonly affected cognitive skills include the ability to pay attention, organize thoughts, plan effective strategies for completing tasks and activities, and/or make sound judgments. More severe changes in cognitive skills may develop years after the traumatic event where the person may appear to have recovered from the previous TBI. �
TBI Diagnosis
Evaluations performed by healthcare professionals to help diagnose traumatic brain injury (TBI) generally include: �
Questions about the traumatic event
Analysis of the person’s level of consciousness and confusion
Neurological tests to analyze memory and thinking, vision, hearing, touch, balance, and reflexes
Let your doctor know if you are taking any drugs and/or medications, especially blood thinners, because they can increase the chance of complications. Also, inform your healthcare professional if you drink alcohol or take illicit drugs. �
Depending on the cause of the TBI and the severity of symptoms, brain imaging with computed tomography (CT) may be necessary to determine if there�s swelling or bleeding in the brain. If you experience a traumatic brain injury, it should be noted in your permanent medical record and mentioned whenever familiarizing a new doctor with your medical history. �
Traumatic Brain Injury Treatment
The most serious traumatic brain injuries commonly require specialized hospital care and can also need several months of rehabilitation. Most traumatic brain injuries are mild and can be treated with either a short hospital stay for observation or at-home monitoring followed by outpatient rehabilitation, if necessary. Treatment of dementia in a person with a history of traumatic brain injuries varies depending on the type of dementia diagnosed. Treatment strategies for Alzheimer’s disease or another type of dementia are ultimately the same for people with and without a history of traumatic brain injury. �
Alzheimer’s disease and other types of dementia which may occur as a long-term result of traumatic brain injury (TBI) are progressive health issues which worsen over time. As with all types of dementia, they can affect a person’s quality of life, shorten lifespan, and complicate the effort to manage other health issues effectively. However, because other types of dementia, such as CTE, are considerably new for researchers and healthcare professionals, clinical guidelines for diagnosis and treatment do not exist. Several research studies are underway to gain further insight into the patterns of TBI and Alzheimer’s disease which may be implicated in CTE and to develop strategies for prevention, diagnosis, and treatment. �
As previously mentioned in the article above, Alzheimer�s disease and other types of dementia which may occur as a long-term result of traumatic brain injury (TBI) are progressive health issues which may ultimately worsen over time. As with all types of dementia, these can affect quality of life, shorten life span, and complicate the effort to manage other health issues effectively. It’s essential for patients and healthcare professionals to diagnose and treat a traumatic brain injury to prevent further health issues in the future, including Alzheimer’s disease and dementia. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
According to research studies, TBI is ultimately associated with Alzheimer�s disease and other types of dementia. Doctors commonly characterize traumatic brain injury as mild, moderate, or severe depending on whether the previous traumatic event causes unconsciousness, how long it lasts, and other well-known symptoms. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
Alzheimer�s disease (AD) is one of the most common types of dementia among older adults. Research studies have demonstrated that pathological changes in the human brain, whether directly or indirectly, can ultimately cause loss of synaptic function, mitochondrial damage, microglial cell activation, and neuronal cell death. However, the pathogenesis of AD is not yet fully understood and there is currently no definitive treatment for the neurological disease. Research studies have demonstrated that the activation and priming of microglial cells may contribute to the pathogenesis of AD. �
A proinflammatory status of the central nervous system (CNS) can also cause changes in the function of the microglial cells or microglia. Neuroinflammation is closely associated with the activation of microglia and astrocytes which are connected to a variety of neurological diseases by the synthesis and secretion of inflammatory mediators such as iNOS, ROS, and proinflammatory cytokines. According to research studies, microglial priming is also caused by the inflammation of the CNS. �
Therefore, whether microglial priming is the result or the cause of neuroinflammation is still controversial. Microglial cell activation commonly causes an increase of A? and tau proteins as well as a decrease of neurotrophic factors, ultimately leading to the loss of healthy brain cells or neurons and the development of neuritic plaques and neurofibrillary tangles which are closely associated with AD. With the progression of Alzheimer’s disease, changes from neuronal dysfunctions which may have no obvious symptoms to memory loss and cognitive impairment may become more noticeable. �
Microglial Priming, Neuroinflammation, and AD
Although the accurate and detailed, fundamental role of the microglial cells continues to be discovered and explained, there is a consensus among many researchers that primed microglia are associated with the inflammatory response of the CNS in AD. It has also been determined that neuroinflammation caused by microglial priming is mainly associated with aging, systemic inflammation, gene regulation, and blood-brain barrier impairment. The purpose of the article below is to discuss how microglial priming and neuroinflammation in Alzheimer’s disease can be caused due to a variety of risk factors. �
Aging
Aging is considered to be one of the main risk factors for AD and it is generally followed by chronic, systemic up-regulation of pro-inflammatory factors and a considerable decrease in an anti-inflammatory response. This change from homeostasis to an inflammatory state occurs through age-related elements which cause an imbalance between anti-inflammatory and pro-inflammatory systems. Microglia is primed into an activated state which can increase the consistent neuroinflammation and inflammatory reactivity in the aged human brain. Research studies have demonstrated that microglia in the brain of rodents developed an activated phenotype during aging characterized by the increased expression of CD11b, CD11c, and CD68. �
Systemic Inflammation
Recent research studies have determined that the neuroinflammation from primed microglial cells can also cause the pathogenesis of AD. Continuous activation of microglia can promote the synthesis and secretion of pro-inflammatory cytokines and trigger a pro-inflammatory response, ultimately causing neuronal damage. Neuroinflammation is an early symptom in the progression of AD. The microglia can have a tremendous effect on the inflammation of the human brain. �
The inflammation and health issues of the CNS can be associated with systemic inflammation through molecular pathways. One research study demonstrated that ROS development of primed microglia decreases the levels of intracellular glutathione and increases nitric oxide in NADPH oxidase subunit NOX2. Moreover, researchers demonstrated that these simultaneously occurring processes ultimately cause the development of more neurotoxic peroxynitrite. This is demonstrated in rodents with peripheral LPS or proinflammatory cytokines, such as TNF-?, IL-1?, and IL-6, IL-33. �
The outcome measures of numerous research studies have demonstrated that systemic inflammation can cause microglial activation. The results of the research studies emphasize the variability of the inflammatory response in the human brain associated with AD and the underlying health issues associated with systemic inflammation and neuroinflammation, as shown in Table 1. MAPK (mitogen-activated protein kinase) signaling pathways regulate mechanisms of the eukaryotic cell and microglial MAPK can also cause an inflammatory response to the aged brain with AD. Furthermore, chronic or continuous systemic inflammation causes neuroinflammation, resulting in the onset and accelerating the progression of AD. �
�
Genetic Regulation
In the aging human brain, gene regulation has ultimately been associated with an innate immune response. Recent preclinical, bioinformatics, and genetic data have demonstrated that the activation of the brain immune system is associated with the pathology of AD and causes the pathogenesis of this neurological disease. Genome-wide association studies (GWAS), functional genomics, and even proteomic evaluations of cerebrospinal fluid (CSF) and blood have demonstrated that dysfunctional immune pathways from genic mutation are risk factors in LOAD, which is the vast majority of AD. �
GWAS have become a fundamental tool in the screening of genes as well as demonstrating several new risk genes associated with AD. Apolipoprotein E (APOE) ?4allele is one of the most considerable and well-known risk genes for sporadic AD and this mutation ultimately increases the risk of neurological disease onset by 15 times in homozygous carriers and by three times in heterozygous carriers. Further research studies have demonstrated how microglial cell function can be affected through a variety of rare mutations which have demonstrated to have an increased risk factor of Alzheimer’s disease. �
An extracellular domain mutation of the TREM2 gene has also demonstrated an almost identical extent with APOE?4 in increasing the risk factor of AD. TREM2 is increasingly demonstrated on the surface of microglia and mediates phagocytosis as well as the removal of neuronal debris. Additionally, several other genes, such as PICALM, Bin1, CLU, CR1, MS4A, and CD33 have been demonstrated as risk genes for AD. Most of the risk mutation genes are expressed by microglial cells. �
Blood-Brain Barrier (BBB) Impairment
The blood-brain barrier (BBB) is a specialized barrier commonly developed between the blood and the brain by tight liner sheets consisting of specific endothelial cells and tight junctions or structures which connects a variety of cells together. The CNS is fundamental for the human body, and the BBB is fundamental for the CNS. The BBB and the blood-nerve barrier develop a defense system to control the communications of cells and soluble factors between blood and neural tissue where it plays a considerable role in maintaining and regulating the homeostasis of the CNS and peripheral nervous system. �
With development, continuous inflammation can also cause damage to the BBB. This damage can ultimately cause loss of hypersensitive neurons, neuroinflammatory regions, and focal white matter impairment following the damage. The compromised BBB also allows more leukocytes to enter into the CNS where an immune response can be aggravated by brain microglia under the condition of peripheral inflammation. These processes may ultimately be under the control of chemokine and cytokine signaling which can also have an effect on brain microglial cells as well as other health issues in AD. �
By way of instance, it has been determined that TNF-?, IL-17A, and IL-1? can reduce the tight junctions and eliminate the BBB. Loss of BBB integrity and abnormal expression of tight junctions are associated with neuroinflammation. Several research studies also demonstrated in an animal model of AD that the vulnerability of BBB to inflammation increases. Current evidence has also demonstrated that the BBB integrity is fundamental while further evidence of the BBB may demonstrate a new treatment approach for AD associated with microglial priming as shown in Figure 2 below. �
�
Conclusion
Microglia play a fundamental role in maintaining and regulating the homeostasis of the CNS’s micro-environment. If the balance of the homeostasis of the human brain is interrupted, the microglial cells can be activated to restore the balance in the CNS by defending against the stimulation and protecting the structure and function of the brain. However, chronic and continuous stimulation can trigger microglia into a state known as microglial priming, which is more sensitive to potentially minor stimulation, causing a variety of health issues, such as central sensitization, chronic pain, and fibromyalgia. �
Microglial priming mainly causes the boost of A?, tau protein as well as neuroinflammation and reduces neurotrophic factors which can cause the loss of healthy brain cells or neurons as well as the development of neuritic plaques and neurofibrillary tangles which are associated with Alzheimer’s disease. Although this �double-edged sword� plays a fundamental role, it can increase the progression of abnormal protein development and aggravate neuronal loss and dysfunction. However, research studies have ultimately demonstrated that aging can cause the progression of AD and there’s not much we can do about it. �
Microglial cells play a fundamental role as the protectors of the brain and they ultimately help maintain as well as regulate the homeostasis of the CNS microenvironment. However, continuous stimulation can cause the microglia to trigger and activate at a much stronger state which is known as microglial priming. Once the microglial cells go into protective mode, however, primed microglia can become much more sensitive to even minor stimulation and they have a much stronger possibility of reacting towards normal cells. Microglial priming has been associated with neuroinflammation and Alzheimer’s disease (AD) as well as central sensitization and fibromyalgia. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
AD is one of the most common types of dementia among older adults. However, the pathogenesis of AD is misunderstood and there is no definitive treatment for the neurological disease. Research studies have ultimately demonstrated that the activation and priming of microglial cells may contribute to the pathogenesis of AD. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
Undetected or “silent” seizures may contribute to some symptoms associated with Alzheimer’s disease, such as confusion, a small study suggests.
The seizures occur in the hippocampus — a part of the brain involved in the consolidation of memories. Researchers suspect that treating these seizures could help manage Alzheimer’s or possibly slow it down.
“While it is not surprising to find dysfunction in brain networks in Alzheimer’s disease, our novel finding that networks involved in memory function can become silently epileptic could lead to opportunities to target that dysfunction with new or existing drugs to reduce symptoms or potentially alter the course of the disease,” said study senior author Dr. Andrew Cole.
Cole directs the Massachusetts General Hospital (MGH) Epilepsy Service.
“We now have to study more individuals to validate this finding and understand how prevalent it is in Alzheimer’s patients, whether it occurs in other neurodegenerative disorders and how it responds to treatment,” he said in a hospital news release.
Prevalence of Seizures to Alzheimer’s Symptoms
The study involved only two women. They were both in their 60s with symptoms associated with Alzheimer’s disease. The women had bouts of confusion or asked the same questions repeatedly.
Brain images and cerebrospinal fluid tests suggested they had Alzheimer’s, but swings in the women’s symptoms were much more dramatic than usual.
Neither of the women had a history of seizures. Normally, a test called an EEG conducted from the scalp can detect abnormal electrical activity in the brain of people who have seizures. But, in these two women, no such abnormalities were found, the researchers said. Since the hippocampus is a key part of the brain affected by Alzheimer’s disease, and also a common source of seizures in people with epilepsy, the researchers honed in on that part of the brain and conducted additional tests.
Electrodes were placed on both sides of the women’s brains through a naturally occurring opening at the base of the skull. Their brain activity was monitored for 24 to 72 hours.
The study found the women had seizure-like activity in the hippocampus. One woman had frequent surges of electrical activity usually associated with seizures that were not picked up by the scalp EEG. Three seizures occurred during sleep. None of these episodes caused any noticeable symptoms. Anti-seizure drugs eliminated the seizure-like activity. In the year that followed, the woman only had one incident of confusion, which occurred when she missed doses of her medicine.
The other woman also had frequent spikes in electrical activity in the hippocampus during sleep. This patient was also treated with anti-seizure medication but the treatment was discontinued due to unwanted mood-related side effects.
“Our findings confirmed the presence of serious dysfunction of the neuronal networks affected by Alzheimer’s disease and confirmed our hypothesis that epileptic phenomena are an important component of that disturbance,” said Cole. But, he added, more study is needed. The researchers hope to develop a way to detect these silent seizures without using the minimally invasive electrodes in the brain.
SOURCE: Massachusetts General Hospital, news release, May 1, 2017
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Additional Topics: Headache and Auto Injury
After being involved in an automobile accident, it’s common for auto injury symptoms to manifest within the first 24 hours following the incident. Neck pain and headaches are some of the most prevalent symptoms associated with whiplash and other auto injuries. Due to the sudden back-and-forth jolt of the head from the impact of a car wreck, the complex structures surrounding the cervical spine or neck can become damaged or injured.
Alzheimer’s disease claims nearly twice as many American lives annually as it did just 15 years ago, a new report shows.
“And that’s frankly alarming,” said Keith Fargo, director of scientific programs and outreach at the Alzheimer’s Association, which produced the report. “Now, a lot of people will think it’s because we’re living longer,” he added. “And there is some truth to that. But there’s also an assumption that we should just expect to get Alzheimer’s disease as we get older. And that’s not true.
“Most people do not get Alzheimer’s, even if they live into their 80s or 90s. It’s not normal. It’s not something that we should accept. We’ve definitely got to do something about it,” Fargo said.
The Cost of Alzheimer’s Disease
The report also found that more than 5 million American seniors aged 65 and older now live with the memory-robbing disease. That represents approximately 10 percent of all the nation’s seniors, and that number is projected to jump to nearly 14 million by 2050. In fact, nearly half a million seniors are expected to develop the disease in 2017 alone.
Another 200,000 Americans under the age of 65 also struggle with the disease, the report found. And those statistics come with a hefty price tag: It costs $259 billion a year for Alzheimer’s care. That amount is expected to reach $$1.1 trillion by 2050, the report estimated.
Dr. Anton Porsteinsson is director of the Alzheimer’s Disease Care, Research and Education Program at the University of Rochester School of Medicine in Rochester, N.Y. He said the rising numbers likely reflect a number of different factors in play.
“Partly, it is due to increasing numbers of older individuals, partly due to success in treating other leading causes of death, and partly due to increasing awareness that AD [Alzheimer’s] is a lethal disease,” Porsteinsson said.
Among the report’s additional findings: Alzheimer’s is now the fifth leading cause of death among seniors; the sixth leading cause of fatalities among all Americans; and the only disease among the nation’s top 10 biggest killers for which there is no prevention, no way to slow progression and no cure.
“And the costs are now completely out of control,” added Fargo, with the total annual cost for Alzheimer’s and dementia care in excess of a quarter trillion dollars.
Another highlighted concern: the “especially burdensome” ordeal Alzheimer’s caregivers experience while attending to the needs of loved ones as the patient suffers across-the-board mental and physical decline.
In 2016, more than 15 million Alzheimer’s caregivers provided just over 18 billion hours of unpaid care, valued at $230 billion.
Alzheimer’s Disease: Mental and Physical Decline
And those caregivers suffer their own health consequences: More than a third (35 percent) report their health has worsened since assuming caregiver duties, compared with 19 percent of caregivers for older people without dementia. Depression and anxiety also plague dementia caregivers more often, the report found. Still, the report was not entirely bleak, spotlighting growing efforts to identify telltale signs of developing disease.
The goal is to hone in on neurological signs — including changes in brain size, shifts in spinal fluid content, and/or the growth of nerve plaques in the brain — that could allow rapid detection of pre-symptomatic Alzheimer’s.
“It’s a window into the future,” Fargo said. “If you ask where Alzheimer’s disease research is headed, that’s where it’s headed.” “We believe that in the coming years we’ll have tests that you can do in the doctor’s office that will let you know your risk for Alzheimer’s,” he noted. And that, he suggested, “could open the door for prevention.”
Fargo noted that, even in the absence of effective treatments or a cure, early diagnosis would be a boon for research and would give patients a head start on planning for their future. Yet, Porsteinsson suggested that the future of these telltale signs, known as biomarkers, remains unclear.
“Biomarkers are particularly important when it comes to research and development of future potential treatments,” he said.
On the other hand, he stressed that “the utility of biomarkers in current care is intensely debated.
“The biomarkers are expensive,” Porsteinsson noted. “And it is a question how much a positive or negative finding will change approach to care. “Having said that,” he added, “it often matters greatly to patients and their families to know exactly what they have and what to expect.”
SOURCES: Keith Fargo, Ph.D., director, scientific programs and outreach, Alzheimer’s Association, New York City; Anton Porsteinsson, M.D., professor, psychiatry, and director, Alzheimer’s Disease Care, Research and Education Program, University of Rochester School of Medicine, Rochester, N.Y.; March 7, 2017, 2017 Alzheimer’s Disease Facts and Figures
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Brain injuries are common complications in our modern world. Approximately 2 million individuals experience a head injury in the United States alone each year. Although most brain or head injuries are not considered life threatening, they could sum up to billions of dollars in annual revenue. Brain injuries are often categorized according to patient response. Only 1 out of 4 reported brain injuries are considered moderate or severe.
Alzheimer’s patients given sedatives such as Valium or Xanax may have an increased risk for pneumonia, a new study warns.
People with Alzheimer’s disease are often given these drugs, called benzodiazepines, over the long term, the researchers said. Examples of benzodiazepines include alprazolam (Xanax), clonazepam (Klonopin), diazepam (Valium), and lorazepam (Ativan).
“An increased risk of pneumonia is an important finding to consider in treatment of patients with Alzheimer disease. Pneumonia often leads to admission to hospital, and patients with dementia are at increased risk of death related to pneumonia,” Dr. Heidi Taipale, of Kuopio Research Center of Geriatric Care at the University of Eastern Finland, and co-authors wrote.
For the study, the researchers reviewed data from nearly 50,000 Alzheimer’s patients in Finland. The patients’ average age was 80 and about two-thirds were women. The study found that people with Alzheimer’s who took benzodiazepines were 30 percent more likely to develop pneumonia than those who weren’t given the sedatives.
Increased Risk of Pneumonia in Patients Taking Drugs
The risk of pneumonia was highest in the first 30 days after starting the drugs, the findings showed. The researchers said their findings are consistent with previous studies. Because benzodiazepines are sedating, it’s possible that people taking them may breathe saliva or food into the lungs, increasing the risk of pneumonia, the study authors suggested.
Taipale’s team said the benefits and risks of these drugs — including pneumonia — need to be carefully considered before giving them to someone with Alzheimer’s disease. The study was published April 10 in the CMAJ (Canadian Medical Association Journal).
The study is “a good reminder to clinicians to ‘first do no harm’ when prescribing these drugs for frail older women and men with dementia,” Dr. Paula Rochon and her co-authors wrote in an accompanying editorial in the journal. Rochon is from Women’s College Hospital and the University of Toronto.
Non-drug “approaches should be the starting point when managing neuropsychiatric symptoms in this patient population, which should help to limit inappropriate use of these drugs,” the editorial authors said.
SOURCE: CMAJ (Canadian Medical Association Journal), news release, April 10, 2017
News stories are written and provided by HealthDay and do not reflect federal policy, the views of MedlinePlus, the National Library of Medicine, the National Institutes of Health, or the U.S. Department of Health and Human Services.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Brain injuries are common complications in our modern world. Approximately 2 million individuals experience a head injury in the United States alone each year. Although most brain or head injuries are not considered life threatening, they could sum up to billions of dollars in annual revenue. Brain injuries are often categorized according to patient response. Only 1 out of 4 reported brain injuries are considered moderate or severe.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine









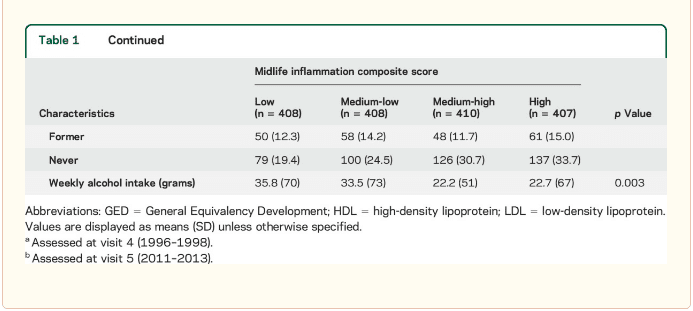 Inflammatory markers and brain volume. Each SD increase in inflammation composite score at baseline was associated with a 532 mm3 smaller AD signature region volume (95% confidence interval [CI] ?922 to ?141), a 519 mm3 smaller occipital lobe volume (CI ?906 to ?132), a 110 mm3 smaller hippocampal volume (CI ?196 to ?24), and a 1,788 mm3 larger ventricular volume (CI 371 to 3,205) at follow-up (table 2). We found the estimated effect of a 1 SD increase in inflammation composite score during midlife on occipital lobe, ventricular, and hippocampal volume to be similar to the effect associated with possession of a single APOE ?4 allele in our multivariable regression analyses. No association was found for the total brain, frontal lobe, temporal lobe, or parietal lobe volume (ps > 0.071). Our findings did not change meaningfully after excluding participants who regularly used anti-inflammatory medication during the follow-up period (table e-2) and after including participants who met the criteria for dementia at visit 5 (table e-3). For descriptive purposes, associations between individual inflammatory markers and AD signature region volume are provided in a table e-4. �
Inflammatory markers and brain volume. Each SD increase in inflammation composite score at baseline was associated with a 532 mm3 smaller AD signature region volume (95% confidence interval [CI] ?922 to ?141), a 519 mm3 smaller occipital lobe volume (CI ?906 to ?132), a 110 mm3 smaller hippocampal volume (CI ?196 to ?24), and a 1,788 mm3 larger ventricular volume (CI 371 to 3,205) at follow-up (table 2). We found the estimated effect of a 1 SD increase in inflammation composite score during midlife on occipital lobe, ventricular, and hippocampal volume to be similar to the effect associated with possession of a single APOE ?4 allele in our multivariable regression analyses. No association was found for the total brain, frontal lobe, temporal lobe, or parietal lobe volume (ps > 0.071). Our findings did not change meaningfully after excluding participants who regularly used anti-inflammatory medication during the follow-up period (table e-2) and after including participants who met the criteria for dementia at visit 5 (table e-3). For descriptive purposes, associations between individual inflammatory markers and AD signature region volume are provided in a table e-4. � 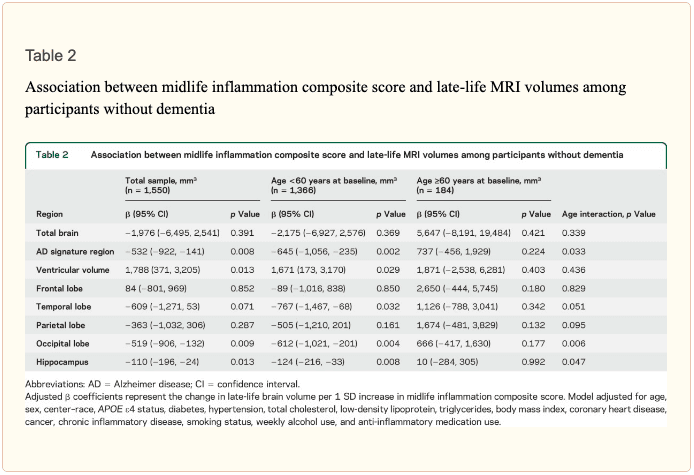 An assessment of linear trend revealed that compared to individuals with 0 elevated (?75th %tile) inflammatory biomarkers at baseline (reference), those with 1�2 and 3�5 elevated biomarkers had lower AD signature region (p trend = 0.001), occipital lobe (p trend = 0.007), and hippocampal volume (p trend = 0.041) 24 years later (figure 1). Compared to the reference group, participants with 3 or more elevated markers demonstrated 5.3% smaller AD signature region volumes, 5.7% smaller occipital lobe volumes, and 4.6% smaller hippocampal volumes, on average. However, this pattern was not statistically supported for the total brain, ventricular, frontal lobe, temporal lobe, and parietal lobe volume (p trends >0.072).
An assessment of linear trend revealed that compared to individuals with 0 elevated (?75th %tile) inflammatory biomarkers at baseline (reference), those with 1�2 and 3�5 elevated biomarkers had lower AD signature region (p trend = 0.001), occipital lobe (p trend = 0.007), and hippocampal volume (p trend = 0.041) 24 years later (figure 1). Compared to the reference group, participants with 3 or more elevated markers demonstrated 5.3% smaller AD signature region volumes, 5.7% smaller occipital lobe volumes, and 4.6% smaller hippocampal volumes, on average. However, this pattern was not statistically supported for the total brain, ventricular, frontal lobe, temporal lobe, and parietal lobe volume (p trends >0.072).  The modifying effects of age, race, and sex. A significant age-by-inflammation composite score interaction was found for the AD signature region, occipital lobe, and hippocampal volume (table 2). Because a reversal of association was observed at age 60 (figures 2, e-1, and e-2), we stratified the sample into young-midlife and old-midlife subgroups (<60/? 60). As displayed in table 2, the associations between higher midlife inflammation composite score and lower AD signature region, occipital lobe, and hippocampal volume at follow-up were significantly stronger among participants who were 60 or younger at baseline compared to those who were older than 60. A marginal race-by-inflammation composite score interaction was found for occipital lobe volume, whereby a higher midlife inflammation composite score was associated with lower occipital lobe volume among white, but not African American, participants (table 3). No interactions with sex were found (table e-5). �
The modifying effects of age, race, and sex. A significant age-by-inflammation composite score interaction was found for the AD signature region, occipital lobe, and hippocampal volume (table 2). Because a reversal of association was observed at age 60 (figures 2, e-1, and e-2), we stratified the sample into young-midlife and old-midlife subgroups (<60/? 60). As displayed in table 2, the associations between higher midlife inflammation composite score and lower AD signature region, occipital lobe, and hippocampal volume at follow-up were significantly stronger among participants who were 60 or younger at baseline compared to those who were older than 60. A marginal race-by-inflammation composite score interaction was found for occipital lobe volume, whereby a higher midlife inflammation composite score was associated with lower occipital lobe volume among white, but not African American, participants (table 3). No interactions with sex were found (table e-5). � 
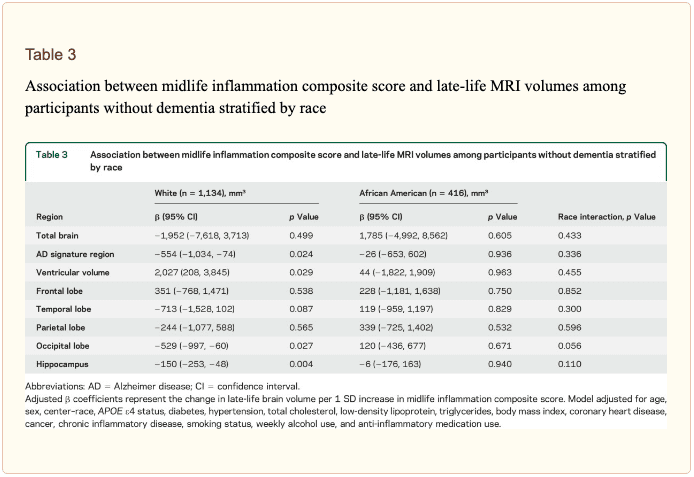 Inflammatory markers and episodic memory. Late-life episodic memory, which was associated with hippocampal and AD signature region volume after controlling for age (partial rs > 0.21, ps < 0.001), was reduced among participants with higher levels of the inflammation composite score. Each SD increase in inflammation composite score was associated with a ?0.08 SD performance decrement on the DWR after adjusting for covariates (CI ?0.15 to 0.00; p = 0.046). Similarly, a higher number of elevated inflammatory biomarkers at baseline was associated with reduced DWR performance (p trend = 0.009; figure 1). �
Inflammatory markers and episodic memory. Late-life episodic memory, which was associated with hippocampal and AD signature region volume after controlling for age (partial rs > 0.21, ps < 0.001), was reduced among participants with higher levels of the inflammation composite score. Each SD increase in inflammation composite score was associated with a ?0.08 SD performance decrement on the DWR after adjusting for covariates (CI ?0.15 to 0.00; p = 0.046). Similarly, a higher number of elevated inflammatory biomarkers at baseline was associated with reduced DWR performance (p trend = 0.009; figure 1). �


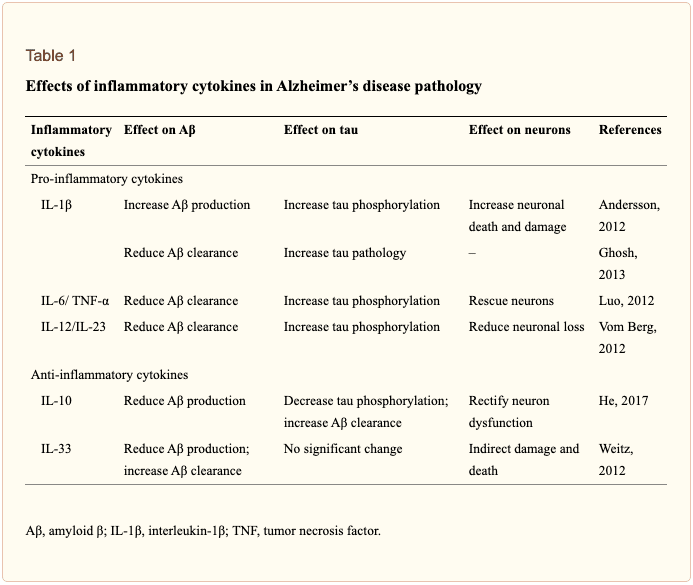 �
�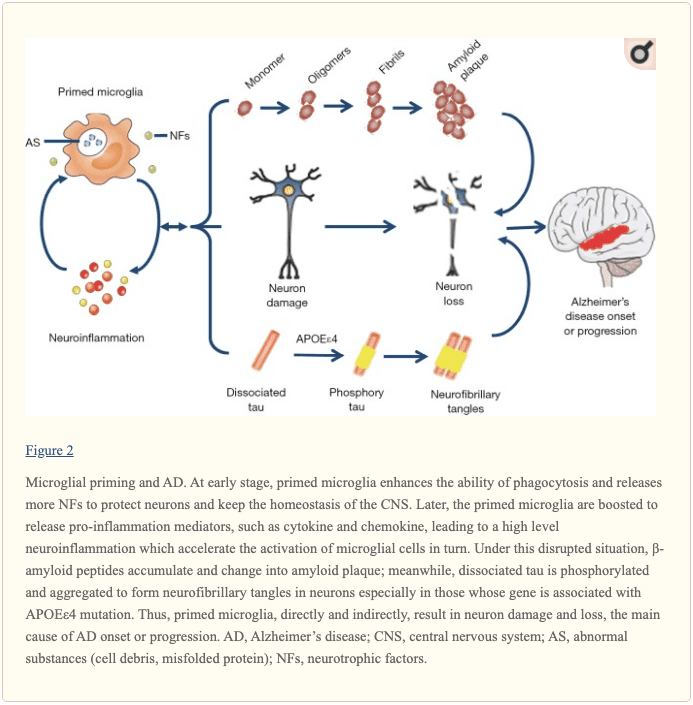 �
�









