Fish oil is used as a natural health supplement that treats a variety of issues. It provides beneficial omega-3 fatty acids that promote good health throughout the body and helps to cure or prevent certain health conditions. However, some people are not convinced. They view fish oil as nothing more than snake oil with no real health benefits. Nothing could be further from the truth. Researchers at Harvard University ranked omega-3 fatty acid deficiency as the sixth highest cause of death in the United States.
What is Fish Oil and what are Omega-3 Fatty Acids?
Fish oil is precisely what it sounds like, oil from the tissues of oily fish. While you can get it by eating certain fatty, cold water fish like wild caught salmon, white fish, anchovies, herring, and sardines, many people opt for the fish oil supplements available at health food stores and even supermarket shelves.
Omega-3 fatty acids are highly concentrated fish oil. They are polyunsaturated fatty acids and must be introduced into the body either via the food eaten or supplements. It is not like many other fatty acids that the body can produce. Fish oil has two vital types of omega-3, eicosatetraenoic acid (EPA) and docosahexaenoic acid (DHA).
How is Fish Oil Used?
Fish oil supplements are intended to be taken just like a daily vitamin. Because of its many health benefits like preventing diseases and reducing the symptoms of certain conditions, it has become a standard in most people�s health routines and is even included in some multi-vitamins. It is taken in the form of a capsule. It can be purchased over the counter, but the FDA has approved a prescription version fish oil that lowers high triglyceride levels.
Fish oil omega three gel capsule
What are the Benefits of Fish Oil?
Fish oil provides a number of health benefits ranging from heart health to treating diabetic complications that affect the kidneys. It also helps:
Lowering blood pressure
Lowering cholesterol levels
Preventing heart disease and stroke
Preventing clogged arteries
Relieving certain heart conditions such as irregular heartbeat, heart failure, chest pain, and preventing blood clots
It is used after bypass surgery to aid in healing as well as with heart transplants
Kidney disease
Kidney failure
Cirrhosis
Arthritis
Cancer
Anxiety
Berger�s disease
Brain health including relieving depressing, PTSD, migraines, ADHD, and other mental health issues
There are many other fish oil benefits. It indeed is a wonder health supplement.
How to Take Fish Oil
Fish oil typically comes in a gel-filled capsule. It is essential that it not be punctured before taking. Patients should follow the direction exactly as they are on the label or as the doctor prescribed. It is a good idea for them to talk to their doctor before they start taking fish oil to make sure that it does not interact with any other medications that they are taking.
Potential Side Effects of Fish Oil
Typically, fish oil will not have any side effects. Some mild ones include an upset stomach, back pain, mild rash on the skin, belching, and an unusual or unpleasant taste in the mouth. More severe side effects that should warrant a call to the doctor include flu symptoms: fever, body aches, chills; irregular or uneven heartbeats; and chest pain.
An allergic reaction to fish oil is serious and the patient should seek immediate medical attention if they experience any of these symptoms:
Hives
Breathing difficulties
Swelling: throat, tongue, or face
How to Choose Good Fish Oil
Anyone considering taking fish oil should first talk to their doctor who can recommend a therapeutic dose. Read the label to determine how much omega-3 is in each capsule as well as the recommended dosage. Doctor recommended brands are best, but in the absence of a doctor recommendation, a reputable brand by an established, trusted, trustworthy company is best.
Fish oil is excellent for all-around health and chiropractic patients taking the supplement can enjoy better health and better results from their chiropractic care.
Today we will discuss the fundamentals of functional medicine and how you can build a healthy doctor-patient relationship.
If you visit the doctor because you�ve been experiencing migraines, eczema, irritable bowel syndrome and depression, you�re most likely going to be referred to four different specialists and you may even be prescribed four different drugs and/or medications, at minimum. A functional medicine approach understands that there may be common underlying health issues which can be causing a patient�s symptoms. Once you get to the source of the problem, you can fix the health issues that create the symptoms.
Functional medicine asks, �Why do you have those symptoms and how can we treat the source of the problem and improve your overall health and wellness?� rather than, �What disease do you have and what drug do you use to treat it?�
What is Sick Care vs Health Care?
Hello everyone, my name is Dr. Alex Jimenez. I�m a chiropractor and practicing functional medicine doctor in El Paso, Texas. I�m so happy to introduce you to part one of �Taking Control of Your Healthcare�, where we will discuss the differences between �Sick Care and Health Care�. So, I frequently hear people talk about how difficult it is to find the right doctor, someone who is willing to work with them, who listens to them, and who is open to meeting their demands while teaching them everything they need to know about their problems. A doctor who accepts innovative advances in science and system approaches to determine the source of the problem. This is known as functional medicine, and we will discuss more of that in a minute.
My goal right now is to show you how you can find the right doctor and build the best relationship with them to get the care you deserve. It�s important to ask your doctor several questions to determine if they are the appropriate fit for you, if they�re willing to work with you, to listen to you, and if they�re open to your requests as well as learning about problems they�re not familiar with and following new treatment approaches. By way of instance, if the doctor you choose says that nutrition has nothing to do with disease, then you should probably go find another doctor. Now let�s discuss what questions you should ask your doctor regarding your overall health and wellness in order to be informed about what�s happening in your own body.
I�ve talked to patients who have visited numerous doctors in hopes of finding an answer as to why they�re not feeling well or have some type of disease. Many are frequently referred to one or more specialists and, in some cases, they�re given Prozac, or they�re told that their symptoms are all in their head or sometimes they�re even told that there�s nothing wrong with them after their lab results are all normal. And it�s frequently these same patients who are often sent to various doctors for each part of their body rather than being sent to a doctor who can diagnose and treat their body as a whole. If you go to the doctor and you have migraines, eczema, irritable bowel syndrome, and depression, in most cases, you�re going to be sent to four different specialists and you�re going to be given, at least, four different medicines instead of visiting a specialist who can understand the underlying source of the problem and treat the root of the symptoms.
Have you ever visited a doctor who, after explaining your symptoms to them, said, �Oh, I did a full blood panel and everything came back normal.� This could mean one of two things, either you�re crazy or they�re missing something. And I�m sure they�re often missing something because they�re not looking in the right places for the answers. It�s like the guy who dropped his keys in the street and when his friend sees him looking under a lamppost, he says, �Hey, what are you doing?� He says, �Well, I�m looking for my keys.� �So, where did you lose them.� He says, �Well I lost them down the street.� �Then why are you looking here?� �Well, the light�s better here.� And unfortunately, that happens a lot in medicine. Doctors will look for answers where problems are easy to find. And that is the purpose of this article. To help you understand how you can find the source of the underlying health issues that are making you feel sick.
This reminds me of a case of a woman I saw in my office who had psoriatic arthritis, an autoimmune condition which caused her to have rashes all over her body along with joint pain and swelling. As a result, she was on large amounts of drugs and/or medications which added up to about $60,000 dollars a year or more. She also had other health issues, she had acid reflux, irritable bowel syndrome, pre-diabetes, migraines, insomnia and depression. This woman visited many different specialists and she was taking prescriptions to address each of her symptoms. When it came time for me to see her, all I did was get to the source of the problem.
So, during diagnosis, I said to myself, �Okay, this patient has inflammation, but what�s the cause of her inflammation?� And instead of referring her to numerous other specialists so she could receive medicine for her migraines, acid reflux, depression, etc., I said to myself, �Oh, all of these symptoms are inflammatory, so what�s the root of the inflammation?� Well it turns out that the patient had problems with her gut all along. I then helped her clear out the �bad bugs� in her gut by recommending her an anti-inflammatory diet, I included some supplements, fish oil, vitamin D, probiotics. Honestly, really basic natural remedies. When she returned six weeks later, all of her symptoms had disappeared. She had gotten off all of her prescription medicines and she had lost 20 pounds. I didn�t tell her to stop taking her meds, she just did it on her own. It was absolutely remarkable and that�s what happens when you treat the source of a patient�s underlying health issues. And you don�t have to do a lot to get to the root of the cause.
I understand that it may not always be possible to work with a doctor who�s trained in functional medicine, which we will discuss what that means in a minute, however, it is possible to find a doctor who�s going to be willing to work with you, who�s going to listen, who�s going to have an open mind and who�s going to be your partner during your journey to overall health and wellness. Throughout this article, I�m going to discuss conventional lab testing as well as innovative functional medicine lab testing, demonstrating it all for the purpose of creating well-being rather than viewing it all from the perspective of the disease in order to find the source of a patient�s health issues and correct imbalances through a functional medicine approach.
Taking Control of Your Health Care vs Sick Care
Functional medicine is often referred to as the future of medicine, but it�s currently being offered by many doctors if you visit the right place. The purpose of functional medicine is to diagnose and treat the root cause of a variety of diseases by evaluating the body as a whole, rather than by analyzing each collection of organs independently through separate specialists. Functional medicine treats the whole system, not just the symptoms. Doctors who practice functional medicine frequently ask themselves, �Why does the patient have these symptoms and how can I fix the root causes and improve their overall health and wellness?� rather than �What disease does the patient have and what drug and/or medication do they use to treat it?�
I�ve been a practicing chiropractor for over 25 years. And I�ve witness countless of miracles every day. My patients don�t simply find relief from their symptoms, they truly achieve overall well-being. Unfortunately, our current healthcare system is broken. Many doctors are tremendously affected due to time constraints set by insurance companies to pay bills, causing them to rush through their appointments. In turn, this continuous cycle can frequently end up leaving patients with unanswered questions followed by frustration. Our current healthcare system makes people feel powerless, often keeping them stuck in disease.
As a part of this healthcare system, it�s important that we understand that some diseases are not as easily treatable as a cold. Several diseases also don�t just develop randomly. The majority of diseases which exist today are related to your environment and how these external as well as internal factors alike interact with your genes and lifestyle to influence your health and wellness.
What we know today as the �conventional medicine� approach is typically referred to as the �name it, blame it, and tame it� game. First, the doctor will diagnose the patient and provide them with a label, by way of instance, they say a patient has depression. Now they have the name of the disease. And finally, the doctor will treat the disease with prescription drugs and/or medications. In the end, the patient is left taking an antidepressant. However, depression can be caused by a wide array of factors and the solution isn�t necessarily an antidepressant. Not only is this type of practice outdated, it�s actually considered to be quite unsafe in the long-run. And it�s often not providing patients with the results they need. People are being misdiagnosed and mistreated, frequently being left sick without really getting the proper care they deserve.
Conventional medicine can also be helpful at the very end stages of some diseases as well as for acute diseases. If you have an emergency or you�re feeling very sick, if you break a bone, or if you have a raging infection, conventional medicine, acute care, drugs and/or medications can be the right solution and we should be highly grateful for them. But this is not the approach we need to prevent and cure chronic diseases. If we actually understood how to care for our bodies the way we should, most of us wouldn�t be feeling as sick as we do. And many people will walk around feeling sick, but you don�t have to, it�s not normal. Many doctors now understand that a change is required to turn our entire sick care system into one that actually supports health care.
I would like to empower you to help transform the future of the medicine field by taking your well-being into your own hands. Throughout the next articles I�m going to share with you how you can find a doctor that takes consideration of your personal values and beliefs so you can achieve the results you�re looking for while in a safe and comfortable environment. You can learn how to be your own health advocate and become a true partner with your doctor. And there are many other doctors and functional medicine practitioners like me who are waiting to help.
Furthermore, I�m going to share with you how you can find the best doctor and I�m also going to provide you with many other tools to help you be the leader of your overall health and wellness. How you can take control and make the calls for your own well-being. Including what lab work you should ask your doctor for, and how to understand what the information means and what you should do with it. One of the most common ways doctors utilize labs is to evaluate what goes wrong when a patient isn�t feeling well and to analyze the end of a continuum of disease. If your liver function changes your liver cells may already be dying. If they�re normal, however, many doctors say, �Oh, you�re normal.� But it may actually not be normal. The good news is that you may be able to find imbalances sooner in order to treat them in time.
Although it�s slowly been changing, many doctors have the custom of not giving patients their actual lab tests. And if this isn�t the case, several doctors don�t provide detailed explanations of patient�s lab tests other than, �Your lab tests came back normal,� or �Your cholesterol is a little high,� or, �Your blood sugar is a little high.� As a chiropractor, I believe that everyone should have access to their lab tests and that these should be explained to the patient. We need to start democratizing health care. And this has become more fundamental than ever before.
Now why is this so important? Approximately 133 million Americans are affected by chronic disease and that number is even higher depending on how chronic disease is defined. About one in two individuals in the United States has pre-diabetes or type 2 diabetes. The rate of a variety of diseases, including digestive problems, allergic diseases, heart disease, autoimmune diseases, cancer, obesity, type 2 diabetes, and dementia have all been increasing. Where approximately one in three kids born today will have type 2 diabetes in their lifetime and one in two people over the age of 85 and one in four people over the age of 75, are going to have dementia.
Health issues like these are manifesting throughout our population at a tremendous rate and they can affect everyone, either personally or through the suffering of a loved one. Additionally, chronic diseases have caused a dramatic economic burden within our country.
However, the reason why I�m so happy to share this article with you is because there�s a lot we can do to change the future of our healthcare system. Many doctors and I have the knowledge we need to decrease or even eliminate the suffering of so many people and to save the economy. Every day in my office, I see patients recover their quality of life after they were expecting to suffer their entire lives due to chronic diseases such as, acid reflux, irritable bowel syndrome, headaches, fatigue, and arthritis, among other health issues. Problems like allergies, hormonal issues, obesity, diabetes, heart disease, autoimmune diseases, and depression. And patients can truly get better and thrive, not just cope with or manage their disease. Within a few months, even weeks, of visiting me and my staff, the lives of patients can tremendously change.
Functional medicine looks at how the human body functions as a whole, and its most basic approach is to first understand the factors, genes, and triggers for disease, and how lifestyle and environmental inputs, including diet, stress, toxins, allergens, and microbes, interact with the human body to create imbalances which can commonly lead to chronic health issues.
So, let me take a moment to discuss something. The human body is a system. And this entire system is made up of smaller, �mini-systems� which are all dynamically interacting. But, when one or more of these systems get out of balance, you can become sick. And when these systems get in balance again, you become healthy. And that�s what functional medicine is. Functional medicine is simply understanding what causes imbalances in the human body and treating them to restore balance and provide essential needs to all the systems in the human body. Creating overall health and wellness. It is the science of creating well-being. And doctors achieve this by utilizing a patient�s detailed medical history, combined with targeted lab tests. Doctors who follow a functional medicine approach, like me, by way of instance, generally evaluate your gut and your microbiome, which not many doctors look into. We also want to look at your immune system and whether inflammation is affecting you, something which we refer to as defense and repair. And we want to know how your mitochondria produces energy from food and oxygen. Functional medicine practitioners want to know if you have any dysfunctions in energy production, which is typically the source of numerous diseases, such as Alzheimer�s disease and autism, type 2 diabetes, and fatigue, among many others. We also determine your toxic load and your ability to detoxify, involving the function of other communication systems in your body, such as your hormones. Finally, we evaluate your structural system, from your cells to your biomechanical structures and how these interact with your beliefs, emotions, and more.
I�ve used these procedures, over and over again, to help reverse chronic disease in my patients and educate them on how to achieve long-term health and wellness, all while feeling like the best versions of themselves. We are all given the opportunity to cure or tremendously improve health issues or problems which are often misdiagnosed and mistreated by conventional medicine. Functional medicine provides the opportunity to discover overall well-being at any age.
As a matter of fact, I treated a man named, George, who was 63 years old, weighed 300 pounds, and who had a variety of health problems. He had acid reflux, sinus problems, diabetes, angina heart failure, prostate problems, sexual dysfunction, and edema in his legs. And as a result, he was under a wide array of prescription medicine. He came into my office one day and he said to me, �Can you help me.� I said, �Yes, but you will have to do everything I say.�
So, I recommended him an anti-inflammatory diet, consisting of whole foods and a low intake of sugar, and I advised him to take a variety of supplements in order to optimize his nutrition, all while I guided him into participating on exercises and physical activities. Within a year, it was like a miracle, the patient had lost 155 pounds, he reversed all of his health issues and he stopped using his prescription medicines. Now, he�s planning the rest of his life, when before he came to visit me, he was planning the end of his life. Another patient I treated, named Isabel, struggled with an autoimmune disease. She was only 10 years old and she was already under a pile of drugs, steroids, immunosuppressants, and even chemo drugs. It turns out that her diet and exposure to heavy metals was affecting her gut and causing inflammation. Now, I simply treated the source of her problems and her autoimmune disease went away. She stopped using her prescription medicines and, altogether, her quality of life improved and she thrived.
Functional medicine is an alternative treatment approach which focuses on the interactions between external or environmental factors as well as internal factors associated with the gastrointestinal, endocrine, and immune systems of the human body. Finding the right doctor can make a big difference when it comes to getting health care over sick care. Functional medicine treats the source of the problem rather than treating the symptoms alone. As a chiropractor and functional medicine practitioner, my primary goal is to provide patients with the care they deserve for their health issues as well as to educate them on the fundamentals of functional medicine. The purpose of this article is to help patients find the right doctor and build a healthy doctor-patient relationship. Dr. Alex Jimenez D.C., C.C.S.T. Insight
Sick Care vs Health Care Overview
Over the next few weeks, we�re going to go through some of the fundamental principles and concepts that helped me find the underlying cause of disease through the use of functional medicine. And that will help you achieve overall health and wellness.
In our next article, I�m going to teach you how you can take your own measurements to understand your own well-being and what you can do to improve your vital signs. This procedure is going to help provide you with important baseline data and information to help you better understand your health risks. It�s also going to allow you to evaluate and analyze your own progress as you work towards your ultimate wellness goals.
In the third article, I�m going to try to cover everything about nutrition. I will explain how we can test your nutritional status and how you can utilize food as treatment to start changing your overall health and wellness as soon as possible. Your diet is one of the most effective parts you can control to create a healthier lifestyle. I�ll be sharing tips and tricks for a better nutrition.
Because hormones can impact nearly every aspect of our health, we�re also going to be highlighting them in the fourth article. Unfortunately, a majority of doctors do not understand what optimal hormone levels should look like nor are they aware of the proper methods for testing hormones. I will be preparing you to have an effective conversation with your doctor on which type of hormone test actually matters, what they mean, and what you can do about them.
In article five I�m going to focus on heart health, such as high blood pressure, high cholesterol, and cardiovascular disease. These conditions are extremely common, and unfortunately, conventional medicine frequently tries to treat them by simply controlling the symptoms. Lowering cholesterol, lowering your blood pressure, that does not solve the root cause of the problems. Most of the time, increased levels of blood sugar, obesity and diabetes are the cause of cardiovascular disease. I�m going to demonstrate how we can prevent and reverse these diseases using lifestyle modifications, including nutrition, to improve heart health.
In the sixth article, I�ll be discussing obesity and diabetes, something I�ll be frequently referring to as diabesity. Metabolic disorders ranging from minimal fat and moderate insulin resistance to pre-diabetes to type 2 diabetes. The great thing about these metabolic disorders, however, is that they are completely reversible. But most conventional doctors don�t know it�s reversible. I�m going to help teach you how you can recover a healthy metabolism and how you can reverse the range of problems involved in diabesity, which as you will learn, are a lot of different diseases.
In article seven, I�m going to talk about the immune system, particularly discussing hidden inflammation and disease. As inflammation is described to be the underlying cause of a majority of chronic diseases, we continue to see increasing rates of autoimmune diseases and allergies, which are signs that our immune systems are not functioning properly. However, inflammation is also associated with obesity, type 2 diabetes, heart disease, cancer, dementia, and even depression. I�ll explain how you can talk to your doctor about testing for inflammation, what the markers mean, and how you can care for your immune system on a deeper level.
In article eight, we�re going to move into the topic of the metabolism and mitochondria. Now every one of our cells hold hundreds or thousands of mitochondria, the energy generators of our cells. When these become damaged, we can suffer from a variety of problems, including pain, memory loss, fatigue, and many other symptoms. I�m going to explain how we can care for your mitochondria at the cellular level and why this is a vital piece of optimal health and wellness.
Then, in article nine, we�re going to explore the meaning of detoxification, or the human body�s innate detox system and why this is an essential part of the healing process. From mold to heavy metals, and other toxins, I�m going explain what you need to know to avoid toxins and how you can eliminate those that you are already carrying to optimize your capability to detoxify. With the amount of toxins we�re exposed to on a regular basis, it�s important to identify the causes that may be affecting you and how you can begin eliminating them right away. Fortunately, this is something you can easily do to create a cleaner lifestyle for you and your loved ones.
Finally, in article ten we will be talking about digestion. Digestive health is one of the most commonly discussed topics in functional medicine. Because our digestive system is the center of our health, by diagnosing problems in this system, we can improve everything from mental health, nutrient absorption, and cardiovascular risk to immune system function. In the tenth article, I�m going to guide you through the tests that are available for monitoring your gut health, as well as what you can do to improve your own digestive health, as soon as possible.
I�m so happy you�ll be joining me throughout this series of articles because the future of medicine depends on it. When you learn how you can impact your well-being by being proactive and by creating a partnership with your doctor, everything changes. Through functional medicine, you can also help transform our sick care system into an actual health care system.
So, let�s finish up this article with the questions you want to ask your doctor as you interview them to see if they can be a partner for you and your overall health and wellness. These are just a few high-level questions to start with your discussion. Are you willing to work with me as a partner for my well-being? Also, what�s your point of view on nutrition and health? Do you think food is medicine? Are you willing to give me copies of my test results and explain what they mean? The reason why we�re asking these questions is to make sure that your doctor is willing to work with you and understand the role of functional medicine.
I�m so happy to be a part of your journey to better health and wellness. Thank you very much for joining me today. The scope of our information is limited to chiropractic and spinal health issues as well as functional medicine topics and discussions. To further discuss the subject matter, please feel free to ask Dr. Alex Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion:�Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief. �
Chronic pain caused by accidents and/or aggravated conditions can often be one of the primary reasons for depression in patients. When painful symptoms induce patients to struggle with their everyday physical activities, their mental health can be tremendously influenced. Chiropractic care utilizes spinal adjustments and manual manipulations which could help restore the initial integrity of the backbone. Patients describe how chiropractic care has helped them recover their well-being and they highly recommend Dr. Alex Jimenez, doctor of chiropractic, as the non-surgical choice for chronic pain and depression, one of a variety of other common health issues.
Chiropractic Relief
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life that is fulfilled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life. I have made a life of taking care of every one of my patients.
I assure you, I will only accept the best for you�
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend�us.
Most people don�t think of chiropractic to treat conditions that do not involve the spine, but study after study shows it is effective in treating a wide variety of health issues. Ulcerative colitis seems to have no real connection with the spine, yet patients and researches alike are touting the effectiveness of chiropractic care to treat the condition. This is due, in part to chiropractic�s approach to whole body wellness, but spinal alignments are incorporated into the care as well. Bottom line, chiropractic care is extremely effective in treating uncreative colitis, and many patients are finding relief from their symptoms and discomfort.
What is Ulcerative Colitis?
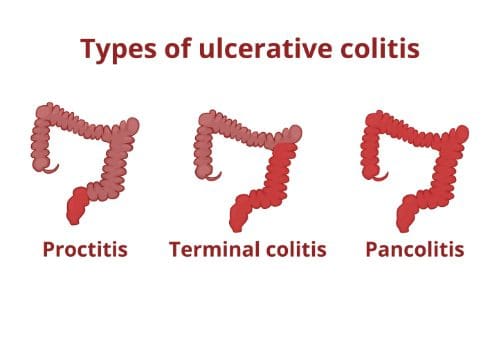
Ulcerative colitis is a disease that causes ulcers (sores) and inflammation in the rectum and colon. Typically, only the sigmoid colon (the lower portion of the colon) is affected, along with the rectum.
However, the entire colon can be affected, and the percentage of the colon that is affected tends to coincide with the disease�s severity of the symptoms. While ulcerative colitis can affect people of any age, the majority of people who are diagnosed with it are younger than 30 years old.
Researchers are not sure what causes ulcerative colitis, but many believe that it occurs when the body�s immune system overreacts to bacteria that naturally occurs within the body, specifically in the digestive tract. There also seems to be a genetic predisposition for the disease; it tends to run in families.
What are the Symptoms of Ulcerative Colitis?
The type and severity of symptoms that present with ulcerative colitis depends upon how advanced, or severe depends on which area of the colon is affected and how severe the condition is. The symptoms may subside or disappear for several weeks at a time (some patient reports are stating they had no symptoms for years), then they return � about half the people with ulcerative colitis experience mild effects.
Diarrhea � This is the most common symptom. Diarrhea may have pus or blood in it, but it is possible to have blood in the stool and not have the ability to see it. In severe cases, the urge to go to the restroom to empty the colon may come on suddenly and powerfully. It may happen after a meal or after eating certain foods. Other times there may be no discernable pattern; it can happen at any time, even waking the patient out of a dead sleep.
Pain � The most common type of pain with ulcerative colitis is in the belly and may feel somewhat cramping. However, some patients report joint soreness and photophobia (sensitivity to light) accompanied by eye pain.
Nausea � The cramping can cause nausea, as well as the condition itself.
Fatigue � The other symptoms such as pain and nausea can cause fatigue, but effects of the disease such as swelling in the colon and bleeding in the colon that depletes the body of red blood cells can also cause extreme tiredness.
Dehydration � This can be caused by diarrhea.
Weight loss � Caused by diarrhea and loss of appetite. The body may not be able to absorb the nutrition from foods due to the disease adequately, so weight loss and malnutrition follow.
Sores � Mouth and skin sores may form as well as rashes.
What Treatments are Available for Ulcerative Colitis?
Different people are affected differently when they are battling ulcerative colitis. Patients with mild symptoms may be able to take an over the counter medication that treats diarrhea.
The majority of patients with the disease take prescription medications that help decrease the immune response in the body. Lifestyle changes may also work. If the condition is very severe, the patient may need to undergo surgery and have their colon removed.
Chiropractic for Ulcerative Colitis
Many patients turn to chiropractic care to treat ulcerative colitis. When the body is out of alignment, it can hinder the function of the organs and other parts of the body. By realigning the spine and pelvis, the chiropractor can help the patient lessen or completely alleviate their symptoms.
The whole body health approach that chiropractic promotes can also help with recommendations regarding lifestyle changes and diet modifications. Many patients who get regular chiropractic care for their ulcerative colitis report a significant decrease in symptoms and often the complete elimination of them.
Regular preventative care and maintenance are integral to good health. The better you treat your body, the better it will treat you. Unfortunately, you can�t always see or know when there is a problem, and regular check-ups can help you stay ahead of potential health problems that could significantly impact your quality of life. However, many people only see their chiropractor when they have a problem like pain or immobility. What they don�t realize is that they may have prevented the issue had they been undergoing regular chiropractic adjustments.
Just as they can prevent serious dental issues when they undergo regular dental check-ups.
The Importance of Regular Dental Exams
Most people get regular dental exams each year without know all of the reasons why it is so important. Dental care is more than just caring for teeth; it is a crucial part of caring for your health.
Dental visits help you maintain healthy teeth and gums. Gum disease and poor dental health have been linked to a variety of health issues, including heart disease. Researchers have drawn a direct line between tooth loss and heart disease. What�s more, regular oral exams and teeth cleaning can lead to the detection of early-stage medical conditions, some of which can be life-threatening which include:
Leukemia
Heart disease
Oral cancer
Diabetes
Kidney disease
Pancreatic cancer
Studies show that these and other systemic diseases have some oral manifestation such as dry mouth, swollen gums, excessive gum problems, and mouth ulcers.
In the long run, good oral care that includes regular dental exams can save you a lot of time and money because you will catch many problems before they get out of hand and can incur significant expense.
The Importance of Regular Chiropractic Adjustments
Regular chiropractic adjustments help to keep the body in balance which allows the organs to function more efficiently. What�s more, regular chiropractic treatments put you in frequent, close contact with a health professional who can spot potential problems or the early stages of chronic diseases.
The benefits extend beyond that though. Regular chiropractic care helps you stay flexible and mobile which prevents many conditions that are related to aging. It also naturally treats a myriad of health conditions including:
Back pain
Blood pressure
Arthritis
Headaches
Joint pain
Ear infections
Asthma
Neck pain
Scoliosis
It also improves organ function and can help you avoid surgery and provides a natural, healthy alternative to medications that can be addictive and have harmful side effects.
Another added benefit of chiropractic care is the whole-body approach to wellness. Your chiropractor will look at your lifestyle, habits, diet, and exercise regimen and recommend changes and modifications that will help you live a healthier, fuller life.
Sure, they are there to help when you have a problem such as pain, but, like your dentist, they can also be the front line to better health care decisions and a healthier you. The natural approach that chiropractors take to healthcare also means that they typically see issues from a different perspective and may pick up on clues that your medical doctor might miss.
So, while you are scheduling your next dental check-up, make it a point to visit your chiropractor as well and talk to him or her about creating a plan for regular chiropractic adjustments. Your body will thank you, and you will find that you are healthier for it.
After a slip-and-fall accident,�Aracely Norte was limited�in her ability to work, that affected her quality of life. Due to chronic pain, Aracely had difficulty engaging in regular, everyday responsibilities. After hearing about El Paso, TX. Chiropractor, Dr. Alex Jimenez, from her lawyer, Aracely found relief from her chronic pain. Aracely describes how Dr. Jimenez cared for her injuries while he educated her about her health issues and the treatment he provided her with. Aracely highly recommends Dr. Jimenez as the non-surgical choice for chronic pain. Chronic pain is a common issue which can occur due to a variety of reasons, including injuries and underlying conditions, however, chiropractic care can help eliminate chronic pain symptoms.�
Chiropractic Rehab
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life that is fulfilled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life. I have made a life of taking care of every one of my patients.
I assure you, I will only accept the best for you�
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend�us.
Asthma is a chronic lung disease that is marked by narrowing and inflammation in the airways. The condition causes recurring periods of symptoms that include shortness of breath, wheezing, coughing, and tightness in the chest. It often starts in childhood, but it affects people of all ages and adults can suddenly experience an asthma attack. According to the American Academy of Allergy, Asthma, and Immunology (AAAI), approximately one in 12 people in the United States have asthma � and that number is growing each year.
Causes of Asthma
Doctors do not know why some people have asthma while others do not. Research suggests that genetics, environmental factors, or a combination of the two likely play some part in it.
Certain substances and irritants can trigger asthma attacks. These are often the same triggers for allergies since asthma and allergies often go hand in hand. Asthma triggers usually vary from person to person, but some of the more common ones include:
Cold air
Stress and strong emotions.
Airborne substances � Particles of cockroach waste, pollen, mold spores, dust mites, and pet dander.
Certain medications � Naproxen, beta-blockers, ibuprofen, and aspirin.
Physical activity � Exercise or physical labor.
Gastroesophageal reflux disease (GERD)
Respiratory infections � Allergies, cold, and bronchitis.
Air pollutants and irritants -Perfume, smoke, and air fresheners.
Additives in some foods � Preservatives, sulfites, additives added to processed potatoes, shrimp, beer, dried fruit, and wine.
Treatments for Asthma
Prevention of asthma attacks has proven to be the most effective method for managing asthma. It is essential for patients to learn to recognize their triggers so they can avoid them. If known to them they can take steps to minimize the attack. This involves tracking your breathing to ensure that your medication is adequately keeping symptoms at bay. However, most asthmatics carry a quick-relief inhaler for emergencies because sometimes prevention is not enough.
There are two types of asthma control medications: long-term and quick relief. The most common asthma medications for each type include:
Long-term
Combination inhalers
Inhaled corticosteroids
Long-acting beta agonists
Theophylline
Leukotriene modifiers
Quick-relief
Ipratropium
Short-acting beta agonists
Oral and intravenous corticosteroids
Allergy medications are an effective asthma treatment. Immunotherapy, or allergy shots, can lead to a decreased immune response to allergens. It can take a while for this to build up so the patient could be waiting for a long time. Omalizuman, or Xolair, is also an injection that is specifically for people with severe allergies or asthma
Chiropractic for Asthma
Regular chiropractic care can be very effective in treating asthma. Some studies have shown that it is effective in adult asthma as well as children with asthma.
One primary reason is that poor spinal health can contribute to an asthmatic condition. When the body is out of alignment, and it puts pressure on the sensitive nerves along the spinal column it can cause serious health problems throughout the body.
Chiropractic�s approach to whole body wellness, coupled with good spinal health and you have an asthma treatment that works.
The chiropractor may also make recommendations to the patient regarding certain lifestyle changes like advising them to stop smoking. He or she may also recommend certain foods that lower the amount of inflammation in the body and to reduce their contact with things in their environment that may be asthma triggers.
They will work with the patient to create a plan that will strengthen the immune system, minimize allergic responses, and decrease the instances of asthma attacks so that the patient can live a full, quality life.
Gartland classification grades minimally displaced subtle injuries treated with simple immobilization vs. posterior elbow dislocation treated operatively
A potential risk of ischemic compromise if care is delayed (Volkmann contracture)
The Radiological exam is crucial: sail sign & posterior fat pad sign with anterior humeral line failed to intersect mid/2/3 of Capitellum.
Incomplete pediatric Fx:
Most in <10 y.o. Greenstick, Torus, Plastic aka Bowing deformity
Typically heal well, treated conservatively with immobilization
Plastic deformity if >20-degrees requires closed reduction
Ping pong skull fracture may develop following trauma, forceps delivery and complications of birth trauma. May need to be assessed by the pediatric neurosurgeo.n
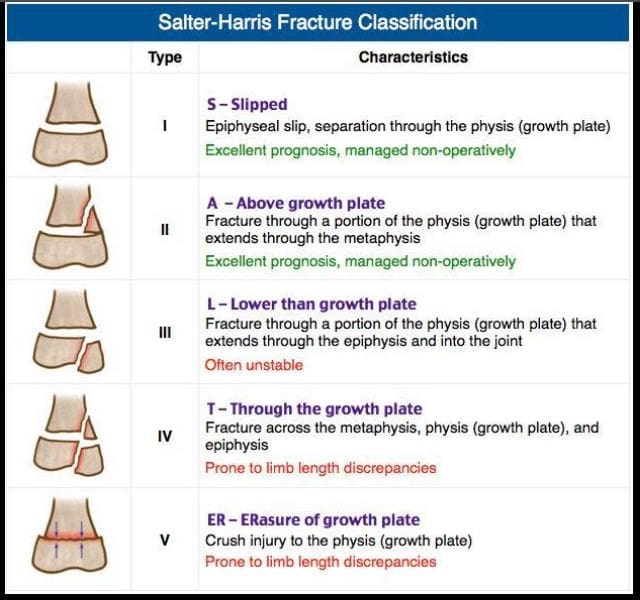
Salter-Harris types of physeal growth plate injuries
Type 1-slip. e.g., Slipped Capital Femoral Epiphysis. Typically no bone fracture noted
Type 2-M/C with good prognosis
Type 3- intra-articular, thus carries the risk of premature osteoarthritis and may require operative care d/t being unstable
Type 4- Fx through all regions about the physis. Unfavorable prognosis and limb shortening
Type 5- often no evidence of actual bone fracture. Poor prognosis d/t crush injury and vascular damage with limb shortening
Imaging evaluation is crucial
Non-Accidental Injury (NAI)in Children
There different forms of child abuse. Physical abuse may range from skin injuries to different MSK/systemic injuries affecting bones and soft tissues. Imaging is crucial and may identify definite signs alerting medical providers and informing child protection services and law enforcement agencies about physical abuse.
In an infant: �shaken baby syndrome� may present with CNS signs d/t tearing of immature bridging vein and subdural hematoma which can be fatal. Retinal hemorrhaging often a clue. Head CT is crucial.
MSK Radiological Red Flags:
1) major bone Fx in an un-ambulatory very young child (0-12 m.o.)
2) Posterior ribs Fx: naturally never occur d/t accidents. Most likely mechanisms: grabbing and squeezing a child or direct hit.
3) Multiple Fractures with different chronological healing rates, i.e., bone calluses indicating repeated physical trauma
4) Metaphyseal corner Fx aka Bucket handle Fx, often pathognomonic for NAI in children. Occurs when the affected extremity is held and violently twisted.
5) Spiral fracture of long bones in a young child is another example of NAI.
Other important clues of NAI. Inconsistent history provided by guardians/caregivers. No evidence of congenital/metabolic bone abnormalities like Osteogenesis Imperfecta or Rickets/osteomalacia etc.
N.B. When child�s guardians state a history that reports fall and accidents in the house, It is important to know that apparently most accidents/falls in the house are very rarely or unlikely result in major bone fractures.
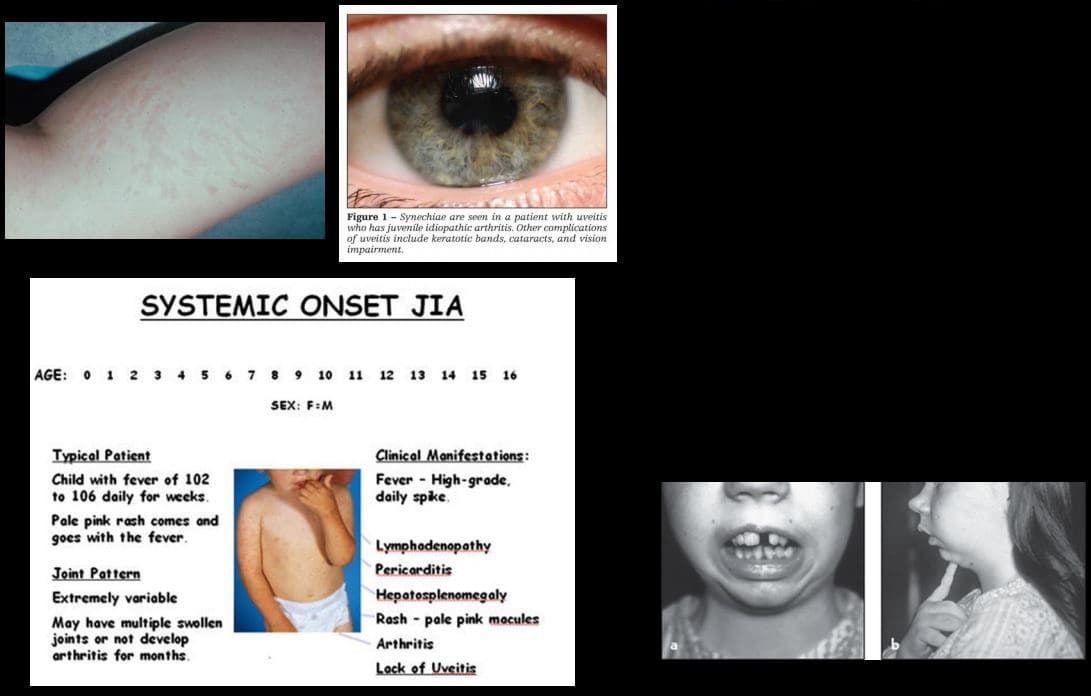
Juvenile Idiopathic Arthritis (JIA)-considered M/C chronic disease of childhood. Clinical Dx: joint pain/swelling for 6-weeks or longer in a child <16-y.o. Different forms exist: Early Dx is crucial to prevent delayed complications
Most familiar forms of JIA:
1) Pauciarticular disease (40%)- m/c form of JIA. Girls are at greater risk. Presents as arthritis in <4 joints: knees, ankles, wrist. Elbow. This type shows high association with ocular involvement as iridocyclitis (25%) that may potentially lead to blindness. Labs: RF-ve, ANA positive.
2) Polyarticular disease (25%): RF-ve. Girls are at greater risk. Affects small and large joints often affect Cervical spine
3) Systemic form of JIA (20%): often presents with acute systemic manifestation as spiking fevers, arthralgias, myalgias, lymphadeno[pathy, hepatosplenomegaly, polyserositis (pericardial/pleural effusion). Important Dx features characteristic evanescent salmon pink rash on the extremities and trunk. The Systemic form has a distinct lack of ocular involvement. Joints typically shoe no erosions compared to other types. Thus joint destruction is not typically seen
Imaging in JIA
Joint effusion bone overgrowth squaring of patella cartilage/bone erosion superimposed DJD
Fingers and long bones early physeal closure/limb shortening
Rad DDx knee/ankle: Hemophilic arthropathy Rx: DMARD.
Osteosarcoma (OSA) & Ewing�s sarcoma (ES) are 1 st and 2nd M/C primary malignant bone neoplasms of childhood (peak at 10-20 y.o.) Clinically: bone pain, change in activity, early metastasis especially pulmonary mets may occur. Poor prognosis
Ewing�s may present with bone pain, fever and elevated ESR/CRP mimicking infection. Early Dx with imaging and staging are crucial.
Imaging of OSA & ES: x-ray, followed by MRI, chest CT, PET/CT. On x-rays: OSA may affect any bone but most present as aggressive bone forming neoplasms about the knee (50% cases) especially as osteoid forming an aggressive lesion in the metaphysis with speculated/sunburst periostitis & Codman triangle. Marked soft tissue invasion.
ES may present in the shaft and show very early soft tissue spread. MRI is crucial to reveal the extent of bone and ST invasion, MRI required for surgical planning
OSA & ES Rx: A combination of surgery, radiation, chemo. Limb salvage techniques are performed in some cases. Poor prognosis if detected late.
Imaging of Ewing�s sarcoma
Permeating bone distraction
Early and extensive soft tissue invasion
Aggressive periosteal reaction with laminated (onion skin) response
Saucerisation of cortical bone (orange arrow)
A Lesion is typically diaphyseal with some metaphyseal extension
Known as Round cell tumor along with Multiple Myeloma and Lymphoma
Common Childhood Malignancies
Neuroblastoma (NBL) M/C malignancy of infancy. Derives from neural crest cells aka PNET tumors (e.g., sympathetic ganglia). Most occur in children <24-months. Some show good prognosis but >50% cases present with advanced disease. 70-80% at age 18-months or older present with advanced metastasis. NBL may develop in the adrenal medulla, sympathetic ganglia and other location. Presents as an abdominal mass, vomiting. >50% presents with bone pain d/t metastasis. Clinically: physical exam, labs, imaging: chest and abd x-rays, CT abdomen and chest is crucial to Dx. MRI may help. NBL may metastasize to the skull and infiltrate sutures with a characteristic presentation as pathological sutural diastasis.
Acute Lymphoblastic Leukemia is the m/c malignancy of childhood. Pathology: leukemic cell infiltration of bone marrow leading to bone pain and replacement of other normal marrow cells with anemia, thrombocytopenia, neutropenia and associated complications. Leukemic cells may infiltrate other sites including CNS, spleen, bone and other regions. Dx: CBC, serum lactate dehydrogenase levels, Bone marrow aspiration biopsy is the key. Imaging may help but not essential to diagnosis. On radiography, leukemic infiltration of the bone may typically appear as radiolucent bands along the physeal growth plate. Rx: chemotherapy and treating complications
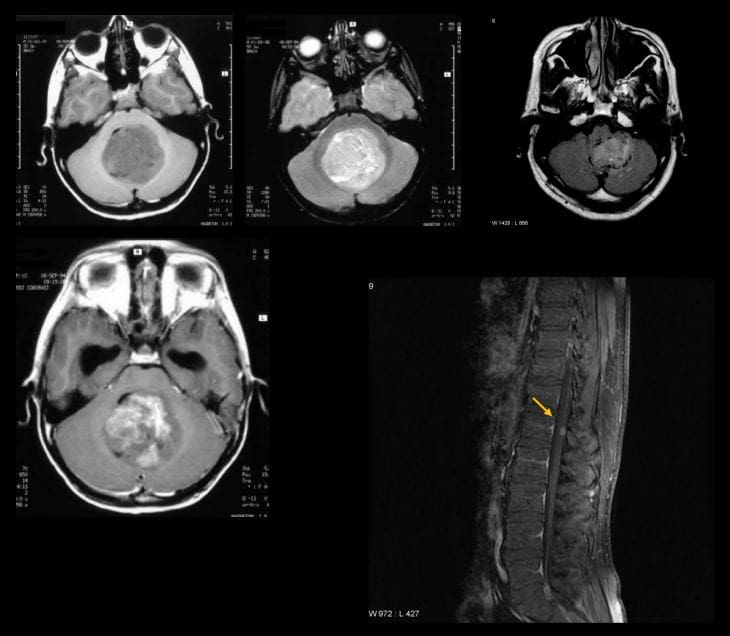
Medulloblastoma: M/C malignant CNS neoplasm in children
Majority develop before 10-y.o.
M/C location: cerebellum and posterior fossa
Histologically represents a PNET type tumor not a glioma as was originally thought
MBL, as well as Ependymoma and CNS lymphoma, may lead to drop metastasis via CSF and additionally represent a unique that unlike other CNS tumors demonstrate metastatic spread outside CNS, m/c to the bone
50% of MBL may be fully resectable
If Dx and treatment begin before metastasis, 5- year survival is 80%
Imaging is crucial: CT scanning may be used but the imaging modality of choice is MRI that will additionally provide a more superior evaluation of the entire neuraxis for metastasis.
MBL typically appears as heterogenous hypo, iso and hyperintense lesion on T1, T2 and FLAIR scans (top images) if compare to surrounding brain tissue. Often compressing 4th ventricle with obstructive hydrocephalus. The tumor typically shows contrast enhancement on T1+C gad (bottom left image). Drop metastasis from MBL with T1+C enhancing lesion in the cord
Important Pediatric Infections
In the neonate/infant <1month: fever >100.4 (38C) may indicate bacterial and some viral infection. Strep B, Listeria, E. Coli may lead to sepsis, meningitis. Approach: chest x-ray, lumbar puncture with culture, blood culture, CBC, urinalysis.
In young children, Hemophilus influenza type B (HIB) may lead to Epiglottitis a rare but serious complication. The current vaccine helps to reduce the number of cases of Epiglottitis and other HIB related illnesses.
Parainfluenza or RSV virus may lead to Croup or acute Laryngotracheobronchitis.
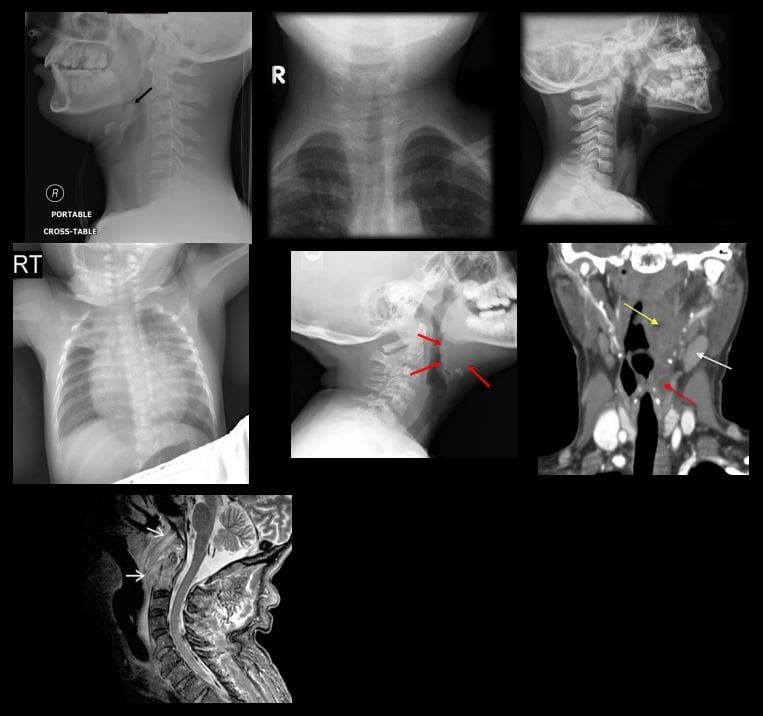
Epiglottitis and Croup are Dx clinically but AP and lateral soft tissue neck x-rays are very helpful
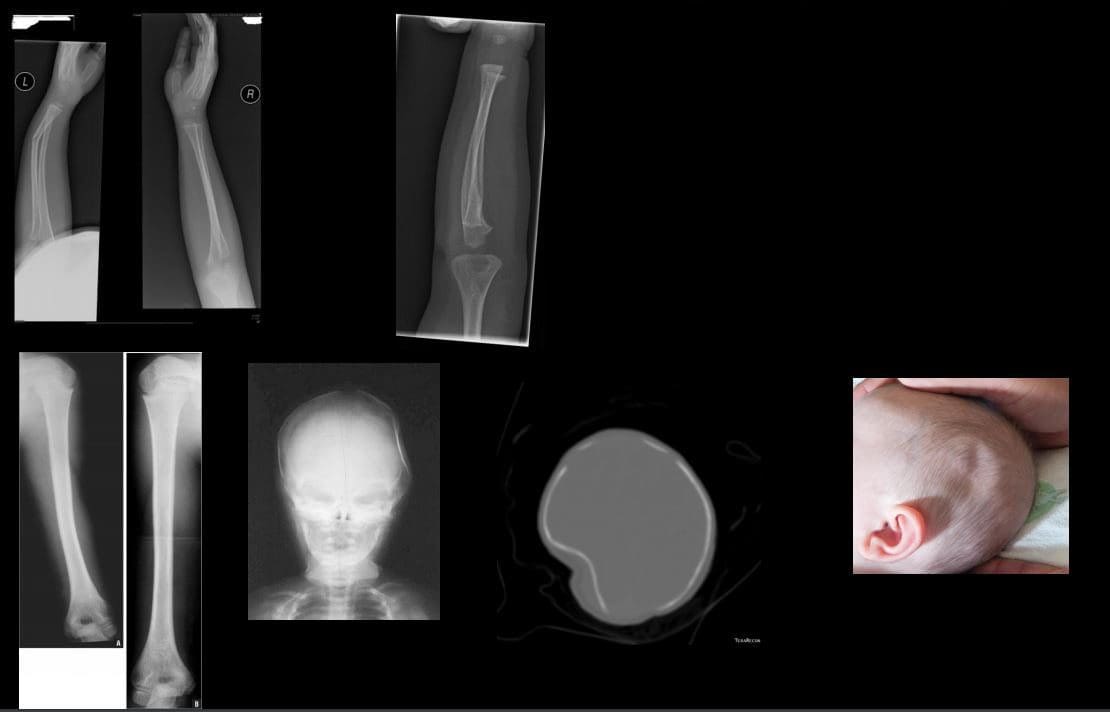
Epiglottitis presents with a characteristic �thumb sign� that is consistent with thickened epiglottis d/t epiglottic edema. This can be a life-threatening emergency compromising airways (top left)
Croup may show a �steeple sign� or �wine bottle sign� with distended hypopharynx as acute narrowing of subglottic airway on AP and lateral neck soft tissue x-ray (top right)
Respiratory Syncytia Virus (RSV) and influenza may lead to viral pneumonia potentially with life-threatening complications in the immunocompromised, very young and children with comorbidities. CXR is crucial (middle left)
Streptococcal pharyngitis with GABHS infection may lead to some acute or delayed complications (e.g., Rheumatic fever)
Peritonsillar abscess (above middle right) may develop in some cases and be complicated by spreading along soft tissue planes in the neck potentially leading to spread into sublingual/submandibular spaces (Ludwig Angina) when airways need to be controlled d/t base of tongue edema
Development of a retropharyngeal abscess may potentially lead to spread of the infection through freely communicating neck fascia resulting in necrotizing mediastinitis, Lemmier syndrome and invasion of carotid spaces (all are potentially life-threatening complications)
Griesel syndrome- (above bottom left) rare complication of regional tonsillar/pharyngeal oral infections that can spread to prevertebral space leading to C1-2 ligaments laxity and instability
Other important infections in children are typical bacterial (Pneumococcal) pneumonia, Urinary tract infection and Acute Pyelonephritis (especially in girls) and Meningococcal Meningitis
Pediatric Metabolic Disease
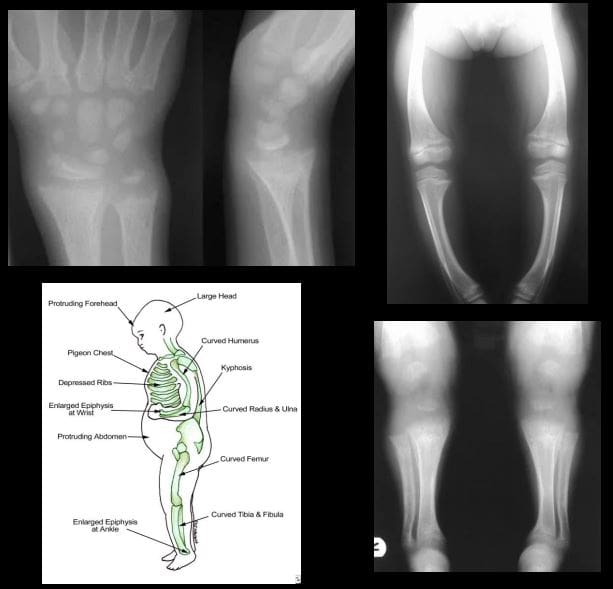
Rickets: considered osteomalacia in skeletally immature. Zone of provisional calcification of the epiphyseal growth plate is particularly affected
Clinically presents with growth retardation, extremity bowing, rachitic rosary, pigeon chest, depressed ribs, enlarged and swollen wrists, and ankles, skull deformity
Pathology: Vit D and calcium abnormality is the m/c cause. Lack of sun exposure esp. dark-skinned individual, restrictive clothing to light exposure, prolonged exclusive breastfeeding, veganism, malabsorption syndromes of the gut, renal damage and others
Imaging: frayed metaphysis aka paint brush metaphysis with flaring, widening of the growth plate, bulbous costochondral junction as a rachitic rosary, extremity bowing
Rx: treat underlying causes, correct nutritional deficit, etc.
Chronic pain is one of the most prevalent conditions in the United States, affecting an estimated 100 million Americans each year. To put that into perspective, that�s more than the number of people suffering from cancer, heart disease, and diabetes, combined.
Many of these chronic pain sufferers are looking for relief beyond pharmaceuticals which can have unpleasant and even harmful side effects. This has brought them to natural pain management methods like chiropractic care as well as natural substances like curcumin. For many people, these treatment options have brought them relief from the pain and help them return to a more normal lifestyle.
How does it work though? And, more importantly, can it work for you?
What is Curcumin?
Natural herbal turmeric capsules with fresh herb leaves and dry curcumin in paper
Curcumin is a spice that is a relative of ginger and is a component of turmeric. Often in the U.S., the terms curcumin and turmeric are used interchangeably. However, curcumin is what gives turmeric its bright yellow color.
While it is often found in curries and other traditional Indian food, it has also long been used to treat a variety of health issues including inflammation that causes pain in the body. These claims have been backed up by several studies that show the tasty spice has tremendous health benefits to offer.
These studies have shown that curcumin has strong anti-inflammatory properties although why it works is not yet completely understood. This information has prompted further studies to determine the efficacy of curcumin in treating a wide range of conditions including chronic pain.
One study examined the spice�s effects on people suffering from arthritis or joint pain. The results determined that turmeric extract (curcumin) supplements were just as effective as ibuprofen in relieving the pain in patients with knee osteoarthritis. It helped to reduce the inflammation that was causing the pain, bringing the patients much-needed relief.
Taking Curcumin for Better Health
You can get curcumin or turmeric supplements, but there is no standard dosage information available. Your chiropractor can advise you on how much to take and which supplement brands are the best.
You can also use the spice in the foods you eat and gain a good bit of the health properties that way. However, it may be more efficient and more comfortable to take curcumin or turmeric supplements, especially when you are treating inflammation and pain.
Curcumin is generally safe with very few side effects. As with any medication or supplement, some people are sensitive to the spice and may experience diarrhea and nausea.
However, that usually occurs at higher doses or after the patient has been using it for a long time. High doses could also pose a risk if the person has ulcers. It can also irritate the skin is applied topically.
If you are considering incorporating curcumin into your daily diet as a health supplement, you should first talk to your doctor or chiropractor to make sure it is safe for you. Women who are pregnant or nursing should not take the supplements.
People with conditions like diabetes, gallbladder issues, bleeding disorders, kidney disease, or immunity problems should take special care when using the supplement. Also, it can interact with medications like NSAIDs, aspirin, diabetes drugs, statins, blood thinners, and blood pressure medications so talk to your health professional, such as your chiropractor, before taking. They may adjust your dosage or recommend certain nutritional therapies to better support the supplement.
Your chiropractor can help you live a more natural, pain-free life and supplements like curcumin may be a part of that plan. They can help put you on the path to a life well lived.
Why is it that the ketogenic diet and intermittent fasting always seem to fall within the same topic of conversation? This is simply because intermittent fasting may be utilized as an instrument to achieve ketosis, the metabolic state associated with the keto diet. During intermittent fasting, the human body is depleted of glycogen stores. Once these glycogen stores are eliminated, fat stores are then released into the bloodstream in order to be converted into energy molecules, known as ketones, from the liver.
What is Ketosis?
Ketosis is a metabolic state which uses ketone bodies, or ketones, as fuel for energy. On a normal carbohydrate-based diet, the human body burns glucose as its main fuel source, where excess glucose is subsequently stored as glycogen. If the human body cannot utilize sugar as fuel for energy, it will utilize glycogen as fuel for energy. Once glycogen is depleted, you begin to burn fat. The ketogenic diet generates a metabolic state which enables you to break down fat into ketones, or ketone bodies, in the liver for energy.
There are 3 major types ketone bodies found in the blood, urine, and breath, including:
Acetoacetate: The type of ketone which is created first. It may be converted to beta-hydroxybutyrate or flipped into acetone.
Acetone: Made spontaneously in the breakdown of acetoacetate. It is a very volatile ketone and it is frequently detectable on the breath once an individual first enters ketosis.
Beta-hydroxybutyrate (BHB): The type of ketone which is utilized for energy and is most abundant on the bloodstream as soon as you’re completely into ketosis. It is the kind that is located in exogenous ketones and what blood tests quantify.
Intermittent Fasting in the Keto Diet
Intermittent fasting is composed of eating within a specific feeding window rather than eating throughout the day. Each individual, whether they are conscious of it or not, fasts intermittently from dinner to breakfast. There are lots of methods to intermittent fasting. A few individuals fast for 16-20 hours intervals on alternate days while others follow a 24-hour day fast. The most common intermittent fasting variety is the 16/8 method, in which you eat in an 8-hour window followed by a 16-hour fasting window.
Other fasting programs incorporate the 20/4 or even 14/10 methods. Other people follow 24-hour fasts one or two times each week. Intermittent fasting can get you in ketosis quicker because your cells will immediately absorb your glycogen stores and begin burning fat. However, what about once you get into ketosis? Is intermittent fasting worth following consistently? Following the ketogenic diet and intermittent fasting can be a great addition towards an individual’s overall health and wellness, providing various health benefits.
The keto diet and intermittent fasting can provide the following health benefits, including:
Healthy weight-loss
Fat reduction, not muscle reduction
Balancing cholesterol levels
Enhancing insulin sensitivity
Maintaining blood glucose levels steady
Health Benefits of the Ketogenic Diet
The ketogenic diet dramatically reduces your caloric intake, forcing your body to burn fat instead of sugar, which makes it a powerful tool for weight reduction. While individual results vary, the keto diet has always resulted in a decrease in body fat in a selection of situations. Within a 2017 study, subjects who followed a very low carbohydrate keto meal program significantly decreased body fat percentage and body fat mass, losing an average of 7.6 lbs and 2.6 percent body fat while preserving lean muscle mass.
Likewise, a 2004 research detecting the long-term consequences of a ketogenic diet in overweight patients discovered that the weight and body mass of those patients diminished dramatically over the span of two decades. Individuals who radically reduced their carb intake saw a substantial decline in LDL (bad) cholesterol, triglycerides, and enhanced insulin sensitivity. In 2012, researchers compared a ketogenic diet to eating fewer calories for overweight kids and adults. The results showed kids after the keto diet lost significantly more body fat. They also revealed a dramatic decline in insulin levels, a biomarker of Type 2 diabetes.
Health Benefits of Intermittent Fasting
Studies have shown that intermittent fasting may be an effective weight loss tool, more powerful than just cutting calories. In one analysis, intermittent fasting has been proven to be as successful as constant calorie restriction in combating obesity. In studies done by the NIH, there was reported weight reduction with over 84 percent of participants, regardless of which fasting program they picked.
Much like ketosis, intermittent fasting increases fat loss while preserving lean muscle mass. In one study, researchers reasoned that fasting led to greater weight loss compared to a low-carb diet, though the overall caloric consumption was exactly the same. If you are attempting to lose weight, then a keto diet or intermittent fasting can be a massive help. But that is not where the rewards stop.
Intermittent Fasting and the Keto Diet for Mental Health
Both intermittent fasting and the ketogenic diet can provide various mental health advantages. Both have been clinically shown to boost memory, improve mental clarity and focus, as well as prevent the development of neurological disorders like Alzheimer’s and epilepsy. On a carb-based diet, changes in glucose can cause changes in energy levels. During ketosis, your brain employs a more consistent supply of fuel: ketones from the fat stores, leading to better productivity and psychological performance.
Whenever you’ve got a consistent and clean energy source from ketones, the brain works better. In addition to this, ketones are better at protecting your brain. Studies reveal that ketone bodies might have antioxidant properties which protect your brain cells from free radicals and oxidative stress. In one study conducted on adults with diminished memory, the growth of BHB ketones in their own blood helped enhance cognition. Also, when you’ve got difficulty staying focused, your hormones can be to blame.
Your brain has two chief neurotransmitters: glutamate and GABA. Glutamate will help you form new memories, and get your brain cells to communicate with one another. GABA is what helps restrain glutamate. If there is too much glutamate, it can cause brain cells to quit working and finally perish. GABA is there to control and slow down glutamate. If GABA levels are reduced, glutamate reigns free and you experience mental fog. Ketones stop damage to cells by processing surplus glutamate into GABA. Considering that ketones raise GABA and lessen glutamate, they assist in preventing cell damage, preventing cell death and enhancing mental focus.
Researchers believe that intermittent fasting enhances memory, decreases oxidative stress, and conserves learning abilities. Since your cells are under moderate strain whilst fasting, the top cells adapt to the stress by improving their particular ability to deal with these circumstances while the weakest tissues die. This is much like the strain that your body gets when you reach the gym.
Exercise is a kind of stress that your body adjusts to improve and get more powerful. This also applies for intermittent fasting: so long as you are still alternate between routine eating habits and fasting, it is going to continue to benefit you. Implying equally that ketosis and intermittent fasting will help improve your cognitive functioning because of the synergistic and protective effects of ketones.
The ketogenic diet and intermittent fasting are two different nutritional strategies which provide many common health benefits. According to various research studies, both the keto diet and intermittent fasting can help boost ketones, helping the body burn fat more efficiently than any other nutritional strategy. And when these are utilized together, they definitely form a powerful dietary program. The article above discusses the differences between the ketogenic diet and intermittent fasting as well as demonstrates the health benefits of both of these dietary programs and how they can help improve overall health and wellness. Dr. Alex Jimenez D.C., C.C.S.T. Insight
The Perks of Intermittent Fasting and the Keto Diet
The ketogenic diet and intermittent fasting possess similar health benefits because both approaches involve ketosis. Ketosis has lots of physical and mental advantages, from weight loss to enhanced brain function. People following a ketogenic diet may use intermittent fasting as a tool to achieve ketosis and enhance their general well-being. The scope of our information is limited to chiropractic and spinal health issues. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion:�Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief. �
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine