Nutraceutical Supplements, Nutrition: And Treatment Of Hypertension
Nutraceutical Abstract:
Vascular biology, endothelial and vascular smooth muscle and cardiac dysfunction play a primary role in the initiation and perpetuation of hypertension, cardiovascular disease and target organ damage. Nutrientgene interactions and epigenetics are predominant factors in promoting beneficial or detrimental effects in cardiovascular health and hypertension. Macronutrients and micronutrients can prevent, control and treat hypertension through numerous mechanisms related to vascular biology. Oxidative stress, inflammation and autoimmune dysfunction initiate and propagate hypertension and cardiovascular disease. There is a role for the selected use of single and component nutraceutical supplements, vitamins, antioxidants and minerals in the treatment of hypertension based on scientifically controlled studies which complement optimal nutrition, coupled with other lifestyle modifications.
Key words: Hypertension; Nutrition; Nutritional supplements;
Cardiovascular disease; Vascular biology
Core tip: Vascular biology and endothelial dysfunction
play a primary roles in hypertension and subsequent cardiovascular disease. Micronutrients, macronutrients and optimal nutrition and nutritional supplements can
prevent, control and treat hypertension through numerous mechanisms related to vascular biology. These treatments are complementary to drug therapy. Oxidative
stress, inflammation and autoimmune dysfunction initiate and propagate hypertension and cardiovascular disease. There is a role for the selected use of single and component nutraceutical supplements, vitamins, antioxidants and minerals in the treatment of hypertension based on scientifically controlled studies which complement optimal nutrition, coupled with other lifestyle modifications.
Nutraceutical Introduction:
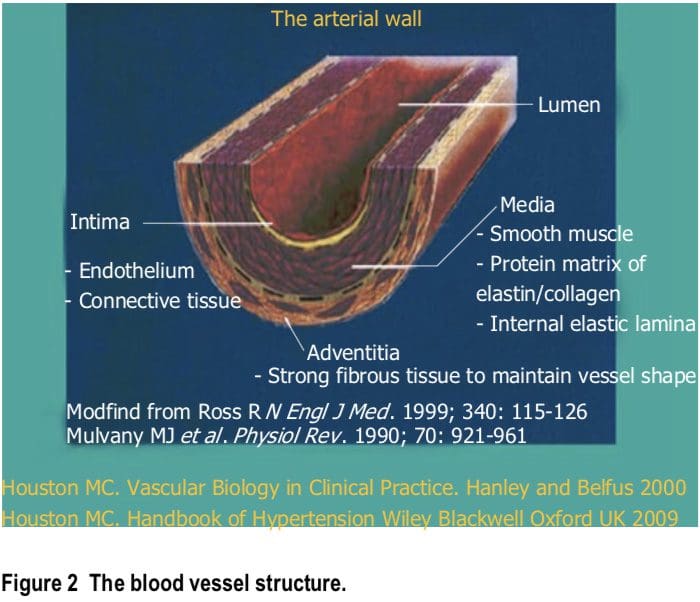
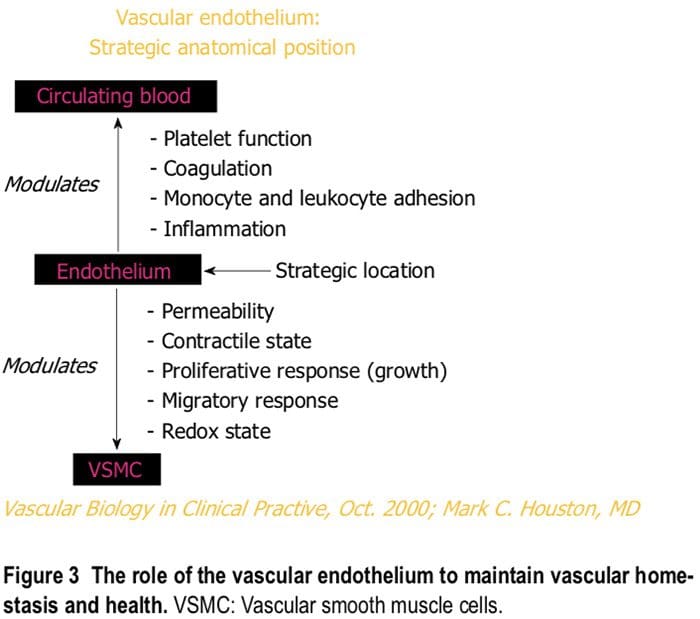
Vascular disease is a balance between vascular injury and repair (Figure 1). The endothelium is in a strategic location between the blood and the vascular smooth muscle
and secretes various substances to maintain vascular homeostasis and health (Figures 2 and 3). Various insults that damage the endothelium, lead to endothelial dysfunction
(ED) and may induce hypertension and other cardiovascular diseases. Hypertension may be a hemodynamic marker of injured endothelium and vascular smooth muscle related to finite responses of inflammation, oxidative stress and immune dysfunction of the arteries leading to ED, vascular and cardiac smooth muscle dysfunction, loss of arterial elasticity with reduced arterial compliance and increased systemic vascular resistance. Hypertension
is a consequence of the interaction of genetics and environment. Macronutrients and micronutrients are crucial in the regulation of blood pressure (BP) and subsequent�target organ damage (TOD). Nutrient-gene interactions, subsequent gene expression, epigenetics, oxidative stress, inflammation and autoimmune vascular dysfunction have positive or negative influences on vascular biology in humans. Endothelial activation with ED and vascular smooth muscle dysfunction (VSMD) initiate and perpetuate essential hypertension.
 Macronutrient and micronutrient deficiencies are very common in the general population and may be even more common in patients with hypertension and cardiovascular
Macronutrient and micronutrient deficiencies are very common in the general population and may be even more common in patients with hypertension and cardiovascular
disease due to genetics, environmental causes and prescription drug use. These deficiencies will have an enormous impact on present and future cardiovascular
health outcomes such as hypertension, myocardial infarction (MI), stroke and renal disease. The diagnosis and treatment of these nutrient deficiencies will reduce BP
and improve vascular health, ED, vascular biology and cardiovascular events.
EPIDEMIOLOGY
Epidemiology underscores the etiologic role of diet and associated nutrient intake in hypertension. The transition from the Paleolithic diet to our modern diet has produced
an epidemic of nutritionally-related diseases (Table 1). Hypertension, atherosclerosis, coronary heart disease (CHD), MI, congestive heart failure (CHF), cerebrovascular
accidents (CVA), renal disease, type 2 diabetes mellitus (T2DM), metabolic syndrome (MS) and obesity are some of these diseases[1,2]. Table 1 contrasts intake of nutrients involved in BP regulation during the Paleolithic Era and modern time. Evolution from a pre-agricultural, hunter-gatherer milieu to an agricultural, refrigeration society has imposed an unnatural and unhealthful nutritional selection process. In sum, diet has changed more than our genetics can adapt.
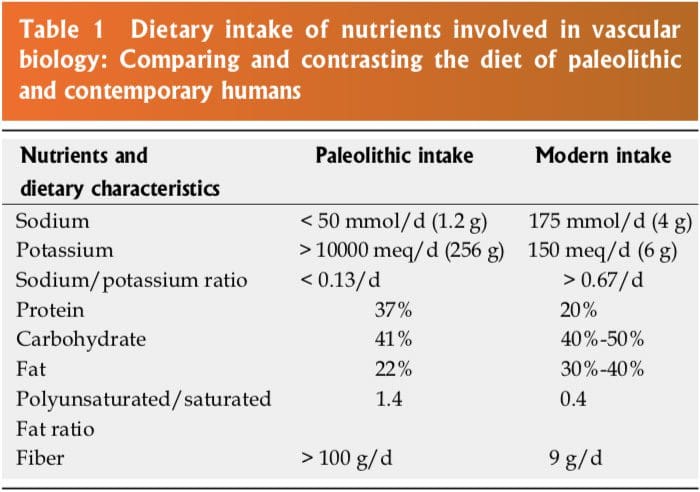 The human genetic makeup is 99.9% that of our Paleolithic ancestors, yet our nutritional, vitamin and mineral intakes are vastly different[3]. The macronutrient and micronutrient variations, oxidative stress from radical oxygen species (ROS) and radical nitrogen species (RNS) and inflammatory mediators such as cell adhesion molecules (CAMs), cytokines, signaling molecules and autoimmune vascular dysfunction of T cells and B cells, contribute
The human genetic makeup is 99.9% that of our Paleolithic ancestors, yet our nutritional, vitamin and mineral intakes are vastly different[3]. The macronutrient and micronutrient variations, oxidative stress from radical oxygen species (ROS) and radical nitrogen species (RNS) and inflammatory mediators such as cell adhesion molecules (CAMs), cytokines, signaling molecules and autoimmune vascular dysfunction of T cells and B cells, contribute
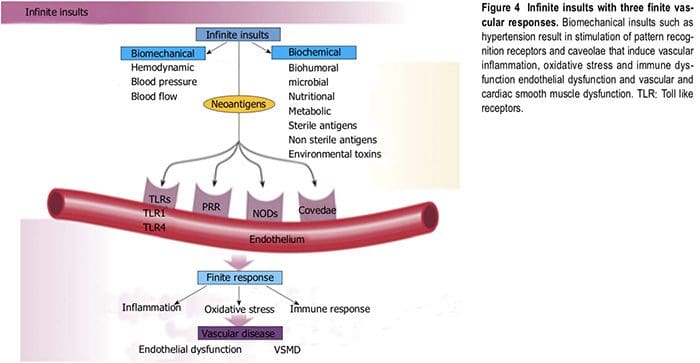
to the higher incidence of hypertension and other cardiovascular diseases through complex nutrient-gene interactions, epigenetic and nutrient-caveolae interactions and nutrient reactions with pattern recognition receptors [toll like receptors (TLR) and nod like receptors] in the endothelium[4-9] (Figure 4). Reduction in nitric oxidebioavailability, increase in angiotensin ? and endothelin coupled with endothelial activation initiate the vascular and cardiac dysfunction and hypertension. Poor nutrition, coupled with obesity and a sedentary lifestyle have resulted in an exponential increase in nutritionally-related
diseases. In particular, the high Na+/K+ ratio of modern diets has contributed to hypertension, CVA, CHD, MI, CHF and renal disease[3,10] as have the relatively low intake
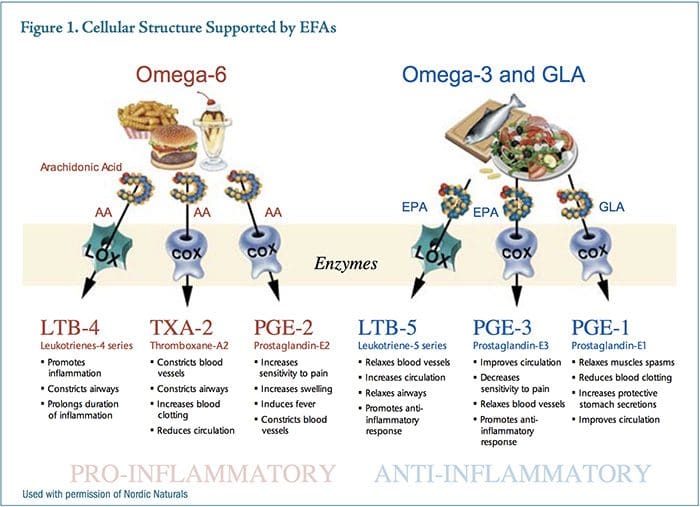
of omega-3 PUFA, increase in omega-6 PUFA, saturated fat and trans fatty acids[11].
 PATHOPHYSIOLOGY
PATHOPHYSIOLOGY
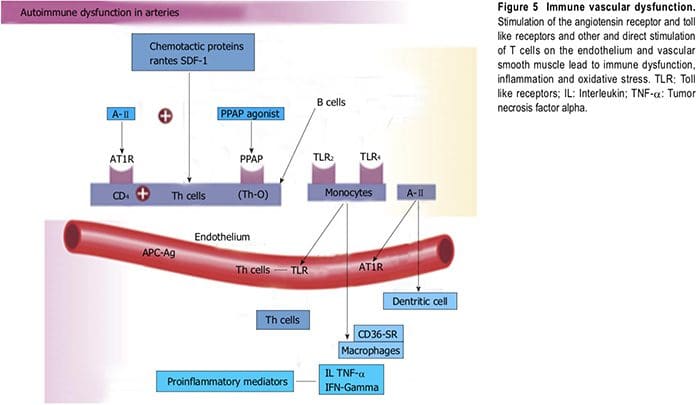
Vascular biology assumes a pivotal role in the initiation and perpetuation of hypertension and cardiovascular TOD[1]. Oxidative stress (ROS and RNS), inflammation (increased expression of redox-sensitive proinflammatory genes, CAMs and recruitment migration�and infiltration of circulating cells) and autoimmune vascular dysfunction (T cells and B cells) are the primary pathophysiologic and functional mechanisms that induce vascular disease[1,12-14] (Figure 5). All three of these are closely inter-related and establish a deadly combination that leads to ED, vascular smooth muscle and cardiac dysfunction, hypertension, vascular disease, atherosclerosis and CVD. Hypertension is not a disease but is the correct and chronically dysregulated response with an exaggerated outcome of the infinite insults to the blood vessel with subsequent environmental-genetic expression
patterns and downstream disturbances in which the vascular system is the innocent bystander. This becomes a maladaptive vascular response that was initially intended
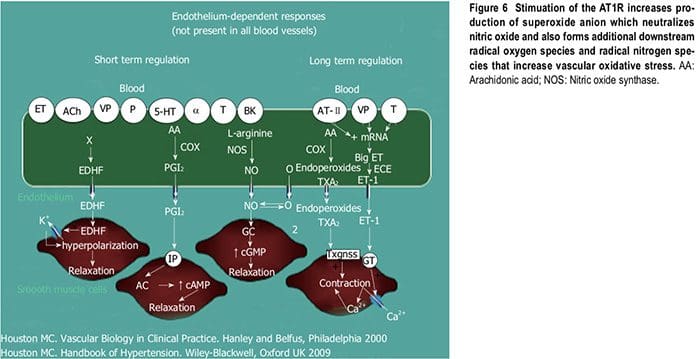
to provide vascular defense to the endothelial insults (Figure 6)[1,13-15]. Hypertension is a vasculopathy characterized by ED, structural remodeling, vascular inflammation, increased arterial stiffness, reduced distensibility and loss of elasticity[13]. These insults are biomechanical (BP, pulse pressure, blood flow, oscillatory flow, turbulence, augmentation, pulse wave velocity and reflected waves) and biohumoral or biochemical which includes all the non-mechanical causes such as metabolic, endocrine, nutritional, toxic, infectious and other etiologies[1] (Figure 4). In addition to the very well established connections for endocrine and nutritional causes of hypertension, toxins and infections also increase BP[16-20]. Various toxins such as polychlorinated biphenyls, mercury, lead, cadmium, arsenic and iron also increase BP and CVD[16,17].
 Numerous microbial organisms have been implicated in hypertension and CHD[18-20]. All of these insults lead to impaired microvascular structure and function which manifests clinically as hypertension[12-14]. The level of BP may not give an accurate indication of the microvascular involvement and impairment in hypertension. Hypertensive patients have abnormal microvasculature in the form of inward eutrophic remodeling of the small resistance arteries leading to impaired vasodilatory capacity, increased vascular resistance, increased media to lumen ratio, decreased maximal organ perfusion and reduced flow reserve, especially in the heart with decreased coronary flow reserve[12-14]. Significant functional then structural microvascular impairment occurs even before the BP begins to rise in normotensive offspring of hypertensive parents evidenced by ED, impaired vasodilation, forearm vascular resistance, diastolic dysfunction, increased left ventricular mass index, increased septal and posterior wall thickness and left ventricular hypertrophy[12,15]. Thus, the cellular processes underlying the vascular perturbations constitute a vascular phenotype of hypertension that may be determined by early life
Numerous microbial organisms have been implicated in hypertension and CHD[18-20]. All of these insults lead to impaired microvascular structure and function which manifests clinically as hypertension[12-14]. The level of BP may not give an accurate indication of the microvascular involvement and impairment in hypertension. Hypertensive patients have abnormal microvasculature in the form of inward eutrophic remodeling of the small resistance arteries leading to impaired vasodilatory capacity, increased vascular resistance, increased media to lumen ratio, decreased maximal organ perfusion and reduced flow reserve, especially in the heart with decreased coronary flow reserve[12-14]. Significant functional then structural microvascular impairment occurs even before the BP begins to rise in normotensive offspring of hypertensive parents evidenced by ED, impaired vasodilation, forearm vascular resistance, diastolic dysfunction, increased left ventricular mass index, increased septal and posterior wall thickness and left ventricular hypertrophy[12,15]. Thus, the cellular processes underlying the vascular perturbations constitute a vascular phenotype of hypertension that may be determined by early life
programming and imprinting which is compounded by vascular aging[12-14].
Oxidative Stress
Oxidative stress, with an imbalance between ROS and RNS and the anti-oxidant defense mechanisms, contributes to the etiology of hypertension in animals[10] and humans[11,12]. Radical oxygen species and RNS are generated�by multiple cellular sources, including nicotinamide adenine dinucleotide phosphate hydrase (NADPH) oxidase,
mitochondria, xanthine oxidase, uncoupled endotheliumderived nitric oxide (NO) synthase (U-eNOS), cyclooxygenase and lipo-oxygenase[11]. Superoxide anion is the predominant ROS species produced by these tissues, which neutralizes NO and also leads to downstream production of other ROS (Figure 3). Hypertensive patients have impaired endogenous and exogenous anti-oxidant defense mechanisms[21], an increased plasma oxidative�stress and an exaggerated oxidative stress response to various stimuli[21,22]. Hypertensive subjects also have lower plasma ferric reducing ability of plasma, lower vitamin C levels and increased plasma 8-isoprostanes, which correlate with both systolic and diastolic BP. Various singlenucleotide polymorphisms (SNP�s) in genes that codify for anti-oxidant enzymes are directly related to hypertension[23]. These include NADPH oxidase, xanthine
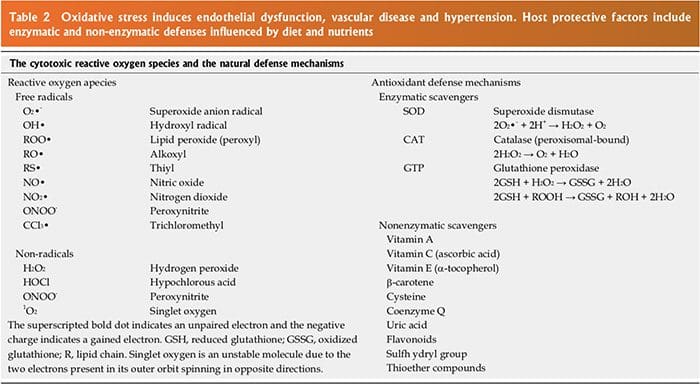
oxidase, superoxide dismutase 3 (SOD 3), catalase, glutathione peroxidase 1 (GPx 1) and thioredoxin. Antioxidant deficiency and excess free radical production have been implicated in human hypertension in numerous�epidemiologic, observational and interventional studies
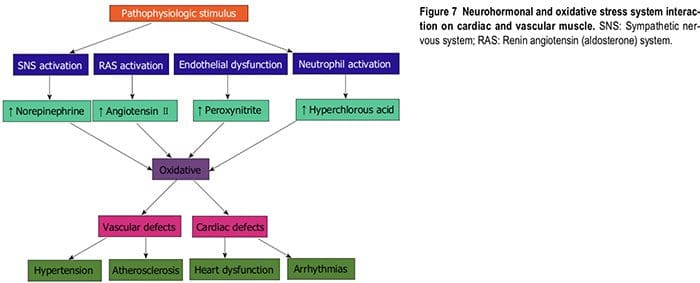
(Table 2)[21,22,24]. Radical oxygen species directly damage endothelial cells, degrade NO, influence eicosanoid metabolism, oxidize LDL, lipids, proteins, carbohydrates, DNA and organic molecules, increase catecholamines, damage the genetic machinery, influence gene expression and transcription factors[1,21,22,25,26]. The inter-relations of neurohormonal systems, oxidative stress and cardiovascular disease are shown in Figures 6 and 7. The increased oxidative stress, inflammation and autoimmune vascular dysfunction in human hypertension results from a combination of increased generation of ROS and RNS, an
exacerbated response to ROS and RNS and a decreased antioxidant reserve[24-29]. Increased oxidative stress in the rostral ventrolateral medulla (RVLM) enhances glutamatergic excitatory inputs and attenuates GABA-ergic inhibitory inputs to the RVLM which contributes to increased sympathetic nervous system (SNS) activity from the paraventricular nucleus[30]. Activation of the AT1R in the RVLM increases NADPH oxidase and increases oxidative stress and superoxide anion, increases SNS outflow causing an imbalance of SNS/PNS activity with elevation of BP, increased heart rate and alterations in
heart rate variability and heart rate recovery time, which can be blocked by AT1R blockers[30,31].
 Inflammation
Inflammation
The link between inflammation and hypertension has been suggested in both cross-sectional and longitudinal studies[32]. Increases in high sensitivity C-reactive protein
(HS-CRP) as well as other inflammatory cytokines such as interleukin-1B, (IL-1B), IL-6, tumor necrosis alpha (TNF-?) and chronic leukocytosis occur in hypertension and hypertensive- related TOD, such as increased carotid IMT[33]. HS-CRP predicts future CV events[32,33]. Elevated HS-CRP is both a risk marker and risk factor�for hypertension and CVD[34,35]. Increases in HS-CRP of over 3 ?g/ml may increase BP in just a few days that is directly proportional to the increase in HS-CRP[34,35]. Nitric oxide and eNOS are inhibited by HS-CRP[34,35]. The AT2R, which normally counterbalances AT1R, is downregulated by HS-CRP[34,35]. Angiotensin ? (A-?) upregulates many of the cytokines, especially IL-6, CAMs and chemokines by activating nuclear factor Kappa B (NF?b)
leading to vasoconstriction. These events, along with the increases in oxidative stress and endothelin-1, elevate BP[32].
Autoimmune Dysfunction
Innate and adaptive immune responses are linked to hypertension and hypertension-induced CVD through at least three mechanisms: cytokine production, central nervous
system stimulation and renal damage. This includes salt-sensitive hypertension with increased renal inflammation as a result of T cell imbalance, dysregulation of CD4+
and CD8+ lymphocytes and chronic leukocytosis with increased neutrophils and reduced lymphocytes[36-38]. Leukocytosis, especially increased neutrophils and decreased
lymphocyte count increase BP in Blacks by 6/2 mmHg in the highest vs the lowest tertile[38]. Macrophages and various T-cell subtypes regulate BP, invade the arterial
wall, activate TLRs and induce autoimmune vascular damage[38,39]. Angiotensin ? activates immune cells (T cells, macrophages and dendritic cells) and promotes cell
infiltration into target organs[39]. CD4+ T lymphocytes express AT1R and PPAR gamma receptors, and release TNF-?, interferon and interleukins within the vascular wall when activated[39] (Figure 5). IL-17 produced by T cells may play a pivotal role in the genesis of hypertension caused by Angiotensin ?[39]. Hypertensive patients have significantly higher TLR 4 mRNA in monocytes compared to normal[40]. Intensive reduction in BP to systolic
BP (SBP) less than 130 mmHg vs SBP to only 140 mmHg lowers the TLR 4 more[40]. A-? activates the TLR expression leading to inflammation and activation of the innate immune system. When TLR 4 is activated there is downstream macrophage activation, migration, increase metalloproteinase 9, vascular remodeling, collagen accumulation in the artery, LVH and cardiac fibrosis[40]. The autonomic nervous system is critical in either increasing
or decreasing immune dysfunction and inflammation[41]. Efferent cholinergic anti inflammatory pathways via the vagal nerve innervate the spleen, nicotine acetylcholine
receptor subunits and cytokine producing immune cells to influence vasoconstriction and BP[41]. Local CNS inflammation or ischemia may mediate vascular inflammation and hypertension[39].
Aldosterone is associated with increased adaptive immunity and autoimmune responses with CD4+ T cell activation and Th 17 polarization with increased IL 17, TGF-? and TNF-? which modulate over 30 inflammatory genes[42,43]. Increased serum aldosterone is an
independent risk factor for CVD and CHD through non-hemodynamic effects as well as through increased BP[42,43]. Blockade of mineralocorticoid receptors in the heart, brain, blood vessels and immune cells reduces CV risk even with the persistence of hypertension[42,43].
TREATMENT
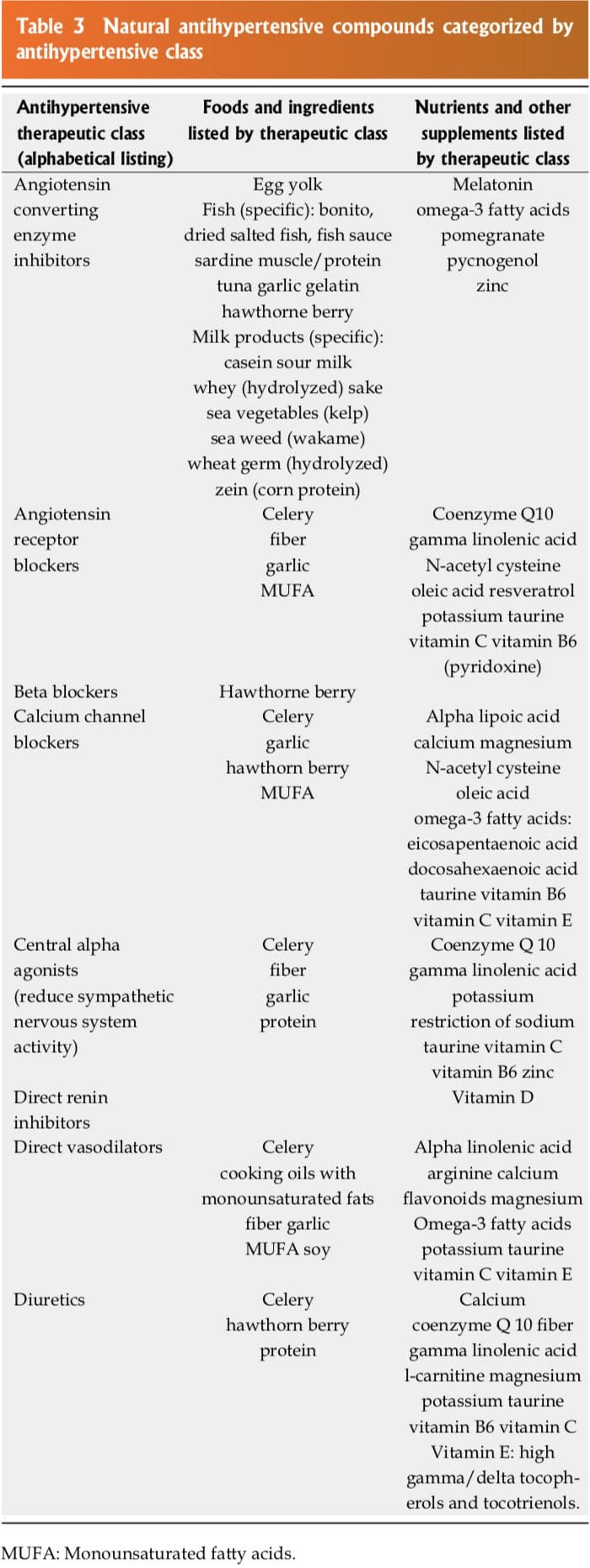
Many of the natural compounds in food, certain nutraceutical supplements, vitamins, antioxidants or minerals function in a similar fashion to a specific class of antihypertensive
drugs. Although the potency of these natural compounds may be less than the antihypertensive drug, when used in combination with other nutrients and nutraceutical
supplements, the antihypertensive effect is additive or synergistic. Table 3 summarizes these natural compounds into the major antihypertensive drug classes such as diuretics, beta blockers, central alpha agonists, direct vasodilators, calcium channel blockers (CCB�s), angiotensin converting enzyme inhibitors (ACEI�s), angiotensin receptor blockers (ARB�s) and direct renin inhibitors (DRI).
 Dietary Approaches To Stop Hypertension Diets
Dietary Approaches To Stop Hypertension Diets
The Dietary Approaches to Stop Hypertension (DASH) ?and ? diets conclusively demonstrated significant reductions in BP in borderline and stage?hypertensive patients[44,45]. In DASH?untreated hypertensive subjects with SBP < 160 mmHg and DBP 80-95 mmHg were placed on one of three diets for 4 wk, control diet, fruit and vegetable diet (F + V) and combined diet that added F + V and low fat dairy[44]. DASH ? added progressive sodium restriction in each group[45]. The control diet consisted of sodium at 3 g/d, potassium, magnesium and calcium at 25% of the US average, macronutrients at US average of 4 servings per day, a sodium/potassium ratio of 1.7 and fiber at 9 g/d. The F + V diet increased the potassium, magnesium and calcium to 75%, macronutrients to greater than the US average, a sodium potassium ratio of 0.7, 31 g of fiber and 8.5 servings of fruits and vegetables per day. The combined diet was similar to the F + V diet but added low fat dairy. At 2 wk the BP was decreased by 10.7/5.2 mmHg in the hypertensive patients in DASH?and 11.5/6.8 mmHg in the hypertensive patients in DASH ?. These reductions persisted as long as the patients were on the diet. The DASH diet increases plasma renin activity (PRA) and serum aldosterone levels in response to the BP reductions[46,47]. The mean increase in PRA was 37 ng/ml per day[47]. There was an associated of response with the G46A polymorphism of beta 2 adrenergic receptor. The A allele of G46A had a greater BP reduction and blunted PRA and aldosterone. The arachidonic acid (AA) genotype had the best response and the GG genotype had no response. Adding an ARB, ACEI or DRI improved BP response to the DASH diet in the GG group due to blockade of the increase in PRA. A low sodium DASH diet decreases oxidative stress (urine F2-isoprostanes), improves vascular function (augmentation index) and lowers BP in salt sensitive subjects[48]. In addition, plasma nitrite increased and pulse wave velocity�decreased at week two on the DASH diet[49].
Sodium (Na+) Reduction
The average sodium intake in the US is 5000 mg/d with some areas of the country consuming 15000-20000 mg/d[50]. However, the minimal requirement for sodium�is probably about 500 mg/d[50]. Epidemiologic, observational and controlled clinical trials demonstrate that an increased sodium intake is associated with higher BP as well as increased risk for CVD, CVA, LVH, CHD, MI, renal insufficiency, proteinuria and over activity of the SNS[1,50]. A reduction in sodium intake in hypertensive patients, especially the salt sensitive patients, will significantly lower BP by 4-6/2-3 mmHg that is proportional to the degree of sodium restriction and may prevent or delay hypertension in high risk patients and reduce future CV events[51-53].
Salt sensitivity (? 10% increase in MAP with salt loading) occurs in about 51% of hypertensive patients and is a key factor in determining the cardiovascular, cerebrovascular, renal and BP responses to dietary salt intake[54]. Cardiovascular events are more common in the salt sensitive patients than in salt resistant ones, independent of BP[55]. An increased sodium intake has a direct positive correlation with BP and the risk of CVA and CHD[56]. The risk is independent of BP for CVA with a relative risk of 1.04 to 1.25 from the lowest to the highest quartile[56]. In addition, patients will convert to a nondipping BP pattern with increases in nocturnal BP as the sodium intake increases[56].
Increased sodium intake has a direct adverse effect on endothelial cells[57-61]. Sodium promotes cutaneous lymphangiogenesis, increases endothelial cell stiffness, reduces size, surface area, volume, cytoskeleton, deformability and pliability, reduces eNOS and NO production, increases asymmetric dimethyl arginine (ADMA), oxidative stress and TGF-?. All of these abnormal vascular responses are increased in the presence of aldosterone[57-61]. These changes occur independent of BP and may be partially counteract by dietary potassium[57-61]. The endothelial cells act as vascular salt sensors[62]. Endothelial cells are targets for aldosterone which activate epithelial sodium channels (ENaCs) and have a negative effects on release of NO and on endothelial function. The mechanical stiffness of the cell plasma membrane and the submembranous actin network (endothelial glcyocalyx) (�shell�) serve as a �firewall� to protect the endothelial cells and are regulated by serum sodium, potassium and aldosterone within the physiologic range[62]. Changes in shear-stress-dependent activity of the endothelial NO synthase located in the caveolae regulate the viscosity in this �shell�[62]. High plasma sodium gelates the shell of the endothelial cell, whereas the shell is fluidized by high potassium. These communications between extracellular ions and intracellular enzymes occur at the plasma membrane barrier, whereas 90% of the total cell mass remains uninvolved in these changes. Blockade of the ENaC with spironolactone (100%) or amiloride (84%) minimizes or stop many of these vascular endothelial responses and increase NO[58,63]. Nitric oxide release follows endothelial nanomechanics and not vice versa and membrane depolarization decreases vascular endothelial cell stiffness which improves flow mediated nitric-oxide dependent vasodilation[64,65]. In the presence of vascular inflammation and increased HS-CRP, the effects of aldosterone on the�ENaC is enhanced further increasing vascular stiffness and BP[66]. High sodium intake also abolishes the AT2Rmediated vasodilation immediately with complete abolition of endothelial vasodilation (EDV) within 30 d[67]. Thus, it has become clear that increased dietary sodium has adverse effects on the vascular system, BP and CVD by altering the endothelial glycocalyx, which is a negatively charged biopolymer that lines the blood vessels and serves as a protective barrier against sodium overload, increased sodium permeability and sodium-induced TOD[68]. Certain SNP�s of salt inducible kinase?which alter Na+ /K+ ATPase, determine sodium induced hypertension and LVH[69].
The sodium intake per day in hypertensive patients should be between 1500 to 2000 mg. Sodium restriction improves BP reduction in those on patients that are on pharmacologic treatment and the decrease in BP is additive with restriction of refined carbohydrates[70,71]. Reducing dietary sodium intake may reduce damage to the brain, heart, kidney and vasculature through mechanisms dependent on the small BP reduction as well as those independent of the decreased BP[72-75].
A balance of sodium with other nutrients, especially potassium, magnesium and calcium is important, not only in reducing and controlling BP, but also in decreasing cardiovascular and cerebrovascular events[3,72,73]. An increase in the sodium to potassium ratio is associated with significantly increased risk of CVD and all-cause mortality[72]. The Yanomamo Indians consume and excrete only 1 meq of sodium in 24 h and consume and excrete 152 meq of potassium in 24 h[73]. The Na+ to K+ ratio is 1/152 and is associated with elevated PRA, but BP does not increase with age. At age 50 the average BP in the Yanomamo is 100-108/64-69 mmHg[73].
Potassium
The average U.S. dietary intake of potassium (K+ ) is 45 mmol/d with a potassium to sodium (K+ /Na+ ) ratio of less than 1:2[10,74]. The recommended intake of K+ is 4700 mg/d (120 mmol) with a K+ /Na+ ratio of about 4-5 to 1[10,74]. Numerous epidemiologic, observational and clinical trials have demonstrated a significant reduction in BP with increased dietary K+ intake in both normotensive and hypertensive patients[10,74,76]. The average BP reduction with a K+ supplementation of 60 to 120 mmol/d is 4.4/2.5 mmHg in hypertensive patients but may be as much as 8/4.1 mmHg with 120 mmol/d (4700 mg)[10,74,76,77]. In hypertensive patients, the linear doseresponse relationship is 1.0 mmHg reduction in SBP and 0.52 mmHg reduction in diastolic BP per 0.6 g/d increase in dietary potassium intake that is independent of baseline dietary potassium ingestion[10]. The response depends on race (black > white), sodium, magnesium and calcium intake[10]. Those on a higher sodium intake have a greater reduction in BP with potassium[10]. Alteration of the K+ /Na+ ratio to a higher level is important for both antihypertensive as well as cardiovascular and cerebrovascular effects[10,77]. High potassium intake reduces the incidence of cardiovascular (CHD, MI) and CVA independent of the BP reduction[10,74,76,77]. There are also reductions in CHF, LVH, diabetes mellitus and cardiac arrhythmias[10]. If the serum potassium is less than 4.0 meq/dL, there is an increased risk of CVD mortality, ventricular tachycardia, ventricular fibrillation and CHF[10]. Red blood cell potassium is a better indication of total body stores and CVD risk than is serum potassium[10]. Gu et al[77] found that potassium supplementation at 60 mmol of KCl per day for 12 wk significantly reduced SBP -5.0 mmHg (range -2.13 to -7.88 mmHg) (p < 0.001) in 150 Chinese men and women aged 35 to 64 years.
Potassium increases natriuresis, modulates baroreflex sensitivity, vasodilates, decreases the sensitivity to catecholamines and Angiotensin ?, increases sodium potassium ATPase and DNA synthesis in the vascular smooth muscle cells and decreases SNS activity in cells with improved vascular function[10]. In addition, potassium increases bradykinin and urinary kallikrein, decreases NADPH oxidase, which lowers oxidative stress and inflammation, improves insulin sensitivity, decreases ADMA, reduces intracellular sodium and lowers production of TGF-?[10].
Each 1000 mg increase in potassium intake per day reduces all cause mortality by approximately 20%. Potassium intake of 4.7 g/d is estimated to decrease CVA by 8% to 15% and MI by 6%-11%[10]. Numerous SNP�s such as nuclear receptor subfamily 3 group C, angiotensin ? type receptor and hydroxysteroid 11 beta dehydrogenase (HSD11B1 and B2) determine an individual�s response to dietary potassium intake[78]. Each 1000 mg decrease in sodium intake per day will decrease all cause mortality by 20%[10,73]. A recent analysis suggested a dose related response to CVA with urinary potassium excretion[79]. There was a RRR of CVA of 23% at 1.5-1.99 g, 27% at 2.0-2.49 g, 29% at 2.5-3 g and 32% over 3 g/d of potassium urinary excretion[79]. The recommended daily dietary intake for patients with hypertension is 4.7 to 5.0 g of potassium and less than 1500 mg of sodium[10]. Potassium in food or from supplementation should be reduced or used with caution in those patients with renal impairment or those on medications that increase renal potassium retention such as ACEI, ARB, DRI and serum aldosterone receptor antagonists[10].
Magnesium
A high dietary intake of magnesium of at least 500-1000 mg/d reduces BP in most of the reported epidemiologic, observational and clinical trials, but the results are less consistent than those seen with Na+ and K+[74,80]. In most epidemiologic studies, there is an inverse relationship between dietary magnesium intake and BP[74,80,81]. A study of 60 essential hypertensive subjects given magnesium supplements showed a significant reduction in BP over an eight week period documented by 24 h ambulatory BP, home and office blood BP[74,80,81]. The maximum reduction in clinical trials has been 5.6/2.8 mmHg but some studies have shown no change in BP[82]. The combination of high potassium and low sodium intake with increased magnesium intake had additive anti-hypertensive effects[82]. Magnesium also increases the effectiveness of all anti-hypertensive drug classe[82].
Magnesium competes with Na+ for binding sites on vascular smooth muscle and acts as a direct vasodilator, like a CCB. Magnesium increases prostaglandin E (PGE), regulates intracellular calcium, sodium, potassium and pH, increases nitric oxide, improves endothelial function, reduces oxLDL, reduces HS-CRP, TBxA2, A-?, and norepinephrine. Magnesium also improves insulin resistance, glucose and MS, binds in a necessary-cooperative manner with potassium, inducing EDV and BP reduction, reduces CVD and cardiac arrhythmias, decreases carotid IMT, lowers cholesterol, lowers cytokine production, inhibits nuclear factor Kb, reduces oxidative stress and inhibits platelet aggregation to reduce thrombosis[74,80-86].
Magnesium is an essential co-factor for the delta6-desaturase enzyme that is the rate-limiting step for conversion of linoleic acid (LA) to gamma linolenic acid (GLA)[74,80,81,83-85] needed for synthesis of the vasodilator and platelet inhibitor PGE1. Altered TRPM7 channels, which are the transporter for magnesium occur in many hypertensive patients[83].
A meta-analysis of 241378 patients with 6477 strokes showed an inverse relationship of dietary magnesium to the incidence of ischemic stroke[84]. For each 100 mg of dietary magnesium intake, ischemic stroke was decreased by 8%. The proposed mechanism include inhibition of ischemia induced glutamate release, NMDA receptor blockade, CCB actions, mitochondrial calcium buffering, decrease in ATP depletion and vasodilation of the cerebral arteries[84]. A meta-analysis showed reductions in BP of 3-4/2-3 mmHg in 22 trials of 1173 patients[87].
Intracellular level of magnesium (RBC) is more indicative of total body stores and should be measured in conjunction with serum and urinary magnesium[83]. Magnesium may be supplemented in doses of 500 to 1000 mg/d. Magnesium formulations chelated to an amino acid may improve absorption and decrease the incidence of diarrhea[82]. Adding taurine at 1000 to 2000 mg/d will enhance the anti-hypertensive effects of magnesium[82]. Magnesium supplements should be avoided or used with caution in patients with known renal insufficiency or in those taking medications that induce magnesium retention[82].
Calcium
Population studies show a link between hypertension and calcium[88], but clinical trials that administered calcium supplements to patients have shown inconsistent effects on BP[88]. The heterogeneous responses to calcium supplementation have been explained by Resnick[89]. This is the �ionic hypothesis�[89] of hypertension, cardiovascular disease and associated metabolic, functional and structural disorders. Calcium supplementation is not recommended at this time as an effective means to reduce BP.
Zinc
Low serum zinc levels in observational studies correlate with hypertension as well as CHD, type ? DM, hyperlipidemia, elevated lipoprotein a [Lp(a)], increased 2 h post�prandial plasma insulin levels and insulin resistance[90,91]. Zinc is transported into cardiac and vascular muscle and other tissues by metallothionein[92]. Genetic deficiencies of metallothionein with intramuscular zinc deficiencies may lead to increased oxidative stress, mitochondrial dysfunction, cardiomyocyte dysfunction and apoptosis with subsequent myocardial fibrosis, abnormal cardiac remodeling, heart disease, heart failure, or hypertension[92]. Intracellular calcium increases oxidative stress which is reduced by zinc[92]. Bergomi et al[93] evaluated Zinc (Zn++) status in 60 hypertensive subjects compared to 60 normotensive control subjects. An inverse correlation of BP and serum Zn++ was observed. The BP was also inversely correlated to a Zn++ dependent enzyme-lysyl oxidase activity. Zn++ inhibits gene expression and transcription through NF-?b and activated protein-1 and is an important cofactor for SOD[90,92]. These effects plus those on insulin resistance, membrane ion exchange, RAAS and SNS effects may account for Zn++ antihypertensive effects[90,92]. Zinc intake should be 50 mg/d[1].
Protein
Observational and epidemiologic studies demonstrate a consistent association between a high protein intake and a reduction in BP and incident BP[94,95]. The protein source is an important factor in the BP effect; animal protein being less effective than non-animal or plant protein, especially almonds[94-97]. In the Inter-Salt Study of over 10000 subjects, those with a dietary protein intake 30% above the mean had a lower BP by 3.0/2.5 mmHg compared to those that were 30% below the mean (81 vs 44 g/d)[94]. However, lean or wild animal protein with less saturated fat and more essential omega-3 fatty acids may reduce BP, lipids and CHD risk[94,97]. A meta-analysis confirmed these findings and also suggested that hypertensive patients and the elderly have the greatest BP reduction with protein intake[95]. Another meta-analysis of 40 trials with 3277 patients found reductions in BP of 1.76/1.15 mmHg compared to carbohydrate intake (p < 0.001)[98]. Both vegetable and animal protein significantly and equally reduced BP at 2.27/1.26 mmHg and 2.54/0.95 mmHg respectively[98]. Increased dietary protein intake is inversely associated with risk for stroke in women with hypertension[99]. A randomized cross-over study in 352 adults with pre-hypertension and stage?hypertension found a significant reduction in SBP of 2.0 mmHg with soy protein and 2.3 mmHg with milk protein compared to a high glycemic index diet over each of the 8 wk treatment periods[100]. There was a non-significant reduction in DBP. Another RDB parallel study over 4 wk of 94 subjects with prehypertension and stage?hypertension found significant reductions on office BP of 4.9/2.7 mmHg in those given a combination of 25% protein intake vs the control group given 15% protein in an isocaloric manner[101]. The protein consisted of 20% pea, 20% soy, 30% egg and 30% milk-protein isolate[101]. The daily recommended intake of protein from all sources is 1.0 to 1.5 g/kg body weight, varying with exercise level, age,�renal function and other factors[1,70,71].
Fermented milk supplemented with whey protein concentrate significantly reduces BP in human studies[102-106]. Administration of 20 g/d of hydrolyzed whey protein supplement rich in bioactive peptides significantly reduced BP over 6 wk by 8.0 � 3.2 mmHg in SBP and 5.5 � 2.1 mm in diastolic BP[103]. Milk peptides which contain both caseins and whey proteins are a rich source of ACEI peptides. Val-Pro-Pro and Ile-Pro-Pro given at 5 to 60 mg/d have variable reductions in BP with an average decrease in pooled studies of about 1.28-4.8/0.59-2.2 mmHg[71,100,104-107]. However several recent meta-analysis did not show significant reductions in BP in humans[106,108]. Powdered fermented milk with Lactobacillus helveticus given at 12 g/d significantly lowered BP by 11.2/6.5 mmHg in 4 wk in one study[104]. Milk peptides are beneficial in treating MS[109]. A dose response study showed insignificant reductions in BP[110]. The clinical response is attributed to fermented milk�s active peptides which inhibit ACE.
Pins et al[111] administered 20 g of hydrolyzed whey protein to 56 hypertensive subjects and noted a BP reduction of 11/7 mmHg compared to controls at one week that was sustained throughout the study. Whey protein is effective in improving lipids, insulin resistance, glucose, arterial stiffness and BP[112]. These data indicate that the whey protein must be hydrolyzed in order to exhibit an antihypertensive effect, and the maximum BP response is dose dependent.
Bovine casein-derived peptides and whey protein-derived peptides exhibit ACEI activity[102-111]. These components include B-caseins, B-lg fractions, B2-microglobulin and serum albumin[102-104,111]. The enzymatic hydrolysis of whey protein isolates releases ACEI peptides.
Marine collagen peptides (MCPs) from deep sea fish have anti-hypertensive activity[113-115]. A double-blind placebo controlled trial in 100 hypertensive subjects with diabetes who received MCPs twice a day for 3 mo had significant reductions in DBP and mean arterial pressure[113]. Bonito protein (Sarda Orientalis), from the tuna and mackerel family has natural ACEI inhibitory peptides and reduces BP 10.2/7 mmHg at 1.5 g/d[114,116].
Sardine muscle protein, which contains Valyl-Tyrosine (VAL-TYR), significantly lowers BP in hypertensive subjects[117]. Kawasaki et al[117] treated 29 hypertensive subjects with 3 mg of VAL-TYR sardine muscle concentrated extract for four wk and lowered BP 9.7/5.3 mmHg (p < 0.05). Levels of A-?increased as serum A-? and aldosterone decreased indicating that VAL-TYR is a natural ACEI. A similar study with a vegetable drink with sardine protein hydrolysates significantly lowered BP by 8/5 mmHg in 13 wk[118].
Soy protein lowers BP in hypertensive patients in most studies[100,119-127]. Soy protein intake was significantly and inversely associated with both SBP and DBP in 45694 Chinese women consuming 25 g/d or more of soy protein over 3 years and the association increased with age[119]. The SBP reduction was 1.9 to 4.9 mm lower and the DBP 0.9 to 2.2 mmHg lower[119]. However, randomized clinical trials and meta-analysis have shown mixed results on BP with no change in BP to reductions of 7% to 10 % for SBP and DBP[121-125]. The recent meta-analysis of 27 trials found a significant reduction in BP of 2.21/1.44 mmHg[120]. Some studies suggest improvement in endothelial function, improved arterial compliance, reduction in HS-CRP and inflammation, ACEI activity, reduction in sympathetic tone, diuretic action and reduction in both oxidative stress and aldosterone levels[125-127]. Fermented soy at about 25 g/d is recommended.
In addition to ACEI effects, protein intake may also alter catecholamine responses and induce a natriuretic effect[117,118]. Low protein intake coupled with low omega 3 fatty acid intake may contribute to hypertension in animal models[128]. The optimal protein intake, depending on level of activity, renal function, stress and other factors, is about 1.0 to 1.5 g/kg per day[1].
Amino Acids And Related Compounds
L-arginine: L-arginine and endogenous methylarginines are the primary precursors for the production of NO, which has numerous beneficial cardiovascular effects, mediated through conversion of L-arginine to NO by eNOS. Patients with hypertension, hyperlipidemia, diabetes mellitus and atherosclerosis have increased levels of HSCRP and inflammation, increased microalbumin, low levels of apelin (stimulates NO in the endothelium), increased levels of arginase (breaks down arginine) and elevated serum levels of ADMA, which inactivates NO[129-133].
Under normal physiological conditions, intracellular arginine levels far exceed the Km [Michaelis Menton constant(MMC)] of eNOS which is less than 5 ?mol[134]. However, endogenous NO formation is dependent on extracellular arginine concentration[134]. The intracellular concentrations of L-arginine are 0.1-3.8 mmol/L in endothelial cells while the plasma concentration of arginine is 80-120 ?mol/L which is about 20-25 times greater than the MMC[135,136]. Despite this, cellular NO formation depends on exogenous L-arginine and this is the arginine paradox. Renal arginine regulates BP and blocks the formation of endothelin, reduces renal sodium reabsorption and is a potent antioxidant[134]. The NO production in endothelial cells is closely coupled to cellular arginine uptake indicating that arginine transport mechanisms play a major role in the regulation of NO-dependent function. Exogenous arginine can increase renal vascular and tubular NO bioavailability and influence renal perfusion, function and BP[132]. Molecular eNOS uncoupling may occur in the absence of tetrahydrobiopterin which stabilizes eNOS, which leads to production of ROS[135].
Human studies in hypertensive and normotensive subjects of parenteral and oral administrations of L-arginine demonstrate an antihypertensive effect as well as improvement in coronary artery blood flow and peripheral blood flow in PAD[129,136-140]. The BP decreased by 6.2/6.8 mmHg on 10 g/d of L-arginine when provided as a supplement or though natural foods to a group of hypertensive subjects[136]. Arginine produces a statistically and biologically significant decrease in BP and improved metabolic effect in normotensive and hypertensive humans that is similar in magnitude to that seen in the DASH?diet[136]. Arginine given at 4 g/d also significantly lowered BP in women with gestational hypertension without proteinuria, reduced the need for anti-hypertensive therapy, decreased maternal and neonatal complications and prolonged the pregnancy[137,138]. The combination of arginine (1200 mg/d) and N-acetyl cysteine (NAC) (600 mg bid) administered over 6 mo to hypertensive patients with type 2 diabetes, lowered SBP and DBP (p < 0.05), increased HDL-C, decreased LDL-C and oxLDL, reduced HSCRP, ICAM, VCAM, PAI-?, fibrinogen and IMT[139]. A study of 54 hypertensive subjects given arginine 4 g three times per day for four weeks had significant reductions in 24 h ABM[140]. A meta-analysis of 11 trials with 383 subjects administered arginine 4-24 g/d found average reduction in BP of 5.39/2.66 mmHg (p < 0.001) in 4 wk[141]. Although these doses of L-arginine appear to be safe, no long term studies in humans have been published at this time and there are concerns of a pro-oxidative effect or even an increase in mortality in patients who may have severely dysfunctional endothelium, advanced atherosclerosis, CHD, ACS or MI[142]. In addition to the arginine-NO path, there exists an nitrate/nitrite pathway that is related to dietary nitrates from vegetables, beetroot juice and the DASH diet that are converted to nitrites by symbiotic, salivary, GI and oral bacteria[143]. Administration of beetroot juice or extract at 500 mg/d will increase nitrites and lower BP, improve endothelial function, increase cerebral, coronary and peripheral blood flow[143].
L-carnitine and acetyl -L-carnitine: L-carnitine is a nitrogenous constituent of muscle primarily involved in the oxidation of fatty acids in mammals. Animal studies indicate that carnitine has both systemic anti-hypertensive effects as well as anti-oxidant effects in the heart by upregulation of eNOS and PPAR gamma, inhibition of RAAS, modulation of NF-?B and down regulation of NOX2, NOX4, TGF-? and CTGF that reduces cardiac fibrosis[144,145]. Endothelial function, NO and oxidative defense are improved while oxidative stress and BP are reduced[144-147]. Human studies on the effects of L-carnitine and acetyl-L-carnitine are limited, with minimal to no change in BP[148-153]. In patients with MS, acetyl-L-carnitine at one gram bid over 8 wk, improved dysglycemia and reduced SBP by 7-9 mmHg, but diastolic BP was significantly decreased only in those with higher glucose[151]. Low carnitine levels are associated with a nondipping BP pattern in Type 2 DM[153]. Carnitine has antioxidant and antiinflammatory effects and may be useful in the treatment of essential hypertension, type ? DM with hypertension, hyperlipidemia, cardiac arrhythmias, CHF and cardiac ischemic syndromes[1,149,150,153]. Doses of 2-3 g twice per day are recommended.
Taurine: Taurine is a sulfonic beta-amino acid that is considered a conditionally-essential amino acid, which is not utilized in protein synthesis, but is found free or in simple peptides with its highest concentration in the brain, retina and myocardium[154]. In cardiomyocytes, it represents about 50% of the free amino acids and has a role of an osmoregulator, inotropic factor and antihypertensive agent[155].
Human studies have noted that essential hypertensive subjects have reduced urinary taurine as well as other sulfur amino acids[1,154,155]. Taurine lowers BP, SVR and HR, decreases arrhythmias, CHF symptoms and SNS activity, increases urinary sodium and water excretion, increases atrial natriuretic factor, improves insulin resistance, increases NO and improves endothelial function. Taurine also decreases A-?, PRA, aldosterone, SNS activity, plasma norepinephrine, plasma and urinary epinephrine, lowers homocysteine, improves insulin sensitivity, kinins and acetyl choline responsiveness, decreases intracellular calcium and sodium, lowers response to beta receptors and has antioxidant, anti-atherosclerotic and anti-inflammatory activities, decreases IMT and arterial stiffness and may protect from risk of CHD[1,154-160]. A lower urinary taurine is associated with increased risk of hypertension and CVD[160,161]. A study of 31 Japanese males with essential hypertension placed on an exercise program for 10 wk showed a 26% increase in taurine levels and a 287% increase in cysteine levels. The BP reduction of 14.8/6.6 mmHg was proportional to increases in serum taurine and reductions in plasma norepinephrine[162]. Fujita et al[155] demonstrated a reduction in BP of 9/4.1 mmHg (p < 0.05) in 19 hypertension subjects given 6 g of taurine for 7 d. Taurine has numerous beneficial effects on the cardiovascular system and BP[156]. The recommended dose of taurine is 2 to 3 g/d at which no adverse effects are noted, but higher doses up to 6 g/d may be needed to reduce BP significantly[1,70,71,154-162].
Omega-3 Fats
The omega-3 fatty acids found in cold water fish, fish oils, flax, flax seed, flax oil and nuts lower BP in observational, epidemiologic and in prospective clinical trials[163-173]. The findings are strengthened by a dose-related response in hypertension as well as a relationship to the specific concomitant diseases associated with hypertension[163-173].
Studies indicate that DHA at 2 g/d reduces BP and heart rate[163,173]. The average reduction in BP is 8/5 mmHg and heart rate falls about 6 beats/min usually in about 6 wk[1,70,71,91-175]. Fish oil at 4-9 g/d or combination of DHA and EPA at 3-5 g/d will also reduce BP[1,168-173]. However, formation of EPA and ultimately DHA from ALA is decreased in the presence of high LA (the essential omega-6 fatty acid), saturated fats, trans fatty acids, alcohol, several nutrient deficiencies (magnesium, vitamin B6) and aging, all of which inhibit the desaturase enzymes[163]. Eating cold water fish three times per week may be as effective as high dose fish oil in reducing BP in hypertensive patients, and the protein in the fish may also have antihypertensive effects[1,163]. In patients with chronic kidney disease 4 g of omega 3 fatty acids reduced BP measured with 24 h ABM over 8 wk by 3.3/2.9 mmHg�compared to placebo (p < 0.0001)[167].
The ideal ratio of omega-6 FA to omega-3 FA is between 1:1 to 1:4 with a polyunsaturated to saturated fat ratio greater than 1.5 to 2:0[2]. Omega 3 fatty acids increase eNOS and nitric oxide, improve endothelial function, improve insulin sensitivity, reduce calcium influx, suppress ACE activity and improve parasympathetic tone[1,163-171]. The omega-6 FA family includes LA, GLA, dihomo-GLA and AA which do not usually lower BP significantly, but may prevent increases in BP induced by saturated fats[176]. GLA may block stress-induced hypertension by increasing PGE1 and PGI2, reducing aldosterone levels, reducing adrenal AT1R density and affinity[175].
The omega-3 FA have a multitude of other cardiovascular consequences which modulates BP such as increases in eNOS and nitric oxide, improvement in ED, reduction in plasma nor-epinephrine and increase in paraSNS tone, suppression of ACE activity and improvement in insulin resistance[176]. The recommended daily dose is 3000 to 5000 mg/d of combined DHA and EPA in a ratio of 3 parts EPA to 2 parts DHA and about 50% of this dose as GLA combined with gamma/delta tocopherol at 100 mg per gram of DHA and EPA to get the omega 3 index to 8% or higher to reduce BP and provide optimal cardioprotection[177]. DHA is more effective than EPA for reducing BP and should be given at 2 g/d if administered alone[163,173].
Omega-9 Fats
Olive oil is rich in the omega-9 monounsaturated fat (MUFA) oleic acid, which has been associated with BP and lipid reduction in Mediterranean and other diets[178-180]. Olive oil and MUFAs have shown consistent reductions in BP in most clinical studies in humans[178-190]. In one study, the SBP fell 8 mmHg (p ? 0.05) and the DBP fell 6 mmHg (p ? 0.01) in both clinic and 24 h ambulatory BP monitoring in the MUFA treated subjects compared to the PUFA treated subjects[178]. In addition, the need for antihypertensive medications was reduced by 48% in the MUFA group vs 4% in the omega-6 PUFA group (p < 0.005). Extra virgin olive oil (EVOO) was more effective than sunflower oil in lowering SBP in a group of 31 elderly hypertensive patients in a double blind randomized crossover study[187]. The SBP was 136 mmHg in the EVOO treated subjects vs 150 mmHg in the sunflower treated group (p < 0.01). Olive oil also reduces BP in hypertensive diabetic subjects[188]. It is the high oleic acid content in olive oil that reduces BP[180]. In stage?hypertensive patients, oleuropein-olive leaf (Olea Eurpoaea) extract 500 mg bid for 8 wk reduced BP 11.5/4.8 mmHg which was similar to captopril 25 mg bid[189]. Olea Eupopea L aqueous extract administered to 12 patients with hypertension at 400 mg qid for 3 mo significantly reduced BP (p < 0.001)[181]. Olive oil intake in the EPIC study of 20343 subjects was inversely associated with both systolic and diastolic BP[182]. In the SUN study of 6863 subjects, BP was inversely associated with olive oil consumption, but only in men[183]. In a study of 40 hypertensive monozygotic twins, olive leaf extract demonstrated a dose response reduction in BP at doses of 500 to 1000 mg/d in 8 wk compared to placebo[184]. The low dose groups decreased BP 3/1 mmHg and the high dose 11/4 mmHg[184]. A double blind, randomized, crossover dietary intervention study over 4 mo using polyphenol rich olive oil 30 mg/d decreased BP in the study group by 7.91/6.65 mmHg and improved endothelial function[185]. The ADMA levels, oxLDL and HS-CRP were reduced in the olive oil group. Plasma nitrites and nitrates increased and hyperemic area after ischemia improved in the treated group. Olive oil inhibits the AT1R receptor, exerts L-type calcium channel antagonist effects and improves wave reflections and augmentation index[191-193].
EVOO is also contains lipid-soluble phytonutrients such as polyphenols. Approximately 5 mg of phenols are found in 10 g of EVOO[178,186]. About 4 tablespoons of EVOO is equal to 40 g of EVOO which is the amount required to get significant reductions in BP.
Fiber
The clinical trials with various types of fiber to reduce BP have been inconsistent[194,195]. Soluble fiber, guar gum, guava, psyllium and oat bran may reduce BP and reduce the need for antihypertensive medications in hypertensive subjects, diabetic subjects and hypertensive-diabetic subjects[1,70,71,194,195]. The average reduction in BP is about 7.5/5.5 mmHg on 40 to 50 g/d of a mixed fiber. There is improvement in insulin sensitivity, endothelial function, reduction in SNS activity and increase in renal sodium loss[1,70,71,194].
Vitamin C
Vitamin C is a potent water-soluble electron-donor. At physiologic levels it is an antioxidant although at supraphysiologic doses such as those achieved with intravenous vitamin C it donates electrons to different enzymes which results in pro-oxidative effects. At physiologic doses vitamin C recycles vitamin E, improves ED and produces a diuresis[196]. Dietary intake of vitamin C and plasma ascorbate concentration in humans is inversely correlated to SBP, DBP and heart rate[196-210].
An evaluation of published clinical trials indicate that vitamin C dosing at 250 mg twice daily will significantly lower SBP 5-7 mmHg and diastolic BP 2-4 mmHg over 8 wk[196-210]. Vitamin C will induce a sodium water diuresis, improve arterial compliance, improve endothelial function, increase nitric oxide and PGI2, decrease adrenal steroid production, improve sympathovagal balance, increase RBC Na/K ATPase, increase SOD, improve aortic elasticity and compliance, improve flow mediated vasodilation, decrease pulse wave velocity and augmentation index, increase cyclic GMP, activate potassium channels, reduce cytosolic calcium and reduce serum aldehydes[208]. Vitamin C prevents ED induced by an oral glucose load. Vitamin C enhances the efficacy of amlodipine, decreases the binding affinity of the AT 1 receptor for angiotensin ? by disrupting the ATR1 disulfide bridges and enhances the anti-hypertensive effects of medications in the elderly�with refractory hypertension[1,70,71,200-205]. In elderly patients with refractory hypertension already on maximum pharmacologic therapy, 600 mg of vitamin C daily lowered the BP by 20/16 mmHg[205]. The lower the initial ascorbate serum level, the better is the BP response. A serum level of 100 ?mol/L is recommended[1,70,71]. The SBP and 24 ABM show the most significant reductions with chronic oral administration of Vitamin C[200-205]. Block et al[206] in an elegant depletion-repletion study of vitamin C demonstrated an inverse correlation of plasma ascorbate levels, SBP and DBP. In a meta-analysis of thirteen clinical trials with 284 patients, vitamin C at 500 mg/d over 6 wk reduced SBP 3.9 mmHg and DBP 2.1 mmHg[207]. Hypertensive subjects were found to have significantly lower plasma ascorbate levels compared to normotensive subjects (40 ?mol/L vs 57 ?mol/L respectively)[211], and plasma ascorbate is inversely correlated with BP even in healthy, normotensive individuals[206].
Vitamin E
Most studies have not shown reductions in BP with most forms of tocopherols or tocotrienols[1,70,71]. Patients with T2DM and controlled hypertension (130/76 mmHg) on prescription medications with an average BP of 136/76 mmHg were administered mixed tocopherols containing 60% gamma, 25% delta and 15% alpha tocopherols[212]. The BP actually increased by 6.8/3.6 mmHg in the study patients (p < 0.0001) but was less compared to the increase with alpha tocopherol of 7/5.3 mmHg (p < 0.0001). This may be a reflection of drug interactions with tocopherols via cytochrome P 450 (3A4 and 4F2) and reduction in the serum levels of the pharmacologic treatments that were simultaneously being given[212]. Gamma tocopherol may have natriuretic effects by inhibition of the 70pS potassium channel in the thick ascending limb of the loop of Henle and lower BP[213]. Both alpha and gamma tocopherol improve insulin sensitivity and enhance adiponectin expression via PPAR gamma dependent processes, which have the potential to lower BP and serum glucose[214]. If vitamin E has an antihypertensive effect, it is probably small and may be limited to untreated hypertensive patients or those with known vascular disease or other concomitant problems such as diabetes or hyperlipidemia.
Vitamin D
Vitamin D3 may have an independent and direct role in the regulation of BP and insulin metabolism[215-225]. Vitamin D influences BP by its effects on calcium-phosphate metabolism, RAA system, immune system, control of endocrine glands and ED[216]. If the Vitamin D level is below 30 ng/ml the circulating PRA levels are higher which increases angiotensin ?, increases BP and blunts plasma renal blood flow[221]. The lower the level of Vitamin D, the greater the risk of hypertension, with the lowest quartile of serum Vitamin D having a 52% incidence of hypertension and the highest quartile having a 20% incidence[221]. Vitamin D3 markedly suppresses renin transcription by a VDR-mediated mechanism via the JGA apparatus. Its role in electrolytes, volume and BP homeostasis indicates that Vitamin D3 is important in amelioration of hypertension. Vitamin D lower ADMA, suppresses pro-inflammatory cytokines such as TNF-?, increases nitric oxide, improves endothelial function and arterial elasticity, decreases vascular smooth muscle hypertrophy, regulates electrolytes and blood volume, increases insulin sensitivity, reduces free fatty acid concentration, regulates the expression of the natriuretic peptide receptor and lowers HS-CRP[217-219,221].
The hypotensive effect of vitamin D was inversely related to the pretreatment serum levels of 1,25(OH)2D3 and additive to antihypertensive medications. Pfeifer et al[225] showed that short-term supplementation with vitamin D3 and calcium is more effective in reducing SBP than calcium alone. In a group of 148 women with low 25(OH)2D3 levels, the administration of 1200 mg calcium plus 800 IU of vitamin D3 reduced SBP 9.3% more (p < 0.02) compared to 1200 mg of calcium alone. The HR fell 5.4% (p = 0.02), but DBP was not changed. The range in BP reduction was 3.6/3.1 to 13.1/7.2 mmHg. The reduction in BP is related to the pretreatment level of vitamin D3, the dose of vitamin D3 and serum level of vitamin D3, but BP is reduced only in hypertensive patients. Although vitamin D deficiency is associated with hypertension in observational studies, randomized clinical trials and their meta-analysis have yielded inconclusive results[223]. In addition, vitamin D receptor gene polymorphisms may effect the risk of hypertension in men[224]. A 25 hydroxyvitamin D level of 60 ng/ml is recommended.
Vitamin B6 (Pyridoxine)
Low serum vitamin B6 (pyridoxine) levels are associated with hypertension in humans[226]. One human study by Aybak et al[227] proved that high dose vitamin B6 at 5 mg/kg per day for 4 wk significantly lowered BP by 14/10 mmHg. Pyridoxine (vitamin B6) is a cofactor in neurotransmitter and hormone synthesis in the central nervous system(norepinephrine, epinephrine, serotonin, GABA and kynurenine), increases cysteine synthesis to neutralize aldehydes, enhances the production of glutathione, blocks calcium channels, improves insulin resistance, decreases central sympathetic tone and reduces end organ responsiveness to glucocorticoids and mineralocorticoids[1,70,71,228,229]. Vitamin B6 is reduced with chronic diuretic therapy and heme pyrollactams. Vitamin B6 thus has similar action to central alpha agonists, diuretics and CCB�s. The recommended dose is 200 mg/d orally.
Flavonoids
Over 4000 naturally occurring flavonoids have been identified in such diverse substances as fruits, vegetables, red wine, tea, soy and licorice[230]. Flavonoids (flavonols, flavones and isoflavones) are potent free radical scavengers that inhibit lipid peroxidation, prevent atherosclerosis, promote vascular relaxation and have antihypertensive properties[230]. In addition, they reduce stroke and provide cardioprotective effects that reduce CHD morbidity and�mortality[231].
Resveratrol is a potent antioxidant and antihypertensive found in the skin of red grapes and in red wine. Resveratrol administration to humans reduces augmentation index, improves arterial compliance and lowers central arterial pressure when administered as 250 ml of either regular or dealcoholized red wine[232]. There was a significant reduction in the aortic augmentation index of 6.1% with the dealcoholized red wine and 10.5% with regular red wine. The central arterial pressure was significantly reduced by dealcoholized red wine at 7.4 mmHg and 5.4 mmHg by regular red wine. Resveratrol increases flow mediated vasodilation in a dose related manner, improves ED, prevents uncoupling of eNOS, increases adiponectin, lowers HS-CRP and blocks the effects of angiotensin ?[233-236]. The recommended dose is 250 mg/d of trans resveratrol[234].
Lycopene
Lycopene is a fat-soluble phytonutrient in the carotenoid family. Dietary sources include tomatoes, guava, pink grapefruit, watermelon, apricots and papaya in high concentrations[237-241]. Lycopene produces a significant reduction in BP, serum lipids and oxidative stress markers[237-241]. Paran et al[241] evaluated 30 subjects with Grade?hypertension, age 40-65, taking no antihypertensive or anti-lipid medications treated with a tomato lycopene extract (10 mg lycopene) for eight weeks. The SBP was reduced from 144 to 135 mmHg (9 mmHg reduction, p < 0.01) and DBP fell from 91 to 84 mmHg (7 mmHg reduction, p < 0.01). Another study of 35 subjects with Grade?hypertension showed similar results on SBP, but not DBP[237]. Englehard gave a tomato extract to 31 hypertensive subjects over 12 wk demonstrating a significant BP reduction of 10/4 mmHg[238]. Patients on various anti-hypertensive agents including ACEI, CCB and diuretics had a significant BP reduction of 5.4/3 mmHg over 6 wk when administered a standardized tomato extract[239]. Other studies have not shown changes in BP with lycopene[240]. Lycopene and tomato extract improve ED and reduce plasma total oxidative stress[242]. The recommended daily intake of lycopene is 10-20 mg in food or supplement form.
Pycnogenol
Pycnogenol, a bark extract from the French maritime pine, at doses of 200 mg/d resulted in a significant reduction in SBP from 139.9 mmHg to 132.7 mmHg (p < 0.05) in eleven patients with mild hypertension over eight weeks in a double-blind randomized placebo crossover trial. Diastolic BP fell from 93.8 mmHg to 92.0 mmHg. Pycnogenol acts as a natural ACEI, protects cell membranes from oxidative stress, increases NO and improves endothelial function, reduces serum thromboxane concentrations, decreases myelo-peroxidase activity, improves renal cortical blood flow, reduces urinary albumin excretion and decreases HS-CRP[243-247]. Other studies have shown reductions in BP and a decreased need for ACEI and CCB, reductions in endothelin-1, HgA1C, fasting glucose, LDL-C and myeloperoxidase[244,245,247].
Garlic
Clinical trials utilizing the correct dose, type of garlic and well absorbed long acting preparations have shown consistent reductions in BP in hypertensive patients with an average reduction in BP of 8.4/7.3 mmHg[248,249]. Not all garlic preparations are processed similarly and are not comparable in antihypertensive potency[1]. In addition, cultivated garlic (allium sativum), wild uncultivated garlic or bear garlic (allium urisinum) as well as the effects of aged, fresh and long acting garlic preparations differ[1,70,71,248,249]. Garlic is also effective in reducing BP in patients with uncontrolled hypertension already on anti-hypertensive medication[249,250]. A garlic homogenate-based supplement was administered to 34 prehypertensive and stage?hypertensive patients at 300 mg/d over 12 wk with a reduction in BP of 6.6-7.5/4.6-5.2 mmHg[249]. Aged garlic at doses of 240 to 960 mg/d given to 79 hypertensive subjects over 12 wk significantly lowered SBP 11.8 � 5.4 mmHg in the high dose garlic group[249]. A time released garlic may reduce BP better than the shorter acting garlic[249]. A Cochrane Database review indicated a net reduction in BP of 10-12/6-9 mmHg in all clinical trials with garlic[249]. In a double-blind parallel randomized placebo-controlled trial of 50 patients, 900 mg of aged garlic extract with 2.4 mg of S-allylcysteine was administered daily for 12 wk and reduced SBP 10.2 mmHg (p = 0.03) more than the control group[250].
Approximately 10000 mcg of allicin (one of the active ingredients in garlic) per day, the amount contained in four cloves of garlic (5 g) is required to achieve a significant BP lowering effect[1,70,71,249,250]. Garlic has ACEI activity, calcium channel blocking activity, reduces catecholamine sensitivity, improves arterial compliance, increases bradykinin and nitric oxide and contains adenosine, magnesium, flavonoids, sulfur, allicin, phosphorous and ajoenes that reduce BP[1,70,71].
Seaweed
Wakame seaweed (Undaria pinnatifida) is the most popular, edible seaweed in Japan[251]. In humans, 3.3 g of dried Wakame for four wk significantly reduced both the SBP 14 � 3 mmHg and the DBP 5 � 2 mmHg (p < 0.01)[252]. In a study of 62 middle-aged, male subjects with mild hypertension given a potassium-loaded, ion-exchanging, sodium-adsorbing, potassium-releasing seaweed preparation, significant BP reductions occurred at four weeks on 12 and 24 g/d of the seaweed preparation (p < 0.01)[253]. The MAP fell 11.2 mmHg (p < 0.001) in the sodium-sensitive subjects and 5.7 mmHg (p < 0.05) in the sodiuminsensitive subjects, which correlated with PRA. Seaweed and sea vegetables contain most all of the seawater�s 77I minerals and rare earth elements, fiber and alginate in a colloidal form[251-253]. The primary effect of Wakame appears to be through its ACEI activity from at least four parent tetrapeptides and possibly their dipeptide�and tripeptide metabolites, especially those containing the amino acid sequence Val-Tyr, Ile-Tyr, Phe-Tyr and Ile-Try in some combination[251,254,255]. Its long-term use in Japan has demonstrated its safety. Other varieties of seaweed may reduce BP by reducing intestinal sodium absorption and increasing intestinal potassium absorption[253].
Sesame
Sesame has been shown to reduce BP in a several small randomized, placebo controlled human studies over 30-60 d[256-264]. Sesame lowers BP alone[257-261] or in combination with nifedipine[256,260] diuretics and beta blockers[257,261]. In a group of 13 mild hypertensive subjects, 60 mg of sesamin for 4 wk lowered SBP 3.5 mmHg (p < 0.044) and DBP 1.9 mmHg (p < 0.045)[258]. Black sesame meal at 2.52 g/d over 4 wk in 15 subjects reduced SBP by 8.3 mmHg (p < 0.05) but there was a non-significant reduction in DBP of 4.2 mmHg[259]. Sesame oil at 35 g/d significantly lowered central BP within 1 h and also maintained BP reduction chronically in 30 hypertensive subjects, reduced heart rate, reduced arterial stiffness, decreased augmentation index and pulse wave velocity, decreased HSCRP, improved NO, decreased endothelin?and improved antioxidant capacity[264]. In addition sesame lowers serum glucose, HgbAIC and LDL-C, increases HDL, reduces oxidative stress markers and increases glutathione, SOD, GPx, CAT, vitamins C, E and A[256,257,258-261]. The active ingredients are natural ACEI�s such as sesamin, sesamolin, sesaminol glucosides, furoufuran lignans which also suppressors of NF-?B[262,263]. All of these effects lower inflammation and oxidative stress, improve oxidative defense and reduce BP[262,263].
Beverages: Tea, Coffee, And Cocoa
Green tea, black tea and extracts of active components in both have demonstrated reduction in BP in humans[265-271]. In a double blind placebo controlled trial of 379 hypertensive subjects given green tea extract 370 mg/d for 3 mo, BP was reduced significantly at 4/4 mmHg with simultaneous decrease in HS CRP, TNF-?, glucose and insulin levels[268].
Dark chocolate (100 g) and cocoa with a high content of polyphenols (30 mg or more) have been shown to significantly reduce BP in humans[272-283]. A metaanalysis of 173 hypertensive subjects given cocoa for a mean duration of 2 wk had a significant reduction in BP 4.7/2.8 mmHg (p = 0.002 for SBP and 0.006 for DBP)[276]. Fifteen subjects given 100 g of dark chocolate with 500 mg of poly-phenols for 15 d had a 6.4 mmHg reduction in SBP (p < 0.05) with a non significant change in DBP[273]. Cocoa at 30 mg of poly-phenols reduced BP in pre-hypertensive and stage?hypertensive patients by 2.9/1.9 mmHg at 18 wk (p < 0.001)[274]. Two more recent meta-analysis of 13 trials and 10 trials with 297 patients found a significant reduction in BP of 3.2/2.0 mmHg and 4.5/3.2 mmHg respectively[276,279]. The BP reduction is the greatest in those with the highest baseline BP and those with at least 50%-70% cocoa at doses of 6 to 100 g/d[280,282]. Cocoa may also improve insulin resistance and endothelial function[276,279,281].
Polyphenols, chlorogenic acids (CGAs), the ferulic acid metabolite of CGAs and di-hydro-caffeic acids decrease BP in a dose dependent manner, increase eNOS and improve endothelial function in humans[284-286]. CGAs in green coffee been extract at doses of 140 mg/d significantly reduced SBP and DBP in 28 subjects in a placebocontrolled randomized clinical trial. A study of 122 male subjects demonstrated a dose response in SBP and DBP with doses of CGA from 46 mg/d to 185 mg/d. The group that received the 185 mg dose had a significant reduction in BP of 5.6/3.9 mmHg (p < 0.01) over 28 d. Hydroxyhydroquinone is another component of coffee beans which reduces the efficacy of CGAs in a dosedependent manner which partially explains the conflicting results of coffee ingestion on BP[284,286]. Furthermore, there is genetic variation in the enzyme responsible for the metabolism of caffeine modifies the association between coffee intake, amount of coffee ingested and the risk of hypertension, heart rate, MI, arterial stiffness, arterial wave reflections and urinary catecholamine levels[287]. Fifty-nine percent of the population has the? F/?A allele of the CYP1A2 genotype which confers slow metabolism of caffeine. Heavy coffee drinkers who are slow metabolizers had a 3.00 HR for developing hypertension. In contrast, fast metabolizers with the?A/? A allele have a 0.36 HR for incident hypertension[288].
Additional Compounds
Melatonin demonstrates significant anti-hypertensive effects in humans in a numerous double-blind randomized placebo controlled clinical trials at 3-5 mg/d[289-299]. The average reduction in BP is 6/3 mmHg. Melatonin stimulates GABA receptors in the CNS and vascular melatonin receptors, inhibits plasma A ? levels, improves endothelial function, increases NO, vasodilates, improves nocturnal dipping, lowers cortisol and is additive with ARBs. Beta blockers reduce melatonin secretion[300].
Hesperidin significantly lowered DBP 3-4 mmHg (p < 0.02) and improved microvascular endothelial reactivity in 24 obese hypertensive male subjects in a randomized, controlled crossover study over 4 wk for each of three treatment groups consuming 500 ml of orange juice, hesperidin or placebo[301].
Pomegranate juice is rich in tannins and has numerous other properties that improve vascular health and reduces the SBP by 5%-12%[302,303]. A study of 51 healthy subjects given 330 mg/d of pomegranate juice had reduction in BP of 3.14/2.33 mmHg (p < 0.001)[303]. Pomegranate juice also suppresses the postprandial increase in SBP following a high-fat meal[303]. Pomegranate juice reduces serum ACE activity by 36%, and has anti-atherogenic, antioxidant and anti-inflammatory effects[302,303]. Pomegranate juice at 50 ml/d reduced carotid IMT by 30% over one year, increased PON 83%, decreased oxLDL by 59%-90%, decreased antibodies to oxLDL by 19%, increased total antioxidant status by 130 %, reduced TGF-?, increased catalase, SOD and GPx, increased eNOS and NO and improved endothelial function[304,305]�Pomegranate juice works like an ACEI.
Grape seed extract (GSE) was administered to subjects in nine randomized trials, meta-analysis of 390 subjects and demonstrated a significant reduction in SBP of 1.54 mmHg (P < 0.02)[304,305]. Significant reduction in BP of 11/8 mmHg (P < 0.05) were seen in another dose response study with 150 to 300 mg/d of GSE over 4 wk[306]. GSE has high phenolic content which activates the PI3K/Akt signaling pathway that phosphorylates eNOS and increases NO[306,307].
Coenzyme Q10 (Ubiquinone)
Coenzyme Q10 has consistent and significant antihypertensive effects in patients with essential hypertension[1,308-317]. The literature is summarized below: (1) Compared to normotensive patients, essential hypertensive patients have a higher incidence (6 fold) of coenzyme Q10 deficiency documented by serum levels[1]; (2) Doses of 120 to 225 mg/d of coenzyme Q10, depending on the delivery method or the concomitant ingestion with a fatty meal, are necessary to achieve a therapeutic level of 3 ug/ml[1,313,314]. This dose is usually 3-5 mg/kg per day of coenzyme Q10. Oral dosing levels may become lower with nanoparticle and emulsion delivery systems intended to facilitate absorption[315]. Adverse effects have not been characterized in the literature; (3) Patients with the lowest coenzyme Q10 serum levels may have the best antihypertensive response to supplementation; (4) The average reduction in BP is about 15/10 mmHg and heart rate falls 5 beats/min based on reported studies and metaanalysis; (5) The antihypertensive effect takes time to reach its peak level at 4 wk. Then the BP remains stable during long term treatment. The antihypertensive effect is gone within two weeks after discontinuation of coenzyme Q10. The reduction in BP and SVR are correlated with the pretreatment and post treatment serum levels of coenzyme Q10. About 50% of patients respond to oral coenzyme Q10 supplementation for BP[309]; (6) Approximately 50% of patients on antihypertensive drugs may be able to stop between one and three agents. Both total dose and frequency of administration may be reduced. (7) Patients administered coenzyme Q10 with enalapril improved the 24 h ABM better than with enalapril monotherapy and also normalized endothelial function[310]; and (8) Coenzyme Q10 is a lipid phase antioxidant and free radical scavenger, increases eNOS and NO, reduces inflammation and NF-?B and improves endothelial function and vascular elasticity[1,311,312].
Other favorable effects on cardiovascular risk factors include improvement in the serum lipid profile and carbohydrate metabolism with reduced glucose and improved insulin sensitivity, reduced oxidative stress, reduced heart rate, improved myocardial LV function and oxygen delivery and decreased catecholamine levels[1,311,312].
Alpha Lipoic Acid
Alpha lipoic acid (ALA) is known as thioctic acid in Europe where it is a prescription medication. It is a sulfurcontaining compound with antioxidant activity both in water and lipid phases[1,70,71]. Its use is well-established in the treatment of certain forms of liver disease and in the delay of onset of peripheral neuropathy in patients with diabetes. Recent research has evaluated its potential role in the treatment of hypertension, especially as part of the MS[318-321]. In a double-blind cross over study of 36 patients over 8 wk with CHD and hypertension, 200 mg of lipoic acid with 500 mg of acetyl-L-carnitine significantly reduced BP 7/3 mmHg and increased brachial artery diameter[320]. The QUALITY study of 40 patients with DM and stage?hypertension showed significant improvements in BP, urinary albumin excretion, FMD and insulin sensitivity over 8 wk with a combination of Quinapril (40 mg/d) and lipoic acid (600 mg/d) that was greater than either alone[320]. Lipoic acid increases levels of glutathione, cysteine, vitamin C and vitamin E, inhibits NF-?B, reduces endothelin-1, tissue factor and VCAM-1, increases cAMP, downregulates CD4 immune expression on mononuclear cells, reduces oxidative stress, inflammation, reduces atherosclerosis in animal models, decreases serum aldehydes and closes calcium channels which improves vasodilation, increases NO and nitrosothiols, improves endothelial function and lowers BP[1,318-321]. Lipoic acid normalizes membrane calcium channels by providing sulfhydryl groups, decreasing cytosolic free calcium and lowers SVR. In addition, lipoic acid improves insulin sensitivity which lowers glucose and advanced glycosylation end products which improves BP control and lowers serum triglycerides. Morcos et al[321], showed stabilization of urinary albumin excretion in DM subjects given 600 mg of ALA compared to placebo for 18 mo (p < 0.05).
The recommended dose is 100 to 200 mg/d of R-lipoic acid with biotin 2-4 mg/d to prevent biotin depletion with long term use of lipoic acid. R-lipoic acid is preferred to the L isomer because of its preferred use by the mitochondria[1,32,71]. NAC: NAC and L arginine (ARG) in combination reduce endothelial activation and BP in hypertensive patients with type 2 DM[141]. Over 6 mo 24 subjects given placebo or NAC with ARG, significantly reduced both systolic and diastolic BP (p = 0.05)[141]. In addition, ox LDL, HSCRP, ICAM, VCAM, fibrinogen and PAI-1 were decreased while HDL, NO and endothelial postischemic vasodilation increased[141]. NAC increases NO via IL-1b and increases iNOS MRNA, increases glutathione by increasing cysteine levels, reduces the affinity for the AT1 receptor by disrupting disulfide groups, blocks the L type calcium channel, lowers homocysteine, and improves IMT[141,322-324]. The recommended dose is 500 to 1000 mg bid. Hawthorne extract has been used for centuries for the treatment of hypertension, CHF and other cardiovascular diseases[325-329]. A recent four-period crossover design, dose response study in 21 subjects with prehypertension or mild hypertension over 3� d, did not show changes in FMD or BP on standardized extract with 50 mg of oligomeric procyanidin per 250 mg extract with 1000 mg, 1500 or 2500 mg of the extract[325]. Hawthorne showed non inferiority of ACEI and diuretics in the treatment of
NAC: NAC and L arginine (ARG) in combination reduce endothelial activation and BP in hypertensive patients with type 2 DM[141]. Over 6 mo 24 subjects given placebo or NAC with ARG, significantly reduced both systolic and diastolic BP (p = 0.05)[141]. In addition, ox LDL, HSCRP, ICAM, VCAM, fibrinogen and PAI-1 were decreased while HDL, NO and endothelial postischemic vasodilation increased[141]. NAC increases NO via IL-1b and increases iNOS MRNA, increases glutathione by increasing cysteine levels, reduces the affinity for the AT1 receptor by disrupting disulfide groups, blocks the L type calcium channel, lowers homocysteine, and improves IMT[141,322-324]. The recommended dose is 500 to 1000 mg bid.
Hawthorne extract has been used for centuries for the treatment of hypertension, CHF and other cardiovascular diseases[325-329]. A recent four-period crossover design, dose response study in 21 subjects with prehypertension or mild hypertension over 3� d, did not show changes in FMD or BP on standardized extract with 50 mg of oligomeric procyanidin per 250 mg extract with 1000 mg, 1500 or 2500 mg of the extract[325]. Hawthorne showed non inferiority of ACEI and diuretics in the treatment of�102 patients with NYHC ? CHF over 8 wk[327]. Patients with hypertension and type 2 DM on medications for BP and DM were randomized to 1200 mg of hawthorne extract for 16 wk showed significant reductions in DBP of 2.6 mmHg (p = 0.035)[328]. Thirty six mildly hypertensive patients were administered 500 mg of hawthorne extract for 10 wk and showed a non significant trend in DBP reduction (p = 0.081) compared to placebo[329]. Hawthorne acts like an ACEI, BB, CCB and diuretic. More studies are needed to determine the efficacy, long term effects and dose of hawthorne for the treatment of hypertension.
Quercetin is an antioxidant flavonol found in apples, berries and onions that reduces BP in hypertensive individuals[330,331] but the hypotensive effects do not appear to be mediated by changes in HSCRP, TNF-?, ACE activity, ET-1, NO, vascular reactivity or FMD[330]. Quercetin is metabolized by CYP 3A4. Quercetin was administered to 12 hypertensive men at an oral dose of 1095 mg with reduction in mean BP by 5 mmHg, SBP by 7 mmHg and DBP by 3 mmHg[330]. The maximal plasma level at 10 h was 2.3 � 1.8 ?mol/L, with return to baseline levels at 17 h. Forty one pre-hypertensive and stage?hypertensive subjects were enrolled in a randomized, double-blind, placebo-controlled, crossover study with 730 mg of quercetin per day vs placebo[331]. In the stage?hypertensive patients, the BP was reduced by 7/5 mmHg (p < 0.05) but there were no changes in oxidative stress markers[331]. Quercetin administered to 93 overweight or obese subjects at 150 mg/d (plasma levels of 269 nmol/L) over 6 wk lowered SBP 2.9 mmHg in the hypertensive group and up to 3.7 mmHg in SBP in the patients 25-50 years of age[332]. The recommended dose of quercetin is 500 mg bid.
CLINICAL CONSIDERATIONS
Combining Food And Nutrients With Medications
Several of the strategic combinations of nutraceutical supplements together or with anti-hypertensive drugs, have been shown to lower BP more than the medication alone: (1) Sesame with beta blockers, diuretics and nifedipine; (2) Pycnogenol with ACEI and CCB; (3) Lycopene with ACEI, CCB and diuretics; (4) ALA with ACEI or acetyl -L Carnitine; (5) Vitamin C with CCB�s; (6) NAC with arginine; (7) Garlic with ACEI, diuretics and beta blockers; (8) Coenzyme Q10 with ACEI and CCB; (9) Taurine with magnesium; (10) Potassium with all antihypertensive agents; and (11) Magnesium with all antihypertensive agents.
Many anti-hypertensive drugs may cause nutrient depletions that can actually interfere with their anti-hypertensive action or cause other metabolic adverse effects manifest through the lab or with clinical symptoms[333]. Diuretics decrease potassium, magnesium, phosphorous, sodium, chloride, folate, vitamin B6, zinc, iodine and coenzyme Q10; increase homocysteine, calcium and creatinine; and elevate serum glucose by inducing insulin resistance. Beta blockers reduce coenzyme Q10. ACEI and ARB�s reduce zinc.
Vascular biology such as endothelial and VSMD plays a primary role in the initiation and perpetuation of hypertension, CVD and TOD. Nutrient-gene interactions and epigenetics are a predominant factor in promoting beneficial or detrimental effects in cardiovascular health and hypertension. Food and nutrients can prevent, control and treat hypertension through numerous vascular biology mechanisms. Oxidative stress, inflammation and autoimmune dysfunction initiate and propagate hypertension and cardiovascular disease. there is a role for the selected use of single and component nutraceutical supplements vitamins, antioxidants and minerals in the treatment of hypertension based on scientifically controlled studies as a complement to optimal nutritional, dietary intake from food and other lifestyle modifications[333]. A clinical approach which incorporates diet, foods, nutrients, exercise, weight reduction, smoking cessation, alcohol and caffeine restriction, and other lifestyle strategies can be systematically and successfully incorporated into clinical practice (Table 4).
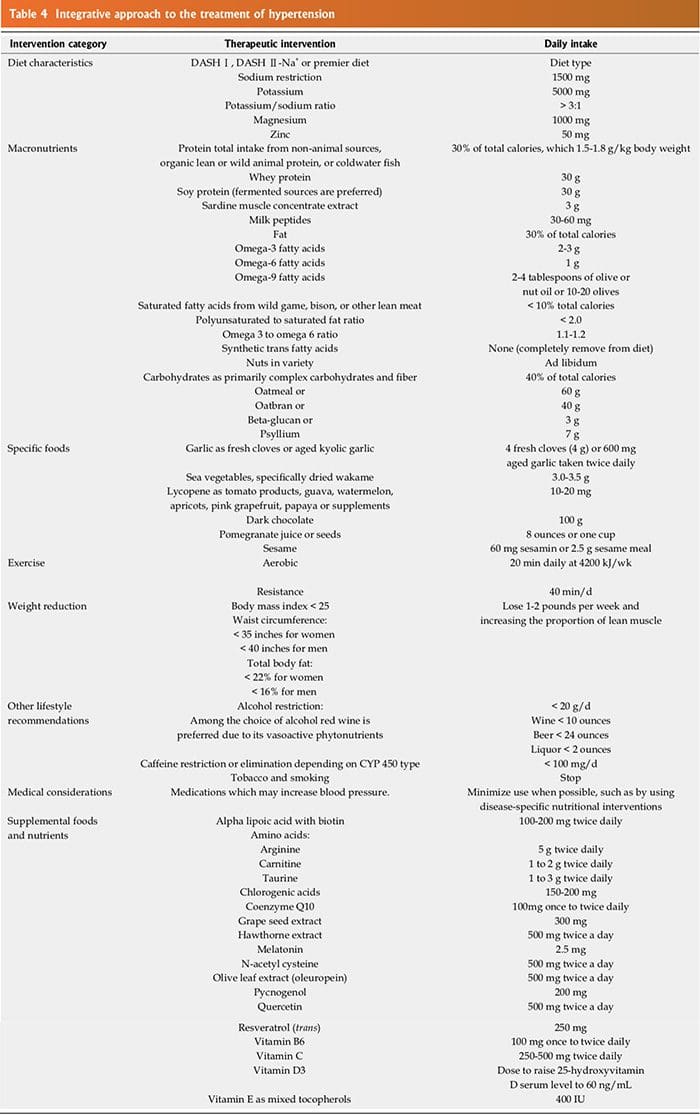
Nutraceutical Conclusion:
Vascular biology, endothelial and vascular smooth muscle and cardiac dysfunction play a primary role in the initiation and perpetuation of hypertension, cardiovascular disease and TOD. Nutrient-gene interactions and epigenetics are predominant factors in promoting beneficial or detrimental effects in cardiovascular health and hypertension. Macronutrients and micronutrients can prevent, control and treat hypertension through numerous mechanisms related to vascular biology. Oxidative stress, inflammation and autoimmune dysfunction initiate and propagate hypertension and cardiovascular disease. There is a role for the selected use of single and component nutraceutical supplements, vitamins, antioxidants and minerals in the treatment of hypertension based on scientifically controlled studies which complement optimal nutrition, coupled with other lifestyle modifications.
blank
References:
1 Houston MC. Treatment of hypertension with nutraceuticals, vitamins, antioxidants and minerals. Expert Rev�Cardiovasc Ther 2007; 5: 681-691 [PMID: 17605647 DOI: 10.1159/000098012]
2 Eaton SB, Eaton SB, Konner MJ. Paleolithic nutrition revisited:
a twelve-year retrospective on its nature and implications.
Eur J Clin Nutr 1997; 51: 207-216 [PMID: 9104571 DOI:
10.1038/sj.ejcn.1600389]
3 Houston MC, Harper KJ. Potassium, magnesium, and calcium:
their role in both the cause and treatment of hypertension.
J Clin Hypertens (Greenwich) 2008; 10: 3-11 [PMID:
18607145 DOI: 10.1111/j.1751-7176.2008.08575.x]
4 Layne J, Majkova Z, Smart EJ, Toborek M, Hennig B. Caveolae:
a regulatory platform for nutritional modulation of inflammatory
diseases. J Nutr Biochem 2011; 22: 807-811 [PMID:
21292468 DOI: 10.1016/j.jnutbio.2010.09.013]
5 Dandona P, Ghanim H, Chaudhuri A, Dhindsa S, Kim SS.
Macronutrient intake induces oxidative and inflammatory
stress: potential relevance to atherosclerosis and insulin
resistance. Exp Mol Med 2010; 42: 245-253 [PMID: 20200475
DOI: 10.3858/emm.2010.42.4.033]
6 Berdanier CD. Nutrient-gene interactions. In: Ziegler EE,
Filer LJ Jr, eds. Present Knowledge in Nutrition, 7th Ed.
Washington. DC: ILSI Press. 1996: 574-580
7 Talmud PJ, Waterworth DM. In-vivo and in-vitro nutrientgene
interactions. Curr Opin Lipidol 2000; 11: 31-36 [PMID:
10750691 DOI: 10.1097/00041433-200002000-00005]
8 Lundberg AM, Yan ZQ. Innate immune recognition receptors
and damage-associated molecular patterns in plaque
inflammation. Curr Opin Lipidol 2011; 22: 343-349 [PMID:
21881501 DOI: 10.1097/MOL.0b013e32834ada80]
9 Zhao L, Lee JY, Hwang DH. Inhibition of pattern recognition
receptor-mediated inflammation by bioactive phytochemicals.
Nutr Rev 2011; 69: 310-320 [PMID: 21631512 DOI:
10.1111/j.1753-4887.2011.00394.x]
10 Houston MC. The importance of potassium in managing
hypertension. Curr Hypertens Rep 2011; 13: 309-317 [PMID:
21403995 DOI: 10.1007/s11906-011-0197-8]
11 Broadhurst CL. Balanced intakes of natural triglycerides for
optimum nutrition: an evolutionary and phytochemical perspective.
Med Hypotheses 1997; 49: 247-261 [PMID: 9293470
DOI: 10.1016/S0306-9877(97)90210-3]
12 Eftekhari A, Mathiassen ON, Buus NH, Gotzsche O, Mulvany
MJ, Christensen KL. Disproportionally impaired microvascular
structure in essential hypertension. J Hypertens
2011; 29: 896-905 [PMID: 21330935 DOI: 10.1097/�HJH.0b013e
3283447a1c]
13 Touyz RM. New insights into mechanisms of hypertension.
Curr Opin Nephrol Hypertens 2012; 21: 119-121 [PMID:
22257800 DOI: 10.1097/MNH.0b013e328350a50f]
14 Xing T, Wang F, Li J, Wang N. Hypertension: an immunologic
disease? J Hypertens 2012; 30: 2440-2441 [PMID:
23151885 DOI: 10.1097/HJH.0b013e32835953f9]
15 Giannattasio C, Cattaneo BM, Mangoni AA, Carugo S, Stella
ML, Failla M, Trazzi S, Sega R, Grassi G, Mancia G. Cardiac
and vascular structural changes in normotensive subjects
with parental hypertension. J Hypertens 1995; 13: 259-264
[PMID: 7615957]
16 Goncharov A, Bloom M, Pavuk M, Birman I, Carpenter
DO. Blood pressure and hypertension in relation to levels of
serum polychlorinated biphenyls in residents of Anniston,
Alabama. J Hypertens 2010; 28: 2053-2060 [PMID: 20644494]
17 Houston MC. Role of mercury toxicity in hypertension, cardiovascular
disease, and stroke. J Clin Hypertens (Greenwich)
2011; 13: 621-627 [PMID: 21806773]
18 Al-Ghamdi A. Role of herpes simplex virus-1, cytomegalovirus
and Epstein-Barr virus in atherosclerosis. Pak J Pharm
Sci 2012; 25: 89-97 [PMID: 22186314]
19 Kotronias D, Kapranos N. Herpes simplex virus as a determinant
risk factor for coronary artery atherosclerosis
and myocardial infarction. In Vivo 2005; 19: 351-357 [PMID:
15796197]
20 Grahame-Clarke C, Chan NN, Andrew D, Ridgway GL,
Betteridge DJ, Emery V, Colhoun HM, Vallance P. Human
cytomegalovirus seropositivity is associated with impaired
vascular function. Circulation 2003; 108: 678-683 [PMID:
12900349 DOI: 10.1161/01.CIR.0000084505.54603.C7]
21 Nayak DU, Karmen C, Frishman WH, Vakili BA. Antioxidant
vitamins and enzymatic and synthetic oxygen-derived
free radical scavengers in the prevention and treatment
of cardiovascular disease. Heart Dis 2001; 3: 28-45 [PMID:
11975768 DOI: 10.1097/00132580-200101000-00006]
22 Kizhakekuttu TJ, Widlansky ME. Natural antioxidants and
hypertension: promise and challenges. Cardiovasc Ther 2010;
28: e20-e32 [PMID: 20370791 DOI: 10.1111/�j.1755-5922.2010.0
0137.x]
23 Kitiyakara C, Wilcox CS. Antioxidants for hypertension.
Curr Opin Nephrol Hypertens 1998; 7: 531-538 [PMID: 9818200
DOI: 10.1097/00041552-199809000-00008]
24 Russo C, Olivieri O, Girelli D, Faccini G, Zenari ML, Lombardi
S, Corrocher R. Anti-oxidant status and lipid peroxidation
in patients with essential hypertension. J Hypertens 1998;
16: 1267-1271 [PMID: 9746113 DOI: 10.1097/00004872-199816
090-00007]
25 Tse WY, Maxwell SR, Thomason H, Blann A, Thorpe GH,
Waite M, Holder R. Antioxidant status in controlled and
uncontrolled hypertension and its relationship to endothelial
damage. J Hum Hypertens 1994; 8: 843-849 [PMID: 7853328]
26 Mansego ML, Solar Gde M, Alonso MP, Mart�nez F, S�ez
GT, Escudero JC, Red�n J, Chaves FJ. Polymorphisms of antioxidant
enzymes, blood pressure and risk of hypertension.
J Hypertens 2011; 29: 492-500 [PMID: 21178785 DOI: 10.1097/
HJH.0b013e328341f1b2]
27 Galley HF, Thornton J, Howdle PD, Walker BE, Webster
NR. Combination oral antioxidant supplementation reduces
blood pressure. Clin Sci (Lond) 1997; 92: 361-365 [PMID:
9176034]
28 Dhalla NS, Temsah RM, Netticadan T. Role of oxidative
stress in cardiovascular diseases. J Hypertens 2000; 18: 655-673
[PMID: 10872549 DOI: 10.1097/00004872-200018060-00002]
29 Saez G, Tormos MC, Giner V, Lorano JV, Chaves FJ, Armengod
ME, Redon J. P-653: Oxidative stress and enzymatic
antioxidant mechanisms in essential hypertension. Am J Hypertens
2001; 14: 248A [DOI: 10.1016/S0895-7061(01)01983-5]
30 Nishihara M, Hirooka Y, Matsukawa R, Kishi T, Sunagawa
K. Oxidative stress in the rostral ventrolateral medulla modulates
excitatory and inhibitory inputs in spontaneously hypertensive
rats. J Hypertens 2012; 30: 97-106 [PMID: 22157590
DOI: 10.1097/HJH.0b013e32834e1df4]
31 Konno S, Hirooka Y, Kishi T, Sunagawa K. Sympathoinhibitory
effects of telmisartan through the reduction of oxidative
stress in the rostral ventrolateral medulla of obesity-induced
hypertensive rats. J Hypertens 2012; 30: 1992-1999 [PMID:
22902874 DOI: 10.1097/HJH.0b013e328357fa98]
32 Ghanem FA, Movahed A. Inflammation in high blood pressure:
a clinician perspective. J Am Soc Hypertens 2007; 1:
113-119 [PMID: 20409841 DOI: 10.1016/j.jash.2007.01.004]
33 Amer MS, Elawam AE, Khater MS, Omar OH, Mabrouk RA,
Taha HM. Association of high-sensitivity C-reactive protein
with carotid artery intima-media thickness in hypertensive
older adults. J Am Soc Hypertens 2011; 5: 395-400 [PMID:
21524639]
34 Vongpatanasin W, Thomas GD, Schwartz R, Cassis LA,
Osborne-Lawrence S, Hahner L, Gibson LL, Black S, Samols
D, Shaul PW. C-reactive protein causes downregulation of
vascular angiotensin subtype 2 receptors and systolic hypertension
in mice. Circulation 2007; 115: 1020-1028 [PMID:
17283257 DOI: 10.1161/CIRCULATIONAHA.106.664854]
35 Razzouk L, Muntner P, Bansilal S, Kini AS, Aneja A, Mozes
J, Ivan O, Jakkula M, Sharma S, Farkouh ME. C-reactive
protein predicts long-term mortality independently of lowdensity
lipoprotein cholesterol in patients undergoing percutaneous coronary intervention. Am Heart J 2009; 158: 277-283 [PMID: 19619706 DOI: 10.1016/j.ahj.2009.05.026]
36 Kvakan H, Luft FC, Muller DN. Role of the immune system
in hypertensive target organ damage. Trends Cardiovasc Med
2009; 19: 242-246 [PMID: 20382349 DOI: 10.1016/�j.�tcm.2010.02.
004]
37 Rodr�guez-Iturbe B, Franco M, Tapia E, Quiroz Y, Johnson
RJ. Renal inflammation, autoimmunity and salt-sensitive hypertension.
Clin Exp Pharmacol Physiol 2012; 39: 96-103 [PMID:
21251049 DOI: 10.1111/j.1440-1681.2011.05482.x]
38 Tian N, Penman AD, Mawson AR, Manning RD, Flessner
MF. Association between circulating specific leukocyte types
and blood pressure: the atherosclerosis risk in communities
(ARIC) study. J Am Soc Hypertens 2010; 4: 272-283 [PMID:
20980213 DOI: 10.1016/j.jash.2010.09.005]
39 Muller DN, Kvakan H, Luft FC. Immune-related effects in
hypertension and target-organ damage. Curr Opin Nephrol
Hypertens 2011; 20: 113-117 [PMID: 21245763 DOI: 10.1097/
MNH.0b013e3283436f88]
40 Marketou ME, Kontaraki JE, Zacharis EA, Kochiadakis GE,
Giaouzaki A, Chlouverakis G, Vardas PE. TLR2 and TLR4
gene expression in peripheral monocytes in nondiabetic
hypertensive patients: the effect of intensive blood pressurelowering.
J Clin Hypertens (Greenwich) 2012; 14: 330-335
[PMID: 22533660 DOI: 10.1111/j.1751-7176.2012.00620.x]
41 Luft FC. Neural regulation of the immune system modulates
hypertension-induced target-organ damage. J Am Soc Hypertens
2012; 6: 23-26 [PMID: 22047671 DOI: 10.1016/�j.�jash.2011.
09.006]
42 Herrada AA, Campino C, Amador CA, Michea LF, Fardella
CE, Kalergis AM. Aldosterone as a modulator of immunity:
implications in the organ damage. J Hypertens 2011; 29:
1684-1692 [PMID: 21826023 DOI: 10.1097/�HJH.0b013e32834a
4c75]
43 Colussi G, Catena C, Sechi LA. Spironolactone, eplerenone
and the new aldosterone blockers in endocrine and primary
hypertension. J Hypertens 2013; 31: 3-15 [PMID: 23011526
DOI: 10.1097/HJH.0b013e3283599b6a]
44 Appel LJ, Moore TJ, Obarzanek E, Vollmer WM, Svetkey LP,
Sacks FM, Bray GA, Vogt TM, Cutler JA, Windhauser MM,
Lin PH, Karanja N. A clinical trial of the effects of dietary
patterns on blood pressure. DASH Collaborative Research
Group. N Engl J Med 1997; 336: 1117-1124 [PMID: 9099655]
45 Sacks FM, Svetkey LP, Vollmer WM, Appel LJ, Bray GA,
Harsha D, Obarzanek E, Conlin PR, Miller ER, SimonsMorton
DG, Karanja N, Lin PH. Effects on blood pressure
of reduced dietary sodium and the Dietary Approaches to
Stop Hypertension (DASH) diet. DASH-Sodium Collaborative
Research Group. N Engl J Med 2001; 344: 3-10 [PMID:
11136953]
46 Sun B, Williams JS, Svetkey LP, Kolatkar NS, Conlin PR.
Beta2-adrenergic receptor genotype affects the reninangiotensin-aldosterone
system response to the Dietary Approaches
to Stop Hypertension (DASH) dietary pattern. Am
J Clin Nutr 2010; 92: 444-449 [PMID: 20519561 DOI: 10.3945/
ajcn.2009.28924]
47 Chen Q, Turban S, Miller ER, Appel LJ. The effects of dietary
patterns on plasma renin activity: results from the Dietary
Approaches to Stop Hypertension trial. J Hum Hypertens
2012; 26: 664-669 [PMID: 22048714 DOI: 10.1038/jhh.2011.87]
48 Al-Solaiman Y, Jesri A, Zhao Y, Morrow JD, Egan BM. LowSodium
DASH reduces oxidative stress and improves vascular
function in salt-sensitive humans. J Hum Hypertens 2009;
23: 826-835 [PMID: 19404315 DOI: 10.1038/jhh.2009.32]
49 Lin PH, Allen JD, Li YJ, Yu M, Lien LF, Svetkey LP. Blood
Pressure-Lowering Mechanisms of the DASH Dietary Pattern.
J Nutr Metab 2012; 2012: 472396 [PMID: 22496969 DOI:
10.1155/2012/472396]
50 Kotchen TA, McCarron DA. Dietary electrolytes and blood
pressure: a statement for healthcare professionals from the
American Heart Association Nutrition Committee. Circulation
1998; 98: 613-617 [PMID: 9714124]
51 Cutler JA, Follmann D, Allender PS. Randomized trials of
sodium reduction: an overview. Am J Clin Nutr 1997; 65:
643S-651S [PMID: 9022560]
52 Svetkey LP, Sacks FM, Obarzanek E, Vollmer WM, Appel
LJ, Lin PH, Karanja NM, Harsha DW, Bray GA, Aickin M,
Proschan MA, Windhauser MM, Swain JF, McCarron PB,
Rhodes DG, Laws RL. The DASH Diet, Sodium Intake and
Blood Pressure Trial (DASH-sodium): rationale and design.
DASH-Sodium Collaborative Research Group. J Am Diet Assoc
1999; 99: S96-104 [PMID: 10450301 DOI: 10.1016/S0002-
8223(99)00423-X]
53 Kawada T, Suzuki S. Attention of salt awareness to prevent
hypertension in the young. J Clin Hypertens (Greenwich)
2011; 13: 933-934 [PMID: 22142354 DOI: 10.1111/�j.1751-7176.
2011.00555.x]
54 Weinberger MH. Salt sensitivity of blood pressure in humans.
Hypertension 1996; 27: 481-490 [PMID: 8613190 DOI:
10.1161/01.HYP.27.3.481]
55 Morimoto A, Uzu T, Fujii T, Nishimura M, Kuroda S, Nakamura
S, Inenaga T, Kimura G. Sodium sensitivity and cardiovascular
events in patients with essential hypertension.
Lancet 1997; 350: 1734-1737 [PMID: 9413464]
56 Tomonari T, Fukuda M, Miura T, Mizuno M, Wakamatsu
TY, Ichikawa T, Miyagi S, Shirasawa Y, Ito A, Yoshida A,
Omori T, Kimura G. Is salt intake an independent risk factor
of stroke mortality? Demographic analysis by regions in
Japan. J Am Soc Hypertens 2011; 5: 456-462 [PMID: 21890446
DOI: 10.1016/j.jash.2011.07.004]
57 Kanbay M, Chen Y, Solak Y, Sanders PW. Mechanisms and
consequences of salt sensitivity and dietary salt intake. Curr
Opin Nephrol Hypertens 2011; 20: 37-43 [PMID: 21088577 DOI:
10.1097/MNH.0b013e32834122f1]
58 Dubach JM, Das S, Rosenzweig A, Clark HA. Visualizing sodium
dynamics in isolated cardiomyocytes using fluorescent
nanosensors. Proc Natl Acad Sci USA 2009; 106: 16145-16150
[PMID: 19805271 DOI: 10.1073/pnas.0905909106]
59 Oberleithner H, Callies C, Kusche-Vihrog K, Schillers H,
Shahin V, Riethm�ller C, Macgregor GA, de Wardener HE.
Potassium softens vascular endothelium and increases nitric
oxide release. Proc Natl Acad Sci USA 2009; 106: 2829-2834
[PMID: 19202069 DOI: 10.1073/pnas.0813069106]
60 Oberleithner H, Riethm�ller C, Schillers H, MacGregor GA,
de Wardener HE, Hausberg M. Plasma sodium stiffens vascular
endothelium and reduces nitric oxide release. Proc Natl
Acad Sci USA 2007; 104: 16281-16286 [PMID: 17911245 DOI:
10.1073/pnas.0707791104]
61 Fels J, Oberleithner H, Kusche-Vihrog K. M�nage � trois: aldosterone,
sodium and nitric oxide in vascular endothelium.
Biochim Biophys Acta 2010; 1802: 1193-1202 [PMID: 20302930
DOI: 10.1016/j.bbadis.2010.03.006]
62 Oberleithner H, Kusche-Vihrog K, Schillers H. Endothelial
cells as vascular salt sensors. Kidney Int 2010; 77: 490-494
[PMID: 20054292 DOI: 10.1038/ki.2009.490]
63 Kusche-Vihrog K, Callies C, Fels J, Oberleithner H. The
epithelial sodium channel (ENaC): Mediator of the aldosterone
response in the vascular endothelium? Steroids
2010; 75: 544-549 [PMID: 19778545 DOI: 10.1016/�j.steroids.2009.09.003]
64 Fels J, Callies C, Kusche-Vihrog K, Oberleithner H. Nitric
oxide release follows endothelial nanomechanics and not
vice versa. Pflugers Arch 2010; 460: 915-923 [PMID: 20809399
DOI: 10.1007/s00424-010-0871-8]
65 Callies C, Fels J, Liashkovich I, Kliche K, Jeggle P, KuscheVihrog
K, Oberleithner H. Membrane potential depolarization
decreases the stiffness of vascular endothelial cells. J
Cell Sci 2011; 124: 1936-1942 [PMID: 21558418 DOI: 10.1242/
jcs.084657]
66 Kusche-Vihrog K, Urbanova K, Blanqu� A, Wilhelmi M,
Schillers H, Kliche K, Pavenst�dt H, Brand E, Oberleithner
H. C-reactive protein makes human endothelium stiff and tight. Hypertension 2011; 57: 231-237 [PMID: 21149827 DOI: 10.1161/HYPERTENSIONAHA.110.163444]
67 Foulquier S, Dupuis F, Perrin-Sarrado C, Maguin Gat� K,
Merhi-Soussi F, Liminana P, Kwan YW, Capdeville-Atkinson
C, Lartaud I, Atkinson J. High salt intake abolishes AT(2)-
mediated vasodilation of pial arterioles in rats. J Hypertens
2011; 29: 1392-1399 [PMID: 21519278 DOI: 10.1097/�HJH.0b01
3e328347050e]
68 Kusche-Vihrog K, Oberleithner H. An emerging concept of
vascular salt sensitivity. F1000 Biol Rep 2012; 4: 20 [PMID:
23112808 DOI: 10.3410/B4-20]
69 Popov S, Silveira A, W�gs�ter D, Takemori H, Oguro R,
Matsumoto S, Sugimoto K, Kamide K, Hirose T, Satoh M,
Metoki H, Kikuya M, Ohkubo T, Katsuya T, Rakugi H, Imai
Y, Sanchez F, Leosdottir M, Syv�nen AC, Hamsten A, Melander
O, Bertorello AM. Salt-inducible kinase 1 influences
Na(+),K(+)-ATPase activity in vascular smooth muscle cells
and associates with variations in blood pressure. J Hypertens
2011; 29: 2395-2403 [PMID: 22045124 DOI: 10.1097/�HJH.0b01
3e32834d3d55]
70 Houston MC. Nutraceuticals, vitamins, antioxidants, and
minerals in the prevention and treatment of hypertension.
Prog Cardiovasc Dis 2005; 47: 396-449 [PMID: 16115519 DOI:
10.1016/j.pcad.2005.01.004]
71 Houston MC. Nutrition and nutraceutical supplements in
the treatment of hypertension. Expert Rev Cardiovasc Ther
2010; 8: 821-833 [PMID: 20528640 DOI: 10.1586/erc.10.63]
72 Messerli FH, Schmieder RE, Weir MR. Salt. A perpetrator of
hypertensive target organ disease? Arch Intern Med 1997; 157:
2449-2452 [PMID: 9385295 DOI: 10.1001/archinte.1997.00440
420077006]
73 Oliver WJ, Cohen EL, Neel JV. Blood pressure, sodium intake,
and sodium related hormones in the Yanomamo Indians,
a �no-salt� culture. Circulation 1975; 52: 146-151 [PMID:
1132118 DOI: 10.1161/01.CIR.52.1.146]
74 Kawasaki T, Delea CS, Bartter FC, Smith H. The effect of
high-sodium and low-sodium intakes on blood pressure and
other related variables in human subjects with idiopathic hypertension.
Am J Med 1978; 64: 193-198 [PMID: 629267 DOI:
10.1016/0002-9343(78)90045-1]
75 Toda N, Arakawa K. Salt-induced hemodynamic regulation
mediated by nitric oxide. J Hypertens 2011; 29: 415-424 [PMID:
21150639 DOI: 10.1097/HJH.0b013e328341d19e]
76 Whelton PK, He J. Potassium in preventing and treating
high blood pressure. Semin Nephrol 1999; 19: 494-499 [PMID:
10511389]
77 Gu D, He J, Wu X, Duan X, Whelton PK. Effect of potassium
supplementation on blood pressure in Chinese: a randomized,
placebo-controlled trial. J Hypertens 2001; 19: 1325-1331
[PMID: 11446724 DOI: 10.1097/00004872-200107000-00019]
78 He J, Gu D, Kelly TN, Hixson JE, Rao DC, Jaquish CE, Chen
J, Zhao Q, Gu C, Huang J, Shimmin LC, Chen JC, Mu J, Ji X,
Liu DP, Whelton PK. Genetic variants in the renin-angiotensin-aldosterone
system and blood pressure responses to
potassium intake. J Hypertens 2011; 29: 1719-1730 [PMID:
21799445 DOI: 10.1097/HJH.0b013e32834a4d1f]
79 O�Donnell MJ, Yusuf S, Mente A, Gao P, Mann JF, Teo K,
McQueen M, Sleight P, Sharma AM, Dans A, Probstfield J,
Schmieder RE. Urinary sodium and potassium excretion and
risk of cardiovascular events. JAMA 2011; 306: 2229-2238
[PMID: 22110105 DOI: 10.1001/jama.2011.1729]
80 Widman L, Wester PO, Stegmayr BK, Wirell M. The dosedependent
reduction in blood pressure through administration
of magnesium. A double blind placebo controlled crossover
study. Am J Hypertens 1993; 6: 41-45 [PMID: 8427660]
81 Laurant P, Touyz RM. Physiological and pathophysiological
role of magnesium in the cardiovascular system: implications
in hypertension. J Hypertens 2000; 18: 1177-1191 [PMID:
10994748 DOI: 10.1097/00004872-200018090-00003]
82 Houston M. The role of magnesium in hypertension and
cardiovascular disease. J Clin Hypertens (Greenwich) 2011;
13: 843-847 [PMID: 22051430 DOI: 10.1111/�j.1751-7176.2011.0
0538.x]
83 Rosanoff A, Weaver CM, Rude RK. Suboptimal magnesium
status in the United States: are the health consequences underestimated?
Nutr Rev 2012; 70: 153-164 [PMID: 22364157
DOI: 10.1111/j.1753-4887.2011.00465.x]
84 Song Y, Liu S. Magnesium for cardiovascular health: time
for intervention. Am J Clin Nutr 2012; 95: 269-270 [PMID:
22218155 DOI: 10.3945/ajcn.111.031104]
85 Kupetsky-Rincon EA, Uitto J. Magnesium: novel applications
in cardiovascular disease–a review of the literature.
Ann Nutr Metab 2012; 61: 102-110 [PMID: 22907037 DOI:
10.1159/000339380]
86 Cunha AR, Umbelino B, Correia ML, Neves MF. Magnesium
and vascular changes in hypertension. Int J Hypertens 2012;
2012: 754250 [PMID: 22518291 DOI: 10.1155/2012/754250]
87 Kass L, Weekes J, Carpenter L. Effect of magnesium supplementation
on blood pressure: a meta-analysis. Eur J Clin Nutr
2012; 66: 411-418 [PMID: 22318649 DOI: 10.1038/ejcn.2012.4]
88 McCarron DA. Role of adequate dietary calcium intake in
the prevention and management of salt-sensitive hypertension.
Am J Clin Nutr 1997; 65: 712S-716S [PMID: 9022571]
89 Resnick LM. Calcium metabolism in hypertension and allied
metabolic disorders. Diabetes Care 1991; 14: 505-520 [PMID:
1864222 DOI: 10.2337/diacare.14.6.505]
90 Garc�a Zozaya JL, Padilla Viloria M. [Alterations of calcium,
magnesium, and zinc in essential hypertension: their relation
to the renin-angiotensin-aldosterone system]. Invest Clin
1997; 38 Suppl 2: 27-40 [PMID: 9471228]
91 Carpenter WE, Lam D, Toney GM, Weintraub NL, Qin Z.
Zinc, copper, and blood pressure: Human population studies.
Med Sci Monit 2013; 19: 1-8 [PMID: 23291705 DOI: 10.12659/
MSM.883708]
92 Shahbaz AU, Sun Y, Bhattacharya SK, Ahokas RA, Gerling
IC, McGee JE, Weber KT. Fibrosis in hypertensive heart disease:
molecular pathways and cardioprotective strategies. J
Hypertens 2010; 28 Suppl 1: S25-S32 [PMID: 20823713 DOI:
10.1097/01.hjh.0000388491.35836.d2]
93 Bergomi M, Rovesti S, Vinceti M, Vivoli R, Caselgrandi E,
Vivoli G. Zinc and copper status and blood pressure. J Trace
Elem Med Biol 1997; 11: 166-169 [PMID: 9442464 DOI: 10.1016/
S0946-672X(97)80047-8]
94 Stamler J, Elliott P, Kesteloot H, Nichols R, Claeys G, Dyer
AR, Stamler R. Inverse relation of dietary protein markers
with blood pressure. Findings for 10,020 men and women in
the INTERSALT Study. INTERSALT Cooperative Research
Group. INTERnational study of SALT and blood pressure.
Circulation 1996; 94: 1629-1634 [PMID: 8840854 DOI:
10.1161/01.CIR.94.7.1629]
95 Altorf-van der Kuil W, Engberink MF, Brink EJ, van Baak
MA, Bakker SJ, Navis G, van �t Veer P, Geleijnse JM. Dietary
protein and blood pressure: a systematic review. PLoS One
2010; 5: e12102 [PMID: 20711407 DOI: 10.1371/journal.
pone.0012102]
96 Jenkins DJ, Kendall CW, Faulkner DA, Kemp T, Marchie
A, Nguyen TH, Wong JM, de Souza R, Emam A, Vidgen E,
Trautwein EA, Lapsley KG, Josse RG, Leiter LA, Singer W.
Long-term effects of a plant-based dietary portfolio of cholesterol-lowering
foods on blood pressure. Eur J Clin Nutr 2008;
62: 781-788 [PMID: 17457340 DOI: 10.1038/sj.ejcn.1602768]
97 Elliott P, Dennis B, Dyer AR. Relation of dietary protein
(total, vegetable, animal) to blood pressure: INTERMAP
epidemiologic study. Presented at the 18th Scientific Meeting
of the International Society of Hypertension, Chicago, IL,
August 20-24, 2000
98 Rebholz CM, Friedman EE, Powers LJ, Arroyave WD, He J,
Kelly TN. Dietary protein intake and blood pressure: a metaanalysis
of randomized controlled trials. Am J Epidemiol 2012;
176 Suppl 7: S27-S43 [PMID: 23035142 DOI: 10.1093/aje/
kws245]
99 Larsson SC, Virtamo J, Wolk A. Dietary protein intake and�risk of stroke in women. Atherosclerosis 2012; 224: 247-251 [PMID: 22854187]
100 He J, Wofford MR, Reynolds K, Chen J, Chen CS, Myers L,
Minor DL, Elmer PJ, Jones DW, Whelton PK. Effect of dietary
protein supplementation on blood pressure: a randomized,
controlled trial. Circulation 2011; 124: 589-595 [PMID:
21768541 DOI: 10.1161/CIRCULATIONAHA.110.009159]
101 Teunissen-Beekman KF, Dopheide J, Geleijnse JM, Bakker
SJ, Brink EJ, de Leeuw PW, van Baak MA. Protein supplementation
lowers blood pressure in overweight adults: effect
of dietary proteins on blood pressure (PROPRES), a randomized
trial. Am J Clin Nutr 2012; 95: 966-971 [PMID: 22357725
DOI: 10.3945/ajcn.111.029116]
102 FitzGerald RJ, Murray BA, Walsh DJ. Hypotensive peptides
from milk proteins. J Nutr 2004; 134: 980S-988S [PMID:
15051858]
103 Pins JJ, Keenan JM. Effects of whey peptides on cardiovascular
disease risk factors. J Clin Hypertens (Greenwich) 2006; 8:
775-782 [PMID: 17086017 DOI: 10.1111/�j.1524-6175.2006.0566
7.x]
104 Aihara K, Kajimoto O, Hirata H, Takahashi R, Nakamura
Y. Effect of powdered fermented milk with Lactobacillus
helveticus on subjects with high-normal blood pressure or
mild hypertension. J Am Coll Nutr 2005; 24: 257-265 [PMID:
16093403 DOI: 10.1080/07315724.2005.10719473]
105 Germino FW, Neutel J, Nonaka M, Hendler SS. The impact of
lactotripeptides on blood pressure response in stage 1 and stage
2 hypertensives. J Clin Hypertens (Greenwich) 2010; 12: 153-159
[PMID: 20433527 DOI: 10.1111/�j.1751-7176.2009.00250.x]
106 Geleijnse JM, Engberink MF. Lactopeptides and human
blood pressure. Curr Opin Lipidol 2010; 21: 58-63 [PMID:
19884823 DOI: 10.1097/MOL.0b013e3283333813]
107 Cicero AF, Aubin F, Azais-Braesco V, Borghi C. Do the lactotripeptides
isoleucine-proline-proline and valine-prolineproline
reduce systolic blood pressure in European subjects?
A meta-analysis of randomized controlled trials. Am J Hypertens
2013; 26: 442-449 [PMID: 23382495 DOI: 10.1093/ajh/
hps044]
108 Usinger L, Reimer C, Ibsen H. Fermented milk for hypertension.
Cochrane Database Syst Rev 2012; 4: CD008118 [PMID:
22513955 DOI: 10.1002/14651858.CD008118.pub2]
109 Ricci-Cabello I, Herrera MO, Artacho R. Possible role of
milk-derived bioactive peptides in the treatment and prevention
of metabolic syndrome. Nutr Rev 2012; 70: 241-255
[PMID: 22458697 DOI: 10.1111/j.1753-4887.2011.00448.x]
110 Jauhiainen T, Niittynen L, Ore�i? M, J�rvenp�� S, Hiltunen
TP, R�nnback M, Vapaatalo H, Korpela R. Effects of longterm
intake of lactotripeptides on cardiovascular risk factors
in hypertensive subjects. Eur J Clin Nutr 2012; 66: 843-849
[PMID: 22617279 DOI: 10.1038/ejcn.2012.44]
111 Pins JJ, Keenan JM. The antihypertensive effects of a hydrolyzed
whey protein isolate supplement. Cardiovasc Drugs
Ther 2002; 16: 68
112 Pal S, Radavelli-Bagatini S. The effects of whey protein
on cardiometabolic risk factors. Obes Rev 2013; 14: 324-343
[PMID: 23167434 DOI: 10.1111/obr.12005]
113 Zhu CF, Li GZ, Peng HB, Zhang F, Chen Y, Li Y. Therapeutic
effects of marine collagen peptides on Chinese patients
with type 2 diabetes mellitus and primary hypertension. Am
J Med Sci 2010; 340: 360-366 [PMID: 20739874 DOI: 10.1097/
MAJ.0b013e3181edfcf2]
114 De Leo F, Panarese S, Gallerani R, Ceci LR. Angiotensin converting
enzyme (ACE) inhibitory peptides: production and
implementation of functional food. Curr Pharm Des 2009; 15:
3622-3643 [PMID: 19925416 DOI: 10.2174/138161209789271834]
115 Lordan S, Ross RP, Stanton C. Marine bioactives as functional
food ingredients: potential to reduce the incidence
of chronic diseases. Mar Drugs 2011; 9: 1056-1100 [PMID:
21747748 DOI: 10.3390/md9061056]
116 Fujita H, Yoshikawa M. LKPNM: a prodrug-type ACEinhibitory
peptide derived from fish protein. Immunopharmacology
1999; 44: 123-127 [PMID: 10604535 DOI: 10.1016/�S0162
-3109(99)00118-6]
117 Kawasaki T, Seki E, Osajima K, Yoshida M, Asada K, Matsui
T, Osajima Y. Antihypertensive effect of valyl-tyrosine, a
short chain peptide derived from sardine muscle hydrolyzate,
on mild hypertensive subjects. J Hum Hypertens 2000;
14: 519-523 [PMID: 10962520 DOI: 10.1038/sj.jhh.1001065]
118 Kawasaki T, Jun CJ, Fukushima Y, Kegai K, Seki E, Osajima
K, Itoh K, Matsui T, Matsumoto K. [Antihypertensive effect
and safety evaluation of vegetable drink with peptides
derived from sardine protein hydrolysates on mild hypertensive,
high-normal and normal blood pressure subjects].
Fukuoka Igaku Zasshi 2002; 93: 208-218 [PMID: 12471719]
119 Yang G, Shu XO, Jin F, Zhang X, Li HL, Li Q, Gao YT, Zheng
W. Longitudinal study of soy food intake and blood pressure
among middle-aged and elderly Chinese women. Am J
Clin Nutr 2005; 81: 1012-1017 [PMID: 15883423]
120 Dong JY, Tong X, Wu ZW, Xun PC, He K, Qin LQ. Effect
of soya protein on blood pressure: a meta-analysis of randomised
controlled trials. Br J Nutr 2011; 106: 317-326 [PMID:
21342608 DOI: 10.1017/S0007114511000262]
121 Teede HJ, Giannopoulos D, Dalais FS, Hodgson J, McGrath
BP. Randomised, controlled, cross-over trial of soy protein
with isoflavones on blood pressure and arterial function in
hypertensive subjects. J Am Coll Nutr 2006; 25: 533-540 [PMID:
17229901 DOI: 10.1080/07315724.2006.10719569]
122 Welty FK, Lee KS, Lew NS, Zhou JR. Effect of soy nuts on
blood pressure and lipid levels in hypertensive, prehypertensive,
and normotensive postmenopausal women. Arch
Intern Med 2007; 167: 1060-1067 [PMID: 17533209 DOI:
10.1001/archinte.167.10.1060]
123 Rosero Arenas MA, Rosero Arenas E, Portaceli Armi�ana
MA, Garc�a Garc�a MA. [Usefulness of phyto-oestrogens in
reduction of blood pressure. Systematic review and metaanalysis].
Aten Primaria 2008; 40: 177-186 [PMID: 18405582]
124 Nasca MM, Zhou JR, Welty FK. Effect of soy nuts on adhesion
molecules and markers of inflammation in hypertensive
and normotensive postmenopausal women. Am
J Cardiol 2008; 102: 84-86 [PMID: 18572041 DOI: 10.1016/
j.amjcard.2008.02.100]
125 He J, Gu D, Wu X, Chen J, Duan X, Chen J, Whelton PK.
Effect of soybean protein on blood pressure: a randomized,
controlled trial. Ann Intern Med 2005; 143: 1-9 [PMID:
15998749 DOI: 10.7326/0003-4819-143-1-200507050-00004]
126 Hasler CM, Kundrat S, Wool D. Functional foods and cardiovascular
disease. Curr Atheroscler Rep 2000; 2: 467-475
[PMID: 11122780 DOI: 10.1007/s11883-000-0045-9]
127 Tikkanen MJ, Adlercreutz H. Dietary soy-derived isoflavone
phytoestrogens. Could they have a role in coronary
heart disease prevention? Biochem Pharmacol 2000; 60: 1-5
[PMID: 10807939]
128 Begg DP, Sinclair AJ, Stahl LA, Garg ML, Jois M, Weisinger
RS. Dietary protein level interacts with omega-3 polyunsaturated
fatty acid deficiency to induce hypertension. Am J
Hypertens 2010; 23: 125-128 [PMID: 19893499 DOI: 10.1038/
ajh.2009.198]
129 Vallance P, Leone A, Calver A, Collier J, Moncada S. Endogenous
dimethylarginine as an inhibitor of nitric oxide
synthesis. J Cardiovasc Pharmacol 1992; 20 Suppl 12: S60-S62
[PMID: 1282988 DOI: 10.1097/00005344-199204002-00018]
130 Sonmez A, Celebi G, Erdem G, Tapan S, Genc H, Tasci I,
Ercin CN, Dogru T, Kilic S, Uckaya G, Yilmaz MI, Erbil MK,
Kutlu M. Plasma apelin and ADMA Levels in patients with
essential hypertension. Clin Exp Hypertens 2010; 32: 179-183
[PMID: 20504125 DOI: 10.3109/10641960903254505]
131 Michell DL, Andrews KL, Chin-Dusting JP. Endothelial
dysfunction in hypertension: the role of arginase. Front Biosci
(Schol Ed) 2011; 3: 946-960 [PMID: 21622244]
132 Rajapakse NW, Mattson DL. Role of L-arginine in nitric oxide
production in health and hypertension. Clin Exp Pharmacol
Physiol 2009; 36: 249-255 [PMID: 19076168 DOI: 10.1111/j.1440-1681.2008.05123.x]
133 Tsioufis C, Dimitriadis K, Andrikou E, Thomopoulos C,
Tsiachris D, Stefanadi E, Mihas C, Miliou A, Papademetriou
V, Stefanadis C. ADMA, C-reactive protein, and albuminuria
in untreated essential hypertension: a cross-sectional study.
Am J Kidney Dis 2010; 55: 1050-1059 [PMID: 20189274 DOI:
10.1053/j.ajkd.2009.11.024]
134 Rajapakse NW, Mattson DL. Role of cellular L-arginine
uptake and nitric oxide production on renal blood flow and
arterial pressure regulation. Curr Opin Nephrol Hypertens
2013; 22: 45-50 [PMID: 23095292 DOI: 10.1097/�MNH.0b013e
32835a6ff7]
135 Ruiz-Hurtado G, Delgado C. Nitric oxide pathway in hypertrophied
heart: new therapeutic uses of nitric oxide donors.
J Hypertens 2010; 28 Suppl 1: S56-S61 [PMID: 20823718 DOI:
10.1097/01.hjh.0000388496.66330.b8]
136 Siani A, Pagano E, Iacone R, Iacoviello L, Scopacasa F, Strazzullo
P. Blood pressure and metabolic changes during dietary
L-arginine supplementation in humans. Am J Hypertens
2000; 13: 547-551 [PMID: 10826408 DOI: 10.1016/�S0895-7061(
99)00233-2]
137 Facchinetti F, Saade GR, Neri I, Pizzi C, Longo M, Volpe
A. L-arginine supplementation in patients with gestational
hypertension: a pilot study. Hypertens Pregnancy 2007; 26:
121-130 [PMID: 17454224 DOI: 10.1080/10641950601147994]
138 Neri I, Monari F, Sgarbi L, Berardi A, Masellis G, Facchinetti
F. L-arginine supplementation in women with chronic hypertension:
impact on blood pressure and maternal and neonatal
complications. J Matern Fetal Neonatal Med 2010; 23: 1456-1460
[PMID: 20958228 DOI: 10.3109/14767051003677962]
139 Martina V, Masha A, Gigliardi VR, Brocato L, Manzato E,
Berchio A, Massarenti P, Settanni F, Della Casa L, Bergamini
S, Iannone A. Long-term N-acetylcysteine and L-arginine
administration reduces endothelial activation and systolic
blood pressure in hypertensive patients with type 2 diabetes.
Diabetes Care 2008; 31: 940-944 [PMID: 18268065 DOI:
10.2337/dc07-2251]
140 Ast J, Jablecka A, Bogdanski P, Smolarek I, Krauss H, Chmara
E. Evaluation of the antihypertensive effect of L-arginine
supplementation in patients with mild hypertension assessed
with ambulatory blood pressure monitoring. Med Sci
Monit 2010; 16: CR266-CR271 [PMID: 20424555]
141 Dong JY, Qin LQ, Zhang Z, Zhao Y, Wang J, Arigoni F,
Zhang W. Effect of oral L-arginine supplementation on
blood pressure: a meta-analysis of randomized, doubleblind,
placebo-controlled trials. Am Heart J 2011; 162: 959-965
[PMID: 22137067 DOI: 10.1016/j.ahj.2011.09.012]
142 Miller GD, Marsh AP, Dove RW, Beavers D, Presley T,
Helms C, Bechtold E, King SB, Kim-Shapiro D. Plasma nitrate
and nitrite are increased by a high-nitrate supplement but
not by high-nitrate foods in older adults. Nutr Res 2012; 32:
160-168 [PMID: 22464802 DOI: 10.1016/j.nutres.2012.02.002]
143 Schulman SP, Becker LC, Kass DA, Champion HC, Terrin
ML, Forman S, Ernst KV, Kelemen MD, Townsend SN,
Capriotti A, Hare JM, Gerstenblith G. L-arginine therapy in
acute myocardial infarction: the Vascular Interaction With
Age in Myocardial Infarction (VINTAGE MI) randomized
clinical trial. JAMA 2006; 295: 58-64 [PMID: 16391217 DOI:
10.1001/jama.295.1.58]
144 Miguel-Carrasco JL, Monserrat MT, Mate A, V�zquez CM.
Comparative effects of captopril and l-carnitine on blood
pressure and antioxidant enzyme gene expression in the heart
of spontaneously hypertensive rats. Eur J Pharmacol 2010; 632:
65-72 [PMID: 20123095 DOI: 10.1016/�j.ejphar.2010.01.017]
145 Zambrano S, Blanca AJ, Ruiz-Armenta MV, Miguel-Carrasco
JL, Ar�valo M, V�zquez MJ, Mate A, V�zquez CM. L-Carnitine
protects against arterial hypertension-related cardiac
fibrosis through modulation of PPAR-? expression. Biochem
Pharmacol 2013; 85: 937-944 [PMID: 23295156 DOI: 10.1016/
j.bcp.2012.12.021]
146 Vilskersts R, Kuka J, Svalbe B, Cirule H, Liepinsh E, Grinberga
S, Kalvinsh I, Dambrova M. Administration of L-carnitine
and mildronate improves endothelial function and
decreases mortality in hypertensive Dahl rats. Pharmacol Rep
2011; 63: 752-762 [PMID: 21857086]
147 Mate A, Miguel-Carrasco JL, Monserrat MT, V�zquez CM.
Systemic antioxidant properties of L-carnitine in two different
models of arterial hypertension. J Physiol Biochem 2010; 66:
127-136 [PMID: 20506010 DOI: 10.1007/s13105-010-0017-7]
148 Digiesi V, Cantini F, Bisi G, Guarino G, Brodbeck B. L-carnitine
adjuvant therapy in essential hypertension. Clin Ter
1994; 144: 391-395 [PMID: 7924177]
149 Ghidini O, Azzurro M, Vita G, Sartori G. Evaluation of the
therapeutic efficacy of L-carnitine in congestive heart failure.
Int J Clin Pharmacol Ther Toxicol 1988; 26: 217-220 [PMID:
3403101]
150 Digiesi V, Palchetti R, Cantini F. [The benefits of L-carnitine
therapy in essential arterial hypertension with diabetes mellitus
type II]. Minerva Med 1989; 80: 227-231 [PMID: 2654758]
151 Ruggenenti P, Cattaneo D, Loriga G, Ledda F, Motterlini N,
Gherardi G, Orisio S, Remuzzi G. Ameliorating hypertension
and insulin resistance in subjects at increased cardiovascular
risk: effects of acetyl-L-carnitine therapy. Hypertension 2009;
54: 567-574 [PMID: 19620516]
152 Mate A, Miguel-Carrasco JL, V�zquez CM. The therapeutic
prospects of using L-carnitine to manage hypertension-related
organ damage. Drug Discov Today 2010; 15: 484-492 [PMID:
20363359 DOI: 10.1016/j.drudis.2010.03.014]
153 Korkmaz S, Y?ld?z G, K?l?�l? F, Y?lmaz A, Ayd?n H, I�a?as?o?lu
S, Candan F. [Low L-carnitine levels: can it be a cause of
nocturnal blood pressure changes in patients with type 2 diabetes
mellitus?]. Anadolu Kardiyol Derg 2011; 11: 57-63 [PMID:
21220248 DOI: 10.5152/akd.2011.008]
154 Huxtable RJ. Physiological actions of taurine. Physiol Rev
1992; 72: 101-163 [PMID: 1731369]
155 Fujita T, Ando K, Noda H, Ito Y, Sato Y. Effects of increased
adrenomedullary activity and taurine in young patients with
borderline hypertension. Circulation 1987; 75: 525-532 [PMID:
3815764 DOI: 10.1161/01.CIR.75.3.525]
156 Huxtable RJ, Sebring LA. Cardiovascular actions of taurine.
Prog Clin Biol Res 1983; 125: 5-37 [PMID: 6348796]
157 Feng Y, Li J, Yang J, Yang Q, Lv Q, Gao Y, Hu J. Synergistic
effects of taurine and L-arginine on attenuating insulin resistance
hypertension. Adv Exp Med Biol 2013; 775: 427-435
[PMID: 23392951 DOI: 10.1007/978-1-4614-6130-2_32]
158 W�jcik OP, Koenig KL, Zeleniuch-Jacquotte A, Pearte C,
Costa M, Chen Y. Serum taurine and risk of coronary heart
disease: a prospective, nested case-control study. Eur J Nutr
2013; 52: 169-178 [PMID: 22322924 DOI: 10.1007/�s00394-011-
0300-6]
159 Abebe W, Mozaffari MS. Role of taurine in the vasculature:
an overview of experimental and human studies. Am J Cardiovasc
Dis 2011; 1: 293-311 [PMID: 22254206]
160 Yamori Y, Taguchi T, Hamada A, Kunimasa K, Mori H, Mori
M. Taurine in health and diseases: consistent evidence from
experimental and epidemiological studies. J Biomed Sci 2010; 17
Suppl 1: S6 [PMID: 20804626 DOI: 10.1186/1423-0127-17-S1-S6]
161 Yamori Y, Taguchi T, Mori H, Mori M. Low cardiovascular
risks in the middle aged males and females excreting greater
24-hour urinary taurine and magnesium in 41 WHO-CARDIAC
study populations in the world. J Biomed Sci 2010; 17 Suppl
1: S21 [PMID: 20804596 DOI: 10.1186/1423-0127-17-S1-S21]
162 Tanabe Y, Urata H, Kiyonaga A, Ikeda M, Tanaka H, Shindo
M, Arakawa K. Changes in serum concentrations of taurine
and other amino acids in clinical antihypertensive exercise
therapy. Clin Exp Hypertens A 1989; 11: 149-165 [PMID:
2565773]
163 Mori TA, Bao DQ, Burke V, Puddey IB, Beilin LJ. Docosahexaenoic
acid but not eicosapentaenoic acid lowers ambulatory
blood pressure and heart rate in humans. Hypertension
1999; 34: 253-260 [PMID: 10454450 DOI: 10.1161/01.
HYP.34.2.253]
164 B�naa KH, Bjerve KS, Straume B, Gram IT, Thelle D. Effect
of eicosapentaenoic and docosahexaenoic acids on blood
pressure in hypertension. A population-based intervention
trial from the Troms� study. N Engl J Med 1990; 322: 795-801
[PMID: 2137901 DOI: 10.1056/NEJM199003223221202]
165 Mori TA, Burke V, Puddey I, Irish A, Cowpland CA, Beilin
L, Dogra G, Watts GF. The effects of [omega]3 fatty acids
and coenzyme Q10 on blood pressure and heart rate in
chronic kidney disease: a randomized controlled trial. J Hypertens
2009; 27: 1863-1872 [PMID: 19705518 DOI: 10.1097/
HJH.0b013e32832e1bd9]
166 Ueshima H, Stamler J, Elliott P, Chan Q, Brown IJ, Carnethon
MR, Daviglus ML, He K, Moag-Stahlberg A, Rodriguez
BL, Steffen LM, Van Horn L, Yarnell J, Zhou B. Food
omega-3 fatty acid intake of individuals (total, linolenic acid,
long-chain) and their blood pressure: INTERMAP study. Hypertension
2007; 50: 313-319 [PMID: 17548718]
167 Mori TA. Omega-3 fatty acids and hypertension in humans.
Clin Exp Pharmacol Physiol 2006; 33: 842-846 [PMID: 16922818
DOI: 10.1111/j.1440-1681.2006.04451.x]
168 Noreen EE, Brandauer J. The effects of supplemental fish
oil on blood pressure and morning cortisol in normotensive
adults: a pilot study. J Complement Integr Med 2012; 9:
1553-3840 [PMID: 23104856 DOI: 10.1515/1553-3840.1467]
169 Bhise A, Krishnan PV, Aggarwal R, Gaiha M, Bhattacharjee
J. Effect of low-dose omega-3 fatty acids substitution
on blood pressure, hyperinsulinemia and dyslipidemia in
Indians with essential hypertension: A pilot study. Indian J
Clin Biochem 2005; 20: 4-9 [PMID: 23105526 DOI: 10.1007/
BF02867393]
170 Cabo J, Alonso R, Mata P. Omega-3 fatty acids and blood
pressure. Br J Nutr 2012; 107 Suppl 2: S195-S200 [PMID:
22591893 DOI: 10.1017/S0007114512001584]
171 Huang T, Shou T, Cai N, Wahlqvist ML, Li D. Associations
of plasma n-3 polyunsaturated fatty acids with blood pressure
and cardiovascular risk factors among Chinese. Int J
Food Sci Nutr 2012; 63: 667-673 [PMID: 22263527 DOI: 10.310
9/09637486.2011.652076]
172 Sagara M, Njelekela M, Teramoto T, Taguchi T, Mori M,
Armitage L, Birt N, Birt C, Yamori Y. Effects of docosahexaenoic
Acid supplementation on blood pressure, heart rate,
and serum lipids in Scottish men with hypertension and hypercholesterolemia.
Int J Hypertens 2011; 2011: 809198 [PMID:
21423683 DOI: 10.4061/2011/809198]
173 Passfall J, Philipp T, Woermann F, Quass P, Thiede M,
Haller H. Different effects of eicosapentaenoic acid and olive
oil on blood pressure, intracellular free platelet calcium, and
plasma lipids in patients with essential hypertension. Clin
Investig 1993; 71: 628-633 [PMID: 8219660]
174 Liu JC, Conklin SM, Manuck SB, Yao JK, Muldoon MF.
Long-chain omega-3 fatty acids and blood pressure. Am J
Hypertens 2011; 24: 1121-1126 [PMID: 21753804 DOI: 10.1038/
ajh.2011.120]
175 Engler MM, Schambelan M, Engler MB, Ball DL, Goodfriend
TL. Effects of dietary gamma-linolenic acid on blood pressure
and adrenal angiotensin receptors in hypertensive rats.
Proc Soc Exp Biol Med 1998; 218: 234-237 [PMID: 9648942]
176 Chin JP. Marine oils and cardiovascular reactivity. Prostaglandins
Leukot Essent Fatty Acids 1994; 50: 211-222 [PMID:
8066094 DOI: 10.1016/0952-3278(94)90156-2]
177 Saravanan P, Davidson NC, Schmidt EB, Calder PC. Cardiovascular
effects of marine omega-3 fatty acids. Lancet
2010; 376: 540-550 [PMID: 20638121 DOI: 10.1016/S0140-
6736(10)60445-X]
178 Ferrara LA, Raimondi AS, d�Episcopo L, Guida L, Dello
Russo A, Marotta T. Olive oil and reduced need for antihypertensive
medications. Arch Intern Med 2000; 160: 837-842
[PMID: 10737284 DOI: 10.1001/archinte.160.6.837]
179 Alonso A, Ruiz-Gutierrez V, Mart�nez-Gonz�lez MA. Monounsaturated
fatty acids, olive oil and blood pressure: epidemiological,
clinical and experimental evidence. Public Health
Nutr 2006; 9: 251-257 [PMID: 16571180]
180 Ter�s S, Barcel�-Coblijn G, Benet M, Alvarez R, Bressani R,
Halver JE, Escrib� PV. Oleic acid content is responsible for
the reduction in blood pressure induced by olive oil. Proc
Natl Acad Sci USA 2008; 105: 13811-13816 [PMID: 18772370
DOI: 10.1073/pnas.0807500105]
181 Cherif S, Rahal N, Haouala M, Hizaoui B, Dargouth F,
Gueddiche M, Kallel Z, Balansard G, Boukef K. [A clinical
trial of a titrated Olea extract in the treatment of essential
arterial hypertension]. J Pharm Belg 1996; 51: 69-71 [PMID:
8786521]
182 Psaltopoulou T, Naska A, Orfanos P, Trichopoulos D,
Mountokalakis T, Trichopoulou A. Olive oil, the Mediterranean
diet, and arterial blood pressure: the Greek European
Prospective Investigation into Cancer and Nutrition (EPIC)
study. Am J Clin Nutr 2004; 80: 1012-1018 [PMID: 15447913]
183 Alonso A, Mart�nez-Gonz�lez MA. Olive oil consumption
and reduced incidence of hypertension: the SUN study. Lipids
2004; 39: 1233-1238 [PMID: 15736920 DOI: 10.1007/�s11745
-004-1352-x]
184 Perrinjaquet-Moccetti T, Busjahn A, Schmidlin C, Schmidt
A, Bradl B, Aydogan C. Food supplementation with an olive
(Olea europaea L.) leaf extract reduces blood pressure in borderline
hypertensive monozygotic twins. Phytother Res 2008;
22: 1239-1242 [PMID: 18729245 DOI: 10.1002/ptr.2455]
185 Moreno-Luna R, Mu�oz-Hernandez R, Miranda ML, Costa
AF, Jimenez-Jimenez L, Vallejo-Vaz AJ, Muriana FJ, Villar J,
Stiefel P. Olive oil polyphenols decrease blood pressure and
improve endothelial function in young women with mild
hypertension. Am J Hypertens 2012; 25: 1299-1304 [PMID:
22914255 DOI: 10.1038/ajh.2012.128]
186 Thomsen C, Rasmussen OW, Hansen KW, Vesterlund M,
Hermansen K. Comparison of the effects on the diurnal
blood pressure, glucose, and lipid levels of a diet rich in
monounsaturated fatty acids with a diet rich in polyunsaturated
fatty acids in type 2 diabetic subjects. Diabet Med 1995;
12: 600-606 [PMID: 7554782 DOI: 10.1111/j.1464-5491.1995.
tb00549.x]
187 Perona JS, Ca�izares J, Montero E, S�nchez-Dom�nguez JM,
Catal� A, Ruiz-Guti�rrez V. Virgin olive oil reduces blood
pressure in hypertensive elderly subjects. Clin Nutr 2004; 23:
1113-1121 [PMID: 15380903 DOI: 10.1016/j.clnu.2004.02.004]
188 Perona JS, Montero E, S�nchez-Dom�nguez JM, Ca�izares
J, Garcia M, Ruiz-Guti�rrez V. Evaluation of the effect of
dietary virgin olive oil on blood pressure and lipid composition
of serum and low-density lipoprotein in elderly type
2 diabetic subjects. J Agric Food Chem 2009; 57: 11427-11433
[PMID: 19902947 DOI: 10.1021/jf902321x]
189 Susalit E, Agus N, Effendi I, Tjandrawinata RR, Nofiarny
D, Perrinjaquet-Moccetti T, Verbruggen M. Olive (Olea europaea)
leaf extract effective in patients with stage-1 hypertension:
comparison with Captopril. Phytomedicine 2011; 18:
251-258 [PMID: 21036583 DOI: 10.1016/�j.phymed.2010.08.016]
190 L�pez-Miranda J, P�rez-Jim�nez F, Ros E, De Caterina R,
Badim�n L, Covas MI, Escrich E, Ordov�s JM, Soriguer F,
Abi� R, de la Lastra CA, Battino M, Corella D, ChamorroQuir�s
J, Delgado-Lista J, Giugliano D, Esposito K, Estruch
R, Fernandez-Real JM, Gaforio JJ, La Vecchia C, Lairon D,
L�pez-Segura F, Mata P, Men�ndez JA, Muriana FJ, Osada
J, Panagiotakos DB, Paniagua JA, P�rez-Martinez P, Perona
J, Peinado MA, Pineda-Priego M, Poulsen HE, Quiles JL,
Ram�rez-Tortosa MC, Ruano J, Serra-Majem L, Sol� R, Solanas
M, Solfrizzi V, de la Torre-Fornell R, Trichopoulou
A, Uceda M, Villalba-Montoro JM, Villar-Ortiz JR, Visioli
F, Yiannakouris N. Olive oil and health: summary of the II
international conference on olive oil and health consensus
report, Ja�n and C�rdoba (Spain) 2008. Nutr Metab Cardiovasc
Dis 2010; 20: 284-294 [PMID: 20303720 DOI: 10.1016/
j.numecd.2009.12.007]
191 Zhang J, Villacorta L, Chang L, Fan Z, Hamblin M, Zhu T,
Chen CS, Cole MP, Schopfer FJ, Deng CX, Garcia-Barrio MT,�Feng YH, Freeman BA, Chen YE. Nitro-oleic acid inhibits angiotensin II-induced hypertension. Circ Res 2010; 107: 540-548 [PMID: 20558825 DOI: 10.1161/CIRCRESAHA.110.218404]
192 Scheffler A, Rauwald HW, Kampa B, Mann U, Mohr FW,
Dhein S. Olea europaea leaf extract exerts L-type Ca(2+)
channel antagonistic effects. J Ethnopharmacol 2008; 120:
233-240 [PMID: 18790040 DOI: 10.1016/j.jep.2008.08.018]
193 Papamichael CM, Karatzi KN, Papaioannou TG, Karatzis
EN, Katsichti P, Sideris V, Zakopoulos N, Zampelas A,
Lekakis JP. Acute combined effects of olive oil and wine on
pressure wave reflections: another beneficial influence of
the Mediterranean diet antioxidants? J Hypertens 2008; 26:
223-229 [PMID: 18192835 DOI: 10.1097/�HJH.0b013e3282f25b
80]
194 He J, Whelton PK. Effect of dietary fiber and protein intake
on blood pressure: a review of epidemiologic evidence. Clin
Exp Hypertens 1999; 21: 785-796 [PMID: 10423101 DOI: 10.310
9/10641969909061008]
195 Pruijm M, Wuerzer G, Forni V, Bochud M, Pech�re-Bertschi
A, Burnier M. [Nutrition and hypertension: more than table
salt]. Rev Med Suisse 2010; 6: 1715-1716, 1718-1720, [PMID:
21294306]
196 Sherman DL, Keaney JF, Biegelsen ES, Duffy SJ, Coffman
JD, Vita JA. Pharmacological concentrations of ascorbic acid
are required for the beneficial effect on endothelial vasomotor
function in hypertension. Hypertension 2000; 35: 936-941
[PMID: 10775565]
197 Ness AR, Khaw KT, Bingham S, Day NE. Vitamin C status
and blood pressure. J Hypertens 1996; 14: 503-508 [PMID:
8761901]
198 Duffy SJ, Gokce N, Holbrook M, Huang A, Frei B, Keaney
JF, Vita JA. Treatment of hypertension with ascorbic acid.
Lancet 1999; 354: 2048-2049 [PMID: 10636373 DOI: 10.1016/
S0140-6736(99)04410-4]
199 Enstrom JE, Kanim LE, Klein MA. Vitamin C intake and
mortality among a sample of the United States population.
Epidemiology 1992; 3: 194-202 [PMID: 1591317 DOI: 10.1097/0
0001648-199205000-00003]
200 Block G, Jensen CD, Norkus EP, Hudes M, Crawford PB. Vitamin
C in plasma is inversely related to blood pressure and
change in blood pressure during the previous year in young
Black and White women. Nutr J 2008; 7: 35 [PMID: 19091068
DOI: 10.1186/1475-2891-7-35]
201 Hatzitolios A, Iliadis F, Katsiki N, Baltatzi M. Is the antihypertensive
effect of dietary supplements via aldehydes
reduction evidence based? A systematic review. Clin Exp
Hypertens 2008; 30: 628-639 [PMID: 18855266 DOI: 10.1080/1
0641960802443274]
202 Mahajan AS, Babbar R, Kansal N, Agarwal SK, Ray PC. Antihypertensive
and antioxidant action of amlodipine and vitamin
C in patients of essential hypertension. J Clin Biochem Nutr
2007; 40: 141-147 [PMID: 18188416 DOI: 10.3164/�jcbn.40.141]
203 Leclerc PC, Proulx CD, Arguin G, B�langer S, Gobeil F, Escher
E, Leduc R, Guillemette G. Ascorbic acid decreases the binding
affinity of the AT1 receptor for angiotensin II. Am J Hypertens
2008; 21: 67-71 [PMID: 18091746 DOI: 10.1038/�ajh.2007.1]
204 Plantinga Y, Ghiadoni L, Magagna A, Giannarelli C, Franzoni
F, Taddei S, Salvetti A. Supplementation with vitamins
C and E improves arterial stiffness and endothelial
function in essential hypertensive patients. Am J Hypertens
2007; 20: 392-397 [PMID: 17386345 DOI: 10.1016/�j.amjhyper.2006.09.021]
205 Sato K, Dohi Y, Kojima M, Miyagawa K, Takase H, Katada
E, Suzuki S. Effects of ascorbic acid on ambulatory blood
pressure in elderly patients with refractory hypertension.
Arzneimittelforschung 2006; 56: 535-540 [PMID: 16927536]
206 Block G, Mangels AR, Norkus EP, Patterson BH, Levander
OA, Taylor PR. Ascorbic acid status and subsequent diastolic
and systolic blood pressure. Hypertension 2001; 37: 261-267
[PMID: 11230282 DOI: 10.1161/01.HYP.37.2.261]
207 McRae MP. Is vitamin C an effective antihypertensive supplement?
A review and analysis of the literature. J Chiropr
Med 2006; 5: 60-64 [PMID: 19674673 DOI: 10.1016/�S0899-346
7(07)60134-7]
208 Simon JA. Vitamin C and cardiovascular disease: a review. J
Am Coll Nutr 1992; 11: 107-125 [PMID: 1578086]
209 Ness AR, Chee D, Elliott P. Vitamin C and blood pressure-an
overview. J Hum Hypertens 1997; 11: 343-350 [PMID:
9249227 DOI: 10.1038/sj.jhh.1000423]
210 Trout DL. Vitamin C and cardiovascular risk factors. Am J
Clin Nutr 1991; 53: 322S-325S [PMID: 1985405]
211 Fulwood R, Johnson CL, Bryner JD; National Center for
Health Statistics. Hematological and Nutritional Biochemistry
Reference Data for Persons 6 Months-74 Years of Age:
United States, 1976-1980. Washington, DC; US Public Health
Service; 1982 Vital and Health Statistics series 11, No. 232,
DHHS publication No. (PHS) 83-1682
212 Ward NC, Wu JH, Clarke MW, Puddey IB, Burke V, Croft
KD, Hodgson JM. The effect of vitamin E on blood pressure
in individuals with type 2 diabetes: a randomized, doubleblind,
placebo-controlled trial. J Hypertens 2007; 25: 227-234
[PMID: 17143195]
213 Murray ED, Wechter WJ, Kantoci D, Wang WH, Pham T,
Quiggle DD, Gibson KM, Leipold D, Anner BM. Endogenous
natriuretic factors 7: biospecificity of a natriuretic gammatocopherol
metabolite LLU-alpha. J Pharmacol Exp Ther 1997;
282: 657-662 [PMID: 9262327]
214 Gray B, Swick J, Ronnenberg AG. Vitamin E and adiponectin:
proposed mechanism for vitamin E-induced improvement
in insulin sensitivity. Nutr Rev 2011; 69: 155-161 [PMID:
21348879 DOI: 10.1111/j.1753-4887.2011.00377.x]
215 Lind L, H�nni A, Lithell H, Hvarfner A, S�rensen OH,
Ljunghall S. Vitamin D is related to blood pressure and other
cardiovascular risk factors in middle-aged men. Am J Hypertens
1995; 8: 894-901 [PMID: 8541004 DOI: 10.1016/0895-7061
(95)00154-H]
216 Bednarski R, Donderski R, Manitius J. [Role of vitamin D3
in arterial blood pressure control]. Pol Merkur Lekarski 2007;
23: 307-310 [PMID: 18293857]
217 Ngo DT, Sverdlov AL, McNeil JJ, Horowitz JD. Does vitamin
D modulate asymmetric dimethylarginine and C-reactive
protein concentrations? Am J Med 2010; 123: 335-341 [PMID:
20362753 DOI: 10.1016/j.amjmed.2009.09.024]
218 Rosen CJ. Clinical practice. Vitamin D insufficiency. N Engl
J Med 2011; 364: 248-254 [PMID: 21247315 DOI: 10.1056/
NEJMcp1009570]
219 Pittas AG, Chung M, Trikalinos T, Mitri J, Brendel M, Patel K,
Lichtenstein AH, Lau J, Balk EM. Systematic review: Vitamin
D and cardiometabolic outcomes. Ann Intern Med 2010; 152:
307-314 [PMID: 20194237 DOI: 10.7326/0003-4819-152-5-2010
03020-00009]
220 Motiwala SR, Wang TJ. Vitamin D and cardiovascular disease.
Curr Opin Nephrol Hypertens 2011; 20: 345-353 [PMID:
21519252 DOI: 10.1097/MNH.0b013e3283474985]
221 Bhandari SK, Pashayan S, Liu IL, Rasgon SA, Kujubu DA,
Tom TY, Sim JJ. 25-hydroxyvitamin D levels and hypertension
rates. J Clin Hypertens (Greenwich) 2011; 13: 170-177
[PMID: 21366848 DOI: 10.1111/j.1751-7176.2010.00408.x]
222 Kienreich K, Tomaschitz A, Verheyen N, Pieber TR, Pilz S.
Vitamin D and arterial hypertension: treat the deficiency!
Am J Hypertens 2013; 26: 158 [PMID: 23382398 DOI: 10.1093/
ajh/hps058]
223 Tamez H, Kalim S, Thadhani RI. Does vitamin D modulate
blood pressure? Curr Opin Nephrol Hypertens 2013; 22: 204-209
[PMID: 23299053 DOI: 10.1097/MNH.0b013e32835d919b]
224 Wang L, Ma J, Manson JE, Buring JE, Gaziano JM, Sesso HD.
A prospective study of plasma vitamin D metabolites, vitamin
D receptor gene polymorphisms, and risk of hypertension
in men. Eur J Nutr 2013; 52: 1771-1779 [PMID: 23262750
DOI: 10.1007/s00394-012-0480-8]
225 Pfeifer M, Begerow B, Minne HW, Nachtigall D, Hansen C.
Effects of a short-term vitamin D(3) and calcium supplementation on blood pressure and parathyroid hormone levels in elderly women. J Clin Endocrinol Metab 2001; 86: 1633-1637 [PMID: 11297596 DOI: 10.1210/jc.86.4.1633]
226 Keniston R, Enriquez J Sr. Relationship between blood pressure
and Plasma Vitamin B6 Levels in Healthy Middle-Aged
Adults. Ann N Y Acad Sci 1990; 585: 499-501 [DOI: 10.1111/
j.1749-6632.1990.tb28087.x]
227 Aybak M, Sermet A, Ayyildiz MO, Karakil�ik AZ. Effect of
oral pyridoxine hydrochloride supplementation on arterial
blood pressure in patients with essential hypertension. Arzneimittelforschung
1995; 45: 1271-1273 [PMID: 8595083]
228 Paulose CS, Dakshinamurti K, Packer S, Stephens NL. Sympathetic
stimulation and hypertension in the pyridoxinedeficient
adult rat. Hypertension 1988; 11: 387-391 [PMID:
3356457 DOI: 10.1161/01.HYP.11.4.387]
229 Dakshinamurti K, Lal KJ, Ganguly PK. Hypertension, calcium
channel and pyridoxine (vitamin B6). Mol Cell Biochem
1998; 188: 137-148 [PMID: 9823019]
230 Moline J, Bukharovich IF, Wolff MS, Phillips R. Dietary
flavonoids and hypertension: is there a link? Med
Hypotheses 2000; 55: 306-309 [PMID: 11000057 DOI:
10.1054/�mehy.2000.1057]
231 Knekt P, Reunanen A, J�rvinen R, Sepp�nen R, Heli�vaara
M, Aromaa A. Antioxidant vitamin intake and coronary
mortality in a longitudinal population study. Am J Epidemiol
1994; 139: 1180-1189 [PMID: 8209876]
232 Karatzi KN, Papamichael CM, Karatzis EN, Papaioannou
TG, Aznaouridis KA, Katsichti PP, Stamatelopoulos KS,
Zampelas A, Lekakis JP, Mavrikakis ME. Red wine acutely
induces favorable effects on wave reflections and central
pressures in coronary artery disease patients. Am J Hypertens
2005; 18: 1161-1167 [PMID: 16182104 DOI: 10.1016/�j.amjhyper.2005.03.744]
233 Biala A, Tauriainen E, Siltanen A, Shi J, Merasto S, Louhelainen
M, Martonen E, Finckenberg P, Muller DN, Mervaala
E. Resveratrol induces mitochondrial biogenesis and ameliorates
Ang II-induced cardiac remodeling in transgenic rats
harboring human renin and angiotensinogen genes. Blood
Press 2010; 19: 196-205 [PMID: 20429690 DOI: 10.3109/08037
051.2010.481808]
234 Wong RH, Howe PR, Buckley JD, Coates AM, Kunz I,
Berry NM. Acute resveratrol supplementation improves
flow-mediated dilatation in overweight/obese individuals
with mildly elevated blood pressure. Nutr Metab Cardiovasc
Dis 2011; 21: 851-856 [PMID: 20674311 DOI: 10.1016/
j.numecd.2010.03.003]
235 Bhatt SR, Lokhandwala MF, Banday AA. Resveratrol prevents
endothelial nitric oxide synthase uncoupling and
attenuates development of hypertension in spontaneously
hypertensive rats. Eur J Pharmacol 2011; 667: 258-264 [PMID:
21640096 DOI: 10.1016/j.ejphar.2011.05.026]
236 Rivera L, Mor�n R, Zarzuelo A, Galisteo M. Long-term resveratrol
administration reduces metabolic disturbances and
lowers blood pressure in obese Zucker rats. Biochem Pharmacol
2009; 77: 1053-1063 [PMID: 19100718 DOI: 10.1016/
j.bcp.2008.11.027]
237 Paran E, Engelhard YN. Effect of lycopene, an oral natural
antioxidant on blood pressure. J Hypertens 2001; 19: S74. Abstract
P 1.204
238 Engelhard YN, Gazer B, Paran E. Natural antioxidants
from tomato extract reduce blood pressure in patients with
grade-1 hypertension: a double-blind, placebo-controlled
pilot study. Am Heart J 2006; 151: 100 [PMID: 16368299]
239 Paran E, Novack V, Engelhard YN, Hazan-Halevy I. The effects
of natural antioxidants from tomato extract in treated
but uncontrolled hypertensive patients. Cardiovasc Drugs
Ther 2009; 23: 145-151 [PMID: 19052855 DOI: 10.1007/�s10557
-008-6155-2]
240 Ried K, Frank OR, Stocks NP. Dark chocolate or tomato
extract for prehypertension: a randomised controlled trial.
BMC Complement Altern Med 2009; 9: 22 [PMID: 19583878
DOI: 10.1186/1472-6882-9-22]
241 Paran E, Engelhard Y. P-333: Effect of tomato�s lycopene on
blood pressure, serum lipoproteins, plasma homocysteine
and oxidative stress markers in grade I hypertensive patients.
Am J Hypertens 2001; 14: 141A. Abstract P-333 [DOI:
10.1016/S0895-7061(01)01854-4]
242 Xaplanteris P, Vlachopoulos C, Pietri P, Terentes-Printzios D,
Kardara D, Alexopoulos N, Aznaouridis K, Miliou A, Stefanadis
C. Tomato paste supplementation improves endothelial
dynamics and reduces plasma total oxidative status in
healthy subjects. Nutr Res 2012; 32: 390-394 [PMID: 22652379
DOI: 10.1016/j.nutres.2012.03.011]
243 Hosseini S, Lee J, Sepulveda RT, Rohdewaldc P, Watson
RR. A randomized, double-blind, placebo-controlled, prospective
16 week crossover study to determine the role of
pycnogenol in modifying blood pressure in mildly hypertensive
patients. Nutr Res 2001; 21: 1251-1260 [DOI: 10.1016/
S0271-5317(01)00342-6]
244 Zibadi S, Rohdewald PJ, Park D, Watson RR. Reduction of
cardiovascular risk factors in subjects with type 2 diabetes
by Pycnogenol supplementation. Nutr Res 2008; 28: 315-320
[PMID: 19083426 DOI: 10.1016/j.nutres.2008.03.003]
245 Liu X, Wei J, Tan F, Zhou S, W�rthwein G, Rohdewald P.
Pycnogenol, French maritime pine bark extract, improves
endothelial function of hypertensive patients. Life Sci 2004;
74: 855-862 [PMID: 14659974 DOI: 10.1016/j.lfs.2003.07.037]
246 van der Zwan LP, Scheffer PG, Teerlink T. Reduction of
myeloperoxidase activity by melatonin and pycnogenol may
contribute to their blood pressure lowering effect. Hypertension
2010; 56: e34; author reply e35 [PMID: 20696986 DOI:
10.1161/HYPERTENSIONAHA.110.158170]
247 Cesarone MR, Belcaro G, Stuard S, Sch�nlau F, Di Renzo
A, Grossi MG, Dugall M, Cornelli U, Cacchio M, Gizzi G,
Pellegrini L. Kidney flow and function in hypertension: protective
effects of pycnogenol in hypertensive participants–a
controlled study. J Cardiovasc Pharmacol Ther 2010; 15: 41-46
[PMID: 20097689 DOI: 10.1177/1074248409356063]
248 Simons S, Wollersheim H, Thien T. A systematic review on
the influence of trial quality on the effect of garlic on blood
pressure. Neth J Med 2009; 67: 212-219 [PMID: 19749390]
249 Reinhart KM, Coleman CI, Teevan C, Vachhani P, White
CM. Effects of garlic on blood pressure in patients with and
without systolic hypertension: a meta-analysis. Ann Pharmacother
2008; 42: 1766-1771 [PMID: 19017826 DOI: 10.1345/
aph.1L319]
250 Ried K, Frank OR, Stocks NP. Aged garlic extract lowers
blood pressure in patients with treated but uncontrolled
hypertension: a randomised controlled trial. Maturitas
2010; 67: 144-150 [PMID: 20594781 DOI: 10.1016/�j.maturitas.2010.06.001]
251 Suetsuna K, Nakano T. Identification of an antihypertensive
peptide from peptic digest of wakame (Undaria pinnatifida).
J Nutr Biochem 2000; 11: 450-454 [PMID: 11091100 DOI:
10.1016/S0955-2863(00)00110-8]
252 Nakano T, Hidaka H, Uchida J, Nakajima K, Hata Y. Hypotensive
effects of wakame. J Jpn Soc Clin Nutr 1998; 20: 92
253 Krotkiewski M, Aurell M, Holm G, Grimby G, Szczepanik
J. Effects of a sodium-potassium ion-exchanging seaweed
preparation in mild hypertension. Am J Hypertens 1991; 4:
483-488 [PMID: 1873002 DOI: 10.1093/ajh/4.6.483]
254 Sato M, Oba T, Yamaguchi T, Nakano T, Kahara T, Funayama
K, Kobayashi A, Nakano T. Antihypertensive effects
of hydrolysates of wakame (Undaria pinnatifida) and
their angiotensin-I-converting enzyme inhibitory activity.
Ann Nutr Metab 2002; 46: 259-267 [PMID: 12464726 DOI:
10.1159/000066495]
255 Sato M, Hosokawa T, Yamaguchi T, Nakano T, Muramoto
K, Kahara T, Funayama K, Kobayashi A, Nakano T. Angiotensin
I-converting enzyme inhibitory peptides derived from
wakame (Undaria pinnatifida) and their antihypertensive
effect in spontaneously hypertensive rats. J Agric Food Chem2002; 50: 6245-6252 [PMID: 12358510 DOI: 10.1021/jf020482t]
256 Sankar D, Sambandam G, Ramakrishna Rao M, Pugalendi
KV. Modulation of blood pressure, lipid profiles and redox
status in hypertensive patients taking different edible oils.
Clin Chim Acta 2005; 355: 97-104 [PMID: 15820483 DOI:
10.1016/j.cccn.2004.12.009]
257 Sankar D, Rao MR, Sambandam G, Pugalendi KV. Effect of
sesame oil on diuretics or Beta-blockers in the modulation
of blood pressure, anthropometry, lipid profile, and redox
status. Yale J Biol Med 2006; 79: 19-26 [PMID: 17876372]
258 Miyawaki T, Aono H, Toyoda-Ono Y, Maeda H, Kiso Y,
Moriyama K. Antihypertensive effects of sesamin in humans.
J Nutr Sci Vitaminol (Tokyo) 2009; 55: 87-91 [PMID: 19352068]
259 Wichitsranoi J, Weerapreeyakul N, Boonsiri P, Settasatian
C, Settasatian N, Komanasin N, Sirijaichingkul S, Teerajetgul
Y, Rangkadilok N, Leelayuwat N. Antihypertensive
and antioxidant effects of dietary black sesame meal in prehypertensive
humans. Nutr J 2011; 10: 82 [PMID: 21827664
DOI: 10.1186/1475-2891-10-82]
260 Sudhakar B, Kalaiarasi P, Al-Numair KS, Chandramohan G,
Rao RK, Pugalendi KV. Effect of combination of edible oils
on blood pressure, lipid profile, lipid peroxidative markers,
antioxidant status, and electrolytes in patients with hypertension
on nifedipine treatment. Saudi Med J 2011; 32: 379-385
[PMID: 21483997]
261 Sankar D, Rao MR, Sambandam G, Pugalendi KV. A pilot
study of open label sesame oil in hypertensive diabetics. J
Med Food 2006; 9: 408-412 [PMID: 17004907 DOI: 10.1089/
jmf.2006.9.408]
262 Harikumar KB, Sung B, Tharakan ST, Pandey MK, Joy B,
Guha S, Krishnan S, Aggarwal BB. Sesamin manifests chemopreventive
effects through the suppression of NF-kappa
B-regulated cell survival, proliferation, invasion, and angiogenic
gene products. Mol Cancer Res 2010; 8: 751-761 [PMID:
20460401 DOI: 10.1158/1541-7786.MCR-09-0565]
263 Nakano D, Ogura K, Miyakoshi M, Ishii F, Kawanishi H, Kurumazuka
D, Kwak CJ, Ikemura K, Takaoka M, Moriguchi S,
Iino T, Kusumoto A, Asami S, Shibata H, Kiso Y, Matsumura
Y. Antihypertensive effect of angiotensin I-converting enzyme
inhibitory peptides from a sesame protein hydrolysate
in spontaneously hypertensive rats. Biosci Biotechnol Biochem
2006; 70: 1118-1126 [PMID: 16717411]
264 Karatzi K, Stamatelopoulos K, Lykka M, Mantzouratou
P, Skalidi S, Manios E, Georgiopoulos G, Zakopoulos N,
Papamichael C, Sidossis LS. Acute and long-term hemodynamic
effects of sesame oil consumption in hypertensive
men. J Clin Hypertens (Greenwich) 2012; 14: 630-636 [PMID:
22947362 DOI: 10.1111/j.1751-7176.2012.00649.x]
265 Hodgson JM, Puddey IB, Burke V, Beilin LJ, Jordan N. Effects
on blood pressure of drinking green and black tea. J
Hypertens 1999; 17: 457-463 [PMID: 10404946 DOI: 10.1097/0
0004872-199917040-00002]
266 Kurita I, Maeda-Yamamoto M, Tachibana H, Kamei M.
Antihypertensive effect of Benifuuki tea containing O-methylated
EGCG. J Agric Food Chem 2010; 58: 1903-1908 [PMID:
20078079 DOI: 10.1021/jf904335g]
267 McKay DL, Chen CY, Saltzman E, Blumberg JB. Hibiscus
sabdariffa L. tea (tisane) lowers blood pressure in prehypertensive
and mildly hypertensive adults. J Nutr 2010; 140:
298-303 [PMID: 20018807 DOI: 10.3945/jn.109.115097]
268 Bogdanski P, Suliburska J, Szulinska M, Stepien M, PupekMusialik
D, Jablecka A. Green tea extract reduces blood
pressure, inflammatory biomarkers, and oxidative stress
and improves parameters associated with insulin resistance
in obese, hypertensive patients. Nutr Res 2012; 32: 421-427
[PMID: 22749178 DOI: 10.1016/j.nutres.2012.05.007]
269 Hodgson JM, Woodman RJ, Puddey IB, Mulder T, Fuchs
D, Croft KD. Short-term effects of polyphenol-rich black tea
on blood pressure in men and women. Food Funct 2013; 4:
111-115 [PMID: 23038021 DOI: 10.1039/c2fo30186e]
270 Medina-Rem�n A, Estruch R, Tresserra-Rimbau A, Vallverd�-Queralt A, Lamuela-Raventos RM. The effect of polyphenol
consumption on blood pressure. Mini Rev Med Chem
2013; 13: 1137-1149 [PMID: 22931531]
271 Jim�nez R, Duarte J, Perez-Vizcaino F. Epicatechin: endothelial
function and blood pressure. J Agric Food Chem 2012; 60:
8823-8830 [PMID: 22440087 DOI: 10.1021/jf205370q]
272 Taubert D, Roesen R, Sch�mig E. Effect of cocoa and tea
intake on blood pressure: a meta-analysis. Arch Intern Med
2007; 167: 626-634 [PMID: 17420419 DOI: 10.1001/�archinte.16
7.7.626]
273 Grassi D, Lippi C, Necozione S, Desideri G, Ferri C. Shortterm
administration of dark chocolate is followed by a
significant increase in insulin sensitivity and a decrease in
blood pressure in healthy persons. Am J Clin Nutr 2005; 81:
611-614 [PMID: 15755830]
274 Taubert D, Roesen R, Lehmann C, Jung N, Sch�mig E. Effects
of low habitual cocoa intake on blood pressure and bioactive
nitric oxide: a randomized controlled trial. JAMA 2007;
298: 49-60 [PMID: 17609490 DOI: 10.1001/jama.298.1.49]
275 Cohen DL, Townsend RR. Cocoa ingestion and hypertension-another
cup please? J Clin Hypertens (Greenwich)
2007; 9: 647-648 [PMID: 17673887 DOI: 10.1111/
j.1524-6175.2007.07291.x]
276 Ried K, Sullivan T, Fakler P, Frank OR, Stocks NP. Does
chocolate reduce blood pressure? A meta-analysis. BMC Med
2010; 8: 39 [PMID: 20584271 DOI: 10.1186/1741-7015-8-39]
277 Egan BM, Laken MA, Donovan JL, Woolson RF. Does dark
chocolate have a role in the prevention and management of
hypertension?: commentary on the evidence. Hypertension
2010; 55: 1289-1295 [PMID: 20404213 DOI: 10.1161/HYPERTENSIONAHA.110.151522]
278 Desch S, Kobler D, Schmidt J, Sonnabend M, Adams V,
Sareban M, Eitel I, Bl�her M, Schuler G, Thiele H. Low vs.
higher-dose dark chocolate and blood pressure in cardiovascular
high-risk patients. Am J Hypertens 2010; 23: 694-700
[PMID: 20203627 DOI: 10.1038/ajh.2010.29]
279 Desch S, Schmidt J, Kobler D, Sonnabend M, Eitel I, Sareban
M, Rahimi K, Schuler G, Thiele H. Effect of cocoa products
on blood pressure: systematic review and meta-analysis. Am
J Hypertens 2010; 23: 97-103 [PMID: 19910929 DOI: 10.1038/
ajh.2009.213]
280 Grassi D, Desideri G, Necozione S, Lippi C, Casale R,
Properzi G, Blumberg JB, Ferri C. Blood pressure is reduced
and insulin sensitivity increased in glucose-intolerant, hypertensive
subjects after 15 days of consuming high-polyphenol
dark chocolate. J Nutr 2008; 138: 1671-1676 [PMID: 18716168]
281 Grassi D, Necozione S, Lippi C, Croce G, Valeri L, Pasqualetti
P, Desideri G, Blumberg JB, Ferri C. Cocoa reduces blood
pressure and insulin resistance and improves endotheliumdependent
vasodilation in hypertensives. Hypertension
2005; 46: 398-405 [PMID: 16027246 DOI: 10.1161/01.
HYP.0000174990.46027.70]
282 Ellinger S, Reusch A, Stehle P, Helfrich HP. Epicatechin
ingested via cocoa products reduces blood pressure in
humans: a nonlinear regression model with a Bayesian approach.
Am J Clin Nutr 2012; 95: 1365-1377 [PMID: 22552030
DOI: 10.3945/ajcn.111.029330]
283 Hooper L, Kay C, Abdelhamid A, Kroon PA, Cohn JS, Rimm
EB, Cassidy A. Effects of chocolate, cocoa, and flavan-3-ols
on cardiovascular health: a systematic review and meta-analysis
of randomized trials. Am J Clin Nutr 2012; 95: 740-751
[PMID: 22301923 DOI: 10.3945/ajcn.111.023457]
284 Yamaguchi T, Chikama A, Mori K, Watanabe T, Shioya Y,
Katsuragi Y, Tokimitsu I. Hydroxyhydroquinone-free coffee:
a double-blind, randomized controlled dose-response study
of blood pressure. Nutr Metab Cardiovasc Dis 2008; 18: 408-414
[PMID: 17951035 DOI: 10.1016/j.numecd.2007.03.004]
285 Chen ZY, Peng C, Jiao R, Wong YM, Yang N, Huang Y.
Anti-hypertensive nutraceuticals and functional foods. J
Agric Food Chem 2009; 57: 4485-4499 [PMID: 19422223 DOI:
10.1021/jf900803r]
286 Ochiai R, Chikama A, Kataoka K, Tokimitsu I, Maekawa Y,
Ohishi M, Rakugi H, Mikami H. Effects of hydroxyhydroquinone-reduced
coffee on vasoreactivity and blood pressure.
Hypertens Res 2009; 32: 969-974 [PMID: 19713967 DOI:
10.1038/hr.2009.132]
287 Kozuma K, Tsuchiya S, Kohori J, Hase T, Tokimitsu I. Antihypertensive
effect of green coffee bean extract on mildly
hypertensive subjects. Hypertens Res 2005; 28: 711-718 [PMID:
16419643 DOI: 10.1291/hypres.28.711]
288 Palatini P, Ceolotto G, Ragazzo F, Dorigatti F, Saladini F,
Papparella I, Mos L, Zanata G, Santonastaso M. CYP1A2
genotype modifies the association between coffee intake
and the risk of hypertension. J Hypertens 2009; 27: 1594-1601
[PMID: 19451835 DOI: 10.1097/HJH.0b013e32832ba850]
289 Scheer FA, Van Montfrans GA, van Someren EJ, Mairuhu
G, Buijs RM. Daily nighttime melatonin reduces blood pressure
in male patients with essential hypertension. Hypertension
2004; 43: 192-197 [PMID: 14732734 DOI: 10.1161/01.
HYP.0000113293.15186.3b]
290 Cavallo A, Daniels SR, Dolan LM, Khoury JC, Bean JA.
Blood pressure response to melatonin in type 1 diabetes.
Pediatr Diabetes 2004; 5: 26-31 [PMID: 15043687 DOI: 10.1111
/�j.1399-543X.2004.00031.x]
291 Cavallo A, Daniels SR, Dolan LM, Bean JA, Khoury JC.
Blood pressure-lowering effect of melatonin in type 1 diabetes.
J Pineal Res 2004; 36: 262-266 [PMID: 15066051 DOI:
10.1111/j.1600-079X.2004.00126.x]
292 Cagnacci A, Cannoletta M, Renzi A, Baldassari F, Arangino
S, Volpe A. Prolonged melatonin administration decreases
nocturnal blood pressure in women. Am J Hypertens 2005; 18:
1614-1618 [PMID: 16364834]
293 Grossman E, Laudon M, Yalcin R, Zengil H, Peleg E, Sharabi
Y, Kamari Y, Shen-Orr Z, Zisapel N. Melatonin reduces night
blood pressure in patients with nocturnal hypertension. Am
J Med 2006; 119: 898-902 [PMID: 17000226 DOI: 10.1016/
j.amjmed.2006.02.002]
294 Rechci?ski T, Kurpesa M, Trzos E, Krzeminska-Paku?a M.
[The influence of melatonin supplementation on circadian
pattern of blood pressure in patients with coronary artery
disease–preliminary report]. Pol Arch Med Wewn 2006; 115:
520-528 [PMID: 17263223]
295 Merkur�eva GA, Ryzhak GA. [Effect of the pineal gland peptide
preparation on the diurnal profile of arterial pressure in
middle-aged and elderly women with ischemic heart disease
and arterial hypertension]. Adv Gerontol 2008; 21: 132-142
[PMID: 18546838]
296 Zaslavskaia RM, Shcherban� EA, Logvinenko SI. [Melatonin
in combined therapy of patients with stable angina and arterial
hypertension]. Klin Med (Mosk) 2008; 86: 64-67 [PMID:
19048842]
297 Zamotaev IuN, Enikeev AKh, Kolomoets NM. [The use of
melaxen in combined therapy of arterial hypertension in
subjects occupied in assembly line production]. Klin Med
(Mosk) 2009; 87: 46-49 [PMID: 19670717]
298 Rechci?ski T, Trzos E, Wierzbowska-Drabik K, Krzemi?skaPaku?a
M, Kurpesa M. Melatonin for nondippers with coronary
artery disease: assessment of blood pressure profile and
heart rate variability. Hypertens Res 2010; 33: 56-61 [PMID:
19876062 DOI: 10.1038/hr.2009.174]
299 Kozir�g M, Poliwczak AR, Duchnowicz P, Koter-Michalak
M, Sikora J, Broncel M. Melatonin treatment improves
blood pressure, lipid profile, and parameters of oxidative
stress in patients with metabolic syndrome. J Pineal Res
2011; 50: 261-266 [PMID: 21138476 DOI: 10.1111/j.1600-
079X.2010.00835.x]
300 De Leersnyder H, de Blois MC, Vekemans M, Sidi D, Villain
E, Kindermans C, Munnich A. beta(1)-adrenergic antagonists
improve sleep and behavioural disturbances in a circadian
disorder, Smith-Magenis syndrome. J Med Genet 2001; 38:
586-590 [PMID: 11546826]
301 Morand C, Dubray C, Milenkovic D, Lioger D, Martin JF,
Scalbert A, Mazur A. Hesperidin contributes to the vascular
protective effects of orange juice: a randomized crossover
study in healthy volunteers. Am J Clin Nutr 2011; 93: 73-80
[PMID: 21068346 DOI: 10.3945/ajcn.110.004945]
302 Basu A, Penugonda K. Pomegranate juice: a heart-healthy
fruit juice. Nutr Rev 2009; 67: 49-56 [PMID: 19146506 DOI:
10.1111/j.1753-4887.2008.00133.x]
303 Aviram M, Rosenblat M, Gaitini D, Nitecki S, Hoffman A,
Dornfeld L, Volkova N, Presser D, Attias J, Liker H, Hayek
T. Pomegranate juice consumption for 3 years by patients
with carotid artery stenosis reduces common carotid intimamedia
thickness, blood pressure and LDL oxidation. Clin
Nutr 2004; 23: 423-433 [PMID: 15158307 DOI: 10.1016/�j.
clnu.2003.10.002]
304 Aviram M, Dornfeld L. Pomegranate juice consumption
inhibits serum angiotensin converting enzyme activity and
reduces systolic blood pressure. Atherosclerosis 2001; 158:
195-198 [PMID: 11500191]
305 Feringa HH, Laskey DA, Dickson JE, Coleman CI. The effect
of grape seed extract on cardiovascular risk markers:
a meta-analysis of randomized controlled trials. J Am Diet
Assoc 2011; 111: 1173-1181 [PMID: 21802563 DOI: 10.1016/�j.
jada.2011.05.015]
306 Sivaprakasapillai B, Edirisinghe I, Randolph J, Steinberg
F, Kappagoda T. Effect of grape seed extract on blood pressure
in subjects with the metabolic syndrome. Metabolism
2009; 58: 1743-1746 [PMID: 19608210 DOI: 10.1016/�j.metabol.2009.05.030]
307 Edirisinghe I, Burton-Freeman B, Tissa Kappagoda C. Mechanism
of the endothelium-dependent relaxation evoked by a
grape seed extract. Clin Sci (Lond) 2008; 114: 331-337 [PMID:
17927567 DOI: 10.1042/CS20070264]
308 Rosenfeldt FL, Haas SJ, Krum H, Hadj A, Ng K, Leong JY,
Watts GF. Coenzyme Q10 in the treatment of hypertension: a
meta-analysis of the clinical trials. J Hum Hypertens 2007; 21:
297-306 [PMID: 17287847]
309 Burke BE, Neuenschwander R, Olson RD. Randomized,
double-blind, placebo-controlled trial of coenzyme Q10
in isolated systolic hypertension. South Med J 2001; 94:
1112-1117 [PMID: 11780680 DOI: 10.1097/00007611-20011100
0-00015]
310 Mikhin VP, Kharchenko AV, Rosliakova EA, Cherniatina
MA. [Application of coenzyme Q(10) in combination therapy
of arterial hypertension]. Kardiologiia 2011; 51: 26-31 [PMID:
21878067]
311 Tsai KL, Huang YH, Kao CL, Yang DM, Lee HC, Chou HY,
Chen YC, Chiou GY, Chen LH, Yang YP, Chiu TH, Tsai CS,
Ou HC, Chiou SH. A novel mechanism of coenzyme Q10
protects against human endothelial cells from oxidative
stress-induced injury by modulating NO-related pathways.
J Nutr Biochem 2012; 23: 458-468 [PMID: 21684136 DOI:
10.1016/j.jnutbio.2011.01.011]
312 Sohet FM, Delzenne NM. Is there a place for coenzyme Q
in the management of metabolic disorders associated with
obesity? Nutr Rev 2012; 70: 631-641 [PMID: 23110642 DOI:
10.1111/j.1753-4887.2012.00526.x]
313 Digiesi V, Cantini F, Oradei A, Bisi G, Guarino GC, Brocchi
A, Bellandi F, Mancini M, Littarru GP. Coenzyme Q10
in essential hypertension. Mol Aspects Med 1994; 15 Suppl:
s257-s263 [PMID: 7752838]
314 Langsjoen P, Langsjoen P, Willis R, Folkers K. Treatment of
essential hypertension with coenzyme Q10. Mol Aspects Med
1994; 15 Suppl: S265-S272 [PMID: 7752851 DOI: 10.1016/009
8-2997(94)90037-X]
315 Ankola DD, Viswanad B, Bhardwaj V, Ramarao P, Kumar
MN. Development of potent oral nanoparticulate formulation
of coenzyme Q10 for treatment of hypertension: can
the simple nutritional supplements be used as first line
therapeutic agents for prophylaxis/therapy? Eur J Pharm
Biopharm 2007; 67: 361-369 [PMID: 17452099 DOI: 10.1016/
j.ejpb.2007.03.010]
316 Trimarco V, Cimmino CS, Santoro M, Pagnano G, Manzi
MV, Piglia A, Giudice CA, De Luca N, Izzo R. Nutraceuticals
for blood pressure control in patients with high-normal or
grade 1 hypertension. High Blood Press Cardiovasc Prev 2012;
19: 117-122 [PMID: 22994579 DOI: 10.2165/11632160-0000000
00-00000]
317 Young JM, Florkowski CM, Molyneux SL, McEwan RG,
Frampton CM, Nicholls MG, Scott RS, George PM. A randomized,
double-blind, placebo-controlled crossover study
of coenzyme Q10 therapy in hypertensive patients with the
metabolic syndrome. Am J Hypertens 2012; 25: 261-270 [PMID:
22113168 DOI: 10.1038/ajh.2011.209]
318 McMackin CJ, Widlansky ME, Hamburg NM, Huang AL,
Weller S, Holbrook M, Gokce N, Hagen TM, Keaney JF, Vita
JA. Effect of combined treatment with alpha-Lipoic acid and
acetyl-L-carnitine on vascular function and blood pressure
in patients with coronary artery disease. J Clin Hypertens
(Greenwich) 2007; 9: 249-255 [PMID: 17396066 DOI: 10.1111/
j.1524-6175.2007.06052.x]
319 Salinthone S, Schillace RV, Tsang C, Regan JW, Bourdette
DN, Carr DW. Lipoic acid stimulates cAMP production
via G protein-coupled receptor-dependent and -independent
mechanisms. J Nutr Biochem 2011; 22: 681-690 [PMID:
21036588 DOI: 10.1016/j.jnutbio.2010.05.008]
320 Rahman ST, Merchant N, Haque T, Wahi J, Bhaheetharan S,
Ferdinand KC, Khan BV. The impact of lipoic acid on endothelial
function and proteinuria in quinapril-treated diabetic
patients with stage I hypertension: results from the QUALITY
study. J Cardiovasc Pharmacol Ther 2012; 17: 139-145 [PMID:
21750253 DOI: 10.1177/1074248411413282]
321 Morcos M, Borcea V, Isermann B, Gehrke S, Ehret T, Henkels
M, Schiekofer S, Hofmann M, Amiral J, Tritschler H,
Ziegler R, Wahl P, Nawroth PP. Effect of alpha-lipoic acid on
the progression of endothelial cell damage and albuminuria
in patients with diabetes mellitus: an exploratory study. Diabetes
Res Clin Pract 2001; 52: 175-183 [PMID: 11323087]
322 Jiang B, Haverty M, Brecher P. N-acetyl-L-cysteine enhances
interleukin-1beta-induced nitric oxide synthase expression.
Hypertension 1999; 34: 574-579 [PMID: 10523329]
323 Vasdev S, Singal P, Gill V. The antihypertensive effect of
cysteine. Int J Angiol 2009; 18: 7-21 [PMID: 22477470 DOI:
10.1055/s-0031-1278316]
324 Meister A, Anderson ME, Hwang O. Intracellular cysteine
and glutathione delivery systems. J Am Coll Nutr 1986; 5:
137-151 [PMID: 3722629 DOI: 10.1080/07315724.1986.107201
21]
325 Asher GN, Viera AJ, Weaver MA, Dominik R, Caughey M,
Hinderliter AL. Effect of hawthorn standardized extract on
flow mediated dilation in prehypertensive and mildly hypertensive
adults: a randomized, controlled cross-over trial.
BMC Complement Altern Med 2012; 12: 26 [PMID: 22458601
DOI: 10.1186/1472-6882-12-26]
326 Ko�yildiz ZC, Birman H, Olga� V, Akg�n-Dar K, Meliko?lu
G, Meri�li AH. Crataegus tanacetifolia leaf extract prevents
L-NAME-induced hypertension in rats: a morphological
study. Phytother Res 2006; 20: 66-70 [PMID: 16397846 DOI:
10.1002/ptr.1808]
327 Schr�der D, Weiser M, Klein P. Efficacy of a homeopathic
Crataegus preparation compared with usual therapy for
mild (NYHA II) cardiac insufficiency: results of an observational
cohort study. Eur J Heart Fail 2003; 5: 319-326 [PMID:
12798830 DOI: 10.1016/S1388-9842(02)00237-4]
328 Walker AF, Marakis G, Simpson E, Hope JL, Robinson PA,
Hassanein M, Simpson HC. Hypotensive effects of hawthorn
for patients with diabetes taking prescription drugs: a
randomised controlled trial. Br J Gen Pract 2006; 56: 437-443
[PMID: 16762125]
329 Walker AF, Marakis G, Morris AP, Robinson PA. Promising
hypotensive effect of hawthorn extract: a randomized double-blind
pilot study of mild, essential hypertension. Phytother
Res 2002; 16: 48-54 [PMID: 11807965 DOI: 10.1002/�ptr.947]
330 Larson A, Witman MA, Guo Y, Ives S, Richardson RS, Bruno
RS, Jalili T, Symons JD. Acute, quercetin-induced reductions
in blood pressure in hypertensive individuals are not secondary
to lower plasma angiotensin-converting enzyme activity
or endothelin-1: nitric oxide. Nutr Res 2012; 32: 557-564
[PMID: 22935338 DOI: 10.1016/j.nutres.2012.06.018]
331 Edwards RL, Lyon T, Litwin SE, Rabovsky A, Symons JD,
Jalili T. Quercetin reduces blood pressure in hypertensive
subjects. J Nutr 2007; 137: 2405-2411 [PMID: 17951477]
332 Egert S, Bosy-Westphal A, Seiberl J, K�rbitz C, Settler U,
Plachta-Danielzik S, Wagner AE, Frank J, Schrezenmeir J,
Rimbach G, Wolffram S, M�ller MJ. Quercetin reduces systolic
blood pressure and plasma oxidised low-density lipoprotein
concentrations in overweight subjects with a high-cardiovascular
disease risk phenotype: a double-blinded, placebocontrolled
cross-over study. Br J Nutr 2009; 102: 1065-1074
[PMID: 19402938 DOI: 10.1017/�S0007114509359127]
333 Trovato A, Nuhlicek DN, Midtling JE. Drug-nutrient interactions.
Am Fam Physician 1991; 44: 1651-1658 [PMID: 1950962]