Inflammatory Bowel Disease: The gastrointestinal mucosal barrier is an effective and powerful defense and repair mechanism, which allows for the proper absorption of energy, nutrients and water when we eat. The functioning of the digestive system with its balanced gut microbiota depends on the function of the mucosal barrier. The intestinal barrier has to be permeable to allow the passage of nutrients, however, when this permeability increases beyond what is necessary, it can lead to a variety of issues, in some instances, even causing disease.
What’s the connection between intestinal permeability and IBD?
Intestinal barrier dysfunction has been determined in a variety of gastrointestinal diseases, or GI diseases, such as inflammatory bowel disease, or IBD. It has now become more accepted that proper gastrointestinal mucosal barrier function plays a major role in the pathophysiology of inflammatory bowel disease. However, further understanding as well as research data is required to determine treatment and therapy options for such gastrointestinal diseases, particularly IBD.
Clinical Evaluation of Intestinal Permeability in Inflammatory Bowel Disease
Changes to intestinal permeability generally manifest early in the development of intestinal inflammation due to Crohn’s disease and other gastrointestinal diseases. Several risk factors, including the conditions themselves, may even exacerbate intestinal inflammation through increased intestinal permeability. According to recent research studies, nonsteroidal anti-inflammatory drugs, or NSAIDs, and stress can also induce symptoms of inflammation through increased gastrointestinal, or GI, mucosal permeability and the release of corticotropin-released factors. Additionally, changes to intestinal permeability can determine a patient’s risk of relapsing Crohn’s disease. Patients who’ve had an altered lactulose/mannitol test, or L/M test, are often 8 times more at risk of relapsing, even when asymptomatic and results demonstrate normal biochemical indices.
The lactulose/mannitol test is specifically used to evaluate small intestinal permeability by measuring urinary excretion after oral administration of these sugars. Lactulose�is a large sized oligosaccharide that generally doesn’t carry out paracellular transport and can be adsorbed in the instance of leaky intercellular junctions while mannitol is a smaller molecule that can freely move across the intestinal epithelium. Both probes are equally affected by gastrointestinal dilution, motility, bacterial degradation, and renal function; consequently, the ratio allows for the correction of possible confounding factors. The lactulose/mannitol test is utilized in clinical practice because of its noninvasiveness, its high sensitivity in detecting active inflammatory bowel disease, or IBD, and its ability to distinguish functional versus organic GI disease, or gastrointestinal disease. An altered L/M test has been reported in approximately 50 percent of patients with Crohn’s disease. Other sugars have also been routinely used to evaluate the upper gastrointestinal tract, for instance, sucrose which has been degraded by duodenal sucrase, may indicate the permeability of the stomach and the proximal duodenum. Accordingly, multisugar tests have been developed, with the latest inclusion of sucralose, which can be barely absorbed through the human intestine, allowing a functional assessment of the entire gastrointestinal tract, extending its use for ulcerative colitis as well.
Other functional tests, such as 51Cr-EDTA or the Ussing chambers, have demonstrated great precision in diagnosing gastrointestinal disease, however, their invasiveness and complex detection methods make their use impossible in humans. Whereas promising results have been demonstrated by novel imaging techniques, particularly confocal laser endomicroscopy. This endoscopic technique allows an in vivo evaluation of the epithelial lining and vasculature with the use of intravenous fluorescein as a molecular contrast agent, which generally doesn’t carry out paracellular transport. Confocal laser endomicroscopy is currently widely utilized to identify and classify gastrointestinal tumors but it has also been used in nonneoplastic conditions, such as celiac disease, collagenous colitis, and irritable bowel syndrome, or IBS. Discovering cellular and subcellular changes, such as cell shedding, is possible through this procedure, which makes it a highly effective technique for the imaging of intestinal barrier dysfunction in inflammatory bowel disease, or IBD. Confocal laser endomicroscopy demonstrated increased density of mucosal gaps after cell shedding in the small intestine of patients with Crohn’s disease as well as in macroscopically normal duodenum in both Crohn’s disease and ulcerative colitis. These alterations could represent impairment of intestinal permeability possibly predicting subsequent clinical relapse. Recently, confocal laser endomicroscopy has been utilized in patients with ulcerative colitis, demonstrating that the occurrence of crypt architectural abnormalities may predict disease relapse in patients with noticeable endoscopic remission, as seen on Figure 1.
Figure 1: Confocal laser endomicroscopy images from a healthy subject (a) and an ulcerative colitis (UC) patient with inactive disease (b). UC patients display increased crypt diameter, intercryptic distance, and perivascular fluorescence.
Intestinal Permeability Treatment for Inflammatory Bowel Disease
Agents routinely used in the therapeutic armamentarium of inflammatory bowel disease, or IBD, may cause and maintain mucosal remission not only for their immunomodulating effect, but also through the recovery of epithelial integrity and permeability, as was demonstrated for anti-TNF-? drugs and medications in Crohn’s disease. Since similar effects are obtained using elemental diets for Crohn’s disease, raising interest is based on dietary strategies with the use of immunomodulatory nutrients and probiotics.
Western diets, with its high content of fat and refined sugars, is a risk factor for the growth of Crohn’s disease, where they’re believed to induce a low-grade inflammation through gut dysbiosis and increased intestinal permeability. Furthermore, there is increasing concern about the use of industrial food additives towards promoting immune-related diseases. A recent research study demonstrated how additives can increase intestinal permeability by interfering with the tight junctions, or TJs, increasing the passage of immunogenic antigens. In addition, certain fatty acids, such as propionate, acetate, butyrate, omega-3, and conjugated linoleic acid, amino acids, such as glutamine, arginine, tryptophan, and citrulline, and oligoelements, which are essential for intestinal surface integrity, when supplemented to experimental subjects with gastrointestinal diseases, GI diseases, can decrease inflammation and restore gastrointestinal mucosal permeability. However, their therapeutic effectiveness, especially in inflammatory bowel disease, remains debatable: butyrate, zinc, and probiotics have the strongest evidence in this aspect.
Butyrate is a short chain fatty acid produced by intestinal microbial fermentation of dietary fibers, which in experimental versions, stimulate mucus production and expression of tight junctions, or TJs, in vitro but a broader selection of action is anticipated. It’s essential for the overall homeostasis of enterocytes that its lack, measured as faecal concentrations, has been taken as an indirect indicator of altered intestinal barrier function. In clinical practice topical butyrate had demonstrated effectiveness in refractory distal ulcerative colitis. Other fatty acids with similar properties have also been proposed as an adjuvant treatment in inflammatory bowel disease, namely, omega-3 and phosphatidylcholine, but their usage in clinical practice remains limited. Zinc is a trace element essential for cell turnover and repair systems. Inflammatory conditions and malnutrition have been known to be risk factors for zinc deficiency and many research studies demonstrated the effectiveness of its supplementation during acute diarrhoea and experimental colitis. Oral zinc treatment may restore intestinal permeability in patients with Crohn’s disease, perhaps through its capacity to regulate tight junctions, or TJs, both in the small and the large intestines.
The reason for the use of probiotics in inflammatory bowel disease is for the above mentioned dysbiosis that characterizes these GI diseases, or gastrointestinal diseases. Several trials have tested the effectiveness of various species of probiotics in inflammatory bowel disease, or IBD, with contradicting results. Those which have demonstrated to be effective are Escherichia coli Nissle 1917, Bifidobacterium, Lactobacillus rhamnosus GG, or the multispecies VSL#3, which consists of eight unique probiotics. Nevertheless, their use remains confined to ulcerative colitis and are frequently aimed at maintaining remission rather than treating the active disease, as emphasized by the meta evaluation by Jonkers et al.. The mechanisms of their effect in ulcerative colitis have yet to be fully understood but likely, together with direct anti-inflammatory effects, they can restore the intestinal barrier and decrease intestinal permeability, regulating tight junction, or TJ, proteins. The favorable effect of probiotics in pouchitis seems to be about the improvement of gastrointestinal mucosal barrier function. Another potential mechanism of action is the recovery of butyrate-producing bacteria: patients with ulcerative colitis have decreased bacterial species like Faecalibacterium prausnitzii, but supplementation with butyrate-producing species or probiotics together with preformed butyrate demonstrated effectiveness in experimental models.
Finally, vitamin D can also be involved to preserve intestinal barrier function. Polymorphisms of its own receptor have been related to the development of inflammatory bowel disease, or IBD. While the expression of vitamin D receptor on intestinal epithelium prevents inflammation-induced apoptosis, its removal contributes to faulty autophagy that boosts experimental colitis. But, additional data and clinical trials are needed to rationalize vitamin D use in inflammatory bowel disease management.
Conclusion
The impairment of intestinal barrier function is just one of the critical events in the pathogenesis of inflammatory bowel disease, or IBD. Whether it precedes and predisposes disease development remains under analysis, particularly in Crohn’s disease, but it perpetuates and enriches chronic mucosal inflammation by increasing paracellular transport of luminal pathogens. Novel imaging and functional techniques allow us to assess intestinal permeability in vivo and help identify patients at risk of relapse guiding therapeutic management. Manipulation of intestinal permeability is a fascinating therapeutic approach but more research on its effectiveness and safety are required before nutritional immune-modulators may be utilized in clinical practice. Information referenced from the National Center for Biotechnology Information (NCBI) and the National University of Health Sciences. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
Nutritional Strategies:� Hard Bones, Soft Arteries, Rather Than Vice Versa
ABSTRACT
Nutritional Strategies: The focus of this paper is to explore better strategies for optimizing bone strength and reducing risk of fracture, while at the same time decreasing risk of cardiovascular disease. The majority of Americans do not consume the current recommended dietary allowance for calcium, and the lifetime risk of osteoporosis is about 50%. However, traditional mono-nutrient calcium supplements may not be ideal. We comprehensively and systematically reviewed the scientific literature in order to determine the optimal dietary nutritional strategies and nutritional supplements for long- term skeletal health and cardiovascular health. To summarize, the following steps may be helpful for building strong bones while maintaining soft and supple arteries: (1) calcium is best obtained from dietary sources rather than supplements; (2) ensure that adequate animal protein intake is coupled with calcium intake of 1000 mg/day; (3) maintain vitamin D levels in the normal range; (4) increase intake of fruits and vegetables to alkalinize the system and promote bone health; (5) concomitantly increase potassium consumption while reducing sodium intake; (6) consider increasing the intake of foods rich in vitamins K1 and K2; (7) consider including bones in the diet; they are a rich source of calcium-hydroxyapatite and many other nutrients needed for building bone.
INTRODUCTION: Nutritional Strategies
Calcium: General Physiology Andepidemiology
Calcium is the most ubiquitous mineral in the human body. An average-sized adult body contains approximately 1000 to 1200 g of calcium, which is predominately incorporated into bones and teeth in the form of calcium-hydroxyapatite (Ca10(PO4)6(OH)2) crystals. The remainder circulates throughout the blood and soft tissues, and plays fundamental roles in cell conduction, muscle function, hormone regulation, vitamin (Vit) K-dependent pathways, and cardiac and blood vessel function.1
Some studies indicate only 30% of the US population consumes the Recommended
Dietary Allowance of calcium, which is 1000� 1200 mg daily.1 Furthermore, humans absorb only about 30% of calcium from foods depend- ing on the specific source.1 The body will demineralize its own skeletal system to maintain serum calcium levels in situations where dietary calcium is insufficient and/or absorption is decreased, and/or excretion is increased.2
Osteopenia/Osteoporosis:�An Epidemic
Starting at about age 50 years, postmenopausal women lose about 0.7�2% of their bone mass each year, while men over age 50 years lose 0.5�0.7% yearly. Between ages 45 and 75years, women, on average, lose 30% of their bone mass, whereas men lose 15%.
According to the US Surgeon General�s Report, 1 in 2 Americans over age 50 years is expected to have or to be at risk of develop- ing osteoporosis.3 Osteoporosis causes 8.9 million fractures annually, with an estimated cumulative cost of incident fractures predicted at US$474 billion over the next�20 years in the USA.3�6 Among adult women over age 45 years, osteoporosis accounts for more days spent in hospital than many other diseases such as diabetes, myocardial infarction (MI), chronic obstructive airway disease and breast cancer.3 Fragility fractures are the primary cause of hospitalization and/or death for US adults ? age 65 years and older; and 44% of nursing home admissions are due to fractures.3
A Mayo Clinic study reported that compared to 30 years ago, forearm fractures have risen more than 32% in boys and 56% in girls. The authors concluded that dietary changes, including insufficient calcium and excess phosphate, were significantly associated with increased fractures.7 Public health approaches are crucial to prevent symptomatic bone disease, but widespread pharmacological prophylaxis is prohibitively expensive and carries potential serious adverse effects.
Cardiovascular Disease & Bone Mineral Disease: A Calcium Nexus
Strong epidemiological associations exist between decreased bone mineral density (BMD) and increased risk of both cardiovascular (CV) disease and CV death.8 For example, individuals with osteoporosis have a higher risk of coronary artery disease, and vice versa. This problem will be magnified if the therapies for osteoporosis (eg, calcium supplements) independently increase risk of MI.
Issues With Dairy As Primary Source Of Calcium
Dairy foods and beverages account for about 70% of all dietary calcium intake among Americans. Dozens of epidemiological and randomized controlled trials in adults and children have used dairy products as the principal source of calcium, and have credited dairy intake with preventive benefits on study end points including bone mass, fractures and osteoporosis. A recent meta-analysis of over 270 000 people showed a strong trend for dairy intake protecting against hip fracture; the relative risk (RR) of hip fracture per daily glass of milk was 0.91, 95% CI 0.81 to 1.01.9
In many industrialized nations, milk is often the most cost-effective strategy for achieving recommended levels of calcium intake at a population level. Yet, legitimate concerns exist regarding potential deleterious effects of chronic dairy intake on health.10�16 Dairy foods, on an evolutionary time scale, are relative �new-comers� to the hominin diet.17 Domestication of cattle, sheep and goats first occurred approximately 11 000�10 000 years Before Present.17 Furthermore, it appears that an estimated 65% of the worldwide population expresses the phenotype of lactase non-persistence.18
Consumption of cow�s milk has been inconsistently associated with cataracts, ovarian and prostate cancers, and Parkinson�s disease, and it has been implicated in certain autoimmune diseases, such as type 1 diabetes and multiple sclerosis. Overall, the evidence for dairy-induced human disease appears to be most consistent for prostate cancer and for type 1 diabetes.19
A recent study of over 106 000 adults followed for 20 years showed that drinking three or more glasses of milk per day was associated with increased risks for bone fracture and higher mortality rates compared with drink- ing not more than one glass of milk per day.20 By contrast, for the women in that study, each daily serving of cheese and/or other fermented milk products such as yogurt was associated with a 10�15% decrease in the rates of mortality and hip fractures (p<0.001). However, this was an observational study with inherent limitations such as residual confounding and reverse causation, and thus, firm conclusions cannot be drawn from the data.
The sugar in milk, lactose, is broken down in the gastrointestinal tract to d-galactose and d-glucose. d-Galactose has been found to increase inflammation and oxidation in adult humans, and in adult animals this sugar triggers accelerated aging, neurodegeneration, and a shortened life span.20
Thus, cow�s milk, though rich in many nutrients, including calcium, has issues that render it less than ideal as a dietary staple for many adults. On the contrary, fermented dairy foods, such as yogurt and cheese, appear to be safer than milk, possibly because the most or all of d-galactose has been metabolized by bacteria.20
Plant-Based Dietary Sources Of Calcium & Protein: Effects On Bone Health
Most vegetarians, especially vegans, appear to absorb less calcium because of the oxalic and phytic acid contained in many plant, grain and legume products.1 Indeed, several studies have reported that risks of bone fracture are higher in vegans�likely due, at least in part, to their lower dietary calcium intake, and/or poor absorption of this key mineral (table 1).21
Dietary Protein, Calcium And Bone Health
Evolutionary evidence suggests that preagricultural diets were net base-yielding, and contributed to the robust�bone health generally seen among hunter-gatherers.10 17�By contrast, processed foods displace base-yielding fruits�and vegetables, thereby shifting to a net acid-yielding diet.2 22�24�
Increased protein intake can raise levels of insulin-like growth factor 1, which is anabolic, and contributes to bone building. Experts currently agree that diets moderate in protein (?1.0�1.5 g/kg/day) are associated with normal calcium metabolism, and do not adversely alter bone metabolism; however, at lower protein intakes (<0.8 g/kg/day), intestinal calcium absorption is reduced and levels of parathyroid hormone rise, causing the mobilization of calcium from bone.25 26
A growing body of evidence indicates that diets higher in animal protein associate with greater bone mass and fewer fractures, particularly if the calcium intake is also sufficient (approximately 1000 mg of calcium/day) (figure 1).26�28 Thus, a diet providing ample dietary calcium, along with alkalizing nutrients, such as fruits and vegetables, and possibly also alkaline mineral waters, may create a milieu where moderate intake of animal protein contributes favorably to bone health. Additionally, intake of protein plus calcium with Vitamin D may reduce fracture rates through mechanisms independent of bone density.29
Magnesium
Maintaining replete magnesium status may reduce risk for the metabolic syndrome, diabetes, hypertension and MI.30 Circumstantial and experimental evidence has also implicated magnesium deficiency in osteoporosis.31�34 Optimal dietary magnesium intake is about 7�10 mg/ kg/day, preferably in the context of a net base-yielding diet, since a net acid-yielding diet increases excretion of both magnesium and calcium (table 2).
Potassium/Sodium Ratio Affects Calcium Metabolism
A potassium/sodium ratio of 1.0 or higher is associated with a 50% lower risk of CVD and total mortality com- pared with a ratio under 1.0.35 Reducing excessive sodium intake is also associated with resultant decreased urinary calcium excretion, which may help to prevent against bone demineralization.36 The average potassium content (about 2600 mg/day) of the typical US diet is substantially lower than its sodium content (about 3300 mg/day).35 Approximately 77% of dietary sodium chloride is consumed in the form of processed foods. By contrast, potassium is naturally abundant in many unprocessed foods, especially vegetables, fruits, tubers, nuts, legumes, fish and seafood. In fact, a high potassium/sodium ratio is a reliable marker for high intake of plant foods and lower intake of processed foods.35 High dietary sodium intake has been associated with endothelial damage, arterial stiffness, decreased nitric�oxide production and increased levels of transforming growth factor ?; whereas, high potassium dietary intake can counteract these effects.35 36
Evidence indicates that the lowest CV event rates occur in the moderate sodium excretion and high potassium excretion groups.37 Thus, it appears that a moderate sodium diet (2800�3300 mg/day) in conjunction with a high potassium intake (>3000 mg/day) might confer the optimal CV benefits for the general population.37
Vitamin K & Bone Health
Emerging evidence suggests that Vitamin K may confer protective effects for both the skeletal and CV systems. Vitamin K operates in the context of other fat-soluble vitamins, such as A and D, all of which are involved in maintenance of serum calcium concentration, along with the manipulation of materials leading to bone morphogenesis and maintenance of bone tissue.38 Specifically, the oxidation of Vitamin K results in activation/carboxylation of matrix Gla protein (MGP) which is partially responsible for mineralizing bone.39
Also, Vit K is required for the activation (?-carboxylation) of osteocalcin; the inactivated form, or per cent of undercaboxylated-osteocalcin (%ucOC), has been found to be a sensitive indicator of Vitamin K nutrition status.38 In cross-sectional and prospective analyses, elevated %ucOC, which occurs when Vitamin K status is low, is a marker of increased risk for hip fracture in the elderly.38
Several large observational studies appear to support the benefits of Vitamin K on bone health.38 A meta-analysis concluded that while supplementation with phytonadione (Vitamin K1) improved bone health, Vitamin K2 was even more effective in this regard.40 This large and statistically rigorous meta-analysis concluded that high Vitamin K2 levels were associated with reduced vertebral fractures by approximately 60% (95% CI 0.25% to 0.65%), hip fractures by 77% (95% CI 0.12% to 0.47%), and all non- vertebral fractures by approximately 81% (95% CI 0.11% to 0.35%). Moreover, the benefit of Vitamin K on bone may not be due to its ability to increase BMD, but rather to its effects at increasing bone strength.41
Vitamin K Benefits In CV Health
Mounting evidence suggests vascular calcification whether in the coronary or peripheral arteries is a powerful predictor of CV morbidity and all-cause mortal- ity.42 Prevention of vascular calcification is therefore important as an early intervention to potentially improve long-term CV prognosis.
A major calcification inhibitory factor, is a Vitamin K-dependent protein synthesized by vascular smooth muscle cells.42 Increased
Vitamin K2 intake has been associated with decreased arterial calcium deposition and the ability to reverse vascular calcification in animal models. Vitamin K2 prevents pathological calcification in soft tissues via the carboxylation of protective MGP. The undercarboxylated (inactive) species of MGP is formed during inadequate Vitamin K status, or as a result of Vitamin K�antagonists.42 Low Vitamin K status is associated with increased vascular calcifications, and can be improved by effective Vitamin K supplementation (table 3).43 44 In two different randomized, double-blind controlled trials, supplemental Vitamin K has been shown to significantly delay both the development of coronary artery calcification and the deterioration of arterial elasticity.45 46
Dietary Vitamin K exists as two major forms: phylloquinone (K1) and menaquinones (MK-n). K1, the predominant dietary form of Vitamin K, is abundant in dark-green leafy vegetables and seeds. The main dietary sources for MK-n in Western populations are fermented foods, especially natto, cheese and curds (mainly MK-8 and MK-9).47
Calcium Supplementation & Bone Health
A recent large meta-analysis of 26 randomized controlled trials reported that calcium supplements lowered the risk of any fracture by a modest but statistically significant 11% (n=58 573; RR 0.89, 95% CI 0.81 to 0.96).48 Even so, the authors concluded that the evidence for calcium supplements on bone health was weak and inconsistent.
Other large meta-analyses found that calcium supplementation was most effective for preventing hip fractures when it was combined with Vitamin D.49�51 Indeed Vitamin D plays a major role in intestinal calcium absorption and bone health (figure 2).52 Additionally, calcium absorption is, in part, dependent on adequate stomach acid, and both these parameters tend to decrease with age. Drugs that markedly reduce stomach acid, such as proton pump inhibitors, have been shown to reduce calcium absorption and increase risk of osteoporosis and fractures.53
A large meta-analysis focusing on calcium intake and fracture risk found that in women (seven prospective cohort studies=170 991 women, 2954 hip fractures), there was no association between total calcium intake and hip fracture risk (pooled RR per 300 mg total=1.01; 95% CI 0.97 to 1.05).50 In men (five prospective cohort studies= 68 606 men, 214 hip fractures), the pooled RR per 300 mg of calcium daily was 0.92 (95% CI 0.82 to 1.03).
Monosupplementation with calcium, especially using the most commonly prescribed formulations (calcium carbonate and calcium citrate) might drive down the absorption of phosphate, thereby contributing to bone demineralization secondary to abnormal calcium to phosphate ratios.54 The recently updated US Preventive Services Task Force (USPSTF) has stated that there is insufficient evidence that calcium and Vitamin D prevent fractures in premenopausal women or in men who have not experienced a prior fracture. Indeed, the USPSTF now recommends against daily calcium supplementation for primary prevention of fragility fractures; stating, �the balance of benefits and harms cannot be determined�.55
Calcium Supplementation & Arterial Health
The Women�s Health Initiative, a 7-year, placebo- controlled randomized trial involving 36 282 participants, found that calcium supplementation with Vitamin D�(1000 mg/400 IU daily) had a neutral effect on coronary risk and cerebrovascular risk.56 By contrast, some subsequent publications have reported data challenging the CV safety of calcium supplementation.57�60
One meta-analysis of placebo-controlled trials involving 28 000 participants reported that a daily calcium supplement was associated with an increased risk of MI (HR 1.24, 95% CI 1.07 to 1.45, p=0.004).58 A prospective study of 388229 men and women with a 12-year follow-up showed that calcium supplementation was associated with elevated risk of heart disease death in men, but not in women.61 Yet, only one randomized controlled trial of calcium supplementation using adverse cardiac events as the primary end point has been published. In that study, daily supplementation using 1200 mg of calcium carbonate did not increase the risk of CV death or hospitalization for 1460 women (mean age 75 years).62
In a prospective cohort study with a mean follow-up of 19 years, both�high and low dietary calcium intakes were associated with increased CV disease and higher all-cause mortality (figure 3).51 Importantly, a low dietary calcium intake with or without calcium supplementation is also associated with higher CV morbidity and mortality rates.51
Other possible mechanisms that have linked calcium supplements with CV disease include coronary artery calcification, impaired vasodilation, increased arterial stiffness, and hypercoagulability.51 66
Nutritional Strategies: Food As The Ideal Source Of Calcium
The traditional focus in nutritional strategies based on supplementation of single isolated nutrients may be especially mis- guided in the case of calcium and bone health. A diet supplemented with calcium as a mononutrient pill is not ideal for promoting bone health, and may instead accelerate arterial plaque growth and vascular calcification, and increase risk of MI. Food-based solutions place evidence-based emphasis on finding the admixture of foods that balance the acid�base status of the body, and that most favorably impact the body�s calcium metabolism and bone health.
A plant-rich, grain-free diet alters the acid�base status so as to be slightly alkaline, which is conducive for bone health. However, plants are relatively poor sources of calcium compared to animal sources such as dairy pro- ducts and animal bones. We suspect that milk, though an excellent source of bioavailable calcium, has potential adverse health effects for some individuals. Additionally, 65% of the world�s population show some decrease in lactase activity during adulthood. Importantly, fermented dairy has been linked to favorable outcomes for bone health and mortality risk.
Benefits Of Consuming Bones Or Bone Meal
Ethnographic and anthropological studies indicate that adult human hunter-gatherers consumed most of their calcium in the form of bones from animals, such as small and large mammals, birds, fish and reptiles.67 68 Indeed through millions of years of evolution, we are genetically adapted to consume a large proportion of our dietary calcium from bones, where calcium is absorbed along with a matrix of nutrients including magnesium, phosphorus, strontium, zinc, iron, copper, collagen protein, aminoglycans and osteocalcin�all of which also support robust bone formation.68 69 Theoretically, including animal bones (sardines, salmon, soft chicken bones, bone broths, etc) may be an effective dietary strategy to ensure adequate calcium intake and to optimize long-term bone health.
Mineral supplements made from bone meal, when taken with food, theoretically might provide a more practical means to ensure
adequate calcium intake without predisposing to CVD risk. Ingestion of micro- crystalline hydroxyapatite (the form of calcium found in bone) produces less of an acute spike in blood calcium levels compared to soluble calcium salts typically used in standard supplements, and thus may be less likely to increase vascular calcification and coronary risk.65 Hydroxyapatite also stimulates bone osteoblast cells and contains virtually all the essential building blocks needed to construct bone tissue. In a small placebo- controlled randomized trial, women who took 1000 mg of calcium in the form of hydroxyapatite in conjunction with oral Vitamin D showed a significant increase in bone thickness, whereas those who took 1000 mg of a standard calcium carbonate supplement did not (figure 4).70 Another double-blind placebo-controlled study found�that supplementing with hydroxyapatite and Vitamin D3 significantly improved serological markers of bone health.15
In theory, the addition of Vitamin K2 and magnesium to an organic bone meal supplement might further enhance its effectiveness and reduce the risk of soft tissue calcification. However, the quantity and quality of the experimental data testing the effects of Vitamin D and calcium on bone health dwarfs the data for bone meal supplementation. Much larger randomized trials will be needed to firmly establish the safety and effectiveness of bone meal as well as Vitamin K and magnesium as supplements for building bone without increasing vascular calcification.
Conclusion: Nutritional Strategies
It is becoming increasingly clear that the fundamental unit for nutrition is the food (eg, milk, nuts, eggs), not the nutrient (eg, calcium, saturated fat, cholesterol). A nutrient perceived as beneficial, such as calcium, may be unhealthy if the parent food, say milk, contains other nutrients, such as galactose, that on the balance might stimulate adverse effects in the body. In theory, consuming calcium-rich foods such as bones, fermented dairy (eg, unsweetened yogurt, kefir, cheese), leafy greens, almonds, and chia seeds may be an effective strategy for improving both calcium intake and long-term health.
James H O�Keefe,1 Nathaniel Bergman,2 Pedro Carrera-Bastos,3 Mae?lan Fontes-Villalba,3 James J DiNicolantonio,1 Loren Cordain4
Twitter Follow Maela?n Fontes-Villalba at @maelanfontes
Contributors NB, PC-B and MF-V assisted with the gathering and review of the data; JD, LC and JHO reviewed the data; NB, PC-B, MF-V, JD, LC and JHO assisted in the concept and design of the manuscript. JHO, NB and PC-B wrote, rewrote and finalised the manuscript.
Funding This manuscript received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. This paper was not commissioned.
Competing interests JHO is Chief Medical Officer and has an ownership interest in CardioTabs, a nutraceutical company that markets products containing vitamins and minerals.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.
Open Access This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non- commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http:// creativecommons.org/licenses/by-nc/4.0/
References:
1. Ross AC, Taylor CL, Yaktine AL, del Valle HB, eds. Dietary
Reference Intakes for Calcium and Vitamin D. Washington DC: The
National Academies Press, 2011:349. http://www.ncbi.nlm.nih.gov/
books/NBK56070/
2. Frassetto L, Morris RC Jr, Sellmeyer DE, et al. Diet, evolution and
aging�the pathophysiologic effects of the post-agricultural inversion
of the potassium-to-sodium and base-to-chloride ratios in the human
diet. Eur J Nutr 2001;40:200�13.
3. Surgeons AAoO. The burden of musculoskeletal diseases in the
United States: prevalence, societal and economic cost. Rosemont,
IL: Amer Academy of Orthopaedic, 2008.
4. Johnell O, Kanis JA. An estimate of the worldwide prevalence and
disability associated with osteoporotic fractures. Osteoporos Int
2006;17:1726�33.
5. Facts and Statistics. http://www.iofbonehealth.org/facts-statistics.
Secondary Facts and Statistics. http://www.iofbonehealth.org/
facts-statistics. 2013. http://www.iofbonehealth.org/facts-statistics
6. Burge R, Dawson-Hughes B, Solomon DH, et al. Incidence and
economic burden of osteoporosis-related fractures in the United
States, 2005�2025. J Bone Miner Res 2007;22:465�75.
7. Khosla S, Melton LJ III, Dekutoski MB, et al. Incidence of childhood
distal forearm fractures over 30 years: a population-based study.
JAMA 2003;290:1479�85.
8. Choi SH, An JH, Lim S, et al. Lower bone mineral density is
associated with higher coronary calcification and coronary plaque
burdens by multidetector row coronary computed tomography
in pre- and postmenopausal women. Clin Endocrinol
2009;71:644�51.
9. Bischoff-Ferrari HA, Dawson-Hughes B, Baron JA, et al. Milk intake
and risk of hip fracture in men and women: a meta-analysis of
prospective cohort studies. J Bone Miner Res 2011;26:833�9.
10. Carrera-Bastos P, Fontes-Villaba M, O�Keefe JH, et al. The western
diet and lifestyle and diseases of civilization. Res Rep Clin Cardio
2011;2011:15�35.
11. Winer S, Astsaturov I, Cheung RK, et al. T cells of multiple sclerosis
patients target a common environmental peptide that causes
encephalitis in mice. J Immunol 2001;166:4751�6.
12. Artaud-Wild SM, Connor SL, Sexton G, et al. Differences in coronary
mortality can be explained by differences in cholesterol and
saturated fat intakes in 40 countries but not in France and Finland.
A paradox. Circulation 1993;88:2771�9.
13. Segall JJ. Plausibility of dietary lactose as a coronary risk factor.
J Nutr Enviro Med 2002;12:217�29.
14. Cordain L, Toohey L, Smith MJ, et al. Modulation of immune
function by dietary lectins in rheumatoid arthritis. Br J Nutr
2000;83:207�17.
15. Disilvestro RA, Crawford B, Zhang W, et al. Effects of micronutrient
supplementation plus resistance exercise training on bone
metabolism markers in young adult woman. J Nutr Enviro Med
2007;16:16�25.
16. Sandler RB, Slemenda CW, LaPorte RE, et al. Postmenopausal
bone density and milk consumption in childhood and adolescence.
Am J Clin Nutr 1985;42:270�4.
17. Cordain L, Eaton SB, Sebastian A, et al. Origins and evolution of the
Western diet: health implications for the 21st century. Am J Clin Nutr
2005;81:341�54.
18. Ingram CJ, Mulcare CA, Itan Y, et al. Lactose digestion and the
evolutionary genetics of lactase persistence. Hum Genet
2009;124:579�91.
19. Melnik BC, John SM, Carrera-Bastos P, et al. The impact of cow�s
milk-mediated mTORC1-signaling in the initiation and progression of
prostate cancer. Nutr Metab 2012;9:74.
20. Michaelsson K, Wolk A, Langenskiold S, et al. Milk intake and risk of
mortality and fractures in women and men: cohort studies. BMJ
2014;349:g6015.
21. Appleby P, Roddam A, Allen N, et al. Comparative fracture risk in
vegetarians and nonvegetarians in EPIC-Oxford. Eur J Clin Nutr
2007;61:1400�6.
22. Sebastian A, Harris ST, Ottaway JH, et al. Improved mineral balance
and skeletal metabolism in postmenopausal women treated with
potassium bicarbonate. N Engl J Med 1994;330:1776�81.
23. Bushinsky DA. Metabolic alkalosis decreases bone calcium efflux by
suppressing osteoclasts and stimulating osteoblasts. Am J Physiol
1996;271(1 Pt 2):F216�22.
24. Sebastian A, Frassetto LA, Sellmeyer DE, et al. Estimation of
the net acid load of the diet of ancestral preagricultural Homo
sapiens and their hominid ancestors. Am J Clin Nutr
2002;76:1308�16.
25. Kerstetter JE, O�Brien KO, Insogna KL. Dietary protein, calcium
metabolism, and skeletal homeostasis revisited. Am J Clin Nutr
2003;78(3 Suppl):584S�92S.
26. Heaney RP, Layman DK. Amount and type of protein influences
bone health. Am J Clin Nutr 2008;87:1567S�70S.
27. Hannan MT, Tucker KL, Dawson-Hughes B, et al. Effect of dietary
protein on bone loss in elderly men and women: the Framingham
Osteoporosis Study. J Bone Miner Res 2000;15:2504�12.
28. Sahni S, Cupples LA, McLean RR, et al. Protective effect of high
protein and calcium intake on the risk of hip fracture in the
Framingham offspring cohort. J Bone Miner Res 2010;25:
2770�6.
29. Rabenda V, Bruyere O, Reginster JY. Relationship between bone
mineral density changes and risk of fractures among patients
receiving calcium with or without vitamin D supplementation:
a meta-regression. Osteoporos Int 2011;22:893�901.
30. He K, Liu K, Daviglus ML, et al. Magnesium intake and incidence of
metabolic syndrome among young adults. Circulation
2006;113:1675�82.
31. Lakshmanan FL, Rao RB, Kim WW, et al. Magnesium intakes,
balances, and blood levels of adults consuming self-selected diets.
Am J Clin Nutr 1984;40(6 Suppl):1380�9.
32. Greger JL, Baligar P, Abernathy RP, et al. Calcium, magnesium,
phosphorus, copper, and manganese balance in adolescent
females. Am J Clin Nutr 1978;31:117�21.
33. Gullestad L, Nes M, Ronneberg R, et al. Magnesium status in
healthy free-living elderly Norwegians. J Am Coll Nutr
1994;13:45�50.
34. Sojka JE, Weaver CM. Magnesium supplementation and
osteoporosis. Nutr Rev 1995;53:71�4.
35. Yang Q, Liu T, Kuklina EV, et al. Sodium and potassium intake and
mortality among US adults: prospective data from the Third National
Health and Nutrition Examination Survey. Arch Intern Med
2011;171:1183�91.
36. Lin PH, Ginty F, Appel LJ, et al. The DASH diet and sodium
reduction improve markers of bone turnover and calcium metabolism
in adults. J Nutr 2003;133:3130�6.
37. O�Donnell MJ, Yusuf S, Mente A, et al. Urinary sodium and
potassium excretion and risk of cardiovascular events. JAMA
2011;306:2229�38.
38. Booth SL. Roles for vitamin K beyond coagulation. Annu Rev Nutr
2009;29:89�110.
39. Kanellakis S, Moschonis G, Tenta R, et al. Changes in parameters
of bone metabolism in postmenopausal women following a
12-month intervention period using dairy products enriched with
calcium, vitamin D, and phylloquinone (vitamin K(1)) or
menaquinone-7 (vitamin K (2)): the Postmenopausal Health Study II.
Calcif Tissue Int 2012;90:251�62.
40. Cockayne S, Adamson J, Lanham-New S, et al. Vitamin K and the
prevention of fractures: systematic review and meta-analysis of
randomized controlled trials. Arch Intern Med 2006;166:1256�61.
41. Knapen MH, Schurgers LJ, Vermeer C. Vitamin K2 supplementation
improves hip bone geometry and bone strength indices in
postmenopausal women. Osteoporos Int 2007;18:963�72.
42. Beulens JW, Bots ML, Atsma F, et al. High dietary menaquinone
intake is associated with reduced coronary calcification.
Atherosclerosis 2009;203:489�93.
43. Rennenberg RJ, de Leeuw PW, Kessels AG, et al. Calcium scores
and matrix Gla protein levels: association with vitamin K status. Eur
J Clin Invest 2010;40:344�9.
44. Schurgers LJ, Barreto DV, Barreto FC, et al. The circulating inactive
form of matrix gla protein is a surrogate marker for vascular
calcification in chronic kidney disease: a preliminary report. Clin J
Am Soc Nephrol 2010;5:568�75.45. Shea MK, O�Donnell CJ, Hoffmann U, et al. Vitamin K
supplementation and progression of coronary artery calcium in older
men and women. Am J Clin Nutr 2009;89:1799�807.
46. Braam LA, Hoeks AP, Brouns F, et al. Beneficial effects of vitamins
D and K on the elastic properties of the vessel wall in
postmenopausal women: a follow-up study. Thromb Haemost
2004;91:373�80.
47. McCann JC, Ames BN. Vitamin K, an example of triage theory: is
micronutrient inadequacy linked to diseases of aging? Am J Clin
Nutr 2009;90:889�907.
48. Bolland MJ, Leung W, Tai V, et al. Calcium intake and risk of
fracture: systematic review. BMJ 2015;351:h4580.
49. Tang BM, Eslick GD, Nowson C, et al. Use of calcium or calcium in
combination with vitamin D supplementation to prevent fractures and
bone loss in people aged 50 years and older: a meta-analysis.
Lancet 2007;370:657�66.
50. Bischoff-Ferrari HA, Dawson-Hughes B, Baron JA, et al. Calcium
intake and hip fracture risk in men and women: a meta-analysis of
prospective cohort studies and randomized controlled trials. Am J
Clin Nutr 2007;86:1780�90.
51. Michaelsson K, Melhus H, Warensjo Lemming E, et al. Long term
calcium intake and rates of all cause and cardiovascular mortality:
community based prospective longitudinal cohort study. BMJ
2013;346:f228.
52. Christakos S. Recent advances in our understanding of
1,25-dihydroxyvitamin D(3) regulation of intestinal calcium
absorption. Arch Biochem Biophys 2012;523:73�6.
53. Khalili H, Huang ES, Jacobson BC, et al. Use of proton pump
inhibitors and risk of hip fracture in relation to dietary and lifestyle
factors: a prospective cohort study. BMJ 2012;344:e372.
54. Heaney RP, Nordin BE. Calcium effects on phosphorus absorption:
implications for the prevention and co-therapy of osteoporosis. J Am
Coll Nutr 2002;21:239�44.
55. Moyer VA. Vitamin D and calcium supplementation to prevent
fractures in adults: U.S. Preventive Services Task Force
recommendation statement. Ann Intern Med 2013;158:691�6.
56. Hsia J, Heiss G, Ren H, et al. Calcium/vitamin D supplementation
and cardiovascular events. Circulation 2007;115:846�54.
57. Bolland MJ, Barber PA, Doughty RN, et al. Vascular events in
healthy older women receiving calcium supplementation:
randomised controlled trial. BMJ 2008;336:262�6.
58. Bolland MJ, Wang TK, van Pelt NC, et al. Abdominal aortic
calcification on vertebral morphometry images predicts incident
myocardial infarction. J Bone Miner Res 2010;25:505�12.
59. Reid IR, Bolland MJ, Grey A. Does calcium supplementation
increase cardiovascular risk? Clin Endocrinol 2010;73:689�95.
60. Pentti K, Tuppurainen MT, Honkanen R, et al. Use of calcium
supplements and the risk of coronary heart disease in 52�
62-year-old women: The Kuopio Osteoporosis Risk Factor and
Prevention Study. Maturitas 2009;63:73�8.
61. Xiao Q, Murphy RA, Houston DK, et al. Dietary and supplemental
calcium intake and cardiovascular disease mortality: The National
Institutes of Health-AARP diet and health study. JAMA Intern Med
2013;173:639�46.
62. Lewis JR, Calver J, Zhu K, et al. Calcium supplementation and the
risks of atherosclerotic vascular disease in older women: results of a
5-year RCT and a 4.5-year follow-up. J Bone Miner Res
2011;26:35�41.
63. Reid IR, Bolland MJ, Avenell A, et al. Cardiovascular effects of
calcium supplementation. Osteoporos Int 2011;22:1649�58.
64. Karp HJ, Ketola ME, Lamberg-Allardt CJ. Acute effects of calcium
carbonate, calcium citrate and potassium citrate on markers of
calcium and bone metabolism in young women. Br J Nutr
2009;102:1341�7.
65. Tucker LA, Nokes N, Adams T. Effect of a dietary supplement on hip
and spine BMD: a randomized, double-blind, placebo-controlled trial:
1515: board #5 May 30 2:00 PM�3:30 PM. Med Sci Sports Exer
2007;39:S230.
66. West SL, Swan VJ, Jamal SA. Effects of calcium on cardiovascular
events in patients with kidney disease and in a healthy population.
Clin J Am Soc Nephrol 2010;5(Suppl 1):S41�7.
67. Reinhard KJ, Ambler JR, Szuter CR. Hunter-gatherer use of small
animal food resources: coprolite evidence. J Osteoarch
2007;17:416�28.
68. Vieugue J, Salanova L, Regert M, et al. The consumption of bone
powder in the early neolithic societies of Southeastern Europe:
evidence of a diet stress? Cambridge Archaeological J
2015;02:495�511.
69. Schulman RC, Weiss AJ, Mechanick JI. Nutrition, bone, and aging:
an integrative physiology approach. Curr Osteoporos Rep
2011;9:184�95.
70. Epstein O, Kato Y, Dick R, et al. Vitamin D, hydroxyapatite, and
calcium gluconate in treatment of cortical bone thinning in
postmenopausal women with primary biliary cirrhosis. Am J Clin
Nutr 1982;36:426�30.
71. Bischoff-Ferrari HA, Kiel DP, Dawson-Hughes B, et al. Dietary
calcium and serum 25-hydroxyvitamin D status in relation to
BMD among U.S. adults. J Bone Miner Res 2009;24:935�42.
The pathogenesis of inflammatory bowel disease, or IBD, suggests that interrupted interactions between the gastrointestinal tract, or GI tract, and the gut microbiota can often be the cause behind the development of the disease. A damaged or unhealthy gastric mucosal barrier may result in increased intestinal permeability which can cause an immunological reaction and result in symptoms of inflammation. Individuals diagnosed with inflammatory bowel disease present several defects in the many specialized components of mucosal barrier function, from the mucous coating makeup to the adhesion molecules that regulate paracellular permeability. These alterations may represent a primary dysfunction in Crohn’s disease, but they may also cause chronic mucosal inflammation in ulcerative colitis.
How does inflammatory bowel disease affect intestinal permeability?
In clinical practice as well as experimental testings, many research studies have reported that changes in intestinal permeability can predict the development of inflammatory bowel disease, or IBD. Functional evaluations, such as the sugar absorption test or the novel imaging technique using confocal laser endomicroscopy, allow an in vivo assessment of intestinal barrier integrity. Antitumor necrosis factor-? (TNF-?) therapy reduces mucosal inflammation and soothes intestinal permeability from IBD patients. Butyrate, zinc, and some probiotics also ameliorate mucosal barrier dysfunction but their use is still limited and further research is required before suggesting permeability manipulation as a therapeutic goal in inflammatory bowel disease.
The gut plays a major role in food digestion and absorption of nutrients as well as in maintaining the overall homeostasis. It is estimated that the entire bacterial count in our entire body exceeds ten times the entire amount of individual cells in it, with more than one million species found in the gastrointestinal tract. The gut microbiota, whose genome includes 100 times more genes in relation to the entire human genome, also plays an important role in nutrition, energy metabolism, host defense, and immune system development. However, modified microbiota has been connected to, not just gastrointestinal disorders, but also to the pathogenesis of systemic conditions, such as obesity and metabolic syndrome. Therefore, the expression “mucosal barrier” seems to properly highlight the critical role of the gut and its interaction with microbiota: it is not a static shield but an active apparatus with specialized components. According to Bischoff et al. “permeability” is described as a functional feature of this barrier which allows the coexistence of bacteria required by our organism and prevents luminal penetration of macromolecules and pathogens. Altered intestinal permeability was documented during several diseases, including, acute pancreatitis, multiple organ failure, major surgery, and severe trauma, and may also explain the high incidence of Gram-negative sepsis and related mortality in critically ill patients. Furthermore, perturbation of the complex mechanism of permeability has been connected to the development of irritable bowel syndrome and steatohepatitis, or NASH.
The pathogenesis of inflammatory bowel disease, or IBD, remains unclear but it most likely is multifactorial and driven by an exaggerated immune response towards the gastrointestinal microbiome in a genetically susceptible host. Increasing evidence suggests that intestinal permeability may be critical and some authors even considered inflammatory bowel disease, or IBD, as a disease, primarily caused by intestinal barrier dysfunction.
Intestinal Barrier Dysfunction in Inflammatory Bowel Disease
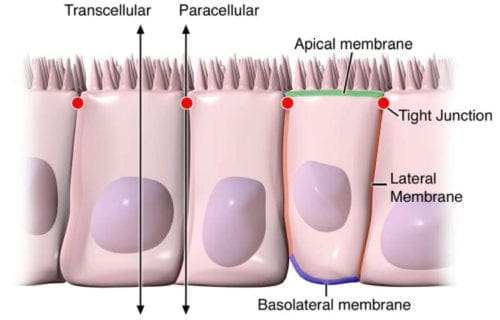
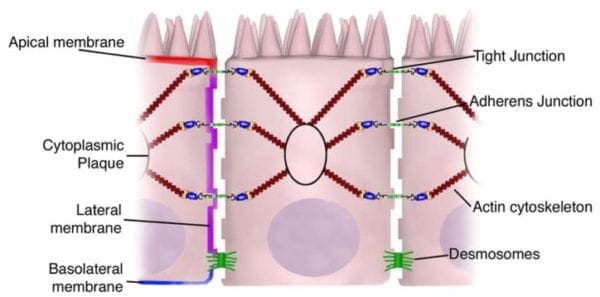
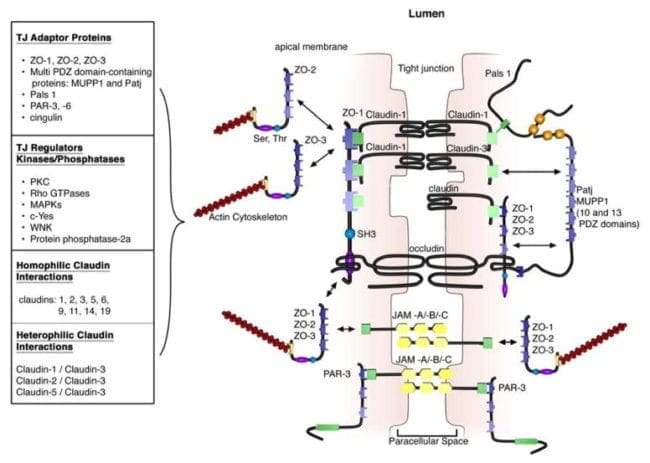
The main component of the mucosal barrier is represented by the intestinal epithelium, which is made up of one layer of various subtypes of cells, including the enterocytes, goblet cells, Paneth cells, and enteroendocrine cells, as well as immune cells, such as intraepithelial lymphocytes and dendritic cells, as seen on Figure 1. The regulation of paracellular permeability of ions and tiny molecules is provided by three kinds of junctional complexes: the tight junctions, or TJs, adherence junctions, and desmosomes.
Figure 1
Individuals with IBD present enhanced paracellular permeability with TJ abnormalities, according to several research studies. These are complex multiprotein structures with an extracellular portion, a transmembrane domain and an intracellular association with the cytoskeleton, referenced from Figure 1. A decreased expression and redistribution of the components, such as occludins, claudins, and junctional adhesion molecules, abbreviated as JAM, have all been demonstrated in IBD, where a current experiment found that eliminating claudin-7 can cause colonic inflammation. In addition, tumour necrosis factor-? (TNF-?), one of the main factors behind IBD inflammation, may regulate the transcription of TJ proteins whereas its antagonists, anti-TNF-?, can ameliorate intestinal permeability. However, TNF-? may contribute to altered intestinal permeability as well, inducing apoptosis of enterocytes, increasing their rate of shedding and preventing the redistribution of TJs which should seal the remaining gaps.
Goblet cells are specialized in the secretion of mucus that covers the surface of the intestinal epithelium. Mucus is made up of carbohydrates, proteins, lipids, and a high amount of water while it also has antimicrobial properties because of antimicrobial peptides, mainly defensins produced by Paneth cells, and secretory IgA. Individuals with ulcerative colitis demonstrate a lesser variety of goblet cells, a reduced thickness of the mucus layer, and an altered mucus composition regarding mucins, phosphatidylcholine, and glycosylation. Moreover, modified Paneth cell distribution and function has been reported in IBD: these cells are typically limited to the small intestines, within the crypts of Lieberk�hn, but in IBD, metaplastic Paneth cells may be found in colonic mucosa, together with subsequent secretion of defensins also from the large intestine. The role of Paneth cells may differ in the two disease phenotypes because the expression of defensins is caused by colonic inflammation in UC but is reduced in patients with colonic Crohn’s disease, or CD. The decreased Paneth cell antimicrobial function might be a main pathogenic component in Crohn’s disease, or CD, particularly ileal CD, although the greater secretion of defensins in UC could be a physiological response to mucosal damage.
Etiology of Intestinal Permeability in Inflammatory Bowel Disease
Whether mucosal barrier dysfunction is a result of the inflammatory response or a primary defect that prompts mucosal inflammation, still remains under debate. However, several research studies suggest that altered intestinal permeability may be an early event in Crohn’s disease pathogenesis. Increased paracellular permeability was found in patients with quiescent IBD and was connected to intestinal symptoms even when endoscopic activity was absent. Furthermore, an ex vivo study with Ussing chambers on colonic biopsies from CD patients revealed a spatially uniform increase in transepithelial conductivity regardless of the presence of minimal mucosal erosions. This finding was attributed to the downregulation of TJ proteins. Lastly, animal models of CD, particularly, IL-10 knockout mice and SAMP1/YitFc mice, also declared that increased permeability can be determined before the onset of mucosal inflammation.
Genes involved in intestinal barrier homeostasis have also been associated with IBD susceptibility, demonstrating a genetic predisposition that’s further supported by the observation that up to 40 percent of first-degree relatives of CD patients have altered small intestinal permeability, with a significant connection to familial CD and NOD2/CARD15 variations. This gene, which is involved in bacterial recognition, regulates both innate and adaptive immune responses and is the main susceptibility locus for the development of Crohn’s disease. Other research studies have not found a correlation between permeability and hereditary polymorphisms but it’s noteworthy they’ve mostly involved sporadic CD instances. However, environmental factors are also principal contributors in determining mucosal permeability because permeability is raised even in a percentage of CD spouses. Additionally, a recent research highlighted the value of age and smoking status rather than genotype in family. There is only one reported instance of CD development predicted by an abnormal permeability test in a healthy relative.
Independently from being genetically determined or caused by environmental factors, intestinal permeability leads to the disruption of the physiological equilibrium between mucosal barrier and luminal challenge which cannot be properly counteracted by inherent resistance of IBD patients, which on the opposite reacts with an underactive immune trigger. As a matter of fact, many defects in bacterial recognition and processing have been documented in CD patients taking certain genetic polymorphisms, mainly of pattern-recognition receptors, such as NOD2/CARD15 and genes involved in autophagy, like ATG16L1 and IRGM. In intestinal mucosa, the absence of feedback between mutated NOD2/CARD15 expression and gut luminal microbiota may result in the breakdown of tolerance. Interestingly, a recent research study by Nighot et al. revealed that autophagy is also involved with the regulation of the TJs by degradation of a pore-forming claudin, connecting autophagy with permeability.
Finally, intestinal microbiota may become altered in IBD, especially in its relative diversity and composition. This could represent a consequence of chronic mucosal inflammation however, the influence of host genotype in shaping microbial community cannot be missed in CD and NOD2/CARD15 genotype has been shown to influence the composition of gut microbiota in humans. This dysbiosis can further exacerbate permeability dysfunction from the reduction of the symbiotic connection between the microbiota and the mucosal barrier integrity. Information referenced from the National Center for Biotechnology Information (NCBI) and the National University of Health Sciences. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Clinical Application of Neuromuscular Techniques: Assessment and Treatment of Hip Flexors � Rectus Femoris, Iliopsoas
Patient lies supine with buttocks (coccyx) as close to end of table as possible, non-tested leg in flexion at hip and knee, held by patient or by having sole of foot of non-tested side placed against the lateral chest wall of the practitioner. Full flexion of the hip helps to maintain the pelvis in full rotation with the lumbar spine flat, which is essential if the test is to be meaningful and stress on the spine is to be avoided.
Notes on Psoas
Lewit (1985b) mentions that in many ways the psoas behaves as if it were an internal organ. Tension in the psoas may be secondary to kidney disease, and one of its frequent clinical manifestations, when in spasm, is that it reproduces the pain of gall-bladder disease (often after the organ has been removed).
The definitive signs of psoas problems are not difficult to note, according to Harrison Fryette (1954). He maintains that the distortions produced in inflammation and/or spasm in the psoas are characteristic and cannot be produced by other dysfunction. The origin of the psoas is from 12th thoracic to (and including) the 4th lumbar, but not the 5th lumbar. The insertion is into the lesser trochanter of the femur, and thus, when psoas spasm exists unilaterally, the patient is drawn forwards and sidebent to the involved side. The ilium on the side will rotate backwards on the sacrum, and the thigh will be everted. When both muscles are involved the patient is drawn forward, with the lumbar curve locked in flexion. This is the characteristic reversed lumbar spine. Chronic bilateral psoas contraction creates either a reversed lumbar curve if the erector spinae of the low back are weak, or an increased lordosis if they are hypertonic.
Lewit says, �Psoas spasm causes abdominal pain, flexion of the hip and typical antalgesic (stooped) posture. Problems in psoas can profoundly influence thoraco-lumbar stability.�
The 5th lumbar is not involved directly with psoas, but great mechanical stress is placed upon it when the other lumbar vertebrae are fixed in either a kyphotic or an increased lordotic state. In unilateral psoas spasms, a rotary stress is noted at the level of 5th lumbar. The main mechanical involvement is, however, usually at the lumbodorsal junction. Attempts to treat the resulting pain (frequently located in the region of the 5th lumbar and sacroiliac) by attention to these areas will be of little use. Attention to the muscular component should be a primary focus, ideally using MET.
Bogduk (Bogduk et al 1992, Bogduk 1997) provides evidence that psoas plays only a small role in the action of the spine, and states that it �uses the lumbar spine as a base from which to act on the hip�. He goes on to discuss just how much pressure derives from psoas compression on discs: �Psoas potentially exerts massive compression loads on the lower lumbar discs � upon maximum contraction, in an activity such as sit-ups, the two psoas muscles can be expected to exert a compression on the L5�S1 disc equal to about 100 kg of weight.�
There exists in all muscles a vital reciprocal agonist�antagonist relationship which is of primary importance in determining their tone and healthy function. Psoas�rectus abdominis have such a relationship and this has important postural implications (see notes on lower crossed syndrome in Ch. 2).
Observation of the abdomen �falling back� rather than mounding when the patient flexes indicates normal psoas function. Similarly, if the patient, when lying supine, flexes knees and �drags� the heels towards the buttocks (keeping them together), the abdomen should remain flat or fall back. If the abdomen mounds or the small of the back arches, psoas is incompetent.
If the supine patient raises both legs into the air and the belly mounds it shows that the recti and psoas are out of balance. Psoas should be able to raise the legs to at least 30� without any help from the abdominal muscles.
Psoas fibres merge with (become �consolidated� with) the diaphragm and it therefore influences respiratory function directly (as does quadratus lumborum).
Basmajian (1974) informs us that the psoas is the most important of all postural muscles. If it is hypertonic and the abdominals are weak and exercise is prescribed to tone these weak abdominals (such as curl-ups with the dorsum of the foot stabilised), then a disastrous negative effect will ensue in which, far from toning the abdominals, increase of tone in psoas will result, due to the sequence created by the dorsum of the foot being used as a point of support. When this occurs (dorsiflexion), the gait cycle is mimicked and there is a sequence of activation of tibialis anticus, rectus femoris and psoas. If, on the other hand, the feet could be plantarflexed during curl-up exercises, then the opposite chain is activated (triceps surae, hamstrings and gluteals) inhibiting psoas and allowing toning of the abdominals.
When treating, it is sometimes useful to assess changes in psoas length by periodic comparison of apparent arm length. Patient lies supine, arms extended above head, palms together so that length can be compared. A shortness will commonly be observed in the arm on the side of the shortened psoas, and this should normalise after successful treatment (there may of course be other reasons for apparent difference in arm length, and this method provides an indication only of changes in psoas length).
If the thigh of the tested leg fails to lie in a horizontal position in which it is parallel to the floor/table, then the indication is that iliopsoas is short. If the lower leg of the tested side fails to achieve an almost 90� angle with the thigh, vertical to the floor, then shortness of the rectus femoris muscle is indicated (Fig. 4.6B). If this is not clearly noted, application of light pressure towards the floor on the lower third of the thigh will produce a compensatory extension of the lower leg only when rectus femoris is short. A slight degree (10�15�) of hip extension should be possible in this position, by pushing downwards on the thigh, without knee extension occurring. This can subsequently be checked by seeing whether or not the heel on that side can easily flex to touch the buttock of the prone patient (if rectus is short heel will not easily reach the buttock). If effort is required to achieve 10� of hip extension, this confirms iliopsoas shortening on that side. If both psoas and rectus are short, rectus should be treated first. If the thigh hangs down below a parallel position, this indicates a degree of laxity in iliopsoas (Fig. 4.6C). A further cause of failure of the thigh to rest parallel to the floor can be due to shortness of tensor fascia lata. If this structure is short (a further test proves it, see later in this chapter) then there should be an obvious groove apparent on the lateral thigh and the patella, and sometimes the whole lower leg will deviate laterally. A further indication of short psoas is seen if the prone patient�s hip is observed to remain in flexion. In this position passive flexion of the knee will result in compensatory lumbar lordosis and increased hip flexion if rectus femoris is also short. (See also functional assessment method for psoas in Ch. 5 and notes on psoas in Box 4.4.)
Figure 4.6A Test position for shortness of hip flexors. Note that the hip on the non-tested side must be fully flexed to produce full pelvic rotation. The position shown is normal.
Figure 4.6B In the test position, if the thigh is elevated (i.e. not parallel with the table) probable psoas shortness is indicated. The inability of the lower leg to hang more or less vertically towards the floor indicates probable rectus femoris shortness (TFL shortness can produce a similar effect).
Figure 4.6C The fall of the thigh below the horizontal indicates hypotonic psoas status. Rectus femoris is once again seen to be short, while the relative external rotation of the lower leg (see angle of foot) hints at probable shortened TFL involvement.
Mitchell�s Strength Test
Before using MET methods to normalise a short psoas, Mitchell recommends that you have the patient at the end of the table, both legs hanging down and feet turned in so that they can rest on your lateral calf areas as you stand facing the patient. The patient should press firmly against your calves with her feet as you rest your hands on her thighs and she attempts to lift you from the floor. In this way you assess the relative strength of one leg�s effort, as against the other. Judge which psoas is weaker or stronger than the other. If a psoas has tested short (as in the test described earlier in this chapter) and also tests strong in this test, then it is suitable for MET treatment, according to Mitchell. If it tests short and weak, then other factors such as tight erector spinae muscles should be treated first until psoas tests strong and short, at which time MET should be applied to start the lengthening process. It is worth recalling Norris�s (1999) advice that a slowly performed isotonic eccentric exercise will normally strengthen a weak postural muscle. (Psoas is classified as postural, and a mobiliser, depending on the model being used. Richardson et al (1999) describe psoas as �an exception� to their deep/superficial rule since, �it is designed to act exclusively on the hip�. There is therefore universal agreement that psoas will shorten in response to stress.) NOTE: It has been found to be clinically useful to suggest that before treating a shortened psoas, any shortness in rectus femoris on that side should first be treated.
MET Treatment for Shortness of Rectus Femoris
Patient lies prone, ideally with a cushion under the abdomen to help avoid hyperlordosis. The practitioner stands on the side of the table of the affected leg so that he can stabilise the patient�s pelvis (hand covering sacral area) during the treatment, using the cephalad hand. The affected leg is flexed at hip and knee. The practitioner can either hold the lower leg at the ankle (as in Fig. 4.7), or the upper leg can be cradled so that the hand curls under the lower thigh and is able to palpate for bind, just above the knee, with the practitioner�s upper arm offering resistance to the lower leg. Either of these holds allows flexion of the knee to the barrier, perceived either as increasing effort, or as palpated bind. If rectus femoris is short, then the patient�s heel will not easily be able to touch the buttock (Fig. 4.7).
Figure 4.7 MET treatment of left rectus femoris muscle. Note the practitioner�s right hand stabilises the sacrum and pelvis to prevent undue stress during the stretching phase of the treatment. Once the restriction barrier has been established (how close can the heel get to the buttock before the barrier is noted?) the decision will have been made as to whether to treat this as an acute problem (from the barrier), or as a chronic problem (short of the barrier). Appropriate degrees of resisted isometric effort are then introduced. For an acute problem a mild 15% of MVC (maximum voluntary contraction), or a longer, stronger (up to 25% of MVC) effort for a chronic problem, is used as the patient tries to both straighten the leg and take the thigh towards the table (this activates both ends of rectus). Appropriate breathing instructions should be given (see notes on breathing earlier in this chapter, Box 4.2).
The contraction is followed, on an exhalation, by taking of the muscle to, or stretching through, the new barrier, by taking the heel towards the buttock with the patient�s help. Remember to increase slight hip extension before the next contraction (using a cushion to support the thigh) as this removes slack from the cephalad end of rectus femoris. Repeat once or twice using agonists or antagonists. Once a reasonable degree of increased range has been gained in rectus femoris it is appropriate to treat psoas, if this has tested as short.
MET Treatment of Psoas
Method (a) (Fig. 4.8) Psoas can be treated in the prone position described for rectus above, in which case the stretch following the patient�s isometric effort to bring the thigh to the table against resistance would be concentrated on extension of the thigh, either to the new barrier of resistance if acute or past the barrier, placing stretch on psoas, if chronic.
Figure 4.8 MET treatment of psoas with stabilising contact on ischial tuberosity as described by Greenman (1996). The patient is prone with a pillow under the abdomen to reduce the lumbar curve. The practitioner stands on the side opposite the side of psoas to be treated, with the table-side hand supporting the thigh. The non-table-side hand is placed so that the heel of that hand is on the sacrum, applying pressure towards the floor, to maintain pelvic stability (see also Fig. 4.11A). The fingers of that hand are placed so that the middle, ring and small fingers are on one side of L2/3 segment and the index finger on the other. This allows these fingers to sense a forwards (anteriorly directed) �tug� of the vertebrae when psoas is stretched past its barrier. (An alternative hand position is offered by Greenman (1996) who suggests that the stabilising contact on the pelvis should apply pressure towards the table, on the ischial tuberosity, as thigh extension is introduced.
The author agrees that this is a more comfortable contact than the sacrum. However, it fails to allow access to palpation of the lumbar spine during the procedure.) The practitioner eases the thigh (knee is flexed) off the table surface and senses for ease of movement into extension of the hip. If there is a strong sense of resistance there should be an almost simultaneous awareness of the palpated vertebral segment moving anteriorly. It should � if psoas is normal � be possible to achieve approximately 10� of hip extension before that barrier is reached, without force. Greenman (1996) suggests that �Normally the knee can be lifted 6 inches [15 cm] off the table. If less, tightness and shortness of psoas is present.� Having identified the barrier, the practitioner either works from this (in an acute setting) or short of it (in a chronic setting) as the patient is asked to bring the thigh towards the table against resistance, using 15�25% of their maximal voluntary contraction potential, for 7�10 seconds. Following release of the effort (with appropriate breathing assistance if warranted), the thigh is eased to its new barrier if acute, or past that barrier, into stretch (with patient�s assistance, �gently push your foot towards the ceiling�). If stretch is introduced, this is held for not less than 10 seconds and ideally up to 30 seconds. It is important that as stretch is introduced no hyperextension occurs of the lumbar spine. Pressure from the heel of hand on the sacrum can usually ensure that spinal stability is maintained. The process is then repeated.
Method (b) (Fig. 4.9A) Grieve�s method involves using the supine test position, in which the patient lies with the buttocks at the very end of the table, non-treated leg fully flexed at hip and knee and either held in that state by the patient, or by placement of the patient�s foot against the practitioner�s lateral chest wall. The leg on the affected side is allowed to hang freely with the medioplantar aspect resting on the practitioner�s far knee or shin.
Figure 4.9A MET treatment of psoas using Grieve�s method, in which there is placement of the patient�s foot, inverted, against the practitioner�s thigh. This allows a more precise focus of contraction into psoas when the hip is flexed against resistance.
Figure 4.9B Psoas treatment variation, with the leg held straight and the pelvis stabilised. The practitioner stands sideways on to the patient, at the foot of the table, with both hands holding the thigh of the extended leg. The practitioner�s far leg should be flexed slightly at the knee so that the patient�s foot can rest as described. This is used as a contact which, with the hands, resists the attempt of the patient to externally rotate the leg and, at the same time, flex the hip. The practitioner resists both efforts, and an isometric contraction of the psoas and associated muscles therefore takes place. This combination of forces focuses the contraction effort into psoas very precisely. Appropriate breathing instructions should be given (see notes on breathing, Box 4.2). If the condition is acute, the treatment of the patient�s leg commences from the restriction barrier, whereas if the condition is chronic, the leg is elevated into a somewhat more flexed position. After the isometric contraction, using an appropriate degree of effort (i.e. is this acute or chronic?), the thigh should, on an exhalation, either be taken to the new restriction barrier, without force (acute), or through that barrier with slight, painless pressure towards the floor on the anterior aspect of the thigh (chronic), and held there for 10�30 seconds (see Fig 4.10B; see also variation Fig. 4.9B). Repeat until no further gain is achieved.
Method (c) (Figs. 4.10A, B) This method is appropriate for chronic psoas problems only. The supine test position is used in which the patient lies with the buttocks at the very end of the table, nontreated leg fully flexed at hip and knee and either held in that state by the patient (Fig 4.10A), or by the practitioner�s hand (Fig 4.7B), or by placement of the patient�s foot against the practitioner�s lateral chest wall. The leg on the affected side is allowed to hang freely. The practitioner resists (for 7�10 seconds) a light attempt of the patient to flex the hip. Appropriate breathing instructions should be given (see notes on breathing, Box 4.2). After the isometric contraction, using an appropriate degree of effort, the thigh should, on an exhalation, be taken very slightly beyond the restriction barrier, with a light degree of painless pressure towards the floor, and held there for 10�30 seconds (Fig. 4.10B). Repeat until no further gain is achieved.
Figure 4.10A MET treatment involves the patient�s effort to flex the hip against resistance.
Figure 4.10B Stretch of psoas, which follows the isometric contraction (Fig. 4.10A) and is achieved by means of gravity plus additional practitioner effort.
Self-Treatment of Psoas
Method (a) Lewit suggests self-treatment in a position as above in which the patient lies close to the end of a bed (Fig 4.10A without the practitioner) with one leg fully flexed at the hip and knee and held in this position throughout, while the other leg is allowed to reach the limit of its stretch, as gravity pulls it towards the floor. The patient then lifts this leg slightly (say 2 cm) to contract psoas, holding this for 7�10 seconds, before slowly allowing the leg to ease towards the floor. This stretch position is held for a further 30 seconds, and the process is repeated three to five times. The counterpressure in this effort is achieved by gravity.
Method (b) Patient kneels on leg on side to be self-stretched so that the knee is behind the trunk, which remains vertical throughout. The non-treated side leg is placed anteriorly, knee flexed to 90�, foot flat on floor. The patient maintains a slight lumbar lordosis throughout the procedure as she lightly contracts psoas by drawing the treated side knee anteriorly (i.e. flexing the hip) without actually moving it. Resistance to this isometric movement is provided by the knee contact with the (carpeted) floor. After 7�10 seconds the patient releases this effort, and while maintaining a lumbar lordosis and vertical trunk, eases her pelvis and trunk anteriorly to initiate a sense of stretch on the anterior thigh and hip area. This is maintained for not less than 30 seconds before a further movement anteriorly of the pelvis and trunk introduces additional psoas stretch (see also Fig. 4.11B).
Figure 4.11A Alternative prone treatment position, not described in text (see also Fig. 4.8). B Psoas self-stretch, not described in text.
Dr. Alex Jimenez offers an additional assessment and treatment of the hip flexors as a part of a referenced clinical application of neuromuscular techniques by Leon Chaitow and Judith Walker DeLany.
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
A number of gastrointestinal diseases, GI diseases, are believed to be caused by intestinal barrier dysfunction, predisposing the gastrointestinal tract, or GI tract, to inflammation, including the development of inflammatory bowel disease, or IBD. While increased intestinal permeability is often considered to be a worsening symptom associated with GI disease, or gastrointestinal disease, clinical and experimental evidence has found that it may in fact be a factor to the development of digestive health issues.
Can increases intestinal permeability cause the development of food allergies?
Similar to IBD, food allergies are also believed to develop due to increased intestinal permeability. Food allergies are adverse, often dangerous immune system reactions which occur after certain food proteins/antigens are consumed. Food allergies are most common in babies and children, however, they can develop at any age. In this article, experimental and clinical data is summarized with current evidence relevant to intestinal permeability and intestinal barrier dysfunction in gastrointestinal diseases, GI diseases, and describe the potential implications of these research studies in disease pathogenesis.
Food Allergies & Intestinal Permeability
It is believed that intestinal barrier dysfunction can lead to both antigen sensitization in addition to the IgE/mast cell-mediated anaphylactic effector stage of disease. The development of food allergies is directly determined by the exposure of the food antigen to the mucosal immune system, which may be the cause for antigen sensitization as well as the production of dietary antigen-specific CD4+ Th2 cells and IgE. It is also believed that changes in intestinal barrier function allows increased amounts of dietary antigen to move across the intestinal barrier, exposing dietary antigens to the mucosal immune system, which can then lead to the development of the dietary antigen-specific reactions. Consistent with this concept, intestinal permeability in children with food allergies evaluated by a lactulose/mannitol ratio found in the urine, was significantly higher compared to that of healthy young children. To determine whether the changes in intestinal barrier function was a result of an adverse allergic reaction to dietary antigen, lactulose/mannitol ratios were analyzed in patients who had been on an allergen-free diet for a minimum of six months. Intestinal permeability remained elevated in these individuals, indicating that increased intestinal permeability continued even in the absence of food antigen stimulation.
Further information supporting a role for increased intestinal permeability in the development of food allergies and food antigen sensitization has been determined by current clinical and experimental research studies which have demonstrated a connection between increased intestinal permeability and the development of new-onset food allergies in patients after liver and heart transplants. Patients treated with the immunosuppressant tacrolimus, FK506 have demonstrated to have increased intestinal permeability as well as increased levels of food antigen-specific IgE. Several of these patients developed new-onset food allergies. The development of food allergies by immunosuppressed post-transplant patients was originally believed to be a result of the passive transfer of food antigen-specific IgE or lymphocytes from food-allergic donors to formerly non-allergic recipients. However, research studies have reported the development of food allergies in patients where the donor had no history of allergies. Interestingly, in vitro and in vivo experiments with rats have shown that tacrolimus triggers a dose-dependent growth in intestinal permeability demonstrating that tacrolimus-induced changes in intestinal barrier function might be a possible explanation for the new-onset food allergies in immunosuppressed post-transplant patients.
Tacrolimus has been demonstrated to detach mitochondrial oxidative phosphorylation, resulting in impaired mitochondrial energy production and a significant decrease in cellular ATP. Essentially, the formation of the intestinal barrier and also the maintenance of intercellular junctional complexes are energy-dependent processes and decreased cellular ATP is responsible for causing a breakdown in TJ complexes as well as intestinal barrier dysfunction. Consistent with this, rats treated with tacrolimus were demonstrated to have a dose-dependent growth in intestinal permeability that correlated with decreased intracellular ATP levels and CO2 release. In the same manner, liver transplant patients treated with tacrolimus were discovered to have decreased mitochondrial energy production associated with increased intestinal permeability and an increase in serum endotoxin levels.
The immunosuppressive activity of tacrolimus is through the inhibition of calcineurin, which is essential for IL-2 triggered T-cell activation Inhibition of IL-2 was demonstrated to promote T-helper 2 immune reactions. Th2 cells secrete IL-4, IL-5 and IL-13, which promote IgE-mediated allergic inflammation and set the stage for food antigen sensitization as well as the development of food allergies. There are probably several mechanisms involved in the pathogenesis of food allergies by tacrolimus-immunosuppressed patients and increased intestinal permeability is seemingly a significant mediator to help with the introduction of food antigens to the immune system and oral antigen sensitization.
Clinical and Experimental Findings in Intestinal Permeability and Food Allergies
Researchers provided experimental evidence supporting a role for intestinal permeability in oral antigen sensitization and the development of food allergies in mice. Researchers created a transgenic mouse that overexpresses the cytokine interleukin-9 specifically from the enterocytes of the small intestine (iIL-9Tg). A result of transgenic overexpression of IL-9 was a pronounced intestinal mastocytosis and changes in intestinal permeability. Repeated oral administration of OVA into iIL-9Tg BALB/c mice instead of WT mice boosted the development of antigen-specific IgE, CD4+ IL-4+ T-cells and symptoms of a food allergy reaction in the absence of preceding systemic sensitization or the utilization of adjuvant. Pharmacological mast cell depletion in iIL-9Tg mice has been found to restore intestinal permeability to levels similar to WT mice. Unexpectedly, regulating intestinal barrier function and decreased intestinal permeability in iIL-9Tg mice prevented orally-induced antigen sensitization. These findings indicate that increased intestinal permeability helps improve antigen uptake as well as the oral introduction of food antigen sensitization.
Intestinal barrier dysfunction is believed to add to the severity of food allergen-induced clinical and experimental symptoms. Oral challenge of food allergic individuals with food allergies developed a rise in lactulose/mannitol ratio in the urine. The level of intestinal barrier dysfunction positively connected to the severity of symptoms. Treatment of this food allergic group with sodium cromoglycate a mast cell stabilizer before ingestion of food allergen, significantly decreased lactulose permeability compared to food allergen-challenged individuals not becoming sodium cromoglycate demonstrating a role for mast cells in dietary antigen-induced intestinal epithelial barrier dysfunction.
Consistent with clinical observations animal variations of GI anaphylaxis and food allergy symptoms also have demonstrated increased intestinal permeability after oral antigen challenge. Intraluminal battle of egg-sensitized rats using egg albumin triggered a 15 times growth in uptake of 51cr-labelled EDTA as compared to rats treated with unrelated protein. Research studies using mast cell-deficient animals or pharmacological agents to deplete mast cells also have provided evidence demonstrating that mast cells are essential for changes to intestinal barrier function through food allergic reactions. Increased permeability after antigen challenge was shown to originally be the result of increased antigen uptake and translocation from the transcellular route, as evidenced by an increase in HRP-containing endosomes within minutes of HRP challenge in rats that were sensitized. The next phase, which occurs after sensitization and is mast cell-dependent, was associated with a disturbance in the TJs and an increase in paracellular permeability. Together, these research studies suggest a role for changes to intestinal barrier function in food allergy.
What’s more, these research studies suggest a role for mast cells in the regulation of intestinal barrier dysfunction in food allergy. Information referenced from the National Center for Biotechnology Information (NCBI) and the National University of Health Sciences. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
Intestinal Permeability: Alcohol and non-steroidal anti-inflammatory drugs, or NSAIDs, are harmful agents which can disrupt the balance of the digestive system, ultimately affecting the gastroduodenal mucosal and damaging the epithelial barrier along the gastrointestinal tract, or GI tract, increasing intestinal permeability. Moreover, it’s not uncommon for patients to have been exposed to the two substances at the same time. It is therefore important to know how simultaneous use can affect intestinal barrier function and acquiring that knowledge was the goal of several research studies.
What is the effect of alcohol and NSAIDs in intestinal barrier function?
Changes in intestinal permeability became more evident after Meddings et al. introduced the sucrose permeability test in 1993 as a non-invasive measure for evaluating the extent of gastrointestinal tract damage induced by non-steroidal anti-inflammatory agents, or NSAIDs. Subsequently, several studies demonstrated that intestinal barrier dysfunction to sucrose is a reasonable marker for the presence of GI tract damage in NSAID users. Other researchers used sucrose permeability tests to assess damage to the gastroduodenal mucosa induced by oral corticosteroids, intense exercise, infection, atrophic gastritis, Crohn�s disease, celiac disease, coffee, smoking, or a combination of these damaging factors. Alcohol is another agent that affects intestinal barrier function. A few studies have also demonstrated that acute alcohol consumption increases intestinal permeability. The effects of chronic exposure to alcohol on intestinal permeability, however, are less well established than that of NSAID use on intestinal permeability.
Intestinal Permeability:�Intestinal Barrier Dysfunction from NSAIDs and Alcohol
Non-Steroidal Anti-Inflammatory Drugs (NSAIDs)
The pathogenesis of NSAIDs is well investigated, but still not fully understood. The use of NSAIDs, or non-steroidal anti-inflammatory drugs, has been associated with the increased risk of developing gastrointestinal disease, or GI disease, as well as other digestive health side effects and issues. Considerable amounts of evidence have also demonstrated that, much like chronic alcohol consumption, constant use of NSAIDs can affect intestinal barrier function, which may cause significant GI tract, or gastrointestinal tract, damage, such as ulcers, perforation, hemorrhage and an exacerbation of inflammatory bowel disease, or IBD. It has been suggested that the effect of NSAIDs has separate phases.
First, NSAIDs are included into biological membranes because of their lipophilic properties. They interact with brush border phospholipids, causing direct damage to intestinal epithelium. NSAIDs also detach oxidative phosphorylation, which leads to mitochondrial dysfunction and, consequently, to a reduction in intracellular ATP. The decrease in ATP results in reduced intestinal epithelial barrier function, as the regulation of the intracellular actin-myosin complex is an ATP-dependent process. The regulation of membrane phospholipids and intracellular ATP levels are followed by leakage of intracellular calcium and increased production of free oxygen radicals. These processes will directly change intestinal permeability by affecting the contraction of the intracellular cytoskeleton and the integrity of the tight junction, or TJ, complex. This increased permeability then triggers the last phase of NSAID-induced enteropathy, which is the transportation of luminal compounds, such as bile acids, bacterial breakdown products, acid and pepsin, into the intestinal mucosa, triggering an immune response as well as inflammation. In addition to the phases mentioned above, NSAIDs can also induce mucosal damage by its prostaglandin-inhibiting properties. After absorption, NSAIDs inhibit cyclooxygenase-1 and -2, or COX-1 and -2. COX-1 inhibition leads to a decrease in mucosal blood flow, whereas inhibition of COX-2 has an effect on immune regulation.
Both acute and chronic use of non-steroidal anti-inflammatory drugs by healthy volunteers and patients demonstrated changes in intestinal barrier dysfunction and hypermotility, abnormal or excessive movement, specifically of the gastrointestinal tract. In vitro research studies utilizing MKN28, a gastric epithelial cell line has also demonstrated that aspirin-induced increase in permeability was characterized by a considerable decrease in the expression of claudin-7, but not claudins-3, -4, ZO-1 or occludin.
NSAID-induced gastrointestinal tract damage was initially found to be a consequence of cyclooxygenase inhibition and decreased prostaglandin synthesis; however, it is now evident that intestinal barrier dysfunction is a multi-stage process. Experimental and clinical research studies have demonstrated a contribution from neutrophils, microcirculatory disturbances, oxygen free radicals and bile acids in NSAID-induced GI tract damage. NSAIDs increase intestinal nitric oxide synthase expression, resulting in increased levels of NO, boosting intestinal permeability. NSAIDs may also detach mitochondrial oxidative phosphorylation, which impairs the mitochondrial energy generation required for TJ complex integrity, resulting in increased intestinal inflammation and permeability. Finally, a recent study demonstrated that aspirin induced an increase in gastric epithelial cell permeability which was mediated by activation of p38 MAPK and a decrease in claudin-7, and treatment where a p38 MAPK inhibitor attenuated this response.
Alcohol
Clinical and experimental research studies have revealed that constant alcohol consumption may often lead to increased intestinal permeability, inhibition of nutrient transportation, such as vitamins and minerals, and a decreased absorption of sodium and water. Research study evaluation results demonstrated the involvement of the byproduct of ethanol metabolism, acetaldehyde and nitric oxide, or NO, in alcohol-mediated intestinal barrier dysfunction. High levels of acetaldehyde were detected along the gastrointestinal tract, or GI tract, of rats following the administration of ethanol. Increased levels of acetaldehyde has also been closely associated with increased intestinal permeability and endotoxin translocation, according to the research studies. In addition, the incubation of Caco2 cells with acetaldehyde demonstrated increased monolayer permeability. The growth was associated with increased tyrosine phosphorylation of both ZO-1, E-cadherin and ?-catenin. Exposing Caco2 monolayers to ethanol also boosts inducible nitric oxide synthase expression, stimulating increased NO, or nitric oxide, production as well as increased monolayer permeability. NO-induced changes were associated with an increase in unstable, non-polymerized tubulin and extensive damage to the microtubule cytoskeleton.
Experimental and clinical research studies in rodents have also demonstrated that acute administration of alcohol can cause mucosal damage in the upper small intestine, such as villus ulceration, submucosal blebbing and hemorrhagic erosions as well as intestinal barrier dysfunction. It has been acknowledged that alcohol-induced intestinal permeability helps enhance translocation of endotoxins across various organs, resulting in tissue damage and inflammation. Intragastric application of endotoxins from alcohol administration in rodents provided considerably higher plasma endotoxin levels than animals fed endotoxin alone. Similar lesions have also been found in healthy volunteers and active alcoholics following acute alcohol consumption while plasma endotoxin levels in alcoholics were found to be 5 times greater than in healthy controls. While not entirely understood, evidence suggests that the mechanism inherent alcohol-induced intestinal barrier dysfunction is connected to the introduction of inflammatory cells and to the release of various mediators, including cytokines, reactive oxygen species, leukotrienes and histamine.
Maintenance of the intestinal barrier function is important for our health, and dysfunction may be a risk factor for a variety of disorders and diseases.�Information referenced from the National Center for Biotechnology Information (NCBI) and the National University of Health Sciences. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
Digestive health can be attributed to the optimal function of the gastrointestinal tract. By way of instance, however, if disease affects the structure of the gut, understanding its anatomy and function, can help healthcare specialists conclude a diagnosis outcome. The intestinal epithelium is a single layer of cells found lining the intestinal lumen, which plays the role of carrying out two essential functions in the digestive system. Its first function is to act as a barrier to prevent the passage of harmful intraluminal entities, such as foreign antigens, microorganisms and their toxins. Its second function is to act as a selective filter, allowing the translocation of important dietary nutrients, electrolytes and water from the intestinal lumen to the blood stream. The intestinal epithelium distinguishes selective permeability through two main pathways: the transepithelial/transcellular and paracellular pathways, as seen on Figure 1.
Transcellular permeability is generally related with the epithelial cells and is largely regulated by specific transporters in charge of also transferring amino acids, electrolytes, short chain fatty acids and sugars throughout the human body. Paracellular permeability is usually related to the transferring distance between epithelial cells and is greatly regulated by intercellular complexes found in the apical-lateral membrane junction and along the lateral membrane of the gastrointestinal tract, or GI tract. Interaction between the intestinal epithelial cells involves three components which can be identified at the ultrastructural level: desmosomes, adherens junctions, or AJs, and tight junctions, or TJs, as seen on Figure 2. The adhesive junctional complexes are made up of transmembrane proteins which connect adjacent cells to the actin cytoskeleton through cytoplasmic scaffolding proteins. The adherens junctions and desmosomes are believed to be more significant than the mechanical link of adjacent cells. The tight junctions, on the other hand, are the apical-most junctional complex, accountable for closing the intercellular space as well as regulating specific paracellular ionic solute transfer. The AJ and TJ complexes are also essential towards the regulation of cellular proliferation, polarization and distinction.
Structural Components of Junctional Complexes
Figure 1
Figure 2
Adherens Junctions (AJs)
The adherens junctions, also known as zonula adherens, are protein complexes located along the lateral membrane which happen in points of cell to cell contact, as seen on Figure 2. They’re shaped by interactions between transmembrane proteins, intracellular adaptor proteins and the cytoskeleton. The major AJs, or adherens junctions are formed by cadherin to catenin interactions. Epithelial (E)-cadherins, or calcium-dependent adhesion molecules, are Type-I single transmembrane spanning glycoproteins that contain an intracellular C-terminus and extracellular N-terminus. The extracellular domain creates homotypical interactions with the cadherins of neighboring cells to develop this cell to cell adhesion. The intracellular domain contains a catenin-binding domain that interacts with members of the armadillo repeat superfamily, ?-, ?- and p120-catenin. The catenins then connect the AJs into the cytoskeletal network through direct binding to the C-terminal domain of F-actin or indirectly through interactions with other adaptor proteins like afadin. Cadherin to catenin complexes are significant not only for connecting adjoining cells, but also for keeping cell polarity and for regulating epithelial migration and proliferation as well as the formation of additional adhesive complexes, such as desmosomes. In order to allow the link of adjoining cells, a decreased regulation of E-cadherin from the intestinal epithelium interrupts cell to cell adhesion which has been associated with affected intestinal epithelial proliferation and migration.
Nectin-afadin interactions create another significant AJ complex. Nectins, specificially nectin-1-4, are immunoglobulin-like proteins that withstand homophilic and heterophilic interactions with nectins on adjacent cells. Nectins can interact with the cytoskeleton through afadin, an F-actin binding protein, or rather preferably through interactions with other F- or ?-actin binding proteins including ponsin/SH3P12, vinculin and afadin dil domain-interacting proteins.
Tight Junctions (TJs)
The tight junctions are the apical-most adhesive junctional complexes in the epithelial cells of mammals which develop a continuous belt-like ring around epithelial cells at the boundary between the apical and lateral membrane regions of the gastrointestinal tract, according to Figure 2. Tight junctions, or TJs, are powerful, multi-protein complexes which serve as a selective/semipermeable paracellular barrier, that eases the passage of ions and solutes through the intercellular space, while also preventing the translocation of luminal antigens, microorganisms and their toxins. The progression of TJ biology began in the 1960’s with the development of electron microscopy. Evaluation and analysis of epithelial cells explained a series of apparent fusions, in which the space between adjacent epithelial cells had been eliminated. These so-called “kissing points” are morphologically different from AJs and desmosomes, where adjoining cell membranes stay approximately 15 to 20nm apart. Since the first observations, TJs have been found to include four families of transmembrane proteins: occludin, claudins, junctional adhesion molecules, or JAMs, and tricellulin.
The extracellular domains of transmembrane TJ proteins in adjoining cells anastomose to shape the TJ isolate. These interactions involve those proteins found in the exact same membrane as well as those including proteins in adjacent cells. Additionally, TJ proteins may form homophilic interactions, with the exact same protein, or heterophilic interactions, between non-identical TJ proteins. Like the adherens junctions, the intracellular domains interact with different scaffolding proteins, adaptor proteins and signaling complexes to moderate cytoskeletal attachment, cell polarity, cell signaling and vesicle trafficking, as seen on Figure 3. The intracellular regions of AJs possess PDZ-binding domains, which gather and come in contact with PDZ domain containing proteins. The PDZ domain (Post synaptic density-95/Drosophila disk large/Zonula occludens-1 protein) is a common structural domain of about 80 to 90 amino acids which play the role of anchoring transmembrane proteins to the cytoskeleton. The intracellular domains may also interact with non-PDZ-binding domain including proteins like cingulin, which can interact with junctional membrane proteins, the actin cytoskeleton and signaling proteins. The complex network of intracellular protein interactions can also be known as the “cytoplasmic plaque”.
Figure 3
Tight Junction Formation in the Gastrointestinal Tract
The intestinal epithelium shapes the largest and most essential barrier between our external and internal gastrointestinal tract environments. The barrier is preserved by the presence of AJs and TJs, such as cadherins, claudins, occludin and JAM proteins, which isolate groups of adjacent cells and maintains cytoskeletal anchorage, as seen on Figure 3. Expression of junctional proteins in the gut are highly regulated and dependent on both the small and/or large intestine, villus/crypt location and cell membrane specificity; apical, lateral or basolateral. The complex pattern of TJ expression from the gut is related to the particular functions of a distinct intestinal region and location. Expression of adherens junctions and tight junctions proteins can also be controlled by phosphorylation, according to Table 1. Phosphorylation can either promote TJ formation and barrier feature, or alternatively promote TJ protein redistribution and intricate destabilization.
Occludin
One of the first integral membrane proteins belonging specifically to the tight junctions to be recognized is the occludin. Occludin are predominantly found at TJs in the epithelial and endothelial cells but can also be located in astrocytes, neurons and dendritic cells. Occludin (60 to 82 kDa) is a tetraspanning integral membrane protein consisting of two extracellular loops, a short cytoplasmic N-terminus and a long cytoplasmic C-terminus. Analysis and evaluation of the function of these have demonstrated that the extracellular loops and transmembrane domains of occludin manage and maintain selective paracellular permeability. Intracellularly, the C-terminus interacts with the PDZ-domain containing protein ZO-1, which is required to connect occludin into the actin cytoskeleton, according to Figure 3.
Several occludin isoforms are characterized and believed to be the result of alternative mRNA splicing. Quite distinctly, many splice variants demonstrate altered subcellular distribution and interaction with other TJ molecules. Evaluation of these splice variants showed that the cytoplasmic C-terminal domain is funcamental for the intracellular exchange of occludin to the lateral cell membrane, which the fourth transmembrane domain name is important for targeting occludin into the TJ as well as for ZO-1 interactions.
The role of occludin is not fully outlined; nonetheless, data suggested another function for occludin from the regulation of paracellular permeability. The major allergen of the house dust mite, Der p 1, was determined to proteolyticly disrupt occludin altering this TJ complex and increasing paracellular permeability. In addition, hydrocortisone treatment of bovine retinal endothelial cells improved occludin expression two-fold and enhanced monolayer barrier properties. Though occludin is an important element of TJs, TJ formation and paracellular permeability barrier function are not dependent on occludin. Experimental investigations of occludin on mice demonstrated equivalent numbers and groups of TJs and corresponding paracellular ion passage as wild mice. Furthermore, epithelial transport and barrier function were normal in mice with occludin. Along with regulating paracellular permeability, there is evidence indicating occludin is included in cellular adhesion. Length of occludin at occludin and rat fibroblasts conferred cell to cell adhesion that has formally been interrupted by synthetic peptides associated to the first extracellular loop of occludin, underscoring the significance of the area of occludin in cell adhesion.
Evaluations indicated that occludin found along the TJ complex is regulated by phosphorylation. Several potential phosphorylation sites at tyrosine, serine, and threonine residues of occludin have been identified where the regulation of occludin phosphorylation is proposed to happen by kinases, for instance, non-receptor tyrosine kinase c-Yes and protein kinase C (PKC), and phosphatases including the serine/threonine protein phosphatase 2A, according to Figure 3. PKC?, a novel protein kinase predominantly expressed in the intestinal epithelium, was demonstrated to directly phosphorylate occludin in threonine residues (T403 and T404). Blockade of all PKC?-mediated occludin phosphorylation interrupted junctional distribution of occludin and ZO-1 and interrupted epithelial barrier function. The data suggest that occludin phosphorylation modulates occludin-ZO-1 interactions and the maintenance of intact TJ complexes and paracellular barrier function.
Claudins
Claudins are 20 to 27 kDa integral membrane proteins with four hydrophobic transmembrane domains, two extracellular loops and N- together with C-terminal cytoplasmic domains. The extracellular loops are crucial for homophilic and/or heterophilic TJ protein to protein interactions alongside the creation of ion-selective channels. The intracellular C-terminal domain is included in anchoring claudin into the cytoskeleton through connections with PDZ-binding domain names, such as ZO-1, -2 and -3, according to Figure 3. Presently, 24 distinct claudin family receptor members are identified in those who have a number of orthologues expressed in various species. They exhibit distinct cell, tissue and developmental stage-specific expression routines.
Claudin to claudin interactions between adjoining cells might be homophilic or heterophilic. Homophilic interactions have been shown for claudins 1, 2, 3, 5, 6, 9, 11, 14 and 19. On the reverse side, heterophilic interactions are more restricted and largely have been detected with claudin-3, which could interact with claudins-1, -2 and -5. Notably, there’s specificity in heterophilic trans-interactions. By way of instance, transfection of fibroblasts with claudins-1, -2 and -3 led to claudin-3 interactions with claudin-1 and -2; yet no interactions involving claudin-1 and -2 were detected. These discerning interactions are considered to describe the diversity in TJ formations and provide a molecular basis for tissue-specific heterogeneity of barrier function.
Recent study, together with claudin-deficient mice also give corroborative information supporting a role for claudins in the law of barrier function. Claudin-1 mice die within a day of birth due to significant transepidermal water loss. Furthermore, transgenic overexpression of both claudin-6 in skin disrupted tight junction formation and increased epithelial permeability. Experimental data indicates that claudins could have differential impacts on paracellular permeability. By way of instance, introduction of claudin-2 to MDCK I cells which state claudin-1 and -4 activates a decrease in transepithelial resistance, or TER; whereas transfection of claudin-3 had no effect indicating that claudin-2 markedly diminished claudin-1/claudin-4 based TJ strand regeneration. In support of the latest experimental evidence indicates that claudins can form measurements and charge-specific paracellular stations. Transfection of claudin-8 into MDCK II cells that lacks endogenous claudin-8 substantially reduced paracellular movement without impacting anion and uncharged solute movement. Experimental investigations suggest that the first extracellular loop of claudins play an essential role in deciding charge selectivity. Interchanging of the earliest or extracellular domains of claudin-4 on claudin-2 profoundly diminished the ion conductance of Na+ relative to Cl? 76. Additionally, substitution of a negatively-charged lysine into some positively charged aspartic acid (K65D) inside the loop of claudin-15 generated an increase in Na+ permeability, whereas mutation in exactly the same place of three positively charged amino acids into negatively charged aspartic acid, arginine and aspartic acid (E46K, D55R and E64K) altered the ion selectivity of claudin-15 in Na+ to Cl? channel. Pore size and density may also impact paracellular movement of non invasive and charged charged solutes.
Claudins also play an essential role in epithelial cell invasion and motility. Overexpression of claudins-3 and -4 in human ovarian epithelial cells, which lack the expression of these proteins, has been connected with enhanced epithelial cell survival and enhanced invasion and motility. Consistent with this observation, siRNA-mediated knockdown of the two claudins-3 and -4 in ovarian cancer cell lines diminished intrusion. The outcome of claudin-3 appear to get connected to altered matrix metalloprotease-2 activity, meaning claudin-induced invasion could possibly be regulated by metalloprotease proteins.
Similar to occludin, claudin localization to the TJ complex and its function are regulated by post-translational phosphorylation and through connections with PDZ-binding domains. The intracellular C-terminal domain of claudin possesses multiple regulatory sites, such as possible serine and theronine phosphorylation sites and PDZ-binding domain names. Phosphorylation of claudins-3 and -4 in prostate cancer cells is closely connected to the regulation of paracellular permeability. By way of instance, patients with pseudohypoaldosteronism type II (PHA II; or vitamin shunt syndrome) present with hyperkalemic metabolic acidosis, hypertension and dysregulated paracellular ion transport. The molecular basis is connected to some loss-of-function mutation from the serine-threonine kinases, WNK1 and WNK4, which regulate epithelial chloride cotransporters. This also contributes to an increase in the phosphorylation of both claudins-1-4 and an increase in paracellular permeability. A lot of signaling pathways are implicated in the phosphorylation of claudins like PKC, Rho GTPases, mitogen-activated protein kinases (MAPKs) and phosphatases. MAPK phosphorylation of claudin-1 is required for claudin-1-mediated barrier function. Furthermore, claudins-1, -2, -7, -8, -16 and -17 have putative PKC phosphorylation websites.
All claudins, except claudin-12, completing from the dipeptide arrangement YV, that’s been shown to interact with PDZ-binding domains comprise ZO-1, -2 and -3, multi-PDZ domain name and PALS1-associated TJ protein, according to Figure 3. Several of those scaffolding proteins contain several PDZ domains, which eases the introduction of dense localized protein complexes, also called “cytoplasmic plaques”. Also, the scaffolding proteins can interact with signaling molecules, such as heterodimeric GTP binding proteins (Rab13 and G?12), transcriptional factors and RNA-processing variables, to connect TJ complexes to the actin-cytoskeleton and modulate aspects of adrenal polarization, differentiation and barrier function.
Junctional Adhesion Molecules (JAMs)
Junctional adhesion molecules are integral membrane proteins which belong to the immunoglobulin superfamily and have two immunoglobulin folds, the VH- and C2-type, from the extracellular domain. JAMs are expressed by multiple cell types, including epithelial, endothelial and immune cells. They’re subdivided based on the expression of Type I or II PDZ-binding themes in the intracellular C-terminus, which implies that the two types interact with exceptional scaffolding and cytoplasmic proteins. JAM-A, -B and -C (or JAM1-3) have Type II binding subjects, while the atypical JAMs, such as JAM-4, coxsackie and adenovirus receptor (CAR) and endothelial selective adhesion molecule make up Type I PDZ-binding domains. Comparable to additional TJ proteins, these JAM-PDZ interactions provide anchorage to the actin cytoskeleton, according to Figure 3.
The extracellular region of JAMs adapting to multiple ligands through homophilic and heterophilic interactions, which can be proposed to regulate the mobile functions and paracellular permeability of JAMs. Homophilic JAM-A or -B interactions govern the creation of operational TJs and cell to cell border formation, while heterophilic JAM interactions play a role in leukocyte-endothelial cell adhesion.
Recent studies demonstrate the significance of JAM-A at the formation and assembly of TJs in intestinal epithelial cells. SiRNA downregulation of JAM-A at SK-C015 epithelial cells triggered an increase in permeability. Consistent with this, JAM-A mice had increased mucosal permeability as indicated by enhanced dextran flux and decreased TER. Nonetheless, these mice also had an increase in claudin-10 and -15 expression, which is believed to shape selective pores from the TJ complex, improving paracellular permeability. Interestingly, JAM-A mice have increased susceptibility to chemical-induced colitis. Dextran sodium sulfate administration to JAM-A mice induced more acute colonic injury as compared to WT control animals. These studies imply altered intestinal permeability for a susceptibility factor to autoimmune disorder.
The above information is evidence-based. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
A healthcare professional at a gastroenterology practice, such as a dietitian specializing in gastrointestinal diseases, will often care for a great deal of individuals who walk into their clinic reporting symptoms which haven’t yet been diagnosed to a specific digestive health issue. Because not many primary care physicians are in charge of diagnosing GI diseases nor are they properly aware of their wide array of symptoms, many people with gastrointestinal diseases will often go undiagnosed for years.
How can you talk to your doctor about your digestive issues?
A healthcare provider specializing in gastrointestinal diseases may look out for certain symptoms, as well as possible dietary triggers, to determine a digestive health issue. Simple lifestyle changes are generally the best treatment method to help improve GI diseases and its symptoms, however, being able to communicate accordingly with your doctor can help them diagnose your problem more accurately in order to begin treatment immediately. By following a few factors the patient can control, they can ensure their medical diagnostic procedure is fast, easy, and correct.
Arrive to your Appointment on Time
While careful planning and preparations can occasionally be sabotaged by events and situations that are out of our control, it’s essential for you to initially intend to reach your appointment on time. It’s recommended to arrive at least 15 minutes before your original appointment time, especially if you are a new patient as you will need to complete the necessary paperwork on your first visit. If you show up 15 minutes late for a 15 minute appointment, there is a great chance you’ll be hurried through your visit without ample time to go over your issues thoroughly with your doctor.
Bring Evaluation Results & Procedure Reports
It can’t be emphasized enough how common it is for patients to not know which previous diagnostic tests or even surgeries they’ve gone through for their specific disease and/or condition. If you show up to a healthcare professional’s appointment for further diagnosis and a second opinion regarding your symptoms without being aware of this information, your doctor may waste valuable time and money re-testing you for digestive health issues which may have already been ruled out by another healthcare specialist. Furthermore, without previous evaluation results and/or procedure reports, doctors can miss an obvious diagnosis based on your health history, or worse, they may perform yet another invasive procedure which you no longer needed.
If you have had an endoscopy or a colonoscopy, what were the signs? If you’ve had surgery somewhere on your gastrointestinal tract, which process was it? If you have experienced a breath test, what were they checking for and what were the results? If blood has been drawn lately, what was being checked and also what, if anything, has been discovered? Have you had any specialized tests that involved imaging of your gastrointestinal tract? These are all important questions you must know before visiting a doctor’s office.
Also, to get to a faster diagnosis, your best option is to bring copies of all relevant tests and reports you have undergone related to your digestive health issues. It may take some effort to collect these results from previous doctors or even hospitals, though medical practices offering online patient portals may make this procedure easier. If you can’t obtain the true exam results, then compiling a summarized “medical resume” may be the next best thing. Just type up a list of all of the test names or procedure reports you’ve had; who ran them (as well as where and when they were performed); and exactly what they discovered, based on those evaluations and procedures. Hand the sheet to your healthcare professional. Their office can then track down copies of any relevant results after you leave from your first appointment.
Describe your Symptoms in Detail
It can be quite embarrassing to describe your digestive symptoms to a healthcare professional and you might even feel unsure of whether you may actually have a digestive issue based on your “normal” collection of gut sounds, backed up stools and that occasional nausea you experience after eating a heavy meal. You may be tempted to use more conservative, generic phrases to describe your symptoms but healthcare specialists say you don’t have to be considerate. Your doctor has literally heard it all and it is as routine to them as speaking about the weather is to everyone else.
If you say that you “get sick to your stomach” when referring to having diarrhea, for instance, the healthcare professional may actually think you are referring to nausea. If you say “constipated” to refer to straining to have a daily bowel movement, your doctor may presume you mean you are unable to move your bowels more than once or twice per week. If you say you get a “stomachache” after eating, it could refer to sharp pain, cramps or dull pain and it doesn’t properly inform your doctor where the pain is located. Tell your doctor exactly what you mean, along with all of the extra descriptive details. What’s happening and where, what it looks like, what it smells like, what it feels like and how frequently it happens. Correctly describing your symptoms is key to a correct diagnosis.
Mention When your Symptoms Started
At times, telling your healthcare specialist when your symptoms all started can be the clue to your diagnosis. Did you notice your digestive health issues after you recovered from a bout of food poisoning in your holiday? Did things change for you in the bathroom after having your gallbladder removed? Did your digestive discomfort increase after switching to a brand new diet, such as a 30-day cleanse, Weight Watchers or a paleo-style diet? Do your symptoms coincide with starting or stopping a particular drug/medication or supplement? Have you experienced this digestive health issue since you were a child? Did your issue get better or worse during pregnancy? Putting your complaints in context will help your doctor perform a better medical diagnostic procedure.
Inform your Doctor of What you Have & Haven’t Tried
Doctors often learn just as much out of what hasn’t helped you feel better as they do from what has helped you feel better. If you have already tried a drug/medication, supplement, lifestyle changes, including diet modifications and physical activities, to address your gastrointestinal issues and it has not worked, make sure you incorporate this in your conversation with your healthcare specialist. It will help them narrow down the list of possibilities and help point to more likely gastrointestinal diseases and conditions.
Keep an Open Mind
Now that we all have access to the internet, we’ll often arrive to a doctor’s appointment with a preconceived notion about what we believe we may have. Because of this, many patients may attempt to steer the conversation toward this self-diagnosis and accidentally leave out important information that could shed light on the correct diagnosis. It is absolutely appropriate to share your own hypothesis about your digestive health issue with your healthcare provider and this can be particularly more important if you’ve got a family medical history which may accurately indicate your problem. But be sure to share all the details of your conclusion, and be open to the possibility that your doctor may see matters in a different light than all the other articles you may have read on the internet. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine





 Nutritional Strategies: The focus of this paper is to explore better strategies for optimizing bone strength and reducing risk of fracture, while at the same time decreasing risk of cardiovascular disease. The majority of Americans do not consume the current recommended dietary allowance for calcium, and the lifetime risk of osteoporosis is about 50%. However, traditional mono-nutrient calcium supplements may not be ideal. We comprehensively and systematically reviewed the scientific literature in order to determine the optimal dietary nutritional strategies and nutritional supplements for long- term skeletal health and cardiovascular health. To summarize, the following steps may be helpful for building strong bones while maintaining soft and supple arteries: (1) calcium is best obtained from dietary sources rather than supplements; (2) ensure that adequate animal protein intake is coupled with calcium intake of 1000 mg/day; (3) maintain vitamin D levels in the normal range; (4) increase intake of fruits and vegetables to alkalinize the system and promote bone health; (5) concomitantly increase potassium consumption while reducing sodium intake; (6) consider increasing the intake of foods rich in vitamins K1 and K2; (7) consider including bones in the diet; they are a rich source of calcium-hydroxyapatite and many other nutrients needed for building bone.
Nutritional Strategies: The focus of this paper is to explore better strategies for optimizing bone strength and reducing risk of fracture, while at the same time decreasing risk of cardiovascular disease. The majority of Americans do not consume the current recommended dietary allowance for calcium, and the lifetime risk of osteoporosis is about 50%. However, traditional mono-nutrient calcium supplements may not be ideal. We comprehensively and systematically reviewed the scientific literature in order to determine the optimal dietary nutritional strategies and nutritional supplements for long- term skeletal health and cardiovascular health. To summarize, the following steps may be helpful for building strong bones while maintaining soft and supple arteries: (1) calcium is best obtained from dietary sources rather than supplements; (2) ensure that adequate animal protein intake is coupled with calcium intake of 1000 mg/day; (3) maintain vitamin D levels in the normal range; (4) increase intake of fruits and vegetables to alkalinize the system and promote bone health; (5) concomitantly increase potassium consumption while reducing sodium intake; (6) consider increasing the intake of foods rich in vitamins K1 and K2; (7) consider including bones in the diet; they are a rich source of calcium-hydroxyapatite and many other nutrients needed for building bone. Most vegetarians, especially vegans, appear to absorb less calcium because of the oxalic and phytic acid contained in many plant, grain and legume products.1 Indeed, several studies have reported that risks of bone fracture are higher in vegans�likely due, at least in part, to their lower dietary calcium intake, and/or poor absorption of this key mineral (table 1).21
Most vegetarians, especially vegans, appear to absorb less calcium because of the oxalic and phytic acid contained in many plant, grain and legume products.1 Indeed, several studies have reported that risks of bone fracture are higher in vegans�likely due, at least in part, to their lower dietary calcium intake, and/or poor absorption of this key mineral (table 1).21
 Maintaining replete magnesium status may reduce risk for the metabolic syndrome, diabetes, hypertension and MI.30 Circumstantial and experimental evidence has also implicated magnesium deficiency in osteoporosis.31�34 Optimal dietary magnesium intake is about 7�10 mg/ kg/day, preferably in the context of a net base-yielding diet, since a net acid-yielding diet increases excretion of both magnesium and calcium (table 2).
Maintaining replete magnesium status may reduce risk for the metabolic syndrome, diabetes, hypertension and MI.30 Circumstantial and experimental evidence has also implicated magnesium deficiency in osteoporosis.31�34 Optimal dietary magnesium intake is about 7�10 mg/ kg/day, preferably in the context of a net base-yielding diet, since a net acid-yielding diet increases excretion of both magnesium and calcium (table 2). Vitamin K2 intake has been associated with decreased arterial calcium deposition and the ability to reverse vascular calcification in animal models. Vitamin K2 prevents pathological calcification in soft tissues via the carboxylation of protective MGP. The undercarboxylated (inactive) species of MGP is formed during inadequate Vitamin K status, or as a result of Vitamin K�
Vitamin K2 intake has been associated with decreased arterial calcium deposition and the ability to reverse vascular calcification in animal models. Vitamin K2 prevents pathological calcification in soft tissues via the carboxylation of protective MGP. The undercarboxylated (inactive) species of MGP is formed during inadequate Vitamin K status, or as a result of Vitamin K�

 adequate calcium intake without predisposing to CVD risk. Ingestion of micro- crystalline hydroxyapatite (the form of calcium found in bone) produces less of an acute spike in blood calcium levels compared to soluble calcium salts typically used in standard supplements, and thus may be less likely to increase vascular calcification and coronary risk.65 Hydroxyapatite also stimulates bone osteoblast cells and contains virtually all the essential building blocks needed to construct bone tissue. In a small placebo- controlled randomized trial, women who took 1000 mg of calcium in the form of hydroxyapatite in conjunction with oral Vitamin D showed a significant increase in bone thickness, whereas those who took 1000 mg of a standard calcium carbonate supplement did not (figure 4).70 Another double-blind placebo-controlled study found�
adequate calcium intake without predisposing to CVD risk. Ingestion of micro- crystalline hydroxyapatite (the form of calcium found in bone) produces less of an acute spike in blood calcium levels compared to soluble calcium salts typically used in standard supplements, and thus may be less likely to increase vascular calcification and coronary risk.65 Hydroxyapatite also stimulates bone osteoblast cells and contains virtually all the essential building blocks needed to construct bone tissue. In a small placebo- controlled randomized trial, women who took 1000 mg of calcium in the form of hydroxyapatite in conjunction with oral Vitamin D showed a significant increase in bone thickness, whereas those who took 1000 mg of a standard calcium carbonate supplement did not (figure 4).70 Another double-blind placebo-controlled study found�