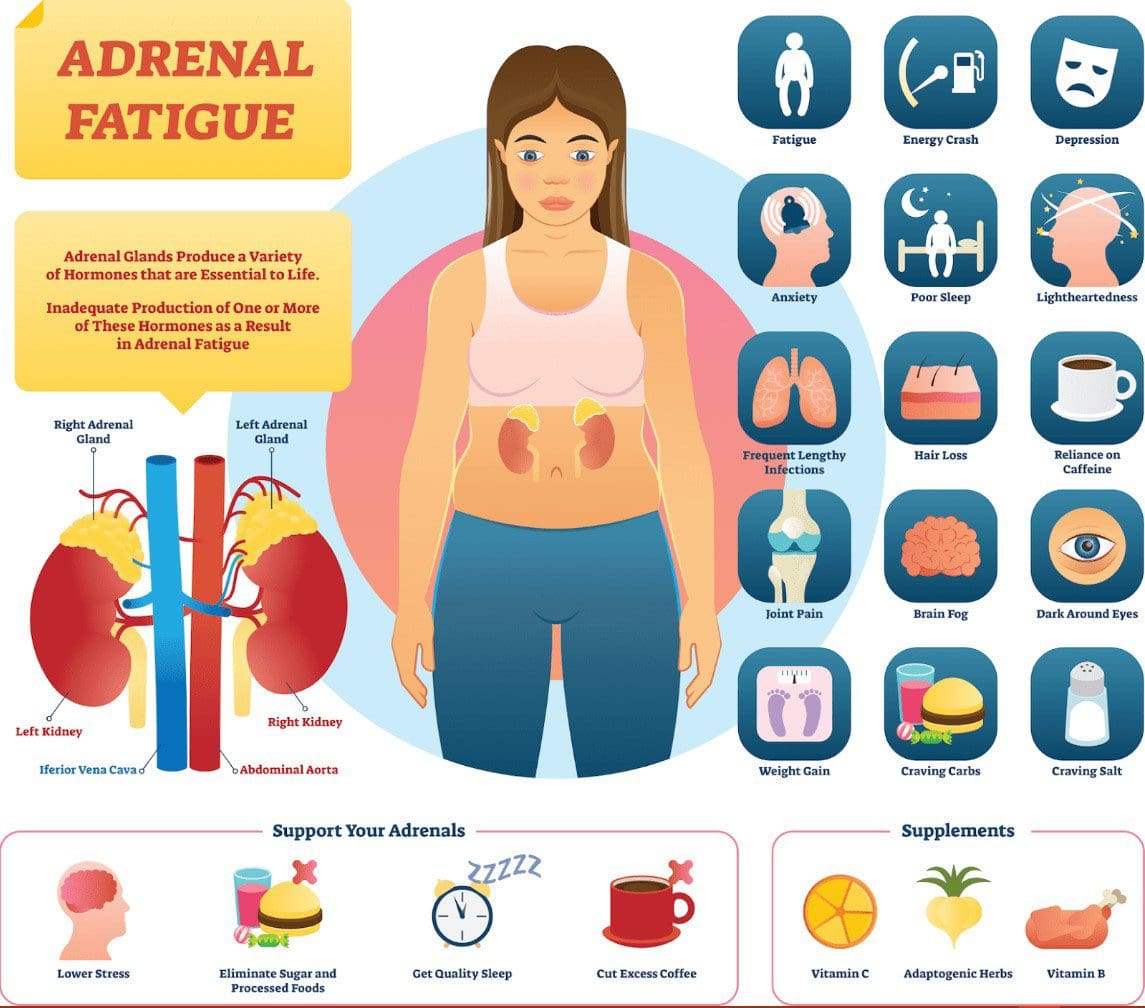
The adrenal glands are small and sit above the kidneys. The glands help the body burn fat and protein and regulate sugar, blood pressure, and stress response. They create, release, and regulate hormones like cortisol and adrenaline. Conditions like chronic fatigue, brain fog, and burnout cause individuals to be exhausted during the day and unable to fall asleep at night. Symptoms can also include hair loss, weight fluctuation, increased cravings, and difficulty recovering from illness. Nutrition support plays a major role in healing adrenal fatigue.
Nutrition Support
Adrenal fatigue nutrition support is a food-based approach to optimize adrenal gland function. The objective is to increase energy levels naturally, so the body doesn’t burn stored nutrients. Adrenal gland optimization involves learning ways to reduce and manage stress, getting healthy sleep, and making lifestyle adjustments.
Adrenal Fatigue
When stress activates, the adrenal glands release cortisol. Researchers theorize that when the body experiences high levels of chronic stress, the adrenal glands may not be able to produce enough cortisol to maintain healthy function, which can lead to adrenal fatigue.
Adrenal fatigue should not be confused with adrenal insufficiency, a verified medical condition where the adrenal glands cannot produce enough hormones.
Fatigue Symptoms
Symptoms of adrenal fatigue include:
Chronic low energy levels
Difficulty waking up
Difficulty falling asleep
Increased cravings for salt or sugar
Dependence on stimulants like caffeine
Other health conditions could also cause symptoms.
Foods to Avoid
Decreasing foods and drinks high in refined and processed sugar and unhealthy fats are recommended. Some foods to limit include:
It’s also recommended to time meals to help manage blood sugar levels. Skipping meals forces the body to burn stored nutrients that can reduce energy levels. Maintaining breakfast and lunch and regular balanced snacks can help maintain energy levels throughout the day. Maintaining hydration is also important, as dehydration can influence stress levels and cause the adrenal glands to produce cortisol.
Recommended Foods
Doctors and nutritionists recommend balancing nutrient-dense sources of protein, healthy fats, and carbohydrates. Nutrition support foods include:
Lean meats
Fatty fish – Salmon and sardines are great protein sources as they are loaded with healthy omega-3 fatty acids, which can reduce inflammation and promote improved brain health.
Leafy greens – These vegetables contain magnesium, like spinach, kale, and Swiss chard. The body needs magnesium to carry out various functions, which also helps the body relax and manage stress more effectively. When there is trouble falling asleep, it could be a deficiency in this mineral.
Sea salt – Individuals with adrenal fatigue experience electrolyte imbalances. This is caused by a deficiency in the steroid hormone aldosterone. Adding sea salt will help balance electrolytes and minimize symptoms, specifically those related to blood pressure.
Olive oil
Avocado – The body needs a good amount of healthy fat to help the body heal. A low-fat diet is not ideal for dealing with hormonal issues like adrenal fatigue, as the body needs fat and cholesterol to produce hormones. Avocados contain high monounsaturated fats and fiber that help the body detox and digest food more efficiently.
Healing
A nutrition plan addressing adrenal fatigue can increase energy levels, regulate blood pressure, and promote healthier eating habits. Talking with your doctor and a nutritionist is recommended for optimal results, as they can develop a personalized health plan that addresses the following:
Lifestyle adjustments
Healthy sleep schedule
Managing stress
Physical activity
We are here for you at Injury Medical Chiropractic and Functional Wellness Clinic to learn more about adrenal fatigue and how to manage it. Contact us for more information on our services or to schedule an appointment for a consultation.
Adrenal Dysfunction Patterns
References
ABDULLA, Jehan, and B. DJ Torpy. “Chronic Fatigue Syndrome.” Endotext, edited by Kenneth R Feingold et al., MDText.com, Inc., 20 April 2017.
Allen, Loyd V Jr. “Adrenal fatigue.” International journal of pharmaceutical compounding vol. 17,1 (2013): 39-44.
Galland, Leo. “The gut microbiome and the brain.” Journal of medicinal food vol. 17,12 (2014): 1261-72. doi:10.1089/jmf.2014.7000
Immune system health and keeping the system strong and healthy can be accomplished by maintaining healthy eating habits. Eating foods rich in specific vitamins and supplements can help the immune system fight off illness, maintain energy levels, and help during injury recovery. Here we look at choosing foods with the right vitamins to build and strengthen the immune system throughout the year.
Immune System Health
The immune system consists of complex cells, processes, and chemicals that constantly defend the body against invading pathogens, including viruses, toxins, and bacteria. Keeping the immune system healthy year-round is key to infection and disease prevention. Healthy lifestyle choices consist of the following:
Nutritious food, healthy sleep, physical activity, and exercise are the most important ways to strengthen the immune system.
Supplementing certain vitamins, minerals, and herbs can help improve immune response.
However, some supplements can interact with prescription or over-the-counter medications.
Certain supplements may not be recommended for individuals with certain health conditions.
Research has found that selenium activates the immune system when there is a threat and signals when to slow or shut down immune responses.
Selenium keeps the immune system from overworking.
Selenium protects from chronic inflammation and autoimmune diseases like rheumatoid arthritis, Crohn’s disease, and psoriasis.
Selenium Foods
Foods from highest to lowest levels of selenium.
Brazil nuts
Tuna
Halibut
Canned sardines
Lean meats
Cottage cheese
Brown rice
Eggs
Oatmeal
Milk
Yogurt
Lentils
Nuts
Seeds
Peas
Increase Water Intake
Maintaining healthy hydration can increase immune health.
Water helps the body produce lymph, which carries white blood cells and other immune system cells.
Try to balance out dehydrating beverages, like coffee and soda.
Try eating more hydrating foods like cucumbers, celery, lettuce, and strawberries.
Immune System Health
References
Chaplin, David D. “Overview of the immune response.” The Journal of allergy and clinical immunology vol. 125,2 Suppl 2 (2010): S3-23. doi:10.1016/j.jaci.2009.12.980
Halliwell, B. “Antioxidants in human health and disease.” Annual review of nutrition vol. 16 (1996): 33-50. doi:10.1146/annurev.nu.16.070196.000341
Lewis, Erin Diane, et al. “Regulatory role of vitamin E in the immune system and inflammation.” IUBMB life vol. 71,4 (2019): 487-494. doi:10.1002/iub.1976
Mora, J Rodrigo, et al. “Vitamin effects on the immune system: vitamins A and D take center stage.” Nature reviews. Immunology vol. 8,9 (2008): 685-98. doi:10.1038/nri2378
Nicholson, Lindsay B. “The immune system.” Essays in biochemistry vol. 60,3 (2016): 275-301. doi:10.1042/EBC20160017
Shakoor, Hira, et al. “Immune-boosting role of vitamins D, C, E, zinc, selenium and omega-3 fatty acids: Could they help against COVID-19?.” Maturitas vol. 143 (2021): 1-9. doi:10.1016/j.maturitas.2020.08.003
The holidays are a wonderful time to gather with family and friends and celebrate. However, it can be a time of overindulgence and overeating. Managing holiday eating habits is achievable by having options to help you make better choices so you can indulge and enjoy the festive food and drinks without overdoing it. Here are a few techniques to be successful.
Managing Holiday Eating
Many individuals overeat during the holidays. It’s understandable as the holiday season means letting loose, relaxing with friends and family, and enjoying the moment are major factors in overeating as auto-pilot is engaged. The next thing you know, the plate is clean, and more food is being added. It’s all about maintaining a healthy balance. Here are a few ways to manage holiday eating.
Adding superfoods to your holiday nutrition plan to help balance food indulgences. These are foods with high levels of vitamins and nutrients, dietary fiber that helps reduce cholesterol, and antioxidants that fight free radicals.
Nutrients
Vitamin A – Protects against infections and promotes eye and skin health.
Vitamin C – Helps heal wounds and aids in iron absorption.
Vitamin K – Supports healthy digestion and blood clotting.
Superfoods include dark leafy greens, nuts, fruits, dark chocolate, olive oil, and oily/fatty fish. Here are a few superfoods you can enjoy:
Sweet Potatoes
Rich in vitamins A and C, fiber, and potassium.
Beans
They are high in fiber and protein, magnesium, and potassium.
Pumpkins
High in fiber and vitamin A.
Pomegranates
Rich in flavonoids and tannins are a healthy source of folate, potassium, and vitamin K.
Cranberries
Contain antioxidants with anti-inflammatory properties that help reduce the risk of cardiovascular disease.
Kale
Low in calories.
High in vitamins A, C, and K, manganese, potassium, and fiber.
From the Injury Medical Chiropractic and Functional Medicine Team, have a happy, safe, and healthy Thanksgiving!
Functional Nutrition
References
Seven tips for reining in holiday overeating https://www.mayoclinichealthsystem.org/hometown-health/speaking-of-health/7-tips-for-reining-in-holiday-overeating
Brown, Tanya, et al. “Have a Food-Safe Holiday Season.” Journal of the Academy of Nutrition and Dietetics vol. 117,11 (2017): 1722-1723. doi:10.1016/j.jand.2017.08.123
Díaz-Zavala, Rolando G et al. “Effect of the Holiday Season on Weight Gain: A Narrative Review.” Journal of obesity vol. 2017 (2017): 2085136. doi:10.1155/2017/2085136
Get Your Superfood Nutrition for Good Health https://www.scripps.org/news_items/4431-get-your-superfood-nutrition-for-good-health.
Healthline, 2019; Ruled by Food? 5 Strategies to Break the Cycle of Overeating https://health.clevelandclinic.org/ruled-by-food-5-strategies-to-break-the-cycle-of-overeating/
Healthline, 2019; 23 Simple Things You Can Do to Stop Overeating https://www.healthline.com/nutrition/how-to-stop-overeating.
Lobo, V et al. “Free radicals, antioxidants, and functional foods: Impact on human health.” Pharmacognosy reviews vol. 4,8 (2010): 118-26. doi:10.4103/0973-7847.70902
What Is a Superfood, Anyway? https://health.clevelandclinic.org/what-is-a-superfood/
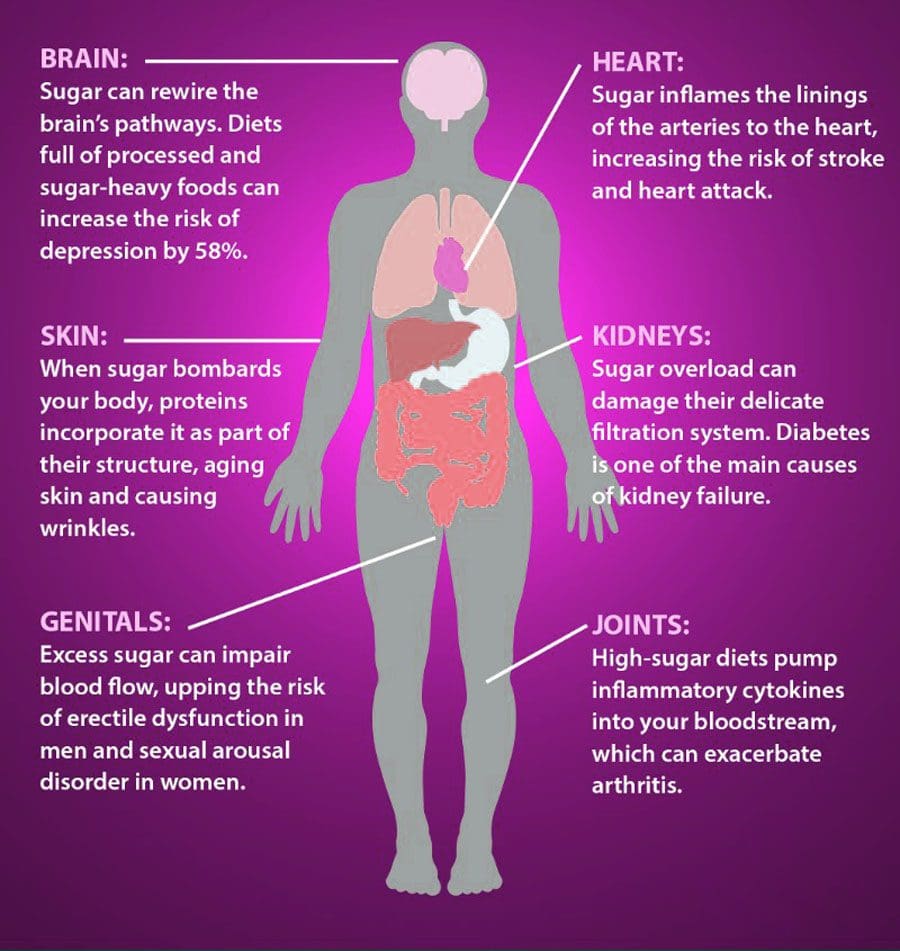
The fascia is important for connecting the musculoskeletal system, stabilizing function, and keeping the body healthy and balanced. Sugar consumption and the abundance of sugar in the body that doesn’t get burned directly negatively affect the fascia, making it lose its elasticity and affecting other connective tissues. Excess sugar in the blood leads to a pathological process called glycation. One effect of glycation is binding sugar molecules to fascial proteins, causing them to thicken and stiffen. The body sees the tangled molecules as foreign bodies initiating an inflammatory response to get rid of them. This can lead to chronic inflammation causing various symptoms. The Injury Medical Chiropractic and Functional Medicine Clinic Team will address soreness, pain, and discomfort associated with fascia problems.
Myofascial Tissue
Myofascia or fascia is a layer of tissue that connects and supports the spine and muscles. It wraps and links internal body parts in bands, fusing them. This ensures the muscles can move freely without experiencing friction with other body parts.
Fascia is made of collagen, creating a tough and flexible texture that provides tension and elasticity.
Fascia is found around muscles, nerves, blood vessels, blood and cells, organs, and bones.
When the body stays or moves in repetitive patterns, the fascia can memorize certain positions/postures and hold the fascia in a contracted state. For example, sitting at a desk workstation causes the gluteal muscles, tendons, and ligaments to stretch and pull the muscles around them. The gluteal muscles can become restricted without releasing and training the fascia to return to a retracted position, causing tension and myofascial discomfort. When the body is in balance/homeostasis, and the fascia is healthy:
The viscoelastic gel flows without restriction in all directions.
The collagen fiber network moves freely.
Lymph and blood circulation flow correctly.
Communication between cells, the nervous system, and all tissues in the body work correctly.
In the event of an injury and activation of the healing process, specific components interact with cells to create the condition for healing and generate inflammation, allowing new cells to easily move and heal the tissue. An obstruction in the circulation increases pressure where the fluid sits stationary, preventing tissue communication. Sometimes the healing process doesn’t stop, and the inflammation response worsens and can become chronic.
Sugar Consumption
Many think of sugar as candy, sweets, chocolates, and desserts. However, all carbohydrates are sugar, and eating too much bread, pasta, grains, fruit, and cereals, contributes to a lot more sugar consumption.
Foods believed to be healthy such as wholemeal bread, low-fat alternatives, and granola cereal, have high amounts of sugar.
The connective tissues need collagen for the smooth functioning of joints.
High blood sugar exacerbates aches and pains and can lead to impaired joint movement and, eventually, arthritis.
Fascia Problems
Impaired flow and mobility
Fascia that has thickened and hardened impairs gliding ability.
In places where the body has become stiff and numb, the nervous system can’t transmit signals as quickly to control movements.
Muscles can constantly twitch or go into convulsions from misinterpreted signals.
A tight connective tissue chain can distort the skeleton causing the joints to wear faster.
Chiropractic Myofascial Massage Release
Chiropractic myofascial massage and release provides several benefits to the body’s health and well-being, including:
Relieves the overall effects of stress on the body.
Relieves soreness and pain.
Increases blood and lymph circulation.
Improves tissue recovery.
Improves joint range of motion.
Restores proper-length-tension relationships for dynamic movement.
Maintains normal functional muscular length.
Improves neuromuscular function.
Nutritional Guidelines Fascial Health
References
Barros-Neto, João Araújo et al. “Selenium and Zinc Status in Chronic Myofascial Pain: Serum and Erythrocyte Concentrations and Food Intake.” PloS one vol. 11,10 e0164302. 18 Oct. 2016, doi:10.1371/journal.pone.0164302
Dong, Shoubin, et al. “A three-dimensional collagen-fiber network model of the extracellular matrix for the simulation of the mechanical behaviors and microstructures.” Computer methods in biomechanics and biomedical engineering vol. 20,9 (2017): 991-1003. doi:10.1080/10255842.2017.1321113
Mattei, Giorgio et al. “Engineering Gels with Time-Evolving Viscoelasticity.” Materials (Basel, Switzerland) vol. 13,2 438. 16 Jan. 2020, doi:10.3390/ma13020438
Okumus, M et al. “The relationship between serum trace elements, vitamin B12, folic acid and clinical parameters in patients with myofascial pain syndrome.” Journal of back and musculoskeletal rehabilitation vol. 23,4 (2010): 187-91. doi:10.3233/BMR-2010-0264
Vlassara, Helen, and Jaime Uribarri. “Advanced glycation end products (AGE) and diabetes: cause, effect, or both?.” Current diabetes reports vol. 14,1 (2014): 453. doi:10.1007/s11892-013-0453-1
It is difficult for individuals to achieve health and fitness goals when they don’t like to eat vegetables. Intermittent fasting, Paleo, vegan, Mediterranean, or New Nordic, almost all healthy nutrition plans require vegetable consumption to achieve optimal health. However, it is never too late to learn to enjoy vegetables. Injury Medical Chiropractic and Functional Medicine Clinic can recommend ways not just to eat vegetables because they are healthy but to truly enjoy them.
Training Oneself To Enjoy Vegetables
Everyone’s taste preferences are different.
Many individuals grew up in homes where vegetables were prepared in unappetizing ways.
Over boiling and steaming are common preparation methods that many had experience with, including broccoli, cauliflower, asparagus, and Brussels sprouts, which made them flavorless, mushy and is where many decided they were not going to eat these foods.
Vegetables are full of nutrients that are very beneficial to the body.
Vegetables contain antioxidants, vitamins, minerals, fiber, and phytonutrients.
These nutrients help keep the mind and body healthy and avoid deficiencies.
Vegetables add fiber that provides a feeling of fullness by giving volume to fill the stomach without added calories.
This controls energy balance/calories in vs. calories out, which helps shed body fat without feeling hungry and maintain body weight.
Vegetables feed the intestinal bacteria that help the digestive tract.
Vegetables provide hydration that helps the fiber eliminate waste products.
Vegetables add variety to help maintain healthy nutrition.
Branching Out
The key is to branch out incrementally. Most individuals will have a vegetable or two that they can tolerate. This could be a starting point by expanding on new variations on those tolerable vegetables that will lead to broadened taste preferences. This can be done through different cooking methods that include:
Regardless of where you’re starting, there are simple ways to make the vegetable bitterness less intense, more palatable, and more enjoyable that consists of:
Vegetable Challenge
Vegetable Complement
Vegetable Cushion
Vegetable Challenge
Pick a vegetable that you would not normally eat that requires effort to try.
Motivate yourself to try it – health reasons, children, family, friends, etc.
Take a small bite; you may hate it, like it, or it has no effect.
You at least tried it.
Research suggests that individuals may need to try new foods many times (prepared differently) before tolerating or liking them.
It means pairing food with a vegetable to activate various tastes and flavors pleasing to the palate simultaneously.
Vegetable Cushion
On the tongue are a variety of receptors that bind to the chemicals in food.
When these receptors are activated, they send a chemical signal to the brain about the taste.
Variations in the number and type of receptors help develop flavor preferences.
Basic tastes – sweet, sour, spicy, salty, bitter, and umami.
Pairingbitterness with other distinct flavors, like sweet and spicy, can develop and change the brain’s perception of bland or bitter vegetables to tasty and delicious.
Cushions for bitterness include honey, real maple syrup, sour cream, Mexican crema, hot sauce, oils, almonds, and butter used in balance to enhance and bring out flavors.
The objective is to start small and work your way to becoming more comfortable with experimenting and combining more flavors. Consultation with a professional nutritionist can help individuals get on a healthy nutrition plan that they can enjoy.
Tip From A Dietitian
References
Christoph, Mary J et al. “Intuitive Eating is Associated With Higher Fruit and Vegetable Intake Among Adults.” Journal of nutrition education and behavior vol. 53,3 (2021): 240-245. doi:10.1016/j.jneb.2020.11.015
Melis M, Yousaf NY, Mattes MZ, Cabras T, Messana I, Crnjar R, Tomassini Barbarossa I, Tepper BJ. Sensory perception of salivary protein response to astringency as a function of the 6-n-propylthioural (PROP) bitter-taste phenotype. Physiol Behav. 2017 Jan 24;173:163-173.
Mennella JA. Development of food preferences: Lessons learned from longitudinal and experimental studies. Food Qual Prefer. 2006 Oct;17(7-8):635-637.
Tordoff, Michael G, and Mari A Sandell. “Vegetable bitterness is related to calcium content.” Appetite vol. 52,2 (2009): 498-504. doi:10.1016/j.appet.2009.01.002
Wallace, Taylor C et al. “Fruits, vegetables, and health: A comprehensive narrative, umbrella review of the science and recommendations for enhanced public policy to improve intake.” Critical reviews in food science and nutrition vol. 60,13 (2020): 2174-2211. doi:10.1080/10408398.2019.1632258
Wieczorek, Martyna N et al. “Bitter taste of Brassica vegetables: The role of genetic factors, receptors, isothiocyanates, glucosinolates, and flavor context.” Critical reviews in food science and nutrition vol. 58,18 (2018): 3130-3140. doi:10.1080/10408398.2017.1353478
Workout recovery is as important as working out. Pushing muscle past its normal levels creates tiny tears in the muscle tissue. It is the repairing process that generates muscle growth. Muscles that aren’t allowed to recover will not grow or gain muscle mass, and muscle strength could be reduced, making working out a struggle and hindering health goal progress. The body needs time to repair the muscles to reduce the risk of injury. Allowing enough time for recovery reduces overuse-related muscle breakdown and injuries. Muscle recovery supplements can expedite the healing process.
Muscle Recovery Supplements
Reasons for taking supplements include their ability to heal damaged muscles faster, aid in injury recovery, reduce muscle soreness, reduce muscle fatigue, and provide the muscle cells with energy during recovery.
Some studies have found that taking a creatine supplement may aid muscle recovery and greater muscle strength during recovery.
Citrulline Malate
Citrulline is a non-essential amino acid found in watermelon that converts into nitric oxide.
Nitric oxide helps open blood vessels and improve blood circulation.
This allows oxygen and nutrients to reach the muscle faster, speeding the recovery process.
Citrulline also improves the bioavailability of L-arginine, another amino acid that aids protein synthesis.
Magnesium
Magnesium assists with muscle recovery by helping the muscles relax.
When the body doesn’t have enough magnesium, there is a greater chance of muscle cramps.
Magnesium helps support healthy muscle contraction.
Tart Cherry Juice Extract
This extract works by reducing inflammation in the muscle.
Inflammation is normal, but too much can increase muscle soreness and the risk of injury.
One study found that cherry juice helps minimize post-exercise muscle pain.
Supplement Plan
After selecting a supplement plan that is the most beneficial for the individual, the next step is to devise a schedule for taking them.
When using a muscle recovery supplement can either be a pre-workout supplement or a post-workout supplement.
The recommended time to take a specific supplement is based on the type.
Individuals should talk with their doctor and a nutritionist before starting any new supplement regimen.
This helps ensure the supplements are safe and minimize negative side effects given health and medical conditions.
Nutrition In Recovery
References
Cooke, M.B., Rybalka, E., Williams, A.D. et al. Creatine supplementation enhances muscle force recovery after eccentrically-induced muscle damage in healthy individuals. J Int Soc Sports Nutr 6, 13 (2009). https://doi.org/10.1186/1550-2783-6-13
DiNicolantonio, James J et al. “Subclinical magnesium deficiency: a principal driver of cardiovascular disease and a public health crisis.” Open heart vol. 5,1 e000668. 13 Jan. 2018, doi:10.1136/openhrt-2017-000668
Gough, Lewis A et al. “A critical review of citrulline malate supplementation and exercise performance.” European journal of applied physiology vol. 121,12 (2021): 3283-3295. doi:10.1007/s00421-021-04774-6
Kuehl, Kerry S et al. “Efficacy of tart cherry juice in reducing muscle pain during running: a randomized controlled trial.” Journal of the International Society of Sports Nutrition vol. 7 17. 7 May. 2010, doi:10.1186/1550-2783-7-17
Vitale, Kenneth C et al. “Tart Cherry Juice in Athletes: A Literature Review and Commentary.” Current sports medicine reports vol. 16,4 (2017): 230-239. doi:10.1249/JSR.0000000000000385
Weinert, Dan J. “Nutrition and muscle protein synthesis: a descriptive review.” The Journal of the Canadian Chiropractic Association vol. 53,3 (2009): 186-93.
Wolfe, Robert R. “Branched-chain amino acids and muscle protein synthesis in humans: myth or reality?.” Journal of the International Society of Sports Nutrition vol. 14 30. 22 Aug. 2017, doi:10.1186/s12970-017-0184-9
Zhang, Shihai, et al. “Novel metabolic and physiological functions of branched-chain amino acids: a review.” Journal of animal science and biotechnology vol. 8 10. 23 Jan. 2017, doi:10.1186/s40104-016-0139-z
Sugar is a highly addictive carbohydrate linked to obesity, diabetes, metabolic disorders, and mood disorders. Individuals ready to phase out sugar will improve overall health, regardless of age and health status, but the transition can be challenging. A sugar-free or low-sugar diet can help individuals with blood sugar or systemic inflammation, including pre-diabetes, diabetes, heart disease, PCOS, hormonal imbalances, and autoimmune diseases.
Phase Out Sugar
Low-Sugar Diet
A low-sugar nutrition plan focuses on maintaining a low overall sugarintake that limits sugar to avoid blood sugar instability and general inflammation.
This means choosing food with natural sugars like fruit, certain dairy products, vegetables, and natural sugars.
Reducing and replacing packaged or prepared foods with added sugars, like store-bought tomato sauce, cured meats, or frozen meals.
Reducing and replacing processed foods like snack items and fast food.
Reducing restaurant food that can add sugar for flavor and appetite stimulation.
Recommended Ways
Consult a healthcare provider, dietician, or nutritionist before altering diet, physical activity, or supplement routine.
Eat More Healthy Fat
Healthy fat is more satisfying, making the body feel fuller for longer.
Not getting enough sleep negatively impacts the appetite-regulating hormones leptin and ghrelin, causing cravings for instant energy that typically comes from sugar snack products.
Individuals are recommended to get at least 7-9 hours per night. Enough sleep will balance the appetite hormones and decrease sugar cravings.
Manage Stress to Control Emotional Eating
Emotional eating is common when stressed out. Finding something to take the mind off sugar cravings is necessary when having a stressful day. This includes:
If sugar cravings are more serious, then professional help is recommended.
Drink More Water
When school, work, and life is happening, individuals can think they’re hungry; however, it is not hunger but the body needing hydration.
Drink one to two glasses of water when cravings kick in to satisfy the craving.
Drinking water throughout the day helps keep cravings down and helps with sugar withdrawal symptoms.
Individuals who have difficulty drinking water should add slices of fruit, cucumber, or mint to make it more pleasing.
Try sparkling mineral water or naturally flavored carbonated waters.
Try healthy juices, like celery, beet, or carrot juice, instead of water.
Sugar-Free Substitutes
Sugar substitutes are available, but not all are considered healthy.
Individuals should be cautious about using sugar-free alternatives to phase out sugar.
A study found that zero-calorie sweeteners such as aspartame and sucralose were actually found to increase, not decrease, weight.
Stevia and monk fruit extract has been shown to be safe and has no negative side effects.
Consult a dietician or nutritionist to determine the healthiest for you.
What Happens To The Body
References
Azad, Meghan B et al. “Nonnutritive sweeteners and cardiometabolic health: a systematic review and meta-analysis of randomized controlled trials and prospective cohort studies.” CMAJ : Canadian Medical Association journal = journal de l’Association medicale canadienne vol. 189,28 (2017): E929-E939. doi:10.1503/cmaj.161390
Bayon, Virginie et al. “Sleep debt and obesity.” Annals of medicine vol. 46,5 (2014): 264-72. doi:10.3109/07853890.2014.931103
DiNicolantonio, James J et al. “Sugar addiction: is it real? A narrative review.” British journal of sports medicine vol. 52,14 (2018): 910-913. doi:10.1136/bjsports-2017-097971
Franklin, Jane L et al. “Extended exposure to sugar and/or caffeine produces distinct behavioral and neurochemical profiles in the orbitofrontal cortex of rats: Implications for neural function.” Proteomics vol. 16,22 (2016): 2894-2910. doi:10.1002/pmic.201600032
Freeman, Clara R et al. “Impact of sugar on the body, brain, and behavior.” Frontiers in bioscience (Landmark edition) vol. 23,12 2255-2266. 1 Jun. 2018, doi:10.2741/4704
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine






 Myofascial Tissue
Myofascial Tissue