Can individuals dealing with pain and inflammation in their bodies can incorporate a ketogenic diet and have beneficial results?
Introduction
When it comes to a person’s health and wellness journey, many people often wonder where to start making changes in their bodies. Many people begin exercising not only to reduce stress levels in the musculoskeletal system but also to help clear their minds. This is a great cause, as any form of physical activity can help reduce muscle fatigue and weakness and strengthen the extremities and quadrants in the musculoskeletal system. However, even though exercising is part of the health and wellness journey, another component plays a crucial part in the health and wellness journey: eating nutritional foods and dieting. Now, dieting can be scary for some newcomers who are just entering their health and wellness journey, but when people start making small changes to their eating habits, like incorporating more vegetables and fruits in their meals, making more meals at home, and doing portion control to eat enough till they are full can provide beneficial results. These small changes can empower individuals to take control of their health and wellness journey. Dieting and changing eating habits can give useful results for people dealing with chronic issues correlated with environmental factors. In today’s article, we will look at a particular diet known as the ketogenic diet, its beneficial properties, and how to incorporate it to reduce chronic conditions affecting the body. We talk with certified associated medical providers who provide our patients’ information to assess how incorporating the ketogenic diet can help reduce chronic conditions. We also inform patients while asking their associated medical provider intricate questions to formulate customized treatment plans to help with chronic conditions by incorporating the ketogenic diet along with physical activities. Dr. Alex Jimenez, D.C., includes this information as an academic service. Disclaimer.
What Is the Ketogenic Diet?
Do you often feel extremely thirsty throughout the day, and do you chug at least a couple of gallons of water daily? Do you feel heat or see redness in various locations around your body that seem tender when touched? Or do your joints become stiff in the mornings when you wake up and feel better throughout the entire day? Often, people have a love-hate relationship with food. However, it all depends on what the person is eating and what environmental factors correlate with their food. So, when a person has chronic conditions that cause pain and inflammation in their joints, muscles, and organs, the negative side effects are that the food they consume can induce the inflammatory effects. In contrast, the positive impact of food can help individuals dampen the pain and inflammation in the body. (Fifi & Holton, 2020) Many individuals dealing with inflammation and pain in their bodies can incorporate a ketogenic diet to reduce the inflammatory effects.
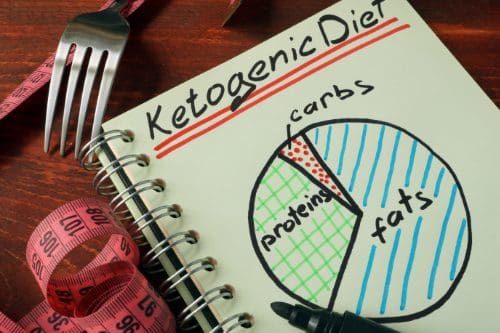
Now, what is the ketogenic diet? The ketogenic diet is where carbohydrates are low, and various levels of lean proteins and healthy fats induce ketosis. (McGaugh & Barthel, 2022) This, in turn, helps with alternating the metabolic pathways to induce weight loss, improve health conditions like lipid profile improvements, and reduce hyperglycemia. When environmental factors like obesity, sedentary lifestyles, or physical inactivity can cause chronic issues like lipedema, the body will cause overlapping risk profiles to induce inflammation. When the body is dealing with lipedema, it can cause the body to be in a constant inflammatory state that induces cell damage and cell death through apoptosis. Hence, when a person is going to do a ketogenic diet, it can help reduce the inflammatory effects while alleviating pain symptoms. (Verde et al., 2023)
Eating Right To Feel Better-Video
The Beneficial Properties Of A Ketogenic Diet
One of the beneficial properties that a person can take with a ketogenic diet is that it can help reduce cardiovascular diseases with its anti-inflammatory properties. Since a ketogenic diet helps place the body in a state of nutritional ketosis, incorporating omega-3 fatty acids can help the body exert systemic anti-inflammatory effects and begin healing. (Dynka et al., 2023) At the same time, the ketogenic diet can help individuals who are suffering from chronic conditions like epilepsy, diabetes, or obesity to not only induce weight loss but also help improve body composition. (Sjodin et al., 2020) This is because when individuals get a customized treatment plan incorporating the ketogenic diet, it must include physical activities that help strengthen muscles in the body’s quadrants. In contrast, the ketogenic diet helps slow down muscle glycogen depletion. Additionally, the ketogenic diet is beneficial by:
Reducing glucose levels so individuals with diabetes don’t need insulin.
When it comes to the ketogenic diet, many individuals have dealt with chronic conditions like epilepsy, diabetes, or cardiovascular conditions. Understand that incorporating a healthy diet filled with healthy fats, lean protein, plenty of fruits and vegetables, and physical activity can benefit many individuals in the long run. The ketogenic diet can help the liver by producing more ketone bodies to help with the production of ATPs and reduce ROS (reactive oxygen species); this, in turn, helps improve a person’s quality of life. (Abboud et al., 2021) Informing individuals who are dealing with chronic conditions that they must make small changes to their routines. This can be incorporated into their customized treatment plan and help reduce the pain-like effects from the person’s chronic conditions correlating to the inflammatory effects. The ketogenic diet can be a stepping stone to a person’s health and wellness and help them be motivated to see positive results.
References
Abboud, M., AlAnouti, F., Georgaki, E., & Papandreou, D. (2021). Effect of Ketogenic Diet on Quality of Life in Adults with Chronic Disease: A Systematic Review of Randomized Controlled Trials. Nutrients, 13(12). https://doi.org/10.3390/nu13124463
Dowis, K., & Banga, S. (2021). The Potential Health Benefits of the Ketogenic Diet: A Narrative Review. Nutrients, 13(5), 1654. https://doi.org/10.3390/nu13051654
Dynka, D., Kowalcze, K., Charuta, A., & Paziewska, A. (2023). The Ketogenic Diet and Cardiovascular Diseases. Nutrients, 15(15). https://doi.org/10.3390/nu15153368
Sjodin, A., Hellstrom, F., Sehlstedt, E., Svensson, M., & Buren, J. (2020). Effects of a Ketogenic Diet on Muscle Fatigue in Healthy, Young, Normal-Weight Women: A Randomized Controlled Feeding Trial. Nutrients, 12(4). https://doi.org/10.3390/nu12040955
Verde, L., Camajani, E., Annunziata, G., Sojat, A., Marina, L. V., Colao, A., Caprio, M., Muscogiuri, G., & Barrea, L. (2023). Ketogenic Diet: A Nutritional Therapeutic Tool for Lipedema? Curr Obes Rep, 12(4), 529-543. https://doi.org/10.1007/s13679-023-00536-x
Can individuals support their parasympathetic nervous system to maintain a relaxed state and avoid excessive agitation, stress, anxiety, and dysregulation?
Parasympathetic Nervous System
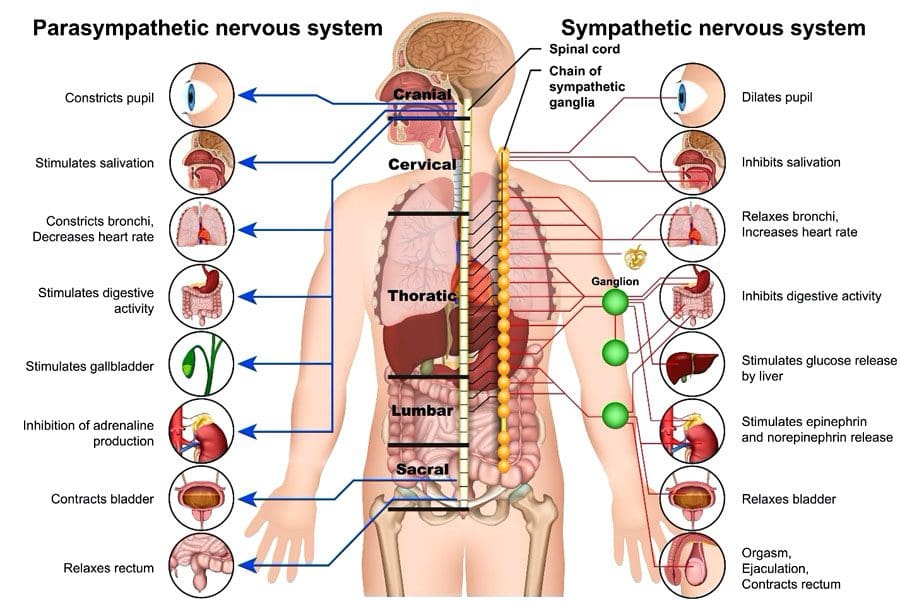
The parasympathetic nervous system (PSNS) involves organs and cells that release neurotransmitters that help the body maintain essential functions like heart rate, breathing, digestion, relaxation, thinking, and sleep. It is part of the autonomic nervous system, which includes the nerves and neurotransmitters that control the body’s internal organs to maintain reliable function. The autonomic nervous system regulates a continual balance between the parasympathetic nervous system’s rest-and-digest functions and the sympathetic nervous system’s fight-or-flight responses.
Functions and Responses
The parasympathetic nervous system includes nerves and neurotransmitters (chemical messengers) distributed throughout the body and is often described as promoting the body’s rest-and-digest state. The body’s needs regulate the control and effects of the system. Certain medications and health issues can modify or alter the function of the autonomic nervous system, including sympathetic and parasympathetic areas. The parasympathetic and sympathetic nervous systems collaborate to control cells, tissues, and organs. The body requires constant functioning and adjustment of both systems. (McQuade J. D. et al., 2017) Functions include: (Valenti V. E. et al., 2024)
Saliva secretion to break down food.
Maintaining blood pressure, resting heart, and breathing rate.
Producing enzymes in the stomach and intestines to break down food further and absorb nutrients.
Kidney balancing of fluid and mineral levels by producing urine.
Constricting pupils (making the dark circle in the eye smaller) to see details up close.
Maintaining focus and concentration to think, remember, and make decisions.
Releasing hormones to fall asleep and stay asleep.
Providing consistent muscle stimulation to maintain endurance for muscle activity.
All functions are adjusted based on the body’s needs.
Activation
The parasympathetic response constantly works to keep the body active, engaged, and healthy and can be stimulated simply by relaxing and resting. Individuals can sometimes focus on promoting their body’s parasympathetic activity through stretching, slow movements, relaxing sounds or music, meditation, and similar activities. Individuals who frequently feel anxious or stressed and have difficulty relaxing could benefit from guidance from a therapist or coach on learning to engage the parasympathetic nervous system. (Goren O. et al., 2024) This can involve activities such as guided meditation or talk therapy, which can help individuals work through fears and anxieties.
Dysregulation
Some medical conditions are associated with dysregulation. Heart disease, respiratory disease, sleep disorders, mental health conditions, and behavioral conditions can be associated with overactive or underactive parasympathetic or sympathetic nervous system regulation. (Veerakumar A. et al., 2022) Various mental health and physical health disorders can involve symptom fluctuations that affect the autonomic nervous system. For example, anxiety disorders can cause periods of overeating as well as loss of appetite and episodic indigestion, nausea, and vomiting. Symptoms of dysregulation can include: (McQuade J. D. et al., 2017)
Excessive sleepiness
Insomnia
Difficulty concentrating
Confusion
Anxiety – nervousness or agitation
A feeling of a rapid heart rate
Shortness of breath
Dry mouth
Throat tightness
Indigestion
Stomachaches
Nausea
Vomiting
Cold hands and feet
Sweating or clammy hands
Sadness
Depression
Dizziness or feeling physically off-balance
Any of these symptoms can develop and resolve quickly. Most individuals experience symptoms or parasympathetic nervous system dysfunction when an unexpected stressful event occurs, and the response is considered normal in traumatic, shocking, sad, or high-stress circumstances. (Veerakumar A. et al., 2022)
Medications may induce parasympathetic overactivity or underactivity until the medicine is broken down and removed from the body. (Valenti V. E. et al., 2024)
Nerves
The system comprises nerves that release hormones and neurotransmitters and nerves that respond to the hormones and neurotransmitters. Parasympathetic activation and response include: (Valenti V. E. et al., 2024)
The nerves that activate the parasympathetic nervous system run throughout the body, primarily in the brain, heart, lungs, stomach, and intestines.
The brain, heart, lungs, stomach, intestines, muscles, liver, kidneys, reproductive organs, eyes, and mouth are among the areas of the body that respond to stimulation.
The vagus nerve, one of the cranial nerves, is closely associated with parasympathetic nervous system activity. It runs from the brainstem down into the throat, heart, lungs, and digestive system. (Valenti V. E. et al., 2024) Surgical, medical, and alternative interventions are used to regulate the activity of the parasympathetic nervous system and are targeted toward regulating and controlling the activity of the vagus nerve. (Hernández-Domínguez R. A. et al., 2024)
PSNS Support
Living with any parasympathetic nervous system dysfunction can be challenging. For individuals with heart or lung disease, healthcare providers will evaluate the medical condition and recommend surgery or medication to control symptoms and avoid complications. (Hernández-Domínguez R. A. et al., 2024) Individuals who are living with a mental health disorder or behavioral disorder that is associated with any dysregulation of the parasympathetic nervous system activity may benefit from a combination of behavioral interventions and medication to help control symptoms long term. (Goren O. et al., 2024)
Injury Medical Chiropractic and Functional Medicine Clinic
The spinal cord has multiple functions in restoring, rejuvenating, and strengthening the nervous system. Chiropractic care has a highly responsive therapeutic effect on the nervous system because of its focus on the spine. Spinal decompression, traction, soft tissue manipulation, and other treatments help regulate and restore the function of the nervous system. Chiropractic benefits:
Reduce and/or eliminate pain.
Improves the quality of sleep.
Increases energy.
Improves cognition and clarity.
Reduces or eliminates headaches and migraines.
Improves digestive function.
Improves balance and coordination.
Increases flexibility and mobility.
Regulates respiration.
Regulates lower heart rate.
At Injury Medical Chiropractic and Functional Medicine Clinic, our areas of practice include Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Wellness & Nutrition, Functional Medicine Treatments, and in-scope care protocols. We focus on what works for every patient to restore function. If other treatment is needed, individuals will be referred to a clinic or physician best suited to their injury, condition, or ailment.
Chiropractic Secrets Exposed
References
McQuade, J. D., Penzel, T. E., Silk, J. S., & Lee, K. H. (2017). Parasympathetic Nervous System Reactivity Moderates Associations Between Children’s Executive Functioning and Social and Academic Competence. Journal of abnormal child psychology, 45(7), 1355–1367. https://doi.org/10.1007/s10802-016-0246-5
Valenti, V. E., Vanderlei, L. C. M., & Godoy, M. F. (2024). Editorial: Understanding the role of the autonomic nervous system in health and disease. Frontiers in neuroscience, 18, 1446832. https://doi.org/10.3389/fnins.2024.1446832
Goren, O., Paz, A., Bar-Kalifa, E., Gilboa-Schectman, E., Wolff, M., & Atzil-Slonim, D. (2024). Clients’ and therapists’ parasympathetic interpersonal and intrapersonal regulation dynamics during psychotherapy for depression. Psychotherapy research : journal of the Society for Psychotherapy Research, 1–15. Advance online publication. https://doi.org/10.1080/10503307.2024.2378038
Veerakumar, A., Yung, A. R., Liu, Y., & Krasnow, M. A. (2022). Molecularly defined circuits for cardiovascular and cardiopulmonary control. Nature, 606(7915), 739–746. https://doi.org/10.1038/s41586-022-04760-8
Hernández-Domínguez, R. A., Herrera-Orozco, J. F., Salazar-Calderón, G. E., Chávez-Canales, M., Márquez, M. F., González-Álvarez, F., Totomoch-Serra, A., Reyes-Cruz, T., Lip, F., & Aceves-Buendía, J. J. (2024). Optogenetic modulation of cardiac autonomic nervous system. Autonomic neuroscience : basic & clinical, 255, 103199. https://doi.org/10.1016/j.autneu.2024.103199
Can healthcare professionals implement H.E.A.R.T. protocols for trafficked individuals while providing a safe space?
Introduction
Across the world, many local media and organizations are paying close attention to a phenomenon that many people should be aware of. This phenomenon is known as trafficking, and it can be associated with numerous activities, from forced labor to sex labor, and can affect a person’s sense of self-worth. While many people will correlate that trafficking affects many women and children, it can affect many individuals regardless of age, gender, and background. While many survivors of trafficking are dealing with the psychological and physical injuries that they obtain from their traffickers, many medical professionals can implement protocols and roles through the implementation of H.E.A.R.T. to provide a safe space for individuals suffering from trafficking. Today’s article focuses on the definition of trafficking, what H.E.A.R.T. is, and how it is used in a clinical setting. We discuss with certified associated medical providers who consolidate our patients’ information to assess and identify trafficking in a clinical approach while providing a safe space. We also inform and guide patients while asking their associated medical provider intricate questions to formulate customized treatment plans for their pain and provide them with a safe space and positive experience. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
The Definition Of Trafficking
When it comes to defining trafficking, it can be challenging as it is frequently associated with other issues. However, the main definition for trafficking is “recruiting, transporting, transferring, or harboring many individuals or a person that are threatened or forced to achieve the consent of a person having control of the individuals for exploitation.” With human trafficking being a pressing public concern that affects all races, social classes, demographics, and genders, it can impact society and the individual who is being trafficked. (Toney-Butler et al., 2024) Additionally, many people often mistake trafficking and smuggling as they are completely different. Smuggling requires a person to be transported into a nation through voluntary illicit means. While trafficking can come in two forms, which are labor and commercial sex, it can happen within the person’s own home. (Rambhatla et al., 2021) This is because many survivors who are going to get healthcare services will feel various emotions of fear or shame that can prevent them from asking for help due to what they have been through with their trafficker. However, when many individuals who are trafficking survivors are suffering from significant physical, mental, and social health problems and are seeking healthcare services, many healthcare professionals play an important role by creating a safe and responsive space for them. (The Lancet Regional Health-Western, 2022)
Beyond the Surface: Understanding the Effects of Personal Injury- Video
What is H.E.A.R.T In A Clinical Setting
When it comes to creating a safe and positive space in a clinical setting, many healthcare professionals often miss the signs of trafficking due to a lack of training or confidence to identify and treat patients who are trafficking victims. (Lee et al., 2021) However, healthcare protocols should be implemented, and H.E.A.R.T. should be incorporated into a clinical approach to assess and develop a customized treatment plan for the patient. Healthcare professionals can engage with the patient in a one-on-one discussion away from their trafficker and can offer important medical and psychological care resources. (Exeni McAmis et al., 2022) By incorporating H.E.A.R.T. protocols in a healthcare clinic, many doctors and medical professionals can help many patients be in a safe environment. Below is what H.E.A.R.T. stands for.
H-Hearing
The “H” in H.E.A.R.T. is for hearing as many medical professionals not only to hear but to see what is going on in the clinic and to establish environmental awareness. This is due to looking at the patient and who is accompanied by them. With healthcare providers being at the front, they interact with patients and may not know what health concerns are affecting them. This could be due to the following:
By incorporating the hearing aspect in H.E.A.R.T., many healthcare professionals can provide a safe, thoughtful, and engaging approach to the patient and know what to look for when a patient is coming in for treatment.
E-Evaluating
The “E“ in H.E.A.R.T. is used to evaluate its importance in enhancing patient interactions in a trauma-informed care facility. This is highly important because the individual is seeking health care. For the patients being trafficked, it is important to notice the red flags the individual is experiencing. Some of the red flags that many healthcare providers should look for are:
Physical health
Behavioral Health
The patient is with a controlling person
The patient does not have possession of their I.D.
Additionally, it is always important to show compassion, be sensitive to the individual while addressing their needs and concerns, and use a non-judgmental approach during the interview process. This helps the individual ensure they are in a safe environment when discussing sensitive topics. At the same time, it is important not to let the patient be re-traumatized while avoiding the impulse to rescue and overpromise the patient to mental health as we want them to have their self-worth. At the same time, it is best to remember the four “Rs“ when doing a trauma-informed approach; they are:
Realize: Understanding how trauma can affect people.
Recognize: Recognizing the signs of trauma.
Respond: Have all staff trained, use evidence-based practices, and provide a safe environment.
Resist Re-trauma: Recognizing how some practices may trigger painful memories while avoiding re-traumatizing the patient.
By implementing the four “Rs“ and the “E“ in H.E.A.R.T., many healthcare professionals can provide valuable resources to trafficking survivors with a strong support system.
A-Activating
The “A“ in H.E.A.R.T. stands for activating, where healthcare professionals must have proper protocols to engage all employees. This allows the healthcare providers to understand how beneficial it is to develop a protocol for a person who is being trafficked, understand their state and federal reporting laws, and list key elements of effective trauma-informed screening procedures when assessing the patient. This allows a foundational structure to support a response for suspected patients who are being trafficked. At the same time, by following HIPAA laws and organization policies, many healthcare providers must explain the reporting process to the right officials. Additionally, the benefits of developing a protocol for trafficking are by:
Clarifying procedures
Enhance staff training
Optimize the interactions with the trafficking patients
Improve staff confidence
Prepare for any threatening situations
Maximizing preparedness to aid trafficking patients
Optimize support for patients
Develop collaborative outside resources
R-Resourcing
The “R“ in H.E.A.R.T. stands for resourcing, as many healthcare providers must identify the referral systems. This allows healthcare professionals to understand the important message to convey when assessing trafficking victims and the importance of responding to safety, emergency, and reporting requirements. When assessing and interviewing the patient, many will have to recognize that their patient may be a possible victim of trafficking, what their immediate needs are, and what long-term resources can help.
T-Training
The “T” in H.E.A.R.T. stands for training, as it is important that many healthcare providers continuously train to spot trafficking; this provides confidence to many healthcare workers and can help save a person’s life. By implementing H.E.A.R.T. protocols, the “T” allows the doctor to respect the individual’s decision to want help, providing a positive support system while encouraging them to come back, offering to help with a safety plan, and building a resource network. This is because if the patient is accompanied by someone who is controlling and answering for the patient, handing out information discreetly can provide a bit of hope to the individual to make the move. At the same time, providing local and immediate assistance resources can help the individual in the long run. This allows healthcare providers to build a trusting relationship and even help individuals to have a safe and positive experience on their health and wellness journey.
References
Exeni McAmis, N. E., Mirabella, A. C., McCarthy, E. M., Cama, C. A., Fogarasi, M. C., Thomas, L. A., Feinn, R. S., & Rivera-Godreau, I. (2022). Assessing healthcare provider knowledge of human trafficking. PLOS ONE, 17(3), e0264338. https://doi.org/10.1371/journal.pone.0264338
Gutfraind, A., Yagci Sokat, K., Muscioni, G., Alahmadi, S., Hudlow, J., Hershow, R., & Norgeot, B. (2023). Victims of human trafficking and exploitation in the healthcare system: a retrospective study using a large multi-state dataset and ICD-10 codes. Front Public Health, 11, 1243413. https://doi.org/10.3389/fpubh.2023.1243413
Lee, H., Geynisman-Tan, J., Hofer, S., Anderson, E., Caravan, S., & Titchen, K. (2021). The Impact of Human Trafficking Training on Healthcare Professionals’ Knowledge and Attitudes. J Med Educ Curric Dev, 8, 23821205211016523. https://doi.org/10.1177/23821205211016523
Rambhatla, R., Jamgochian, M., Ricco, C., Shah, R., Ghani, H., Silence, C., Rao, B., & Kourosh, A. S. (2021). Identification of skin signs in human-trafficking survivors. Int J Womens Dermatol, 7(5Part B), 677-682. https://doi.org/10.1016/j.ijwd.2021.09.011
Individuals getting into fitness may wonder whether they should join a gym or exercise at home. Is there an advantage to one versus the other?
Gym or Home
Exercising, whether at the gym or at home, depends on individual preference and budget. The first step is committing to a fitness health plan. Where to work out depends on the individual and their characteristics. For those who are self-motivated and will exercise no matter what, a home workout may be the best option. (Essery R. et al., 2017) Going to a gym may be a better choice for those who find too many distractions at home and other things to do besides the workout, like laundry, checking the phone, cleaning, etc. Working out at home is convenient; it takes driving out of the equation, changing into gym clothes, and going at the right time. However, the gym provides fewer distractions, community access, equipment like weights and cardiovascular machines, and group fitness classes. Each has pros and cons.
Pros and Cons – The Gym
Pros
Gym features and resources
Motivation
Focus
Classes
Community
Cons
Membership fees
Inconvenience
Too many people
Pros of a Gym
Features and Resources
Exercise can be so much easier when there are plenty of options.
There are various machines, such as treadmills, ellipticals, stair climbers, stationary bikes, and rowing machines.
Weights and machines, free weights, cable machines, bands, and more.
Motivation
Paying for a membership can be a motivating factor to regularly working out.
There is a friendly, competitive vibe with the other members who can help motivate each other.
Focus
Exercising at the gym can help maintain focus on fitness goals.
No chores, kids, or distractions to break off from the workouts.
Classes
Working out in a class can increase motivation and make working out fun.
There are online classes for working out at home, but it’s not the same as going to the gym and being around people.
Other features like a swimming pool, hot tub, tennis courts, etc may be available.
Community
Working out with others can give a sense of community.
People draw energy from others, pushing us to work harder.
Cons of a Gym
Gym membership drawbacks.
Cost
Membership fees can cause stress.
Some high-end gyms charge more than $100 monthly, while smaller gyms may charge only $10.
Inconvenience
Going to the gym includes packing a bag, driving there, parking, and waiting for the machines, weights, etc.
Total time will be longer because of the drive time.
Too Many People
At times, the gym can be packed with people.
Sometimes, individuals talk too loudly on their phones, leave sweat on the machines, and do not put weights away.
These could be the days or nights to work out at the house.
At Home Workouts
Pros
Cost
Convenience
Mix workouts
Cons
Space
Excuses
Boredom
Pros at Home
For some, home workouts could be the better option, and the benefits include:
Cost
There’s no membership fee.
Individuals can do bodyweight workouts that require no equipment.
Develop a house gym with inexpensive resistance bands, a few weights, and an exercise ball.
Convenience
Individuals do not have to get their gym bag, drive, and arrange for child care.
Individuals can work out in pajamas or underwear.
Individuals can also work out whenever they like if they need to split their workouts or work out at a specific time.
Mix Workouts
Although gyms also mix things up, individuals can do it at home at their convenience.
Combining weights and cardio and finishing up with yoga.
Individuals can go outside, watch exercise videos, stream live classes, use fitness mirrors, play exercise games, or download workout apps.
There is also versatile home gym equipment.
Cons at Home
These can cause individuals to lose home workout motivation.
Space
Although not much space is needed to work out, wanting to use a treadmill or other large equipment might not be practical, which could lead to boredom.
Excuses
There can be endless excuses to skip a workout.
Individuals who are not self-motivated might avoid workouts with chores or other important home tasks.
Boredom
At a gym, there is energy potential that motivates individuals to move.
If there is not enough exercise variety at home, boredom can set in.
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic treats patients’ injuries and chronic pain syndromes. We focus on improving ability through flexibility, mobility, and agility programs tailored to the individual. We use in-person and virtual health coaching and comprehensive care plans to ensure every patient’s personalized care and wellness outcomes. Our providers use an integrated approach to create customized care plans that include Functional Medicine, Acupuncture, Electro-Acupuncture, and Sports Medicine principles. Our goal is to relieve pain naturally by restoring health and function to the body. Suppose he feels the individual needs other treatment. In that case, they will be referred to a clinic or physician best suited for them. Dr. Jimenez has teamed up with the top surgeons, clinical specialists, medical researchers, and premier rehabilitation providers to provide our community with the best clinical treatments.
The Right Way To Implement an Exercise Prescription
References
Essery, R., Geraghty, A. W., Kirby, S., & Yardley, L. (2017). Predictors of adherence to home-based physical therapies: a systematic review. Disability and rehabilitation, 39(6), 519–534. https://doi.org/10.3109/09638288.2016.1153160
Can electrolyte chewing gum help physically active individuals, fitness enthusiasts, and athletes experiencing extreme heat and dehydration?
Electrolyte Chewing Gum
Electrolyte powder mix and drinks have been marketed as efficient and time-saving for fast-paced lives. Now, electrolytes are in chewing gum form. These gums work by activating salivary glands and making the mouth water. Manufacturers claim the gum’s sour taste makes the mouth water, quenches thirst, and replenishes some electrolytes. Some brands don’t list the percentages or amounts of ingredients, making determining each gum’s electrolyte content difficult. However, electrolyte chewing gum is designed to eliminate feelings of thirst and is not meant to hydrate the body. This can be dangerous because it gives the individual a false sense of hydration. When the thirst mechanism is impaired, an individual may not drink enough fluids, leading to dehydration. The Food and Drug Administration has not studied the effectiveness of electrolyte gum.
Signs The Body Is Not Getting Enough Electrolytes
Electrolyte deficiency can result from insufficient fluids or excessive sweating (National Library of Medicine, 2024). Signs that the body is not getting enough electrolytes can vary because the body needs each electrolyte for specific functions. The symptoms can range from neurological symptoms such as headaches and seizures in the case of low sodium to muscle cramps and weakness when there are low potassium levels. (National Library of Medicine, 2023) (National Library of Medicine, 2023) However, individuals can still have electrolyte imbalances even if they do not have symptoms. This is why proper hydration and intake of electrolytes through water and food are important.
Ingredients
The ingredients listed on electrolyte chewing gum include:
Sugar
Gum base
Corn syrup
Citric acid
Glycerin
Natural flavors
Soy lecithin
Artificial sweeteners
Artificial color
Electrolytes in sodium citrate and potassium citrate
However, gum brands fail to include the percentages of the ingredients, making it hard to figure out the actual electrolyte content. The amount can determine their effectiveness. Given their size, estimates point to very little electrolyte content, possibly around 10 milligrams of sodium per piece, which is insufficient to hydrate the body.
Rehydrating the Body
Food and fluids are reliable sources of electrolytes that the body can absorb. Sources include:
Fruits like bananas and oranges contain potassium and magnesium.
Vegetables also contain potassium and magnesium.
Dairy for calcium.
Electrolyte supplements are generally unnecessary if you eat a balanced diet. However, these products could be useful during exercise, especially for their sodium content (National Library of Medicine, 2024). When exposed to the heat, consider a rehydration solution like sports drinks or making your own. The presence of sugar increases the absorption of sodium by the intestine. Sugar in electrolyte solutions does not add calories; it helps the intestine absorb the sodium faster and holds water in the bloodstream, helping maintain blood pressure. While chewing a piece of electrolyte gum might make it easy to get balanced electrolytes, it is not enough to replenish the body. Individuals who need more electrolytes should talk to their healthcare provider about the best way to meet their body’s needs. They may recommend drinks or powders specially formulated to provide an electrolyte boost.
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop highly effective treatment plans through an integrated approach for each patient and restore health and function to the body through nutrition and wellness, functional medicine, acupuncture, Electroacupuncture, and integrated medicine protocols. If the individual needs other treatment, they will be referred to a clinic or physician best suited for them. Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, nutritionists, and health coaches to provide the most effective clinical treatments.
Balancing Body and Metabolism
References
National Library of Medicine, MedlinePlus. (2024). Fluid and electrolyte balance. Retrieved from https://medlineplus.gov/fluidandelectrolytebalance.html
National Library of Medicine, MedlinePlus. (2023). Low blood sodium. Retrieved from https://medlineplus.gov/ency/article/000394.htm
National Library of Medicine MedlinePlus. (2023). Low blood potassium. Retrieved from https://medlineplus.gov/ency/article/000479.htm
Replenishing electrolytes and maintaining hydration is essential for individuals who work out, fitness enthusiasts, and those who play recreational or serious sports and want to improve overall health. Can making a homemade sugar-free electrolyte drink help individuals achieve health goals faster?
Homemade Electrolyte Drink
Sports drinks can help replenish the body’s lost electrolytes. Individuals who follow a low-carb diet and exercise or who are on a low-carb diet and get sick need double the added electrolytes. There is evidence that electrolytes are very effective in regulating the body’s fluid balance, especially during and after exercise or illness, and for those on a strict low-carb diet. (Maughan R. J. 1991)
Why More Electrolytes Are Needed
On a low-carb diet, insulin levels drop, so the kidneys retain less sodium. As the body excretes water, important minerals, such as the electrolytes calcium, sodium, magnesium, chloride, and potassium, are also excreted from the body’s system. Therefore, it is important to replenish them to avoid negative symptoms like lightheadedness and dehydration—especially when exercising or ill. (Bostock E. C. S. et al., 2020)
Two tablespoons of lemon juice contain almost the same amount of potassium in an 8-ounce sports drink.
A pinch of salt supplies 110 milligrams of sodium, the same amount in 8 ounces of a sports drink.
Individuals can make a low-carb homemade electrolyte sports drink. Many sports drinks contain a lot of sugar and other additives. The science behind why many of these drinks contain sugar is that a quick hit of sugar provides glucose for replenishing energy stores. Most individuals benefit from having small amounts of carbohydrates during heavy exercise. However, those who want to avoid sugar might want a sugar-free option to replace fluids and electrolytes.
Basic Recipe
Homemade Electrolyte Drink Mix:
1 cup or 8 ounces of non-carbonated water
Two tablespoons of lemon juice
A small pinch of salt—a teaspoon contains 2,300 milligrams of sodium, but the body needs 1/20th of a teaspoon.
Flavoring and sweetener for taste are optional. Try unsweetened Kool-Aid, Crystal Light Drink Mix, or sugar-free flavored syrups.
If avoiding artificial sweeteners, Stevia could be an option.
Sports Drink Ingredients
What goes into most sports drinks and adapting to a low-carb diet?
Water
Water is a primary ingredient, as the goal is to hydrate the body.
Sugar
Sports drinks can contain a lot of sugar, but only about half the sugar of most commercial beverages. For example,
A 20-ounce bottle of Gatorade has about 34 grams of sugar.
A 20-ounce soda has about 69 grams of sugar.
Sports drinks have less sugar to prevent gastrointestinal cramping during exercise and strenuous physical activity. Although Gatorade contains less sugar than soda, depending on individual health goals, it may not be the best option. Studies of nutritional needs during exercise for those restricting carbohydrates are not extensive. However, it is known that when individuals cut carbs, their bodies switch from primarily using carbohydrates to using fat for energy. This change, known as keto-adaptation, can take two to three weeks. Native populations, like the Inuit, traditionally ate a very low-carbohydrate diet and could maintain vigorous endurance for a long time without ill effects. (Phinney S. D. 2004) This suggests that bodies adapt to using fat for energy during physical activity and exercise over time. However, cutting carbohydrates too much and too soon can lead to symptoms like the keto flu. (Harvard Medical School, 2018). Individuals may need to replace carbohydrates during training for longer, more vigorous workouts, such as running longer than an hour. In addition, what is eaten before and after exercise can also affect physical performance. Working with a registered dietitian, nutritionist, or health coach could be helpful to achieve specific fitness goals.
Electrolytes
Electrolytes are molecules of certain minerals that contain an electrical charge. The nervous system runs on those charges generated by manipulating molecules called ions. (Faber D. S. and Pereda A. E. 2018) Every body function that depends on the nervous system, which includes muscle movement, breathing, digestion, thinking, etc., requires electrolyte activity. Those who exercise strenuously for long periods, individuals who follow a low-carb diet, or those with illness may need extra salt and potassium. Sports drinks contain small amounts of sodium and potassium. A balanced diet will supply plenty of minerals for electrolyte needs for individuals engaged in moderate exercise.
Using an integrated approach to treat and prevent injuries and chronic pain syndromes, improve flexibility, mobility, and agility, and help individuals return to normal activities, Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop a personalized treatment, nutrition, and fitness programs. Each case is different and requires reviewing individual medical history and physical examination to determine the proper and most effective plan. Dr. Jimenez has teamed up with top trainers, clinical specialists, medical researchers, and rehabilitation providers to provide the most effective treatments and training.
Is Intermittent Fasting the Ultimate Weight Loss Hack?
References
Maughan R. J. (1991). Fluid and electrolyte loss and replacement in exercise. Journal of sports sciences, 9 Spec No, 117–142. https://doi.org/10.1080/02640419108729870
Bostock, E. C. S., Kirkby, K. C., Taylor, B. V., & Hawrelak, J. A. (2020). Consumer Reports of “Keto Flu” Associated With the Ketogenic Diet. Frontiers in nutrition, 7, 20. https://doi.org/10.3389/fnut.2020.00020
Phinney S. D. (2004). Ketogenic diets and physical performance. Nutrition & metabolism, 1(1), 2. https://doi.org/10.1186/1743-7075-1-2
Harvard Medical School, Harvard Health Publishing, Marcelo Campos, M., Contributor. (2018). What is keto flu? Harvard Health Blog. https://www.health.harvard.edu/blog/what-is-keto-flu-2018101815052
Faber, D. S., & Pereda, A. E. (2018). Two Forms of Electrical Transmission Between Neurons. Frontiers in molecular neuroscience, 11, 427. https://doi.org/10.3389/fnmol.2018.00427
Do individuals with muscle pain know the difference between heat stroke and heat exhaustion and can find ways to stay cool?
Introduction
As the temperature rises worldwide, many individuals are enjoying their time outside and getting more sun in their lives. However, rising temperatures also mean the rise of heat-related illnesses. The two most common heat-related illnesses are heat stroke and heat exhaustion, which can impact an individual’s musculoskeletal system and have different symptoms in terms of severity. Today’s article focuses on the differences between these two heat-related illnesses, how they affect the musculoskeletal system and treatments to stay cool while reducing muscle pain. We discuss with certified associated medical providers who consolidate our patients’ information to assess heat-related illnesses associated with muscle pain. We also inform and guide patients while asking their associated medical provider intricate questions to integrate treatments and ways to stay cool when temperatures rise and reduce muscle pain. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
Heat Exhaustion VS Heat Stroke
By understanding the differences between heat stroke and heat exhaustion is crucial. Do you often feel overheated after simple activities? Have you experienced muscle pain or cramps? Or do you struggle to cool down? These are all signs of heat-related illnesses. Heat-related illnesses often occur when the body cannot dissipate heat, leading to dysfunctional thermoregulation. (Gauer & Meyers, 2019) The two most common types are heat exhaustion and heat stroke. While they share similar causes, they differ significantly in terms of severity, symptoms, and treatment. (Prevention, 2022)
Heat exhaustion is a mild condition that often occurs when the human body loses excessive water and salt from profusely sweating. This causes the external temperatures to be more moderate when associated with intense physical activity. (Leiva & Church, 2024) Additionally, when a person is dealing with heat exhaustion, some of the symptoms that they will experience include:
Heavy sweating
Fatigue
Headaches
Muscle cramps
Pale, cool, moist skin
Fast, weak pulse
Even though heat exhaustion is a mild heat-related condition, it can develop into severe heat-related conditions like heat stroke if not treated immediately. Heat stroke is a severe heat-related illness that is not only life-threatening buthas two forms that can affect a person’s body temperature: classic and exertional. Classic heat stroke often affects elderly individuals who have chronic medical conditions, while exertional heat stroke affects healthy individuals who are doing strenuous physical activities. (Morris & Patel, 2024) Some of the symptoms associated with heat stroke include:
High body temperature (104°F or higher)
Hot, red, dry skin
Rapid, strong pulse
Confusion
Seizures
Loss of consciousness
How Do Both Conditions Affect The Muscles?
Both heat-related illnesses can have a significant effect on the musculoskeletal system and cause muscle pain to not only the extremities but also the entire body system. The issue affects the musculoskeletal system and can lead to painful muscle cramps, involuntary muscle contractions, and muscle pain. Since muscle pain is a multi-factorial condition, heat-related illnesses like heat stroke and exhaustion can influence a person’s lifestyle and comorbid health factors. (Caneiro et al., 2021) When that happens, many individuals can seek treatments to stay cool from heat exhaustion and heat stroke and reduce muscle pain.
Secrets Of Optimal Wellness-Video
Treatments For Staying Cool & Reduce Muscle Pain
While it is important to understand the difference between heat stroke and heat exhaustion due to the crucial timing and effective interventions, finding various treatments to reduce muscle pain and find ways to stay cool is important. Many individuals can wear technology to monitor the person’s physiological status actively and prevent injuries while providing early detection for heat-related illnesses. (Dolson et al., 2022) This can reduce the chances of muscle pain and help regulate body temperature. For individuals dealing with heat exhaustion, they can:
Move to a cooler environment
Be well-hydrated with water and electrolyte-rich drinks
Rest
Wear cool clothes to lower body temperature
For individuals dealing with heat stroke, they can:
Call emergency services immediately
Apply cool clothes or ice packs to the body
Monitor vital signs
Both treatments can ensure positive results in preventing life-threatening situations that can affect the musculoskeletal system.
Conclusion
Given the significant impact both heat stroke and heat exhaustion can have on the musculoskeletal system, it’s essential to take proactive measures. Proper hydration, cooling, and rest can help manage and alleviate muscle pain associated with these heat-related illnesses. By staying informed, maintaining hydration, and taking proactive steps to protect yourself from excessive heat, you can significantly reduce the chances of these heat-related illnesses affecting your outdoor activities.
References
Caneiro, J. P., Bunzli, S., & O’Sullivan, P. (2021). Beliefs about the body and pain: the critical role in musculoskeletal pain management. Braz J Phys Ther, 25(1), 17-29. https://doi.org/10.1016/j.bjpt.2020.06.003
Dolson, C. M., Harlow, E. R., Phelan, D. M., Gabbett, T. J., Gaal, B., McMellen, C., Geletka, B. J., Calcei, J. G., Voos, J. E., & Seshadri, D. R. (2022). Wearable Sensor Technology to Predict Core Body Temperature: A Systematic Review. Sensors (Basel), 22(19). https://doi.org/10.3390/s22197639
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine