The skin and the gut have a unique connection. The gut system is home to trillions of microorganisms that help metabolize the body’s homeostasis while keeping the immune system functioning for the body to be working correctly. The skin has its set of functions as well as it is the largest organ and helps protect the body from external factors from harm. When these disruptive factors start to affect either the gut or the skin, it can lead to numerous conditions that cause the body to be dysfunctional. When the gut becomes affected by these disruptive factors, it can cause gut disorders and inflammation, affecting the skin and causing disruptions. Today’s article will discuss a skin disorder known as psoriasis and how the gut-skin connection is affected by psoriasis. Referring patients to certified, skilled providers who specialize in gastroenterology treatments. We provide guidance to our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is critical for asking insightful questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions or concerns, please call Dr. Jimenez at 915-850-0900.
What Is Psoriasis?
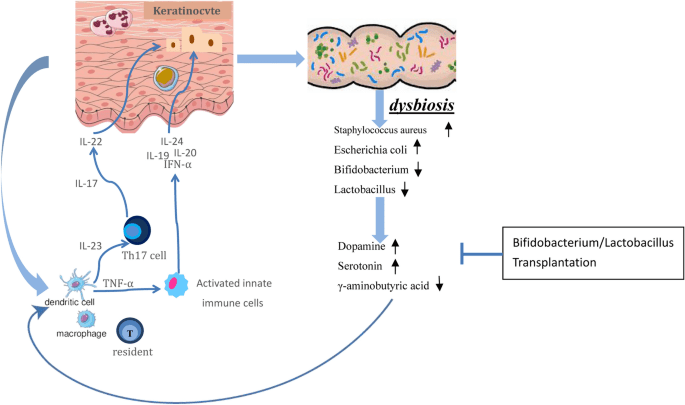
Do you have severe itching along your face and arms? Do certain foods seem to aggravate your digestive tract or skin? Or have you experienced any gut disorders that are affecting your wellbeing? Many of these symptoms are signs of inflammatory issues affecting the gut and are associated with a skin disorder known as psoriasis. Research studies have defined psoriasis as a chronic inflammatory skin disease that is an autoimmune process in which abnormal differentiation and hyper-proliferation of the epidermis occur with redness and scaling. Psoriasis affects about 2% of the general population in the world and is an autoimmune process driven by abnormally activated helper T cells. Additional studies have mentioned that psoriasis is sustained by inflammation that causes the keratinocyte proliferation to be uncontrollable and has dysfunctional differentiation. The inflammatory pathways activate psoriasis in different body locations, causing the individual to become miserable because they are itching and becoming miserable.
An Overview Of Psoriasis-Video
Do you have scaly, patchy lesions in certain areas of your body? Do you feel any gut issues affecting you constantly? Do you feel inflammatory effects disrupting your gut and skin? Many of these conditions are signs that you are experiencing gut disorders associated with a skin disorder known as psoriasis. The video above explains how the gut and skin are affected due to psoriasis and how to heal it naturally. Research studies have mentioned that when the individual is suffering from psoriasis-prone skin, it is due to the alternation of the gut microbiota. When a person scratches the area where psoriasis is formed, it might damage the skin and cause the bacteria to colonize while invoking inflammation to occur in the affected area. Additional research has found that gut disorders like IBD (inflammatory bowel disease) and psoriasis are interlinked due to the increased interaction of inflammatory receptor pathogens disrupting the body’s immune cells.
How The Gut-Skin Connection Is Affected By Psoriasis
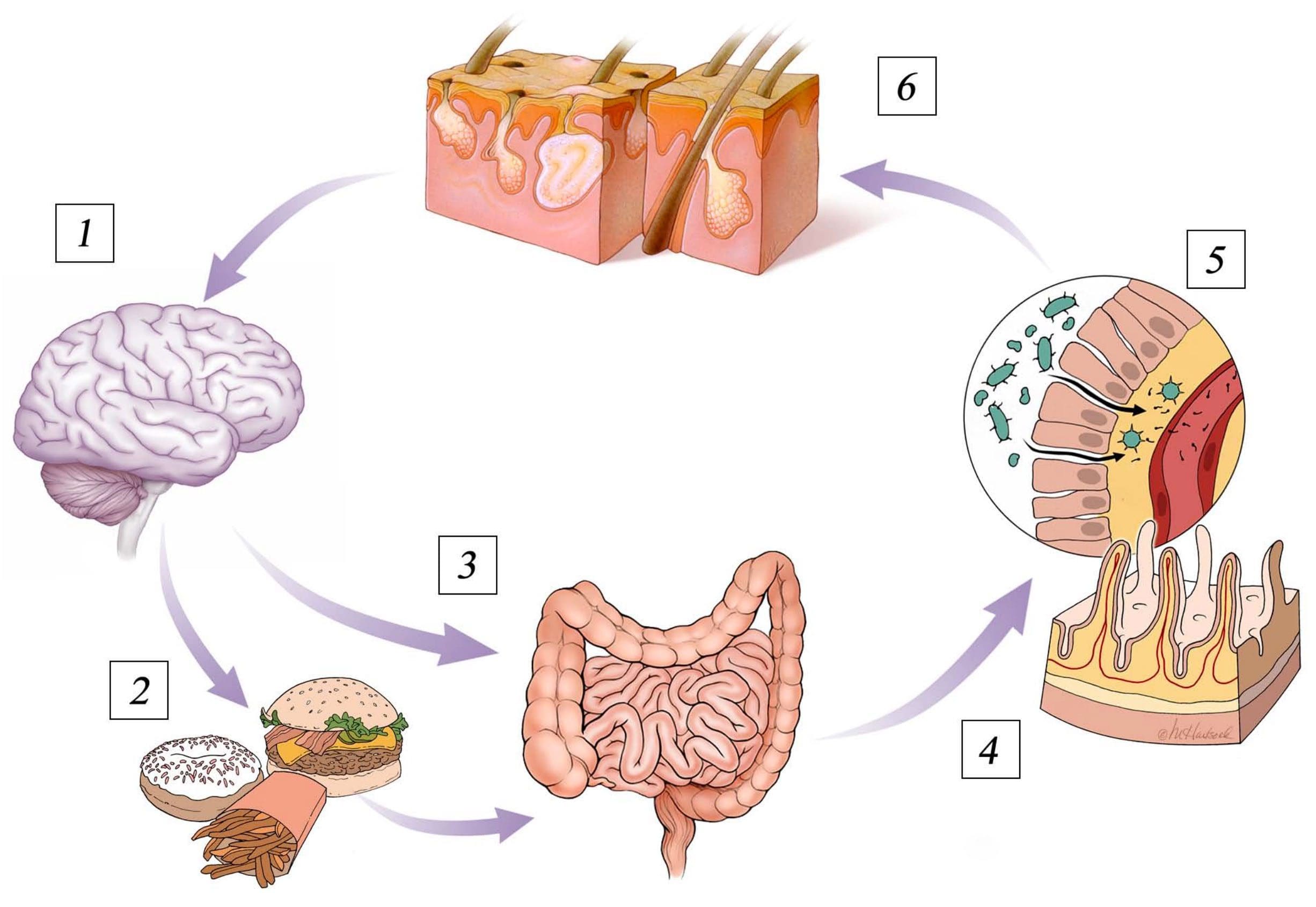
The gut is home to trillions of microorganisms that help metabolize the body’s homeostasis while regulating the immune system. Since the body inhabits microorganisms in various locations, including the skin and gut, it helps maintain homeostasis. The skin helps protect the body from external factors and has bidirectional communication with the gut system. However, like with any autoimmune process, it always starts with the gut. Research studies have mentioned that psoriasis is a multifactorial chronic skin disease that infiltrates the body’s immune cells, causing an increase in skin inflammation and making a person’s life miserable. With the gut system also being inflicted by inflammatory markers, many suffering individuals will experience IBD, SIBO, and other gut disorders that can disrupt the body. Additional information has shown that changes in the microflora in the gut-skin axis from genetic or environmental factors can contribute to various diseases. But when these factors begin to cause an increase in inflammatory markers in the body, it can affect a person’s quality of life through habits that make them miserable.
Conclusion
The body needs the gut and skin to maintain homeostasis and metabolize the immune system. The gut microbiota helps transport the nutrients that the body needs and regulates the body’s immunity, while the skin protects the body from outside factors while being the largest organ. The gut and skin have a bi-directional connection that allows them to keep the body from suffering from dysbiosis. When disruptive factors affect either the gut or the skin, it can lead to many disorders and make a person’s life miserable. The skin suffers from a condition known as psoriasis, a chronic inflammatory disease that causes itchy, patchy lesions that can affect the areas around the body. Psoriasis is associated with gut disorders, as many factors aggravate the inflammatory markers and can be a nuisance if not treated early. Incorporating small changes that benefit both the gut and skin health can help relieve the individual from psoriasis and bring back their quality of life.
References
Chen, Lihui, et al. “Skin and Gut Microbiome in Psoriasis: Gaining Insight into the Pathophysiology of It and Finding Novel Therapeutic Strategies.” Frontiers in Microbiology, Frontiers Media S.A., 15 Dec. 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7769758/.
De Francesco, Maria Antonia, and Arnaldo Caruso. “The Gut Microbiome in Psoriasis and Crohn’s Disease: Is Its Perturbation a Common Denominator for Their Pathogenesis?” Vaccines, MDPI, 5 Feb. 2022, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8877283/.
Ellis, Samantha R, et al. “The Skin and Gut Microbiome and Its Role in Common Dermatologic Conditions.” Microorganisms, MDPI, 11 Nov. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6920876/.
Nair, Pragya A, and Talel Badri. “Psoriasis.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 6 Apr. 2022, https://www.ncbi.nlm.nih.gov/books/NBK448194/.
Olejniczak-Staruch, Irmina, et al. “Alterations of the Skin and Gut Microbiome in Psoriasis and Psoriatic Arthritis.” International Journal of Molecular Sciences, MDPI, 13 Apr. 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8069836/.
Rendon, Adriana, and Knut Schäkel. “Psoriasis Pathogenesis and Treatment.” International Journal of Molecular Sciences, MDPI, 23 Mar. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6471628/.
The skin is the largest organ in the body and encounters numerous factors that can either benefit or harm the body. The skin helps protect the organs and intestines in the gut system, keeps the musculoskeletal system structure functional, and even helps the nervous system send out signals for motor-sensory functions to the rest of the body. The skin is associated with the gut system as the gut microbiota host trillions of beneficial gut flora that send out nutrients to help promote tissue growth, improve the body’s immunity, and metabolize skin health by protecting it from disruptive pathogens. When these pathogens cause inflammatory issues in the gut system, it can affect the body’s skin, brain, and immune health by making them dysfunctional. Today’s article will look at a skin condition known as atopic dermatitis, how it affects the gut-skin system, and what treatments are available for relieving gut issues and atopic dermatitis in individuals. Referring patients to certified, skilled providers who specialize in gastroenterology treatments. We provide guidance to our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is critical for asking insightful questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions or concerns, please call Dr. Jimenez at 915-850-0900.
What Is Atopic Dermatitis?
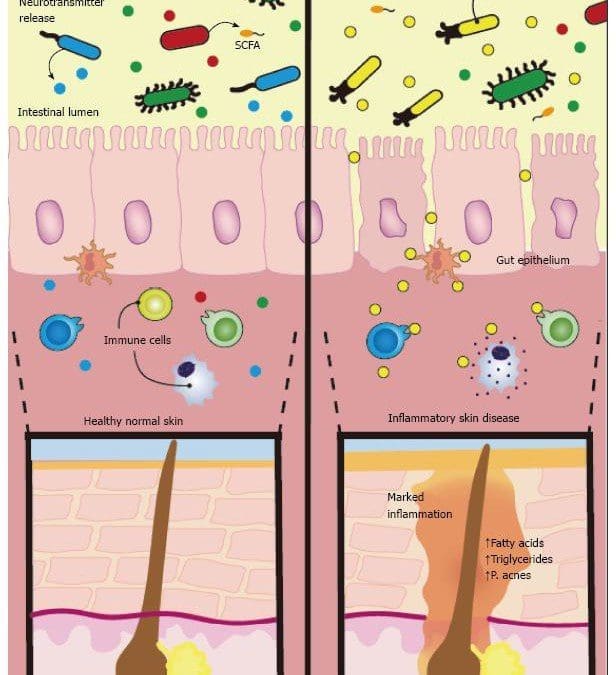
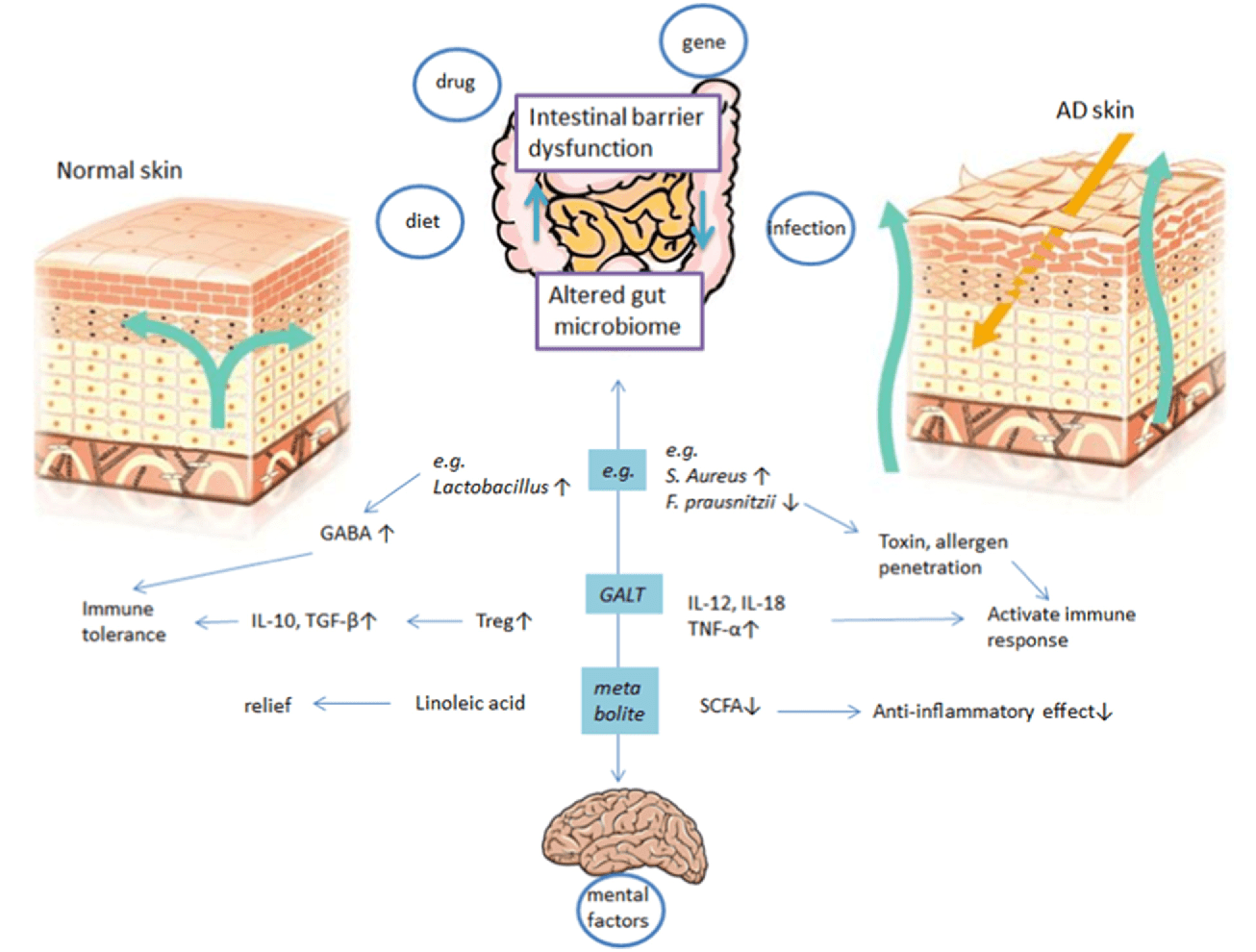
Have you experienced inflammation around your gut or in certain areas of your skin? Do issues like SIBO, IBD, leaky gut, or bloating become more frequent? Do certain foods trigger inflammatory markers in your skin and gut? The numerous signs and symptoms are due to a skin disorder known as atopic dermatitis. Atopic dermatitis or eczema is a pruritic, hereditary skin disorder. The lifetime prevalence is 10% to 20%, with many cases starting as a baby and rising to 20% to 40% as adults continue to have atopic dermatitis. Research studies have defined atopic dermatitis as one of the most common skin diseases that cause chronic inflammation in the skin. The pathophysiology of atopic dermatitis is both complex and multifactorial. It involves the elements of barrier dysfunction, alterations in cell-mediated immune responses, IgE-mediated hypersensitivity, and environmental factors that cause flare-ups. Additional research studies have mentioned that the pathology of atopic dermatitis is being looked at as the skin’s structural abnormalities and immune dysregulation play their roles as this condition progress. Other genetic changes have also been identified, altering the skin’s barrier function, resulting in an atopic dermatitis phenotype. The imbalance of Th2 to Th1 cytokines is observed as it alters cell-mediated immune responses. Atopic dermatitis can promote IgE-mediated hypersensitivity in the skin as part of its development. This can also be due to the environmental factors that be the causing development of atopic dermatitis.
How Does It Affect The Gut-Skin Connection?
Since atopic dermatitis is a chronic inflammatory skin disease, many factors do come to play in its development. For example, food allergies cause atopic dermatitis in 25% to 50% of children. Some of the food allergens that are commonly linked to atopic dermatitis include:
Eggs
Soy
Milk
Wheat
Fish
Shellfish
Peanuts
One of the other factors that can cause the development of atopic dermatitis is gut issues. Research studies have shown that any alterations in the gut microbiome due to atopic dermatitis affect the immune system balance in the body. When the gut microbiome becomes altered, it affects metabolite production and reduces the body’s immune system. When bacteria overgrowth in the GI tract, it has been suggested as a causative factor in allergic diseases, including atopic dermatitis. Another factor is when individuals consume trans fats, which increase the development of atopic dermatitis since they interfere with the metabolism and use of essential fatty acids.
The Microbiome Of Atopic Dermatitis-Video
Have you experienced inflammation in your digestive tract or particular areas of your skin? Does your body feel fatigued constantly? Do you have any gut issues or disorders that are affecting your health? Most of these symptoms are signs that you are experiencing atopic dermatitis caused by gut issues. Research studies have found that various factors can trigger atopic dermatitis, affect the immune system, and disrupt the gut microbiota. The video above explains the microbiome in atopic dermatitis and how it affects the gut, skin, and the entire body. Luckily there are available treatments to relieve atopic dermatitis and gut disorders from wreaking havoc on the body.
Treatments For Relieving Atopic Dermatitis & The Gut
When a person begins to find treatments for relieving atopic dermatitis usually involves:
Early diagnosis.
Skin barrier function support.
Mitigation of cutaneous inflammation.
Concomitant risk stratification
Another way that many individuals can alleviate atopic dermatitis is with a healthy GI tract. This will help many individuals suffering from a food allergy, asthma, allergic rhinitis, and environmental allergies to relieve atopic dermatitis from progressing further. A study showed that probiotics and prebiotics are essential in preventing food allergies and eczema. Probiotics and prebiotics help replenish the beneficial bacteria in the gut and regulate the immune system. This prevents atopic dermatitis from stopping progressing and restor the body back.
Conclusion
Many factors cause atopic dermatitis progression to become severe, as it is crucial to find the root cause of the flare-ups and alleviate them at the source. Overall having gut issues associated with atopic dermatitis is no laughing matter. When the gut microbiome is being affected by inflammatory disorders, it can disrupt the immune system and cause atopic dermatitis to develop on the skin. Incorporating probiotics and prebiotics can help replenish the gut bacteria and figure out what causes the inflammatory symptoms to spike up from certain foods will benefit the gut and the skin to become healthier.
References
Fang, Zhifeng, et al. “Gut Microbiota, Probiotics, and Their Interactions in Prevention and Treatment of Atopic Dermatitis: A Review.” Frontiers in Immunology, Frontiers Media S.A., 14 July 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8317022/.
Kapur, Sandeep, et al. “Atopic Dermatitis.” Allergy, Asthma, and Clinical Immunology : Official Journal of the Canadian Society of Allergy and Clinical Immunology, BioMed Central, 12 Sept. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6157251/.
Kim, Jung Eun, and Hei Sung Kim. “Microbiome of the Skin and Gut in Atopic Dermatitis (AD): Understanding the Pathophysiology and Finding Novel Management Strategies.” Journal of Clinical Medicine, MDPI, 2 Apr. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6518061/.
Kolb, Logan, and Sarah J Ferrer-Bruker. “Atopic Dermatitis – Statpearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 13 Aug. 2021, https://www.ncbi.nlm.nih.gov/books/NBK448071/.
Lee, So Yeon, et al. “Microbiome in the Gut-Skin Axis in Atopic Dermatitis.” Allergy, Asthma & Immunology Research, The Korean Academy of Asthma, Allergy and Clinical Immunology; The Korean Academy of Pediatric Allergy and Respiratory Disease, July 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6021588/.
The body is always going through many factors that constantly test the durability that can affect the entire microbiome itself. The gut helps the body’s homeostasis by metabolizing the nutrients that provide the energy for functionality. The gut system is home to trillions of microorganisms that communicate to the brain system, endocrine system, immune system, and skin to ensure that it is healthy. When disruptive factors enter the gut system, they can cause various issues that can make the dysfunctional body while affecting its communication with the body’s axis. Today’s article focuses on a skin condition that everyone has suffered in their lives known as acne and how the gut-skin axis is being affected by acne. Referring patients to certified, skilled providers who specialize in gastroenterology treatments. We provide guidance to our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is critical for asking insightful questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions or concerns, please call Dr. Jimenez at 915-850-0900.
What Is Acne Vulgaris?
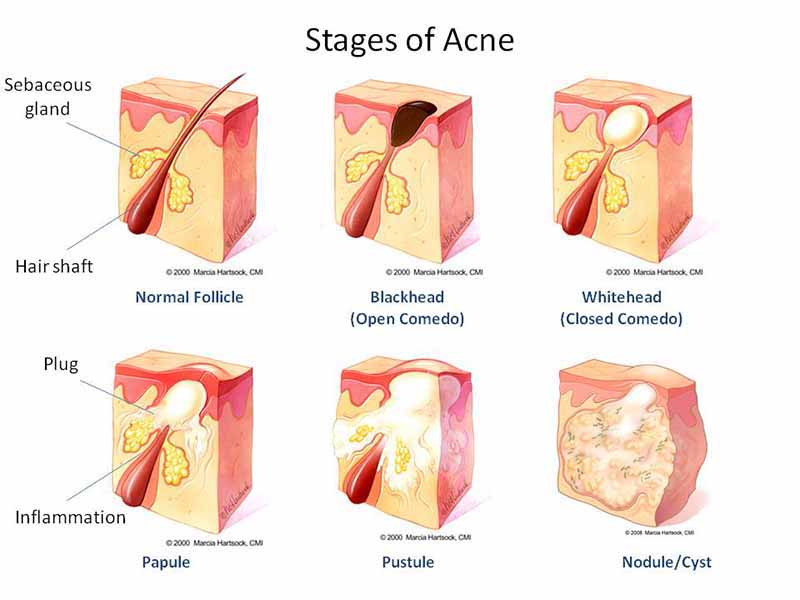
Have you noticed bumps along your face, especially in the nose, forehead, and cheek regions? How about inflammatory reactions that are affecting your skin? Do issues like GERD, IBS, leaky gut, or SIBO affect your gut? Most of these issues are due to disruptive factors that affect the gut-skin connection and cause a skin condition known as acne vulgaris. Everybody suffers from acne when they are young, and it is a common condition with follicular papules or comedones and inflammatory papules and pustules. Research studies have shown that acne vulgaris is an inflammatory disorder triggered by many factors that can cause it to become aggravated and inflamed. Some of the contributing factors that can cause acne vulgaris to form due to the following:
Infection (Propionibacterium acnes)
Tissue inflammation
Plugging of hair follicles due to epidermal hyperproliferation
Hormone imbalance
Endocrine disorders
Excess sun exposure
Other research studies have shown that other factors like gut disorders can also affect the development of acne vulgaris. Acne vulgaris can be associated with the emotional factors that affect the brain and the gut’s inflammatory factors as they go hand in hand. When a person becomes stressed or anxious, their skin will flare up and develop acne around some skin regions. Additional studies have mentioned that emotional factors like stress and anxiety can alter the gut microbiota and increase intestinal permeability. When gut disorders start to contribute to skin inflammation, it can aggravate acne to develop and form on the skin.
Gut Health & Acne- Video
Have you experienced gut disorders that seem to affect your quality of life? Have you noticed that particular foods you consume are not sitting well in your gut system? How about feeling overly stressed and anxious that acne forms around your face? The video above explains how the gut microbiome affects a person when making dietary changes that can provide beneficial results to the gut microbiota. Research studies have found that the intestinal microbiota is essential for forming acne lesions while being responsible for proper immunity and defense of the microorganisms. The GI tract and acne condition are closely associated because they provide the neuroendocrine and immune functions to the body.
The Gut-Skin Axis & How It Affects Acne
Since the gut is the host to trillions of bacteria, its primary job is to maintain constant communication with the skin to dampen unnecessary inflammatory markers that can cause the skin to break out. Research studies have found that the gut-skin axis, when affected by acne, produces significantly higher metabolites that generate ROS (reactive oxygen species) and induce inflammation in both the gut and skin. Additional research has shown that the gut microbiome plays an essential role in skin disorders and vice versa. When changes affect either the gut or the skin, it can drastically change a person’s outcome in life. Say, for instance, dietary habits that cause inflammation in the gut. This is due to processed foods that cause the gut to become inflamed and make the skin begin the development of acne in different portions of the skin. Research shows that the gut microbiome can vastly influence the immune system by regulating it. This builds a tolerance to dietary changes in the gut to promote acne-free skin. So incorporating a low-glycemic-load diet has been linked to improved acne, possibly through gut changes or attenuation of insulin levels.
Conclusion
Overall, the gut plays a massive role in the body in its homeostasis as it helps the body metabolize the nutrients to keep it functioning and moving. The gut microbiota also has bidirectional communication with the skin as common skin disorders like acne tend to show up. Acne is very common amongst individuals, especially in younger individuals, as it can affect their moods and cause changes to their mental health and their gut health. Incorporating small changes like eating healthy food, maintaining a stress-free environment, and even exercising can help not only lower gut inflammation but also clear up the skin from acne.
References
Bowe, Whitney P, and Alan C Logan. “Acne Vulgaris, Probiotics and the Gut-Brain-Skin Axis – Back to the Future?” Gut Pathogens, BioMed Central, 31 Jan. 2011, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3038963/.
Chilicka, Karolina, et al. “Microbiome and Probiotics in Acne Vulgaris-A Narrative Review.” Life (Basel, Switzerland), MDPI, 15 Mar. 2022, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8953587/.
De Pessemier, Britta, et al. “Gut-Skin Axis: Current Knowledge of the Interrelationship between Microbial Dysbiosis and Skin Conditions.” Microorganisms, MDPI, 11 Feb. 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7916842/.
Lee, Young Bok, et al. “Potential Role of the Microbiome in Acne: A Comprehensive Review.” Journal of Clinical Medicine, MDPI, 7 July 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6678709/.
Salem, Iman, et al. “The Gut Microbiome as a Major Regulator of the Gut-Skin Axis.” Frontiers in Microbiology, Frontiers Media S.A., 10 July 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6048199/.
Sutaria, Amita H, et al. “Acne Vulgaris.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 8 May 2022, https://www.ncbi.nlm.nih.gov/books/NBK459173/.
As everyone knows, the gut helps the body metabolize nutrients and vitamins that it needs to function correctly. The gut system also allows the body’s immunity to perform while staying in communication with the brain. The gut helps sends signals back and forth to regulate the body’s hormones signals and other beneficial substances that the body requires. The gut is also in communication with the largest organ in the body, which is the skin. When intolerable factors start to wreck the gut and cause chaos inside the gut system, it disrupts the brain signals in the nervous system and can also take a toll on the skin. Today’s article will focus on a skin condition known as rosacea, how it affects the gut system, and what is the gut-skin connection. Referring patients to certified, skilled providers who specialize in gastroenterology treatments. We provide guidance to our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is critical for asking insightful questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions or concerns, please call Dr. Jimenez at 915-850-0900.
What Is Rosacea?
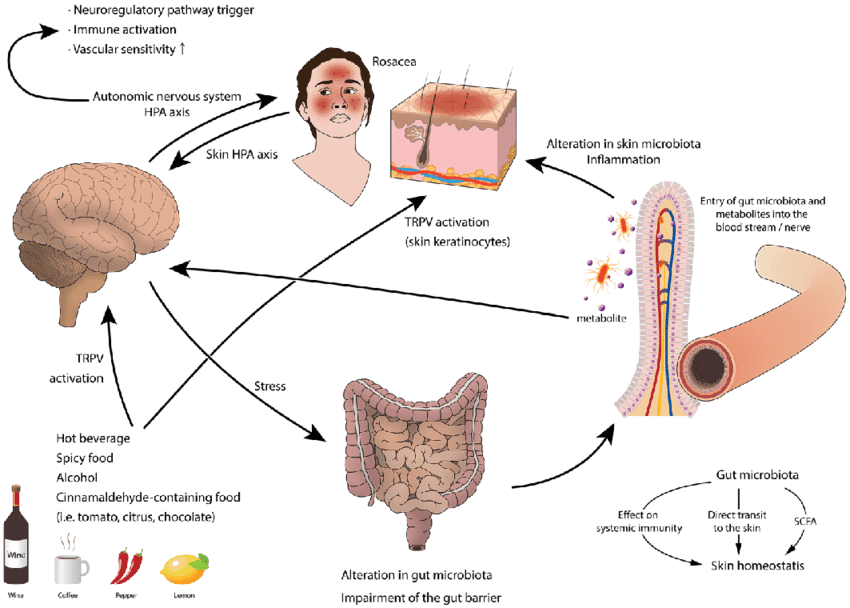
Have you felt any gut disorders like IBS, leaky gut, or GERD affecting your mid-section? How about redness around your face, especially the nose and cheek areas? Does your skin seem to feel tender to the touch in certain areas? Most of these symptoms are related to a chronic inflammatory disease known as rosacea. It is usually indicated by genetic and environmental components that can trigger rosacea initiation on the skin. Rosacea is generally aggravated by dysregulation of the body’s innate and adaptive immune system. Research studies have mentioned that rosacea is usually developed by lymphatic dilation and blood vessels exposed to extreme temperatures, spices, or alcohol which causes rosacea to affect the cheeks and nose. Not only that, but genetics, immune reaction, microorganisms, and environmental factors lead to various mediators such as keratinocytes, endothelial cells, mast cells, macrophages, T helper type 1 (TH1), and TH17 cells.
How Does It Affect The Gut System?
Since rosacea is developed through exposure to high temperatures, spices, or alcohol, research studies have shown that particular food and drinks cause the inflammatory cytokines to become triggered in the face. Additionally, many trigger factors can directly communicate to the cutaneous nervous system; neurovascular and neuro-immune active neuropeptides are lead to the manifestation of rosacea lesions. Some of the other triggers that can cause rosacea to develop is an unhealthy gut system. A study showed that more than 50% had low stomach acid among patients who had both rosacea and dyspepsia. The bacteria H.pylori resides in the stomach and has been recognized to trigger inflammation and gastrin-induced flushing, thus causing rosacea. Additional studies have mentioned that rosacea individuals will experience some gut disorders to occur. Since the gut system can succumb to various factors, it can affect the gut’s composition and trigger rosacea. Since the gut microbiota has influenced the body’s homeostasis, it can also influence the skin. When there are factors that trigger the intestinal barrier of the gut, it can affect the skin, causing the inflammatory cytokines to proceed with the development of rosacea.
Uncovering The Gut-Skin Connection-Video
Does your skin feel flushed due to extreme temperatures or consuming spicy food? Have you experienced gut disorders like SIBO, GERD, or leaky gut? Has your skin seemed to break out even more than it should? Your skin could be affected by your gut microbiota, as the video above shows what the gut-skin connection is and how they work with each other. Research studies have shown that since the gut microbiome is the key regulator of the body’s immune system, it plays a vital role in various skin disorders. This means that when environmental factors affect the gut’s microbiome, it also affects the skin through dysbiosis.
What Is The Gut-Skin Connection?
As stated earlier, the gut system is home to trillions of microorganisms that help metabolize the body’s homeostasis, including the largest organ, the skin. Research studies have found that when the gut microbial and the skin communicate with each other. It creates a bidirectional connection. The gut microbiome is also an essential mediator of inflammation in the gut and affects the skin. When there are factors like insulin resistance, imbalances in the sex hormones, gut inflammation, and microbial dysbiosis wrecking the gut system, the effects can cause the pathology of many inflammatory disorders to affect the skin. Any changes to the gut can also affect the skin as the gut consumes food to be biotransformed into nutrients that the body needs. But when food allergies and sensitivities affect the gut, the skin also gets involved, causing skin disorders like rosacea.
Conclusion
Overall the gut makes sure that the body is functioning correctly by metabolizing nutrients from consumed foods. The gut system has a connection to not only the brain and immune system but also the skin. The gut-skin connection goes hand in hand as factors that affect the gut can also affect the skin in developing skin disorders like rosacea. When a person is suffering from gut disorders, their skin is also damaged by factors like stress, food sensitivities, and skin disorders that can become a nuisance. This can be alleviated through small changes like reducing stress, eating healthy foods, and exercising, which are beneficial for relieving gut and skin disorders for individuals who want to get their health back.
References
Daou, Hala, et al. “Rosacea and the Microbiome: A Systematic Review.” Dermatology and Therapy, Springer Healthcare, Feb. 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7859152/.
De Pessemier, Britta, et al. “Gut-Skin Axis: Current Knowledge of the Interrelationship between Microbial Dysbiosis and Skin Conditions.” Microorganisms, MDPI, 11 Feb. 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7916842/.
Farshchian, Mehdi, and Steven Daveluy. “Rosacea.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 30 Dec. 2021, https://www.ncbi.nlm.nih.gov/books/NBK557574/.
Kim, Hei Sung. “Microbiota in Rosacea.” American Journal of Clinical Dermatology, Springer International Publishing, Sept. 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7584533/.
Mikkelsen, Carsten Sauer, et al. “Rosacea: A Clinical Review.” Dermatology Reports, PAGEPress Publications, Pavia, Italy, 23 June 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5134688/.
Salem, Iman, et al. “The Gut Microbiome as a Major Regulator of the Gut-Skin Axis.” Frontiers in Microbiology, Frontiers Media S.A., 10 July 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6048199/.
If you are experiencing any of these situations, then your collagen peptides might be low.
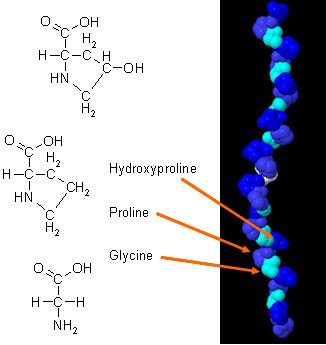
There have been new studies on how collagen can improve body composition when it is combined with daily exercises. Collagen in the body has a unique amino acid composition that plays an essential role in the body’s anatomy. Collagen protein is a concentrated source of glycine, proline, and hydroxyproline, and when it is being compared to all the other dietary proteins, it makes collagen a potential practical choice as a structural protein.
In a 2015 study, researchers have demonstrated how efficient collagen supplements can improve body composition in active males. The results show how each male individuals are participating in weight training at least three times a week and have to supplement with at least 15 grams of collagen peptides to achieve maximum health. The assessments that the test provide are strength test, bioimpedance analysis (BIA), and muscle biopsies. These tests make sure that the male individuals are performing well after taking the collagen supplements, and the results show how their body mass had an increase of fat-free body mass. Another study showed how collagen protein supplementation when it is combined with resistance training that can increase muscle mass and muscle strength with the elderly as well as people with sarcopenia.
Beneficial Properties With Collagen
There are many beneficial properties that collagen supplements can provide to the body when it is consumed. There are hydrolyzed collagen and gelatin and can help improve a person’s skin structure. Even though there are not many studies on collagen supplements, there are excellent promises for the areas on the body. They are:
Muscles mass: Collagen supplements, when combined with strength training, can increase muscle mass and strength in the body.
Arthritis: Collagen supplements can help people with osteoarthritis. Studies show that when people osteoarthritis take collagen supplements, they discovered a massive decline in the pain they were experiencing.
Skin elasticity: In a 2014 study, it stated that women who took collagen supplements and has shown improvements in skin elasticity. Collagen can also be used in topical treatments to help improve the appearance of a person�s skin by minimizing fine lines and wrinkles.
Not only collagen supplements provide beneficial properties to the specific areas on the body, but there are the four main types of collagen and what is their roles in the human body as well as their functions:
Type 1: Type 1 collagen took account of 90% of the body’s collagen and made up of densely packed fibers that provide structures to the skin, bones, connective tissues, and teeth that are in the body.
Type 2: Type 2 collagen is made up of loosely packed fibers that are found in the elastic cartilage, which helps cushion the joints in the body.
Type 3: Type 3 collagen helps support the structure of the muscles, organs, and arteries that make sure that the body is functioning correctly.
Type 4: Type 4 collagen is found in the layers of everyone�s skin and helps with the filtration in the body.
Since these four types of collagen are in the body, it is essential to know that collagen can naturally decrease over time with age since the body will produce a lesser lower quality of collagen. One of the visible signs of decrease collagen is when the skin on the human body becomes less firm and supple as well as weaken cartilage due to aging.
Factors That Can Damage Collagen
Even though collagen can decrease naturally with age, many factors can destroy collagens that are harmful to the skin. The harmful factors can include:
Sugar and Carbs: Refined sugars and carb can interfere with collagen�s ability to repair itself on the skin. So by minimizing sugar and carb consumption in the body, it can reduce the effects of vascular, renal, and cutaneous tissue dysfunction.
Sun Exposure: Even though getting enough sun can help a person enjoy the day, however, being exposed to the sun for an extended period can cause damaged to the skin and destroy collagen peptides. The effects of overexposure of the sun can cause the skin to photo age and produce oxidative stress in the body.
Smoking: When a person smokes, it can reduce collagen production in the body, causing the body to have premature wrinkles, and if the body is wounded, the healing process will be slower and can lead to ailments in the body.
Autoimmune Diseases: Some autoimmune diseases can also damage collagen production like lupus.
Conclusion
Collagen is vital for the body as it helps the skin be gentle and firm. Naturally, it will decrease as a person gets older, so taking collagen supplements can make sure that the body can function correctly. When harmful factors are affecting the body, they can stop or even damage collagen production and accelerate the process of premature wrinkles from forming, making a person look older than they are. Some products can help the body’s cellular activity by providing more excellent stability, bioavailability, and digestive comfort.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
References:
Bosch, Ricardo, et al. �Mechanisms of Photoaging and Cutaneous Photocarcinogenesis, and Photoprotective Strategies with Phytochemicals.� Antioxidants (Basel, Switzerland), MDPI, 26 Mar. 2015, www.ncbi.nlm.nih.gov/pmc/articles/PMC4665475/.
Danby, F William. �Nutrition and Aging Skin: Sugar and Glycation.� Clinics in Dermatology, U.S. National Library of Medicine, 2010, www.ncbi.nlm.nih.gov/pubmed/20620757.
Jennings, Kerri-Ann. � Collagen – What Is It and What Is It Good For?� Healthline, 9 Sept. 2016, www.healthline.com/nutrition/collagen.
Jurgelewicz, Michael. �New Study Demonstrates the Benefits of Collagen Peptides for Improving Body Composition Combined with Exercise.� Designs for Health, 31 May 2019, blog.designsforhealth.com/node/1031.
Knuutinen, A, et al. �Smoking Affects Collagen Synthesis and Extracellular Matrix Turnover in Human Skin.� The British Journal of Dermatology, U.S. National Library of Medicine, Apr. 2002, www.ncbi.nlm.nih.gov/pubmed/11966688.
Proksch, E, et al. �Oral Supplementation of Specific Collagen Peptides Has Beneficial Effects on Human Skin Physiology: a Double-Blind, Placebo-Controlled Study.� Skin Pharmacology and Physiology, U.S. National Library of Medicine, 2014, www.ncbi.nlm.nih.gov/pubmed/23949208.
Schauss, Alexander G, et al. �Effect of the Novel Low Molecular Weight Hydrolyzed Chicken Sternal Cartilage Extract, BioCell Collagen, on Improving Osteoarthritis-Related Symptoms: a Randomized, Double-Blind, Placebo-Controlled Trial.� Journal of Agricultural and Food Chemistry, U.S. National Library of Medicine, 25 Apr. 2012, www.ncbi.nlm.nih.gov/pubmed/22486722.
Zdzieblik, Denise, et al. �Collagen Peptide Supplementation in Combination with Resistance Training Improves Body Composition and Increases Muscle Strength in Elderly Sarcopenic Men: a Randomised Controlled Trial.� The British Journal of Nutrition, Cambridge University Press, 28 Oct. 2015, www.ncbi.nlm.nih.gov/pmc/articles/PMC4594048/.
By informing individuals about how the National University of Health Sciences provides the knowledge for future generations, the University offers a wide variety of medical professions for functional medicine.
The most important thing about summer is the food. Hotdogs and burgers on the grill and the seasonal fruits and vegetables that are ripe for the picking.� As much as we love the summer sun, it is still dangerous and can be harmful to our skin. We still put on sun cream, wear hats, and wear sun-protective clothing, but, did you know that certain foods can help heal your skin from sun damage and when possible can be eaten raw.
In the previous article, we talked about the 9 nutrients your skin needs to be protected from the harmful sun�s rays. Here is the top 9 food that will protect you from the sun and perfect for the summer.
Guava:
When we think of vitamin C, our minds think of any citrus fruit like oranges, lemon, limes, and grapefruit. But did you know that guava contains vitamin C as well? In fact, guava contains about 5 times more of vitamin C as much as any citrus fruit.
Guava contains about 228.3 mg of vitamin C and has antioxidants that attack free radicals and helps boost your immune system. Vitamin C has been known to battle scurvy. Plus guava can help improve your skin. By eating the fruit or using the guava leaves, your skin will be toned and the antioxidants from the fruit can keep your skin glowing, fight wrinkles and reduce signs of premature aging.
Sweet Potato:
Who doesn�t love potatoes? We eat them as fries, baked, saut�ed, mashed and use them as filling for pies. The sweet potato is no exception. There are many variations of sweet potatoes as they come in orange, white, and purple, depending on where you get them from and which region.
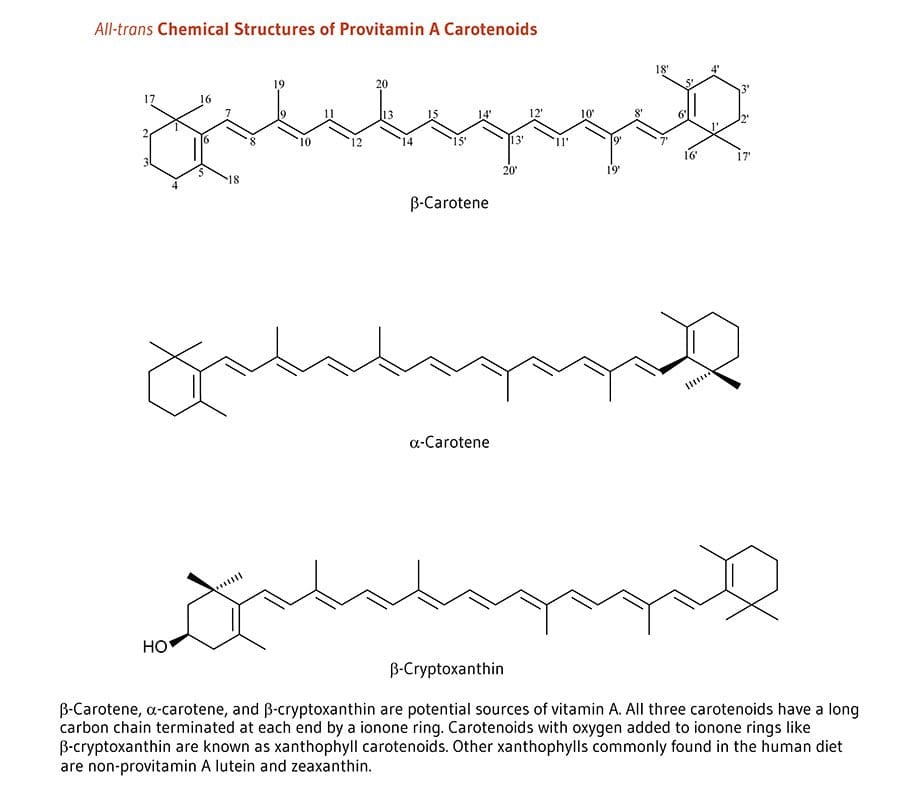
The sweet potatoes we are familiar with have an orange hue due to the carotenoids; which gives us that lovely orange color and has antioxidants to protect our skin from sun damage. Not only that but; sweet potatoes are very high in vitamin A, which is very good when they are cooked. Some people say that potatoes are known to be very starchy and can be used to soothe a sunburn by drawing out the heat from the skin.
Strawberries and Blueberries:
Both of these berries are great on their own but together, they are the dynamic duo to help our bodies combat the sun. Blueberries are richly filled with antioxidants as they combat the free radicals in our systems and can reduce the chances of cancer showing up.
Strawberries are really great as they are called �nature�s natural sunblock.� They contained about 108% of vitamin C as well as ellagic acid, which cleans up the free radicals and reduce sun-damaged pigmentation.� The Journal of Agricultural Food Chemistry stated that strawberries have anthocyanins, which gives the fruit its lovely red color to protect our cells.
Green Tea:
Who doesn�t love green tea? Not only it contains L-theanine, but it has many astounding health benefits that are wonderful and protects our body. Green tea can be consumed or used as a topical cream to soothe and hydrate your skin from the harsh sun rays. Green tea is jammed packed with vitamins B2 and E, as well as large amounts of polyphenol including, EGCG (Epigallocatechin Gallate).
These polyphenols help our inflammatory system repair our DNA from anything harsh in our bodies. Plus green tea has been known to lower the risk of various types of cancers.
Oatmeal:
Oatmeal is one of those foods that we all eat for breakfast. However, did you know that oatmeal can be used to soothe sunburns and exfoliate sun-damaged skin? Not only that but when oatmeal is finely grounded it is known as �colloidal oatmeal.�
You may have seen this type of oatmeal in the health/medical section in your local stores and it may be called, �Aveeno.� �Colloidal oatmeal has been approved by the FDA since 2003 and has been used as a topical ointment for anyone with eczema. Anyone with eczema experiences an abundance of itchiness when they are overly exposed by the sun�s rays or due to the heat of the summer knows this all too well.
With colloidal oatmeal, it helps relieve the symptoms of eczema by being applied with water and gently patting the topical on the source of eczema to lower the inflamed skin, thus calming it down.
Cucumber:
Cucumbers are used for anything that we can think of. In the spa, in our salads, or as a wonderful snack. This green vegetable is packed with vitamins C and K as well as, caffeic acid and potassium. Not only that but cucumbers are made up of 96% of water, which is very refreshing and great for the skin. Since our bodies lose water when we sweat and cucumbers actually replenishes our water intake and�helps cool off our bodies when we are sunburned.
Tomatoes:
Just like strawberries, tomatoes contain lycopene, which gives tomatoes that gorgeous red color and has vitamins C. K1, and B9 and potassium. Tomatoes can be eaten raw and are rich with antioxidants that help balance our bodies pH balance. As well as, protecting our skin from the sun.
Watermelon:
Oh, watermelon� not only you are the most consumed fruit for the 4th of July but you are one of the best summer fruits to be consumed. Watermelons contain not only vitamins A, B6 and C; but they also contained lycopene like tomatoes. Which helps our skin from photoaging from the sun but it�s in the top 30 most hydrating foods, next to cucumbers with 92% of water for excellent hydration properties for our skin.
Carrots:
Carrots are not only good for our eyes but did you know that carrots are jammed pack with beta-carotene, which turns to vitamin A when we eat it. Plus the sun exposure gives carrots vitamin C to help us protect our skin. Carrots have a wonderful source of carotenoids to produce photoprotection for our skin health.
Here at the clinic, we strive to inform our patients about the nutrients that food provides to our bodies. As well as, making our patients feel good with whole, nutritious options. Whether it is by adjustments or leading them to different food options for a healthy life, these top 9 foods not only help protect your skin from the sun but they also taste really good. So enjoy the summer months but remember to eat your photoprotective food.
NCBI Resources
A healthy diet is the cornerstone of good health.�You should maintain a diet�that includes lean meats, fresh fruits and vegetables, and whole grains. The key is choosing fresh, seasonal foods that are local to your area. Foods grown in their season have certain vitamins and minerals that the body needs for the time of year in which they are ripe and ready.
Anti-inflammatory activities of colloidal oatmeal (Avena sativa) contribute to the effectiveness of oats in the treatment of itch associated with dry, irritated skin: https://www.ncbi.nlm.nih.gov/pubmed/25607907
Everyone in the world wants healthy skin. We see it advertised on television with lotions and vitamin supplements. When we exercise and change our eating habits, we see our skin getting firmer with the foods we consume. However, whenever we are stressed, anxious, consuming junk food, or staying out in the sun too long; our skin takes a huge toll on our body. Our skin is the largest organ that covers our entire skeleton structure. When we expose our skin to harsh environments or have skin ailments that we contracted during our birth, our skin is depleted with the certain nutrients that our skin needs.
Glutathione:
Glutathione is known as the �wonder drug� for skin lightening. For some darker toned individuals, it will lighten up their natural melanin. This stigma has been popularized by media influences so people can have �porcelain skin.� However, glutathione actually made up of three amino acids:
Glutamine
Glycine
Cysteine
Melanin
This powerful antioxidant fights off free radicals in our immune system and is compatible with Vitamin E and C. For a natural way to make sure that your body keeps the glutathione nutrients when you get older with age, here are some vegetables that are enriched with glutathione:
Garlic
Onions
Avocado
Cabbage
Okra
Spinach
Kale
Cauliflower
Omega-3:
Omega-3s is one of the most common supplements that is known for healthy skin. This supplement keeps the body healthy as well as preventing inflammation. Omega-3s are mostly in:
Fish
Legumes
Walnuts
Avocados
Eggs
Spinach
But, there are certain limitations on taking Omega-3 supplements if you have a seafood allergy or an egg allergy. People with these types of food allergens can talk with their physician about taking the omega-3 supplements in a pill form in low dosages or eat omega-3 enriched food.
Other patients with omega-3 deficiency have been known to have psoriasis, thus using a topical lotion infused with omega-3s have been known to calm down the inflammation.
Biotin is the three-for-one supplements that target your nails, hair, and skin. This supplement can be found in vitamin pills at your local stores and is highly recommended by dermatologists. However, some people have biotin and zinc deficiency that can be linked to skin abnormalities, thus, biotin plays an important role in our skin health.
You can either take the vitamin pill or incorporate certain food groups like eggs, nuts, whole grains, some dairy products, and certain vegetables in your diet to get the beneficiary nutrients to keep your skin healthy.
Niacin:
Also known as vitamin B3, has been known to support skin health. This nutrient has many beneficial effects to promote skin wellness. It is one of the most essential nutrients we consume since our bodies can�t produce it on their own. Some of the food groups are in the meat department and vegetarian department:
Mushrooms
Potatoes
Legumes
Whole grains
Meat
Fish
Eggs
Milk
Vitamin A:
Vitamin A is filled with nutrients as it contains beta-carotene, thus it is mostly fruits and vegetables that contain this supplement. This supplement plays an important role as it helps repair any skin deficiencies and eye health. Some of the foods that boost up vitamin A are:
Carrots
Broccoli
Cantaloupe
Squash
Vitamin C:
Vitamin C is one of the most top tiers of improving skin health and has many beneficial factors in our immune system. Some patients develop scurvy when they don�t have enough vitamin C in their system. It is mostly found in citrus fruit, which is one of the best ways to consume the vitamin into your system.
But, there is a catch when you are taking vitamin C. Vitamin C when exposed to light, can oxidize and become unstable. So if you are taking the supplement, it should be stored in a dark place and the PH should be at 3.5.
Zinc:
Zinc is one of the supplements that support healthy skin. This micronutrient can protect our skin from the sun and supports our inflammatory system. Some of the food that actually can help us prevent sun damage and give us a zinc supplement boost include seeds, meat, shellfish, dairy and dark chocolate.
When our skin needs these 9 nutrients, they are thanking us for taking the time to get the necessary supplements to make sure our bodies are still functional and that we live a long healthy life. Granted that the media has televised about many ways to promote skin health, but it actually starts with eating the right foods that our body craves. When we eat processed food and ingest artificial sugars into our bodies, we feel sluggish, our skin takes a toll on the lack of nutrients we are not giving and so many health problems that we will face.
Yes, we can take topical creams and lotions to nourish our skin and combat the dryness that our skin faces. But that can only go for so long unless we change our eating styles. Some people may freak out because they hear the word, �diet� and are limited to what they can eat. However, when it�s a health issue and our physicians tell us that we need to eat healthier, we give it a go. Therefore, eating right is a lifestyle choice and it starts with these 9 nutrients to make sure our largest organ is taken care of as well as the rest of our body system. When we cut back on the bad food and focusing on good food, our bodies feel so much better.
NCBI Resources
Living a healthy lifestyle and eating your basic food groups; whether it be plant-based or omnivorous, as well as, exercising a couple of times out of the year. A bad healthy lifestyle is eating processed food and not exercising, which leads to obesity and cardiac arrest. Depending on the person and the efforts that they are willing to maintain a healthy lifestyle, they can achieve longevity by taking care of their gut first and foremost.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine