Any vehicle crash, collision, or accident can cause various injuries, with back pain issues as a primary injury or a side effect from other injuries. Usually, injury symptoms begin right after the collision, but in other cases, individuals may not start experiencing symptoms until hours, days, or even weeks later. This is from the adrenaline that rushes throughout the body during the collision/fight or flight response delaying the injury symptoms. There are reports of individuals who walk away from an accident unscathed but require urgent medical treatment a short while later. Chiropractic care can provide manual and spinal motorized decompression benefits.
Decompression Benefits
Head Injuries
Head injuries occur when drivers and/or passengers hit their heads on the steering wheel, windows, dashboard, metal frame, and sometimes each other.
A head injury is considered a severe condition that can cause concussions, skull fractures, comas, hearing loss, cognitive and memory issues, and vision problems.
A significant head injury can cause extensive and costly medical treatment with the possibility of long-term medical care.
Neck Injuries
Neck injuries are common in vehicle collisions.
The most common is whiplash, with the head and neck-snapping from indirect blunt force, like being rear-ended.
Whiplash can cause significant damage to the ligaments and muscles, like swelling and neck pain, and temporary paralysis of the vocal cords.
Injury patterns of whiplash can differ depending on the speed, force, and overall health of the individual involved.
Back Injuries
Back injuries can range in severity from sprains to significant damage involving the nerves and/or the spinal cord.
If the damage is severe, it can lead to loss of sensation in the body, loss of limb control, or permanent paralysis.
Disc herniation/s can lead to disability, muscle weakness, tingling and numbness in the limbs, and radiating body pain.
Chest and Torso Injuries
Vehicle collision forces can result in severe chest injuries that include broken ribs.
Broken ribs might not sound dangerous by themselves; they can puncture the lungs leading to other injuries and internal bleeding.
The legs, feet, arms, and hands are frequently injured, broken, and sometimes dislocated.
Motorcyclists are also at a higher risk for significant injury that includes:
Multiple fractures, internal injury, head injuries, and severe ligament damage.
Pedestrians struck by a vehicle have an increased risk for a combination of all injuries at once.
Non-Surgical Decompression Benefits
Chiropractors are trained to identify and treat injuries from vehicle collisions.
Non-surgical spinal decompression gently stretches the spine using a motorized traction device to help reposition the spine and remove the pressure.
As the pressure is taken off, the spinal discs regain their natural height, relieving the pressure on the nerves and other spinal structures.
Optimal healing is promoted by an improved circulation of nutrients, water, and oxygen to the injury site.
Decompression helps to strengthen the muscles in the affected area.
It provides positive spinal structural changes.
Improves nervous system function.
Non-surgical decompression is a tool for correcting injuries and relieving pain, allowing optimal health for the individual.
DOC Decompression Table
References
Apfel, Christian C et al. “Restoration of disk height through non-surgical spinal decompression is associated with decreased discogenic low back pain: a retrospective cohort study.” BMC musculoskeletal disorders vol. 11 155. 8 Jul. 2010, doi:10.1186/1471-2474-11-155
Koçak, Fatmanur Aybala et al. “Comparison of the short-term effects of the conventional motorized traction with non-surgical spinal decompression performed with a DRX9000 device on pain, functionality, depression, and quality of life in patients with low back pain associated with lumbar disc herniation: A single-blind randomized controlled trial.” Turkish Journal of physical medicine and rehabilitation vol. 64,1 17-27. 16 Feb. 2017, doi:10.5606/tftrd.2017.154
Macario, Alex, and Joseph V Pergolizzi. “Systematic literature review of spinal decompression via motorized traction for chronic discogenic low back pain.” Pain practice: the Official Journal of World Institute of Pain vol. 6,3 (2006): 171-8. doi:10.1111/j.1533-2500.2006.00082.x
Tremors are extremely rare, but they can result from spinal compression and not necessarily a brain condition like Parkinson’s disease. Tremors are abnormal, involuntary body movements with various causes, most of which are connected to the brain and not the spine. A study reports that more than 75% of individuals with Parkinson’s experienced a resting tremor, and about 60% experience tremors while moving. Sometimes the spine is the contributor caused by compression of the spinal cord.
Spinal Compression Study
A 90-year-old man was hospitalized after having tremors, with Parkinson’s being the initial diagnosis. The tremors progressed to the point where the man could not feed himself or walk without support. The case became the focus of a medical report published by physicians in the Department of Orthopaedic Surgery, Division of the Spine, Singapore Tan Tock Seng Hospital. Along with the tremors, symptoms progressed to:
Difficulty with fine motor skills like buttoning a shirt.
However, it was ruled out because the patient was not presenting with other Parkinson’s symptoms.
For individuals with cervical spondylotic myelopathy tremors, surgery can be used to help the condition. However, with cervical myelopathy, there is often some permanent damage. Individuals have shown that post-surgery and decompression, symptoms still present, maybe not as much, but there will be a need for a symptom management plan.
Prevention
The best way to prevent tremors associated with cervical spondylotic myelopathy is to minimize the strain on the spine that can lead to herniated discs and/or other spinal injuries. The discs in the spine degenerate, dry out and start cracking with age, increasing the risk of rupture. If a tremor develops, contact a doctor, spine specialist, or chiropractor to help diagnose the condition. These doctors can perform physical and neurological tests to determine the cause and treatment options.
Body Composition
Aging Health
Steady weight gain throughout life can lead to adult-onset diabetes. This is partly caused by having more body fat and progressive muscle loss. Loss of skeletal muscle mass is linked to insulin resistance that involves:
The less muscle is available, the less insulin sensitive the body becomes.
As insulin sensitivity decreases, the body becomes more resistant, increasing risk factors for type II diabetes.
This can lead to osteoporosis, where the old bone is reabsorbed more and less new bone is created.
Both men and women can experience decreased muscle mass that can lead to:
Thinner bones
Weaker bones
Increased risk of osteoporosis and severe injury from falls.
To help prevent these issues, it is recommended to:
It is recommended to space out protein intake across meals rather than consuming it all at once. This helps to ensure the proper amount is acquired.
Monitoring body composition regularly can help minimize muscle mass loss and fat mass gain as the body ages.
A regular strength training routine will help strengthen bones muscles and maintain optimal circulation.
References
Heusinkveld, Lauren E et al. “Impact of Tremor on Patients With Early Stage Parkinson’s Disease.” Frontiers in neurology vol. 9 628. 3 Aug. 2018, doi:10.3389/fneur.2018.00628
Jancso, Z et al. “Differences in weight gain in hypertensive and diabetic elderly patients primary care study.” The Journal of nutrition, health & aging vol. 16,6 (2012): 592-6. doi:10.1007/s12603-011-0360-6
Srikanthan, Preethi, and Arun S Karlamangla. “Relative muscle mass is inversely associated with insulin resistance and prediabetes. Findings from the third National Health and Nutrition Examination Survey.” The Journal of clinical endocrinology and metabolism vol. 96,9 (2011): 2898-903. doi:10.1210/jc.2011-0435
Tapia Perez, Jorge Humberto et al. “Treatment of Spinal Myoclonus Due to Degenerative Compression Myelopathy with Cervical Spinal Cord Stimulation: A Report of 2 Cases.” World neurosurgery vol. 136 (2020): 44-48. doi:10.1016/j.wneu.2019.12.170
Sciatica motor vehicle crash. After an automobile crash/accident, symptoms of pain and discomfort can immediately follow the force of impact, indicating an injury. Many injuries and symptoms appear right away, like:
Pain from high-impact trauma and cuts.
Bone fractures.
Dislocations.
Neck whiplash.
Back pain.
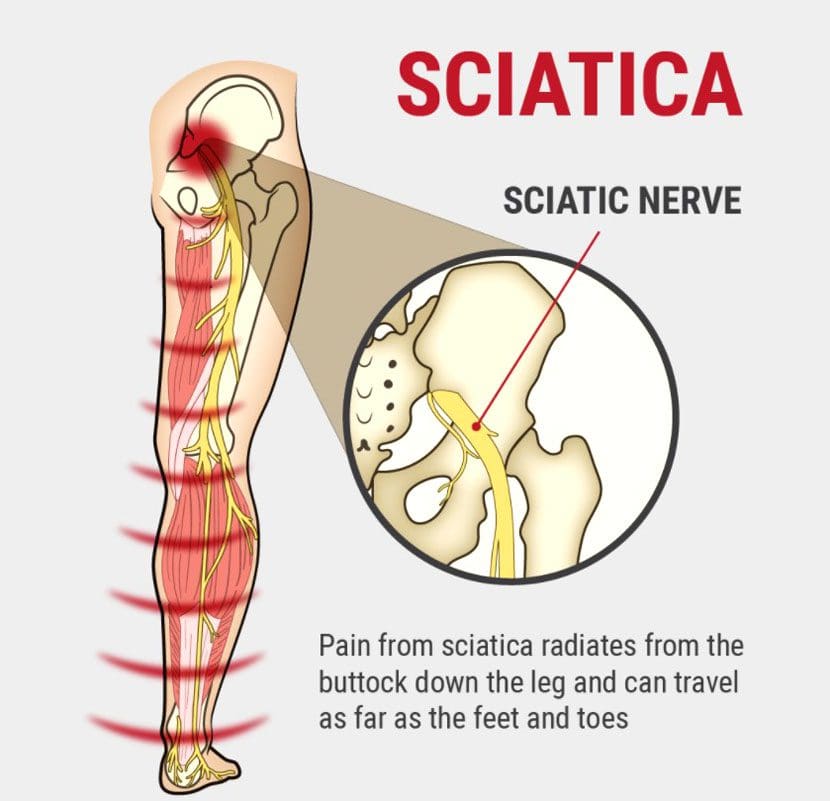
The sciatic nerve is the largest in the body, and any damage can cause pain in one or both sides of the body. Pressure and compression on the nerves, ligaments, and muscles accompanied by weakness or numbness in the lower back, legs, or feet could cause delayed sciatica symptoms hours, days, even weeks later. It is critical to meet with a doctor and auto accident chiropractor after any type of accident, large or small, to develop a thorough personalized treatment plan.
Sciatica Motor Vehicle Crash
Sciatica can be brought on by a pinched nerve, which is often the result of the spine shifting out of place, causing herniation and compression on the sciatic nerve. The trauma from a motor vehicle accident can cause the spinal discs to be knocked out of place, rupture, and leak out, irritating the surrounding tissue and nerve endings. Back injuries are among the most common forms of damage/injury resulting from a motor vehicle accident/crash that can lead to sciatica. Broken and/or fractured vertebral, hip, or pelvis bone fragments can compress the sciatic nerve. Even when the initial result of the impact does not result in sciatica, over time, an untreated back injury could lead to sciatica symptoms.
Symptoms
Motor vehicle crashes often activate or aggravate pre-existing conditions like asymptomatic degenerative disc disease, affecting the sciatic nerve causing discomfort and pain. Common symptoms include:
Mild discomfort or achiness.
Tingling sensations from the lower back and down the back of the leg.
Weakness, numbness, or difficulty moving the leg and foot.
Inability to bend the foot upward at the ankle- known as foot drop.
Constant pain in one side of the buttocks or leg.
Sharp pain that makes it difficult to stand up and walk
Difficulty sitting.
Burning or tingling in one leg can worsen when sitting.
Intense pain.
Sharp burning and/or what feels like shooting electricity pain.
Diagnosis
A spine doctor and chiropractor will use diagnostic imaging tools like X-rays, and CT scans to see the scope of the injured area.
An X-ray will show a detailed image of the spine and affected bones in the area.
A CT scan will include a 3D image that shows the surrounding musculature, tissues, and nerves that could be damaged/injured.
Treatment
The doctor and chiropractor will then develop an appropriate and personalized treatment plan that could utilize various methods and techniques.
Chiropractic is commonly the first treatment to realign the spine and relieve pressure on the nerve.
A pain management specialist or physical therapist will be brought in for rehabilitation/recovery as adjustments progress.
Orthopedists and neurologists may be brought in for less conservative treatment in more severe cases, including surgical options.
Other treatments can include steroid injections or anti-inflammatory medicines to relieve nerve pressure.
Body Composition
Injury Rehabilitation Phase
Current in-clinic methods of measuring the composition of an injured body are indirect, while medically advanced techniques limit the frequency of testing. InBody provides cost-effective, comprehensive, and timely measurements that identify areas of weakness from damage, injury, or recent surgery and develop a customized rehabilitation program to improve functional status.
During the rehabilitation phase, increased sedentary behavior and/or immobilization causes muscle loss in the injured or operated region. By independently evaluating lean mass in each segment of the arms, legs, and torso, a chiropractor or physical therapist gathers baseline information on the body segments with restricted mobility.
InBody can help provide further insight into an individual’s body composition to analyze long-term health risks and develop a personalized exercise intervention to improve overall health and reduce health risks. This provides beneficial information for identifying potential imbalances related to muscle loss post-injury/surgery that can be targeted and improved. Identifying these imbalances allows the therapists to increase functional fitness and mobility, helping the individual reduce the risk of re-injury or new injuries.
References
Defouilloux, B et al. “A propos de trois observations chez des polytraumatisées de la route présentag une fracture du bassin associée à des signes neurologiques” [Apropos of 3 cases of multiple traffic injuries presenting pelvic fractures associated with neurologic signs]. Journal de radiologie, d’electrologie, et de medecine nucleaire vol. 48,8 (1967): 505-6.
Noble, J et al. “Analysis of upper and lower extremity peripheral nerve injuries in a population of patients with multiple injuries.” The Journal of trauma vol. 45,1 (1998): 116-22. doi:10.1097/00005373-199807000-00025
Walsh, K et al. “Risk of low back pain in people admitted to hospital for traffic accidents and falls.” Journal of epidemiology and community health vol. 46,3 (1992): 231-3. doi:10.1136/jech.46.3.231
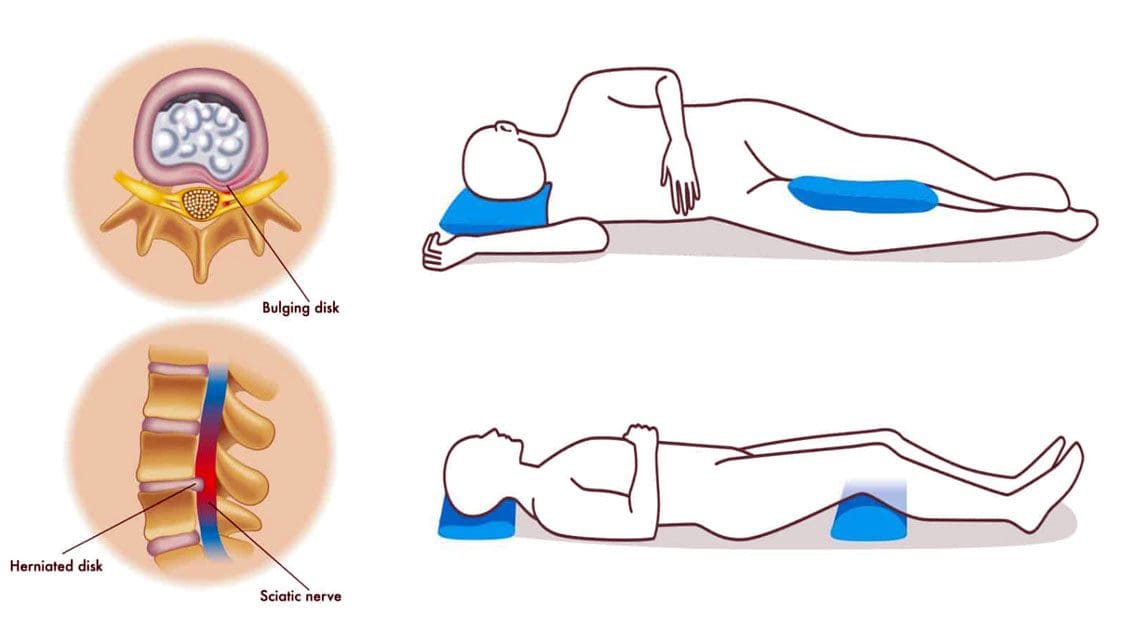
Sleeping with a bulging disc can be challenging for the body to achieve the proper rest. And sleeping in an awkward position can add stress to the spine, making the bulge worse, which can cause tingling, numbness, pain, and digestive problems. This can disrupt the sleep cycle and prevent proper healing of the spinal injury.
Sleeping With a Bulging Disc
When sleeping, most back pain occurs in the lumbar or lower back, in one of two places where the spine meets the pelvis. Around 95% of lower back herniations happen in the L4-L5 spinal segment or the L5-S1 Lumbosacral joint. Any back pain can turn into a vicious cycle of:
Sleeping with a bulging disc requires maintaining the ears, shoulders, and hips aligned to keep the spine aligned.
Sleeping on The Back
Back sleeping done correctly is the best way to sleep for the spine’s health. The important thing is to ensure the entire back is supported when sleeping. If there is a gap or space between the mattress and the back, the weight and gravity force the spine to lower in an unnatural way to fill the space. This can cause back muscle soreness, injury, and sciatica. A thin pillow, blanket, or towel can be used to fill the space, giving the spine the support it needs. Back sleepers can also benefit from a pillow or two under the knees to elevate the legs and help maintain the natural curve of the pine.
Sleeping on The Side
Side sleepers can try pulling the legs up toward the chest, and placing a pillow between the knees can provide relief when sleeping with a bulging disc. Pulling the legs up in the fetal position can relieve pressure on the discs. It is recommended to switch sides to keep the spine balanced. This helps maintain hip alignment, which helps keep the spine in a neutral position.
Sleeping On The Stomach
It is recommended to avoid sleeping on the stomach. This pulls the spine down into an unnatural curve that can cause and exacerbate back pain. For individuals that naturally stomach sleep, it is recommended to place a pillow under the hips and lower abdomen to prevent unnatural spinal positioning.
Chiropractic Relief
Utilizing the right sleeping position can provide pain relief and thorough rest. However, sleeping with a herniated disc is far from what is needed to get back to a normal healthy sleeping pattern. This depends on the location of the bulging disc, severity, and cause. A chiropractor can:
Help the individual develop an optimal sleeping routine and positioning.
Body Composition
Sleep and Growth Hormone In Children
Growth, in all ages, is primarily controlled by growth hormone. The hormone is regulated by the hypothalamus and pituitarygland which plays an important role in sleep. Growth hormone has been found:
It peaks during the beginning of deep sleep.
There are multiple smaller peaks during the other stages of sleep.
Those who have a delay at the beginning of deep sleep have delayed rises in growth hormone levels.
For children to grow they need to have proper levels of growth hormone. This means they need to have the proper amount of sleep for proper body composition. Research has found that increased levels of sleep resulted in less overall fat mass and a reduced percentage of body fat allowing their bodies to grow.
References
Al Qaraghli MI, De Jesus O. Lumbar Disc Herniation. [Updated 2021 Aug 30]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560878/
Desouzart, Gustavo et al. ‘Effects of Sleeping Position on Back Pain in Physically Active Seniors: A Controlled Pilot Study. 1 Jan. 2016: 235 – 240.
Kose, Gulsah et al. “The Effect of Low Back Pain on Daily Activities and Sleep Quality in Patients With Lumbar Disc Herniation: A Pilot Study.” The Journal of neuroscience nursing: Journal of the American Association of Neuroscience Nurses vol. 51,4 (2019): 184-189. doi:10.1097/JNN.0000000000000446
Sener, Sevgi, and Ozkan Guler. “Self-reported data on sleep quality and psychologic characteristics in patients with myofascial pain and disc displacement versus asymptomatic controls.” The International Journal of prosthodontics vol. 25,4 (2012): 348-52.
Sciatic nerve injury happens from trauma to the nerve and can cause numbness, tingling, loss of muscle power, and pain. The traumatic experience can be a muscle spasm that pulls and/or pinches the sciatic nerve, force/pressure impact injury, over-stretching injury, or a laceration/cutting injury. A slipped disk, or herniated disk, is the most common cause of irritation on the sciatic nerve. A slipped disk occurs when one becomes slightly dislodged, pushing out from the spine. This places pressure/compression on the sciatic nerve.
Trauma to the lower back, buttocks, or leg from an automobile accident, sports injury, work injury.
Medical treatment causes:
Direct surgical trauma.
Total hip replacement surgery can cause nerve compression and stretch during the procedure, causing damage to the sciatic nerve resulting in dysfunction.
Injection injuries via intramuscular injection in the gluteal region. This is a situation where there is a loss of movement and or lack of sensation at the affected lower extremity with or without pain.
Injection palsy can begin suddenly or hours following damage to the sciatic nerve.
A misplaced intramuscular injection at the gluteal region is the most common cause of injury. It is attributed to frequent injections or poor techniques resulting from inadequately trained or unqualified staff.
Complaints of radiating pain in the leg, which follows a sensory nerve pattern.
Pain radiates below the knee, into the foot.
Complaints of low back pain, which is often less severe than leg pain.
Report of electrical, burning, numbing sensations.
Diagnosis
A detailed subjective and objective physical examination is necessary to figure out the severity of the sciatic nerve injury. Diagnostic studies include:
Chiropractic and physical therapy exercises and stretches improve nerve regeneration after nerve damage.
Electrical Muscle Stimulation
TENS and Electroacupuncture have been shown to help enhance nerve regrowth.
Bio-laser stimulation can help with nerve nutrition and regeneration.
Joint or Soft Tissue mobilization
Helps to retain muscle, nerve, and soft tissue flexibility and prevent deformity.
Balance Training
Coordination, strength, and flexibility exercises help to restore balance.
Splinting
In the early stages after a sciatic nerve injury, bracing may be needed to prevent deformity and new injury or re-injury risks.
Ankle Foot Orthosis – AFO can help prevent foot drop, muscle damage, and falls risk.
Body Composition
Optimize Diet for Fat Loss
Individuals that want to lose fat need to create a calorie deficit. Individuals need to consistently eat less than they need for Total Daily Energy Expenditure – TDEE. The safest way to handle a caloric reduction is to reduce calorie intake in small doses like 200-300 calories, for example. After a week or two, perform a body composition analysis. If Fat Mass numbers begin to drop or not, adjust calorie needs accordingly. Restricting calories is the most common way, a deficit can also be created by increasing calorie needs through exercise.
References
Kline, D G et al. “Management and results of sciatic nerve injuries: a 24-year experience.” Journal of neurosurgery vol. 89,1 (1998): 13-23. doi:10.3171/jns.1998.89.1.0013
Schmalzried, TP et al. “Update on nerve palsy associated with total hip replacement.” Clinical Orthopedics and related research,344 (1997): 188-206.
Shim, Ho Yong et al. “Sciatic nerve injury caused by a stretching exercise in a trained dancer.” Annals of rehabilitation medicine vol. 37,6 (2013): 886-90. doi:10.5535/arm.2013.37.6.886
Suszyński, Krzysztof et al. “Physiotherapeutic techniques used in the management of patients with peripheral nerve injuries.” Neural regeneration research vol. 10,11 (2015): 1770-2. doi:10.4103/1673-5374.170299
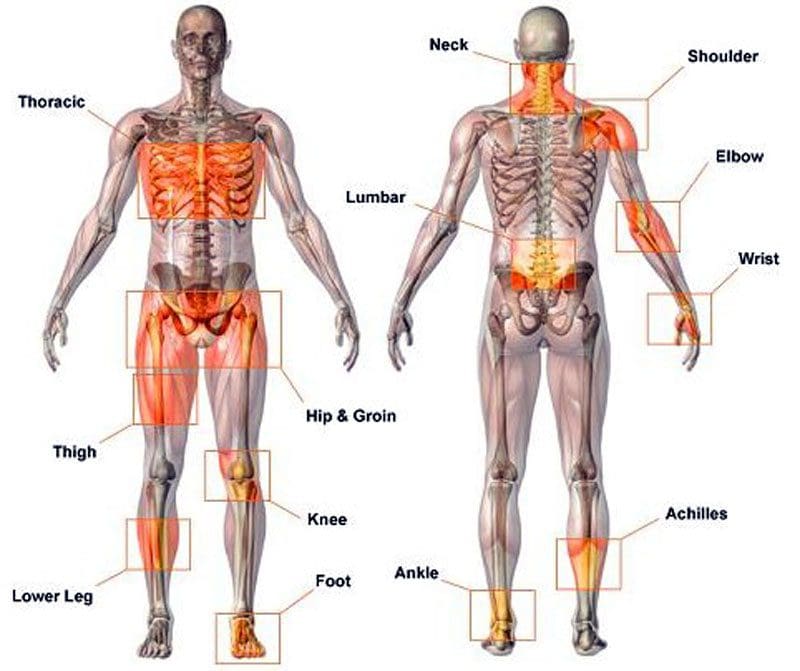
Musculoskeletal Disorders, or MSDs, are injuries, conditions, and disorders that affect the body’s musculoskeletal system. It includes the muscles, tendons, ligaments, nerves, discs, blood vessels, bones, and joints. MSDs are common, and the risk of developing them increases with age. The severity of an MSD can vary. They cause discomfort, recurrent pain, stiffness, swelling, and aching that interfere with everyday activities. Early diagnosis and treatment can alleviate symptoms and improve long-term health. Common disorders include:
The term musculoskeletal disorder is used as it accurately describes the injury or condition. Other terms used are repetitive motion injury, repetitive stress injury, and overuse injury. When individuals are exposed to MSD risk factors, they begin to fatigue. This can start a musculoskeletal imbalance. With time, fatigue completely overtakes recovery/healing, and the musculoskeletal imbalance continues, a musculoskeletal disorder develops. The risk factors are broken into two categories: work-related/ergonomic risk factors and individual-related risk factors.
Ergonomic Factors:
Force
Repetition
Posture
High Task Repetition
Many work tasks and cycles are repetitive and are typically controlled by hourly or daily production targets and work processes.
High task repetition combined with other risks factors like high force and/or awkward postures can contribute to the formation of MSD.
A job is considered highly repetitive if the cycle time is 30 seconds or less.
Forceful Exertions
Many job tasks require high force loads on the body.
Muscle effort increases in response to high force requirements. This increases associated fatigue.
Repetitive or Sustained Awkward Postures
Awkward postures place excessive force on joints, overload the muscles and tendons around affected joints.
The joints of the body are most efficient when they operate close to the mid-range motion of the joint.
The risk of MSD is increased when the joints are worked outside of this mid-range repetitively for sustained periods without a proper amount of recovery time.
Individual Factors
Unhealthy work practices
Lack of physical activity/fitness
Unhealthy habits
Poor diet
Unhealthy Work Practices
Individuals that engage in poor work practices, body mechanics, and lifting techniques are introducing unnecessary risk factors.
These poor practices create unnecessary stress on the body that increases fatigue and decreases the body’s ability to recover properly.
Poor Health Habits
Individuals who smoke, drink excessively, are obese, or exhibit numerous other poor health habits put themselves at risk for musculoskeletal disorders and other chronic diseases.
Insufficient Rest and Recovery
Individuals that do not get adequate rest and recovery put themselves at higher risk.
MSDs develop when fatigue outruns the individual’s recovery system, causing a musculoskeletal imbalance.
Poor Diet, Fitness, and Hydration
Individuals who eat unhealthily are dehydrated, at a poor level of physical fitness, and do not take care of their bodies are putting themselves at a higher risk of developing musculoskeletal and chronic health problems.
Causes
The causes of musculoskeletal disorders are varied. Muscle tissue can be damaged with the wear and tear of daily work, school, and physical activities. Trauma to the body can come from:
Postural strain
Repetitive movements
Overuse
Prolonged immobilization
Jerking movements
Sprains
Dislocations
Falling injuries
Auto accident injuries
Fractures
Direct trauma to the muscle/s
Poor body mechanics can cause spinal alignment problems and muscle shortening, causing other muscles to be strained, causing problems and pain.
Treatment Rehabilitation
A doctor will recommend a treatment plan based on the diagnosis and severity of the symptoms. They may recommend moderate exercise and over-the-counter medications like ibuprofen or acetaminophen to address occasional discomfort or pain. They often recommend chiropractic and physical therapy rehabilitation to learn how to manage pain and discomfort, maintain strength, range of motion, and adjust everyday activities. Different types of manual therapy, or mobilization, can treat body alignment problems. A doctor may prescribe medications like nonsteroidal anti-inflammatories NSAIDs to reduce inflammation and pain for more severe symptoms. For individuals with musculoskeletal disorders like fibromyalgia, medications to increase the body’s level of serotonin and norepinephrine may be prescribed in low doses to modulate sleep, pain, and immune system function.
Body Composition
Types of Pain
Pain can be grouped into three categories:
Early Warning Pain
This is most recognizable after having just touched a pan, and the hand jerks away before realizing how hot the pan is, also known as the withdrawal reflex.
This is a protective mechanism that helps avoid danger and is vital for survival.
Inflammatory Pain
This type of pain happens after an injury or surgery while the body is healing and recovering.
Inflammation prevents the body from performing movements to prevent and avoid re-injury.
Pathological Pain
This type of pain can happen after the body has healed, but the nervous system has been damaged.
This is often the case with individuals who sustain an injury and inform doctors that the injured area is never the same.
If the rehabilitation does not correctly heal the nervous system, protective pain measures can generate a false alarm causing pain signals to fire off.
References
Asada, Fuminari, and Kenichiro Takano. Nihon eiseigaku zasshi. Japanese journal of hygiene vol. 71,2 (2016): 111-8. doi:10.1265/jjh.71.111
da Costa, Bruno R, and Edgar Ramos Vieira. “Risk factors for work-related musculoskeletal disorders: A systematic review of recent longitudinal studies.” American journal of industrial medicine vol. 53,3 (2010): 285-323. doi:10.1002/ajim.20750
Malińska, Marzena. “Dolegliwości układu mięśniowo-szkieletowego u operatorów komputerowych” [Musculoskeletal disorders among computer operators]. Medycyna pracy vol. 70,4 (2019): 511-521. doi:10.13075/mp.5893.00810
Musculoskeletal system diseases. (n.d.). dmu.edu/medterms/musculoskeletal-system/musculoskeletal-system-diseases/
Roquelaure, Yves et al. “Troubles musculo-squelettiques liés au travail” [Work-related musculoskeletal disorders]. La Revue du praticien vol. 68,1 (2018): 84-90.
Villa-Forte A. (n.d.). Diagnosis of musculoskeletal disorders. merckmanuals.com/home/bone,-joint,-and-muscle-disorders/diagnosis-of-musculoskeletal-disorders/introduction
Sciatica Causes: The sciatic nerve forms by the union of Lumbar4 to Sacral31 nerve roots and exits the pelvis through the greater sciatic foramen, below the piriformis muscle located deep in the buttocks. The nerve runs down the back of the thigh, into the leg, and ends in the foot. The sciatic nerve becomes inflamed, irritated, and/or mechanically compressed. Any type of pain and/or neurological symptom/s from the sciatic nerve is referred to as sciatica. Sciatica is a type of lumbar radiculopathy, which means that the pain originates from the low back and/or sacral nerve roots.
Sciatica Causes
Physical forces on the nerve can cause mechanical compression due to the following conditions:
Herniated Discs
A disc in the lower back can bulge or herniate, causing irritation and/or compression of a sciatic nerve root.
Foraminal Stenosis
Stenosis, the intervertebral opening through which the nerve roots travel, begins to narrow/close in, can compress or irritate the sciatic nerve.
Degeneration
Degenerative changes in the spine like the thickening of facet joint capsules and/or ligaments can compress the sciatic nerve.
Segmental Instability
Instability of a spinal vertebral segment that happens if one vertebra slips over the one beneath it – spondylolisthesis
Complete dislocation of one or more vertebrae can compress the nerve root/s of the nerve.
Other Sciatica Causes
Tumors, cysts, infections, or abscesses in the lower spine or pelvic region can also cause sciatic nerve compression.
Chemical Inflammation
Chemical irritants can include hyaluronic acid and/or fibronectin/protein fragments that leak out of degenerated or herniated discs. These irritants can cause inflammation and/or irritation of the sciatic nerve.
Degenerated discs can cause nerve tissues to grow into the disc, penetrating the outer and inner layers of the disc, causing sciatica. Immune system responses can contribute to pain when exposed to disc fluid.
Substances such as glycosphingolipids/fats and neurofilaments /protein polymers secreted by the immune system are increased in individuals with sciatica. These substances are released from the reaction between nerve roots and exposed disc material, causing inflammation.
Job Occupation
Individuals with specific jobs have an increased risk of developing sciatica. Examples include:
Truck drivers
Desk workers
Teachers
Warehouse workers
Machine workers
Plumbers
Electricians
Carpenters
Fitness trainers
Sitting and standing for long periods, using improper posture, constantly bending, twisting, reaching, and regularly lifting are risk factors for sciatica.
Piriformis Syndrome
Piriformis syndrome is a condition where the piriformis muscle swells and spasms from overuse or inflammation irritating the sciatic nerve that is right underneath. The nerve can get trapped in the muscle causing sciatica-like symptoms that include:
Pain follows the same pattern in the leg as a compressed sciatic nerve root.
Tingling
Numbness
Discomfort from piriformis syndrome feels similar to sciatica, but it is not caused by compressed sciatic nerve root. Piriformis pain comes from compression of the sciatic nerve near the piriformis muscle.
Genetic Sciatica Causes
Sciatica caused by degenerated and/or herniated discs can be genetic. Research has shown that certain genetic factors are more prevalent in individuals with back and spinal problems. These congenital disabilities can cause the discs to become weak and susceptible to external stress. With time the proteins in the disc break down, compromising the integrity and function.
Arthritis and Joint Issues
Arthritis or other inflammatory conditions around the hip joint can cause pain down the leg, similar to sciatica. This is referred pain that spreads out from the source and is not radicular nerve pain that originates in the nerve roots.
Conditions like sacroiliac joint dysfunction or sacroiliitiscan cause sciatica-like pain that runs down the back of the thigh but usually ends before or at the knee.
The pain can be acute and debilitating, like sciatica but is caused by an abnormal motion or malalignment of the sacroiliac joint.
Body Composition
Normal Cholesterol Ranges
High cholesterol can lead to severe consequences when left untreated, but it can be difficult to spot with no noticeable warning signs. This is why it’s essential to monitor cholesterol levels with blood tests, especially if there is an increased risk. Example of normal cholesterol levels for adults 20 years of age or older:
Total cholesterol 125-200 mg/dL
LDL <100 mg/dL
HDL >40 mg/dL men, >50 mg/dL women
Lifestyle
Lack of physical activity contributes to high cholesterol levels.
Diets that mainly consist of processed foods and saturated fats increase the risk of high LDL levels.
Smoking can lower HDL levels.
Aging
Individual risk for developing high cholesterol tends to increase as the body advances in age. This is why it is recommended to have regular physicals and blood tests.
Genetics
Some individuals are more genetically predisposed to developing high cholesterol and heart disease.
Knowing family medical history can help predict whether it may become a problem.
References
Davis D, Maini K, Vasudevan A. Sciatica. [Updated 2021 Sep 2]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507908/
Giuffre BA, Jeanmonod R. Anatomy, Sciatic Nerve. [Updated 2021 Jul 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482431/
Hicks BL, Lam JC, Varacallo M. Piriformis Syndrome. [Updated 2021 Jul 18]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448172/
Raj MA, Ampat G, Varacallo M. Sacroiliac Joint Pain. [Updated 2021 Aug 30]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470299/
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine