Everybody all over the world suffers from some headache. It can come in various forms, and the pain can range from a dull ache that can go away in a few hours to an excruciating throbbing pain that can make a person stay in bed all day and last for weeks. Headaches can also cause muscle tension on the neck and can dampen a person’s daily life if it is not treated right away. Luckily the use of cervical decompression therapy can help alleviate any pain that the cervical spine is suffering from and can cause instant relief to many individuals suffering from headaches. This article looks at different types of headaches, including migraines, and how cervical decompression therapy can help relieve migraine headaches for many individuals. By referring patients to qualified and skilled providers specializing in spinal decompression therapy. To that end, and when appropriate, we advise our patients to refer to our associated medical providers based on their examination. We find that education is the key to asking valuable questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions, please call Dr. Jimenez at 915-850-0900.
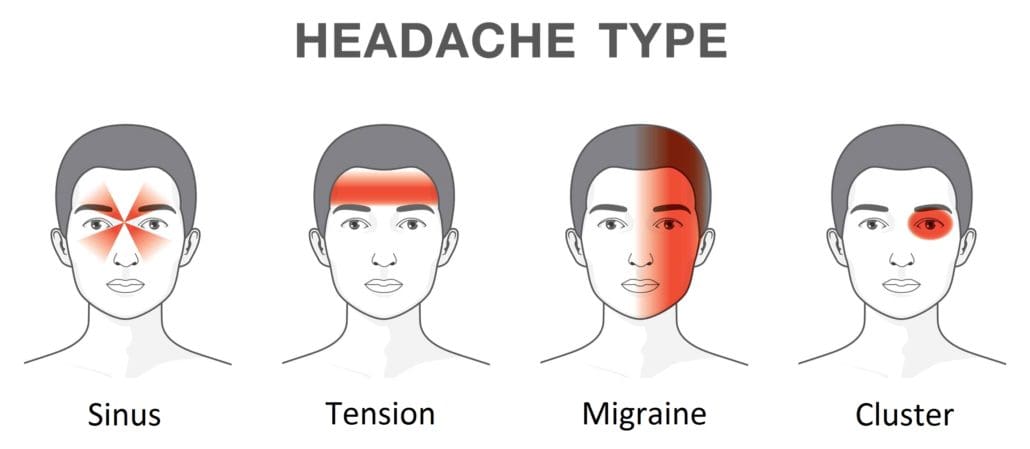
Different Forms Of Headaches
Have you ever felt excruciating throbbing pain from the forehead that becomes a nuisance throughout the day? How about tension and pain on either side of the face that constantly pounds that laying in a dark, quiet room can only be the cure? Or turning your head causes muscle restriction on the neck and limits the range of motion? These are the many forms of headaches that can affect anybody on any given day. Research studies have defined headaches as pain from various disorders that usually affect the cervical spine. These disorders can range from muscle tension around the neck, being overly stressed, having an inadequate sleep, to wearing something tight around the head. Having headaches in their acute form can last for a few hours until they dissipate, but their chronic condition can cause severe neck and cervical spine issues.
When a person starts to feel pain in their neck, it can cause them to have a limited range of motion and cause reoccurring headaches known as cervicogenic headaches. Research studies have shown that cervicogenic headaches are mainly caused when the cervical root is compressed on the lower parts of the cervical spine, causing cervical radiculopathy. When this happens, it can cause many individuals to have neck pain and headaches from the neck to the head. Cervicogenic headaches can limit a person’s range of motion when they turn their head and irritate the cervical nerve root spread out from the neck to the shoulders.
Migraine Headaches
Have you ever felt a severe headache that makes you feel nauseated and become sensitive to light and that you only feel relief by just laying down in a dark, quiet room? This type of headache is known as a migraine, and research studies classified migraines as headaches with moderate to severe episodes considered unilateral. Having migraines can affect a person’s quality of life as they can last from a few days to a few weeks, depending on how severe the migraine is. Other research studies have shown that since migraines are the commonest causes of severe headaches, the pain is accompanied by a constellation of symptoms that can affect the body and the neck. Some of the common symptoms that are accompanied by migraines are:
Non-surgical Decompression Therapy For Cervical Spine- Video
Still feeling excruciating pain from the neck, and it is causing you headaches? How about a limited range of motion when turning your head? Well, cervical decompression therapy could be the answer to alleviating headaches and neck pain. The video above shows what cervical decompression therapy does by using the DRX9000. Cervical decompression allows the individual to lay on a traction table, strapping their head. In contrast, the traction table gently stretches the cervical spine to enable the compressed spinal discs to return to their original form and relieve the pressure on the cervical nerve root. This will alleviate neck pain symptoms like muscle stiffness and help treat severe headaches like migraines. If you want to learn more about spinal decompression therapy, this link will explain the benefits of spinal decompression and how it can alleviate cervical pain symptoms.
Cervical Decompression Therapy For Relieving Migraines
Finding any kind of relief for migraines usually involves a quiet, dark room to minimize the associated symptoms that can dampen a person’s day. Since research studies have stated that when the greater occipital nerve is being entrapped and compressed, it can actually cause the posterior part of the head excruciating pain. This can affect the upper parts of the cervical spine and cause migraines to become much worst. The best way to get the pressure off the greater occipital nerve and the cervical spine nerve root is through cervical decompression therapy.
Research studies have shown that cervical decompression has often been used to help treat many individuals suffering from neck pain. What cervical decompression does, is that it allows traction to be utilized on the cervical spine causing the muscles, tendons, and ligaments that encompass the cervical spine to be gently stretched. This will cause them to relax and reduce the sensory fibers’ pain transmission, causing instant relief. This gentle stretching from cervical decompression takes the compressed disc from the cervical spine and releases the pressure of the cervical nerve root, thus alleviating severe headaches like migraines.
Conclusion
When a person has a headache and neck pain, it can affect a person’s quality of life. Having headaches can dampen a person’s quality of life, depending on the severity. Headaches can range from a dull ache like a cluster headache to excruciating throbbing pain like a migraine. Luckily cervical decompression therapy allows the individual to have their cervical spine be gently stretched and takes the pressure off the cervical nerve root. This will cause the cervical spinal discs to be decompressed and allow an increase in disc height, alleviating the symptoms that are causing a person to have migraines and headaches. Incorporating cervical decompression therapy as part of your wellness journey will give you the relief you need to get by with your daily activities.
References
Bogduk, Nikolai. “The Neck and Headaches.” Neurologic Clinics, U.S. National Library of Medicine, Feb. 2004, https://pubmed.ncbi.nlm.nih.gov/15062532/.
Eskilsson, Anja, et al. “Decompression of the Greater Occipital Nerve Improves Outcome in Patients with Chronic Headache and Neck Pain – a Retrospective Cohort Study.” Acta Neurochirurgica, Springer Vienna, Sept. 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8357752/.
Lee, Chang-Hyung, et al. “The Functional and Morphological Changes of the Cervical Intervertebral Disc after Applying Lordotic Curve Controlled Traction: A Double-Blind Randomized Controlled Study.” International Journal of Environmental Research and Public Health, MDPI, 19 June 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6617374/.
Persson, Liselott C G, et al. “Headache in Patients with Cervical Radiculopathy: A Prospective Study with Selective Nerve Root Blocks in 275 Patients.” European Spine Journal: Official Publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society, Springer-Verlag, July 2007, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2219654/.
Pescador Ruschel, Marco A, and Orlando De Jesus. “Migraine Headache – Statpearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing, 30 Aug. 2021, https://www.ncbi.nlm.nih.gov/books/NBK560787/.
Weatherall, Mark W. “The Diagnosis and Treatment of Chronic Migraine.” Therapeutic Advances in Chronic Disease, SAGE Publications, May 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4416971/.
Posture is the positioning of the body. There are two types of posture. Dynamic posture is how individuals position themselves when moving, like walking, running, or bending to lift an object. And static posture is how individuals position themselves when not in motion, like standing, sitting, or sleeping. Minimal stress is applied to the muscles and joints when practicing healthy posture. High-stress work and school combined with unhealthy body positions can cause health consequences to the spine, extremities, and musculoskeletal imbalances.
Health Consequences
Poor postures do not always present with spine or extremity pain right away. This is because individuals will feel discomfort and have the strength and mobility to correct unhealthy/awkward positions and minimize stress. However, eventually, the pain will begin to present as the muscles and joints can only take so much that the ability to correct poor positioning does not matter as there is a developing injury taking place, causing inflammation, letting the body know there is something not right. This often leads to chronic stress and the unnecessary wearing down of the joints to compensate for the unhealthy positions.
Early Signs
Early signs of postural problems can include:
Inability to sit or stand for a long time.
Stiffness when rising from a chair.
Feeling of added physical exhaustion.
Leaving the condition untreated often leads to:
Muscle imbalances.
Loss of normal flexibility.
Discomfort and pain present for no apparent reason.
Unhealthy Posture Symptoms
Symptoms can include:
Slouching
Rounded shoulders.
Potbelly.
Bent knees when standing or walking.
Muscle fatigue.
Aches and pains.
Back pain.
Headache.
Postural Structure
Poor posture interferes and disrupts several of the body’s posture structures. These include:
The static slow-twitch muscle fibers help maintain posture without exerting too much energy and contribute to balance by sensing the body’s position.
Static muscle fibers burn energy slowly and can work for a long time without tiring.
The fast-twitch or phasic muscle fibers are used for movement and activity. These fibers quickly use up their energy.
Because the phasic fibers have to work overtime instead of the static fibers to maintain the body’s position, muscle fatigue, weakness, and pain begin to set in.
Health
Health consequences can include:
Misaligned musculoskeletal system.
The advanced wearing of the spine making it fragile and prone to injury.
Chronic pain.
Decreased flexibility.
Joint mobility is affected.
Balance issues.
Increased risk of falling.
Difficulty digesting food.
Difficulty breathing.
Chiropractic and Physical Therapy
Chiropractors and physical therapists specialize in evaluating and treating musculoskeletal dysfunctions and disorders, identifying and screening for postural dysfunction. Chiropractic adjustments can be highly effective combined with other treatment modalities like massaging the soft tissues to improve circulation, reduce swelling inflammation, and promote healing. Spinal decompression therapy can help stretch and realign the spine to relieve back and/or leg pain. A customized exercise program will stretch and strengthen the body to maintain a healthy posture. Health coaching combined with dietary management can help with pain and inflammation and strengthen muscles and bones.
DRX9000 Spinal Decompression
References
American Chiropractic Association. Maintaining good posture. https://acatoday.org/content/posture-power-how-to-correct-your-body-alignment. Accessed Jan. 28, 2019.
American Academy of Orthopaedic Surgeons. Spine basics. https://orthoinfo.aaos.org/en/diseases–conditions/spine-basics/. Accessed Jan. 30, 2019.
Bauer BA. Chiropractic or osteopathic manipulation. In: Mayo Clinic Guide to Integrative Medicine. Rochester, Minn.: Mayo Foundation for Medical Education and Research; 2017.
Muscolino JE. Posture and the gait cycle. In: Kinesiology: The Skeletal System and Muscle Function. 3rd ed. Elsevier; 2017.
Wang G. Powered traction devices for intervertebral decompression: Health technology assessment update. Washington Department of Labor and Industries, June 14, 2004.
Waters, Thomas R, and Robert B Dick. “Evidence of health risks associated with prolonged standing at work and intervention effectiveness.” Rehabilitation nursing: the official journal of the Association of Rehabilitation Nurses vol. 40,3 (2015): 148-65. doi:10.1002/rnj.166
Do you ever get that stiff feeling just by turning your head, or do your shoulders start to feel tense after a stressful day at work? How about feeling a headache coming on for no apparent reason? This is due to neck pain, and many factors can cause a person to have neck pain. Even though neck pain can be a nuisance to many individuals, there are therapeutic ways to alleviate neck pain: one of them is cervical decompression therapy. This article will look at what neck pain is, its symptoms, and how decompression therapy can help alleviate neck pain for many individuals. By referring patients to qualified and skilled providers specializing in spinal decompression therapy. To that end, and when appropriate, we advise our patients to refer to our associated medical providers based on their examination. We find that education is the key to asking valuable questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions, please call Dr. Jimenez at 915-850-0900.
What Is Neck Pain?
As part of the cervical spine, the neck supports the head while surrounding and protecting the spinal cord and allows a wide range of motion. Research studies have found that the neck has a coordinated network of nerves, bones, joints, and muscles that have an essential job but have several problems that can cause pain. Neck pain is a common complaint among many individuals, as the neck muscles are strained for long periods due to poor posture. Other research studies have found any injuries or conditions affecting the neck, causing a restricted range of motion. This can be scary for many individuals due to being hunched over by looking at their phones, being on the computer, even minor things like reading a book or suffering from an auto accident, and having rheumatoid arthritis can affect the neck.
The Symptoms For Dealing With Neck Pain
Pain can come in two types of forms, which are acute and chronic. Acute pain can become a dull, mild ache that can last from a few hours to a few days, depending on where the person is injured. Chronic pain, however, can become a nuisance as it can send constant radiating pain that can cause a hindrance to any part of the body. As research has shown, the pain can vary for neck pain as it can become mild and uncomfortable to excruciating, where excess movement can make it worst. Some of the most common neck pain symptoms usually involve:
Even though neck pain can become a nuisance for many individuals, there are ways to alleviate the symptoms of neck pain and provide relief.
Cervical Decompression Therapy-Video
Research studies have found that manipulation, stretching, and strengthening of the neck muscle can reduce the chronic pain symptoms that it has caused. The video above shows what cervical decompression does for many individuals suffering from cervical pain and neck pain. Cervical decompression therapy lets individuals lay their heads on the traction table and are strapped in. The traction machine gently stretches the cervical spine to release the compressed spinal disc. Cervical decompression therapy allows the compressed spinal nerve roots to be alleviated from the cervical spine. It will enable the beneficial oxygen to come back into the spinal disc and increase the disc height for the neck. If you want to learn more about spinal decompression therapy, this link will explain the benefits of spinal decompression and how it can alleviate low back pain symptoms.
How Can Decompression Therapy Help With Neck Pain
As stated earlier in the article, feeling stiffness when turning your head, feeling the tension in the shoulders, and having headaches pop up out of nowhere is scary when you don’t know how they happened. When these symptoms start to turn into chronic issues, it can be hard to find relief to get rid of the pain. Luckily there is a solution for alleviating neck pain, and cervical decompression therapy could help get rid of the pain. Cervical decompression therapy allows individuals to lay their heads on the traction table and be strapped in, causing the traction machine to stretch the neck to alleviate the painful symptoms gently. Research studies have found that cervical decompression therapy can relieve tension headaches and improve the range of motion. This will cause the spinal disc to be stretched and alleviate symptoms caused by cervical herniated discs. Combined with light stretching, cervical decompression therapy can also improve cervical disc herniation symptoms. Research shows that this combination of treatments promotes neuromuscular tissue edema and inflammatory absorption from the cervical herniated disc. This will allow the restoration of the curvature of the cervical vertebrae and reduce disc pressure by improving it.
Conclusion
Having any neck pain is a nuisance, and if it is not treated right away, it can become an issue over time. Neck pain can cause stiffness to the neck muscles and disrupt the range of motion, making it unbearable for the individual to turn their heads from left to right and up and down. Luckily treatments like cervical decompression therapy allow individuals to feel relief from neck pain. Cervical decompression therapy provides traction to the individual by stretching the neck ligament gently to release the compressed cervical spinal discs and will enable the reduction of pain that is causing discomfort to the neck. When this happens, many individuals suffering from neck pain will feel instant relief and an improvement in their range of motion from their necks.
References
Binder, Allan I. “Neck Pain.” BMJ Clinical Evidence, BMJ Publishing Group, 4 Aug. 2008, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2907992/.
Landers, Merrill R, et al. “Anterior Cervical Decompression and Fusion on Neck Range of Motion, Pain, and Function: A Prospective Analysis.” The Spine Journal: Official Journal of the North American Spine Society, U.S. National Library of Medicine, Nov. 2013, https://pubmed.ncbi.nlm.nih.gov/24041918/.
Staff, Mayo Clinic. “Neck Pain.” Mayo Clinic, Mayo Foundation for Medical Education and Research, 31 July 2020, https://www.mayoclinic.org/diseases-conditions/neck-pain/symptoms-causes/syc-20375581.
Xu, Qing, et al. “Nonsurgical Spinal Decompression System Traction Combined with Electroacupuncture in the Treatment of Multi-Segmental Cervical Disc Herniation: A Case Report.” Medicine, Lippincott Williams & Wilkins, 21 Jan. 2022, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8772752/.
The body can bend, twist, turn, and move without pain, while the spine allows the body to be held upright. When the body gets injured, and the spine starts to feel pain from the ligaments, the nerve root, the spinal discs, and the spinal cord, it can cause either leg pain, back pain, or both depending on the severity. The pain can range from a dull, mild ache to a sudden, sharp shooting pain that can radiate from the leg to the feet. Luckily there are many treatments to help alleviate lumbar pain and can bring back a person’s quality of life. In this article, we will be looking at what leg pain is, its factors, and its symptoms, as well as how decompression can relieve leg pain for many individuals. By referring patients to qualified and skilled providers specializing in spinal decompression therapy. To that end, and when appropriate, we advise our patients to refer to our associated medical providers based on their examination. We find that education is the key to asking valuable questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions, please call Dr. Jimenez at 915-850-0900.
What Is Leg Pain?
Ever wonder, “why are my legs aching so much?” or “my legs can’t stop twitching even when I am sitting down?” How about feeling a sharp pain from the buttock down to the back of the leg to the feet. This is known as leg pain, and research shows that leg pain can be intermittent or constant in the body. Not only that, but leg pain can have a range of sensations, from a dull ache to a throbbing, burning sensation that travels the leg itself. Now many causes can contribute to leg pain, and it usually starts in the lower back, the pelvis, or even the leg itself. Some of the common causes include:
As stated earlier, one of the causes contributing to leg pain is low back pain. Research studies have noted that around 60% of individuals with low back pain have also suffered leg pain. When leg pain is associated with low back pain, it is known as radicular pain. Leg pain can also affect the spinal nerve root involvement, and other research studies have found that low back-related leg pain is one of the most common variations of low back pain and can contribute to sciatica. Some of the symptoms that individuals are experiencing with leg pain include:
Leg weakness due to the lumbar or sacral spinal nerve being compressed
The video above shows how non-surgical decompression is used for the lumbar spine and can help alleviate a wide variety of issues that are not only affecting the back but can also alleviate other symptoms that are associated with low back pain like sciatica, herniated discs, and leg pain to name a few. What decompression therapy does to the individual is that it utilizes traction by gently stretching the spine allowing the compressed spinal discs to relieve themselves and stop touching the nerve roots spread out from the spine. This causes relief to many individuals that are suffering from sciatica and leg pain that is associated with low back pain. When the spine is being decompressed, the beneficial nutrients rehydrate the spinal discs and increase their disc height, allowing a person to get back their quality of life. If you want to learn more about spinal decompression therapy, this link will explain the benefits of spinal decompression and how it can alleviate low back pain symptoms.
Decompression Therapy Can Relieve Leg Pain
As stated earlier, the questions of “Why are my legs aching so much?” or “Why can’t my legs stop twitching when I am sitting down?” or even feeling a sudden sharp pain that runs from the lower back down to the leg have been searched all over the internet. The search results have stated that this is due to leg pain. How about treatments for leg pain? Most of the results show that light stretches, leg surgery, or taking pain medication can help; however, non-surgical treatments can help alleviate leg pain, and that is by utilizing decompression therapy.
Research studies have found that low back pain is one of the most common musculoskeletal disorders and that leg pain is associated with low back pain causing radicular symptoms. The lumbar spinal nerve roots are compressed when this happens, causing a burning, electric sharp pain that affects the back and legs. With decompression therapy, it allows the individual to feel the gentle stretch on their spine, causing a reduction in the intra-disc pressure and disc protrusion while also increasing the disc space and improving leg mobility. Other research studies have also found that the combination of both manual and spinal decompression therapy can help decrease the internal pressure of the intervertebral disc while increasing its height and taking pressure off the nerve root that is causing pain to the lower back and the leg. Decompression therapy also helps rehydrate the spinal discs and extend the annulus fibrosis and posterior ligaments to alleviate nerve root adhesion and disc herniation.
Conclusion
When the body is suffering from an injury that starts to affect the back and leg, it can cause severe issues for the individual. The pain ranges from a mild, dull ache to a sharp, sudden pain that can radiate down the lower back to the leg. Therefore, leg pain is associated with low back pain as the compressed spinal discs affect the nerve roots that are spread throughout the entire body. When a nerve root is irritated or compressed on the legs, it can cause symptoms like sciatica to initiate a sharp pain running down the leg itself. Luckily treatments like decompression therapy can help alleviate leg pain in a non-surgical way by utilizing traction to gently stretch the spinal disc off the compressed nerve root to alleviate symptoms causing low back and leg pain. Incorporating decompression therapy as part of your wellness journey can provide tremendous benefits to becoming pain-free.
References
Amjad, Fareeha, et al. “Effects of Non-Surgical Decompression Therapy in Addition to Routine Physical Therapy on Pain, Range of Motion, Endurance, Functional Disability and Quality of Life versus Routine Physical Therapy Alone in Patients with Lumbar Radiculopathy; a Randomized Controlled Trial.” BMC Musculoskeletal Disorders, BioMed Central, 16 Mar. 2022, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8924735/.
Cooper, Grant. “Leg Pain and Numbness: What Might These Symptoms Mean?” Spine, Spine-Health, 30 Sept. 2019, https://www.spine-health.com/conditions/leg-pain/leg-pain-and-numbness-what-might-these-symptoms-mean.
Konstantinou, Kika, et al. “Characteristics of Patients with Low Back and Leg Pain Seeking Treatment in Primary Care: Baseline Results from the Atlas Cohort Study.” BMC Musculoskeletal Disorders, BioMed Central, 4 Nov. 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4634730/.
Oh, Hyunju, et al. “Effects of the Flexion-Distraction Technique and Drop Technique on Straight Leg Raising Angle and Intervertebral Disc Height of Patients with an Intervertebral Disc Herniation.” Journal of Physical Therapy Science, The Society of Physical Therapy Science, Aug. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6698474/.
Stynes, Siobhán, et al. “Classification of Patients with Low Back-Related Leg Pain: A Systematic Review.” BMC Musculoskeletal Disorders, BioMed Central, 23 May 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4877814/.
Individuals drive to jobs, to school, run errands, take road trips, spending a lot of time on the road. Accidents and crashes happen more frequently with all kinds of injuries. The National Highway Traffic Safety Commission has found that 37% of car accidents and crashes involve leg injuries and damage. Chiropractic physical rehabilitation and functional medicine can help heal injuries getting the individual back to everyday life.
Bruising and cuts are typical from the impact and the body getting slammed around. Lacerations can be noticed right away, but bruising comes from blood pooling underneath the skin and can take time to present, possibly 24 to 48 hours. Most bruises and cuts heal independently from home first aid care. A standard recovery used to take care of bruising is R.I.C.E or rest, ice, compression, and elevation. This helps the healing process; however, if the injury/s are more severe, chiropractic can help with therapeutic massage to relieve pain and strengthen the injured muscles, tendons, and ligaments.
ACL Injuries
The femur or thigh bone has several bands of tissue connecting it to the patella or kneecap and tibia or shin bone. One of the bands is the anterior cruciate ligament or ACL. Injuries to this band of tissue are common in sports. Car accidents and crashes are another common cause, specifically tearing the ligament. Individuals experiencing a tear may notice some or all of the following symptoms:
A cracking or popping sound when the accident or crash took place.
Swelling in and around the knee.
Severe pain in and around the knee.
Unstable and unsteady when walking or standing.
Reduced range of motion that makes walking or moving difficult.
A chiropractor can help treat the injury and help correct any muscular imbalances.
Meniscus Tears
Tears to the meniscus are also common in car accidents and crashes. The meniscusis a part of the knee. Two wedge-shaped pieces of cartilage provide a cushion where the femur and tibia meet to absorb shock. The wedges are called menisci.
When the meniscus tears, individuals might feel or hear a pop and could feel the leg suddenly give out.
Swelling in the knee.
Some pain but still be able to walk.
The knee will be stiff for the next few days.
More difficulty bearing weight or walking.
The RICE method is a recommended method of self-care. Many meniscus tears do not require surgery to improve knee function. Mild to moderate meniscus tears can be successfully treated with chiropractic techniques like soft tissue work, corrective stretches, and exercises. Surgery could eventually be necessary for severe cases to repair the meniscus to prevent long-term complications.
Chiropractic care can help the body heal and recover from a bone fracture. A patient’s bone density is evaluated and tested with an individualized treatment plan to help regain and maintain optimal bone strength. The treatments strengthen the muscles, reduce stiffness, improve nutrition, and relieve pain. Manipulation adjustments, rehabilitation, relaxation techniques, and dietary health coaching help individuals heal faster and strengthen their bones. The objective is to help regain increased mobility and range of motion.
Sciatica
Car accidents and crashes are one instance where the spine can be damaged enough to bring on sciatic pain where no back problems were present before. The impact from a car accident can cause the discs to be knocked out of place, damaged, and/or rupture around the surrounding tissue. Any of these results can pinch the sciatic nerve, leading to pain and other sciatica symptoms. Chiropractic can realign the spine and relieve pressure from the nerve/s.
DOC Spinal Decompression Table
References
Atkinson, T, and P Atkinson. “Knee injuries in motor vehicle collisions: a study of the National Accident Sampling System database for the years 1979-1995.” Accident; analysis and prevention vol. 32,6 (2000): 779-86. doi:10.1016/s0001-4575(99)00131-1
Foulk, David M, and Brian H Mullis. “Hip dislocation: evaluation and management.” The Journal of the American Academy of Orthopaedic Surgeons vol. 18,4 (2010): 199-209. doi:10.5435/00124635-201004000-00003
Wilson, L S Jr et al. “Foot and ankle injuries in motor vehicle accidents.” Foot & ankle international vol. 22,8 (2001): 649-52. doi:10.1177/107110070102200806
The body utilizes the spine to make sure that everything is moving, bending, twisting, and turning without feeling any pain from the back. The spine is an S-shaped curve protected by ligaments, soft tissue from the musculoskeletal system, the spinal cord, and spinal discs. When the back suffers from an injury or has pulled a muscle, it can cause chronic issues to the back and make a person’s life miserable. Luckily there are therapeutic ways to relieve chronic back issues and can alleviate the symptoms it has caused to the individual. In this article, we will be looking at musculoskeletal disorders and their symptoms and how decompression therapy has an effect on alleviating musculoskeletal disorders from the back. By referring patients to qualified and skilled providers specializing in spinal decompression therapy. To that end, and when appropriate, we advise our patients to refer to our associated medical providers based on their examination. We find that education is the key to asking valuable questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions, please call Dr. Jimenez at 915-850-0900.
What Are Musculoskeletal Disorders?
As research studies have stated, the musculoskeletal system combines bone, muscles, tendons, ligaments, and soft tissues that work together to support the body’s weight and help individuals move. The spine is located at the back of the body, where it connects to the musculoskeletal tissues and keeps it upright. Many individuals must keep their musculoskeletal system healthy and functional; however, a wide range of disorders and conditions can affect the musculoskeletal system making the body succumb to diseases and injuries that can limit its movement. This is known as musculoskeletal disorders.
Research studies have found that musculoskeletal pain and disorders affect the bones, joints, ligaments, muscles, and tendons throughout the entire body. Sometimes the pain can become acute, and it can become sudden and severe or chronic, which can hinder a person’s ability to do any daily activities. Some of the most common types of musculoskeletal disorders that can affect the body include:
Tendon and ligament pain: Sprains, strains, and overused tissues
The Symptoms
Research studies have shown that musculoskeletal disorders are the leading source of pain and disability worldwide. With a variety of back and neck disorders, arthritic conditions, and soft tissue syndromes that involve the tendons, ligaments, muscles, and cartilages that make up the main bulk of musculoskeletal disorders, it can cause many people to go to their primary physician and get time off work. Other research studies have shown that the symptoms that are caused by musculoskeletal disorders include:
The video above shows how the Chattanooga Triton is being used to alleviate back issues that have been affected by musculoskeletal disorders. Traction therapy is a form of spinal decompression therapy that utilizes traction on a person’s spine, gently stretching it. This will cause the beneficial nutrients and oxygen to go back into the spine and alleviate pain in the back. Since back pain is one of the most common types of musculoskeletal pain that can make a person miserable, decompression therapy can help with low back pain and make a person get back their quality of life. If you want to learn more about spinal decompression therapy, this link will explain the benefits of spinal decompression and how it can alleviate low back pain symptoms.
How Does Decompression Therapy Help Musculoskeletal Disorders?
Decompression therapy is a non-surgical treatment that allows for individuals who have musculoskeletal disorders like low back pain. Decompression therapy allows the individual to lie down on the traction table, be strapped in, and the traction machine gently pulls on the spine to cause instant relief. Research studies have found that utilizing decompression therapy and even physical therapy can help improve the lumbar range of motion, back muscle endurance, and functional disability that musculoskeletal disorders have caused. Other research studies have also shown that non-surgical spinal decompression therapy can reduce pain in the back and promote an increase in the spinal disc height and restore it. When individuals start to feel relief from their back, they can continue with their wellness journey.
Conclusion
All in all, musculoskeletal disorders are a wide variety of disorders that affects the bones, ligaments, tissues, and muscles all over the body. Low back pain is one of the most common musculoskeletal disorders that causes the individual to have pain and stiffness in the back muscles. Luckily treatments like spinal decompression therapy allow individuals who are suffering from feel relief from chronic back issues and gently stretch the spine to allow the beneficial nutrients to re-hydrate the spinal disc. With the combination of physical therapy, many individuals won’t have to suffer any longer, knowing that decompression may be their relief.
References
Amjad, Fareeha, et al. “Effects of Non-Surgical Decompression Therapy in Addition to Routine Physical Therapy on Pain, Range of Motion, Endurance, Functional Disability and Quality of Life versus Routine Physical Therapy Alone in Patients with Lumbar Radiculopathy; a Randomized Controlled Trial.” BMC Musculoskeletal Disorders, BioMed Central, 16 Mar. 2022, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8924735/.
Apfel, Christian C, et al. “Restoration of Disk Height through Non-Surgical Spinal Decompression Is Associated with Decreased Discogenic Low Back Pain: A Retrospective Cohort Study.” BMC Musculoskeletal Disorders, BioMed Central, 8 July 2010, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2912793/.
Malik, Khalid M, et al. “Musculoskeletal Disorders a Universal Source of Pain and Disability Misunderstood and Mismanaged: A Critical Analysis Based on the U.S. Model of Care.” Anesthesiology and Pain Medicine, Kowsar, 15 Dec. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6348332/.
Medical Professionals, Cleveland Clinic. “Musculoskeletal Pain: Types, Causes, Symptoms & Treatment.” Cleveland Clinic, 10 Mar. 2021, https://my.clevelandclinic.org/health/diseases/14526-musculoskeletal-pain.
Medical Professionals, Cleveland Clinic. “Musculoskeletal System: Arthritis, Lower Back Pain, Bones, Muscles.” Cleveland Clinic, 11 Dec. 2020, https://my.clevelandclinic.org/health/articles/12254-musculoskeletal-system-normal-structure–function.
Inside the body, the spine allows it to move around and do all sorts of things without pain. The spine is protected by ligaments, soft tissue from the musculoskeletal system, spinal discs, and the spinal cord in an S-shaped curve that holds the body together. When the back gets injured or pulls a muscle, it can cause unwanted back issues that can cause a person to be in pain. When this happens, the individual suffering from back pain will be hindered from their daily activities and be miserable if it is not treated right away. Luckily, treatments like spinal decompression therapy can help alleviate back pains and other issues that affect the body’s back and spine. In this article, we will be looking at what DDD is, its symptoms, and how spinal decompression can help relieve DDD. By referring patients to qualified and skilled providers specializing in spinal decompression therapy. To that end, and when appropriate, we advise our patients to refer to our associated medical providers based on their examination. We find that education is the key to asking valuable questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions, please call Dr. Jimenez at 915-850-0900.
What Is DDD?
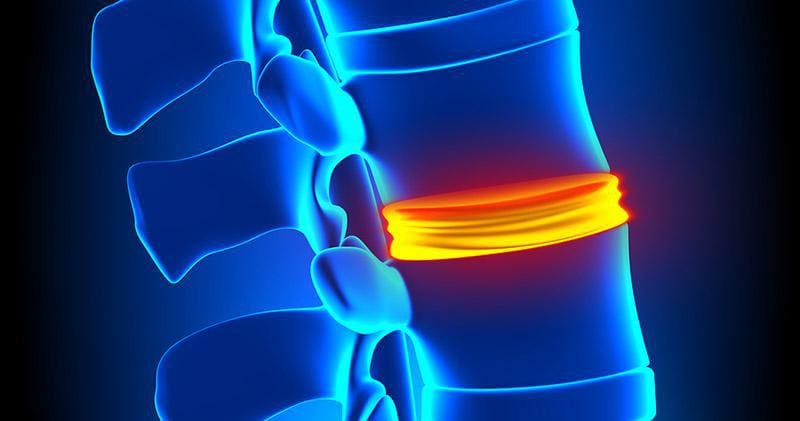
Since low back pain is common for many individuals worldwide, some of the causes of low back pain are DDD or degenerative disc disease. Research studies show that DDD (degenerative disc disease) usually happens when the spinal discs start to wear down naturally due to age. The spinal disc is a rubbery cushion between the spine’s vertebrae, and they help people move comfortably. When the spinal disc starts to wear and tear naturally through age, it can cause the vertebrae to rub against each other and cause pain.
Other research studies have found that DDD is often misunderstood since the symptoms affect either the neck or the back, causing sudden shooting pain in the arms or legs. DDD can also progress over time if it is not treated right away, causing the individual to be in pain and can make them unstable. Research studies have found that the two main factors of DDD are inflammation and abnormal micro-motion instability. How inflammation plays in DDD is that the inflammatory proteins from the spinal disc interiors are leaked when degeneration affects the spinal disc and causes swelling around the spinal structure. Abnormal micro-motion instability starts to affect the spinal discs’ outer layer by causing small, unnatural motions in-between the vertebrae, thus causing irritation and tension to the surrounding muscles, joints, and nerve roots, making the person become unstable and be in more pain.
The Symptoms Of DDD
Research studies have shown that when DDD affects the spine, it also affects the nervous system surrounding the spinal disc. DDD also causes structural failure, a radial tear in the annulus fibrosis, herniated disc, and calcification to the endplate of the spine. Since flare-up pains and abnormal stress on the spine can be due to recent activities or suddenly come up for no apparent reason, research studies have shown that pain episodes from DDD can last between a few days to several weeks before going back to be low-level back pain. Some of the common symptoms of DDD can include:
Increased pain from lifting heavy objects, bending or twisting the spine
Sudden sharp, radiating pain from the cervical or lumbar parts of the spine
Increased pain from holding a position for too long
Spinal Decompression Therapy & DDD-Video
The video above shows how spinal decompression can help alleviate DDD (degenerative disc disease). Spinal decompression therapy is utilized for many individuals suffering from chronic back issues like DDD, herniated disc, and low back pain. What spinal decompression therapy does is that it allows the individual to lay on a traction table and start to gently stretch their spine to relieve any issues that were causing back pain. The beneficial nutrients are reabsorbed into the spinal disc when the spine is gently pulled. The individual will begin to feel instant relief after a couple of sessions. If you want to learn more about spinal decompression therapy, this link will explain the benefits of spinal decompression and how it can alleviate low back pain symptoms.
How Spinal Decompression Therapy Relieves DDD
Many treatments help alleviate DDD symptoms and chronic low back pain as they provide relief to many individuals. One of the treatments that have been getting attention is spinal decompression therapy. Research studies have shown that many individuals suffering from DDD utilize non-surgical spinal decompression therapy to reduce pain and cause an increase in spinal disc height. This will allow the compressed spinal disc to be decompressed and improve disc health. Other research studies have also shown that since the degenerative process and mechanical effects of DDD can affect the spine, spinal decompression therapy allows traction to reduce the pressure off the spinal disc by gravity and soft tissue, enabling sufficient tension to extend spinal separation and the intervertebral disc. Spinal decompression also allows negative pressure within the intervertebral disc by increasing its hydration and reducing pressure off the nerve root.
Conclusion
The spine is an S-shaped curve protected by ligaments, soft tissue from the musculoskeletal system, the spinal discs, and the spinal cord allowing it to hold the body together. The body is home to the spine, where it can move around without feeling any sort of pain. When a person injures their back or pulls a muscle, it can cause unwanted back issues to hinder them from doing various daily activities. Sometimes the spinal disc wear and tear naturally causes symptoms like a herniated disc or DDD (degenerative disc disease) to affect the spine and the back by causing sharp, shooting radiate pain to affect the body. Luckily, treatments like spinal decompression therapy alleviate these symptoms by gently stretching the spine and causing instant relief to the individual.
References
Apfel, Christian C, et al. “DRX9000 BMC Study.” DRX9000® & DRX9000c® Global Trusted Suppliers Excite Medical, 18 Apr. 2022, https://excitemedical.com/drx9000-research/drx9000-bmc-study/#section-tab|0.
Choi, Jioun, et al. “Influences of Spinal Decompression Therapy and General Traction Therapy on the Pain, Disability, and Straight Leg Raising of Patients with Intervertebral Disc Herniation.” Journal of Physical Therapy Science, The Society of Physical Therapy Science, Feb. 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4339166/.
Choi, Yong-Soo. “Pathophysiology of Degenerative Disc Disease.” Asian Spine Journal, Korean Society of Spine Surgery, June 2009, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2852042/.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine