The spine is encompassed by ligaments, the spinal cord, nerves, and discs that ensure that the entire body is upright and allow it to move, bend, twist, and turn. The spine also holds parts of the musculoskeletal system as the muscles make sure that the muscles are doing their job correctly. When a person suffers from an injury or a pulled muscle on the back, it can cause unwanted symptoms that can affect the back and affect the entire body. When the spine gets injured, it can also cause many individuals to be in pain, affecting their daily activities. Many treatments can relieve the painful symptoms of back and spinal injury, including spinal decompression. In this article, we will be looking at sensory nerve dysfunction and how the effects of spinal decompression therapy can alleviate sensory nerve dysfunction. By referring patients to qualified and skilled providers specializing in spinal decompression therapy. To that end, and when appropriate, we advise our patients to refer to our associated medical providers based on their examination. We find that education is the key to asking valuable questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions, please call Dr. Jimenez at 915-850-0900.
What Is Sensory Nerve Dysfunction?
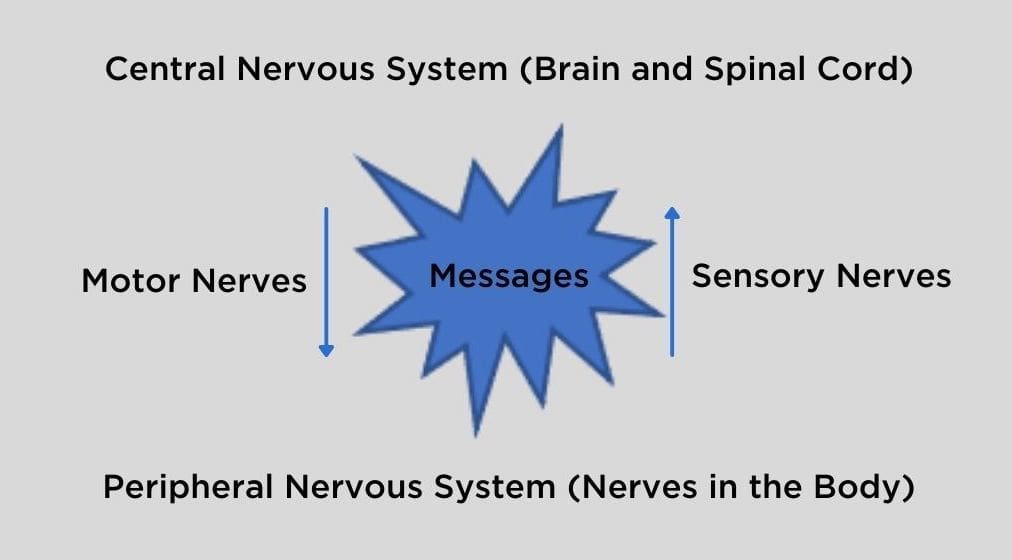
As part of the central nervous system, the sensory nerves send information from the peripheral nervous system to the spinal cord to the brain. These nerves make sure that the body feels something that a person is touching. When there is an injury affecting the peripheral nerves, it is known as peripheral nerve injury. Research studies have shown that peripheral nerve injury is when there is nerve damage to the body, affecting the brain’s ability to communicate with the muscles and organs. When the sensory nerve becomes damaged from an injury, this will cause many individuals to have a tingling sensation on their hands and feet.
Other research studies have also stated that neuropathic pain can damage the sensory nerve receptor that sends the signals from the spinal cord to the brain. It can cause many symptoms that can be altered and disorder the sensory nerves to develop neuropathic pain symptoms. Since the nerves from the central nervous system send the information from the spinal cord to the entire body, nerve pain damage can disrupt the signals and cause the individual to fall, causing injury to the body, especially on the back. Research studies have shown that many individuals suffering from peripheral nerve damage can result from traumatic injury, metabolic problems, exposure to toxins, and inherited causes that cause the nerve signals to be disrupted.
What Is Spinal Decompression Therapy?-Video
Spinal decompression therapy is a non-surgical treatment that gently stretches the spine using a traction table to relieve back and leg pain. Research studies have found that spinal decompression therapy is used on the spine. It creates a negative intradiscal pressure to retract and reposition herniated or bulging disc material back to its original position in the spine. The gentle stretching from the traction machine allows the nutrients and other beneficial substances to go back to the spine and relieve the painful symptoms that cause injury to the spine. If you want to learn more about spinal decompression therapy, this link will explain the benefits of spinal decompression and how it can alleviate low back pain symptoms.
How Spinal Decompression Can Alleviate Sensory Nerve Dysfunction
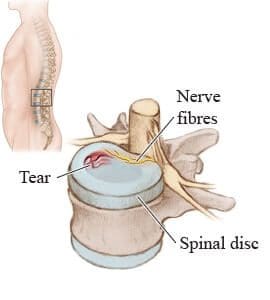
The spine is encompassed by ligaments, the spinal cord, and discs that protect the spine from injury. When the spinal disc gets injured or naturally wears and tears due to age, it can cause the disc to lose the fluid that makes them sponge-like and compressed. When there is compression on the spinal disc, it can cause pain in the back. There is no pain when there is compression on the peripheral nerves unless the peripheral nerves have been irritated or pinched earlier. There are therapeutic treatments that can help alleviate the painful symptoms caused by the pinched nerves and bring back a person’s quality of life.
Research studies have found that ice treatments, electric treatments, and spinal decompression therapy allow individuals to get back their quality of life to about 90%. Since spinal decompression has a direct mechanical effect and a biochemical effect, the gentle traction will allow the intradiscal pressure from the damaged nerves to be reduced and retract the herniated disc. Spinal decompression therapy can influence sensory nerve dysfunction and restore motor functions in the body. Other research studies have also found that stretching, infrared radiation, and spinal decompression traction can significantly improve the pain and disability levels that are causing the individual pain in their lower back. Spinal decompression therapy will even alter the biomechanics and biochemistry of the spinal disc and nerve root, causing many individuals relief.
Conclusion
Therefore, the spine’s primary function is to make sure that the body can twist, bend, turn, and stay upright. When the back gets injured from a pulled muscle or an accident, it can immobilize the individual and disrupt their quality of life. If there is nerve damage from the injury, it can disrupt the nerve signals in the brain and cause the individual to lose balance and injure themselves even more. Utilizing non-surgical treatments like ice treatments, stretching, and physical therapy with the combination of spinal decompression therapy can help restore the back by gently stretching the spine with a traction table and restoring the lost nutrients of the spinal disc as well as restoring the motor and sensory nerve functions to the body.
References
Alrwaily, Muhammad, et al. “Assessment of Variability in Traction Interventions for Patients with Low Back Pain: A Systematic Review.” Chiropractic & Manual Therapies, BioMed Central, 17 Sept. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6139896/.
Colloca, Luana, et al. “Neuropathic Pain.” Nature Reviews. Disease Primers, U.S. National Library of Medicine, 16 Feb. 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5371025/.
Daniel, Dwain M. “Non-Surgical Spinal Decompression Therapy: Does the Scientific Literature Support Efficacy Claims Made in the Advertising Media?” Chiropractic & Osteopathy, BioMed Central, 18 May 2007, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1887522/.
Staff, Mayo Clinic. “Peripheral Nerve Injuries.” Mayo Clinic, Mayo Foundation for Medical Education and Research, 17 Apr. 2020, https://www.mayoclinic.org/diseases-conditions/peripheral-nerve-injuries/symptoms-causes/syc-20355631.
Staff, Mayo Clinic. “Peripheral Neuropathy.” Mayo Clinic, Mayo Foundation for Medical Education and Research, 3 July 2021, https://www.mayoclinic.org/diseases-conditions/peripheral-neuropathy/symptoms-causes/syc-20352061.
The body needs the spine to stay upright, bend, move, twist, and turn to function properly. The spine is an S-shaped curve structure protected by ligaments, soft tissues, the spinal cord, and muscle tissue if the back gets injured. When the body gets injured, or a back muscle is pulled, it can affect the spine and cause the individual to be in pain. Many individuals will experience some back pain that can affect their daily activity and try to find relief for their back pain. Some therapeutic treatments can help relieve back pain and help decompress the spine to cause instant relief. This article will look at what causes chronic low back pain, why it is expensive, and how efficient spinal decompression therapy is for chronic low back pain. By referring patients to qualified and skilled providers specializing in spinal decompression therapy. To that end, and when appropriate, we advise our patients to refer to our associated medical providers based on their examination. We find that education is the key to asking valuable questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions, please call Dr. Jimenez at 915-850-0900.
What Causes Chronic Low Back Pain?
Since the spine is an S-shaped curve protected by joints, ligaments, nerves, and muscles, its primary function is to provide the body with the support, strength, and flexibility it needs to move and function. Research studies have found that the low back supports the upper body’s weight, and when there is an injury to the muscles, ligaments, joints, or spinal disc, it can cause minor to severe pain to the back. When there is a significant overlap of nerves, it causes some difficulty for the brain to sense where the pain originates accurately. Other research studies have found that back pain is common due to soft tissue injury and mechanical issues that can cause low back pain to be chronic. Some of the factors that can cause chronic low back pain include:
Since chronic low back pain is an expensive benign condition in most industrialized countries, it is often one of the most frequent reasons for many individuals to visit their primary care physicians. This will allow them to take time off from work due to sickness or short-term disability and hospital admission and surgery. Research studies have stated that chronic low back pain can range from mild to severe, making it difficult for individuals to do everyday activities. About one-third to two-thirds of adults will suffer from low back pain at some time, and the prevalence of low back pain increases with age, and women are affected more often than men.
What Is Discogenic Pain?
Research studies have shown that discogenic low back pain is one of the common types of chronic low back pain that causes the formation of vascularized granulation tissue to degenerate. Discogenic pain most commonly affects the lower back, buttocks, and hips. Discogenic pain also involves:
The degenerative changes in the intervertebral disc in the spine.
Causing structural defects in the spine.
Causing the result of biomechanical instability and inflammation of the back.
Other research studies have found that discogenic back pain is multifactorial, causing physicians to struggle to identify the source of pain coming from the back.
How Efficient Is The DRX9000?-Video
The DRX9000 is a spinal decompression traction machine that helps alleviate chronic lower back pain in individuals. Research studies have found that the DRX9000 uses a motor pulley that causes traction force on the spine to pull, causing it to decompress gently. The traction force from the DRX9000 allows the spine to stretch the soft tissues and separate joint surfaces causing instant relief to individuals suffering from lower back pain. Many individuals who use the DRX9000 as part of their spinal decompression therapy will begin to feel instant relief from their spine and regain their quality of life. If you want to learn more about spinal decompression therapy, this link will explain the benefits of spinal decompression and how it can alleviate low back pain symptoms.
The Efficacy Of Spinal Decompression
The efficacy of spinal decompression on chronic low back pain can provide immense relief to many individuals suffering from low back pain. Research studies have shown that spinal decompression therapy is effective for many individuals suffering from lumbar disc herniation as it helps with the resorption of the herniation disc back in the spine and increases the disc height. Research studies have shown that many individuals who completed an entire 6-week course of spinal decompression therapy have reported much improvement from the pain and disability they had suffered from chronic low back pain.
Conclusion
Chronic lower back pain is common for many individuals and can be expensive as the symptoms can range from a dull, mild ache to severe sharp, throbbing pain in the lower back. Chronic low back pain causes many individuals to go to their health care providers, allowing them to get out of work and causing early retirement for many working individuals. Incorporating spinal decompression therapy as part of chronic low back pain treatment can cause instant relief to many individuals as the spinal disc are getting the necessary beneficial nutrients back into their spine and improving their quality of life pain-free. All in all, spinal decompression utilizes gentle stretching on the spine using a traction machine, causing instant relief to many individuals that are suffering from chronic lower back pain.
References
Choi, Jioun, et al. “Influences of Spinal Decompression Therapy and General Traction Therapy on the Pain, Disability, and Straight Leg Raising of Patients with Intervertebral Disc Herniation.” Journal of Physical Therapy Science, U.S. National Library of Medicine, Feb. 2015, https://pubmed.ncbi.nlm.nih.gov/25729196/.
Demirel, Ayunur, et al. “Regression of Lumbar Disc Herniation by Physiotherapy. Does Non-Surgical Spinal Decompression Therapy Make a Difference? Double-Blind Randomized Controlled Trial.” Journal of Back and Musculoskeletal Rehabilitation, U.S. National Library of Medicine, Nov. 2016, https://pubmed.ncbi.nlm.nih.gov/28505956/.
Fujii, Kengo, et al. “Discogenic Back Pain: Literature Review of Definition, Diagnosis, and Treatment.” JBMR Plus, John Wiley and Sons Inc., 4 Mar. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6524679/.
Koçak, Fatmanur Aybala, et al. “Comparison of the Short-Term Effects of the Conventional Motorized Traction with Non-Surgical Spinal Decompression Performed with a DRX9000 Device on Pain, Functionality, Depression, and Quality of Life in Patients with Low Back Pain Associated with Lumbar Disc Herniation: A Single-Blind Randomized-Controlled Trial.” Turkish Journal of Physical Medicine and Rehabilitation, Bayçınar Medical Publishing, 16 Feb. 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6709608/.
Medical Professionals, Cleveland Clinic. “Low Back Pain: Causes, Diagnosis & Treatments.” Cleveland Clinic, 18 Jan. 2021, https://my.clevelandclinic.org/health/diseases/7936-lower-back-pain.
Peloza, John. “Causes of Lower Back Pain.” Spine, Spine-Health, 20 Apr. 2017, https://www.spine-health.com/conditions/lower-back-pain/causes-lower-back-pain.
Peloza, John. “Lower Back Pain Symptoms, Diagnosis, and Treatment.” Spine, Spine-Health, 20 Apr. 2017, https://www.spine-health.com/conditions/lower-back-pain/lower-back-pain-symptoms-diagnosis-and-treatment.
Peng, Bao-Gan. “Pathophysiology, Diagnosis, and Treatment of Discogenic Low Back Pain.” World Journal of Orthopedics, Baishideng Publishing Group Co., Limited, 18 Apr. 2013, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3631950/.
The body goes through many scenarios that sometimes can get injured depending on the situation. When that happens, the immune system goes on full alert and starts to heal the affected area, and the body will begin to feel better. Sometimes, the injuries will affect the back and spine as the spine makes sure that the body can bend, move, sit, and turn. The back muscles also do the same thing the spine does and even protect the spine from injuries. When injuries or a pulled muscle start to affect the back, it can cause many unwanted problems to rise and cause chronic low back pain and even herniated disc on the spine. Some treatments are non-surgical and can alleviate chronic low back pain for many individuals. In this article, we will be looking at what discogenic low back pain is and its symptoms, and how low back decompression can help many individuals. By referring patients to qualified and skilled providers specializing in spinal decompression therapy. To that end, and when appropriate, we advise our patients to refer to our associated medical providers based on their examination. We find that education is the key to asking valuable questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions, please call Dr. Jimenez at 915-850-0900.
What Is Discogenic Low Back Pain?
Since it is widespread for individuals to have back pain at some point in their lives and have to go to their primary physician to get time off their jobs to rest, there are two forms of back pain which are acute and chronic. Acute back pain only lasts between a few days to a week with rest and minimal light activity. Chronic back pain is defined as pain that lasts longer than 12 weeks and is considered an expensive benign condition in many industrialized countries. Some of the causes of chronic back pain can be an injury to the lumbosacral muscles and ligaments or even discogenic disorders like DDD (degenerative disc disease) or some form of trauma.
Discogenic low back pain is a common cause of chronic low back pain. It involves degenerative changes in the intervertebral disc in the spine while causing structural defects that result in biomechanical instability and inflammation. Research studies have stated that discogenic low back pain is considered multifactorial due to many physicians struggling to identify where the underlying source of pain is located at. Disogenic low back pain can also cause other types of back pain symptoms to pop up and cause the spinal nerve roots to compress and tear, causing chronic issues like herniated disc, spondylolysis, and foraminal stenosis to cause havoc on the back and making the individual suffering from chronic back pain miserable.
The Symptoms
Research studies have shown that discogenic low back pain symptoms usually start when there is an increased activity that causes intradiscal pressure on the spine. Some of the signs that it causes include:
Bending forward can increase low back discogenic pain
Many of these symptoms can be the underlying issue when dealing with chronic back pain. If the pain is left untreated, it can develop into chronic problems that can cause immense pain to the back and the rest of the body. There are ways to treat chronic discogenic low back pain, and that is through low back decompression.
How The DOC Decompression Table Works-Video
The video above shows how the DOC decompression table works for individuals suffering from chronic low back pain. The DOC decompression table is part of a non-surgical treatment known as spinal decompression therapy. Research studies have stated that spinal decompression therapy allows gentle spine stretching using a traction machine like the DOC decompression table to relieve low back pain. The machine creates negative intradiscal pressure on the low back and allows the nutrients to return to the spinal disc and restore them. The DOC decompression table also enables many individuals suffering from low back pain to feel instant relief. If you want to learn more about spinal decompression therapy, this link will explain the benefits of spinal decompression and how it can alleviate low back pain symptoms.
How Does Low Back Decompression Help?
There are many ways to help treat low back pain, as there are surgical and non-surgical approaches to help alleviate low back pain. However, studies have shown that when many individuals suffering from low back pain go through a 6-week treatment, the results show a reduction in the pressure of the affected disc, causing facilitation of their regeneration and increasing the disc height. Another way to optimize low back decompression is when combined with physical therapy. Research studies have shown that it is more effective as it helps improve the pain, lumbar range of motion, and back muscle endurance. Incorporating these two treatments will help reduce low back pain and help improve the individual’s quality of life.
Conclusion
Since chronic low back pain is common for many working individuals, it is essential to know where the pain is located for many physicians to incorporate low back decompression to restore the nutrients in the spine and cause instant relief for many individuals. It is crucial to utilize non-surgical treatments like low back decompression to help alleviate chronic discogenic low back pain in many individuals. With physical therapy and low back decompression, many individuals can regain their quality of life and be worry-free from low back pain.
References
Amjad, Fareeha, et al. “Effects of Non-Surgical Decompression Therapy in Addition to Routine Physical Therapy on Pain, Range of Motion, Endurance, Functional Disability and Quality of Life versus Routine Physical Therapy Alone in Patients with Lumbar Radiculopathy; a Randomized Controlled Trial.” BMC Musculoskeletal Disorders, BioMed Central, 16 Mar. 2022, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8924735/.
Apfel, Christian C, et al. “Restoration of Disk Height through Non-Surgical Spinal Decompression Is Associated with Decreased Discogenic Low Back Pain: A Retrospective Cohort Study.” BMC Musculoskeletal Disorders, BioMed Central, 8 July 2010, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2912793/.
Fujii, Kengo, et al. “Discogenic Back Pain: Literature Review of Definition, Diagnosis, and Treatment.” JBMR Plus, John Wiley and Sons Inc., 4 Mar. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6524679.
Mummaneni, Praveen V. “Discogenic Low Back Pain.” SpineUniverse, SPU, 21 May 2019, https://www.spineuniverse.com/conditions/back-pain/discogenic-low-back-pain.
The spine is encompassed by ligaments, soft tissues, joints, and the spinal cord, where it is protected. The spine also holds the body together by ensuring that the musculoskeletal system keeps the body upright and that it can twist, turn, bend, and move around when it is in motion. When the body sustains an injury from an accident or pulls a muscle, it can significantly affect the spine, causing immense pain to the lower back. When this happens, many treatments can help lower back pain by dampening the inflammation and causing relief to the individual. In this article, we will be looking at what is a herniated disc and its symptoms, as well as how decompression can help repair herniated disc in the spine. By referring patients to qualified and skilled providers specializing in spinal decompression therapy. To that end, and when appropriate, we advise our patients to refer to our associated medical providers based on their examination. We find that education is the key to asking valuable questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions, please call Dr. Jimenez at 915-850-0900.
What Is Herniated Disc?
Since mainly everyone has dealt with chronic back pain from an injury or pulling a back muscle at some point in their lives, this will cause many individuals to miss work and get treatment from their primary physicians as the pain is excruciating and can cause many people to miss out on everyday activities. Research studies have shown that lower back pain is one of the most common problems. With the different diagnoses for low back pain, DDD (degenerative disc disease) and lumbar disc herniation are considered the most common back pain. Research shows that herniated discs are formed when someone is lifting something heavy or twisting motions on the lower back, causing added stress on the spinal disc.
Research studies have stated that herniated disc has been the known cause of neck, back, and leg pain, and it is due to an injury to the spine. Herniated discs are caused because, usually, spinal discs have a soft, gel-like center on the inside and are protected by a firm outer layer between the spinal joints. Within time and age, the firm outer layer becomes weak and will eventually crack, causing the inner soft gel-like center to push through the cracks of the outer layer and press on the nearby spinal nerves. This will cause sharp shooting pain in the sciatic nerve, causing it to go from the buttock down to the foot.
The Symptoms
Since most herniated discs usually occur in the lower back, research studies stated that they could also occur in the neck. Depending on where the herniated disc is located and pressing on a nerve, it will usually affect one side of the body. Some of the symptoms that herniated discs are causing on the neck and lower back include:
Other research studies have also found that lumbar disc herniation can be compressed and irritate the lumbar nerve root and the dural sac of the spine and cause sciatica to form. Since lumbar disc herniation is one of the most common diagnoses for degenerative abnormalities of the lumbar spine, there are ways to treat lumbar disc herniation.
How Lumbar Traction Rehydrates Lumbar Disc-Video
The video shows how a decompression machine uses traction to gently stretch the lumbar spine to rehydrate the lumbar disc back to its original state. As part of spinal decompression therapy, the decompression machine uses a traction machine to gently stretch the spine, causing instant relief to the individual suffering from low back pain or even herniated disc. When the spine gets a gentle stretch, the beneficial nutrients will go to the spinal disc, rehydrate them back into the spine, and improve the disc height. If you want to learn more about spinal decompression therapy, this link will explain the benefits of spinal decompression and how it can alleviate low back pain symptoms.
Repairing Herniated Disc With Decompression
With many treatments that can alleviate lumbar disc herniation, one of the non-surgical treatments providing relief to many individuals is spinal decompression therapy. Research studies have found that spinal decompression therapy has been used to help reduce the pressure of lumbar disc herniation and repair it by supplying nutrients and oxygen back to the lumbar disc. This will cause many individuals to feel instant relief as the herniated disc goes back into the spine with the nutrients and oxygen and repair them back to their original state. Other research studies also found that when combined with physical therapy, spinal decompression therapy is highly effective in the reabsorption of herniation and can increase the disc height for many individuals with lumbar disc herniation.
Conclusion
The spine’s primary function is to make sure that the body is upright and can bend, move, twist, and turn without any problems. The spine is encompassed by ligaments, soft tissues, the musculoskeletal system, the spinal cord, and the spinal disc. When a person accidentally pulls a muscle or sustains an injury, it can compress the spinal disc or cause it to develop a herniation and cause the person pain in their lower back. Luckily, treatments like spinal decompression allow gentle stretching on the spine to repair, restore, and rehydrate the spinal disc back to its original state. When this happens, many individuals will begin to feel instant relief and continue their day pain-free.
References
Al Qaraghli, Mustafa I, and Orlando De Jesus. “Lumbar Disc Herniation – Statpearls – NCBI Bookshelf.” StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 30 Aug. 2021, https://www.ncbi.nlm.nih.gov/books/NBK560878/.
Choi, Jioun, et al. “Influences of Spinal Decompression Therapy and General Traction Therapy on the Pain, Disability, and Straight Leg Raising of Patients with Intervertebral Disc Herniation.” Journal of Physical Therapy Science, The Society of Physical Therapy Science, Feb. 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4339166.
Demirel, Aynur, et al. “Regression of Lumbar Disc Herniation by Physiotherapy. Does Non-Surgical Spinal Decompression Therapy Make a Difference? Double-Blind Randomized Controlled Trial.” Journal of Back and Musculoskeletal Rehabilitation, U.S. National Library of Medicine, 22 Sept. 2017, https://pubmed.ncbi.nlm.nih.gov/28505956/.
Härtl, Roger. “Lumbar Herniated Disc: What You Should Know.” Spine, Spine-Health, 6 July 2016, https://www.spine-health.com/conditions/herniated-disc/lumbar-herniated-disc.
Medical Professionals, Cleveland Clinic. “Herniated Disk: What It Is, Diagnosis, Treatment & Outlook.” Cleveland Clinic, 1 July 2021, https://my.clevelandclinic.org/health/diseases/12768-herniated-disk.
Staff, Mayo Clinic. “Herniated Disk.” Mayo Clinic, Mayo Foundation for Medical Education and Research, 8 Feb. 2022, https://www.mayoclinic.org/diseases-conditions/herniated-disk/symptoms-causes/syc-20354095.
Vialle, Luis Roberto, et al. “Lumbar Disc Herniation.” Revista Brasileira De Ortopedia, Elsevier, 16 Nov. 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4799068/.
The spine is an S-shaped curve located in the back that makes sure that the body is standing upright, twisting, turning, bending, and moving from one place to another without any pain or problems. The spine is also protected by ligaments, the spinal cord, soft tissues from the musculoskeletal system, and spinal discs that ensure it doesn’t get injured. When a person gets injured from pulling a back muscle or is in an accident, the spine suffers the most as they are suffering from a variety of back pains that can hinder their quality of life and become miserable. There are many treatments for back pain that can provide relief to individuals suffering from back issues. In this article, we will be looking at the different types of radiculopathies that can affect the spine and how spinal decompression can help treat radiculopathy. By referring patients to qualified and skilled providers specializing in spinal decompression therapy. To that end, and when appropriate, we advise our patients to refer to our associated medical providers based on their examination. We find that education is the key to asking valuable questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions, please call Dr. Jimenez at 915-850-0900.
What Is Radiculopathy?
Since low back pain is common for many individuals, it can affect them in some way or form as the pain can range from a dull, mild ache to a severe sharp pain that can hinder a person. The variety of back pains can also vary from strains, ruptured discs, and pinched nerves, to name a few. One of the back pain conditions is radiculopathy, and research studies have shown that it is often described as a range of symptoms produced by a pinched nerve root in the spinal column. Radiculopathy can occur in different areas along the spine. The most common ones are in the lumbar and cervical spine. Other studies have also demonstrated that radicular back pain is one of the most common reasons many individuals have low back pain and can cause the person to be in pain and lose sensation and motor function depending on how severe the nerves are compressed in the spine.
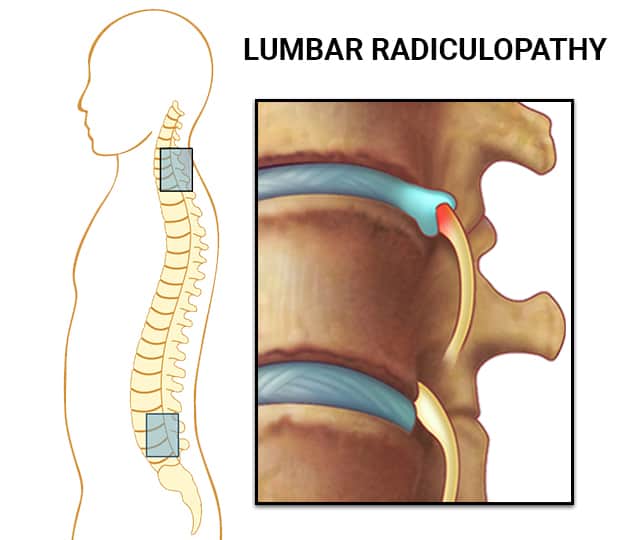
Lumbar Radiculopathy
Radicular back pain is most often the painful secondary condition to compression or inflammation of the spinal cord. When it comes to lumbar radiculopathy, research studies have stated that the pain is being radiated on the lower half of the body, causing it to travel down from the back of the leg to the calf and the foot, hitting the sciatic nerve, thus developing sciatica. When this happens, many individuals will begin to feel worse from the leg pain than the low back pain since the sciatic nerve is inflamed and sending sharp, shooting pain along the leg, causing a person to be miserable.
Other research studies have shown that lumbar radiculopathy can cause by lumbar disc herniation and degeneration of the spinal vertebra. Some of the symptoms of lumbar radiculopathy usually depend on how severe the damaged nerve signals are and what degenerative conditions are happening to the spine. Some of the conditions include:
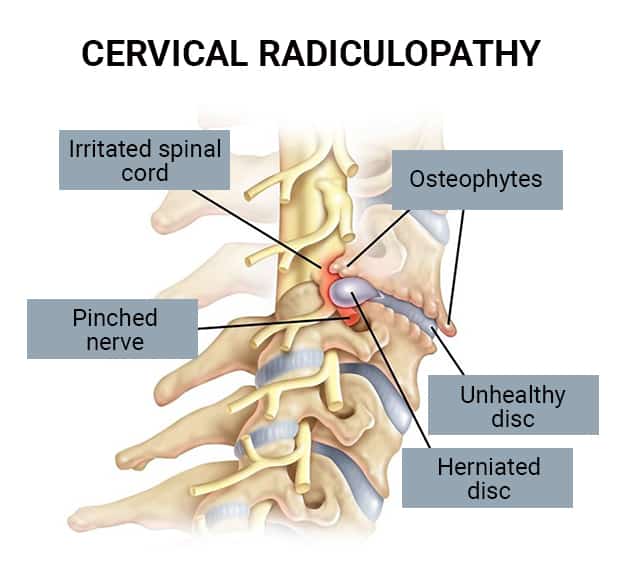
Research studies have stated that cervical radiculopathy is described when the nerve root from the cervical spine has become inflamed or damaged. Since the nerve roots are branched out from the spinal cord and help supply many motor functions to the neck, shoulders, arms, hands, and fingers, nerve damage to the cervical spine can cause immense pain. This can cause neurological deficits that can result from changes in neurological function in the body.
Other research studies have shown that when individuals are suffering from cervical radiculopathy, it is due to either the nerve root being compressed or inflamed that can cause a variety of symptoms that can affect the quality of life of a person. Some of the signs that are caused by cervical radiculopathy include:
The video above explains how the DRX9000 is used on lower back pain individuals. The DRX9000 is often used for spinal decompression therapy as it gently stretches the spine and helps relieve unwanted back pain that the individual is suffering from. The DRX9000 is a traction machine that will help elongate the spine as it helps decompress the compressed and irritated spinal discs. The spinal disc will feel negative traction pull, and the necessary beneficial nutrients and oxygen rehydrating those discs and reabsorb the herniation back into the spine. Many individuals that utilize spinal decompression with the combination of physical therapy as part of their wellness journey will begin to get their quality of life back. If you want to learn more about spinal decompression therapy, this link will explain the benefits of spinal decompression and how it can alleviate low back pain symptoms.
How Spinal Decompression Treats Radiculopathies
Research studies have shown that when spinal decompression is combined with a routine physical therapy can help improve the pain caused by radiculopathy while also providing a lumbar range of motion, back muscle endurance, and bringing the quality of life back to many individuals. Since spinal decompression is when a person is lying on a traction table, fully strapped and gently pulled, that will allow relief to their spine. Other studies have shown that when lumbar traction is applied to individuals that are suffering from radiculopathies will feel a decreased pressure by vertebral separation to reduce the pinched nerve. Individuals who utilize spinal decompression for at least six weeks of treatment recommended by their primary physicians will begin to feel less pain in their back and feel better throughout the day.
Conclusion
All in all, radiculopathy is often described as a range of symptoms that can occur in different parts of the spine. Both lumbar and cervical radiculopathy have the exact causes as it involves a pinched nerve root that is compressed and inflamed, causing pain symptoms from the neck to the foot. With spinal decompression and physical therapy, many individuals will begin to feel instant relief as their spine is being gently stretched and the beneficial nutrients are reabsorbed back into the spine. Afterward, many individuals will be able to get back their quality of life pain-free.
References
Alexander, Christopher E, and Matthew Varacallo. “Lumbosacral Radiculopathy – Statpearls – NCBI Bookshelf.” StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 12 Feb. 2022, https://www.ncbi.nlm.nih.gov/books/NBK430837/.
Amjad, Fareeha, et al. “Effects of Non-Surgical Decompression Therapy in Addition to Routine Physical Therapy on Pain, Range of Motion, Endurance, Functional Disability and Quality of Life versus Routine Physical Therapy Alone in Patients with Lumbar Radiculopathy; a Randomized Controlled Trial – BMC Musculoskeletal Disorders.” BioMed Central, BioMed Central, 16 Mar. 2022, https://bmcmusculoskeletdisord.biomedcentral.com/articles/10.1186/s12891-022-05196-x.
Dydyk, Alexander M, et al. “Radicular Back Pain – Statpearls – NCBI Bookshelf.” StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 2 Nov. 2021, https://www.ncbi.nlm.nih.gov/books/NBK546593/.
Kang, Kyung-Chung, et al. “Cervical Radiculopathy Focus on Characteristics and Differential Diagnosis.” Asian Spine Journal, Korean Society of Spine Surgery, Dec. 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7788378/.
Khan, Rehan Ramzan, et al. “Effectiveness of Mechanical Traction in Supine versus Prone Lying Position for Lumbosacral Radiculopathy.” Pakistan Journal of Medical Sciences, Professional Medical Publications, 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8377889/.
Medical Professionals, John Hopkins. “Radiculopathy.” Johns Hopkins Medicine, 2022, https://www.hopkinsmedicine.org/health/conditions-and-diseases/radiculopathy.
Dr. Alex Jimenez DC introduces Dr. Brian Self DC, as he explains the procedures of how to treat patients that are dealing with back pain by using the DOC decompression machine. The DOC decompression machine is used for spinal decompression therapy as it utilizes traction by gently stretching the spine to allow nutrients and oxygen back to the compressed spinal discs and increasing the disc height for many individuals that are suffering from a herniated or bulging discs. If you want to learn more about spinal decompression therapy, this link will explain the benefits of spinal decompression and how it can alleviate low back pain symptoms. By referring patients to qualified and skilled providers specializing in spinal decompression therapy. To that end, and when appropriate, we advise our patients to refer to our associated medical providers based on their examination. We find that education is the key to asking valuable questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions, please call Dr. Jimenez at 915-850-0900.
[00:00:02] Dr. Brian Self DC: So the first thing we’re going to do is lumber supine. OK, so before the patient gets on the table, a couple of things for them to know, you want everything out of their front and back pockets, keys, wallets, cell phones, everything in their pockets. Have them take their belts off if they’re wearing belts, and then have them use the restroom before they get on the table. I don’t let patients use their phones on the table. I prefer that they relax and fall asleep if they can. The more relaxed the patient is on the table, the better the treatment will be. So when we’re doing a lumbar supine, this would be good for heavier or older patients who can’t lay on their stomachs. Also, flexion-based conditions would be the best supine. So spondylolisthesis or stenosis, or anything where flexion makes it better and the extension makes it worse. When we’re doing a lumbar supine, we’re looking for this red line at the bottom of this thoracic cushion. So we’re going to line this one up where we want it. And then, these two red tabs are equal to the distance from the top of the iliac crest to the lowest rib. OK, so as the patient gets taller, this will slide up. So on our shortest patient, these two red tabs will be touching each other just like that as the patient gets taller; this thoracic harness will slide up. So the pelvic harness always stays; the thoracic harness will slide up as needed. So a two to three-inch gap would be for a patient that’s about five foot four to about six foot tall. A four-to-five-inch gap would be about six foot to about six foot seven. So the shorter patient, this thoracic harness comes down, the taller the patient, the thoracic harness slides up to make more gaps here. So once we know where we want these harnesses, let’s say I’m treating somebody who’s a normal male height. I will put these harnesses exactly where I want them, and then I will tighten this. So that this one is not going to move, and then I’m going to grab one seat belt in each hand, and then I’m going to lay this down one time with the red line right at the cushion where we talked about. So I’m going to lay it down one time. So I’m not messing with the velcro, and I’m going to velcro it right here to kind of hold it in place. And then what I’m going to do is I’m going to spin around and hold everything with my left hand, with my right hand. I’m going to point to where I want the patient to sit, which is right about here at this angle. If they sit too low on the table, then the top of their iliac crest will only be about right here when they lay back. If I have them sit right when they lay back, the top of their iliac crest will be about where you want it, the top of the pelvic harness. So hold all these, so they don’t move around too much. Have the patient sit about right here and then have them lay back. Now, once they lay back, then what you’re going to do is you’re going to take this with your right hands. I think it’s easiest to grab this with your right hand, bring it across, tuck it under, reach across it with your left hand, and then bring it straight across so it’s nice and snug. And with my right hand, I tuck my thumb underneath there so my hands are not in the way. Next, we’re going to do the seatbelt. And we’re going to bring this across now; the easiest way to tighten the seatbelt is not to grab this and pull hard this way because that will move the patient if they’re in pain, OK? The easiest way is to grab this with your right hand. Grab this one with your left hand and feed it through, so you’re feeding it with your right as you’re pulling it with your left hand. So you’re feeding that through to get that nice and snug. And then what we want is this metal ring to be centered on the patient, OK? Now, when the patient sits down on the harness, this will bunch up, and there will be a lot of extra fabric under their rear ends. So what you want to do is grab this and pull it this way. Pull it away from the patient to get all the extra fabric out so that it’s nice and tight. You will go through this ring and back up and attach it to the bottom here. OK. So again, this is all nice and tight now, with no extra fabric in there. And then what we can do is put the knee pillows under. If we want the knee pillows to be taller, we can rotate them like this. So if we want more flexion in the spine, we can use the taller position. OK? So always do your lumbar harness first, and then do your upper harness last. So on our upper harness, we’re looking to come around and down to make an X pattern. OK. You want the patient’s lowest rib to be right in the middle here.
Lumbar Treatment
Dr. Brian Self DC explains how to set up the DOC decompression traction table for many individuals that are going in for a lumbar treatment. Lumbar treatment is used for many individuals who are suffering from low back pain and is treated by laying on their back.
[00:07:08] Dr. Brian Self DC: OK, so you’re coming across and down to encapsulate the patient’s lowest rib, and that should make an X if you did it correctly. Next, what we want to do is we want to choose the angle that we’re going to be treating. So we go to the computer, and then we’ll go to elevation in targeting. And then, we could do a pre-programmed level to hit L5 S1 on a computer and then begin targeting setup. And then, we can treat it at that predetermined angle. Now, suppose we don’t want to do the predetermined angle. We can constantly adjust the lumbar flex or lumbar flex down until we find the comfortable angle centralizing the symptoms. The most important thing is finding the angle that centralizes the pain, the numbness, the tingling. Anything that makes the pain go farther down the leg into the foot is making it worse. Anything that centralizes and brings those symptoms to the spine probably makes it better. So you’re looking for that comfortable position that centralizes the symptoms. Now, at this point, we could add some lateral flexion if we wanted. So if we go to the bottom of the table here? The table will flex left and right laterally if you squeeze just the left mechanism. OK, so this would be for a lateral bulging disk. The table will rotate left and right if we squeeze just the right one. When that comes into play, if you have a patient sitting in the waiting room and leaning like this to take the pressure off the nerve, you will recreate whatever lean they have on the table and treat it in that position. So if they’re in left lateral flexion with left rotation, you would put the table into left lateral flexion with left rotation. So, recreate whatever position and centralize their symptoms on the table itself. So whether that’s flexion or lateral flexion or rotation or a combination, you want to figure out what positions bring them relief and put the table into that position, OK? Or if they’re walking down the hallway and leaning to the left while they’re walking, then you would just recreate that position on the table and do the treatment in that position. So now that we’ve chosen our angle, we want to tighten everything down so we would come up here, pull this nice and tight, and then go up to this upper one up here. So we go up here for this one, nice and tight, making sure all the slacks are out of there, and then we would be ready to treat. And then so we would go here, go to our automatic decompression menu. If it’s their first week, we will select legacy number one. And then we’re going to hit confirm lumbar treatment; since we’re doing a lumber treatment. And then, we would choose their treatment kilograms, which will be based on one-third of the patient’s body weight for a lumbar or 10 percent for cervical. So we put in our kilograms and then select the number of cycles that we want to do. The number of cycles determines the amount of time that the treatment takes. I recommend starting with one cycle for the first visit and seeing how they do. And then going up one cycle per visit for the first five visits. So visit one, one cycle, visit two, two cycles, visit three, three cycles, visit four, four cycles, and then visit five, five cycles. And then that’s about the most you would want to do on legacy one because that’s going to be about a twenty-five-minute treatment that would allow you to do a 30-minute appointment time. And your treatment time is going to be about twenty-four minutes, which gives you six minutes to take the patient on and off the table and still maintain 30-minute appointment times. So around twenty-three minutes is about the most I would do on a lumber treatment. With your cervical treatments, you can get away with less time. You can do as low as 15 minutes on the cervical and get good results. Once we’re all set up here, once we’ve set up our treatment parameters in the computer, we would just hit start and start the treatment.
[00:12:36] Dr. Alex Jimenez DC: Remind me that we start on legacy one cycle one on the first day, correct?
[00:12:48] Dr. Brian Self DC: Correct.
[00:12:50] Dr. Alex Jimenez DC: And every day, one cycle.
[00:12:53] Dr. Brian Self DC: Correct, and only up to five cycles on that.
[00:12:56] Dr. Alex Jimenez DC: Five cycles. OK. And we should continue with those five cyles?
[00:13:07] Dr. Brian Self DC: Until you feel like they’re stable and until you feel like you’re not going to make them worse and they’re ready to go on to a more aggressive treatment, which would be K one if it’s a herniated or a bulging disc or K five if it’s a degenerative disc.
[00:13:28] Dr. Alex Jimenez DC: Well, I’ll clarify one thing. I’m just asking if we should maintain the five cycles after 14 days?
[00:14:00] Dr. Brian Self DC: Yes, unless you feel like you’re going to maintain those five cycles until you feel like they’re ready to progress to K1. Now, that might be after one week. It might be after two weeks, but do the five cycles until you feel like they’re ready to go to the following protocol.
[00:14:22] Dr. Alex Jimenez DC: Is it normal to continue the cycles for one week or two weeks?
[00:14:29] Dr. Brian Self DC: Yeah, one to two weeks is usually average for most people.
[00:14:34] Dr. Alex Jimenez DC: Right.
[00:14:37] Dr. Brian Self DC: Now, if the patient is stable on their end, they’re not that bad every once in a while. You might progress a little bit faster. Or sometimes, patients are just prolonged to respond. And in that case, then you might want to do the legacy one, you know, for a lot longer. It just depends on the patient.
[00:15:03] Dr. Brian Self DC: OK, so that’s lumber supine.
[00:15:09] Dr. Alex Jimenez DC: So we continue the cycles for the next two weeks, and when we feel the patient is now ready to progress to the following protocol, can we go for the K1 protocol?
[00:15:43] Dr. Brian Self DC: Yes, you can go for K1 whenever you feel the patient is ready.
[00:15:49] Dr. Alex Jimenez DC: And how long is the K1 protocol?
[00:15:52] Dr. Brian Self DC: Generally that the whole rest of the treatment. So if it’s a herniated or a bulging disc, you would do K1 for weeks two through six, or if it’s a degenerative disc, you will do K5 for weeks two through six.
Prone Treatment
Dr. Brian Self DC explains how the DOC decompression is used for prone treatment. Prone spinal treatments are for many individuals that are suffering from posterior-lateral herniated or bulging disks and are treated by laying down on their stomachs either at an angle or flat on the DOC table.
[00:16:45] Dr. Brian Self DC: So next, it will be prone. Prone is suitable for younger patients with a posterior or a posterior-lateral herniated disk. So any patient that comes in between like 20 and 40 years old, that’s got a posterior bulging disk. And they say that flexion makes it worse. And extension makes it better; you’re probably going to put them prone. You would do prone because if they’re lying on their stomach on a poster bulging disk, the disk will be pointing up. Gravity is working in the direction you want the disk to go. So on a posterior bulging disc, prone is generally going to be a better treatment position. Now for prone, you’re probably starting with the table flat. So for prone, you’re probably going to start with the table flat, and then I’ll usually go up a couple of degrees per treatment if they can tolerate it. So for the first visit in prone, you don’t need these knee pillows, you would just lay them flat, and then you may come up into extension about two or three degrees per treatment. So as long as they can tolerate it, you can go up to extension with each treatment as long as they’re handling it. Now, it might not be super comfortable, but it can be more effective from a treatment standpoint, and then you can even add some extension here in the cervical. So this is putting them almost into like a MacKenzie type of protocol. And again, this is best for a herniated or bulging disc in a young patient where flexion makes it worse, and the extension makes it better. Now they may only be able to tolerate prone completely flat, and that’s OK. That’s a good position too. So just do prone, but completely flat. The only difference is with your armrests; you will have your armrests in the lower slots facing forward for a prone. OK, so your armrests are down there in the lower slots. Whereas supine, they’re going to be in the upper slots in line with the table.
[00:19:52] Dr. Brian Self DC: If the patient is supine, this would go in the upper slots just directly in line with the table there. OK, so that’s going to be supine, and then down here is where you put your armrests for your prone treatment.
[00:21:46] Dr. Brian Self DC: So there’s no predetermined angle for prone. Everything is going to be the same as supine. The only difference is you’re just going to manually go up or down depending on how much flexion or extension you are. You’re still going to choose legacy one and then confirm a lumber treatment.
Cervical Treatment
Dr. Brian Self DC explains how the DOC decompression machine is used for cervical treatment. Cervical treatment is used for many individuals that are suffering from neck and shoulder pains. The DOC decompression machine gently stretches the neck for the individual to have relief.
[00:22:40] Dr. Brian Self DC: So next, I want to go over cervical. So for cervical, what you’re going to do is you’re going to take your pelvic harness. And I usually just drap it off the end of the table out of the way with your thoracic harness. You need to remember that you want to take this post out with a thoracic harness, OK? So never pull this through this clamp because most people will put it back in the wrong way, and then it doesn’t work. So always when you’re doing this cervical, always take this whole bar out with this and then just set it to the side. So what you’re going to do is you’re going to take your cervical headpiece, and the first thing you’re going to do is adjust the width of the head posts. So a number two on each side is about a small female neck, or a number three on each side would be like a larger female neck and a smaller male neck. So number three on each side. And number four on each side would be a large male head now, once you get up to number four. Then I recommend taking this pad out because if you have a really large head, you want it to sit a little deeper in there. So if you get a huge head and this is pulling out from underneath their head, then take this out so it can sink a little bit.
[00:25:23] Dr. Brian Self DC: So next, what you’ll do is you’ll go ahead and place this in between the two face cushions. OK, so please don’t put it in the slot where you took the other post out; it will go in between the two face cushions there. Next, what you want to do is you want to come to the table and adjust the flexion that you want, depending on which disc we’re treating. So if you go into your elevation and targeting menu, you’ll see where it says cervical flexion angle. And then, you would go to your chart and know that negative 18 degrees is C6 C7.
[00:26:07] Dr. Brian Self DC: If we were treating C6 C7, we would take our cervical flexion angle on our computer until it says negative 18 degrees. Now what I like to do is just take a hand towel and put it over the cervical headpiece. Kind of tuck it down under.
[00:26:39] Dr. Brian Self DC: So tuck your towel in there, lay the patient down, and then you’re going to bring this up over their forehead start and then bring this just above their eyebrows. OK, so now the towel will keep all of the makeup, sweat, and everything off of your headpiece. OK, so that way, you don’t have to wipe everything down every time you can when the treatment is done. This covers everything.
[00:27:28] Dr. Brian Self DC: You can put the knee pillows under for comfort, for the knees, and then everything else would be the same except that your force will be about 10 percent of the patient’s body weight. So on the lumbar, we were about a third of the bodyweight. We’re going to be about 10 percent of the bodyweight on the cervical.
[00:28:11] Dr. Brian Self DC: You just go to the main menu and then elevation in targeting. And then just watch your cervical flexion angle in your bottom left-hand corner, and then you would look at your chart that I sent you, and then you would say, “OK, C7-T1 is negative.”
[00:28:34] Dr. Brian Self DC: You would look at the chart and say, “OK, C7-T1 is negative twenty-two degrees.” So you would just go up until your cervical flexion angle says negative twenty-two degrees.
[00:28:52] Dr. Brian Self DC: Or if it were C6 C7, you would go down until it says negative 18 degrees.
[00:29:19] Dr. Brian Self DC: So that’s it for cervical. And then you would just choose legacy number one for the first one to two weeks, and then you would go to K1 if it’s a herniated or bulging disc for weeks two through six or K5, if it’s a degenerative disc, for weeks two through six.
[00:29:39] Dr. Alex Jimenez DC: Now, what is the length or duration of treatment for cervical?
Conclusion
Dr. Brian Self DC recaps the number of sessions for spinal decompression using the DOC decompression machine. Whether it is for lumbar, prone, or cervical treatment, spinal decompression will provide instant relief for many individuals.
[00:29:50] Dr. Brian Self DC: You will probably do it every day for two weeks and then three times a week for two weeks and two times a week for two weeks.
[00:30:04] Dr. Alex Jimenez DC: And lumbar is every four weeks?
[00:30:06] Dr. Brian Self DC: Yes. The cervical will generally respond faster and easier, so you can get away with it three times a week for six or seven weeks if you have to on cervical. Now lumbar, I recommend every day, with cervical; you could do a little bit less and still get excellent results. Now I will tell you that patients don’t tolerate the cervical sometimes. They complain that it makes the area go numb back here or complain about a temporary headache over the forehead. Right? That’s OK. That’s perfectly normal. I tell patients, you know, just to be patient. The results will still be excellent, but it’s not comfortable for some patients. The other thing I forgot to tell you is if patients are wearing glasses, have them take off their glasses. If they have huge earrings like big hoop earrings, then have them take off the earrings. But other than that, it’s pretty straightforward.
[00:31:12] Dr. Alex Jimenez DC: So, if you feel some numbness on the back or have a headache on the forehead, what should be the way to manage the patient? I mean, if somebody is complaining, then how should we do that?
[00:31:26] Dr. Brian Self DC: You can add this if you want. So this will go in between the two black occipital posts. So you can add this, I wouldn’t say I like to use this if I don’t have to, but you can add that and then add the towel over that to make it a little more comfortable.
Non-surgical spinal decompression relieves pain related to spinal conditions, injuries, and disorders that provides a comfortable, affordable alternative treatment option to costly and invasive surgical procedures. Non-surgical spinal decompression can also relieve pain associated with post-surgical rehabilitation. A key to successful outcomes is including added components of the treatment that includes spinal decompression nutrition.
Spinal Decompression Nutrition
Proper nutrition and a balanced diet are essential elements of overall health. Individuals suffering from herniated discs, bulging discs, degenerated discs, sciatica, and chronic low back and neck pain are often deficient in vitamins and minerals, leading to inflammation and pain. These deficiencies can cause or exacerbate the pain and prevent or slow down healing. The bones, muscles, and other structures in the spine need proper nutrition to be strong enough to support the body and perform functions optimally. A health coach and nutritionist can recommend the proper diet and supplements to expedite healing, depending on the patient, the circumstances, and the individual situation. A non-inflammatory diet can make a big difference in patients’ symptoms and the effectiveness of decompression therapy.
The Right Foods
Eating a balanced diet with the right amount and variety of vitamins and nutrients can reduce back problems by nourishing the spine’s bones, muscles, discs, and other structures. While a healthy diet calls for various vitamins and nutrients, several healthy choices can directly benefit the spine. First and foremost is:
Sugar and Nitrate Reduction
High sugar diets lack the nutrients needed to prevent the release of inflammatory mediators.
The average individual consumes around 100 lbs of sugar per year.
Dessert foods are high infatty acids, which increase inflammation.
Any foods containing high fructose corn syrup like salad dressings and sodas.
Processed foods high in nitrates like hot dogs, sausage, and lunch meats.
Super Foods
Increase healing of the spine at the cellular level with superfoods that include:
Water – maintaining hydration is important for re-hydrating degenerated, dried-out discs.
Pre Spinal Decompression Nutrition
The human body was created to heal itself; however, getting the proper nutrition can be difficult as circulation is impeded/blocked when going through a back injury or spinal condition. Eating and/or supplementing with essential nutrients and minerals could be recommended to encourage and engage the healing process. Using nutrients to improve recovery and healing is known as immunonutrition. Pre-decompression allows the tissues to begin healing. Then the chiropractic health team can prepare the tissues for decompression through therapeutic massage, heat, low-level laser therapy, and ultrasound.
DRX9000 Explained by a Neurosurgeon
References
Calder, Philip C. “Fatty acids and inflammation: the cutting edge between food and pharma.” European journal of pharmacology vol. 668 Suppl 1 (2011): S50-8. doi:10.1016/j.ejphar.2011.05.085
Gay R. “All About Spinal Decompression Therapy.” Spine-health. http://www.spine-health.com/treatment/chiropractic/all-about-spinal-decompression-therapy. Published September 2013. Accessed April 2015.
InformedHealth.org [Internet]. Cologne, Germany: Institute for Quality and Efficiency in Health Care (IQWiG); 2006-. What is inflammation? 2010 Nov 23 [Updated 2018 Feb 22]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK279298/
Innes, Jacqueline K, and Philip C Calder. “Omega-6 fatty acids and inflammation.” Prostaglandins, leukotrienes, and essential fatty acids vol. 132 (2018): 41-48. doi:10.1016/j.plefa.2018.03.004
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine