Throughout the entire world, the body is in constant motion and has to have the ability to do everyday movements. For the body, the back and the spine make sure that the body is upright, can do certain things like bend and twist, and even do everyday activities. When the back and spine get injured, it can cause unwanted symptoms like low back pain to occur and if not treated right away, it can turn into chronic low back pain over time. Sometimes the injuries could also be due to other factors that are ordinary actions like poor posture, lifting heavy objects, or overusing the soft tissues in the lower back can cause low back pain to occur and hinder a person. Fortunately, there are treatments that can help alleviate low back pain and reduce the pain that the person is in. Today’s article looks at how physical and decompression therapy can help alleviate low back pain and get back a person’s quality of life. By referring patients to qualified and skilled providers specializing in spinal decompression therapy. To that end, and when appropriate, we advise our patients to refer to our associated medical providers based on their examination. We find that education is the key to asking valuable questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions, please call Dr. Jimenez at 915-850-0900.
How Does Physical Therapy Help With Low Back Pain?
Ever feel muscle tightness around your lower back? How about a dull ache when you wake up and stretch? How about muscle strain from your torso when you are bent over working at your desk? This could be low back pain, and some treatments can help alleviate low back pain as research has stated that low back is common for many individuals worldwide at some point in their lives and is the most expensive to treat. When individuals suffer from low back pain, it causes them to miss out on work and try to find ways to alleviate low back pain. Luckily treatments like physical therapy can help alleviate low back pain and allow individuals to prevent it.
Incorporating physical therapy as part of recovery for low back pain is beneficial for many individuals that want to strengthen their back muscles. Research studies have found that individuals suffering from low back pain will go to physical therapy to alleviate the pain symptoms and increase the functionality of the back. Utilizing physical therapy for individuals suffering from low back pain can help strengthen the surrounding muscles on the back and provide less stress on the spine’s disc and joints since it is a non-surgical treatment. Other research studies have found that when individuals suffering from chronic low back pain do physical therapy, the exercises used to improve the back muscles can help produce a considerable reduction in low back disability and pain.
How Does Spinal Decompression Help With Low Back Pain?
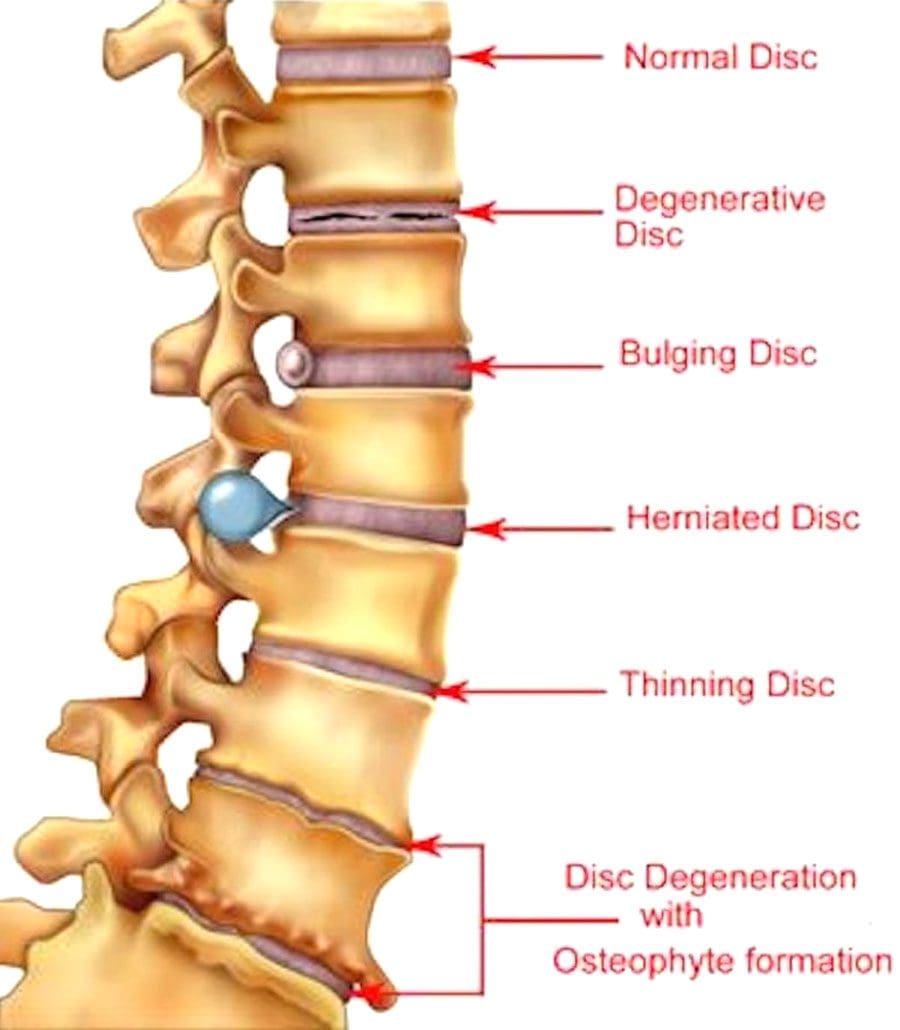
As part of the various non-surgical therapies out there to help alleviate low back pain, spinal decompression can help reduce the symptoms of low back pain for many suffering individuals. Like chiropractic therapy and physical therapy, spinal decompression helps relax the tense back muscles and ligaments and decompresses the spinal discs on the spine. Research studies have shown that spinal decompression helps decrease the intensity of low back pain symptoms by reducing the back’s disability to function, increasing its endurance, and even improving the lumbar muscles’ range of motion. Incorporating spinal decompression can even help reduce symptoms of other issues that are associated with low back pain, like sciatica, herniated discs, DDD (degenerative disc disease), and pinched nerves.
Spinal Decompression & Low Back Pain-Video
Does twisting your body from side to side feel sore? How about feeling a dull, mild ache on your lower back when you bend over to pick something up? Or how about feeling numbness or a tingling sensation that travels from the lower back down to the feet? You might be experiencing low back pain, and spinal decompression may be the answer to alleviate these symptoms. The video above shows and explains how the DRX9000, a spinal decompression machine, is used to help individuals suffering from lower back pain. Spinal decompression does to the lower back is that it incorporates traction when a person lays down on the DRX9000 and is strapped in. This allows the person’s spine to be gently stretched and causes the compressed spinal discs to take pressure off the nerve roots spread out throughout the spine. This treatment provides instant relief to the back and spine while the necessary nutrients traveling throughout the body return to the spine to re-hydrate the spinal discs. Suppose you want to learn more about how decompression therapy can benefit you. In that case, this link will explain what spinal decompression therapy does to help reduce low back pain.
How Physical & Decompression Alleviate Low Back Pain Together?
Since mostly everybody suffers from low back pain at some point, it can develop into chronic low back pain when it is not treated right away. If it progresses gradually, it can cause degenerative lumbar spinal stenosis and cause many issues for the individual. Fortunately, low back pain treatments that are non-surgical can help the lower back and reduce the symptoms. Since physical and decompression therapy work together to alleviate low back pain, research studies have found that combining these two can reduce low back pain in many individuals. It is essential to know that after doing a spinal decompression treatment, it is best to wait for a few weeks before getting back into physical therapy. This allows the spine to recuperate before doing an intense workout out. However, research studies showed that combined physical and decompression treatment reduces the pain and disability of chronic pain on the lumbar discs for individuals.
Conclusion
Overall, the combination of physical and decompression therapy can help many individuals suffering from low back pain. Each of the treatments alone can treat low back pain symptoms and reduce the pain, but when combined, it can help with the longevity of the spine and back muscles. Having low back pain is common for many individuals and can cause them to go to their primary physicians to get time off work. Utilizing non-surgical treatments for low back pain allows individuals to get their lives back together pain-free.
References
Amjad, Fareeha, et al. “Effects of Non-Surgical Decompression Therapy in Addition to Routine Physical Therapy on Pain, Range of Motion, Endurance, Functional Disability and Quality of Life versus Routine Physical Therapy Alone in Patients with Lumbar Radiculopathy; a Randomized Controlled Trial.” BMC Musculoskeletal Disorders, BioMed Central, 16 Mar. 2022, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8924735/.
Casiano, Vincent E, et al. “Back Pain – Statpearls – NCBI Bookshelf.” StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 22 Feb. 2022, https://www.ncbi.nlm.nih.gov/books/NBK538173/.
Dickerman, Rob. “Physical Therapy for Low Back Pain Relief.” Spine, Spine-Health, 20 Dec. 2005, https://www.spine-health.com/treatment/physical-therapy/physical-therapy-low-back-pain-relief.
F;, Gaowgzeh RAM;Chevidikunnan MF;BinMulayh EA;Khan. “Effect of Spinal Decompression Therapy and Core Stabilization Exercises in Management of Lumbar Disc Prolapse: A Single Blind Randomized Controlled Trial.” Journal of Back and Musculoskeletal Rehabilitation, U.S. National Library of Medicine, 2020, https://pubmed.ncbi.nlm.nih.gov/31282394/.
Hoffman, Haydn, et al. “Minimally Invasive Decompression and Physiotherapy for Lumbar Spinal Stenosis in Geriatric Patients.” Cureus, Cureus, 11 June 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6089476/.
Maher, C G. “Effective Physical Treatment for Chronic Low Back Pain.” The Orthopedic Clinics of North America, U.S. National Library of Medicine, Jan. 2004, https://pubmed.ncbi.nlm.nih.gov/15062718/.
Injury Medical Spinal Decompression: Spinal decompression therapy/treatment can be surgical or non-surgical, with differences in the procedure, recovery time, and results. Individuals who experience compression-related problems can have severe and prolonged spinal conditions that can lead to various health issues. Individuals experiencing persistent or chronic neck, back, or leg pain should know the differences between surgical and non-surgical spinal decompression. Spinal decompression aims to relieve pressure on the discs and reduce stress on the nervesto eliminate the pain associated with compression on the spine,restoring optimal circulation and improving spinal function.
Surgical Procedure
It is invasive, must be performed by a surgeon, and can have a recovery time of up to 6 weeks.
Surgery is usually suggested as a last resort after alternative therapies have not succeeded or when the compression is so severe that surgery is the only option.
Surgical spinal decompression is directed towards removal to reduce pressure instead of adjusting or stretching the discs.
In cases of severe nerve compression, surgery can be an effective option.
Risks include infection, damage to the spinal cord, and blood clots.
Types of Spinal Decompression Surgery
Types of surgeries; spinal fusion could be necessary to stabilize the spine. Common types of back surgery:
Discectomy
This procedure removes a portion of the disc to relieve pressure on nerves.
Laminotomy
The procedureremoves a small portion of the bone or a section of the bony arch to increase the size of the spinal canal and relieve pressure.
Laminectomy
The procedureremoves theentire bony arch or lamina to increase the size of the spinal canal and relieve pressure.
Foraminotomy
This procedure removes bone and other tissue to widen the openings for the nerve roots to pass through.
The procedure removes a vertebral body along with discs.
Injury Medical Spinal Decompression
Surgery for a damaged/injured spine is not always necessary. Treatment regimes vary depending on each individual’s medical condition. Non-surgical motorized spinal decompression is a non-invasive back treatment that uses a mechanized decompression table to slowly and gently stretch the spine. The therapy gradually relieves the pressure on the compressed nerve root/s resulting in reduced or complete alleviation of pain.
Oxygen, water, and nutrients circulate abundantly, promoting healing as the discs re-hydrate, and are re-nourished, improving and enhancing spine function. Individuals can enjoy increased levels of mobility, strength in the spine and muscles, and more flexibility.
Descompresión Espinal Con La DRX9000
References
American Spinal Decompression Association: “Spinal Decompression Therapy.”
Daniel, D.M. Chiropractic and Osteopathy, 2007.
Macario, Alex, and Joseph V Pergolizzi. “Systematic literature review of spinal decompression via motorized traction for chronic discogenic low back pain.” Pain practice: the official journal of World Institute of Pain vol. 6,3 (2006): 171-8. doi:10.1111/j.1533-2500.2006.00082.x
O’Hara K, editor. Decompression: a treatment for back pain. Vol. 11. National Association of Healthcare Professionals; 2004. pp. 1-2.http://www.naohp.com/menu/publications/mccu/bibliography.htm#10 [Google Scholar]
The body is a fine-tuned machine that is on the move constantly. Whether it is everyday movements, lifting objects, going to work, or doing some sort of physical activity, the body is on the move and needs to rest when it is tired. Sometimes different scenario factors can affect the body like an injury, a condition that can cause autoimmune responses, or ordinary factors like reading a book, texting, or working with a computer can cause the body to slouch or develop poor posture. Luckily all is not lost as there are ways to help alleviate poor posture through non-surgical treatments. Today’s article focuses on poor posture, how it affects the back, and how decompression therapy can help individuals in correcting their poor posture. By referring patients to qualified and skilled providers specializing in spinal decompression therapy. To that end, and when appropriate, we advise our patients to refer to our associated medical providers based on their examination. We find that education is the key to asking valuable questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions, please call Dr. Jimenez at 915-850-0900.
What Is Poor Posture?
Have you ever felt a dull ache around your shoulders and neck? How about hunching forward while working on the computer and feeling a pulled muscle on the side of your back? Or how about walking with a slouch? These types of scenario factors are all examples of poor posture. Research studies have found that when individuals do a combination of everyday actions, it can develop over time into a poor posture in the future. Poor posture does to the body is that it starts to weaken the lower back tissues and causes the back muscles, spinal discs, and joints to be pushed over the limit. This causes discomfort and pain to the body and the back.
Other research studies have found that the effects of poor posture cause a disturbance in the symmetry body axis that causes the body to develop poor posture. It also stated that when a person has developed poor posture and continues to perform work-related tasks in a slouch or hunched position, it can increase their chances of having back pain.
How Does Poor Posture Affect The Back?
Since poor posture happens unintentionally to everybody. It causes them to hunch forward for long periods while they are texting, reading a book, or working on their laptop, which can cause the neck and back muscles to strain. Research studies have shown that people who have poor posture and chronic low back pain have altered activation muscle patterns in their trunk muscles. What this does, is that it causes the trunk muscles that are around the body to decrease their movement, become stiff and rigid, and causes postural instability. Other research studies have stated that poor posture can contribute to prolonged sitting and standing, awkward positions, and heavy physical work can cause low back pain. Luckily there are ways to correct poor posture while also alleviating low back pain on the body.
DRX9000 Decompression Therapy For Poor Posture-Video
Do you feel intense pain in your neck and shoulders after working on the computer all day? How about stiffness around your torso area? How about aches on your lower back? This could be due to poor posture, and spinal decompression therapy can help alleviate that. The video above shows how the DRX9000, a decompression therapy machine, can help with poor posture and alleviate low back pain symptoms. Research studies have stated that when individuals sit for more extended periods, it can cause discomfort to the lower back muscles and cause the individual to be in a slouched sitting position. Decompression therapy helps the individual find relief by gently pulling on the spine and allowing the necessary nutrients to return to the spine. This causes the tense back muscles to relax and increases the spinal discs’ height. Suppose you want to learn more about how decompression therapy can benefit you. In that case, this link will explain what spinal decompression therapy does to help correct poor posture.
How Decompression Therapy Can Help With Poor Posture
Even though it is natural for people to develop a hunched position while doing everyday activities, this can lead to poor posture if not corrected right away. Sometimes it can happen naturally as the body ages causing the muscles to hunch over and straining the back muscles. Luckily there are ways to help many individuals that have developed poor posture. Some people do physical activities to strengthen the back muscles by working in their correct forms. Others go to chiropractic therapy to have their spine realigned, and some go to spinal decompression therapy to relieve back pain and get their spine gently pulled. Research studies have found that decompression therapy uses non-gravity to adjust the direction angle of how the traction will ease the pressure of the intervertebral disc on the spine. This will help many individuals who have suffered from poor posture. Other studies have shown that decompression therapy can also reduce the ligament stenosis around the spine, decrease the pressure on the spinal disc and nerve roots, and slowly help correct the individual’s posture. This allows many individuals to feel an instant relief on their back and become more mindful of their posture.
Conclusion
Having a correct posture can prevent back issues like low back pain, stiff muscles, and compressed nerves that can cause pain to an individual. Naturally, as the body age, it causes the back muscles to lean forward and cause strain on the lower back, shoulders, and neck. This causes discomfort and muscle weakness that can hinder a person’s daily life. Luckily, treatments like spinal decompression can help individuals slowly get their posture back and alleviate their lower back pain. Spinal decompression allows the spine to be stretched out gently and causes an increase in the height of the spinal disc. This allows the individual to be feeling instant relief on their back and continue on their wellness journey.
References
Vad, Vijay. “Is Poor Posture Causing Your Back Pain?” Spine, Spine-Health, 9 Jan. 2020, https://www.spine-health.com/blog/poor-posture-causing-your-back-pain.
Choi, Jioun, et al. “Effects of Flexion-Distraction Manipulation Therapy on Pain and Disability in Patients with Lumbar Spinal Stenosis.” Journal of Physical Therapy Science, The Society of Physical Therapy Science, June 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4500015/.
Cramer, Holger, et al. “Postural Awareness and Its Relation to Pain: Validation of an Innovative Instrument Measuring Awareness of Body Posture in Patients with Chronic Pain.” BMC Musculoskeletal Disorders, BioMed Central, 6 Apr. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5889545/.
Jung, Kyoung-Sim, et al. “Effects of Prolonged Sitting with Slumped Posture on Trunk Muscular Fatigue in Adolescents with and without Chronic Lower Back Pain.” Medicina (Kaunas, Lithuania), MDPI, 23 Dec. 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7822118/.
Nowotny, Janusz, et al. “Body Posture and Syndromes of Back Pain.” Ortopedia, Traumatologia, Rehabilitacja, U.S. National Library of Medicine, 2011, https://pubmed.ncbi.nlm.nih.gov/21393649/.
Swain, Christopher T V, et al. “No Consensus on Causality of Spine Postures or Physical Exposure and Low Back Pain: A Systematic Review of Systematic Reviews.” Journal of Biomechanics, U.S. National Library of Medicine, 26 Mar. 2020, https://pubmed.ncbi.nlm.nih.gov/31451200/.
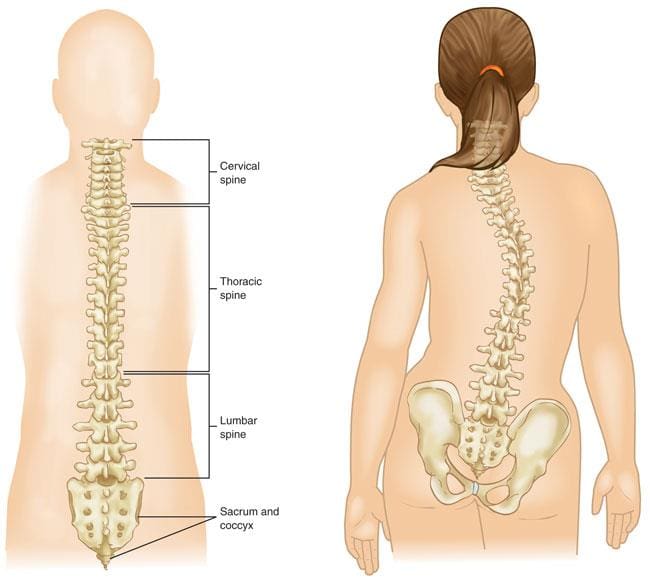
As part of the body in an S-shaped curve, the spine allows the body to move functionally and that it is being supported. The spine makes sure the body stays upright and can do everyday functions. The spine is also composed of ligaments, muscles, the spinal cord, and discs that protect the spine from injury. However, different conditions and injuries do occur in the spine that can cause a person to suffer and even develop symptoms that affect the spine. Spinal conditions like scoliosis, DDD (degenerative disc disease), and a herniated disc can affect a person’s quality of life. Luckily non-surgical treatments can help alleviate symptoms that affect the spine. Today’s article will discuss lumbar scoliosis, its symptoms, and how decompression therapy can help alleviate scoliosis symptoms for many individuals. By referring patients to qualified and skilled providers specializing in spinal decompression therapy. To that end, and when appropriate, we advise our patients to refer to our associated medical providers based on their examination. We find that education is the key to asking valuable questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions, please call Dr. Jimenez at 915-850-0900.
What Is Lumbar Scoliosis?
Do you feel uneven when you are walking? How about feeling back pain occurring in your lower back? Or does your range of motion feel limited? Any of these symptoms that you are experiencing could signify lumbar scoliosis. Research studies have found that scoliosis is a spinal deformity that causes the spine to be in a lateral curve and rotates the vertebrae themselves. Now scoliosis usually occurs when a person is a child, and their spine is curved. Naturally, the spine itself is in an S-shaped curve straight in the back; however, lumbar scoliosis is a sideways curvature of the lumbar region of the spine. Lumbar scoliosis usually occurs in adolescents to adulthood, depending on the severity of lumbar scoliosis is causing on the spine.
Other research studies have found that since the spinal disc naturally decreases due to average age can be one of the causes of lumbar scoliosis. This occurs when the spinal discs degenerate and lose their height and stability, causing stress on the facet joints. This causes degenerative changes to the spine and causes it to curve sideways and become deformed in the lumbar regions of the spine. When this happens, unwanted symptoms and factors will occur in the individual suffering from lumbar scoliosis.
The Symptoms
Depending on how severe the progress is with lumbar scoliosis individuals, it can range from having no symptoms to developing symptoms over time. Research studies have stated that some of the signs that occur for individuals who have lumbar scoliosis can include back pain and the development of numbness in the legs. This is due to the spine curving sideways in the lumbar region, causing the spinal disc and joints to press on the nerve roots spread throughout the spine, thus causing low back pain. Some of the other symptoms that research studies found for lumbar scoliosis include:
Are the aches in your back ranging from a mild, dull ache to severe radiating pain that goes down to your feet? How about feeling unstable when you are walking around doing errands? Or do you feel a limited range of motion when bending down or turning side to side? You could have lumbar scoliosis, and spinal decompression therapy can help alleviate these symptoms. The video explains how spinal decompression therapy can treat chronic back symptoms and issues like lumbar scoliosis and even low back pain. What spinal decompression does is help stretch the spine slowly and gently to alleviate the pressure that the nerve roots are suffering from. Spinal decompression therapy also allows the spinal disc to be restored in the spinal column. Combining chiropractic therapy can help restore the spine suffering from lumbar scoliosis back to its original placement. Suppose you want to learn more about how decompression therapy can benefit you. In that case, this link will explain what spinal decompression therapy does to the spine and how it can alleviate lumbar scoliosis.
How Spinal Decompression Therapy Alleviates Lumbar Scoliosis
As stated in previous articles, spinal decompression therapy is a non-surgical treatment that helps alleviate painful symptoms affecting the spine and back. What this treatment does is that it uses motorized traction on the spine itself and starts to gently pull the spinal joints to cause the relief to the back. Now spinal decompression can help individuals with lumbar scoliosis and back pain with chiropractic therapy to help position the spine back in its original form through traction and manipulation. Research studies have found that individuals with mild degenerative lumbar scoliosis have had excellent results since spinal decompression has helped improve radicular symptoms causing pain in the spinal joints. This allows many individuals to feel relief after being in pain. Other research studies have found spinal decompression combined with spinal fusion is another form of treatment. It is safe and effective for older individuals suffering from spinal conditions like osteoporosis and osteoarthritis. Compared with other therapies, decompression therapy can help restore a person’s quality of life and spinal health.
Conclusion
In conclusion, the spine allows everyday movement to the body without any issues or pain affecting the entire body structure. Spinal conditions like lumbar scoliosis can develop gradually over time and cause many individuals to suffer from spinal pain. Lumbar scoliosis causes a wide variety of symptoms in the spine as the vertebrae joints are rotated and curved sideways, causing pressure on the nerve roots and limiting the body’s range of motion. Treatments like spinal decompression therapy and other non-surgical treatments for the spine and back can help relieve the symptoms of lumbar scoliosis and allow the spine to return to its original state. With spinal decompression therapy, people can get back to their wellness journey pain-free and not have to feel miserable due to spinal conditions like lumbar scoliosis.
Janicki, Joseph A, and Benjamin Alman. “Scoliosis: Review of Diagnosis and Treatment.” Paediatrics & Child Health, Pulsus Group Inc, Nov. 2007, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2532872/.
Tsutsui, Shunji, et al. “Can Decompression Surgery Relieve Low Back Pain in Patients with Lumbar Spinal Stenosis Combined with Degenerative Lumbar Scoliosis?” European Spine Journal : Official Publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society, Springer Berlin Heidelberg, Sept. 2013, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3777068/.
York, Philip J, and Han Jo Kim. “Degenerative Scoliosis.” Current Reviews in Musculoskeletal Medicine, Springer US, Dec. 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5685967/.
Diabetes and severe blood sugar fluctuations can lead to back pain and spinal conditions. The negative impacts on the body from diabetes can be destructive as it is a state of chronic inflammation.
Spine Conditions and Diabetes
Spinal conditions being researched and their link to diabetes can affect each condition and its development differently.
Spinal Stenosis
Spinal stenosis is when the spine’s openings foraminabegin to shrink and narrow, causing the nerve roots that branch off the spinal cord to have less space to function.
The stenosis can compress one or more lumbar spinal nerves.
Pain, tingling, weakness, and/or numbness in the legs can begin to present.
Spinal Epidural Abscess
Spinal epidural abscess is an infection between the vertebral bones and the spinal cord membrane.
Diabetes increases the risk of infection and increases the risk of developing an abscess.
Hypertension and obesity can also increase the risk of infection.
Lumbar Disc Degeneration
The back contains spinal discs between each vertebra that are the shock absorbers.
Lumbar disc degeneration occurs when one or more discs begin to break down.
The disc’s deterioration causes changes in the lumbar/lower back structure.
The degeneration also causes back pain.
Disc degeneration is a normal part of aging and is expected. However, those who have lived with diabetes for over ten years have a higher risk of developing advanced lumbar disc degeneration. To prevent disc degeneration and/or minimize the adverse effects, it’s essential to maintain blood sugar levels.
Vertebral Osteomyelitis
Vertebral osteomyelitis is a rare spinal infection resulting from a spinal injury or post-surgical complication/s.
It is a bacterial infection that can travel to the spine from another location.
Diabetes increases susceptibility to infections.
For example, an individual with diabetes could have a foot ulcer, lower back pain, and a fever, symptoms that could indicate the development of vertebral osteomyelitis.
Chiropractic and Decompression Therapy
Spinal decompression is an effective non-surgical technique that can relieve back pain, leg pain, and symptoms associated with spinal conditions and disorders. It works by gently creating traction/pulling force with a specialized mechanical decompression table combined with chiropractic massage and adjustments. Benefits include:
Pain relief
Decompression relieves tension in tight, spasming, or injured muscles.
Stimulates the nervous system to release chemical signals that bring pain relief.
Heals spinal disc tissues
Decompression creates a vacuum force on the spinal discs, helping to circulate much-needed fluids, cells, and other substances to the damaged tissue/s.
Restores spinal disc and joint alignment
Stress, poor posture, poor body mechanics, and other factors can cause joints to shift out of place or the discs to herniate.
The vacuum force helps realign the joints and discs.
Prevents further pain and inflammation.
Restores mobility and function.
Relieves pressure on nerves
Spinal nerves can get pinched when discs, bones, or other tissues compress the small spaces causing inflammation and pain.
Non-surgical decompression increases the space around the nerves, allowing the nerves to heal.
Injury Medical Chiropractic and Functional Medicine Clinic offer spinal decompression as one of many treatment approaches to restore a high quality of life.
DOC Decompression Table
References
Anekstein, Yoram, et al. “Diabetes mellitus as a risk factor for the development of lumbar spinal stenosis.” The Israel Medical Association journal: IMAJ vol. 12,1 (2010): 16-20.
Eivazi, Maghsoud, and Laleh Abadi. “Low back pain in diabetes mellitus and importance of preventive approach.” Health promotion perspectives vol. 2,1 80-8. 1 Jul. 2012, doi:10.5681/hpp.2012.010
Heuch, Ingrid et al. “Associations between serum lipid levels and chronic low back pain.” Epidemiology (Cambridge, Mass.) vol. 21,6 (2010): 837-41. doi:10.1097/EDE.0b013e3181f20808
Rinaldo, Lorenzo, et al. “Diabetes and Back Pain: Markers of Diabetes Disease Progression Are Associated With Chronic Back Pain.” Clinical diabetes: a publication of the American Diabetes Association vol. 35,3 (2017): 126-131. doi:10.2337/cd16-0011
The spine allows the body to do various things like move, bend, twist, and turn without pain and making sure that it is kept in an upright position. The spine is also protected by ligaments, soft tissues, muscles, and spinal columns that make sure that no injuries are affecting the spine. However, when a person overworks their back, it can cause the back muscles to be sustained a variety of injuries like a pulled muscle, slipped spinal disc, herniation, and many others that can cause harm to the spine. Luckily there are many treatments that can help restore the back and spine through non-surgical procedures. Today’s article focuses on spinal osteoarthritis, its symptoms, and how spinal decompression can help individuals alleviate spinal osteoarthritis symptoms. By referring patients to qualified and skilled providers specializing in spinal decompression therapy. To that end, and when appropriate, we advise our patients to refer to our associated medical providers based on their examination. We find that education is the key to asking valuable questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions, please call Dr. Jimenez at 915-850-0900.
What Is Spinal Osteoarthritis?
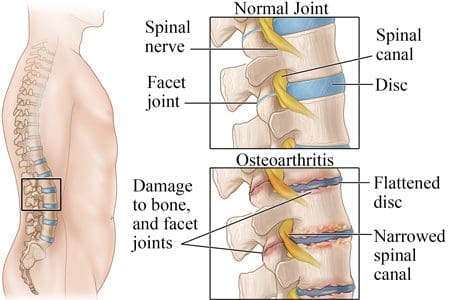
An S-shaped curve in the back known as the spine is encompassed by ligaments, the spinal cord, back muscles from the musculoskeletal system, and spinal discs that help the body with everyday movement and become mobile. Research studies have found that spinal osteoarthritis is a common condition associated with low back pain. However, as the body naturally ages, so does the spine as the spinal discs begin to degenerate and cause inflammation in the spinal joints, known as spinal osteoarthritis. Spinal osteoarthritis can develop gradually over time in the spine, causing a restriction of motion and pain.
Other research studies have found that low back pain and spinal osteoarthritis are both common and have the process of degeneration in the spine, causing the spinal disc space to be narrow while reducing the spine’s mobility. This causes the facet joints to develop other conditions like rheumatoid arthritis, spondyloarthritis, and gout to pop up and affect the spine.
The Symptoms
When the spine suffers from spinal osteoarthritis, it can cause various painful symptoms that affect a person’s quality of life. Research studies have shown that since spinal osteoarthritis is a gradual condition that is developed over time, it can cause stiffness in the spinal joints when a person is waking up in the morning, then eases throughout the day with physical activity, and flares right back up again at the end of the day. This happens when fluid build-up in the spinal joints can swell and cause inflammation to the spine. Other symptoms that are caused by spinal osteoarthritis can include:
Stiffness on the back and neck
Loss of joint flexibility
Swelling joints due to weather changes
Tenderness in some regions of the spine
Creptis (bone rubbing against each other)
Joint pain
Spinal Decompression For The Spine-Video
Do you feel tenderness around some regions of your back? How about feeling stiff on your lower back or neck? Or the weather seems to be causing swelling on your back? You could be suffering from spinal osteoarthritis, and spinal decompression therapy can help alleviate these symptoms. Spinal decompression therapy can help the spine through traction and gentle stretching. Spinal decompression helps alleviate the spinal disc and joints by slowly increasing their height and alleviating the painful symptoms. This will allow the necessary components like nutrients and oxygen to hydrate the compressed spinal discs and take the pressure off on the nerve roots. When individuals utilize decompression therapy, they can feel instant relief and get back their lives pain-free. Suppose you want to learn more about how decompression therapy can benefit you. In that case, this link will explain what decompression therapy does to the spine and how it can relieve spinal osteoarthritis symptoms.
Spinal Decompression Therapy For Spinal Osteoarthritis
Many treatments can help lower the inflammation that spinal osteoarthritis has caused on the spine, which many people can do and bring back their range of motion. Some people utilize anti-inflammatory supplements like omega-3s and turmeric to lower joint inflammation. Others use massages to relax the tense muscles while also being careful with the spine. In contrast, others use spinal decompression therapy to help alleviate the painful symptoms that spinal osteoarthritis has caused. Research studies have found that the spinal joints and spinal discs affected by spinal osteoarthritis cause a “second inflammatory” symptom. When individuals use spinal decompression, they feel relief. What spinal decompression does is that it lays the individual in a supine position and causes negative pressure on the spine. Other research studies have found that decompression can reduce the stress inside the spinal intervertebral disc and alleviate the painful symptoms that spinal osteoarthritis has caused. This non-surgical treatment provides impressive results for individuals who incorporate this in their wellness journey.
Conclusion
Spinal osteoarthritis causes joint stiffness and swelling in the spine, making a person feel miserable. The spine allows the body to be kept upright and move through various scenarios without causing the body to be in pain. When spinal conditions like spinal osteoarthritis cause inflammation in the spinal joints, it can lead to low back problems for the individual. Spinal decompression can gently stretch the spine and cause the relief to the joints as the necessary nutrients return to the spinal columns and increase the disc height. This will allow many individuals suffering from spinal osteoarthritis to feel instant relief and be pain-free.
References
Choi, Jioun, et al. “Influences of Spinal Decompression Therapy and General Traction Therapy on the Pain, Disability, and Straight Leg Raising of Patients with Intervertebral Disc Herniation.” Journal of Physical Therapy Science, The Society of Physical Therapy Science, Feb. 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4339166/.
Goode, Adam P, et al. “Low Back Pain and Lumbar Spine Osteoarthritis: How Are They Related?” Current Rheumatology Reports, U.S. National Library of Medicine, Feb. 2013, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3606549/.
Kang, Jeong-Il, et al. “Effect of Spinal Decompression on the Lumbar Muscle Activity and Disk Height in Patients with Herniated Intervertebral Disk.” Journal of Physical Therapy Science, The Society of Physical Therapy Science, Nov. 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5140813/.
Lieberman, Daniel. “Symptoms of Arthritis of the Spine.” Spine, Spine-Health, 26 Oct. 2016, https://www.spine-health.com/conditions/arthritis/symptoms-arthritis-spine.
Lindsey, Thomas, and Alexander M Dydyk. “Spinal Osteoarthritis – Statpearls – NCBI Bookshelf.” StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 12 July 2021, https://www.ncbi.nlm.nih.gov/books/NBK553190/.
The body functions throughout the world in a variety of scenarios. Whether the person is doing a sports activity, doing physical therapy, or commuting to get to their destination, the body has to be able to do these things without being in pain. However, things tend to affect the body, like a pulled muscle, an injury caused by an accident, autoimmune diseases, and others that can affect the body and the back. Today’s article focuses on muscle strains in the lumbar area of the back, their symptoms, and how decompression therapy can help alleviate lumbar muscle strains in the back. By referring patients to qualified and skilled providers specializing in spinal decompression therapy. To that end, and when appropriate, we advise our patients to refer to our associated medical providers based on their examination. We find that education is the key to asking valuable questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions, please call Dr. Jimenez at 915-850-0900.
What Are Lumbar Muscle Strains?
Have you felt a pinched nerve on your lower back? How about feeling a gradual, dull ache in your lower back muscles? Or how about tenderness in certain muscle areas of the lower back? You could be suffering from lumbar muscle strains on your lower back. The lower back of the body helps it move, twist, turn, and supports the weight of the upper body, keeping it upright. Research studies have stated that when the lower back is under an excruciating amount of stress, it can cause the soft tissues to become injured and painful to the touch. When the soft tissues in the low back are under a lot of stress and are over-stretched, the surrounding area where the soft tissue resides is inflamed. This will cause the area to be tender to the touch, cause muscle cramps, or cause intense pain when it contracts tightly.
The Symptoms
Since the soft tissues on the lower back help support the body and can be succumbed to injuries, it is essential to know that low back pain is one of the most common issues for many individuals worldwide. As one of the causes of disabilities and the highest healthcare expenses, many people who suffer from low back pain or muscle strains call off work. Research studies have shown that muscle strains are acute low back pains that can turn chronic over time. Some of the symptoms that muscle sprains do cause in the lower back include:
Other research studies have found that individuals with musculoskeletal disorders have noticed that they complained about radicular pain in their lower back and suffer muscle spasms. This is due to the overstretched lower back muscles, causing the spine to become herniated and pressing on the nerve roots spread out in the lower back.
Decompression Therapy Demonstration- Video
Feeling your lower back muscles ache and tender to the touch? How about muscle stiffness whenever you are walking or standing for long periods? Or how about pain in your lower back that is causing you to not go to work? If this has happened to you, then decompression therapy could benefit you. Decompression therapy allows traction to gently pull the spine and supply it with the necessary nutrients to restore the spinal discs to their original form. This will allow the spine to increase its disc height and take the pressure off the nerve roots causing the individual pain. After a couple of treatments, many individuals suffering from low back pain will begin to feel relief in their lower back. If you want to learn more on how decompression therapy can help you, this link will explain its benefits and how it can relieve muscle strains.
With many treatments that help alleviate muscle strain and low back pain, decompression therapy can help individuals by placing them on a motorized traction table and gently stretching their spine out. Research studies have stated that decompression therapy can reduce the pressure off the nerve roots and gradually increase mobility to the joints and relax the soft tissues caused by muscle sprains. This negative pressure allows the lumbar muscle region to be loose and prevents the intervertebral disc from herniated. Other research studies have shown that the ligaments from the back lumbar region will begin to relax, and the lumbar spine will increase disc height due to the negative pressure on the back. Many individuals will feel instant relief and continue on their wellness journey.
Conclusion
Overall, the soft tissues of the lower back allow the body to twist, turn, and move while making sure that it stays upright without feeling any pain whatsoever. When the lower back goes under a tremendous amount of stress, it can cause the soft tissues to be overworked and lead to injuries, low back pain, and muscle spasms. Luckily non-surgical treatments like decompression therapy allow the tight, overused muscles to relax while gently stretching the back to allow the necessary oxygen and nutrients to come back into the spinal disc. Traction on the spine allows the herniated disc to be pulled back into the spine and takes the pressure off the nerve roots in the lower back. This will decrease the inflammation in certain lower back areas, restore the torn muscles, and bring back a person’s quality of life.
References
Choi, Jioun, et al. “Influences of Spinal Decompression Therapy and General Traction Therapy on the Pain, Disability, and Straight Leg Raising of Patients with Intervertebral Disc Herniation.” Journal of Physical Therapy Science, The Society of Physical Therapy Science, Feb. 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4339166/.
El Sayed, Moustafa, and Avery L Callahan. “Mechanical Back Strain – Statpearls – NCBI Bookshelf.” StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 24 Jan. 2022, https://www.ncbi.nlm.nih.gov/books/NBK542314/.
Hamilton, Kojo. “Pulled Back Muscle and Lower Back Strain.” Spine, Spine-Health, 8 Sept. 2017, https://www.spine-health.com/conditions/lower-back-pain/pulled-back-muscle-and-lower-back-strain.
Hirayama, Jiro, et al. “Relationship between Low-Back Pain, Muscle Spasm and Pressure Pain Thresholds in Patients with Lumbar Disc Herniation.” European Spine Journal : Official Publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society, Springer-Verlag, Jan. 2006, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3454558/.
Kang, Jeong-Il, et al. “Effect of Spinal Decompression on the Lumbar Muscle Activity and Disk Height in Patients with Herniated Intervertebral Disk.” Journal of Physical Therapy Science, The Society of Physical Therapy Science, Nov. 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5140813/.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine