Avoiding Common Christmas Accidents: Prevention and Recovery at El Paso Back Clinic®
After lying in an awkward position, the woman is suffering from back pain on the couch at home.
The Christmas season fills homes with lights, laughter, and loved ones. But it can also bring unexpected risks. From slips on icy paths to burns in the kitchen, holiday accidents happen more often than you might think. In El Paso, Texas, where winter weather can mix with the festive rush, these issues send many seeking help. Distracted or drunk driving spikes too, making roads risky. At El Paso Back Clinic®, we focus on wellness chiropractic care to help you prevent and heal from these mishaps. This article explains common Christmas accidents, their causes, and tips for prevention. It also shows how our integrative approach, led by Dr. Alexander Jimenez, DC, APRN, FNP-BC, offers holistic recovery. Using spinal adjustments, massage, nutritional guidance, and NP-partnered care, we support your body’s natural healing to help you have a pain-free holiday.
Common Christmas Holiday Accidents at El Paso Back Clinic®
At our clinic in El Paso, TX, we see a rise in holiday-related injuries each year. These range from home mishaps to road incidents. Here’s a list of the most common ones we treat.
Falls: Decorating ladders or icy El Paso sidewalks leads to slips. These cause sprains, fractures, or head trauma. Nationwide, about 160 decorating falls occur daily, accounting for half of decorating injuries. Kids might tumble from unstable trees or during outdoor fun.
Fires: Faulty lights, dry trees, or candles spark fires. In homes across Texas, Christmas tree fires average 155 per year, causing injuries and property damage. We advise checking decorations to avoid these dangers.
Burns: Holiday cooking with hot oil or deep fryers can result in scalds. Touching lit decorations adds risk. Turkey fryers alone cause 5 deaths and 60 injuries annually. Even hot foods like fried treats can burn mouths.
Cuts: Knife slips while wrapping or carving happen often. Broken glass ornaments or toy packaging lead to ER visits – about 6,000 yearly for gift-opening cuts.
Strains: Lifting decorations, gifts, or snow strains muscles. Back issues account for 15% of holiday accidents, and 11,500 ER visits are due to shoveling. In El Paso, our patients often come in after heavy lifting.
Alcohol-Related Incidents: Festive drinks cause falls or “holiday heart” – heart rhythm problems from overdrinking. This leads to dizziness and more.
Food Poisoning: Rushed meals with undercooked food or leftovers breed bacteria. About 48 million cases occur in the U.S. each year, peaking during holidays.
Injuries Related to Toys and Gifts: Choking on small parts injures 251,700 kids yearly. Faulty gifts cause cuts or trips.
Distracted or Drunk Driving: Busy El Paso roads see more crashes from texting or drinking. Drunk driving deaths rose to 1,013 in December 2021.
These issues increase ER visits by 5-12% in the U.S. and by over 80,000 in the UK during festivities. At El Paso Back Clinic®, we help locals recover quickly.
Causes of Holiday Injuries Seen at Our Clinic
Many injuries stem from everyday tasks gone wrong. To stop recurrences, we at El Paso Back Clinic® pinpoint these causes.
Overexertion: Heavy lifting, like trees or bags, strains backs. Bending incorrectly causes 80% of lower back pain. Travel luggage accounts for 72,000 doctor visits each year.
Cooking: Burns from oils or knives in busy kitchens. One in ten child injuries comes from cooking. Grease fires are frequent.
Decorating: Ladder falls, electrical shocks, or ornament cuts. Decorating sends 13,000 to ERs yearly. Cord trips cause 2,000 injuries.
Accidents on the Road or at Home: Distracted driving in El Paso’s traffic or at home. Stress slows reflexes.
Winter sports add 186,000 injuries, though they are less common here. Plants like mistletoe can poison if eaten.
Prevention Tips from El Paso Back Clinic®
Prevent accidents with simple steps. Our team at El Paso Back Clinic® shares these to keep your holidays safe.
For Falls: Use stable ladders and salt icy paths. Get help when climbing.
For Fires and Burns: Inspect wires, water trees, and use LED candles. Watch stoves closely.
For Cuts and Strains: Cut safely and lift with your knees. Team up for heavy items.
For Alcohol and Driving: Designate a driver or use a ride. Drink moderately.
For Food and Toys: Cook thoroughly and chill food fast. Pick safe, age-appropriate toys.
Keep a first aid kit handy and manage stress. Visit us for pre-holiday check-ups.
How Integrative Chiropractic Care at El Paso Back Clinic® Helps
If injured, turn to El Paso Back Clinic® for natural healing. Our integrative chiropractic care, in partnership with NPs, treats the whole person. Dr. Alexander Jimenez, with over 30 years in El Paso, observes that holiday injuries often stem from poor posture or stress, leading to misalignment of the spine. We use non-invasive techniques to ease pain without meds or surgery.
Adjustments for Spinal and Joint Pain: Realign the spine to relieve strain from falls or lifts. This boosts movement and cuts swelling.
Massage and Physiotherapy for Muscle Problems: Ease tension from overwork. Improves circulation for faster recovery.
NP-Led Care for Holistic Wellness: Our NPs manage overall health, including burn care and effects of poisoning, with a natural focus.
Nutrition Guidance: Counter rich holiday foods with diet tips to aid digestion and immunity. Fiber-rich choices help.
Managing Underlying Conditions: Reduce stress hormones for better sleep and mood. Prevents further harm.
Dr. Jimenez’s team uses functional medicine to develop personalized plans that address issues like sciatica from slips. Chiropractic enhances the nervous system for better health during the holidays.
Enjoy a Healthy Holiday with El Paso Back Clinic®
Make Christmas memorable for the right reasons. Know the risks, prevent them, and seek our care if needed. At El Paso Back Clinic®, we’re here for your wellness. Contact us in El Paso, TX, for expert chiropractic support. Happy holidays!
Best Magnesium Supplements for Pain Relief: Types, Benefits, and Chiropractic Insights
A chiropractor and nurse practitioner discuss magnesium supplements for pain relief.
Magnesium is a mineral that your body needs for many tasks. It helps muscles work, nerves send signals, and bones stay strong. Many people do not get enough magnesium from food like nuts, seeds, and greens. This can lead to problems such as muscle pain, fatigue, and stress. Supplements can help fill the gap. In this article, we look at how magnesium eases pain. We focus on forms such as malate, glycinate, and topical. These can help with muscle soreness, nerve pain, and more. Chiropractors often suggest them to boost treatments. We base this on health sites and expert views. Read on to learn which type might work for you.
Pain comes in many forms. It can be sore muscles after a workout or chronic issues like fibromyalgia. Magnesium helps relax muscles and calm nerves. It also cuts down on swelling. Studies show it can lower pain without strong drugs. For example, it supports energy production, helping counter fatigue associated with pain. Different forms absorb in unique ways. Oral pills go through the gut. Topical ones soak into the skin. This matters for how fast they help. Always talk to a doctor before starting supplements. They can check if it’s safe for you.
Understanding Magnesium’s Role in Pain Management
Magnesium plays a big part in how your body handles pain. It blocks pain signals in nerves and helps muscles relax. Low levels can make pain worse. About half of adults in the U.S. lack enough magnesium (Team Red White & Blue, n.d.). This leads to cramps, spasms, and soreness. Supplements fix this by boosting levels.
Here are key ways magnesium helps with pain:
Muscle Relaxation: It controls contractions to stop cramps and tension.
Nerve Calming: It balances signals to reduce nerve pain.
Less Swelling: It fights inflammation that causes discomfort.
Better Recovery: It supports energy for healing after injury.
Chiropractors use magnesium with adjustments. It improves treatment outcomes by loosening tight spots. For acute pain, like after surgery, it cuts down on opioid needs (MedCentral, n.d.). For long-term pain, it eases symptoms in conditions such as migraines and back pain.
Magnesium Malate: Effective for Muscle Soreness and Fatigue in Fibromyalgia
Magnesium malate mixes magnesium with malic acid. This form absorbs well in the gut. It boosts energy by helping make ATP, the body’s fuel (Miye Care, n.d.). That’s why it’s beneficial for fatigue and soreness. People with fibromyalgia often feel worn out and achy. This type can help manage those symptoms.
Benefits include:
Eases Muscle Soreness: Reduces pain after exercise or daily strain.
Fights Fatigue: Supports energy to lessen tiredness in chronic conditions.
Helps with Fibromyalgia: Limited studies show it may lower pain severity (Healthline, n.d.).
Good Absorption: Less likely to cause stomach upset than other forms.
Chiropractors like malate for chronic pain. It supports metabolism and reduces fatigue (Sonoma Sports Chiro, n.d.). Take 200-400 mg a day. Start low to see how your body reacts. It’s often available in pill or powder form.
Magnesium Glycinate: Suitable for Nerve Pain and Relaxation
Magnesium glycinate binds to glycine, an amino acid that calms the brain. This form is easily absorbed and gentle on the stomach (Trace Minerals, n.d.). It’s great for nerve pain and stress. It helps regulate signals to stop overexcitement that causes pain.
Key advantages:
Calms Nerves: Lowers anxiety and eases nerve-related pain.
Relaxes Muscles: Reduces tension and spasms.
Aids Sleep: Promotes rest, which helps pain recovery (NMB Chiro, n.d.).
Fewer Side Effects: No laxative issues like some types.
For chiropractic patients, it cuts inflammation and boosts adjustments (SanTe Chiropractic, n.d.). It’s ideal for back or joint pain. Dose is 300-400 mg daily, often at night.
Topical Magnesium Chloride or Sulfate: Direct Muscle Relief Through Baths or Oils
Topical magnesium goes on the skin. Chloride absorbs well and targets sore spots (Health.com, n.d.). Sulfate, or Epsom salts, is for baths. It soothes muscles without gut processing.
Why choose topical:
Localized Relief: Applies right to the painful areas.
Quick Action: Bypasses digestion for faster help.
No Stomach Issues: Avoids diarrhea from oral forms.
Good for Baths: Epsom salts relax the whole body (Team Red White & Blue, n.d.).
Absorption varies by skin type. Studies are mixed, but many feel relief from soreness (Pierce Chiropractic, n.d.). Use oils or soaks 2-3 times a week.
Selecting the Right Form: Malate for Energy, Glycinate for Nerves, Topical for Localized Pain
Choose based on your pain type. Absorption differs: Oral forms, such as malate and glycinate, are absorbed through the gut; topical forms are absorbed through the skin (Drugs.com, n.d.).
Selection tips:
For Energy and Chronic Pain: Pick malate.
For Nerve Calm: Go with glycinate.
For Spot Relief: Use topical chloride or sulfate.
Consider Absorption: Glycinate is best overall (MN Spine and Sport, n.d.).
Chiropractors’ Preferences: Glycinate and Malate for Pain Management
Chiropractors favor glycinate and malate. Glycinate calms muscles and nerves, aiding adjustments (Everybodys Chiropractic, n.d.). Malate boosts energy for recovery.
How they work together:
Relax Muscles: Lessens tension for better alignment.
Cut Inflammation: Reduces joint swelling.
Boost Nerve Function: Improves signals for less pain.
Support Healing: Speeds recovery after treatments (ChiroCredit, n.d.).
Even phosphate forms help energy and relaxation in care (Edinburgh Chiropractic, n.d.).
Clinical Observations from Dr. Alexander Jimenez
Dr. Alexander Jimenez, DC, APRN, FNP-BC, focuses on integrative pain care. His work stresses non-drug methods for back pain and neuropathy (Jimenez, n.d.). He sees magnesium fitting into plans that mix chiropractic with nutrition. It helps reduce reliance on opioids and boosts recovery. In his clinic, such approaches ease chronic pain by improving mobility and reducing inflammation.
Conclusion
Magnesium offers natural pain relief. Malate helps fight fatigue in fibromyalgia, glycinate calms nerves, and topical forms provide spot relief. Chiropractors use them to enhance care. Pick the right type for your needs. Always check with a health pro. This can lead to less pain and a better life.
Real-Life Posture Rehab: How El Paso Back Clinic Helps You Move Better Every Day
Move around and change posture positions throughout the day.
Improving posture is one of the fastest ways to feel stronger, breathe easier, and protect your spine—especially if you live with long commutes, heavy work, or hours at a desk, like many people in El Paso. At El Paso Back Clinic, Dr. Alexander Jimenez, DC, APRN, FNP-BC, and his team see every day how targeted physical activity, along with integrative chiropractic and nurse practitioner (NP) care, can turn slouching and stiffness into confident, upright movement. El Paso, TX Doctor Of Chiropractic+1
This article explains, in simple language:
What good posture really is
Recommended physical activities and exercises to enhance posture
How yoga, Pilates, and mind-body practices improve alignment
Easy desk and “tech neck” fixes
How integrative chiropractic care supports posture
How nurse practitioners help with medical, ergonomic, and lifestyle support
How the El Paso Back Clinic combines all of this in real-world care
What “Good Posture” Means (and Why It Matters in Daily Life)
Good posture means your body is stacked in a natural, balanced way:
Ears over shoulders
Shoulders over hips
Hips over knees and ankles
Spine holding its natural curves (neck, mid-back, low back)
When posture is poor—like slouching over a phone or leaning forward at a desk—stress builds up in your neck, shoulders, and back. Over time, this can lead to:
Chronic neck and back pain
Tension headaches
Fatigue and shallow breathing
Tight hip flexors and weak glutes
Early joint wear and tear
Research and clinical guides show that specific exercises and posture-friendly habits can reduce pain and improve alignment by strengthening postural muscles and keeping you moving throughout the day. Healthline+2Harvard Health+2
At El Paso Back Clinic, Dr. Jimenez often reminds patients that posture is not about “standing stiff.” It is about a strong, relaxed, and mobile spine that can handle work, sports, and life in the desert heat. El Paso, TX Doctor Of Chiropractic+1
Core Principles of Posture-Focused Exercise
Most effective posture plans share the same core goals:
Strengthen the core and back—so your spine has solid support
Activate glutes and shoulders—to counter slumping and hip stress
Improve flexibility—especially in chest, hip flexors, and hamstrings
Train body awareness—so you notice and correct slouching
Add low-impact cardio—to boost circulation and recovery
Think of Your Program in Simple Pieces
Try to include each week:
2–3 days of core and back strengthening
2–3 days of mobility and stretching
2–4 days of low-impact cardio like walking or swimming
Daily micro-breaks from sitting or driving
That may sound like a lot, but many of these can be done in 10–20 minute blocks and woven into your normal day.
Foundational Strength Exercises for Better Posture
Many posture programs start with bodyweight moves you can do at home—no machines, no fancy equipment. Sources on physical therapy and spine health support these exercises. Healthline+2Primal Physical Therapy+2
Planks (Front and Side Planks)
Why they help: Planks strengthen your deep core, shoulders, and glutes. A strong core keeps your spine from sagging or arching too much.
Basic front plank:
Start on your forearms and toes
Keep your body in a straight line from head to heels
Gently pull your belly toward your spine
Hold 20–30 seconds, rest, repeat 2–3 times
Side planks add extra stability for your sides and hips, which support upright posture. Woodlands Sports Medicine
Bird-Dog
Why it helps: Bird-dog builds core and back strength while training balance and control.
How to do it:
Start on hands and knees
Extend your right arm forward and left leg back
Keep your hips level; don’t twist
Hold 3–5 seconds, then switch sides
Do 8–10 reps per side
Physical therapists often use this exercise to improve posture and relieve back pain. Primal Physical Therapy+1
Glute Bridges
Why they help: Bridges work the glutes and hamstrings and relieve stress on the lower back.
Lie on your back, knees bent, feet flat
Press through your heels and lift your hips
Squeeze your glutes at the top
Hold 3–5 seconds, then lower
Repeat 10–15 times
Strong glutes help balance tight hip flexors from long periods of sitting, which is very common among drivers and office workers in El Paso. Primal Physical Therapy+1
Superman Exercise
Why it helps: The Superman move targets the “posterior chain,” the muscles along the back of your body that help prevent slouching. Woman & Home
Lie face down
Lift your chest, arms, and legs slightly off the floor
Hold briefly and lower with control
Start with 5–8 reps
This move is especially useful if you sit a lot or look down at screens, as it helps your back muscles stay active.
Rowing Movements (Bands or Dumbbells)
Why they help: Rowing exercises strengthen the upper back and shoulder stabilizers that pull your shoulders back.
Use a resistance band or light dumbbells
Pull your elbows back and squeeze your shoulder blades together
Mobility and Stretching: Releasing the “Posture Brakes”
If strength is the “engine,” tight muscles are the “brakes.” You need both to work well. Stretching and mobility exercises help open areas that tend to tighten up, such as the chest, neck, hips, and upper back. Illinois Back Institute+1
Key Posture Stretches
Chest Opens / Doorway Stretch
Stand in a doorway with your forearms on the frame
Gently lean forward until you feel a stretch across your chest
Gently slide your chin straight back (like a mini “double chin”)
Hold 3–5 seconds
Repeat 10 times
Cat-Cow
On hands and knees
Slowly round your back toward the ceiling, then gently arch it
Move with your breath for 8–10 cycles
Hip Flexor Stretch
In a half-kneeling position, gently shift your hips forward
Keep your torso upright; avoid over-arching your back
Hold 20–30 seconds on each side
These stretches are simple but powerful when done daily—especially if you spend long hours driving I-10 or sitting at a workstation in El Paso. Illinois Back Institute+1
Mind-Body Practices: Yoga, Pilates, and Tai Chi
Mind-body exercises are excellent for posture because they combine strength, flexibility, and body awareness.
Yoga for Alignment and Awareness
Yoga routines often include:
Mountain Pose (Tadasana)—teaches what upright alignment feels like
Child’s Pose and Cat-Cow – gently move and decompress the spine
Bridge Pose – strengthens glutes and back
Chest opener poses—counter phone and computer hunching
Research-based guides show yoga can improve postural muscle endurance and help people become more aware of how they carry themselves. Healthline+1
Pilates for Core Control
Pilates focuses on:
Deep core strength
Controlled breathing
Smooth, precise movements
Many physical therapy and rehab programs use Pilates-style exercises to support spinal alignment and postural stability. Primal Physical Therapy+1
Tai Chi for Balance and Relaxed Upright Posture
Tai chi uses slow, flowing movements with calm breathing. It helps:
Improve balance and coordination
Encourage relaxed, upright posture
Reduce stress and muscle guarding
Chiropractic resources often recommend swimming, walking, yoga, and tai chi as ideal companions to chiropractic care. Muscle and Joint Chiropractic+1
Everyday Physical Activities That Support Posture
You don’t have to become a gym athlete to help your posture. Many everyday activities, done with good form, support a healthier spine.
Helpful posture-friendly options include:
Walking:
Encourages natural spinal motion
Easy to fit into breaks or evenings
Swimming:
Full-body, low-impact workout
Strengthens back and shoulder muscles with less joint stress
Dancing:
Builds coordination and body awareness
Helps you practice an upright chest and an active core
Cycling (with proper bike fit):
Strengthens hips and legs
Supports overall fitness and endurance
Clinics that treat back pain often highlight walking and swimming as key activities for long-term spinal health. Illinois Pain & Spine Institute+1
Desk, Phone, and “Tech Neck”: Quick Fixes You Can Actually Use
Long hours on a computer or phone are a major reason posture has become such a problem. Harvard Health and orthopedic clinics stress the importance of frequent movement breaks and simple desk exercises. Harvard Health+2barringtonortho.com+2
Desk-Friendly Posture Break Routine
Try this mini-routine a few times each day:
Chin tucks – 10 reps
Shoulder blade squeezes – hold 5 seconds × 10 reps
Seated Cat-Cow – 5–10 slow breaths
Forward fold stretch next to your desk—hold 20–30 seconds
Simple Ergonomic Tips
Keep feet flat on the floor
Hips and knees are near 90 degrees
Screen at or just below eye level
Use a small lumbar support or rolled towel behind your low back
Stand and walk at least every 30–60 minutes
Recent expert tips also support using standing desks, wireless headphones for “walking meetings,” and light resistance bands at your station to keep postural muscles awake. Harvard Health+1
How Integrative Chiropractic Care at El Paso Back Clinic Supports Posture
Chiropractic care focuses on the spine, joints, and nervous system. Integrative chiropractic care goes further, combining adjustments with corrective exercises, lifestyle coaching, and medical input from NPs. Advanced Spine & Posture+1
What a Posture-Focused Chiropractic Visit Often Includes
The Nurse Practitioner’s Role in Supporting Posture
At El Paso Back Clinic, Dr. Jimenez works not only as a chiropractor but also as a board-certified family nurse practitioner, which provides a broader, medically informed perspective on posture-related problems. El Paso, TX Doctor Of Chiropractic+1
A nurse practitioner can:
Review your full medical history
Identify arthritis, osteoporosis, nerve issues, or autoimmune conditions that affect posture.
Order and interpret imaging and labs
X-rays, MRIs, and blood work when appropriate
Prescribe or adjust medications
Short-term pain or muscle-relaxant use when necessary
Coordinate referrals
Physical therapy, pain management, and surgical consults if needed
Give lifestyle and ergonomic counseling
Weight management, sleep, stress, and work setup
Use telemedicine for follow-up
To keep you on track with your exercise and pain management plan
This integrative model makes it easier to catch red flags early, adjust plans safely, and provide each patient with a personalized path rather than a one-size-fits-all list of exercises.
How Dr. Alexander Jimenez Combines Physical Activity, Chiropractic Care, and NP Expertise
With decades of experience in personal injury, sports, and functional medicine, Dr. Jimenez has seen the same pattern again and again: posture improves the most when hands-on care, smart exercise, and patient education are combined. El Paso, TX Doctor Of Chiropractic+2El Paso, TX Doctor Of Chiropractic+2
In his clinical observations at El Paso Back Clinic:
Agility and functional training (such as controlled squats, lunges, and balance drills) help patients return to sports, warehouse work, or family life with greater resilience.
Posture work is often integrated with nutrition, sleep, and stress management, because tired, inflamed bodies struggle to maintain good alignment. El Paso, TX Doctor Of Chiropractic+1
This dual license (DC + APRN, FNP-BC) allows Dr. Jimenez to move comfortably between spine mechanics and whole-person health, which is ideal for complex posture and pain cases.
Sample Weekly Posture-Boosting Plan (General Example)
This is a general example for educational purposes, not a personal prescription. Always consult your provider—especially if you have pain, injuries, or medical conditions.
Posture check around your home and car: adjust chairs, pillows, and monitor height
Patients at El Paso Back Clinic often have a plan customized to their injury type (auto accident, work injury, or sports strain) and their job or sport. El Paso Back Clinic® • 915-850-0900+1
Safety Tips: When to Get Help
Stop and get professional care if posture exercises cause:
Sharp or stabbing pain
Numbness or tingling in arms or legs
New weakness or loss of coordination
Trouble walking or standing
Loss of bladder or bowel control (emergency—seek urgent care)
A chiropractor can evaluate your spine and joints; a nurse practitioner can check for underlying medical causes. At El Paso Back Clinic, the team works together to decide whether you need imaging, medication, rehab, or a referral to another specialist. El Paso, TX Doctor Of Chiropractic+1
Bringing It All Together
To enhance posture and protect your spine:
Strengthen your core, back, and glutes with planks, bridges, bird-dogs, rows, and Supermans
Stretch your chest, neck, and hips to release tight, “slouching” muscles
Use mind-body practices like yoga, Pilates, and tai chi to build body awareness
Add low-impact activities like walking and swimming to support overall spine health
Fix your desk and phone habits with regular movement breaks and better ergonomics
At El Paso Back Clinic, integrative chiropractic care and nurse practitioner support bring all of these pieces together. With Dr. Alexander Jimenez’s dual training, patients receive:
Spinal and joint adjustments
Corrective exercise and posture coaching
Medical evaluation, imaging, and medication management when needed
Telemedicine and follow-up plans that fit real life in El Paso
The goal is simple: help you stand taller, move with less pain, and feel stronger in everything you do—from lifting kids or boxes at work to walking the trails of the Franklin Mountains.
Faster Recovery After Spine Surgery: Enhanced Surgical Recovery (ESR) Programs at El Paso Back Clinic® in El Paso, TX
The doctor administers a local anesthetic into the patient’s affected area, using ultrasound to visualize the spine’s anatomical components.
Spine surgery can help treat serious back problems, such as pain from injuries, disc issues, or aging. At El Paso Back Clinic® in El Paso, TX, we focus on helping patients recover faster and more safely through modern methods. Enhanced Surgical Recovery (ESR), also called Enhanced Recovery After Surgery (ERAS), is a team-based plan that reduces the need for strong pain medications, shortens hospital stays, and lowers the risk of readmission. Led by Dr. Alexander Jimenez, DC, APRN, FNP-BC, our clinic combines chiropractic care, nurse practitioner expertise, and new tools to support healing. This article explains the main parts of ESR for spine surgery, how it cuts opioid use, shortens hospital stays, and reduces readmissions. We also cover the big roles of integrative chiropractic care and nurse practitioners, plus exciting new tech like virtual reality (VR) for building strength after surgery.
Many people in El Paso face back pain from work, accidents, or daily life. Surgery may be necessary, but traditional methods can make recovery challenging. ESR improves this process by planning care before, during, and after the operation. It uses simple steps, such as teaching patients, eating better, and moving early. Studies show these measures can cut opioid use a lot and help people go home sooner (Dagal et al., 2023). At El Paso Back Clinic®, we work with surgeons to add non-drug options for even better results.
What Is Enhanced Surgical Recovery (ESR)?
ESR is a proven plan to make surgery recovery easier and quicker. It started in other surgeries, but now helps a lot with spine operations, such as fusions or disc repairs. The idea is to lower body stress and speed natural healing. Instead of staying in bed and taking many pain pills, patients move soon and use gentler pain control.
Key parts of ESR include:
Team Approach — Doctors, nurses, chiropractors, and therapists all work together.
Step-by-Step Care — Planning starts before surgery and continues at home.
Personal Plans — Care fits each person’s health needs.
Research shows ESR helps with many spine issues, from small fixes to big ones (Zaed et al., 2023). Reviews find that most programs use around 12 key steps, such as better pain management and early walking (Berk et al., 2025).
Main Components of ESR for Spine Surgery
ESR has steps before, during, and after surgery to make things smoother.
Before Surgery (Pre-Op)
Getting ready early helps avoid problems.
Teaching Patients: Learn what to expect, how to manage pain, and why moving matters. This lowers worry and helps follow the plan (Zaed et al., 2023).
Better Nutrition: Check for low energy or anemia. Eat protein and carbs to build strength. Nutritious food helps healing (Soffin et al., 2022).
Pain Prep: Start gentle meds like acetaminophen. Quit smoking to lower risks (American Association of Nurse Anesthesiology, n.d.).
Prehab Exercises: Build strength with walks or stretches.
These make surgery safer.
During Surgery (Intra-Op)
The team uses ways to protect the body.
Better Anesthesia: Short drugs to wake up fast. Add non-opioid options (Dagal et al., 2023).
Careful Fluids: Just the right amount to avoid issues.
Small Cuts: Less muscle damage for quicker recovery (Dietz et al., 2019).
Pain Blocks: Numb the area for hours after.
Patients feel better right away.
After Surgery (Post-Op)
Focus on rapid healing.
Early Walking: Get up soon and walk daily (Zaed et al., 2023).
Mixed Pain Control: Use non-opioids, ice, and movement.
Quick Eating: Start foods and drinks early.
Checks for Safety: Watch for clots or other issues.
These steps lower risks.
How ESR Reduces Opioid Use
Strong pain drugs like opioids help, but can lead to problems like addiction. ESR cuts its use by at least half (Dagal et al., 2023). At El Paso Back Clinic®, we add chiropractic methods for even less need.
Mixed Pain Options: Non-opioids first, like NSAIDs and nerve meds. Some programs use almost no IV opioids (HCA Healthcare, n.d.).
Teaching Non-Drug Ways: Ice, breathing, and adjustments.
Blocks and Early Move: Numb areas and walk to ease pain.
In fusions, opioids dropped considerably without worse pain (Dagal et al., 2023). This helps avoid side effects and promotes natural healing.
Shortening Hospital Stays with ESR
Long hospital time raises costs and risks. ESR cuts stay by 1-2 days (HCA Healthcare Today, 2022).
Early Movement: Prevents issues and builds strength.
Fast Nutrition: Energy for recovery.
Good Pain Control: Less bedtime.
Team Reviews: Go home when ready.
One example shows noticeable shortened stays (Dagal et al., 2023). Patients heal better at home.
Lowering Readmission Rates
Going back to the hospital is tough. ESR lowers this risk (HCA Healthcare Today, 2022).
Home Care Teaching: Know warning signs.
Follow-Ups: Calls from our team at El Paso Back Clinic®.
Fewer Problems: Better prep means fewer infections.
Full Care: Controls swelling early.
Fewer complications overall (Berk et al., 2025).
Integrative Chiropractic Care at El Paso Back Clinic®
Chiropractic care fits perfectly with ESR. At our clinic, Dr. Jimenez uses hands-on adjustments to align and relieve symptoms.
Before Surgery: Improve posture and movement.
Pain Without Drugs: Soft tissue work eases tension.
After Surgery: Reduce scar tissue and build mobility (New York City Spine, n.d.).
Nerve Help: Better signals for less pain.
We complement therapy for smoother recovery (Active Health Center, n.d.).
Role of Nurse Practitioners
Nurse practitioners (NPs) like Dr. Jimenez coordinate care.
Team Links: Connect everyone.
Teaching and Meds: Focus on safe, non-opioid options.
Tracking Progress: Adjust plans.
NPs help stick to ESR paths (American Association of Nurse Anesthesiology, n.d.).
New Tech: Virtual Reality (VR) for Recovery
VR uses games and guides to make rehab more enjoyable. It helps spine patients build strength.
Fun Exercises: Improves engagement and movement.
Less Pain Feel: Distraction helps.
Strength Gains: Tailored for muscles and focus.
Home Options: Practice alone.
Recent studies show VR speeds recovery after spine issues, like in cervical cases or general neurorehab (Bolton et al., 2025; various 2025 trials).
Insights from Dr. Alexander Jimenez at El Paso Back Clinic®
Dr. Alexander Jimenez, DC, APRN, FNP-BC, leads El Paso Back Clinic® with dual expertise in chiropractic and nursing. He uses team care for pain management and rehab after injuries or surgery. His plans include adjustments, nutrition, and integrative methods for better mobility without heavy drugs. He stresses whole-body healing for lasting results (Dr. Alex Jimenez, n.d.; LinkedIn, n.d.).
Conclusion
ESR programs accelerate spine surgery recovery and make it safer. With education, nutrition, movement, and team support, they reduce opioids, shorten stays, and lower readmissions. At El Paso Back Clinic® in El Paso, TX, we add chiropractic care and NP guidance for full support. New VR tech adds exciting ways to build strength. If facing spine surgery, ask about ESR and our integrative options. Contact us at 915-850-0900 for help.
How Telemedicine Can Assist in the Management of Sciatica (with Integrative Chiropractic Care)
A man at home consults a chiropractor via telemedicine for back pain and sciatica.
Sciatica can make even simple tasks—like getting out of bed, sitting at a desk, or driving—feel almost impossible. When pain shoots down your leg or feels like burning, stabbing, or tingling, the idea of driving across town to sit in a waiting room can be overwhelming.
Telemedicine offers a way to get expert help for sciatica without leaving home. Telemedicine can significantly improve the quality of life for many individuals experiencing limited mobility or frequent flare-ups of pain. Spine specialists and integrative chiropractic teams now use secure video visits to evaluate symptoms, design treatment plans, and follow patients through recovery. UT Southwestern Medical Center+1
Dr. Alexander Jimenez, DC, APRN, FNP-BC, is a dual-licensed chiropractor and nurse practitioner in El Paso, Texas. His integrative model combines medical decision-making (such as imaging and prescriptions) with chiropractic and functional medicine. This blended approach fits perfectly with telemedicine because it allows him to assess nerve pain, guide movement, and adjust treatment plans over time—even when the patient is at home. El Paso, TX Doctor Of Chiropractic
What Is Sciatica?
Sciatica is not a disease by itself. It is a pattern of symptoms caused by irritation or compression of the sciatic nerve. This nerve starts in the lower back, runs through the hips and buttocks, and travels down each leg.
Common symptoms include:
Sharp or burning pain in the lower back, buttocks, and legs
Numbness, tingling, or “pins and needles” in the leg or foot
Weakness when trying to stand, walk, or lift the leg
Pain that worsens with sitting, coughing, or bending
Sciatica is usually caused by:
Herniated or bulging discs pressing on a nerve root
Spinal stenosis (narrowing of the spinal canal)
Degenerative disc disease
Muscle or joint dysfunction in the pelvis and lower back
Less commonly, tumors, infections, or serious conditions
Because sciatica can have many causes, proper evaluation and treatment planning are very important—this is where telemedicine can help you start sooner and stay on track.
What Is Telemedicine and How Does It Work for Back and Nerve Pain?
Telemedicine (also called telehealth) is health care delivered via secure video or phone rather than an in-person visit. You use a smartphone, tablet, or computer to speak with your provider, similar to a video call with family or friends.
Clinics that treat spine and nerve problems have made telemedicine a core part of their care model. They use it for first visits, follow-ups, second opinions, and surgical planning, especially for conditions like back pain, neck pain, and sciatica. UT Southwestern Medical Center+1
During a typical telemedicine visit for sciatica, your provider can:
Ask detailed questions about your pain pattern
Watch how you move on camera
Guide simple movement and strength tests
Review MRI, X-ray, or CT results
Explain treatment options, including chiropractic, physical therapy, injections, or surgery if needed
Many clinics report that they can accurately diagnose spine issues through video visits and that most telemedicine-based surgical plans do not require major changes after in-person exams. UT Southwestern Medical Center
Why Telemedicine Is Especially Helpful for Sciatica
People with sciatica often have trouble sitting, driving, or walking long distances. Telemedicine meets them where they are—literally.
Key benefits for sciatica patients
Less travel and less pain getting to care
No long car rides or sitting in waiting rooms
Easier for patients who have mobility issues or rely on others for transportation Southeast Texas Spine+1
Faster access to evaluation and treatment
Many clinics can schedule telemedicine visits sooner than in-person visits
You can start treatment earlier instead of waiting weeks to be seen
Better continuity of care
Telemedicine makes it easier to attend follow-ups, especially during long recovery plans
Providers can adjust medications, exercises, and activity limits in real time Southeast Texas Spine+1
Home-based evaluation of your real environment
Your provider can see your work setup, couch, bed, or home office
Straight-leg raise or seated leg raise while on camera
Heel and toe walking to assess nerve strength
Balance and gait observation
Imaging and tests
Your nurse practitioner or physician can order MRI, X-rays, or CT scans when needed
They may also recommend nerve tests (EMG/NCS) through in-person referrals
Spine centers and orthopedic clinics report that telemedicine visits can help determine when conservative care is sufficient and when urgent in-person care or surgery is needed. UT Southwestern Medical Center+1
Integrative Chiropractic Telemedicine for Sciatica
Integrative chiropractic telemedicine combines:
Medical care—history, diagnosis, imaging orders, prescriptions, and referrals
Chiropractic care—movement analysis, spinal and pelvic mechanics, and guided home-based therapies
Dr. Jimenez’s dual-scope role as a chiropractor and nurse practitioner is a strong example of this model. In his practice, he uses telemedicine to:
Review MRI and other imaging results with patients
Coordinate conservative care (chiropractic, physical therapy, massage, acupuncture, and functional medicine)
Monitor nerve symptoms and red flags that require fast in-person intervention
Looks for patterns of dysfunction in the lower back, pelvis, and hips
Guides you through gentle tests and movements
Designs a home exercise and stretching plan
Educates you about ergonomics, sleep positions, and movement habits
Even without hands-on adjustments, chiropractic expertise is used to understand mechanics and guide safe self-care at home. Evolve Chiropractic+2HealthCentral+2
Telemedicine and Medication Management for Sciatica
Telemedicine is also useful for medication oversight and pain management. Virtual pain management services can:
Review current medications and supplements
Start or adjust anti-inflammatory drugs, muscle relaxers, or nerve pain medications when appropriate
Help taper short-term medications to avoid long-term dependence
Coordinate with other therapies like physical therapy and chiropractic care Everlywell+1
This is important because the goal is not just to reduce pain for a few days but to manage it safely while addressing the underlying cause.
Guided Home Exercises and Self-Care for Sciatica via Telemedicine
A large part of sciatica management involves what you do every day at home. Telemedicine allows your integrative provider to coach you in real time.
Types of exercises a provider may guide over video
Always follow your own provider’s instructions. The list below is for education, not a personal prescription.
An integrative chiropractor, such as Dr. Jimenez, will often blend chiropractic reasoning (how joints and muscles are moving) with physical therapy-style exercise progressions to build strength and reduce nerve irritation over time. Integrative Medical of DFW+1
Telemedicine and Physical Therapy for Sciatica
Physical therapy is a key part of long-term sciatica care. Telemedicine makes it easier for your team to coordinate and supervise this care.
An NP–chiropractor team can:
Refer you to in-person physical therapy when you need hands-on manual work
Work with therapists to align goals: pain reduction, nerve mobility, strength, and posture
Review PT progress notes with you by video
Add or modify home exercises between in-person therapy visits
Modern integrative clinics describe physical therapy as treatment focused on your goals, your function, and your time—whether you are recovering from an acute episode of sciatica or managing long-term spine issues. Integrative Medical of DFW+1
Telemedicine for Office Workers and Remote Workers with Sciatica
Many people with sciatica sit for long periods at desks or work remotely at kitchen tables, couches, or beds. Poor ergonomics can worsen nerve pain.
Telemedicine allows providers to see your real work setup and give specific advice.
They may help you:
Adjust chair height, screen level, and keyboard position
Chiropractic-based telemedicine visits for office workers often focus on spinal alignment, hip position, and load sharing between joints — even if the provider cannot physically adjust the spine during the visit, they can teach you how to move better and reduce pressure on the sciatic nerve. tigardchiropracticautoinjury.com+1
How to Prepare for a Telemedicine Visit for Sciatica
Preparing well can make your telemedicine visit smoother and more helpful.
Before your appointment
Check your technology
Test your camera, microphone, and internet connection
Charge your device and have a backup (like a phone) ready
Choose your space
Find a quiet, private room
Make sure you have enough room to stand, walk, and lie down if needed
Gather information
List your current medications and supplements
Have your medical history and imaging reports handy
Dr. Jimenez’s clinical experience shows that when patients feel seen and supported—through regular check-ins, education, and coordinated care—they are more likely to stay consistent with their home program and achieve better long-term outcomes. El Paso, TX Doctor Of Chiropractic+1
Practical Tips for Getting the Most from Telemedicine for Sciatica
Here are some simple strategies to make telemedicine work for you:
Treat the visit like an in-person appointment
Show up on time and minimize distractions
Have a notebook handy for instructions
Be specific about your goals
“I want to sit for 30 minutes without pain”
“I want to walk around the block again”
Clear goals help your provider design better plans
Use photos or videos
Take a short video of how you walk or how you get out of a chair during painful times
Share this with your provider if their platform allows
Stay consistent with home exercises
Put reminders in your phone
Tie exercises to habits (after brushing teeth, after lunch, etc.)
Ask for a written or emailed summary
Many clinics send a visit summary through the patient portal
This can include your diagnosis, exercise plan, and red-flag symptoms
The Future: Telemedicine, Sciatica, and Integrative Care
Telemedicine is no longer just an emergency backup plan—it is a core part of modern spine and pain care. Spine centers, pain clinics, and integrative practices across the country use telemedicine to: UT Southwestern Medical Center+2NJ Spine & Orthopedic+2
Speed up diagnosis and treatment
Improve convenience for patients in pain
Coordinate care between specialists, therapists, and primary providers
Support long-term recovery with flexible follow-ups
For people with sciatica, this means you can:
Get expert guidance without leaving your home
Partner with an integrative chiropractor and nurse practitioner who can see both the nerve problem and the whole person
Combine remote consultations, at-home exercises, and lifestyle changes into a comprehensive plan
Under the care of a dual-licensed provider like Dr. Alexander Jimenez, telemedicine becomes more than a video call. It becomes a bridge between medical science, chiropractic biomechanics, and day-to-day life—helping you move from intense nerve pain toward safer movement, better function, and long-term relief. El Paso, TX Doctor Of Chiropractic+2Evolve Chiropractic+2
How Head Trauma Can Trigger Sciatica: The Hidden Link and Ways to Heal
A doctor of chiropractic explains to an automobile accident patient how a head injury can cause sciatica and lower back problems.
Head injuries can occur in car crashes, sports-related falls, or everyday slips. They shake the brain and body in ways you might not expect. One surprising outcome? Sciatica. That’s the sharp pain shooting down your leg from a pinched sciatic nerve. Many people don’t connect a bump on the head to that nagging leg ache. However, science reveals a clear connection between the two. This article breaks it down simply. We’ll explore how head trauma messes with your spine and nerves. We’ll also cover how gentle chiropractic care can help ease pain and speed up recovery. If you’ve had a head injury and now feel leg pain, this could explain why—and what to do next.
What Is Head Trauma and How Does It Relate to Sciatica?
Head trauma means any blow to the skull that jars the brain. It ranges from mild concussions to severe traumatic brain injuries (TBI). A concussion might leave you dizzy for days. A serious TBI could mean hospital stays and long-term changes. These injuries don’t just affect thinking. They ripple through the whole body.
Sciatica is a type of pain caused by the sciatic nerve. This nerve starts in your lower back and runs down each leg. It’s the longest nerve in your body. When irritated, it causes burning, tingling, or shooting pain from the butt to the foot. Common causes include herniated discs or tight muscles. But head trauma adds a twist. It can trigger changes deep within your nervous system that lead to nerve trouble.
Studies show that up to 78% of TBI survivors deal with ongoing pain. That includes back and leg aches, such as sciatica. Why? The brain controls everything, including how your spine moves. A head hit disrupts that control.
Dr. Alexander Jimenez, a chiropractor in El Paso, Texas, frequently observes this phenomenon in his clinic. As a Doctor of Chiropractic and Nurse Practitioner, he treats patients after accidents. He notes that head trauma often hides as simple bumps but leads to widespread pain. In his observations, many patients come in with leg pain that they attribute to old falls or crashes. His team uses functional medicine to trace the issue back to the brain-spine connection.
How Head Trauma Alters Brain Control Over Spinal Muscles
Your brain is like a boss for your muscles. It sends signals down the spinal cord to maintain balance. Head trauma throws that off. A TBI damages brain areas that regulate movement. This leads to spasticity—tight, jerky muscles in the legs and back.
Think of it this way: Normally, your brain tells spinal muscles to relax and stretch smoothly. After a head injury, those signals glitch. Muscles in the lower back get out of sync. They pull unevenly on the spine. Over time, this puts strain on the sciatic nerve roots as they exit the lower back.
One study found that mild TBIs cause extra sensitivity in the legs. It’s as if the brain amplifies pain signals through chemicals called chemokines. These build up in the spinal cord, making nerves fire too easily. For sciatica, this means even small movements cause more pain.
Dr. Jimenez observes this in athletes after concussions. “Patients tell me their legs feel heavy, like they’re fighting their own body,” he shares in his wellness podcasts. His clinic uses nerve tests to spot these glitches early. By addressing them, they prevent the pain from becoming chronic.
This muscle chaos doesn’t stop at the back. It can weaken core support, leading to poor posture. Slouching adds pressure on the sciatic nerve. It’s a slow build, but real.
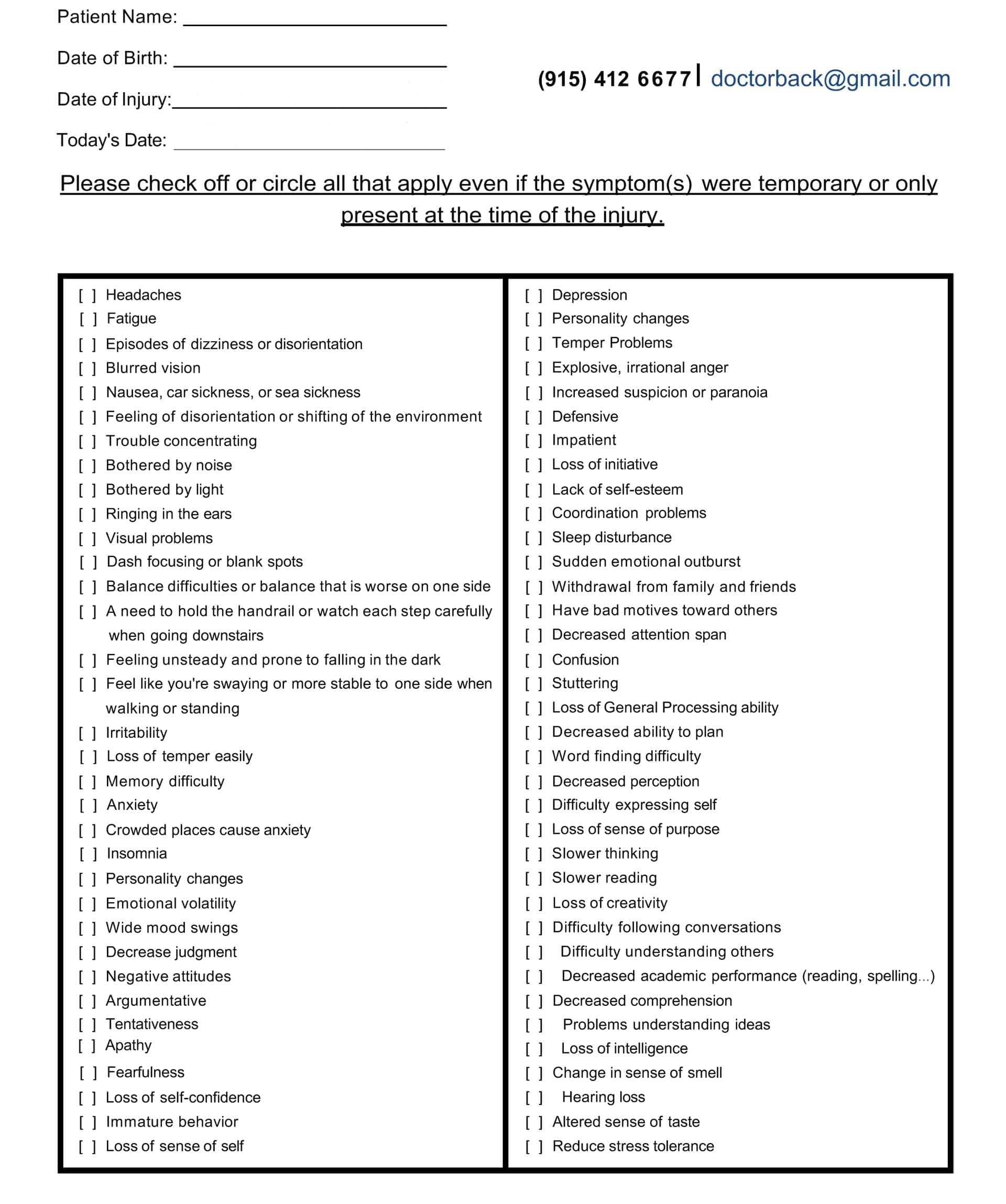
Head Injury/TBI Symptom Questionnaire:
Head Injury/TBI Symptom Questionnaire
Misalignment and Muscle Impairment: Irritating the Sciatic Nerve
Head trauma often hits the neck hard. The force whips the head forward and back—like in a car crash. This misaligns the upper spine, particularly the top vertebrae, known as the atlas and axis. That misalignment travels down like a domino fall.
Impaired muscles from brain signals exacerbate the condition. Tight neck muscles pull the spine off-kilter. In the lower back, this squeezes discs and nerves. The sciatic nerve can become pinched between bones or become inflamed. Result? That classic leg zap.
Research backs this. Up to 8% of severe TBI cases come with spine injuries. Even mild ones raise the risk. A study on 180 patients showed that older folks or those with low consciousness scores face higher odds. The neck shift stresses the whole chain, irritating the sciatic nerve.
Concussions alone can spark lower back pain. The brain’s balance center gets knocked. Muscles overwork to compensate, tiring the back. Dr. Jimenez refers to this as the “cascade effect” in his LinkedIn posts. He treats it with targeted adjustments to reset muscle tone.
Raising the Risk of Further Spinal Damage
Head trauma doesn’t just irritate—it invites more trouble. A damaged brain means slower reflexes. You might stumble more easily, leading to falls that jar the spine again. Plus, inflammation from TBI spreads. It swells the tissues around the spine, causing the discs to bulge and the nerves to become vulnerable.
One key risk: Concomitant injuries. That’s when head and spine hits happen together. In motor vehicle crashes—the top TBI cause—neck strains often tag along. This doubles the chance of disc slips that pinch the sciatic nerve.
Dr. Jimenez observes this in patients involved in car accidents. “A rear-end collision jars the brain and twists the lumbar spine,” he explains in his functional medicine series. His observations show early chiropractic checks cut re-injury risks by improving stability.
The Role of Swelling and Heterotopic Ossification in Nerve Crushing
TBI triggers swelling fast. Brain tissue bruises, and fluids build up. This chaos can spread to the body. In rare but serious cases, it leads to heterotopic ossification (HO). That’s when bone grows in soft tissues—like muscles or around nerves.
Around the sciatic nerve, HO is sneaky. It starts after hip or pelvic trauma, tied to the head hit. Scar tissue hardens into bone, encasing the nerve. Over months, this crushes it. Symptoms creep in: Numbness, weakness, foot drop.
A case report described a young man following traumatic brain injury (TBI). Seventeen months later, bilateral sciatic entrapment from hip HO caused severe pain. Surgery freed the nerve, but prevention is key. Anti-inflammatory drugs or radiation cut HO risks.
Dr. Jimenez warns of this in his injury recovery blogs. He uses imaging to identify early signs of HO in TBI patients with leg pain. His integrative plans include nutrition to fight inflammation and slow bone overgrowth.
Upper Neck Misalignment: Starting a Pain Cascade to the Sciatic Nerve
The upper neck is ground zero for many head traumas. Whiplash from falls or sports bends it unnaturally. This throws off the atlas—the top bone. It shifts pressure down the spine.
The cascade? Misaligned neck pinches nerves there. Signals to the lower back get scrambled. Muscles tighten unevenly, pulling on the lumbar joints. This stresses the sciatic nerve roots, causing inflammation and pain.
Inflammation plays a big role. Concussion swelling in the neck disrupts blood flow and nerve signals, causing significant complications. It causes the brain to misread pain, amplifying the sensation of hurt in the leg.
Dr. Jimenez’s clinical notes highlight this in veterans with whiplash-TBI. “Neck shifts create a domino pain chain,” he says. His team uses precise X-rays to map it, then adjusts to break the cycle.
Integrative Chiropractic: A Path to Relief and Recovery
Integrative chiropractic blends hands-on care with wellness tools. It’s perfect for post-head injury sciatica. No drugs or surgery—just realignment and support.
First, it realigns the spine. Gentle adjustments fix neck and back shifts. This eases nerve pressure fast. For sciatica, lumbar tweaks reduce the disc bulge on the nerve.
Second, it boosts nervous system function. Adjustments reduce interference, allowing brain signals to flow more smoothly. This calms spastic muscles and dials down pain sensitivity.
Third, it fights inflammation. Soft tissue work, like massage, releases tight spots. Add nutrition advice, including anti-inflammatory foods, and use swelling drops.
Finally, it restores cerebrospinal fluid (CSF) flow. CSF cushions the brain and spine. Trauma clogs it, raising pressure. Craniosacral therapy—light touches on the skull and sacrum—clears the path. Patients report clearer heads and less pain.
Dr. Jimenez integrates all this. His clinic mixes adjustments with functional tests. “We trace sciatica back to the head hit, then rebuild from there,” he observes. Patients who have been in accidents often experience mobility gains within weeks. One testimonial: A crash survivor ditched leg braces after targeted care.
Studies agree. Chiropractic reduces TBI pain by 50% in some individuals. For post-concussion, it eases dizziness and back aches.
Real-Life Stories and Expert Tips
Take Sarah, a soccer player Dr. Jimenez treated. A header caused a concussion and later sciatica. Adjustments realigned her neck, easing leg pain. Now she plays pain-free.
Tips from experts: Start care early. Get imaging if pain lingers post-injury. Pair chiropractic care with rest and omega-3 fatty acids for managing inflammation.
Wrapping It Up: Take Control of Your Recovery
Head trauma to sciatica seems far-fetched, but the links are strong. From brain glitches to bone growth, it stresses the sciatic nerve. Integrative chiropractic offers hope—realigning, calming, and healing.
Don’t ignore the signs. See a pro like Dr. Jimenez for a check. Your body can bounce back stronger.
Overcoming Sciatic Nerve Pain: Expert Insights from El Paso Back Clinic® in El Paso, TX
At El Paso Back Clinic®, located in the heart of El Paso, Texas, we specialize in helping people get back to their active lives without the constant burden of pain. Led by Dr. Alexander Jimenez, DC, APRN, FNP-BC, our team combines chiropractic care with modern wellness strategies to treat conditions like sciatic nerve issues. Whether you’re dealing with sharp leg pain from a work injury or numbness after a car accident, our clinic offers personalized plans to ease your symptoms and promote long-term health. We focus on non-invasive methods that address the root causes, not just the signs. If you’re in El Paso and searching for effective sciatica relief, our integrated approach could be the key to feeling better.
Sciatica isn’t just a back problem—it’s a nerve issue that can disrupt your daily routine. The sciatic nerve, which is like a thick cable running from your lower spine down each leg, gets irritated or squeezed, causing discomfort that travels far. At our clinic, we’ve seen how this affects everyone from athletes to office workers. In this guide, we’ll dive into what sciatica really is, why it happens, and how our team at El Paso Back Clinic® uses proven techniques to help. We’ll cover the physical side of nerve damage, common triggers, signs to watch for, and recovery steps. Plus, we’ll share how our chiropractic integrative care stands out in treating these issues right here in El Paso.
The Basics of the Sciatic Nerve and How Pressure Affects It
The sciatic nerve is your body’s main pathway for signals between the brain and legs. It begins at the lower back, where several nerve roots join, then branches through the buttocks and down to the feet. This nerve handles movement in your hamstrings, calves, and feet, as well as sensation in those areas. When something, like a slipped disk or tight muscle, presses on it, problems start.
When the sciatic nerve is compressed, pinched, or crushed, it suffers physical damage that disrupts its ability to transmit signals, leading to pain, numbness, and muscle weakness. The severity of the physical changes depends on the nature and duration of the pressure. Inside the nerve, axons carry messages, protected by myelin sheaths for fast travel. Pressure squishes these, causing swelling and blocking blood flow, which starves cells of oxygen—a state called ischemia (Verywell Health, 2023). In mild squeezes, like poor posture, the myelin gets worn but regrows. But harder crushes break axons, triggering degeneration where the nerve falls apart below the spot (Menorca et al., 2013).
Think of it like a garden hose: a light kink slows water, but a stomp cuts it off. Short pressure might cause temporary numbness, but ongoing force leads to scarring and chronic issues. At El Paso Back Clinic®, we use advanced checks to spot these changes early, helping prevent lasting harm.
Recognizing the Signs of Sciatic Nerve Trouble
Sciatica shows up in ways that can sneak up on you. The classic sign is radiating pain—starting in the lower back and zipping down one leg like an electric shock. It might burn, tingle, or feel sharp, worse when you sit, stand, or sneeze (Penn Medicine, n.d.). Numbness follows, making parts of your leg feel asleep or prickly. Weakness hits muscles, causing limps or trouble with stairs (Align Wellness Center, n.d.).
In our El Paso clinic, patients often describe it as a “leg giving out” or a constant ache. Severe cases bring muscle shrinking or even bladder issues if nerves are badly pinched (ADR Spine, n.d.). We see this in folks from all walks—drivers with long hauls, athletes pushing limits, or those in desk jobs. Early signs? Pay attention to one-sided pain that doesn’t fade with rest.
What Causes Sciatic Nerve Compression in Everyday Life
Life in El Paso means active days, but that can lead to sciatica triggers. A herniated disk, where the cushy part bulges and presses on the spinal cord roots, is common from lifting heavy boxes at work (Mayo Clinic, 2023). Aging narrows the spine in stenosis, squeezing nerves (Physio Pretoria, n.d.). Tight piriformis muscles in the butt can pinch the sciatic nerve, too, especially in runners or cyclists.
Accidents amp it up—car crashes crush nerves directly (MedStar Health, n.d.). Bone growths from arthritis add pressure, and extra weight strains everything (Advanced Orthopaedics & Sports Medicine, n.d.). Double crush? That’s when two spots squeeze, such as the back and leg, worsening the condition (Southwest Regional Wound Care Center, n.d.). At our clinic, we trace these in locals from border commutes to sports fields.
How We Diagnose Sciatica at El Paso Back Clinic®
Getting the right diagnosis is step one to relief. At our El Paso locations, we start with a full chat about your history—when the pain started and what makes it worse. Then, during hands-on exams, we test reflexes, strength, and perform the leg raise to pinpoint nerve irritation (Penn Medicine, n.d.).
We use top tools like MRI for disk views, EMG for signal checks, and X-rays for bones (ICliniq, 2023). Dr. Jimenez’s dual training as a chiropractor and nurse practitioner allows for a dual-scope diagnosis—blending medical tests with chiropractic insights for a full picture (Jimenez, n.d.). This helps link injuries to symptoms accurately, especially in complex cases from MVAs or sports.
Physical Damage from Compression: A Closer Look
Diving deeper, compression physically alters the nerve. Mild pressure causes neurapraxia: myelin dents, slowing signals without axon breaks. You feel weak but recover fast (Menorca et al., 2013). Stronger pinches lead to axonotmesis: axons snap, walls degenerate, and swelling builds. Healing takes time as new growth crawls along (Horton Mendez, n.d.).
Crushes bring neurotmesis: full sever, with scars blocking regrowth (Bhatia, 2023). Pressure cuts off blood, causing ischemia and cell death (Verywell Health, 2023). Chronic? Fibrosis hardens tissue (Mackinnon, 1998). Our clinic spots these via imaging, guiding treatments to reduce pressure and aid repair.
Integrative Chiropractic Care: Our Approach at El Paso Back Clinic®
We believe in whole-body healing. Our chiropractic integrative care combines spinal adjustments, soft tissue work, and exercises to correct alignment, enhance muscle function, and improve nerve signals. Adjustments ease pressure on the sciatic nerve, while massage loosens tight spots (AMTA, n.d.). Rehab builds strength to prevent repeats (Byington, n.d.).
This holistic method tackles pain now and builds stability for tomorrow. We add nutrition and stress tips, as gut health and emotions affect recovery. For El Paso folks, it’s about getting back to hikes or family time pain-free.
Dr. Alexander Jimenez’s Clinical Observations and Clinic Breakdown
With over 30 years, Dr. Jimenez brings unique insights. His dual credentials allow clinical correlations: linking injuries to assessments via advanced imaging like MRI for neuromusculoskeletal views (LinkedIn, n.d.). We treat work strains, sports sprains, personal slips, and MVAs with tailored plans.
Our process: Dual-scope diagnosis merges chiropractic and medical for thorough checks. Treatments include adjustments, non-surgical decompression, acupuncture, and functional medicine. We handle legal documents for accident claims, ensuring smooth care (Jimenez, n.d.). Observations? Stress worsens posture, and gut issues slow healing—we address all.
Recovery and Prevention Tips from Our El Paso Team
Recovery varies: Mild cases heal in weeks with rest and therapy, while severe cases require months (ADR Spine, n.d.). We guide with exercises, avoiding surgery when possible.
Prevent? Good posture, regular moves, and weight control. At our clinic, we teach these in sessions.
In El Paso, sciatica doesn’t have to hold you back. El Paso Back Clinic® offers expert, local care to restore your life.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine