Sciatica is a set of symptoms characterized by pain which extends down the length of the thighs from the spine. When a disk herniation compresses a nerve along the lumbar spinal column, approximately 90 percent of sciatic nerve pain, or sciatica, develops. Pregnancy and piriformis syndrome are common causes of sciatica.
Chiropractic care is a treatment option which focuses on the treatment of injuries and/or conditions associated with the nervous and musculoskeletal system, an alternative option. Patients explain how Dr. Alex Jimenez has helped them achieve pain relief through chiropractic care. Edgar M. Reyes and Truide Torres highly recommend Dr. Alex Jimenez as the non-invasive choice for sciatica.
El Paso Back Clinic
We are blessed to present to you El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center, we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life filled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life.
I assure you, I will only accept the best for you�
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend us.
Involvement in a car crash is an unfortunate situation that can result in various automobile accident injuries. People suffering from whiplash, neck pain, and back pain due to an auto accident can struggle to continue their regular activities. Dr. Alexander Jimenez is a personal injury chiropractor who focuses on treating automobile accident injuries, among other health issues.
Patients describe how their quality of life was affected after a car crash and discuss how chiropractic care with Dr. Jimenez helped them recover their overall health and wellness. The patients highly recommend Dr. Alex Jimenez as the non-surgical choice for personal injuries and auto accident injuries, among other health issues, such as whiplash, neck pain, and back pain.
El Paso Back Clinic
https://youtu.be/1MFwLhYbTRU
We are blessed to present El Paso’s Premier Wellness & Injury Care Clinic to you.
As El Paso’s Chiropractic Rehabilitation Clinic & Integrated Medicine Center, we are passionately focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life filled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life.
I assure you, I will only accept the best for you
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend us.
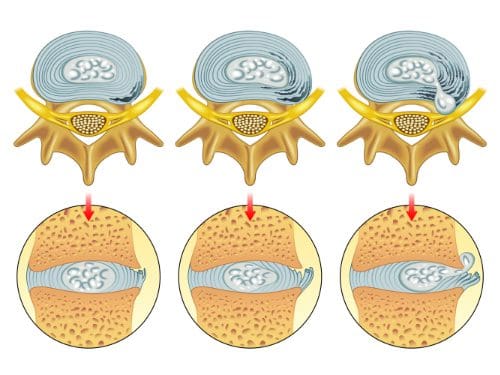
A herniated disc is a common spinal disc issue. The spine is a very intricate structure, and when one component fails to function correctly, it can affect the entire body, causing pain and loss of mobility.
Tiny bones, called vertebrae, are stacked on each other to form the spine. They are joined in such a way to facilitate movement, flexibility, and a wide range of motion. There are small, fluid-filled discs that rest between each vertebra, providing a cushion between the bones. When one of these discs becomes damaged, it can affect the surrounding nerves, causing pain and making movement difficult.
What is It?
A herniated disc is a common spinal condition that typically affects the cervical spine (neck region) or the lumbar spine (lower back), although it can occur in any part of the spine. Most often, a herniated disc happens at the L4 � L5 and the L5 � S1. This is because this portion of the spine, the lumbar region, bears the bulk of the body�s weight.
It is often referred to as a ruptured disc or slipped disc and occurs when the disc moves or slips out of place. It can also be the result of a disc that has a small tear and is leaking the jelly-like substance that is inside. This can put pressure on the surrounding nerves, causing pain and discomfort.
The first two stages are called incomplete herniations while the last two stages are called complete herniations.
Symptoms of a herniated disc may increase or worsen as the condition progresses although some patients do not experience any at all Typical symptoms include:
Pain in the affected area
Tingling
Numbness
Weakness
Leg or arm pain
Loss of reflex
Loss of mobility
Loss of flexibility
Decreased range of motion
What Causes It?
There are several causes. The most common are aging and degeneration, overuse, and normal wear and tear on the body.
A herniated disc resulting from an injury or trauma, such as a blow to the back, is less common, but it does happen. Because the back does bear most of the body�s weight, it can put a significant amount of pressure on the spine and discs. Over time, the discs may begin to weaken and a herniation can occur.
Injury or trauma that results in a herniation may include a car accident that involves sudden jerking, or incorrectly lifting heaving objects can put excessive pressure on the spine, causing it to herniate.
How is it Diagnosed?
A physical examination is usually the first step in diagnosing a herniated disc. The physician or chiropractor will examine the spine while the patient is standing, then while they are lying down. Depending on the severity and location of the herniation, they may note a decrease in spinal curvature.
Radicular pain will also be assessed, when the spine is unmoving, while in motion, and when pressure is applied. Other tests may also be administered. X-rays may also be taken, but an MRI is usually more accurate and provides greater detail.
What are the Treatments?
Medications may be recommended or prescribed, including NSAIDs, narcotics, muscle relaxers, and anticonvulsants. Some doctors may advise cortisone injections to reduce inflammation. Physical therapy may be recommended as a stand-alone treatment or in conjunctions with other treatments. Surgery for herniated discs is rare and usually reserved as a last resort option.
Chiropractic has been very effective in helping patients manage their pain and regain their mobility so they can return to their normal life. Therefore, it should be your first option for treatment before you go down the road with drugs or surgery.
Sciatica is a collection of symptoms characterized by pain, discomfort, tingling sensations, and numbness, in the low back. The painful symptoms of sciatica can affect a person’s quality of life. Edgar M. Reyes was unable to walk or engage in his regular physical activities, and he was diagnosed with sciatica.
Dr. Jimenez, a doctor of chiropractic in El Paso, TX, has tremendously helped Mr. Reyes find relief from his painful symptoms. He expresses how much Dr. Jimenez has helped him with his sciatic nerve pain, and he highly recommends Dr. Jimenez and his staff as the non-surgical choice for sciatica and low back pain.
El Paso Back Clinic
Professional worker carrying pipes and smiling.
We are blessed to present to you El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center, we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life filled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life.
I assure you, I will only accept the best for you�
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend us.
Individuals with diabetes have a 35 percent risk of developing neck pain and back pain, according to a recent research study. The researchers conducted eight research studies on separate occasions which revealed that individuals with diabetes have a higher chance of developing neck pain and back pain. According to the researchers, chronic pain is common in people with diabetes.
Approximately 80 percent of the population will experience some type of back pain throughout their lifetime and nearly half of that number will also suffer from neck pain, according to researchers. Meanwhile, diabetes has become an increasingly common health issue. About 382 million individuals have been diagnosed with type 2 diabetes, according to the World Health Organization.
Despite the outcome measures, it seems there’s still inadequate evidence in the research study to establish a causal connection between diabetes and chronic pain,” stated Manuela Ferreira, Ph.D., the research study’s senior author and associate professor in the university’s Institute of Bone and Joint Research. “The evidence requires further evaluation of this institution,” he explained.
“Type 2 diabetes and chronic back pain both have a strong connection with lack of physical activity or exercise and obesity. Thus, a logical development of the research study may be required to evaluate these outcome measures in further detail,” he explained. “Our evaluation adds to the proof that weight management and physical activity or exercise play essential roles in health and wellness.”
The research study also demonstrated that diabetes drugs and/or medications might also influence chronic pain, possibly via its effect on blood sugar levels. However, this connection also requires further research studies. Additionally, the research study advocated that health professionals should consider screening for diabetes in patients looking for chronic pain relief, such as back pain or neck pain.
Chronic pain affects many individuals with diabetes. The most common type of chronic pain frequently reported by patients with diabetes include neck pain, back pain, and neuropathic pain in the hands and feet. Chronic pain can affect an individual’s daily physical activities. According to researchers, individuals with diabetes have a higher risk of developing chronic pain, or painful symptoms which persist for more than six months.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
The scope of our information is limited to chiropractic, spinal health issues, and functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Acute Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly, Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
Although oral devices, such as splints and bite guards, are the most prevalent treatments for facial pain associated with temporomandibular disorders, or TMD, patients have found that these remedies are frequently less effective than self-care techniques, such as jaw exercises or warm compresses, according to a new research study published by researchers at the New York University (NYU) College of Dentistry in New York City.
The research study, published in the journal Clinical Oral Investigations, demonstrates that self-care techniques should primarily be utilized to help treat muscle-related temporomandibular disorders or TMD.
TMD, occasionally known as TMJ after the temporomandibular joint, is a collection of prevalent painful conditions which develop in the jaw joint and its surrounding muscles. Myofascial temporomandibular disorder, or mTMD, is a muscular condition which affects over 10 percent of women. Individuals with TMD often suffer from other chronic pain conditions. Research studies found that 7 to 18 percent of people with TMD also experience fibromyalgia, a condition characterized by widespread pain.
Treatments for TMD and Fibromyalgia
Dentists and patients utilize an assortment of treatments to help manage facial pain, such as oral devices like splints and bite guards, pain medicines, including nonsteroidal anti-inflammatory drugs, and self-care methods like jaw exercises and hot compresses.
Oral devices are a prevalent first-line treatment for TMD, regardless of research study outcome measures regarding their advantages, stated Vivian Santiago, Ph.D., MPH, research study scientist at the Department of Oral and Maxillofacial Pathology, Radiology, and Medicine at NYU College of Dentistry, and the research study’s leading author.
“While oral splints have been discovered to have some benefits, they have yet to be found to be as successful for patients who have widespread pain when treating mTMD,” she explained.
In this research study, the researchers evaluated what non-medication remedies women with mTMD utilized to handle their pain as well as how successful patients perceived these remedies. The researchers interviewed a total of 125 women including 26 women who had fibromyalgia and mTMD, so as to find out whether treatment differed for patients.
The most frequent treatments reported were oral devices (utilized by 59 percent of participants), physical therapy (utilized by 54 percent of participants), and at-home jaw exercises (utilized by 34 percent of participants). The least frequent treatments reported were acupuncture (utilized by 20 percent), chiropractic care (utilized by 18 percent), trigger point injections (utilized by 14 percent), yoga (utilized by 7 percent), and meditation (utilized by 6 percent). Participants frequently used more than one treatment.
Participants reported the most improvement in their pain from well-known self-care techniques, such as jaw exercises, yoga, meditation, massage, and warm compresses, with over 84 percent reporting that these techniques helped reduce painful symptoms. Only 64 percent of participants who used the oral devices reported that they helped improve their pain. About 11 percent of women who used oral devices stated that these made their pain worse, an area which warrants further research studies.
Oral devices failed to outperform self-care techniques in improving facial pain, according to Karen Raphael, Ph.D., professor at the Department of Oral and Maxillofacial Pathology, Radiology, and Medicine at NYU College of Dentistry, and the research study’s co-author.
“Our outcome measures encourage utilizing self-care techniques as the first line of treatment for mTMD before contemplating more costly interventions,” stated Raphael.
The researchers didn’t find substantial differences between the amount of remedies reported by women with and without fibromyalgia. While the use of alternative treatment options for mTMD was reported among women with fibromyalgia, further research studies are still required. Pain relief tended to be greater through the use of self-care techniques in women with and without fibromyalgia.
“While fibromyalgia is diagnosed by a healthcare professional, such as a rheumatologist, TMD is typically diagnosed and treated by a dentist,” said Santiago. “Our research study demonstrates that dentists must ask patients with facial pain if they also have widespread chronic pain because this might provide more information to help plan their treatment.”
Fibromyalgia is a health issue characterized by widespread chronic pain accompanied by fatigue, sleep, memory and mood problems. Fibromyalgia has been associated with a variety of other health issues, such as TMD and/or TMJ. Individuals with this painful disorder may often struggle to engage in their everyday physical activities. As a qualified and experienced chiropractor, I’ve helped treat numerous patients with fibromyalgia. It’s important for patients to know that they are not alone when it comes to treating their painful symptoms. Chiropractic care is an alternative treatment option which can help treat a variety of health issues, including fibromyalgia.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
The scope of our information is limited to chiropractic, spinal health issues, and functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Acute Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly, Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
Do you sometimes feel like your chronic pain becomes worse after eating certain foods? As a matter of fact, research studies have demonstrated that eating several types of foods can trigger an inflammatory response in the human body. And we all know that inflammation can be one of the primary causes for your chronic pain flare-ups. Before we discuss the foods that can cause inflammation and the foods that can fight against inflammation, let’s discuss what is inflammation and how you can measure inflammation.
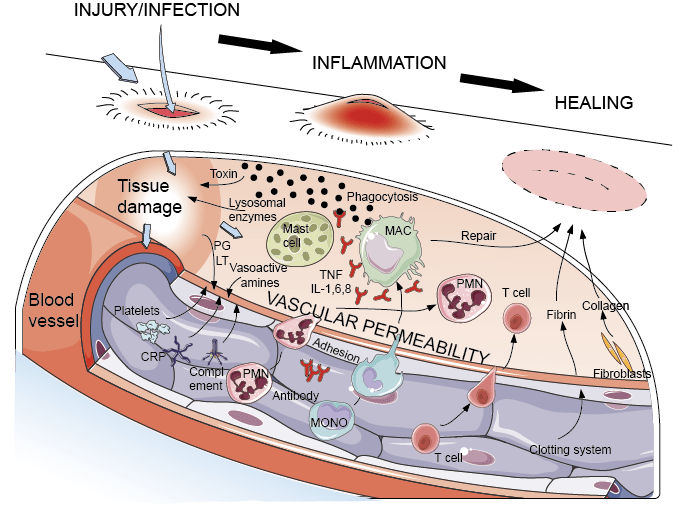
What is Inflammation?
Inflammation is the immune system’s natural defense mechanism. It functions by protecting the human body from injury, illness, and infection. Inflammation helps to maintain overall health and wellness. Allergic reactions can also result in inflammation. When you’re injured or you have an infection, you can see symptoms of inflammation: or swollen, red, and hot spots. However, inflammation may occur seemingly without a cause. The ideal way to diagnose inflammation is to measure specific biomarkers through blood tests.
The C-reactive protein, or CRP, a substance produced by the liver, is one of the best biomarkers of inflammation. CRP levels increase as inflammation increases, therefore, you can know a lot about what’s happening inside your own body by looking at your CRP levels. According to the American Heart Association and the Centers for Disease Control and Prevention, a CRP concentration of under 1.0 mg/L suggests a low risk for heart issues; between 1.0 to 3.0 mg/L suggests an average risk for heart issues; and over 3.0 mg/L suggests a high risk for heart issues. Substantial levels of CRP (greater than 10 mg/L) may also suggest a risk of developing other health issues.
Other biomarkers like activated monocytes, cytokines, chemokines, various adhesion molecules, adiponectin, fibrinogen, and serum amyloid alpha, are other biomarkers which can be measured through blood tests to diagnose inflammation. Inflammatory responses consist of sympathetic activity, oxidative stress, nuclear factor kappaB (NF-kB) activation, and proinflammatory cytokine production.
White blood cells play an important part in the human body’s immune system. Every time a bacteria or virus enters the bloodstream, the white blood cells, or leukocytes, recognize and destroy the foreign invaders. You might believe that an increased white blood cell count may be beneficial since white blood cells fight infection, however, this may not necessarily be the case. An increased white blood cell count may indicate the presence of another health issue, although a large white blood cell count is not a problem itself.
Foods that Cause Inflammation
Not surprisingly, the same types of foods which can cause inflammation are also generally considered to be bad for our health, such as refined carbohydrates, and sodas as well as red meat, and processed meats. Inflammation is an important underlying mechanism which has been associated with an increased risk for chronic diseases like type 2 diabetes and heart disease, among other health issues.
Unhealthy foods also contribute to weight gain, which is itself a risk factor for inflammation. In several research studies, even after researchers took obesity into account, the connection between inflammation and these foods remained, which suggests that weight gain is not a cause of inflammation. Some foods have an increased effect on inflammation and increased caloric consumption.
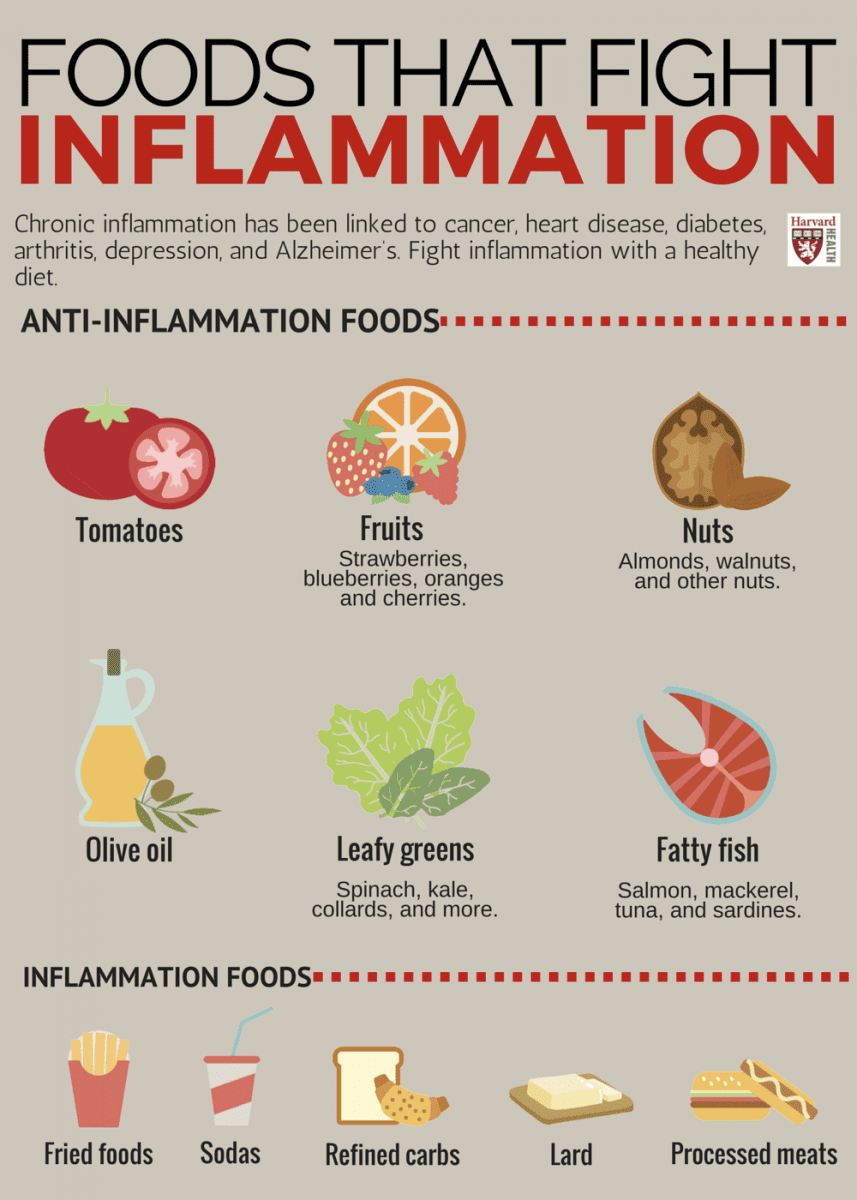
Foods that can cause inflammation include:
Refined carbohydrates, such as white bread and pastries
French fries and other fried foods
Sodas and other sugar-sweetened drinks
Red meat like burgers and steaks as well as processed meat like hot dogs and sausage
Margarine, shortening, and lard
Foods that Fight Against Inflammation
Alternatively, there are foods that fight against inflammation, and with it, chronic disease. Certain fruits and vegetables, such as blueberries, apples, and leafy greens, are high in polyphenols and antioxidants, which are components that may have anti-inflammatory effects. Research studies also have associated nuts with reduced biomarkers of inflammation and a decreased risk of diabetes and cardiovascular disease. Coffee may protect against inflammation, as well. Choose anti-inflammatory foods and you could improve your overall health and wellness. Choose inflammatory foods and you might increase the risk of inflammation and chronic pain.
Foods that can fight against inflammation include:
Tomatoes
Olive oil
Green leafy vegetables, such as spinach, kale, and collards
Nuts like almonds and walnuts
Fatty fish, such as salmon, tuna, mackerel, and sardines
Fruits like strawberries, blueberries, cherries, and oranges
Healthcare professionals are learning that one of the greatest ways to reduce inflammation is found. not in the medicine cabinet, but in the refrigerator. An anti-inflammatory diet can ultimately help reduce the human body’s inflammatory response. The immune system triggers inflammation to protect the human body from injury, illness, and infection. But if inflammation continues, it can cause a variety of health issues, including chronic pain symptoms. Research studies have demonstrated that certain food can influence the effects of inflammation in the human body.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
Anti-Inflammatory Diets
To reduce inflammation, focus on following an overall healthier diet. If you’re looking for an anti-inflammatory diet, consider following the Mediterranean diet, which is high in fruits, vegetables, nuts, whole grains, fish, and oils. The Longevity Diet Plan, presented in the book by Dr. Valter Longo, also eliminates foods which can cause inflammation, promoting well-being and longevity. Fasting, or caloric restriction, has long been known to decrease oxidative stress and slow down the mechanisms of aging in various organisms.
And if fasting is not for you, Dr. Valter Longo’s longevity diet plan also includes the fasting mimicking diet, or FMD, which allows you to experience the benefits of traditional fasting without depriving your body of food. The main difference of the FMD is that instead of eliminating all food for several days or even weeks, you only restrict your calorie intake for five days out of the month. The FMD can be practiced once a month to help promote overall health and wellness as well as to help reduce inflammation and chronic pain.
While anyone can follow the FMD on their own, Dr. Valter Longo offers the ProLon� fasting mimicking diet, a 5-day meal program which has been individually packed and labeled to serves the foods you need for the FMD in precise quantities and combinations. The meal program consists of ready-to-eat and easy-to-prepare, plant-based foods, including bars, soups, snacks, supplements, a drink concentrate, and teas. However, before starting the ProLon� fasting mimicking diet, 5-day meal program, or any of the lifestyle modifications described above, please make sure to talk to a doctor to find out which chronic pain treatment is right for you.
In addition to reducing inflammation, a more natural, less processed diet can have noticeable effects on your physical and emotional health. The scope of our information is limited to chiropractic, spinal health issues, and functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Acute Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly, Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine