Origin: The most common cause of�migraines/headaches�can relate to neck complications. From spending excessive time looking down at a laptop, desktop, iPad, and even from constant texting, an incorrect posture for extended periods of time can begin to place pressure on the neck and upper back leading to problems that can cause headaches. The majority of these type of headaches occurs as a result of tightness between the shoulder blades, which in turn causes the muscles on the top of the shoulders to also tighten and radiate pain into the head.
Arteriovenous malformations and expanding aneurysms
Lupus cerebritis
Venous sinus thrombosis
Cervical fracture or malformation
Fracture or dislocation
Occipital neuralgia
Vertebral artery dissection
Chiari malformation
Metabolic
Hypoglycemia
Hypercapnea
Carbon monoxide
Anoxia
Anemia
Vitamin A toxicity
Glaucoma
Subarachnoid Hemorrhage
Usually due to ruptured aneurysm
Sudden onset of severe pain
Often vomiting
Patient appears ill
Often nuchal rigidity
Refer for CT and possibly lumbar puncture
Meningitis
Patient appears ill
Fever
Nuchal rigidity (except in elderly and young children)
Refer for lumbar puncture – diagnostic
Neoplasms
Unlikely cause of HA in average patient population
Mild and nonspecific head pain
Worse in the morning
May be elicited by vigorous head shaking
If focal symptoms, seizures, focal neurologic signs, or evidence of increased intracranial pressure are present rule our neoplasm
Subdural Or Epidural Hemorrhage
Due to hypertension, trauma or defects in coagulation
Most often occurs in the context of acute head trauma
Onset of symptoms may be weeks or months after an injury
Differentiate from the common post-concussion headache
Post-Concussive HA may persist for weeks or months after an injury and be accompanied by dizziness or vertigo and mild mental changes, which will all subside
Exquisite tenderness and/or swelling over the temporal or occipital arteries
Evidence of arterial insufficiency in the distribution of branches of the cranial vessels
High ESR
Cervical Region HA
Neck trauma or with symptoms or signs of cervical root or cord compression
Order MR or CT cord compression due to fracture or dislocation
Cervical instability
Order cervical spine x-rays lateral flexion and extension views
Ruling Out Dangerous HA
Rule our history of serious head or neck injury, seizures or focal neurologic symptoms, and infections that may predispose to meningitis or brain abscess
Check for fever
Measure blood pressure (concern if diastolic >120)
Ophthalmoscopic exam
Check neck for rigidity
Auscultate for cranial bruits.
Complete neurologic examination
If needed order complete blood cell count, ESR, cranial or cervical imaging
Episodic Or Chronic?
<15 days per month = Episodic
>15 days per month = Chronic
Migraine HA
Generally due to dilation or distension of cerebral vasculature
Serotonin In Migraine
AKA 5-hydroxytryptamine (5-HT)
Serotonin becomes depleted in migraine episodes
IV 5-HT can stop or reduce severity
Migraine With Aura
History of at least 2 attacks fulfilling the following criteria
One of the following fully reversible aura symptoms:
Visual
Somatic sensory
Speech or language difficulty
Motor
Brain stem
2 of the following 4 characteristics:
1 aura symptom spreads gradually over ?5 min, and/or 2 symptoms occur in succession
Each individual aura symptom lasts 5-60 min
1 aura symptom is unilateral
Aura accompanied or followed in <60 min by headache
Not better accounted for by another ICHD-3 diagnosis, and TIA excluded
Migraine Without Aura
History of at least 5 attacks fulfilling the following criteria:
Headache attacks lasting 4-72 h (untreated or unsuccessfully treated)
Unilateral pain
Pulsing/pounding quality
Moderate to severe pain intensity
Aggravation by or causing avoidance of routine physical activity
During headache nausea and/or sensitivity to light and sound
Not better accounted for by another ICHD-3 diagnosis
Cluster Headache
Severe unilateral orbital, supraorbital and/or temporal pain
�Like an ice pick stabbing me the eye�
Pain lasts 15-180 minutes
At least one of the following on the side of headache:
Conjunctival injection
Facial sweating
Lacrimation
Miosis
Nasal congestion
Ptosis
Rhinorrhea
Eyelid edema
History of similar headaches in the past
Tension Headache
Headache pain accompanied by two of the following:
Pressing/tightening (non-pulsing) quality
�Feels like a band around my head�
Bilateral location
Not aggravated by routine physical activity
Headache should be lacking:
Nausea or vomiting
Photophobia and phonophobia (one or the other may be present)
History of similar headaches in the past
Rebound Headache
Headache occurring on ?15 days a month in a patient with a pre-existing headache disorder
Regular overuse for >3 months of one or more drugs that can be taken for acute and/or symptomatic treatment of headache
Due to medication overuse/withdrawal
Not better accounted for by another ICHD-3 diagnosis
Sources
Alexander G. Reeves, A. & Swenson, R. Disorders of the Nervous System. Dartmouth, 2004.
Headaches are very common health issues, and lots of people treat themselves by using basic painkillers, drinking additional water, with rest, or by simply waiting for the headache to go away on its own. As a matter of fact, a headache is among the most common reasons for doctor office visits.
Just about everyone will experience a headache sometime during their life. Most headaches are not caused by serious or sinister conditions. However, people understandably worry if headaches feel different, whether they’re especially severe, particularly frequent or unusual in any other manner. But, the most common concern is whether the headache may be a symptom of an underlying health issue, such as a brain tumor.
The following article discusses headaches generally. It explains the various types of headaches you may experience and describes those very rare situations where a headache may be a symptom of a serious disease.
Types of Headaches
Headaches can be categorized as primary, or they can be classified as secondary, meaning they are a side-effect of another injury or condition.
A healthcare professional can usually determine the possible cause of your headaches from speaking to you and examining you. When they have found the cause then you’ll have the ability to decide the best treatment approach for your head pain symptoms. This may involve taking drugs only when you get the headaches, taking daily medication to stop them altogether, and/or even stopping medication you’re already taking. Very occasionally, headaches may need further diagnosis to rule out more serious underlying causes. Chiropractic care and physical therapy are also commonly utilized to help treat headaches. Below, we will discuss the different types of headaches.
Primary Headaches
The most common types of headaches, by far, are tension headaches and migraines.
Tension Headaches
Tension headaches are generally felt as a band around the forehead. They may last for many days. They may be tiring and uncomfortable, but they don’t normally disturb sleep. Most people can carry on working with a tension headache. These often have a tendency to worsen as the day progresses, however, they aren’t usually made worse with physical activities, though it’s not strange to be somewhat sensitive to bright light or noise.
Migraines
Migraines are also very common types of headaches. A typical migraine is described as a throbbing sensation. Headaches which are one-sided, headaches which throb and headaches that make you feel sick are more inclined to be migraines compared to anything else. Migraines are often severe enough to be disabling. Some individuals will need to go to bed to sleep off their aggravation.
Cluster Headaches
Cluster headaches are extremely severe headaches, sometimes called “suicide headaches”. They occur in clusters, often every day for a number of days or maybe weeks. Then they vanish for weeks on end. These types of headaches are rare and often occur particularly in adult male smokers. They’re intense, one-sided headaches, which are very disabling, meaning they stop routine activity. People often describe them as the worst pain they have ever felt. Cluster headaches are typically one-sided. Patients frequently have a red watery eye on the other hand, a stuffy runny nose and a droopy eyelid.
Chronic Tension Headaches
Chronic tension headaches (or chronic daily headache) is generally caused by muscle tension in the back of the neck and affects women more frequently than men. Chronic means that the problem is persistent and ongoing. These headaches can develop due to neck injuries or tiredness and may worsen with drug/medication overuse. A headache that occurs virtually every day for 3 weeks or more is known as a chronic daily headache or a chronic tension headaches.
Medication-Overuse Headaches
Medication-overuse headaches or medication-induced aggravation, is an unpleasant and long-term headache. It’s brought on by taking painkillers usually meant for headaches. Unfortunately, when painkillers are taken regularly for headaches, the body reacts by creating additional pain sensors in the brain. Finally, the pain sensors are so many that the head becomes super-sensitive and the headache won’t go away. Individuals who have these headaches often take an increasing number of painkillers to attempt and feel much better. But, the painkillers may have regularly long ceased to work. Medication-overuse headaches are the most common cause of secondary headache.
Exertional Headaches/Sexual Headaches
Exertional headaches are headaches associated with physical activity. They may get severe very quickly following a strenuous activity like coughing, running, with intercourse, and straining with bowel movements. They’re more commonly experienced by patients that also have migraines, or who have relatives with migraine.
Headaches associated with sex particularly worry patients. They can occur as sex starts, at orgasm, or following sex. Headaches at orgasm would be the most common type. They are generally acute, at the back of the head, behind the eyes or all around. They last about twenty minutes and aren’t usually an indication of any other underlying health issues or problems.
Exertional and sexual intercourse-related headaches aren’t typically an indication of serious underlying problems. Very occasionally, they can be a sign that there is a leaky blood vessel on the surface of the brain. As a result, if they are marked and repeated, it’s sensible to talk about them with your healthcare professional.
Primary Stabbing Headaches
Primary traumatic headaches are sometimes called “ice-pick headaches” or “idiopathic stabbing headache”. The term “idiopathic” is used by doctors for something that comes without a clear cause. These are brief, stabbing headaches that are extremely sudden and severe. They generally last between 5 and 30 seconds and they occur at any time of the day or night. They feel as though a sharp object, like an ice pick, is being stuck into your head. They frequently occur in or just behind the ear and they are sometimes quite frightening. Even though they aren’t migraines they’re more prevalent in those who suffer from migraines, nearly half of individuals who experience migraines have principal stabbing headaches.
They are often felt at the place on the head where the migraines have a tendency to happen. Primary stabbing headaches are too brief to take care of, even though migraine prevention medications may reduce their number.
Hemicrania Continua
Hemicrania continua is a major chronic daily headache. It typically induces a continuous but shifting pain on one side of the brain. The pain is generally continuous with episodes of severe pain, which can last between 20 minutes and several days. During those episodes of severe pain there may be other symptoms, such as watering or redness of the eye, runny or blocked nose, and drooping of the eyelid, around precisely the same side as the aggravation. Similar to a migraine, there may also be sensitivity to light, feeling sick, such as nausea, and being sick, such as vomiting. The headaches do not go away but there may be periods when you don’t have any headaches. Hemicrania continua headaches respond to medicine called indometacin.
Trigeminal Neuralgia
Trigeminal neuralgia causes facial pain. The pain consists of very short bursts of electric shock-like sensations in the face, particularly at the area of the eyes, nose, scalp, brow, lips or limbs. It’s usually one-sided and is more common in people over age 50. It may be triggered by touch or a light breeze on the surface area.
Headache Causes
Occasionally, headaches have underlying causes, and treatment of the headache involves treating the cause. Individuals often fear that headaches are caused by serious illness, or by high blood pressure. Both of these are extremely uncommon causes of headache, really increased blood pressure usually causes no symptoms in any way.
Chemicals, Drugs and Substance Withdrawal
Headaches can be because of a substance, or its withdrawal, for example:
Carbon monoxide, that is made by gas heaters which aren’t properly ventilated
Drinking alcohol, with headache often experienced the morning afterwards
Deficiency of body fluid or dehydration
Headaches Due to Referred Pain
Some headaches may be caused by pain in some other portion of the head, such as ear or tooth pain, pain in the jaw joint and pain in the neck.
Sinusitis is also a frequent cause of headaches. The sinuses are “holes” in the skull which are there to stop it from becoming too heavy for the neck to transport around. They are lined with mucous membranes, such as the lining of the nose, and this creates mucus in response to colds or allergy. The liner membranes also swell and can block the drainage of the mucus out of the space. It subsequently becomes cracked and infected, resulting in headache. The headache of sinusitis is often felt at the front of the head and also in the face or teeth.
Frequently the face feels tender to tension, particularly just below the eyes beside the nose. You might have a stuffy nose and the pain is often worse when you bend forwards. Acute sinusitis is the kind that comes on fast in conjunction with a cold or abrupt allergy. You may have a temperature and be generating a lot of mucus. Chronic sinusitis may be caused by allergy, by overusing decongestants or with the acute sinusitis that doesn’t settle. The sinuses become chronically infected and the nasal linings chronically swollen. The contents of this uterus may be thick but frequently not infected.
Acute glaucoma can cause severe headaches. In this condition, the pressure inside the eyes goes up suddenly and this causes a surprisingly, very severe headache behind the eye. Even the eyeball can feel really hard to touch, the eye is red, the front part of the eye, or cornea, can seem cloudy and the eyesight is generally blurred.
What Types of Headaches are Dangerous or Serious?
All headaches are unpleasant and some, such as headache from medication abuse, are serious in the sense that if not treated correctly they might never go away. But a few headaches are indications of serious underlying issues. These are uncommon, in many cases very rare. Dangerous headaches often occur suddenly, and also eventually become increasingly worse over time. They are more common in elderly people. They comprise of the following:
Bleeding Around the Brain (Subarachnoid Haemorrhage)
Subarachnoid haemorrhage is a really serious condition which occurs when a tiny blood vessel pops on the surface of the brain. Patients develop a serious headache and stiff neck and may become unconscious. This is a rare cause of acute headache.
Meningitis and Brain Infections
Meningitis is infection of the tissues around and on the surface of the brain and encephalitis is infection of the brain itself. Brain infections can be caused by germs called bacteria, viruses or parasites and they are thankfully rare. They cause a severe, disabling headache. Normally, patients may feel sick or vomit and can’t bear bright lights, something known as photophobia. Often they have a rigid neck, too stiff for your physician to have the ability to bend the head down so that the chin touches the chest, even in the event that you attempt to relax. Patients are generally also unwell, experiencing hot, sweaty and overall sick sensations.
Giant Cell Arteritis (Temporal Arteritis)
Giant cell arteritis (temporal arteritis) is, generally, just seen in people over the age of 50. It is due to swelling, or inflammation, of the arteries at the temples and behind the eye. It causes a headache behind the forehead, also referred to as a sinus headache. Typically the blood vessels at the forehead are tender and individuals detect pain from the scalp when they comb their own hair. Frequently the pain gets worse with chewing. Temporal arteritis is severe because if it’s not treated it can cause sudden loss of eyesight. Treatment is with a course of steroids. The need to keep these steroids is generally monitored by the GP through blood tests, and they are typically needed for several months.
Brain Tumors
Brain tumors are a very uncommon cause of headache, although most patients with long-term, severe or persistent headaches start to worry that this might be the reason. Brain tumors can lead to headaches. Usually the aggravation of brain tumors exists on waking in the morning, is worse on sitting up, and becoming steadily worse in the day to day, never easing and never disappearing. It can sometimes be worse on coughing and sneezing, as may sinus headaches and migraines.
When Should I Worry About a Headache?
Most headaches do not have a serious underlying cause. However, healthcare professionals are trained to ask you about the signs and symptoms that might suggest your headache needs further diagnosis, just to make certain it’s nothing serious.
The things which would suggest to your physician and nurse that your headache may need additional evaluation include the following. They don’t mean that your headache is severe or sinister, but they imply that the healthcare professional may wish to do some additional evaluations to make sure if:
You have had a substantial head injury in the previous three months.
Your headaches are worsening and accompanied with high temperature or fever.
Your headaches begin extremely unexpectedly.
You’ve developed problems with speech and balance as well as headache.
You’ve developed problems with your memory or changes in your behavior or personality in addition to headache.
You’re confused or muddled along with your headache.
Your headache started when you coughed, sneezed or strained.
Your headache is much worse when you sit or stand.
Your headache is associated with red or painful eyes.
Your headaches are not like anything you’ve ever experienced before.
You have unexplained nausea together with the aggravation.
You have low immunity, for instance, when you have HIV, or are about oral steroid medicine or immune suppressing drugs.
You have or have had a type of cancer that can spread throughout the body.
Dr. Alex Jimenez’s Insight
Headaches are extremely common health issues which affect a wide range of the population around the world. Although frequent, a headache which is described to be like no other ever experienced before, may often become a concern. There are several types of headaches which can be caused by a variety of injuries and/or underlying conditions. As a healthcare professional, it’s essential to be able to determine between sinister or dangerous types of headaches and benign types of headaches, in order to decide the best treatment approach. By properly diagnosing the source of a patient’s headaches, both benign and sinister types of headaches can be treated accordingly.
Overview
Many headaches, whilst unpleasant, are harmless and react to a variety of treatments, including chiropractic care. Migraine, tension headaches and medication-overuse headaches are very common. The majority of the populace will experience one or more of these. Working out exactly the underlying cause of any headaches through discussion with your doctor is often the best method to resolve them. It is possible to develop a persistent or chronic and constant headache through taking drugs and/or medications that you took to get rid of your headache. Your physician can support you through the practice of quitting painkillers when that is the case.
Headaches are, quite infrequently, an indication of a serious or sinister underlying illness, and many headaches go away on their own.
If you have a headache which is uncommon for you then you need to discuss it with your doctor. You should also speak to your doctor about headaches which are particularly severe or that affect your regular activities, those that are associated with other symptoms, such as tingling or weakness, and those which make your own scalp tender, especially if you’re over 50 years old. Finally, always speak to a healthcare professional when you have an unremitting morning headache which is present for at least three days or is becoming gradually worse.
Remember that headaches are not as likely to occur in people who:
Handle their anxiety levels well.
Eat a balanced, regular diet.
Take balanced routine exercise.
Focus on posture and core muscles.
Sleep on two pillows or fewer.
Drink loads of water.
Have plenty of sleep.
Anything that you can do to enhance one or more of these aspects of your life will improve your health and well-being and cut back the number of headaches you experience. Make sure to seek the appropriate medical attention from a qualified and experienced healthcare professional in the event of a severe headache unlike anything you’ve ever experienced before. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Chiropractic Benefits: If you have ever had a migraine before then you know that it is much more than a simple headache. The symptoms of a migraine can be debilitating, lasting hours and even days. According to the Migraine Research Foundation, it is the eighth most disabling disease in the world. It is estimated that 38 million people in the United States alone suffer from migraine headaches. That�s around one in every ten people.
According to the Migraine Research Foundation, migraine headaches are extremely difficult to treat and even more difficult to control. This is mainly due to the fact that doctors still don�t know exactly what causes it. This leaves it undiagnosed in many patients and often terribly under treated in those with a diagnosis.
The best many doctors seem to be able to do is prescribe pain medication that has undesirable side effects in an effort to manage the symptoms. However, chiropractic has been shown in several studies to not only effectively manage the pain of migraines, it also helps stop and prevent them.
Anatomy Of A Migraine Headache
There are two types of migraines, those with an aura and those without an aura. An aura can appear up to an hour before the onset of a migraine. It is a warning sign that usually presents as a disturbance that is either visual or olfactory. The person may see flashes of light or smell particular odors before the headache begins. About one in six migraines are preceded by an aura.
Once the migraine itself begins, the pain is typically on one side of the head, although this is not always the case. Other symptoms may include nausea, vomiting, sensitivity to noise, sensitivity to light, and sensitivity to smell. Some patients experience an inability to concentrate, hot or cold flashes, stiffness in neck or shoulders, slurred speech, loss of coordination, and in rare cases, loss of consciousness.
The migraine can last several minutes, hours, or even days. Afterwards the patient may feel fatigued or washed out. They may be unable to concentrate and either lethargic or extremely energetic.
Studies Show: Chiropractic As A Migraine Treatment
There have been several clinical studies on chiropractic as a treatment for migraine headaches. The results of one study reported that 22 percent of patients who received chiropractic treatment for their migraines reported that their attacks were reduced by more than 90 percent. Additionally, 49 percent reported that the intensity of their migraines was significantly reduced.
Another study randomly assigned people with migraine headaches several different treatments. One group was given Elavil, a daily medication, another group was given chiropractic treatment and a third group received a combination of the two treatments. The results showed that chiropractic was as effective in reducing migraines as the medication and it had fewer side effects. Other studies have also found that chiropractic is as effective as medication for the treatment and prevention of migraine or tension headaches.
Chiropractic Benefits For Migraines Headaches
Spinal adjustments are very effective as a treatment for migraines. The whole body approach of chiropractic also utilizes dietary recommendations, including foods to avoid, as well as lifestyle changes.
The patient may be counseled on managing stress, advised to engage in exercise, and given supplements. The treatments may be used to reduce the pain and severity of a migraine once it begins or it can be used to prevent migraines and reduce their frequency.
Chiropractic benefits everyone and is a safer treatment with fewer side effects than�prescription medications. Chiropractic is quickly becoming the treatment of choice for many migraine sufferers. As the studies show, it works! So if you or a loved one suffer from migraines, give us a call. Our Doctor of Chiropractic is here to help!
Suffer Migraines: If you�ve ever had a migraine you know that it�s more than just a headache. The debilitating pain can be accompanied by nausea and other symptoms � and it�s more common than you may think. Research shows that in every four American households, one person is a migraine sufferer. In fact, 12 percent of the U.S. population suffers from migraines, including children. This means migraines affect more people that asthma and diabetes combined.
It is estimated that 18 percent of women suffer from migraines while 6 percent of men are migraine sufferers. It most commonly affects people who are between the ages of 25 and 55, but even young children have been diagnosed. Migraines can stop you in your tracks, but there are treatments that can help. Chiropractic care has been shown to help ease the pain, intensity, and frequency of migraines.
Suffer From Migraines
What Is A Migraine?
Migraines are vicious headaches that can last several minutes to several hours or even days. It is characterized by intense pulsing or a throbbing sensation that is typically confined to one area of the head. It is often accompanied by vomiting, nausea, and extreme sensitivity to sound and light. The pain can be so severe that you can barely function. Many people find themselves confined to bed in a darkened room, waiting for it to pass.
Many times migraine sufferers report experiencing an aura, or sensory warning symptoms, such as strange smells, blind spots, flashes of light, or tingling in your leg or arm. They also tend to run in families. If one parent is a migraine sufferer the child has a 40 percent chance of having migraines as well. If both parents get migraines that chance jumps to 90 percent. It is the 8th most debilitating illness on a global scale.
For the most part, doctors do not know much about what causes migraines. However, there are some things that have been identified as migraine triggers:
Hormonal changes � at certain times during the month, women experience fluctuations in estrogen which can trigger migraines
Oral contraceptives � medications that change or replace hormones can make headaches worse
Certain foods � processed foods, MSG, salty foods, aged cheeses
Fasting or skipping meals
Aspartame
Alcohol
Stress
Sensory overstimulation
Dehydration
Intense physical exertion
Too much or too little sleep
Medications
How Chiropractic Care Can Help Migraine Sufferers
Many doctors believe that headaches and migraines may be caused by a spine that is out of alignment. When your spine is misaligned your entire body suffers. It can irritate the nerves that run from the brain to the spine causing a headache. Chiropractic adjustments can help relieve the pain of migraines. In fact, many people report a distinct difference after just one session.
A Doctor of Chiropractic will align your spine and work with you to create a wellness plan that includes lifestyle changes and diet. Making changes to your sleep patterns and eliminating certain foods from your diet can help prevent migraines. By creating a whole body wellness program, you and your chiropractor can not only help prevent your migraines, but other health conditions as well.
Your chiropractor may also recommend that you keep a journal to help you pinpoint your own unique migraine triggers. You will record the foods you eat, environmental factors that may affect you, stressors, and sleep patterns, as well as when you have migraines, how long they last, and their severity. By tracking these things, you can determine what may be causing your migraines and make adjustments to your lifestyle, thus preventing them. Incorporating chiropractic care as part of your whole body maintenance, as well as migraine prevention, can help you stave off these headaches so you can get on with your life.
If you or a loved one suffers from migraine headaches, make sure you give us a call. Our Doctor of Chiropractic is here to help!
Damaris Foreman started chiropractic care with Dr. Alex Jimenez for her migraine headache pain. When every traditional treatment she received proved ineffective, she turned to spinal adjustments and manual manipulations for relief. Damaris Foreman experienced the benefits of chiropractic care almost immediately after her first visit with Dr. Alex Jimenez and she experienced reduced migraine headache pain symptoms. Furthermore, Damaris Foreman highly recommends chiropractic care with Dr. Alex Jimenez as a non-surgical choice for the effective treatment of migraines.
Globally, approximately 15 percent of people are affected by migraines. It often begins at puberty and is worst through middle age. In many women they become common during menopause. As of 2016, it is among the most common cause of disability. Migraines present with recurrent severe headache associated symptoms. Approximately 15 to 30 percent of people with migraines experience an aura. Those who have migraines with aura also frequently have migraines without aura. The seriousness of the pain, length of the headache, and frequency of the migraine may differ.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
Damaris Foreman suffered from migraines for about 23 years. After receiving traditional treatment for her migraine pain without much improvement, she was finally recommended to seek migraine pain treatment with Dr. Alex Jimenez, a chiropractor in El Paso, TX. Damaris greatly benefitted from chiropractic care and she experienced a tremendous sense of relief following her first spinal adjustment and manual manipulation. Damaris Foreman was able to confront many of her misconceptions and she learned very much about her migraine pain. Damaris describes Dr. Alex Jimenez’s migraine pain treatment as one of the best treatment she’s received and she highly recommends chiropractic care as the best non-surgical choice for improving and managing her migraines.
A migraine can be identified as a primary headache disorder characterized by recurrent headaches characterized from moderate to severe in intensity. Typically, the headaches affect one half of the head, are pulsating in nature, and can last from two to 72 hours. Associated symptoms may include nausea, vomiting, and sensitivity to light, sound, or smell. The pain may be aggravated by physical activity. Up to one-third of people who suffer from migraines experience migraine with aura: typically a brief period of visual disturbance that signals that the headache will soon happen. An aura can occur with little or no headache pain following it.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
Everyone experiences pain from time to time. Pain is a physical feeling of discomfort caused by injury or illness. When you pull a muscle or cut your finger, for instance, a signal is sent through the nerve roots to the brain, signaling you that something is wrong in the body. Pain may be different for everyone and there are several ways of feeling and describing pain. After an injury or illness heals, the pain will subside, however, what happens if the pain continues even after you’ve healed?
Chronic pain is often defined as any pain which lasts more than 12 weeks. Chronic pain can range from mild to severe and it can be the result of previous injury or surgery, migraine and headache, arthritis, nerve damage, infection and fibromyalgia. Chronic pain can affect an individual’s emotional and mental disposition, making it more difficult to relieve the symptoms. Research studies have demonstrated that psychological interventions can assist the chronic pain recovery process. Several healthcare professionals, like a doctor of chiropractic, can provide chiropractic care together with psychological interventions to help restore the overall health and wellness of their patients. The purpose of the following article is to demonstrate the role of psychological interventions in the management of patients with chronic pain, including headache and back pain.
The Role of Psychological Interventions in the Management of Patients with Chronic Pain
Abstract
Chronic pain can be best understood from a biopsychosocial perspective through which pain is viewed as a complex, multifaceted experience emerging from the dynamic interplay of a patient�s physiological state, thoughts, emotions, behaviors, and sociocultural influences. A biopsychosocial perspective focuses on viewing chronic pain as an illness rather than disease, thus recognizing that it is a subjective experience and that treatment approaches are aimed at the management, rather than the cure, of chronic pain. Current psychological approaches to the management of chronic pain include interventions that aim to achieve increased self-management, behavioral change, and cognitive change rather than directly eliminate the locus of pain. Benefits of including psychological treatments in multidisciplinary approaches to the management of chronic pain include, but are not limited to, increased self-management of pain, improved pain-coping resources, reduced pain-related disability, and reduced emotional distress � improvements that are effected via a variety of effective self-regulatory, behavioral, and cognitive techniques. Through implementation of these changes, psychologists can effectively help patients feel more in command of their pain control and enable them to live as normal a life as possible despite pain. Moreover, the skills learned through psychological interventions empower and enable patients to become active participants in the management of their illness and instill valuable skills that patients can employ throughout their lives.
Chronic pain has previously been determined to affect the psychological health of those with persistent symptoms, ultimately altering their overall mental and emotional disposition. In addition, patients with overlapping conditions, including stress, anxiety and depression, can make treatment a challenge. The role of chiropractic care is to restore as well as maintain and improve the original alignment of the spine through the use of spinal adjustments and manual manipulations. Chiropractic care allows the body to naturally heal itself without the need for drugs/medications and surgical interventions, although these can be referred to by a chiropractor if needed. However, chiropractic care focuses on the body as a whole, rather than on a single injury and/or condition and its symptoms. Spinal adjustments and manual manipulations, among other treatment methods and techniques commonly used by a chiropractor, require awareness of the patient’s mental and emotional disposition in order to effectively provide them with overall health and wellness. Patients who visit my clinic with emotional distress from their chronic pain are often more susceptible to experience psychological issues as a result. Therefore, chiropractic care can be a fundamental psychological intervention for chronic pain management, along with those demonstrated below.
Introduction
Pain is a ubiquitous human experience. It is estimated that approximately 20%�35% of adults experience chronic pain.[1,2] The National Institute of Nursing Research reports that pain affects more Americans than diabetes, heart disease, and cancer combined.[3] Pain has been cited as the primary reason to seek medical care in the United States.[4] Furthermore, pain relievers are the second most commonly prescribed medications in physicians� offices and emergency rooms.[5] Further solidifying the importance of adequate assessment of pain, the Joint Commission on the Accreditation of Healthcare Organizations issued a mandate requiring that pain be evaluated as the fifth vital sign during medical visits.[6]
The International Association for the Study of Pain (IASP) defines pain as �an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage�.[7] The IASP�s definition highlights the multidimensional and subjective nature of pain, a complex experience that is unique to each individual. Chronic pain is typically differentiated from acute pain based on its chronicity or persistence, its physiological maintenance mechanisms, and/or its detrimental impact on an individual�s life. Generally, it is accepted that pain that persists beyond the expected period of time for tissue healing following an injury or surgery is considered chronic pain. However, the specific timeframe constituting an expected healing period is variable and often difficult to ascertain. For ease of classification, certain guidelines suggest that pain persisting beyond a 3�6 month time window is considered chronic pain.[7] Nevertheless, classification of pain based solely on duration is a strictly practical and, in some instances, arbitrary criterion. More commonly, additional factors such as etiology, pain intensity, and impact are considered alongside duration when classifying chronic pain. An alternative way to characterize chronic pain has been based on its physiological maintenance mechanism; that is, pain that is thought to emerge as a result of peripheral and central reorganization. Common chronic pain conditions include musculoskeletal disorders, neuropathic pain conditions, headache pain, cancer pain, and visceral pain. More broadly, pain conditions may be primarily nociceptive (producing mechanical or chemical pain), neuropathic (resulting from nerve damage), or central (resulting from dysfunction in the neurons of the central nervous system).[8]
Unfortunately, the experience of pain is frequently characterized by undue physical, psychological, social, and financial suffering. Chronic pain has been recognized as the leading cause of long-term disability in the working- age American population.[9] Because chronic pain affects the individual at multiple domains of his/her existence it also constitutes an enormous financial burden to our society. The combined direct and indirect costs of pain have been estimated to range from $125 billion to $215 billion, annually.[10,11] The widespread implications of chronic pain include increased reports of emotional distress (eg, depression, anxiety, and frustration), increased rates of pain-related disability, pain-related alterations in cognition, and reduced quality of life. Thus, chronic pain can be best understood from a biopsychosocial perspective through which pain is viewed as a complex, multifaceted experience emerging from the dynamic interplay of a patient�s physiological state, thoughts, emotions, behaviors, and sociocultural influences.
Pain Management
Given the widespread prevalence of pain and its multi-dimensional nature, an ideal pain management regimen will be comprehensive, integrative, and interdisciplinary. Current approaches to the management of chronic pain have increasingly transcended the reductionist and strictly surgical, physical, or pharmacological approach to treatment. Current approaches recognize the value of a multidisciplinary treatment framework that targets not only nociceptive aspects of pain but also cognitive-evaluative, and motivational-affective aspects alongside equally unpleasant and impacting sequelae. The interdisciplinary management of chronic pain typically includes multimodal treatments such as combinations of analgesics, physical therapy, behavioral therapy, and psychological therapy. The multimodal approach more adequately and comprehensively addresses pain management at the molecular, behavioral, cognitive-affective, and functional levels. These approaches have been shown to lead to superior and long-lasting subjective and objective outcomes including pain reports, mood, restoration of daily functioning, work status, and medication or health care use; multimodal approaches have also been shown to be more cost-effective than unimodal approaches.[12,13] The focus of this review will be specifically on elucidating the benefits of psychology in the management of chronic pain.
Patients will typically initially present to a physician�s office in the pursuit of a cure or treatment for their ailment/acute pain. For many patients, depending on the etiology and pathology of their pain alongside biopsychosocial influences on the pain experience, acute pain will resolve with the passage of time, or following treatments aimed at targeting the presumed cause of pain or its transmission. Nonetheless, some patients will not achieve resolution of their pain despite numerous medical and complementary interventions and will transition from an acute pain state to a state of chronic, intractable pain. For instance, research has demonstrated that approximately 30% of patients presenting to their primary-care physician for complaints related to acute back pain will continue to experience pain and, for many others, severe activity limitations and suffering 12 months later.[14] As pain and its consequences continue to develop and manifest in diverse aspects of life, chronic pain may become primarily a biopsychosocial problem, whereby numerous biopsychosocial aspects may serve to perpetuate and maintain pain, thus continuing to negatively impact the affected individual�s life. It is at this point that the original treatment regimen may diversify to include other therapeutic components, including psychological approaches to pain management.
Psychological approaches for the management of chronic pain initially gained popularity in the late 1960s with the emergence of Melzack and Wall�s �gate-control theory of pain�[15] and the subsequent �neuromatrix theory of pain�.[16] Briefly, these theories posit that psychosocial and physiological processes interact to affect perception, transmission, and evaluation of pain, and recognize the influence of these processes as maintenance factors involved in the states of chronic or prolonged pain. Namely, these theories served as integral catalysts for instituting change in the dominant and unimodal approach to the treatment of pain, one heavily dominated by strictly biological perspectives. Clinicians and patients alike gained an increasing recognition and appreciation for the complexity of pain processing and maintenance; consequently, the acceptance of and preference for multidimensional conceptualizations of pain were established. Currently, the biopsychosocial model of pain is, perhaps, the most widely accepted heuristic approach to understanding pain.[17] A biopsychosocial perspective focuses on viewing chronic pain as an illness rather than disease, thus recognizing that it is a subjective experience and that treatment approaches are aimed at the management, rather than the cure, of chronic pain.[17] As the utility of a broader and more comprehensive approach to the management of chronic pain has become evident, psychologically-based interventions have witnessed a remarkable rise in popularity and recognition as adjunct treatments. The types of psychological interventions employed as part of a multidisciplinary pain treatment program vary according to therapist orientation, pain etiology, and patient characteristics. Likewise, research on the effectiveness of psychologically based interventions for chronic pain has shown variable, albeit promising, results on key variables studied. This overview will briefly describe frequently employed psychologically based treatment options and their respective effectiveness on key outcomes.
Current psychological approaches to the management of chronic pain include interventions that aim to achieve increased self-management, behavioral change, and cognitive change rather than directly eliminate the locus of pain. As such, they target the frequently overlooked behavioral, emotional, and cognitive components of chronic pain and factors contributing to its maintenance. Informed by the framework offered by Hoffman et al[18] and Kerns et al,[19] the following frequently employed psychologically-based treatment domains are reviewed: psychophysiological techniques, behavioral approaches to treatment, cognitive behavioral therapy, and acceptance-based interventions.
Psychophysiological Techniques
Biofeedback
Biofeedback is a learning technique through which patients learn to interpret feedback (in the form of physiological data) regarding certain physiological functions. For instance, a patient may use biofeedback equipment to learn to recognize areas of tension in their body and subsequently learn to relax those areas to reduce muscular tension. Feedback is provided by a variety of measurement instruments that can yield information about brain electrical activity, blood pressure, blood flow, muscle tone, electrodermal activity, heart rate, and skin temperature, among other physiological functions in a rapid manner. The goal of biofeedback approaches is for the patient to learn how to initiate physiological self-regulatory processes by achieving voluntary control over certain physiological responses to ultimately increase physiological flexibility through greater awareness and specific training. Thus a patient will use specific self-regulatory skills in an attempt to reduce an undesired event (eg, pain) or maladaptive physiological reactions to an undesired event (eg, stress response). Many psychologists are trained in biofeedback techniques and provide these services as part of therapy. Biofeedback has been designated as an efficacious treatment for pain associated with headache and temporomandibular disorders (TMD).[20] A meta-analysis of 55 studies revealed that biofeedback interventions (including various biofeedback modalities) yielded significant improvements with regard to frequency of migraine attacks and perceptions of headache management self-efficacy when compared to control conditions.[21] Studies have provided empirical support for biofeedback for TMD, albeit more robust improvements with regard to pain and pain-related disability have been found for protocols that combine biofeedback with cognitive behavioral skills training, under the assumption that a combined treatment approach more comprehensively addresses the gamut of biopsychosocial problems that may be encountered as a result of TMD.[22]
Behavioral Approaches
Relaxation Training
It is generally accepted that stress is a key factor involved in the exacerbation and maintenance of chronic pain.[16,23] Stress can be predominantly of an environmental, physical, or psychological/emotional basis, though typically these mechanisms are intricately intertwined. The focus of relaxation training is to reduce tension levels (physical and mental) through activation of the parasympathetic nervous system and through attainment of greater awareness of physiological and psychological states, thereby achieving reductions in pain and increasing control over pain. Patients can be taught several relaxation techniques and practice them individually or in conjunction with one another, as well as adjuvant components to other behavioral and cognitive pain management techniques. The following are brief descriptions of relaxation techniques commonly taught by psychologists specializing in the management of chronic pain.
Diaphragmatic breathing. Diaphragmatic breathing is a basic relaxation technique whereby patients are instructed to use the muscles of their diaphragm as opposed to the muscles of their chest to engage in deep breathing exercises. Breathing by contracting the diaphragm allows the lungs to expand down (marked by expansion of abdomen during inhalation) and thus increase oxygen intake.[24]
Progressive muscle relaxation (PMR). PMR is characterized by engaging in a combination of muscle tension and relaxation exercises of specific muscles or muscle groups throughout the body.[25] The patient is typically instructed to engage in the tension/relaxation exercises in a sequential manner until all areas of the body have been addressed.
Autogenic training (AT). AT is a self-regulatory relaxation technique in which a patient repeats a phrase in conjunction with visualization to induce a state of relaxation.[26,27] This method combines passive concentration, visualization, and deep breathing techniques.
Visualization/Guided imagery. This technique encourages patients to use all of their senses in imagining a vivid, serene, and safe environment to achieve a sense of relaxation and distraction from their pain and pain-related thoughts and sensations.[27]
Collectively, relaxation techniques have generally been found to be beneficial in the management of a variety of types of acute and chronic pain conditions as well as in the management of important pain sequelae (eg, health-related quality of life).[28�31] Relaxation techniques are usually practiced in conjunction with other pain management modalities, and there is considerable overlap in the presumed mechanisms of relaxation and biofeedback, for instance.
Operant Behavior Therapy
Operant behavior therapy for chronic pain is guided by the original operant conditioning principles proposed by Skinner[32] and refined by Fordyce[33] to be applicable to pain management. The main tenets of the operant conditioning model as it relates to pain hold that pain behavior can eventually evolve into and be maintained as chronic pain manifestations as a result of positive or negative reinforcement of a given pain behavior as well as punishment of more adaptive, non-pain behavior. If reinforcement and the ensuing consequences occur with sufficient frequency, they can serve to condition the behavior, thus increasing the likelihood of repeating the behavior in the future. Therefore, conditioned behaviors occur as a product of learning of the consequences (actual or anticipated) of engaging in the given behavior. An example of a conditioned behavior is continued use of medication � a behavior that results from learning through repeated associations that taking medication is followed by removal of an aversive sensation (pain). Likewise, pain behaviors (eg, verbal expressions of pain, low activity levels) can be become conditioned behaviors that serve to perpetuate chronic pain and its sequelae. Treatments that are guided by operant behavior principles aim to extinguish maladaptive pain behaviors through the same learning principles that these may have been established by. In general, treatment components of operant behavior therapy include graded activation, time contingent medication schedules, and use of reinforcement principles to increase well behaviors and decrease maladaptive pain behaviors.
Graded activation. Psychologists can implement graded activity programs for chronic pain patients who have vastly reduced their activity levels (increasing likelihood of physical deconditioning) and subsequently experience high levels of pain upon engaging in activity. Patients are instructed to safely break the cycle of inactivity and deconditioning by engaging in activity in a controlled and time-limited fashion. In this manner, patients can gradually increase the length of time and intensity of activity to improve functioning. Psychologists can oversee progress and provide appropriate reinforcement for compliance, correction of misperceptions or misinterpretations of pain resulting from activity, where appropriate, and problem-solve barriers to adherence. This approach is frequently embedded within cognitive-behavioral pain management treatments.
Time-contingent medication schedules. A psychologist can be an important adjunct healthcare provider in overseeing the management of pain medications. In some cases, psychologists have the opportunity for more frequent and in-depth contact with patients than physicians and thus can serve as valuable collaborators of an integrated multidisciplinary treatment approach. Psychologists can institute time-contingent medication schedules to reduce the likelihood of dependence on pain medications for attaining adequate control over pain. Furthermore, psychologists are well equipped to engage patients in important conversations regarding the importance of proper adherence to medications and medical recommendations and problem-solve perceived barriers to safe adherence.
Fear-avoidance. The fear-avoidance model of chronic pain is a heuristic most frequently applied in the context of chronic low back pain (LBP).[34] This model draws largely from the operant behavior principles described previously. In essence, the fear-avoidance model posits that when acute pain states are repeatedly misinterpreted as danger signals or signs of serious injury, patients may be at risk of engaging in fear-driven avoidance behaviors and cognitions that further reinforce the belief that pain is a danger signal and perpetuate physical deconditioning. As the cycle continues, avoidance may generalize to broader types of activity and result in hypervigilance of physical sensations characterized by misinformed catastrophic interpretations of physical sensations. Research has shown that a high degree of pain catastrophizing is associated with maintenance of the cycle.[35] Treatments aimed at breaking the fear-avoidance cycle employ systematic graded exposure to feared activities to disconfirm the feared, often catastrophic, consequences of engaging in activities. Graded exposure is typically supplemented with psychoeducation about pain and cognitive restructuring elements that target maladaptive cognitions and expectations about activity and pain. Psychologists are in an excellent position to execute these types of interventions that closely mimic exposure treatments traditionally used in the treatment of some anxiety disorders.
Though specific graded exposure treatments have been shown to be effective in the treatment of complex regional pain syndrome type I (CRPS-1)[36] and LBP[37] in single-case designs, a larger-scale randomized controlled trial comparing systematic graded exposure treatment combined with multidisciplinary pain program treatment with multidisciplinary pain program treatment alone and with a wait-list control group found that the two active treatments resulted in significant improvements on outcome measures of pain intensity, fear of movement/injury, pain self-efficacy, depression, and activity level.[38] Results from this trial suggest that both interventions were associated with significant treatment effectiveness such that the graded exposure treatment did not appear to result in additional treatment gains.[38] A cautionary note in the interpretation of these results highlights that the randomized controlled trial (RCT) included a variety of chronic pain conditions that extended beyond LBP and CRPS-1 and did not exclusively include patients with high levels of pain-related fear; the interventions were also delivered in group formats rather than individual formats. Although in-vivo exposure treatments are superior at reducing pain catastrophizing and perceptions of harmfulness of activities, exposure treatments seem to be as effective as graded activity interventions in improving functional disability and chief complaints.[39] Another clinical trial compared the effectiveness of treatment-based classification (TBC) physical therapy alone to TBC augmented with graded activity or graded exposure for patients with acute and sub-acute LBP.[40] Outcomes revealed that there were no differences in 4-week and 6-month outcomes for reduction of disability, pain intensity, pain catastrophizing, and physical impairment among treatment groups, although graded exposure and TBC yielded larger reductions in fear-avoidance beliefs at 6 months.[40] Findings from this clinical trial suggest that enhancing TBC with graded activity or graded exposure does not lead to improved outcomes with regard to measures associated with the development of chronic LBP beyond improvements achieved with TBC alone.[40]
Cognitive-Behavioral Approaches
Cognitive-behavioral therapy (CBT) interventions for chronic pain utilize psychological principles to effect adaptive changes in the patient�s behaviors, cognitions or evaluations, and emotions. These interventions are generally comprised of basic psychoeducation about pain and the patient�s particular pain syndrome, several behavioral components, coping skills training, problem-solving approaches, and a cognitive restructuring component, though the exact treatment components vary according to the clinician. Behavioral components may include a variety of relaxation skills (as reviewed in the behavioral approaches section), activity pacing instructions/graded activation, behavioral activation strategies, and promotion of resumption of physical activity if there is a significant history of activity avoidance and subsequent deconditioning. The primary aim in coping skills training is to identify current maladaptive coping strategies (eg, catastrophizing, avoidance) that the patient is engaging in alongside their use of adaptive coping strategies (eg, use of positive self-statements, social support). As a cautionary note, the degree to which a strategy is adaptive or maladaptive and the perceived effectiveness of particular coping strategies varies from individual to individual.[41] Throughout treatment, problem-solving techniques are honed to aid patients in their adherence efforts and to help them increase their self-efficacy. Cognitive restructuring entails recognition of current maladaptive cognitions the patient is engaging in, challenging of the identified negative cognitions, and reformulation of thoughts to generate balanced, adaptive alternative thoughts. Through cognitive restructuring exercises, patients become increasingly adept at recognizing how their emotions, cognitions, and interpretations modulate their pain in positive and negative directions. As a result, it is presumed that the patients will attain a greater perception of control over their pain, be better able to manage their behavior and thoughts as they relate to pain, and be able to more adaptively evaluate the meaning they ascribe to their pain. Additional components sometimes included in a CBT intervention include social skills training, communication training, and broader approaches to stress management. Via a pain-oriented CBT intervention, many patients profit from improvements with regard to their emotional and functional well-being, and ultimately their global perceived health-related quality of life.
CBT interventions are delivered within a supportive and empathetic environment that strives to understand the patient�s pain from a biopsychosocial perspective and in an integrated manner. Therapists see their role as �teachers� or �coaches� and the message communicated to patients is that of learning to better manage their pain and improve their daily function and quality of life as opposed to aiming to cure or eradicate the pain. The overarching goal is to increase the patients� understanding of their pain and their efforts to manage pain and its sequelae in a safe and adaptive manner; therefore, teaching patients to self-monitor their behavior, thoughts, and emotions is an integral component of therapy and a useful strategy to enhance self-efficacy. Additionally, the therapist endeavors to foster an optimistic, realistic, and encouraging environment in which the patient can become increasingly skilled at recognizing and learning from their successes and learning from and improving upon unsuccessful attempts. In this manner, therapists and patients work together to identify patient successes, barriers to adherence, and to develop maintenance and relapse-prevention plans in a constructive, collaborative, and trustworthy atmosphere. An appealing feature of the cognitive behavioral approach is its endorsement of the patient as an active participant of his/her pain rehabilitation or management program.
Research has found CBT to be an effective treatment for chronic pain and its sequelae as marked by significant changes in various domains (ie, measures of pain experience, mood/affect, cognitive coping and appraisal, pain behavior and activity level, and social role function) when compared with wait-list control conditions.[42] When compared with other active treatments or control conditions, CBT has resulted in notable improvements, albeit smaller effects (effect size ~ 0.50), with regard to pain experience, cognitive coping and appraisal, and social role function.[42] A more recent meta-analysis of 52 published studies compared behavior therapy (BT) and CBT against treatment as usual control conditions and active control conditions at various time-points.[43] This meta-analysis concluded that their data did not lend support for BT beyond improvements in pain immediately following treatment when compared with treatment as usual control conditions.[43] With regard to CBT, they concluded that CBT has limited positive effects for pain disability, and mood; nonetheless, there are insufficient data available to investigate the specific influence of treatment content on selected outcomes.[43] Overall, it appears that CBT and BT are effective treatment approaches to improve mood; outcomes that remain robust at follow-up data points. However, as highlighted by several reviews and meta-analyses, a critical factor to consider in evaluating the effectiveness of CBT for the management of chronic pain is centered on issues of effective delivery, lack of uniform treatment components, differences in delivery across clinicians and treatment populations, and variability in outcome variables of interest across research trials.[13] Further complicating the interpretation of effectiveness findings are patient characteristics and additional variables that may independently affect treatment outcome.
Acceptance-Based Approaches
Acceptance-based approaches are frequently identified as third-wave cognitive-behavioral therapies. Acceptance and commitment therapy (ACT) is the most common of the acceptance-based psychotherapies. ACT emphasizes the importance of facilitating the client�s progress toward attaining a more valued and fulfilling life by increasing psychological flexibility rather than strictly focusing on restructuring cognitions.[44] In the context of chronic pain, ACT targets ineffective control strategies and experiential avoidance by fostering techniques that establish psychological flexibility. The six core processes of ACT include: acceptance, cognitive defusion, being present, self as context, values, and committed action.[45] Briefly, acceptance encourages chronic pain patients to actively embrace pain and its sequelae rather than attempt to change it, in doing so encouraging the patient to cease a futile fight directed at the eradication of their pain. Cognitive defusion (deliteralization) techniques are employed to modify the function of thoughts rather than to reduce their frequency or restructure their content. In this manner, cognitive defusion may simply alter the undesirable meaning or function of negative thoughts and thus decrease the attachment and subsequent emotional and behavioral response to such thoughts. The core process of being present emphasizes a non-judgmental interaction between the self and private thoughts and events. Values are utilized as guides for electing behaviors and interpretations that are characterized by those values an individual strives to instantiate in everyday life. Finally, through committed action, patients can realize behavior changes aligned with individual values. Thus, ACT utilizes the six core principles in conjunction with one another to take a holistic approach toward increasing psychological flexibility and decreasing suffering. Patients are encouraged to view pain as inevitable and accept it in a nonjudgmental manner so that they can continue to derive meaning from life despite the presence of pain. The interrelated core processes exemplify mindfulness and acceptance processes and commitment and behavior change processes.[45]
Results of research on the effectiveness of ACT-based approaches for the management of chronic pain are promising, albeit still warranting further evaluation. A RCT comparing ACT with a waitlist control condition reported significant improvements in pain catastrophizing, pain-related disability, life satisfaction, fear of movements, and psychological distress that were maintained at the 7 month follow-up.[46] A larger trial reported significant improvements for pain, depression, pain-related anxiety, disability, medical visits, work status, and physical performance.[47] A recent meta-analysis evaluating acceptance-based interventions (ACT and mindfulness-based stress reduction) in patients with chronic pain found that, in general, acceptance-based therapies lead to favorable outcomes for patients with chronic pain.[48] Specifically, the meta-analysis revealed small to medium effect sizes for pain intensity, depression, anxiety, physical wellbeing, and quality of life, with smaller effects found when controlled clinical trials were excluded and only RCTs were included in the analyses.[48] Other acceptance-based interventions include contextual cognitive-behavioral therapy and mindfulness-based cognitive therapy, though empirical research on the effectiveness of these therapies for the management of chronic pain is still in its infancy.
Expectations
An important and vastly overlooked common underlying element of all treatment approaches is consideration of the patient�s expectation for treatment success. Despite the numerous advances in the formulation and delivery of effective multidisciplinary treatments for chronic pain, relatively little emphasis has been placed on recognizing the importance of expectations for success and on focusing efforts on enhancement of patients� expectations. The recognition that placebo for pain is characterized by active properties leading to reliable, observable, and quantifiable changes with neurobiological underpinnings is currently at the vanguard of pain research. Numerous studies have confirmed that, when induced in a manner that optimizes expectations (via manipulation of explicit expectations and/or conditioning), analgesic placebos can result in observable and measurable changes in pain perception at a conscious self-reported level as well as a neurological pain-processing level.[49,50] Analgesic placebos have been broadly defined as simulated treatments or procedures that occur within a psychosocial context and exert effects on an individual�s experience and/or physiology.[51] The current conceptualization of placebo emphasizes the importance of the psychosocial context within which placebos are embedded. Underlying the psychosocial context and ritual of treatment are patients� expectations. Therefore, it is not surprising that the placebo effect is intricately embedded in virtually every treatment; as such, clinicians and patients alike will likely benefit from recognition that therein lies an additional avenue by which current treatment approaches to pain can be enhanced.
It has been proposed that outcome expectancies are core influences driving the positive changes attained through the various modes of relaxation training, hypnosis, exposure treatments, and many cognitive-oriented therapeutic approaches. Thus, a sensible approach to the management of chronic pain capitalizes on the power of patients� expectations for success. Regrettably, too often, health care providers neglect to directly address and emphasize the importance of patients� expectations as integral factors contributing to successful management of chronic pain. The zeitgeist in our society is that of mounting medicalization of ailments fueling the general expectation that pain (even chronic pain) ought to be eradicated through medical advancements. These all too commonly held expectations leave many patients disillusioned with current treatment outcomes and contribute to an incessant search for the �cure�. Finding the �cure� is the exception rather than the rule with respect to chronic pain conditions. In our current climate, where chronic pain afflicts millions of Americans annually, it is in our best interest to instill and continue to advocate a conceptual shift that instead focuses on effective management of chronic pain. A viable and promising route to achieving this is to make the most of patients� positive (realistic) expectations and educate pain patients as well as the lay public (20% of whom will at some future point become pain patients) on what constitutes realistic expectations regarding the management of pain. Perhaps, this can occur initially through current, evidence-based education regarding placebo and nonspecific treatment effects such that patients can correct misinformed beliefs they may have previously held. Subsequently clinicians can aim to enhance patients� expectations within treatment contexts (in a realistic fashion) and minimize pessimistic expectations that deter from treatment success, therefore, learning to enhance their current multidisciplinary treatments through efforts guided at capitalizing on the improvements placebo can yield, even within an �active treatment�. Psychologists can readily address these issues with their patients and help them become advocates of their own treatment success.
Emotional Concomitants of Pain
An often challenging aspect of the management of chronic pain is the unequivocally high prevalence of comorbid emotional distress. Research has demonstrated that depression and anxiety disorders are upward to three times more prevalent among chronic pain patients than among the general population.[52,53] Frequently, pain patients with psychiatric comorbidities are labeled �difficult patients� by healthcare providers, possibly diminishing the quality of care they will receive. Patients with depression have poorer outcomes for both depression and pain treatments, compared with patients with single diagnoses of pain or depression.[54,55] Psychologists are remarkably suited to address most of the psychiatric comorbidities typically encountered in chronic pain populations and thus improve pain treatment outcomes and decrease the emotional suffering of patients. Psychologists can address key symptoms (eg, anhedonia, low motivation, problem-solving barriers) of depression that readily interfere with treatment participation and emotional distress. Moreover, irrespective of a psychiatric comorbidity, psychologists can help chronic pain patients process important role transitions they may undergo (eg, loss of job, disability), interpersonal difficulties they may be encountering (eg, sense of isolation brought about by pain), and emotional suffering (eg, anxiety, anger, sadness, disappointment) implicated in their experience. Thus, psychologists can positively impact the treatment course by reducing the influence of emotional concomitants that are addressed as part of therapy.
Conclusion
Benefits of including psychological treatments in multidisciplinary approaches to the management of chronic pain are abundant. These include, but are not limited to, increased self-management of pain, improved pain-coping resources, reduced pain-related disability, and reduced emotional distress-improvements that are effected via a variety of effective self-regulatory, behavioral, and cognitive techniques. Through implementation of these changes, a psychologist can effectively help patients feel more in command of their pain control and enable them to live as normal a life as possible despite pain. Moreover, the skills learned through psychological interventions empower and enable patients to become active participants in the management of their illness and instill valuable skills that patients can employ throughout their lives. Additional benefits of an integrated and holistic approach to the management of chronic pain may include increased rates of return to work, reductions in health care costs, and increased health-related quality of life for millions of patients throughout the world.
Footnotes
Disclosure:No conflicts of interest were declared in relation to this paper.
In conclusion, psychological interventions can be effectively used to help relieve symptoms of chronic pain along with the use of other treatment modalities, such as chiropractic care. Furthermore, the research study above demonstrated how specific psychological interventions can improve the outcome measures of chronic pain management. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
According to statistics, approximately 80% of people will experience symptoms of back pain at least once throughout their lifetimes. Back pain is a common complaint which can result due to a variety of injuries and/or conditions. Often times, the natural degeneration of the spine with age can cause back pain. Herniated discs occur when the soft, gel-like center of an intervertebral disc pushes through a tear in its surrounding, outer ring of cartilage, compressing and irritating the nerve roots. Disc herniations most commonly occur along the lower back, or lumbar spine, but they may also occur along the cervical spine, or neck. The impingement of the nerves found in the low back due to injury and/or an aggravated condition can lead to symptoms of sciatica.
1.�Boris-Karpel S. Policy and practice issues in pain management. In: Ebert MH, Kerns RD, editors.�Behavioral and psychopharmacologic pain management.�New York: Cambridge University Press; 2010. pp. 407�433.
2.�Harstall C, Ospina M. How prevalent is chronic pain?�Pain: Clinical Updates.�2003;11(2):1�4.
4.�Abbot FV, Fraser MI. Use and abuse of over-the-counter analgesic agents.�J Psychiatry Neurosci.�1998;23(1):13�34.�[PMC free article]�[PubMed]
5.�Schappert SM, Burt CW. Ambulatory care visits to physician offices, hospital outpatient departments, and emergency departments: United States, 2001�02.�Vital Health Stat.�2006;13(159):1�66.�[PubMed]
6.�Joint Commission of Accreditation of Healthcare Organizations.�Pain assessment and management: an organizational approach.�Oakbrook, IL: 2000.
7.�Merskey H, Bogduk N, editors.�Classification of chronic pain.�2nd edition. Seattle, WA: IASP Press; 1994. Task Force on Taxonomy of the IASP Part III: Pain terms, a current list with definitions and notes on usage; pp. 209�214.
8.�Woessner J. A conceptual model of pain: treatment modalities.�Pract Pain Manag.�2003;3(1):26�36.
9.�Loeser JD. Economic implications of pain management.�Acta Anaesthesiol Scand.�1999;43(9):957�959.[PubMed]
10.�National Research Council.�Musculoskeletal disorders and the workplace: low back and upper extremities.�Washington, DC: National Academy Press; 2001.�[PubMed]
11.�US Bureau of the Census.�Statistical abstract of the United States: 1996.�116th edition. Washington, DC:
12.�Flor H, Fydrich T, Turk DC. Efficacy of multidisciplinary pain treatment centers: a meta-analytic review.�Pain.�1992;49(2):221�230.�[PubMed]
13.�McCracken LM, Turk DC. Behavioral and cognitive-behavioral treatment for chronic pain: outcome, predictors of outcome, and treatment process.�Spine.�2002;27(22):2564�2573.�[PubMed]
14.�Von Korff M, Saunders K. The course of back pain in primary care.�Spine.�1996;21(24):2833�2837.[PubMed]
15.�Melzack R, Wall PD. Pain mechanisms: a new theory.�Science.�1965;150(699):971�979.�[PubMed]
16.�Melzack R. Pain and stress: a new perspective. In: Gatchel RJ, Turk DC, editors.�Psychosocial factors in pain: critical perspectives.�New York: Guilford Press; 1999. pp. 89�106.
17.�Gatchel RJ. The conceptual foundations of pain management: historical overview. In: Gatchel RJ, editor.�Clinical essentials of pain management.�Washington, DC: American Psychological Association; 2005. pp. 3�16.
18.�Hoffman BM, Papas RK, Chatkoff DK, Kerns RD. Meta-analysis of psychological interventions for chronic low back pain.�Health Psychol.�2007;26(1):1�9.�[PubMed]
19.�Kerns RD, Sellinger J, Goodin BR. Psychological treatment of chronic pain.�Annu Rev Clin Psychol.�2010 Sep 27;�[Epub ahead of print]
20.�Yucha C, Montgomery D.�Evidence-based practice in biofeedback and neurofeedback.�Wheat Ridge, CO: AAPB; 2008.
21.�Nestoriuc Y, Martin A. Efficacy of biofeedback for migraine: a meta-analysis.�Pain.�2007;128(1�2):111�127.�[PubMed]
22.�Gardea MA, Gatchel RJ, Mishra KD. Long-term efficacy of biobehavioral treatment of temporomandibular disorders.�J Behav Med.�2001;24(4):341�359.�[PubMed]
23.�Turk DC, Monarch ES. Biopsychosocial perspective on chronic pain. In: Turk DC, Gatchel RJ, editors.�Psychosocial approaches to pain management: a practitioner�s handbook.�2nd edition. New York: Guilford Press; 2002. pp. 3�29.
24.�Philips HC.�The psychological management of chronic pain: a treatment manual.�New York: Springer Publishing; 1988. Orientation: chronic pain and the self-management approach; pp. 45�60.
25.�Bernstein DA, Borkovek TD.�Progressive muscle relaxation training: a manual for helping professions.Champaign, IL: Research Press; 1973.
26.�Linden W.�Autogenic training: a clinical guide.�New York: Guilford; 1990.
27.�Jamison RN.�Mastering chronic pain: a professional�s guide to behavioral treatment.�Sarasota, FL: Professional Resource Press; 1996.
28.�Baird CL, Sands L. Effect of guided imagery with relaxation on health-related quality of life in older women with osteoarthritis.�Res Nurs Health.�2006;29(5):442�451.�[PubMed]
29.�Carroll D, Seers K. Relaxation for the relief of chronic pain: a systematic review.�J Adv Nurs.�1998;27(3):476�487.�[PubMed]
30.�Morone NE, Greco CM. Mind-body interventions for chronic pain in older adults: a structured review.�Pain Med.�2007;8(4):359�375.�[PubMed]
31.�Mannix LK, Chandurkar RS, Rybicki LA, Tusek DL, Solomon GD. Effect of guided imagery on quality of life for patients with chronic tension-type headache.�Headache.�1999;39(5):326�334.�[PubMed]
32.�Skinner BF.�Science and human behavior.�New York: Free Press; 1953.
33.�Fordyce WE.�Behavioural methods for chronic pain and illness.�London, UK: The CV Mosby Company; 1976.
34.�Vlayen JW, Linton SJ. Fear-avoidance and its consequences in chronic musculoskeletal pain: a state of the art.�Pain.�2000;85(3):317�332.�[PubMed]
35.�Vlayen JW, de Jong J, Sieben J, Crombez G. Graded exposure�in vivo�for pain-related fear. In: Turk DC, Gatchel RJ, editors.�Psychosocial approaches to pain management: a practitioner�s handbook.�2nd edition. New York: Guilford Press; 2002. pp. 210�233.
36.�De Jong JR, Vlaeyen JW, Onghena P, Cuypers C, den Hollander M, Ruijgrok J. Reduction of pain-related fear in complex regional pain syndrome type I: the application of graded exposure in vivo.�Pain.�2005;116(3):264�275.�[PubMed]
37.�Boersma K, Linton S, Overmeer T, Jansson M, Vlaeyen J, de Jong J. Lowering fear-avoidance and enhancing function through exposure in vivo: a multiple baseline study across six patients with back pain.�Pain.�2004;108(1�2):8�16.�[PubMed]
38.�Bliokas VV, Cartmill TK, Nagy BJ. Does systematic graded exposure in vivo enhance outcomes in multidisciplinary chronic pain management groups?�Clin J Pain.�2007;23(4):361�374.�[PubMed]
39.�Leeuw M, Goossens ME, van Breukelen GJ, et al. Exposure in vivo versus operant graded activity in chronic low back pain patients: results of a randomized controlled trial.�Pain.�2008;138(1):192�207.[PubMed]
40.�George SZ, Zeppieri G, Cere AL, et al. A randomized trial of behavioral physical therapy interventions for acute and sub-acute low back pain (NCT00373867)�Pain.�2008;140(1):145�157.�[PMC free article][PubMed]
41.�Roditi D, Waxenberg LB, Robinson ME. Frequency and perceived effectiveness of coping define important subgroups of patients with chronic pain.�Clin J Pain.�2010;26(8):677�682.�[PubMed]
42.�Morley S, Eccleston C, Williams A. Systematic review and meta-analysis of randomized controlled trials of cognitive behaviour therapy and behaviour therapy for chronic pain in adults, excluding headache.�Pain.�1999;80(1�2):1�13.�[PubMed]
43.�Eccleston C, Williams AC, Morley S. Psychological therapies for the management of chronic pain (excluding headache) in adults.�Cochrane Database Syst Rev.�2009;(2):CD007407.�[PubMed]
44.�Blackledge JT, Hayes SC. Emotion regulation in acceptance and commitment therapy.�J Clin Psychol.�2001;57(2):243�255.�[PubMed]
45.�Hayes SC, Luoma JB, Bond FW, Masuda A, Lillis J. Acceptance and commitment therapy: model, processes, and outcomes.�Behav Res Ther.�2006;44(1):1�25.�[PubMed]
46.�Wicksell RK, Ahlqvist J, Bring A, Melin L, Olsson GL. Can exposure strategies improve functioning and life satisfaction in people with chronic pain and whiplash-associated disorders (WAD)? A randomized controlled trial.�Cogn Behav Ther.�2008;37(3):169�182.�[PubMed]
47.�Vowles KE, McCracken LM. Acceptance and values-based action in chronic pain: a study of treatment effectiveness and process.�J Consult Clinl Psychol.�2008;76(3):397�407.�[PubMed]
48.�Veehof MM, Oskam MJ, Schreurs KMG, Bohlmeijer ET. Acceptance-based interventions for the treatment of chronic pain: a systematic review and meta-analysis.�Pain.�2011;152(3):533�542.�[PubMed]
49.�Wager TD, Rilling JK, Smith EE, et al. Placebo-induced changes in�f�MRI in the anticipation and experience of pain.�Science.�2004;303(5661):1162�1167.�[PubMed]
50.�Price DD, Craggs J, Verne GN, Perlstein WM, Robinson ME. Placebo analgesia is accompanied by large reductions in pain-related brain activity in irritable-bowel syndrome patients.�Pain.�2007;127(1�2):63�72.�[PubMed]
51.�Price D, Finniss D, Benedetti F. A comprehensive review of the placebo effect: recent advances and current thought.�Annu Rev Psychol.�2008;59:565�590.�[PubMed]
52.�Holroyd KA. Recurrent headache disorders. In: Dworkin RH, Breitbart WS, editors.�Psychosocial aspects of pain: a handbook for health care providers.�Seattle, WA: IASP Press; 2004. pp. 370�403.
53.�Fishbain DA. Approaches to treatment decisions for psychiatric comorbitity in the management of the chronic pain patient.�Med Clin North Am.�1999;83(3):737�760.�[PubMed]
54.�Bair MJ, Robinson RL, Katon W, Kroenke K. Depression and pain comorbidity � a literature review.�Arch Intern Med.�2003;163(20):2433�2445.�[PubMed]
55.�Poleshuck EL, Talbot NL, Su H, et al. Pain as a predictor of depression treatment outcomes in women with childhood sexual abuse.�Compr Psychiatry.�2009;50(3):215�220.�[PMC free article]�[PubMed]
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine
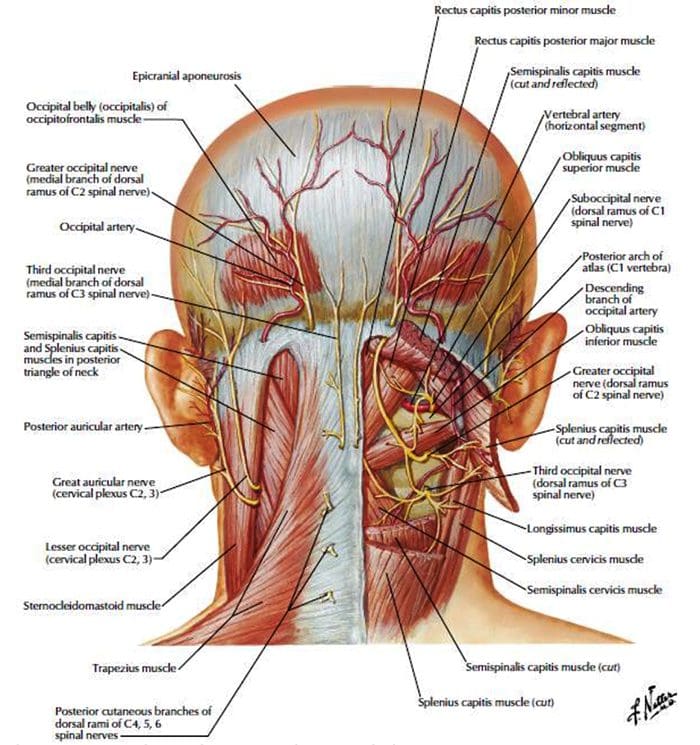 http://dailymedfact.com/neck-anatomy-the-suboccipital-triangle/
http://dailymedfact.com/neck-anatomy-the-suboccipital-triangle/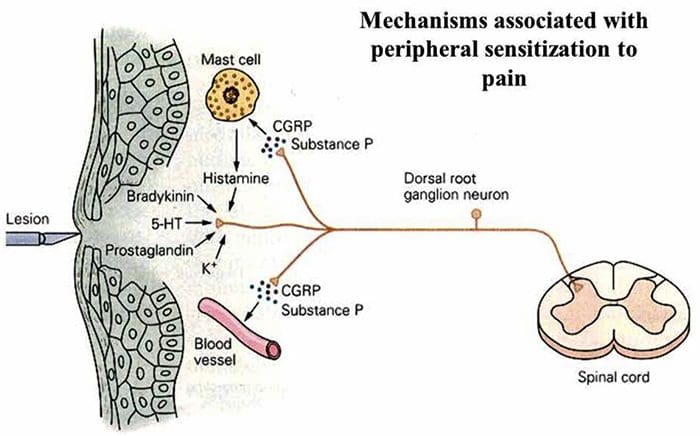
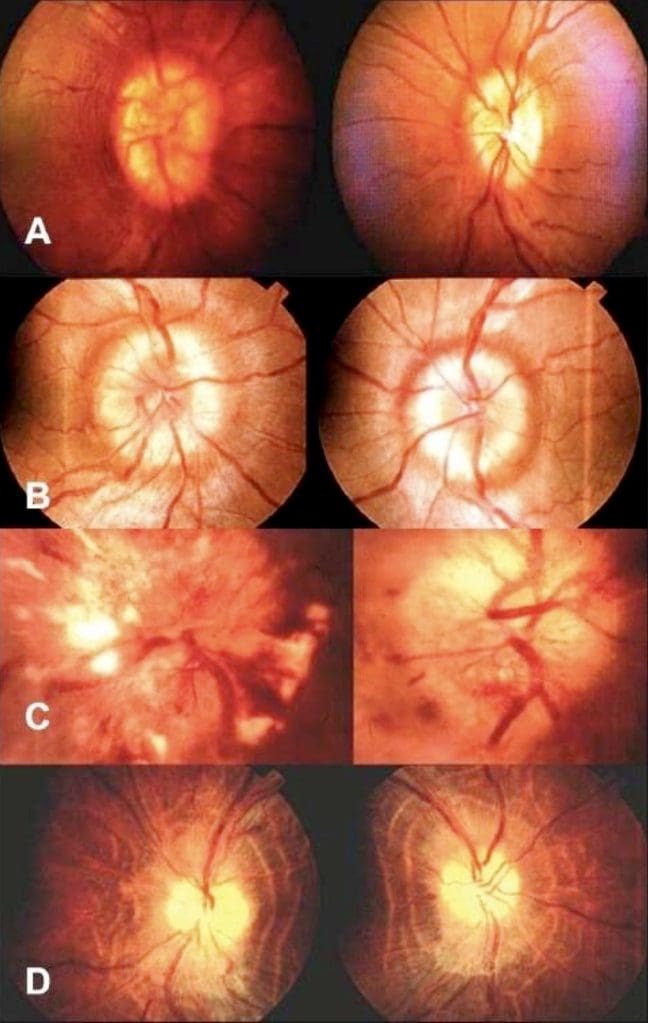
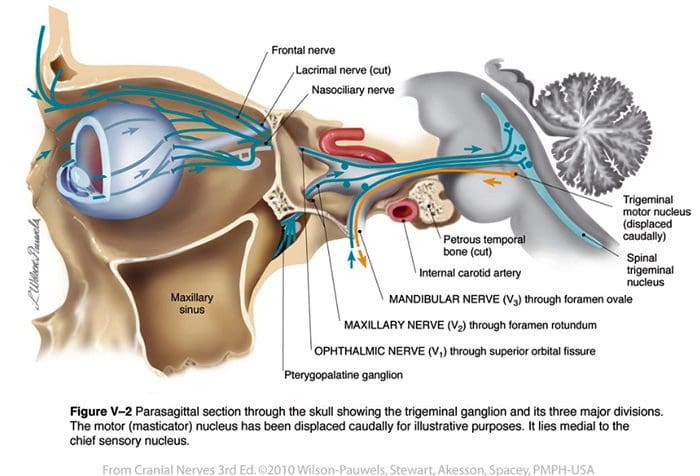










 Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.












