Approximately 8 out of 10 people living in the United States will experience back pain at least once throughout their lifetime. Fortunately, many healthcare professionals, including chiropractors and physical therapists, are qualified and experienced in the treatment of back pain. Because symptoms of back pain may occur due to a variety of health issues, however, properly diagnosing the source of an individual’s back pain in order to treat them accordingly may often be difficult.
Chiropractic care is a well-known, alternative treatment option commonly utilized to diagnose, treat and prevent a variety of injuries and/or conditions associated with the musculoskeletal and nervous system. A chiropractor, or doctor of chiropractic, will carefully use spinal adjustments and manual manipulations, among other treatment methods, to safely and effectively correct any spinal misalignment, or subluxation, found along the length of the spine which may be causing symptoms of back pain. By restoring the original alignment of the spine, a chiropractor can improve the function of the spine, allowing the human body to naturally heal itself without the need for invasive procedures and/or the use of drugs and/or medications.
Chiropractic care can improve a patient’s ability to better manage their back pain symptoms because it can help reduce pain and discomfort, decreases inflammation, and improves strength, mobility, and flexibility. Furthermore, a chiropractor may recommend lifestyle modifications, including nutritional changes and fitness advice, to speed up the patient’s recovery process. However, before seeking any type of treatment for your specific symptoms of back pain, it’s essential to understand the different types of back pain, its symptoms and its causes as well as what you can expect from a doctor visit for back pain.
Upper, Mid Back, Low and Lower Back
Back pain is one of the most common complaints frequently reported in doctor office visits on a regular basis. As a matter of fact, back pain has been identified to affect approximately three in four adults at least once through their lifetime. When referring to “back pain” healthcare professionals utilize the term loosely to medically define it as pain which originates anywhere between the upper back, or the cervical spine, and the lower back, or the lumbar spine, regardless of the cause of the symptoms.
Other Symptoms Associated with Back Pain
Back pain can also be characterized by different types of pain. Acute back pain is identified as short-term but severe in nature. Chronic back pain is long-term and may vary in intensity. It can often be severe, but it may also be identified as mild, deep, achy, burning, or electric-like in nature. Back pain which radiates into another part of the body, including the upper and/or lower extremities, is identified as radicular pain, particularly when it radiates below the knee, into the feet. This type of back pain is commonly known as lumbar radiculopathy. Fortunately, not all types of back pain include radiating pain symptoms.
It is not uncommon for back pain to cause other symptoms, such as numbness and tingling sensations, stiffness, achiness, and weakness. Furthermore, specific activities are known to aggravate existing back pain symptoms. Everyday activities like sitting, walking, standing, bending over, and twisting at the waist are several movements which can make back pain worse. However, not every patient will experience every symptoms associated with their specific type of back pain. Symptoms of back pain generally depend on the diagnosis, level of the injury and/or condition affecting the spine, or cause of back pain.
Dr. Alex Jimenez’s Insight
Back pain is a common symptom which affects about 80 percent of the population at least once throughout their lifetime. Because a variety of injuries and/or conditions may be the cause of back pain symptoms, many healthcare professionals consider the diagnosis of back pain to be difficult, however, back pain specialists, including chiropractors and physical therapists, can safely and effectively diagnose the source of an individual’s back pain symptoms. As a chiropractor, the use of spinal adjustments and manual manipulations can help naturally restore the original structure and function of the spine, without the need for drugs and/or medications or surgical interventions.
Understanding Back Pain Doctor Terms
When you visit a doctor regarding your symptoms, they may often use terms such as thoracic, lumbar, lumbosacral, or sacrum to describe your type of back pain. Back pain can originate anywhere along the spine, therefore, a healthcare professional will use the following terms to describe the source of the patient’s symptoms. The different regions of the spine are explained below.
The cervical spine refers to your neck.
The thoracic spine is found along the upper and middle regions of the back and where your ribs attach to the spinal column.
The lumbar spine refers to your low back.
The lumbosacral is found along the low back, sacrum, and the tailbone, also referred to as the coccyx.
The sacrum�refers to the part of the spine that is at the back of your pelvis.
Back pain can be challenging to properly diagnose because the spine consists of 17 vertebral bones, from the upper back to the tailbone, many joints, the sacrum and tailbone. In addition, the spine is made up of other fibrous and muscular supporting structures, intervertebral discs, the spinal cord and nerve roots, as well as blood vessels. Trauma from an injury, such as a back sprain/strain from lifting and twisting simultaneously, can cause immediate and severe back pain which may often become debilitating if left untreated.
Not all cases of back pain are due to trauma from an injury. Many other spinal health issues are congenital, meaning they developed since birth, degenerative or associated with age, due to disease, and they may even be connected to poor posture, obesity or the result of an unhealthy lifestyle habit, such as smoking. In other cases, the back pain may be worse than the severity of the injury and/or conditions causing it, which raises the question, �When should I seek medical attention for back pain?� If you are experiencing symptoms of back pain, among others commonly associated with spine health issues, you should seek immediate medical attentions if:
You cannot stand upright;
Fever accompanies pain;
Loss of bladder or bowel function or control occurs;
Leg pain and/or weakness progressively worsens; or if
Pain is relentless or worsens.
It’s normal for patients with back pain to feel afraid and anxious about seeking medical attention for their symptoms. Most individuals who experience severe and debilitating back pain will intuitively known when it’s time to receive the proper health care they need for their spinal health issues. Many healthcare professionals, such as chiropractors and physical therapists, are qualified and experienced back pain specialists who will help safely and effectively treat your specific back pain.
What to Expect from a Back Pain Specialist
Whether your doctor office visit is due to the urgent symptoms above or if you’re simply seeking immediate medical attention to prevent worsening back pain, below is a list of what you can expect in a back pain specialist visit. In order to properly diagnose the source of the patient’s back pain symptoms, a healthcare professional will first:
Review your medical history, including that of immediate family members who also have spinal health issues. Some instances of back pain, like scoliosis and osteoporosis, have a genetic potential.
Discuss when back pain started, what you were doing when the symptoms started, current severity and characteristics of your back pain as well as how these may have changed since they began, among other questions. Your doctor wants to learn as much about your pain and discomfort before they evaluate you accordingly�while the exam may be uncomfortable at first, your doctor doesn�t want to make the process intolerable.
Physical examination�to evaluate your vital signs, including heart rate. Blood pressure levels may become elevated as a result of pain. The doctor will examine your spine, feeling for abnormalities and areas of tenderness.
Neurological examination involves assessing sensation and function. The doctor may employ the pin prick test to determine if feeling is the same on both sides of particular parts of the body. Function, strength, mobility and flexibility are assessed while you walk, bend forward and backward (if able to), and during other movements. The doctor may also test your reflexes.
After a thorough examination, a healthcare professional should then be able to come up with a proper diagnosis for the patient’s back pain. To obtain more information and to help confirm the diagnosis, the doctor may order an X-ray, CT scan, or MRI. Sometimes lab tests may be ordered as well. It’s essential to keep in mind that an accurate diagnosis is essential towards a well-developed treatment plan. Once a proper diagnosis has been established, a healthcare professional will begin treatment accordingly, utilizing the recommended treatment methods for the patient’s specific cause of their back pain. Furthermore, a doctor may also be able to advice the patient regarding the best treatment methods to prevent further back pain.
In conclusion, back pain is a�common�symptoms which affects a majority of the population in the United States on a regular basis. Understanding the different types of back pain, its symptoms and its causes is essential towards receiving the right treatment from a qualified and experienced healthcare professional. Several procedures can be expected in a doctor office visit for back pain. Chiropractic care is a popular, alternative treatment option commonly utilized to help treat back pain and other injuries and/or conditions associated with the musculoskeletal and nervous system. A chiropractor, or doctor of chiropractic, will utilize spinal adjustments and manual manipulations to carefully restore the natural integrity of the spine, reducing symptoms of back pain. The overview above can help patient’s understand the process they must undergo in order to find relief from their back pain.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
According to statistics, approximately 80% of people will experience symptoms of back pain at least once throughout their lifetimes. Back pain is a common complaint which can result due to a variety of injuries and/or conditions. Often times, the natural degeneration of the spine with age can cause back pain. Herniated discs occur when the soft, gel-like center of an intervertebral disc pushes through a tear in its surrounding, outer ring of cartilage, compressing and irritating the nerve roots. Disc herniations most commonly occur along the lower back, or lumbar spine, but they may also occur along the cervical spine, or neck. The impingement of the nerves found in the low back due to injury and/or an aggravated condition can lead to symptoms of sciatica.
Low back pain represents one of the most common complaints in healthcare settings. While various injuries and conditions associated with the musculoskeletal and nervous system can cause low back pain, many healthcare professionals believe that work injury may have a prevalent connection to low back pain. For instance, improper posture and repetitive movements may often cause work-related injuries. In other cases, environmental accidents at work may cause work injuries. In any case, diagnosing the source of a patient’s low back pain to correctly determine which would be the best treatment method to restore the individual’s original health and wellness is generally challenging.
First and foremost, getting the right doctors for your specific source of low back pain is essential for finding relief from your symptoms. Many healthcare professionals are qualified and experienced in treating work-related low back pain, including doctors of chiropractic or chiropractors. As a result, several work injury treatment guidelines have been established to manage low back pain in healthcare settings. Chiropractic care focuses on diagnosing, treating, and preventing various injuries and conditions, such as LBP, associated with the musculoskeletal and nervous system. By carefully correcting the misalignment of the spine, chiropractic care can help improve symptoms of low back pain, among other symptoms. The purpose of the following article is to discuss occupational health guidelines for the management of low back pain.
Occupational Health Guidelines for the Management of Low Back Pain: an International Comparison
Abstract
Background: The enormous socioeconomic burden of low back pain emphasizes the need to manage this problem, especially in an occupational context effectively. To address this, occupational guidelines have been issued in various countries.
Aims: To compare available international guidelines for managing low back pain in an occupational health care setting.
Methods: The guidelines were compared regarding generally accepted quality criteria using the AGREE instrument and also summarised regarding the guideline committee, the presentation, the target group, and assessment and management recommendations (that is, advice, return to work strategy, and treatment).
Results and Conclusions: The results show that the guidelines variously met the quality criteria. Common flaws concerned the absence of proper external reviewing in the development process, lack of attention to organizational barriers and cost implications, and lack of information on the extent to which editors and developers were independent. There was general agreement on numerous issues fundamental to occupational health management of back pain. The assessment recommendations included diagnostic triage, screening for red flags and neurological problems, and identifying potential psychosocial and workplace barriers to recovery. The guidelines also agreed on advice that low back pain is a self-limiting condition and that remaining at work or an early (gradual) return to work, if necessary with modified duties, should be encouraged and supported.
Dr. Alex Jimenez’s Insight
Low back pain is one of the most prevalent health issues treated in chiropractic offices. Although the following article describes low back pain as a self limiting condition, the cause of an individual’s LBP can also trigger debilitating and severe pain and discomfort of left untreated. It’s important for an individual with symptoms of low back pain to seek proper treatment with a chiropractor to properly diagnose and treat their health issues as well as prevent them from returning in the future. Patients who experience low back pain for more than 3 months are less than 3 percent likely to return to work. Chiropractic care is a safe and effective alternative treatment option which can help restore the original function of the spine. Furthermore, a doctor of chiropractic, or chiropractor, can provide lifestyle modifications, such as nutritional and fitness advice, to speed up the patient’s recovery process. Healing through movement is essential for LBP recovery.
Low back pain (LBP) is one of the industrial countries’ most common health problems. Despite its benign nature and sound course, LBP is commonly associated with incapacity, productivity loss due to sick leave, and high societal costs.[1]
Because of that impact, there is an obvious need for effective management strategies based on scientific evidence derived from studies of sound methodological quality. Usually, these are randomized controlled trials (RCTs) on the effectiveness of therapeutic interventions, diagnostic studies, or prospective observational studies on risk factors or side effects. The scientific evidence, summarised in systematic reviews and meta-analyses, provides a solid basis for guidelines on managing LBP. In a previous paper, Koes et al. compared various existing clinical guidelines for managing LBP targeted at primary healthcare professionals, showing a considerable commonality.[2]
The problems in occupational health care are different. Management focuses mainly on counseling the worker with LBP and addressing the issues of assisting them to continue working or return to work (RTW) after sick listing. However, LBP is also an important issue in occupational health care because of the associated incapacity for work, productivity loss, and sick leave. Several guidelines, or sections of guidelines, have now been published dealing with the specific issues of management in an occupational health care setting. Since the evidence is international, it would be expected that the recommendations of different occupational guidelines for LBP would be more or less similar. However, it is not clear whether the guidelines meet currently accepted quality criteria.
This paper critically appraises available occupational guidelines on managing LBP and compares their assessment and management recommendations.
Main Messages
In various countries, occupational health guidelines are issued to improve the management of low back pain in an occupational context.
Common flaws of these guidelines concern the absence of proper external reviewing in the development process, lack of attention to organizational barriers and cost implications, and lack of information on the independence of editors and developers.
In general, the assessment recommendations in the guidelines consisted of diagnostic triage, screening for red flags and neurological problems, and identifying potential psychosocial and workplace barriers to recovery.
There is general agreement on advice that low back pain is a self-limiting condition and that remaining at work or an early (gradual) return to work, if necessary with modified duties, should be encouraged and supported.
Methods
Guidelines on the occupational health management of LBP were retrieved from the authors’ personal files. Retrieval was checked by a Medline search using the keywords low back pain, guidelines, and occupational up to October 2001, and personal communication with experts in the field. Policies had to meet the following inclusion criteria:
Guidelines aimed at managing workers with LBP (in occupational health care settings or addressing occupational issues) or separate sections of policies that dealt with these topics.
Guidelines are available in English or Dutch (or translated into these languages).
The exclusion criteria were:
Guidelines on primary prevention (that is, prevention before the onset of the symptoms) of work-related LBP (for example, lifting instructions for workers).
Clinical guidelines for the management of LBP in primary care.[2]
The quality of the included guidelines was appraised using the AGREE instrument, a generic tool designed primarily to help guideline developers and users assess the methodological quality of clinical practice guidelines.[3]
The AGREE instrument provides a framework for assessing the quality on 24 items (table 1), each rated on a four-point scale. The full operationalization is available on www.agreecollaboration.org.
Two reviewers (BS and HH) independently rated the quality of the guidelines and then met to discuss disagreements and to reach a consensus on the ratings. When they could not agree, a third reviewer (MvT) reconciled the remaining differences and decided on the ratings. To facilitate analysis in this review, ratings were transformed into dichotomous variables of whether each quality item was or was not met.
The assessment recommendations were summarised and compared to recommendations on advice, treatment, and return to work strategies. The selected guidelines were further characterized and reached regarding the guideline committee, the presentation of the procedure, the target group, and the extent to which the recommendations were based on available scientific evidence. All of this information was extracted directly from the published guidelines.
Policy Implications
The management of low back pain in occupational health care should follow evidence-based guidelines.
Future occupational guidelines for managing low back pain and updates of those guidelines should consider the criteria for proper development, implementation, and evaluation of approaches as suggested by the AGREE collaboration.
Results
Selection of Studies
Our search found ten guidelines, but four were excluded because they dealt with the management of LBP in primary care,[15] were aimed at the guidance of sick-listed employees in general (not specifically LBP),[16] were intended for the primary prevention of LBP at work,[17] or were not available in English or Dutch.[18] The final selection, therefore, consisted of the following six guidelines, listed by date of issue:
(1) Canada (Quebec). A scientific approach to the assessment and management of activity-related spinal disorders. A monograph for clinicians. Report of the Quebec Task Force on Spinal Disorders. Quebec Canada (1987).[4]
(2) Australia (Victoria). Guidelines for the management of employees with compensable low back pain. Victorian WorkCover Authority, Australia (1996).[5] (This is a revised version of guidelines developed by the South Australian WorkCover Corporation in October 1993.)
(3) the USA. Occupational Medicine Practice Guidelines. American College of Occupational and Environmental Medicine. USA (1997).[6]
(4) New Zealand
(a)Active and working! Managing acute low back pain in the workplace. Accident Compensation Corporation and National Health Committee. New Zealand (2000).[7]
(b)Patient guide to acute low back pain management. Accident Compensation Corporation and National Health Committee. New Zealand (1998).[8]
(c) Assess psychosocial yellow flags in acute low back pain. Accident Compensation Corporation and National Health Committee. New Zealand (1997).[9]
(5) the Netherlands. Dutch guideline for managing occupational physicians of employees with low back pain. Dutch Association of Occupational Medicine (NVAB). Netherlands (1999).[10]
(6) the UK
(a)Occupational health guidelines for managing low back pain at work principal recommendations. Faculty of Occupational Medicine. UK (2000).[11]
(b)Occupational health guidelines for managing low back pain at work leaflet for practitioners. Faculty of Occupational Medicine. UK (2000).[12]
(c)Occupational health guidelines for managing low back pain at work evidence review. Faculty of Occupational Medicine. UK (2000).[13]
(d)The Back Book, The Stationery Office. UK (1996).[14]
Two guidelines (4 and 6) could not be evaluated independently from additional documents to which they refer (4bc, 6bd), so these documents were also included in the review.
Appraisal of the Quality of the Guidelines
Initially, there was an agreement between the two reviewers regarding 106 (77%) of the 138 item ratings. After two meetings, the consensus was reached for all but four items, which required adjudication by the third reviewer. Table 1 presents the final ratings.
All included guidelines presented the different options for managing LBP in occupational health. In five of the six policies, the overall objectives of the procedure were explicitly described,[46, 1014] the target users of the system were clearly defined,[514] easily identifiable key recommendations were included,[4, 614] or critical review criteria were presented for monitoring and audit purposes.[49, 1114]
The results of the AGREE appraisal showed that none of the guidelines paid sufficient attention to potential organizational barriers and cost implications in implementing the recommendations. It was also unclear for all included guidelines whether or not they were editorially independent of the funding body and whether or not there were conflicts of interest for the members of the guideline development committees. Furthermore, it was unclear for all guidelines whether experts had externally reviewed the policies before publication. Only the UK guideline clearly described the method used to formulate the recommendations and provided for updating the approach.[11]
Development of the Guidelines
Table 2 presents background information on the development process of the guidelines.
The target users for the guidelines were physicians and other healthcare providers in the field of occupational healthcare. Several policies were also directed at informing employers, workers [68, 11, 14], or members of organizations interested in occupational health.[4] The Dutch guideline was only targeted at the occupational health physician.[10]
The guideline committees responsible for developing the guidelines were generally multidisciplinary, including disciplines like epidemiology, ergonomics, physiotherapy, general practice, occupational medicine, occupational therapy, orthopedics, and representatives of employers’ associations and trade unions. Chiropractic and osteopathic representatives were in the guideline committee of the New Zealand guidelines.[79] The Quebec task force (Canada) also included representatives of rehabilitation medicine, rheumatology, health economics, law, neurosurgery, biomechanical engineering, and library sciences. In contrast, the guideline committee of the Dutch guideline consisted only of occupational physicians.[10]
The guidelines were issued as a separate document,[4, 5, 10] as a chapter in a textbook,[6] or as several interrelated documents.[79, 1114]
The UK,[13] the USA,[6] and Canadian[4] guidelines provided information on the search strategy applied to the identification of relevant literature and the weighing of the evidence. On the other hand, the Dutch[10] and the Australian[5] guidelines supported their recommendations only by references. The New Zealand guidelines showed no direct links between suggestions and concerns [79]. The reader was referred to other literature for background information.
Patient Population and Diagnostic Recommendations
Although all guidelines focused on workers with LBP, it was often unclear whether they dealt with acute or chronic LBP or both. Acute and chronic LBP were often not defined, and cut-off points were given (for example, <3 months). It was usually unclear whether these referred to the onset of symptoms or absence from work. However, the Canadian guideline introduced a classification system (acute/subacute/ chronic) based on the distribution of claims of spinal disorders by time since absence from work.[4]
All guidelines distinguished specific and non-specific LBP. Specific LBP concerns the potentially serious red flag conditions like fractures, tumors, or infections, and the Dutch and UK guidelines also distinguish the radicular syndrome or nerve root pain.[1013] All procedures were consistent in their recommendations to take a clinical history and to carry out a physical examination, including neurological screening. In cases of suspected specific pathology (red flags), x-ray examinations were recommended by most guidelines. In addition, New Zealand and the US guideline also recommended an x-ray examination when symptoms did not improve after four weeks.[6, 9] The UK guideline stated that x-ray examinations are not indicated and do not assist occupational health management of the patient with LBP (distinct from any clinical indications).[1113]
Most guidelines considered psychosocial factors as yellow flags as obstacles to recovery that healthcare providers should address. The New Zealand[9] and UK guidelines [11, 12] explicitly listed factors and suggested questions to identify those psychosocial yellow flags.
All guidelines addressed the importance of the clinical history identifying physical and psychosocial workplace factors relevant to LBP, including physical demands of work (manual handling, lifting, bending, twisting, and exposure to whole-body vibration), accidents or injuries, and perceived difficulties in returning to work or relationships at work. The Dutch and the Canadian guidelines contained recommendations to carry out a workplace investigation[10] or an assessment of occupational skills when necessary.[4]
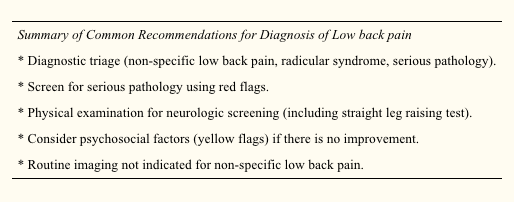
Summary of Recommendations for the Assessment of LBP
Diagnostic triage (non-specific LBP, radicular syndrome, specific LBP).
Exclude red flags and neurological screening.
Identify psychosocial factors and potential obstacles to recovery.
Identify workplace factors (physical and psychosocial) that may be related to the LBP problem and return to work.
X-Ray examinations are restricted to suspected cases of specific pathology.
Recommendations Regarding Information and Advice, Treatment, and Return to Work Strategies
Most guidelines recommended reassuring the employee and providing information about LBP’s self-limiting nature and good prognosis. Encouragement of return to ordinary activity as generally as possible was frequently advised.
In line with the recommendation to return to regular activity, all guidelines also stressed the importance of returning to work as rapidly as possible, even if there is still some LBP and, if necessary, starting with modified duties in more severe cases. Work duties could then be increased gradually (hours and tasks) until total return to work was reached. The US and Dutch guidelines provided detailed time schedules for return to work. The Dutch approach proposed a return to work within two weeks with an adaptation of duties when necessary.[10] The Dutch system also stressed the importance of time-contingent management about a return to work.[10] The US guideline proposed every attempt to maintain the patient at maximal levels of activity, including work activities; targets for disability duration in terms of return to work were given as 02 days with modified duties and 714 days if modified duties are not used/available.[6] In contrast to the others, the Canadian guideline advised return to work only when symptoms and functional restrictions had improved.[4]
The most frequently recommended treatment options in all the included guidelines were: medication for pain relief,[5, 7, 8] gradually progressive exercise programs,[6, 10] and multidisciplinary rehabilitation.[1013] The US guideline recommended referral within two weeks to an exercise program consisting of aerobic exercises, conditioning exercises for trunk muscles, and exercise quota.[6] The Dutch guideline recommended that if there is no progress within two weeks of work absence, workers should be referred to a graded activity program (gradually increasing exercises) and, if there is no improvement by four weeks, to a multidisciplinary rehabilitation program.[10] The UK guideline recommended that workers who have difficulty returning to regular occupational duties by 412 weeks should be referred to an active rehabilitation program. This rehabilitation program should include education, reassurance and advice, a progressive vigorous exercise and fitness program, and pain management according to behavioral principles; it should be embedded in an occupational setting and directed firmly toward a return to work.[11-13] Extensive lists of possible treatment options were presented in the guidelines of Canada and Australia [4, 5], although most of these were not based on scientific evidence.
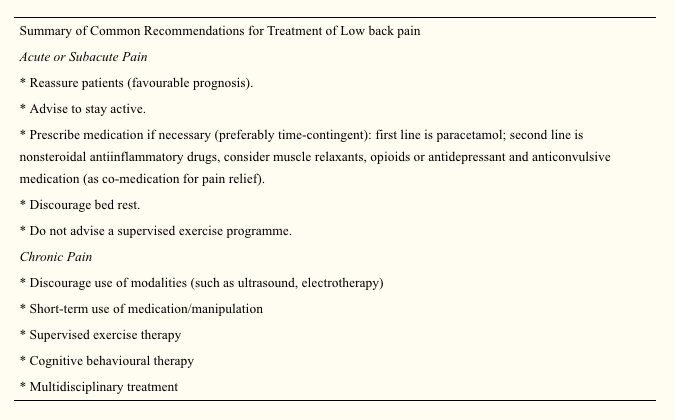
Summary of Recommendations Regarding Information, Advice, Return to Work Measures, and Treatment in Workers with LBP
Reassure the worker and provide adequate information about LBP’s self-limiting nature and good prognosis.
Advise the worker to continue ordinary activities or to return to regular exercise and work as soon as possible, even if there is still some pain.
Most workers with LBP return to more or less regular duties quite rapidly. Consider temporary adaptations of work duties (hours/tasks) only when necessary.
When a worker fails to return to work within 212 weeks (there is considerable variation in the time scale in different guidelines), refer them to a gradually increasing exercise program, or multidisciplinary rehabilitation (exercises, education, reassurance, and pain management following behavioral principles). These rehabilitation programs should be embedded in an occupational setting.
Discussion
The management of LBP in an occupational health setting must address the relation between low back complaints and work and develop strategies aimed at a safe return to work. This review compared available occupational health guidelines from various countries. Policies are rarely indexed in Medline, so when searching for guidelines, we had to rely primarily on personal files and personal communication.
Quality Aspects and Development Process of the Guidelines
The assessment by the AGREE instrument[3] showed some differences in the quality of the guidelines reviewed, which may partly reflect the variation in the dates of development and publication of the guidelines. The Canadian guideline, for example, was published in 1987 and the Australian guideline in 1996.[4, 5] The other guidelines were more recent and incorporated a more extensive evidence base and more up to date guideline methodology.
Several common flaws related to the development process of the guidelines were shown by the assessment by the AGREE instrument. Firstly, it is important to make clear whether a guideline is editorially independent from the funding body, and whether there are conflicts of interest for the members of the guideline committee. None of the included guidelines clearly reported these issues. Further, reported external review of the guideline by clinical and methodological experts prior to publication was also lacking in all guidelines included in this review.
Several guidelines provided comprehensive information on the way relevant literature was searched and translated into recommendations.[4, 6, 11, 13] Other guidelines supported their recommendations by references,[5, 7, 9, 10] but this does not permit assessment of the robustness of the guidelines or their recommendations.
Guidelines depend on the scientific evidence, which changes over time, and it is striking that only one guideline provided for future update.[11, 12] Possibly there are updates planned for the other guidelines but they are not explicitly stated (and conversely stating there will be future update does not mean it will actually occur). This lack of reporting may also hold true for other AGREE criteria that we rated negatively. The use of the AGREE framework as a guide for both the development and the reporting of guidelines should help to improve the quality of future guidelines.
Assessment and Management of LBP
The diagnostic procedures recommended in the occupational health guidelines were largely similar to the recommendations of clinical guidelines,[2] and, logically, the main difference was the emphasis on addressing occupational issues. The reported methods for addressing workplace factors in the assessment of LBP of the individual worker concerned the identification of difficult tasks, risk factors, and obstacles for return to work by occupational histories. Obviously, these obstacles for return to work not only concern physical load factors, but also work related psychosocial problems regarding responsibilities, cooperation with co-workers, and the social atmosphere at the workplace.[10] Screening for work related psychosocial yellow flags may help to identify those workers who are at risk for chronic pain and disability.[1113]
A potentially important feature of the guidelines is that they were consistent regarding their recommendations to reassure the employee with LBP, and to encourage and support return to work even with some persisting symptoms. There is general consensus that most workers do not have to wait until they are completely free of pain before returning to work. The lists of treatment options provided by the Canadian and Australian guidelines may reflect the lack of evidence at that time,[4, 5] leaving users of the guidelines to choose for themselves. It is, however, questionable whether such lists really contribute to improved care, and in our view guideline recommendations should be based on sound scientific evidence.
The US, Dutch, and UK occupational guidelines[6, 1013] recommend that active multidisciplinary treatment is the most promising intervention for return to work, and this is supported by strong evidence from RCTs.[19, 20] However, more research is still needed to identify the optimum content and intensity of those treatment packages.[13, 21]
Despite some evidence for a contribution of workplace factors in the aetiology of LBP,[22] systematic approaches for workplace adaptations are lacking, and are not offered as recommendations in the guidelines. Perhaps this represents a lack of confidence in the evidence on the overall impact of workplace factors, a difficulty of translation into practical guidance, or because these issues are confounded with local legislation (which was hinted at in the UK guideline[11]). It may be that the participatory ergonomics intervention, which proposes consultations with the worker, the employer, and an ergonomist, will turn out to be a useful return to work intervention.[23, 24] The potential value of getting all the players onside[25] was stressed in the Dutch and the UK guidelines,[1113] but further evaluation of this approach and its implementation is required.
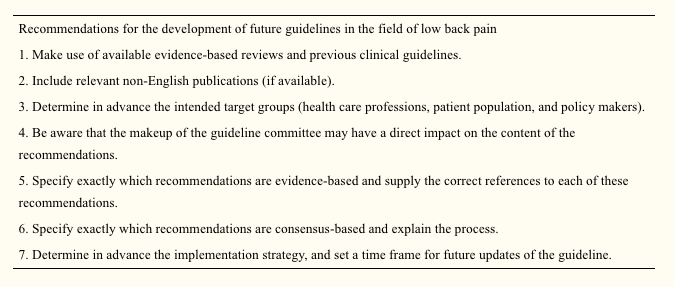
Development of Future Guidelines in Occupational Health Care
The purpose of this review was to give both an overview and a critical appraisal of occupational guidelines for the management of LBP. The critical appraisal of the guidelines is meant to help direct future development and planned updates of guide- lines. In the still emerging field of guideline methodology we consider all past initiatives as laudable; we recognise the need for clinical guidance, and appreciate that guidelines developers cannot wait for research to provide all the methodology and evidence required. However, there is room for improvement and future guidelines and updates should consider the criteria for proper development, implementation, and evaluation of guidelines as suggested by the AGREE collaboration.
The implementation of the guidelines is beyond the scope of this review, but it was noted that none of the guideline documents specifically described implementation strategies, so it is uncertain to what extent the target groups may have been reached, and what effects that may have had. This may be a fruitful area for further research.
The very existence of these occupational health guidelines shows that existing primary care clinical guidelines for LBP2 are considered inappropriate or insufficient for occupational health care. There is a clear perception internationally that the needs of the worker experiencing back pain are intrinsically linked to a variety of occupational issues not covered by usual primary care guidance and, consequently, practice. What emerges is that, despite the methodological flaws, considerable agreement is evident on a range of fundamental occupational health strategies for managing the worker with back pain, some of which are innovative and challenge previously held views. There is agreement on the fundamental message that prolonged work loss is detrimental, and that early work return should be encouraged and facilitated; there is no need to wait for complete symptom resolution. Although the recommended strategies vary somewhat, there is considerable agreement on the value of positive reassurance and advice, availability of (temporary) modified work, addressing workplace factors (getting all the players onside), and rehabilitation for workers having difficulty returning to work.
Acknowledgements
This study was supported by the Dutch Health Care Insurance Council (CVZ), grant DPZ no. 169/0, Amstelveen, Netherlands. J B Staal is currently working at the Department of Epidemiology, Maastricht University, PO Box 616 6200 MD Maastricht, Netherlands. W van Mechelen is also part of the Research Centre on Physical Activity, Work and Health, Body@work TNO-VUmc.
In conclusion, symptoms of low back pain are one of the most common health issues associated with work injuries. Because of it, several occupational health guidelines have been established for the management of low back pain. Chiropractic care, among other treatment methods, may be utilized in order to help the patient find relief from their LBP. Furthermore, the article above demonstrated the safety and effectiveness of a variety of traditional as well as alternative treatment options in the diagnosis, treatment and prevention of a variety of low back pain cases. However, further research studies are required in order to properly determine the efficiency of each individual treatment method. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
According to statistics, approximately 80% of people will experience symptoms of back pain at least once throughout their lifetimes. Back pain is a common complaint which can result due to a variety of injuries and/or conditions. Often times, the natural degeneration of the spine with age can cause back pain. Herniated discs occur when the soft, gel-like center of an intervertebral disc pushes through a tear in its surrounding, outer ring of cartilage, compressing and irritating the nerve roots. Disc herniations most commonly occur along the lower back, or lumbar spine, but they may also occur along the cervical spine, or neck. The impingement of the nerves found in the low back due to injury and/or an aggravated condition can lead to symptoms of sciatica.
1. Van Tulder MW, Koes BW, Bouter LM. A cost-of-illness study of back pain in the Netherlands. Pain 1995;62:233�40.
2. Koes BW, van Tulder MW, Ostelo R, et al. Clinical guidelines for the management of low back pain in primary care: an international
comparison. Spine 2001;26:2504�14.
3. The AGREE Collaboration. Appraisal of Guidelines Research &
Evaluation Instrument, www.agreecollaboration.org.
4. Spitzer WO, Leblanc FE, Dupuis M. Scientific approach to the
assessment and management of activity-related spinal disorders. A monograph for clinicians. Report of the Quebec Task Force on Spinal Disorders. Spine 1987;12(suppl 7S):1�59.
5. Victorian WorkCover Authority. Guidelines for the management of employees with compensable low back pain. Melbourne: Victorian WorkCover Authority, 1996.
6. Harris JS. Occupational medicine practice guidelines. Beverly, MA: OEM Press, 1997.
7. Accident Compensation Corporation and National Health Committee. Active and working! Managing acute low back pain in the workplace. Wellington, New Zealand, 2000.
8. Accident Compensation Corporation and National Health Committee, Ministry of Health. Patient guide to acute low back pain management. Wellington, New Zealand, 1998.
9. Kendall, Linton SJ, Main CJ. Guide to assessing psychosocial yellow flags in acute low back pain. Risk factors for long-term disability and work loss. Wellington, New Zealand, Accident Rehabilitation & Compensation Insurance Corporation of New Zealand and the National Health Committee, 1997.
10. Nederlandse Vereniging voor Arbeids- en Bedrijfsgeneeskunde (Dutch Association of Occupational Medicine, NVAB). Handelen van de bedrijfsarts bij werknemers met lage-rugklachten. Richtlijnen voor Bedrijfsartsen. [Dutch guideline for the management of occupational physicians of employees with low back pain]. April 1999.
11. Carter JT, Birell LN. Occupational health guidelines for the management of low back pain at work�principal recommendations. London: Faculty of Occupational Medicine, 2000 (www.facoccmed.ac.uk).
12. Occupational health guidelines for the management of low back pain at work�leaflet for practitioners. London: Faculty of Occupational Medicine, 2000 (www.facoccmed.ac.uk).
13. Waddell G, Burton AK. Occupational health guidelines for the management of low back pain at work�evidence review. Occup Med 2001;51:124�35.
14. Roland M, et al. The back book. Norwich: The Stationery Office, 1996.
15. ICSI. Health care guideline. Adult low back pain. Institute for Clinical Systems Integration, 1998 (www.icsi.org/guide/).
16. Kazimirski JC. CMA policy summary: The physician�s role in helping patients return to work after an illness or injury. CMAJ 1997;156:680A�680C.
17. Yamamoto S. Guidelines on worksite prevention of low back pain. Labour standards bureau notification, No. 57. Industrial Health 1997;35:143�72.
18. INSERM. Les Lombalgies en milieu professionel: quel facteurs de risque et quelle prevention? [Low back pain at the workplace: risk factors and prevention]. Paris: les editions INSERM, Synthese bibliographique realise a la demande de la CANAM, 2000.
19. Lindstro?m I, Ohlund C, Eek C, et al. The effect of graded activity on patients with subacute low back pain: a randomised prospective clinical study with an operant-conditioning behavioural approach. Physical Therapy 1992;72:279�93.
20. Karjalainen K, Malmivaara A, van Tulder M, et al. Multidisciplinary biopsychosocial rehabilitation for subacute low back pain in working-age adults: a systematic review within the framework of the Cochrane Collaboration Back Review Group. Spine 2001;26:262�9.
21. Staal JB, Hlobil H, van Tulder MW, et al. Return-to-work interventions for low back pain: a descriptive review of contents and concepts of working mechanisms. Sports Med 2002;32:251�67.
22. Hoogendoorn WE, van Poppel MN, Bongers PM, et al. Physical load during work and leisure time as risk factors for back pain. Scand J Work Environ Health 1999;25:387�403.
23. Loisel P, Gosselin L, Durand P, et al. A population-based, randomised clinical trial on back pain management. Spine 1997;22:2911�18.
24. Loisel P, Gosselin L, Durand P, et al. Implementation of a participatory ergonomics program in the rehabilitation of workers suffering from subacute back pain. Appl Ergon 2001;32:53�60.
25. Frank J, Sinclair S, Hogg-Johnson S, et al. Preventing disability from work-related low-back pain. New evidence gives new hope�if we can just get all the players onside. CMAJ 1998;158:1625�31.
Chronic Pain Treatment: Sandra Rubio has worked with Dr. Alex Jimenez for about 6 years, providing health care services to patients at Dr. Jimenez’s clinic. As a result, Sandra has learned and witnessed how many health benefits chiropractic care can provide for patients who begin treatment with Dr. Alex Jimenez. Although chiropractic care may sometimes require more than a single treatment session as well as regular maintenance to completely improve the patient’s symptoms, Dr. Alex Jimenez offers positive, trustworthy, safe and effective non-invasive alternative treatment options without the use of drugs and/or medications and he also makes sure to educate patients thoroughly regarding their specific health issue. Sandra Rubio discusses how essential it is for people with chronic pain to first seek chiropractic care with Dr. Alex Jimenez as the non-surgical choice for their injuries and/or conditions in order for them to achieve overall health and wellness.
Chronic Pain Treatment
Chronic pain is medically defined as pain which lasts for an extended amount of time. The distinction between acute and chronic pain is sometimes determined by an arbitrary interval of time since onset; the two most commonly used markers being 3 months and 6 months since onset, although many healthcare professionals have established the transition from acute to chronic pain at 12 months. Other healthcare specialists and researchers apply the definition of acute pain symptoms to pain that lasts less than 30 days, while the definition of chronic pain symptoms to pain that lasts more than six months. Subacute pain is medically defined as pain that lasts from one to six months. Chronic pain may originate anywhere in the body, such as in the case of chronic back pain, or it may originate in the brain or spinal cord, such as in the case of fibromyalgia. While chronic pain is considered difficult to treat, many healthcare professionals, including chiropractors, can effectively improve chronic pain.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
Thank You & God Bless.
Dr. Alex Jimenez DC, C.C.S.T
According to the American Chiropractic Association, approximately 31 million people in the United States experience low back pain throughout their lifetime. Low back pain can occur due to a variety of injuries and/or conditions and it can range in severity. Trauma from an injury or an aggravated condition can cause symptoms ranging from mild and annoying to intense and debilitating. The most common type of low back pain is described as a dull, achy, burning or spasming sensation.
Diagnosing the source of a patient’s low back pain can be challenging, however, several healthcare professionals are qualified and experienced in the treatment of spinal health issues, including chiropractors and physical therapists. As a matter of fact, new guidelines from the American Medical Association, or the AMA, have suggested that people affected with low back pain should seek chiropractic care before seeking treatment from conventional medical doctors because chiropractors primarily focus on the diagnosis, treatment and prevention of injuries and/or conditions affecting the musculoskeletal and nervous system.
Chiropractic care is a well-known alternative treatment option commonly utilized to treat injuries and/or conditions causing low back pain. Regular chiropractic care can provide safe and effective, non-invasive treatment without the need to utilize drugs and/or medications. A chiropractor, or doctor of chiropractic, will commonly use spinal adjustments and manual manipulations to carefully correct any spinal misalignment, or subluxation, along the lumbar spine which may be causing symptoms of low back pain. Other treatment methods commonly utilized in chiropractic care include, hot or cold compresses, massage and physical therapy modalities like interferential therapy or transcutaneous electrical nerve stimulations, or TENS and spinal decompression therapy. A chiropractor may also offer nutritional advice and fitness plans to speed up the patient’s recovery process.
By restoring the original alignment of the spine, a chiropractor can help improve the function of the spine by reducing pain and discomfort, decreasing inflammation, and improving range of motion and flexibility as well as increasing strength. Chiropractic care allows the human body to naturally heal itself in order to better be able to manage symptoms associated with low back pain. Based on the diagnosis of a patient, a doctor of chiropractic may also refer patients to other healthcare professionals for further treatment. The purpose of the following article is to demonstrate an overview of updated clinical treatment guidelines for the proper management of non-specific low back pain in a primary care setting.
An Updated Overview of Clinical Guidelines for the Management of Non-Specific Low Back Pain in Primary Care
Abstract
The aim of this study was to present and compare the content of (inter)national clinical guidelines for the management of low back pain. To rationalise the management of low back pain, evidence-based clinical guidelines have been issued in many countries. Given that the available scientific evidence is the same, irrespective of the country, one would expect these guidelines to include more or less similar recommendations regarding diagnosis and treatment. We updated a previous review that included clinical guidelines published up to and including the year 2000. Guidelines were included that met the following criteria: the target group consisted mainly of primary health care professionals, and the guideline was published in English, German, Finnish, Spanish, Norwegian, or Dutch. Only one guideline per country was included: the one most recently published. This updated review includes national clinical guidelines from 13 countries and 2 international clinical guidelines from Europe published from 2000 until 2008. The content of the guidelines appeared to be quite similar regarding the diagnostic classification (diagnostic triage) and the use of diagnostic and therapeutic interventions. Consistent features for acute low back pain were the early and gradual activation of patients, the discouragement of prescribed bed rest and the recognition of psychosocial factors as risk factors for chronicity. For chronic low back pain, consistent features included supervised exercises, cognitive behavioural therapy and multidisciplinary treatment. However, there are some discrepancies for recommendations regarding spinal manipulation and drug treatment for acute and chronic low back pain. The comparison of international clinical guidelines for the management of low back pain showed that diagnostic and therapeutic recommendations are generally similar. There are also some differences which may be due to a lack of strong evidence regarding these topics or due to differences in local health care systems. The implementation of these clinical guidelines remains a challenge for clinical practice and research.
Keywords:Low back pain, Clinical guidelines, Review, Diagnosis, Treatment
Dr. Alex Jimenez’s Insight
Low back pain is one of the most common reasons for doctor office visits each year. In fact, about 80 percent of the population in the United States will suffer from back pain at least once throughout their lifetime. Regular chiropractic care can help prevent, treat and manage low back pain symptoms. Chiropractic care can provide many other benefits as well. Patient’s who have received chiropractic care for injuries and/or conditions affecting the musculoskeletal and nervous systems have experienced improvements to their digestive health and have reported better and deeper sleep after a visit to a chiropractor office. Furthermore, research studies have demonstrated that chiropractic care can help build your immune system. Chiropractic care has even been associated with stress management, reducing depression and anxiety levels. Chiropractic care can provide low back pain relief and improve overall health and wellness.
Introduction
Low back pain remains a condition with a relatively high incidence and prevalence. Following a new episode, the pain typically improves substantially but does not resolve completely during the first 4�6 weeks. In most people the pain and associated disability persist for months; however, only a small proportion remains severely disabled [1]. For those whose pain does resolve completely, recurrence during the next 12 months is not uncommon [2, 3].
There is a wide acceptance that the management of low back pain should begin in primary care. The challenge for primary care clinicians is that back pain is but one of many conditions that they manage. For example while back pain, in absolute numbers, is the eighth most common condition managed by Australian GPs, it only accounts for 1.8% of their case load [4]. To assist primary care practitioners to provide care that is aligned with the best evidence, clinical practice guidelines have been produced in many countries around the world.
The first low back pain guideline was published in 1987 by the Quebec Task Force with authors pointing to the absence of high-quality evidence to guide decision making [5]. Since that time there has been a strong growth in research addressing diagnosis and prognosis but especially research on therapy. As an example of this growth, at the time of the Spitzer guideline [5] there were only 108 randomised controlled trials evaluating physiotherapy treatments for low back pain but as at April 2009 there were 958.1 The Cochrane database (Central) currently lists more than 2500 controlled trials evaluating treatment for back and neck pain. The evidence from these trials for most interventions is summarised in systematic reviews and meta-analysis. The Cochrane Back Review Group, for example, has now published 32 systematic reviews of randomised controlled trials evaluating interventions for low back pain. In the near future, systematic reviews of studies evaluating diagnostic intervention for low back pain will also be included in the Cochrane Library.
This dramatic growth in research would be a comfort to those who were members of the original Quebec Task Force but perhaps a challenge to those who served on committees for later guidelines. With a large and ever increasing research base to inform guidelines two potential problems arise. The first and most obvious is that the recommendations in the guidelines may become out of date. The second is that with a wealth of information to consider, the various committees producing guidelines may produce quite different treatment recommendations. At the same time one can argue that if more precise and valid information becomes available recommendations will become more similar. A previous systematic review of clinical practice guidelines was conducted in 2001 [6]. In that review we assessed the available clinical guidelines from 11 countries and concluded that the guidelines provided generally similar recommendations regarding the diagnostic classification (diagnostic triage) and the use of diagnostic and therapeutic interventions. Consistent features were the early and gradual activation of patients, the discouragement of prescribed bed rest, and the recognition of psychosocial factors as risk factors for chronicity. However, there were discrepancies for recommendations regarding exercise therapy, spinal manipulation, muscle relaxants, and patient information.
Bouwmeester et al. [7] concluded recently that the quality of mono- and multidisciplinary clinical guidelines for the management of low back pain, as measured with the AGREE instrument has improved over time. The present article focuses on the actual content of national clinical guidelines on low back pain which have been issued since 2001. These guidelines are compared regarding the content of their recommendations, the target group, the guideline committee and its procedures, and the extent to which the recommendations were based on the available literature (the scientific evidence). We also highlight any changes in recommendations that have occurred over time in comparison with our previous review [6].
Methods
Clinical guidelines were searched using electronic databases covering the period 2000�2008: Medline (key words: low back pain, clinical guidelines), PEDro (key words: low back pain, practice guidelines, combined with AND), National Guideline Clearinghouse (www.guideline.gov; key word: low back pain), and National Institute for Health and Clinical Excellence (NICE) (www.nice.org.uk; key word: low back pain). Guidelines used in the previous review were checked for updates. We also checked the content and reference list of relevant reviews on guidelines, included a search on the Web of Science citation index for articles citing the previous review and asked experts in the field. To be included in this review, the guidelines had to meet the following criteria: (1) the guideline concerned the diagnosis and clinical management of low back pain, (2) the guideline was targeted at a multidisciplinary audience in the primary care setting, and (3) the guideline was available in English, German, Finnish, Spanish, Norwegian or Dutch because documents in these languages could be read by the reviewers. Only one guideline was included per country unless there were separate guidelines for acute and chronic low back pain. Where more than one eligible guideline was available for a country, we included the most recent guideline issued by a national body. Guidelines from the following countries/regions and agencies (year of publication) were included:
Australia, National Health and Medical Research Council (2003) [8];
Austria, Center for Excellence for Orthopaedic Pain Management Speising (2007) [9];
Canada, Clinic on Low back Pain in Interdisciplinary Practice (2007) [10];
Europe, COST B13 Working Group on Guidelines for the Management of Acute Low Back Pain in Primary Care (2004) [11];
Europe, COST B13 Working Group on Guidelines for the Management of Chronic Low Back Pain in Primary Care (2004) [12];
Finland, Working group by the Finnish Medical Society Duodecim and the Societas Medicinae Physicalis et Rehabilitationis Fenniae. Duodecim (2008) [13];
France, Agence Nationale d�Accreditation et d�Evaluation en Sante (2000) [14];
Germany, Drug Committee of the German Medical Society (2007) [15];
Italy, Italian Scientific Spine Institute (2006) [16];
New Zealand, New Zealand Guidelines Group (2004) [17];
Norway, Formi & Sosial- og helsedirectorated (2007) [18];
Spain, the Spanish Back Pain Research Network (2005) [19];
The Netherlands, The Dutch Institute for Healthcare Improvement (CBO) (2003) [20];
United Kingdom, National Health Service (2008) [21]; and
United States, American College of Physicians and the American Pain Society (2007) [22].
Data regarding the diagnostic and therapeutic recommendations as well as background information of the guideline process were extracted from the guidelines by four of the authors, each assessing 3�4 guidelines. The Finnish and Norwegian guidelines were assessed by colleagues with relevant language skills from The Netherlands and Finland. The focus was on the process of guideline development and the recommendations for diagnosis and treatment. We used the same data categories as in the previous review to facilitate comparisons (see Tables 1, ?,2,2, ?,33).
Results
Patient Population
Each of the guidelines considered the duration of symptoms but they vary in their scope and definitions. For example, the guidelines from Australia and New Zealand focus on acute low back pain whereas the guidelines from Austria and Germany consider acute, subacute, chronic and recurrent low back pain. The cut-off for chronic is not always specified but when it was, 12 weeks was used. Sometimes the word persistent rather than chronic was used. Two guidelines (Austrian and German) provide recommendations for recurrent low back pain but do not explicitly define �recurrent�.
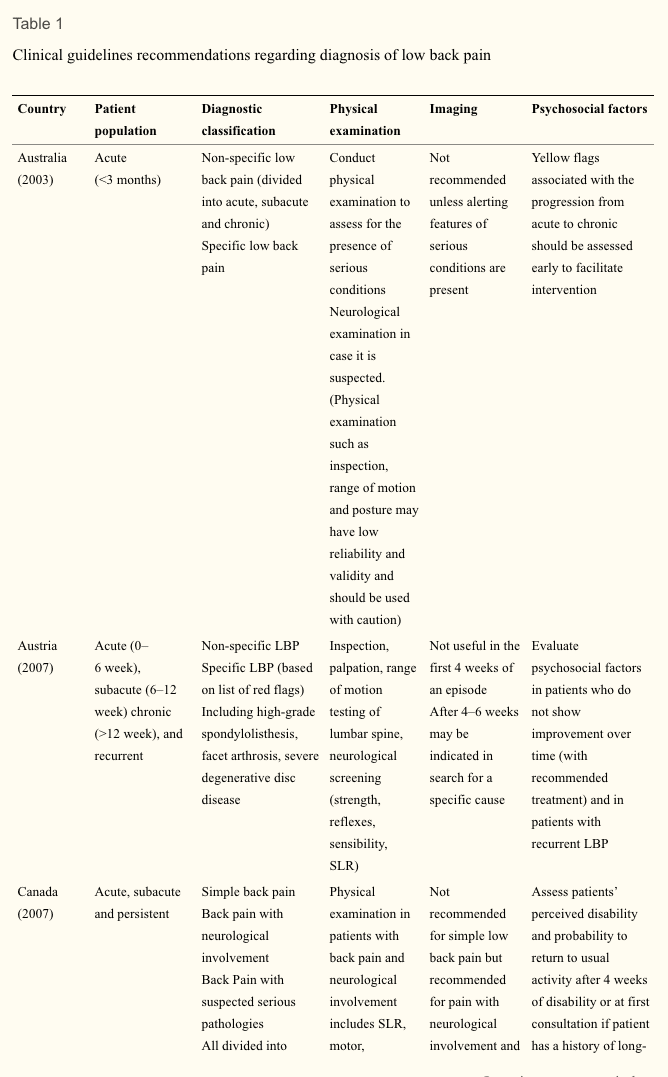
Diagnostic Recommendations
Table 1 compares the diagnostic classification and the recommendations on diagnostic procedures in the various guidelines. All guidelines recommend a diagnostic triage where patients are classified as having (2) non-specific low back pain, (2) suspected or confirmed serious pathology (�red flag� conditions such as tumour, infection or fracture) and (3) radicular syndrome. Some guidelines, e.g. the Australian and New Zealand guidelines, do not distinguish between non-specific low back pain and radicular syndrome. The German guideline also classifies a group of patients who are at risk for chronicity, based on �yellow flags�.
All guidelines are consistent in their recommendations that diagnostic procedures should focus on the identification of red flags and the exclusion of specific diseases (sometimes including radicular syndrome). Red flags include, for example, age at onset (<20 or >55 years), significant trauma, unexplained weight loss and widespread neurologic changes. The types of physical examination and physical tests that are recommended show some variation. Some, such as the European guideline, limit the examination to a neurological screen whereas others advocate a more comprehensive musculoskeletal (including inspection, range of motion/spinal mobility, palpation, and functional limitation) and neurological examination. The components of the neurologic screening are not always explicit but where they are, comprise testing of strength, reflexes, sensation and straight leg raising.
None of the guidelines recommend routine use of imaging, with imaging recommended at the initial visit only for cases of suspected serious pathology (e.g. Australian, European) or where the proposed treatment (e.g. manipulation) requires the exclusion of a specific cause of low back pain (French). Imaging is sometimes recommended where sufficient progress is not being made but the time cut-off varies from 4 to 7 weeks. Guidelines often recommend MRI in cases with red flags (e.g. European, Finland, Germany).
All guidelines mention psychosocial factors associated with poor prognosis with some describing them as �yellow flags�. There is, however, considerable variation in the amount of details given about how to assess �yellow flags� or the optimal timing of the assessment. The Canadian and the New Zealand guidelines provide specific tools for identifying yellow flags and clear guidelines for what should be done once yellow flags are identified.
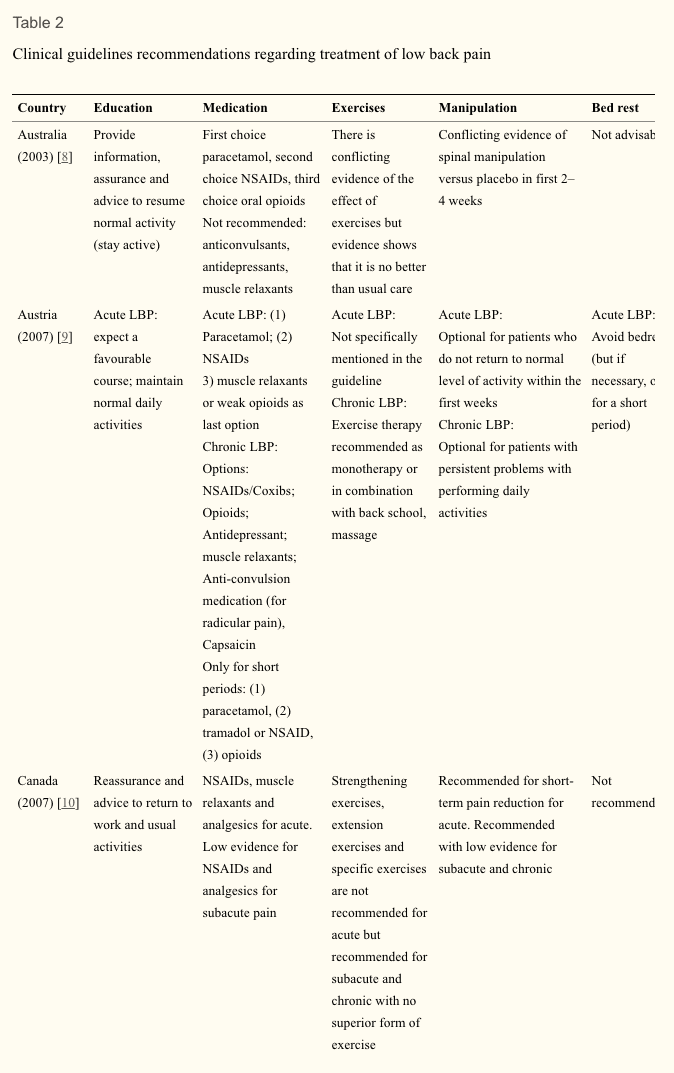
Therapeutic Recommendations
Table 2 compares therapeutic recommendations given in the various guidelines. Patient advice and information is recommended in all guidelines. The common message is that patients should be reassured that they do not have a serious disease, that they should stay as active as possible and progressively increase their activity levels. Compared with the previous review, the current guidelines increasingly mention early return to work (despite having low back pain) in their list of recommendations.
Recommendations for the prescription of medication are generally consistent. Paracetamol/acetaminophen is usually recommended as a first choice because of the lower incidence of gastrointestinal side effects. Nonsteroidal anti-inflammatory drugs are the second choice in cases where paracetamol is not sufficient. There is some variation between guidelines with regard to recommendations for opioids, muscle relaxants, steroids, antidepressant and anticonvulsive medication as co-medication for pain relief. Where the mode of consumption of analgesics is described, time-contingent rather than pain-contingent use, is advocated.
There is now broad consensus that bed rest should be discouraged as a treatment for low back pain. Some guidelines state that if bed rest is indicated because of severity of pain, then it should not be advised for more than 2 days (e.g., Germany, New Zealand, Spain, Norway). The Italian guideline advises 2�4 days of bed rest for major sciatica but does clearly describe how major sciatica differs from sciatica where bed rest is contraindicated.
There is also consensus that a supervised exercise programme (as distinct from encouraging resumption of normal activity) is not indicated for acute low back pain. Those guidelines that consider subacute and chronic low back pain recommend exercise but note that there is no evidence that one form of exercise is superior to another. The European guideline advises against exercise that requires expensive training and machines. The one area of therapy that is contentious is the use of spinal manipulation. Some guidelines do not recommend the treatment (e.g. Spanish, Australian), some advise that it is optional (e.g. Austrian, Italian) and some suggest a short course for those who do not respond to the first line of treatment (e.g. US, the Netherlands). For some it is optional only in the first weeks of an episode in acute low back pain (e.g. Canada, Finland, Norway, Germany, New Zealand). The French guideline advises that there is no evidence to recommend one form of manual therapy over another.
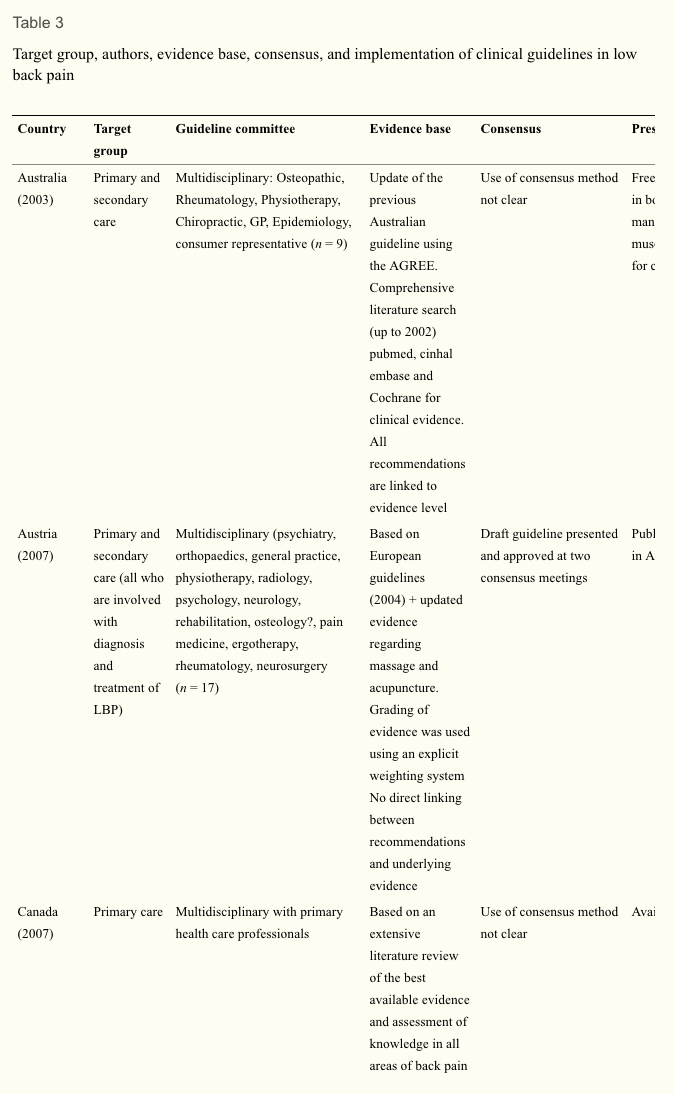
Setting. Table 3 shows some background variables related to the development of the guidelines in the various countries. Most of the guidelines focus on primary care though some also include secondary care. The Spanish guideline is written for health professions that treat low back pain.
Guideline committee. The various committees responsible for the development and publication of guidelines appear to be different in size and in the professional disciplines involved. Most committees are characterised by their multidisciplinary membership. These usually included primary care physicians, physical and manual therapists, orthopaedic surgeons, rheumatologists, radiologists, occupational and rehabilitation physicians. The number of members varied from 7 to 31. Only three committees included consumer representation (Australia, New Zealand, the Netherlands).
Evidence-based review. All guidelines are more or less based on a comprehensive literature search, including Cochrane Library, Medline, Embase. Some committees (Austria, Germany, Spain) based their recommendations, entirely or in part, on the European guidelines. Most guidelines use an explicit weighting of the strength of the evidence.
The Dutch, UK, European, Finnish, German, Norwegian and Australian guidelines give direct links between the actual recommendations and the evidence (via specific references) on which the recommendations are based. Other guidelines do not present a direct link but state that for recommendation there is at least moderate or fair evidence (New Zealand, US). Most committees use consensus methods, mostly by group discussions when the evidence was not convincing or not available.
Presentation and implementation. The activities related to the publication and dissemination of the various guidelines show some differences and some similarities. In most cases, the guidelines are accompanied by easily accessible summaries for practitioners and booklets for patients. Systematic implementation activities are rare. In most cases, the printed versions of the guidelines are published in national journals and/or disseminated through professional organisations to the target practitioners. Most guidelines are available on the websites of participating organisation. In many countries, regular updates of the guidelines are planned with time horizons of 3�5 years.
Discussion
In the past decade many countries have issued (updated) clinical guidelines for the management of low back pain. In general these guidelines provide similar advice on the management of low back pain. Common recommendations are the diagnostic triage of patients with low back pain, restricted use of radiographs, advice on early and progressive activation of patients, and the related discouragement of bed rest. The recognition of psychosocial factors as a risk factor for chronicity is also consistent across all guidelines, though with varying emphasis and detail. There are also differences in the recommendations provided by the guidelines, but these are few and probably less than could expected for different health care systems and cultures. One of the reasons for the similarity of the guidelines might be that guideline committees are usually aware of the content of other guidelines and are motivated to produce similar recommendations that are deemed sensible and relevant. In some instances the guidelines are a national adaptation (e.g. in Spain) of the European guidelines.
We do not present an exhaustive overview of all clinical guidelines available, but focused on national multidisciplinary guidelines. This enables a reasonable comparison of recommended approaches across countries. A limitation is thus that not all available guidelines, including mono-disciplinary guidelines, are included.
Use of Available Evidence
Most reviews are based on extensive literature reviews. Cochrane reviews are frequently used, comprehensive searches in databases such as Medline, Embase and PEDro. Increasingly the literature reviews of other and previous guidelines are used as starting point for the (additional) searches. Most committees also use some kind of weighting system and rating of the evidence. There is some variation in the way the recommendations are presented. In some guidelines all the recommendations are directly linked with references to the supporting evidence, and in others a general remark is made that for all recommendations that there is at least moderate evidence available.
Differences in Recommendations
Recommendations about the prescription of analgesic medication remain fairly consistent. Most guidelines recommend paracetamol as the first option and nonsteroidal anti-inflammatory preparations as the second option. Further recommendations about other drugs like opioids, muscle relaxants and benzodiazepines and antidepressants vary quite considerably. Part of these variations might reflect the setting and custom in different countries. Since all the guidelines were issued within a relative short time frame, the availability of underlying evidence did not vary much.
The recommendations regarding spinal manipulation continue to show some variation. In some guidelines manipulation is recommended, or presented as a therapeutic option, usually for short-term benefit, but others do not recommend it. This holds true for acute as well as chronic low back pain. The reasons for these differences remain speculative. Probably the underlying evidence is not strong enough to result in similar recommendations regarding manipulation across all guidelines, leaving the committees some more room for interpretation, but also local or political reasons may be involved.
There is now relatively large consensus across the various guidelines that specific back exercises (as opposed to the advice to stay active, including for example walking, cycling) are not recommended for patients with acute low back pain. At the same time back exercises are recommended in chronic low back pain. Most guidelines do not recommend a particular type of exercises for chronic low back pain, but some state that they should be intense.
Recommendations in guidelines are based not only on scientific evidence but also on consensus and discussion in the guideline committees. Usually it is stated that consensus was based on group discussion, but the details of these discussions are seldom reported. It is also generally unclear which recommendations are based mainly on scientific evidence and which are based on (mainly) consensus.
There is little information on whether cost-effectiveness played an important role as a basis for the recommendation in a guideline. Of course, there are not yet many cost-effectiveness studies available [23], but it is not fully clear to what extent the published studies were used.
Most guidelines state that the prognosis of an episode of low back pain is good. This holds especially true for patients with acute episodes of low back pain. For patients presenting with a longer duration with low back pain or with recurrent low back pain the prognosis may be less favourable. More individualised and precise estimates of the prognosis of an episode of low back pain may be desirable in the future.
Few Changes in Management Recommendations Over Time
This update showed that overall the recommendations in the current guidelines regarding diagnosis and treatment of low back pain did not change substantially compared to the guidelines issued about a decade ago. This may well illustrate the lack of new evidence showing better results with new diagnostic and therapeutic approaches and/or new evidence showing the inefficacy of existing interventions. A less nihilistic view could be that already a decade ago the most valid recommendations for the management of low back pain were identified. Some may argue that this is indeed the case, and that much more effort should now be given to implementation of guidelines (see below).
Some recommendations did change over time. We now see diagnostic recommendations appearing concerning the value of MRI and CT scans (i.e. in relation to exclusion and further diagnosis of red flags and serious spinal disorders). However, these recommendations are not yet strong, possibly because there are not many diagnostic studies available evaluating the value of MRI in patients with low back pain. Also, the recommendations regarding the assessment of psychosocial risk factors for chronicity are more firm in the current guidelines than that a decade ago. This reflects the insight of the importance of these risk factors for the development of chronicity and future disability. At the same time we must conclude that we are not yet very successful in effective screening of the patients at risk and subsequent therapeutic management of them [24].
Most apparent changes regarding therapeutic interventions include the advice to continue work (despite having low back pain) and or return to work as soon as possible. There are now more recommendations of second line medications such as antidepressants, opioids, benzodiazepines and compound medications. But these recommendations are not consistent across countries, potentially because of weak underlying evidence. There are now also more firm recommendations in favour of exercise therapy in patients with subacute and chronic low back pain. The latter is partly due to the fact that currently more guidelines include recommendation for the management of chronic low back pain as compared to a decade ago. Finally, the reasons and options for referral within primary care and secondary care are now more explicitly presented. It appears that the global approach regarding the management of low back pain remained largely unchanged in the past decade, although some refinements have been suggested.
Implementation
The extent to which currently available guidelines are used and followed in the various countries remains largely unknown. A few studies evaluating various implementation strategies for low back pain guidelines show that changing clinical practice is not an easy task [25, 26]. The publication and dissemination of guidelines alone is usually not enough to change the behaviour of health care providers [27]. The development of effective implementation strategies in this area remains a challenge.
Future Developments in Research and Guideline Development
The present study was primary aimed at presenting an update of the current clinical guidelines for the management of low back pain in primary care. Clinical guidelines focused at secondary care settings, occupational care settings, or specific subgroups of patients with lumbosacral radicular syndrome were not considered. Separate studies need to be undertaken to present an overview for these settings.
We assessed various aspects of the guideline development in Table 3. A formal assessment of the quality, e.g. with the AGREE instrument was not included. This was the topic of a separate paper which concluded that the quality of the guidelines indeed has improved over time [7].
The development of future guidelines in this field may benefit from previous experiences, evidence-based reviews, and various (inter) national guidelines as presented in this overview. The previous review of clinical guidelines listed the following recommendations (slightly modified) for the development of future guidelines in this field. Similar to a recent review on the quality of guidelines [7], this review shows that the quality of guidelines has improved over time and some of the recommendations have been followed. This includes recommendations 1, 3, and 4 (see below). For others, there still is room for improvement Recommendation 2 is not consistently applied. Recommendations 5 and 6 have improved over time, but not all recommendations in the guidelines are directly linked to the underlying evidence, and the process of the consensus methods used is not well described. Finally, the implementation strategies and the time frame of future updates are not well presented.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Footnotes
Based upon search of PEDro database April 29, 2009.
In conclusion,�low back pain is a prevalent medical complaint which affects million of people in the United States alone. Although it may seem difficult to diagnose low back pain because of its many possible causes, a chiropractor, or doctor of chiropractic, can properly diagnose the source of a patient’s low back pain to treat as well as prevent a variety of injuries and/or conditions associated with the musculoskeletal and nervous system. Chiropractic care utilizes spinal adjustments and manual manipulations, among other treatment methods, to carefully restore the original alignment of the spine, allowing the human body to naturally heal itself. The purpose of the article above is to present updated treatment guidelines fot the management of low back pain in a primary care setting.� Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
According to statistics, approximately 80% of people will experience symptoms of back pain at least once throughout their lifetimes. Back pain is a common complaint which can result due to a variety of injuries and/or conditions. Often times, the natural degeneration of the spine with age can cause back pain. Herniated discs occur when the soft, gel-like center of an intervertebral disc pushes through a tear in its surrounding, outer ring of cartilage, compressing and irritating the nerve roots. Disc herniations most commonly occur along the lower back, or lumbar spine, but they may also occur along the cervical spine, or neck. The impingement of the nerves found in the low back due to injury and/or an aggravated condition can lead to symptoms of sciatica.
1.�Koes BW, Tulder MW, Thomas S. Diagnosis and treatment of low back pain.�BMJ.�2006;332(7555):1430�1434. doi: 10.1136/bmj.332.7555.1430.�[PMC free article]�[PubMed]�[Cross Ref]
2.�Pengel L, Herbert R, Maher CG, Refshauge K. Acute low back pain: systematic review of its prognosis.�BMJ.�2003;327:323�327. doi: 10.1136/bmj.327.7410.323.�[PMC free article]�[PubMed]�[Cross Ref]
3.�Henschke N, Maher CG, Refshauge KM, Herbert RD, Cumming RG, Bleasel J, York J, Das A, McAuley JH. Prognosis in patients with recent onset low back pain in Australian primary care: inception cohort study.�BMJ.�2008;337:171. doi: 10.1136/bmj.a171.�[PMC free article]�[PubMed]�[Cross Ref]
4.�Australian Institute of Health and Welfare (2004) Australia�s Health 2004. AIHW, Canberra
5.�Spitzer W. Scientific approach to the assessment and management of activity-related spinal disorders.�Spine.�1987;12:1�58. doi: 10.1097/00007632-198701000-00001.�[PubMed]�[Cross Ref]
6.�Koes BW, Tulder MW, Ostelo R, et al. Clinical guidelines for the management of low back pain in primary care: an international comparison.�Spine.�2001;26:2504�2513. doi: 10.1097/00007632-200111150-00022.�[PubMed]�[Cross Ref]
7.�Bouwmeester W, Enst A, Tulder MW. Quality of low back pain guidelines improved.�Spine.�2009;34:2562�2567. doi: 10.1097/BRS.0b013e3181b4d50d.�[PubMed]�[Cross Ref]
8.�Evidence-based management of acute musculoskeletal pain.�Bowen Hills: Australian Academic Press; 2003.
9.�Friedrich M, Likar R. Evidenz- und konsensusbasierte �sterreichische Leitlinien f�r das Management akuter und chronischer unspezifischer Kreuzschmerzen.�Wien Klin Wochenschr.�2007;119(5�6):189�197. doi: 10.1007/s00508-006-0754-3.�[PubMed]�[Cross Ref]
11.�Tulder MW, Becker A, Bekkering T, et al. European guidelines for the management of acute low back pain in primary care.�Eur Spine J.�2006;15(Suppl 2):S169�S191. doi: 10.1007/s00586-006-1071-2.[PMC free article]�[PubMed]�[Cross Ref]
12.�Airaksinen O, Brox JI, Cedraschi C, et al. European guidelines for the management of chronic non-specific low back pain.�Eur Spine J.�2006;15(2):S192�S300. doi: 10.1007/s00586-006-1072-1.[PMC free article]�[PubMed]�[Cross Ref]
13.�Malmivaara A, Erkintalo M, Jousimaa J, Kumpulainen T, Kuukkanen T, Pohjolainen T, Seitsalo S, �sterman H (2008) Aikuisten alaselk�sairaudet. (Low back pain among adults. An update within the Finnish Current Care guidelines). Working group by the Finnish Medical Society Duodecim and the Societas Medicinae Physicalis et Rehabilitationis, Fenniae. Duodecim 124:2237�2239
14.�Agence Nationale d�Accreditation et d�Evaluation en Sante (2000) Guidelines department, diagnosis and management of acute low back pain (<3�months) with or without sciatica & diagnosis, management and follow-up of patients with chronic low back pain, Paris.�www.anaes.fr�or�www.sante.fr
15.�Drug Committee of the German Medical Society (2007) Recommendations for treatment of low back pain [in German]. K�ln, Germany
16.�Negrini S, Giovannoni S, Minozzi S, et al. Diagnostic therapeutic flow-charts for low back pain patients: the Italian clinical guidelines.�Euro Medicophys.�2006;42(2):151�170.�[PubMed]
17.�National Health Committee (2004) National Advisory Committee on Health and Disability, Accident Rehabilitation and Compensation Insurance Corporation. New Zealand Acute Low back pain Guide. Wellington, New Zealand
18.�Laerum E, Storheim K, Brox JI. New clinical guidelines for low back pain.�Tidsskr Nor Laegeforen.�2007;127(20):2706.�[PubMed]
19.�Spain, the Spanish Back Pain Research Network (2005) Guia de practica clinica. Lumbalgia Inespecifica. Version espnola de la Guia de Practica Clinica del Programa Europeo COST B13
20.�The Dutch Institute for Healthcare Improvement (CBO) (2003) Clinical guideline for non-specific low back pain [in Dutch]
22.�Chou R, Qaseem A, Snow V, et al. Clinical Efficacy Assessment Subcommittee of the American College of Physicians American College of Physicians American Pain Society Low back pain Guidelines Panel Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of Physicians and the American Pain Society.�Ann Intern Med.�2007;147(7):478�491.�[PubMed]
23.�Roer N, Goossens ME, Evers SM, Tulder MW. What is the most cost-effective treatment for patients with low back pain? A systematic review.�Best Pract Res Clin Rheumatol.�2005;19(4):671�684. doi: 10.1016/j.berh.2005.03.007.�[PubMed]�[Cross Ref]
24.�Jellema P, Windt DA, Horst HE, Blankenstein AH, Bouter LM, Stalman WA. Why is a treatment aimed at psychosocial factors not effective in patients with (sub)acute low back pain?�Pain.�2005;118(3):350�359. doi: 10.1016/j.pain.2005.09.002.�[PubMed]�[Cross Ref]
25.�Bekkering GE, Tulder MW, Hendriks EJM, Koopmanschap MA, Knol DL, Bouter LM, Oostendorp RAB. Implementation of clinical guidelines on physical therapy for patients with low back pain: randomized trial comparing patient outcomes after a standard and active implementation strategy.�Phys Ther.�2005;85(6):544�555.�[PubMed]
26.�Engers AJ, Wensing M, Tulder MW, Timmermans A, Oostendorp RA, Koes BW, Grol R. Implementation of the Dutch low back pain guideline for general practitioners: a cluster randomized controlled trial.�Spine.�2005;30(6):595�600. doi: 10.1097/01.brs.0000155406.79479.3a.�[PubMed][Cross Ref]
27.�Becker A, Leonhardt C, Kochen MM, Keller S, Wegscheider K, Baum E, Donner-Banzhoff N, Pfingsten M, Hildebrandt J, Basler HD, Chenot JF. Effects of two guideline implementation strategies on patient outcomes in primary care: a cluster randomized controlled trial.�Spine.�2008;33(5):473�480. doi: 10.1097/BRS.0b013e3181657e0d.�[PubMed]�[Cross Ref]
Everyone experiences pain from time to time. Pain is a physical feeling of discomfort caused by injury or illness. When you pull a muscle or cut your finger, for instance, a signal is sent through the nerve roots to the brain, signaling you that something is wrong in the body. Pain may be different for everyone and there are several ways of feeling and describing pain. After an injury or illness heals, the pain will subside, however, what happens if the pain continues even after you’ve healed?
Chronic pain is often defined as any pain which lasts more than 12 weeks. Chronic pain can range from mild to severe and it can be the result of previous injury or surgery, migraine and headache, arthritis, nerve damage, infection and fibromyalgia. Chronic pain can affect an individual’s emotional and mental disposition, making it more difficult to relieve the symptoms. Research studies have demonstrated that psychological interventions can assist the chronic pain recovery process. Several healthcare professionals, like a doctor of chiropractic, can provide chiropractic care together with psychological interventions to help restore the overall health and wellness of their patients. The purpose of the following article is to demonstrate the role of psychological interventions in the management of patients with chronic pain, including headache and back pain.
The Role of Psychological Interventions in the Management of Patients with Chronic Pain
Abstract
Chronic pain can be best understood from a biopsychosocial perspective through which pain is viewed as a complex, multifaceted experience emerging from the dynamic interplay of a patient�s physiological state, thoughts, emotions, behaviors, and sociocultural influences. A biopsychosocial perspective focuses on viewing chronic pain as an illness rather than disease, thus recognizing that it is a subjective experience and that treatment approaches are aimed at the management, rather than the cure, of chronic pain. Current psychological approaches to the management of chronic pain include interventions that aim to achieve increased self-management, behavioral change, and cognitive change rather than directly eliminate the locus of pain. Benefits of including psychological treatments in multidisciplinary approaches to the management of chronic pain include, but are not limited to, increased self-management of pain, improved pain-coping resources, reduced pain-related disability, and reduced emotional distress � improvements that are effected via a variety of effective self-regulatory, behavioral, and cognitive techniques. Through implementation of these changes, psychologists can effectively help patients feel more in command of their pain control and enable them to live as normal a life as possible despite pain. Moreover, the skills learned through psychological interventions empower and enable patients to become active participants in the management of their illness and instill valuable skills that patients can employ throughout their lives.
Chronic pain has previously been determined to affect the psychological health of those with persistent symptoms, ultimately altering their overall mental and emotional disposition. In addition, patients with overlapping conditions, including stress, anxiety and depression, can make treatment a challenge. The role of chiropractic care is to restore as well as maintain and improve the original alignment of the spine through the use of spinal adjustments and manual manipulations. Chiropractic care allows the body to naturally heal itself without the need for drugs/medications and surgical interventions, although these can be referred to by a chiropractor if needed. However, chiropractic care focuses on the body as a whole, rather than on a single injury and/or condition and its symptoms. Spinal adjustments and manual manipulations, among other treatment methods and techniques commonly used by a chiropractor, require awareness of the patient’s mental and emotional disposition in order to effectively provide them with overall health and wellness. Patients who visit my clinic with emotional distress from their chronic pain are often more susceptible to experience psychological issues as a result. Therefore, chiropractic care can be a fundamental psychological intervention for chronic pain management, along with those demonstrated below.
Introduction
Pain is a ubiquitous human experience. It is estimated that approximately 20%�35% of adults experience chronic pain.[1,2] The National Institute of Nursing Research reports that pain affects more Americans than diabetes, heart disease, and cancer combined.[3] Pain has been cited as the primary reason to seek medical care in the United States.[4] Furthermore, pain relievers are the second most commonly prescribed medications in physicians� offices and emergency rooms.[5] Further solidifying the importance of adequate assessment of pain, the Joint Commission on the Accreditation of Healthcare Organizations issued a mandate requiring that pain be evaluated as the fifth vital sign during medical visits.[6]
The International Association for the Study of Pain (IASP) defines pain as �an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage�.[7] The IASP�s definition highlights the multidimensional and subjective nature of pain, a complex experience that is unique to each individual. Chronic pain is typically differentiated from acute pain based on its chronicity or persistence, its physiological maintenance mechanisms, and/or its detrimental impact on an individual�s life. Generally, it is accepted that pain that persists beyond the expected period of time for tissue healing following an injury or surgery is considered chronic pain. However, the specific timeframe constituting an expected healing period is variable and often difficult to ascertain. For ease of classification, certain guidelines suggest that pain persisting beyond a 3�6 month time window is considered chronic pain.[7] Nevertheless, classification of pain based solely on duration is a strictly practical and, in some instances, arbitrary criterion. More commonly, additional factors such as etiology, pain intensity, and impact are considered alongside duration when classifying chronic pain. An alternative way to characterize chronic pain has been based on its physiological maintenance mechanism; that is, pain that is thought to emerge as a result of peripheral and central reorganization. Common chronic pain conditions include musculoskeletal disorders, neuropathic pain conditions, headache pain, cancer pain, and visceral pain. More broadly, pain conditions may be primarily nociceptive (producing mechanical or chemical pain), neuropathic (resulting from nerve damage), or central (resulting from dysfunction in the neurons of the central nervous system).[8]
Unfortunately, the experience of pain is frequently characterized by undue physical, psychological, social, and financial suffering. Chronic pain has been recognized as the leading cause of long-term disability in the working- age American population.[9] Because chronic pain affects the individual at multiple domains of his/her existence it also constitutes an enormous financial burden to our society. The combined direct and indirect costs of pain have been estimated to range from $125 billion to $215 billion, annually.[10,11] The widespread implications of chronic pain include increased reports of emotional distress (eg, depression, anxiety, and frustration), increased rates of pain-related disability, pain-related alterations in cognition, and reduced quality of life. Thus, chronic pain can be best understood from a biopsychosocial perspective through which pain is viewed as a complex, multifaceted experience emerging from the dynamic interplay of a patient�s physiological state, thoughts, emotions, behaviors, and sociocultural influences.
Pain Management
Given the widespread prevalence of pain and its multi-dimensional nature, an ideal pain management regimen will be comprehensive, integrative, and interdisciplinary. Current approaches to the management of chronic pain have increasingly transcended the reductionist and strictly surgical, physical, or pharmacological approach to treatment. Current approaches recognize the value of a multidisciplinary treatment framework that targets not only nociceptive aspects of pain but also cognitive-evaluative, and motivational-affective aspects alongside equally unpleasant and impacting sequelae. The interdisciplinary management of chronic pain typically includes multimodal treatments such as combinations of analgesics, physical therapy, behavioral therapy, and psychological therapy. The multimodal approach more adequately and comprehensively addresses pain management at the molecular, behavioral, cognitive-affective, and functional levels. These approaches have been shown to lead to superior and long-lasting subjective and objective outcomes including pain reports, mood, restoration of daily functioning, work status, and medication or health care use; multimodal approaches have also been shown to be more cost-effective than unimodal approaches.[12,13] The focus of this review will be specifically on elucidating the benefits of psychology in the management of chronic pain.
Patients will typically initially present to a physician�s office in the pursuit of a cure or treatment for their ailment/acute pain. For many patients, depending on the etiology and pathology of their pain alongside biopsychosocial influences on the pain experience, acute pain will resolve with the passage of time, or following treatments aimed at targeting the presumed cause of pain or its transmission. Nonetheless, some patients will not achieve resolution of their pain despite numerous medical and complementary interventions and will transition from an acute pain state to a state of chronic, intractable pain. For instance, research has demonstrated that approximately 30% of patients presenting to their primary-care physician for complaints related to acute back pain will continue to experience pain and, for many others, severe activity limitations and suffering 12 months later.[14] As pain and its consequences continue to develop and manifest in diverse aspects of life, chronic pain may become primarily a biopsychosocial problem, whereby numerous biopsychosocial aspects may serve to perpetuate and maintain pain, thus continuing to negatively impact the affected individual�s life. It is at this point that the original treatment regimen may diversify to include other therapeutic components, including psychological approaches to pain management.
Psychological approaches for the management of chronic pain initially gained popularity in the late 1960s with the emergence of Melzack and Wall�s �gate-control theory of pain�[15] and the subsequent �neuromatrix theory of pain�.[16] Briefly, these theories posit that psychosocial and physiological processes interact to affect perception, transmission, and evaluation of pain, and recognize the influence of these processes as maintenance factors involved in the states of chronic or prolonged pain. Namely, these theories served as integral catalysts for instituting change in the dominant and unimodal approach to the treatment of pain, one heavily dominated by strictly biological perspectives. Clinicians and patients alike gained an increasing recognition and appreciation for the complexity of pain processing and maintenance; consequently, the acceptance of and preference for multidimensional conceptualizations of pain were established. Currently, the biopsychosocial model of pain is, perhaps, the most widely accepted heuristic approach to understanding pain.[17] A biopsychosocial perspective focuses on viewing chronic pain as an illness rather than disease, thus recognizing that it is a subjective experience and that treatment approaches are aimed at the management, rather than the cure, of chronic pain.[17] As the utility of a broader and more comprehensive approach to the management of chronic pain has become evident, psychologically-based interventions have witnessed a remarkable rise in popularity and recognition as adjunct treatments. The types of psychological interventions employed as part of a multidisciplinary pain treatment program vary according to therapist orientation, pain etiology, and patient characteristics. Likewise, research on the effectiveness of psychologically based interventions for chronic pain has shown variable, albeit promising, results on key variables studied. This overview will briefly describe frequently employed psychologically based treatment options and their respective effectiveness on key outcomes.
Current psychological approaches to the management of chronic pain include interventions that aim to achieve increased self-management, behavioral change, and cognitive change rather than directly eliminate the locus of pain. As such, they target the frequently overlooked behavioral, emotional, and cognitive components of chronic pain and factors contributing to its maintenance. Informed by the framework offered by Hoffman et al[18] and Kerns et al,[19] the following frequently employed psychologically-based treatment domains are reviewed: psychophysiological techniques, behavioral approaches to treatment, cognitive behavioral therapy, and acceptance-based interventions.
Psychophysiological Techniques
Biofeedback
Biofeedback is a learning technique through which patients learn to interpret feedback (in the form of physiological data) regarding certain physiological functions. For instance, a patient may use biofeedback equipment to learn to recognize areas of tension in their body and subsequently learn to relax those areas to reduce muscular tension. Feedback is provided by a variety of measurement instruments that can yield information about brain electrical activity, blood pressure, blood flow, muscle tone, electrodermal activity, heart rate, and skin temperature, among other physiological functions in a rapid manner. The goal of biofeedback approaches is for the patient to learn how to initiate physiological self-regulatory processes by achieving voluntary control over certain physiological responses to ultimately increase physiological flexibility through greater awareness and specific training. Thus a patient will use specific self-regulatory skills in an attempt to reduce an undesired event (eg, pain) or maladaptive physiological reactions to an undesired event (eg, stress response). Many psychologists are trained in biofeedback techniques and provide these services as part of therapy. Biofeedback has been designated as an efficacious treatment for pain associated with headache and temporomandibular disorders (TMD).[20] A meta-analysis of 55 studies revealed that biofeedback interventions (including various biofeedback modalities) yielded significant improvements with regard to frequency of migraine attacks and perceptions of headache management self-efficacy when compared to control conditions.[21] Studies have provided empirical support for biofeedback for TMD, albeit more robust improvements with regard to pain and pain-related disability have been found for protocols that combine biofeedback with cognitive behavioral skills training, under the assumption that a combined treatment approach more comprehensively addresses the gamut of biopsychosocial problems that may be encountered as a result of TMD.[22]
Behavioral Approaches
Relaxation Training
It is generally accepted that stress is a key factor involved in the exacerbation and maintenance of chronic pain.[16,23] Stress can be predominantly of an environmental, physical, or psychological/emotional basis, though typically these mechanisms are intricately intertwined. The focus of relaxation training is to reduce tension levels (physical and mental) through activation of the parasympathetic nervous system and through attainment of greater awareness of physiological and psychological states, thereby achieving reductions in pain and increasing control over pain. Patients can be taught several relaxation techniques and practice them individually or in conjunction with one another, as well as adjuvant components to other behavioral and cognitive pain management techniques. The following are brief descriptions of relaxation techniques commonly taught by psychologists specializing in the management of chronic pain.
Diaphragmatic breathing. Diaphragmatic breathing is a basic relaxation technique whereby patients are instructed to use the muscles of their diaphragm as opposed to the muscles of their chest to engage in deep breathing exercises. Breathing by contracting the diaphragm allows the lungs to expand down (marked by expansion of abdomen during inhalation) and thus increase oxygen intake.[24]
Progressive muscle relaxation (PMR). PMR is characterized by engaging in a combination of muscle tension and relaxation exercises of specific muscles or muscle groups throughout the body.[25] The patient is typically instructed to engage in the tension/relaxation exercises in a sequential manner until all areas of the body have been addressed.
Autogenic training (AT). AT is a self-regulatory relaxation technique in which a patient repeats a phrase in conjunction with visualization to induce a state of relaxation.[26,27] This method combines passive concentration, visualization, and deep breathing techniques.
Visualization/Guided imagery. This technique encourages patients to use all of their senses in imagining a vivid, serene, and safe environment to achieve a sense of relaxation and distraction from their pain and pain-related thoughts and sensations.[27]
Collectively, relaxation techniques have generally been found to be beneficial in the management of a variety of types of acute and chronic pain conditions as well as in the management of important pain sequelae (eg, health-related quality of life).[28�31] Relaxation techniques are usually practiced in conjunction with other pain management modalities, and there is considerable overlap in the presumed mechanisms of relaxation and biofeedback, for instance.
Operant Behavior Therapy
Operant behavior therapy for chronic pain is guided by the original operant conditioning principles proposed by Skinner[32] and refined by Fordyce[33] to be applicable to pain management. The main tenets of the operant conditioning model as it relates to pain hold that pain behavior can eventually evolve into and be maintained as chronic pain manifestations as a result of positive or negative reinforcement of a given pain behavior as well as punishment of more adaptive, non-pain behavior. If reinforcement and the ensuing consequences occur with sufficient frequency, they can serve to condition the behavior, thus increasing the likelihood of repeating the behavior in the future. Therefore, conditioned behaviors occur as a product of learning of the consequences (actual or anticipated) of engaging in the given behavior. An example of a conditioned behavior is continued use of medication � a behavior that results from learning through repeated associations that taking medication is followed by removal of an aversive sensation (pain). Likewise, pain behaviors (eg, verbal expressions of pain, low activity levels) can be become conditioned behaviors that serve to perpetuate chronic pain and its sequelae. Treatments that are guided by operant behavior principles aim to extinguish maladaptive pain behaviors through the same learning principles that these may have been established by. In general, treatment components of operant behavior therapy include graded activation, time contingent medication schedules, and use of reinforcement principles to increase well behaviors and decrease maladaptive pain behaviors.
Graded activation. Psychologists can implement graded activity programs for chronic pain patients who have vastly reduced their activity levels (increasing likelihood of physical deconditioning) and subsequently experience high levels of pain upon engaging in activity. Patients are instructed to safely break the cycle of inactivity and deconditioning by engaging in activity in a controlled and time-limited fashion. In this manner, patients can gradually increase the length of time and intensity of activity to improve functioning. Psychologists can oversee progress and provide appropriate reinforcement for compliance, correction of misperceptions or misinterpretations of pain resulting from activity, where appropriate, and problem-solve barriers to adherence. This approach is frequently embedded within cognitive-behavioral pain management treatments.
Time-contingent medication schedules. A psychologist can be an important adjunct healthcare provider in overseeing the management of pain medications. In some cases, psychologists have the opportunity for more frequent and in-depth contact with patients than physicians and thus can serve as valuable collaborators of an integrated multidisciplinary treatment approach. Psychologists can institute time-contingent medication schedules to reduce the likelihood of dependence on pain medications for attaining adequate control over pain. Furthermore, psychologists are well equipped to engage patients in important conversations regarding the importance of proper adherence to medications and medical recommendations and problem-solve perceived barriers to safe adherence.
Fear-avoidance. The fear-avoidance model of chronic pain is a heuristic most frequently applied in the context of chronic low back pain (LBP).[34] This model draws largely from the operant behavior principles described previously. In essence, the fear-avoidance model posits that when acute pain states are repeatedly misinterpreted as danger signals or signs of serious injury, patients may be at risk of engaging in fear-driven avoidance behaviors and cognitions that further reinforce the belief that pain is a danger signal and perpetuate physical deconditioning. As the cycle continues, avoidance may generalize to broader types of activity and result in hypervigilance of physical sensations characterized by misinformed catastrophic interpretations of physical sensations. Research has shown that a high degree of pain catastrophizing is associated with maintenance of the cycle.[35] Treatments aimed at breaking the fear-avoidance cycle employ systematic graded exposure to feared activities to disconfirm the feared, often catastrophic, consequences of engaging in activities. Graded exposure is typically supplemented with psychoeducation about pain and cognitive restructuring elements that target maladaptive cognitions and expectations about activity and pain. Psychologists are in an excellent position to execute these types of interventions that closely mimic exposure treatments traditionally used in the treatment of some anxiety disorders.
Though specific graded exposure treatments have been shown to be effective in the treatment of complex regional pain syndrome type I (CRPS-1)[36] and LBP[37] in single-case designs, a larger-scale randomized controlled trial comparing systematic graded exposure treatment combined with multidisciplinary pain program treatment with multidisciplinary pain program treatment alone and with a wait-list control group found that the two active treatments resulted in significant improvements on outcome measures of pain intensity, fear of movement/injury, pain self-efficacy, depression, and activity level.[38] Results from this trial suggest that both interventions were associated with significant treatment effectiveness such that the graded exposure treatment did not appear to result in additional treatment gains.[38] A cautionary note in the interpretation of these results highlights that the randomized controlled trial (RCT) included a variety of chronic pain conditions that extended beyond LBP and CRPS-1 and did not exclusively include patients with high levels of pain-related fear; the interventions were also delivered in group formats rather than individual formats. Although in-vivo exposure treatments are superior at reducing pain catastrophizing and perceptions of harmfulness of activities, exposure treatments seem to be as effective as graded activity interventions in improving functional disability and chief complaints.[39] Another clinical trial compared the effectiveness of treatment-based classification (TBC) physical therapy alone to TBC augmented with graded activity or graded exposure for patients with acute and sub-acute LBP.[40] Outcomes revealed that there were no differences in 4-week and 6-month outcomes for reduction of disability, pain intensity, pain catastrophizing, and physical impairment among treatment groups, although graded exposure and TBC yielded larger reductions in fear-avoidance beliefs at 6 months.[40] Findings from this clinical trial suggest that enhancing TBC with graded activity or graded exposure does not lead to improved outcomes with regard to measures associated with the development of chronic LBP beyond improvements achieved with TBC alone.[40]
Cognitive-Behavioral Approaches
Cognitive-behavioral therapy (CBT) interventions for chronic pain utilize psychological principles to effect adaptive changes in the patient�s behaviors, cognitions or evaluations, and emotions. These interventions are generally comprised of basic psychoeducation about pain and the patient�s particular pain syndrome, several behavioral components, coping skills training, problem-solving approaches, and a cognitive restructuring component, though the exact treatment components vary according to the clinician. Behavioral components may include a variety of relaxation skills (as reviewed in the behavioral approaches section), activity pacing instructions/graded activation, behavioral activation strategies, and promotion of resumption of physical activity if there is a significant history of activity avoidance and subsequent deconditioning. The primary aim in coping skills training is to identify current maladaptive coping strategies (eg, catastrophizing, avoidance) that the patient is engaging in alongside their use of adaptive coping strategies (eg, use of positive self-statements, social support). As a cautionary note, the degree to which a strategy is adaptive or maladaptive and the perceived effectiveness of particular coping strategies varies from individual to individual.[41] Throughout treatment, problem-solving techniques are honed to aid patients in their adherence efforts and to help them increase their self-efficacy. Cognitive restructuring entails recognition of current maladaptive cognitions the patient is engaging in, challenging of the identified negative cognitions, and reformulation of thoughts to generate balanced, adaptive alternative thoughts. Through cognitive restructuring exercises, patients become increasingly adept at recognizing how their emotions, cognitions, and interpretations modulate their pain in positive and negative directions. As a result, it is presumed that the patients will attain a greater perception of control over their pain, be better able to manage their behavior and thoughts as they relate to pain, and be able to more adaptively evaluate the meaning they ascribe to their pain. Additional components sometimes included in a CBT intervention include social skills training, communication training, and broader approaches to stress management. Via a pain-oriented CBT intervention, many patients profit from improvements with regard to their emotional and functional well-being, and ultimately their global perceived health-related quality of life.
CBT interventions are delivered within a supportive and empathetic environment that strives to understand the patient�s pain from a biopsychosocial perspective and in an integrated manner. Therapists see their role as �teachers� or �coaches� and the message communicated to patients is that of learning to better manage their pain and improve their daily function and quality of life as opposed to aiming to cure or eradicate the pain. The overarching goal is to increase the patients� understanding of their pain and their efforts to manage pain and its sequelae in a safe and adaptive manner; therefore, teaching patients to self-monitor their behavior, thoughts, and emotions is an integral component of therapy and a useful strategy to enhance self-efficacy. Additionally, the therapist endeavors to foster an optimistic, realistic, and encouraging environment in which the patient can become increasingly skilled at recognizing and learning from their successes and learning from and improving upon unsuccessful attempts. In this manner, therapists and patients work together to identify patient successes, barriers to adherence, and to develop maintenance and relapse-prevention plans in a constructive, collaborative, and trustworthy atmosphere. An appealing feature of the cognitive behavioral approach is its endorsement of the patient as an active participant of his/her pain rehabilitation or management program.
Research has found CBT to be an effective treatment for chronic pain and its sequelae as marked by significant changes in various domains (ie, measures of pain experience, mood/affect, cognitive coping and appraisal, pain behavior and activity level, and social role function) when compared with wait-list control conditions.[42] When compared with other active treatments or control conditions, CBT has resulted in notable improvements, albeit smaller effects (effect size ~ 0.50), with regard to pain experience, cognitive coping and appraisal, and social role function.[42] A more recent meta-analysis of 52 published studies compared behavior therapy (BT) and CBT against treatment as usual control conditions and active control conditions at various time-points.[43] This meta-analysis concluded that their data did not lend support for BT beyond improvements in pain immediately following treatment when compared with treatment as usual control conditions.[43] With regard to CBT, they concluded that CBT has limited positive effects for pain disability, and mood; nonetheless, there are insufficient data available to investigate the specific influence of treatment content on selected outcomes.[43] Overall, it appears that CBT and BT are effective treatment approaches to improve mood; outcomes that remain robust at follow-up data points. However, as highlighted by several reviews and meta-analyses, a critical factor to consider in evaluating the effectiveness of CBT for the management of chronic pain is centered on issues of effective delivery, lack of uniform treatment components, differences in delivery across clinicians and treatment populations, and variability in outcome variables of interest across research trials.[13] Further complicating the interpretation of effectiveness findings are patient characteristics and additional variables that may independently affect treatment outcome.
Acceptance-Based Approaches
Acceptance-based approaches are frequently identified as third-wave cognitive-behavioral therapies. Acceptance and commitment therapy (ACT) is the most common of the acceptance-based psychotherapies. ACT emphasizes the importance of facilitating the client�s progress toward attaining a more valued and fulfilling life by increasing psychological flexibility rather than strictly focusing on restructuring cognitions.[44] In the context of chronic pain, ACT targets ineffective control strategies and experiential avoidance by fostering techniques that establish psychological flexibility. The six core processes of ACT include: acceptance, cognitive defusion, being present, self as context, values, and committed action.[45] Briefly, acceptance encourages chronic pain patients to actively embrace pain and its sequelae rather than attempt to change it, in doing so encouraging the patient to cease a futile fight directed at the eradication of their pain. Cognitive defusion (deliteralization) techniques are employed to modify the function of thoughts rather than to reduce their frequency or restructure their content. In this manner, cognitive defusion may simply alter the undesirable meaning or function of negative thoughts and thus decrease the attachment and subsequent emotional and behavioral response to such thoughts. The core process of being present emphasizes a non-judgmental interaction between the self and private thoughts and events. Values are utilized as guides for electing behaviors and interpretations that are characterized by those values an individual strives to instantiate in everyday life. Finally, through committed action, patients can realize behavior changes aligned with individual values. Thus, ACT utilizes the six core principles in conjunction with one another to take a holistic approach toward increasing psychological flexibility and decreasing suffering. Patients are encouraged to view pain as inevitable and accept it in a nonjudgmental manner so that they can continue to derive meaning from life despite the presence of pain. The interrelated core processes exemplify mindfulness and acceptance processes and commitment and behavior change processes.[45]
Results of research on the effectiveness of ACT-based approaches for the management of chronic pain are promising, albeit still warranting further evaluation. A RCT comparing ACT with a waitlist control condition reported significant improvements in pain catastrophizing, pain-related disability, life satisfaction, fear of movements, and psychological distress that were maintained at the 7 month follow-up.[46] A larger trial reported significant improvements for pain, depression, pain-related anxiety, disability, medical visits, work status, and physical performance.[47] A recent meta-analysis evaluating acceptance-based interventions (ACT and mindfulness-based stress reduction) in patients with chronic pain found that, in general, acceptance-based therapies lead to favorable outcomes for patients with chronic pain.[48] Specifically, the meta-analysis revealed small to medium effect sizes for pain intensity, depression, anxiety, physical wellbeing, and quality of life, with smaller effects found when controlled clinical trials were excluded and only RCTs were included in the analyses.[48] Other acceptance-based interventions include contextual cognitive-behavioral therapy and mindfulness-based cognitive therapy, though empirical research on the effectiveness of these therapies for the management of chronic pain is still in its infancy.
Expectations
An important and vastly overlooked common underlying element of all treatment approaches is consideration of the patient�s expectation for treatment success. Despite the numerous advances in the formulation and delivery of effective multidisciplinary treatments for chronic pain, relatively little emphasis has been placed on recognizing the importance of expectations for success and on focusing efforts on enhancement of patients� expectations. The recognition that placebo for pain is characterized by active properties leading to reliable, observable, and quantifiable changes with neurobiological underpinnings is currently at the vanguard of pain research. Numerous studies have confirmed that, when induced in a manner that optimizes expectations (via manipulation of explicit expectations and/or conditioning), analgesic placebos can result in observable and measurable changes in pain perception at a conscious self-reported level as well as a neurological pain-processing level.[49,50] Analgesic placebos have been broadly defined as simulated treatments or procedures that occur within a psychosocial context and exert effects on an individual�s experience and/or physiology.[51] The current conceptualization of placebo emphasizes the importance of the psychosocial context within which placebos are embedded. Underlying the psychosocial context and ritual of treatment are patients� expectations. Therefore, it is not surprising that the placebo effect is intricately embedded in virtually every treatment; as such, clinicians and patients alike will likely benefit from recognition that therein lies an additional avenue by which current treatment approaches to pain can be enhanced.
It has been proposed that outcome expectancies are core influences driving the positive changes attained through the various modes of relaxation training, hypnosis, exposure treatments, and many cognitive-oriented therapeutic approaches. Thus, a sensible approach to the management of chronic pain capitalizes on the power of patients� expectations for success. Regrettably, too often, health care providers neglect to directly address and emphasize the importance of patients� expectations as integral factors contributing to successful management of chronic pain. The zeitgeist in our society is that of mounting medicalization of ailments fueling the general expectation that pain (even chronic pain) ought to be eradicated through medical advancements. These all too commonly held expectations leave many patients disillusioned with current treatment outcomes and contribute to an incessant search for the �cure�. Finding the �cure� is the exception rather than the rule with respect to chronic pain conditions. In our current climate, where chronic pain afflicts millions of Americans annually, it is in our best interest to instill and continue to advocate a conceptual shift that instead focuses on effective management of chronic pain. A viable and promising route to achieving this is to make the most of patients� positive (realistic) expectations and educate pain patients as well as the lay public (20% of whom will at some future point become pain patients) on what constitutes realistic expectations regarding the management of pain. Perhaps, this can occur initially through current, evidence-based education regarding placebo and nonspecific treatment effects such that patients can correct misinformed beliefs they may have previously held. Subsequently clinicians can aim to enhance patients� expectations within treatment contexts (in a realistic fashion) and minimize pessimistic expectations that deter from treatment success, therefore, learning to enhance their current multidisciplinary treatments through efforts guided at capitalizing on the improvements placebo can yield, even within an �active treatment�. Psychologists can readily address these issues with their patients and help them become advocates of their own treatment success.
Emotional Concomitants of Pain
An often challenging aspect of the management of chronic pain is the unequivocally high prevalence of comorbid emotional distress. Research has demonstrated that depression and anxiety disorders are upward to three times more prevalent among chronic pain patients than among the general population.[52,53] Frequently, pain patients with psychiatric comorbidities are labeled �difficult patients� by healthcare providers, possibly diminishing the quality of care they will receive. Patients with depression have poorer outcomes for both depression and pain treatments, compared with patients with single diagnoses of pain or depression.[54,55] Psychologists are remarkably suited to address most of the psychiatric comorbidities typically encountered in chronic pain populations and thus improve pain treatment outcomes and decrease the emotional suffering of patients. Psychologists can address key symptoms (eg, anhedonia, low motivation, problem-solving barriers) of depression that readily interfere with treatment participation and emotional distress. Moreover, irrespective of a psychiatric comorbidity, psychologists can help chronic pain patients process important role transitions they may undergo (eg, loss of job, disability), interpersonal difficulties they may be encountering (eg, sense of isolation brought about by pain), and emotional suffering (eg, anxiety, anger, sadness, disappointment) implicated in their experience. Thus, psychologists can positively impact the treatment course by reducing the influence of emotional concomitants that are addressed as part of therapy.
Conclusion
Benefits of including psychological treatments in multidisciplinary approaches to the management of chronic pain are abundant. These include, but are not limited to, increased self-management of pain, improved pain-coping resources, reduced pain-related disability, and reduced emotional distress-improvements that are effected via a variety of effective self-regulatory, behavioral, and cognitive techniques. Through implementation of these changes, a psychologist can effectively help patients feel more in command of their pain control and enable them to live as normal a life as possible despite pain. Moreover, the skills learned through psychological interventions empower and enable patients to become active participants in the management of their illness and instill valuable skills that patients can employ throughout their lives. Additional benefits of an integrated and holistic approach to the management of chronic pain may include increased rates of return to work, reductions in health care costs, and increased health-related quality of life for millions of patients throughout the world.
Footnotes
Disclosure:No conflicts of interest were declared in relation to this paper.
In conclusion, psychological interventions can be effectively used to help relieve symptoms of chronic pain along with the use of other treatment modalities, such as chiropractic care. Furthermore, the research study above demonstrated how specific psychological interventions can improve the outcome measures of chronic pain management. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
According to statistics, approximately 80% of people will experience symptoms of back pain at least once throughout their lifetimes. Back pain is a common complaint which can result due to a variety of injuries and/or conditions. Often times, the natural degeneration of the spine with age can cause back pain. Herniated discs occur when the soft, gel-like center of an intervertebral disc pushes through a tear in its surrounding, outer ring of cartilage, compressing and irritating the nerve roots. Disc herniations most commonly occur along the lower back, or lumbar spine, but they may also occur along the cervical spine, or neck. The impingement of the nerves found in the low back due to injury and/or an aggravated condition can lead to symptoms of sciatica.
1.�Boris-Karpel S. Policy and practice issues in pain management. In: Ebert MH, Kerns RD, editors.�Behavioral and psychopharmacologic pain management.�New York: Cambridge University Press; 2010. pp. 407�433.
2.�Harstall C, Ospina M. How prevalent is chronic pain?�Pain: Clinical Updates.�2003;11(2):1�4.
4.�Abbot FV, Fraser MI. Use and abuse of over-the-counter analgesic agents.�J Psychiatry Neurosci.�1998;23(1):13�34.�[PMC free article]�[PubMed]
5.�Schappert SM, Burt CW. Ambulatory care visits to physician offices, hospital outpatient departments, and emergency departments: United States, 2001�02.�Vital Health Stat.�2006;13(159):1�66.�[PubMed]
6.�Joint Commission of Accreditation of Healthcare Organizations.�Pain assessment and management: an organizational approach.�Oakbrook, IL: 2000.
7.�Merskey H, Bogduk N, editors.�Classification of chronic pain.�2nd edition. Seattle, WA: IASP Press; 1994. Task Force on Taxonomy of the IASP Part III: Pain terms, a current list with definitions and notes on usage; pp. 209�214.
8.�Woessner J. A conceptual model of pain: treatment modalities.�Pract Pain Manag.�2003;3(1):26�36.
9.�Loeser JD. Economic implications of pain management.�Acta Anaesthesiol Scand.�1999;43(9):957�959.[PubMed]
10.�National Research Council.�Musculoskeletal disorders and the workplace: low back and upper extremities.�Washington, DC: National Academy Press; 2001.�[PubMed]
11.�US Bureau of the Census.�Statistical abstract of the United States: 1996.�116th edition. Washington, DC:
12.�Flor H, Fydrich T, Turk DC. Efficacy of multidisciplinary pain treatment centers: a meta-analytic review.�Pain.�1992;49(2):221�230.�[PubMed]
13.�McCracken LM, Turk DC. Behavioral and cognitive-behavioral treatment for chronic pain: outcome, predictors of outcome, and treatment process.�Spine.�2002;27(22):2564�2573.�[PubMed]
14.�Von Korff M, Saunders K. The course of back pain in primary care.�Spine.�1996;21(24):2833�2837.[PubMed]
15.�Melzack R, Wall PD. Pain mechanisms: a new theory.�Science.�1965;150(699):971�979.�[PubMed]
16.�Melzack R. Pain and stress: a new perspective. In: Gatchel RJ, Turk DC, editors.�Psychosocial factors in pain: critical perspectives.�New York: Guilford Press; 1999. pp. 89�106.
17.�Gatchel RJ. The conceptual foundations of pain management: historical overview. In: Gatchel RJ, editor.�Clinical essentials of pain management.�Washington, DC: American Psychological Association; 2005. pp. 3�16.
18.�Hoffman BM, Papas RK, Chatkoff DK, Kerns RD. Meta-analysis of psychological interventions for chronic low back pain.�Health Psychol.�2007;26(1):1�9.�[PubMed]
19.�Kerns RD, Sellinger J, Goodin BR. Psychological treatment of chronic pain.�Annu Rev Clin Psychol.�2010 Sep 27;�[Epub ahead of print]
20.�Yucha C, Montgomery D.�Evidence-based practice in biofeedback and neurofeedback.�Wheat Ridge, CO: AAPB; 2008.
21.�Nestoriuc Y, Martin A. Efficacy of biofeedback for migraine: a meta-analysis.�Pain.�2007;128(1�2):111�127.�[PubMed]
22.�Gardea MA, Gatchel RJ, Mishra KD. Long-term efficacy of biobehavioral treatment of temporomandibular disorders.�J Behav Med.�2001;24(4):341�359.�[PubMed]
23.�Turk DC, Monarch ES. Biopsychosocial perspective on chronic pain. In: Turk DC, Gatchel RJ, editors.�Psychosocial approaches to pain management: a practitioner�s handbook.�2nd edition. New York: Guilford Press; 2002. pp. 3�29.
24.�Philips HC.�The psychological management of chronic pain: a treatment manual.�New York: Springer Publishing; 1988. Orientation: chronic pain and the self-management approach; pp. 45�60.
25.�Bernstein DA, Borkovek TD.�Progressive muscle relaxation training: a manual for helping professions.Champaign, IL: Research Press; 1973.
26.�Linden W.�Autogenic training: a clinical guide.�New York: Guilford; 1990.
27.�Jamison RN.�Mastering chronic pain: a professional�s guide to behavioral treatment.�Sarasota, FL: Professional Resource Press; 1996.
28.�Baird CL, Sands L. Effect of guided imagery with relaxation on health-related quality of life in older women with osteoarthritis.�Res Nurs Health.�2006;29(5):442�451.�[PubMed]
29.�Carroll D, Seers K. Relaxation for the relief of chronic pain: a systematic review.�J Adv Nurs.�1998;27(3):476�487.�[PubMed]
30.�Morone NE, Greco CM. Mind-body interventions for chronic pain in older adults: a structured review.�Pain Med.�2007;8(4):359�375.�[PubMed]
31.�Mannix LK, Chandurkar RS, Rybicki LA, Tusek DL, Solomon GD. Effect of guided imagery on quality of life for patients with chronic tension-type headache.�Headache.�1999;39(5):326�334.�[PubMed]
32.�Skinner BF.�Science and human behavior.�New York: Free Press; 1953.
33.�Fordyce WE.�Behavioural methods for chronic pain and illness.�London, UK: The CV Mosby Company; 1976.
34.�Vlayen JW, Linton SJ. Fear-avoidance and its consequences in chronic musculoskeletal pain: a state of the art.�Pain.�2000;85(3):317�332.�[PubMed]
35.�Vlayen JW, de Jong J, Sieben J, Crombez G. Graded exposure�in vivo�for pain-related fear. In: Turk DC, Gatchel RJ, editors.�Psychosocial approaches to pain management: a practitioner�s handbook.�2nd edition. New York: Guilford Press; 2002. pp. 210�233.
36.�De Jong JR, Vlaeyen JW, Onghena P, Cuypers C, den Hollander M, Ruijgrok J. Reduction of pain-related fear in complex regional pain syndrome type I: the application of graded exposure in vivo.�Pain.�2005;116(3):264�275.�[PubMed]
37.�Boersma K, Linton S, Overmeer T, Jansson M, Vlaeyen J, de Jong J. Lowering fear-avoidance and enhancing function through exposure in vivo: a multiple baseline study across six patients with back pain.�Pain.�2004;108(1�2):8�16.�[PubMed]
38.�Bliokas VV, Cartmill TK, Nagy BJ. Does systematic graded exposure in vivo enhance outcomes in multidisciplinary chronic pain management groups?�Clin J Pain.�2007;23(4):361�374.�[PubMed]
39.�Leeuw M, Goossens ME, van Breukelen GJ, et al. Exposure in vivo versus operant graded activity in chronic low back pain patients: results of a randomized controlled trial.�Pain.�2008;138(1):192�207.[PubMed]
40.�George SZ, Zeppieri G, Cere AL, et al. A randomized trial of behavioral physical therapy interventions for acute and sub-acute low back pain (NCT00373867)�Pain.�2008;140(1):145�157.�[PMC free article][PubMed]
41.�Roditi D, Waxenberg LB, Robinson ME. Frequency and perceived effectiveness of coping define important subgroups of patients with chronic pain.�Clin J Pain.�2010;26(8):677�682.�[PubMed]
42.�Morley S, Eccleston C, Williams A. Systematic review and meta-analysis of randomized controlled trials of cognitive behaviour therapy and behaviour therapy for chronic pain in adults, excluding headache.�Pain.�1999;80(1�2):1�13.�[PubMed]
43.�Eccleston C, Williams AC, Morley S. Psychological therapies for the management of chronic pain (excluding headache) in adults.�Cochrane Database Syst Rev.�2009;(2):CD007407.�[PubMed]
44.�Blackledge JT, Hayes SC. Emotion regulation in acceptance and commitment therapy.�J Clin Psychol.�2001;57(2):243�255.�[PubMed]
45.�Hayes SC, Luoma JB, Bond FW, Masuda A, Lillis J. Acceptance and commitment therapy: model, processes, and outcomes.�Behav Res Ther.�2006;44(1):1�25.�[PubMed]
46.�Wicksell RK, Ahlqvist J, Bring A, Melin L, Olsson GL. Can exposure strategies improve functioning and life satisfaction in people with chronic pain and whiplash-associated disorders (WAD)? A randomized controlled trial.�Cogn Behav Ther.�2008;37(3):169�182.�[PubMed]
47.�Vowles KE, McCracken LM. Acceptance and values-based action in chronic pain: a study of treatment effectiveness and process.�J Consult Clinl Psychol.�2008;76(3):397�407.�[PubMed]
48.�Veehof MM, Oskam MJ, Schreurs KMG, Bohlmeijer ET. Acceptance-based interventions for the treatment of chronic pain: a systematic review and meta-analysis.�Pain.�2011;152(3):533�542.�[PubMed]
49.�Wager TD, Rilling JK, Smith EE, et al. Placebo-induced changes in�f�MRI in the anticipation and experience of pain.�Science.�2004;303(5661):1162�1167.�[PubMed]
50.�Price DD, Craggs J, Verne GN, Perlstein WM, Robinson ME. Placebo analgesia is accompanied by large reductions in pain-related brain activity in irritable-bowel syndrome patients.�Pain.�2007;127(1�2):63�72.�[PubMed]
51.�Price D, Finniss D, Benedetti F. A comprehensive review of the placebo effect: recent advances and current thought.�Annu Rev Psychol.�2008;59:565�590.�[PubMed]
52.�Holroyd KA. Recurrent headache disorders. In: Dworkin RH, Breitbart WS, editors.�Psychosocial aspects of pain: a handbook for health care providers.�Seattle, WA: IASP Press; 2004. pp. 370�403.
53.�Fishbain DA. Approaches to treatment decisions for psychiatric comorbitity in the management of the chronic pain patient.�Med Clin North Am.�1999;83(3):737�760.�[PubMed]
54.�Bair MJ, Robinson RL, Katon W, Kroenke K. Depression and pain comorbidity � a literature review.�Arch Intern Med.�2003;163(20):2433�2445.�[PubMed]
55.�Poleshuck EL, Talbot NL, Su H, et al. Pain as a predictor of depression treatment outcomes in women with childhood sexual abuse.�Compr Psychiatry.�2009;50(3):215�220.�[PMC free article]�[PubMed]
Psychological therapy, also known as psychotherapy, refers to the use of psychological methods to help change an individual’s way of thinking as well as improve their coping skills in order for them to learn how to best deal with stress. Psychological therapies have widely been utilized as a part of the multidisciplinary management of chronic pain. Common psychotherapies include, cognitive-behavioral therapy, mindfulness-based stress reduction and even chiropractic care. The connection between the mind and the body in relation to disease and illness have long been discussed in many research studies.
Evidence-based research studies have demonstrated that proper stress management through the use of psychological therapy as well as mindfulness interventions can effectively benefit patients with chronic pain. By way of instance, chiropractic care can safely and effectively help reduce stress, anxiety and depression by correcting spinal misalignments, or subluxation. A balanced spine can improve mood and mental health. Chiropractic care can include lifestyle modifications, such as nutritional advice, physical activity and exercise recommendations, and promote better sleeping habits, to further enhance the benefits of the treatment. The purpose of the following article is to demonstrate how psychological therapies impact the management of chronic pain.
Psychological Therapies for the Management of Chronic Pain
Abstract
Pain is a complex stressor that presents a significant challenge to most aspects of functioning and contributes to substantial physical, psychological, occupational, and financial cost, particularly in its chronic form. As medical intervention frequently cannot resolve pain completely, there is a need for management approaches to chronic pain, including psychological intervention. Psychotherapy for chronic pain primarily targets improvements in physical, emotional, social, and occupational functioning rather than focusing on resolution of pain itself. However, psychological therapies for chronic pain differ in their scope, duration, and goals, and thus show distinct patterns of treatment efficacy. These therapies fall into four categories: operant-behavioral therapy, cognitive-behavioral therapy, mindfulness-based therapy, and acceptance and commitment therapy. The current article explores the theoretical distinctiveness, therapeutic targets, and effectiveness of these approaches as well as mechanisms and individual differences that factor into treatment response and pain-related dysfunction and distress. Implications for future research, dissemination of treatment, and the integration of psychological principles with other treatment modalities are also discussed.
Chiropractic care is an alternative treatment option which utilizes spinal adjustments and manual manipulations to treat injuries and/or conditions associated with the musculoskeletal and nervous system. Chiropractic treatment primarily focuses on spinal health, however, because the spine is the root of the nervous system, chiropractic care can also be effectively used to treat a variety of mental health issues. As a chiropractor, I make sure to focus on the body as a whole, rather than treating the symptoms of a single injury and/or condition. The truth of the matter is, chiropractic treatment must also deal with the emotional component of each health issue in order to provide overall relief. Psychosomatic disorders, refers to a physical illness caused or aggravated by a mental factor, such as stress. Chiropractic care can be utilized as a psychological therapy, in which, a chiropractor may recommend a series of lifestyle modifications to help reduce stress, anxiety and depression, together with spinal adjustments and manual manipulations to reduce symptoms associated with mental health issues. Furthermore, the understanding of the connection between the mind and body is essential in chiropractic treatment towards overall health and wellness.
Introduction to the Non-Pharmacological Treatment of Pain
Pain is an essential biological function that signals disturbance or damage in the body, prevents further harm through overuse of the afflicted area, and promotes physiological homeostasis.[1] Whether through abnormal healing, additional bodily damage, or failed medical intervention, pain may become chronic. Chronic pain no longer signals damage to the body and is instead a detriment to the physical and psychological well-being of the sufferer. Unfortunately, medical intervention frequently cannot resolve chronic pain, resulting in increased need for management approaches to pain, as is the approach to other chronic medical conditions.[2] In recent years, the biopsychosocial model has informed research and intervention in pain psychology, wherein physical, cognitive, affective, and interpersonal factors are used to inform treatment.[2] Currently, psychological interventions for chronic pain target a variety of domains, including physical functioning, pain medication use, mood, cognitive patterns, and quality of life, while changes in pain intensity may be secondary.[3] As such, psychological interventions for pain are ideally suited as complementary treatments to medical treatment.[4] In order to articulate the distinct philosophies and effects of each psychological intervention, it is important to first consider the variety of ways that pain affects psychological functioning.
Psychological Reactions to Pain
Recurrent pain may contribute to development of maladaptive cognitions and behavior that worsen daily functioning, increase psychiatric distress, or prolong the experience of pain.[5] Individuals suffering from chronic pain tend to show increased vulnerability to a variety of psychiatric conditions, including depressive disorders,[6] anxiety disorders,[7] and posttraumatic stress disorder.[7] However, the relationship between depression and pain is likely bidirectional, as the presence of a major depressive disorder has been identified as a key risk factor in the transition from acute pain to chronic pain.[8] Additionally, individuals with pain may suffer from significant anxiety and depressive symptomatology that does not reach the severity of a clinical diagnosis.[9] Further, chronic pain negatively impacts quality of life[10] and contributes to higher levels of disability.[10] Individuals with chronic pain are also vulnerable to higher rates of obesity,[11] sleep disturbance,[12] and fatigue,[13] show greater rates of medical utilization,[10] and are vulnerable to problematic pain medication use.[14] Given the negative psychological consequences of chronic pain, it is worthwhile to consider three psychological mechanisms related to pain-related distress that have proven to be suitable targets for intervention: pain catastrophizing, fear of pain, and pain acceptance.
Pain catastrophizing is defined as a negative cognitive and affective mental set related to expected or actual pain experience.[15] Pain catastrophizing is characterized by magnification of the negative effects of pain, rumination about pain, and feelings of helplessness in coping with pain.[16] Pain catastrophizing has been associated with various forms of dysfunction, including increased rates of depression[17] and anxiety,[16] greater functional impairment and disability due to pain,[17] and lower overall quality of life.[18] Individuals who catastrophize about their pain report lower levels of perceived control over pain,[19] poorer emotional and social functioning,[20] and poorer responses to medical intervention.[21] Pain catastrophizing also contributes to poorer pain coping and overall functioning, making pain catastrophizing a viable target for psychological intervention. Addressing catastrophic thoughts about pain improves physical and psychological functioning in the short term[22] and improves the likelihood of returning to work despite the presence of persistent pain.[23]
Pain-related fear is another psychological mechanism that has significant implications for physical and psychological functioning in chronic pain. Pain-related fear reflects a fear of injury or worsening of one�s physical condition through activities that may trigger pain.[24] Pain-related fear is associated with increased pain intensity[25] and increased disability.[26] Pain-related fear contributes to disability by fostering passive or avoidant pain-coping behaviors that contribute to physical deconditioning and pain.[27] If left unaddressed, fear of pain can impair gains in physical rehabilitation settings.[28] Evidence suggests that pain catastrophizing precedes pain-related fear,[24] but both of these mechanisms uniquely contribute to pain and physical disability.[5,29]
Recently, there has been increased attention to the psychological flexibility model, which extends the fear-avoidance model of chronic pain and proposes to improve treatment outcomes through fostering of accepting attitudes towards pain.[30] Psychological flexibility has been defined as an ability to engage in the present moment in a way that allows the individual to either maintain or adjust his or her behavior in the way that is most consistent with internally held goals and values;[31] this idea is especially important in times of greater pain, given the narrowing of focus that is common during times of pain.[32] Similar to psychological acceptance, which fosters a nonjudgmental approach to distressing thoughts and emotions, pain acceptance is defined as a process of nonjudgmentally acknowledging pain, stopping maladaptive attempts to control pain, and learning to live a richer life in spite of pain.[33] Pain acceptance influences emotional functioning through two distinct mechanisms: a willingness to experience pain, which buffers against negative emotional reactions to pain, and continued engagement in valued activities despite the presence of pain, which bolsters positive emotions.[34] Acceptance of pain is theorized to uncouple the occurrence of catastrophic thoughts about pain from subsequent emotional suffering[35] and reduces reliance on control- or avoidance-based coping,[36] thereby freeing cognitive and emotional resources for more meaningful pursuits.[33] Pain acceptance has demonstrated positive associations with cognitive, emotional, social, and occupational functioning in chronic pain populations.[36] Acceptance of pain predicts lower levels of pain catastrophizing[37] and greater levels of positive affect, which in turn reduce the association between pain intensity and negative emotions.[38] Pain acceptance is a particularly salient target for intervention in mindfulness- and acceptance-based therapies for chronic pain, which will be discussed later (see Table 1).
Table 1: Descriptions of psychological therapies for pain.
Psychological Intervention as an Approach to Pain Management
Operant Behavioral Approaches
Fordyce[39] proposed a behavioral model of pain adaptation in which maladaptive behavioral responses to pain develop through contingent relief from pain or pain-related fear. According to this theory, a behavioral drive to avoid pain leads individuals to avoid behaviors that are painful but maintain their physical and emotional health; this avoidance contributes to the development and maintenance of pain chronicity, deconditioning, and depression.[40] Operant therapy for chronic pain utilizes reinforcement and punishment contingencies to reduce pain-related behaviors and foster more adaptive behaviors, including graded patterns of activity, activity pacing, and time-contingent medication management.[40] Behavioral therapy for pain has shown positive effects on a variety of domains, including pain experience, mood, negative cognitive appraisals, and functioning in social roles.[3]
A recent application of learning theory to chronic pain involves in vivo exposure treatment for pain-related fear, which focuses on decreasing the perceived harmfulness of physical activity.[41] Learning theory posits that the aversive signal of pain may be passed to neutral stimuli (like physical movement behaviors), which contributes to avoidant behavior. In vivo exposure therapy extinguishes threat, fear, and behavioral avoidance through progressively increasing engagement in painful behaviors in the absence of catastrophic outcomes; when these behaviors are performed without serious negative consequences, patients may realize that their expectations about the consequences of physical movement and pain are unrealistic.[24,42] Consistent with exposure treatments for phobias and other anxiety disorders, in vivo exposure treatment for fear of pain involves development of a personalized, graded hierarchy of activities that elicit a fearful response, psychoeducation related to pain, fear, and behavior, and ultimately slow and systematic exposure to activities related to the individual�s fear hierarchy.[41] In vivo exposure treatment for pain-related fear has demonstrated efficacy in improving pain, pain catastrophizing, and functional disability,[41] and in decreasing pain-related fear and anxiety, depression, and anxiety.[43] Exclusively behavioral approaches to pain have been less prevalent in recent years but have demonstrated efficacy in lower back pain samples, among others (see Table 2). The effects of in vivo exposure on functional disability appear to be mediated by decreased catastrophizing and perceived harmfulness of activity[41] but may be differentially effective for patients of differing baseline levels of functionality.[40]
Table 2: Demonstrated efficacy of psychological interventions by pain population.
Cognitive-Behavioral Therapy
Cognitive-behavioral therapy (CBT) adopts a biopsychosocial approach to the treatment of chronic pain by targeting maladaptive behavioral and cognitive responses to pain and social and environmental contingencies that modify reactions to pain.[44] CBT principles have demonstrated efficacy for a variety of psychiatric disorders and physical illnesses, in addition to pain.[45] CBT for pain develops coping skills intended to manage pain and improve psychological functioning, including structured relaxation, behavioral activation and scheduling of pleasurable events, assertive communication, and pacing of behavior in order to avoid prolongation or exacerbation of pain flares. Unlike operant-behavioral approaches, CBT for pain also addresses maladaptive beliefs about pain and pain catastrophizing through formal use of cognitive restructuring: identification and replacement of unrealistic or unhelpful thoughts about pain with thoughts that are oriented towards adaptive behavior and positive functioning.[44] CBT for pain has been widely implemented as a standard treatment for pain and constitutes the current �gold standard� for psychological intervention for pain.[44]
According to recent meta-analytic studies,[45] CBT for pain demonstrates small-to-medium effect sizes in a variety of domains and shows effects on pain and functioning comparable to standard medical care for pain.[3] CBT significantly improves disability and pain catastrophizing after treatment and yields longer-term improvements in disability, above and beyond the effects of usual medical care,[3] as well as smaller effects on pain, catastrophizing, and mood when compared to no treatment.[3] CBT-related changes in helplessness and catastrophizing are uniquely predictive of later changes in pain intensity and pain-related interference in daily functioning.[22] CBT is also a valuable adjunct treatment in physical rehabilitation programs.[46] The benefits of CBT for pain have been noted in many chronic pain populations (see Table 2) but may not be as robust in some populations, including fibromyalgia.[47] Further, some have suggested that the effects of CBT are at best moderately sized and not maintained long-term.[30] The intractable nature of chronic pain may make adaptation difficult as attempts to control pain may prove ineffectual, ultimately contributing to greater psychological distress.[36] Recent efforts have thus expanded the cognitive-behavioral model of pain intervention to address these issues, which has yielded two newer treatment modalities: mindfulness-based stress reduction (MBSR) and acceptance and commitment therapy (ACT). Unlike CBT, these approaches focus on fostering acceptance of chronic pain rather than emphasizing strategies for controlling pain, thereby improving emotional well-being and greater engagement in nonpain-related pursuits. Though these interventions both target acceptance of pain, they differ in their therapeutic implementation and approach to meditation and daily practice.
Mindfulness-Based Stress Reduction
Mindfulness-based interventions approach seeks to uncouple the sensory aspects of pain from the evaluative and emotional aspects of pain,[48] and promote detached awareness of the somatic and psychological sensations within the body.[48] As the chronic pain signal often cannot be extinguished, this detachment may enhance individual responses to chronic pain.[48] Through mindful awareness and meditation, thoughts about pain can be viewed as discrete events rather than an indication of an underlying problem that necessitates immediate and possibly maladaptive responses.[49] An individual may then recognize these sensations or thoughts as something familiar, which may serve to ameliorate emotional or maladaptive behavioral responses to pain.
MBSR is a form of meditation developed in Eastern philosophy and later adapted to Western intervention that enhances awareness and acceptance of physical, cognitive, and emotional states and disconnects psychological reactions from the uncontrollable experience of pain flares.[44] MBSR interventions have traditionally been structured as 2-hour sessions occurring weekly over 10 weeks that develop awareness of the body and proprioceptive signals, awareness of the breath and physical sensations, and development of mindful activities (such as eating, walking, and standing).[48] MBSR promotes mindfulness through daily meditation, which is a requisite component of the treatment.[50] The mechanisms underlying effective MBSR intervention may be similar to desensitization to pain, as meditations involve motionless sitting practices that expose participants to painful sensations in the absence of catastrophic consequences.[48,50] In this way, MBSR interventions may function similarly to in vivo exposure for pain but serve the additional purpose of increasing tolerance for negative emotions, thereby fostering more adaptive responses to pain.[50] MBSR also reduces rumination[51] and interoception of distressing physical signals[52] and increases mindful awareness[51] and acceptance of pain.[53] MBSR necessitates cultivation of daily mindfulness practices,[48] yet compliance rates of MBSR have been found to compare favorably to behavioral pain management techniques.[54] However, evidence on the importance of daily practice is mixed; the amount of time devoted to these mindful activities correlates with symptom improvement in some studies,[55] yet compliance rates appear to correlate only modestly with improvement in others.[54] Unlike CBT, which identifies thoughts as distorted and in need of change, practitioners of mindfulness adopt a nonjudgmental approach to thoughts as �discrete events� that encourage emotional distance from thoughts.[44,50] Further, CBT is a goal-oriented treatment modality, targeting an increased relaxation response or an altered behavioral or thought response, whereas mindfulness does not prescribe specific goals, relying instead on nonjudgmental observation.[50] Further, mindfulness instructors are expected to engage in their own daily mindfulness practices, whereas CBT practitioners do not necessarily need daily practice in CBT to teach it effectively.[50]
MBSR has demonstrated efficacy in addressing the severity of medical symptoms and psychological symptoms,[48] pain intensity,[56] and coping with stress and pain;[54] these treatment gains may last up to 4 years after intervention in many domains.[54] MBSR has been effective in diverse pain samples,[48,54,56] and in individuals with irritable bowel syndrome,[52] neck pain,[57] migraine,[57] fibromyalgia,[58] and chronic musculoskeletal pain.[59] Additionally, MBSR addresses co-occurring symptoms of depression in individuals with some chronic pain conditions like fibromyalgia[60] and enhances the effects of multidisciplinary treatment on disability, anxiety, depression, and catastrophizing.[61] Meta-analytic studies of MBSR in chronic pain have shown small to moderate effects of MBSR on anxiety, depression, and psychological distress in patients with chronic illnesses including pain,[62] and these benefits tend to be robust across studies.[63] However, as with CBT, MBSR may be differentially effective across populations; a recent longitudinal study noted greater improvements in pain, health-related quality of life, and psychological well-being for back or neck pain than in fibromyalgia, chronic migraine, or headache.[57]
Acceptance and Commitment Therapy
ACT adopts a theoretical approach that thoughts do not need to be targeted or changed; instead, responses to thoughts may be altered so that their negative consequences are minimized.[31] ACT interventions improve well-being through nonjudgmental and purposeful acknowledgment of mental events (ie, thoughts and emotions), fostering acceptance of these events, and increasing the ability of the individual to remain present and aware of personally relevant psychological and environmental factors; in doing so, individuals are able to adjust their behavior in a way that is consistent with their goals or values, rather than focusing on immediate relief from thoughts and emotions.[31] In the treatment of pain, ACT fosters purposeful awareness and acceptance of pain, thereby minimizing the focus on reducing pain or thought content and instead directing efforts towards fulfilling behavioral functioning.[44] ACT shares conceptual similarity with MBSR due to shared goals of promoting mindfulness and acceptance of pain but, unlike MBSR, ACT does not utilize daily mindful meditation and instead focuses on identification of the values and goals of the individual, which serve to direct behavior.[64] ACT-based interventions have demonstrated benefits on various aspects of mental health in chronic pain populations, including mental health quality of life, self-efficacy, depression, and anxiety.[65] Some studies of ACT interventions for chronic pain have reported medium or larger effect sizes for improvements in pain-related anxiety and distress, disability, number of medical visits, current work status, and physical performance,[66,67] with smaller effects of this intervention noted on pain and depression.[64] However, meta-analytic studies of acceptance-based therapies for pain have revealed that ACT does not show incrementally greater efficacy in comparison to other established psychological treatments for chronic pain.[64]
Future Directions and Remaining Questions
The extant literature suggests that each of the previously reviewed psychological interventions has retained value for the treatment of chronic pain. At present, there is little evidence of the superiority of any treatment approach, with one exception: CBT has demonstrated incrementally greater benefit in many areas than the effects of behavioral therapy.[3] As previously noted, however, operant-behavioral principles have been adopted for newer treatment approaches like in vivo exposure for fear of pain, which has demonstrated good benefit in multidisciplinary treatment with some pain populations.[41] Recent reviews have concluded that MBSR and ACT are promising but yield generally comparable effects to CBT, despite their distinct intervention methods.[64] The ability to draw conclusions regarding treatment superiority is further limited by the smaller number of high-quality studies of ACT or MBSR compared to the more robust CBT literature.[64]
Some critical questions remain regarding the comparative effectiveness of these interventions. First, the effects of CBT are significant in the short term but are not consistently maintained across time, possibly due to decreased adherence.[3] It is conceivable that acceptance-based approaches, which are predicated less on mechanistic coping strategies and instead foster accepting attitudes towards pain, may show greater rates of long-term adherence and longer-term benefits than CBT, though future study of this question is needed. Further, some pain disorders (such as fibromyalgia) have shown comparatively poorer treatment response to CBT than other pain disorders in some studies, which highlights the possible benefit of alternative interventions in such populations. Indeed, ACT and MBSR have also shown efficacy in fibromyalgia populations, though there remains a need to identify predictors of differential treatment response.[65]
Safety and Tolerability of Psychological Therapies
Psychological therapies for pain are presumed to be at low risk for adverse effects to the recipient; as a result, there is a dearth of empirical evidence regarding the risks of psychological interventions.[68] Some have suggested that patients who enter psychological treatment face risks of incorrect psychological diagnosis, psychological dependence, undermining of a patient�s ability to make their own decisions, or manipulation by the therapist to achieve nontherapeutic goals.[69,70] However, these concerns are alleviated through proper clinical and ethical training of practitioners and are not typically considered salient risks of psychological therapies when they are properly administered.[70] Recently, there has been a call for additional research to address the possibility of adverse psychotherapeutic effects[71] as well as a more systematic method of monitoring and identifying adverse events related to psychotherapy.[68] Though the rates of adverse effects of psychotherapy are still largely unknown, it is encouraging that recent studies have begun to specifically report the incidence of adverse events directly.[72]
Factors Affecting the Outcomes of Psychological Intervention
Practitioners should be cautioned against the assumption of homogeneity among patients with pain disorders, as a variety of factors may predict treatment response.[69,71] Turk[73] proposed that individuals coping with comparable levels of pain show distinct patterns of response that could be clustered into recognizable subclasses: �dysfunctional� patients, who report high levels of pain-related interference and distress; �interpersonally distressed� patients, who report lacking the support of loved ones in coping with their pain; and �adaptive copers,� who report notably higher levels of function and perceived social support and lower levels of pain-related dysfunction. Turk proposed that these patient subgroups respond differently to psychological intervention, and subsequent findings have supported this idea: �dysfunctional� patients have demonstrated greater response to interdisciplinary treatment involving psychological care than �interpersonally distressed� patients.[74] Identification of patient subgroups may be accomplished using instruments like the Multidisciplinary Pain Inventory[75] and through detailed assessment of chronic pain intensity and disability.[76] Additionally, patients� readiness to adopt a self-management approach to their own chronic pain appears to have significant implications for treatment response;[77] patients who are in the precontemplation stage of treatment readiness may benefit more from insight-focused therapy, versus those in an action stage, who may benefit more from establishing relaxation-based and other active coping strategies.[77] Patient readiness to self-manage pain may be assessed using the Pain Stages of Change Questionnaire.[77] Additionally, treatment response may be subject to patient beliefs about the importance of intervention-specific behaviors and about one�s own ability to perform these actions.[78]
Additionally, there may be demographic, psychological, and medical differences among patients that are relevant to treatment response, including the etiology of pain conditions, socioeconomic status, and cultural and ethnic background; these factors require further empirical research in order to optimize clinical outcomes but have not yet received adequate attention in the clinical literature.[79] For example, baseline levels of physical functioning appear to predict response to certain psychological treatment modalities like in vivo exposure for fear of pain.[40] Further, baseline levels of pain, depression, and anxiety have been found to predict dropout rates in some samples,[80,81] though these effects are not apparent in all samples.[3] In addition to being an important mechanism of treatment, there is evidence that baseline levels of fear of pain may also predict differential treatment response; individuals more fearful of pain at the outset of a multidisciplinary pain treatment program showed greater responsiveness to in vivo exposure for this problem.[28] The presence of medical comorbidities that are likely to impact future functioning is also important to consider; recently, psychological interventions have been developed that address comorbid symptoms of sleep,[82] obesity,[29] and fatigue[83] that may accompany chronic pain. Hybrid treatments may be more important in independent clinical practice, where comorbidity is more common.[82] Notably, there is little evidence that personality variables factor significantly into treatment response; most of the connections between personality traits and variables relevant to psychological intervention for pain are theoretical and have not consistently emerged in empirical research.[84,85]
Patient age is also an important consideration in examining responses to interventions for pain. Older adults have increased risks of various ailments related to pain, including arthritis and osteoporosis, but may have poor tolerance to medications for these conditions.[86] Further, age may alter psychological reactions to pain; the emotional aspects of pain are more strongly correlated with pain catastrophizing in younger adults than older adults while sensory aspects of pain appear more strongly related to pain catastrophizing in older adults.[87] Additionally, treatment protocols may require accommodation for elderly populations; addressing an elderly patient�s fear of movement may be complicated by a fear of falling that is absent in younger populations.[88] As memory concerns are more common in older adulthood, treatment protocols may be improved if they minimize the demand for memorized tasks.[89] Unfortunately, research is lacking for specific psychological interventions in elderly populations.[86] In general, psychological interventions are presumed to be of low risk for older adults,[90] and CBT for pain has received comparatively greater empirical support for older adults.[88] Overall, the efficacy of psychological intervention for pain in older adults is an area that warrants additional study in the future.
Treatment availability is a key consideration for psychological intervention, especially for patients in poverty or living in remote geographical locations. Though it is beyond the scope of this paper to review ethnic and socioeconomic contributors to health, low socioeconomic status is a significant risk factor for the development of chronic pain and factors heavily into racial disparities in health outcomes.[91] As financial challenges may restrict access to traditional psychological interventions, the importance of alternative modalities for provision of mental health interventions for chronic pain is paramount. Teleinterventions[92] and Internet-based interventions[93] may be viable for psychological treatment of chronic pain; Internet-based programs delivering ACT,[94] CBT,[46] and mindfulness interventions[95] have demonstrated benefits in psychosocial functioning, mood, and pain coping. However, methodologically rigorous clinical trials and evidence for maximally effective and efficient implementation of these programs are needed, as many interventions have shown modest effects and comparatively high dropout rates.[96]
Combining psychological treatment modalities with one another and with other medical interventions may constitute the next logical step in enhancing treatment outcomes. Institution of a flexible, goal-oriented approach, akin to ACT, may enhance engagement and adherence in CBT.[97] Additionally, a combination of graded in vivo exposure and ACT may show incremental benefit in addressing pain-related fear and anxiety.[98] Effects of CBT may also be enhanced in conjunction with treatments like biofeedback[99] and hypnosis.[100] A word of caution: presentation of psychological treatment by nontraditional practitioners may show variable effectiveness unless treatment approaches are adjusted appropriately.[101] If trained properly, however, appropriately-designed cognitive-behavioral interventions can be effectively administered by physiotherapists,[102] physical therapists,[103] nurses, and occupational therapists.[104]
Conclusion
Psychotherapy constitutes a valuable modality for addressing the behavioral, cognitive, emotional, and social factors that both result from and contribute to pain-related dysfunction and distress through enhancement of self-management strategies. There are several distinct psychological interventions that differ in their theoretical approaches, therapeutic targets, and areas of efficacy, but CBT, ACT, MBSR, and operant behavioral approaches to pain may all play important roles for enhancing the self-management abilities of individuals with chronic pain. However, there remains a need to identify predictors of differential treatment response and salient patient subgroups to optimize treatment outcomes, as well as additional and alternative means to provision of psychological services for those who are unwilling or unable to engage in traditional psychotherapy. More empirical research into contributing factors of differential treatment response and the dissemination of psychological treatment for pain may result in significant savings to the physical, emotional, and financial costs of chronic pain.
Footnotes
Disclosure:�The author reports no conflicts of interest in this work.
In conclusion, psychological therapies, such as cognitive-behavioral therapy, mindfulness-based stress reduction and even chiropractic care, have been demonstrated to effective help treat chronic pain, according to research studies. The connection between the mind and body has previously been referenced as a cause for a variety of health issues, including chronic pain. Finally, the article above demonstrated the effects of psychological therapy for chronic pain management. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
According to statistics, approximately 80% of people will experience symptoms of back pain at least once throughout their lifetimes. Back pain is a common complaint which can result due to a variety of injuries and/or conditions. Often times, the natural degeneration of the spine with age can cause back pain. Herniated discs occur when the soft, gel-like center of an intervertebral disc pushes through a tear in its surrounding, outer ring of cartilage, compressing and irritating the nerve roots. Disc herniations most commonly occur along the lower back, or lumbar spine, but they may also occur along the cervical spine, or neck. The impingement of the nerves found in the low back due to injury and/or an aggravated condition can lead to symptoms of sciatica.
1.�Craig AD. A new view of pain as a homeostatic emotion.�Trends Neurosci.�2003;26(6):303�307.[PubMed]
2.�Gatchel RJ. Comorbidity of chronic pain and mental health disorders: the biopsychosocial perspective.�Am Psychol.�2004;59(8):795�805.�[PubMed]
3.�Williams AC, Eccleston C, Morley S. Psychological therapies for the management of chronic pain (excluding headache) in adults.�Cochrane Database Syst Rev.�2012;11:CD007407.�[PubMed]
4.�Turk DC, Audette J, Levy RM, Mackey SC, Stanos S. Assessment and treatment of psychosocial comorbidities in patients with neuropathic pain.�Mayo Clin Proc.�2010;85(Suppl 3):S42�S50.[PMC free article]�[PubMed]
5.�Thibault P, Loisel P, Durand MJ, Catchlove R, Sullivan MJ. Psychological predictors of pain expression and activity intolerance in chronic pain patients.�Pain.�2008;139(1):47�54.�[PubMed]
6.�Bair MJ, Robinson RL, Katon W, Kroenke K. Depression and pain comorbidity: a literature review.�Arch Intern Med.�2003;163(20):2433�2445.�[PubMed]
7.�McWilliams LA, Cox BJ, Enns MW. Mood and anxiety disorders associated with chronic pain: an examination in a nationally representative sample.�Pain.�2003;106(1�2):127�133.�[PubMed]
8.�Young Casey C, Greenberg MA, Nicassio PM, Harpin RE, Hubbard D. Transition from acute to chronic pain and disability: a model including cognitive, affective, and trauma factors.�Pain.�2008;134(1�2):69�79.[PubMed]
9.�Geenen R, Newman S, Bossema ER, Vriezekolk JE, Boelen PA. Psychological interventions for patients with rheumatic diseases and anxiety or depression.�Best Pract Res Clin Rheumatol.�2012;26(3):305�319.[PubMed]
10.�Winkelmann A, Perrot S, Schaefer C, et al. Impact of fibromyalgia severity on health economic costs: results from a European cross- sectional study.�Appl Health Econ Health Policy.�2011;9(2):125�136.[PubMed]
11.�Wright LJ, Schur E, Noonan C, Ahumada S, Buchwald D, Afari N. Chronic pain, overweight, and obesity: findings from a community-based twin registry.�J Pain.�2010;11(7):628�635.�[PMC free article][PubMed]
12.�Smith MT, Haythornthwaite JA. How do sleep disturbance and chronic pain inter-relate? Insights from the longitudinal and cognitive- behavioral clinical trials literature.�Sleep Med Rev.�2004;8(2):119�132.[PubMed]
13.�Kato K, Sullivan PF, Eveng�rd B, Pedersen NL. Chronic widespread pain and its comorbidities: a population-based study.�Arch Intern Med.�2006;166(15):1649�1654.�[PubMed]
14.�Richardson LP, Russo JE, Katon W, et al. Mental health disorders and long-term opioid use among adolescents and young adults with chronic pain.�J Adolesc Health.�2012;50(6):553�558.�[PMC free article][PubMed]
15.�Sullivan MJ, Thorn B, Haythornthwaite JA, et al. Theoretical perspectives on the relation between catastrophizing and pain.�Clin J Pain.�2001;17(1):52�64.�[PubMed]
16.�Sullivan MJL, Bishop SR, Pivik J. The pain catastrophizing scale: development and validation.�Psychol Assess.�1995;7(4):524�532.
17.�Keefe FJ, Brown GK, Wallston KA, Caldwell DS. Coping with rheumatoid arthritis pain: catastrophizing as a maladaptive strategy.�Pain.�1989;37(1):51�56.�[PubMed]
18.�Wollaars MM, Post MW, van Asbeck FW, Brand N. Spinal cord injury pain: the influence of psychologic factors and impact on quality of life.�Clin J Pain.�2007;23(5):383�391.�[PubMed]
19.�Crisson JE, Keefe FJ. The relationship of locus of control to pain coping strategies and psychological distress in chronic pain patients.�Pain.�1988;35(2):147�154.�[PubMed]
20.�Hamilton NA, Karoly P, Zautra AJ. Health goal cognition and adjustment in women with fibromyalgia.�J Behav Med.�2005;28(5):455�466.�[PubMed]
21.�Mankovsky T, Lynch M, Clark A, Sawynok J, Sullivan MJ. Pain catastrophizing predicts poor response to topical analgesics in patients with neuropathic pain.�Pain Res Manag.�2012;17(1):10�14.[PMC free article]�[PubMed]
22.�Burns JW, Glenn B, Bruehl S, Harden RN, Lofland K. Cognitive factors influence outcome following multidisciplinary chronic pain treatment: a replication and extension of a cross-lagged panel analysis.�Behav Res Ther.�2003;41(10):1163�1182.�[PubMed]
23.�Sullivan MJL, Adams H, Ellis T. Targeting catastrophic thinking to promote return to work in individuals with fibromyalgia.�J Cogn Psychother.�2012;26(2):130�142.
24.�Leeuw M, Goossens ME, Linton SJ, Crombez G, Boersma K, Vlaeyen JW. The fear-avoidance model of musculoskeletal pain: current state of scientific evidence.�J Behav Med.�2007;30(1):77�94.�[PubMed]
25.�Demmelmaier I, Asenl�f P, Lindberg P, Denison E. Biopsychosocial predictors of pain, disability, health care consumption, and sick leave in first-episode and long-term back pain: a longitudinal study in the general population.�Int J Behav Med.�2010;17(2):79�89.�[PubMed]
26.�Zale EL, Lange KL, Fields SA, Ditre JW. The relation between pain-related fear and disability: a meta-analysis.�J Pain.�2013;14(10):1019�1030.�[PMC free article]�[PubMed]
27.�Samwel HJ, Evers AW, Crul BJ, Kraaimaat FW. The role of helplessness, fear of pain, and passive pain-coping in chronic pain patients.�Clin J Pain.�2006;22(3):245�251.�[PubMed]
28.�Werneke MW, Hart DL, George SZ, Stratford PW, Matheson JW, Reyes A. Clinical outcomes for patients classified by fear-avoidance beliefs and centralization phenomenon.�Arch Phys Med Rehabil.�2009;90(5):768�777.�[PubMed]
29.�Somers TJ, Keefe FJ, Pells JJ, et al. Pain catastrophizing and pain-related fear in osteoarthritis patients: relationships to pain and disability.�J Pain Symptom Manage.�2009;37(5):863�872.�[PMC free article][PubMed]
30.�Pincus T, McCracken LM. Psychological factors and treatment opportunities in low back pain.�Best Pract Res Clin Rheumatol.�2013;27(5):625�635.�[PubMed]
31.�Hayes SC, Luoma JB, Bond FW, Masuda A, Lillis J. Acceptance and commitment therapy: model, processes and outcomes.�Behav Res Ther.�2006;44(1):1�25.�[PubMed]
32.�Eccleston C, Crombez G, Aldrich S, Stannard C. Worry and chronic pain patients: a description and analysis of individual differences.�Eur J Pain.�2001;5(3):309�318.�[PubMed]
33.�McCracken LM. Learning to live with the pain: acceptance of pain predicts adjustment in persons with chronic pain.�Pain.�1998;74(1):21�27.�[PubMed]
34.�Kranz D, Bollinger A, Nilges P. Chronic pain acceptance and affective well-being: a coping perspective.�Eur J Pain.�2010;14(10):1021�1025.�[PubMed]
35.�Vowles KE, McCracken LM, Eccleston C. Patient functioning and catastrophizing in chronic pain: the mediating effects of acceptance.�Health Psychol.�2008;27(Suppl 2):S136�S143.�[PubMed]
36.�McCracken LM, Eccleston C. A prospective study of acceptance of pain and patient functioning with chronic pain.�Pain.�2005;118(1�2):164�169.�[PubMed]
37.�Vowles KE, McCracken LM, Eccleston C. Processes of change in treatment for chronic pain: the contributions of pain, acceptance, and catastrophizing.�Eur J Pain.�2007;11(7):779�787.�[PubMed]
38.�Kratz AL, Davis MC, Zautra AJ. Pain acceptance moderates the relation between pain and negative affect in female osteoarthritis and fibromyalgia patients.�Ann Behav Med.�2007;33(3):291�301.[PMC free article]�[PubMed]
39.�Fordyce WE.�Behavioral Methods for Chronic Pain and Illness.�St Louis, MO: Mosby; 1976. p. 1.
40.�Gatzounis R, Schrooten MG, Crombez G, Vlaeyen JW. Operant learning theory in pain and chronic pain rehabilitation.�Curr Pain Headache Rep.�2012;16(2):117�126.�[PubMed]
41.�Leeuw M, Goossens ME, van Breukelen GJ, et al. Exposure in vivo versus operant graded activity in chronic low back pain patients: results of a randomized controlled trial.�Pain.�2008;138(1):192�207.[PubMed]
42.�den Hollander M, de Jong JR, Volders S, Goossens ME, Smeets RJ, Vlaeyen JW. Fear reduction in patients with chronic pain: a learning theory perspective.�Expert Rev Neurother.�2010;10(11):1733�1745.[PubMed]
43.�Woods MP, Asmundson GJ. Evaluating the efficacy of graded in vivo exposure for the treatment of fear in patients with chronic back pain: a randomized controlled clinical trial.�Pain.�2008;136(3):271�280.[PubMed]
44.�Day MA, Thorn BE, Burns JW. The continuing evolution of biopsychosocial interventions for chronic pain.�J Cogn Psychother.�2012;26(2):114�129.
45.�Hofmann SG, Asnaani A, Vonk IJ, Sawyer AT, Fang A. The efficacy of cognitive behavioral therapy: a review of meta-analyses.�Cognit Ther Res.�2012;36(5):427�440.�[PMC free article]�[PubMed]
46.�Buhrman M, Fredriksson A, Edstr�m G, et al. Guided Internet-delivered cognitive behavioural therapy for chronic pain patients who have residual symptoms after rehabilitation treatment: randomized controlled trial.�Eur J Pain.�2013;17(5):753�765.�[PubMed]
47.�Bennett R, Nelson D. Cognitive behavioral therapy for fibromyalgia.�Nat Clin Pract Rheumatol.�2006;2(8):416�424.�[PubMed]
48.�Kabat-Zinn J. An outpatient program in behavioral medicine for chronic pain patients based on the practice of mindfulness meditation: theoretical considerations and preliminary results.�Gen Hosp Psychiatry.�1982;4(1):33�47.�[PubMed]
49.�Lauwerier E, Van Damme S, Goubert L, Paemeleire K, Devulder J, Crombez G. To control or not? A motivational perspective on coping with pain.�Acta Neurol Belg.�2012;112(1):3�7.�[PubMed]
50.�Baer RA. Mindfulness training as a clinical intervention: a conceptual and empirical review.�Clin Psychol: Sci Pract.�2003;10(2):125�143.
51.�Campbell TS, Labelle LE, Bacon SL, Faris P, Carlson LE. Impact of Mindfulness-Based Stress Reduction (MBSR) on attention, rumination and resting blood pressure in women with cancer: a waitlist-controlled study.�J Behav Med.�2012;35(3):262�271.�[PubMed]
52.�Garland EL, Gaylord SA, Palsson O, Faurot K, Douglas Mann J, Whitehead WE. Therapeutic mechanisms of a mindfulness-based treatment for IBS: effects on visceral sensitivity, catastrophizing, and affective processing of pain sensations.�J Behav Med.�2012;35(6):591�602.�[PMC free article]�[PubMed]
53.�Kabat-Zinn J.�Full Catastrophe Living: The Program of the Stress Reduction Clinic at the University of Massachusetts Medical Center.�New York, NY: Delta; 1990.
54.�Kabat-Zinn J, Lipworth L, Burney R, Sellers W. Four-year follow-up of a meditation-based program for the self-regulation of chronic pain: treatment outcomes and compliance.�Clin J Pain.�1986;2(3):159�173.
55.�Carmody J, Baer RA. Relationships between mindfulness practice and levels of mindfulness, medical and psychological symptoms and well-being in a mindfulness-based stress reduction program.�J Behav Med.�2008;31(1):23�33.�[PubMed]
56.�Randolph P, Caldera YM, Tacone AM, Greak BL. The long-term combined effects of medical treatment and a mindfulness-based behavioral program for the multidisciplinary management of chronic pain in West Texas.�Pain Digest.�1999;9:103�112.
57.�Rosenzweig S, Greeson JM, Reibel DK, Green JS, Jasser SA, Beasley D. Mindfulness-based stress reduction for chronic pain conditions: variation in treatment outcomes and role of home meditation practice.�J Psychosom Res.�2010;68(1):29�36.�[PubMed]
58.�Grossman P, Tiefenthaler-Gilmer U, Raysz A, Kesper U. Mindfulness training as an intervention for fibromyalgia: evidence of postintervention and 3-year follow-up benefits in well-being.�Psychother Psychosom.�2007;76(4):226�233.�[PubMed]
59.�Plews-Ogan M, Owens JE, Goodman M, Wolfe P, Schorling J. A pilot study evaluating mindfulness-based stress reduction and massage for the management of chronic pain.�J Gen Intern Med.�2005;20(12):1136�1138.�[PMC free article]�[PubMed]
60.�Sephton SE, Salmon P, Weissbecker I, et al. Mindfulness meditation alleviates depressive symptoms in women with fibromyalgia: results of a randomized clinical trial.�Arthritis Rheum.�2007;57(1):77�85.[PubMed]
61.�Cassidy EL, Atherton RJ, Robertson N, Walsh DA, Gillett R. Mindfulness, functioning and catastrophizing after multidisciplinary pain management for chronic low back pain.�Pain.�2012;153(3):644�650.�[PubMed]
62.�Bohlmeijer E, Prenger R, Taal E, Cuijpers P. The effects of mindfulness-based stress reduction therapy on mental health of adults with a chronic medical disease: a meta-analysis.�J Psychosom Res.�2010;68(6):539�544.�[PubMed]
63.�Merkes M. Mindfulness-based stress reduction for people with chronic diseases.�Aust J Prim Health.�2010;16(3):200�210.�[PubMed]
64.�Veehof MM, Oskam MJ, Schreurs KM, Bohlmeijer ET. Acceptance-based interventions for the treatment of chronic pain: a systematic review and meta-analysis.�Pain.�2011;152(3):533�542.�[PubMed]
65.�Wicksell RK, Kemani M, Jensen K, et al. Acceptance and commitment therapy for fibromyalgia: a randomized controlled trial.�Eur J Pain.�2013;17(4):599�611.�[PubMed]
66.�McCracken LM, MacKichan F, Eccleston C. Contextual cognitive-behavioral therapy for severely disabled chronic pain sufferers: effectiveness and clinically significant change.�Eur J Pain.�2007;11(3):314�322.�[PubMed]
67.�Vowles KE, McCracken LM. Acceptance and values-based action in chronic pain: a study of treatment effectiveness and process.�J Consult Clin Psychol.�2008;76(3):397�407.�[PubMed]
68.�Dimidjian S, Hollon SD. How would we know if psychotherapy were harmful?�Am Psychol.�2010;65(1):21�33.�[PubMed]
69.�Berk M, Parker G. The elephant on the couch: side-effects of psychotherapy.�Aust N Z J Psychiatry.�2009;43(9):787�794.�[PubMed]
70.�Green B. Adverse effects of psychotherapy.�Advances in Psychiatric Treatment.�2011;17(6):476.
71.�Barlow DH. Negative effects from psychological treatments: a perspective.�Am Psychol.�2010;65(1):13�20.�[PubMed]
72.�Shadick NA, Sowell NF, Frits ML, et al. A randomized controlled trial of an internal family systems-based psychotherapeutic intervention on outcomes in rheumatoid arthritis: a proof-of-concept study.�J Rheumatol.�2013;40(11):1831�1841.�[PubMed]
73.�Turk DC. The potential of treatment matching for subgroups of patients with chronic pain: lumping versus splitting.�Clin J Pain.�2005;21(1):44�55.�discussion 69�72.�[PubMed]
74.�Turk DC, Okifuji A, Sinclair JD, Starz TW. Differential responses by psychosocial subgroups of fibromyalgia syndrome patients to an interdisciplinary treatment.�Arthritis Care Res.�1998;11(5):397�404.[PubMed]
75.�Kerns RD, Turk DC, Rudy TE. The West Haven-Yale multidimensional pain inventory (WHYMPI)�Pain.�1985;23(4):345�356.�[PubMed]
76.�Von Korff M, Ormel J, Keefe FJ, Dworkin SF. Grading the severity of chronic pain.�Pain.�1992;50(2):133�149.�[PubMed]
77.�Kerns RD, Rosenberg R, Jamison RN, Caudill MA, Haythornthwaite J. Readiness to adopt a self-management approach to chronic pain: the Pain Stages of Change Questionnaire (PSOCQ)�Pain.�1997;72(1�2):227�234.�[PubMed]
78.�Kratz AL, Molton IR, Jensen MP, Ehde DM, Nielson WR. Further evaluation of the Motivational Model of Pain Self-Management: coping with chronic pain in multiple sclerosis.�Ann Behav Med.�2011;41(3):391�400.�[PMC free article]�[PubMed]
79.�Reese C, Mittag O. Psychological interventions in the rehabilitation of patients with chronic low back pain: evidence and recommendations from systematic reviews and guidelines.�Int J Rehabil Res.�2013;36(1):6�12.�[PubMed]
80.�Kraaimaat F, Brons MR, Geenen R, Bijlsma JW. The effect of cognitive behavior therapy in patients with rheumatoid arthritis.�Behav Res Ther.�1995;33(5):487�495.�[PubMed]
81.�Wetherell JL, Afari N, Rutledge T, et al. A randomized, controlled trial of acceptance and commitment therapy and cognitive-behavioral therapy for chronic pain.�Pain.�2011;152(9):2098�2107.�[PubMed]
82.�Tang NK, Goodchild CE, Salkovskis PM. Hybrid cognitive-behaviour therapy for individuals with insomnia and chronic pain: a pilot randomised controlled trial.�Behav Res Ther.�2012;50(12):814�821.[PubMed]
83.�Knoop H, Stulemeijer M, Prins JB, van der Meer JW, Bleijenberg G. Is cognitive behaviour therapy for chronic fatigue syndrome also effective for pain symptoms?�Behav Res Ther.�2007;45(9):2034�2043.[PubMed]
84.�Bishop SR. What do we really know about mindfulness-based stress reduction?�Psychosom Med.�2002;64(1):71�83.�[PubMed]
85.�Turner JA, Holtzman S, Mancl L. Mediators, moderators, and predictors of therapeutic change in cognitive-behavioral therapy for chronic pain.�Pain.�2007;127(3):276�286.�[PubMed]
86.�Park J, Hughes AK. Nonpharmacological approaches to the management of chronic pain in community-dwelling older adults: a review of empirical evidence.�J Am Geriatr Soc.�2012;60(3):555�568.[PubMed]
87.�Kraaij V, Pruymboom E, Garnefski N. Cognitive coping and depressive symptoms in the elderly: a longitudinal study.�Aging Ment Health.�2002;6(3):275�281.�[PubMed]
88.�Keefe FJ, Porter L, Somers T, Shelby R, Wren AV. Psychosocial interventions for managing pain in older adults: outcomes and clinical implications.�Br J Anaesth.�2013;111(1):89�94.�[PMC free article][PubMed]
89.�Nicholson NL, Blanchard EB. A controlled evaluation of behavioral treatment of chronic headache in the elderly.�Behav Ther.�1993;24(3):395�408.
90.�Morone NE, Greco CM. Mind-body interventions for chronic pain in older adults: a structured review.�Pain Med.�2007;8(4):359�375.�[PubMed]
91.�Fuentes M, Hart-Johnson T, Green CR. The association among neighborhood socioeconomic status, race and chronic pain in black and white older adults.�J Natl Med Assoc.�2007;99(10):1160�1169.[PMC free article]�[PubMed]
92.�Naylor MR, Naud S, Keefe FJ, Helzer JE. Therapeutic Interactive Voice Response (TIVR) to reduce analgesic medication use for chronic pain management.�J Pain.�2010;11(12):1410�1419.�[PMC free article][PubMed]
93.�Hoch DB, Watson AJ, Linton DA, et al. The feasibility and impact of delivering a mind-body intervention in a virtual world.�PLoS One.�2012;7(3):e33843.�[PMC free article]�[PubMed]
94.�Buhrman M, Skoglund A, Husell J, et al. Guided internet-delivered acceptance and commitment therapy for chronic pain patients: a randomized controlled trial.�Behav Res Ther.�2013;51(6):307�315.[PubMed]
95.�Davis MC, Zautra AJ. An online mindfulness intervention targeting socioemotional regulation in fibromyalgia: results of a randomized controlled trial.�Ann Behav Med.�2013;46(3):273�284.�[PubMed]
96.�Macea DD, Gajos K, Daglia Calil YA, Fregni F. The efficacy of Web-based cognitive behavioral interventions for chronic pain: a systematic review and meta-analysis.�J Pain.�2010;11(10):917�929.[PubMed]
97.�Schrooten MG, Vlaeyen JW, Morley S. Psychological interventions for chronic pain: reviewed within the context of goal pursuit.�Pain Management.�2012;2(2):141�150.�[PubMed]
98.�Bailey KM, Carleton RN, Vlaeyen JW, Asmundson GJ. Treatments addressing pain-related fear and anxiety in patients with chronic musculoskeletal pain: a preliminary review.�Cogn Behav Ther.�2010;39(1):46�63.�[PubMed]
99.�Glombiewski JA, Sawyer AT, Gutermann J, Koenig K, Rief W, Hofmann SG. Psychological treatments for fibromyalgia: a meta-analysis.�Pain.�2010;151(2):280�295.�[PubMed]
100.�Castel A, Casc�n R, Padrol A, Sala J, Rull M. Multicomponent cognitive-behavioral group therapy with hypnosis for the treatment of fibromyalgia: long-term outcome.�J Pain.�2012;13(3):255�265.[PubMed]
101.�Gross AR, Kaplan F, Huang S, et al. Psychological care, patient education, orthotics, ergonomics and prevention strategies for neck pain: a systematic overview update as part of the ICON Project.�Open Orthop J.�2013;7:530�561.�[PMC free article]�[PubMed]
102.�Hunt MA, Keefe FJ, Bryant C, et al. A physiotherapist-delivered, combined exercise and pain coping skills training intervention for individuals with knee osteoarthritis: a pilot study.�Knee.�2013;20(2):106�112.�[PubMed]
103.�Bruflat AK, Balter JE, McGuire D, Fethke NB, Maluf KS. Stress management as an adjunct to physical therapy for chronic neck pain.�Phys Ther.�2012;92(10):1348�1359.�[PMC free article]�[PubMed]
104.�Lamb SE, Mistry D, Lall R, et al. Back Skills Training Trial Group Group cognitive behavioural interventions for low back pain in primary care: extended follow-up of the Back Skills Training Trial (ISRCTN54717854)�Pain.�2012;153(2):494�501.�[PubMed]
Being involved in an automobile accident is an undesirable situation which can result in a variety of physical trauma or injury as well as lead to the development of a number of aggravating conditions. Auto accident injuries, such as whiplash, can be characterized by painful symptoms, including chronic neck pain, however, recent research studies have found that emotional distress resulting from an auto collision could manifest into physical symptoms. Stress, anxiety, depression and post traumatic stress disorder, or PTSD, are common psychological issues which may occur as a result of an automobile accident.
The researchers of the research studies also determined that cognitive-behavioral therapy may be an effective treatment for emotional distress and psychological issues which may have developed as a result of the auto accident injuries. Additionally, auto accident injuries may also cause stress, anxiety, depression and even PTSD if left untreated for an extended amount of time. The purpose of the article below is to demonstrate the effects of cognitive-behavioral therapy, together with alternative treatment options like chiropractic care and physical therapy. for auto accident injuries, such as whiplash.
Neck Exercises, Physical and Cognitive Behavioural-Graded Activity as a Treatment for Adult Whiplash Patients with Chronic Neck Pain: Design of a Randomised Controlled Trial
Abstract
Background
Many patients suffer from chronic neck pain following a whiplash injury. A combination of cognitive, behavioural therapy with physiotherapy interventions has been indicated to be effective in the management of patients with chronic whiplash-associated disorders. The objective is to present the design of a randomised controlled trial (RCT) aimed at evaluating the effectiveness of a combined individual physical and cognitive behavioural-graded activity program on self-reported general physical function, in addition to neck function, pain, disability and quality of life in patients with chronic neck pain following whiplash injury compared with a matched control group measured at baseline and 4 and 12 months after baseline.
Methods/Design
The design is a two-centre, RCT-study with a parallel group design. Included are whiplash patients with chronic neck pain for more than 6 months, recruited from physiotherapy clinics and an out-patient hospital department in Denmark. Patients will be randomised to either a pain management (control) group or a combined pain management and training (intervention)group. The control group will receive four educational sessions on pain management, whereas the intervention group will receive the same educational sessions on pain management plus 8 individual training sessions for 4 months, including guidance in specific neck exercises and an aerobic training programme. Patients and physiotherapists are aware of the allocation and the treatment, while outcome assessors and data analysts are blinded. The primary outcome measures will be Medical Outcomes Study Short Form 36 (SF36), Physical Component Summary (PCS). Secondary outcomes will be Global Perceived Effect (-5 to +5), Neck Disability Index (0-50), Patient Specific Functioning Scale (0-10), numeric rating scale for pain bothersomeness (0-10), SF-36 Mental Component Summary (MCS), TAMPA scale of Kinesiophobia (17-68), Impact of Event Scale (0-45), EuroQol (0-1), craniocervical flexion test (22 mmHg – 30 mmHg), joint position error test and cervical range of movement. The SF36 scales are scored using norm-based methods with PCS and MCS having a mean score of 50 with a standard deviation of 10.
Discussion
The perspectives of this study are discussed, in addition to the strengths and weaknesses.
The Danish National Board of Health estimates that 5-6,000 subjects per year in Denmark are involved in a traffic accident evoking whiplash-induced neck pain. About 43% of those will still have physical impairment and symptoms 6 months after the accident [1]. For Swedish society, including Swedish insurance companies, the economic burden is approximately 320 million Euros [2], and this burden is likely to be comparable to that of Denmark. Most studies suggest that patients with Whiplash-Associated Disorders (WAD) report chronic neck symptoms one year after the injury [3]. The main problems in whiplash patients with chronic neck pain are cervical dysfunction and abnormal sensory processing, reduced neck mobility and stability, impaired cervicocephalic kinaesthetic sense, in addition to local and possibly generalised pain [4,5]. Cervical dysfunction is characterised by reduced function of the deep stabilising muscles of the neck.
Besides chronic neck pain, patients with WAD may suffer from physical inactivity as a consequence of prolonged pain [6,7]. This influences physical function and general health and can result in a poor quality of life. In addition, WAD patients may develop chronic pain followed by sensitisation of the nervous system [8,9], a lowering of the threshold for different sensory inputs (pressure, cold, warm, vibration and electrical impulses) [10]. This can be caused by an impaired central pain inhibition [11] – a cortical reorganisation [12]. Besides central sensitisation, the group with WAD may have poorer coping strategies and cognitive functions, compared with patients with chronic neck pain in general [13-15].
Studies have shown that physical training, including specific exercises targeting the deep postural muscles of the cervical spine, is effective in reducing neck pain [16-18] for patients with chronic neck pain, albeit there is a variability in the response to training with not every patient showing a major change. Physical behavioural-graded activity is a treatment approach with a focus on increasing general physical fitness, reducing fear of movement and increasing psychological function [19,20]. There is insufficient evidence for the long-term effect of treatment of physical and cognitive behavioural-graded activity, especially in chronic neck pain patients. Educational sessions, where the focus is on understanding complex chronic pain mechanisms and development of appropriate pain coping and/or cognitive behavioural strategies, have shown reduced general pain [6,21-26]. A review indicated that interventions with a combination of cognitive, behavioural therapy with physiotherapy including neck exercises is effective in the management of WAD patients with chronic neck pain [27], as also recommended by the Dutch clinical guidelines for WAD [28]. However, the conclusions regarding the guidelines are largely based on studies performed on patients with either acute or sub-acute WAD [29]. A more strict conclusion was drawn for WAD patients with chronic pain in the Bone and Joint Decade 2000-2010 Task Force, stating, that ‘because of conflicting evidence and few high-quality studies, no firm conclusions could be drawn about the most effective non-invasive interventions for patients with chronic WAD” [29,30]. The concept of combined treatment for WAD patients with chronic pain has been used in a former randomised controlled trial [31]. The results indicated that a combination of non-specific aerobic exercises and advice containing standardised pain education and reassurance and encouragement to resume light activity, produced better outcomes than advice alone for patients with WAD 3 months after the accident. The patients showed improvements in pain intensity, pain bothersomeness and functions in daily activities in the group receiving exercise and advice, compared with advice alone. However, the improvements were small and only apparent in the short term.
This project is formulated on the expectation that rehabilitation of WAD patients with chronic neck pain must target cervical dysfunctions, training of physical function and the understanding and management of chronic pain in a combined therapy approach. Each single intervention is based upon former studies that have shown effectiveness [6,18,20,32]. This study is the first to also include the long-term effect of the combined approach in patients with chronic neck pain after whiplash trauma. As illustrated in Figure ?Figure1,1, the conceptual model in this study is based upon the hypothesis that training (including both individually-guided specific neck exercises and graded aerobic training) and education in pain management (based on a cognitive behavioural approach) is better for increasing the patients’ physical quality of life, compared with education in pain management alone. Increasing the physical quality of life includes increasing the general physical function and level of physical activity, decreasing fear of movement, reducing post-traumatic stress symptoms, reducing neck pain and increasing neck function. The effect is anticipated to be found immediately after the treatment (i.e. 4 months; short-term effect) as well as after one year (long-term effect).
Figure 1: Hypothesis of the intervention effect for patients with chronic neck pain after a whiplash accident.
Using a randomised controlled trial (RCT) design, the aim of this study is to evaluate the effectiveness of: graded physical training, including specific neck exercises and general aerobic training, combined with education in pain management (based on a cognitive behavioural approach) versus education in pain management (based on a cognitive behavioural approach), measured on physical quality of life’, physical function, neck pain and neck functions, fear of movement, post-traumatic symptoms and mental quality of life, in patients with chronic neck pain after whiplash injury.
Methods/Design
Trial Design
The study is conducted in Denmark as an RCT with a parallel group design. It will be a two-centre study, stratified by recruitment location. Patients will be randomised to either the Pain Management group (control) or the Pain Management and Training group (intervention). As illustrated in Figure ?Figure2,2, the study is designed to include a secondary data assessment 12 months after baseline; the primary outcome assessment will be performed immediately after the intervention program 4 months after baseline. The study utilises an allocation concealment process, ensuring that the group to which the patient is allocated is not known before the patient is entered into the study. The outcome assessors and data analysts will be kept blinded to the allocation to intervention or control group.
Figure 2: Flowchart of the patients in the study.
Settings
The participants will be recruited from physiotherapy clinics in Denmark and from The Spine Centre of Southern Denmark, Hospital Lilleb�lt via an announcement at the clinics and the Hospital. Using physiotherapy clinics spread across Denmark, the patients will receive the intervention locally. The physiotherapy clinics in Denmark receive patients via referral from their general practitioners. The Spine Centre, a unit specialising in treating patients with musculoskeletal dysfunctions and only treating out-patients, receives patients referred from general practitioners and/or chiropractors.
Study Population
Two hundred adults with a minimum age of 18 years, receiving physiotherapy treatment or having been referred for physiotherapy treatment will be recruited. For patients to be eligible, they must have: chronic neck pain for at least 6 months following a whiplash injury, reduced physical neck function (Neck Disability Index score, NDI, of a minimum of 10), pain primarily in the neck region, finished any medical /radiological examinations, the ability to read and understand Danish and the ability to participate in the exercise program. The exclusion criteria include: neuropathies/ radiculopathies (clinically tested by: positive Spurling, cervical traction and plexus brachialis tests) [33], neurological deficits (tested as in normal clinical practice through a process of examining for unknown pathology), engagement in experimental medical treatment, being in an unstable social and/or working situation, pregnancy, known fractures, depression according to the Beck Depression Index (score > 29) [18,34,35], or other known coexisting medical conditions which could severely restrict participation in the exercise program. The participants will be asked not to seek other physiotherapy or cognitive treatment during the study period.
Intervention
Control
The Pain Management (control) group will receive education in pain management strategies. There will be 4 sessions of 11/2 hours, covering topics regarding pain mechanisms, acceptance of pain, coping strategies, and goal-setting, based upon pain management and cognitive therapy concepts [21,26,36].
Intervention
The Pain Management plus Training (intervention) group will receive the same education in pain management as those in the control group plus 8 treatment sessions (instruction in neck exercises and aerobic training) with the same period of 4 months length. If the treating physiotherapist estimates additional treatments are needed, the treatment can be extended with 2 more sessions. Neck training: The treatment of neck-specific exercises will be progressed through different phases, which are defined by set levels of neck function. At the first treatment session, patients are tested for cervical neuromuscular function to identify the specific level at which to start neck training. A specific individually tailored exercise program will be used to target the neck flexor and extensor muscles. The ability to activate the deep cervical neck flexor muscles of the upper cervical region to increase their strength, endurance and stability function is trained progressively via the craniocervical training method using a biopressure feedback transducer [18,37]. Exercises for neck-eye coordination, neck joint positioning, balance and endurance training of the neck muscles will be included as well, since it has been shown to reduce pain and improve sensorimotor control in patients with insidious neck pain [17,38]. Aerobic training: The large trunk and leg muscles will be trained with a gradually increasing physical training program. Patients will be allowed to select activities such as walking, cycling, stick walking, swimming, and jogging. The baseline for training duration is set by exercising 3 times at a comfortable level, that does not exacerbate pain and aims at a rated perceived exertion (RPE) level of between 11 and 14 on a Borg scale [39]. The initial duration of training is set 20% below the average time of the three trials. Training sessions are carried out every second day with a prerequisite that pain is not worsened, and that RPE is between 9 and 14. A training diary is used. If patients do not experience a relapse, and report an average RPE value of 14 or less, the exercise duration for the following period (1 or 2 weeks) is increased by 2-5 minutes, up to a maximum of 30 minutes. If the RPE level is 15 or higher, the exercise duration will be reduced to an average RPE score of 11 to 14 every fortnight [20,40]. By using these pacing principles, the training will be graded individually by the patient, with a focus on perceived exertion – with the aim of increasing the patient’ s general physical activity level and fitness.
Patients’ compliance will be administered by registration of their participation in the control and intervention group. The patients in the control group will be considered to have completed the pain management if they have attended 3 out of 4 sessions. The patiesnts in the intervention group will be considered to have completed if the patient has attended a minimum of 3 out of 4 pain management sessions and a minimum of 5 out of 8 trainings sessions. Each patient’s home training with neck exercises and aerobic training will be registered by him/her in a logbook. Compliance with 75% of the planned home training will be considered as having completed the intervention.
Physiotherapists
The participating physiotherapists will be recruited via an announcement in the Danish Physiotherapy Journal. The inclusion criteria consist of: being a qualified physiotherapist, working at a clinic and having at least two years of working experience as a physiotherapist, having attended a course in the described intervention and passed the related exam.
Outcome Measures
At baseline the participants’ information on age, gender, height and weight, type of accident, medication, development of symptoms over the last two months (status quo, improving, worsening), expectation of treatment, employment and educational status will be registered. As a primary outcome measure, Medical Outcomes Study Short Form 36 (SF36) – Physical Component Summary (PCS) will be used [41,42]. The PCS scales are scored using norm-based methods [43,44] with a mean score of 50 with a standard deviation of 10. The primary outcome with respect to having an effect, will be calculated as a change from baseline [45]. Secondary outcomes contain data on both clinical tests and patient-reported outcomes. Table ?Table11 presents clinical tests for measuring the intervention effect on neuromuscular control of the cervical muscles, cervical function and mechanical allodynia. Table ?Table22 presents the patient-related outcomes from questionnaires used to test for perceived effect of the treatment, neck pain and function, pain bothersomeness, fear of movement, post-traumatic stress and quality of life and potential treatment modifiers.
Table 1: Clinical outcomes used for measurement of treatment effect on muscle strategy, function and treatment modifiers.
Table 2: Patient reported outcomes used for measured of treatment effect on pain and function.
Patients will be tested at baseline, 4 and 12 months after baseline, except for GPE, which will only be measured 4 and 12 months after baseline.
Power and Sample Size Estimation
The power and sample size calculation is based on the primary outcome, being SF36-PCS 4 months after baseline. For a two-sample pooled t-test of a normal mean difference with a two-sided significance level of 0.05, assuming a common SD of 10, a sample size of 86 per group is required to obtain a power of at least 90% to detect a group mean difference of 5 PCS points [45]; the actual power is 90.3%, and the fractional sample size that achieves a power of exactly 90% is 85.03 per group. In order to adjust for an estimated 15% withdrawal during the study period of 4 months, we will include 100 patients in each group. For sensitivity, three scenarios were applied: firstly, anticipating that all 2 � 100 patients complete the trial, we will have sufficient power (> 80%) to detect a group mean difference as low as 4 PCS points; secondly, we will be able to detect a statistically significant group mean difference of 5 PCS points with sufficient power (> 80%) even with a pooled SD of 12 PCS points. Thirdly and finally, if we aim for a group mean difference of 5 PCS points, with a pooled SD of 10, we will have sufficient power (> 80%) with only 64 patients in each group. However, for logistical reasons, new patients will no longer be included in the study 24 months after the first patient has been included.
Randomisation, Allocation and Blinding Procedures
After the baseline assessment, the participants are randomly assigned to either the control group or the intervention group. The randomisation sequence is created using SAS (SAS 9.2 TS level 1 M0) statistical software and is stratified by centre with a 1:1 allocation using random block sizes of 2, 4, and 6. The allocation sequence will be concealed from the researcher enrolling and assessing participants in sequentially numbered, opaque, sealed and stapled envelopes. Aluminium foil inside the envelope will be used to render the envelope impermeable to intense light. After revealing the content of the envelope, both patients and physiotherapists are aware of the allocation and the corresponding treatment. Outcome assessors and data analysts are however kept blinded. Prior to the outcome assessments, the patients will be asked by the research assistant not to mention the treatment to which they have been allocated.
Statistical Analysis
All the primary data analyses will be carried out according to a pre-established analysis plan; all analyses will be done applying SAS software (v. 9.2 Service Pack 4; SAS Institute Inc., Cary, NC, USA). All descriptive statistics and tests are reported in accordance with the recommendations of the ‘Enhancing the QUAlity and Transparency Of health Research’ (EQUATOR) network; i.e., various forms of the CONSORT statement [46]. Data will be analysed using a two-factor Analysis of Covariance (ANCOVA), with a factor for Group and a factor for Gender, using the baseline value as covariate to reduce the random variation, and increase the statistical power. Unless stated otherwise, results will be expressed as the difference between the group means with 95% confidence intervals (CIs) and associated p-values, based on a General Linear Model (GLM) procedure. All the analyses will be performed using the Statistical Package for Social Sciences (version 19.0.0, IBM, USA) as well as the SAS system (v. 9.2; SAS Institute Inc., Cary, NC, USA). A two-way analysis of variance (ANOVA) with repeated measures (Mixed model) will be performed to test the difference over time between the intervention and the control groups; interaction: Group � Time. An alpha-level of 0.05 will be considered as being statistically significant (p < 0.05, two- sided). The data analysts will be blinded to the allocated interventions for primary analyses.
The baseline scores for the primary and secondary outcomes will be used to compare the control and intervention groups. The statistical analyses will be performed on the basis of the intention-to-treat principle, i.e. patients will be analysed in the treatment group to which they were randomly allocated. In the primary analyses, missing data will be replaced with the feasible and transparent ‘Baseline Observation Carried Forward’ (BOCF) technique, and for sensitivity also a multiple imputation technique will apply.
Secondarily, to relate the results to compliance, a ‘per protocol’ analysis will be used as well. The ‘per protocol’ population he patients who have ‘completed’ the intervention to which they were allocated, according to the principles described in the intervention section above.
Ethical Considerations
The Regional Scientific Ethical Committee of Southern Denmark approved the study (S-20100069). The study conformed to The Declaration of Helsinki 2008 [47] by fulfilling all general ethical recommendations.
All subjects will receive information about the purpose and content of the project and give their oral and written consent to participate, with the possibility to drop out of the project at any time.
Dr. Alex Jimenez’s Insight
Managing stress, anxiety, depression and symptoms of post traumatic stress disorder, or PTSD, after being involved in an automobile accident can be difficult, especially if the incident caused physical trauma and injuries or aggravated a previously existing condition. In many cases, the emotional distress and the psychological issues caused by the incident may be the source of the painful symptoms. In El Paso, TX, many veterans with PTSD visit my clinic after manifesting worsening symptoms from a previous auto accident injury. Chiropractic care can provide patients the proper stress management environment they need to improve their physical and emotional symptoms. Chiropractic care can also treat a variety of auto accident injuries, including whiplash, head and neck injuries, herniated disc and back injuries.
Discussion
This study will contribute to a better understanding of treating patients with chronic neck pain following a whiplash accident. The knowledge from this study can be implemented into clinical practice, as the study is based on a multimodal approach, mirroring the approach, which in spite of the current lack of evidence, is often used in a clinical physiotherapy setting. The study may also be included in systematic reviews thereby contributing to updating the knowledge about this population and to enhancing evidence-based treatment.
Publishing the design of a study before the study is performed and the results obtained has several advantages. It allows the design to be finalised without its being influenced by the outcomes. This can assist in preventing bias as deviations from the original design can be identified. Other research projects will have the opportunity to follow a similar approach with respect to population, interventions, controls and outcome measurements. The challenges of this study are related to standardising the interventions, treating a non-homogeneous population, defining and standardising relevant outcome measures on a population with long-lasting symptoms and having a population from two different clinical settings. Standardisation of the interventions is obtained by teaching the involved physiotherapists in an instructional course. Population homogeneity will be handled by strict inclusion and exclusion criteria and by monitoring the baseline characteristics of the patients, and differences between groups based on other influences than the intervention/control will be possible to analyse statistically. This research design is composed as an ‘add-on’ design: both groups receive pain education; the intervention group receives additional physical training, including specific neck exercises and general training. Today there is insufficient evidence for the effect of treatment for patients with chronic neck pain following a whiplash accident. All participating patients will be referred for a treatment (control or intervention), as we consider it unethical not to offer some form of treatment, i.e. randomising the control group to a waiting list. The add-on design is chosen as a pragmatic workable solution in such a situation [48].
For whiplash patients with chronic pain, the most responsive disability measures (for the individual patient, not for the group as a whole) are considered to be the Patient Specific Functional Scale and the numerical rating scale of pain bothersomeness [49]. By using these and NDI (the most often used neck disability measure) as secondary outcome measures, it is anticipated that patient-relevant changes in pain and disability can be evaluated. The population will be recruited from and treated at two different clinical settings: the out-patient clinic of The Spine Centre, Hospital Lilleb�lt and several private physiotherapy clinics. To avoid any influence of the different settings on the outcome measures, the population will be block randomised related to the settings, securing equal distribution of participants from each setting to the two intervention groups.
Competing Interests
The authors declare that they have no competing interests.
Authors’ Contributions
IRH drafted the manuscript. IRH, BJK and KS participated in the design of the study. All contributed to the design. RC, IRH; BJK and KS participated in the power and sample size calculation and in describing the statistical analysis as well as the allocation and randomization procedure. All authors read and approved the final manuscript. Suzanne Capell provided writing assistance and linguistic corrections.
This study has received funding from the Research Fund for the Region of Southern Denmark, the Danish Rheumatism Association, the Research Foundation of the Danish Association of Physiotherapy, the Fund for Physiotherapy in Private Practice, and the Danish Society of Polio and Accident Victims (PTU). The Musculoskeletal Statistics Unit at the Parker Institute is supported by grants from the Oak Foundation. Suzanne Capell provided writing assistance and linguistic correction.
A Randomized Controlled Trial of Cognitive-Behavioral Therapy for the Treatment of PTSD in the context of Chronic Whiplash
Abstract
Objectives
Whiplash-associated disorders (WAD) are common and involve both physical and psychological impairments. Research has shown that persistent posttraumatic stress symptoms are associated with poorer functional recovery and physical therapy outcomes. Trauma-focused cognitive-behavioral therapy (TF-CBT) has shown moderate effectiveness in chronic pain samples. However, to date, there have been no clinical trials within WAD. Thus, this study will report on the effectiveness of TF-CBT in individuals meeting the criteria for current chronic WAD and posttraumatic stress disorder (PTSD).
Method
Twenty-six participants were randomly assigned to either TF-CBT or a waitlist control, and treatment effects were evaluated at posttreatment and 6-month follow-up using a structured clinical interview, self-report questionnaires, and measures of physiological arousal and sensory pain thresholds.
Results
Clinically significant reductions in PTSD symptoms were found in the TF-CBT group compared with the waitlist at postassessment, with further gains noted at the follow-up. The treatment of PTSD was also associated with clinically significant improvements in neck disability, physical, emotional, and social functioning and physiological reactivity to trauma cues, whereas limited changes were found in sensory pain thresholds.
Discussion
This study provides support for the effectiveness of TF-CBT to target PTSD symptoms within chronic WAD. The finding that treatment of PTSD resulted in improvements in neck disability and quality of life and changes in cold pain thresholds highlights the complex and interrelating mechanisms that underlie both WAD and PTSD. Clinical implications of the findings and future research directions are discussed.
In conclusion, being involved in an automobile accident is an undesirable situation which can result in a variety of physical trauma or injury as well as lead to the development of a number of aggravating conditions. However, stress, anxiety, depression and post traumatic stress disorder, or PTSD, are common psychological issues which may occur as a result of an automobile accident. According to research studies, physical symptoms and emotional distress may be closely connected and treating both physical and emotional injuries could help patients achieve overall health and wellness. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
According to statistics, approximately 80% of people will experience symptoms of back pain at least once throughout their lifetimes. Back pain is a common complaint which can result due to a variety of injuries and/or conditions. Often times, the natural degeneration of the spine with age can cause back pain. Herniated discs occur when the soft, gel-like center of an intervertebral disc pushes through a tear in its surrounding, outer ring of cartilage, compressing and irritating the nerve roots. Disc herniations most commonly occur along the lower back, or lumbar spine, but they may also occur along the cervical spine, or neck. The impingement of the nerves found in the low back due to injury and/or an aggravated condition can lead to symptoms of sciatica.
1. The National Institute of Public H. Folkesundhedsrapporten, 2007 (engl: Public Health Report, Denmark, 2007) 2007. p. s.112.
2. Whiplash kommisionen och Svenska Lkl. Diagnostik och tidigt omh�ndertagande av whiplashskador (engl: Diagnostics and early treatment of Whiplash Injuries) Sandviken: Sandvikens tryckeri; 2005.
3. Carroll LJ, Hogg-Johnson S, van dV, Haldeman S, Holm LW, Carragee EJ, Hurwitz EL, Cote P, Nordin M, Peloso PM. et al. Course and prognostic factors for neck pain in the general population: results of the Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders. Spine. 2008;12(4 Suppl):S75�S82. [PubMed]
4. Nijs J, Oosterwijck van J, Hertogh de W. Rehabilitation of chronic whiplash: treatment of cervical dysfunctions or chronic pain syndrome? ClinRheumatol. 2009;12(3):243�251. [PubMed]
5. Falla D. Unravelling the complexity of muscle impairment in chronic neck pain. ManTher. 2004;12(3):125�133. [PubMed]
6. Mannerkorpi K, Henriksson C. Non-pharmacological treatment of chronic widespread musculoskeletal pain. BestPractResClinRheumatol. 2007;12(3):513�534. [PubMed]
7. Kay TM, Gross A, Goldsmith C, Santaguida PL, Hoving J, Bronfort G. Exercises for mechanical neck disorders. CochraneDatabaseSystRev. 2005. p. CD004250. [PubMed]
8. Kasch H, Qerama E, Kongsted A, Bendix T, Jensen TS, Bach FW. Clinical assessment of prognostic factors for long-term pain and handicap after whiplash injury: a 1-year prospective study. EurJNeurol. 2008;12(11):1222�1230. [PubMed]
9. Curatolo M, Arendt-Nielsen L, Petersen-Felix S. Central hypersensitivity in chronic pain: mechanisms and clinical implications. PhysMedRehabilClinNAm. 2006;12(2):287�302. [PubMed]
10. Jull G, Sterling M, Kenardy J, Beller E. Does the presence of sensory hypersensitivity influence outcomes of physical rehabilitation for chronic whiplash?–A preliminary RCT. Pain. 2007;12(1-2):28�34. doi: 10.1016/j.pain.2006.09.030. [PubMed] [Cross Ref]
11. Davis C. Chronic pain/dysfunction in whiplash-associated disorders95. JManipulative Physiol Ther. 2001;12(1):44�51. doi: 10.1067/mmt.2001.112012. [PubMed] [Cross Ref]
12. Flor H. Cortical reorganisation and chronic pain: implications for rehabilitation. JRehabilMed. 2003. pp. 66�72. [PubMed]
13. Bosma FK, Kessels RP. Cognitive impairments, psychological dysfunction, and coping styles in patients with chronic whiplash syndrome14. Neuropsychiatry NeuropsycholBehavNeurol. 2002;12(1):56�65. [PubMed]
14. Guez M. Chronic neck pain. An epidemiological, psychological and SPECT study with emphasis on whiplash-associated disorders9. Acta OrthopSuppl. 2006;12(320):receding-33. [PubMed]
15. Kessels RP, Aleman A, Verhagen WI, van Luijtelaar EL. Cognitive functioning after whiplash injury: a meta-analysis5. JIntNeuropsycholSoc. 2000;12(3):271�278. [PubMed]
16. O’Sullivan PB. Lumbar segmental ‘instability’: clinical presentation and specific stabilizing exercise management. ManTher. 2000;12(1):2�12. [PubMed]
17. Jull G, Falla D, Treleaven J, Hodges P, Vicenzino B. Retraining cervical joint position sense: the effect of two exercise regimes. JOrthopRes. 2007;12(3):404�412. [PubMed]
18. Falla D, Jull G, Hodges P, Vicenzino B. An endurance-strength training regime is effective in reducing myoelectric manifestations of cervical flexor muscle fatigue in females with chronic neck pain. ClinNeurophysiol. 2006;12(4):828�837. [PubMed]
19. Gill JR, Brown CA. A structured review of the evidence for pacing as a chronic pain intervention. EurJPain. 2009;12(2):214�216. [PubMed]
20. Wallman KE, Morton AR, Goodman C, Grove R, Guilfoyle AM. Randomised controlled trial of graded exercise in chronic fatigue syndrome. MedJAust. 2004;12(9):444�448. [PubMed]
21. Hayes SC, Luoma JB, Bond FW, Masuda A, Lillis J. Acceptance and commitment therapy: model, processes and outcomes. BehavResTher. 2006;12(1):1�25. [PubMed]
22. Lappalainen R, Lehtonen T, Skarp E, Taubert E, Ojanen M, Hayes SC. The impact of CBT and ACT models using psychology trainee therapists: a preliminary controlled effectiveness trial. BehavModif. 2007;12(4):488�511. [PubMed]
23. Linton SJ, Andersson T. Can chronic disability be prevented? A randomized trial of a cognitive-behavior intervention and two forms of information for patients with spinal pain. Spine (Phila Pa 1976) 2000;12(21):2825�2831. doi: 10.1097/00007632-200011010-00017. [PubMed] [Cross Ref]
24. Moseley L. Combined physiotherapy and education is efficacious for chronic low back pain. AustJPhysiother. 2002;12(4):297�302. [PubMed]
25. Soderlund A, Lindberg P. Cognitive behavioural components in physiotherapy management of chronic whiplash associated disorders (WAD)–a randomised group study6. GItalMedLavErgon. 2007;12(1 Suppl A):A5�11. [PubMed]
26. Wicksell RK. Exposure and acceptance in patients with chronic debilitating pain – a behavior therapy model to improve functioning and quality of life. Karolinska Institutet; 2009.
27. Seferiadis A, Rosenfeld M, Gunnarsson R. A review of treatment interventions in whiplash-associated disorders70. EurSpine J. 2004;12(5):387�397. [PMC free article] [PubMed]
28. van der Wees PJ, Jamtvedt G, Rebbeck T, de Bie RA, Dekker J, Hendriks EJ. Multifaceted strategies may increase implementation of physiotherapy clinical guidelines: a systematic review. AustJPhysiother. 2008;12(4):233�241. [PubMed]
29. Verhagen AP, Scholten-Peeters GG, van WS, de Bie RA, Bierma-Zeinstra SM. Conservative treatments for whiplash34. CochraneDatabaseSystRev. 2009. p. CD003338.
30. Hurwitz EL, Carragee EJ, van dV, Carroll LJ, Nordin M, Guzman J, Peloso PM, Holm LW, Cote P, Hogg-Johnson S. et al. Treatment of neck pain: noninvasive interventions: results of the Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders. Spine. 2008;12(4 Suppl):S123�S152. [PubMed]
31. Stewart MJ, Maher CG, Refshauge KM, Herbert RD, Bogduk N, Nicholas M. Randomized controlled trial of exercise for chronic whiplash-associated disorders. Pain. 2007;12(1-2):59�68. doi: 10.1016/j.pain.2006.08.030. [PubMed] [Cross Ref]
32. Ask T, Strand LI, Sture SJ. The effect of two exercise regimes; motor control versus endurance/strength training for patients with whiplash-associated disorders: a randomized controlled pilot study. ClinRehabil. 2009;12(9):812�823. [PubMed]
33. Rubinstein SM, Pool JJ, van Tulder MW, Riphagen II, de Vet HC. A systematic review of the diagnostic accuracy of provocative tests of the neck for diagnosing cervical radiculopathy. EurSpine J. 2007;12(3):307�319. [PMC free article] [PubMed]
34. Peolsson M, Borsbo B, Gerdle B. Generalized pain is associated with more negative consequences than local or regional pain: a study of chronic whiplash-associated disorders7. JRehabilMed. 2007;12(3):260�268. [PubMed]
35. Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. ArchGenPsychiatry. 1961;12:561�571. [PubMed]
36. Wicksell RK, Ahlqvist J, Bring A, Melin L, Olsson GL. Can exposure and acceptance strategies improve functioning and life satisfaction in people with chronic pain and whiplash-associated disorders (WAD)? A randomized controlled trial. Cogn BehavTher. 2008;12(3):169�182. [PubMed]
37. Falla D, Jull G, Dall’Alba P, Rainoldi A, Merletti R. An electromyographic analysis of the deep cervical flexor muscles in performance of craniocervical flexion. PhysTher. 2003;12(10):899�906. [PubMed]
38. Palmgren PJ, Sandstrom PJ, Lundqvist FJ, Heikkila H. Improvement after chiropractic care in cervicocephalic kinesthetic sensibility and subjective pain intensity in patients with nontraumatic chronic neck pain. JManipulative Physiol Ther. 2006;12(2):100�106. doi: 10.1016/j.jmpt.2005.12.002. [PubMed] [Cross Ref]
39. Borg G. Psychophysical scaling with applications in physical work and the perception of exertion. ScandJWork EnvironHealth. 1990;12(Suppl 1):55�58. [PubMed]
40. Wallman KE, Morton AR, Goodman C, Grove R. Exercise prescription for individuals with chronic fatigue syndrome. MedJAust. 2005;12(3):142�143. [PubMed]
41. McCarthy MJ, Grevitt MP, Silcocks P, Hobbs G. The reliability of the Vernon and Mior neck disability index, and its validity compared with the short form-36 health survey questionnaire. EurSpine J. 2007;12(12):2111�2117. [PMC free article] [PubMed]
42. Bjorner JB, Damsgaard MT, Watt T, Groenvold M. Tests of data quality, scaling assumptions, and reliability of the Danish SF-36. JClinEpidemiol. 1998;12(11):1001�1011. [PubMed]
43. Ware JE Jr, Kosinski M, Bayliss MS, McHorney CA, Rogers WH, Raczek A. Comparison of methods for the scoring and statistical analysis of SF-36 health profile and summary measures: summary of results from the Medical Outcomes Study. MedCare. 1995;12(4 Suppl):AS264�AS279. [PubMed]
44. Ware JE Jr. SF-36 health survey update. Spine (Phila Pa 1976) 2000;12(24):3130�3139. doi: 10.1097/00007632-200012150-00008. [PubMed] [Cross Ref]
45. Carreon LY, Glassman SD, Campbell MJ, Anderson PA. Neck Disability Index, short form-36 physical component summary, and pain scales for neck and arm pain: the minimum clinically important difference and substantial clinical benefit after cervical spine fusion. Spine J. 2010;12(6):469�474. doi: 10.1016/j.spinee.2010.02.007. [PubMed] [Cross Ref]
46. Moher D, Hopewell S, Schulz KF, Montori V, Gotzsche PC, Devereaux PJ, Elbourne D, Egger M, Altman DG. CONSORT 2010 Explanation and Elaboration: Updated guidelines for reporting parallel group randomised trials. JClinEpidemiol. 2010;12(8):e1�37. [PubMed]
47. Subjects WDoH-EPfMRIH. WORLD MEDICAL ASSOCIATION DECLARATION OF HELSINKI. WMA Declaration of Helsinki – Ethical Principles for Medical Research Involving Human Subjects. 2008.
48. Dworkin RH, Turk DC, Peirce-Sandner S, Baron R, Bellamy N, Burke LB, Chappell A, Chartier K, Cleeland CS, Costello A. et al. Research design considerations for confirmatory chronic pain clinical trials: IMMPACT recommendations. Pain. 2010;12(2):177�193. doi: 10.1016/j.pain.2010.02.018. [PubMed] [Cross Ref]
49. Stewart M, Maher CG, Refshauge KM, Bogduk N, Nicholas M. Responsiveness of pain and disability measures for chronic whiplash. Spine (Phila Pa 1976) 2007;12(5):580�585. doi: 10.1097/01.brs.0000256380.71056.6d. [PubMed] [Cross Ref]
50. Jull GA, O’Leary SP, Falla DL. Clinical assessment of the deep cervical flexor muscles: the craniocervical flexion test. JManipulative Physiol Ther. 2008;12(7):525�533. doi: 10.1016/j.jmpt.2008.08.003. [PubMed] [Cross Ref]
51. Revel M, Minguet M, Gregoy P, Vaillant J, Manuel JL. Changes in cervicocephalic kinesthesia after a proprioceptive rehabilitation program in patients with neck pain: a randomized controlled study. ArchPhysMedRehabil. 1994;12(8):895�899. [PubMed]
52. Heikkila HV, Wenngren BI. Cervicocephalic kinesthetic sensibility, active range of cervical motion, and oculomotor function in patients with whiplash injury. ArchPhysMedRehabil. 1998;12(9):1089�1094. [PubMed]
53. Treleaven J, Jull G, Grip H. Head eye co-ordination and gaze stability in subjects with persistent whiplash associated disorders. Man Ther. 2010. [PubMed]
54. Williams MA, McCarthy CJ, Chorti A, Cooke MW, Gates S. A systematic review of reliability and validity studies of methods for measuring active and passive cervical range of motion. JManipulative Physiol Ther. 2010;12(2):138�155. doi: 10.1016/j.jmpt.2009.12.009. [PubMed] [Cross Ref]
55. Kasch H, Qerama E, Kongsted A, Bach FW, Bendix T, Jensen TS. Deep muscle pain, tender points and recovery in acute whiplash patients: a 1-year follow-up study. Pain. 2008;12(1):65�73. doi: 10.1016/j.pain.2008.07.008. [PubMed] [Cross Ref]
56. Sterling M. Testing for sensory hypersensitivity or central hyperexcitability associated with cervical spine pain. JManipulative Physiol Ther. 2008;12(7):534�539. doi: 10.1016/j.jmpt.2008.08.002. [PubMed] [Cross Ref]
57. Ettlin T, Schuster C, Stoffel R, Bruderlin A, Kischka U. A distinct pattern of myofascial findings in patients after whiplash injury. ArchPhysMedRehabil. 2008;12(7):1290�1293. [PubMed]
58. Vernon H, Mior S. The Neck Disability Index: a study of reliability and validity. JManipulative Physiol Ther. 1991;12(7):409�415. [PubMed]
59. Vernon H. The Neck Disability Index: state-of-the-art, 1991-2008. JManipulative Physiol Ther. 2008;12(7):491�502. doi: 10.1016/j.jmpt.2008.08.006. [PubMed] [Cross Ref]
60. Vernon H, Guerriero R, Kavanaugh S, Soave D, Moreton J. Psychological factors in the use of the neck disability index in chronic whiplash patients. Spine (Phila Pa 1976) 2010;12(1):E16�E21. doi: 10.1097/BRS.0b013e3181b135aa. [PubMed] [Cross Ref]
61. Sterling M, Kenardy J, Jull G, Vicenzino B. The development of psychological changes following whiplash injury. Pain. 2003;12(3):481�489. doi: 10.1016/j.pain.2003.09.013. [PubMed] [Cross Ref]
62. Stalnacke BM. Relationship between symptoms and psychological factors five years after whiplash injury. JRehabilMed. 2009;12(5):353�359. [PubMed]
63. Rabin R, de CF. EQ-5D: a measure of health status from the EuroQol Group. AnnMed. 2001;12(5):337�343. [PubMed]
64. Borsbo B, Peolsson M, Gerdle B. Catastrophizing, depression, and pain: correlation with and influence on quality of life and health – a study of chronic whiplash-associated disorders4. JRehabilMed. 2008;12(7):562�569. [PubMed]
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine





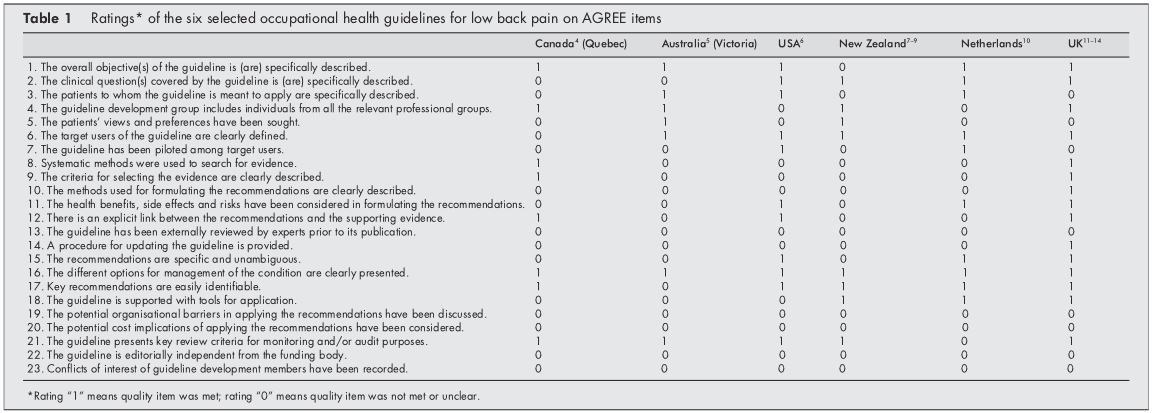
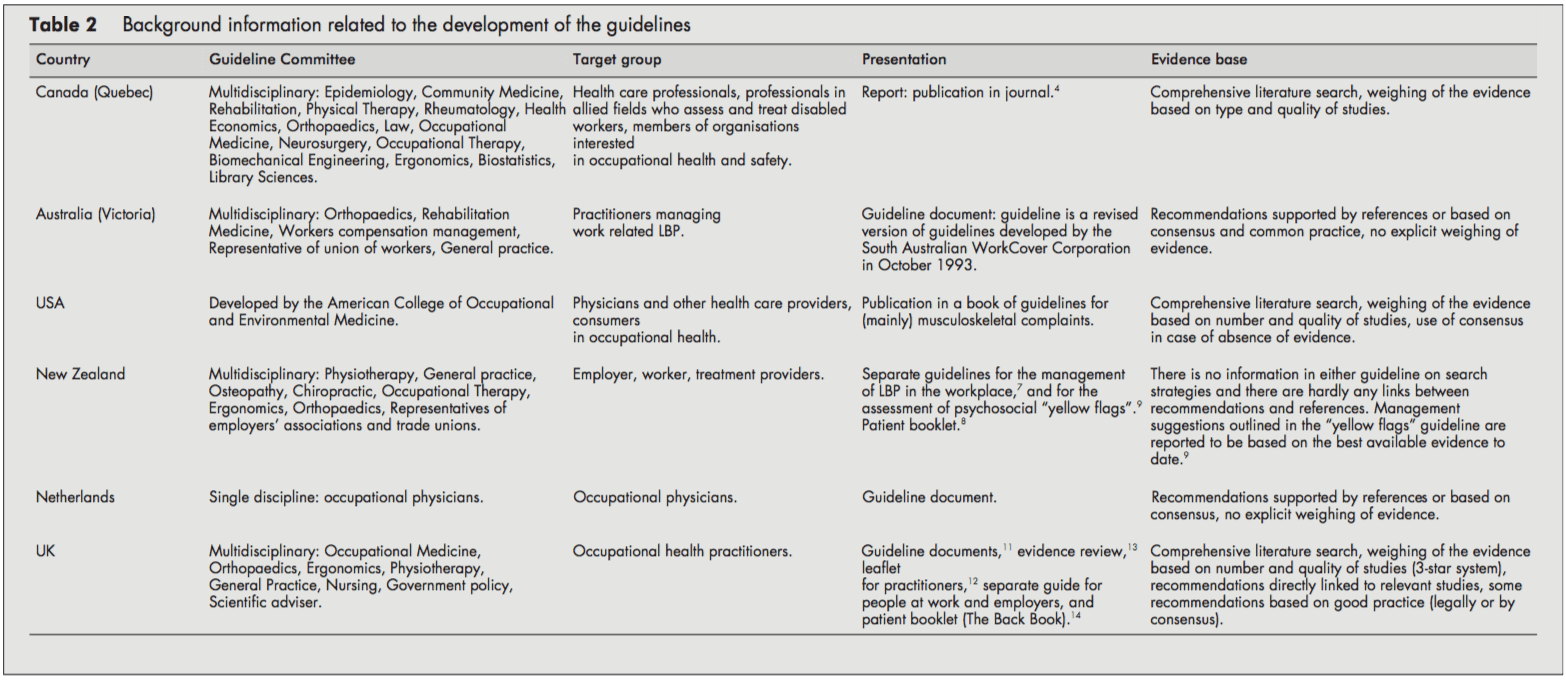
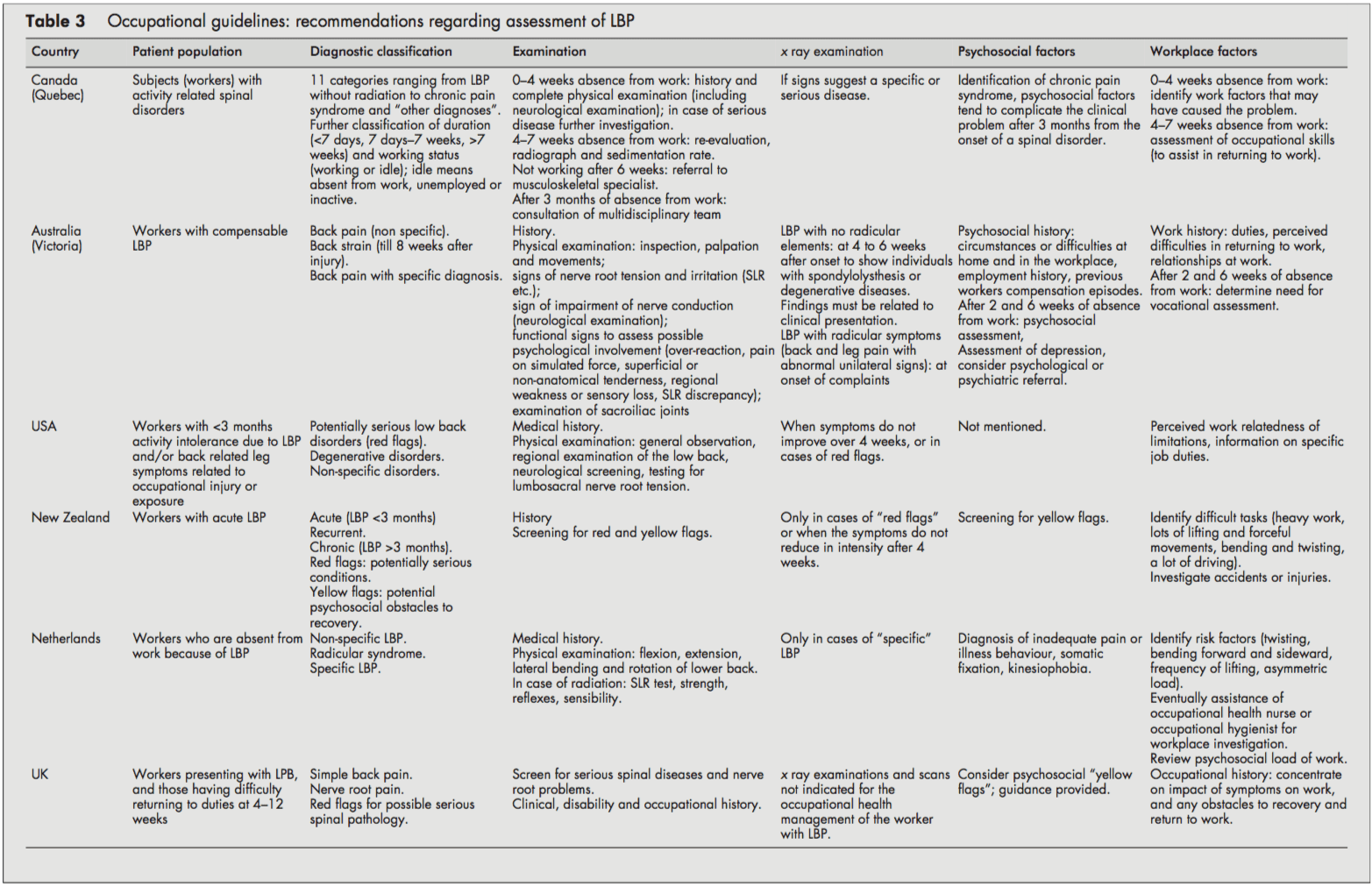
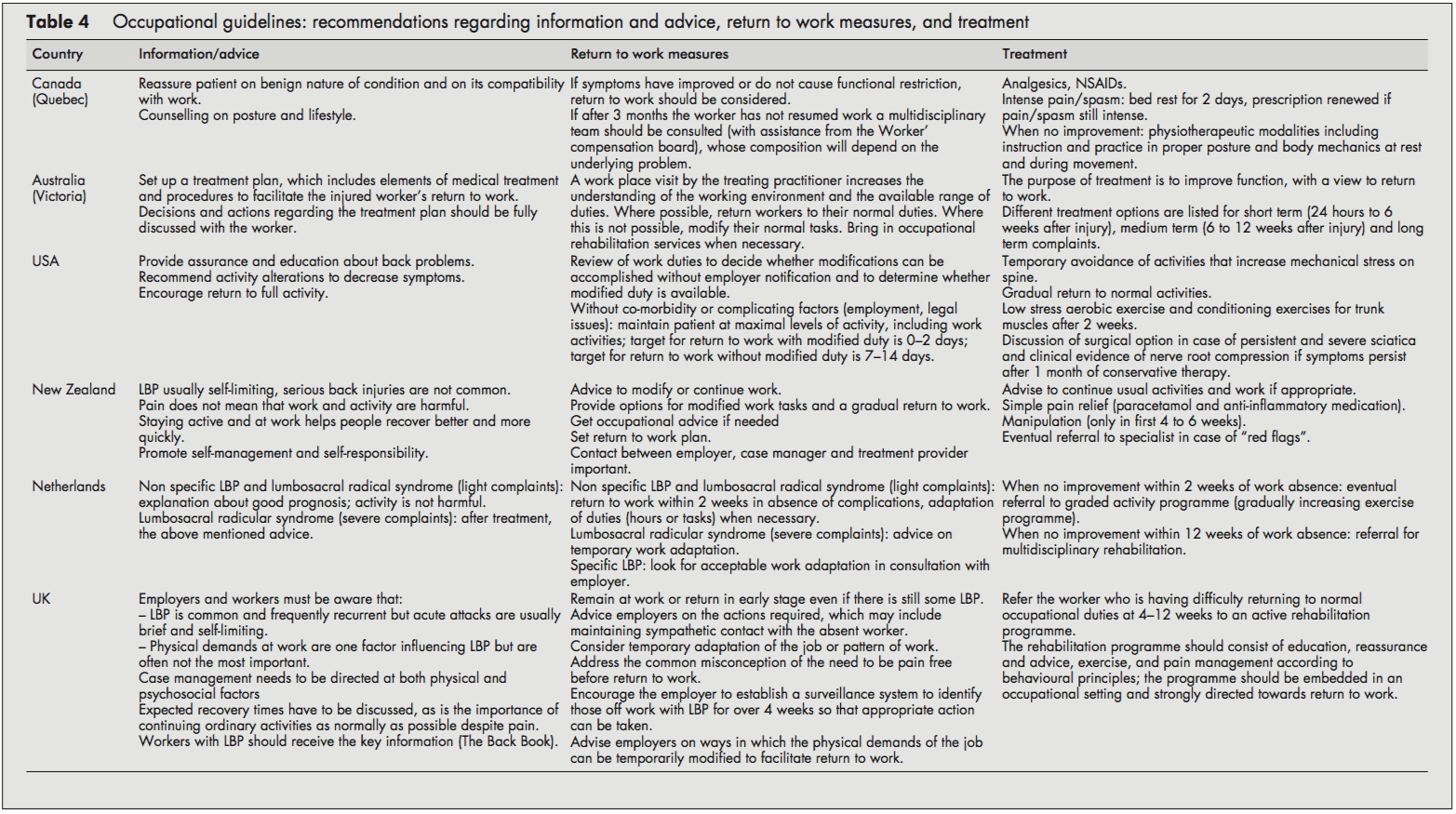
 If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.