Dr. Jimenez, D.C., presents how to prevent atherosclerosis through various therapies that can help reduce the effects of cardiovascular diseases. By understanding the risk factors causing these issues, many specialists associated with cardiovascular disorders can develop a solution to minimize these symptoms that correlate with the vital organs and muscles with a personalized treatment plan. We acknowledge patients to certified providers that provide treatment options for cardiovascular disorders that can restore body functionality and improve a person’s health. We assess each individual and their symptoms by entrusting them to our associated medical providers based on their diagnosis results for a better understanding. We recognize that education is a tremendous way to ask our providers questions about the patient’s knowledge and symptoms. Dr. Jimenez, D.C., implements this information as an educational service. Disclaimer
The Cardiovascular System & Atherosclerosis
Dr. Alex Jimenez, D.C., presents: When the body deals with various issues causing muscle and joint pain, it could be due to overlapping risk profiles affecting the cardiovascular system. In a normal functioning body, the cardiovascular system works with different systems, including the musculoskeletal system, the pulmonary system, the endocrine system, the central nervous system, and the gut system. The heart is one of the main vital organs in the cardiovascular system that supplies oxygen-riched blood to the different muscles, tissues, and organs to function properly. The oxygen-rich blood also carries other items to circulate in the body, like hormones, protein, and nutrients, to be used later. However, when environmental factors start to disrupt the body, they can affect the cardiovascular system and can do serious damage. To that point, it can develop cardiovascular diseases over time and cause body pain. Many studies and research have shown cardiovascular diseases are still the number one in the world that causes mortality and morbidity in the body. They can cause other issues that can affect the body.
One of the cardiovascular diseases that can lead to heart dysfunction is atherosclerosis. Atherosclerosis is a buildup of plaque (fats, cholesterol, and other hard, sticky substances) that builds up over time along the artery walls that can slow down the blood flow, causing less circulation in the arteries. When the circulation becomes obstructed, it can lead to ischemia associated with a blood clot due to the different body areas not getting enough blood and oxygen to function properly.
Inflammation Associated With Atherosclerosis
Dr. Alex Jimenez, D.C., presents: When this happens, there can be an imbalance of LDLs (low-density lipoproteins) which can then develop various symptoms over time that can lead to muscle and joint pain. Some of the most common underlying reasons that can cause LDL imbalances associated with atherosclerosis could include the following:
Chronic inflammation
Immune dysfunction
Oxidative stress in the vascular system
Poor diet
Tobacco exposure
Genetics
Pre-existing cardiovascular disease
When various disruptors can damage LDL, it can become oxidized over time, damage the cardiovascular endothelium wall, and cause macrophage and platelet activation. To that point, once the macrophages start to eat, they form into foam cells and then explode and release peroxidation, which means that they damage the lining of the blood vessel.
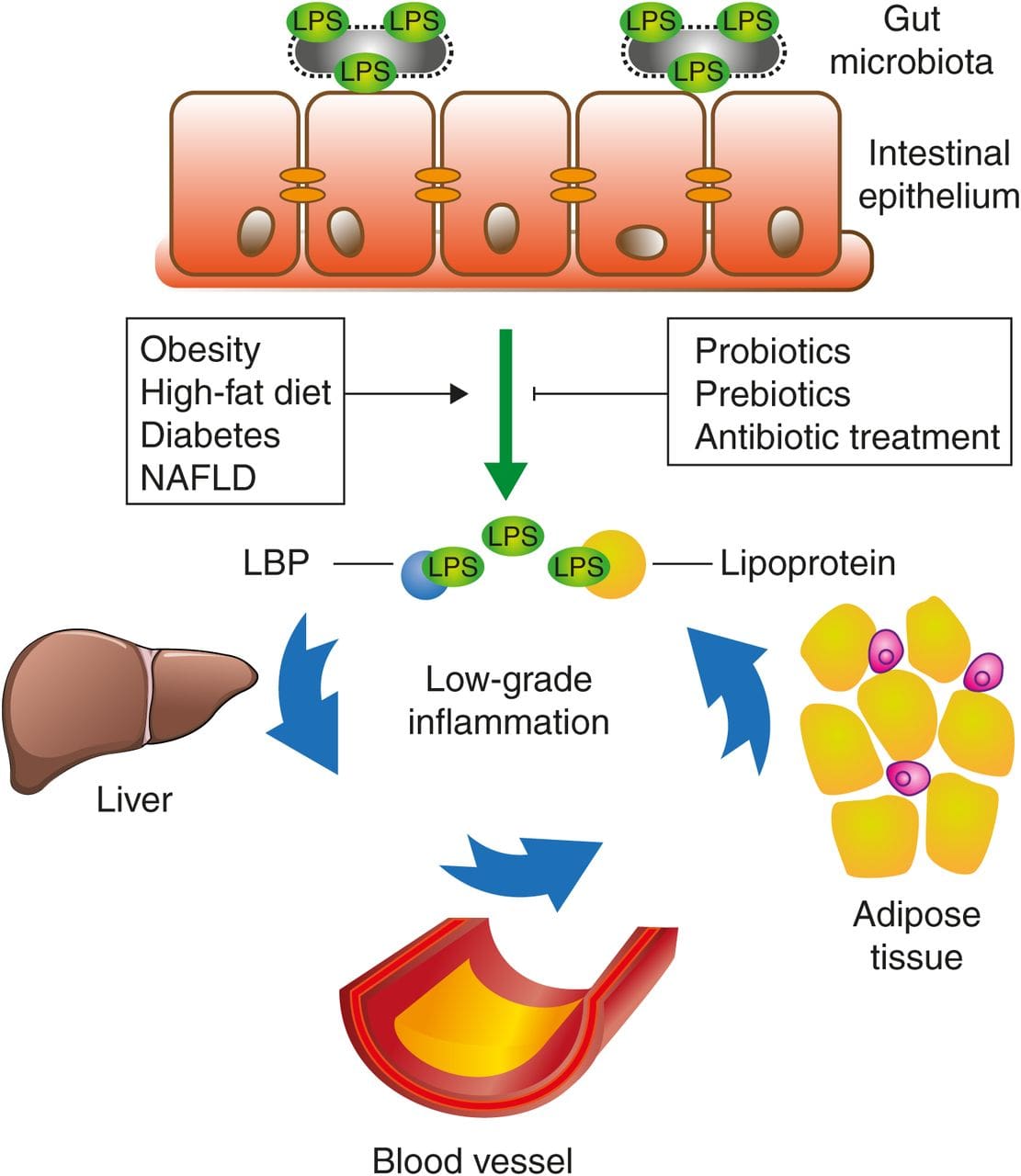
Looking closer at the oxidized LDL, it can biotransform into pro-inflammatory markers and is correlated with vascular inflammation. When dealing with vascular inflammation, the body can develop metabolic endotoxemia. Metabolic endotoxemia is where LPS (lipopolysaccharides) levels elevate even though there is a presence of infections in the body. To that point, it can correlate to gut dysbiosis and chronic inflammatory diseases to stimulate the immune system to increase NFkB inflammatory cytokines and cause muscle and joint pain.
When there is an increase in inflammation due to atherosclerosis or any cardiovascular disease an individual may have, the signs and symptoms can vary depending on their environment. Excessive weight gain, hypertension, increased oxidative stress, high triglycerides, low HDLs, etc., can affect the body and make it dysfunctional. These mechanic factors can influence dysbiosis in the cardiovascular and gut systems, leading to chronic conditions like IBS, metabolic syndrome, and cardiovascular diseases.
Treatments To Lower Inflammation
Dr. Alex Jimenez, D.C., presents: So what can we do to reduce the inflammation associated with atherosclerosis causing muscle and joint pain? Well, one of the ways that many people can do this is by eating less refined carbohydrates, and high sugar can lower high glycemic levels in the body can reduce the risk of cardiovascular diseases. Another way is to try the Mediterranean diet, which includes lean proteins, nuts, extra virgin olive oil, heart-healthy vegetables, fresh fruits, and whole grains to reduce inflammatory markers from proceeding further to causing issues in the body. Even supplements and nutraceuticals like glutathione and omega-3s can reduce chronic inflammation and cardiovascular disease complications by enhancing their antioxidant properties to preserve redox homeostasis while regulating oxidative stress in the body.
Another way people can prevent atherosclerosis is by exercising regularly. An exercise routine is an excellent way to keep the heart pumping and allow the muscles to move. Any exercise like yoga, Crossfit, dancing, swimming, walking, and running will allow more oxygen intake to the lungs, allowing the heart to pump out more blood to allow more circulation to the various organs, muscles, and tissues. Plus, any exercise can reduce plaque buildup in the arteries and reduce inflammation in the muscles and joints affecting the body.
Chiropractic Care & Inflammation
Dr. Alex Jimenez, D.C., presents: And finally, treatments like chiropractic care can help restore functionality to the body through spinal manipulation. Now, how does chiropractic care correlate with cardiovascular diseases like atherosclerosis? When the body is dealing with inflammation and chronic stress associated with atherosclerosis, the decrease in blood circulation can cause internal organ dysfunction and disrupt the transmitted signals to reach the brain. So when the transmitted signals become blocked, it can cause spinal subluxation to the spine and invokes pain in the upper, middle, and lower sections of the back, neck, hips, and shoulders. To that point, a chiropractor incorporates mechanical and manual manipulation to realign the spine and allow joint and muscle function back to the body. At the same time, chiropractic care can work with other associated medical providers to develop a personal treatment plan that allows the body to begin its recovery process.
Conclusion
Our goal is to reduce inflammation and oxidative stress in the body to dampen the effects of cardiovascular diseases associated with pain. Covering some of the different ways to prevent atherosclerosis from affecting the cardiovascular system in the body can help the vital organs and muscles from producing more inflammation associated with pain. Incorporating heart-healthy and anti-inflammatory food, taking supplements, exercising, and going to treatments can make big changes to the body. The process may be tedious, but the results will slowly improve the body’s functionality and help the individual stay on the path of health and wellness.
Dr. Jimenez, D.C., presents how to reverse dyslipidemia and atherosclerosis through various therapies that can help the body function. By understanding the risk factors causing these issues, many specialists associated with these cardiovascular risk factors can develop a solution to reduce these and other pre-existing symptoms that correlate with the vital organs and muscles. We acknowledge patients to certified providers that provide treatment options for cardiovascular disorders that can restore body functionality and improve a person’s health. We assess each individual and their symptoms by entrusting them to our associated medical providers based on their diagnosis results for a better understanding. We recognize that education is a tremendous way to ask our providers questions that apply to the patient’s knowledge and symptoms. Dr. Jimenez, D.C., implements this information as an educational service. Disclaimer
Coming Up With A Treatment Plan
Dr. Alex Jimenez, D.C., presents: Today, we will look at how to reverse dyslipidemia and atherosclerosis functionally. In the previous article, we observed the risk factors of dyslipidemia and how it is associated with metabolic syndrome. Today’s objective looks at the emerging biomarkers that could lead to dyslipidemia and atherosclerosis. Looking at the fundamental guidelines from lifestyle, nutrition, physical activity, stress response, and incorporating supplements and nutraceuticals can help many individuals transform their health from a personal perspective. To that point, everyone is different, and their treatment plans are unique as they cater to each individual regarding health and wellness.
When it comes to functional medicine, tools like the Living Matrix and the IFM allow doctors to look at results that are being presented to the patient allowing them to see their cholesterol and the history that could lead to these cardiovascular disorders. Some of the earlier studies would enable doctors to prescribe their patients to go through nutrient depletion from statin therapy to reduce the effects of cardiovascular diseases. Supplements like CoQ10, vitamin K2, omega-3 fatty acids, vitamin D, zinc, and copper are all heart-healthy supplements that can give an insight into what the individual is missing to prevent dyslipidemia and atherosclerosis. Another thing is that statin therapies could also note how the hormone levels are also being affected in the body as these cardiovascular risk factors can cause hormone levels to be lower than they are and can affect both men and women.
Cardiovascular Risk Factors & Treatments
Dr. Alex Jimenez, D.C., presents: Now, this can be a double edge sword because we know that erectile dysfunction is a vascular issue, and it allows blood flow to the reproductive system. So say, for example, if someone has poor endothelial function reduction in nitric oxide vascular disease, they will have erectile dysfunction. So when this happens, statin therapy can help the individual and improve endothelial function. Utilizing these therapies is important when dysfunction in the body can cause overlapping risk profiles to the cardiovascular system and disrupt hormone reproduction. Without these various treatments, it can lead to pain associated with these symptoms that make the body have an imbalance of hormones, high cholesterol, and other issues that affect the body. As stated earlier, everybody is different, and the treatment plans are unique as they cater to each individual.
How can we tell when a person is dealing with dyslipidemia and atherosclerosis? After the examination and listening to how the patient is doing, many doctors would combine the AAPIER and SBAR protocol to come up with a diagnosis and look at the risk factors that correlate with these disorders. When the body is dealing with various environmental factors like poor sleep quality, being under constant stress, eating food high in saturated fats, and not getting enough exercise, it can cause the body to develop high cholesterol that can lead to building up plaque in the artery walls, causing chest pain associated with the heart. This is known as somato-visceral referred pain, where the affected muscle is causing issues to the corresponding organs related to pain. Another thing is that these environmental risk factors could overlap with inflammation and cause muscle and joint pain, which can cause complaints of limited mobility and stiffness that can cause a person to feel tight and miserable.
Inflammation Is A Key Factor
Dr. Alex Jimenez, D.C., presents: Factoring inflammation as a key player affecting the body is the first step in functional medicine. When it comes to the body being in constant pain due to inflammation, chronic stress, dyslipidemia, or atherosclerosis, it can cause the brain to transmit signals through the spinal cord and cause the surrounding muscles to be sensitive. The inflammatory markers can cause many individuals to be easily confused as they think they are dealing with back pain instead of somato-visceral pain. This is because inflammation can be good or bad, depending on the severity. When the immune system begins to release inflammatory cytokines, despite no infections, bacteria, or viruses, into the cardiovascular, gut, and musculoskeletal systems, it can cause symptoms of swelling, pain, redness, and heat that can affect the corresponding organs. So inflammation affects the heart; it can cause overlapping symptoms of shortness of breath, fluid buildup, and mimic chest pains. At the same time, inflammation in the gut can lead to unwanted factors that can cause harmful changes that can impair the homeostatic mechanism and activate multiple pathways that can trigger cardiovascular disease risk factors like atherosclerosis and dyslipidemia.
Now how would atherosclerosis be correlated with the heart? When the body deals with factors that can correlate with inflammation, many factors like high blood pressure or plaque buildup cause a blockage in the arteries, which can cause blood flow reduction to the heart for circulation. When this happens, it can lead to cardiovascular disease associated with chest pains. In functional medicine, figuring out where the inflammatory effects are coming from, which is most likely in the gut, can help many individuals to reduce and reverse dyslipidemia and atherosclerosis.
Reducing Cardiovascular Risk Factors
Dr. Alex Jimenez, D.C., presents: When it comes to reducing the development of dyslipidemia and atherosclerosis, various ways can help protect vital organs and reduce the inflammatory effects in the musculoskeletal system. One of the treatments that functional medicine corresponds with is chiropractic treatment. When it comes to the organs and spinal nerves in the body, there is a connection, as all internal organs are connected through the spinal cord that sends signals to the brain. When the transmitted signals are blocked or interrupted by risk factors that have entered the body, the vital organs can not function properly. So how would chiropractic treatment help with this? A chiropractor would use manual and mechanized manipulation to realign the spine from subluxation. This will allow the blockage to interrupt the transmitted signals to function properly and restore joint function while preventing degeneration, slowing the disease’s progress in the bones, muscles, and organs.
Another way to reduce inflammatory effects in the body is by incorporating heart and gut-healthy foods that can lower inflammation and improve gut microbiome health. Eating nutritious foods that are rich in prebiotics, have anti-inflammatory properties, and have soluble fibers can help the body turn them into SCFAs (short-chain fatty acids) that allow the large intestines to create more energy for the body. Incorporating these various ways as part of the treatment plan for individuals dealing with dyslipidemia or atherosclerosis can help reverse the effects slowly.
Conclusion
Combining heart-healthy foods, exercising regularly, and changing lifestyle habits can provide amazing results when these small changes are gradually incorporated. This will allow the person to see what works and what doesn’t while constantly communicating with their medical providers to ensure they get the amazing benefits that will improve their health and wellness.
Dr. Jimenez, D.C., presents how dyslipidemia can increase the chances of various issues associated with multiple risk factors that can cause muscle and joint pain. By understanding where these issues affect the body, many specialists associated with dyslipidemia can come up with a solution to reduce dyslipidemia symptoms and other pre-existing symptoms that correlate with high cholesterol. We acknowledge patients to certified providers that provide treatment options for dyslipidemia that can restore body functionality and improve a person’s health. We assess each individual and their symptoms by entrusting them to our associated medical providers based on their diagnosis results for a better understanding. We recognize that education is a tremendous way to ask our providers questions that apply to the patient’s knowledge and symptoms. Dr. Jimenez, D.C., implements this information as an educational service. Disclaimer
The Risk Factors Of Dyslipidemia
Dr. Alex Jimenez, D.C., presents: Today we will look at the guidelines and the risk factors of dyslipidemia. When specialists utilize these guidelines that involve lipid production in the patient’s body, they use these guidelines to emphasize lifestyle therapies that can encourage more patient involvement and decision-making regarding their health. When an issue involves an increase or decrease in lipid production in the body, it can be due to lifestyle choices that can affect anyone and correlate to metabolic syndrome. In functional medicine, it is important to look, follow, and know these guidelines to understand better what is going on with the patients and come up with a treatment plan that can help reduce the risk factors of dyslipidemia and treat the symptoms associated with these risk factors.
Regarding these guidelines, doctors work with associated medical specialists that look into lipid production and develop a personalized list for the patients that shows the risk-enhancing factors causing dyslipidemia associated with cardiovascular diseases causing metabolic syndrome. Dyslipidemia is when an imbalance of lipid production in the body causes an increase in high cholesterol due to various factors that can lead to cardiovascular diseases. To that point, when a patient is dealing with high cholesterol due to a sedentary lifestyle or being constantly stressed, it can lead to an imbalance of lipid production and cause doctors to not just look at the standard lipid panels but also figure out how to come up with a treatment plan for their patients to regulate their lipid production.
How To Look For The Risk Factors Of Dyslipidemia?
Dr. Alex Jimenez, D.C., presents: So when it comes to looking at the risk factors that are developing dyslipidemia, functional medicine allows doctors to look at advanced lipid tests and evaluate the risk factors causing dyslipidemia. The evaluations of these tests find various risk factors that conventional medicine would not see, and it shows patients the importance of these results and gets their attention. To that point, many risk factors can enhance the progress of dyslipidemia. Risk factors include:
Having a family history of premature atherosclerotic cardiovascular diseases (ASCVD).
High levels of lipoprotein and triglycerides.
Excessive sedentary lifestyle.
Lack of physical activity.
Having pre-existing chronic inflammatory disorders that can cause hypersensitivity to the body.
All these risk factors can cause dyslipidemia to develop and can even overlap risk factors related to metabolic syndrome that can cause muscle and joint pain. Now how is metabolic syndrome associated with dyslipidemia?
Metabolic Syndrome & Dyslipidemia
Dr. Alex Jimenez, D.C., presents: Metabolic syndrome is a cluster of disorders that could be associated with dyslipidemia, as it can cause a person to feel miserable and affect their quality of life. When individuals have high cholesterol due to physical inactivity, not consuming lots of healthy fruits, vegetables, protein, and whole grains, smoking, or being in constant stress, it can affect the body both inside and out as it can cause a person to have imbalances of lipid and hormone function. When these imbalances affect the body, they can affect the individual’s mentality, bring down their energy to feel sluggish, and cause inflammatory issues in their joints and muscles that can lead to various injuries and diseases.
An example would be an individual who comes in dealing with back pain associated with obesity and has been dealing with high blood pressure and high cholesterol. When that person is being examined by their doctor, their results show an imbalance of how much their body produces lipids. To that point, many individuals are unaware that they have dyslipidemia unless they have a routine blood test and if it has gone severe. Other symptoms that dyslipidemia can cause in the body include:
Leg pain
Chest pain and tightness
Pain in the neck, jaw, shoulders, and back
Heart palpitations
Sleep problems
Leg swelling
If it is not treated right away, it can lead to more issues that can cause pain to the body and leave them feeling hopeless. When these unwanted symptoms and pathogens start to affect the body, it can cause the vital organs that monitor lipid production to be dysfunctional and cause chronic symptoms to rise over time.
Treatments & Guidelines For Dyslipidemia
Dr. Alex Jimenez, D.C., presents: By looking at the guidelines, we can assess the situation that the patient is dealing with, come up with an evaluation of how to reduce these risk factors that are causing dysfunction in the patient’s body, and come up with a personalized treatment plan that encourages the patient to participate in and work with other associated medical providers to ensure health and wellness to the person. All is not lost, as there are ways to reduce dyslipidemia associated with metabolic syndrome.
Treatments like chiropractic care can help restore the body’s systems through spinal manipulation in the cervical, thoracic, and lumbar regions to reduce stiffness and restore mobility to the person. An anti-inflammatory diet and exercise can help lower inflammatory effects and lower the high cholesterol the person is dealing with. And finally, exercise can help reduce stress and improve the range of motion of the body’s joints and muscles. All these treatments work together regarding a person’s health and wellness, as the body is a complex machine. The combination of functional medicine and chiropractic care can allow individuals to start making small changes in their lives to restore their health and become pain-free from metabolic syndrome associated with dyslipidemia. Remembering that it takes time for these treatments to show results of feeling good can make the journey to a healthier version of yourself worth it.
Dr. Alex Jimenez, D.C., presents how to look for signs of hormonal imbalances in men and how different treatment strategies, like chiropractic care, can help regulate hormonal functionality in the body. We direct patients to certified providers that provide functional hormonal replacement treatments that can restore body functionality. We acknowledge each patient and their symptoms by referring them to our associated medical providers based on their diagnosis to understand better what they are dealing with. We understand that education is a tremendous way to ask our providers various questions that apply to the patient’s knowledge. Dr. Jimenez, D.C., applies this information as an educational service. Disclaimer
Hormone Imbalances
Dr. Alex Jimenez, D.C., presents: Today, we will be looking at how to look for the signs of hormonal imbalances in men and how chiropractic care can help with the symptoms associated with hormonal imbalances. We need to understand the subtypes of hormonal deficiency to enable appropriate treatment strategies like chiropractic care. So when it comes to hormones in the body, it is important to know how hormones function in the body and what happens when comorbidities are associated with hormonal imbalances. The hormonal imbalances in the male body could cause physiologic effects of low testosterone correlating with disruptive factors.
Now hormones in both male and female bodies provide various actions that make the body functional. This includes:
Regulating body temperature
Sexual function
Work with other hormones (insulin, DHEA, cortisol)
Support the major body systems
When it comes to the male body, the two main hormones, androgen and testosterone, can help with cognitive function. However, when the body begins to age naturally, the hormonal process begins to decrease in the male body and causes chronic illnesses to start to cause problems in the body. When this happens, it can cause the individual to be in pain and disrupt daily activities.
Dr. Alex Jimenez, D.C., presents: Since many environmental disruptors can affect the body and cause hormonal imbalances, they can cause various symptoms in many test results when patients are being examined by their primary doctors. Signs of chronic fatigue, brain fog, depression, increased muscle mass, and low libido correlates with testosterone deficiency and can make the body dysfunctional. And if there is chronic hormonal dysfunction in the body, it can also lead to inflammation associated with hormonal deficiency. When inflammation starts to affect the muscles and joints of the male body, it can lead to issues affecting the back, hips, legs, shoulders, and neck that can cause limited mobility, muscle fatigue, increased body fat, and a decrease in bone mineral density.
Low testosterone levels in the body can overlap with pre-existing conditions that correlate with metabolic syndrome associated with hypogonadism. Hypogonadism is when the body’s reproductive organs produce little to no hormones for sexual function. Hypogonadism can affect about 30% of all males between the ages of 40-79. To that point, it causes the male body to produce more leptin hormones and can negatively affect the brain when it comes to releasing these hormones to the body. At the hypothalamic level of gonadotropin-releasing hormones, we have increased sensitivity at the hypothalamus to negative feedback from androgens. This can be many factors that can contribute to low male testosterone levels:
Diet
Stress
Toxin exposure
Osteoporosis
Decreased hair density
Erectile dysfunction
Andropause
When the reproductive organs produce little to no hormones, they can develop andropause and cause testosterone levels to diminish. Andropause is the male version of menopause for females, which can contribute to other conditions like dementia, Alzheimer’s, diabetes, and metabolic syndrome. How is metabolic syndrome associated with andropause when it comes to hormone imbalances? Well, low levels of testosterone in the body can increase insulin levels, causing insulin resistance, which then leads to an increase in BMI in the body. To that point, disorders like chronic stress can lower DHEA and testosterone hormone levels, which can then increase insulin levels and cause more pain-like issues in the body.
Chiropractic Care & Hormones
Dr. Alex Jimenez, D.C., presents: Now all is not lost, as there are ways to improve hormone production in the body. Many individuals can exercise regularly to lower cortisol and insulin levels while boosting testosterone levels. Another way to improve hormone dysfunction is by going to various therapies like chiropractic care to help reduce some of the symptoms associated with hormonal imbalances. Now how would chiropractic care be correlated with hormonal imbalances? Isn’t just manual manipulation to the back?
Surprisingly chiropractic care is more than just manipulating the spine when it is in subluxation. As stated earlier, hormonal imbalances can lead to chronic muscle and joint stress that can become inflamed and lead to chronic issues. When hormonal imbalances in the body cause low testosterone production, it can cause stress on the muscle groups and affect the joints. To that point, the body will be in constant pain or succumb to various injuries. So, incorporating chiropractic care as part of treatment can help improve the body’s musculoskeletal structure and how to deal with stress, allowing the nervous system, where hormones are being sent to different areas in the body, to function properly and operate normally. Chiropractic care enables the musculoskeletal structure to be pain-free from musculoskeletal dysfunction associated with hormone imbalances and can be combined with other treatments.
Conclusion
Utilizing and incorporating chiropractic care and hormone therapy can allow the body to function with normal hormone levels and reduce the pain-like symptoms that may affect the body’s muscles and joints. Chiropractic care combined with a nutritional diet that helps with hormone regulation and physical therapy can help the body’s hormone levels to be normal. To that point, this combination of treatments can improve muscle growth and reduce the symptoms associated with hormone imbalances that can cause muscle and joint pain associated with other pre-existing conditions related to hormone balance.
Dr. Alex Jimenez, D.C., presents the effects of metabolic syndrome that can disrupt the body’s functionality. Metabolic syndrome is a common disorder that can range from insulin resistance to inflammation and muscle pain. Considering how every person is different, we look at how metabolic syndrome is associated with insulin dysfunction and correlated with inflammation. We direct patients to certified providers that provide functional medicine treatments related to metabolic syndrome to restore body functionality. We acknowledge each patient and their symptoms by referring them to our associated medical providers based on their diagnosis for a better understanding of what they are dealing with. We understand that education is a tremendous way to ask our providers various questions that apply to the patient’s knowledge. Dr. Jimenez, D.C., applies this information as an educational service. Disclaimer
The Effects Of Metabolic Syndrome
Dr. Alex Jimenez, D.C., presents: Metabolic syndrome is a cluster of disorders that can affect the body and cause other issues to vital organs and muscle and joint functionality. Metabolic syndrome can also correlate with other conditions like diabetes and insulin resistance, which can cause referred pain in different body locations. For example, back pain associated with metabolic syndrome could overlap with obesity. So in the last article, we looked at how to recognize the causes of metabolic syndrome. In trying to understand how many people are prone to develop metabolic syndrome, we need to look at what they are eating, what kind of lifestyle they have, and if they have any pre-existing conditions. All these matters when they undergo an examination with their primary doctor.
Another thing to look into when diagnosing patients for metabolic syndrome is by looking at their genes. Whether it is a person’s lifestyle or environment, looking at a person’s genes, you will get a certain phenotype in the DNA sequence. To that point, if someone has an inflammatory lifestyle combined with a unique genetic code, functional medicine doctors can identify a bunch of comorbidities affecting the individual. With this information, doctors can inform their patients that if they don’t make small lifestyle changes, they could be at risk of developing overlapping conditions that can affect their bodies and invoke pain in the muscles, organs, and joints.
Functional Medicine & Metabolic Syndrome
Dr. Alex Jimenez, D.C., presents: That’s what the functional medicine conversation is about because we are trying to catch the issue before microvascular and macrovascular complications even set in the body. Since metabolic syndrome is a cluster of disorders, can it potentially correlate with other problems like insulin dysfunction?
Well, it can. When the body doesn’t produce enough insulin to provide energy to the body, it can lead to chronic inflammation. So whether it’s a poor lifestyle, microbiome dysfunction, visceral adiposity, or constant stress, inflammation associated with insulin dysfunction can drive the HPA axis into overdrive. Sometimes it could be not inflammation based. It could be related to mitochondrial dysfunction. So by looking at the analysis of the person dealing with metabolic syndrome, you look at their timeline, lifestyle, and the clinical imbalances driving the inflammatory markers to affect the body. The data can also look for signs of mitochondrial insults and comorbidities that could create insulin dysfunction that can lead to the development of the metabolic syndrome. This information will give functional medicine doctors a sense of what they are genetically predisposed to in their bodies.
Everyone is different, and catering to unique treatment plans for them can provide lasting results in the future. So when it comes to the functional and conventional approaches to metabolic syndrome associated with other various disorders, it is important to compare and contrast both methods to determine what the patient should consider doing to regain their health and wellness. This could be from the treatments that can work for the individual, what kind of foods can reduce the inflammatory markers and regulate hormone production, or their physical activity level. To that point, we will treat the cause through various techniques beyond pharmaceuticals and surgery as much as possible and, simultaneously, meet the patients where they are because sometimes people do well with lifestyle intervention. In contrast, others with more risks need more screening time and diagnostic tests.
Insulin Dysfunction Associated With Inflammation
Dr. Alex Jimenez, D.C., presents: Our main goal is to detect insulin dysfunction associated with inflammation that correlates with early metabolic syndrome. The lab results from our associated medical providers can tell us a story of what the patient is going through and determine whether we need to either put in nutrients that the body needs to correct or take out toxins, let’s say, that are interfering with the ability of the body to self-correct insulin dysfunction. Because preventing these comorbidities associated with metabolic syndrome can help many individuals regain their health and wellness.
Since we all have different microbiomes, the beautiful thing about functional medicine is that it brings awareness that needs to be addressed when our bodies are dealing with inflammation and insulin dysfunction that causes us to respond and use that response as an understanding of our microbiome. It allows us to reduce the effects of many issues and symptoms associated with metabolic syndrome that we may not even know about if we left it untreated. By being aware of what is causing problems in our bodies, we can make small changes in our daily life to better ourselves and our health.
Conclusion
Dr. Alex Jimenez, D.C., presents: With that being said, as stated earlier, metabolic syndrome can be a cluster of conditions that includes inflammation, insulin resistance, obesity, and hormonal dysfunction that can develop into somato-visceral or visceral-somatic issues that affect the organs and muscle groups. When all these issues begin to affect the body, they can lead to pre-existing conditions that can lead to joint and muscle pain. Regarding health and wellness, treating the effects of metabolic syndrome can do wonders for the body, mind, and soul. Making small changes to a lifestyle can provide numerous positive results and can restore functionality to the body.
Dr. Alex Jimenez, D.C., presents how many people can recognize the cause of metabolic syndrome. Metabolic syndrome is a cluster of conditions ranging from insulin resistance to muscle and joint pain. Considering how every person is different, we look at how metabolic syndrome is associated with cardiovascular disorders. We refer patients to certified providers that provide cardiovascular treatments associated with metabolic syndrome to relieve issues affecting the body while ensuring optimal wellness for the patient through various treatments. We acknowledge each patient by referring them to our associated medical providers based on their diagnosis to understand better what they are dealing with appropriately. We understand that education is an excellent way to ask our providers various intricated questions to the patient’s knowledge. Dr. Jimenez, D.C., utilizes this information as an educational service. Disclaimer
What Is Metabolic Syndrome?
Dr. Alex Jimenez, D.C., presents: Today, we are going to start widening the lens on metabolic syndrome. From a functional medicine perspective, many didn’t always call it metabolic syndrome. Other terms used to describe the diagnosis were:
Dysmetabolic syndrome
Hypertriglyceridemic waist
Insulin resistance syndrome
Obesity syndrome
Syndrome X
Metabolic syndrome is a cluster of disorders that can affect an individual’s daily life and cause various issues that can cause the body to be dysfunctional. So in 2005, the ATP three guidelines told us that patients must meet three out of five criteria to get the diagnosis of metabolic syndrome. So these are around waist circumference, which is about visceral adiposity, blood pressure, blood glucose, triglycerides, and HDL. And then you see the cutoffs there. So in the International Diabetes Federation diagnosis criteria, notice that it’s required to have central obesity, but per ethnicity-specific cutoffs for waist circumference. So instead of three out of five, you have to have one, and then the other two out of four must be met. So you see the other ones the same as before, but they’re just compartmentalized differently in this diagnosis scheme. Now let’s talk about these ethnicity-specific cutoffs.
So if you are a standard corn-fed American, your waist circumference cutoff is 40 inches as a male and 35 inches as a female. Now, if you were from different parts of the world, the numbers for waist circumference are different whether the ethnicity is Asian, Hispanic, African, European, or Middle Eastern. By looking at the diagnosis of metabolic syndrome by looking more into the ethnicity-specific cutoffs, you can see that more people would start to meet the criteria for metabolic syndrome if doctors use the stringent ethnicity-specific standards to diagnose their patients for metabolic syndrome. Other diagnoses would also notice where the visceral adiposity is at during the cutoff and see additional hints of insulin resistance. Other factors besides insulin resistance can cause the body’s systems to be dysfunctional, which will drive the common risk factors to cause the pain associated with metabolic syndrome to affect the muscles and muscle groups. When the body becomes dysfunctional due to metabolic syndrome, it can also affect vital organ systems like the cardiovascular system. Now how does metabolic syndrome correlate with the cardiovascular system?
How Does Metabolic Syndrome Associated With Cardiovascular System?
Dr. Alex Jimenez, D.C., presents: If you look at how a person’s lifestyle habits affect their body, you can see that the data shows how metabolic factors contribute to total cardiometabolic risk. This information lets the doctors and patients know about their LDL cholesterol, BMIs, family history, and blood pressure. Suppose a person has pre-existing cardiovascular issues associated with metabolic syndrome. In that case, it is important to know if their glucose levels have elevated or dropped and to see how to control those risk factors associated with cardiometabolic syndrome. These are important risk factors that have to be brought up in a metabolic dysfunction conversation to have a better understanding.
Now there are ways to reduce the effects of metabolic syndrome associated with cardiovascular diseases. By expanding the data from the patient’s test results, we can look beyond the cardiometabolic risk; we can determine the causes that are the progression of these issues affecting the body. This can be numerous issues like how much exercise the person is doing, how they deal with stress and inflammation, and what foods they eat.
By recognizing these results, we can identify things beyond metabolic syndrome and figure out what other disorders are contributing to metabolic syndrome. Many doctors will inform their patients about how their insulin levels can become elevated, which can cause them to develop insulin resistance and lose their beta cells. When insulin resistance corresponds with metabolic syndrome, many people need to realize that their genes can also play into effect. Some people have genes that drive them with the same kind of lifestyle dysfunction, inflammation, dysfunction, and insulin resistance. Their genes will also equal blood pressure issues or crazy lipid disturbances. When cardiometabolic risk factors are contributing to underlying problems affecting the body, it is really important to have functional medicine be the main focus to figure out where the issues are causing dysfunction in the body.
Insulin Resistance & Metabolic Syndrome
Dr. Alex Jimenez, D.C., presents: So when it comes to insulin resistance, it is important to take note of the abnormal beta cell function in the body if the pancreas can’t produce enough insulin to be turned into glucose. When this happens, people will begin to have elevated glucose levels, and if it continues to rise at a certain point, they will already be prone to having type 2 diabetes. To that point, the body will have this relative insulin deficiency, causing the body’s receptors not to be as sticky and functional.
When enough insulin is circulating the body and doing its job, the blood glucose levels don’t hit the threshold to become diabetes. Now, suppose the body maintains normal beta cell function. In that case, however, the insulin receptors are not working, which allows the pancreas to start pumping out insulin to be able to keep up with this resistance, causing the individual to be at a compensatory high insulin state. By stabilizing insulin levels, many individuals can control how much glucose is in their bodies. However, suppose a person is prone to becoming diabetic. In that case, all that insulin is being pumped out is a massive system biology dysfunction signaling many other nondiabetic downstream diseases.
Conclusion
So insulin dysfunction can be associated with cardiovascular disease due to poor lifestyle choices, dietary habits, and physical activity. When dealing with metabolic syndrome associated with these risk factors, it can cause the body to be dysfunctional and cause pain in the organs, muscles, and joints. This can lead to obesity and diabetes if it is not handled properly. Getting a routine started can help lower insulin resistance by eating properly, getting adequate sleep, practicing mindfulness, and exercising can help improve the body and mind.
Dr. Alex Jimenez, D.C., presents how the cause and effects of cardiometabolic risk can affect a person’s health and wellness. Cardiometabolic syndrome can affect any person through lifestyle factors and cause pain-like symptoms that can affect their well-being. We refer patients to certified providers that provide cardiovascular treatments associated with metabolic syndrome to relieve issues affecting the body while ensuring optimal wellness for the patient through various treatments. We acknowledge each patient by referring them to our associated medical providers based on their diagnosis to understand better what they are dealing with appropriately. We understand that education is an excellent way to ask our providers various intricated questions to the patient’s knowledge. Dr. Jimenez, D.C., utilizes this information as an educational service. Disclaimer
The Cause & Effects Of Cardiometabolic Risk
Dr. Alex Jimenez, D.C., presents: Now, as we enter this new era, many individuals are trying to find ways of managing cardiometabolic risk. So in this presentation, we will look at the number one killer in many modern countries; cardiovascular disease is defined as a cluster of conditions that affect the heart. Many factors are associated with cardiovascular disease that overlaps with metabolic syndrome. The word cardiometabolic hints that we will discuss something broader than cardiovascular risk.
The goal is to gain perspective on the old conversation about the cardiovascular risk associated with the circulatory system. We all know that the body’s circulatory, respiratory, and skeletal systems have different compartments that have different jobs to make the body functional. The problem is that the body operates in various systems independent of each other. They come together and interconnect like a web.
The Circulatory System
Dr. Alex Jimenez, D.C., presents: So the circulatory system helps transport blood vessels and allows the lymphatic vessels to carry cells and other items like hormones from one place to another. An example would be your insulin receptors moving information throughout your body and your glucose receptors being utilized for energy. And obviously, all other types of communicators govern how transportation happens in the body. Now the body is not a closed fixed circuit connected through the outside. Many factors can influence the body inside and outside that can affect the arterial wall and cause overlapping issues affecting the cardiovascular system. Now, what is happening to the arterial wall causing overlapping matters in the body?
When factors start to affect the arterial wall inside, it can cause plaque to form in the arterial walls and even affect the integrity of the outer walls of the arteries. When this happens, LDL or low-density lipoprotein could grow in size and cause a spike in cholesterol levels. To that point, when the body is dealing with poor lifestyle habits, it can influence the body to be at high cardiovascular risk. When the body is dealing will cardiovascular diseases at high risk, it can cause correlate to high blood pressure, diabetes, or metabolic syndrome. This causes the body to have muscular and joint pain in the back, neck, hips, and chest, to name a few, and can cause the individual to deal with inflammation in the gut, joints, and muscles.
Factors Associated With Cardiometabolic Risk Factors
Dr. Alex Jimenez, D.C., presents: But, interestingly, it’s not until recently that institutions that govern our standard of care are taking this seriously, saying it needs to be a part of the guidelines because the data is so evident that how a person’s lifestyle matters when it comes to their health. The data can range from the correlation of how certain diets, like the Mediterranean diet, can change a person’s nutritional habits. To how stress is associated with cardiometabolic disorders. Or how much exercise or sleep you are getting. These environmental factors correlate to how cardiometabolic risk factors affect the body. By informing patients what is going on with their bodies, they can finally make small changes to their lifestyle habits. Now let’s look at how nutrition can impact a person with cardiometabolic risk profiles.
By having a conversation about nutrition, many people can see the impact of the standard American diet and how it can lead to a caloric increase in central adiposity. When conversing about nutrition, it is best to note what the person is eating, causing cardiometabolic risk issues in their bodies. Doctors work with nutritionists to devise a solution to implement the right amount of protein the individual needs, how much vegetables and fruits they can consume, and what food allergies or sensitivities to avoid. To that point, informing patients about eating healthy, organic, and nutritional food will allow them to understand what they put in their bodies and how to reverse the effects. Now each person is different as certain diets are for some people while others don’t, and it is also important that by advising patients about what they are taking in and consuming but also about timing. Some people do fasting to cleanse their bodies of toxins and allow the body’s cells to find different ways to consume energy.
How Nutrition Plays A Role In Cardiometabolic Syndrome
Dr. Alex Jimenez, D.C., presents: But did you know the quality of calories in the standard American diet can damage our intestinal lining, making it vulnerable to permeability, creating this very common scenario called metabolic endotoxemia that triggers inflammation? The quality and quantity of foods can disrupt our microbiome, leading to dysbiosis as a different mechanism of inflammation. And so you get this immune activation and dysregulation that makes a constant bath in which your genes are bathing. Inflammation can be good or bad depending on the severity of what is happening in the body. If the body suffers from an injury or deals with minor issues, inflammation can help heal. Or if the inflammation is severe, it can cause the intestinal wall lining to become inflamed and leak out toxins and other microbes into the rest of the body. This is known as a leaky gut, potentially leading to muscle and joint pain associated with obesity. So we want to broaden that conversation around nutrition because obesity impacts poor nutrition. It’s commonly said that we are overfed and undernourished as a human population. So we want to be able to mitigate the trends of obesity responsibly. And we want to bring in this larger conversation about social determinants of health. As the years go by, many people are more aware of how their environment and lifestyle play a role in developing cardiovascular or cardiometabolic conditions.
We must recognize that the human body lives in this social ecosystem that determines the health potential. We want to engage the patient to bring awareness to the most potent anti-inflammatory signal into their lives and their lifestyle choice. And we are not discussing fads like putting on spandex and going to the gym once a month; we’re talking about daily movement and how to reduce sedentary behavior associated with the cardiometabolic syndrome. We discussed how even the impact of stress could promote atherosclerosis, arrhythmias, and metabolic dysfunction in the body and cause various issues that can affect a person’s well-being.
Stress & Inflammation’s Role In The Body
Dr. Alex Jimenez, D.C., presents: Stress, like inflammation, can be good or bad, depending on the scenario. So stress can impact a person’s ability to function in the world as we dive into the systems biology dysfunctions that occur from acute and chronic stress and how we can help our patients. We must understand that we should put ourselves in our patient’s shoes by figuring out how to lower chronic stress to reduce cardiometabolic risk factors and improve quality of life.
So by not being so fixated on trying everything at once to reduce cardiometabolic risk factors, taking everything that we learn and incorporating it slowly into our daily lives can make a huge impact on how we look, feel, and what we eat can improve our well-being. Dr. David Jones stated, “If all we do is talk about this and all we do is know this stuff, it doesn’t do the full service we have as an intention for our patients.”
We must get ourselves from the knowing stage into the doing stage because that’s when results will occur. So by looking at the bigger picture, we can take back our health from cardiometabolic syndrome by focusing on where the problem is happening in our bodies and going to various specialists that can develop a treatment plan to lower the stress and inflammation in our bodies that can reduce the effects of cardiometabolic syndrome.
Conclusion
Dr. Alex Jimenez, D.C., presents: So if many people are dealing with cardiometabolic risks, they have these very common systems, biology dysfunctions, whether it’s related to inflammation, oxidative stress, or insulin dysfunction, are all happening under the surface. . In functional medicine, we want to go upstream in this new era of cardiometabolic health. We want to leverage the environment and lifestyle to manipulate the system’s biology so it can be in a favorable setting to allow the epigenetic potential of the patient to be at its highest expression of health.
By providing the right tools for the patients, many functional medicine doctors can educate their patients on how to take back their health a little bit each time. For example, a person is dealing with chronic stress, causing stiffness in their necks and backs, making them unable to move around. Their doctors can devise a plan to incorporate meditation or take a yoga class to ease the stress out of their bodies and become mindful. So by gathering important clinical information about how a person is suffering from cardiometabolic, many doctors can work with their associated medical providers to devise a treatment plan to cater to each suffering from symptoms associated with cardiometabolic.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine