Common Sports Head Injuries: From Concussions to Severe Trauma
Sports bring excitement, fitness, and teamwork, but they also come with risks. One of the biggest dangers is head injuries. These can happen in any sport, from a quick bump in soccer to a hard tackle in football. The most common sports head injury is a concussion, which is a mild traumatic brain injury. But more serious ones, like brain contusions, intracranial hematomas, and skull fractures, can also occur. Understanding these injuries helps athletes, coaches, and families stay safe. This article examines the causes, signs, and treatment options, including the role of chiropractic and integrative care.
What Are Sports Head Injuries?
Head injuries in sports happen when there’s a strong force to the head or body that makes the brain move inside the skull. This can damage brain cells and change how the brain works. Common types include concussions, which are mild, and more severe ones like fractures or bleeds. According to experts, concussions make up most of these injuries, often from a blow to the head or violent shaking (Cleveland Clinic, 2024). These shakes or hits stretch nerves and blood vessels, leading to problems.
Sports head injuries are a big issue because they can affect thinking, balance, and even emotions. In the U.S., about 300,000 concussions happen each year from sports (Bailes & Cantu, 2001). While many people recover quickly, ignoring them can lead to long-term troubles like memory loss or mood changes.
The Most Common Injury: Concussions
A concussion is the top head injury in sports. It’s a mild traumatic brain injury that changes how the brain functions for a short time. It occurs when the brain bounces against the skull due to a hit or jolt. You don’t always pass out; many people stay awake but feel off.
Causes of Concussions
Concussions come from direct hits, like a helmet clash in football, or indirect ones, like a body check that shakes the head. In soccer, heading the ball can cause one to suffer a concussion (Arsenian Law Offices, n.d.). Rotational forces, where the head twists, are especially bad because they shear brain tissues (Bailes & Cantu, 2001). Sports like football, soccer, and hockey are the most prone to collisions.
Data shows that in high school sports, football has the highest rate, with tackling causing 63% of concussions (CDC, n.d.). Girls’ soccer follows, with heading the ball linked to one in three cases. Even non-contact sports like basketball can lead to them from falls or player bumps.
Symptoms of Concussions
Symptoms can appear immediately or develop later. Common ones include headache, dizziness, nausea, confusion, and sensitivity to light or noise (Mayo Clinic, 2024a). You might feel foggy, have trouble focusing, or forget things. Emotional signs, such as irritability or sadness, can also appear (Cleveland Clinic, 2024).
In some cases, people look dazed, slur their speech, or have seizures (Mayo Clinic, 2024a). Drowsiness is another sign (American Academy of Orthopaedic Surgeons, n.d.). If symptoms worsen, such as repeated vomiting or unequal pupils, it’s an emergency.
Headaches are a big part of concussions. They can come from a brain injury or related neck strain. In sports, post-traumatic headaches happen after impacts, and things like dehydration or poor posture make them worse (Studio Athletica, n.d.).
Diagnosis of Concussions
Doctors evaluate for concussions with a physical exam, asking about symptoms and testing balance, memory, and reflexes. Tools like the Sport Concussion Assessment Tool (SCAT) help evaluate (Kazl & Giraldo, 2013). Imaging, like CT scans, isn’t always needed unless symptoms are severe, as concussions don’t usually show on scans (American Academy of Orthopaedic Surgeons, n.d.).
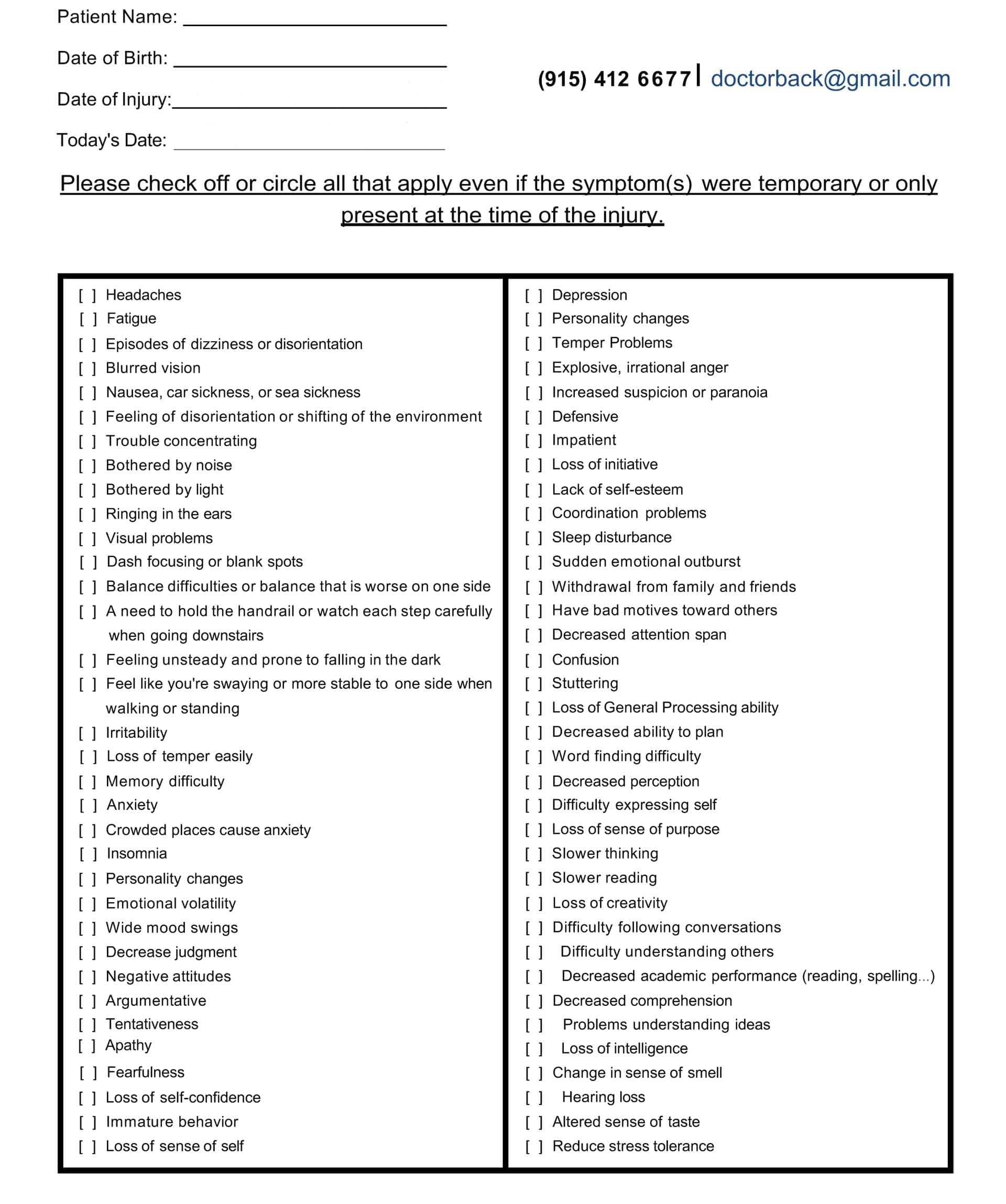
Head Injury/TBI Symptom Questionnaire
More Severe Sports Head Injuries
While concussions are common, sports can cause worse injuries. These need immediate medical help to avoid lasting damage or death.
Skull Fractures
A skull fracture is a break in the bone around the brain. In sports, it often results from hard falls or hits, such as in cycling or hockey (Children’s Minnesota, n.d.). Symptoms include headaches, swelling, bruising around the eyes or ears, and fluid from the nose or ears. It often comes with a concussion.
Treatment is rest and pain meds. Surgery is typically only required when the fracture is depressed or open. Follow-up checks ensure healing, and activity limits help recovery (Children’s Minnesota, n.d.).
Brain Contusions and Bleeds
Brain contusions are bruises on the brain from impacts. They cause swelling and can lead to bleeding. Symptoms depend on location but include confusion, weakness, or coma (Bailes & Cantu, 2001).
Intracranial hematomas are blood clots inside the skull. Types include:
Epidural Hematoma: From artery tears, often with skull fractures. It begins with a lucid period, followed by headache and confusion (Bailes & Cantu, 2001).
Subdural Hematoma: From vein tears, common in sports. It’s the top cause of severe head injury deaths in athletes. Symptoms range from alert to coma (Bailes & Cantu, 2001; Slobounov et al., 2020).
These need CT scans for diagnosis. Treatment may include surgery to remove blood and reduce pressure (WebMD, n.d.).
Sports with the Highest Risk
Some sports have more head injuries due to contact. Football tops the list, with 38.9% of concussions (Neural Effects, n.d.). Soccer, lacrosse, hockey, and wrestling follow (CDC, n.d.). In wrestling, takedowns cause 59% of concussions. Even basketball sees them from collisions.
Other risky sports include boxing, where repeated head blows lead to chronic issues, and cycling from crashes (Arsenian Law Offices, n.d.). Knowing these helps with prevention.
When to Seek Help
Any head hit needs watching. Go to a doctor if you have headaches, confusion, vomiting, or seizures (Cleveland Clinic, n.d.). Emergency signs include loss of consciousness, fluid from the ears, or worsening symptoms.
For athletes, stop playing right away. Second impacts can cause swelling or death (Cleveland Clinic, 2024).
Treatment and Recovery
Most concussions heal with rest. Avoid screens, exercise, and thinking tasks at first. Gradually add activities (Mayo Clinic, 2024b). Pain meds like acetaminophen help headaches.
For severe injuries, hospital stays, scans, and surgery may be needed (WebMD, n.d.). Recovery follows a 6-stage plan: rest, light exercise, sport drills, non-contact practice, full-contact practice, and then play (Kazl & Giraldo, 2013).
Chiropractic and Integrative Care
Chiropractic care helps with concussion symptoms by fixing spine misalignments from the injury. These can cause neck pain, headaches, and nerve issues. Adjustments improve alignment, reduce inflammation, and boost blood flow to the brain (Aurora Chiropractic, n.d.).
It targets musculoskeletal symptoms, such as stiffness, and neurological ones, including dizziness and focus problems. Techniques include spinal manipulation, soft tissue work, and exercises for balance (Mountain Movement Center, n.d.). This supports the body’s natural healing process.
Chiropractors work in teams with doctors, therapists, and nutritionists. Integrative care includes diet changes for anti-inflammation and gradual activity (Think Vida, n.d.). It helps athletes return stronger (Grant Chiropractic, n.d.).
Dr. Alexander Jimenez, a chiropractor with over 30 years of experience, notes that head injuries are frequently associated with spinal issues. He employs integrative methods, such as adjustments and functional medicine, to address root causes, thereby helping patients alleviate pain, improve balance, and promote recovery without surgery (Jimenez, n.d.; LinkedIn, n.d.). His work demonstrates that chiropractic care reduces chronic symptoms and enhances performance.
Prevention Tips
Wear helmets and gear. Learn safe techniques, like proper tackling. Coaches should educate themselves on concussion signs (CDC, n.d.). Rules against head-first contact help too.
Conclusion
Sports head injuries, especially concussions, are serious but manageable with knowledge and care. From causes like blows to treatments including chiropractic, staying informed keeps everyone safe. Always seek help for hits, and use team approaches for the best recovery.
Bailes, J. E., & Cantu, R. C. (2001). Classification of sport-related head trauma: A spectrum of mild to severe injury. Journal of Athletic Training, 36(3), 236–243. https://pmc.ncbi.nlm.nih.gov/articles/PMC155412/
Kazl, C., & Giraldo, C. (2013). Sports chiropractic management of concussions using the Sport Concussion Assessment Tool 2 symptom scoring, serial examinations, and graded return to play protocol: A retrospective case series. Journal of Chiropractic Medicine, 12(4), 252–259. https://pmc.ncbi.nlm.nih.gov/articles/PMC3838718/
Marshall, S., Bayley, M., McCullagh, S., Velikonja, D., & Berrigan, L. (2012). Clinical practice guidelines for mild traumatic brain injury and persistent symptoms. Canadian Family Physician, 58(3), 257–267. https://pmc.ncbi.nlm.nih.gov/articles/PMC3959977/
Slobounov, S. M., Haibach, P., & Newell, K. M. (2020). A foundational “survival guide” overview of sports-related head injuries. Frontiers in Neurology, 11, 571125. https://pmc.ncbi.nlm.nih.gov/articles/PMC7755598/
How Head Injuries Affect Movement—and How Chiropractic Care Gives It Back
A physiotherapist is conducting a consultation on a possible traumatic brain injury; the patient complains of back pain and mobility problems.
Head injuries and traumatic brain injuries (TBIs) can turn simple steps into big challenges. A fall, a car crash, or a sports hit can damage the brain and the nerves that tell your body how to walk, reach, or stand tall. This guide explains exactly how these injuries cause muscle fatigue, shaky balance, stiff joints, and even paralysis. You will also learn how gentle chiropractic adjustments, soft-tissue work, and targeted exercises help people move better, feel less pain, and live fuller lives.
What Happens Inside the Body After a Head Injury
When the skull jolts, the brain bounces inside. That sudden movement can tear tiny nerve wires and swell delicate tissues. The messages that once zipped from brain to legs now arrive late, weak, or not at all (Model Systems Knowledge Translation Center, 2023).
Muscle Fatigue Hits Fast
Even mild TBIs make muscles tire in minutes instead of hours. A short walk to the mailbox can feel like a marathon. Dr. Alexander Jimenez, a chiropractor and nurse practitioner in El Paso, Texas, sees this every week. “Patients tell me their legs feel like wet sandbags after five minutes of standing,” he says in his clinic videos (Jimenez, 2025).
Balance Becomes a Wobbly Game
The brain’s balance center sits deep inside the cerebellum. When it gets bruised, the ground seems to tilt. People sway, stumble, or freeze in place. One study found that even “mild” head injuries change walking patterns enough to raise fall risk by 50% (Brain Injury Association of America, 2024).
Coordination Turns Clumsy
Reaching for a coffee cup can knock over the whole table. Fine finger skills vanish. Buttons stay undone, handwriting turns shaky, and stairs feel like mountains. Physiopedia refers to this as “loss of motor dexterity” (Physiopedia, 2024).
Pain and Tiredness Make Everything Worse
Chronic headaches, neck pain, and shoulder aches are common after TBIs. When pain flares, muscles guard and stiffen. Add normal daily fatigue, and movement shuts down completely (Irvine, 2023).
Symptom Questionnaire:
From Stiffness to Locked Joints: The Contracture Trap
If a person rests too much to avoid pain, muscles shorten like dried rubber bands. Joints freeze. Doctors call these locked positions contractures. Elbows, knees, and ankles can bend only a few degrees. Contractures typically develop within weeks and become permanent within months if left untreated (Physiopedia, 2024).
Headway, a UK brain-injury charity, warns: “Lack of movement is the biggest enemy of recovery” (Headway, 2023).
How Chiropractic and Integrative Care Unlock the Body
Chiropractors do more than crack backs. They use gentle moves, hands-on muscle work, and brain-retraining exercises to restart motion and calm pain.
1. Spinal Adjustments Re-Open Nerve Highways
Misaligned neck bones pinch nerves that control arms and legs. A precise chiropractic adjustment lifts that pressure. Blood and cerebrospinal fluid flow better. Patients often feel looser the same day (Northwest Florida Physicians Group, 2023).
Dr. Jimenez films before-and-after videos: one patient who dragged her foot for two years took ten smooth steps after three visits (Jimenez, 2025).
2. Soft-Tissue Therapy Melts Tight Muscles
Fascia—the thin sleeve around every muscle—can knot after injury. Chiropractors use tools and fingers to smooth these knots. Shoulders drop, necks turn, and hips swing again (Function First, 2024).
3. Balance Boards and Eye-Tracking Drills Rewire the Brain
Simple wobble boards teach the brain to steady the body. Following a finger with the eyes rebuilds coordination pathways. These “neuro-drills” are fun and fast. Most patients notice steadier steps in four weeks (HML Functional Care, 2024).
4. Stretching Plans Stop Contractures Before They Start
Daily 10-minute routines keep joints supple. A chiropractor demonstrates the exact angle and hold time to ensure muscles lengthen safely (NR Times, 2024).
5. Posture Fixes End Headache Cycles
Slumped shoulders strain the neck and starve the brain of oxygen. One posture taping session plus two adjustments can cut headache days in half (Cognitive FX, 2024).
Real Stories That Prove It Works
Mark, age 34, car crash survivor “I couldn’t lift my toddler. After six weeks of chiropractic care, I carried her across the park.” (Patient testimonial, Apex Chiropractic, 2024)
Sarah, age 19, soccer concussion “Balance boards felt silly—until I walked the graduation stage without my cane.” (Crumley House, 2024)
Midday 10-minute walk with trekking poles, Soft-tissue massage on tight calves
Evening Wobble-board “surfing” while brushing teeth, Gentle foam-roll under guidance
Follow this for 90 days, and most people regain 70–80% of normal motion (Impact Medical Group, 2024).
When to See a Chiropractic Neurologist
Look for these red-flag signs:
Your legs drag or cross when you walk
Arms stay glued to your sides
You fall more than once a month
Painkillers no longer help
A chiropractic neurologist assesses your gait on video, tests eye reflexes, and develops a customized plan (NeuroChiro, 2024).
Science Backs the Gentle Touch
A 2022 review of 14 studies found that spinal adjustments, combined with exercise, reduced TBI pain by 41% more than exercise alone (Jimenez, 2025). Another trial showed that balance scores increased by 28 points in eight weeks with integrative care (PMC, 2022).
Safe, Drug-Free, and Covered by Many Insurances
Chiropractic care for head injuries is a non-invasive approach. No needles, no scalpels, no opioids. Most auto-insurance PIP plans and major health plans pay for 12–20 visits (Sam’s Chiropractic, 2024).
Your Next Step Today
Call a local chiropractor who lists “TBI” or “concussion” on their website.
Bring a 1-page list: “I trip, my left knee locks, headaches every afternoon.”
Traumatic Brain Injury Recovery: Effective Exercises and Chiropractic Care for Head Injuries
Rehabilitation exercises after an auto accident with head injuries.
Traumatic brain injury, or TBI, happens when a strong hit to the head harms the brain. This can come from falls, car crashes, sports, or other accidents. Head injuries are much like TBIs because they often involve the same kinds of damage to the brain and body. Recovery from these injuries requires time and effort. It focuses on getting back physical strength, mental sharpness, and balance. Rehabilitation utilizes a combination of exercises to aid recovery. These include activities that get the heart pumping, build muscle, improve steadiness, and sharpen the mind. Chiropractic care can also play a significant role, particularly in addressing issues such as headaches and dizziness. This article examines ways to recover, with a strong focus on training and improving step by step.
People with TBI or head injuries often face problems like pain, trouble moving, forgetfulness, or feeling off-balance. Starting recovery early is crucial, but it must be done slowly and safely. Doctors and therapists guide the process. Exercises help the brain rewire itself through something called neuroplasticity. This means the brain can create new pathways to repair damaged ones. Training helps build these paths. Recovery is not limited to a single type of exercise. It combines various types to cater to all needs. Let’s dive into the details.
Physical Exercises for Strength and Aerobic Health
Physical exercises are a big part of getting better from TBI or head injuries. They help rebuild muscle, boost energy, and enhance overall bodily function. Start slow because rushing can cause more harm. Always check with a doctor first.
Aerobic activities get the heart rate up without too much strain. Walking is a simple start. It can be done inside or outside, and it helps blood flow to the brain. This brings oxygen and nutrients for the healing process. Jogging on a treadmill or using a stationary bike are other options. Swimming is great too because the water supports the body, making movement easier. Aim for 150 minutes a week of moderate aerobic work, spread out over days. This could be 20 to 40 minutes per session, three to four times a week. These activities lower the risk of other health issues like heart problems or diabetes, which can slow recovery. They also lift mood and reduce tiredness.
Strength training builds muscle power. This is important because injuries can weaken muscles. Squats are a good exercise. Stand with your feet apart, as if your shoulders are wide, bend your knees as if sitting back in a chair, then stand up. Do this 10 times. Rows work the back and arms. Sit or stand, pull your elbows back like squeezing something between your shoulder blades. Use light weights or resistance bands if possible. Bicep curls are simple: Hold a water bottle, bend your elbow to bring it to your shoulder, then lower it. Repeat 10 times per arm. For legs, try seated marching. Sit in a chair and lift one knee up, then the other, like walking in place. These exercises help with daily tasks, such as getting up from a chair or carrying objects.
Other strength moves include push-ups against a wall or chair for the chest and arms. Shoulder presses: Lift arms overhead with light weights. Do these in sets, with rests in between. Strength training should be done two to three times a week, focusing on the larger muscle groups. It helps with posture and stops falls. As you become stronger, add more reps or increase the weight. But listen to your body. If it hurts, stop and rest.
Seated exercises are beneficial for individuals who are unable to stand or walk. Seated hip rotations: Sit and turn your hips side to side. This builds core strength. Alternating heel-toe raises: Lift your heels, then your toes, while sitting. These improve lower-body control and blood flow. Arm push: Push a bottle across a table with your wrist. This strengthens arms without much effort. Mixing aerobic and strength training keeps the workout fun and covers more ground for recovery.
Balance Exercises to Regain Stability
Balance problems are common after TBI or head injuries. They can cause falls and make walking hard. Balance training helps the brain and body work together better. It uses neuroplasticity to fix these issues.
Tandem stance is a basic exercise. Stand with one foot right in front of the other, like on a tightrope. Hold for 30 seconds, then switch feet. If it’s too hard, spread feet wider. Close your eyes to make it tougher once you’re ready. Weight shifts: Stand with your feet apart, shift your weight to one side, and lift the other foot slightly. Hold 30 seconds per side. This builds steadiness.
Romberg stance: Stand with feet together, eyes closed. Hold as long as you can, up to two minutes. It trains the body to use senses apart from sight for balance. Alternating heel-to-toe raises: Stand and rise on your toes, then rock back onto your heels. Do it 10 times. This strengthens legs and improves coordination.
For more challenge, use tools. A gym ball: Sit on it and reach for objects. This makes the surface unstable, forcing better control. Balance boards: Stand on a wobbly board and try not to lose your balance. Start with help. Walking on various surfaces, such as grass or sand, trains the body to adapt.
Vestibular exercises help with dizziness. These include head turns while focusing on a point, as well as eye movements such as following a finger. They retrain the inner ear and brain. Do balance work daily, but in short sessions to avoid fatigue. Progress slowly from a seated to a standing position. Good balance means safer movement and less fear of falling.
Mix balance with other training. For example, do squats while on one leg. Or walk while turning your head. This makes exercises more realistic. Recovery improves when training mimics daily activities.
Cognitive Exercises for Mental Sharpness
Mental skills can be affected after TBI or head injuries. Aspects such as memory, focus, and problem-solving require improvement. Cognitive exercises challenge the brain to build new connections.
Try new things: Walk a different path or try a new food. This sparks neuron growth. Use your non-dominant hand for tasks such as brushing your teeth. It activates the other side of the brain and strengthens thinking. Brain-training games: Play chess, Sudoku, or apps like Lumosity. These improve logic and memory.
Memorization: Recall a grocery list or song lyrics. Start small and build up. Draw maps from memory, like your route to the store. This boosts spatial thinking. Read out loud: It works reading, speaking, and listening parts of the brain.
Puzzles and games: Jigsaw puzzles or board games like Connect Four help develop planning and hand-eye coordination skills. Mental math: Add numbers in your head or count backwards by sevens. Keep a journal of senses: Note what you see, hear, and smell each day. This mixes memory and senses.
Start slow with easy tasks. Increase difficulty as you improve. Do 15-20 minutes a day. Combine with physical exercises for a complete recovery. Cognitive training helps with daily life, like remembering names or following recipes.
Integrative Chiropractic Therapy for Support
Chiropractic care helps with TBI and head injury recovery. It focuses on the spine and nervous system. This can help alleviate headaches and dizziness caused by injuries.
Adjustments align the spine, reducing nerve pressure. This improves blood flow to the brain and cuts inflammation. Craniosacral therapy: Light touch on the head and spine boosts fluid flow around the brain. It helps with headaches and brain function.
Chiropractors offer lifestyle tips, such as healthy eating and adequate sleep. They also suggest exercises, such as those for strength and balance. Combining chiropractic care with physical therapy can accelerate recovery. It addresses both body and mind.
For long-term care, regular visits prevent chronic pain. Chiropractic supports neuroplasticity by stimulating the nervous system. It’s non-invasive and can be used in conjunction with other treatments.
Insights from Dr. Alexander Jimenez
Dr. Alexander Jimenez, a chiropractor with over 30 years of experience, shares observations on TBI and head injuries. He uses integrative care for recovery. His work includes functional medicine to fix root causes. For injuries, he emphasizes the importance of prompt action with rehabilitation programs. These include exercises for mobility and nerve health. He helps with symptoms like pain and weakness through adjustments and nutrition. His clinic focuses on achieving full healing without the use of drugs or surgery.
Jimenez notes that personalized plans are most effective. He combines chiropractic with exercises to boost recovery. His insights demonstrate how training can rebuild strength and function after head injuries.
Putting It All Together for Recovery
Recovery from TBI or head injuries needs a mix of exercises and care. Focus on training: Do aerobic exercises for heart health, strength training for muscles, balance training for stability, and cognitive exercises for the mind. Add chiropractic for extra support. Start slow, be consistent, and track progress. With time, these steps lead to a better quality of life.
Always work with pros. Recovery is a journey, but training makes it possible.
How Traumatic Brain Injuries Affect Posture: From Balance Issues to Abnormal Stiffening and How Chiropractic Care Can Help
The doctor consults with the patient using the medical traumatic brain injury symptom questionnaire.
Traumatic brain injuries, or TBIs, happen when a sudden bump or blow to the head damages the brain. These injuries can range from mild, like a concussion, to severe, where the brain suffers major harm. One key way TBIs impact the body is through changes in posture—the way we hold and balance ourselves. In mild cases, individuals may experience persistent balance issues that make standing or walking difficult. In severe cases, the body can lock into stiff, unnatural positions known as abnormal posturing. TBIs can also cause the spine to shift out of place, especially in the neck and upper back areas, leading to more issues like headaches and dizziness.
This article explores these effects in detail. It examines how damage to specific brain areas, such as those involved in sensory processing, vision, or inner ear balance, can disrupt postural control. We will also discuss how chiropractic care, which focuses on fixing spine alignments, can help by improving nerve signals, blood flow, and body coordination. Drawing from medical sources and experts, such as Dr. Alexander Jimenez, a chiropractor with over 30 years of experience, we see how integrated treatments support recovery without the need for drugs or surgery.
Understanding Traumatic Brain Injuries and Their Range
TBIs affect millions each year, from sports accidents to falls or car crashes. Mild TBIs, often called concussions, might seem minor at first but can have a lasting effect on how the body maintains balance. Severe TBIs, on the other hand, can cause immediate and life-threatening changes, including rigid body positions that signal deep brain damage. Balance relies on the brain working with muscles, eyes, and the inner ear systems to keep us steady. When a TBI affects these areas, posture suffers, making everyday tasks more challenging.
Research shows that even after mild TBIs heal, people can have subtle shifts in how they control their posture. For example, studies using special tests found that those with past concussions show different patterns in body sway compared to healthy people. These changes may not be apparent in basic balance checks but become visible in more detailed analyses. This means that the brain’s ability to adapt and remain stable can weaken over time, increasing the risk of falls.
In severe TBIs, the damage often hits deeper brain parts, leading to reflexive stiffening. This is the body’s way of reacting without conscious control, and it requires prompt medical attention to prevent worse outcomes.
Symptom Questionnaire:
Subtle and Long-Lasting Balance Problems from Mild TBIs
Mild TBIs don’t always cause obvious symptoms right away, but they can quietly change postural control for months or years. Postural control refers to the brain’s ability to maintain the body’s upright and balanced position during movement or rest. It involves integrating signals from the eyes (visual system), inner ear (vestibular system), and body sensors (sensory system). A TBI can disrupt any of these, leading to dizziness, unsteadiness, or trouble walking straight.
For instance, about 30% to 65% of people with brain injuries report balance issues. These problems stem from weakened muscle strength, poor coordination, or faulty signals from the central nervous system. In one study of over 900 adults with TBIs, only 16% had normal standing balance soon after injury, showing how common these issues are. Factors like age play a role—younger people under 50 tend to recover balance more quickly—but severe injuries or complications, such as infections, can worsen the condition.
These balance changes can be subtle. People might lean to one side without noticing or feel dizzy in crowded places. Over time, this affects daily life, from climbing stairs to playing sports. The brain’s vestibular system, which regulates head position and motion, is often the most severely affected, leading to ongoing instability. Visual problems, such as blurry vision, add to the mix, making it harder for the brain to process where the body is in space.
Dr. Alexander Jimenez, a chiropractor and family nurse practitioner in El Paso, Texas, notes in his clinical work that hidden TBI symptoms, such as these balance shifts, are often overlooked. He emphasizes the importance of early checks and integrative care to identify and address issues before they worsen. His approach combines chiropractic adjustments with nutrition to support long-term healing.
Severe TBIs and Abnormal Posturing: Decorticate and Decerebrate Types
In severe TBIs, the body can exhibit abnormal posturing—stiff, reflexive poses that indicate serious brain damage. These aren’t voluntary; they’re automatic responses from damaged areas of the brain. Two main types are decorticate and decerebrate posturing, both of which require urgent care.
Decorticate posturing happens when damage affects the brain’s outer layers or midbrain pathways. The arms bend inward toward the chest, with clenched fists and curled wrists. Legs stay straight and extended, toes pointing down. The flexed upper body and rigid lower body give the person a stiff and unbalanced appearance. It’s often a sign of a head injury and can happen on one or both sides. The survival rate is about 37%, which is better than the other type, but it still means coma or deep unconsciousness.
Decerebrate posturing is more severe and often associated with deeper brain damage, such as in the brainstem. Here, arms and legs extend straight out, toes point down, and the head arches back with the neck stiff. Muscles tighten rigidly, sometimes with severe spasms called opisthotonos. This extended pose signals life-threatening issues and has only a 10% survival rate. Both types respond to pain or stimuli in unconscious people and require immediate help, like breathing support or ICU care.
These postures render balance impossible, as the body becomes rigid and inflexible. They result from disrupted nerve paths that control movement. Quick treatment focuses on stabilizing the brain to stop more damage.
Spinal Misalignments from TBIs: Adding to Posture Problems
TBIs not only damage the brain, but they can also cause spinal misalignment, particularly in the cervical and thoracic regions of the neck. This occurs due to the force of the injury, such as in whiplash resulting from a car accident. Misalignments, or subluxations, mess up posture by causing uneven weight distribution and muscle strain.
Poor spinal alignment worsens TBI symptoms. Headaches intensify from pinched nerves, and dizziness increases because blood and fluid flow to the brain gets blocked. Studies show TBIs often lead to ongoing musculoskeletal pain, like in the back or shoulders, from these shifts. In one hospital study, 85% of brain injury patients had pain, often from spine issues.
Dr. Jimenez notes a connection between TBIs and spinal issues such as disc herniations, which lead to inflammation and pain. He uses chiropractic to realign the spine and reduce these effects, promoting better posture and less dizziness.
Chiropractic Integrated Care: A Path to Recovery
Chiropractic care provides a natural approach to addressing TBI-related posture issues. It begins with spinal adjustments—gentle movements to correct misalignments. This optimizes the nervous system, as the spine protects the nerves that link the brain to the body. Better alignment means clearer signals, helping with balance and coordination.
For TBIs, chiropractic care can enhance blood and cerebrospinal fluid flow to the brain, facilitating healing and reducing inflammation. This reduces headaches, dizziness, and fatigue. Integrated care incorporates sensory and motor therapies, such as balance exercises or eye movement drills, to retrain the brain. These help rebuild postural control by strengthening muscles and improving proprioception—the sense of body position.
One approach includes soft tissue massage to ease tension and rehab exercises for strength. Lifestyle tips, such as eating anti-inflammatory foods and managing stress, support overall recovery.
Dr. Jimenez’s work highlights this integration. At his clinic, he combines chiropractic with functional medicine for TBIs, focusing on root causes like spinal shifts. His insights demonstrate how adjustments can restore mobility and reduce pain, often in conjunction with a balanced diet to combat inflammation. Patients experience improved posture and reduced symptoms through personalized plans.
Chiropractic care isn’t a cure-all, but it works well in conjunction with medical care. For mild TBIs, it alleviates ongoing balance issues; for severe cases, it supports recovery after acute treatment. The costs of TBIs run high—over $13 billion annually—so non-invasive options like this can be beneficial.
Wrapping Up: Hope Through Awareness and Care
TBIs change posture in ways big and small, from wobbly balance in mild cases to rigid posturing in severe ones. Spinal misalignments add layers of trouble, worsening headaches and instability. But chiropractic integrated care provides tools to fight back—adjustments for alignment, therapies for coordination, and holistic steps for healing.
Experts like Dr. Jimenez remind us that early action and combined treatments make a difference. If you or someone you know has a TBI, talk to a doctor about these options. With the right support, achieving better posture and an improved quality of life is possible.
Detecting Hidden Traumatic Brain Injury: How Chiropractors and Nurse Practitioners Work Together for Better Recovery
Patient answers the doctor’s traumatic brain injury questions.
Traumatic brain injuries (TBIs) affect millions each year, often in ways that are hard to spot right away. These injuries happen from falls, car crashes, sports hits, or other sudden jolts to the head or body. While severe cases show clear signs like unconsciousness or seizures, milder ones can hide in plain sight. This can lead to ongoing problems with thinking, feelings, and daily life if not caught early. Healthcare providers like chiropractors and nurse practitioners play key roles in spotting these hidden signs through careful talks with patients. By asking the right questions, they uncover subtle clues that point to brain damage.
An integrative approach combines chiropractic adjustments with nurse-led medical care. This team effort targets both the body’s frame and the brain’s wiring, helping people heal better after a TBI. Treatments include gentle spine work, muscle therapies, and custom exercises to fix imbalances and boost brain power. Nurse practitioners add layers of support for mood, energy, and overall health. Advanced tools help confirm diagnoses, starting from simple checks to high-tech scans. Missing a TBI is easy because symptoms mimic stress or fatigue, but thorough checks and treatments can change lives. This article dives into how to detect, treat, and recover from these “invisible” wounds.
The Sneaky Nature of Traumatic Brain Injuries
TBIs disrupt brain function through direct hits or shaking forces. Mild forms, like concussions, might seem minor at first but can linger. According to the Mayo Clinic, symptoms can start right after the injury or pop up days later (Mayo Clinic, 2023). This delay makes them tricky. For example, someone might walk away from a car accident feeling fine, only to struggle with focus at work weeks later. Without prompt care, these issues can worsen, leading to long-term changes in how a person thinks or feels.
The brain controls everything from movement to emotions, so damage shows up in varied ways. Physical signs include headaches that won’t quit or a constant feeling of tiredness. Cognitive hints involve forgetting simple things or zoning out during talks. Emotional shifts, like sudden anger bursts, strain relationships. Sensory changes, such as a weird metallic taste in food or a loss of smell, add to the puzzle. These aren’t always dramatic, which is why they’re often ignored. Friends or family might notice first, saying, “You’ve been off since the fall.” Early spotting is vital because the brain can rewire itself if helped soon (Hauger et al., 2024).
Statistics paint a stark picture: About 1.7 million TBIs occur yearly in the U.S., with many going undiagnosed (Reis, 2022). Military personnel and athletes face higher risks, but anyone can be hit. Children and older adults show unique signs, such as kids losing interest in play or elders stumbling more often. The key? Listen to the body’s quiet signals. Untreated TBIs raise the chances of depression, job loss, or even repeat injuries. But with awareness, recovery paths open up.
Spotting Hidden Signs: A Step-by-Step Guide for Providers
Chiropractors and nurse practitioners are on the front lines for catching TBIs. They start with a deep dive into the patient’s story. This isn’t a quick chat—it’s a series of targeted questions to peel back layers. For instance, a chiropractor might ask, “Have you noticed foods tasting off, or smells fading since your accident?” This uncovers sensory shifts linked to brain areas involved in taste and smell (Fisher Stark, P.C., n.d.). Such details often slip past standard checkups.
A thorough history covers the injury event, immediate aftermath, and ongoing quirks. Questions probe cognitive slips: “Do tasks that used to take 10 minutes now drag on for hours?” This flags concentration woes common in TBIs (BrainLine, 2023). Emotional probes include, “Have small frustrations sparked big anger lately?” Irritability or mood swings signal disrupted emotional centers (U.S. Air Force, 2017). Balance checks ask, “Do you feel wobbly in crowds or after standing quickly?” These point to coordination hits.
Symptom questionnaire:
Nurse practitioners layer in health checks, asking about sleep: “Are you crashing early but waking foggy?” Disturbed rest is a red flag (Mayo Clinic, 2023). Fatigue questions follow: “Does everyday stuff leave you wiped out?” Together, these inquiries build a full picture. Dr. Alexander Jimenez, a chiropractor and nurse practitioner, stresses personalized histories in his practice. He notes that linking subtle symptoms to past traumas helps tailor care, drawing from his work in integrative injury recovery (Jimenez, n.d.a). By cross-checking answers, providers spot patterns missed in rushed visits.
This method shines in real cases. One patient described headaches as “just stress,” but questions revealed post-accident timing, leading to TBI confirmation (Denver Chiropractic, LLC, n.d.). Multiple angles—physical, mental, sensory—ensure nothing hides. It’s simple yet powerful: Listen actively, ask openly, and connect dots.
Nuanced Symptoms: What to Watch For
TBI signs aren’t always obvious; they whisper through daily life. Cognitive disturbances top the list. Trouble focusing might mean rereading the same page over and over or missing deadlines. Memory lapses, like forgetting recent chats, disrupt routines (BrainLine, 2023). These stem from damaged brain pathways handling attention and recall.
Emotional turbulence follows closely. Anger flares over minor things, or flat moods replace joy. Depression creeps in, with unexplained sadness (U.S. Air Force, 2017). Loved ones often spot this first, as the injured person might downplay it. Dr. Jimenez observes in his clinic that these shifts strain families, urging early emotional screens (Jimenez, n.d.b).
Sensory oddities add intrigue. Taste changes turn meals bland or metallic; smells vanish, making cooking a chore (Fisher Stark, P.C., n.d.). Vision blurs, or lights sting eyes. These links to brain regions processing senses are hit hard by jolts.
Physical clues include relentless headaches, pulsing behind the eyes. Fatigue hits like a wall, even after rest. Sleep goes haywire—too much or too little, with nightmares or insomnia (Mayo Clinic, 2023). Balance falters, turning walks into teeters; coordination slips, fumbling keys or tripping.
In kids, signs differ: cranky spells, play changes, or nap shifts (BrainLine, 2023). Elders might show confusion mimicking dementia. These nuances demand vigilance. As one source notes, symptoms overlap with those of stress, delaying help-seeking (Reis, 2022). Recognizing them early prevents cascades, like poor sleep fueling more fatigue.
Building an Integrative Recovery Team
Recovery thrives on teamwork. Chiropractic care fixes body mechanics, while nurse practitioners oversee whole-body health. This blend heals the brain’s hardware and software. Spinal tweaks ease nerve pressure, boosting signals to damaged areas (Northwest Florida Physicians Group, LLC, n.d.). Nurses handle meds, nutrition, and mood support, creating balance.
Dr. Jimenez embodies this, merging his DC and APRN roles for seamless care. His clinic uses functional assessments to link spine health to brain function, echoing collaborative models (Jimenez, n.d.a). Studies back this: Teams reduce recovery time by addressing root causes (Holden et al., 2010).
Chiropractic Tools for Brain and Body Healing
Chiropractors target the spine-brain link. Adjustments realign vertebrae, improving fluid flow and nerve flow (Pinnacle Health Chiropractic, 2023). This cuts headaches and fog. Soft-tissue work kneads tight muscles, easing tension from impacts (Calibration Mansfield, n.d.).
Targeted exercises build strength and balance. Simple drills, like ball tosses, retrain coordination (HML Functional Care, n.d.). Vestibular therapies steady dizziness. Low-level lasers reduce swelling, aiding neuron repair (Reis, 2022).
Benefits stack: Better circulation delivers oxygen to the brain; balanced nerves sharpen focus (Apex Chiropractic, n.d.). One case saw a survivor return to EMT work after such care (Reis, 2022). It’s drug-free, focusing on the body’s own fixes.
Nurse Practitioners: Holistic Health Guardians
Nurses round out the plan with metabolic and emotional aid. They monitor blood sugar and electrolytes, preventing crashes that slow healing (Kim et al., 2024). Nutrition plans help fight inflammation, a key factor in TBI recovery.
Mental support includes therapy referrals and family coaching. Sedation eases agitation; family visits calm nerves (Kim et al., 2024). Dr. Jimenez integrates this, using coaching for stress and hormones (Jimenez, n.d.b). This full-spectrum care lifts mood, energy, and resilience.
Diagnostic Tools: From Basics to High-Tech
Diagnosis starts simple, scaling with needs. Basic tools include the Glasgow Coma Scale (GCS), scoring eye, verbal, and motor responses for quick severity checks (Mayo Clinic, 2023). Vital signs track blood pressure and heart rate, spotting brain pressure rises.
Next, CT scans image bleeds or swells—fast for emergencies (Mayo Clinic, 2023). MRIs detail soft tissue damage, revealing axon tears invisible on CT.
Advanced options: EEGs catch hidden seizures via brain waves (Kim et al., 2024). Neuropsychological tests probe memory and focus. Functional MRIs map active brain areas; diffusion tensor imaging traces nerve paths (HML Functional Care, n.d.).
Eye-tracking tools like RightEye assess gaze for subtle deficits (Calibration Mansfield, n.d.). Blood tests measure biomarkers for the extent of damage. Order matters: Basics rule out crises; advanced confirm and guide plans.
Why TBIs Slip Through Cracks—and How to Fix It
Traumatic Brain Injuries (TBIs) often go unnoticed because their symptoms can be mistaken for everyday life stresses. A headache? Blame work. Irritability? “Bad day.” This oversight delays care, worsening outcomes (BrainLine, 2023). Providers miss them without deep histories, as one study shows that up to 50% of mild cases go undiagnosed (Reis, 2022).
Meticulous evaluation changes this. Multi-question intakes and team huddles catch clues. Treatment urgency: Early adjustments prevent scarring; holistic plans build lasting gains. Paula’s story proves it— from bedbound to marathon training via integrated care (Reis, 2022).
In military settings, recognition cuts long-term woes (U.S. Air Force, 2017). For all, it means reclaiming life. Push for thorough checks; the brain deserves it.
Holden, C. Q., et al. (2010). Chiropractors and collaborative care: An overview illustrated with a case report. Chiropractic & Osteopathy, 18(21). https://doi.org/10.1186/1746-1340-18-21
Kim, J., et al. (2024). Nursing interventions to prevent secondary injury in critically ill patients with traumatic brain injury: A scoping review. Journal of Clinical Medicine, 13(8), 2396. https://doi.org/10.3390/jcm13082396
Chiropractic & Manual Therapies. (2018). Be good, communicate, and collaborate: A qualitative analysis of stakeholder perspectives on adding a chiropractor to the multidisciplinary rehabilitation team. Chiropractic & Manual Therapies, 26(17). https://doi.org/10.1186/s12998-018-0200-4
Achieve pain relief with heel pain chiropractic care targeting Achilles tendon concerns for a better quality of life.
Understanding Achilles Tendon Heel Pain: A Comprehensive Guide to Chiropractic Care and Natural Recovery
Heel pain affecting the Achilles tendon is one of the most common complaints among active individuals, weekend warriors, and even those with sedentary lifestyles. This debilitating condition can significantly impact your quality of life, limiting your ability to walk, run, or even stand comfortably. While many people immediately think of medications or surgery as solutions, chiropractic care offers a comprehensive, non-invasive approach to addressing the root causes of Achilles tendon pain and promoting natural healing. This guide explores the anatomy, biomechanics, causes, and evidence-based treatments for Achilles tendon heel pain, with a special focus on how chiropractic care can restore function and reduce discomfort.
Understanding the Achilles Tendon: The Body’s Strongest and Most Vulnerable Tendon
The Achilles tendon holds the distinction of being both the largest and strongest tendon in the human body, yet it remains paradoxically one of the most commonly injured structures in the lower extremity. This remarkable structure connects the powerful calf muscles to the heel bone, creating a critical link in the kinetic chain that allows us to walk, run, jump, and stand on our toes.
Despite its impressive strength, the Achilles tendon is uniquely vulnerable to injury. Research shows that this tendon can bear loads up to 12 times body weight during running and up to 3,500 Newtons of force before rupture. However, a hypovascular area exists approximately 2 to 6 centimeters proximal to the calcaneal insertion, where blood supply is significantly reduced. This zone of poor vascularity makes the tendon particularly susceptible to degenerative changes and injury.
Understanding the complexity of the Achilles tendon helps us appreciate why a comprehensive, whole-body approach like chiropractic care can be so effective. Rather than simply treating the symptoms at the site of pain, chiropractors evaluate the entire musculoskeletal system to identify biomechanical imbalances that may contribute to excessive stress on the tendon.
Anatomy and Biomechanics of the Achilles Tendon: A Marvel of Engineering
Structural Composition
The Achilles tendon, also known as the calcaneal tendon or triceps surae tendon, is formed by the confluence of three muscles: the gastrocnemius (with its medial and lateral heads) and the soleus muscle. The gastrocnemius originates from the posterior aspect of the femoral condyles, while the soleus arises from the posterior surface of the fibula and medial border of the tibia. These muscles coalesce distally to form the common Achilles tendon, which inserts onto the middle portion of the posterior calcaneal surface.
Compositionally, the Achilles tendon consists of approximately 95% type I collagen fibers, which provide exceptional tensile strength and flexibility. The remaining 5% includes type III collagen, elastin (accounting for up to 2% of dry mass), proteoglycans, and glycosaminoglycans. This hierarchical structure organizes into fibrils, fibers, and fascicles bound together by small matrix molecules.
A distinctive feature of the Achilles tendon is its spiral configuration. As the tendon descends toward its insertion, the fibers rotate approximately 90 degrees, causing the medial gastrocnemius fibers to become superficial while the lateral gastrocnemius and soleus fibers become deeper. This spiraling creates an area of concentrated stress but also confers a significant mechanical advantage during propulsion activities.
The Paratenon: A Unique Protective Sheath
Unlike many tendons, the Achilles does not possess a true synovial sheath. Instead, it is surrounded by a paratenon—a thin layer of loose connective tissue that provides a significant portion of the tendon’s blood supply and allows for gliding movement of up to 2-3 centimeters. The paratenon contains elastin and extends into the tendon, binding collagen bundles together while permitting movement among them.
Blood Supply and Vulnerability
The vascular supply to the Achilles tendon comes from three sources: the musculotendinous junction, vessels in the surrounding connective tissue (primarily the paratenon), and the osteotendinous junction. The vascular territories can be classified into three regions, with the midsection supplied by the peroneal artery and the proximal and distal sections supplied by the posterior tibial artery. This arrangement leaves a relatively hypovascular area in the mid-portion of the tendon—precisely where most pathology occurs.
Biomechanical Properties
The Achilles tendon demonstrates nonlinear mechanical properties at low strains, exhibiting what is known as a “toe region” in its force-displacement curve. This nonlinearity arises from the uncrimping of collagen fibers and an associated increase in collagen alignment as load is applied. Under polarized light, tendons exhibit periodic banding due to their waveform configuration known as “crimp,” which extends hierarchically from macro- to nano-structural scales.
At higher strains, the tendon deforms linearly prior to yield and rupture. While traditionally described as viscoelastic (containing both elastic and viscous components), recent evidence in humans suggests that its elastic properties dominate. These spring-like properties allow the Achilles tendon to store and release energy efficiently during ambulation, delivering explosive propulsion while protecting soft tissues from damage.
Functions of the Achilles Tendon in the Lower Body and Extremities
Primary Function: Plantarflexion
The primary function of the Achilles tendon is to enable plantarflexion of the foot—the movement that points the toes downward and lifts the heel off the ground. This action is fundamental to virtually all lower extremity movements, including walking, running, jumping, climbing stairs, and standing on tiptoes. The gastrocnemius muscle also contributes to knee flexion, adding another dimension to lower extremity function.
Force Transmission and Lever Action
The calcaneus (heel bone) acts as a lever arm for the triceps surae muscles, and the Achilles tendon serves as the critical link that transmits force from the calf muscles to the heel bone. This arrangement allows for efficient transfer of muscular force to the foot during the propulsive phase of gait. The heel bone projects posterior to the tibia and fibula, creating a mechanical advantage that amplifies the force generated by the calf muscles.
Shock Absorption and Energy Storage
During walking, the heel can absorb approximately 110% of body weight, and during running, this increases to 200% of body weight. The Achilles tendon, in conjunction with the plantar fascia and the specialized fat pad beneath the heel, functions as part of an integrated shock absorption system. The elastic properties of the tendon allow it to store mechanical energy during the loading phase of gait and release it during toe-off, improving efficiency and reducing metabolic cost.
Role in Postural Control and Balance
Vibration studies have demonstrated that the Achilles tendon plays a crucial role in postural orientation and balance. When the tendon is vibrated without visual input, subjects experience movement backwards and the illusion of forward body tilt. This occurs because vibrations stimulate muscle spindles in the calf muscles, alerting the brain to body position and initiating compensatory movements through the central nervous system.
Integration with the Kinetic Chain
The Achilles tendon does not function in isolation but rather as an integral component of the lower extremity kinetic chain. Problems with foot alignment, ankle mobility, knee position, hip alignment, or even spinal posture can alter the biomechanical forces acting on the Achilles tendon. This interconnected system explains why chiropractors examine the entire body when evaluating Achilles tendon pain, rather than focusing solely on the local area of discomfort.
Factors Leading to the Development of Heel Pain Associated with the Achilles Tendon
Achilles tendinopathy develops through a complex interplay of intrinsic and extrinsic factors that create an imbalance between the loading demands placed on the tendon and its capacity to adapt and recover.
Intrinsic Risk Factors
Muscle Strength and Weakness: Expert consensus identifies muscle strength, particularly plantarflexor weakness, as the primary modifiable risk factor for Achilles tendinopathy. Studies of military recruits have shown that plantarflexor strength is predictive of tendinopathy development. When the calf muscles are weak or fatigued, the Achilles tendon must bear disproportionate loads, increasing the risk of microtrauma and degeneration.
Previous Injuries and Incomplete Rehabilitation: A history of prior Achilles tendinopathy or incomplete recovery from previous injuries significantly increases the risk of recurrent problems. Residual strength deficits, altered neuromuscular control, and persistent structural changes may explain why previous injury is such a strong risk factor.
Age and Degenerative Changes: While age itself is not directly causal, age-related reductions in tendon vascularity, collagen quality, and muscle strength contribute to increased vulnerability. Achilles tendinopathy is most commonly seen in individuals aged 30-50 years, with middle-aged recreational athletes being particularly susceptible.
Anatomical Factors: Foot structure and alignment play crucial roles in tendinopathy development. Excessive pronation (rolling inward of the foot), high arches (pes cavus), flat feet (pes planus), limited ankle dorsiflexion, varus alignment with functional hyperpronation, leg length discrepancies, and excessive tibial torsion can all alter the distribution of forces through the Achilles tendon.
Systemic Conditions: Metabolic and systemic diseases can affect tendon health and increase vulnerability to injury. These include diabetes mellitus, thyroid and parathyroid disorders, gout, collagen deficiencies, hypercholesterolemia, and autoimmune conditions. Blood group O has also been associated with increased incidence of Achilles tendinopathy and rupture.
Genetic Factors: Family history appears to be a risk factor, with individuals who have a positive family history of Achilles tendinopathy having a five-fold greater risk for such injuries. Genetic factors may influence collagen structure, muscle fiber composition, and tendon morphology.
Extrinsic Risk Factors
Training Errors and Load Management: Changes in loading patterns represent the most consistently ranked extrinsic risk factor for Achilles tendinopathy. Sudden increases in training volume or intensity, particularly after layoffs or recovery periods, create a mismatch between tendon capacity and demands. Other problematic training errors include changes in training type (such as adding hill work), alterations in training due to events or competitions, excessive training intensity, inadequate recovery between sessions, and abrupt increases in weekly distance.
Overuse and Insufficient Recovery: The concept of “training errors” encompasses insufficient recovery periods between bouts of activity. Studies have shown that muscle weakness and fatigue may persist for up to 47 days after a single exercise session, even when individuals report feeling “recovered”. Continuing to train despite ongoing neuromuscular deficits inadvertently increases tendinopathy risk.
Footwear Issues: Improper footwear can contribute to Achilles problems through inadequate support, insufficient cushioning, worn-out shoes, heel counter pressure against the posterior heel, and inappropriate shoes for specific activities. For cyclists, low saddle height resulting in excessive ankle dorsiflexion during pedaling may be a causative factor.
Training Surface: Hard or uneven training surfaces can increase impact forces and alter biomechanics, contributing to overload of the Achilles tendon. Sudden changes in training surface (such as moving from a treadmill to outdoor pavement) can precipitate symptoms.
Medications: Certain medications, particularly fluoroquinolone antibiotics, corticosteroids, and anabolic steroids, have been associated with increased risk of Achilles tendinopathy and rupture. These medications may affect collagen synthesis, reduce tendon strength, or impair healing processes.
Pathophysiology: From Overload to Degeneration
The pathological process in Achilles tendinopathy represents failed healing or degenerative changes resulting from continuous overloading. Contrary to traditional understanding, chronic Achilles tendinopathy is not primarily an inflammatory condition (despite the term “tendinitis” suggesting inflammation). Histological examination reveals degenerative changes including collagen disorganization, increased type III collagen production, proteoglycan accumulation, neovascularization (new blood vessel formation), and nerve ingrowth.
The repetitive microtrauma hypothesis suggests that excessive stretching and loading create microscopic tears in the collagen matrix. When recovery time is insufficient, these microtears accumulate, overwhelming the tendon’s repair mechanisms. The resulting degenerative process involves tenocyte death, collagen fiber disruption, and areas filled with vessels and nerves that may contribute to pain.
How Heel Pain Can Mimic Sciatica Pain: Understanding Referred Pain Patterns
One of the most clinically challenging aspects of heel pain is its potential to mimic or coexist with sciatica, creating diagnostic complexity and potentially delaying appropriate treatment.
The Sciatic Nerve and Referred Pain
The sciatic nerve is the largest nerve in the human body, originating from the L4-S3 nerve roots in the lower spine and traveling through the buttocks and down the leg to the foot. When this nerve becomes compressed or irritated—a condition known as sciatica—it can produce pain, tingling, numbness, and weakness that radiates along its entire pathway.
Critically, sciatica can cause referred pain in the heel through several mechanisms. The L5-S1 nerve root provides segmental innervation to the posterior thigh, gluteal muscles, and the anterior, posterior, and lateral leg muscles, as well as sensory innervation to the heel. Compression or irritation of this nerve root can produce heel pain that patients may attribute to a local foot problem rather than a spinal origin.
Distinguishing Features
Understanding the differences between true Achilles tendinopathy and sciatica-related heel pain is essential for appropriate treatment:
Achilles Tendinopathy Characteristics:
Pain localized to the posterior heel and along the tendon
Tenderness to palpation of the Achilles tendon
Morning stiffness that improves with initial movement but may worsen with continued activity
Pain worsens with activities that load the tendon (walking, running, jumping)
No radiating pain up the leg
No neurological symptoms such as numbness or tingling
Sciatica-Related Heel Pain Characteristics:
Pain radiating from the lower back through the buttocks and down the leg to the heel
Numbness, tingling, or burning sensations in the leg or foot
Weakness in the leg or foot muscles
Pain may worsen with prolonged sitting, standing, or certain movements
Possible positive findings on nerve tension tests (straight leg raise)
Possible altered reflexes, particularly the ankle reflex
Chiropractic Care for Leg Instability- Video
The Double-Crush Phenomenon
Clinicians must also be aware of the “double-crush syndrome,” in which concomitant proximal and distal nerve entrapments occur simultaneously. A patient could have both lumbar radiculopathy causing sciatic symptoms and local nerve compression in the foot (such as tarsal tunnel syndrome), creating complex and overlapping pain patterns.
Clinical Implications for Chiropractic Care
The potential for sciatica to cause or contribute to heel pain underscores the importance of comprehensive evaluation by healthcare providers trained in whole-body assessment. Chiropractors are uniquely positioned to evaluate both spinal and peripheral sources of heel pain, ensuring that treatment addresses all contributing factors rather than focusing exclusively on local symptoms.
Clinical Rationale: Why Chiropractic Care Can Help Reduce Heel Pain in the Achilles Tendon
Chiropractic care offers a comprehensive, evidence-informed approach to managing Achilles tendon heel pain that addresses both local tissue dysfunction and systemic biomechanical imbalances.
Addressing Biomechanical Dysfunction in the Kinetic Chain
A fundamental principle of chiropractic philosophy is that the body functions as an integrated kinetic chain, where dysfunction in one area creates compensatory stress in others. The feet serve as the foundation for the entire skeletal system, and problems with foot alignment can cause cascading effects upward through the ankles, knees, hips, and spine.
Research confirms this interconnected relationship. Excessive pronation causes the arches to flatten and ankles to roll inward, forcing internal leg rotation, pelvic tilt, and lower back stress. Conversely, spinal misalignments, pelvic imbalances, or hip dysfunction can alter gait patterns and weight distribution, placing abnormal stress on the Achilles tendon.
Chiropractic adjustments to the spine, pelvis, hips, knees, ankles, and feet help restore proper alignment throughout the kinetic chain. By correcting misalignments (subluxations) in these areas, chiropractors reduce compensatory strain on the Achilles tendon and surrounding structures.
Improving Joint Mobility and Function
Limited ankle dorsiflexion and restricted foot and ankle joint mobility are established risk factors for Achilles tendinopathy. Chiropractic adjustments specifically directed at the foot and ankle can improve joint mobility, decrease pain, and enhance function.
A case series published in the Journal of Physical Therapy Science demonstrated that the addition of joint mobilization and manipulation to eccentric exercise programs produced immediate within-session improvements in pain, heel raise repetitions, and pressure pain thresholds in runners with chronic Achilles tendinopathy. At discharge and nine-month follow-up, patients showed improvements in self-reported function, pain levels, joint mobility, ankle motion, and single-leg heel raises.
The mechanisms underlying these improvements include decreased nociceptive reflex excitability, enhanced conditioned pain modulation, reduction of bilateral hyperalgesia following unilateral joint mobilization, and improved biomechanical function through restored joint alignment.
Enhancing Blood Flow and Tissue Healing
The Achilles tendon receives relatively poor blood supply, particularly in the vulnerable mid-portion region. Chiropractic care can assist in recovery from tendon injuries by improving circulation to the area. Manual techniques, including soft tissue mobilization and specific adjustments, may stimulate local blood flow, enhancing nutrient delivery and waste removal from the healing tendon.
Research on manual therapy for tendinopathy suggests that soft tissue and joint-directed techniques can decrease pain, improve mobility, and enhance muscle performance—all relevant for persons with Achilles tendinopathy. While manual therapy effects are typically short-lived, when performed prior to exercise and reinforced with subsequent activities, it can reduce pain sensitivity and increase range of motion, allowing individuals to participate more actively in tendon loading progressions.
Reducing Compensatory Muscle Tension
Muscle imbalances and excessive tension in the calf muscles (gastrocnemius and soleus) contribute to increased stress on the Achilles tendon. Chiropractors employ various soft tissue techniques, including myofascial release, trigger point therapy, instrument-assisted soft tissue mobilization (IASTM), and massage therapy to release tension in the calf muscles, plantar fascia, and surrounding structures.
These techniques not only provide pain relief but also improve tissue extensibility and flexibility, allowing for more normal tendon loading during movement. By addressing muscle dysfunction both locally and remotely (including muscles of the hip and trunk), chiropractors help reduce the overall stress on the Achilles tendon.
Neurological Effects and Pain Modulation
Chiropractic adjustments and manual therapy techniques produce neurophysiological effects that extend beyond simple mechanical realignment. Research demonstrates that spinal and extremity manipulation can increase stimulability of alpha motor neurons, enhance activity in corticospinal pathways, alter sensorimotor cortex activity, and modulate pain processing through effects on the central nervous system.
Joint mobilization has been associated with reduced sensitivity to pain, improved pain tolerance, and enhanced endogenous pain inhibition mechanisms. These neurological effects complement the biomechanical benefits of chiropractic care, providing multi-level pain relief for patients with Achilles tendinopathy.
Evidence Supporting Chiropractic Management
Multiple studies and case reports support the effectiveness of chiropractic care for Achilles tendinopathy:
A 2012 case study published in the Journal of Canadian Chiropractic Association reported successful management of midportion Achilles tendinopathy using chiropractic interventions, with rapid cessation of pain.
Research comparing chiropractic adjustments with daily stretching to custom orthotics alone found significant improvements in both groups, with the chiropractic care group showing advantages in pain ratings at the 15-day mark.
Case series combining manual therapy with eccentric exercise have demonstrated superior outcomes compared to exercise alone, particularly in the first four weeks of treatment.
Dr. Alexander Jimenez’s Clinical Approach: Integrating Advanced Diagnostics with Dual-Scope Care
Dr. Alexander Jimenez, DC, APRN, FNP-BC, CFMP, IFMCP, brings a unique dual-licensed perspective to the treatment of Achilles tendon heel pain and lower extremity injuries. As both a licensed chiropractor and a board-certified Family Practice Nurse Practitioner, Dr. Jimenez combines the biomechanical expertise of chiropractic care with advanced diagnostic capabilities and medical management.
Comprehensive Patient Evaluation
Dr. Jimenez’s approach begins with thorough patient assessment that examines not only the local site of pain but the entire musculoskeletal and neuromuscular system. His evaluation protocols include detailed medical history taking, comprehensive physical examination of the spine, pelvis, lower extremities, and feet, gait analysis to identify biomechanical abnormalities, orthopedic and neurological testing, and assessment of functional movement patterns.
This comprehensive evaluation allows Dr. Jimenez to identify all contributing factors to a patient’s heel pain, including spinal misalignments affecting the kinetic chain, muscle imbalances and weakness, joint restrictions in the foot and ankle, faulty foot mechanics (pronation/supination), and potential systemic factors influencing tissue health.
Advanced Imaging and Diagnostic Evaluation
One of Dr. Jimenez’s distinguishing characteristics is his ability to integrate advanced imaging and diagnostic evaluations into treatment planning. His dual licensure enables him to order and interpret diagnostic studies including musculoskeletal ultrasound for visualizing tendon structure and pathology, magnetic resonance imaging (MRI) to assess tendon integrity, inflammation, and surrounding structures, X-rays to evaluate bone alignment and rule out fractures or bone spurs, and specialized laboratory testing when systemic conditions are suspected.
This diagnostic capability ensures accurate diagnosis and allows for monitoring of treatment progress and tissue healing. Dr. Jimenez can differentiate between insertional and non-insertional Achilles tendinopathy, identify concurrent pathologies such as retrocalcaneal bursitis or Haglund’s deformity, assess the degree of tendon degeneration or partial tearing, and rule out other causes of heel pain that may require different treatment approaches.
Integrative Treatment Protocols
Dr. Jimenez’s treatment philosophy emphasizes integrative, patient-centered care that combines the best of chiropractic medicine, functional medicine, and evidence-based rehabilitation. His protocols for Achilles tendon heel pain typically include chiropractic adjustments to the spine, pelvis, and lower extremity joints to restore proper biomechanics, extremity-specific adjustments targeting the foot and ankle, soft tissue therapies including myofascial release and instrument-assisted techniques, customized rehabilitation exercises with progressive loading, functional medicine interventions addressing nutrition, inflammation, and tissue healing, and patient education on activity modification and injury prevention.
Dr. Jimenez recognizes that successful outcomes require addressing not just the symptoms but the underlying causes of tendon pathology. His functional medicine training allows him to consider factors such as nutritional deficiencies affecting collagen synthesis, metabolic conditions influencing tissue healing, inflammatory status and oxidative stress, hormonal imbalances that may affect musculoskeletal health, and lifestyle factors contributing to injury risk.
Collaborative Care Model
When necessary, Dr. Jimenez collaborates with orthopedic surgeons, physical therapists, podiatrists, and other specialists to ensure patients receive comprehensive care. If he determines that a patient would benefit from interventions outside his scope of practice, such as advanced imaging procedures, specialized injections, or surgical consultation, he refers to the appropriate providers while continuing to support the patient’s overall recovery.
This collaborative approach ensures that patients receive the most appropriate care for their specific condition while benefiting from Dr. Jimenez’s unique ability to bridge conventional medical evaluation with chiropractic and functional medicine interventions.
Different Nonsurgical Treatments for Heel Pain in the Lower Extremities
Effective management of Achilles tendon heel pain typically requires a multimodal approach combining various evidence-based interventions.
Eccentric Exercise Programs
Eccentric exercise has the highest level of evidence supporting its ability to reduce Achilles tendinopathy pain (Grade A recommendation). The most well-known protocol is the Alfredson protocol, which consists of a 12-week program where patients perform eccentric heel-drop exercises—three sets of 15 repetitions, twice daily, seven days a week.
The exercises are performed in two variations: with the knee straight (emphasizing the gastrocnemius muscle) and with the knee bent (emphasizing the soleus muscle). Patients start in a raised heel position, slowly lower the heel below the level of the step over three seconds (eccentric phase), then use the opposite leg to return to the starting position.
For insertional Achilles tendinopathy, the protocol is modified to reduce ankle dorsiflexion range of motion, avoiding compression of soft tissues at the tendon insertion. This modification has been shown to decrease pain from baseline to follow-up, with 67% of patients able to resume pre-injury activity levels.
Acupuncture for Achilles Tendinopathy
Acupuncture offers a holistic approach to treating Achilles tendinopathy by addressing both pain and underlying inflammation. A 2013 randomized controlled trial found that acupuncture intervention significantly improved pain and activity in patients with chronic Achilles tendinopathy compared to eccentric exercises alone.
In this study, the mean VISA-A score improved to 67.1 points in the acupuncture group versus 48.5 points in the control group after eight weeks—an 18.6-point advantage for acupuncture. Pain scores diminished by 3.7 cm after activity and 3.2 cm at rest in the acupuncture group, significantly more than the control group.
Mechanisms of Acupuncture for Tendinopathy:
Stimulates the body’s natural anti-inflammatory response, reducing pain and swelling
Enhances blood circulation to the Achilles tendon, promoting faster healing and recovery
Releases endorphins and neurochemicals that provide pain relief
Deactivates myofascial trigger points in the calf muscles contributing to tendon stress
Addresses underlying energy imbalances according to traditional Chinese medicine principles
Electroacupuncture, which adds electrical stimulation to traditional needle placement, has shown particular promise. A case series reported successful treatment using direct tendon needle insertion with electrostimulation at specific acupuncture points, resulting in symptomatic reduction and functional improvement.
Rest, Ice, Compression, and Elevation (RICE)
The RICE protocol remains a foundational component of acute Achilles tendon injury management. Rest or immobilization allows the tendon time to heal without continued mechanical stress. Doctors may recommend walking boots to keep the foot immobile for two to three weeks after an Achilles tendinitis diagnosis.
Ice application 2-3 times daily for 5-10 minutes helps alleviate pain and swelling. Compression with flexible bandaging during the first few days after injury reduces swelling. Elevation of the foot three times daily for 15 minutes also helps manage inflammation.
Extracorporeal Shock Wave Therapy (ESWT)
When exercise programs are unsuccessful, extracorporeal shock wave therapy appears to be the next best non-operative treatment option to reduce Achilles tendinopathy pain (Grade B recommendation). ESWT uses acoustic waves to stimulate healing processes in tendon tissue.
A randomized controlled trial by Rompe and colleagues found that ESWT was more effective at reducing pain than full-range eccentric exercise in patients who had not responded to other conservative treatments. The ESWT group experienced pain reduction from 7.0 to 3.0, while the eccentric exercise group improved from 6.8 to 5.0. Multiple clinical trials have demonstrated 2-point or greater decreases in pain with ESWT.
Physical Therapy and Manual Therapy
Physical therapy combines therapeutic exercise, manual techniques, and modalities to address Achilles tendinopathy comprehensively. Manual therapy techniques include joint mobilization to improve ankle and foot mobility, soft tissue mobilization targeting the calf muscles and surrounding tissues, trigger point release for myofascial dysfunction, nerve mobilization when neural tension is present, and massage therapy to improve circulation and reduce muscle tension.
Research demonstrates that adding manual therapy to eccentric exercise protocols can enhance rehabilitation outcomes, particularly in the first four weeks of treatment when manual therapy accelerates recovery compared to exercise alone.
Orthotic Interventions
Custom foot orthoses help correct biomechanical abnormalities contributing to Achilles stress. These devices support proper arch height, correct pronation or supination issues, balance leg length discrepancies, redistribute pressure across the foot, and improve overall foot alignment.
Heel lifts can temporarily reduce strain on the Achilles tendon by decreasing ankle dorsiflexion during walking and standing. While heel lifts do not address underlying pathology, they can provide symptomatic relief during the healing phase.
Nutritional Interventions
Emerging research supports nutritional supplementation to enhance tendon healing. Vitamin C plays a crucial role in collagen synthesis, and supplementation (particularly when combined with gelatin or hydrolysed collagen) may accelerate tendon recovery.
Studies suggest that 15 grams of gelatin containing 225mg of vitamin C taken one hour before resistance training increases collagen synthesis twofold. Vitamin C supplementation aids tendon healing through antioxidant activity, promotion of type I collagen fiber production, and reduction of oxidative stress parameters.
Various Stretches and Exercises to Stretch and Strengthen the Achilles Tendon
A comprehensive exercise program for Achilles tendinopathy should include eccentric strengthening, progressive loading, flexibility work, and neuromuscular training.
The Alfredson Eccentric Protocol
Exercise 1: Straight-Knee Heel Drops
Stand on the edge of a step on the affected leg, with the heel hanging over the edge. Rise up on the toes using both legs for assistance. Slowly lower the affected heel below the level of the step over 3 seconds (eccentric phase only). Use the unaffected leg to return to the starting position. Perform 3 sets of 15 repetitions, twice daily.
Exercise 2: Bent-Knee Heel Drops
Perform the same movement as above, but with the knee slightly bent (approximately 15-20 degrees). This variation emphasizes the soleus muscle. Slowly lower the heel below step level over 3 seconds. Return to starting position using the opposite leg. Perform 3 sets of 15 repetitions, twice daily.
Progression: As pain decreases and strength improves, add weight using a backpack or weighted vest to increase the load on the tendon. The exercises should be performed “into pain”—meaning some discomfort is acceptable and even desirable, as it indicates appropriate tendon loading.
Calf Stretching Exercises
Gastrocnemius Stretch: Stand facing a wall with the affected leg straight behind you and the unaffected leg bent in front. Keep the heel of the back leg on the ground and lean forward until a stretch is felt in the upper calf. Hold for 20-30 seconds, repeat 3 times, perform 3 times daily.
Soleus Stretch: Similar to the gastrocnemius stretch, but bend the knee of the back leg while keeping the heel on the ground. This targets the deeper soleus muscle. Hold for 20-30 seconds, repeat 3 times, perform 3 times daily.
Plantar Fascia Stretch: Sit with the affected leg crossed over the opposite knee. Pull the toes back toward the shin until a stretch is felt along the bottom of the foot and heel. Hold for 20-30 seconds, repeat 3 times, perform 3 times daily.
Progressive Strengthening Exercises
Double-Leg Heel Raises: Stand on a flat surface with feet hip-width apart. Rise up on both toes as high as possible. Lower back down with control. Perform 3 sets of 15-20 repetitions once daily.
Single-Leg Heel Raises (on flat surface): Progress to performing heel raises on the affected leg only when double-leg raises can be performed pain-free. Rise up on one toe as high as possible. Lower with control. Perform 3 sets of 10-15 repetitions once daily.
Calf Raises with Weight: Add progressive resistance using a backpack, weighted vest, or holding dumbbells to increase load through the Achilles tendon. Perform 3 sets of 8-12 repetitions 2-3 times per week.
Balance and Proprioception Training
Single-Leg Balance: Stand on the affected leg with eyes open for 30-60 seconds. Progress to eyes closed when able. Perform 3 sets once daily.
Wobble Board Training: Stand on an unstable surface (wobble board or balance pad) on the affected leg. Maintain balance for 30-60 seconds. Perform 3 sets once daily.
Return-to-Activity Progressions
Gradual return to running and jumping activities should follow a structured progression based on symptom response and functional testing:
Phase 1: Walking program—begin with 20 minutes daily, gradually increasing duration and pace.
Phase 3: Continuous jogging—transition to sustained jogging at comfortable pace.
Phase 4: Running with progressive intensity increases—gradually increase speed and distance.
Phase 5: Sport-specific training—incorporate movements specific to the athlete’s sport.
Throughout all phases, monitoring pain response is critical. The pain-monitoring model suggests that some discomfort during activity (rated 3-5 out of 10) is acceptable if pain returns to baseline within 24 hours and does not progressively worsen session to session.
Conclusion and Important Disclaimer
Achilles tendon heel pain represents a complex condition influenced by anatomical vulnerability, biomechanical dysfunction, training errors, and systemic factors. Understanding the intricate anatomy and biomechanics of this remarkable tendon helps us appreciate why comprehensive, whole-body approaches like chiropractic care can be so effective in promoting healing and preventing recurrence.
Chiropractic care addresses Achilles tendinopathy through multiple mechanisms: restoring proper alignment throughout the kinetic chain, improving joint mobility in the foot and ankle complex, enhancing blood flow to the relatively hypovascular tendon, reducing compensatory muscle tension and imbalances, and modulating pain through neurophysiological effects. When combined with evidence-based interventions such as eccentric exercise programs, acupuncture, appropriate rest and activity modification, progressive strengthening and stretching, nutritional support for tissue healing, and patient education, chiropractic care offers a comprehensive, non-invasive pathway to recovery.
The clinical insights from practitioners like Dr. Alexander Jimenez, DC, APRN, FNP-BC, CFMP, IFMCP, demonstrate the value of integrating advanced diagnostics with chiropractic and functional medicine approaches. His dual-scope practice allows for comprehensive evaluation of patient injuries, correlation with advanced imaging findings, and development of individualized treatment protocols that address both local tissue pathology and systemic contributing factors.
Serious Note and Medical Disclaimer
IMPORTANT: This article is intended for informational and educational purposes only and should be taken seriously as part of your health education. The information provided is not a substitute for professional medical advice, diagnosis, or treatment. You should NEVER disregard professional medical advice or delay seeking medical care because of information you have read in this article. Always consult with a qualified healthcare provider, such as a physician, chiropractor, or physical therapist, before beginning any new treatment program, exercise regimen, or making changes to your existing healthcare routine. If you are experiencing severe or worsening heel pain, sudden inability to bear weight, signs of tendon rupture (sudden “pop” with immediate severe pain and weakness), or symptoms that have not improved with conservative care, seek immediate medical evaluation. The exercises and treatments discussed in this article should only be performed under the guidance of a qualified healthcare professional who can assess your individual condition and provide personalized recommendations. Improper performance of exercises or inappropriate treatment can potentially worsen your condition or cause new injuries. Individual results may vary significantly based on the specific nature and severity of your condition, your overall health status, adherence to treatment recommendations, and other factors. No guarantees of specific outcomes can be made. The references to Dr. Alexander Jimenez and his clinical approach are provided for informational purposes to illustrate integrative treatment philosophies. They do not constitute an endorsement or recommendation of any specific provider. You should make your own informed healthcare decisions in consultation with providers you have selected. Please take this disclaimer seriously and prioritize your health by working with qualified healthcare professionals for the diagnosis and treatment of any musculoskeletal condition.
References
American Academy of Family Physicians. (2018). Heel pain: Diagnosis and management. American Family Physician, 97(2), 86-93. https://pubmed.ncbi.nlm.nih.gov/29365222/
Chimenti, R. L., & Dilger, C. P. (2019). Nonsurgical treatment options for insertional Achilles tendinopathy. Foot and Ankle Clinics, 24(3), 505-513. https://pmc.ncbi.nlm.nih.gov/articles/PMC7216975/
Dilger, C. P., & Chimenti, R. L. (2022). Successful treatment of Achilles tendinopathy with electroacupuncture: Two cases. Medical Acupuncture, 29(3). https://pmc.ncbi.nlm.nih.gov/articles/PMC5512315/
Dimou, E. S., Brantingham, J. W., & Wood, T. (2004). Conservative therapy for plantar fasciitis: A narrative review of randomized controlled trials. Journal of Canadian Chiropractic Association, 49(4). https://pmc.ncbi.nlm.nih.gov/articles/PMC1839987/
Doral, M. N., et al. (2010). Functional anatomy of the Achilles tendon. Knee Surgery, Sports Traumatology, Arthroscopy, 18(5), 638-643. https://pubmed.ncbi.nlm.nih.gov/20182867/
Jimenez, A. (2024). El Paso, TX, doctor of chiropractic. Injury Medical & Chiropractic Clinic. https://dralexjimenez.com
Martin, R. L., et al. (2021). Management of plantar heel pain: A best practice guide. British Journal of Sports Medicine, 55(19), 1106-1118. https://pubmed.ncbi.nlm.nih.gov/33785535/
Pearson, S. J., et al. (2013). Acupuncture for chronic Achilles tendinopathy: A randomized controlled study. Acupuncture in Medicine, 31(1), 142-146. https://pubmed.ncbi.nlm.nih.gov/23263998/
Reinking, M. F., et al. (2015). A Delphi study of risk factors for Achilles tendinopathy. International Journal of Sports Physical Therapy, 10(6). https://pmc.ncbi.nlm.nih.gov/articles/PMC5046962/
Silbernagel, K. G., et al. (2015). A proposed return-to-sport program for patients with midportion Achilles tendinopathy. Journal of Orthopaedic & Sports Physical Therapy, 45(11). https://www.jospt.org/doi/10.2519/jospt.2015.5885
Understanding Core Overtraining Injuries: Wellness Strategies and Chiropractic Solutions at El Paso Back Clinic
A man is training in a gym to build strong and healthy muscles.
Pushing your core muscles too far without proper rest can create big issues for your overall health, especially your back. At El Paso Back Clinic® in El Paso, TX, we specialize in wellness chiropractic care that helps people recover from these problems and stay strong. Core overtraining affects the muscles around your midsection, which support your spine and daily movements. This article breaks down the injuries that can happen, why they occur, ways to stop them, and how our chiropractic methods provide relief. We focus on natural wellness to keep your back and body in balance.
The Role of Core Muscles in Back Health and Overtraining Basics
Your core is like the foundation of a house—it holds everything together. It includes muscles in your stomach, sides, lower back, and hips. These help with bending, twisting, and standing straight. When you overtrain, you repeat exercises like sit-ups or lifts too much, without breaks. This wears down tissues faster than they can heal. Wellness experts note that this leads to lasting soreness, reduced energy, and risks to your spine.
At our clinic, we treat many cases where core issues cause back pain. Overtraining disrupts the natural alignment, pulling on the back. Science shows repetitive stress changes how muscles and bones work together, leading to problems.
Everyday Muscle Strains from Pushing the Core Too Hard
Strains are pulls or small tears in muscles. They are common when the core gets overworked and can’t support the body well.
Strains Around the Groin
These happen in the inner thigh muscles tied to the core. Quick stops and starts in activities like hiking or playing kickball can trigger them. If the core is weak from too much training, it adds extra pull. You feel a sudden sharp pain, maybe see bruising, and have trouble moving your legs inward. In the back, this strain can tug on the lower spine, causing aches there too.
Strains in the Stomach Area
Abdominal strains come from forceful turns, like swinging a racket or carrying heavy bags. Overdoing core workouts builds up damage over time. Pain hits when you tense up or laugh, and the area feels sore to the touch. This connects to back health because weak abs force the back muscles to overcompensate, leading to stiffness.
Problems with Hip Flexors
These muscles help raise your legs and link directly to the core. Running uphill or doing too many leg raises without rest inflames them. Symptoms include a tight feeling in the front of the hip and pain when stepping up. Poor core balance makes the back arch unnatural, adding pressure.
Our wellness approach at El Paso Back Clinic uses gentle checks to find these strains early and guide healing without harsh methods.
Deeper Issues: Fractures and Bone Stress from Core Overuse
When overtraining goes on, it can harm bones, which support the core and back.
Fractures in the Ribs
Rib stress fractures are tiny breaks from constant tugging by core muscles. This shows up in paddling sports or even heavy coughing fits from overuse. The muscles contract hard, stressing the bone until it cracks. Pain sharpens with deep breaths or twists, and it can feel tender. Since ribs protect the upper back area, this injury often leads to posture problems and back discomfort.
Other Stress Fractures
These small cracks appear in weight-bearing bones like the pelvis or lower spine from ongoing impact. Walkers or dancers who ignore rest will experience issues when bone repair lags behind damage. Early signs are dull aches that worsen with activity. In young active people, it might involve cartilage issues, too. Back clinic patients often report these symptoms linked to core weakness, causing spinal instability.
Healing takes rest, but our chiropractic wellness plans speed it up safely.
Extra Effects Like Ongoing Pain, Loss of Power, and Stiffness
Overtraining doesn’t stop at big injuries—it brings smaller but nagging problems.
Lasting Pain and Rigid Muscles
You might wake up stiff or feel constant soreness in the core. This spreads to the back, making sitting or standing tough. It’s a sign the body is inflamed and needs recovery time.
Weaker Muscles Overall
Tired core muscles can’t hold strong, leading to drops in power. One side might become too tight while the other weakens, throwing off balance. This imbalance pulls on the back, increasing the risk of slips or strains during daily tasks.
Tight Spots in the Legs and Sides
Muscles like the back of the thighs (hamstrings) or the outer thigh band (IT band) tighten to make up for a worn-out core. This causes knee or hip issues that refer pain to the lower back. Wellness care addresses these chains of problems.
Signs also include getting sick more or feeling down, as the body fights overload.
How These Injuries Develop and What Increases the Risk
Injuries build from too much activity without balance. Body mechanics play a part—bad posture during exercises adds uneven stress. Muscles need time to fix small wear, but skipping rest lets damage grow.
In jobs with lifting or sports with jumps, core pulls transfer to bones. Poor shoes or low nutrients weaken things further. At our back clinic, we look at the whole picture, including how back alignment affects core strain.
Smart Ways to Avoid Core Overtraining Problems
Wellness starts with prevention. Ramp up workouts slowly, adding just a bit more each week. Switch activities to give muscles variety. Take full rest days and stretch gently.
Eat foods rich in vitamins for strong bones, and use supportive gear. Pay attention to body signals like unusual tiredness. Our clinic offers wellness checks to catch risks early.
Chiropractic Wellness Care for Healing Core Injuries
At El Paso Back Clinic, we use integrated chiropractic to resolve core issues and boost back health.
Adjustments to the Spine
These hands-on moves realign the back, easing nerve pressure and helping muscles relax. It improves how the core and back communicate, reducing pain fast.
Therapies for Soft Tissues
Massage-like techniques release tight spots, increase blood flow, and calm inflammation. This works well for strains and stiffness.
Our methods treat current pain while building wellness to avoid repeats. They enhance flexibility, strength, and nerve health for long-term back care.
Expertise from Dr. Alexander Jimenez at El Paso Back Clinic
Dr. Alexander Jimenez, DC, APRN, FNP-BC, leads our wellness efforts with deep knowledge in chiropractic science.
Linking Injuries to Patient Histories
He connects core overtraining to back pain through detailed stories, exams, and imaging. For instance, work lifts or sports twists can lead to patterns in muscle and nerve issues.
Diagnosis with Dual Expertise
Using his skills as a nurse practitioner and chiropractor, he does thorough assessments. Advanced scans reveal hidden bone or tissue problems in core areas.
Step-by-Step Treatments
Procedures include spine adjustments, tissue work, and guided exercises. For sports or personal injuries, he adds strength training. In car accidents, focus is on impact-related core and back strains.
Care for Medical and Legal Needs
The clinic manages full treatment plans, including reports for insurance or court in injury cases. This covers work, auto, or everyday accidents with clear documentation.
Dr. Jimenez promotes education on wellness to empower patients.
Bringing It All Together for Better Health
Core overtraining brings strains, fractures, pain, and imbalances that hit the back hard. Prevention through smart habits and chiropractic care keeps you moving well. At El Paso Back Clinic®, our wellness focus helps restore balance naturally.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine