Integrated: Brian Filidor is an aspiring wrestler who’s had a life-changing experience through chiropractic and agility training with Dr. Alex Jimenez. Over a variety of lifestyle modifications, Brian Filidor has achieved a higher conditioning, including improved performance in his strength, reaction time and overall health. Brian Filidor appreciates the help of all the trainers towards helping him become a better athlete.
Integrated Chiro & Rehab
Physical fitness is a state of health and well-being and, more specifically, the capacity to perform aspects of sports, jobs and daily activities. Physical fitness is usually accomplished through proper nourishment, moderate-vigorous physical exercise, and adequate rest. Fitness is defined as the quality or state of being healthy.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
Low back pain occurs due to a variety of causes, which is why it is often poorly diagnosed and treated. As there are many mechanisms by which lower back pain happens, such as trauma, overuse from weight lifting for example, and repetitive motion, it’s important to mention that this article will only focus on sciatic nerve pain, or sciatica.
Sciatica refers to pain and other symptoms which radiate or travel down the leg, associated with numbness, tingling or burning sensations, and weakness in one or both lower extremities. Many patients complain of sharp, intense pain and discomfort when sitting and driving, affecting their capacity to bear weight properly when one has to walk or move. Their pain can shoot down the length of the sciatic nerve, into the buttocks, down the back of the leg, into the calf, and lastly, into the ankle and foot. The sciatic nerve, which is the longest nerve in the body, can become compressed or entrapped by certain muscles leading to sciatica.
Based on the location of this impingement, the individual will present with a variety of symptoms. If the health issue is diagnosed to originate in the low back, then the problem normally occurs around the hole in which the nerve exits the spine, resulting in symptoms surrounding the entire lower extremity. If the health issue is correctly diagnosed to originate from the buttocks, it most often includes the piriformis muscle because the sciatic nerve travels beneath it as it makes its way down the length of the leg. The source of this type of sciatica may involve different muscles just below the piriformis, otherwise known as a group of muscles called the hip rotators.
If the health issue is not in the lower back, or buttocks, then the problem is very likely to have occurred in the hamstrings, primarily at one of the muscles where the plantar nerve divides the hamstrings at the back of the thigh. The sciatic nerve may also manifest symptoms when compressed in the calf, however, these symptoms will often only be reported below the knee.
ART and PNF Treatment for Sciatic Nerve Pain
In regards to treatment, sciatica can be worked out by performing active release techniques, or ART, through the release of the entire nerve where it is being compressed. The objective when using ART for sciatic nerve pain would be to maneuver the nerve while trapping the muscle(s) in their own position. The nerve is then pulled from beneath the muscle. Also, using rehabilitation exercises through specific stretches and strengthening exercises of the muscle groups involved may allow for faster healing alongside chiropractic care to boost the communication between the spine and the positioning of the nerve entrapment/compression.
One of the most common stretching methods for sciatica is PNF or proprioceptive neuromuscular facilitation. PNF is a sort of stretch that produces a rebound relaxation of the muscle. PNF is a more advanced kind of flexibility training that involves both the contraction and stretching of the muscle group being targeted. PNF is a stretching technique utilized to increase range of motion and flexibility. PNF increases range of motion by increasing the length of the muscle and increasing neuromuscular efficiency. PNF stretching has been found to increase ROM in trained, as well as untrained, individuals. Effects can last 90 minutes or more after the stretching has been completed. PNF stretching was initially created as a form of rehabilitation, and to that effect, it is very effective. It’s also excellent for targeting specific muscle groups as well as increasing flexibility and enhancing muscle power and strength.
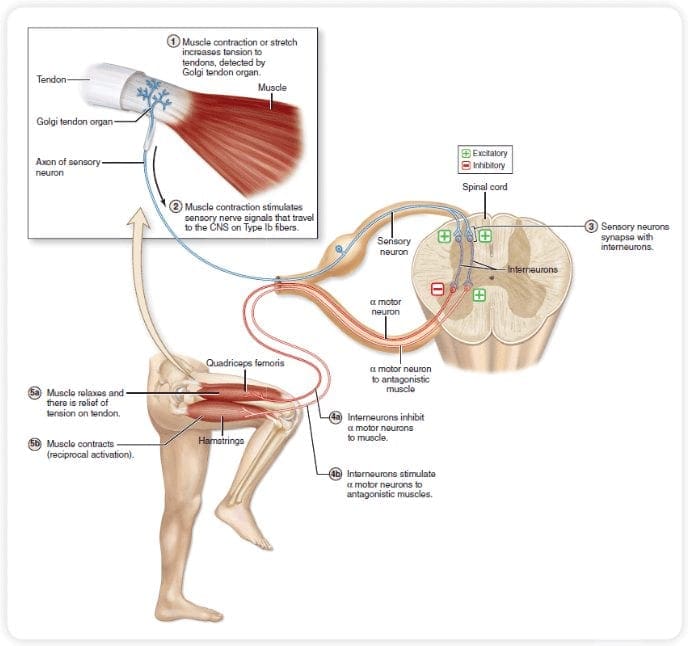
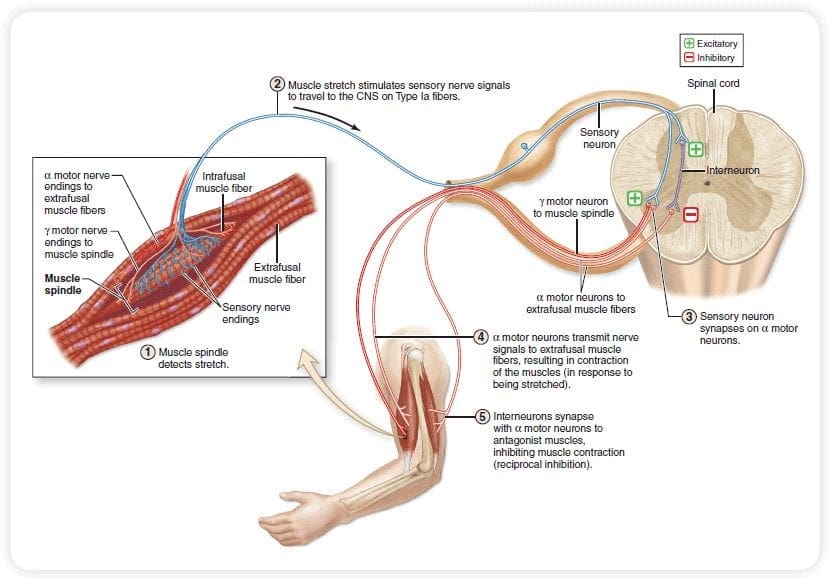
Four theoretical physiological mechanisms for increasing range of motion were identified using PNF stretching: autogenic inhibition, reciprocal inhibition, stress relaxation, and the gate control theory.�Autogenic Inhibition is what occurs in a contracted or stretched muscle in the form of a decrease in the excitability because of inhibitory signals sent from the same muscle.�Reciprocal inhibition is what occurs in the TM when the opposing muscle is contracted voluntarily in the form of decreased neural activity. It occurs when an opposing muscle is contracted in order to maximize its contraction force, and it relaxes.�Stress relaxation is what occurs when the musculotendinous unit (MTU), which involves the muscles and the connected tendons, is under a constant stress.�The gate control theory is what occurs when two kinds of stimuli, such as pain and pressure, activate their respective receptors at the same time.
How to Perform a PNF Stretch
The practice of doing a PNF stretch involves the next steps. The muscle group to be stretched is first placed so that the muscles are stretched and under pressure. The individual then contracts the muscle, using a band for 5 to 6 seconds while a partner, or immovable object, applies sufficient resistance to inhibit motion. Please be aware, the effort of contraction ought to be relevant to the individual’s amount of conditioning. The contracted muscle group is then relaxed and a controlled stretch is used for approximately 20 to 30 seconds. The muscle band is then allowed 30 seconds to recover and the process is repeated 2 to 4 more times.
Information differs marginally regarding time recommendations for PNF stretching, determined by which healthcare professional you’re speaking to. Although there are conflicting responses to the question of how long should a patient contract the specific muscle group for and how long should they rest for between each stretch, it’s been found through a study of research and patient experience, that the above timing recommendations offer the most advantages from proprioceptive neuromuscular facilitation stretching.
Furthermore, certain precautions will need to be taken when performing PNF stretches because they may put additional stress on the targeted muscle group, which can boost the possibility of soft tissue injury. To reduce this risk, it’s essential for the patient to include a conditioning phase before a maximum, or intense effort is utilized.
About the Active Release Technique or ART
The active release technique, or ART, is among the newest treatments in the world of chiropractic. ART is used to target muscle, nerve, and tendon problems. It is also used to treat blood vessel problems. Quite a few studies have been conducted and these have generated positive results which reveal that ART is really an effective treatment method. A lot of individuals nowadays try ART since so many are experiencing muscle problems.
Oftentimes, individuals, particularly the older ones, wake up and they feel that their body is quite hard to move. There are also those who start to feel their range of motion getting more and more limited with time. A number of the most common body parts that suffer from limited selection of motion include the neck, the arms, and the back. For many individuals, there is also restricted range of motion. There are numerous factors that cause restricted range of movement. The active release technique can be used to improve limited mobility as well as improve sciatica symptoms associated with a variety of health issues.
How ART Affects Limited Range of Motion
ART therapists initial assess the muscles that they are supposed to take care of. They check the texture, the stiffness, and needless to say, their freedom. Since the groundwork is conducted, the therapists would then attempt to elongate the muscles so as to break the adhesions. The stretching is usually conducted with the management of vein in consideration. Also, the practitioner would need to ask the patient to move the affected body parts in ways prescribed by the practitioner. So essentially, ART is a joint-venture. Practitioner and patients work together in order to generate great medical outcomes.
Dr. Alex Jimenez’s Insight
The active release techniques, or ART, and the proprioceptive neuromuscular facilitator, or PNF, stretches are therapeutic procedures commonly utilized for the common practice of releasing tension in the soft tissues as well as increasing the range of motion of the human body. Although a variety of treatment options are available to help treat sciatica, ART and PNF can be used by qualified and experienced healthcare professionals to safely and effectively improve and manage sciatic nerve pain. Moreover, alternative treatment options, such as chiropractic care, and strengthening exercises can also be used in combination with these therapeutic methods to help speed up the recovery process.
The Future of ART and PNF
It’s important to remember that both ART and PNF should only be run by accredited practitioners. Healthcare professionals are not just expected to find basic instruction and permit but they are also expected to have attended numerous workshops and seminars about the subject. In some countries, credential tests even must be passed. In addition, it ought to be noted that ART and PNF must be conducted on muscle stiffness not due to blunt trauma. The condition should also not involve inflammation.
There are many healthcare professionals who focus on ART and PNF. A few of these include chiropractors, physical therapists, massage therapists, medical physicians, and even athlete trainers. The active release technique and the proprioceptive neuromuscular facilitation stretches helps people do things that they used to do. It helps them become more efficient at work as well as be practical in their daily lives. Due to the health benefits of ART and PNF, more and more people from the medical and therapeutic world are learning how to concentrate on it. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is medically referred to as a collection of symptoms, rather than a single injury and/or condition. Symptoms of sciatic nerve pain, or sciatica, can vary in frequency and intensity, however, it is most commonly described as a sudden, sharp (knife-like) or electrical pain that radiates from the low back down the buttocks, hips, thighs and legs into the foot. Other symptoms of sciatica may include, tingling or burning sensations, numbness and weakness along the length of the sciatic nerve. Sciatica most frequently affects individuals between the ages of 30 and 50 years. It may often develop as a result of the degeneration of the spine due to age, however, the compression and irritation of the sciatic nerve caused by a bulging or herniated disc, among other spinal health issues, may also cause sciatic nerve pain.
Active release therapy, more specifically referred to as the active release technique, is a patented system designed by Dr. P. Michael Leahy which focuses on the treatment of developed scar tissue in damaged muscles all across the human body. When Dr. Leahy first developed the technique about two decades ago, he realized that the damage in the complex soft tissues of the muscles might perhaps be able to be sensed as well as addressed directly through movement in the form of specialized techniques. With its proven ability to cure pain, its own acronym, ART, provides the active release therapy with some ironical link to being a true art form in chiropractic care.
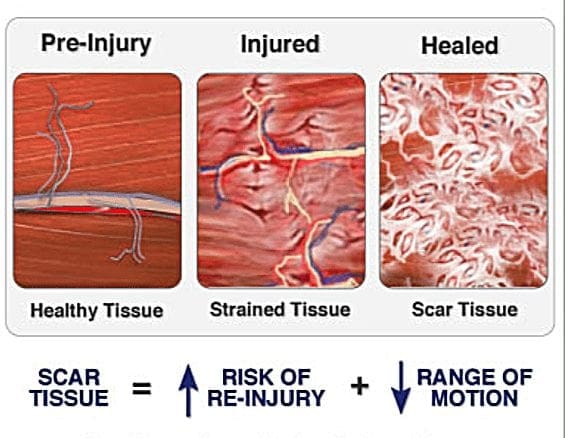
When athletes overwork their muscles from playing sports or even through just everyday activities, many individuals don’t understand how scar tissue can develop on our muscles in the first place. The scar issue forms in order to help heal damaged muscles, however, it can ultimately create painful symptoms which may last long after these have healed. Scar tissue most commonly develops as a result of pulled muscles or muscle tears, or even from a lack of oxygen, called hypoxia.
As the scar tissue builds in the damaged or injured muscles, if the individual does not maintain a proper level of mobility in the affected area, it can progressively cause muscles to become stiff or tight and weak, eventually leading to health issues such as tendonitis or nerve problems. This explains why some people with pain or limited range of motion, often will need to visit a healthcare professional immediately. Fortunately, many doctors are certified to treat these type of problems using active release therapy.
Using the Active Release Technique to Relieve Pain
Together with providing tension to the targeted sore muscle and utilizing specific body motions, the painful symptoms associated with scar tissue improves through active release therapy. As of now, there are approximately 500 different active release techniques designed to alleviate the tightness or stiffness and weakness in all of the body’s soft tissues, from the muscles to the nerves. Many of these movements are particularly chosen for each individual based on the specific muscle issue and location.
Active release techniques can also be helpful for small traumatic injuries caused by accumulative trauma or repetitive strain. More specifically, ART functions to break up fibrous tissues called adhesions. These adhesions result from a tear onto a tendon, ligament or muscle. Adhesions commonly develop in different ways, including from trauma as a result of acute injury or from repetitive motion injury caused by overuse, most commonly from sports injuries. It may also be a result of poor posture which has been aggravated by continuous pressure in addition to tension produced in the soft tissues for extended amounts of time.
Such adhesions, when left untreated, can also limit blood flow as well as shorten muscles, causing the well-known symptoms. Worsened symptoms can also result in pain, discomfort or weakness and at times numbness, most notably when scar tissue applies pressure on the nerves. When adhesions occur, the patient will surely complain of distress much more due to the simple fact that they will not be able to engage in the physical activities they were used to performing in before.
The active release technique, or ART,� works by implementing a couple of movements and motions on the affected muscle, tendon or fascia. In comparison to other soft tissue therapies, it’s said to achieve better end results. Primarily, ART aims to help improve the symptoms of the damaged or injured area by applying pressure and force on it. From there, the individual will be tasked to perform a technique which will help release the tension from the treatment. This can essentially improve motion for the treated region.
The combination of this tension out of the active release technique and that of the movement of muscles and its soft tissues will loosen and break up the adhesions. Because of this, there’ll be lesser pain felt on the injured region. This technique works well with active strengthening in addition to biomechanics training. The combination of these therapies will make patients feel improved body awareness, strength, flexibility and mobility even after a few ART sessions.
How Different is ART from Traditional Soft Tissue Treatments?
When compared with traditional manners of soft tissue therapy, ART boasts of a very comprehensive strategy. The active release technique is performed by certified healthcare practitioners who’ve underwent a very rigorous training procedure. Healthcare professionals must participate in sit-in classes and they must also have hands-on testing. Their certificate doesn’t stop after they pass the 90 percent mark on the hands on test though. They’ll also have to maintain their ART certification by getting annual recertification. This may work by honing the healthcare professional’s abilities and at the exact time, this will boil to the benefit of patients undergoing the therapy.
How Successful is ART as a Treatment?
Current research has demonstrated how effective the procedure is when it comes to treating hamstring pain and dysfunction in addition to hip pain, turf toe and lymph nodes. While the efficacy of ART has been demonstrated along these areas, several studies are still being made to check into its potential for treating disorders for other body components.
Using the Active Release Technique for Sciatica
Sciatica is an issue which affects a large number of people. It is essentially a pain syndrome, characterized by a collection of common symptoms which are caused when the sciatic nerve, the largest and most important nerve supplying the lower spine and the lower extremities, is compressed by the small muscles in the pelvis. The piriformis muscle is the one most implicated in the compression of the sciatic nerve, particularly because it moves through this muscle when emerging from the pelvis and entering the lower limbs. The active release technique, or ART, may be used in the treatment of sciatica brought on by piriformis syndrome.
Pathophysiology of Sciatica
When sciatica is caused by the compression of the sciatic nerve by the piriformis muscle, the latter generally goes into a spasm for an extended period of time, leading to the compression of this fundamental nerve. The spasm may result in a compromise in the blood supply to the muscle itself as well as the nerve, which will further complicate the issue. Nerve communications are important in order for the human body to maintain its outmost efficiency. Sciatica often can also be caused by disc injuries and herniations, as generally is a differential diagnosis to piriformis syndrome. Specific orthopedic tests can help, doctors of chiropractic, or chiropractors, evaluate the source of the patient’s sciatica prior to commencing any type treatment.
Consequences of Sciatic Nerve Pain
There are a number of effects that could arise as a result of sciatica. Reduction in overall body ranges of movement can be anticipated, accompanied by searing or sharp pain that can be excruciating. This can make it very difficult for an individual’s quality of life, especially when carrying out daily tasks like going to school and work, might become impossible due to the seriousness of the health issue. When the issue isn’t treated on time, it might cause permanent damage to the sciatic nerve.
Conventional Treatments for Sciatic Nerve Pain
There are a range of conventional treatments that may be utilized based on the intensity of the sciatic nerve pain, or sciatica. One of these is an injection of a drug/medication that can relax the muscle so that it stops compressing the nerve. Additionally, it has been proven that drugs and/or medications, such as steroids, may also have an impact on reducing the pain and impairment related to the symptoms. When the pharmacological methods don’t result in any progress, surgical ones can be attempted. The most usual of these is a surgery to release the nerve from the muscle by cutting away a portion of it. Although these have been listed as conventional treatments which may be used to treat sciatica, alternative treatment options and secondary opinions should be considered before considering surgical interventions. Only when no other treatment has demonstrated any improvements, should surgery be considered by a patient.
The Role of Active Release Techniques for Sciatica
The active release technique, or ART, is a form of therapy that focuses on the manipulation of soft tissues, including nerves, fascia and muscles, so as to achieve relief of painful symptoms, in this case for sciatica. For sciatic nerve pain, ART is utilized to reduce spasm and remove adhesions of the muscle that may be entrapping the sciatic nerve. Since the adhesions are removed through specific manual methods, the nerve can slide under the soft tissues, and sciatica symptoms can solve relatively quickly. There are a range of things that a patient can do in order to increase the efficacy of the active release technique. Early start to treatment assists in long-term resolution of sciatica symptoms.
Dr. Alex Jimenez’s Insight
The active release technique, also known as active release therapy or ART, is a soft tissue treatment based on a series of movement and motion techniques utilized to relieve pain and discomfort as well as promote the healing of muscles, joints and nerves, among other soft tissues. When performed by a certified healthcare professional, including a chiropractor, ART can help break down adhesions which may have developed following scar tissue formation after a damaged or injured muscle has healed. The active release technique has become one of the most common therapy for soft tissue treatment.
ART therapy is usually provided by skilled therapists like chiropractors, who have to keep their accreditation through continuing education on a yearly suface. This treatment is a specialized procedure that needs quite a bit of expertise and skill so as to work and supply rapid results. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is medically referred to as a collection of symptoms, rather than a single injury and/or condition. Symptoms of sciatic nerve pain, or sciatica, can vary in frequency and intensity, however, it is most commonly described as a sudden, sharp (knife-like) or electrical pain that radiates from the low back down the buttocks, hips, thighs and legs into the foot. Other symptoms of sciatica may include, tingling or burning sensations, numbness and weakness along the length of the sciatic nerve. Sciatica most frequently affects individuals between the ages of 30 and 50 years. It may often develop as a result of the degeneration of the spine due to age, however, the compression and irritation of the sciatic nerve caused by a bulging or herniated disc, among other spinal health issues, may also cause sciatic nerve pain.
The rule of 4 of the brainstem: a simplified method for understanding brainstem anatomy and brainstem vascular
syndromes for the non-neurologist.
The Rule Of 4 & The Brainstem
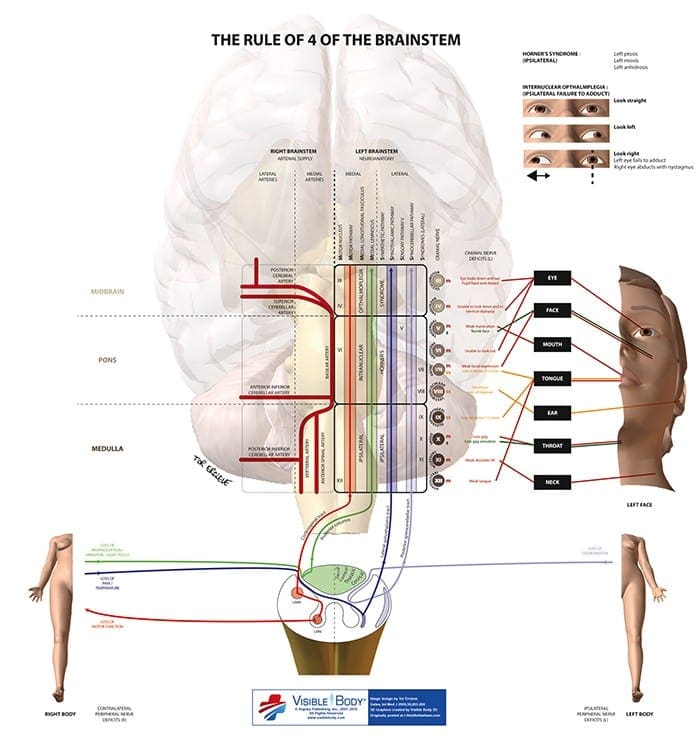
The rule of 4 is a simple method developed to help �students of neurology� to remember the anatomy of the brainstem and thus the features of the various brainstem vascular syndromes. As medical students, we are taught detailed anatomy of the brainstem containing a bewildering number of structures with curious names such as superior colliculi, inferior olives, various cranial nerve nuclei and the median longitudinal fasciculus. In reality when we do a neurological examination we test for only a few of these structures. The rule of 4 recognizes this and only describes the parts of the brainstem that we actually examine when doing a neurological examination. The blood supply of the brainstem is such that there are paramedian branches and long circumferential branches (the anterior inferior cerebellar artery (AICA), the posterior inferior cerebellar artery (PICA) and the superior cerebellar artery (SCA). Occlusion of the paramedian branches results in medial (or paramedian) brainstem syndromes and occlusion of the circumferential branches results in lateral brainstem syndromes. Occasionally lateral brainstem syndromes are seen in unilateral vertebral occlusion. This paper describes a simple technique to aid in the understanding of brainstem vascular syndromes.
Any attempt to over simplify things runs the risk of upsetting those who like detail and I apologize in advance to the anatomists among us, but for more than 15 years this simple concept has helped numerous students and residents understand, often for the first time, brainstem anatomy and the associated clinical syndromes that result.
In The Rule Of 4 There Are 4 Rules:
There are 4 structures in the �midline� beginning with M.
There are 4 structures to the side beginning with S.
There are 4 cranial nerves in the medulla, 4 in the pons and 4 above the pons (2 in the midbrain).
The 4 motor nuclei that are in the midline are those that divide equally into 12 except for 1 and 2, that is 3, 4, 6 and 12 (5, 7, 9 and 11 are in the lateral brainstem).
If you can remember these rules and know how to examine the nervous system, in particular the cranial nerves, then you will be able to diagnose brainstem vascular syndromes with ease.
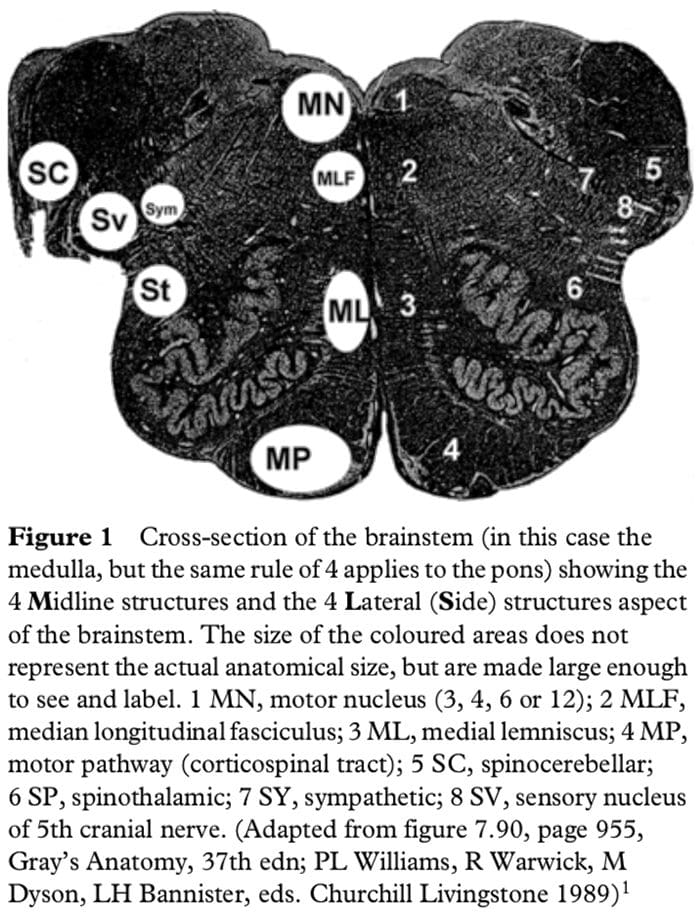
Figure 1 shows a cross-section of the brainstem, in this case at the level of the medulla, but the concept of 4 lateral and 4 medial structures also applies to the pons, only the 4 medial structures relate to midbrain vascular syndromes.
The 4 Medial Structures & The Associated Deficit Are:
The Motor pathway (or corticospinal tract): contra lateral weakness of the arm and leg.
The Medial Lemniscus: contra lateral loss of vibration and proprioception in the arm and leg.
The Medial longitudinal fasciculus: ipsilateral inter- nuclear ophthalmoplegia (failure of adduction of the ipsilateral eye towards the nose and nystagmus in the opposite eye as it looks laterally).
The Motor nucleus and nerve: ipsilateral loss of the cranial nerve that is affected (3, 4, 6 or 12).
The 4 Lateral Structures & The Associated Deficit Are:
The Spinocerebellar pathways: ipsilateral ataxia of the arm and leg.
The Spinothalamic pathway: contra lateral alteration of pain and temperature affecting the arm, leg and rarely the trunk.
The Sensory nucleus of the 5th: ipsilateral alteration of pain and temperature on the face in the distribution of the 5th cranial nerve (this nucleus is a long vertical structure that extends in the lateral aspect of the pons down into the medulla).
The Sympathetic pathway: ipsilateral Horner�s syndrome, that is partial ptosis and a small pupil (miosis)
These pathways pass through the entire length of the brainstem and can be likened to �meridians of longitude� whereas the various cranial nerves can be regarded as �parallels of latitude�. If you establish where the meridians of longitude and parallels of latitude intersect then you have established the site of the lesion.
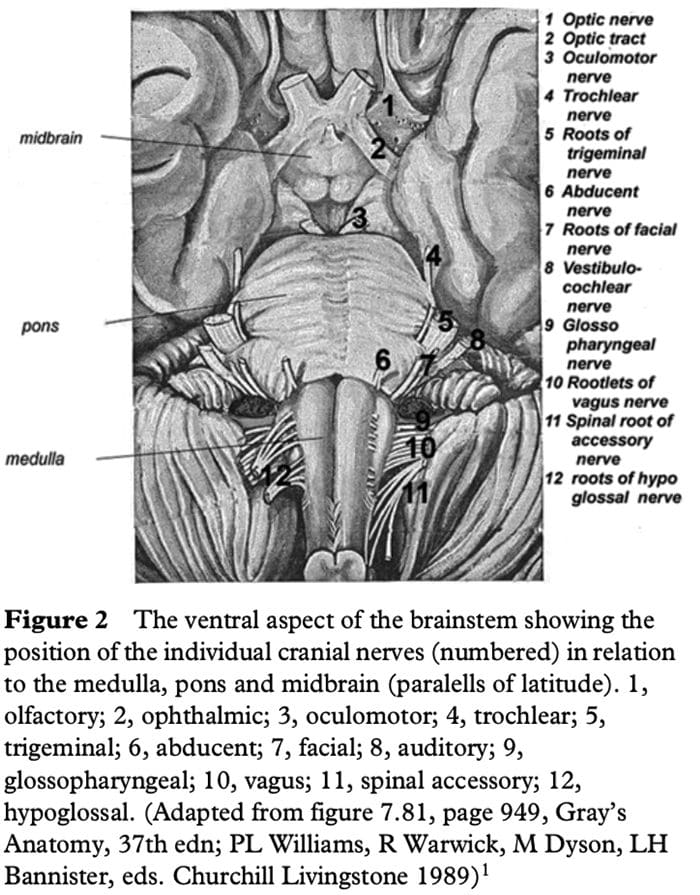
Figure 2 shows the ventral aspect of the brainstem.
The 4 Cranial Nerves In The Medulla Are:
9 Glossopharyngeal: ipsilateral loss of pharyngeal sensation. 10 Vagus: ipsilateral palatal weakness. 11 Spinal accessory: ipsilateral weakness of the trapezius and sternocleidomastoid muscles. 12 Hypoglossal: ipsilateral weakness of the tongue.
The 12th cranial nerve is the motor nerve in the midline of the medulla. Although the 9th, 10th and 11th cranial nerves have motor components, they do not divide evenly into 12 (using our rule) and are thus not the medial motor nerves.
The 4 Cranial Nerves In The Pons Are:
5 Trigeminal: ipsilateral alteration of pain, temperature and light touch on the face back as far as the anterior two-thirds of the scalp and sparing the angle of the jaw. 6 Abducent: ipsilateral weakness of abduction (lateral movement) of the eye. 7 Facial: ipsilateral facial weakness. 8 Auditory: ipsilateral deafness.
The 6th cranial nerve is the motor nerve in the pons.
The 7th is a motor nerve but it also carries pathways of taste, and using the rule of 4 it does not divide equally in to 12 and thus it is not a motor nerve that is in the midline. The vestibular portion of the 8th nerve is not included in order to keep the concept simple and to avoid confusion. Nausea and vomiting and vertigo are often more common with involvement of the vestibular connections in the lateral medulla.
The 4 Cranial Nerves Above The Pons Are:
4 Olfactory: not in midbrain. 5 Optic: not in midbrain. 6 Oculomotor: impaired adduction, supraduction and infraduction of the ipsilateral eye with or without a dilated pupil. The eye is turned out and slightly down. 7 Trochlear: eye unable to look down when the eye is looking in towards the nose.
The 3rd and 4th cranial nerves are the motor nerves in the midbrain.
Thus a medial brainstem syndrome will consist of the 4 M�s and the relevant motor cranial nerve, and a lateral brainstem syndrome will consist of the 4 S�sand either the 9�11th cranial nerve if in the medulla, or the 5th, 7th and 8th cranial nerve if in the pons.
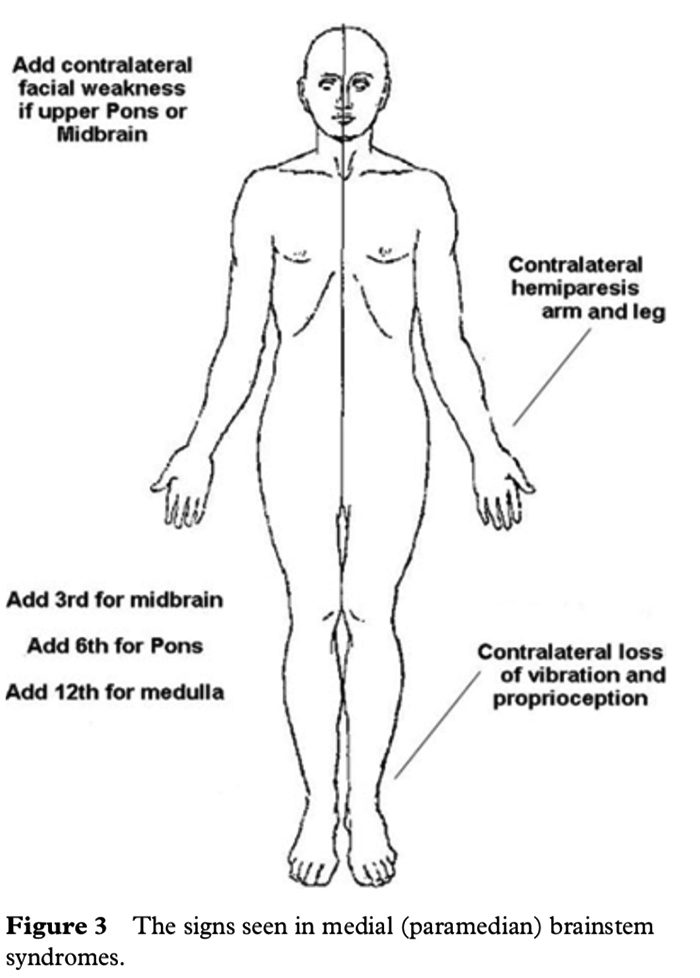
MEDIAL (PARAMEDIAN) BRAINSTEM SYNDROMES
Let us assume that the patient you are examining has a brainstem stroke. If you find upper motor neurone signs in the arm and the leg on one side then you know the patient has a medial brainstem syndrome because the motor pathways is paramedian and crosses at the level of the foramen magnum (decussation of the pyramids). The involvement of the motor pathway is the �meridian of longitude�. So far the lesion could be anywhere in the medial aspect of the brainstem, although if the face is also affected it has to be above the mid pons, the level where the 7th nerve nucleus is.
The motor cranial nerve �the parallels of latitude� indicates whether the lesion is in the medulla (12th), pons (6th) or midbrain (3rd). Remember the cranial nerve palsy will be ipsilateral to the side of the lesion and the hemiparesis will be contralateral. If the medial lemniscus is also affected then you will find a contra lateral loss of vibration and proprioception in the arm and leg (the same side affected by the hemiparesis) as the posterior columns also cross at or just above the level of the foramen magnum. The median longitudinal fasciculus (MLF) is usually not affected when there is a hemiparesis as the MLF is further back in the brainstem.
The MLF can be affected in isolation �a lacunar infarct� and this results in an ipsilateral internuclear ophthalmoplegia, with failure of adduction (movement towards the nose) of the ipsilateral eye and leading eye nystagmus on looking laterally to the opposite side of the lesion in the contra lateral eye. If the patient had involvement of the left MLF then, on being asked to look to the left, the eye movements would be normal, but on looking to the right the left eye would not go past the midline, while there would be nystagmus in the right eye as it looked to the right.
Figure 3 shows the clinical features of the medial brainstem syndromes.
LATERAL BRAINSTEM SYNDROMES
Once again we are assuming that the patient you are seeing has a brainstem problem, most likely a vascular lesion. The 4 S�s or �meridians of longitude� will indicate that you are dealing with a lateral brainstem problem and the cranial nerves or �parallels of latitude� will indicate whether the problem is in the lateral medulla or lateral pons.
A lateral brainstem infarct will result in ipsilateral ataxia of the arm and leg as a result of involvement of the Spinocerebellar pathways, contralateral alteration of pain and temperature sensation as a result of involvement of the Spinothalamic pathway, ipsilateral loss of pain and temperature sensation affecting the face within the distribution of the Sensory nucleus of the trigeminal nerve (light touch may also be affected with involvement of the spinothalamic pathway and/or sensory nucleus of the trigeminal nerve). An ipsilateral Horner�s syndrome with partial ptosis and a small pupil (miosis) is because of involvement of the Sympathetic pathway. The power tone and the reflexes should all be normal. So far all we have done is localize the problem to the lateral aspect of the brainstem; by adding the relevant 3 cranial nerves in the medulla or the pons we can localize the lesion to this region of the brain.
The lower 4 cranial nerves are in the medulla and the 12th nerve is in the midline so that 9th, 10th and 11th nerves will be in the lateral aspect of the medulla. When these are affected, the result is dysarthria and dysphagia with an ipsilateral impairment of the gag reflex and the palate will pull up to the opposite side; occasionally there may be weakness of the ipsilateral trapezius and/or sternocleidomastoid muscle. This is the lateral medullary syndrome usually resulting from occlusion of the ipsilateral vertebral or posterior inferior cerebellar arteries.
The 4 cranial nerves in the pons are: 5th, 6th, 7th and 8th. The 6th nerve is the motor nerve in the midline, the 5th, 7th and 8th are in the lateral aspect of the pons, and when these are affected there will be ipsilateral facial weakness, weakness of the ipsilateral masseter and pterygoid muscles (muscles that open and close the mouth) and occasionally ipsilateral deafness. A tumour such as an acoustic neuroma in the cerebello-pontine angle will result in ipsilateral deafness, facial weakness and impairment of facial sensation; there may also be ipsilateral limb ataxia if it compresses the ipsilateral cerebellum or brainstem. The sympathetic pathway is usually too deep to be affected.
If there are signs of both a lateral and a medial (paramedian) brainstem syndrome, then one needs to consider a basilar artery problem, possibly an occlusion.
In summary, if one can remember that there are 4 pathways in the midline commencing with the letter M, 4 pathways in the lateral aspect of the brainstem commencing with the letter S, the lower 4 cranial nerves are in the medulla, the middle 4 cranial nerves in the pons and the first 4 cranial nerves above the pons with the 3rd and 4th in the midbrain, and that the 4 motor nerves that are in the midline are the 4 that divide evenly into 12 except for 1 and 2, that is 3, 4, 6 and 12, then it will be possible to diagnose brainstem vascular syndromes with pinpoint accuracy.
P. GATES
The Geelong Hospital, Barwon Health, Geelong, Victoria, Australia
Physicians, neurologists, and other healthcare professionals may often run a cranial nerve examination as part of a neurological evaluation to analyze the operation of the cranial nerves. This involves a highly formalized series of tests that evaluate the status of each cranial nerve. A cranial nerve test begins with observation of the patient partly due to the fact that cranial nerve lesions may ultimately affect the symmetry of the face or eyes, among other signs and symptoms.
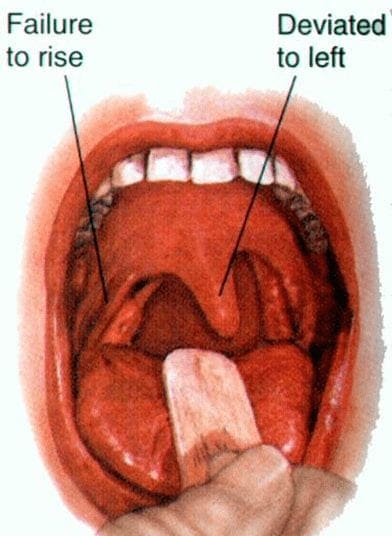
The visual fields for neural lesions or nystagmus�are tested via an evaluation of particular eye movements. The sensation of the face is tested by asking patients to execute different facial movements, like puffing out their cheeks. Hearing is tested through voice and tuning forks. The position of the individual’s uvula is also examined because asymmetry in its placement could indicate a lesion of the glossopharyngeal nerve. After the capability of the individual to use their shoulder to test the accessory nerve (XI), the patient’s tongue operation is generally assessed by detecting various tongue movements.
Damage or Injury of the Cranial Nerves
Compression
Cranial nerves may be compressed due to increased intracranial pressure, a profound effect of an intracerebral haemorrhage, or tumour which presses against the cranial nerves and interferes with the communication of impulses along the length of a nerve. In some instances, a loss of functionality of one cranial nerve may on occasion be the first symptom of an intracranial or skull base cancer.
An increase in intracranial pressure can lead to dysfunction of the optic nerves (II) because of the compression of the surrounding veins and capillaries, resulting in swelling of the eyeball, known as papilloedema. A cancer, such as an optic glioma, can also affect the optic nerve (II). A pituitary tumour can compress the optic tracts or the optic chiasm of the optic nerve (II), causing visual field loss. A pituitary tumour may also extend into the cavernous sinus, compressing the oculuomotor nerve (III), the trochlear nerve (IV) and the abducens nerve (VI), often leading to double-vision and strabismus. These cranial nerves may also be impacted by herniation of the temporal lobes of the brain via the falx cerebri.
The cause of trigeminal neuralgia, where one side of the face experiences painful signs and symptoms, is believed to be due to the compression of a cranial nerve by an artery as the nerve exits from the brain stem. An acoustic neuroma, especially at the junction between the pons and medulla, may compress the facial nerve (VII) and the vestibulocochlear nerve (VIII), resulting in hearing and sensory loss on the affected side.
Stroke
Occlusion of blood vessels which supply the cranial nerves or their nuclei, or an ischemic stroke, might cause specific signs and symptoms which could localize where the occlusion happened. A clot in a blood vessel draining the cavernous sinus, also known as the cavernous sinus thrombosis, may affect the oculomotor (III), the trochlear (IV), and the opthalamic branch of the trigeminal nerve (V1) and the abducens nerve (VI).
Inflammation
Inflammation caused by an infection may impair the operation of any of the cranial nerves. Infection of the facial nerve (VII), for instance, can result in Bell’s palsy. Multiple sclerosis, an inflammatory process which can produce a loss of the myelin sheathes that encircle the cranial nerves, may cause a variety of shifting signs and symptoms which can ultimately affect multiple cranial nerves.
Other
Trauma to the skull, bone disease like Paget’s disease, and damage or injury to the cranial nerves through neurosurgery, by way of instance, through tumor removal, are other potential causes of cranial nerve health issues.
Dr. Alex Jimenez’s Insight
There are 12 pairs of cranial nerves which exit the brain, one in each side. These cranial nerves are named and numbered (I-XII) according to their location in the brain as well as their specific function in the body. Common conditions, such as multiple sclerosis, may affect one or more of the cranial nerves, resulting in dysfunction of the specific regions innervated by them. Signs and symptoms associated with health issues affecting specific cranial nerves can help healthcare professionals determine the source of the problem. Testing the cranial nerves involves a number of steps in order to be certain which function of the human body has been ultimately affected.
Clinical Significance of the Cranial Nerves
Most commonly, humans are believed to have twelve pairs of cranial nerves which have been assigned Roman numerals I-XII for identification. The numbering of the cranial nerves is based on the order in which they emerge from the brain, or from the front to the back of the brainstem. These include: the olfactory nerve (I), the optic nerve (II), the oculomotor nerve (III), the trochlear nerve (IV), the trigeminal nerve (V), the abducens nerve (VI), the facial nerve (VII), the vestibulocochlear nerve (VIII), the glossopharyngeal nerve (IX), the vagus nerve (X), the accessory nerve (XI), and the hypoglossal nerve (XII). Below we will narrow down the clinical significance of the cranial nerves.
Olfactory Nerve (I)
The olfactory nerve (I) communicates the sensation of smell to the brain. Lesions resulting in anosmia, or loss of the sense of smell, have been previously described to occur through trauma, damage or injury to the head, especially in the instance that a patient hits the back of their head. In addition, frontal lobe masses, tumors, and SOL have also been associated with the loss of the sense of smell. Healthcare professionals have previously identified that the loss of the sense of smell is one of the first symptoms seen in Alzheimer’s and early dementia patients.
Healthcare professionals may test the function of the olfactory nerve (I) by having the patient close their eyes and cover one nostril at a time in order to have them breathe out through their nose while placing a scent under the nostril and having them breathe in. The doctor will ask the patient, “do you smell anything?”, and record the findings. This tests whether the nerve is operating appropriately. If the patient says yes, the doctor will then ask the patient to identify the scent. This tests whether the processing pathway, known as the temporal lobe, is functioning accordingly.
Optic Nerve (II)
The optic nerve (I) communicates visual information to the retina. Lesions to this cranial nerve can be the result of CNS disease, such as MS, or CNS tumors and SOL. Most health issues associated with the visual system emerge from direct trauma, metabolic or vascular diseases. FOV lost in the periphery can also indicate that SOL may be affecting the optic chiasm, including a pituitary tumor.
A healthcare professional will often test the function of the optic nerve (II) by asking whether the patient can see. If the patient describes having vision in each eye, the optic nerve is functional. Doctors may also perform visual acuity testing using the Snellen chart, first one eye at a time, then the two eyes together, or they may perform distance vision testing. Near vision testing will often involve the Rosenbaum chart, first one eye at a time, then the two eyes together. Additional associated testing for the visual system can include, the ophthalmoscopic or funduscopic exam, which assess the A/V ratio and vein/artery health as well as assess cup to disc ratio of the visual system. Other testing methods include field of vision testing, intraoccular pressure testing and the iris shadow test.
Oculomotor Nerve (III), Trochlear Nerve (IV), and Abducens Nerve (VI)
The oculomotor nerve (III), the trochlear nerve (IV), the abducens nerve (VI) and the ophthalmic division of the trigeminal nerve (V1) travel through the cavernous sinus to the superior orbital fissure, passing out of the skull into the orbit. These cranial nerves control the tiny muscles that move the eye and also offer sensory innervation to the eye and orbit.
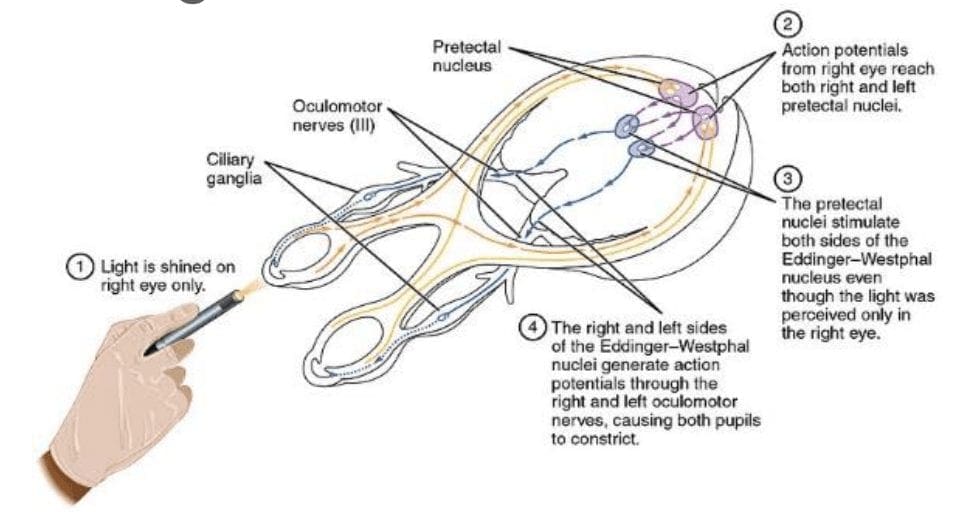
The clinical significance of the oculomotor nerve (III) includes diplopia, lateral strabismus (unopposed lateral rectus m.), head rotation away from the side of the lesion, a dilated pupil (unopposed dilator pupillae m.), and ptosis of the eyelid (loss of function of the levator palpebrae superioris m.). Lesions to the oculomotor nerve (III) can occur due to inflammatory diseases, such as syphilitic and tuberculous meningitis, aneurysms of the posterior cerebral or superior cebellar aa., and SOL in the cavernous sinus or displacing the cerebral peduncle to the opposite side. Testing this cranial nerve is performed by moving a light in front of the patient’s pupil from the lateral side and hold for 6 seconds. The doctor should watch for direct (ispilateral eye) and consensual (contralateral eye) pupillary constriction in order to distinguish dysfunction of the oculomotor nerve (III).
The clinical significance of the trochlear nerve (IV) is characterized where the patient presents diplopia and difficulty while maintaining a downward gaze, often complaining of having difficulties when walking down stairs, resulting in more frequent tripping and/or falling, followed by extortion of the affected eye (unopposed inferior oblique m.) and a head tilt to the unaffected side. Lesions to the trochlear nerve (IV) can commonly be the result of inflammatory diseases, aneurysms of the posterior cerebral or superior cerebellar aa., SOL in the cavernous sinus or superior orbital fissure and surgical damage during mesencephalon procedures. Head tilts in superior oblique palsy (CN IV failure) may also be identified.
The clinical significance of the abducens nerve (VI) includes diplopia, medial strabismus (unopposed medial rectus m.), and head rotation towards the side of the lesion. Lesions to this cranial nerve can be the result of aneurysms of the posterior inferior cerebellar or basilar aa., SOL in the cavernous sinus or 4th ventricle, such as a cerebellar tumor, fractures of the posterior cranial fossa, and increased intracranial pressure. Testing this cranial nerve is performed through the H-Pattern testing, where the healthcare professional will have the patient follow an object no bigger than 2 inches. It’s essential for the doctor to follow these specific guidelines as patient’s can have difficulties focusing on items that are too large, and it’s also important for the doctor not to hold the object too close to the patient. Convergence and accommodation testing is performed by bringing the object close to the bridge of the patient’s nose and back out at least 2 times. The physician must look for pupillary constriction response as well as convergence of the eyes.
Trigeminal Nerve (V)
The trigeminal nerve (V) is made up of three different parts: The . When put together, these nerves provide sensation to the skin of the face and also controls the muscles of mastication, or chewing. Cranial nerve dysfunction along any of the separate sections of the trigeminal nerve (V) can manifest as decreased bite strength on the ipsilateral side of the lesion, loss of sensation along the distribution of V1, V2, and V3, and loss of corneal reflex. Lesions to the trigeminal nerve (V) can be the result of aneurysms or SOL affecting the pons, particularly tumors at the cerebellopontine angle, skull fractures on the facial bones or damage to the foramen ovale, and Tic doloureux, most frequently referred to as trigeminal neuralgia, characterized by sharp pain along the distributions of the different parts of the trigeminal nerve (V). Physicians may utilize analgesic, anti-inflammatory or contralateral stimulation to control the signs and symptoms.
Testing the trigeminal nerve (V) includes pain & light touch testing along the ophthalmic (V1), the maxillary (V2), as well as the Mandibular (V3) nerves of the cranial nerve.�Testing is best done toward the more medial or proximal areas of
the face, where the V1, the V2 and the V3 are better delineated. A healthcare professional may also assess dysfunction along this cranial nerve using the blink/corneal reflex testing, performed by puffing air or doing a small tissue tap from the lateral side of the eye on the cornea. If normal, the patient blinks. The CN V provides the sensory (afferent) arc of this reflex. Bite strength may also be tested by having the patient bite down on a tongue depressor while the doctor tries to remove it. The jaw jerk/Masseter reflex may also be performed with the patient�s mouth slightly open, by placing the thumb on a patient�s chin and tapping the own thumb with a reflex hammer. Strong closure of the mouth indicates UMN lesion. CN V provides both the motor and sensory of this reflex.
Facial Nerve (VII) and Vestibulocochlear Nerve (VIII)
The facial nerve (VII) and the vestibulocochlear nerve (VIII) both input the inner auditory canal in the temporal bone. The facial nerve subsequently extends to the side of the face then distributes to control and reach all of the muscles in charge of facial expressions. The vestibulocochlear nerve reaches the organs which control equilibrium and hearing in the temporal bone.
As with all cranial nerves, signs and symptoms along the facial nerve (VII) describe the location of the lesion. Lesion in the lingual nerve will manifest as loss of taste, general sensation in the tongue and salivary secretion. Lesion proximal to the branching of the chorda tympani, such as in the facial canal, will result in the same signs and symptoms, without the loss of general sensation of the tongue, partly due because the V3 has not yet joined the facial nerve (VII). Corticobulbar innervation is asymmetric to the upper and lower parts of the facial motor nucleus. In the instance of an UMN lesion, or a lesion to the corticobulbar fibers, the patient will experience paralysis of the muscles in charge of facial expression in the contralateral lower quadrant. If there is an LMN lesion, or a lesion to the facial nerve itself, the patient will experience paralysis of the muscles of facial expression in the ipsilateral half of the face, otherwise known as Bell’s palsy.
A healthcare professional will test the facial nerve (VII) initially by asking the patient to mimic or follow specific instructions to make certain facial expressions. The doctor should make sure to evaluate all four quadrants of the face by asking the patient to raise their eyebrows, puff their cheeks, smile and then close their eyes tightly. Subsequently, the doctor will test the facial nerve (VII) by checking the strength of the buccinator muscle against resistance. The healthcare professional will achieve this by asking the patient to hold air in their cheeks as they press gently from the outside. The patient should be able to hold air in against the resistance.
Signs and symptoms of dysfunction in the vestibulocochlear nerve (VIII) often involve changes in hearing alone, most commonly as a result of infections in the otitis media and/or as a result of skull fractures. The most common lesion to this nerve is caused by an acoustic neuroma which affects the CN VII and the CN VIII, particularly the cochlear and vestibular divisions, as a result of proximity in the internal auditory meatus. Signs and symptoms of the health issue include nausea, vomiting, dizziness, hearing loss, tinnitus, and Bell’s palsy, etc.
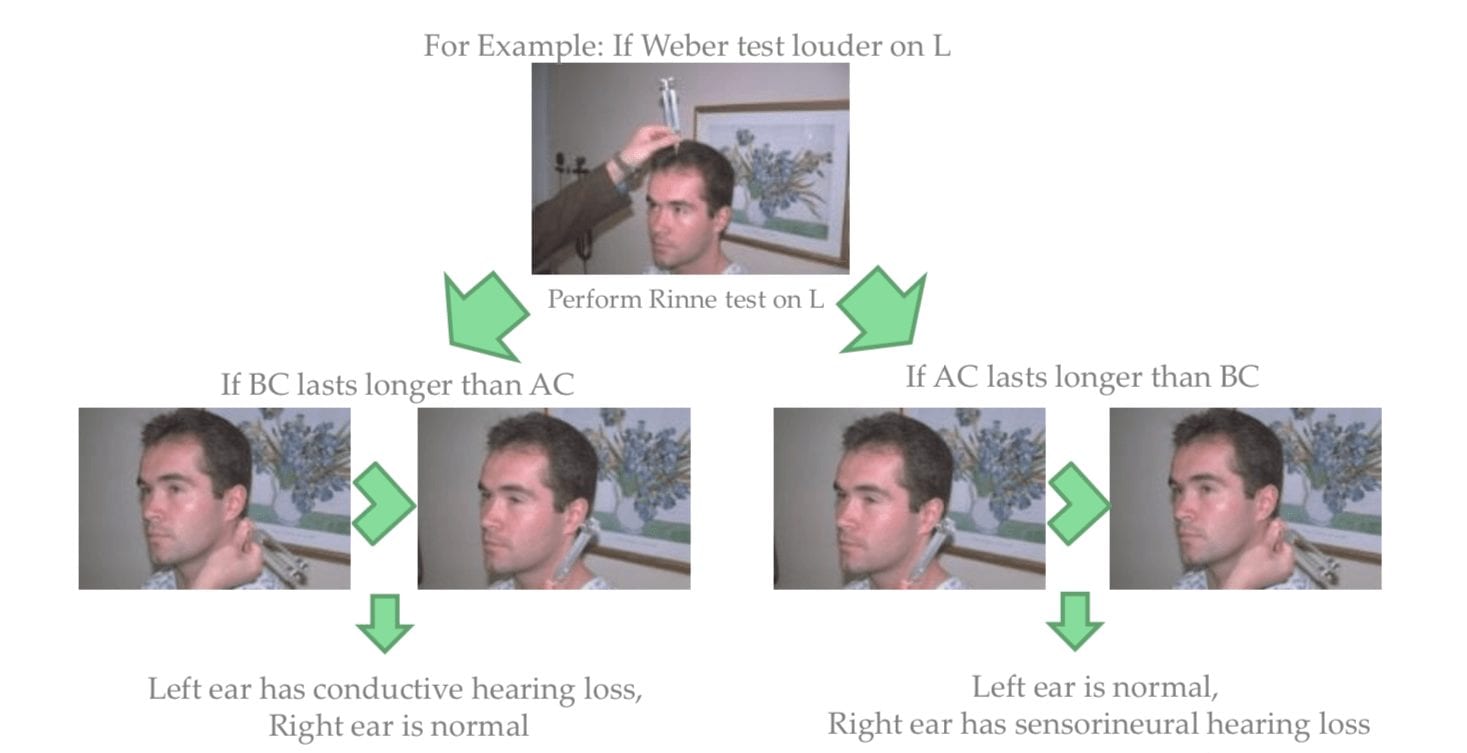
Testing the vestibulocochlear nerve (VIII) for dysfunction commonly involves an otoscopic exam, the scratch test, which determines whether a patient can hear equally on both sides, the Weber test, tests for lateralization, a 256 Hz tuning fork placed on top of the patient�s head in the center, which can help point out whether a patient hears it louder on one side than the other, and finally the Rinne test, which compares air conduction to bone conduction. Normally, air conduction should last twice as long as bone conduction.
Glossopharyngeal Nerve (IX), Vagus Nerve (X) and Accessory Nerve (XI)
The glossopharyngeal (IX), the vagus nerve (X) and the accessory nerve (XI) all emerge from the skull to enter the neck. The glossopharyngeal nerve (IX) provides innervation to the upper throat and the back of the tongue, the vagus nerve (X) offers innervation to the muscles at the voicebox, and proceeds down to provide parasympathetic innervation to the chest and abdomen. The accessory nerve (XI) controls the trapezius and sternocleidomastoid muscles at the neck and shoulder.
The glossopharyngeal nerve (IX) is rarely damaged alone, due to it�s proximity to the CN X and XI. A healthcare professional should perform a test to look for signs of CN X & XI damage as well if CN IX involvement is suspected.
Patients with clinical signs and symptoms caused by vagus nerve (X) dysfunction may experience dysarthria, or difficulty speaking clearly, as well as dysphagia, or difficulty swallowing. These may present as food or liquid coming out of their nose or frequent chocking or coughing when eating and/or drinking. Further clinical presentations include hyperactivity of a visceral motor component, leading to the hypersecretion of gastric acid and resulting in ulcers. Hyper-stimulation of the general sensory component can cause coughing, fainting, vomiting and reflex visceral motor activity. The visceral sensory component of this nerve only provides general feelings of un-wellness but visceral pain may transfer on to the sympathetic nerves.
Testing for the glossopharyngeal nerve (IX) and the vagus nerve (X) can include the gag reflex, where the�CN IX provides the afferent (sensory) arc and the�CN X provides the efferent (motor) arc. Approximately 20 percent�of patients have a minimal or absent gag reflex. Other tests may include wwallowing, gargling, etc., as it requires CN X function. Healthcare professionals may also test palatal elevation because it requires CN X function. Furthermore, the doctor will see whether the palate elevates and uvula deviates
contralateral to damaged side. Finally, the healthcare professional will test the auscultation of the heart, since the R CN X innervates SA node (more rate regulation) and the L CN X the AV node (more rhythm regulation).
Lesions in the accessory nerve (XI)�may occur due to radical surgeries in the neck area, such as the removal of the laryngeal carcinomas. Testing for the accessory nerve (XI) may include the strength test SCM m. Patients with clinical signs and symptoms due to lesions in the accessory nerve (XI) will experience difficulties turning their head against the resistance of a healthcare professional, particularly toward the side opposite of the lesion. Testing for the accessory nerve (XI) may also include the strength test trapezius m. Patients with clinical signs and symptoms due to lesions in the accessory nerve (XI) will experience difficulties with shoulder elevation on the side of the lesion.
Hypoglossal Nerve (XII)
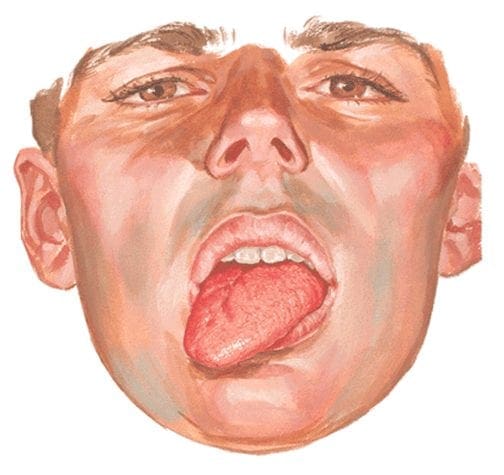
The hypoglossal nerve (XII) originates from the skull to reach the tongue in order to control essentially all of the muscles involved in the movements of the tongue. The clinical significance of health issues associated to the hypoglossal nerve (XII) can manifest as a deviating tongue towards the side of an inactive genioglossus m. upon tongue protrusion. This may often be contralateral to a corticobulbar, or UMN, lesion or from an ipsilateral to a hypoglossal n., or LMN, lesion.
Testing for the hypoglossal nerve (XII) involves the healthcare professional asking a patient to stick out their tongue. The doctor will look for any deviation which may signal a health issue along the length of the hypoglossal nerve (XII). Another test the doctor may perform as a part of the evaluation may include the physician asking the patient to place their tongue inside their cheek and apply light resistance, one side at a time. The patient should be able to resist moving their tongue with pressure.
The clinical significance of the signs and symptoms which manifest as a result of cranial nerve dysfunction are essential in order for the healthcare professional to properly diagnose the patient’s specific health issue. The clinical findings described above are often unique to the affected cranial nerve and the tests and evaluations for each can help confirm a diagnosis. Proper diagnosis is fundamental in order for the doctor to continue with the patient’s appropriate treatment. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is medically referred to as a collection of symptoms, rather than a single injury and/or condition. Symptoms of sciatic nerve pain, or sciatica, can vary in frequency and intensity, however, it is most commonly described as a sudden, sharp (knife-like) or electrical pain that radiates from the low back down the buttocks, hips, thighs and legs into the foot. Other symptoms of sciatica may include, tingling or burning sensations, numbness and weakness along the length of the sciatic nerve. Sciatica most frequently affects individuals between the ages of 30 and 50 years. It may often develop as a result of the degeneration of the spine due to age, however, the compression and irritation of the sciatic nerve caused by a bulging or herniated disc, among other spinal health issues, may also cause sciatic nerve pain.
Ataxia is a degenerative disease of the nervous system. Symptoms can mimic those of being inebriated/intoxicated, with� slurred speech, stumbling, falling, and unable to maintain coordination. This comes from degeneration of the cerebellum, which is the part of the brain responsible for coordinating movement. It is a disease that affects people of all ages. However, age of symptom onset can vary, from childhood to late adulthood. Complications from the disease can be serious, even debilitating and life shortening.
Symptoms can vary from person to person, as well as, the type of Ataxia. Symptom onset and progression can vary as well. Symptoms can worsen slowly, over decades or quickly, over a few months. The common symptoms are lack of coordination, slurred speech, trouble eating, swallowing, eye movement abnormalities, motor skill deterioration, difficulty walking, gait abnormalities, tremors, and heart problems. People with Ataxia usually require wheelchairs, walkers, and/or scooters to aid in mobility.
Ataxia
The Loss Of Full Control Of Bodily Movements, Especially Gait
History Of Ataxia
How long has it been present?
Slow onset ? Degenerative disease?
Acute onset ? Stroke?
When does it occur?
If worsened by walking on uneven surfaces, or with limited vision ? Sensory ataxia?
Are there any coexisting symptoms?
Vertigo, weakness, stiffness, cognitive changes, etc.
Have others noticed this gait disturbance?
If no, consider psychogenic cause
Is the gait change explainable by physical problems such as pain or weakness?
Antalgic gait, limp, etc.
Weakness
Proximal muscle weakness�? Myopathy?
Distal muscle weakness ? Neuropathy?
UMN signs?
LMN signs?
Has the patient fallen? Or at risk for fall?
Is ataxia limiting ADLs?
Balance
Utilizes
Vestibular system
Cerebellar system
Conscious proprioceptive information (joint position sense)
Visual information
Motor strength and coordination
Vestibular System
Generally, if the problem lies in the vestibular system the patient will experience dizziness, possibly having vertigo or nystagmus
Does the dizziness feel similar to when you stand up too fast?
Pre-Syncope
�Light-headedness�
CardiacOrigin
Output disorders
Arrhythmias
Holter monitor testing
Postural/Orthostatic hypotension
May be secondary to other problems (diabetic neuropathy, adrenal hypofunction, Parkinsons, certain medications, etc.)
Vasovagal episodes
Slow heart rate with low blood pressure
Often brought on by stress, anxiety or hyperventilation
Migraine
Due to cerebrovascular instability
Blood sugar dysregulation
Disequilibrium Hx Questions
Does the dizziness only occur when you�re on your feet?
Does it get better if you touch/hold onto something?
Disequilibrium
Common in the elderly
Due to sensory deficits
Gradual onset
Worsened by reduced vision
Dark
Eyes closed
Visual acuity losses
Improved by touching a stationary object
Subjective of dizziness often improves with a gait assistive device (cane, walker, etc.)
Other Causes
Psychological stress
Often patient will describe dizziness as �floating�
Rule out hyperventilation and other types of dizziness
Sources
Blumenfeld, Hal. Neuroanatomy through Clinical Cases. Sinauer, 2002.
Alexander G. Reeves, A. & Swenson, R. Disorders of the Nervous System. Dartmouth, 2004.
You have been diagnosed with Benign Paroxysmal Positional Vertigo. This brochure is designed to help increase your understanding of this disorder and its potential treatments.
Benign Paroxysmal Positional Vertigo
What Is BPPV?
Benign paroxysmal positional vertigo (BPPV) is a disorder of the inner ear. People with BPPV typically experi�ence brief episodes of vertigo (dizziness) when they change the position of their head with respect to gravity. Approximately 20 percent of all vertigo is due to BPPV.
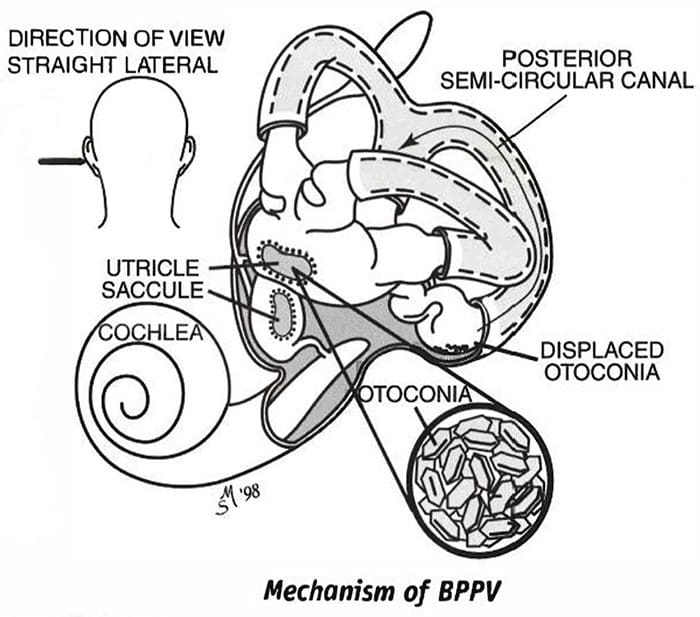
What Causes BPPV?
Benign Paroxysmal Positional Vertigo is thought to be due to tiny crystals, called otoconia, that have collected within a sensitive part of the inner ear. Otoconia are crystals of calcium carbonate that are normally located in a structure of the ear called the utricle.
Dizziness occurs when the crystals are displaced from the utricle into the semicircular canals of the inner ear.
Otoconia may become displaced when the utricle is injured, if there is an infection or other disorder of the inner ear, or simply due to advanced age. When you change the position of your head, the otoconia move within the semicircular canals and this causes the dizziness. The dizziness subsides when the otoconia stop moving.
The most common cause of BPPV in people under age 50 is head injury. In older people, the most common cause is degeneration of the vestibular system of the inner ear. BPPV becomes much more common with advancing age. Other causes include minor strokes, Meniere’s disease, and viruses such as those causing vestibular neuritis. In approximately half of all BPPV cases, no cause can be determined.
What Are The Symptoms?
The symptoms of BPPV include dizziness or vertigo, lightheadedness, imbalance, and nausea. Activities that
bring on symptoms vary among individuals, but symptoms are usually associated with a change in the position of the head with respect to gravity. Getting out of bed, rolling over in bed, and tipping the head back to look up are common “problem” motions. The use of shampoo bowls in hair salons may bring on symptoms. An intermittent pattern is common. BPPV may be present for a few weeks, then stop, and then come back again.
How Is Benign Paroxysmal Positional Vertigo (BPPV) Diagnosed?
BPPV is diagnosed with the Dix-Hallpike test. This test involves observing the eyes with the head and body positioned in specific ways. It can be performed either by the clinician, or as part of a laboratory test called an electronystagmography, or ENG. If the Dix-Hallpike test is abnormal and the findings are “dassic” for BPPV, then additional testing is not necessary. If the results are normal or not “classic” then the diagnosis of BPPV is less certain and other tests may be suggested.
What Are The Treatments For BPPV?
There are four approaches to treating BPPV.
1. Do Nothing And Wait For It To Go Away By Itself
BPPV symptoms sometimes go away within six months of onset, therefore you might want to wait and see if your symptoms subside on their own. During this waiting period, medications to prevent motion sickness or nausea are sometimes helpful in controlling the nausea associated with BPPV.
2. Physical Maneuvers Performed In The Clinic
(The Epley and Semont Maneuvers)
The Epley and Semont maneuvers, named for their inventors, are treat�ments that are performed in the clinic. These treatments are specifi�cally intended to move the otoconia from the semicircular canals to a less sensitive location within the inner ear. Your clinician will select the treatment that is most appropriate for you.
Each of these treatments takes about 15 minutes and alleviates symptoms in about 80 percent of patients. In the remaining 20 percent, a second treatment may be necessary, or you may be instructed to perform the Brandt-Daroff exercises (see “Home Treatment”).
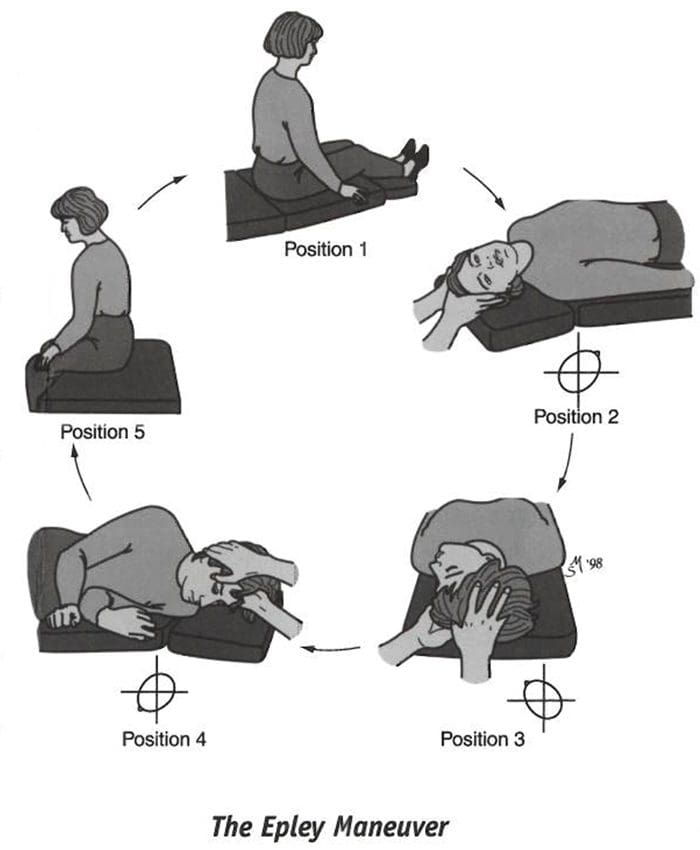
The Epley maneuver, also called the canalith reposi�tioning procedure (CRP) and particle repositioning, is a procedure in which the clinician moves your head into five positions, maintaining each position for ap�proximately 30 seconds. The Semont maneuver (also called the liberatory maneuver) is a procedure in which the clinician rapidly moves you from lying on one side to lying on the other side. These maneuvers may not be appropriate for patients with neck or back problems. Pa�tients who experience nausea or anxiety may wish to take medication prior to the treatment.
INSTRUCTIONS FOR PATIENTS AFTER CLINIC TREATMENTS
Follow these instructions after the Epley or Semont maneuver. B.Y doing so you will minimize the opportunity for otoconia to return to the semicircular canals of the inner ear and reduce the potential that your dizziness will recur.
Wait at least 10 minutes after the maneuver before going home.
This is to avoid “quick spins” or brief bursts of vertigo as the otoconia reposition themselves immedi�ately after the maneuver. If possible, arrange to have someone drive you home.
The following two days:
Sleep semi-recumbent for the next two nights. This means sleeping with your head halfway between flat and upright, at a 45-degree angle. This is most easily done by sleeping in a recliner chair or by sleeping with pillows appropriately arranged on a couch.
During the day, try to keep your head vertical. A soft neck brace may be helpful.
Do not go to the barber, hairdresser or dentist.
When shaving, keep your head vertical by bending forward at your hips with your neck extended.
If you need to administer eye drops, try to keep your head as vertical as possible.
Sham�poo only under the shower.
During the following week, avoid provoking head positions that might bring on BPPV.
Use two pillows when you sleep.
Avoid sleeping on the affected side.
Don’t turn your head far up or far down.
Avoid tilting your head back especially when lying on your back with your head turned toward the affected side.
If possible, postpone elective surgery and going to the beauty parlor or the dentist’s office.
Avoid far head-forward positions and exercises where the head is not kept upright, for example toe touches.
The effectiveness of the clinic treatment cannot be determined for one week.
Wait one week after treatment to test the effectiveness of treatment. Place yourself in the position that usually makes you dizzy. Be sure to position yourself cautiously and under conditions in which you can’t fall or hurt yourself.
3. Home Treatment Of Benign Paroxysmal Positional Vertigo (Brandt-Daroff Exercises)
When the clinic treatment (Epley or Semont) fails, when the involved side is not determined, or when a case is mild, the Brandt-Daroff exercises may be recommended. These exercises succeed in 95 percent of cases but take longer to work than the clinic treatments. You should perform these exercises only if instructed to do so by your clinician. If your clini�cian performed the Epley or Semont maneuver, you must wait one week after that treatment before you begin the Brandt-Daroff exercises.
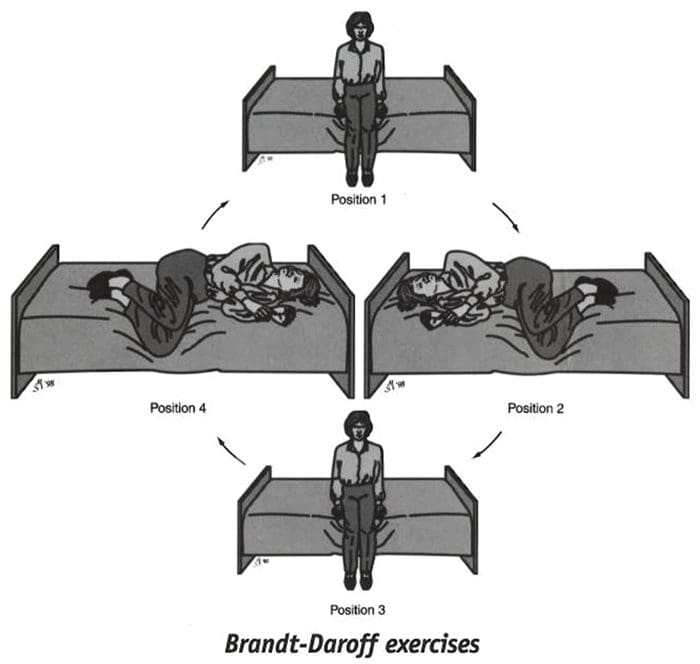
These exercises should be performed on a flat surface, without a pillow.
Start sitting upright on the edge of the bed or on the floor.
(Position 1)�Turn your head 45 degrees to the left and lie down on your right side.
(Position 2)�When in the right side-lying position, your head should be at a 45-degree angle turned halfway between the flat surface and the ceiling. Stay in the side-lying position for at least 30 seconds. If you are still dizzy, stay until the dizziness subsides or one minute, whichever is less.
Then sit up (Position 3} and stay in the sitting posi�tion for 30 seconds. Turn your head 45 degrees to the right and lie down on your left side.
(Position 4)�Again keeping your head turned halfway toward the ceiling for 30 seconds or until the dizziness subsides. Return to Position 1 (sit upright) for 30 seconds. This is one repetition.
One set (five repetitions) takes about 10 minutes to complete and should be performed each morning, mid-day and evening.
The Brandt-Daroff exercises should be performed for two weeks, three sets each day, or for three weeks, two sets each day (52 sets total). In most individuals, complete relief from symptoms is obtained after 30 sets, or about 10 days. In approximately 30 percent of patients, BPPV will recur within one year. If BPPV recurs you may wish to add one 10-minute exercise (one set) to your daily routine.
If the maneuvers or exercises do not control symptoms that have persisted for a year or longer and the diagnosis is very clear, surgery may be recommended. The most common surgical procedure, called posterior canal plugging, blocks most of the posterior canal’s function without affecting the functions of the other canals or parts of the ear. There is, however, a small risk of hearing loss. This surgery is effective in about 90 percent of individuals who have not responded to other treatments and when symptoms are severe and long-standing.
�?2000 Northwestern University. Authors: Timothy C. Hain, MD, Janet Odiry Helminski, PhD, PT.
This information is for educational purposes and is not intended as a substitute for examination, diagnosis, or medical care provided by a licensed and qualified health professional. This work was supported by the Center for Sensory and Communicotion Disorders at Northwestern University, a national research and training center funded by the National Institute on Deafness and Other Communication Disorders.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine







 LATERAL BRAINSTEM SYNDROMES
LATERAL BRAINSTEM SYNDROMES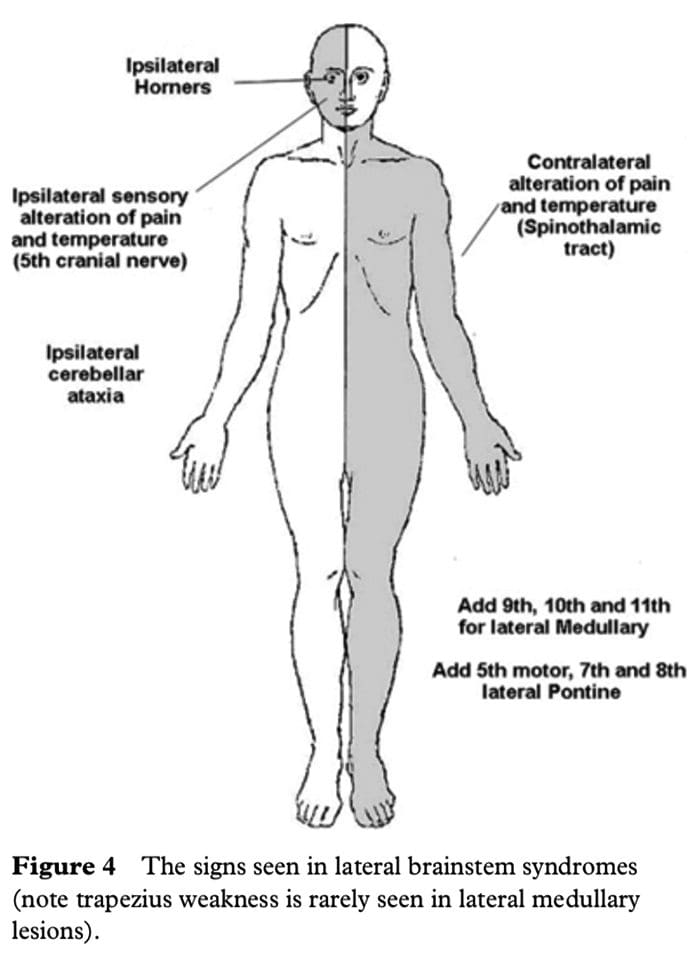 The lower 4 cranial nerves are in the medulla and the 12th nerve is in the midline so that 9th, 10th and 11th nerves will be in the lateral aspect of the medulla. When these are affected, the result is dysarthria and dysphagia with an ipsilateral impairment of the gag reflex and the palate will pull up to the opposite side; occasionally there may be weakness of the ipsilateral trapezius and/or sternocleidomastoid muscle. This is the lateral medullary syndrome usually resulting from occlusion of the ipsilateral vertebral or posterior inferior cerebellar arteries.
The lower 4 cranial nerves are in the medulla and the 12th nerve is in the midline so that 9th, 10th and 11th nerves will be in the lateral aspect of the medulla. When these are affected, the result is dysarthria and dysphagia with an ipsilateral impairment of the gag reflex and the palate will pull up to the opposite side; occasionally there may be weakness of the ipsilateral trapezius and/or sternocleidomastoid muscle. This is the lateral medullary syndrome usually resulting from occlusion of the ipsilateral vertebral or posterior inferior cerebellar arteries.
 May develop spontaneously, especially in the elderly
May develop spontaneously, especially in the elderly
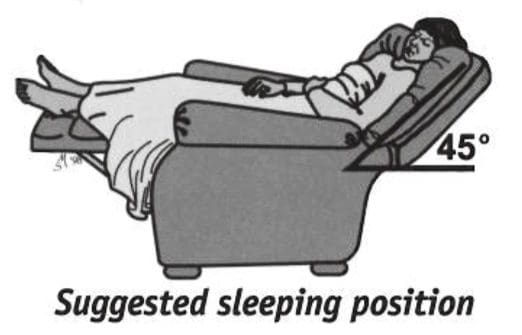 Sleep semi-recumbent for the next two nights. This means sleeping with your head halfway between flat and upright, at a 45-degree angle. This is most easily done by sleeping in a recliner chair or by sleeping with pillows appropriately arranged on a couch.
Sleep semi-recumbent for the next two nights. This means sleeping with your head halfway between flat and upright, at a 45-degree angle. This is most easily done by sleeping in a recliner chair or by sleeping with pillows appropriately arranged on a couch.