Uncover the connection between TMJ disorders and auto injuries, and explore ways to manage this common issue effectively.
Introduction
Imagine cruising down the road, enjoying a sunny day in El Paso, when—bam!—a car accident throws your world into a spin. Beyond the fender bender, you might start feeling pain in your jaw or neck that wasn’t there before. These could be signs of a Temporomandibular Joint (TMJ) disorder, a condition often linked to neck injuries from motor vehicle accidents (MVAs). In this comprehensive guide, we’ll explore why TMJ disorders and neck pain often go hand-in-hand after MVAs, the symptoms to watch for, nonsurgical treatment options, and the pivotal role of Dr. Alexander Jimenez, a distinguished chiropractor and nurse practitioner in El Paso, Texas. With a touch of humor to keep things light, we’ll also ensure you understand the serious nature of seeking professional care for these conditions.
Section 1: The Clinical Rationale for TMJ Disorders and Neck Pain from MVAs
Why Do TMJ Disorders Occur After MVAs?
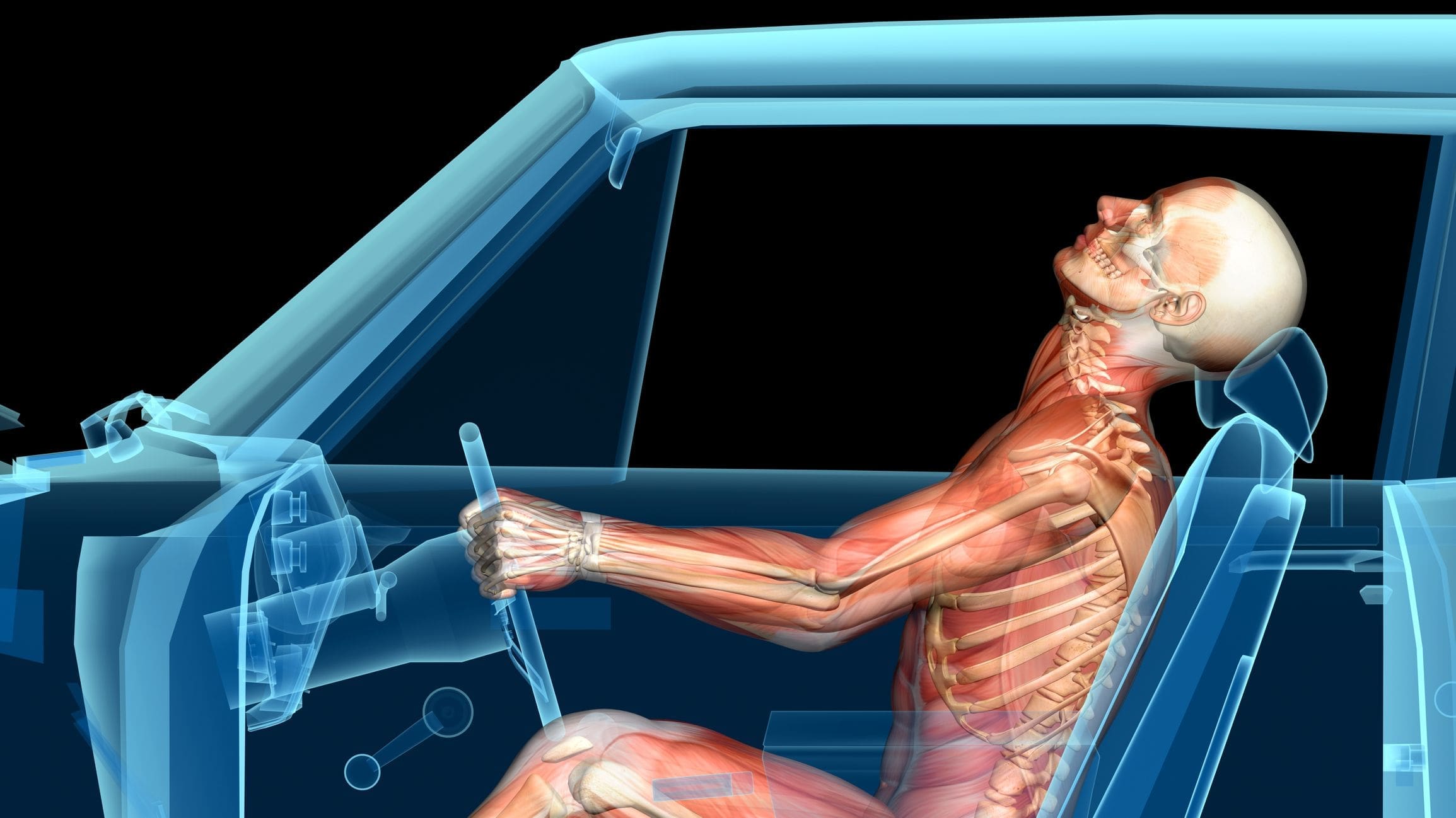
The temporomandibular joint connects your lower jaw to your skull, enabling essential functions like chewing and speaking. When you’re involved in a motor vehicle accident, the sudden jolt—especially in rear-end collisions—can cause whiplash, a neck injury that strains muscles, ligaments, and the cervical spine. This trauma can ripple to the TMJ, even if your jaw wasn’t directly hit.
Research suggests that the connection between TMJ disorders and neck pain lies in the body’s neurological wiring. Pain signals from the neck travel to the brainstem, where they can overlap with signals from the jaw. This phenomenon, known as referred pain, means a neck injury can manifest as jaw pain or TMJ dysfunction. A 1998 study in Clinical Oral Investigations highlighted that patients with cervical spine issues often experience TMJ symptoms, reinforcing this link (Caring Medical, 2025).
The Role of Whiplash
Whiplash is a hallmark injury of MVAs, occurring when the head is forcefully thrown forward and back. This motion can damage the cervical spine and surrounding tissues, leading to chronic neck pain. According to a study in PMC (2008), individuals with MVA-related neck pain report higher levels of continuous pain compared to other causes, which can exacerbate TMJ issues. The chronic inflammation and muscle tension from whiplash can overstimulate nerves, causing jaw muscle tightness and pain, further contributing to TMJ disorders.
Neurological and Muscular Connections
The brainstem acts like a busy switchboard, where nerves from the neck and jaw converge before sending pain signals to the brain. This convergence can lead to “crossed signals,” similar to how arm pain can signal a heart attack. As a result, neck injuries from MVAs can trigger or worsen TMJ symptoms. Additionally, chronic neck pain can lead to compensatory behaviors, like jaw clenching, which further stress the TMJ.
Section 2: Symptoms of TMJ Disorders Related to Auto Injuries
Recognizing TMJ Symptoms
TMJ disorders can manifest in various ways, often overlapping with neck pain symptoms. Common signs include:
Jaw Pain and Tenderness: Pain around the jaw or ear, especially when chewing or speaking.
Difficulty Chewing: Discomfort or pain while eating, sometimes making it hard to open the mouth fully.
Jaw Locking or Restricted Movement: The jaw may feel stuck or limited in its range of motion.
Clicking or Popping Sounds: Noises when opening or closing the mouth, which may or may not be painful.
Neck and Shoulder Pain: Stiffness or ascending order or pain radiating from the neck.
Headaches: Often, tension-type headaches are linked to muscle tension.
Dizziness or Tinnitus: Less common but possible symptoms include dizziness or ringing in the ears.
A 2022 study cited in Medical News Today found that nearly 60% of individuals with TMJ disorders also experience neck pain, highlighting the prevalence of this dual issue (Medical News Today, 2023).
Delayed Onset of Symptoms
One tricky aspect of TMJ disorders post-MVA is that symptoms may not appear immediately. According to the El Paso Chiropractor Blog (2016), these issues can develop weeks or even months after the accident, making it critical to monitor for symptoms over time. This delay can complicate diagnosis, as patients may not initially connect their jaw pain to the earlier accident.
Chiropractic Care After Accidents & Injuries- Video
Section 3: Nonsurgical Treatments for TMJ Disorders and Neck Pain
Conservative Approaches to Relief
Most TMJ disorders and associated neck pain from MVAs can be managed without surgery, focusing on reducing pain and restoring function. Here are the primary nonsurgical treatments:
Physical Therapy: Specialized exercises and stretches improve jaw mobility and reduce muscle tension. Soft tissue massages targeting muscles like the pterygoids can relieve trigger points, as noted in Dr. Jimenez’s work on TMJ and anxiety (Dr. Alex Jimenez, 2016).
Chiropractic Care: Spinal adjustments and manual manipulation correct misalignments in the neck and jaw, reducing pain and improving function. Chiropractic care is particularly effective for whiplash-related injuries (El Paso Chiropractor Blog, 2016).
Medications: Over-the-counter pain relievers (e.g., ibuprofen), muscle relaxants, or anti-inflammatory drugs help manage pain and inflammation. In some cases, anxiety medications or antidepressants may address related stress or jaw clenching (Medical News Today, 2023).
Oral Appliances: Custom-fitted mouthguards or splints reposition the jaw to reduce clenching or grinding, which can worsen TMJ symptoms.
Lifestyle Modifications: Avoiding hard foods, practicing stress-reduction techniques (such as meditation), and maintaining good posture can all support recovery.
Acupuncture: This alternative therapy can reduce pain and muscle tension, offering relief for some patients.
Personalized Treatment Plans
Each patient’s condition is unique, so treatments should be tailored to their specific symptoms and severity. Consulting a healthcare professional, like Dr. Jimenez, ensures a comprehensive plan that addresses both TMJ and neck pain effectively.
Section 4: Dr. Alexander Jimenez’s Expertise in El Paso
A Leader in Personal Injury Care
Dr. Alexander Jimenez, DC, APRN, FNP-BC, is a cornerstone of personal injury care in El Paso, Texas, with over 25 years of experience as a chiropractor and nurse practitioner. His dual licensure allows him to bridge chiropractic and medical approaches, offering holistic care for MVA-related injuries, including TMJ disorders and neck pain.
Advanced Diagnostics and Dual-Scope Procedures
Dr. Jimenez stands out for his use of advanced imaging techniques, such as MRI and CT scans, to precisely pinpoint the extent of injuries. His diagnostic evaluations are thorough, identifying both primary injuries (e.g., whiplash) and secondary conditions (e.g., TMJ disorders). His dual-scope procedures combine chiropractic adjustments with medical treatments, addressing biomechanical and physiological aspects of recovery. This integrative approach promotes long-term healing and metabolic resilience (Injury Medical & Chiropractic Clinic, n.d.).
Liaison Between Medical and Legal Services
In personal injury cases, Dr. Jimenez plays a vital role by providing detailed medical reports and expert testimonies. These documents help legal professionals understand the full impact of injuries, ensuring victims receive fair compensation. His clinic, Injury Medical & Chiropractic Clinic, specializes in MVA-related conditions like cervical spine issues, whiplash, and chronic inflammation, making him a trusted resource in El Paso (El Paso Back Clinic, n.d.).
Service
Description
Benefit
Advanced Imaging (MRI/CT)
Accurate diagnosis of MVA-related injuries
Precise treatment planning
Dual-Scope Procedures
Combining chiropractic and medical treatments
Holistic recovery
Legal Documentation
Detailed reports and testimonies for personal injury cases
Supports fair compensation
Specialized MVA Care
Focus on whiplash, cervical spine issues, and related conditions
Let’s take a moment to chuckle with Herman Munster from The Munsters: “Folks, your jaw’s like the creaky hinge on my old coffin—when it starts acting up after a car crash, it’s no laughing matter! That neck of yours gets a shake, and suddenly your jaw’s throwing a tantrum. Don’t stay stiff like me on a bad day; head to Dr. Jimenez in El Paso, and he’ll have you moving smoother than Grandpa Munster dodging a garlic clove!”
Section 6: The Importance of Personal Injury Care in El Paso
Why Seek Care After an MVA?
Motor vehicle accidents can leave lasting effects, from neck pain to TMJ disorders, that impact daily life. In El Paso, where personal injury cases are common due to the high volume of traffic, seeking expert care is crucial. Dr. Jimenez’s clinic is a beacon for victims, offering not only medical treatment but also support for legal claims. His comprehensive approach ensures that injuries are thoroughly documented, aiding in fair settlements while promoting recovery.
Community Impact
Dr. Jimenez’s work extends beyond individual patients, contributing to the El Paso community by raising awareness about motor vehicle accident (MVA)- related injuries. His clinic’s resources, including blog posts and patient testimonials, educate residents on recognizing and treating conditions such as TMJ disorders, thereby fostering a healthier community (Dr. Alexander Jimenez, LinkedIn).
Conclusion
TMJ disorders and neck pain from motor vehicle accidents are interconnected conditions that can significantly affect quality of life. The clinical link stems from shared neurological pathways and the impact of whiplash, with symptoms ranging from jaw pain to headaches and neck stiffness. Nonsurgical treatments, including physical therapy, chiropractic care, and oral appliances, provide effective relief for most patients. In El Paso, Dr. Alexander Jimenez stands out as a leader in personal injury care, using advanced diagnostics and dual-scope procedures to treat these conditions while supporting legal claims with detailed documentation. If you’ve been in an MVA and are experiencing jaw or neck pain, don’t delay—seek professional care to prevent long-term complications and restore your well-being.
Disclaimer: This blog post is for informational purposes only and should not be taken as medical advice. Always consult a qualified healthcare professional for diagnosis and treatment of any medical condition. The information provided is based on general knowledge and should not be used as a substitute for personalized medical care.
Discover the connection between the nervous system, auto injuries, and long-term health consequences in this informative article.
Introduction: The Sneaky Nature of Whiplash
Picture this: you’re cruising along, maybe singing to your favorite tune, when—BAM!—another car rear-ends you. Your head snaps back and forth like a bobblehead on a bumpy road. That’s whiplash, and it’s not just a pain in the neck (pun intended). Whiplash is a common injury from motor vehicle accidents (MVAs), particularly rear-end collisions, and it can wreak havoc on your nervous system and even cause low back pain. It’s like that one guest at a party who spills punch on your carpet and then rearranges your furniture—disruptive and far-reaching.
In this comprehensive guide, we’ll explore how whiplash affects your nervous system, why it might lead to low back pain, and what symptoms to watch for. We’ll also delve into nonsurgical treatments, with a focus on chiropractic care, and highlight the expertise of Dr. Alexander Jimenez, a leading practitioner in El Paso, Texas, who specializes in helping accident victims recover. With a touch of humor to keep things light (think Uncle Fester from The Addams Family chuckling through the pain), we’ll make this journey informative and engaging. Let’s get started!
Understanding Whiplash: What’s Happening to Your Body?
Whiplash occurs when your neck undergoes a rapid back-and-forth motion, typically resulting from a car accident. This sudden force can stretch or tear muscles, ligaments, and tendons in your neck, like overstretching a rubber band. According to the National Safety Council, over 3 million car accidents happen annually in the U.S., with rear-end collisions being a leading cause of whiplash. The injury doesn’t always scream “I’m here!” right away—symptoms can sneak up days or even weeks later, making it a tricky condition to pin down.
Whiplash isn’t just about sore muscles. It can affect your spine, discs, and nerves, leading to a condition called whiplash-associated disorders (WADs). These disorders can range from mild discomfort to chronic pain, impacting your quality of life. The economic toll is also significant, with whiplash-related costs in the U.S. estimated at $10 billion annually, encompassing medical bills, lost work, and legal fees (Whaangaard et al., 2017).
Whiplash and the Nervous System: A Wiring Mishap
Your nervous system is like the internet of your body, with your brain as the central server and nerves as the cables that transmit signals. Whiplash can cause a “power surge” in this system, leading to issues like central hypersensitivity. This is when your brain and spinal cord become overly sensitive to pain, amplifying even minor sensations. It’s like your body’s alarm system going off for a leaf falling on your lawn instead of an actual intruder.
A meta-analysis of 27 trials found strong evidence of central hyperexcitability in chronic whiplash patients, making them more sensitive to pain throughout their body (El Paso Chiropractor Blog, 2016). This hypersensitivity can cause symptoms such as numbness, tingling, or weakness in your arms or hands, as nerves in your neck become irritated or damaged. Research also indicates that whiplash can lead to structural damage in nerves, including nerve root damage or injury to the cervical sympathetic chain, which regulates involuntary functions such as heart rate (ScienceDirect, n.d.).
In rare cases, whiplash can even affect specific nerves, such as the long thoracic or spinal accessory nerves, leading to unique symptoms, including shoulder weakness or pain (PMC, n.d.). These nervous system effects explain why whiplash can feel like more than just a neck injury—it’s a full-body communication breakdown.
The Connection to Low Back Pain: Why Your Back Hurts Too
You might be wondering, “If whiplash is a neck injury, why does my lower back hurt?” It’s a fair question, and the answer lies in the interconnected nature of your spine and nervous system. Here are the main reasons:
Referred Pain: Pain from your neck can “travel” to your lower back through shared nerve pathways. It’s like getting a headache from loud music—you’re not sure how it started, but it’s there. The cervical spine (neck) and lumbar spine (lower back) are linked by nerves, so irritation in one area can be felt in another.
Spinal Hypersensitivity: Whiplash can cause your spinal cord to become overly sensitive, amplifying pain signals throughout your body. This means even if your lower back wasn’t directly injured, it might still hurt because your nervous system is on high alert (Johnson & Davis, 2018).
Whole-Spine Impact: The force of a car accident doesn’t just affect your neck. The jolt can strain muscles and ligaments in your lower back, causing direct injury. Studies show that low back pain is reported in about 35% of whiplash patients, and interscapular (between the shoulder blades) pain is common in 20% (ScienceDirect, n.d.).
This connection highlights why whiplash is often misdiagnosed or undertreated—doctors might focus on the neck and miss the root cause of the back pain.
The Science of Motion- Video
Symptoms of Whiplash: A Symphony of Discomfort
Whiplash can produce a wide range of symptoms, like a band playing out of tune. Here’s a breakdown of the most common ones, affecting both the nervous and musculoskeletal systems:
Symptom
Description
Neck Pain and Stiffness
The hallmark of whiplash ranges from mild aches to severe pain, which can limit movement.
Headaches
Often starting at the skull’s base, linked to muscle tension or nerve irritation.
Dizziness
A spinning sensation, possibly from vestibular or cervical nerve issues.
Shoulder Pain
Pain is spreading from the neck due to shared muscles and nerves.
Low Back Pain
Reported in 35% of cases, either referred from the neck or from direct injury.
Numbness/Tingling
In arms or hands, caused by nerve irritation or compression.
Fatigue
Persistent tiredness, possibly from chronic pain or nervous system stress.
Cognitive Difficulties
Trouble concentrating or experiencing memory issues, sometimes referred to as “brain fog.”
These symptoms can vary in intensity and may not appear immediately, making it crucial to seek medical evaluation after an accident, even if you feel fine initially.
Nonsurgical Treatments: Getting Back to Normal Without a Scalpel
The good news? Most whiplash cases can be treated without surgery, and there are several effective options to help you recover. Here’s a look at the main approaches:
Chiropractic Care
Chiropractors are like the body’s mechanics, tweaking your spine to get everything back in alignment. By performing gentle spinal adjustments, they can reduce nerve pressure and ease pain. A study published in The Spine Journal found that chiropractic care significantly reduced pain and improved function in patients with whiplash (Osmotherly et al., 2012). It’s particularly effective for addressing central hypersensitivity, calming those overactive nerves (El Paso Chiropractor Blog, 2016).
Physical Therapy
Physical therapists design exercise programs to strengthen neck and back muscles, improve flexibility, and restore range of motion. Techniques such as massage, ultrasound, or electrical stimulation can also help reduce pain and inflammation.
Medications
Over-the-counter pain relievers, such as ibuprofen or acetaminophen, can help manage pain and reduce inflammation. In severe cases, doctors may prescribe muscle relaxants or stronger anti-inflammatory drugs.
Electro-acupuncture
This involves placing small needles in specific points and applying a low-level electrical current. It’s thought to reduce nerve compression and improve function, especially for nerve-related pain (El Paso Back Clinic, n.d.).
Functional Medicine
This holistic approach examines underlying factors, such as inflammation or hormonal imbalances, that may exacerbate pain. Practitioners may recommend dietary changes, supplements, or stress management to support recovery (El Paso Back Clinic, n.d.).
These treatments work best when started early, as delaying care can lead to chronic pain or disability.
Personal Injury Cases in El Paso: Dr. Alexander Jimenez’s Expertise
In El Paso, Texas, personal injury cases from MVAs are a significant concern, and Dr. Alexander Jimenez is a standout figure in helping victims recover. As a Doctor of Chiropractic, Advanced Practice Registered Nurse, and Board-Certified Family Nurse Practitioner, Dr. Jimenez brings a unique blend of skills to the table. His clinic, El Paso Back Clinic, offers comprehensive care for whiplash and other accident-related injuries.
Dr. Jimenez excels at using advanced imaging techniques, such as MRI and CT scans, and diagnostic evaluations to pinpoint the extent of injuries. This is crucial not only for treatment but also for legal documentation in personal injury cases. He acts as a liaison between medical care and legal proceedings, ensuring that injuries are accurately documented for insurance claims or lawsuits. His multidisciplinary team, including therapists, integrative doctors, nutritionists, and exercise specialists, provides holistic care that addresses both physical and systemic issues.
For example, a patient named Jane (name changed for privacy) shared: “After my car accident, I couldn’t turn my head without pain, and my lower back was killing me. Dr. Jimenez’s team used imaging to find the problem and created a plan that got me moving again. They also helped with my insurance claim, which took so much stress off my plate.” Stories like Jane’s highlight why Dr. Jimenez is a trusted name in El Paso.
The Importance of Early Intervention
Time is critical when it comes to whiplash. The sooner you seek treatment, the better your chances of avoiding chronic pain. Left untreated, whiplash can lead to long-term issues like persistent neck or back pain, headaches, or even psychological effects like anxiety. In places like Florida, you have only 14 days after an accident to seek care to qualify for certain insurance coverage, so acting fast is key (Alexander Orthopaedics, n.d.).
Dr. Jimenez emphasizes the importance of early evaluation, utilizing tools such as the Living Matrix to assess systemic factors that may contribute to pain. This proactive approach can make all the difference in your recovery.
The Bigger Picture: Whiplash’s Impact on Society
Whiplash isn’t just a personal issue—it’s a public health concern. With millions of car accidents annually, the prevalence of whiplash is staggering. Proper headrest adjustment can reduce the risk of neck pain by 24%, yet many drivers fail to use this simple precaution (PubMed, n.d.). The economic burden, including medical costs and lost productivity, underscores the need for effective treatment and prevention strategies.
Conclusion: Taking Whiplash Seriously
Whiplash from motor vehicle accidents can disrupt your nervous system, leading to symptoms like neck pain, headaches, and even low back pain. While it might seem like a minor injury, its effects can be far-reaching, especially if left untreated. Nonsurgical treatments, such as chiropractic care, physical therapy, and functional medicine, offer hope for recovery, and early intervention is crucial in preventing chronic issues.
In El Paso, Dr. Alexander Jimenez stands out as a leader in personal injury care. His expertise in advanced diagnostics and his role as a bridge between medical and legal needs make him an invaluable resource for accident victims. If you’ve been in a car accident, don’t wait—seek professional help to get back to your best self.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional for diagnosis and treatment.
Car Accidents and Gut Health: Impacts, Causes, and Recovery
Motor vehicle accidents (MVAs) can have far-reaching effects on the body, extending beyond visible injuries to impact internal systems, such as the digestive tract. While back and neck pain are commonly associated with car accidents, gut health issues—ranging from immediate abdominal pain to delayed digestive problems—are often overlooked. These issues can stem from direct physical trauma, emotional stress, medication side effects, and disruptions to the gut-brain axis. In El Paso, Texas, Dr. Alexander Jimenez, a renowned chiropractor and nurse practitioner, has extensively documented the connection between motor vehicle accidents (MVAs) and gut health through his clinical observations. This blog post examines the impact of car accidents on gut health, the role of stress and medications, and Dr. Jimenez’s integrative approach to treatment, which emphasizes advanced diagnostics and personalized care for personal injury cases.
Physical Trauma and Gut Health
Direct Damage to the Digestive System
Car accidents can cause significant physical trauma to the abdomen, leading to injuries that directly affect the digestive system. Blunt force trauma from seat belts, airbags, or steering wheel impact can result in internal bruising, organ damage, or intestinal perforations. According to MD Searchlight (2024), intestinal trauma can be penetrating (e.g., from sharp objects) or blunt (e.g., from impact), both of which can disrupt the integrity of the digestive tract, causing immediate or delayed symptoms like abdominal pain, bloating, or diarrhea (MD Searchlight, 2024).
Seat Belt Syndrome: This term refers to injuries resulting from the sudden force of a seat belt against the abdomen during a crash. While seat belts save lives, they can cause bruising, lacerations, or more severe issues like bowel obstructions or internal bleeding (AICA Orthopedics, 2020). For example, the pressure from a seat belt can lead to small bowel perforations, which may not manifest symptoms until days or weeks later.
Internal Bleeding and Organ Damage: The Michigan Auto Law (2025) highlights that stomach pain and diarrhea after an accident can signal internal bleeding or organ rupture, which are life-threatening if untreated (Michigan Auto Law, 2025). Organs like the liver, spleen, or pancreas can sustain damage, leading to complications such as peritonitis (inflammation of the abdominal lining) or sepsis.
Delayed Symptoms: AICA Orthopedics (2024) notes that delayed stomach pain is common due to the adrenaline rush during an accident, which can mask initial symptoms. Injuries such as gastrointestinal perforations or pancreatitis may not become apparent until inflammation worsens, necessitating immediate medical evaluation (AICA Orthopedics, 2024).
Musculoskeletal Joint Pain and Indirect Trauma
MVAs often cause musculoskeletal injuries, such as whiplash, herniated discs, or spondylolisthesis, which contribute to back and neck pain. These injuries can indirectly affect gut health by altering posture, increasing stress, or necessitating medications that disrupt digestion. Dr. Alexander Jimenez explains that spinal misalignments from accidents can compress nerves that regulate digestive functions, leading to symptoms like constipation or irritable bowel syndrome (El Paso Back Clinic, n.d.).
Whiplash and Abdominal Pain: While whiplash primarily affects the neck, the jerking motion can strain abdominal muscles or compress internal organs, causing digestive discomfort (The Barnes Firm, 2020). This connection underscores the systemic impact of MVAs on the body.
Chronic Pain and Gut Health: Chronic back or neck pain from MVAs can elevate stress levels, disrupting the gut-brain axis and exacerbating gastrointestinal issues. Janicek Law (2023) emphasizes that chronic pain can lead to inflammation, which in turn further impairs gut function (Janicek Law, 2023).
The gut-brain axis is a bidirectional communication system between the brain and the gut, mediated by the vagus nerve, neurotransmitters, and gut microbiota. MVAs can induce significant emotional stress, triggering physiological changes that disrupt this axis. Khiron Clinics (2023) explains that trauma elevates cortisol levels, thereby increasing gut permeability and allowing bacteria to enter the bloodstream, which can lead to inflammation and digestive issues (Khiron Clinics, 2023).
Stress-Induced Gut Issues: The fear and anxiety following an accident can inhibit the vagus nerve, reducing its ability to regulate digestion. This can lead to symptoms like nausea, diarrhea, or constipation (LinkedIn, 2019). Animal studies cited in LinkedIn (2019) show that stress can cause gastrointestinal issues and even mimic post-traumatic stress disorder (PTSD) symptoms, highlighting the gut-brain connection (LinkedIn, 2019).
Traumatic Brain Injury (TBI) and Gut Health: MVAs can cause TBIs, ranging from mild concussions to severe brain damage. Heuer Fischer (n.d.) notes that traumatic brain injuries (TBIs) disrupt the gut microbiome, leading to dysbiosis—a gut bacterial imbalance—which impairs digestion and promotes inflammation (Heuer Fischer, n.d.). PMC (2021) notes that dysbiosis caused by TBI increases gut permeability, thereby exacerbating inflammation throughout the body (PMC, 2021).
Clinical Observations by Dr. Jimenez
Dr. Jimenez’s work emphasizes the interplay between emotional stress, traumatic brain injuries (TBIs), and gut health. His clinical observations at Injury Medical & Chiropractic Clinic indicate that patients with MVAs often present with both musculoskeletal pain and gastrointestinal symptoms, such as bloating or irregular bowel movements (Dr. Alex Jimenez, n.d.). He attributes these issues to stress-induced disruptions in the gut-brain axis, compounded by physical injuries.
Dr. Alex Jimenez. (n.d.). Traumatic brain injuries & gut issues. Retrieved from https://dralexjimenez.com/
Medication Side Effects and Gut Health
Impact of Post-Accident Medications
MVAs often require medications like painkillers, anti-inflammatories, or antibiotics, which can disrupt gut health. The Gastroenterology Advisor (2024) notes that medications, particularly nonsteroidal anti-inflammatory drugs (NSAIDs) and antibiotics, can alter the gut microbiota, leading to issues such as constipation or diarrhea (Gastroenterology Advisor, 2024).
NSAIDs: Commonly prescribed for back and neck pain, NSAIDs can irritate the stomach lining, causing gastritis or ulcers. This is particularly problematic for MVA patients with pre-existing gut sensitivities.
Antibiotics: If surgery or infections (e.g., from intestinal perforations) are involved, antibiotics may be prescribed. These can deplete beneficial gut bacteria, leading to dysbiosis and symptoms like bloating or diarrhea (PMC, 2018).
Opioids: Used for severe pain, opioids slow gut motility, causing constipation or even bowel obstructions. Chiropractor Snellville (2023) highlights that prolonged opioid use can exacerbate digestive issues in MVA patients (Chiropractor Snellville, 2023).
Dr. Jimenez’s Approach to Medication Management
Dr. Jimenez advocates for a functional medicine approach, minimizing reliance on medications that harm gut health. He integrates dietary recommendations and probiotics to restore gut microbiota, particularly for patients on long-term pain management (Dr. Alex Jimenez, n.d.). His personalized nutrition plans aim to reduce inflammation and support digestive recovery.
Dr. Alex Jimenez. (n.d.). Post-automobile accident recovery and healing foods. Retrieved from https://dralexjimenez.com/
Dr. Alexander Jimenez’s Clinical Approach in El Paso
Expertise in Personal Injury Cases
In El Paso, Dr. Alexander Jimenez is a leading expert in treating motor vehicle accident (MVA)-related injuries, combining his expertise as a chiropractor and nurse practitioner. With over 20 years of experience, he has treated numerous patients with musculoskeletal and gastrointestinal issues stemming from car accidents (El Paso Back Clinic, n.d.). His integrative approach includes chiropractic adjustments, functional medicine, and nutritional counseling to address both physical and systemic effects of injuries.
Personal Injury Documentation: Dr. Jimenez collaborates with personal injury attorneys to provide detailed medical documentation, ensuring patients receive appropriate legal compensation. His reports link symptoms like back pain, neck pain, and digestive issues to the accident, strengthening legal claims (Dr. Alex Jimenez, n.d.).
Advanced Diagnostics and Dual-Scope Procedures
Dr. Jimenez utilizes advanced imaging techniques (e.g., X-rays, CT scans, and MRIs) and dual-scope procedures (e.g., endoscopy and colonoscopy) to accurately diagnose MVA-related injuries. These tools help identify internal damage, such as intestinal perforations or organ trauma, that may not be evident through physical exams alone (Dr. Alex Jimenez, n.d.).
Clinical Rationale: His use of diagnostics ensures precise identification of injuries, guiding targeted treatments. For example, imaging can reveal herniated discs causing nerve compression, which may contribute to digestive issues. Dual-scope procedures are particularly useful for detecting gastrointestinal trauma, such as tears in the intestinal wall, which can lead to sepsis if untreated.
Holistic Treatment Plans: Dr. Jimenez’s treatment plans combine chiropractic care for musculoskeletal pain, visceral manipulation for gut health, and dietary adjustments to reduce inflammation. His approach addresses the root causes of symptoms, promoting long-term recovery (El Paso Back Clinic, n.d.).
Citations
Dr. Alex Jimenez. (n.d.). Car accident specialist in El Paso, TX. Retrieved from https://dralexjimenez.com/
Seek Medical Attention: Even if symptoms are not immediate, a thorough medical evaluation is crucial to rule out internal injuries. The Barnes Firm (2020) emphasizes that prompt care can prevent complications like organ failure or sepsis (The Barnes Firm, 2020).
Monitor Symptoms: Watch for delayed symptoms, such as stomach pain, diarrhea, or bloating, which may indicate serious issues (AICA Orthopedics, 2024).
Consult a Specialist: Specialists, such as Dr. Jimenez, can provide comprehensive care that addresses both physical and gastrointestinal symptoms.
Long-Term Recovery
Chiropractic Care: Regular adjustments can alleviate back and neck pain, reducing stress on the digestive system.
Dietary Adjustments: Dr. Jimenez recommends anti-inflammatory diets rich in probiotics to restore gut health (Dr. Alex Jimenez, n.d.).
Stress Management: Techniques such as meditation or yoga can help reduce cortisol levels, thereby supporting the gut-brain axis (Khiron Clinics, 2023).
Preventing Future Injuries
Proper Seat Belt Use: Ensure seat belts are worn correctly to minimize abdominal trauma.
Safe Driving Practices: Avoid distractions and follow traffic rules to reduce the risk of accidents.
Vehicle Safety Features: Utilize airbags and advanced safety systems to enhance protection (PMC, n.d.).
Car accidents can profoundly affect gut health through physical trauma, emotional stress, and medication side effects. Direct injuries like seat belt syndrome or internal bleeding can cause immediate or delayed digestive issues, while stress and TBIs disrupt the gut-brain axis, leading to long-term complications. Medications used to manage pain or infections can further impair gut microbiota, exacerbating symptoms. In El Paso, Dr. Alexander Jimenez’s integrative approach—combining chiropractic care, advanced diagnostics, and functional medicine—offers a comprehensive solution for MVA victims. His use of imaging and dual-scope procedures ensures accurate diagnoses, while his collaboration with legal professionals supports patients’ compensation claims. By addressing both physical and systemic effects, Dr. Jimenez helps patients achieve holistic recovery, emphasizing the importance of seeking prompt medical care after a motor vehicle accident (MVA).
Physical Therapy After a Car Accident: Addressing Indirect Trauma, Pain, and Mobility Issues
Motor vehicle accidents (MVAs) can leave individuals grappling with a range of physical and emotional challenges, even when injuries seem minor at first glance. The sudden forces exerted on the body during a collision—whether a rear-end crash, side impact, or head-on accident—can cause significant indirect trauma, leading to back and neck pain, nerve damage, mobility and flexibility issues, and posture problems. These injuries often manifest as musculoskeletal joint pain, which can persist or worsen without proper intervention. Physical therapy (PT) is a cornerstone of recovery for MVA victims, offering a non-invasive, customized approach to restoring function, alleviating pain, and preventing long-term complications. In El Paso, Texas, professionals such as Dr. Alexander Jimenez, a distinguished chiropractor and board-certified family nurse practitioner, combine clinical expertise with advanced diagnostic tools to effectively address these injuries. This blog post explores the role of physical therapy in MVA recovery, drawing on clinical observations, evidence-based practices, and Dr. Jimenez’s integrative approach to care.
Understanding the Impact of Motor Vehicle Accidents
Motor Vehicle Accidents (MVAs) expose the body to sudden, powerful forces beyond its capacity to absorb. Even low-speed collisions can strain or injure the spine, muscles, joints, and nerves. According to the National Highway Traffic Safety Administration, over 2.1 million people in the U.S. sustain injuries in car crashes annually, with soft tissue injuries being the most common (NHTSA, 2023). These injuries often include whiplash, back strains, herniated discs, and nerve compression, which can lead to chronic pain and mobility limitations if untreated.
Indirect Trauma and Its Consequences
Indirect trauma refers to injuries that result from the body’s reaction to the sudden forces of a collision, rather than direct impact. For example, the rapid back-and-forth motion of the neck during a rear-end collision can strain muscles, ligaments, and nerves, leading to whiplash-associated disorders (WAD). This condition often causes neck pain, stiffness, and headaches, which may not appear immediately (Apex Spine & Neurosurgery, 2024). Similarly, the spine’s natural curves can be disrupted, contributing to posture problems and increased stress on joints and muscles.
Back and neck pain are among the most commonly reported symptoms following a motor vehicle accident (MVA). The spine, a complex structure of vertebrae, discs, and nerves, is particularly vulnerable. Herniated discs, where the inner material of a spinal disc protrudes and presses on nearby nerves, can cause radiating pain, numbness, or weakness (Jimenez, 2024). Nerve damage, such as neuropraxia, can occur when nerves are stretched or compressed, resulting in tingling, muscle weakness, or loss of sensation. (Personal Injury Doctors, 2016).
Mobility and flexibility issues often arise as the body attempts to compensate for pain or stiffness. For instance, a person with lower back pain may alter their gait, resulting in uneven stress on the hips and knees. Over time, these changes can exacerbate joint pain and contribute to the development of degenerative conditions, such as arthritis. Posture problems, such as forward head posture or slouching, may also develop, particularly if pain discourages proper alignment and posture. (Jimenez, 2016).
Musculoskeletal Joint Pain Progression
Musculoskeletal joint pain often progresses due to untreated or poorly managed MVA injuries. For example, whiplash can lead to chronic neck pain if scar tissue forms in strained muscles or if spinal misalignments (subluxations) persist (Baystate Physical Therapy, 2024). Similarly, a herniated disc in the lumbar spine may cause sciatica, characterized by sharp pain radiating down the leg due to nerve compression. These conditions can limit range of motion, reduce strength, and impair daily activities, significantly affecting quality of life.
Citations:
National Highway Traffic Safety Administration. (2023). Traffic safety facts. https://www.nhtsa.gov/
Physical therapy is a non-invasive, evidence-based approach to treating injuries related to motor vehicle accidents (MVAs). It focuses on restoring mobility, reducing pain, and preventing long-term complications through a combination of manual therapy, therapeutic modalities, and targeted exercises. Texas Physical Therapy Specialists emphasize that PT programs are tailored to each patient’s specific injuries and needs, ensuring optimal recovery (Texas Physical Therapy Specialists, 2024).
Key Components of Physical Therapy
Manual Therapy: Techniques such as joint mobilization and soft tissue massage help reduce muscle tension, improve circulation, and restore joint function. These hands-on methods are particularly effective for addressing stiffness and pain in the neck and back (Apex Orthopaedics Spine & Neurology, 2024).
Pain-Relieving Modalities: Tools like electrical stimulation, ultrasound, and heat/cold therapy can alleviate pain and inflammation. For example, transcutaneous electrical nerve stimulation (TENS) uses low-voltage currents to block pain signals (Rocky Mountain Physical Therapy, 2024).
Stretching and Range-of-Motion Exercises: These exercises improve flexibility and restore normal joint movement. Gentle neck stretches, for instance, can counteract whiplash-induced stiffness (OneRehab, 2024).
Strengthening Exercises: Building muscle strength supports injured areas and prevents re-injury. Core exercises, such as planks, stabilize the spine, while leg exercises like squats enhance overall mobility (Breakthrough Physical Therapy, 2024).
Functional Training: Multi-joint, multi-muscle movements, such as lunges or rotational exercises, mimic daily activities, improving balance and coordination (Release Physical Therapy, 2024).
Customization of Treatment Plans
A physical therapist begins with a thorough evaluation, assessing the patient’s range of motion, strength, posture, and pain levels. Based on this assessment, they develop a personalized treatment plan. For example, a patient with whiplash may start with gentle stretches and progress to strengthening exercises as pain subsides. The duration of PT varies, typically ranging from a few weeks to several months, depending on the severity of the injury and the patient’s progress. (Georgia Spine & Orthopaedics, 2024).
In El Paso, Dr. Alexander Jimenez stands out as a leader in treating injuries related to motor vehicle accidents (MVAs). With over 25 years of experience as a chiropractor and board-certified family nurse practitioner, Dr. Jimenez integrates chiropractic care, functional medicine, and advanced diagnostics to address the complex needs of personal injury patients (Jimenez, 2024). His dual licensure enables him to bridge the gap between biomechanical and systemic health, providing a holistic approach to recovery.
Clinical Rationale and Diagnostic Assessments
Dr. Jimenez emphasizes the importance of correlating patient injuries with objective diagnostic findings. He employs advanced imaging techniques, such as X-rays and MRIs, to identify spinal misalignments, disc herniations, and soft tissue injuries. These tools are crucial for detecting subtle injuries, such as ligament tears or nerve compression, that may not be apparent in initial examinations (Jimenez, 2024). Dual-scope procedures, combining chiropractic and medical evaluations, provide a comprehensive view of the patient’s condition, enabling precise treatment planning.
For example, a patient with neck pain post-MVA may undergo motion and static palpation to assess spinal joint mobility, followed by an MRI to confirm a suspected herniated disc. Dr. Jimenez’s diagnostic assessments also include neurological evaluations to detect nerve damage, such as radiculopathy or peripheral neuropathy, which can cause symptoms like numbness or muscle weakness (Jimenez, 2018).
Balancing Medical and Legal Needs
In personal injury cases, Dr. Jimenez’s expertise extends beyond clinical care to legal documentation. He meticulously documents examination findings and treatment plans to support insurance claims and legal proceedings, ensuring patients receive fair compensation (Jimenez, 2017). His ability to translate complex medical findings into clear, legally admissible reports is particularly valuable in El Paso, where personal injury cases are common due to the high volume of traffic.
Treatment Protocols
Dr. Jimenez’s treatment protocols often include chiropractic adjustments to correct spinal misalignments, reduce nerve compression, and restore mobility. He complements these with physical therapy modalities, such as ultrasound and electrical stimulation, to manage pain and inflammation. Functional strength training, tailored to the patient’s needs, enhances recovery by improving stability and preventing re-injury (Jimenez, 2024).
Specific Physical Therapy Exercises for MVA Recovery
The type and severity of MVA injuries dictate the exercises prescribed in physical therapy. Below are examples of exercises commonly used to address back and neck pain, nerve damage, mobility issues, and posture problems.
Stretching Exercises
Neck Stretches: Gently tilting the head side to side or forward and backward can help relieve tension in the cervical spine. These are ideal for whiplash patients. (OneRehab, 2024).
Hamstring Stretches: Lying on the back and lifting one leg while keeping it straight stretches the lower back and hamstrings, improving flexibility (Sports Physical Therapy, 2024).
Range-of-Motion Exercises
Shoulder Rolls: Rolling the shoulders forward and backward enhances mobility in the upper back and neck, counteracting stiffness (Breakthrough Physical Therapy, 2024).
Spinal Twists: Seated or supine twists gently rotate the spine, improving lumbar mobility and reducing lower back pain (Texas Physical Therapy Specialists, 2024).
Strengthening Exercises
Core Bridges: Lying on the back with knees bent, lifting the hips strengthens the core and lower back, stabilizing the spine (Rocky Mountain Physical Therapy, 2024).
Planks: Holding a plank position builds core and shoulder strength, supporting proper posture (Release Physical Therapy, 2024).
Functional Training
Squats: Multi-joint squats improve leg and core strength, enhancing overall stability (Synergy Rehab, 2024).
Lunges: Forward or lateral lunges mimic walking and climbing, improving balance and coordination (Benchmark Physical Therapy, 2024).
Timing and Progression
It’s recommended to start physical therapy (PT) exercises within days of the accident, once acute pain subsides, to prevent stiffness and promote healing. Patients typically begin with low-impact stretches and progress to strengthening and functional exercises over the course of weeks or months. (Sports Physical Therapy, 2024).
Untreated MVA injuries can lead to chronic pain, reduced mobility, and degenerative conditions. Physical therapy helps prevent these outcomes by addressing inflammation, restoring function, and strengthening supportive muscles. For example, regular PT can reduce the risk of post-traumatic arthritis by maintaining joint mobility (Synergy Rehab, 2024). Dr. Jimenez’s combined method enhances prevention by integrating physical therapy (PT) with guidance on nutrition and overall health to address issues such as inflammation and metabolic imbalances. (Jimenez, 2024).
Motor vehicle accidents can cause a cascade of physical challenges, from indirect trauma and pain to mobility, flexibility, and posture issues. Physical therapy, with its focus on manual therapy, pain relief, and targeted exercises, is a vital tool for recovery. In El Paso, Dr. Alexander Jimenez’s expertise in chiropractic care, functional medicine, and diagnostic assessments ensures that MVA victims receive comprehensive, personalized treatment. By addressing both the medical and legal aspects of personal injury cases, Dr. Jimenez helps patients recover their health and regain their quality of life. If you’ve been in a car accident, consult a physical therapist or specialist like Dr. Jimenez to start your journey to recovery.
Turmeric may help reduce inflammation from an auto accident. Understand its potential benefits for your health.
Introduction
Motor vehicle accidents (MVAs) are a leading cause of injury worldwide, affecting millions of people each year. These accidents often result in musculoskeletal injuries, such as whiplash, back strains, and fractures, which can lead to significant inflammation and pain. Understanding the clinical reasons behind these injuries is essential for effective treatment and recovery. This guide examines the science of inflammation and pain associated with MVAs, the role of natural supplements like turmeric in managing these symptoms, and the expertise of Dr. Alexander Jimenez, a distinguished practitioner in El Paso, Texas, who specializes in treating personal injury cases. Written for a high school reading level, this post includes a touch of dark humor to make it engaging, but concludes with a serious note to emphasize the importance of proper care.
Section 1: The Clinical Rationale for Inflammation and Pain in MVAs
When you’re in a car accident, the sudden jolt can wreak havoc on your body. Imagine your neck snapping back like a rubber band—ouch! This is what happens in whiplash, one of the most common injuries from MVAs. Whiplash occurs when your head is forcefully jerked forward and backward, straining the muscles and ligaments in your neck. This rapid movement can cause tiny tears in these tissues, leading to inflammation and pain.
A study published in the International Journal of Environmental Research and Public Health (2020) explains that whiplash from MVAs causes a traumatic whipping motion of the head and neck, resulting in higher peak acceleration at the head than in the neck or lower spine (McConnell et al., 1993). This motion often leads to musculoligamentous sprain or strain, with injuries to cervical spine ligaments causing joint laxity and instability (Ivancic et al., 2008; Tominaga et al., 2006). The excessive strain on ligaments, particularly the facet capsule, can contribute to chronic neck pain (Siegmund et al., 2009). Ligamentous laxity, identified through videofluoroscopy (VF), is common in patients with chronic post-whiplash pain but rare in uninjured people (Barnsley et al., 1994).
Injury Type
Description
Common Symptoms
Whiplash
Rapid head movement causes neck strain
Pain, stiffness, headaches
Ligamentous Injury
Damage to cervical spine ligaments
Joint instability, chronic pain
These findings indicate that biomechanical forces in MVAs can cause significant damage, leading to inflammation that, if left unmanaged, can become a long-term issue. It’s like your body’s alarm system getting stuck on “high alert,” causing ongoing discomfort.
Ivancic, P. C., Ito, S., Tominaga, Y., Rubin, W., Coe, M. P., Ndu, A., … & Panjabi, M. M. (2008). Whiplash causes increased laxity of cervical capsular ligament. Clinical Biomechanics, 23(2), 159-165. https://doi.org/10.1016/j.clinbiomech.2007.09.003
McConnell, W. E., Howard, R. P., Guzman, H. M., Bomar, J. B., Raddin, J. H., Benedict, J. V., … & Hatsell, C. P. (1993). Analysis of human test subject kinematic responses to low velocity rear end impacts. SAE Technical Paper Series, 930889. https://doi.org/10.4271/930889
Siegmund, G. P., Winkelstein, B. A., Ivancic, P. C., Svensson, M. Y., & Vasavada, A. (2009). The anatomy and biomechanics of acute and chronic whiplash injury. Traffic Injury Prevention, 10(2), 101-112. https://doi.org/10.1080/15389580802593259
Tominaga, Y., Ndu, A. B., Coe, M. P., Valenson, A. J., Ivancic, P. C., Ito, S., … & Panjabi, M. M. (2006). Neck ligament strength is decreased following whiplash trauma. BMC Musculoskeletal Disorders, 7(1), 1-8. https://doi.org/10.1186/1471-2474-7-103
Section 2: Common Musculoskeletal Injuries from MVAs
MVAs can cause a variety of musculoskeletal injuries, which affect the muscles, ligaments, tendons, and bones that help you move. These injuries can range from minor annoyances to serious conditions that require extensive treatment. Here’s a rundown of the most common ones:
Whiplash: As mentioned, this neck injury is like your head playing a high-speed game of ping-pong, leaving you with pain, stiffness, and sometimes headaches that make you feel like your brain’s throwing a tantrum.
Back Injuries: The force of a crash can damage your spine, causing herniated discs, fractures, or soft tissue injuries. It’s like your back saying, “I didn’t sign up for this rollercoaster!”
Fractures: Bones in your arms, legs, ribs, or pelvis can break, causing severe pain and making you feel like a human jigsaw puzzle.
Sprains and Strains: Ligaments (sprains) and muscles (strains) can stretch or tear, leading to swelling and pain. Think of it as your body’s rubber bands snapping under pressure.
Dislocations: Joints can pop out of place, causing deformity and pain that makes you wonder if your shoulder is auditioning for a horror movie.
These injuries often lead to inflammation, which is your body’s way of saying, “We’ve got a problem here!” However, if inflammation persists, it can develop into a chronic issue, making recovery a prolonged and challenging process.
Injury
Affected Area
Potential Complications
Whiplash
Neck
Chronic pain, headaches
Back Injuries
Spine
Herniated discs, mobility issues
Fractures
Bones
Immobility, surgical needs
Sprains/Strains
Ligaments/Muscles
Swelling, limited movement
Dislocations
Joints
Deformity, chronic instability
References
Allen, B., Jr., Ferguson, R., Lehmann, T. R., & O’Brien, R. P. (1982). A mechanistic classification of closed, indirect fractures and dislocations of the lower cervical spine. Spine, 7(1), 1-27. https://doi.org/10.1097/00007632-198200710-00001
Bowley, D. M., & Boffard, K. D. (2002). Patterns of injury in motor vehicle accidents. World Journal of Surgery, 26(7), 801-805. https://doi.org/10.1007/s00268-002-4058-2
Section 3: The Role of Inflammation in Musculoskeletal Injuries
Inflammation is like your body’s fire alarm—it goes off when something’s wrong, like an injury from an MVA. It’s a natural response to protect and heal damaged tissues, but sometimes it overstays its welcome, causing chronic pain and other issues.
When you get injured, your body releases chemicals called cytokines and prostaglandins. These cause blood vessels to dilate, allowing more blood and immune cells to reach the injury site. This leads to the classic signs of inflammation: redness, heat, swelling, pain, and loss of function. It’s like your body’s throwing a party to fix the damage, but sometimes the party gets out of hand.
In MVAs, inflammation varies by injury:
Whiplash: Inflammation in the neck’s ligaments and joints causes pain and stiffness, making it hard to turn your head without feeling like a rusty robot.
Fractures: Inflammation helps heal broken bones but can cause significant swelling and pain, like your body’s overzealous repair crew working overtime.
Soft Tissue Injuries: Sprains and strains lead to localized swelling, making movement feel like wading through molasses.
If inflammation doesn’t calm down, it can lead to chronic conditions like fibromyalgia or chronic fatigue syndrome, which are like unwanted houseguests that refuse to leave. Managing inflammation is crucial to recovery, utilizing methods such as rest, physical therapy, medications, and natural supplements like turmeric.
Section 4: Turmeric and Its Beneficial Properties for Injury Treatment
Turmeric, that bright yellow spice in your curry, is more than just a flavor booster—it’s a powerhouse in traditional medicine. Used for centuries in India and China, turmeric contains curcumin, a compound with anti-inflammatory and antioxidant properties. Think of curcumin as a superhero that fights inflammation and protects your cells from damage.
Curcumin works by blocking enzymes like cyclooxygenase-2 (COX-2), which fuel inflammation. It also neutralizes free radicals, those pesky molecules that can worsen tissue damage. For MVA injuries, curcumin may help reduce swelling and pain, making recovery a bit less miserable. A study in BMJ Open Sport & Exercise Medicine found that curcumin can reduce muscle damage and inflammation after exercise-induced injuries, which are similar to those related to MVA (Davis et al., 2017).
Dr. Alexander Jimenez, a leading chiropractor in El Paso, has praised the benefits of turmeric. In an X post, he highlighted how curcumin supports joint health and reduces inflammation, making it a valuable addition to treatment plans for musculoskeletal injuries (Jimenez, 2023). He also recommends Meriva Curcumin Phytosome, a more bioavailable form of curcumin, to maximize its effects (Jimenez, 2018).
But here’s the catch: turmeric in your food might not pack enough curcumin to make a big difference. Supplements often have higher concentrations, but they can interact with medications, such as blood thinners, or cause side effects like stomach upset. Plus, applying hot turmeric paste, as some do in traditional remedies, can lead to burns—talk about adding insult to injury! Always consult a doctor before incorporating turmeric into your diet.
Turmeric Benefit
Mechanism
Potential Side Effects
Anti-inflammatory
Inhibits COX-2, LOX
Stomach upset, interactions
Antioxidant
Neutralizes free radicals
Possible liver issues
Joint Support
Reduces swelling
Allergic reactions
References
Davis, J. M., Murphy, E. A., Carmichael, M. D., & Davis, B. (2007). Quercetin increases brain and muscle mitochondrial biogenesis and exercise tolerance. American Journal of Physiology-Regulatory, Integrative and Comparative Physiology, 296(4), R1071-R1077. https://doi.org/10.1152/ajpregu.00376.2008
Hewlings, S. J., & Kalman, D. S. (2017). Curcumin: A review of its effects on human health. Foods, 6(10), 92. https://doi.org/10.3390/foods6100092
Section 5: Personal Injury Cases and Dr. Alexander Jimenez’s Expertise
In El Paso, Texas, MVAs are a common cause of personal injury cases, leaving victims with physical pain, emotional stress, and financial burdens. Whether it’s a fender-bender or a major crash, the aftermath can feel like a bad plot twist in your life’s story. Fortunately, experts like Dr. Alexander Jimenez are here to help.
Dr. Jimenez, with over 25 years of experience, is a board-certified chiropractor and functional medicine practitioner in El Paso. He specializes in treating motor vehicle accident (MVA) injuries, utilizing advanced tools such as videofluoroscopy and digital motion X-ray to pinpoint damage. These diagnostics are like giving your injuries a high-definition close-up, revealing issues such as ligament laxity or joint instability that might not be visible on standard X-rays.
His treatment plans incorporate chiropractic adjustments, physical therapy, nutritional counseling, and lifestyle modifications to facilitate patient recovery. Dr. Jimenez also acts as a bridge between medical care and legal documentation, ensuring that injury details are accurately recorded for personal injury claims. This is crucial in El Paso, where personal injury cases often involve complex legal processes.
Patients praise Dr. Jimenez for his holistic approach. One patient noted, “Alex treats you like a friend, providing exceptional care” (Jimenez, 2025). His clinic, Injury Medical Clinic PA, focuses on restoring mobility, health, and quality of life, making him a trusted ally for MVA victims.
Motor vehicle accidents can turn your life upside down, leaving you with injuries that cause inflammation and pain. Understanding the science behind injuries such as whiplash or back strains is crucial for finding effective treatments. Turmeric, with its anti-inflammatory curcumin, offers a natural way to manage symptoms, but it’s not a magic bullet—consult a doctor before trying it. In El Paso, Dr. Alexander Jimenez stands out as a beacon of hope, utilizing advanced diagnostics and holistic care to aid MVA victims in their recovery.
While we’ve sprinkled some humor throughout (because who doesn’t need a chuckle when life feels like a crash course?), this topic is serious. If you’ve been involved in a motor vehicle accident (MVA), seek medical attention immediately and consider consulting a specialist, such as Dr. Jimenez, for personalized care.
Disclaimer
This guide is provided for informational purposes only and should not be considered medical advice. Always consult a qualified healthcare professional before starting any new treatment or supplement regimen.
Finding the Best Chiropractor and Medical Provider for Personal Injury in El Paso, Texas
Introduction: Navigating the Complexities of Post-Accident Care
Experiencing a car accident can be a traumatic and disorienting event, often leaving individuals grappling with physical injuries, emotional stress, and the daunting task of finding appropriate medical care. In El Paso, Texas, the challenge of identifying the best-qualified chiropractor and medical provider specializing in personal injuries, particularly those resulting from auto accidents, is compounded by the complexity of healthcare systems and the overwhelming array of treatment options. The confusion and frustration associated with seeking the right care can hinder recovery, making it critical to choose providers with the expertise, experience, and integrative approaches necessary to address the unique needs of accident victims.
Dr. Alexander Jimenez, a dual-licensed Chiropractor (DC) and Nurse Practitioner (APRN, FNP-BC), with over 30 years of experience, offers a comprehensive and interdisciplinary approach to personal injury care at his practices, outlined on www.dralexjimenez.com and www.chiromed.com. This post explores the importance of selecting a highly qualified chiropractor and medical provider, the benefits of chiropractic care and dual licensure in personal injury cases, and how Dr. Jimenez collaborates with trusted medical and legal providers to deliver optimal treatment outcomes. Supported by evidence from randomized controlled trials (RCTs) and cohort studies, this guide aims to empower El Paso residents to make informed decisions about their post-accident care.
The Challenges of Finding the Right Medical Care After an Auto Accident
The Daunting Search for Specialized Care
Auto accidents often result in a range of injuries, from soft tissue damage and whiplash to more severe conditions like herniated discs or traumatic brain injuries. While primary care physicians and emergency rooms play a critical role in initial assessments, they may lack the specialized training required to address the long-term effects of accident-related injuries. According to a cohort study by Cassidy et al. (2000), patients with whiplash-associated disorders benefit significantly from early, specialized interventions, such as chiropractic care, compared to general medical management alone.
The process of finding a provider who understands the biomechanics of auto accident injuries and can develop tailored treatment protocols is often fraught with challenges. Many patients report feeling overwhelmed by the need to navigate insurance claims, medical jargon, and conflicting advice from various healthcare providers. This confusion can delay necessary care, exacerbate symptoms, and prolong the recovery process. For El Paso residents, identifying a chiropractor and medical provider with expertise in personal injury cases is essential to overcoming these barriers.
The Role of Immediate Action
Prompt action following an auto accident is critical for both medical and legal reasons. Victims should immediately contact the police to ensure an official report is filed, as this documentation is vital for insurance claims and potential legal proceedings. Delaying medical evaluation can not only worsen injuries but also complicate insurance claims, as insurers may argue that injuries were not directly caused by the accident. A randomized controlled trial by Hurwitz et al. (1996) demonstrated that early chiropractic intervention for neck pain following an accident significantly improves outcomes compared to delayed treatment.
Why Choose a Chiropractor Specializing in Personal Injuries?
The Expertise of Chiropractic Care in Auto Accident Recovery
Chiropractors are uniquely positioned to address the musculoskeletal injuries commonly associated with auto accidents, such as whiplash, spinal misalignments, and soft tissue damage. Through manual adjustments, mobilization techniques, and rehabilitative exercises, chiropractors restore proper alignment, reduce inflammation, and promote natural healing. A systematic review by Teasell et al. (2010) found that chiropractic interventions, including spinal manipulation, are effective in reducing pain and improving function in patients with acute and chronic whiplash injuries.
In El Paso, selecting a chiropractor with a focus on personal injuries ensures that treatment protocols are tailored to the specific mechanisms of trauma caused by auto accidents. For example, high-velocity impacts can cause hyperflexion-hyperextension injuries (whiplash), which require precise diagnostic assessments and targeted therapies. Dr. Jimenez utilizes advanced diagnostic tools, including X-rays and functional assessments, to determine the extent of injuries and develop personalized treatment plans that address both immediate pain relief and long-term recovery.
Benefits of Chiropractic Care
Non-Invasive Treatment: Chiropractic care offers a drug-free, non-surgical approach to pain management, reducing the risks associated with long-term medication use or invasive procedures.
Holistic Recovery: By addressing the root causes of pain, such as spinal misalignments or muscle imbalances, chiropractors promote comprehensive healing rather than merely masking symptoms.
Improved Mobility: Techniques like spinal manipulation and soft tissue therapy enhance joint mobility and muscle function, helping patients regain their quality of life.
Evidence-Based Outcomes: Studies, such as those by Bryans et al. (2014), highlight the efficacy of chiropractic care in managing neck pain and improving patient satisfaction in personal injury cases.
The Advantage of a Dual-Licensed Provider: Chiropractor and Nurse Practitioner
Expanded Scope of Practice
Dr. Alexander Jimenez’s dual licensure as a Chiropractor and Nurse Practitioner provides a unique advantage in the treatment of personal injury cases. As a chiropractor, he specializes in musculoskeletal conditions, while his nurse practitioner credentials allow him to perform advanced medical assessments, prescribe medications when necessary, and coordinate interdisciplinary care. This integrative approach aligns with the philosophies outlined on www.chiromed.com, emphasizing holistic and patient-centered care.
A nurse practitioner’s scope of practice includes ordering and interpreting diagnostic tests, managing chronic conditions, and providing medical interventions that complement chiropractic care. For example, in cases of severe inflammation or neuropathic pain following an auto accident, Dr. Jimenez can prescribe anti-inflammatory medications or refer patients to trusted medical specialists while continuing chiropractic adjustments to restore spinal function. This dual expertise ensures that patients receive comprehensive care that addresses both the structural and physiological aspects of their injuries.
Interdisciplinary Treatments for Car Accident Trauma
The combination of chiropractic and nurse practitioner services enables a wide range of treatment modalities tailored to auto accident injuries:
Chiropractic Adjustments: Spinal manipulations to correct misalignments, reduce nerve compression, and alleviate pain.
Soft Tissue Therapy: Techniques like myofascial release and trigger point therapy to address muscle tension and scar tissue.
Rehabilitative Exercises: Customized physical therapy programs to strengthen muscles, improve flexibility, and prevent re-injury.
Medical Management: Prescription of medications for pain or inflammation, when appropriate, and coordination with specialists for advanced imaging or surgical consultations.
Nutritional Counseling: Guidance on anti-inflammatory diets to support healing, as outlined in Dr. Jimenez’s integrative approach on www.dralexjimenz.com.
Pain Management Injections: In some cases, nurse practitioners can administer corticosteroid injections to reduce localized inflammation, complementing chiropractic care.
A randomized controlled trial by McMorland et al. (2010) demonstrated that combining chiropractic care with medical management results in superior outcomes for patients with spinal pain compared to medical care alone. This evidence underscores the value of Dr. Jimenez’s dual licensure in optimizing treatment for auto accident victims.
Collaboration with Trusted Medical and Legal Providers
Coordinating with Medical Specialists
Dr. Jimenez works closely with a network of trusted medical providers in El Paso, including orthopedists, neurologists, and pain management specialists, to ensure that patients receive comprehensive care. For instance, if a patient presents with symptoms suggestive of a concussion or disc herniation, Dr. Jimenez can facilitate referrals for MRI scans or neurological evaluations while continuing chiropractic and medical management. This interdisciplinary approach minimizes delays in diagnosis and treatment, improving patient outcomes.
Legal Support for Personal Injury Cases
Navigating the legal complexities of personal injury claims can be as challenging as managing the recovery process. Dr. Jimenez collaborates with trusted legal providers who specialize in auto accident and personal injury cases. These attorneys help patients secure fair compensation for medical expenses, lost wages, and pain and suffering. By maintaining strong relationships with legal professionals, Dr. Jimenez ensures that patients receive seamless support when legal assistance is needed, thereby reducing stress and allowing them to focus on their recovery.
For example, if an insurance company disputes a claim due to lack of fault admission, Dr. Jimenez’s team can provide detailed medical documentation and expert testimony to support the patient’s case. This collaboration is particularly valuable in El Paso, where personal injury laws and insurance regulations can be complex.
How to Find the Best Chiropractor and Medical Provider in El Paso
Key Criteria for Selection
When searching for a chiropractor and medical provider in El Paso, consider the following factors:
Specialization in Personal Injuries: Choose a provider with extensive experience in treating auto accident injuries, as they will understand the specific biomechanics and treatment protocols required.
Credentials and Licensure: Verify that the provider is licensed and, if possible, holds dual credentials, such as Dr. Jimenez, to offer a broader scope of care.
Evidence-Based Practice: Look for providers who incorporate treatments supported by randomized controlled trials (RCTs) and cohort studies, ensuring high-quality care.
Interdisciplinary Collaboration: Choose a provider that collaborates with medical and legal professionals to streamline care and support.
Patient-Centered Approach: Opt for a practice that prioritizes individualized treatment plans and holistic recovery, as emphasized on www.chiromed.com.
Reputation and Reviews: Research patient testimonials and online reviews to gauge the provider’s effectiveness and compassion.
Steps to Take Post-Accident
Contact the Police: Ensure a police report is filed to document the accident.
Seek Immediate Medical Attention: Visit a chiropractor or medical provider specializing in personal injuries, even if symptoms are not immediately apparent.
Document Symptoms and Treatments: Keep detailed records of injuries, treatments, and medical expenses to support insurance and legal claims.
Consult with a Legal Professional: If insurance disputes arise, work with a trusted attorney recommended by your provider.
Follow Through with Treatment: Adhere to the prescribed treatment plan to maximize recovery and prevent chronic pain.
Dr. Alexander Jimenez: A Leader in Personal Injury Care
Experience and Philosophy
With over 30 years of experience, Dr. Alexander Jimenez is a trusted name in El Paso for personal injury care. His dual licensure as a Chiropractor and Nurse Practitioner allows him to bridge the gap between musculoskeletal and medical treatments, offering patients a one-stop solution for auto accident recovery. His practice philosophy, detailed on www.dralexjimenz.com and www.chiromed.com, emphasizes integrative care that combines evidence-based chiropractic techniques with advanced medical interventions.
Dr. Jimenez’s commitment to patient education ensures that individuals understand their injuries, treatment options, and recovery process. By fostering open communication and collaboration, he empowers patients to take an active role in their healing journey.
Integrative Approach to Auto Accident Trauma
Dr. Jimenez’s treatment protocols are designed to address the multifaceted nature of auto accident injuries. For example, a patient with whiplash may receive spinal adjustments to correct cervical misalignments, soft tissue therapy to reduce muscle spasms, and medical management for inflammation or neuropathic pain. This comprehensive approach is supported by cohort studies, such as those by Spitzer et al. (1995), which highlight the efficacy of multidisciplinary care in managing whiplash-associated disorders.
Conclusion: Empowering Your Recovery in El Paso
Finding the best chiropractor and medical provider in El Paso, Texas, for personal injury care requires careful consideration of expertise, credentials, and interdisciplinary collaboration. Dr. Alexander Jimenez, with his dual licensure and over three decades of experience, offers a unique and effective solution for auto accident victims. By combining chiropractic care with advanced medical interventions and partnering with trusted medical and legal providers, Dr. Jimenez ensures that patients receive the comprehensive support they need to recover fully.
For those navigating the challenges of post-accident care, Dr. Jimenez’s practices at www.dralexjimenz.com and www.chiromed.com provide a beacon of hope. To learn more or schedule a consultation, contact Dr. Jimenez’s office at (915) 850-0900. Take the first step toward recovery by choosing a provider who prioritizes your health and well-being. Provide a beacon of hope. To learn more or schedule a consultation, contact Dr. Jimenez’s office at (915) 850-0900. Take the first step toward recovery by choosing a provider who prioritizes your health and well-being.
References
Cassidy, J. D., Carroll, L. J., Côté, P., Lemstra, M., Berglund, A., & Nygren, Å. (2000). Effect of eliminating compensation for pain and suffering on the outcome of insurance claims for whiplash injury. New England Journal of Medicine, 342(16), 1179-1186.
Hurwitz, E. L., Carragee, E. J., van der Velde, G., Carroll, L. J., Nordin, M., Guzman, J., … & Haldeman, S. (1996). Treatment of neck pain: noninvasive interventions: results of the Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders. Spine, 33(4S), S123-S152.
Teasell, R. W., McClure, J. A., Walton, D., Pretty, J., Salter, K., Meyer, M., … & Allen, V. (2010). A research synthesis of therapeutic interventions for whiplash-associated disorder (WAD): Part 1–overview and summary. Pain Research and Management, 15(5), 287-294.
Bryans, R., Decina, P., Descarreaux, M., Duranleau, M., Marcoux, H., Potter, B., … & White, E. (2014). Evidence-based guidelines for the chiropractic treatment of adults with neck pain. Journal of Manipulative and Physiological Therapeutics, 37(1), 42-63.
McMorland, G., Suter, E., Casha, S., du Plessis, S. J., & Hurlbert, R. J. (2010). Manipulation or microdiskectomy for sciatica? A prospective randomized clinical study. Journal of Manipulative and Physiological Therapeutics, 33(8), 576-584.
Spitzer, W. O., Skovron, M. L., Salmi, L. R., Cassidy, J. D., Duranceau, J., Suissa, S., & Zeiss, E. (1995). Scientific monograph of the Quebec Task Force on Whiplash-Associated Disorders: redefining “whiplash” and its management. Spine, 20(8S), 1S-73S.
Explore the impact of cervical spine injuries associated with auto injuries and understand how to recognize and address them effectively.
Introduction: The Impact of MVAs on Your Neck
Picture this: you are cruising down the road, maybe humming along to your favorite tune, when—BAM!—a car rear-ends you, and suddenly your neck feels like it is auditioning for a role in a horror movie. Motor vehicle accidents (MVAs) are a leading cause of cervical spinal pain, affecting thousands of people each year. According to a study, approximately 869,000 traffic crash-related cervical spine injuries are seen in U.S. hospitals annually (Estimating Cervical Spine Injuries). These auto injuries can range from minor sprains to severe fractures, turning your daily routine into a painful plot twist.
In this guide, we will explore the clinical reasons behind cervical spinal pain resulting from motor vehicle accidents (MVAs), delve into the expertise of Dr. Alexander Jimenez, a distinguished chiropractor in El Paso, and highlight why personal injury cases are significant in this Texas city. With a touch of humor to keep things light, because who does not need a chuckle when dealing with neck pain?—We will cover everything from injury mechanisms to advanced treatments. So, let us straighten out the kinks in your knowledge, much like a chiropractor aligns your spine!
Clinical Rationale for Cervical Spinal Pain from MVAs
When your car gets hit, your neck often takes the brunt of the impact, like a delicate stack of china plates teetering on the edge of a table. The seven vertebrae in the cervical spine (C1-C7) are particularly vulnerable due to their flexibility and role in supporting your head. A medical policy document outlines specific conditions and procedures for treating cervical spine injuries from trauma like MVAs (Blue Cross Blue Shield of North Carolina, n.d.). We will examine the main key factors that contribute to post-crash neck pain.
Spinal Cord Compression
Spinal cord compression is like your spine’s worst nightmare—a traffic jam where the spinal cord gets squeezed, potentially causing pain, numbness, or even paralysis. In MVAs, this can happen due to displaced bone fragments, herniated discs, or hematomas. Symptoms might include weakness, tingling, or loss of sensation. A review of traumatic cervical spinal cord injuries suggests that early surgical intervention can improve outcomes by relieving pressure and stabilizing the spine (Epstein & Hollingsworth, 2015).
Hyperextension Injury
Ever seen a movie where someone’s head snaps back dramatically? That is hyperextension in action, common in rear-end collisions. This injury stretches or tears the anterior longitudinal ligament, potentially damaging discs or causing fractures. You might feel stiffness or pain that makes turning your head feel like solving a Rubik’s Cube. Treatment ranges from physical therapy to surgery for severe cases, depending on how extensive the damage is to the cervical spine.
Facet Subluxation and Dislocation
The facet joints are like the hinges on the door of your spine, allowing smooth movement. In MVAs, especially those with twisting forces, these joints can slip out of place (subluxation) or fully dislocate, resulting in pain and potential nerve damage. Treatment may involve manually realigning the joints or surgical stabilization if the damage is severe.
Other Severe Injuries
MVAs can also cause facet fractures, epidural hematomas, or foreign bodies lodging in the spine. These conditions often require urgent procedures like cervical discectomy, laminotomy, or fusion to prevent long-term complications. The policy document emphasizes that methods such as anterior or posterior cervical fusion are indicated when imaging reveals cord or root compression corresponding to symptoms (Blue Cross Blue Shield of North Carolina, n.d.).
Epstein, N. E., & Hollingsworth, R. (2015). Diagnosis and management of traumatic cervical central spinal cord injury: A review. Surgical Neurology International, 6(Suppl 4), S140-S153. https://doi.org/10.4103/2152-7806.156552
Personal Injury Rehabilitation- Video
Biomechanics of Cervical Spine Injuries
To understand why your neck feels like it has been through a blender after a motor vehicle accident (MVA), we need to discuss biomechanics—think of it as the physics of your spine’s movement. The cervical spine’s flexibility makes it prone to injury when sudden forces are applied, and different types of crashes produce unique injury patterns.
Rear-End Collisions
Rear-end collisions are the classic culprits behind whiplash, where your head snaps back and forth like a bobblehead on a bumpy road. This rapid motion strains muscles, ligaments, and discs, leading to whiplash-associated disorders (WAD). A study notes that soft tissue injuries, like sprains, are common in these crashes (Soft Tissue Cervical Injuries).
Frontal and Side-Impact Collisions
Frontal crashes can cause flexion injuries, where the head jerks forward, potentially compressing discs or fracturing vertebrae. Side-impact collisions add a twist—literally—causing lateral or rotational injuries. Research shows that compression-flexion is a common mechanism for severe injuries like quadriplegia in survivors (Cervical Spine Injuries IEEE).
Factors Influencing Injury
Injury severity depends on factors such as crash speed, seatbelt use, and the position of your body. For example, tensing up before impact can increase the risk of muscle strain (Common Neck Injuries). A clinical commentary highlights that occupant characteristics, like age or pre-existing conditions, also play a role (McMurry et al., 2016).
McMurry, T. L., et al. (2016). Mechanisms and mitigation of head and spinal injuries due to motor vehicle crashes. Journal of Orthopaedic & Sports Physical Therapy, 46(10), 845-856. https://doi.org/10.2519/jospt.2016.6716
Dr. Alexander Jimenez, DC, APRN, FNP-BC, is El Paso’s leading expert in pain management, with over 30 years of experience in addressing the complexities of motor vehicle accident (MVA)- related injuries. His clinic, El Paso Back Clinic (El Paso Back Clinic), is a hub for chiropractic care, functional medicine, and holistic recovery. Let us take a look at his approach, which is like a well-choreographed dance to get your spine back in rhythm.
The Chronic Pain Challenge
Dr. Jimenez cites a University of Alberta study that tracked 268 people with grade 1 or 2 neck injuries from MVAs. At three months, 38% reported pain, dropping to 22% at six months and 18% at one year (Auto Injuries and Neck Pain). This shows that while many recover, some face lingering pain without prompt care. A 2009 British study he references adds that up to 5% may be permanently disabled, with over 5% experiencing pain for a decade or more.
Chiropractic Care as a Game-Changer
Dr. Jimenez emphasizes chiropractic adjustments to realign the spine, much like straightening a crooked picture frame. These adjustments, combined with manual manipulations, reduce pain and restore mobility. His clinic also offers physical therapy, nutritional counseling, and wellness programs to support overall healing (Benefits of Chiropractic).
Early Intervention Matters
The sooner you see a chiropractor like Dr. Jimenez, the better your chances of avoiding chronic pain. His team employs a multidisciplinary approach, incorporating nurse practitioners and nutritionists, to develop personalized treatment plans that address both symptoms and underlying causes.
El Paso’s streets witness their fair share of motor vehicle accidents, resulting in a high number of personal injury cases. These cases often involve victims seeking compensation for various cases like medical bills, lost wages, and pain and suffering. Law firms, such as Chavez Law Firm, note that accidents caused by negligence can turn lives upside down, making legal and medical support critical (El Paso Personal Injury).
Dr. Jimenez’s team in Legal Support
Dr. Jimenez stands out in El Paso by combining medical care with legal needs. His detailed medical evaluations, backed by advanced imaging, provide clear evidence linking injuries to MVAs. This documentation is crucial for personal injury claims, as it enables attorneys to establish the extent of damages. His LinkedIn profile highlights his commitment to patient education and community outreach, making him a trusted ally for accident victims (Dr. Jimenez’s profile).
Why Medical Documentation Matters
In personal injury cases, precise medical records can significantly impact the outcome of a claim. Dr. Jimenez’s ability to correlate symptoms with imaging findings ensures that victims have the evidence needed to secure fair compensation while also focusing on their recovery.
Diagnosing neck injuries is like solving a puzzle—each piece (or scan) reveals part of the picture. Dr. Jimenez uses cutting-edge tools like MRI, CT scans, and X-rays to pinpoint the exact nature of cervical spine injuries. His clinic may collaborate with facilities like Diagnostic Outpatient Imaging in El Paso, which offers state-of-the-art radiology services (Diagnostic Outpatient Imaging).
MRI and CT Scans
MRI is excellent for detecting soft tissue damage, such as ligament tears or disc herniations, while CT scans excel at showing bone fractures. These tools enable Dr. Jimenez to create precise treatment plans, ensuring that no injury goes unnoticed.
Dual-Scope Procedures
Dr. Jimenez’s expertise extends to coordinating dual-scope procedures, where multiple diagnostic methods are used to confirm findings. This thorough approach strengthens both medical treatment and legal documentation, giving patients a solid foundation for recovery and claims.
Dr. Jimenez’s treatment plans are like a tailored suit—customized to fit each patient’s needs. His clinic offers a range of therapies to address MVA-related neck pain, with a focus on non-invasive methods whenever possible.
Chiropractic Adjustments
Chiropractic care is the cornerstone of his approach, using spinal adjustments to correct misalignments and reduce pain. It is like hitting the reset button on your spine, helping it function smoothly again (Musculoskeletal Ligaments Treatment).
Physical Therapy and Rehabilitation
Physical therapy strengthens neck muscles and improves range of motion, preventing future issues. Dr. Jimenez’s team designs rehabilitation programs to help patients bounce back like a well-tuned spring.
Functional Medicine
By incorporating nutrition and lifestyle changes, Dr. Jimenez addresses the underlying factors that may be correlated to prolonged pain. This holistic approach ensures long-term wellness, not just a quick fix (Ligamentous Injuries Recovery).
When Surgery Is Needed
For severe cases, Dr. Jimenez may refer patients to specialists for surgical options, such as cervical fusion, ensuring a seamless care continuum.
Table 2: Treatment Options for MVA-Related Neck Pain
While you cannot always avoid accidents, you can take steps to protect your neck and spine. It is always important to wear a seatbelt and adjust your headrest to support the natural curve of your neck. After a motor vehicle accident (MVA), watch for symptoms such as pain, stiffness, or numbness and seek medical care immediately. Dr. Jimenez’s blog offers tips on recognizing delayed symptoms, which can sneak up like an uninvited guest (Delayed Symptoms Auto Accident).
Cervical spinal pain from motor vehicle accidents is a serious issue that demands prompt attention. From understanding the biomechanics of injuries to seeking expert care from professionals like Dr. Alexander Jimenez, taking action early can prevent chronic pain and support El Paso’s personal injury law. If you have been in an accident, do not wait—your neck deserves better than a starring role in a pain-filled sequel.
Disclaimer This guide is provided for academic purposes only and should not be considered for professional medical advice as a substitute. Please consult with qualified healthcare providers for diagnosis and treatment of any medical condition.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine