As a business owner at El Paso, Texas, Louie Martinez depends upon his general health to have the ability to execute his daily physical activities. And thanks to Dr. Alex Jimenez, a chiropractor in El Paso, Texas, Louie has found pain relief for a variety of wellness issues.
Louie describes how Dr. Jimenez has revived his wellness. Louie Martinez is thankful for the chiropractic care Dr. Jimenez has provided for him, and he highly recommends him as the non-surgical choice for many different health issues, including back pain and sports injuries.
El Paso Back Clinic
We are blessed to present to you El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center, we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life filled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life.
I assure you, I will only accept the best for you�
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend us.
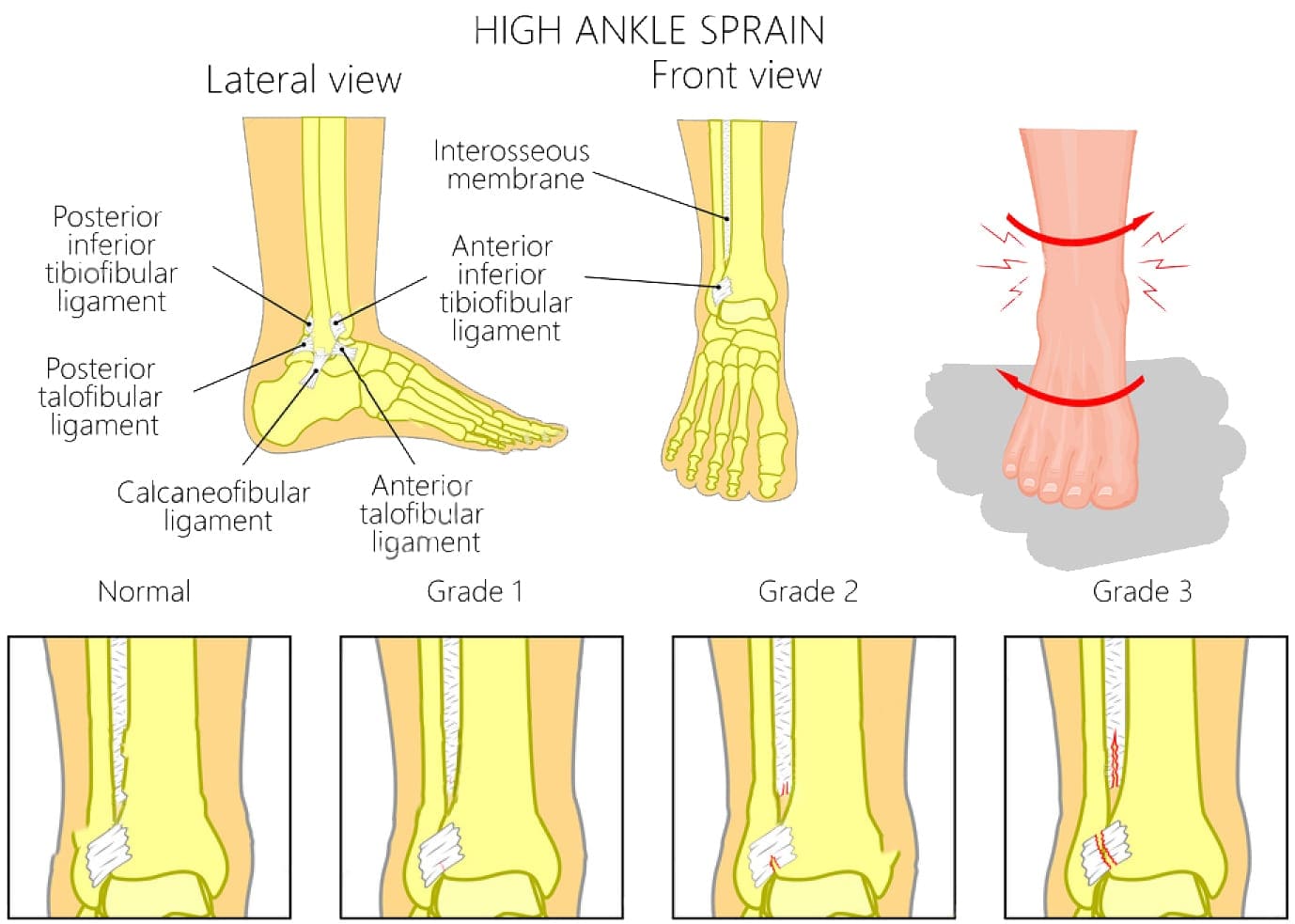
Hiking�with the family and you twist your ankle. It hurts, but you make it back without much problem. You notice you have some swelling and soreness, so you head home for some R.I.C.E. (rest, ice, compression, elevation).
You pass it off, saying, �Oh, it�s just a sprain.� But when your doctor checks you out the next day, he tells you that it is �strained.� Sprain vs. strain, what�s the difference?
While many people use the two terms interchangeably, they are not the same. There are some distinct differences although many of the symptoms are almost identical. In short, when a ligament is injured, it is called a sprain. When a muscle or tendon is injured, it is called a strain.
What Exactly are Sprains & Strains?
Ligaments are tough bands of tissue that connect two bones as they sit in a joint. For example, the tibia and fibula come together to fit in the ankle joint. Tendons join those two bones together to keep the ankle stable. A joint sprain occurs when these ligaments are torn or overstretched. The ankle is the most commonly sprained joint.
Tendons are cords of tissue made up of a dense network of fibers. They connect the muscle to the bone. A joint strain occurs when the tendons or muscles tear or overstretch. The lower back and hamstrings are the most common areas for muscle strain.
Both injuries are very similar, so it stands to reason that the symptoms of the injuries are also almost identical. This is why they are so commonly confused.
Symptoms of Sprains & Strains
The symptoms for each condition is very similar, but there are some differences.
Symptoms of Sprains include:
Pain around the area that is affected
Bruising in the affected area
Swelling in the immediate area but can expand to encompass more area
Limited range of motion
Decreased flexibility
Symptoms of Strains include:
Pain at the site of the joint that is affected
Muscle spasm
Swelling in the immediate area but can expand to encompass more area
Limited range of motion
Decreased flexibility
As you can see, the symptoms of sprains and strains are very close. The primary differences though are that bruising may occur with a sprain while a strain may elicit muscle spasms in the muscle that is affected.
What Causes Sprains and Strains?
Experiencing a sprain or strain every once in a while is not out of the ordinary. We put our bodies through a lot in a day. However, certain activities can make you more susceptible to movements that can lead to these injuries. They include:
Exercise or athletic activities, especially those that are high impact
Walking
Repetitive motion for a long period of time
Overexertion
Jogging or running
Slipping or falling
Standing or sitting in an unnatural or awkward position
Walking or running on unstable surfaces, like rocks or ice
Lifting objects that are too heavy
The most common areas for these injuries include:
Back
Ankle
Wrist
Knee
Thumb
How to Avoid Sprains and Strains
Sometimes injuries just happen and there�s nothing you can do about it. However, in most cases, you can take proactive steps to minimize your risks. These are some of the most common risk factors:
Being in poor physical condition
Using proper form when exercising
Failing to warm up before activities like exercising
Not using the right equipment for your workout or sporting activity.
Maintaining a hazardous environment at home, such as clutter on the floor or things you can trip over or slip on.
Fatigue or overly tired
Failure to avoid hazardous areas like floors that are wet and slippery or sidewalks that are iced over and slick.
If you have a sprain or strain and notice that the swelling has not subsided or if you still have pain after a week or so, you need to follow up with your doctor to make sure you don�t have a more severe injury.
*Sciatica Pain* Treatment Relief | El Paso, TX (2019)
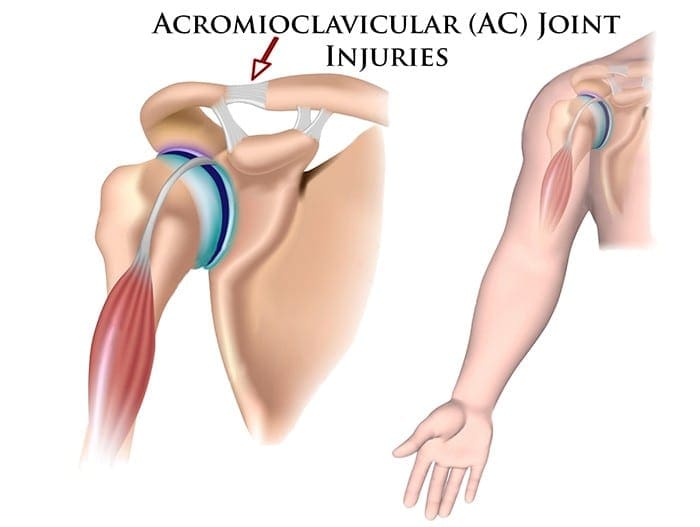
When a patient comes in with complaints of pain in the shoulder and restricted motion in the joint, one possible diagnosis may be acromicioclavicular (AC) joint injury. While it is often an injury that is common among athletes, it can happen to anyone. Fortunately, chiropractic is a very effective treatment. While most people think of chiropractors, the first thing that comes to mind is back pain. Yes, chiropractors do specialize in back/spine issues, but chiropractic care is used to treat a variety of conditions from joint pain to migraines, fitness, and diet.
What is an acromioclavicular joint injury?
There are two bones, the clavicle, and acromion, that make up the AC joint. Four ligaments hold the joint together. When those ligaments are strained to stress, it results in an AC joint injury, often causing at least some joint separation. AC injuries fall into one of two categories: overuse and traumatic.
Overuse injury occurs over a period of time and is caused by excessive stress on the joint that is repeated or consistent. This causes damage to the cartilage and can lead to AC joint arthritis.
Traumatic injury occurs when the damaged ligaments disrupt the joint called a shoulder separation. This is different from a shoulder dislocation which involves the actual ball and socket shoulder joint.
What causes acromioclavicular joint injury?
The cause of an AC joint injury depends on the type of injury.
Overuse AC joint injuries are caused by overuse and are commonly seen in people who perform tasks that involve lifting heavy weight (including military or bench presses) or that perform physical labor that involves often stretching their arms over their heads.
A fall often causes traumatic AC joint injuries. The person may fall and land on their shoulder or fall on their hand then they put it out to brace their fall. It is often seen in cyclists who are involved in crashes, football players when they are tackles or a laborer who falls from a high place, such as a ladder. These injuries are graded from mild to severe, depending on how much the separation there is in the joint.
What are the symptoms of acromioclavicular joint pain?
A patient with AC joint pain may experience the following symptoms:
A bump that sits above the shoulder and is easily visible
A catching sensation or popping sound when the shoulder moves
Pain and swelling in the shoulder
Loss of range of motion of the shoulder
Loss or decrease in shoulder strength
Tenderness and swelling over the AC joint
Pain when lying on the affected side
Discomfort and pain in the shoulder when performing activities that place stress on the AC joint, including:
Carrying heavy objects at the side
Reaching across the body
Lifting objects overhead
What are the treatments for acromioclavicular joint pain?
Mild cases of traumatic AC joint injuries are often treated with physical therapy and chiropractic. Ice, rest, and immobilization can also be used to manage the pain.
Overuse AC joint injuries can also be treated with immobilization and ice as well as physical therapy and chiropractic. More severe cases may require surgery. Doctors may prescribe muscle relaxants, pain medication, or NSAIDs to help manage the pain.
Is chiropractic for acromioclavicular joint pain effective?
Chiropractic has been proven to be very effective for AC joint pain. The chiropractor performs what is called an AC adjustment which involves manipulation of the shoulder.
While it can be a little uncomfortable for the patient, it is one of the best ways to quickly decrease the pain. After the procedure, the chiropractor may recommend icing the area to minimize or prevent swelling and pain. Regular chiropractic care can ensure continued mobility and continued decrease in pain.
The knee is the largest, complicated joint in the human body. The knee joint is exposed to many different wellness issues. Knee injuries related to sports are a common issue that can affect playing time. Dr. Jimenez helps many athletes recover from knee injuries along with a variety of other sports-related injuries. Individuals share their experience of knee injury rehabilitation and treatment Dr. Jimenez has provided them. As an added benefit it has enhanced their�sports performance. Chiropractic rehabilitation is an alternative treatment option focusing on spinal adjustments and manual manipulations to deal with many different accidents and/or conditions related to the musculoskeletal and nervous system. Patients say Dr. Jimenez is the non-surgical, chiropractic choice.
Non-Surgical Injury Rehabilitation
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life filled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life.
I assure you, I will only accept the best for you�
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend�us.
Most healthcare providers use x-rays as a diagnostic tool to treat a variety of patient complaints, including chiropractors. They can help doctors identify the source of a problem or if there is something more going on. X-rays can also help chiropractors determine the best course of action for treatment. To understand more, let’s take a closer look at what they are and how they’re used in most chiropractic offices.
What are x-rays?
An x-ray is a very vigorous form of electromagnetic radiation that is similar to radio waves, ultraviolet radiation, microwaves, or visible light that is used to view the internal composition of a person or thing. A beam is focused on a specific part of a person�s body, such as the back, it produces a digital image of the skeletal structure.
The beam passes easily through skin and other soft tissues�but is unable to pass through bone and teeth. Soft tissue that is denser, such as organs, ligaments, and muscles, will be visible�but will be captured in shades of gray. Areas like the bowel or lungs appear on the film as black.
The use of chiropractic x-rays
Chiropractic x-rays provide vital information that can affect how the chiropractor chooses to treat a patient. In some cases, chiropractic care or spinal manipulation may not be an appropriate course of action at that time, and the patient may be started on a different, gentler therapy.
Other times, it can show the chiropractor how to best proceed in treating the patient. In short, patients can receive better, more well-rounded care which can better facilitate their healing and pain management.
Identify a condition or symptom, such as a spinal tumor or lesion�that would provide a medical reason that a specific course of care should not be done.
Obtain important biomechanical information that can aid in guiding treatment.
To stay apprised and maintain a record of a patient�s degenerative process.
Aid in identifying anomalies in the spine and joints that can affect treatment.
Allows patients to understand their condition and treatment plan better, allowing them to take ownership of the process and be more involved in their therapy and healing.
What does a chiropractor look for on an x-ray film?
When a chiropractor takes an x-ray of a patient, they are looking for things in several particular areas. The first thing they check is to make sure that there are no dislocations, fractures, cancer, infections, tumors, or other potentially dangerous conditions.
They then look for disk height and other signs of disk degeneration, bone density, bone spurs, joint spaces, and alignment. This allows them to identify conditions like scoliosis and other conditions that may require specific forms of treatment.
Many chiropractors prefer that the patient is in a weight-bearing position when taking spinal x-rays. This differs from the majority of medical facilities which have the patient lie down.
The advantage of weight-bearing x-rays as a diagnostic tool�is that it allows for measuring, i.e., leg length deficiency, scoliosis, and the narrowing of joint space. It can also show that certain bones, such as the tibia and fibula, are separating which can be an indication of a torn tendon or problem with the joint. A non-weight bearing x-ray cannot provide the same perspective,�and vital clues to a patient�s condition may be missed.
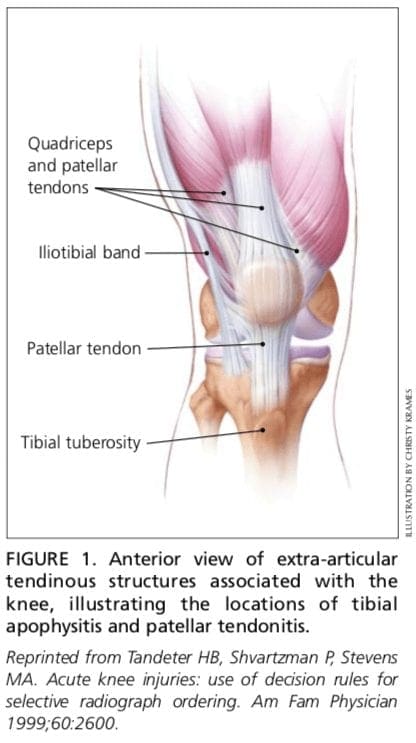
The knee is one of the most complex joints in the human body, consisting of the thigh bone, or femur, the shin bone, or tibia, and the kneecap, or patella, among other soft tissues. Tendons connect the bones to the muscles while ligaments connect the bones of the knee joint. Two wedge-shaped pieces of cartilage, known as the meniscus, provide stability to the knee joint. The purpose of the article below is to demonstrate as well as discuss the anatomy of the knee joint and its surrounding soft tissues.
Abstract
Context: Information regarding the structure, composition, and function of the knee menisci has been scattered across multiple sources and fields. This review contains a concise, detailed description of the knee menisci�including anatomy, etymology, phylogeny, ultrastructure and biochemistry, vascular anatomy and neuroanatomy, biomechanical function, maturation and aging, and imaging modalities.
Evidence Acquisition: A literature search was performed by a review of PubMed and OVID articles published from 1858 to 2011.
Results: This study highlights the structural, compositional, and functional characteristics of the menisci, which may be relevant to clinical presentations, diagnosis, and surgical repairs.
Conclusions: An understanding of the normal anatomy and biomechanics of the menisci is a necessary prerequisite to understanding the pathogenesis of disorders involving the knee.
Keywords:knee, meniscus, anatomy, function
Introduction
Once described as a functionless embryonic remnant,162 the menisci are now known to be vital for the normal function and long-term health of the knee joint.� The menisci increase stability for femorotibial articulation, distribute axial load, absorb shock, and provide lubrication and nutrition to the knee joint.4,91,152,153
Injuries to the menisci are recognized as a cause of significant musculoskeletal morbidity. The unique and complex structure of menisci makes treatment and repair challenging for the patient, surgeon, and physical therapist. Furthermore, long-term damage may lead to degenerative joint changes such as osteophyte formation, articular cartilage degeneration, joint space narrowing, and symptomatic osteoarthritis.36,45,92 Preservation of the menisci depends on maintaining their distinctive composition and organization.
Anatomy of Menisci
Meniscal Etymology
The word meniscus comes from the Greek word m?niskos, meaning �crescent,� diminutive of m?n?, meaning �moon.�
Meniscal Phylogeny and Comparative Anatomy
Hominids exhibit similar anatomic and functional characteristics, including a bicondylar distal femur, intra-articular cruciate ligaments, menisci, and asymmetrical collateral.40,66 These similar morphologic characteristics reflect a shared genetic lineage that can be traced back more than 300 million years.40,66,119
In the primate lineage leading to humans, hominids evolved to bipedal stance approximately 3 to 4 million years ago, and by 1.3 million years ago, the modern patellofemoral joint was established (with a longer lateral patellar facet and matching lateral femoral trochlea).164 Tardieu investigated the transition from occasional bipedalism to permanent bipedalism and observed that primates contain a medial and lateral fibrocartilaginous meniscus, with the medial meniscus being morphologically similar in all primates (crescent shaped with 2 tibial insertions).163 By contrast, the lateral meniscus was observed to be more variable in shape. Unique in Homo sapiens is the presence of 2 tibial insertions�1 anterior and 1 posterior�indicating a habitual practice of full extension movements of the knee joint during the stance and swing phases of bipedal walking.20,134,142,163,168
Embryology and Development
The characteristic shape of the lateral and medial menisci is attained between the 8th and 10th week of gestation.53,60 They arise from a condensation of the intermediate layer of mesenchymal tissue to form attachments to the surrounding joint capsule.31,87,110 The developing menisci are highly cellular and vascular, with the blood supply entering from the periphery and extending through the entire width of the menisci.31 As the fetus continues to develop, there is a gradual decrease in the cellularity of the menisci with a concomitant increase in the collagen content in a circumferential arrangement.30,31 Joint motion and the postnatal stress of weightbearing are important factors in determining the orientation of collagen fibers. By adulthood, only the peripheral 10% to 30% have a blood supply.12,31
Despite these histologic changes, the proportion of tibial plateau covered by the corresponding meniscus is relatively constant throughout fetal development, with the medial and lateral menisci covering approximately 60% and 80% of the surface areas, respectively.31
Gross Anatomy
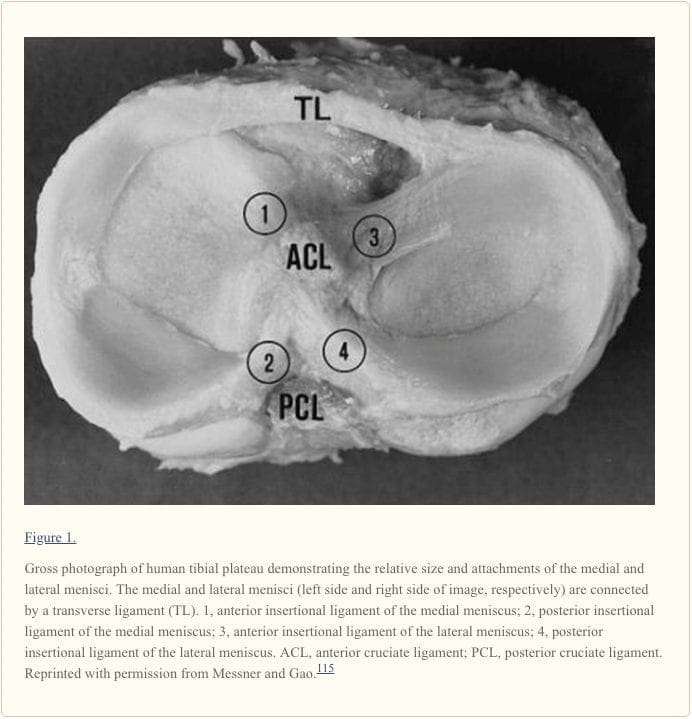
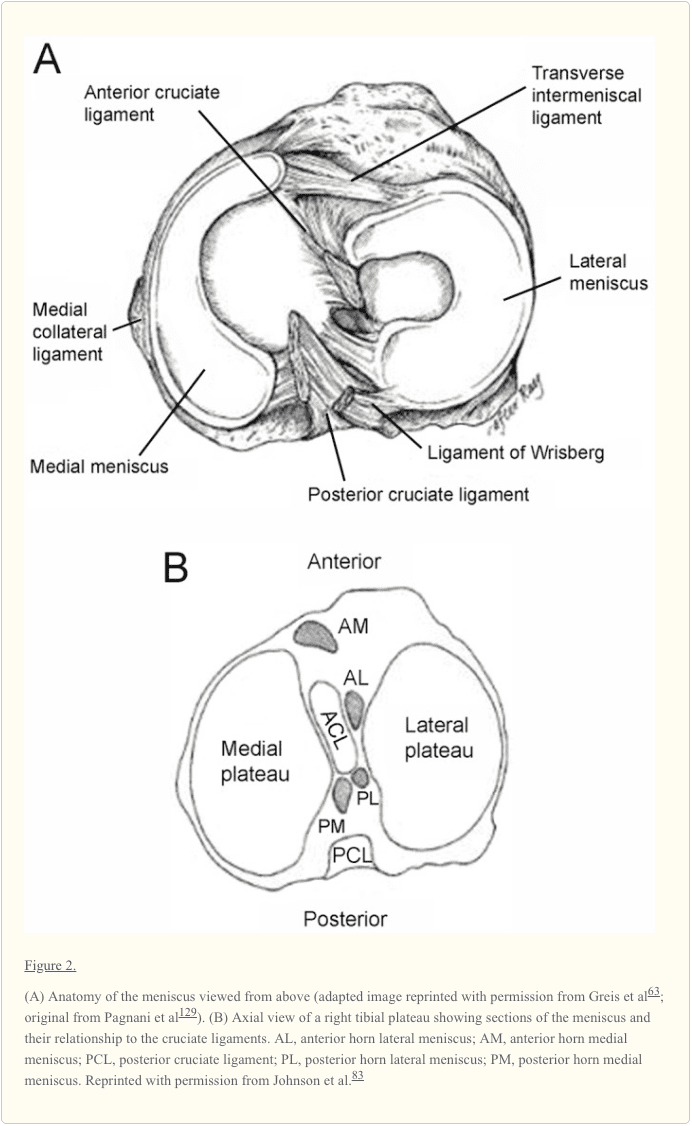
Gross examination of the knee menisci reveals a smooth, lubricated tissue (Figure 1). They are crescent-shaped wedges of fibrocartilage located on the medial and lateral aspects of the knee joint (Figure 2A). The peripheral, vascular border (also known as the red zone) of each meniscus is thick, convex, and attached to the joint capsule. The innermost border (also known as the white zone) tapers to a thin free edge. The superior surfaces of menisci are concave, enabling effective articulation with their respective convex femoral condyles. The inferior surfaces are flat to accommodate the tibial plateau (Figure 1).28,175
Medial meniscus. The semicircular medial meniscus measures approximately 35 mm in diameter (anterior to posterior) and is significantly broader posteriorly than it is anteriorly.175 The anterior horn is attached to the tibia plateau near the intercondylar fossa anterior to the anterior cruciate ligament (ACL). There is significant variability in the attachment location of the anterior horn of the medial meniscus. The posterior horn is attached to the posterior intercondylar fossa of the tibia between the lateral meniscus and the posterior cruciate ligament (PCL; Figures 1 and and2B).2B). Johnson et al reexamined the tibial insertion sites of the menisci and their topographic relationships to surrounding anatomic landmarks of the knee.82 They found that the anterior and posterior horn insertion sites of the medial meniscus were larger than those of the lateral meniscus. The area of the anterior horn insertion site of the medial meniscus was the largest overall, measuring 61.4 mm2, whereas the posterior horn of the lateral meniscus was the smallest, at 28.5 mm2.82
The tibial portion of the capsular attachment is the coronary ligament. At its midpoint, the medial meniscus is more firmly attached to the femur through a condensation in the joint capsule known as the deep medial collateral ligament.175 The transverse, or �intermeniscal,� ligament is a fibrous band of tissue that connects the anterior horn of the medial meniscus to the anterior horn of the lateral meniscus (Figures 1 and and2A2A).
Lateral meniscus. The lateral meniscus is almost circular, with an approximately uniform width from anterior to posterior (Figures 1 and and2A).2A). It occupies a larger portion (~80%) of the articular surface than the medial meniscus (~60%) and is more mobile.10,31,165 Both horns of the lateral meniscus are attached to the tibia. The insertion of the anterior horn of the lateral meniscus lies anterior to the intercondylar eminence and adjacent to the broad attachment site of the ACL (Figure 2B).9,83 The posterior horn of the lateral meniscus inserts posterior to the lateral tibial spine and just anterior to the insertion of the posterior horn of the medial meniscus (Figure 2B).83 The lateral meniscus is loosely attached to the capsular ligament; however, these fibers do not attach to the lateral collateral ligament. The posterior horn of the lateral meniscus attaches to the inner aspect of the medial femoral condyle via the anterior and posterior meniscofemoral ligaments of Humphrey and Wrisberg, respectively, which originate near the origin of the PCL (Figures 1 and and22).75
Meniscofemoral ligaments. The literature reports significant inconsistencies in the presence and size of meniscofemoral ligaments of the lateral meniscus. There may be none, 1, 2, or 4.? When present, these accessory ligaments transverse from the posterior horn of the lateral meniscus to the lateral aspect of the medial femoral condyle. They insert immediately adjacent to the femoral attachment of the PCL (Figures 1 and and22).
In a series of studies, Harner et al measured the cross-sectional area of the ligaments and found that the meniscofemoral ligament averaged 20% of the size of the PCL (range, 7%-35%).69,70 However, the size of the insertional area alone without knowledge of the insertional angle or collagen density does not indicate their relative strength.115 The function of these ligaments remains unknown; they may pull the posterior horn of the lateral meniscus in an anterior direction to increase the congruity of the meniscotibial fossa and the lateral femoral condyle.75
Ultrastructure and Biochemistry
Extracellular Matrix
The meniscus is a dense extracellular matrix (ECM) composed primarily of water (72%) and collagen (22%), interposed with cells.9,55,56,77 Proteoglycans, noncollagenous proteins, and glycoproteins account for the remaining dry weight.� Meniscal cells synthesize and maintain the ECM, which determines the material properties of the tissue.
The cells of the menisci are referred to as fibrochondrocytes because they appear to be a mixture of fibroblasts and chondrocytes.111,177 The cells in the more superficial layer of the menisci are fusiform or spindle shaped (more fibroblastic), whereas the cells located deeper in the meniscus are ovoid or polygonal (more chondrocytic).55,56,178 Cell morphology does not differ between the peripheral and central locations in the menisci.56
Both cell types contain abundant endoplasmic reticulum and Golgi complex. Mitochondria are only occasionally visualized, suggesting that the major pathway for energy production of fibrochondrocytes in their avascular milieu is probably anaerobic glycolysis.112
Water
In normal, healthy menisci, tissue fluid represents 65% to 70% of the total weight. Most of the water is retained within the tissue in the solvent domains of proteoglycans. The water content of meniscal tissue is higher in the posterior areas than in the central or anterior areas; tissue samples from surface and deeper layers had similar contents.135
Large hydraulic pressures are required to overcome the drag of frictional resistance of forcing fluid flow through meniscal tissue. Thus, interactions between water and the matrix macromolecular framework significantly influence the viscoelastic properties of the tissue.
Collagens
Collagens are primarily responsible for the tensile strength of menisci; they contribute up to 75% of the dry weight of the ECM.77 The ECM is composed primarily of type I collagen (90% dry weight) with variable amounts of types II, III, V, and VI.43,44,80,112,181 The predominance of type I collagen distinguishes the fibrocartilage of menisci from articular (hyaline) cartilage. The collagens are heavily cross-linked by hydroxylpyridinium aldehydes.44
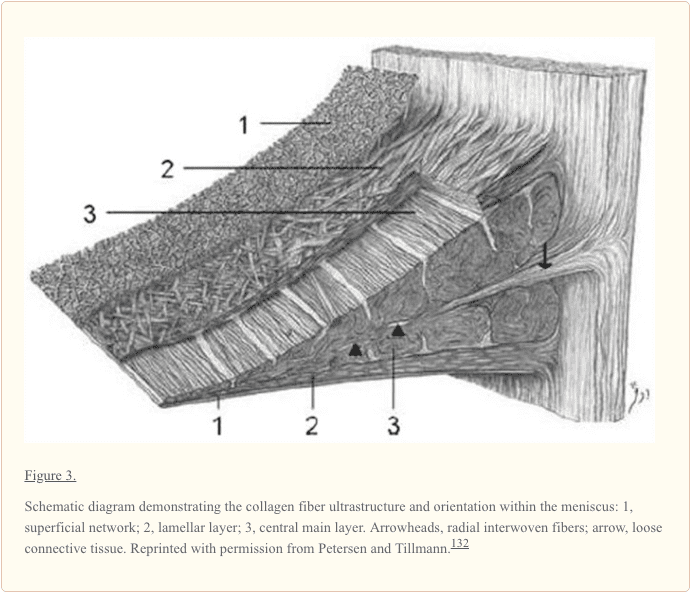
The collagen fiber arrangement is ideal for transferring a vertical compressive load into circumferential �hoop� stresses (Figure 3).57 Type I collagen fibers are oriented circumferentially in the deeper layers of the meniscus, parallel to the peripheral border. These fibers blend the ligamentous connections of the meniscal horns to the tibial articular surface (Figure 3).10,27,49,156 In the most superficial region of the menisci, the type I fibers are oriented in a more radial direction. Radially oriented �tie� fibers are also present in the deep zone and are interspersed or woven between the circumferential fibers to provide structural integrity (Figure 3).# There is lipid debris and calcified bodies in the ECM of human menisci.54 The calcified bodies contain long, slender crystals of phosphorous, calcium, and magnesium on electron-probe roentgenographic analysis.54 The function of these crystals in not completely understood, but it is believed that they may play a role in acute joint inflammation and destructive arthropathies.
Noncollagenous matrix proteins, such as fibronectin, contribute 8% to 13% of the organic dry weight. Fibronectin is involved in many cellular processes, including tissue repair, embryogenesis, blood clotting, and cell migration/adhesion. Elastin forms less than 0.6% of the meniscus dry weight; its ultrastructural localization is not clear. It likely interacts directly with collagen to provide resiliency to the tissue.**
Proteoglycans
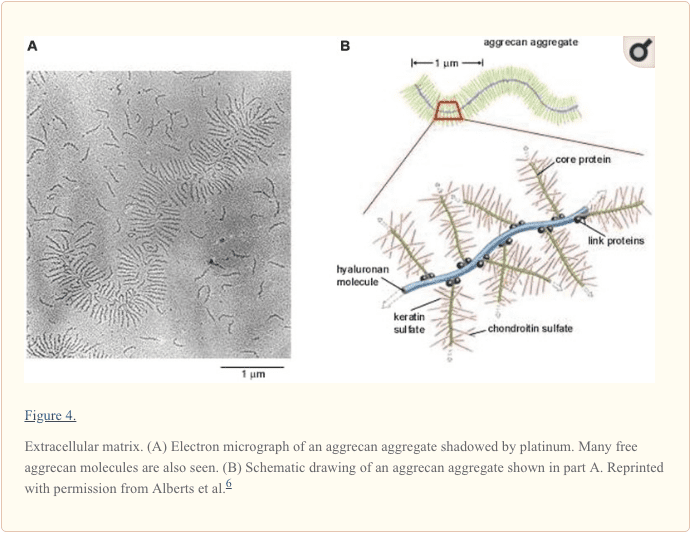
Located within a fine meshwork of collagen fibrils, proteoglycans are large, negatively charged hydrophilic molecules, contributing 1% to 2% of dry weight.58 They are formed by a core protein with 1 or more covalently attached glycosaminoglycan chains (Figure 4).122 The size of these molecules is further increased by specific interaction with hyaluronic acid.67,72 The amount of proteoglycans in the meniscus is one-eighth that of articular cartilage,2,3 and there may be considerable variation depending on the site of the sample and the age of the patient.49
By virtue of their specialized structure, high fixed-charge density, and charge-charge repulsion forces, proteoglycans in the ECM are responsible for hydration and provide the tissue with a high capacity to resist compressive loads.� The glycosaminoglycan profile of the normal adult human meniscus consists of chondroitin-6-sulfate (40%), chondroitin-4-sulfate (10% to 20%), dermatan sulfate (20% to 30%), and keratin sulfate (15%; Figure 4).65,77,99,159 The highest glycosaminoglycan concentrations are found in the meniscal horns and the inner half of the menisci in the primary weightbearing areas.58,77
Aggrecan is the major proteoglycan found in the human menisci and is largely responsible for their viscoelastic compressive properties (Figure 5). Smaller proteoglycans, such as decorin, biglycan, and fibromodulin, are found in smaller amounts.124,151 Hexosamine contributes 1% to the dry weight of ECM.57,74 The precise functions of each of these small proteoglycans on the meniscus have yet to be fully elucidated.
Matrix Glycoproteins
Meniscal cartilage contains a range of matrix glycoproteins, the identities and functions of which have yet to be determined. Electrophoresis and subsequent staining of the polyacrylamide gels reveals bands with molecular weights varying from a few kilodaltons to more than 200 kDa.112 These matrix molecules include the link proteins that stabilize proteoglycan�hyaluronic acid aggregates and a 116-kDa protein of unknown function.46 This protein resides in the matrix in the form of disulfide-bonded complex of high molecular weight.46 Immunolocalization studies suggest that it is predominantly located around the collagen bundles in the interterritorial matrix.47
The adhesive glycoproteins constitute a subgroup of the matrix glycoproteins. These macromolecules are partly responsible for binding with other matrix molecules and/or cells. Such intermolecular adhesion molecules are therefore important components in the supramolecular organization of the extracellular molecules of the meniscus.150 Three molecules have been identified within the meniscus: type VI collagen, fibronectin, and thrombospondin.112,118,181
Vascular Anatomy
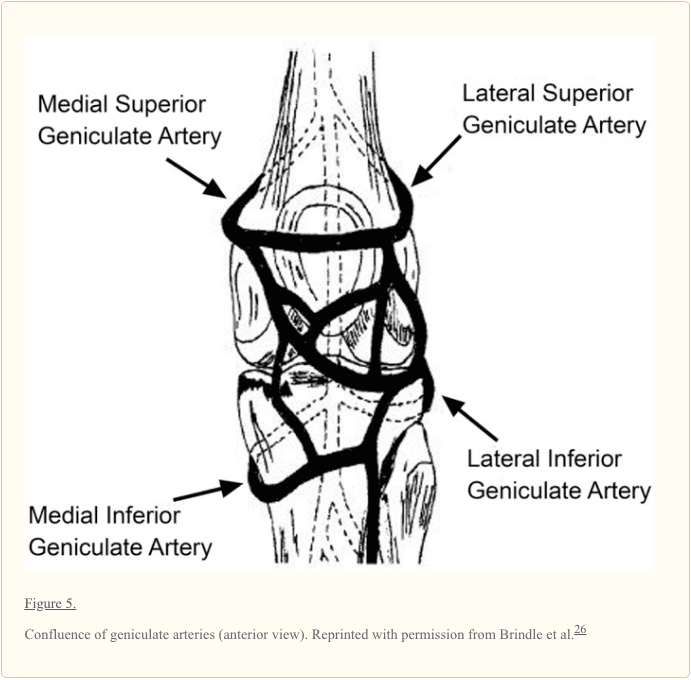
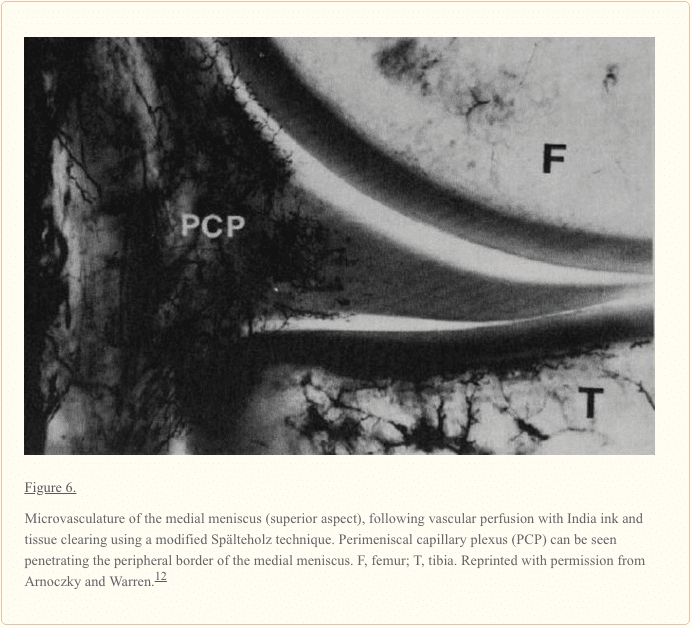
The meniscus is a relatively avascular structure with a limited peripheral blood supply. The medial, lateral, and middle geniculate arteries (which branch off the popliteal artery) provide the major vascularization to the inferior and superior aspects of each meniscus (Figure 5).9,12,33-35,148 The middle geniculate artery is a small posterior branch that perforates the oblique popliteal ligament at the posteromedial corner of the tibiofemoral joint. A premeniscal capillary network arising from the branches of these arteries originates within the synovial and capsular tissues of the knee along the periphery of the menisci. The peripheral 10% to 30% of the medial meniscus border and 10% to 25% of the lateral meniscus are relatively well vascularized, which has important implications for meniscus healing (Figure 6).12,33,68 Endoligamentous vessels from the anterior and posterior horns travel a short distance into the substance of the menisci and form terminal loops, providing a direct route for nourishment.33 The remaining portion of each meniscus (65% to 75%) receives nourishment from synovial fluid via diffusion or mechanical pumping (ie, joint motion).116,120
Bird and Sweet examined the menisci of animals and humans using scanning electron and light microscopy.23,24 They observed canal-like structures opening deep into the surface of the menisci. These canals may play a role in the transport of fluid within the meniscus and may carry nutrients from the synovial fluid and blood vessels to the avascular sections of the meniscus.23,24 However, further study is needed to elucidate the exact mechanism by which mechanical motion supplies nutrition to the avascular portion of the menisci.
Neuroanatomy
The knee joint is innervated by the posterior articular branch of the posterior tibial nerve and the terminal branches of the obturator and femoral nerves. The lateral portion of the capsule is innervated by the recurrent peroneal branch of the common peroneal nerve. These nerve fibers penetrate the capsule and follow the vascular supply to the peripheral portion of the menisci and the anterior and posterior horns, where most of the nerve fibers are concentrated.52,90 The outer third of the body of the meniscus is more densely innervated than the middle third.183,184 During extremes of flexion and extension of the knee, the meniscal horns are stressed, and the afferent input is likely greatest at these extreme positions.183,184
The mechanoreceptors within the menisci function as transducers, converting the physical stimulus of tension and compression into a specific electrical nerve impulse. Studies of human menisci have identified 3 morphologically distinct mechanoreceptors: Ruffini endings, Pacinian corpuscles, and Golgi tendon organs.�� Type I (Ruffini) mechanoreceptors are low threshold and slowly adapting to the changes in joint deformation and pressure. Type II (Pacinian) mechanoreceptors are low threshold and fast adapting to tension changes.�� Type III (Golgi) are high-threshold mechanoreceptors, which signal when the knee joint approaches the terminal range of motion and are associated with neuromuscular inhibition. These neural elements were found in greater concentration in the meniscal horns, particularly the posterior horn.
The asymmetrical components of the knee act in concert as a type of biological transmission that accepts, transfers, and dissipates loads along the femur, tibia, patella, and femur.41 Ligaments act as an adaptive linkage, with the menisci representing mobile bearings. Several studies have reported that various intra-articular components of the knee are sensate, capable of generating neurosensory signals that reach spinal, cerebellar, and higher central nervous system levels.?? It is believed that these neurosensory signals result in conscious perception and are important for normal knee joint function and maintenance of tissue homeostasis.42
The meniscus is cartilage which provides structural and functional integrity to the knee. The menisci are two pads of fibrocartilaginous tissue which spread out friction in the knee joint when it undergoes tension and torsion between the shin bone, or tibia, and the thigh bone, or femur. The understanding of the anatomy and biomechanics of the knee joint is essential towards the understanding of knee injuries and/or conditions. Dr. Alex Jimenez D.C., C.C.S.T. Insight
�
Biomechanical Function
The biomechanical function of the meniscus is a reflection of the gross and ultrastructural anatomy and of its relationship to the surrounding intra-articular and extra-articular structures. The menisci serve many important biomechanical functions. They contribute to load transmission,�� shock absorption,10,49,94,96,170 stability,51,100,101,109,155 nutrition,23,24,84,141 joint lubrication,102-104,141 and proprioception.5,15,81,88,115,147 They also serve to decrease contact stresses and increase contact area and congruity of the knee.91,172
Meniscal Kinematics
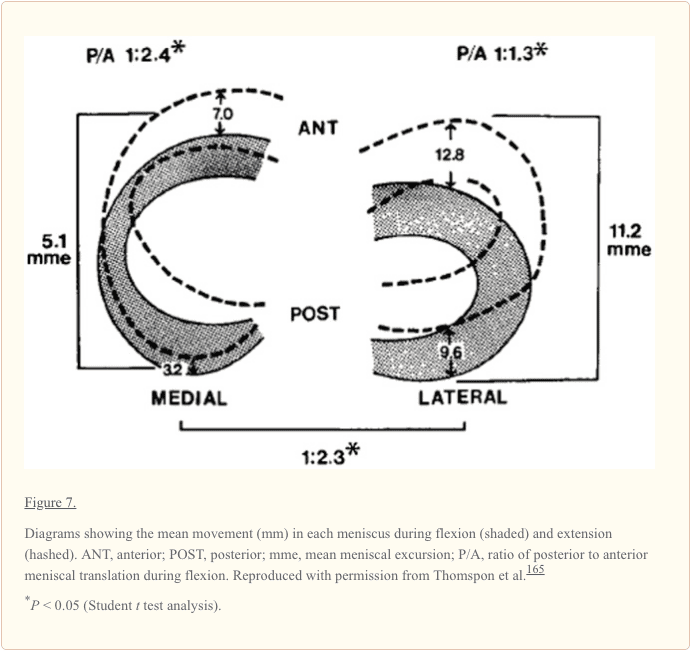
In a study on ligamentous function, Brantigan and Voshell reported the medial meniscus to move an average 2 mm, while the lateral meniscus was markedly more mobile with approximately 10 mm of anterior-posterior displacement during flexion.25 Similarly, DePalma reported that the medial meniscus undergoes 3 mm of anterior-posterior displacement, while the lateral meniscus moves 9 mm during flexion.37 In a study using 5 cadaveric knees, Thompson et al reported the mean medial excursion to be 5.1 mm (average of anterior and posterior horns) and the mean lateral excursion, 11.2 mm, along the tibial articular surface (Figure 7).165 The findings from these studies confirm a significant difference in segmental motion between the medial and lateral menisci. The anterior and posterior horn lateral meniscus ratio is smaller and indicates that the meniscus moves more as a single unit.165 Alternatively, the medial meniscus (as a whole) moves less than the lateral meniscus, displaying a greater anterior to posterior horn differential excursion. Thompson et al found that the area of least meniscal motion is the posterior medial corner, where the meniscus is constrained by its attachment to the tibial plateau by the meniscotibial portion of the posterior oblique ligament, which has been reported to be more prone to injury.143,165 A reduction in the motion of the posterior horn of the medial meniscus is a potential mechanism for meniscal tears, with a resultant �trapping� of the fibrocartilage between the femoral condyle and the tibial plateau during full flexion. The greater differential between anterior and posterior horn excursion may place the medial meniscus at a greater risk of injury.165
The differential of anterior horn to posterior horn motion allows the menisci to assume a decreasing radius with flexion, which correlates to the decreased radius of curvature of the posterior femoral condyles.165 This change of radius allows the meniscus to maintain contact with the articulating surface of both the femur and the tibia throughout flexion.
Load Transmission
The function of the menisci has been clinically inferred by the degenerative changes that accompany its removal. Fairbank described the increased incidence and predictable degenerative changes of the articular surfaces in completely meniscectomized knees.45 Since this early work, numerous studies have confirmed these findings and have further established the important role of the meniscus as a protective, load-bearing structure.
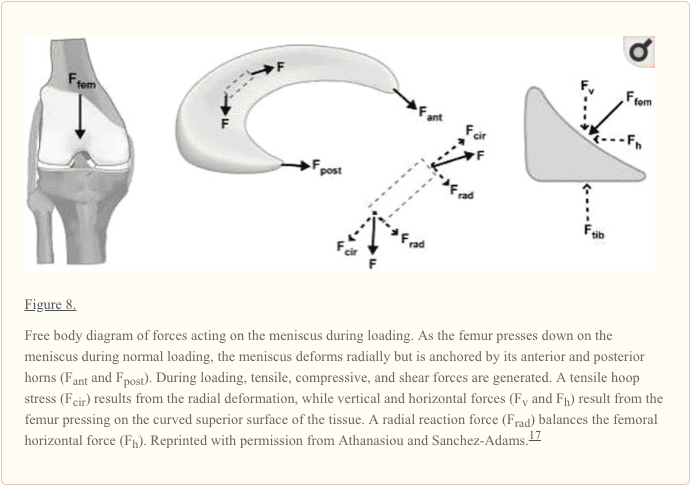
Weightbearing produces axial forces across the knee, which compress the menisci, resulting in �hoop� (circumferential) stresses.170 Hoop stresses are generated as axial forces and converted to tensile stresses along the circumferential collagen fibers of the meniscus (Figure 8). Firm attachments by the anterior and posterior insertional ligaments prevent the meniscus from extruding peripherally during load bearing.94 Studies by Seedhom and Hargreaves reported that 70% of the load in the lateral compartment and 50% of the load in the medial compartment is transmitted through the menisci.153 The menisci transmit 50% of compressive load through the posterior horns in extension, with 85% transmission at 90� flexion.172 Radin et al demonstrated that these loads are well distributed when the menisci are intact.137 However, removal of the medial meniscus results in a 50% to 70% reduction in femoral condyle contact area and a 100% increase in contact stress.4,50,91 Total lateral meniscectomy results in a 40% to 50% decrease in contact area and increases contact stress in the lateral component to 200% to 300% of normal.18,50,76,91 This significantly increases the load per unit area and may contribute to accelerated articular cartilage damage and degeneration.45,85
Shock Absorption
The menisci play a vital role in attenuating the intermittent shock waves generated by impulse loading of the knee with normal gait.94,96,153 Voloshin and Wosk showed that the normal knee has a shock-absorbing capacity about 20% higher than knees that have undergone meniscectomy.170 As the inability of a joint system to absorb shock has been implicated in the development of osteoarthritis, the meniscus would appear to play an important role in maintaining the health of the knee joint.138
Joint Stability
The geometric structure of the menisci provides an important role in maintaining joint congruity and stability.## The superior surface of each meniscus is concave, enabling effective articulation between the convex femoral condyles and flat tibial plateau. When the meniscus is intact, axial loading of the knee has a multidirectional stabilizing function, limiting excess motion in all directions.9
Markolf and colleagues have addressed the effect of meniscectomy on anterior-posterior and rotational knee laxity. Medial meniscectomy in the ACL-intact knee has little effect on anterior-posterior motion, but in the ACL-deficient knee, it results in an increase in anterior-posterior tibial translation of up to 58% at 90o of flexion.109 Shoemaker and Markolf demonstrated that the posterior horn of the medial meniscus is the most important structure resisting an anterior tibial force in the ACL-deficient knee.155 Allen et al showed that the resultant force in the medial meniscus of the ACL-deficient knee increased by 52% in full extension and by 197% at 60� of flexion under a 134-N anterior tibial load.7 The large changes in kinematics due to medial meniscectomy in the ACL-deficient knee confirm the important role of the medial meniscus in knee stability. Recently, Musahl et al reported that the lateral meniscus plays a role in anterior tibial translation during the pivot-shift maneuver.123
Joint Nutrition and Lubrication
The menisci may also play a role in the nutrition and lubrication of the knee joint. The mechanics of this lubrication remains unknown; the menisci may compress synovial fluid into the articular cartilage, which reduces frictional forces during weightbearing.13
There is a system of microcanals within the meniscus located close to the blood vessels, which communicates with the synovial cavity; these may provide fluid transport for nutrition and joint lubrication.23,24
Proprioception
The perception of joint motion and position (proprioception) is mediated by mechanoreceptors that transduce mechanical deformation into electric neural signals. Mechanoreceptors have been identified in the anterior and posterior horns of the menisci.*** Quick-adapting mechanoreceptors, such as Pacinian corpuscles, are thought to mediate the sensation of joint motion, and slow-adapting receptors, such as Ruffini endings and Golgi tendon organs, are believed to mediate the sensation of joint position.140 The identification of these neural elements (located mostly in the middle and outer third of the meniscus) indicates that the menisci are capable of detecting proprioceptive information in the knee joint, thus playing an important afferent role in the sensory feedback mechanism of the knee.61,88,90,158,169
Maturation and Aging of The Meniscus
The microanatomy of the meniscus is complex and certainly demonstrates senescent changes. With advancing age, the meniscus becomes stiffer, loses elasticity, and becomes yellow.78,95 Microscopically, there is a gradual loss of cellular elements with empty spaces and an increase in fibrous tissue in comparison with elastic tissue.74 These cystic areas can initiate a tear, and with a torsional force by the femoral condyle, the superficial layers of the meniscus may shear off from the deep layer at the interface of the cystic degenerative change, producing a horizontal cleavage tear. Shear between these layers may cause pain. The torn meniscus may directly injure the overlying articular cartilage.74,95
Ghosh and Taylor found that collagen concentration increased from birth to 30 years and remained constant until 80 years of age, after which a decline occurred.58 The noncollagenous matrix proteins showed the most profound changes, decreasing from 21.9% � 1.0% (dry weight) in neonates to 8.1% � 0.8% between the ages of 30 to 70 years.80 After 70 years of age, the noncollagenous matrix protein levels increased to 11.6% � 1.3%. Peters and Smillie observed an increase in hexosamine and uronic acid with age.131
McNicol and Roughley studied the variation of meniscal proteoglycans in aging113; small differences in extractability and hydrodynamic size were observed. The proportions of keratin sulfate relative to chondroitin-6-sulfate increased with aging.146
Petersen and Tillmann immunohistochemically investigated human menisci (ranging from 22 weeks of gestation to 80 years), observing the differentiation of blood vessels and lymphatics in 20 human cadavers. At the time of birth, nearly the entire meniscus was vascularized. In the second year of life, an avascular area developed in the inner circumference. In the second decade, blood vessels were present in the peripheral third. After 50 years of age, only the peripheral quarter of the meniscal base was vascularized. The dense connective tissue of the insertion was vascularized but not the fibrocartilage of the insertion. Blood vessels were accompanied by lymphatics in all areas.���
Arnoczky suggested that body weight and knee joint motion may eliminate blood vessels in the inner and middle aspects of the menisci.9 Nutrition of meniscal tissue occurs via perfusion from blood vessels and via diffusion from synovial fluid. A requirement for nutrition via diffusion is the intermittent loading and release on the articular surfaces, stressed by body weight and muscle forces.130 The mechanism is comparable with the nutrition of articular cartilage.22
Magnetic Resonance Imaging of The Meniscus
Magnetic resonance imaging (MRI) is a noninvasive diagnostic tool used in the evaluation, diagnosis, and monitoring of the menisci. MRI is widely accepted as the optimal imaging modality because of superior soft tissue contrast.
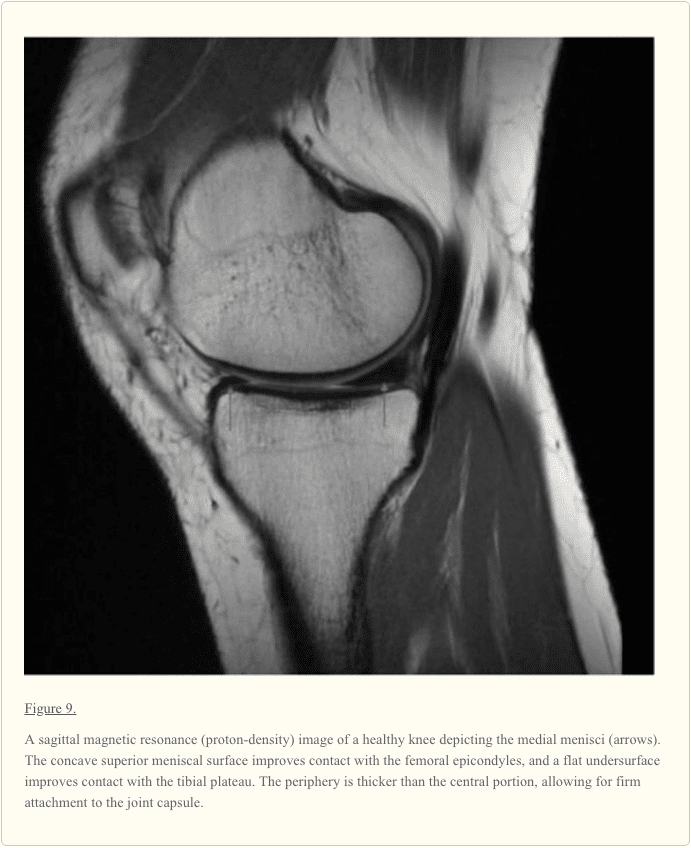
On cross-sectional MRI, the normal meniscus appears as a uniform low-signal (dark) triangular structure (Figure 9). A meniscal tear is identified by the presence of an increased intrameniscal signal that extends to the surface of this structure.
Several studies have evaluated the clinical utility of MRI for meniscal tears. In general, MRI is highly sensitive and specific for tears of the meniscus. The sensitivity of MRI in detecting meniscal tears ranges from 70% to 98%, and the specificity, from 74% to 98%.48,62,105,107,117 The MRI of 1014 patients before an arthroscopic examination had an accuracy of 89% for pathology of the medial meniscus and 88% for the lateral meniscus.48 A meta-analysis of 2000 patients with an MRI and arthroscopic examination found 88% sensitivity and 94% accuracy for meniscal tears.105,107
There have been discrepancies between MRI diagnoses and the pathology identified during arthroscopic examination.��� Justice and Quinn reported discrepancies in the diagnosis of 66 of the 561 patients (12%).86 In a study of 92 patients, discrepancies between the MRI and arthroscopic diagnoses were noted in 22 of the 349 (6%) cases.106 Miller conducted a single-blind prospective study comparing clinical examinations and MRI in 57 knee examinations.117 He found no significant difference in sensitivity between the clinical examination and MRI (80.7% and 73.7%, respectively). Shepard et al assessed the accuracy of MRI in detecting clinically significant lesions of the anterior horn of the meniscus in 947 consecutive knee MRI154 and found a 74% false-positive rate. Increased signal intensity in the anterior horn does not necessarily indicate a clinically significant lesion.154
Conclusions
The menisci of the knee joint are crescent-shaped wedges of fibrocartilage that provide increased stability to the femorotibial articulation, distribute axial load, absorb shock, and provide lubrication to the knee joint. Injuries to the menisci are recognized as a cause of significant musculoskeletal morbidity. Preservation of the menisci is highly dependent on maintaining its distinctive composition and organization.
In conclusion, the knee is the largest and most complex�joint in the human body. However, because the knee can commonly become damaged as a result of an injury and/or condition, it’s essential to understand the anatomy of the knee joint in order for patients to receive proper treatment.� The scope of our information is limited to chiropractic and spinal health issues. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Relieving Knee Pain without Surgery
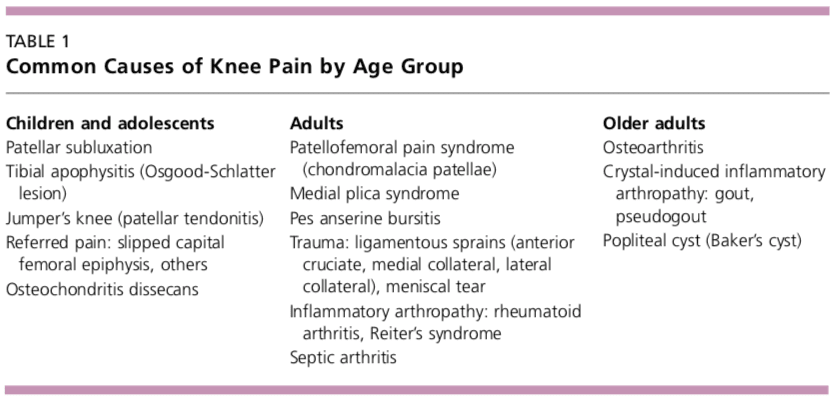
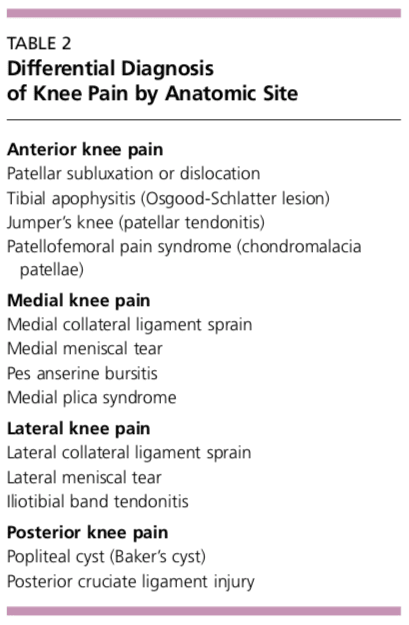
Knee pain is a well-known symptom which can occur due to a variety of knee injuries and/or conditions, including�sports injuries. The knee is one of the most complex joints in the human body as it is made-up of the intersection of four bones, four ligaments, various tendons, two menisci, and cartilage. According to the American Academy of Family Physicians, the most common causes of knee pain include patellar subluxation, patellar tendinitis or jumper’s knee, and Osgood-Schlatter disease. Although knee pain is most likely to occur in people over 60 years old, knee pain can also occur in children and adolescents. Knee pain can be treated at home following the RICE methods, however, severe knee injuries may require immediate medical attention, including chiropractic care.
1. Adams ME, Hukins DWL. The extracellular matrix of the meniscus. In: Mow VC, Arnoczky SP, Jackson DW, editors. eds. Knee Meniscus: Basic and Clinical Foundations. New York, NY: Raven Press; 1992:15-282016
2. Adams ME, McDevitt CA, Ho A, Muir H. Isolation and characterization of high-buoyant-density proteoglycans from semilunar menisci. J Bone Joint Surg Am. 1986;68:55-64 [PubMed]
3. Adams ME, Muir H. The glycosaminoglycans of canine menisci. Biochem J. 1981;197:385-389 [PMC free article][PubMed]
4. Ahmed AM, Burke DL. In-vitro measurement of static pressure distribution in synovial joints: part I. Tibial surface of the knee. J Biomech Eng. 1983;185:290-294 [PubMed]
5. Akgun U, Kogaoglu B, Orhan EK, Baslo MB, Karahan M. Possible reflex pathway between medial meniscus and semi-membranous muscle: an experimental study in rabbits. Knee Surg Sports Traumatol Arthrosc. 2008;16(9):809-814 [PubMed]
6. Alberts B, Johnson A, Lewis J, Raff M, Roberts K, Walter P. Molecular Biology of the Cell. 4th ed. Bethesda, MD: National Center for Biotechnology Information; 2002
7. Allen CR, Wong EK, Livesay GA, Sakane M, Fu FH, Woo SL. Importance of the medial meniscus in the anterior cruciate ligament-deficient knee. J Orthop Res. 2000;18(1):109-115 [PubMed]
8. Arnoczky SP. Building a meniscus: biologic considerations. Clin Orthop Relat Res. 1999;367S:244-253[PubMed]
9. Arnoczky SP. Gross and vascular anatomy of the meniscus and its role in meniscal healing, regeneration and remodeling. In: Mow VC, Arnoczky SP, Jackson DW, editors. , eds. Knee Meniscus: Basic and Clinical Foundations. New York, NY: Raven Press; 1992:1-14
10. Arnoczky SP, Adams ME, DeHaven KE, Eyre DR, Mow VC. The meniscus. In: Woo SL-Y, Buckwalter J, editors. , eds. Injury and Repair of Musculoskeletal Soft Tissues. Park Ridge, IL: American Academy of Orthopaedic Surgeons; 1987:487-537
11. Arnoczky SP, Warren RF. Anatomy of the cruciate ligaments. In: Feagin JA, editor. , ed. The Crucial Ligaments. New York, NY: Churchill Livingstone; 1988:179-195
12. Arnoczky SP, Warren RF. Microvasculature of the human meniscus. Am J Sports Med. 1982;10:90-95[PubMed]
13. Arnoczky SP, Warren RF, Spivak JM. Meniscal repair using exogenous fibrin clot: an experimental study in dogs. J Bone Joint Surg Am. 1988;70:1209-1217 [PubMed]
14. Aspden RM, Yarker YE, Hukins DWL. Collagen orientations in the meniscus of the knee joint. J Anat. 1985;140:371. [PMC free article][PubMed]
15. Assimakopoulos AP, Katonis PG, Agapitos MV, Exarchou EI. The innervations of the human meniscus. Clin Orthop Relat Res. 1992;275:232-236 [PubMed]
16. Atencia LJ, McDevitt CA, Nile WB, Sokoloff L. Cartilage content of an immature dog. Connect Tissue Res. 1989;18:235-242 [PubMed]
17. Athanasiou KA, Sanchez-Adams J. Engineering the Knee Meniscus. San Rafael, CA: Morgan & Claypool Publishers; 2009
18. Baratz ME, Fu FH, Mengato R. Meniscal tears: the effect of meniscectomy and of repair on the intraarticular contact areas and stress in the human knee. A preliminary report. Am J Sports Med. 1986;14:270-275 [PubMed]
19. Barrack RL, Skinner HB, Buckley SL. Proprioception in the anterior cruciate deficient knee. Am J Sports Med. 1989;17:1-6 [PubMed]
21. Beaupre A, Choukroun R, Guidouin R, Carneau R, Gerardin H. Knee menisci: correlation between microstructure and biomechanics. Clin Orthop Relat Res. 1986;208:72-75 [PubMed]
22. Benninghoff A. Form und Bau der Gelenkknorpel in ihren Beziehungen zur Funktion. Erste Mitteilung: Die modellierenden und formerhaltenden Faktoren des Knorpelreliefs. Z Anat Entwickl Gesch. 1925;76:4263
23. Bird MDT, Sweet MBE. Canals of the semilunar meniscus: brief report. J Bone Joint Surg Br. 1988;70:839. [PubMed]
24. Bird MDT, Sweet MBE. A system of canals in semilunar menisci. Ann Rheum Dis. 1987;46:670-673 [PMC free article][PubMed]
25. Brantigan OC, Voshell AF. The mechanics of the ligaments and menisci of the knee joint. J Bone Joint Surg Am. 1941;23:44-66
26. Brindle T, Nyland J, Johnson DL. The meniscus: review of basic principles with application to surgery and rehabilitation. J Athl Train. 2001;32(2):160-169 [PMC free article][PubMed]
27. Bullough PG, Munuera L, Murphy J, et al. The strength of the menisci of the knee as it relates to their fine structure. J Bone Joint Surg Br. 1979;52:564-570 [PubMed]
28. Bullough PG, Vosburgh F, Arnoczky SP, et al. The menisci of the knee. In: Insall JN, editor. , ed. Surgery of the Knee. New York, NY: Churchill Livingstone; 1984:135-149
29. Burr DB, Radin EL. Meniscal function and the importance of meniscal regeneration in preventing late medial compartment osteoarthrosis. Clin Orthop Relat Res. 1982;171:121-126 [PubMed]
30. Carney SL, Muir H. The structure and function of cartilage proteoglycans. Physiol Rev. 1988;68:858-910 [PubMed]
31. Clark CR, Ogden JA. Development of the menisci of the human knee joint. J Bone Joint Surg Am. 1983;65:530 [PubMed]
32. Clark FJ, Horsh KW, Bach SM, Larson GF. Contributions of cutaneous and joint receptors to static knee-position sense in man. J Neurophysiol. 1979;42:877-888 [PubMed]
33. Danzig L, Resnik D, Gonsalves M, Akeson WH. Blood supply to the normal and abnormal meniscus of the human knee. Clin Orthop Relat Res. 1983;172:271-276 [PubMed]
34. Davies D, Edwards D. The vascular and nerve supply of the human meniscus. Am R Coll Surg Engl. 1948;2:142-156
35. Day B, Mackenzie WG, Shim SS, Leung G. The vascular and nerve supply of the human meniscus. Arthroscopy. 1985;1:58-62 [PubMed]
36. DeHaven KE. Meniscectomy versus repair: clinical experience. In: Mow VC, Arnoczky SP, Jackson DW, editors. , eds. Knee Meniscus: Basic and Clinical Foundations. New York, NY: Raven Press; 1992:131-139
37. DePalma AF. Diseases of the Knee. Philadelphia, PA: JB Lippincott Co; 1954
38. De Smet AA, Graf BK. Meniscal tears missed on MR imaging: relationship to meniscal tear patterns and anterior cruciate ligament tears. AJR Am J Roentgenol. 1994;162:905-911 [PubMed]
39. De Smet AA, Norris MA, Yandow DR, et al. MR diagnosis of meniscal tears of the knee: importance of high signal in the meniscus that extends to the surface. AJR Am J Roentgenol. 1993;161:101-107[PubMed]
40. Dye SF. Functional morphologic features of the human knee: an evolutionary perspective. Clin Orthop Relat Res. 2003;410:19-24 [PubMed]
41. Dye SF. The knee as a biologic transmission with an envelope of function: a theory. Clin Orthop Relat Res. 1996;325:10-18 [PubMed]
42. Dye SF, Vaupel GL, Dye CC. Conscious neurosensory mapping of the internal structures of the human knee without intraarticular anesthesia. Am J Sports Med. 1998;26(6):773-777 [PubMed]
43. Eyre DR, Koob TJ, Chun LE. Biochemistry of the meniscus: unique profile of collagen types and site dependent variations in composition. Orthop Trans. 1983;8:56
44. Eyre DR, Wu JJ. Collagen of fibrocartilage: a distinctive molecular phenotype in bovine meniscus. FEBS Lett. 1983;158:265. [PubMed]
45. Fairbank TJ. Knee joint changes after meniscectomy. J Bone Joint Surg Br. 1948;30:664-670[PubMed]
46. Fife RS. Identification of the link proteins and a 116,000-dalton matrix protein in canine meniscus. Arch Biochem Biophys. 1985;240:682. [PubMed]
47. Fife RS, Hook GL, Brandt KD. Topographic localization of a 116,000 dalton protein in cartilage. J Histochem Cytochem. 1985;33:127. [PubMed]
48. Fischer SP, Fox JM, Del Pizzo W, et al. Accuracy of diagnoses from magnetic resonance imaging of the knee: a multi-center analysis of one thousand and fourteen patients. J Bone Joint Surg Am. 1991;73:2-10[PubMed]
49. Fithian DC, Kelly MA, Mow VC. Material properties and structure-function relationships in the menisci. Clin Orthop Relat Res. 1990;252:19-31 [PubMed]
50. Fukubayashi T, Kurosawa H. The contact area and pressure distribution pattern of the knee: a study of normal and osteoarthritic knee joints. Acta Orthop Scand. 1980;51:871-879 [PubMed]
51. Fukubayashi T, Torzilli PA, Sherman MF, Warren RF. An in vivo biomechanical analysis of anterior-posterior motion of the knee, tibial displacement rotation and torque. J Bone Joint Surg Am. 1982;64:258-264 [PubMed]
52. Gardner E. The innervations of the knee joint. Anat Rec. 1948;101:109-130 [PubMed]
53. Gardner E, O�Rahilly R. The early development of the knee joint in staged human embryos. J Anat. 1968;102:289-299 [PMC free article][PubMed]
54. Ghadially FN, LaLonde JMA. Intramatrical lipidic debris and calcified bodes in human semilunar cartilages. J Anat. 1981;132:481. [PMC free article][PubMed]
55. Ghadially FN, LaLonde JMA, Wedge JH. Ultrastructure of normal and torn menisci of the human knee joint. J Anat. 1983;136:773-791 [PMC free article][PubMed]
56. Ghadially FN, Thomas I, Yong N, LaLonde JMA. Ultrastructure of rabbit semilunar cartilage. J Anat. 1978;125:499. [PMC free article][PubMed]
57. Ghosh P, Ingman AM, Taylor TK. Variations in collagen, non-collagenous proteins, and hexosamine in menisci derived from osteoarthritic and rheumatoid arthritic knee joints. J Rheumatol. 1975;2:100-107[PubMed]
58. Ghosh P, Taylor TKF. The knee joint meniscus: a fibrocartilage of some distinction. Clin Orthop Relat Res. 1987;224:52-63 [PubMed]
59. Ghosh P, Taylor TKF, Pettit GD, Horsburgh BA, Bellenger CR. Effect of postoperative immobilization on the regrowth of knee joint semilunar cartilage: an experimental study. J Orthop Res. 1983;1:153.[PubMed]
60. Gray DJ, Gardner E. Pre-natal development of the human knee and superior tibial fibula joints. Am J Anat. 1950;86:235-288 [PubMed]
61. Gray JC. Neural and vascular anatomy of the menisci of the human knee. J Orthop Sports Phys Ther. 1999;29(1):23-30 [PubMed]
62. Gray SD, Kaplan PA, Dussault RG. Imaging of the knee: current status. Orthop Clin North Am. 1997;28:643-658 [PubMed]
63. Greis PE, Bardana DD, Holmstrom MC, Burks RT. Meniscal injury: I. Basic science and evaluation. J Am Acad Orthop Surg. 2002;10:168-176 [PubMed]
64. Gronblad M, Korkala O, Liesi P, Karaharju E. Innervation of synovial membrane and meniscus. Acta Orthop Scand. 1985;56:484-486 [PubMed]
65. Habuchi H, Yamagata T, Iwata H, Suzuki S. The occurrence of a wide variety of dermatan sulfate-chondroitin sulfate copolymers in fibrous cartilage. J Biol Chem. 1973;248:6019-6028 [PubMed]
67. Hardingham TE, Muir H. Binding of oligosaccharides of hyaluronic acid to proteoglycans. Biochem J. 1973;135 (4):905-908 [PMC free article][PubMed]
68. Harner CD, Janaushek MA, Kanamori A, Yagi AKM, Vogrin TM, Woo SL. Biomechanical analysis of a double-bundle posterior cruciate ligament reconstruction. Am J Sports Med. 2000;28:144-151 [PubMed]
69. Harner CD, Kusayama T, Carlin G, et al. Structural and mechanical properties of the human posterior cruciate ligament and meniscofemoral ligaments. In: Transactions of the 40th Annual Meeting of the Orthopaedic Research Society; 1992
70. Harner CD, Livesgay GA, Choi NY, et al. Evaluation of the sizes and shapes of the human anterior and posterior cruciate ligaments: a comparative study. Trans Orthop Res Soc. 1992;17:123
71. Hascall VC. Interaction of cartilage proteoglycans with hyaluronic acid. J Supramol Struct. 1977;7:101-120 [PubMed]
72. Hascall VC, Heineg�rd D. Aggregation of cartilage proteoglycans: I. The role of hyaluronic acid. J Biol Chem. 1974;249(13):4205-4256 [PubMed]
73. Heinegard D, Oldberg A. Structure and biology of cartilage and bone matrix noncollagenous macromolecules. FASEB J. 1989;3:2042-2051 [PubMed]
74. Helfet AJ. Osteoarthritis of the knee and its early arrest. Instr Course Lect. 1971;20:219-230
75. Heller L, Langman J. The meniscofemoral ligaments of the human knee. J Bone Joing Surg Br. 1964;46:307-313 [PubMed]
76. Henning CE, Lynch MA, Clark JR. Vascularity for healing of meniscal repairs. Arthroscopy. 1987;3:13-18 [PubMed]
77. Herwig J, Egner E, Buddecke E. Chemical changes of human knee joint menisci in various stages of degeneration. Ann Rheum Dis. 1984;43:635-640 [PMC free article][PubMed]
78. H�pker WW, Angres G, Klingel K, Komitowksi D, Schuchardt E. Changes of the elastin compartment in the human meniscus. Virchows Arch A Pathol Anat Histopathol. 1986;408:575-592 [PubMed]
79. Humphry GM. A Treatise on the Human Skeleton Including the Joints. Cambridge, UK: Macmillan; 1858:545-546
80. Ingman AM, Ghosh P, Taylor TKF. Variation of collagenous and non-collagenous proteins of human knee joint menisci with age and degeneration. Gerontologia. 1974;20:212-233 [PubMed]
81. Jerosch J, Prymka M, Castro WH. Proprioception of the knee joints with a lesion of the medial meniscus. Acta Orthop Belg. 1996;62(1):41-45 [PubMed]
82. Johnson DL, Swenson TD, Harner CD. Arthroscopic meniscal transplantation: anatomic and technical considerations. Presented at: Nineteenth Annual Meeting of the American Orthopaedic Society for Sports Medicine; July 12-14, 1993; Sun Valley, ID
83. Johnson DL, Swenson TM, Livesay GA, Aizawa H, Fu FH, Harner CD. Insertion-site anatomy of the human menisci: gross, arthroscopic, and topographical anatomy as a basis for meniscal transplantation. Arthroscopy. 1995;11:386-394 [PubMed]
84. Johnson RJ, Pope MH. Functional anatomy of the meniscus. In: Symposium on Reconstruction of the Knee of the American Academy of Orthopaedic Surgeons. St Louis, MO: Mosby; 1978:3
85. Jones RE, Smith EC, Reisch JS. Effects of medial meniscectomy in patients older than forty years. J Bone Joint Surg Am. 1978;60:783-786 [PubMed]
86. Justice WW, Quinn SF. Error patterns in the MR imaging evaluation of the menisci of the knee. Radiology. 1995;196:617-621 [PubMed]
87. Kaplan EB. The embryology of the menisci of the knee joint. Bull Hosp Joint Dis. 1955;6:111-124[PubMed]
88. Karahan M, Kocaoglu B, Cabukoglu C, Akgun U, Nuran R. Effect of partial medial meniscectomy on the proprioceptive function of the knee. Arch Orthop Trauma Surg. 2010;130:427-431 [PubMed]
89. Kempson GE, Tuke MA, Dingle JT, Barrett AJ, Horsfield PH. The effects of proteolytic enzymes on the mechanical properties of adult human articular cartilage. Biochim Biophys Acta. 1976;428(3):741-760[PubMed]
90. Kennedy JC, Alexander IJ, Hayes KC. Nerve supply of the human knee and its functional importance. Am J Sports Med. 1982;10:329-335 [PubMed]
91. Kettelkamp DB, Jacobs AW. Tibiofemoral contact area: determination and implications. J Bone Joint Surg Am. 1972;54:349-356 [PubMed]
92. King D. The function of the semilunar cartilages. J Bone Joint Surg Br. 1936;18:1069-1076
93. Kohn D, Moreno B. Meniscus insertion anatomy as a basis for meniscus replacement: a morphological cadaveric study. Arthroscopy. 1995;11:96-103 [PubMed]
94. Krause WR, Pope MH, Johnson RJ, Wilder DG. Mechanical changes in the knee after meniscectomy. J Bone Joint Surg Am. 1976;58:599-604 [PubMed]
95. Kulkarni VV, Chand K. Pathological anatomy of the aging meniscus. Acta Orthop Scand. 1975;46:135-140 [PubMed]
96. Kurosawa H, Fukubayashi T, Nakajima H. Load-bearing mode of the knee joint: physical behavior of the knee joint with or without menisci. Clin Orthop Relat Res. 1980;149:283-290 [PubMed]
97. LaPrade RF, Burnett QM, II, Veenstra MA, et al. The prevalence of abnormal magnetic resonance imaging findings in asymptomatic knees: with correlation of magnetic resonance imaging to arthroscopic finding in symptomatic knees. Am J Sports Med. 1994;22:739-745 [PubMed]
98. Last RJ. Some anatomical details of the knee joint. J Bone Joint Surg Br. 1948;30:368-688 [PubMed]
99. Lehtonen A, Viljanto J, K�rkk�inen J. The mucopolysaccharides of herniated human intervertebral discs and semilunar cartilages. Acta Chir Scand. 1967;133(4):303-306 [PubMed]
100. Levy IM, Torzilli PA, Warren RF. The effect of lateral meniscectomy on motion of the knee. J Bone Joint Surg Am. 1989;71:401-406 [PubMed]
101. Levy IM, Torzilli PA, Warren RF. The effect of medial meniscectomy on anterior-posterior motion of the knee. J Bone Joint Surg Am. 1982;64:883-888 [PubMed]
102. MacConaill MA. The function of intra-articular fibrocartilages with special reference to the knee and inferior radio-ulnar joints. J Anat. 1932;6:210-227 [PMC free article][PubMed]
103. MacConaill MA. The movements of bones and joints: III. The synovial fluid and its assistants. J Bone Joint Surg Br. 1950;32:244. [PubMed]
104. MacConaill MA. Studies in the mechanics of synovial joints: II. Displacements on articular surfaces and the significance of saddle joints. Ir J Med Sci. 1946;6:223-235 [PubMed]
105. Mackenzie R, Dixon AK, Keene GS, et al. Magnetic resonance imaging of the knee: assessment of effectiveness. Clin Radiol. 1996;41:245-250 [PubMed]
106. Mackenzie R, Keene GS, Lomas DJ, Dixon AK. Errors at knee magnetic resonance imaging: true or false?Br J Radiol. 1995;68:1045-1051 [PubMed]
107. Mackenzie R, Palmer CR, Lomas DJ, et al. Magnetic resonance imaging of the knee: diagnostic performance studies. Clin Radiol. 1996;51:251-257 [PubMed]
108. Markolf KL, Bargar WL, Shoemaker SC, Amstutz HC. The role of joint load in knee instability. J Bone Joint Surg Am. 1981;63:570-585 [PubMed]
109. Markolf KL, Mensch JS, Amstutz HC. Stiffness and laxity of the knee: the contributions of the supporting structures. J Bone Joint Surg Am. 1976;58:583-597 [PubMed]
110. McDermott LJ. Development of the human knee joint. Arch Surg. 1943;46:705-719
111. McDevitt CA, Miller RR, Sprindler KP. The cells and cell matrix interaction of the meniscus. In: Mow VC, Arnoczky SP, Jackson DW, editors. , eds. Knee Meniscus: Basic and Clinical Foundations. New York, NY: Raven Press; 1992:29-36
112. McDevitt CA, Webber RJ. Ultrastructure and biochemistry of meniscal cartilage. Clin Orthop Relat Res. 1990;252:8-18 [PubMed]
113. McNicol D, Roughley PJ. Extraction and characterization of proteoglycan from human meniscus. Biochem J. 1980;185:705. [PMC free article][PubMed]
114. Merkel KHH. The surface of human menisci and its aging alterations during age: a combined scanning and transmission electron microscopic examination (SEM, TEM). Arch Orthop Trauma Surg. 1980;97:185-191 [PubMed]
115. Messner K, Gao J. The menisci of the knee joint: anatomical and functional characteristics, and a rationale for clinical treatment. J Anat. 1998;193:161-178 [PMC free article][PubMed]
116. Meyers E, Zhu W, Mow V. Viscoelastic properties of articular cartilage and meniscus. In: Nimni M, editor. , ed. Collagen: Chemistry, Biology and Biotechnology. Boca Raton, FL: CRC; 1988
117. Miller GK. A prospective study comparing the accuracy of the clinical diagnosis of meniscal tear with magnetic resonance imaging and its effect on clinical outcome. Arthroscopy. 1996;12:406-413 [PubMed]
118. Miller GK, McDevitt CA. The presence of thrombospondin in ligament, meniscus and intervertebral disc. Glycoconjugate J. 1988;5:312
119. Mossman DJ, Sargeant WAS. The footprints of extinct animals. Sci Am. 1983;250:78-79
120. Mow V, Fithian D, Kelly M. Fundamentals of articular cartilage and meniscus biomechanics. In: Ewing JW, editor. , ed. Articular Cartilage and Knee Joint Function: Basic Science and Arthroscopy. New York, NY: Raven Press; 1989:1-18
121. Mow VC, Holmes MH, Lai WM. Fluid transport and mechanical properties or articular cartilage: a review. J Biomech. 1984;17:377. [PubMed]
122. Muir H. The structure and metabolism of mucopolysaccharides (glycosaminoglycans) and the problem of the mucopolysaccharidoses. Am J Med. 1969;47 (5):673-690 [PubMed]
123. Musahl V, Citak M, O�Loughlin PF, Choi D, Bedi A, Pearle AD. The effect of medial versus lateral meniscectomy on the stability of the anterior cruciate ligament-deficient knee. Am J Sports Med. 2010;38(8):1591-1597 [PubMed]
124. Nakano T, Dodd CM, Scott PG. Glycosaminoglycans and proteoglycans from different zones of the porcine knee meniscus. J Orthop Res. 1997;15:213-222 [PubMed]
125. Newton RA. Joint receptor contributions to reflective and kinaesthetic responses. Phys Ther. 1982;62:22-29 [PubMed]
126. O�Connor BL. The histological structure of the dog knee menisci with comments on its possible significance. Am J Anat. 1976;147:407-417 [PubMed]
127. O�Connor BL, McConnaughey JS. The structure and innervation of cat knee menisci, and their relation to a �sensory hypothesis� of meniscal function. Am J Anat. 1978;153:431-442 [PubMed]
128. Oretorp N, Gillquist J, Liljedahl S-O. Long term results of surgery for non-acute anteromedial rotatory instability of the knee. Acta Orthop Scand. 1979;50:329-336 [PubMed]
129. Pagnani MJ, Warren RF, Arnoczky SP, Wickiewicz TL. Anatomy of the knee. In: Nicholas JA, Hershman EB, editors. , eds. The Lower Extremity and Spine in Sports Medicine. 2nd ed. St Louis, MO: Mosby; 1995:581-614
130. Pauwels F. [Developmental effects of the functional adaptation of bone]. Anat Anz. 1976;139:213-220[PubMed]
131. Peters TJ, Smillie IS. Studies on the chemical composition of the menisci of the knee joint with special reference to the horizontal cleavage lesion. Clin Orthop Relat Res. 1972;86:245-252 [PubMed]
132. Petersen W, Tillmann B. Collagenous fibril texture of the human knee joint menisci. Anat Embryol (Berl). 1998;197:317-324 [PubMed]
133. Poynton AR, Javadpour SM, Finegan PJ, O�Brien M. The meniscofemoral ligaments of the knee. J Bone Joint Surg Br. 1997;79:327-330 [PubMed]
134. Preuschoft H, Tardieu C. Biomechanical reasons for divergent morphology of the knee joint and the distal epiphyseal suture in hominoids. Folia Primatol (Basel). 1996;66:82-92 [PubMed]
135. Proctor CS, Schmidt MB, Whipple RR, Kelly MA, Mow VC. Material properties of the normal medial bovine meniscus. J Orthop Res. 1989;7:771-782 [PubMed]
136. Proske U, Schaible H, Schmidt RF. Joint receptors and kinanesthesia. Exp Brain Res. 1988;72:219-224 [PubMed]
137. Radin EL, de Lamotte F, Maquet P. Role of the menisci in the distribution of stress in the knee. Clin Orthop Relat Res. 1984;185:290-294 [PubMed]
138. Radin EL, Rose RM. Role of subchondral bone in the initiation and progression of cartilage damage. Clin Orthop Relat Res. 1986;213:34-40 [PubMed]
139. Raszeja F. Untersuchungen Bber Entstehung und feinen Bau des Kniegelenkmeniskus. Bruns Beitr klin Chir. 1938;167:371-387
140. Reider B, Arcand MA, Diehl LH, et al. Proprioception of the knee before and after anterior cruciate ligament reconstruction. Arthroscopy. 2003;19(1):2-12 [PubMed]
141. Renstrom P, Johnson RJ. Anatomy and biomechanics of the menisci. Clin Sports Med. 1990;9:523-538 [PubMed]
142. Retterer E. De la forme et des connexions que presentment les fibro-cartilages du genou chez quelques singes d�Afrique. Cr Soc Biol. 1907;63:20-25
143. Ricklin P, Ruttimann A, Del Bouno MS. Diagnosis, Differential Diagnosis and Therapy. 2nd ed. Stuttgart, Germany: Verlag Georg Thieme; 1983
144. Rodkey WG. Basic biology of the meniscus and response to injury. In: Price CT, editor. , ed. Instructional Course Lectures 2000. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2000:189-193 [PubMed]
145. Rosenberg LC, Buckwalter JA, Coutts R, Hunziker E, Mow VC. Articular cartilage. In: Woo SLY, Buckwalter JA, editors. , eds. Injury and Repair of the Musculoskeletal Soft Tissues. Park Ridge, IL: American Academy of Orthopaedic Surgeon; 1988:401
146. Roughley PJ. Changes in cartilage proteoglycan structure during aging: origin and effects: a review. Agents Actions. 1986;518:19 [PubMed]
147. Saygi B, Yildirim Y, Berker N, Ofluoglu D, Karadag-Saygi E, Karahan M. Evaluation of neurosensory function of the medial meniscus in humans. Arthroscopy. 2005;21(12):1468-1472 [PubMed]
148. Scapinelli R. Studies on the vasculature of the human knee joint. Acta Anat. 1968;70:305-331[PubMed]
149. Schutte MJ, Dabezius EJ, Zimny ML, Happe LT. Neural anatomy of the human anterior cruciate ligament. J Bone Joint Surg Am. 1987;69:243-247 [PubMed]
150. Scott JE. Supramolecular organization of extracellular matrix glycosaminoglycans, in vitro and in the tissues. FASEB J. 1992;6:2639-2645 [PubMed]
151. Scott PG, Nakano T, Dodd CM. Isolation and characterization of small proteoglycans from different zones of the porcine knee meniscus. Biochim Biophys Acta. 1997;1336:254-262 [PubMed]
152. Seedhom BB. Loadbearing function of the menisci. Physiotherapy. 1976;62(7):223. [PubMed]
153. Seedhom BB, Hargreaves DJ. Transmission of the load in the knee joint with special reference to the role in the menisci: part II. Experimental results, discussion and conclusion. Eng Med. 1979;8:220-228
154. Shepard MF, Hunter DM, Davies MR, Shapiro MS, Seeger LL. The clinical significance of anterior horn meniscal tears diagnosed on magnetic resonance images. Am J Sports Med. 2002;30(2):189-192[PubMed]
155. Shoemaker SC, Markolf KL. The role of the meniscus in the anterior-posterior stability of the loaded anterior cruciate-deficient knee: effects of partial versus total excision. J Bone Joint Surg Am. 1986;68(1):71-79 [PubMed]
156. Skaags DL, Mow VC. Function of the radial tie fibers in the meniscus. Trans Orthop Res Soc. 1990;15:248
157. Skinner HB, Barrack RL. Joint position sense in the normal and pathologic knee joint. J Electromyogr Kinesiol. 1991;1(3):180-190 [PubMed]
159. Solheim K. Glycosaminoglycans, hydroxyproline, calcium, and phosphorus in healing fractures. Acta Univ Lund. 1965;28:1-22
160. Spilker RL, Donzelli PS. A biphasic finite element model of the meniscus for stress-strain analysis. In: Mow VC, Arnoczky SP, Jackson DW, editors. , eds. Knee Meniscus: Basic and Clinical Foundations. New York, NY: Raven Press; 1992:91-106
161. Spilker RL, Donzelli PS, Mow VC. A transversely isotropic biphasic finite element model of the meniscus. J Biomechanics. 1992;25:1027-1045 [PubMed]
162. Sutton JB. Ligaments: Their Nature and Morphology. 2nd ed. London: HK Lewis; 1897
163. Tardieu C. Ontogeny and phylogeny of femoral-tibial characters in humans and hominid fossils: functional influence and genetic determinism. Am J Phys Anthropol. 1999;110:365-377 [PubMed]
164. Tardieu C, Dupont JY. The origin of femoral trochlear dysplasia: comparative anatomy, evolution, and growth of the patellofemoral joint. Rev Chir Orthop Reparatrice Appar Mot. 2001;87:373-383 [PubMed]
165. Thompson WO, Thaete FL, Fu FH, Dye SF. Tibial meniscal dynamics using three-dimensional reconstruction of magnetic resonance imaging. Am J Sports Med. 1991;19:210-216 [PubMed]
166. Tissakht M, Ahmed AM. Tensile stress-strain characteristics of the human meniscal material. J Biomech. 1995;28:411-422 [PubMed]
167. Tobler T. Zur normalen und pathologischen Histologie des Kniegelenkmeniscus. Arch Klin Chir. 1933;177:483-495
168. Vallois H. Etude anatomique de l�articulation du genou chez les primates. Montpelier, France: L�Abeille; 1914
169. Verdonk R, Aagaard H. Function of the normal meniscus and consequences of the meniscal resection. Scand J Med Sci Sports. 1999;9(3):134-140 [PubMed]
170. Voloshin AS, Wosk J. Shock absorption of meniscectomized and painful knees: a comparative in vivo study. J Biomed Eng. 1983;5:157-161 [PubMed]
171. Wagner H-J. Die kollagenfaserarchitecktur der menisken des menschlichen kniegelenkes. Z Mikrosk Anat Forsch. 1976;90:302. [PubMed]
172. Walker PS, Erkman MJ. The role of the meniscus in force transmission across the knee. Clin Orthop Relat Res. 1975;109:184-192 [PubMed]
173. Wan ACT, Felle P. The menisco-femoral ligaments. Clin Anat. 1995;8:323-326 [PubMed]
174. Warren PJ, Olanlokun TK, Cobb AG, Bentley G. Proprioception after knee arthroplasty: the influence of prosthetic design. Clin Orthop Relat Res. 1993;297:182-187 [PubMed]
175. Warren RF, Arnoczky SP, Wickiewiez TL. Anatomy of the knee. In: Nicholas JA, Hershman EB, editors. , eds. The Lower Extremity and Spine in Sports Medicine. St Louis: Mosby; 1986:657-694
176. Watanabe AT, Carter BC, Teitelbaum GP, et al. Common pitfalls in magnetic resonance imaging of the knee. J Bone Joint Surg Am. 1989;71:857-862 [PubMed]
177. Webber RJ, Norby DP, Malemud CJ, Goldberg VM, Moskowitz RW. Characterization of newly synthesized proteoglycans from rabbit menisci in organ culture. Biochem J. 1984;221(3):875-884 [PMC free article][PubMed]
178. Webber RJ, York JL, Vanderschildren JL, Hough AJ. An organ culture model for assaying wound repair of the fibrocartilaginous knee joint meniscus. Am J Sports Med. 1989;17:393-400 [PubMed]
179. Wilson AS, Legg PG, McNeu JC. Studies on the innervations of the medial meniscus in the human knee joint. Anat Rec. 1969;165:485-492 [PubMed]
180. Wirth CJ. The meniscus: structure, morphology and function. Knee. 1996;3:57-58
181. Wu JJ, Eyre DR, Slayter HS. Type VI collagen of the intervertebral disc: biochemical and electron microscopic characterization of the native protein. Biochem J. 1987;248:373. [PMC free article][PubMed]
182. Yasui K. Three dimensional architecture of normal human menisci. J Jpn Ortho Assoc. 1978;52:391
183. Zimny ML. Mechanoreceptors in articular tissues. Am J Anat. 1988;64:883-888
184. Zimny ML, Albright DJ, Dabezies E. Mechanoreceptors in the human medial meniscus. Acta Anat. 1988;133:35-40 [PubMed]
185. Zivanovic S. Menisco-meniscal ligaments of the human knee joint. Anat Anz. 1974;145:35-42[PubMed]
The knee is the largest joint in the human body, where the complex structures of the lower and upper legs come together. Consisting of three bones, the femur, the tibia, and the patella which are surrounded by a variety of soft tissues, including cartilage, tendons and ligaments, the knee functions as a hinge, allowing you to walk, jump, squat or sit. As a result, however, the knee is considered to be one of the joints that are most prone to suffer injury. A knee injury is the prevalent cause of knee pain.
A knee injury can occur as a result of a direct impact from a slip-and-fall accident or automobile accident, overuse injury from sports injuries, or even due to underlying conditions, such as arthritis. Knee pain is a common symptom which affects people of all ages. It may also start suddenly or develop gradually over time, beginning as a mild or moderate discomfort then slowly worsening as time progresses. Moreover, being overweight can increase the risk of knee problems. The purpose of the following article is to discuss the evaluation of patients presenting with knee pain and demonstrate their differential diagnosis.
Abstract
Knee pain is a common presenting complaint with many possible causes. An awareness of certain patterns can help the family physician identify the underlying cause more efficiently. Teenage girls and young women are more likely to have patellar tracking problems such as patellar subluxation and patellofemoral pain syndrome, whereas teenage boys and young men are more likely to have knee extensor mechanism problems such as tibial apophysitis (Osgood-Schlatter lesion) and patellar tendonitis. Referred pain resulting from hip joint pathology, such as slipped capital femoral epiphysis, also may cause knee pain. Active patients are more likely to have acute ligamentous sprains and overuse injuries such as pes anserine bursitis and medial plica syndrome. Trauma may result in acute ligamentous rupture or fracture, leading to acute knee joint swelling and hemarthrosis. Septic arthritis may develop in patients of any age, but crystal-induced inflammatory arthropathy is more likely in adults. Osteoarthritis of the knee joint is common in older adults. (Am Fam Physician 2003;68:917-22. Copyright� 2003 American Academy of Family Physicians.)
Introduction
Determining the underlying cause of knee pain can be difficult, in part because of the extensive differential diagnosis. As discussed in part I of this two-part article,1 the family physician should be familiar with knee anatomy and common mechanisms of injury, and a detailed history and focused physical examination can narrow possible causes. The patient�s age and the anatomic site of the pain are two factors that can be important in achieving an accurate diagnosis (Tables 1 and 2). �
�
�
Children and Adolescents
Children and adolescents who present with knee pain are likely to have one of three common conditions: patellar subluxation, tibial apophysitis, or patellar tendonitis. Additional diagnoses to consider in children include slipped capital femoral epiphysis and septic arthritis.
Patellar Subluxation
Patellar subluxation is the most likely diagnosis in a teenage girl who presents with giving-way episodes of the knee.2 This injury occurs more often in girls and young women because of an increased quadriceps angle (Q angle), usually greater than 15 degrees.
Patellar apprehension is elicited by subluxing the patella laterally, and a mild effusion is usually present. Moderate to severe knee swelling may indicate hemarthrosis, which suggests patellar dislocation with osteochondral fracture and bleeding.
Tibial Apophysitis
A teenage boy who presents with anterior knee pain localized to the tibial tuberosity is likely to have tibial apophysitis or Osgood- Schlatter lesion3,4 (Figure 1).5 The typical patient is a 13- or 14-year-old boy (or a 10- or 11-year-old girl) who has recently gone through a growth spurt.
The patient with tibial apophysitis generally reports waxing and waning of knee pain for a period of months. The pain worsens with�squatting, walking up or down stairs, or forceful contractions of the quadriceps muscle. This overuse apophysitis is exacerbated by jumping and hurdling because repetitive hard landings place excessive stress on the insertion of the patellar tendon.
On physical examination, the tibial tuberosity is tender and swollen and may feel warm. The knee pain is reproduced with the resisted active extension or passive hyperflexion of the knee. No effusion is present. Radiographs are usually negative; rarely, they show avulsion of the apophysis at the tibial tuberosity. However, the physician must not mistake the normal appearance of the tibial apophysis for an avulsion fracture. �
�
�
�
Patellar Tendonitis
Jumper�s knee (irritation and inflammation of the patellar tendon) most commonly occurs in teenage boys, particularly during a growth spurt2 (Figure 1).5 The patient reports vague anterior knee pain that has persisted for months and worsens after activities such as walking down stairs or running.
On physical examination, the patellar tendon is tender, and the pain is reproduced by resisted knee extension. There is usually no effusion. Radiographs are not indicated.
Slipped Capital Femoral Epiphysis
A number of pathologic conditions result in referral of pain to the knee. For example, the possibility of slipped capital femoral epiphysis must be considered in children and teenagers who present with knee pain.6 The patient with this condition usually reports poorly localized knee pain and no history of knee trauma.
The typical patient with slipped capital femoral epiphysis is overweight and sits on the examination table with the affected hip slightly flexed and externally rotated. The knee examination is normal, but hip pain is elicited with passive internal rotation or extension of the affected hip.
Radiographs typically show displacement of the epiphysis of the femoral head. However, negative radiographs do not rule out the diagnosis in patients with typical clinical findings. Computed tomographic (CT) scanning is indicated in these patients.
Osteochondritis Dissecans
Osteochondritis dissecans is an intra-articular osteochondrosis of unknown etiology that is characterized by degeneration and recalcification of articular cartilage and underlying bone. In the knee, the medial femoral condyle is most commonly affected.7
The patient reports vague, poorly localized knee pain, as well as morning stiffness or recurrent effusion. If a loose body is present, mechanical symptoms of locking or catching of the knee joint also may be reported. On physical examination, the patient may demonstrate quadriceps atrophy or tenderness along the involved chondral surface. A mild joint effusion may be present.7
Plain-film radiographs may demonstrate the osteochondral lesion or a loose body in the knee joint. If osteochondritis dissecans is suspected, recommended radiographs include anteroposterior, posteroanterior tunnel, lateral, and Merchant�s views. Osteochondral lesions at the lateral aspect of the medial femoral condyle may be visible only on the posteroanterior tunnel view. Magnetic resonance imaging (MRI) is highly sensitive in detecting these abnormalities and is indicated in patients with a suspected osteochondral lesion.7 �
�
A knee injury caused by sports injuries, automobile accidents, or an underlying condition, among other causes, can affect the cartilage, tendons and ligaments which form the knee joint itself. The location of the knee pain can differ according to the structure involved, also, the symptoms can vary. The entire knee may become painful and swollen as a result of inflammation or infection, whereas a torn meniscus or fracture may cause symptoms in the affected region. Dr. Alex Jimenez D.C., C.C.S.T. Insight
Adults
Overuse Syndromes
Anterior Knee Pain. Patients with patellofemoral pain syndrome (chondromalacia patellae) typically present with a vague history of mild to moderate anterior knee pain that usually occurs after prolonged periods of sitting (the so-called �theater sign�).8 Patellofemoral pain syndrome is a common cause of anterior knee pain in women.
On physical examination, a slight effusion may be present, along with patellar crepitus on the range of motion. The patient�s pain may be reproduced by applying direct pressure to the anterior aspect of the patella. Patellar tenderness may be elicited by subluxing the patella medially or laterally and palpating the superior and inferior facets of the patella. Radiographs usually are not indicated.
Medial Knee Pain. One frequently overlooked diagnosis is medial plica syndrome. The plica, a redundancy of the joint synovium medially, can become inflamed with repetitive overuse.4,9 The patient presents with acute onset of medial knee pain after a marked increase in usual activities. On physical examination, a tender, mobile nodularity is present at the medial aspect of the knee, just anterior to the joint line. There is no joint effusion, and the remainder of the knee examination is normal. Radiographs are not indicated.
Pes anserine bursitis is another possible cause of medial knee pain. The tendinous insertion of the sartorius, gracilis, and semitendinosus muscles at the anteromedial aspect of the proximal tibia forms the pes anserine bursa.9 The bursa can become inflamed as a result of overuse or a direct contusion. Pes�anserine bursitis can be confused easily with a medial collateral ligament sprain or, less commonly, osteoarthritis of the medial compartment of the knee. �
�
�
The patient with pes anserine bursitis reports pain at the medial aspect of the knee. This pain may be worsened by repetitive flexion and extension. On physical examination, tenderness is present at the medial aspect of the knee, just posterior and distal to the medial joint line. No knee joint effusion is present, but there may be slight swelling at the insertion of the medial hamstring muscles. Valgus stress testing in the supine position or resisted knee flexion in the prone position may reproduce the pain. Radiographs are usually not indicated.
Lateral Knee Pain. Excessive friction between the iliotibial band and the lateral femoral condyle can lead to iliotibial band tendonitis.9 This overuse syndrome commonly occurs in runners and cyclists, although it may develop in any person subsequent to activity involving repetitive knee flexion. The tightness of the iliotibial band, excessive foot pronation, genu varum, and tibial torsion are predisposing factors.
The patient with iliotibial band tendonitis reports pain at the lateral aspect of the knee joint. The pain is aggravated by activity, particularly running downhill and climbing stairs. On physical examination, tenderness is present at the lateral epicondyle of the femur, approximately 3 cm proximal to the joint line. Soft tissue swelling and crepitus also may be present, but there is no joint effusion. Radiographs are not indicated.
Noble�s test is used to reproduce the pain in iliotibial band tendonitis. With the patient in a supine position, the physician places a thumb over the lateral femoral epicondyle as the�patient repeatedly flexes and extends the knee. Pain symptoms are usually most prominent with the knee at 30 degrees of flexion.
Popliteus tendonitis is another possible cause of lateral knee pain. However, this condition is fairly rare.10
Trauma
Anterior Cruciate Ligament Sprain. Injury to the anterior cruciate ligament usually occurs because of noncontact deceleration forces, as when a runner plants one foot and sharply turns in the opposite direction. Resultant valgus stress on the knee leads to anterior displacement of the tibia and sprain or rupture of the ligament.11 The patient usually reports hearing or feeling a �pop� at the time of the injury and must cease activity or competition immediately. Swelling of the knee within two hours after the injury indicates rupture of the ligament and consequent hemarthrosis.
On physical examination, the patient has a moderate to severe joint effusion that limits the range of motion. The anterior drawer test may be positive, but can be negative because of hemarthrosis and guarding by the hamstring muscles. The Lachman test should be positive and is more reliable than the anterior drawer test (see text and Figure 3 in part I of the article1).
Radiographs are indicated to detect possible tibial spine avulsion fracture. MRI of the knee is indicated as part of a presurgical evaluation.
Medial Collateral Ligament Sprain. Injury to the medial collateral ligament is fairly common and is usually the result of acute trauma. The patient reports a misstep or collision that places valgus stress on the knee, followed by the immediate onset of pain and swelling at the medial aspect of the knee.11
On physical examination, the patient with medial collateral ligament injury has point tenderness at the medial joint line. Valgus stress testing of the knee flexed to 30 degrees reproduces the pain (see text and Figure 4 in part I of this article1). A clearly defined endpoint on valgus stress testing indicates a grade 1�or grade 2 sprain, whereas complete medial instability indicates full rupture of the ligament (grade 3 sprain).
Lateral Collateral Ligament Sprain. Injury of the lateral collateral ligament is much less common than the injury of the medial collateral ligament. Lateral collateral ligament sprain usually results from varus stress to the knee, as occurs when a runner plants one foot and then turns toward the ipsilateral knee.2 The patient reports acute onset of lateral knee pain that requires prompt cessation of activity.
On physical examination, point tenderness is present at the lateral joint line. Instability or pain occurs with varus stress testing of the knee flexed to 30 degrees (see text and Figure 4 in part I of this article1). Radiographs are not usually indicated.
Meniscal Tear. The meniscus can be torn acutely with a sudden twisting injury of the knee, such as may occur when a runner suddenly changes direction.11,12 Meniscal tear also may occur in association with a prolonged degenerative process, particularly in a patient with an anterior cruciate ligament-deficient knee. The patient usually reports recurrent knee pain and episodes of catching or locking of the knee joint, especially with squatting or twisting of the knee.
On physical examination, a mild effusion is usually present, and there is tenderness at the medial or lateral joint line. Atrophy of the vastus medialis obliquus portion of the quadriceps muscle also may be noticeable. The McMurray test may be positive (see Figure 5 in part I of this article1), but a negative test does not eliminate the possibility of a meniscal tear.
Plain-film radiographs usually are negative and seldom are indicated. MRI is the radiologic test of choice because it demonstrates most significant meniscal tears.
Infection
Infection of the knee joint may occur in patients of any age but is more common in those whose immune system has been weakened by cancer, diabetes mellitus, alcoholism,�acquired immunodeficiency syndrome, or corticosteroid therapy. The patient with septic arthritis reports abrupt onset of pain and swelling of the knee with no antecedent trauma.13
On physical examination, the knee is warm, swollen, and exquisitely tender. Even slight motion of the knee joint causes intense pain.
Arthrocentesis reveals turbid synovial fluid. Analysis of the fluid yields a white blood cell count (WBC) higher than 50,000 per mm3 (50 ? 109 per L), with more than 75 percent (0.75) polymorphonuclear cells, an elevated protein content (greater than 3 g per dL [30 g per L]), and a low glucose concentration (more than 50 percent lower than the serum glucose concentration).14 Gram stain of the fluid may demonstrate the causative organism. Common pathogens include Staphylococcus aureus, Streptococcus species, Haemophilus influenza, and Neisseria gonorrhoeae.
Hematologic studies show an elevated WBC, an increased number of immature polymorphonuclear cells (i.e., a left shift), and an elevated erythrocyte sedimentation rate (usually greater than 50 mm per hour).
Older Adults
Osteoarthritis
Osteoarthritis of the knee joint is a common problem after 60 years of age. The patient presents with knee pain that is aggravated by weight-bearing activities and relieved by rest.15 The patient has no systemic symptoms but usually awakens with morning stiffness that dissipates somewhat with activity. In addition to chronic joint stiffness and pain, the patient may report episodes of acute synovitis.
Findings on physical examination include decreased range of motion, crepitus, a mild joint effusion, and palpable osteophytic changes at the knee joint.
When osteoarthritis is suspected, recommended radiographs include weight-bearing anteroposterior and posteroanterior tunnel views, as well as non-weight-bearing Merchants and lateral views. Radiographs show�joint-space narrowing, subchondral bony sclerosis, cystic changes, and hypertrophic osteophyte formation.
Crystal-Induced Inflammatory Arthropathy
Acute inflammation, pain, and swelling in the absence of trauma suggest the possibility of a crystal-induced inflammatory arthropathy such as gout or pseudogout.16,17 Gout commonly affects the knee. In this arthropathy, sodium urate crystals precipitate in the knee joint and cause an intense inflammatory response. In pseudogout, calcium pyrophosphate crystals are the causative agents.
On physical examination, the knee joint is erythematous, warm, tender, and swollen. Even minimal range of motion is exquisitely painful.
Arthrocentesis reveals clear or slightly cloudy synovial fluid. Analysis of the fluid yields a WBC count of 2,000 to 75,000 per mm3 (2 to 75 ? 109 per L), a high protein content (greater than 32 g per dL [320 g per L]), and a glucose concentration that is approximately 75 percent of the serum glucose con- centration.14 Polarized-light microscopy of the synovial fluid displays negatively birefringent rods in the patient with gout and positively birefringent rhomboids in the patient with pseudogout.
Popliteal Cyst
The popliteal cyst (Baker�s cyst) is the most common synovial cyst of the knee. It originates from the posteromedial aspect of the knee joint at the level of the gastrocnemio-semimembranous bursa. The patient reports insidious onset of mild to moderate pain in the popliteal area of the knee.
On physical examination, palpable fullness is present at the medial aspect of the popliteal area, at or near the origin of the medial head of the gastrocnemius muscle. The McMurray test may be positive if the medial meniscus is injured. Definitive diagnosis of a popliteal cyst may be made with arthrography, ultrasonography, CT scanning, or, less commonly, MRI.
The authors indicate that they do not have any conflicts of interest. Sources of funding: none reported.
In conclusion, although the knee is the largest joint in the human body where the structures of the lower extremities meet, including the femur, the tibia, the patella, and many other soft tissues, the knee can easily suffer damage or injury and result in knee pain. Knee pain is one of the most common complaints among the general population, however, it commonly occurs in athletes. Sports injuries, slip-and-fall accidents, and automobile accidents, among other causes, can lead to knee pain.
As described in the article above, diagnosis is essential towards determining the best treatment approach for each type of knee injury, according to their underlying cause. While the location and the severity of the knee injury may vary depending on the cause of the health issue, knee pain is the most common symptom. Treatment options, such as chiropractic care and physical therapy, can help treat knee pain. The scope of our information is limited to chiropractic and spinal health issues. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez �
�
�
Additional Topic Discussion: Relieving Knee Pain without Surgery
�
Knee pain is a well-known symptom which can occur due to a variety of knee injuries and/or conditions, including�sports injuries. The knee is one of the most complex joints in the human body as it is made-up of the intersection of four bones, four ligaments, various tendons, two menisci, and cartilage. According to the American Academy of Family Physicians, the most common causes of knee pain include patellar subluxation, patellar tendinitis or jumper’s knee, and Osgood-Schlatter disease. Although knee pain is most likely to occur in people over 60 years old, knee pain can also occur in children and adolescents. Knee pain can be treated at home following the RICE methods, however, severe knee injuries may require immediate medical attention, including chiropractic care.
1. Calmbach WL, Hutchens M. Evaluation of patients presenting with knee pain: part I. History, physical examination, radiographs, and laboratory tests. Am Fam Physician 2003;68:907-12.
2. Walsh WM. Knee injuries. In: Mellion MB, Walsh WM, Shelton GL, eds. The team physician�s hand- book. 2d ed. St. Louis: Mosby, 1990:554-78.
3. Dunn JF. Osgood-Schlatter disease. Am Fam Physi- cian 1990;41:173-6.
4. Stanitski CL. Anterior knee pain syndromes in the adolescent. Instr Course Lect 1994;43:211-20.
5. Tandeter HB, Shvartzman P, Stevens MA. Acute knee injuries: use of decision rules for selective radiograph ordering. Am Fam Physician 1999;60: 2599-608.
6. Waters PM, Millis MB. Hip and pelvic injuries in the young athlete. In: DeLee J, Drez D, Stanitski CL, eds. Orthopaedic sports medicine: principles and practice. Vol. III. Pediatric and adolescent sports medicine. Philadelphia: Saunders, 1994:279-93.
7. Schenck RC Jr, Goodnight JM. Osteochondritis dis- secans. J Bone Joint Surg [Am] 1996;78:439-56.
8. Ruffin MT 5th, Kiningham RB. Anterior knee pain: the challenge of patellofemoral syndrome. Am Fam Physician 1993;47:185-94.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine