Back Clinic Imaging & Diagnostics Team. Dr. Alex Jimenez works with top-rated diagnosticians and imaging specialists. In our association, imaging specialists provide fast, courteous, and top-quality results. In collaboration with our offices, we provide the quality of service our patients’ mandate and deserve. Diagnostic Outpatient Imaging (DOI) is a state-of-the-art Radiology center in El Paso, TX. It is the only center of its kind in El Paso, owned and operated by a Radiologist.
This means when you come to DOI for a radiologic exam, every detail, from the design of the rooms, the choice of the equipment, the hand-picked technologists, and the software which runs the office, is carefully chosen or designed by the Radiologist and not by an accountant. Our market niche is one center of excellence. Our values related to patient care are: We believe in treating patients the way we would treat our family and we will do our best to ensure that you have a good experience at our clinic.
Result from valgus or varus stress with or w/o axial loading
Associated with periarticular soft tissues injury
High-stress injury m/c due to jumps falls and axial loading, often with the splitting of the tibial plateau. Men>women. Patients are in their 30s
Low impact or no trauma in patients with osteoporosis d/t insufficiency fractures
Impaction injury is more common with depression of tibial plateau. Women>men. Patients are in their 70s
Lateral Tibial Plateau Fractures More Common
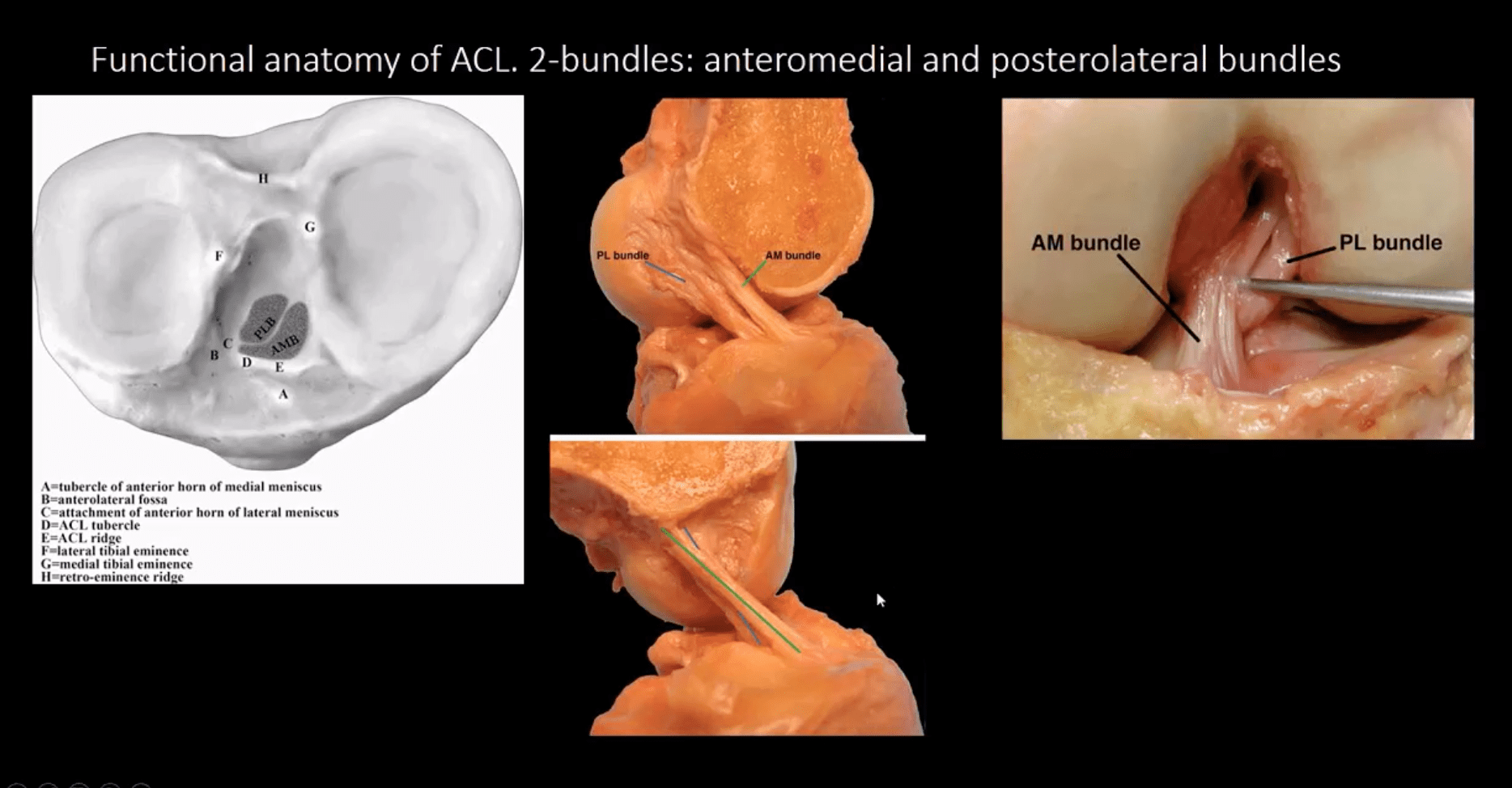
Functional anatomy plays a significant role
60% of weight bearing is by the medial plateau
The medial plateau is more concave
Lateral plateau is slightly higher and more convex. Valgus stress impacts lateral plateau.
Tibial plateau fractures considered intra-articular and prone to delayed healing, non-union, meniscal injury (m/c lateral) ACL tear, secondary OA. Other complications: compartment syndrome, vascular injury.
Management: operative in many cases especially if >3-mm step-off at the plateau
If medial plateau or bicondylar Fxs present, ORIF will be required.
Imaging Plays A Crucial Role
Begins with x-radiography. X-radiography may not reveal the complexity and extent of this injury.
CT scanning w/o contrast will further delineate fracture complexity and pre-operative planning
MR imaging may be considered to evaluate for internal derangement: meniscal, ACL injuries.
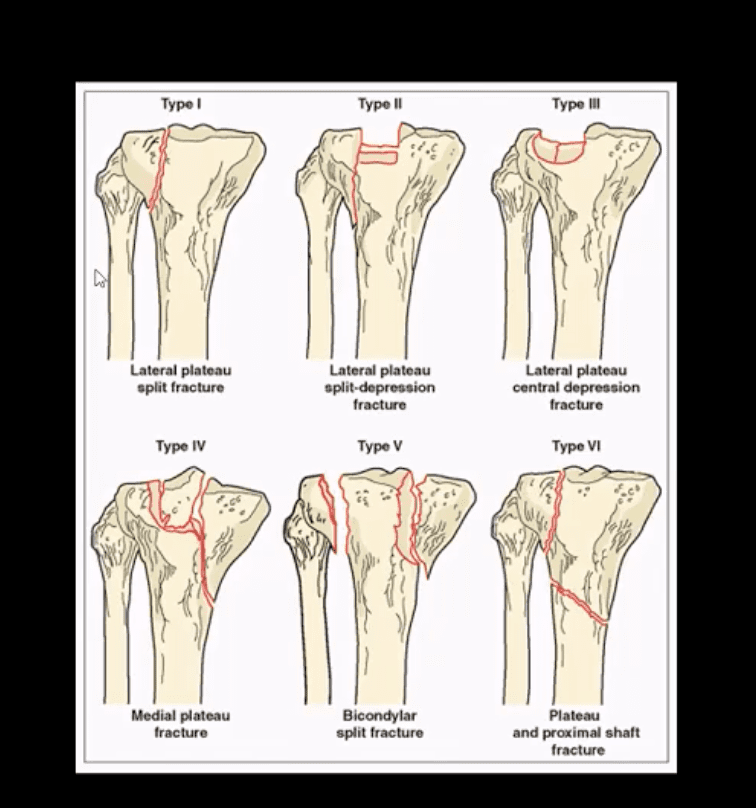
Shatzke classification may help to evaluate the complexity of this injury
Key Diagnostic Sign
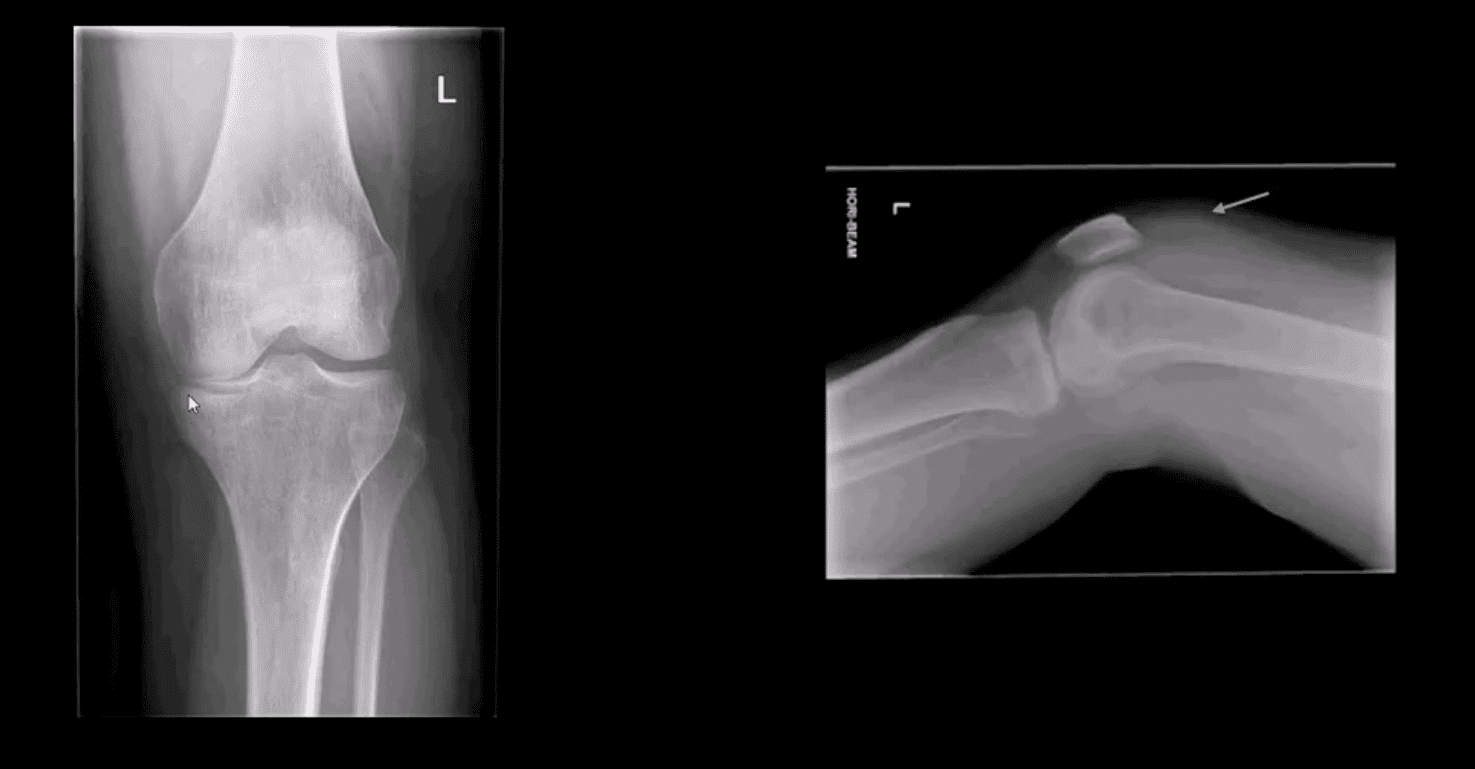
AP and lateral horizontal beam (cross table) left knee radiograph. Note subtle depression of the lateral plateau manifested by the lateral plateau appearing at the same level or lower as the medial. A critical diagnostic sign is the presence of fat-blood-interphase or FBI sign on cross-table lateral (above arrow) indicating intra-articular knee fracture
Lipohemarthorosis aka FBI Sign
Can be detected by radiography, CT or MR imaging
FBI sign is a reliable secondary radiographic sign of intra-articular knee fractures, regardless of how small they are
Mechanism: fracture results with acute hemarthrosis
Hemarthrosis will also occur w/o Fx. However, Fx will result with a fatty marrow being released into the joint cavity. Fat is a less dense medium (lighter) and will appear on the top of the hemorrhage if the patient is held in the supine position for 5-10-minutes before the cross-table radiograph is taken
FBI sign confirms the intra-articular Fx.
ACL/PCL, meniscal tears will not result in FBI sign
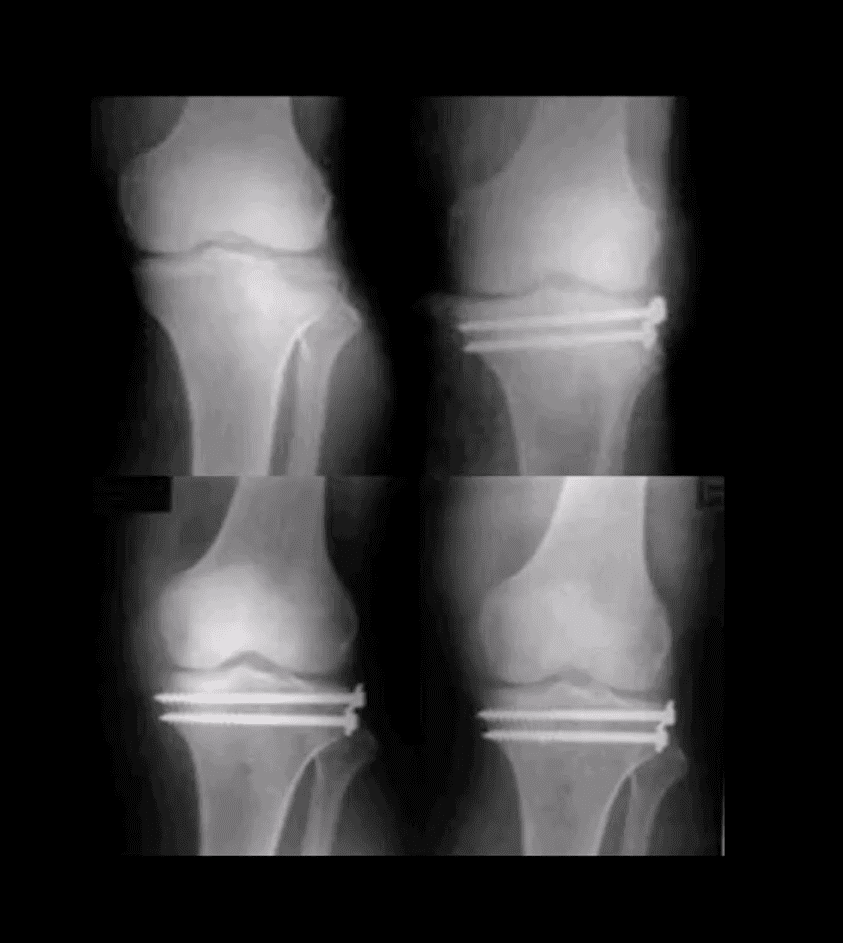
Lateral Tibial Plateau Fx
Lateral tibial plateau Fx that was managed operatively
Most common complication: premature secondary OA
More complex injuries may result in more extensive operative care
Knee Internal Derangement
Acute or chronic injuries of meniscal fibrocartilages and ligamentous restraints
Tears of the ACL and posterior horn of the medial meniscus are the most common
Acute ACL tears, however, often result with a lateral meniscus tear
Acute ACL tear may occur as a combined injury of the ACL, MCL, and medial meniscus
Functional anatomy: ACL prevents anterior displacement of the tibia and secondary varus stress
MCL functions together with ACL in resisting external rotation of the tibia especially when the foot is planted (closed chain position)
MCL is firmly attached to the medial meniscus, explaining the classic triad of ACL, MCL and medial meniscal tear (O’Donahue terrible triad)
Cruciate ligaments (ACL/PCL) are intra-articular but extra-synovial. Less likely to be torn in closed pack position (full extension). When all articular facets of tibia and femur are in full contact, the ACL/PCL are at least tension and stable
When the knee is flexed 20-30-degrees or more ACL is taut and remains unstable
ACL is a significant mechanoreceptor that feeds the info to CNS about the joint position. Thus the majority of previous ACL tears will lead to some degree of knee instability
Functional Anatomy of ACL
Diagnosis of ACL Tear
Diagnosis of ACL tear requires MR imaging
Concerns exist of not only ligamentous injuries but injuries to the articular cartilage and menisci.
Most vendors will perform at least: one T1 WI in coronal or sagittal planes. Sagittal and coronal Proton-density slices to evaluate cartilaginous structures. Fast spin-echo sagittal, axial and coronal T2 fat-saturated or sagittal and coronal STIR images are crucial to demonstrate edema within the substance of knee ligaments
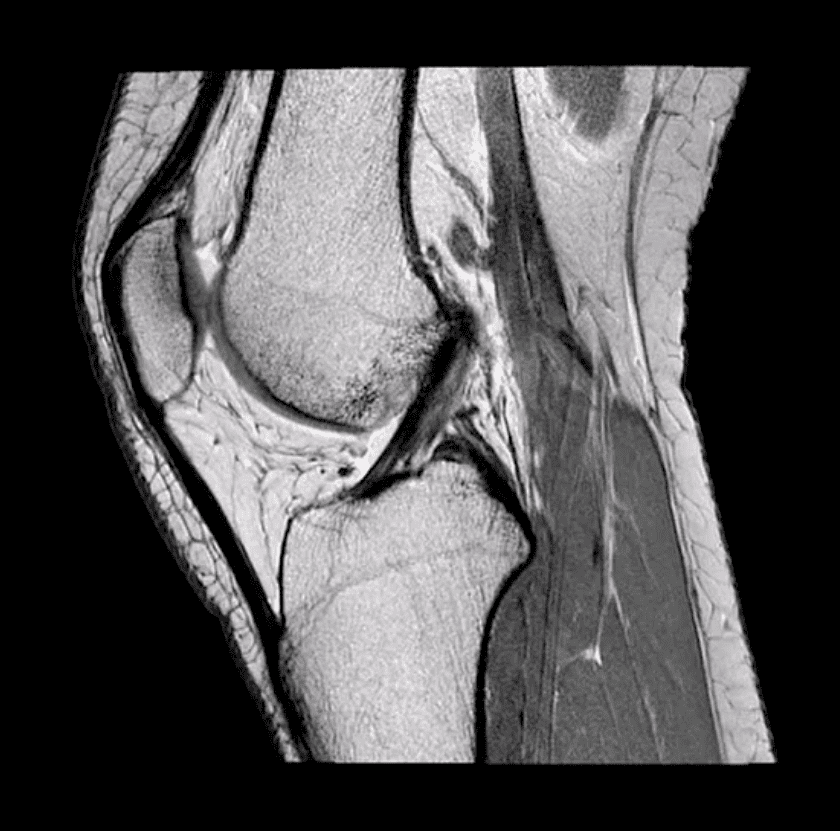
ACL is aligned along the Blumensaat line or oblique line corresponding the intercondylar roof of Femoral condyles. Lack of such alignment by the ACL is significant for ACL tear
Imaging Dx of Internal Derangement
MRI shows 78-100% sensitivity and 78-100% specificity
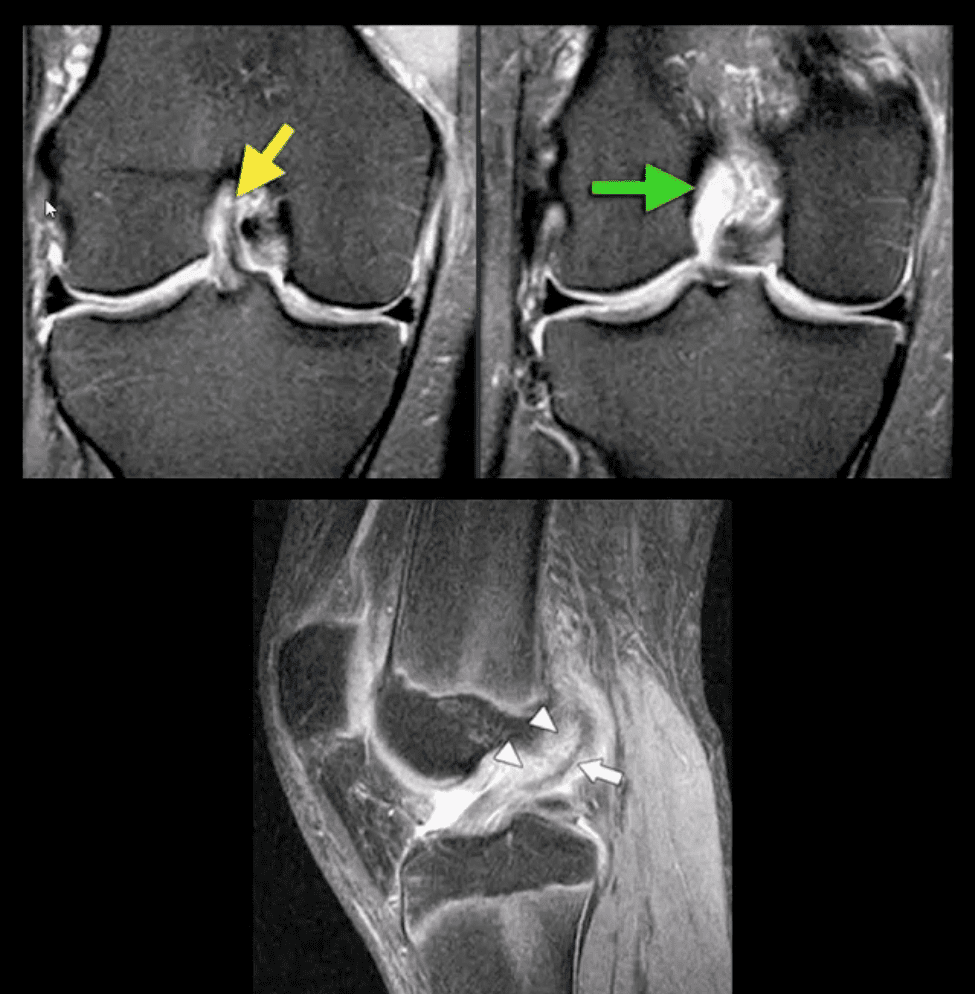
Primary signs of ACL tear: non-visualization of ACL (above green arrow), loss of its axis along the Blumensaat line (above triangle heads), wavy appearance and substance tear (above white arrow) or edema and cloud-like indistinctness (above yellow arrow)
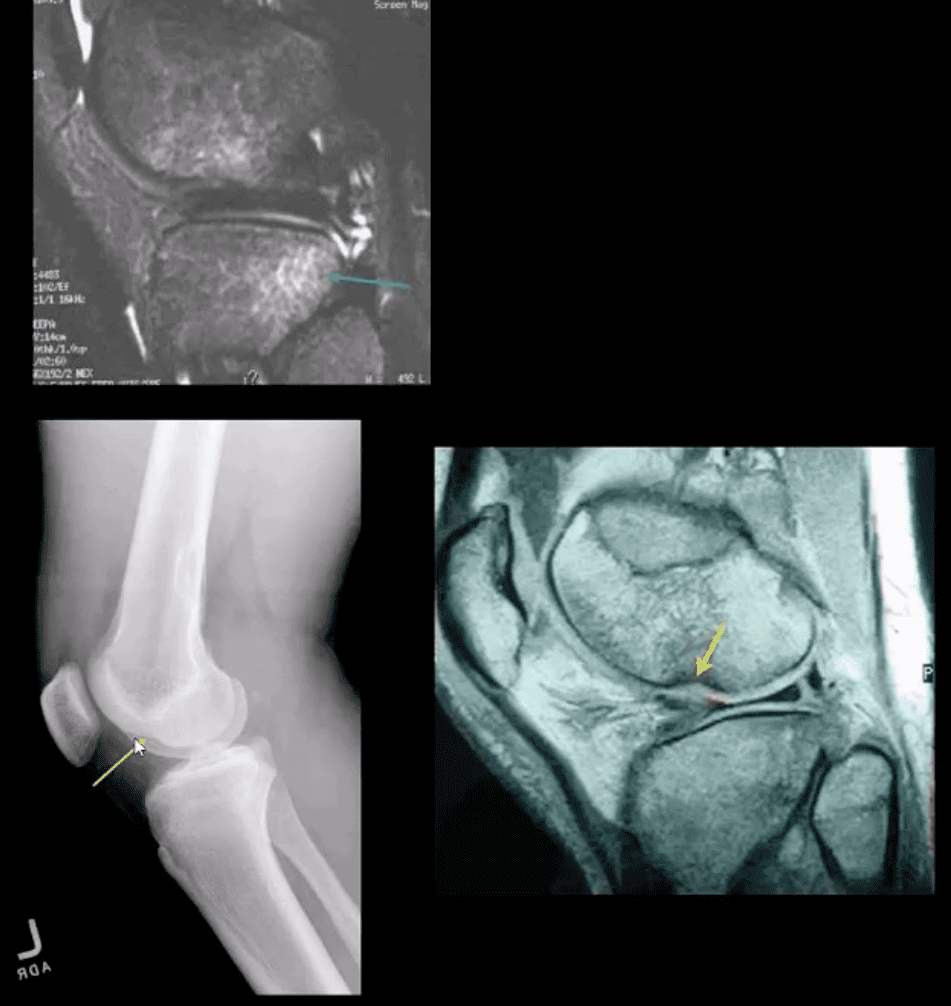
Reliable Secondary Signs of ACL Tear
May be observed on the radiographs and MRI
Segond avulsion fracture (80% specificity for ACL tear) (next slide)
Deep femoral notch sign indicating osteochondral fracture (above bottom images) and
Pivot -shift bone marrow edema in the posterolateral tibial condyle d/t external rotation and often valgus impact by the lateral femoral condyles (above top image)
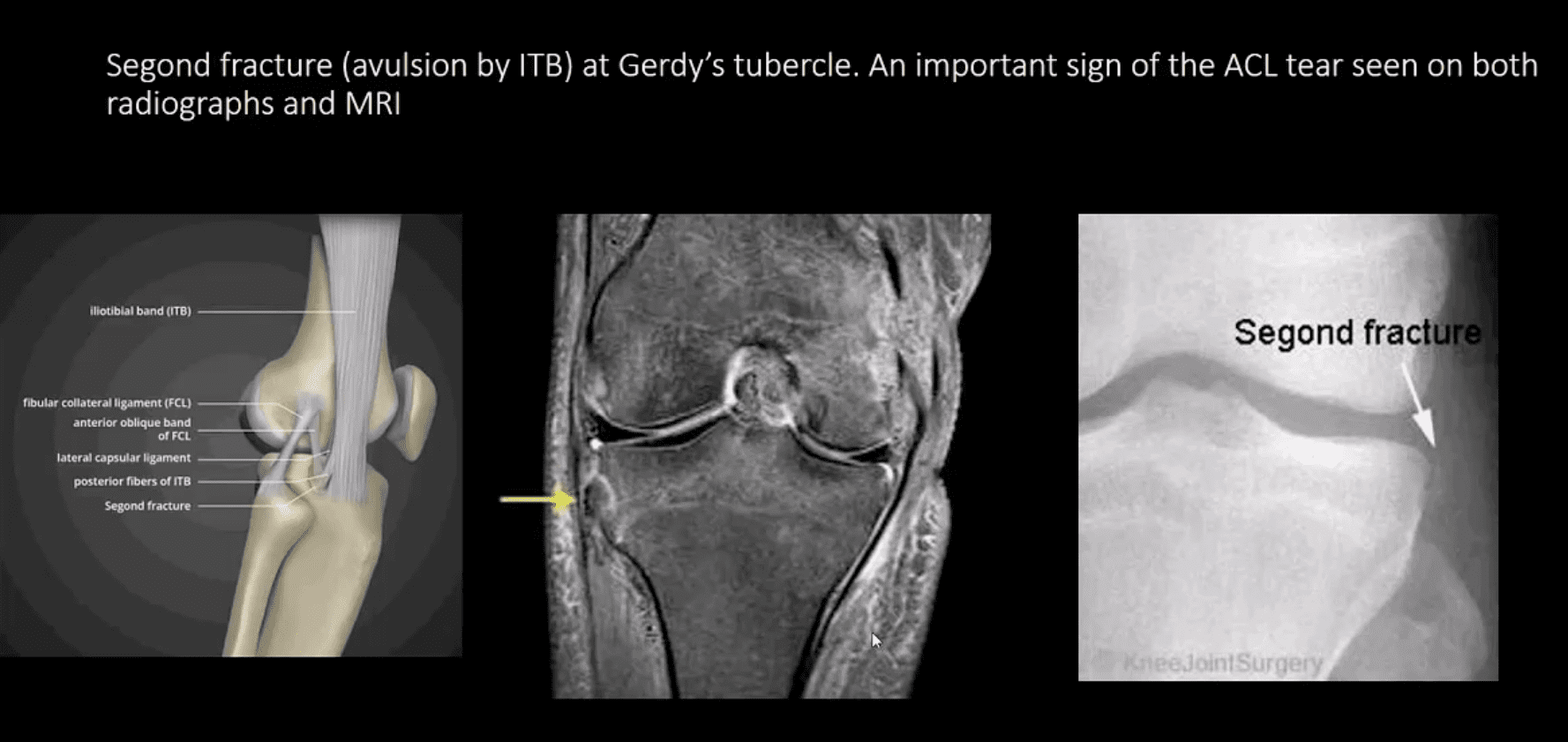
Segond Fracture (Avulsion by ITB)
Segond fracture at Gerdy’s tubercle. A vital sign of the ACL tear seen on both radiographs and MRI
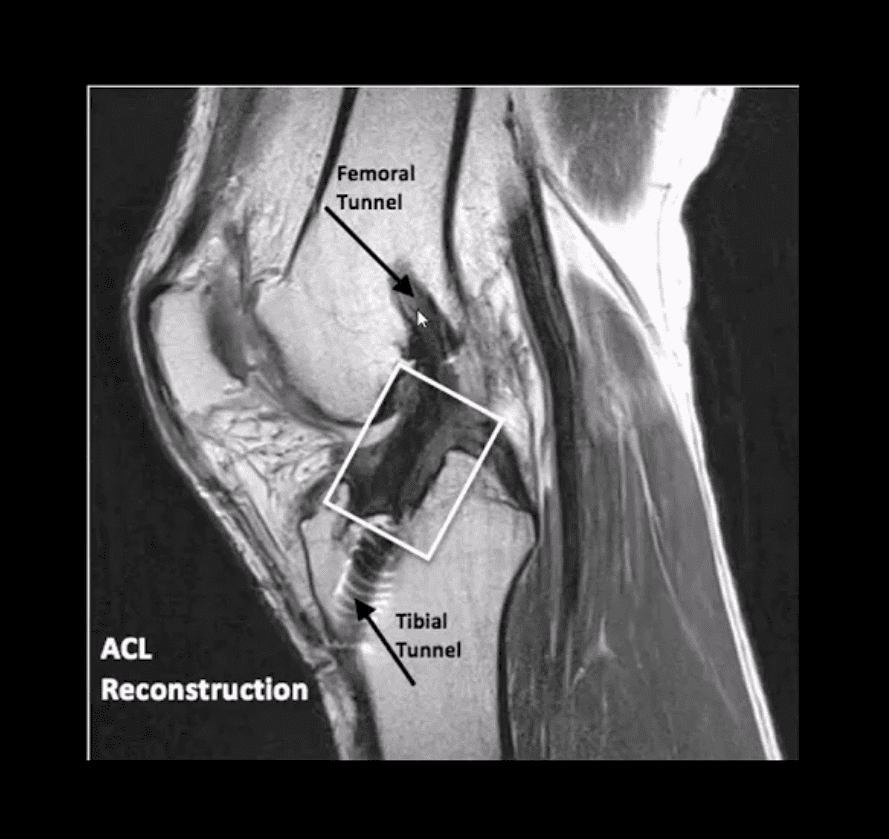
Management of ACL Tears
In acute cases, usually operative using cadaveric or autograft (patella ligament or hamstring) ACL reconstruction
Complications: graft tear, instability and premature DJD, joint stiffness d/t lack of postoperative rehab or gaft shortening. More rare, infection, a formation of intraosseous synovial cysts, etc.
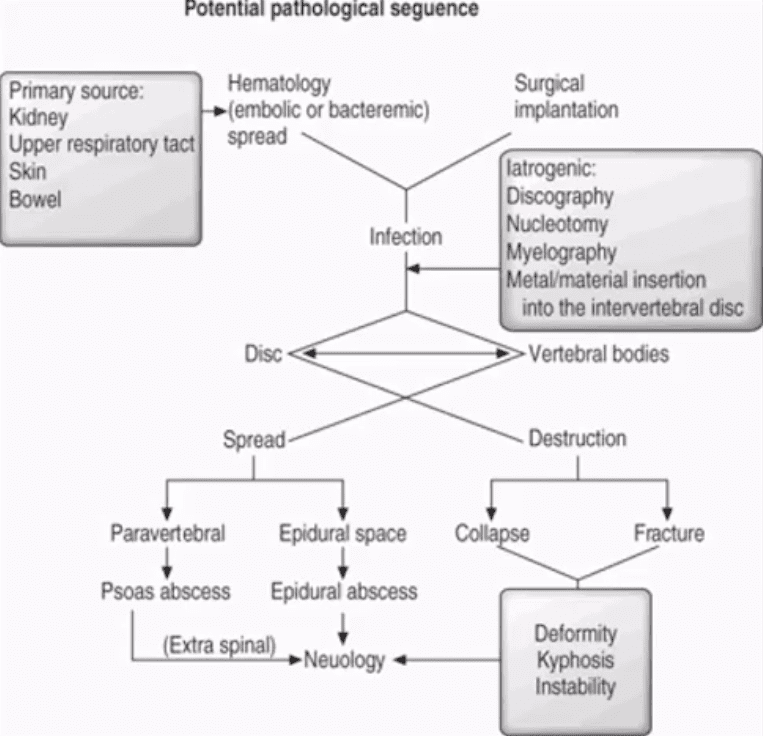
aka Spondylodiscitis and vertebral osteomyelitis overall are relatively infrequent and may present with bimodal distribution: children and adults >50’s
Occasionally considered as two separate entities due to variations in the blood supply of pediatric vs. adult spines
Risk factors/causes: distant site of infection in the body (25-35%), e.g., oropharynx, urogenital infections, bacterial endocarditis, indwelling catheters, florid skin infections furunculosis/abscess, etc.
Iatrogenic:�operative (e.g., discectomy) interventional or diagnostic/therapeutic procedures
Penetrating trauma
Immunocompromised patients
Diabetics
Malnourished patients or patients with low protein
IV drug users
Chronic disease patients, cancer patients etc.
Potential Pathological Sequence
Clinical Presentation
Back pain with or w/o high fever and other “septic” signs. Fever may only present in 50% of children
Exacerbation of pre-existing back pain in post-surgical cases
Neurological complications in advanced cases of vertebral destruction and epidural abscess
Meningitis, septicemia etc.
Labs: Blood tests are unspecific, may or may not indicate elevated ESR/CRP, WBC
Diagnostic imaging is important but
If clinical suspicion is strong, prompt I.V. antibiotics are needed to prevent serious complications
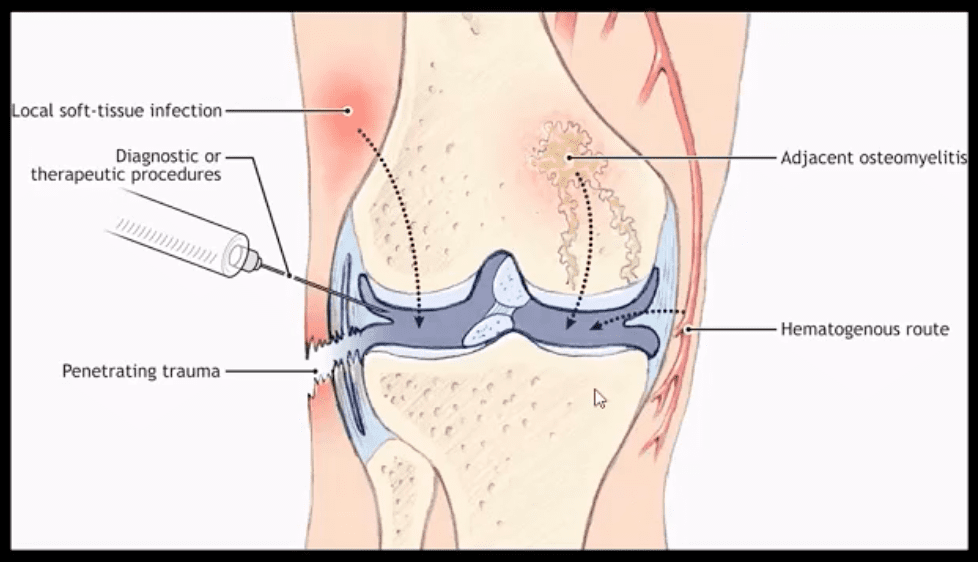
Routes of Infection
Infection routes to the spine are similar to bone in general
3-distinct routes:
1) Hematogenous spread as bacteremia (most common)
2) Adjacent site of infection (e.g., soft tissue abscess)
3)Direct inoculation (e.g., iatrogenic or traumatic)
M/C organism Staph. Aureus
Mycobacterium TB (tuberculous spinal osteomyelitis) aka Pott’s disease can be presented in cases of re-activated or disseminated pulmonary TB
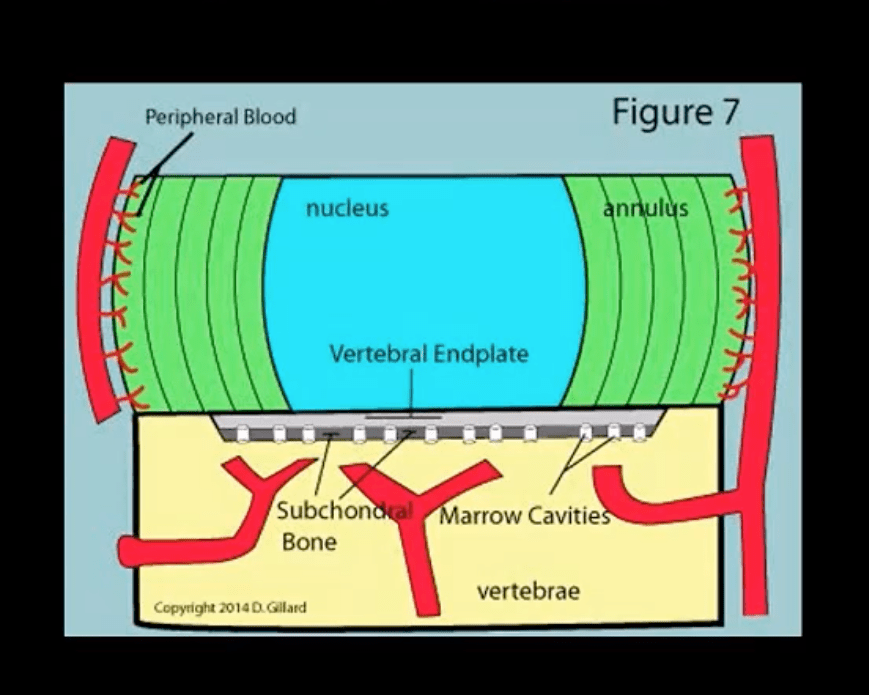
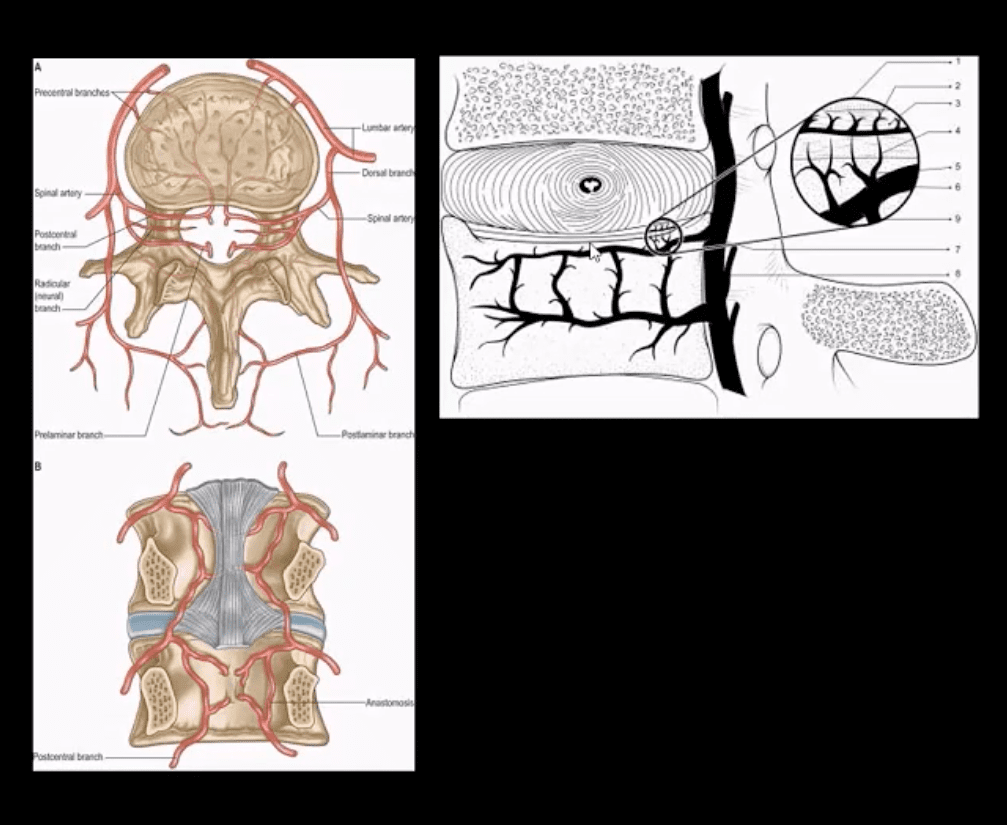
Mechanisms of Spinal Infection
May vary depending on the patients’ age
In children, the IVD receives direct blood supply and can be infected directly spreading to adjacent bone and causing spondylodiscitis
In Adults
The disc is avascular
Pathogens invade adjacent vertebral end-plates via end-arterial supply of the vertebral body that may facilitate infection due to slow, turbulent flow
Organisms may then quickly gain access to disc substance rich in nutrients (discitis) often w/o significant initially visible destruction to the bone
Thus, one of the earliest rad. findings of spinal infection or sudden reduction of disc height
Later end-plate irregularity/sclerosis may develop, subsequently affecting the entire adjacent vertebral bodies
Diagnostic Imaging
Initially, in most cases of MSK complaints, radiography is the 1st imaging step
Initially, X-radiography is often unrewarding and may appear unremarkable for 7-10 days or presents with some subtle soft tissue changes (e.g., obscuration of Psoas shadows etc.)
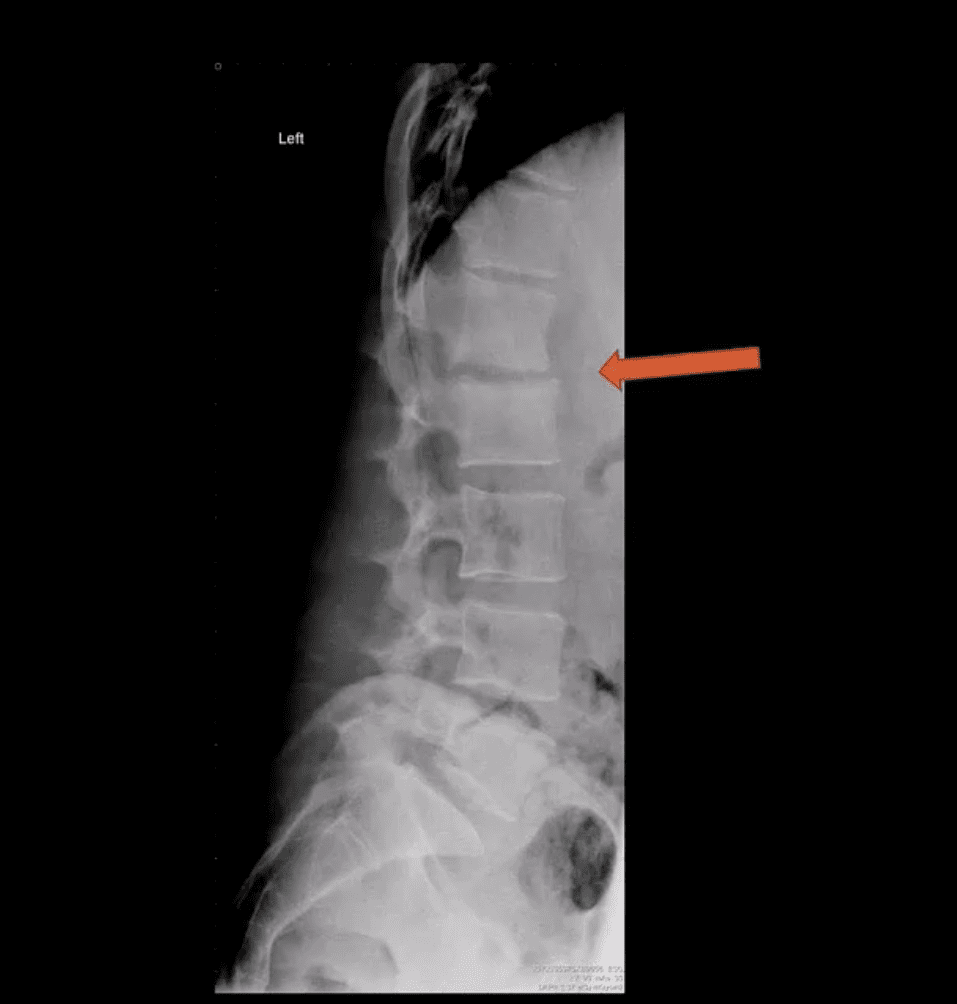
Some of the earliest x-ray signs of pyogenic spondylodiscitis: sudden reduction of disc height (above arrow) during initial 7-10 days
Subsequently (10-20 days) some end-plate irregularity and adjacent sclerosis may be noted
In more advanced cases, subsequent vertebral destruction and collapse may occur
N.B. Reliable feature to DDx between spinal infection and metastasis is the preservation of disc height in the latter
Note:�sudden disc narrowing with no appreciable spondylosis (above the first image) is suspicious for infection (discitis)
MRI +C is required to evaluate suspected infection
N.B. 50-60% of pyogenic spondylodiscitis occur in the lumbar region
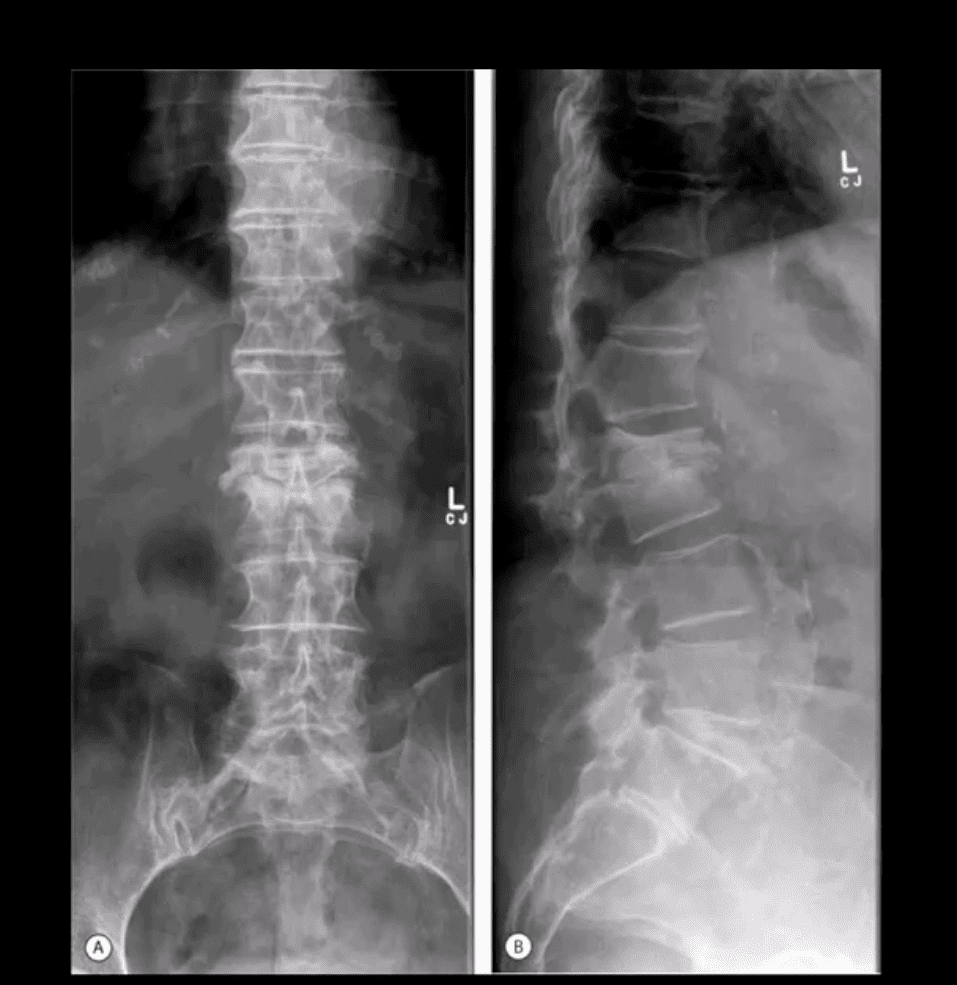
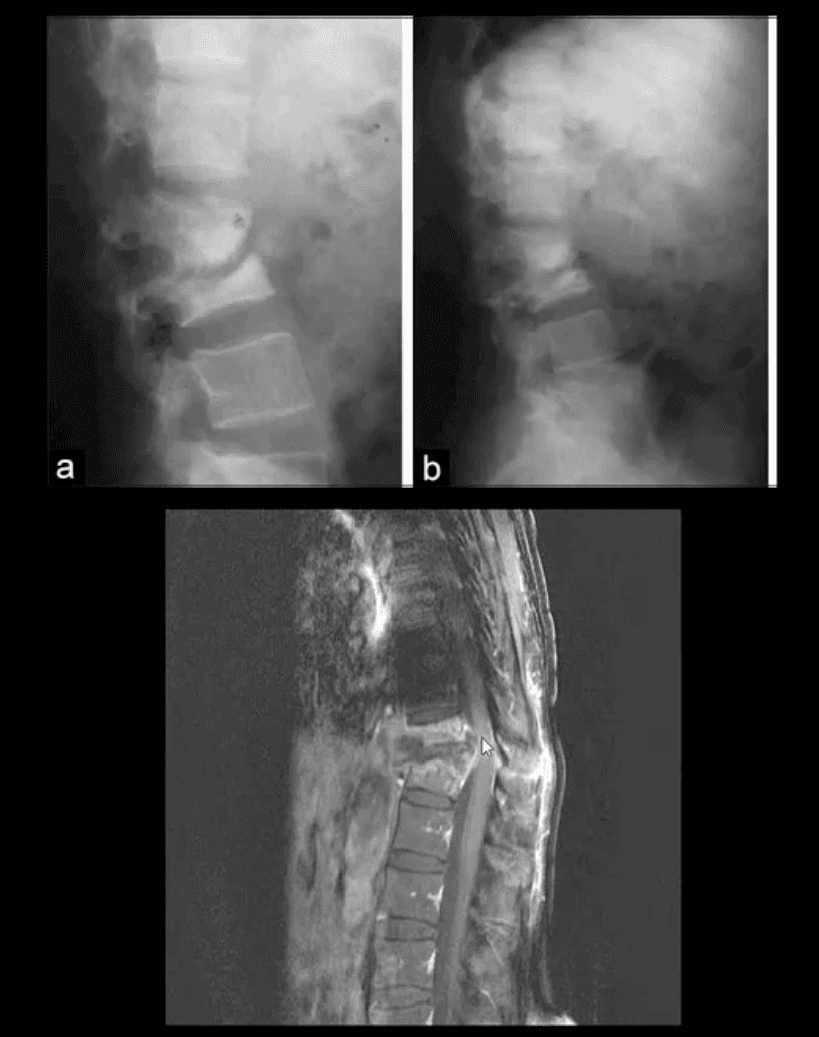
AP & Lateral Lumbar Radiographs
Note severe disc narrowing and adjacent vertebral body destruction at L1-L2 in a 68 -y.o.-female with a known Hx of type 2 DM
Additional imaging modalities should be used to support the Dx
Final Dx: Pyogenic Spondylodiscitis
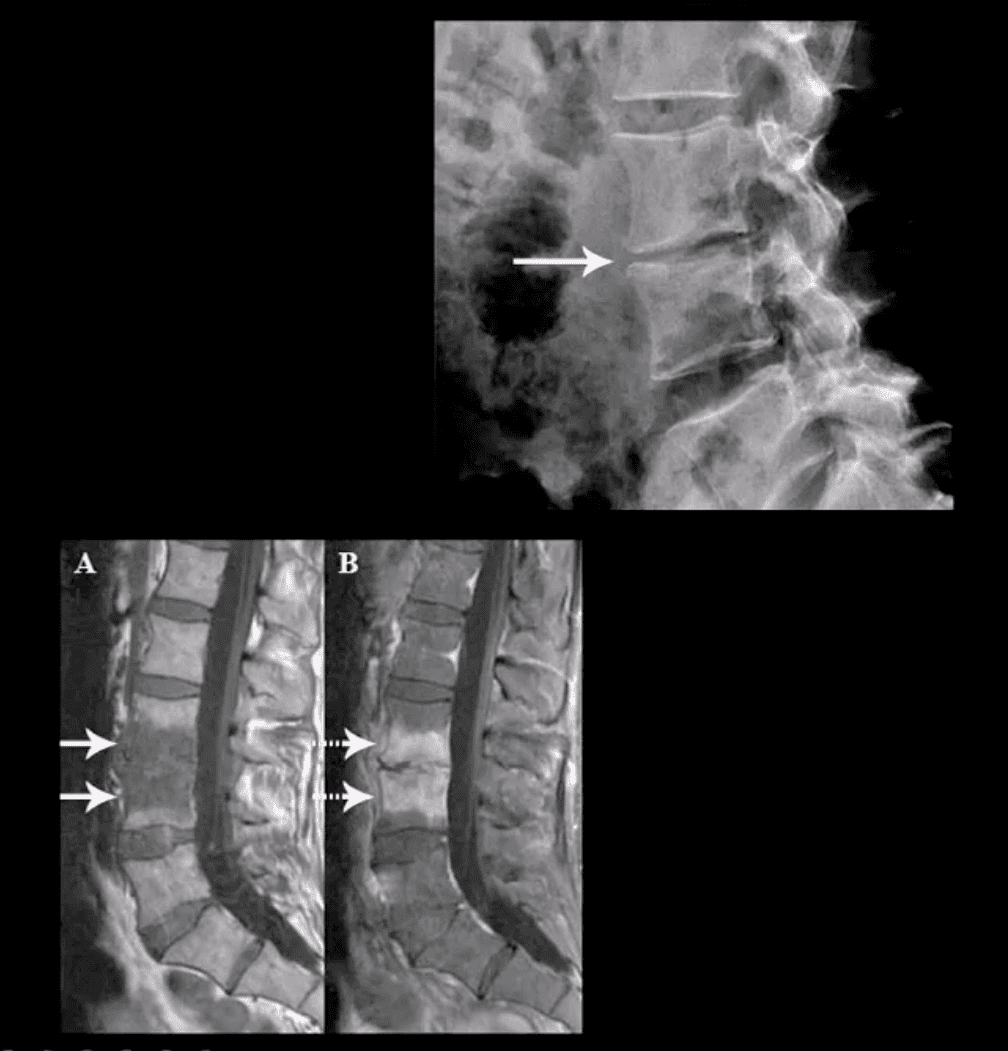
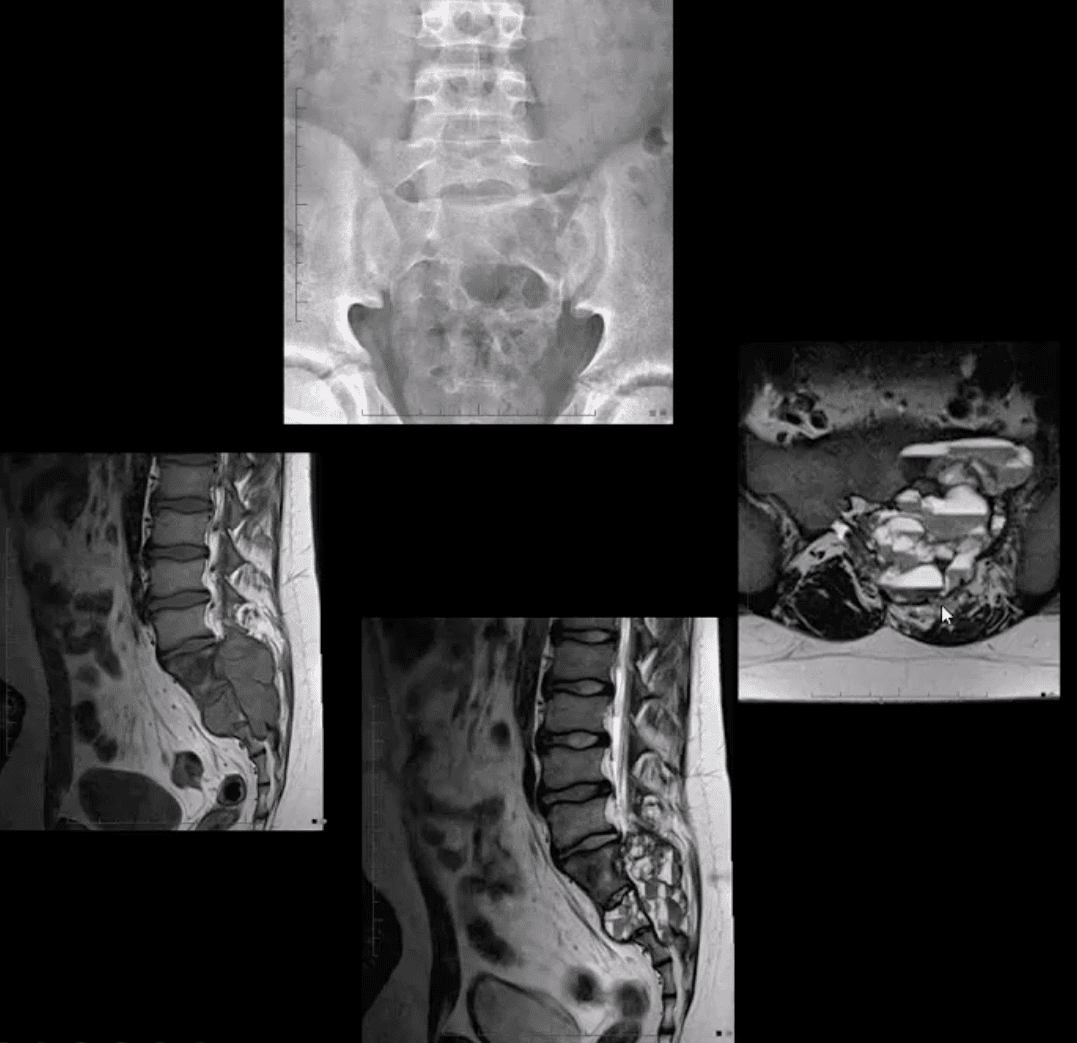
Sagittal T1 & T2 MRI
Weighted MRI slices of a patient who had laminectomy at L4
MR imaging with gad contrast is the modality of choice for Dx of spinal infection
Early septic changes affecting the disc and adjacent vertebral end-plates are readily demonstrated as a low signal on T1 and high T2/STIR d/t edema and inflammation
T1 FS +C gad images show avid enhancement of the lesion due to granulation tissue around the phlegmon. Peripheral enhancement is also characteristic of an abscess.
Epidural extension/abscess can also be successfully detected my MRI
N.B. 50% of epidural abscess cases present with neurological signs
STIR & T1 FS +C Gad Sagittal MRI
Marked septic collection and edema affecting L4-5 disc and vertebral body with some epidural extension and paraspinal soft tissue edema. Avid contrast enhancement is noted surrounding low signal foci within the bone and disc tissue, some gad. Enhancement is noted in posterior paraspinal muscles and dural spaces
Management: Dx of spondylodiscitis requires prompt I.V antibiotics. If instability and neurological complications develop referral to a Neurosurgeon is required
MRI Unavailable or Contraindicated
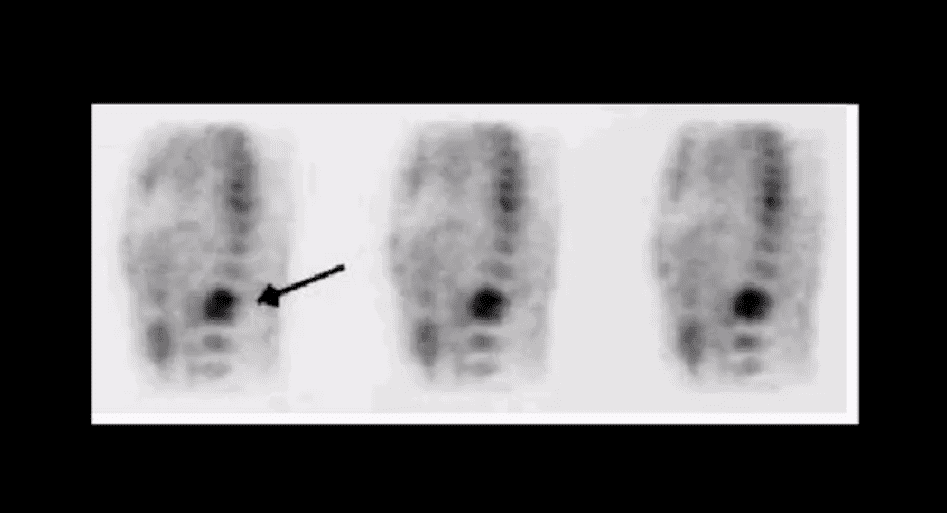
Bone scintigraphy is very sensitive but non-specific for spinal infection but overall is of great value d/t higher sensitivity than x-rays and relatively low cost.
An area of increased flow with radiopharmaceutical uptake is characteristic but not specific sign of spondylodiscitis
If neurological signs are present and MRI is contraindicated than CT myelography may be used
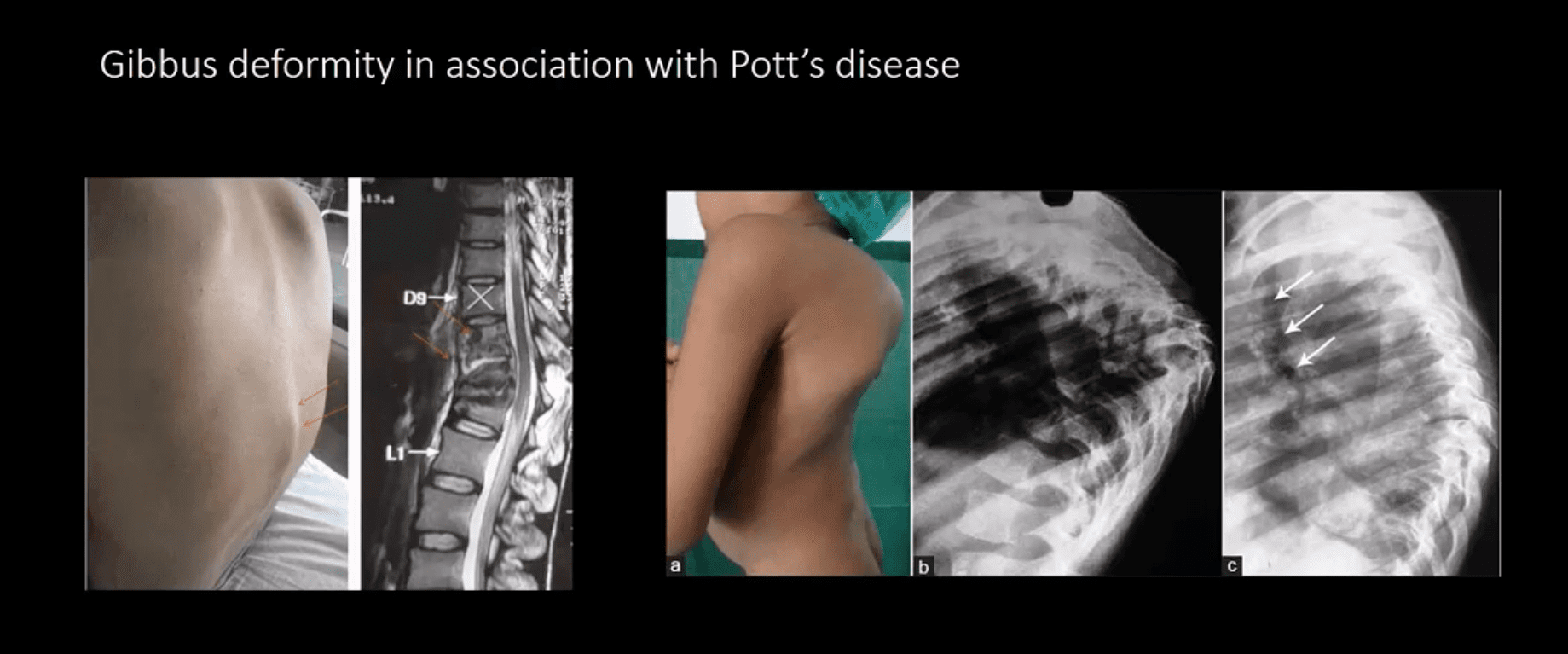
TB Osteomyelitis aka Pott’s Disease
TB osteomyelitis is increasing d/t HIV and other immunocompromised states. Extrapulmonary TB m/c affects the spine and especially the thoracic spine (60%)
Radiographic Pathology:�TB bacillus infects the vertebral body and often spreads subligamentously. “Cold” paraspinal abscess collection may develop and spreads along fascial planes, e.g., Psoas abscess. Disc spaces are preserved until v. late and skip areas are noted helping to DDx TB from pyogenic infection. Severe vertebral destruction aka Gibbus deformity may develop (>60-degree sometimes) and may become permanent. Neurologic and many regional complications may develop
Imagingapproach:�CXR with spinal x-rays 1st step that may be unrewarding but may potentially reveal VB destruction w/o disc narrowing. CT scanning is more superior than x-rays. MRI with gad C is a modality of choice
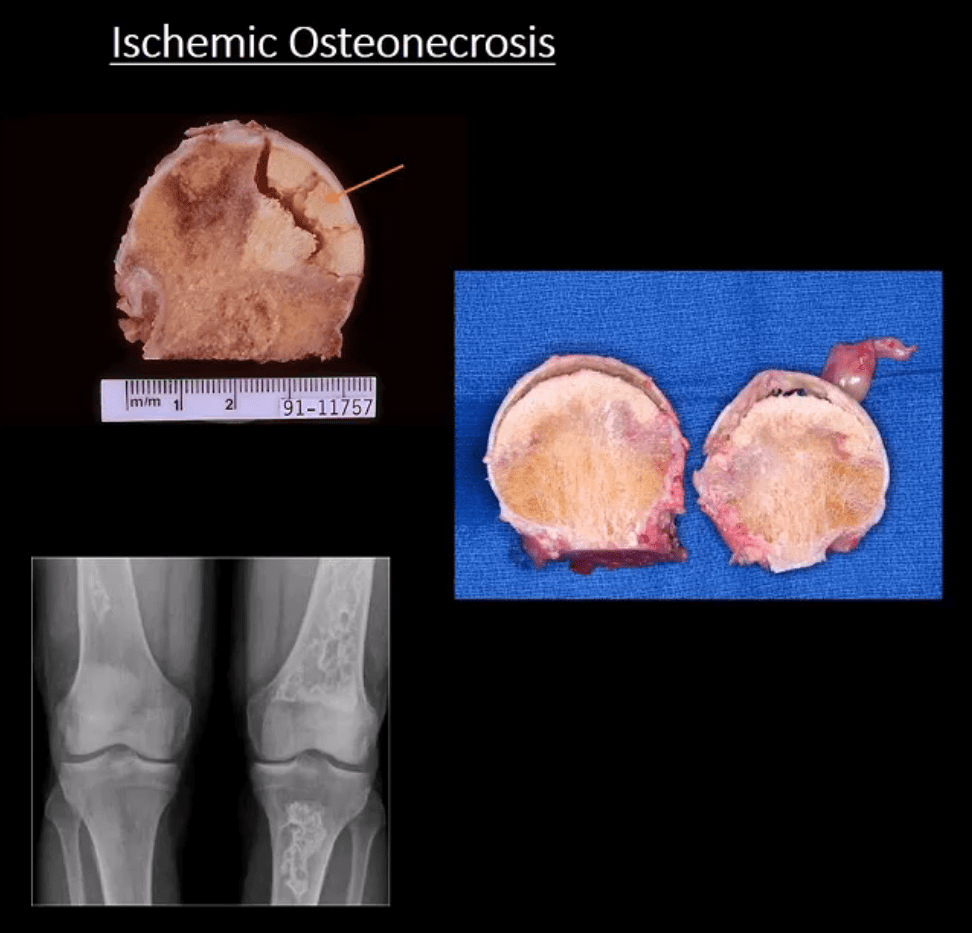
Ischemic Osteonecrosis (More accurate term) aka avascular necrosis AVN: this term describes subarticular (subchondral) bone death
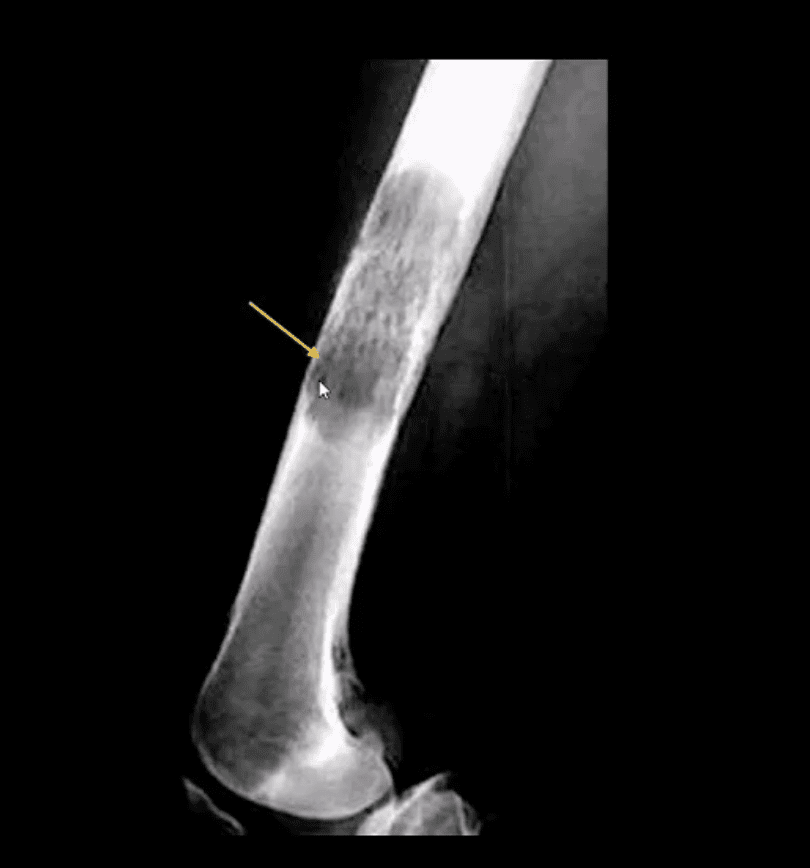
Intramedullary bone infarct: depicts osteonecrosis within the medullary cavity of the bone (above x-ray image)
Causes: m/c: trauma, systemic corticosteroids, diabetes, vasculitis in SLE. The list is long. Other vital causes: Sickle cell disease, Gaucher disease, alcohol, caisson disease, SCFE, LCP, etc.
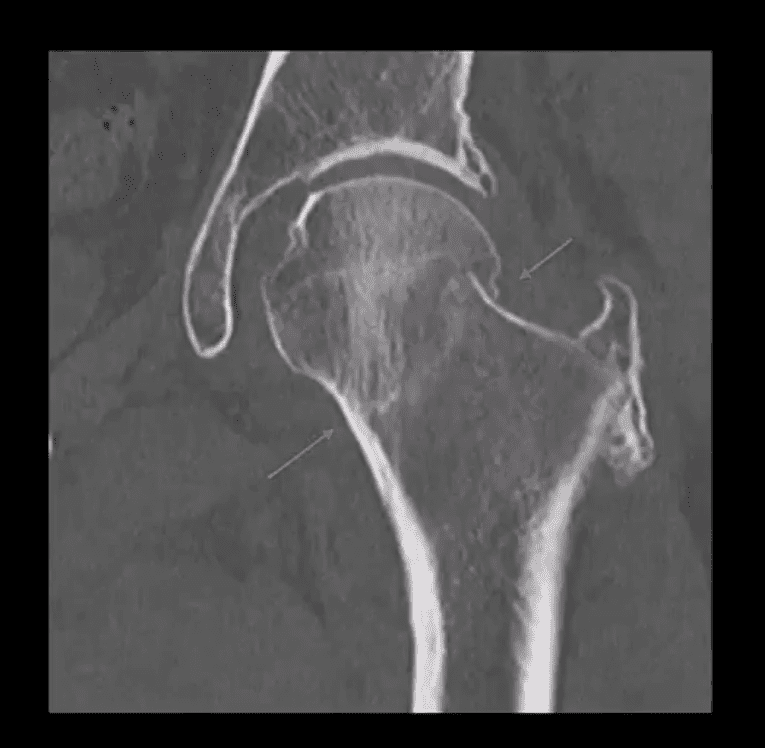
Pathology: ischemia and bone infarct with resultant devitalized center surrounded by ischemia and edema with normal bone on the outer periphery (MRI double line sign)
Sub-articular necrotic bone eventually collapses and fragments leading to progressive bone and cartilage destruction and rapidly progressing DJD
Early Dx often missed but crucial to prevent severe DJD
M/C Sites
Hips, shoulders, talus, scaphoid bone. Many peripheral idiopathic AVN sites are known by their eponyms (e.g., Kienbock aka AVN of the lunate bone, Preisier aka scaphoid AVN)
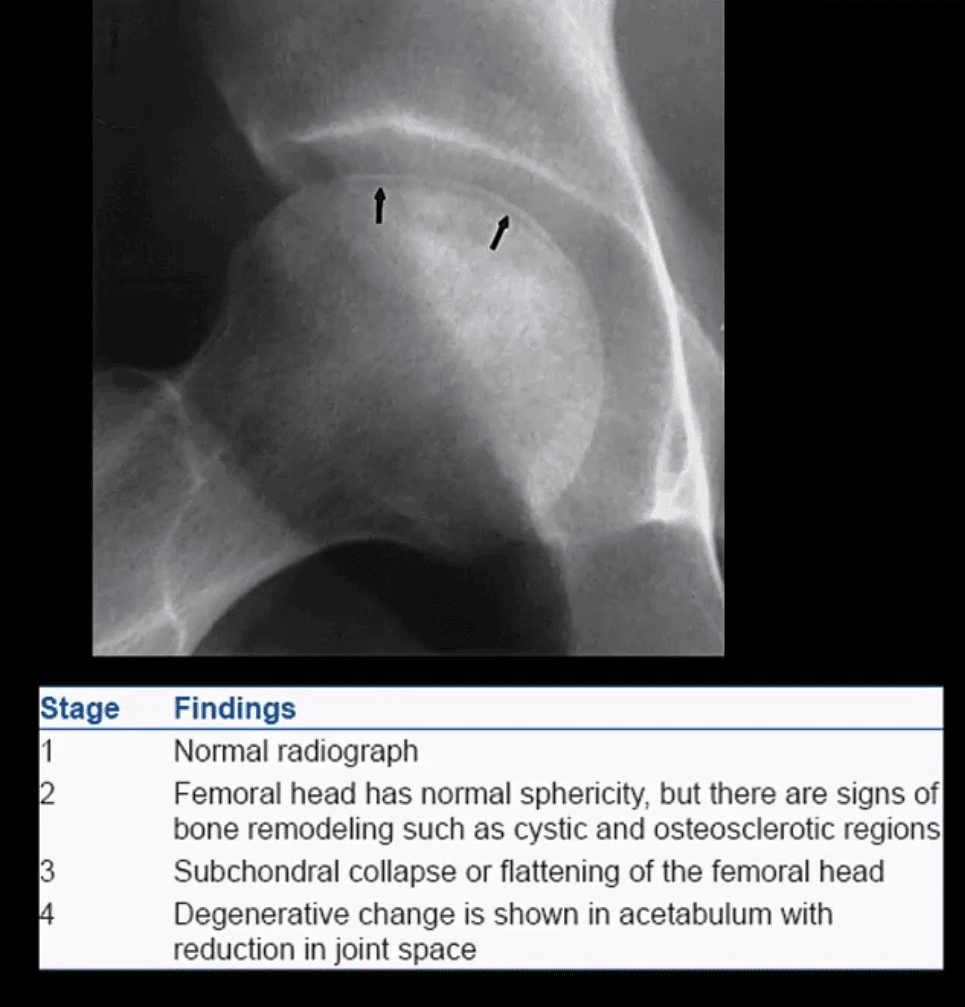
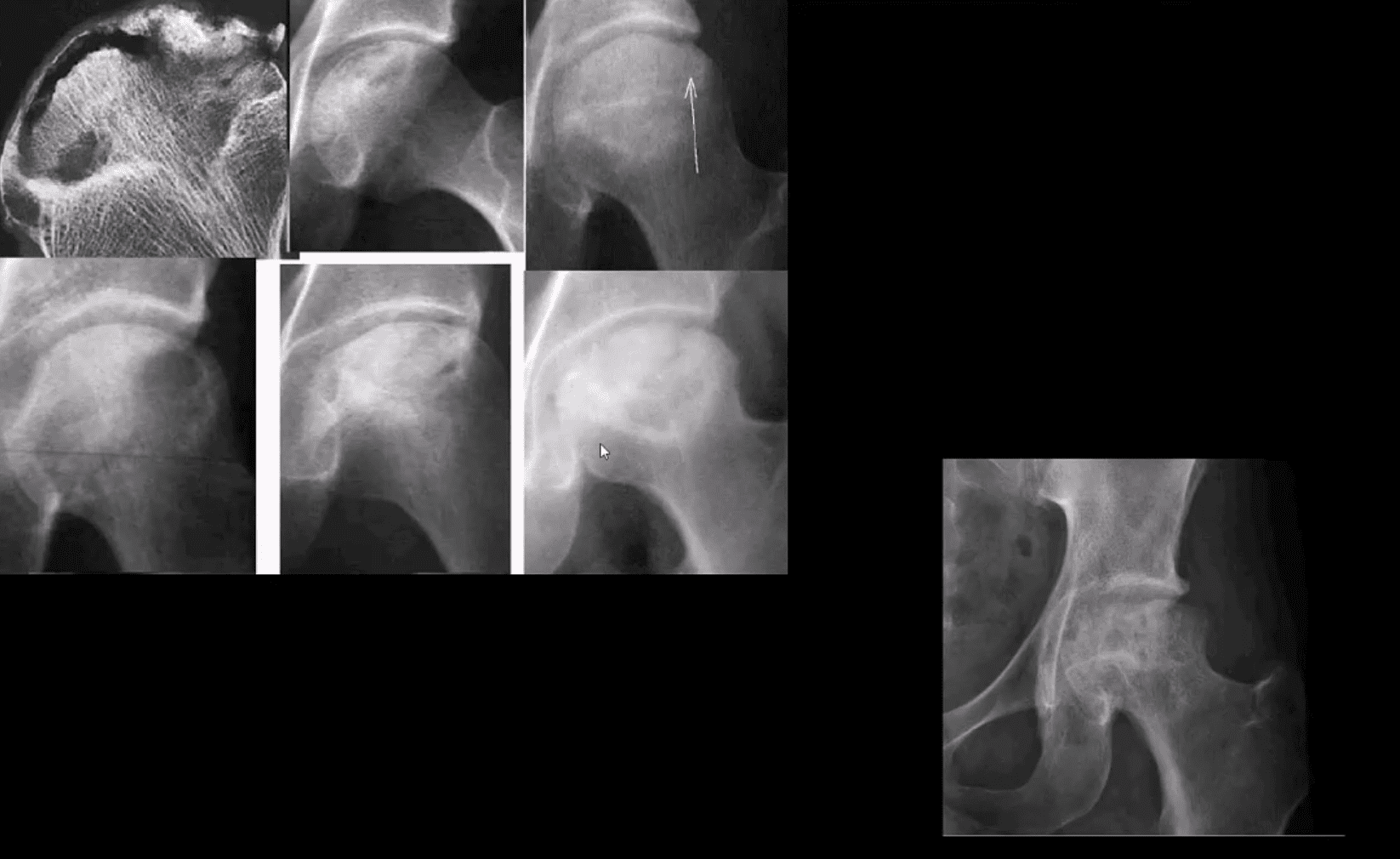
Radiography is insensitive to early AVN and may only present as subtle osteopenia
Some of the early appreciable rad features are increased patchy bone sclerosis followed by sub-articular bone collapse or “crescent sign” signifying stage-3 on Ficat classification (above)
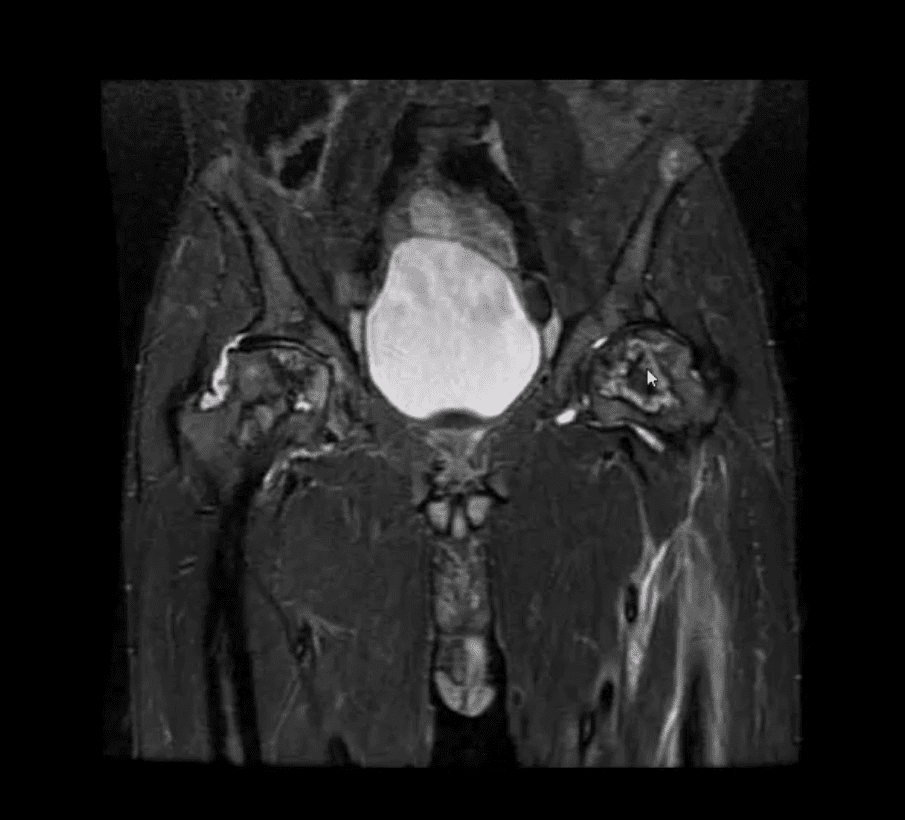
Earliest detection and early intervention can be achieved by MRI (most sensitive modality)
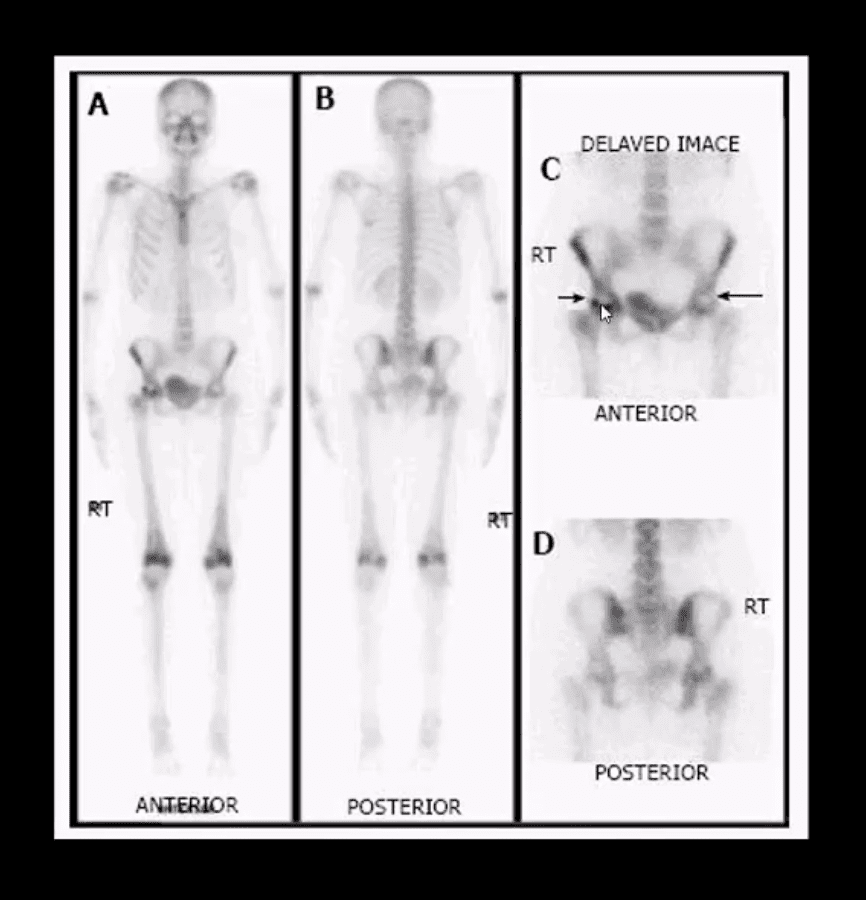
If MRI contraindicated or unavailable, 2nd most sensitive modality is radionuclide bone scan (scintigraphy)
X-ray and CT scanning are of equal value
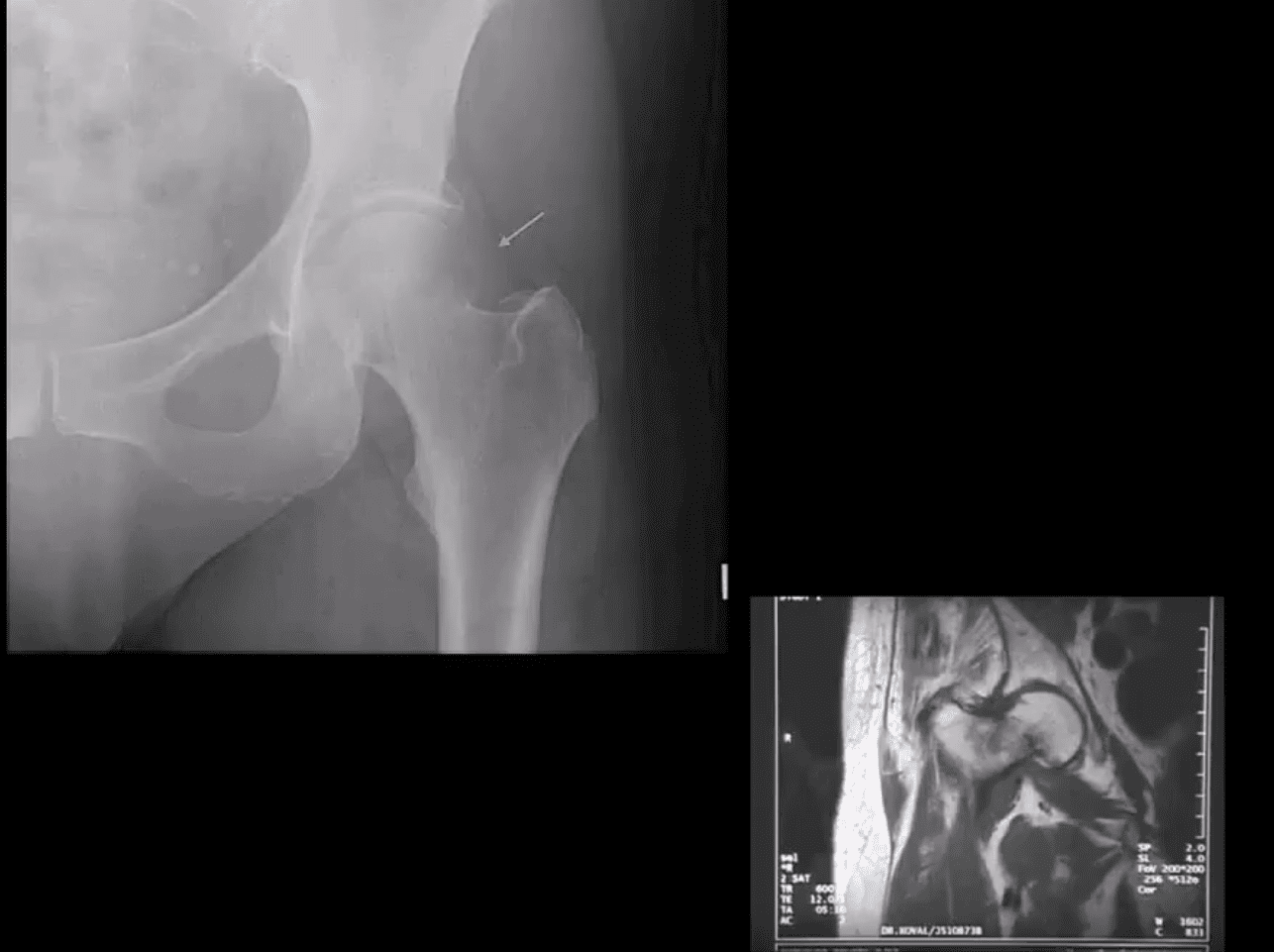
Coronal MRI Slice
Fluid sensitive, sensitive coronal MRI slice revealing bill ischemic osteonecrosis of the femoral head
MRI findings: l
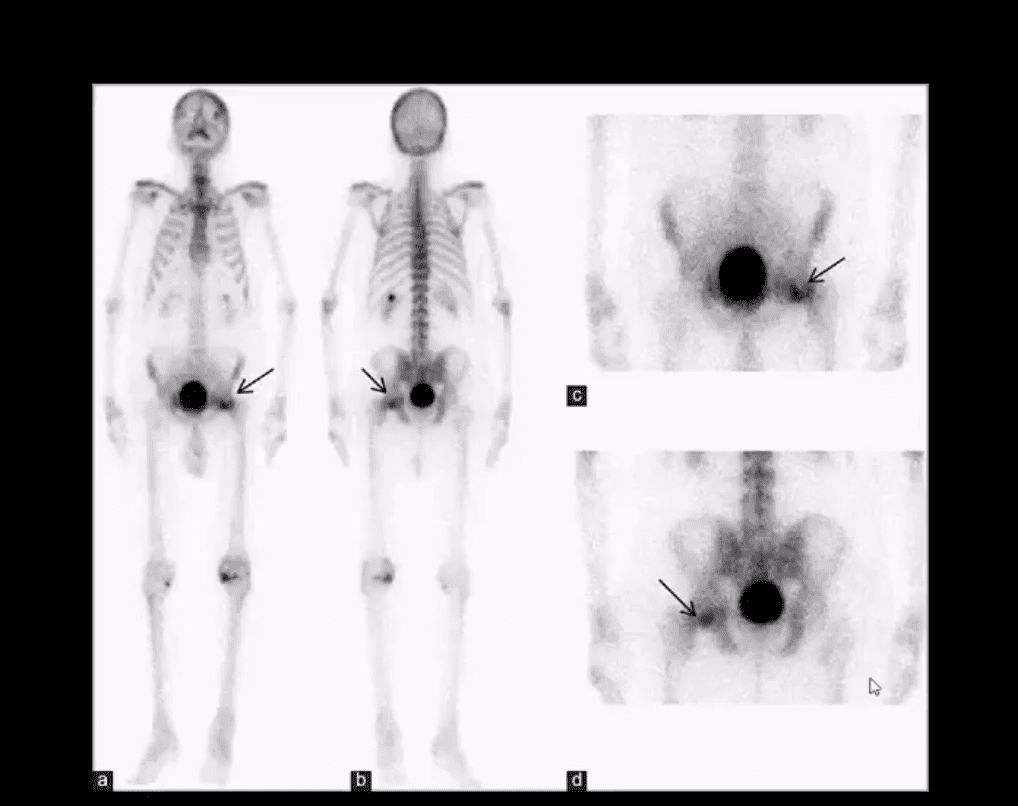
Tc99-MMDP Radionuclide Bone
Bone scan reveals a central area of photopenia (cold spot) d/t necrotic fragment surrounded by increased osteoblastic activity as increased uptake of Tc-99 MDP in the right hip
The patient is a 30-year-old female with breast cancer and chemotherapy treatment who suddenly presented with right hip pain
Radiographic Progression of AVN
Later stages present with articular collapse, subarticular cysts, increased patchy sclerosis and complete flattening of the femoral head with resultant severe DJD. Rx: THA
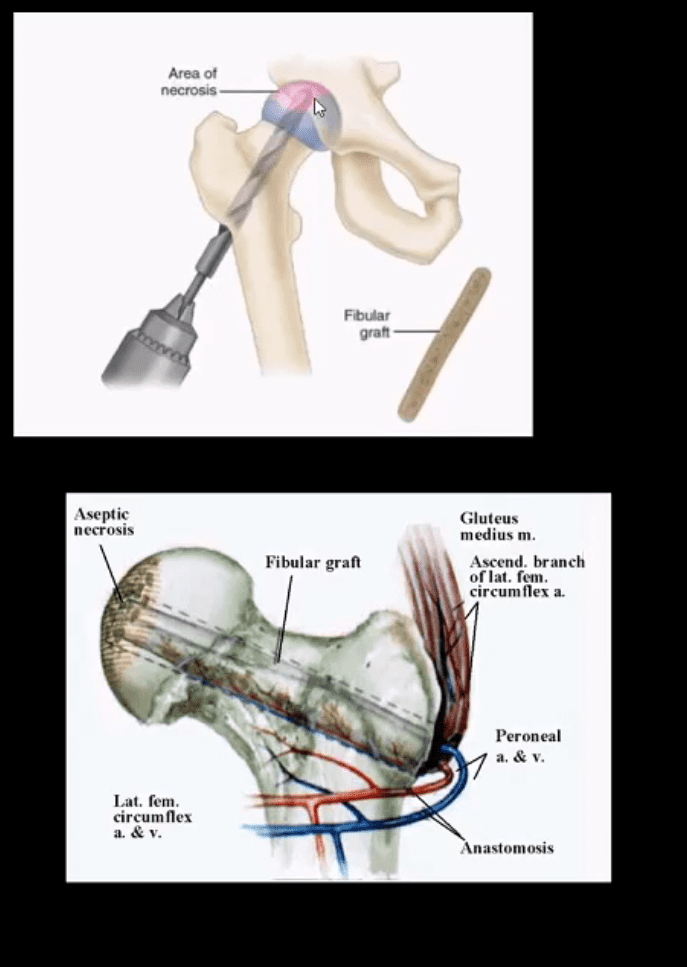
Management
Early imaging Dx with MRI or bone scintigraphy is essential
Referral to the Orthopedic surgeon
Core decompression (above) can be used to revascularize the affected bone during earlier stages but produces mixed results
Delayed changes of AVN: THA as IN severe DJD cases
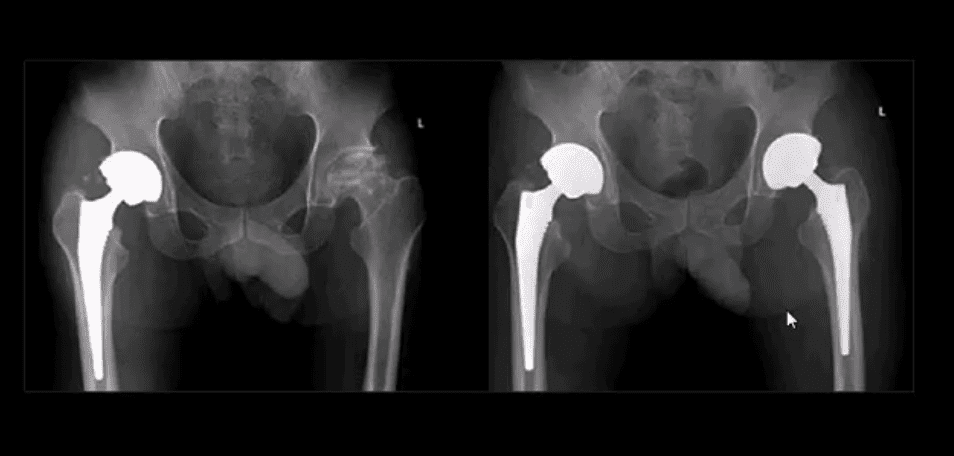
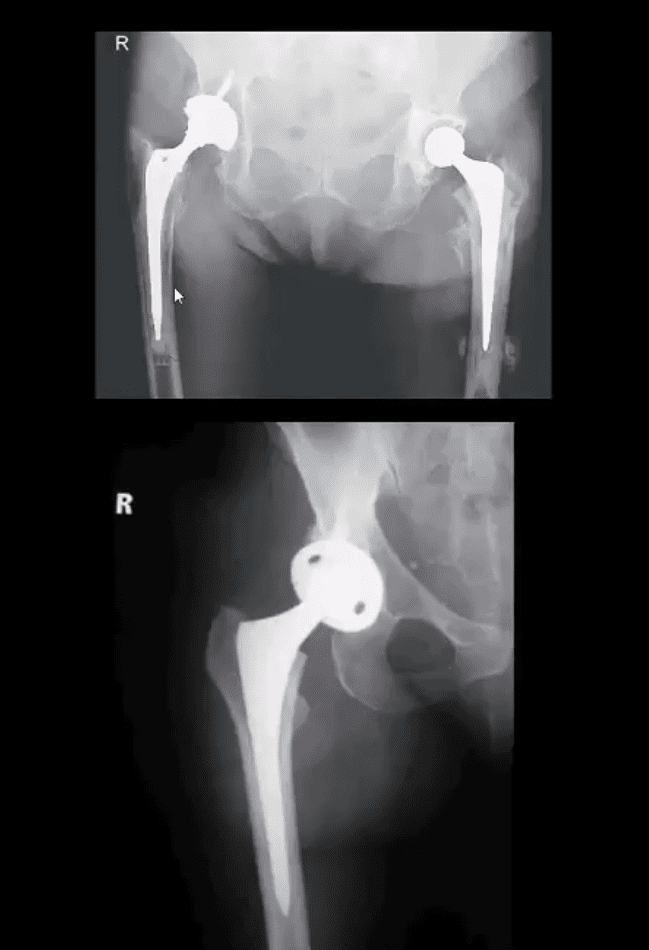
B/L THA
B/L THA in the patient with ischemic osteonecrosis of the right and later left hip
When B/L hip AVN is present, typically consider systemic causes (corticosteroids, diabetes)
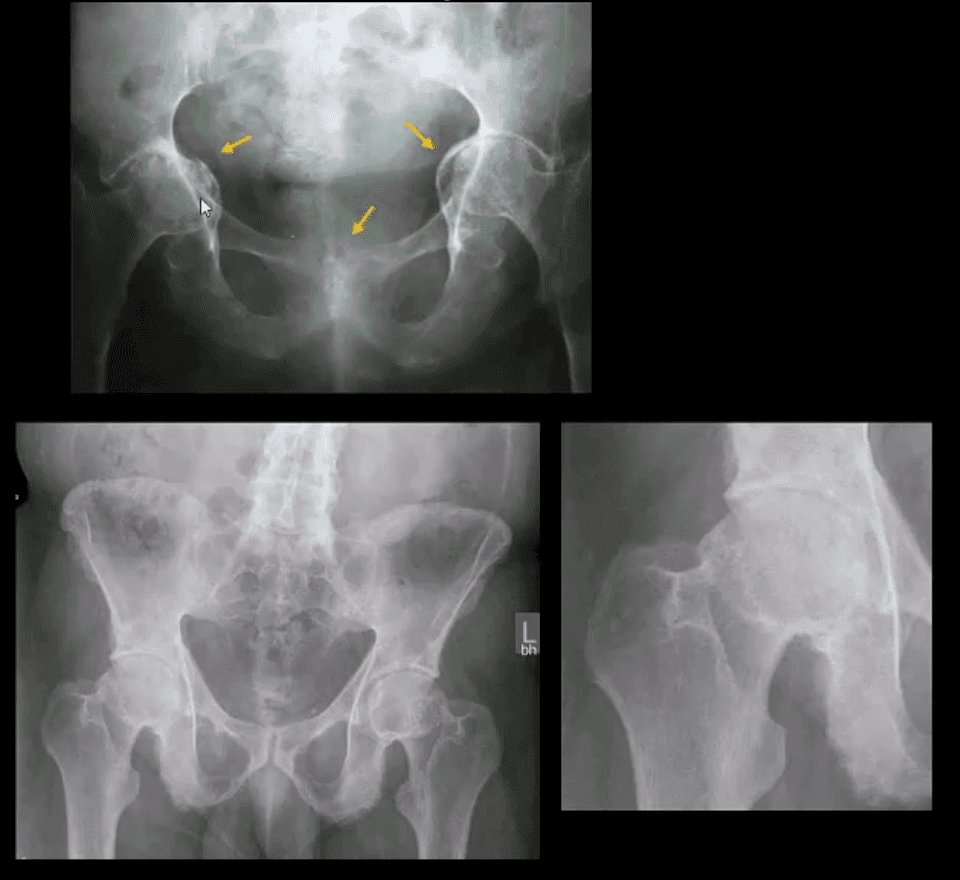
Inflammatory Arthritis Affecting the Hip
Consider common systemic inflammatory condition such as RA and AS/EnA
Hip RA may develop in 30% of patients with RA
Key features to DDx inflammatory arthritis vs. DJD is symmetrical/uniform aka concentric joint loss often leading to axial migration and Protrusion Acetabule in advanced cases
Key element between RA vs. AS: the presence of RA bone erosion w/o productive bone changes or enthesitis in AS d/t inflammatory subperiosteal bone proliferation, whiskering/fluffy periostitis (collar-type enthesitis circumferentially affecting head-neck junction)
Dx: Hx, PE, labs: CRP, RH, anti-CCP Ab (RA)
CRP, HLA-B27, RF- (AS)
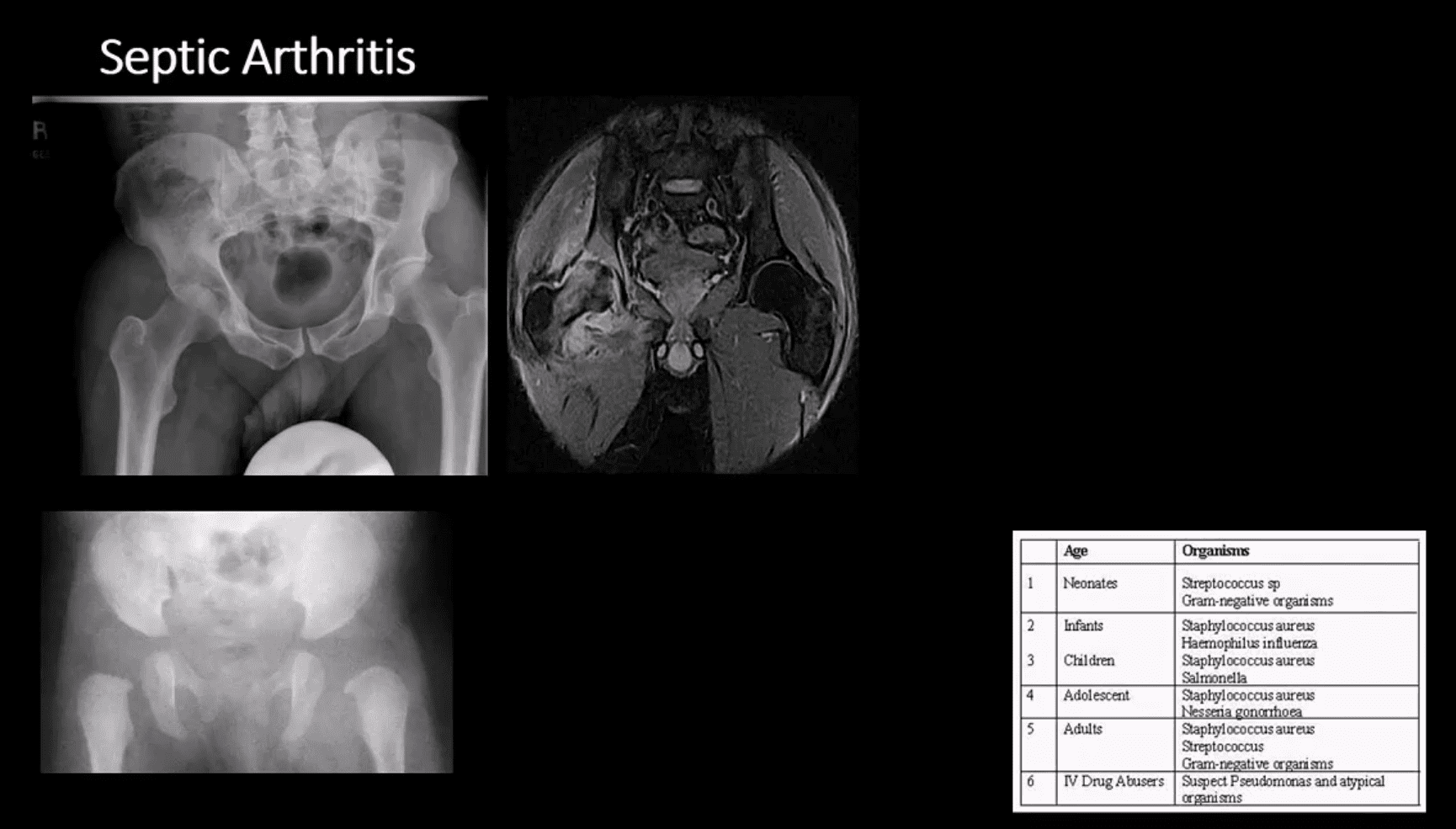
Septic Arthritis
Gonococcal infections, iatrogenic causes, I.V. drug use, and some others
Routes:�hematogenous, adjacent spread, direct inoculation (e.g., iatrogenic)
Clinically: pain and reduced ROM presented as monoarthritis, generalized signs/symptoms. CBC, ESR, CRP changes. ARthrocentesis and culture are crucial
M/C pathogen Staph. Aureus & Neisseria Gonorrhea
1st step: radiography, often unrewarding in the early stage. Later (4-10 days) indistinctness of the white cortical line at the femoral articular epiphysis, loss of joint space, effusion as a widening of the medial joint area (Waldenstrom sign)
MRI – best at early DX: T1, T2, STIR, T1+C may help with early. Early I.V. antibiotics crucial to prevent rapid joint destruction
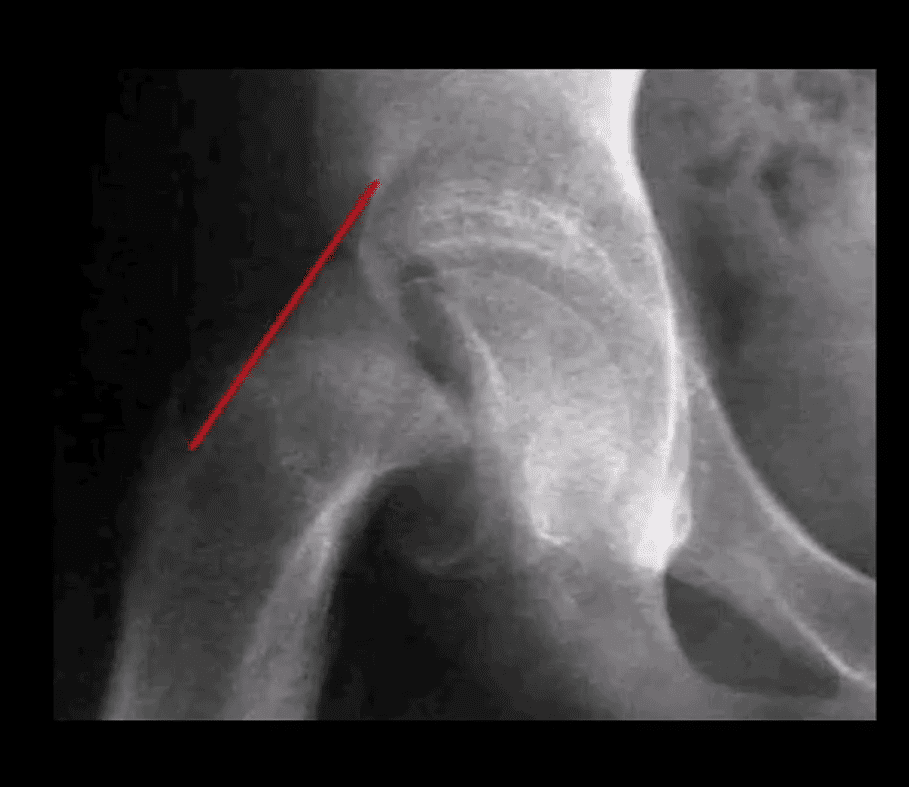
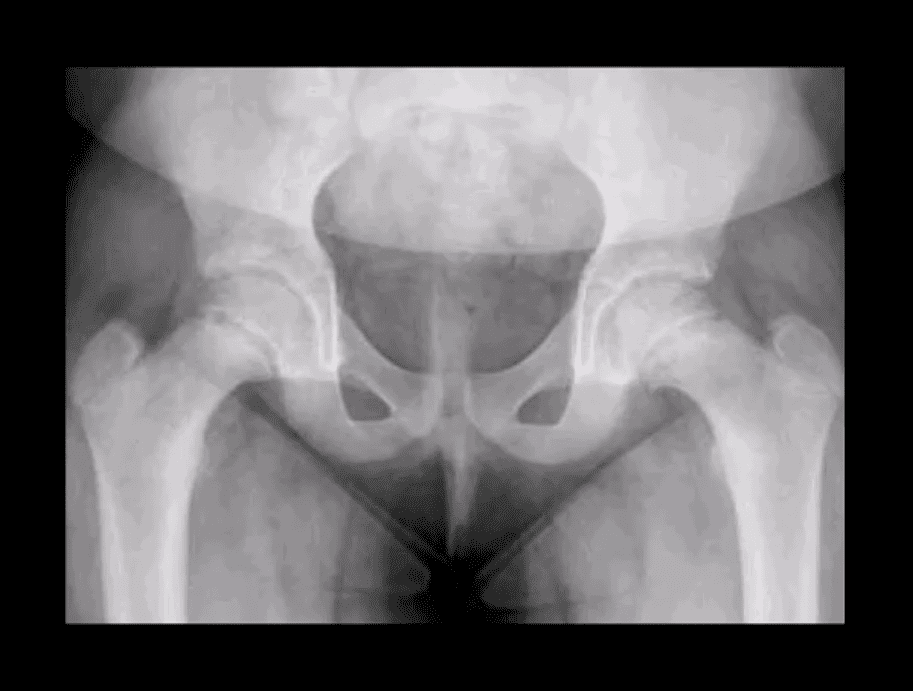
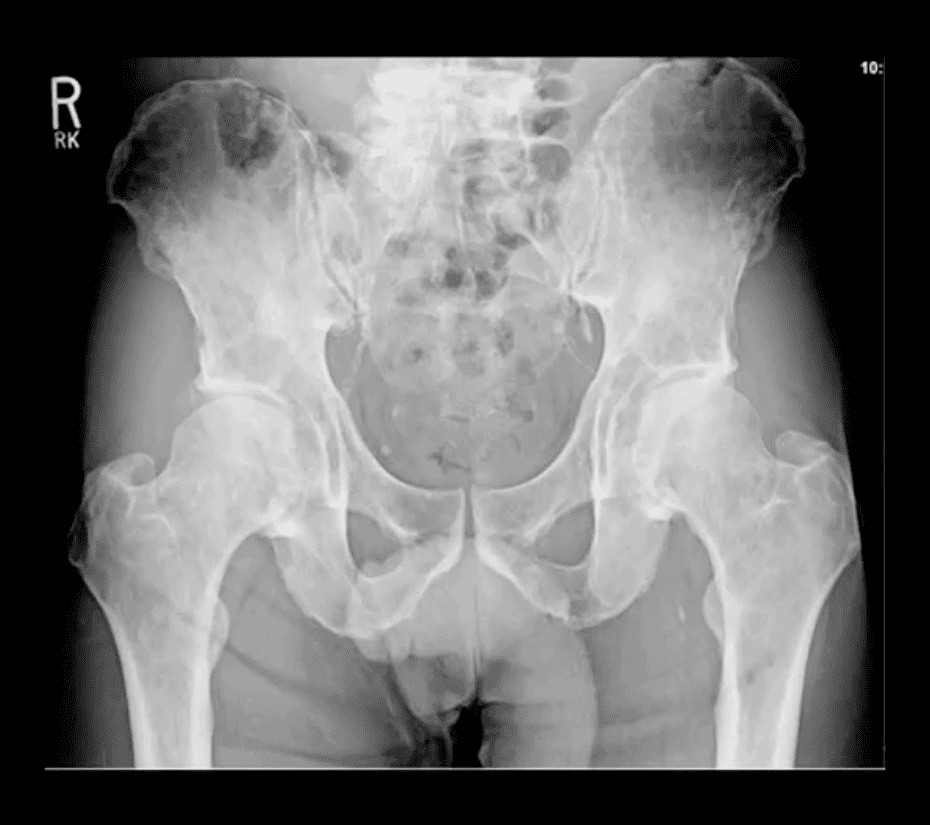
Slipped Capital Femoral Epiphysis (SCFE)
Important to diagnose but easily missed potentially leading to Ischemic Osteonecrosis of the femoral head aka AVN
Presents typically in overweight children (more often boys), age over eight years. Greater incidence in African-American boys
1st step: radiography, especially look for a widened physeal growth plate (so-called pre-slip). Later, slip and disturbed Klein’s line (above image). MRI – best modality for early Dx and early intervention
The frog lateral view often demonstrates the medial slip better than the AP view
Clinically Limping Child or Adolescent
M>F (10-18 years). African-Americans are at greater risk. 20% of cases of SCFE are B/L. Complications: AVN >>DJD
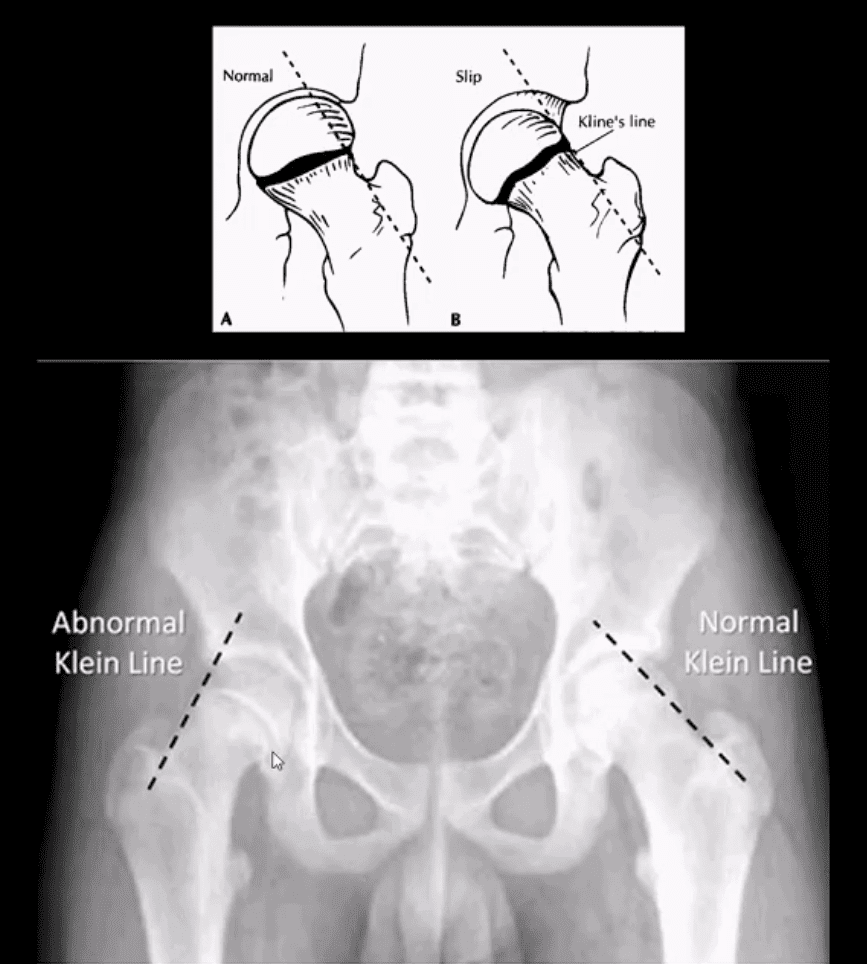
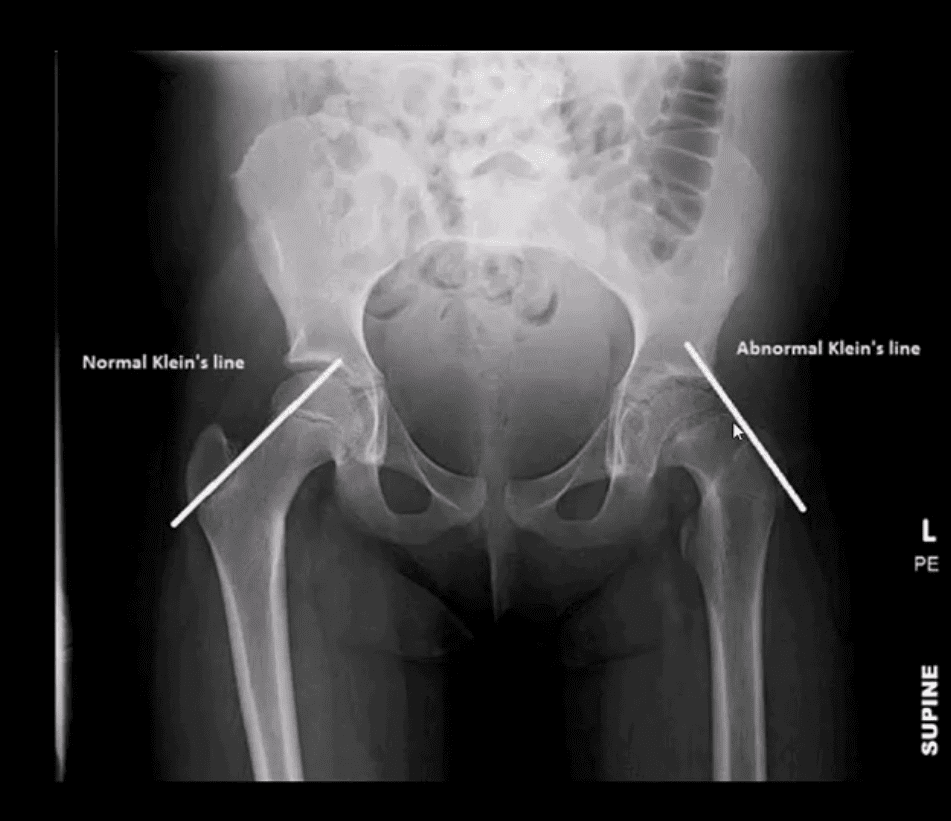
Radiography:�AP pelvis, spot, and frog leg may reveal slippage as Klein line failed to cross through the lateral aspect of the femoral head
Additional features: physis may appear widened
MRI w/o gad, is required for the earliest Dx and prevention of complications (AVN)
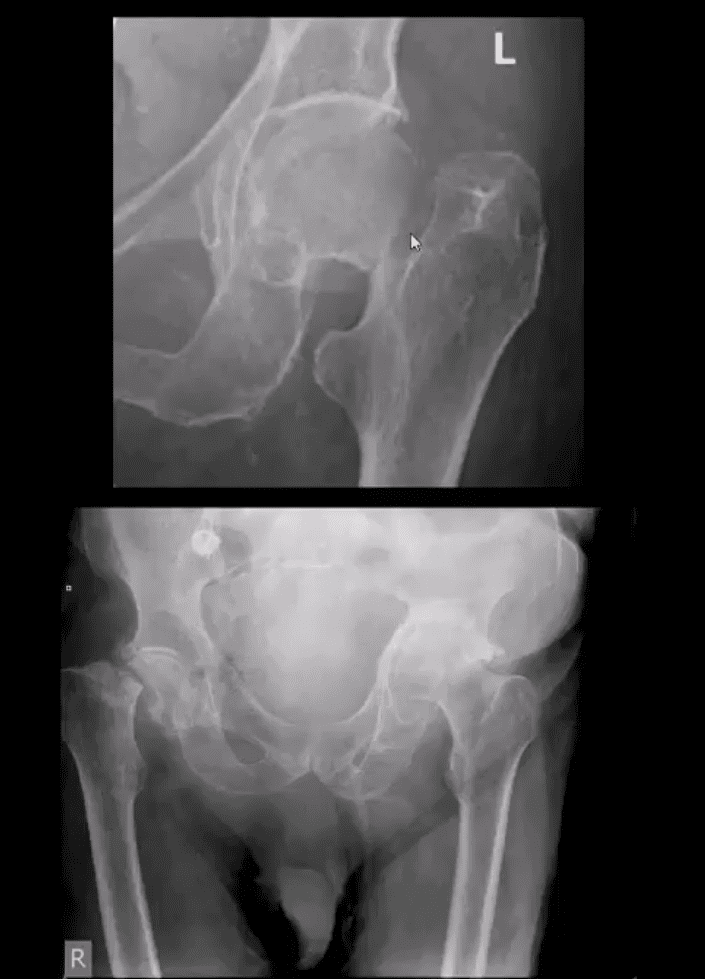
Normal and Abnormal Klein Line
Consistent with SCFE. The physis is also widened. Dx: SCFE
Urgent referral to the Pediatric Orthopedic surgeon
Subtle Changes in Left Hip
Note suspected subtle changes in the left hip that may require MR examination to confirm the Dx
Delay in care may result in major complications
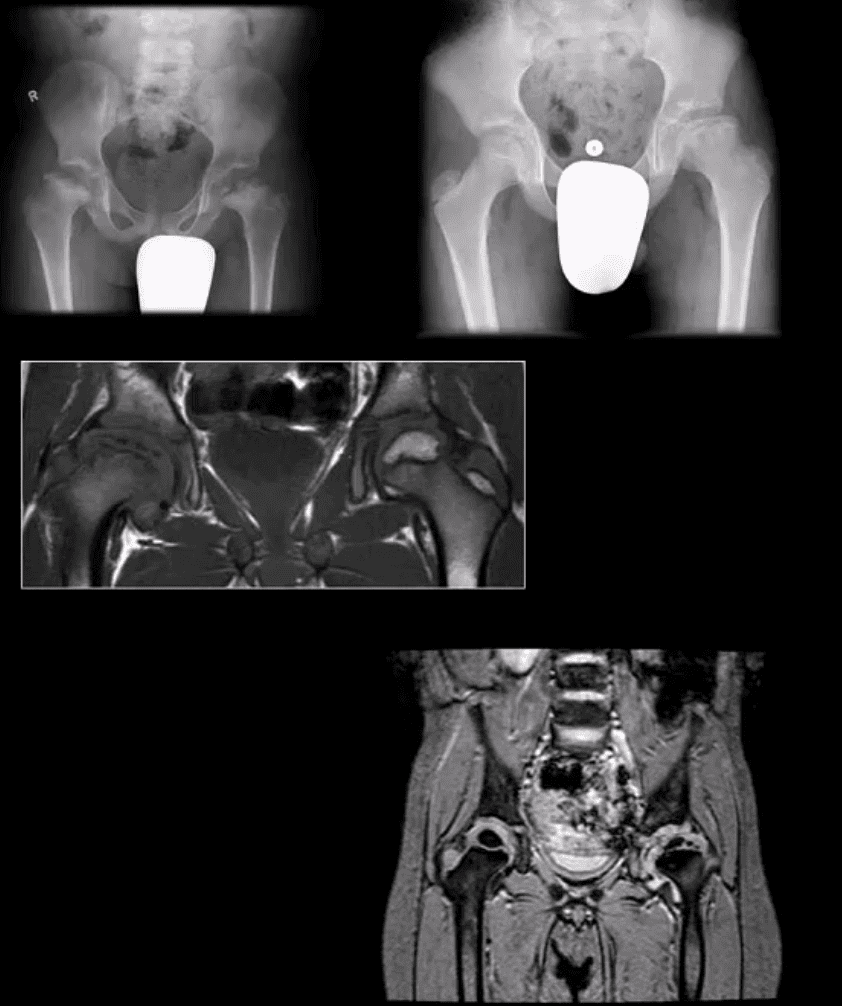
Perthes’ Disease
aka Legg-Calves-Perthes Disease (LCP)
Refers to Osteochondritis of the femoral head with osteonecrosis likely d/t disturbed vascularization of the femoral head
Presents typically in children (more often boys) aged under eight years as atraumatic “limping child.” 15% may have B/L Perthe’s
Imaging steps: 1st step x-radiography, followed by MRI especially in stage 1 (early) w/o x-ray abnormalities
Unspecific signs: joint effusion with Waldenstrome sign+ (>2-mm increase in medial joint space compared to the opposite side). Past approach: Fluoroscopic Arthrography (replaced by MRI)
Pathologic-Radiologic Correlation: in well-established cases, the femoral head characteristically becomes sclerotic, flattened and fragmented due to avascular necrosis (AVN). Later on, an occasional Coxa Magna changes may develop (>10% femoral head enlargement)
Management: symptoms control, bracing. Boys at younger ate show better prognosis d/t more immaturity and better chances of bone/cartilage repair mechanisms. In advanced cases, operative care: osteotomy, hip arthroplasty in adulthood if advanced DJD develops
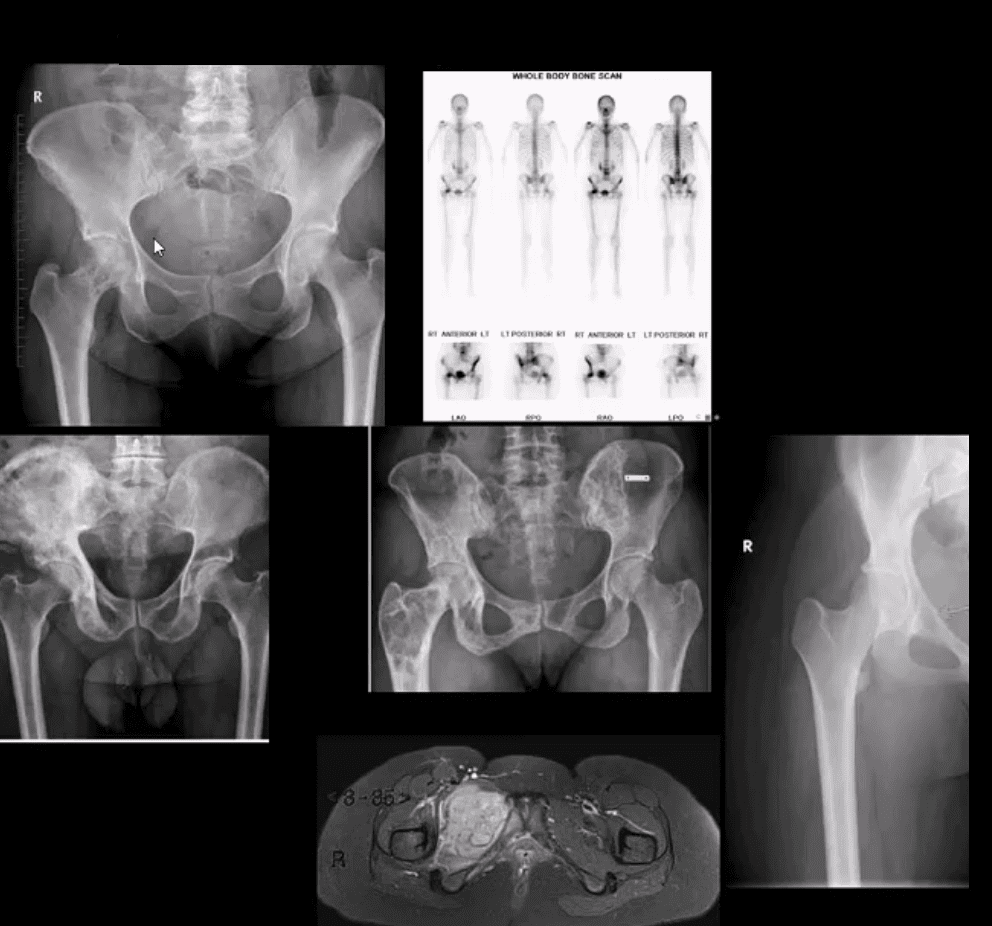
Common Neoplasms & Other Conditions Affecting Hip/Pelvis
M/C hip & pelvis neoplasms in adults: bone metastasis ( above far left), 2nd m/c Multiple Myeloma (M/C primary bone malignancy in adults). Tips: remember Red Marrow distribution. Less frequent: Chondrosarcoma
Paget’s disease of bone (above-bottom left image) is m/c detected in the pelvis and Femurs
Children and young adults ‘limping child’ benign neoplasms: Fibrous Dysplasia (above middle image), Solitary Bone Cyst (21%), Osteoid Osteoma, Chondroblastoma. Malignant pediatric neoplasms: m/c Ewing Sarcoma (above middle right and bottom images) vs. Osteosarcoma. >2y.o-consider Neuroblastoma
Imaging: 1st step: radiography followed by MRI are most appropriate.
If Mets are suspected: Tc99 bone scintigraphy is most sensitive
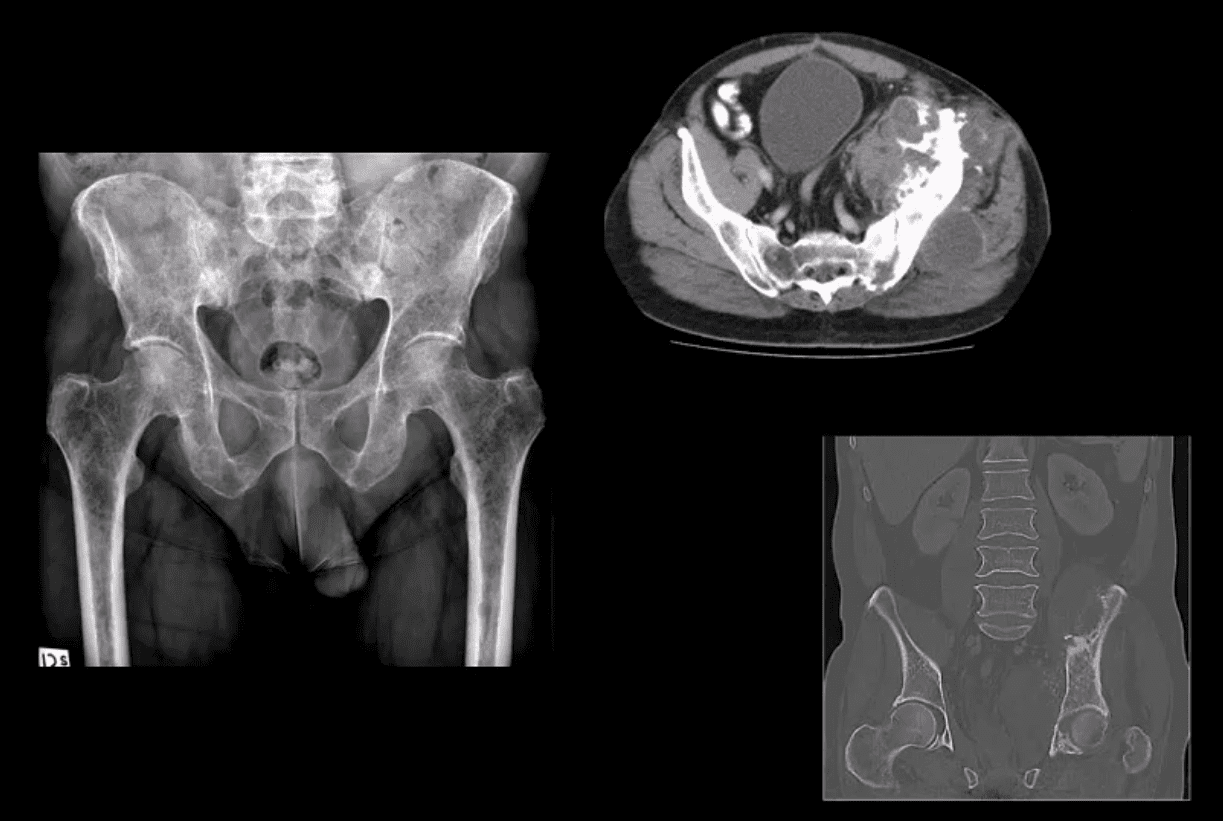
Multiple Myeloma
Multiple Myeloma in a 75-y.o male (AP pelvis view)
Chondrosarcoma in a 60-y.o male (axial and coronal reconstructed CT+C slices in the bone window)
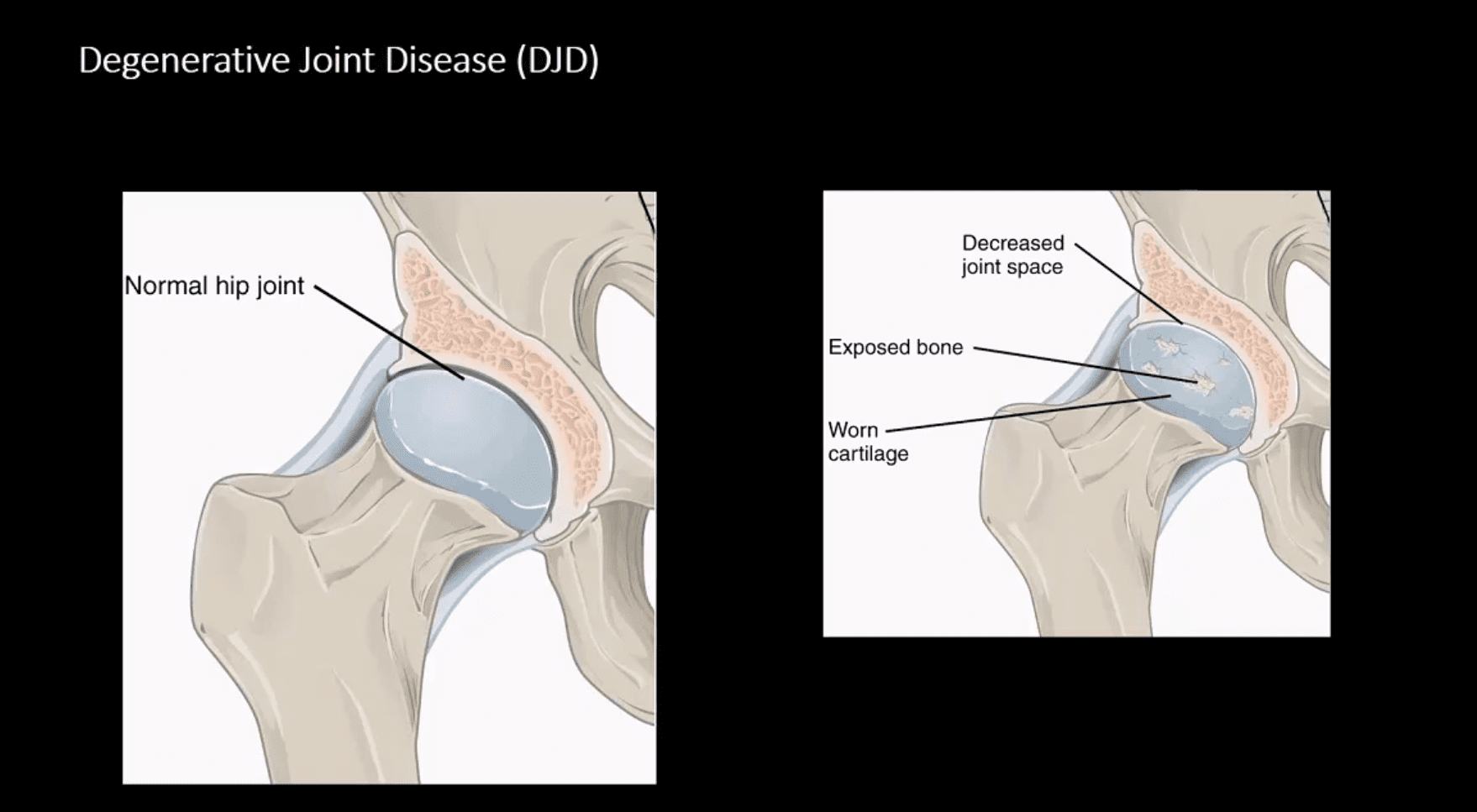
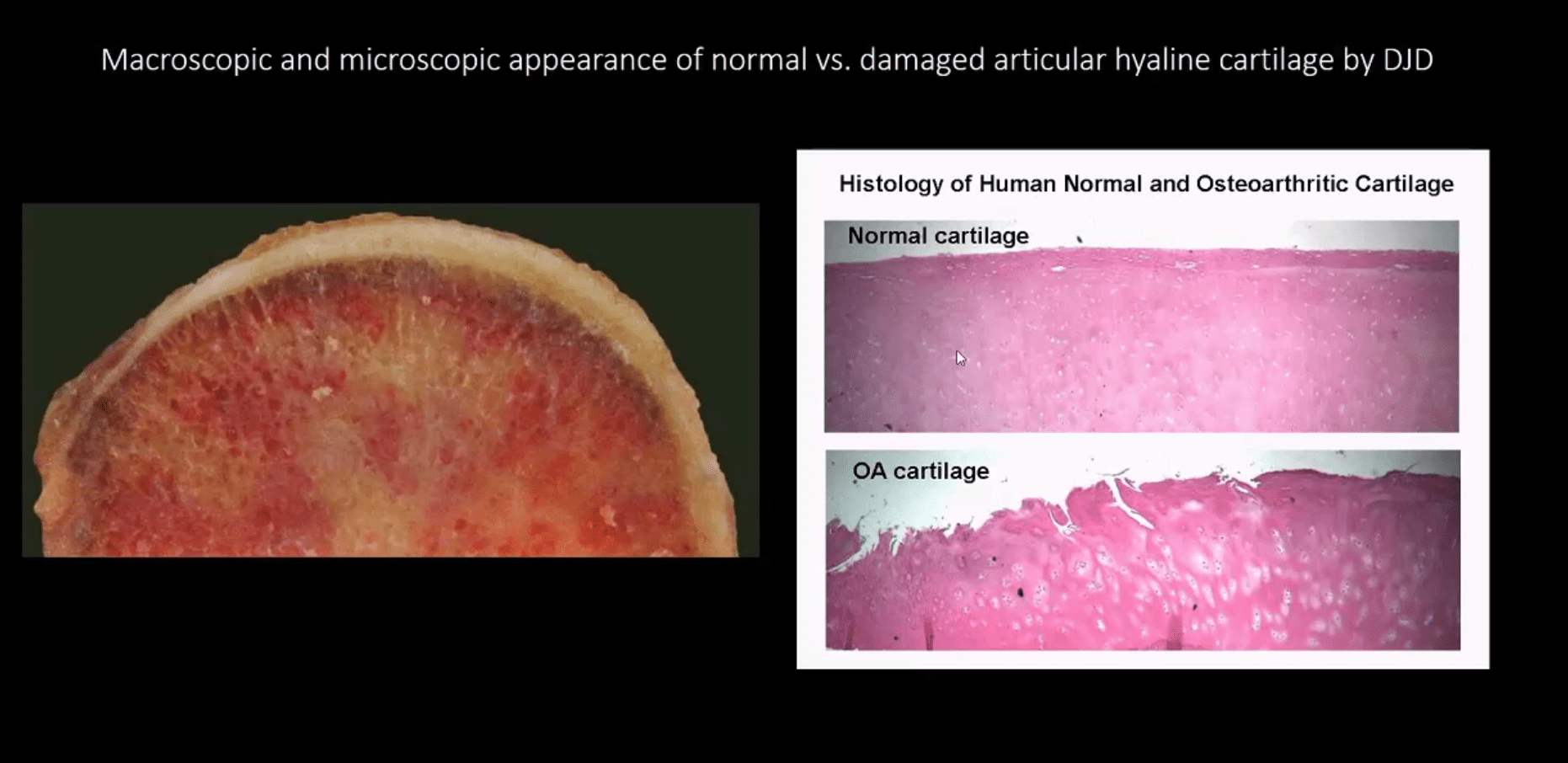
Macroscopic & Microscopic Appearance of Normal vs. Damaged Articular Hyaline Cartilage by DJD
Hip Osteoarthritis (OA) aka Osteoarthrosis
Symptomatic and potentially disabling DJD
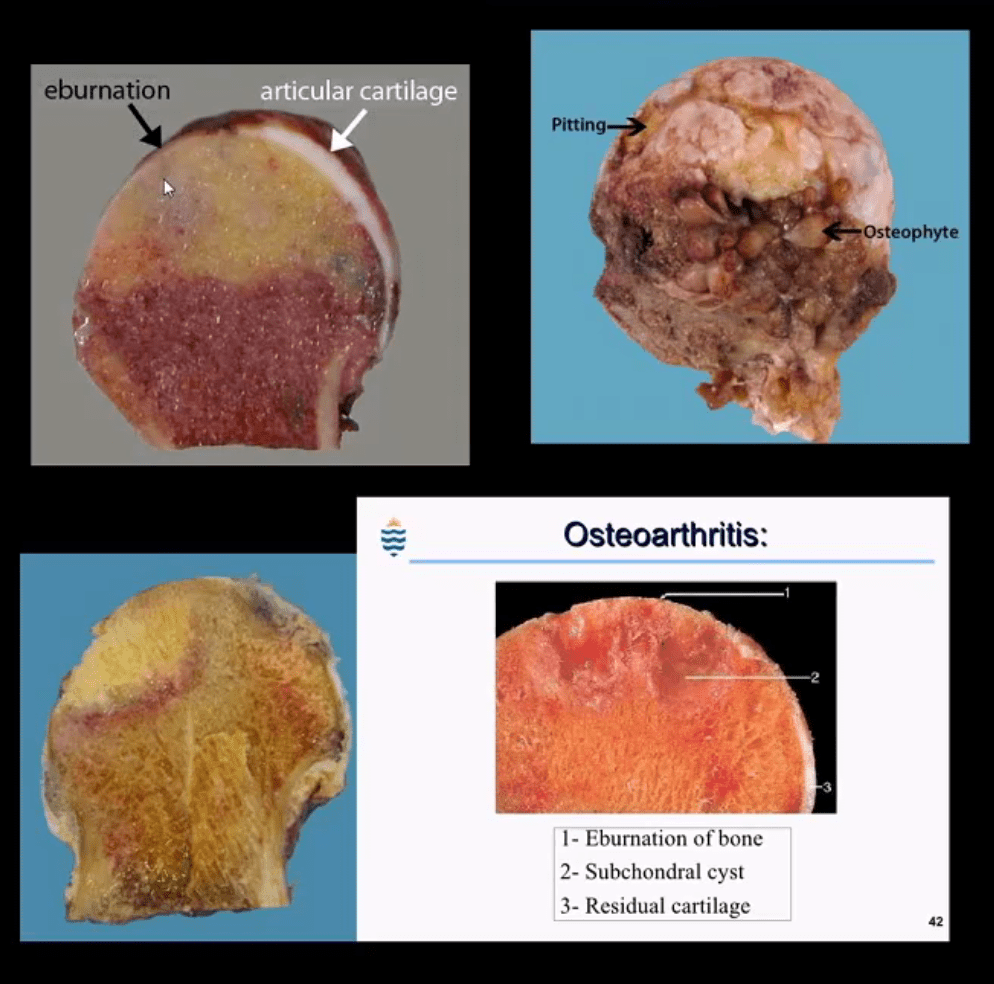
Progressive damage and loss of the articular cartilage causing denudation and eburnation of articular bone
Cystic changes, osteophytes, and gradual joint destruction
Develops d/t repeated joint loading and microtrauma
Obesity, metabolic/genetic factors
Secondary Causes: trauma, FAI syndrome, osteonecrosis, pyrophosphate crystal deposition, previous inflammatory arthritis, Slipped Capital Femoral Epiphysis, Leg-Calves-Perthes disease in children, etc.
Hip OA, 2nd m/c after knee OA. Women>men
88-100 symptomatic cases per 100000
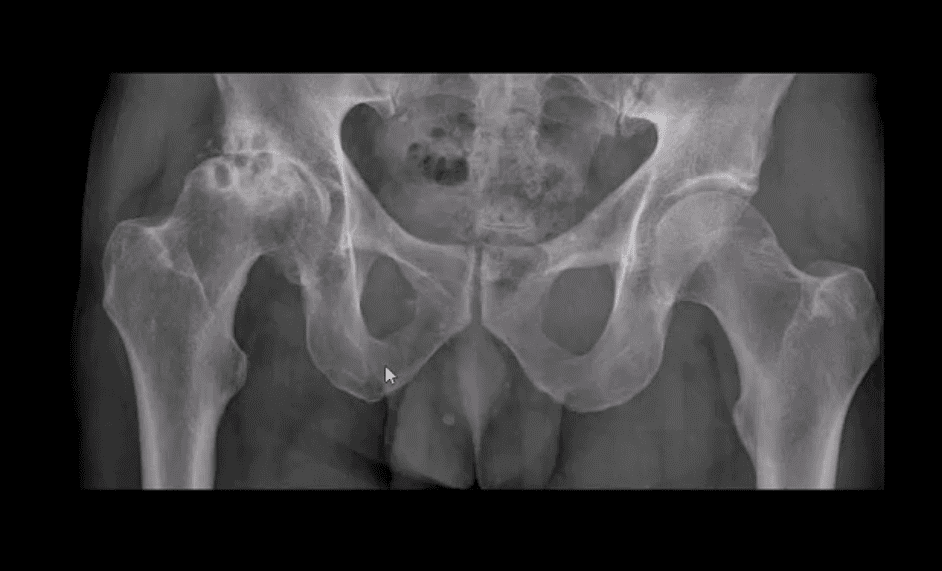
Radiography is the Modality of Choice for the Dx and Grading of DJD
Special imaging is not required unless other complicating factors exist
The acetabular-femoral joint is divided into superior, axial and medial compartments/spaces
Normal joint space at the superior compartment should be 3-4-mm on the AP hip/pelvis view
Understanding the pattern of hip joint narrowing/migration helps with the DDx of DJD vs. Inflammatory arthritis
In DJD, m/c hip narrowing is superior-lateral (non-uniform) vs. inflammatory axial (uniform)
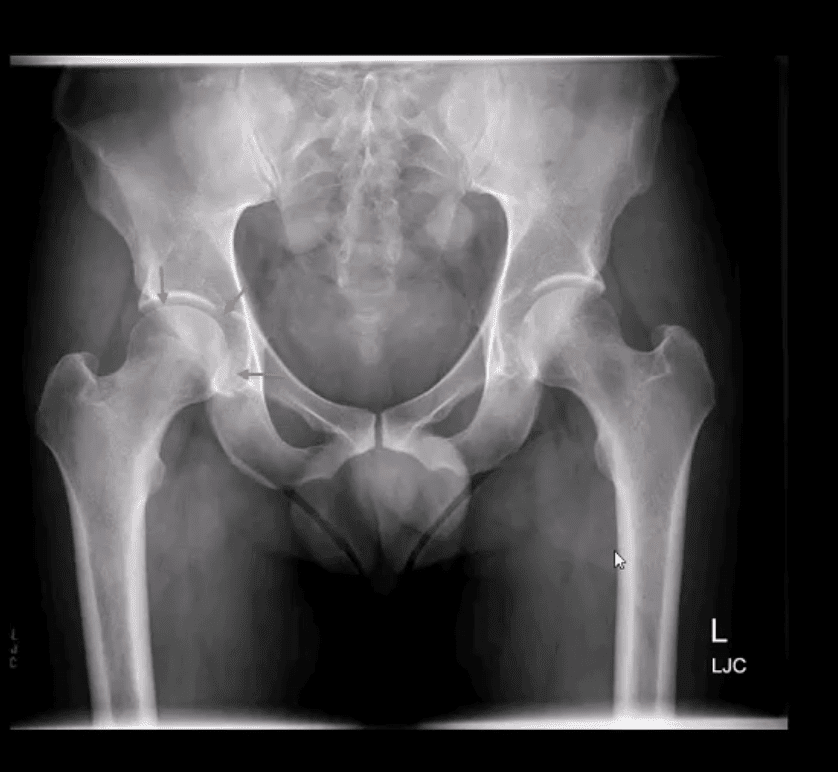
AP Hip Radiograph Demonstrates DJD
With a non-uniform loss of joint space (superior migration), large subcortical cysts and subchondral sclerosis
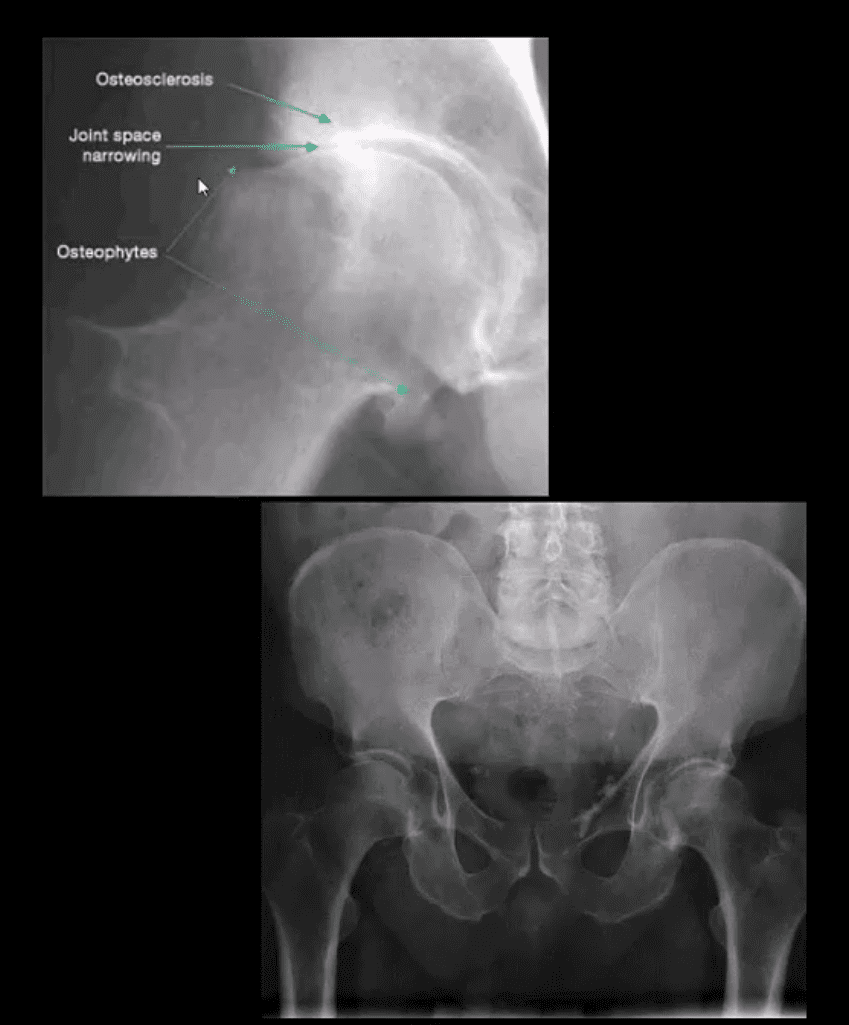
Radiographic features:
Like with any DJD changes: radiography will reveal L.O.S.S.
L: loss of joint space (non-uniform or asymmetrical)
O: osteophytes aka bony proliferation/spurs
S: Subchondral sclerosis/thickening
S: Subcortical aka subchondral cysts “geodes.”
Hip migration is m/c superior resulting in a “tilt deformity.”
Radiographic Presentation of Hip OA May Vary Depending On Severity
Mild OA: mild reduction of joint space often w/o marked osteophytes and cystic changes
During further changes, collar osteophytes may affect femoral head-neck junction with more significant joint space loss and subchondral bone sclerosis (eburnation)
Cyst formation will often occur along the acetabular and femoral head subarticular/subchondral bone “geodes” and usually filled with joint fluid and some intra-articular gas
Subchondral cysts may occasionally be very large and DDx from neoplasms or infection or other pathology
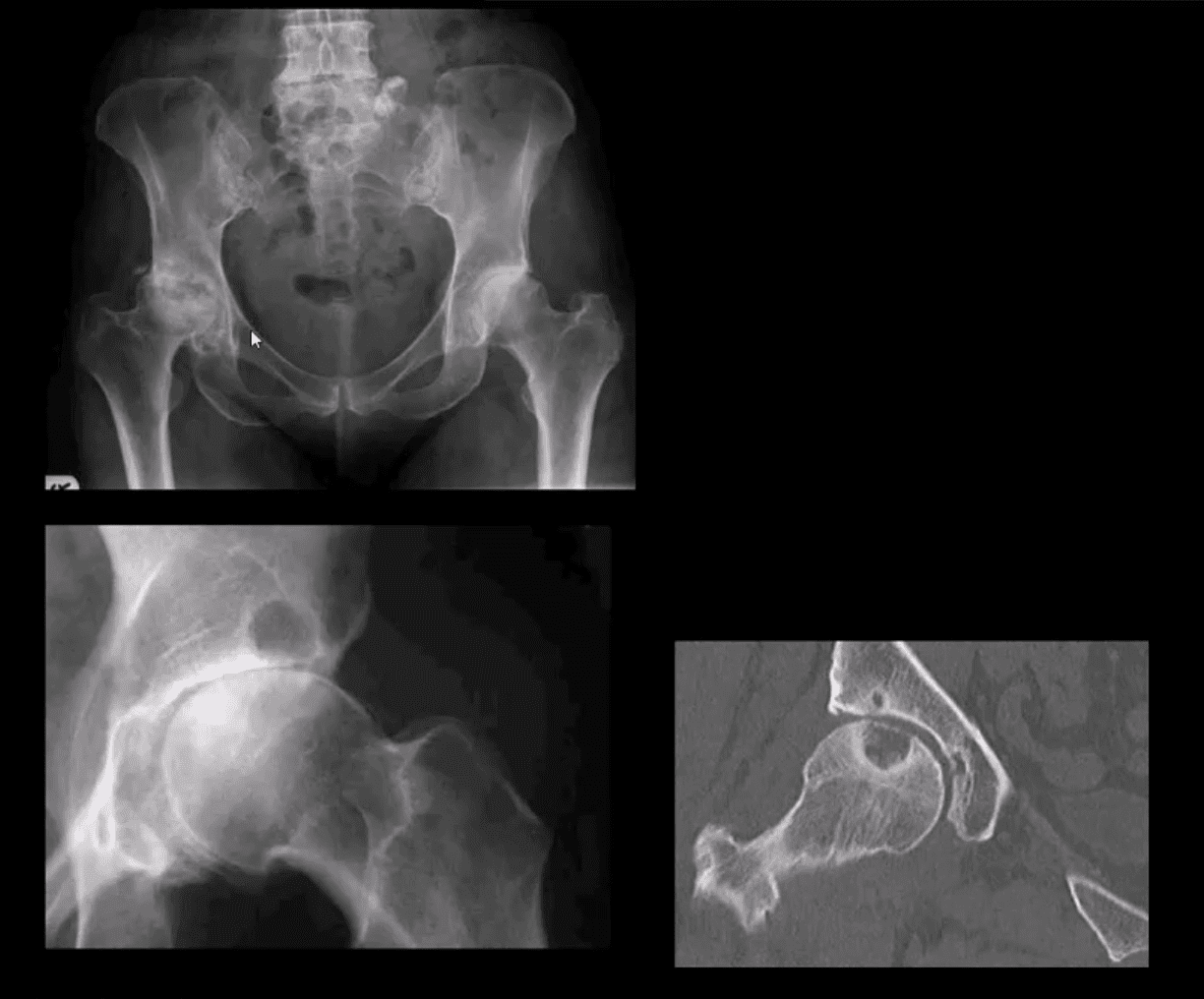
Coronal Reconstructed CT Slices in Bone Window
Note moderate joint narrowing that appears non-uniform
Sub-chondral cysts formation (geodes) are noted along the acetabular and femoral head subchondral bone
Other features include collar osteophytes along head-neck junction
Dx: DJD of moderate intensity
Referral to the Orthopedic surgeon will be helpful for this patient
AP Pelvis (below the first image), AP Hip Spot (below the second image) CT Coronal Slice
Note multiple subchondral cysts, severe non-uniform joint narrowing (superior-lateral) and subchondral sclerosis with osteophytes
Advanced hip arthrosis
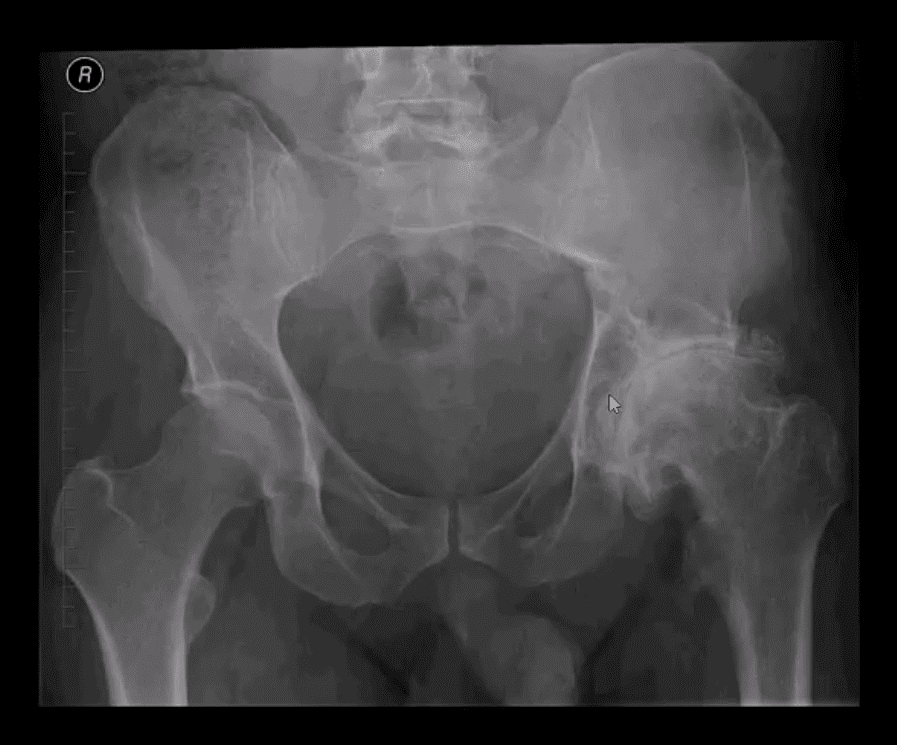
Severe DJD, Left Hip
When reading radiological reports pay particular attention to the grading of hip OA
Most severe (advanced) OA cases require total hip arthroplasty (THA)
Refer your patients to the Orthopedic surgeon for a consultation
Most mild cases are a good candidate for conservative care
Hip Arthroplasty aka Hip Replacement
Can be total or hemiarthroplasty
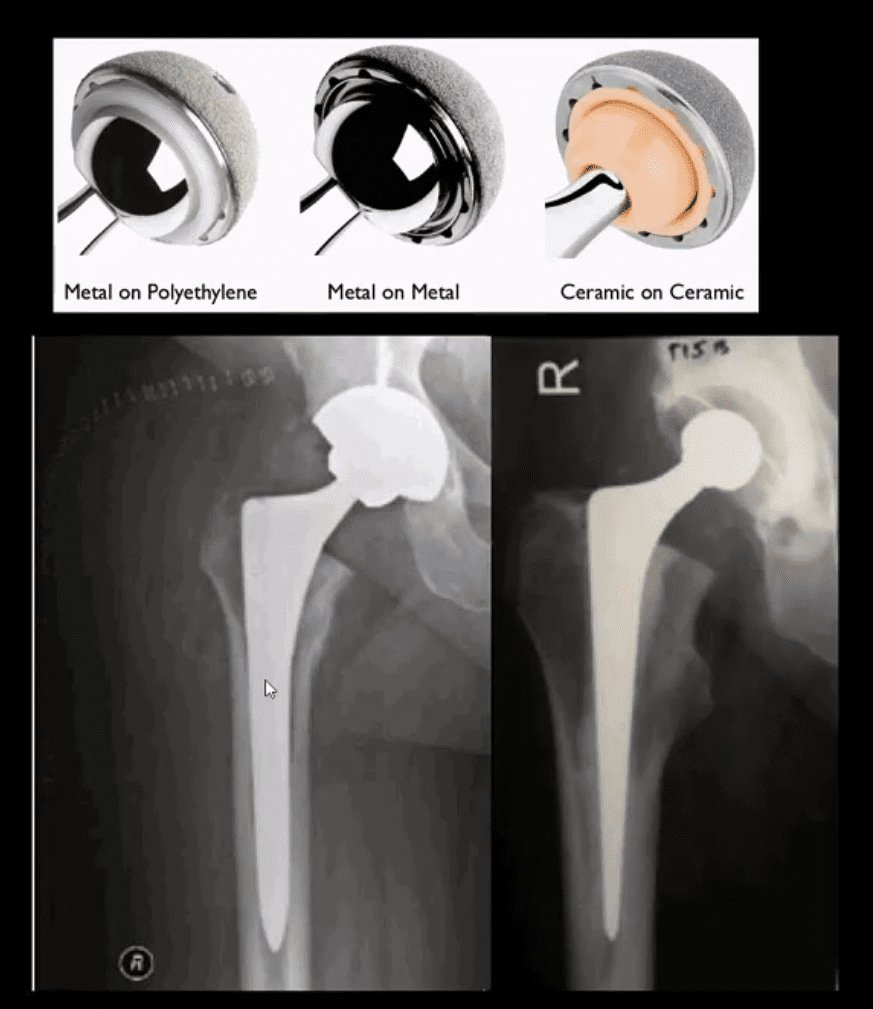
THA can be metal on metal, metal on polyethylene and ceramic on ceramic
A hybrid acetabular component with polyethylene and metal backing is also used (above right image)
THA can be cemented (above right image) and non-cemented (above-left image)
Non-cemented arthroplasty is used on younger patients utilizing porous metallic parts allowing good fusion and bone ingrowth into the prosthesis
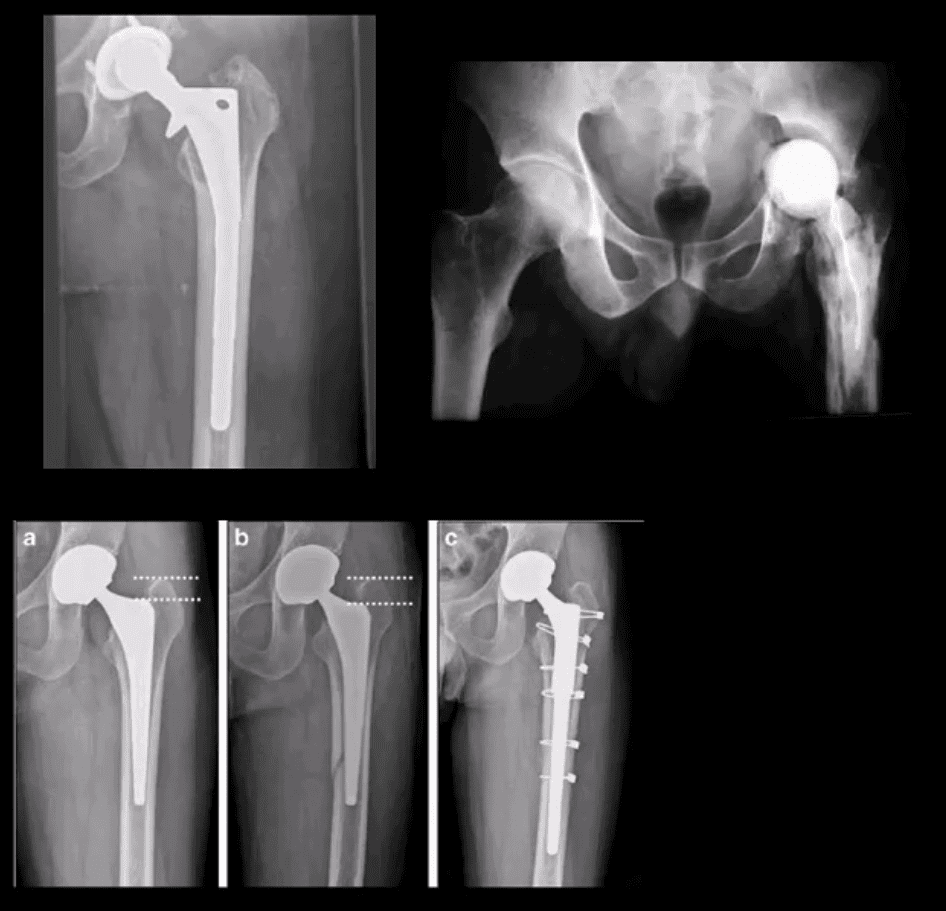
Failed THA May Develop
Most develop within the first year and require revision
Femoral stem may fracture (above left)
Postsurgical infection (above right)
Fracture adjacent to the prosthesis (stress riser)
Particle disease
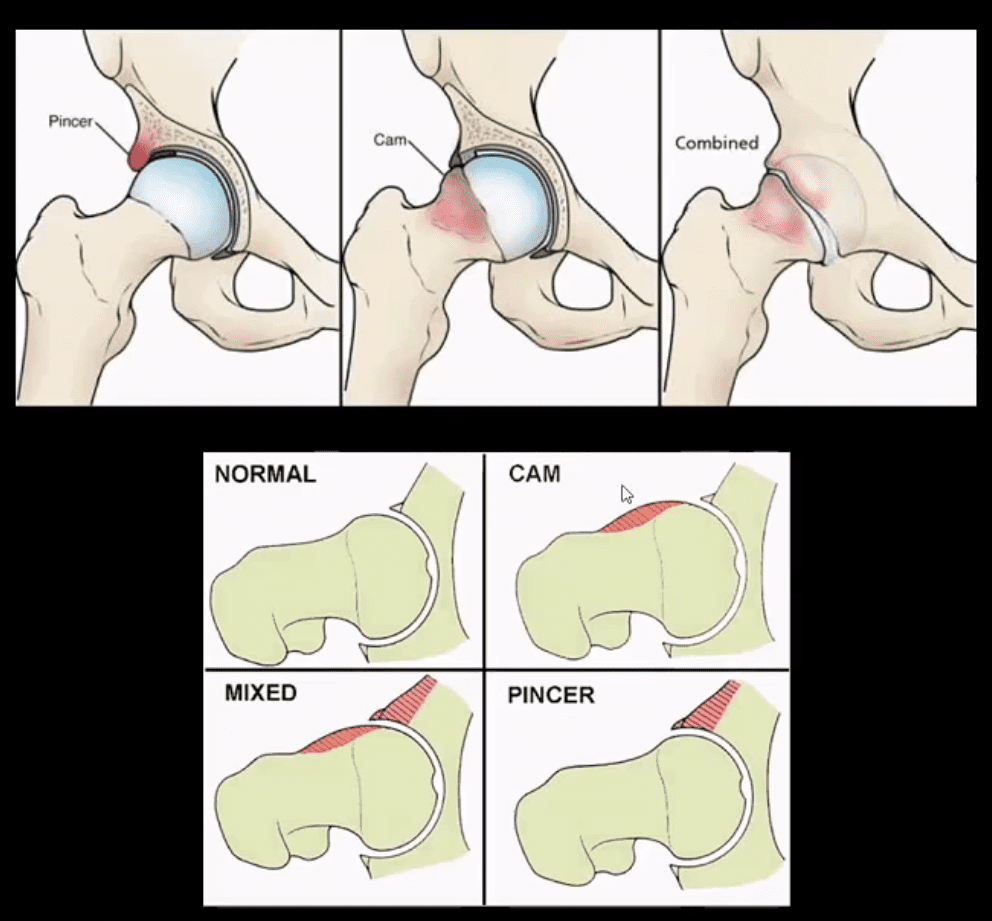
Femoroacetabular Impingement Syndrome
(FAI): abnormality of normal morphology of the hip leading to eventual� cartilage damage and premature DJD
Clinically:�hip/groin pain aggravated by sitting (e.g., hip flexed & externally rotated). Activity related pain on axial loading esp. with hip flexion (e.g., walking uphill)
Pincer-type�acetabulum: > in middle age women potentially� many causes
CAM-type deformity:�> in men in 20-50 m/c 30s
Mixed type (pincer-CAM) is most frequent
Up until the 90s, FAI was not well-recognized
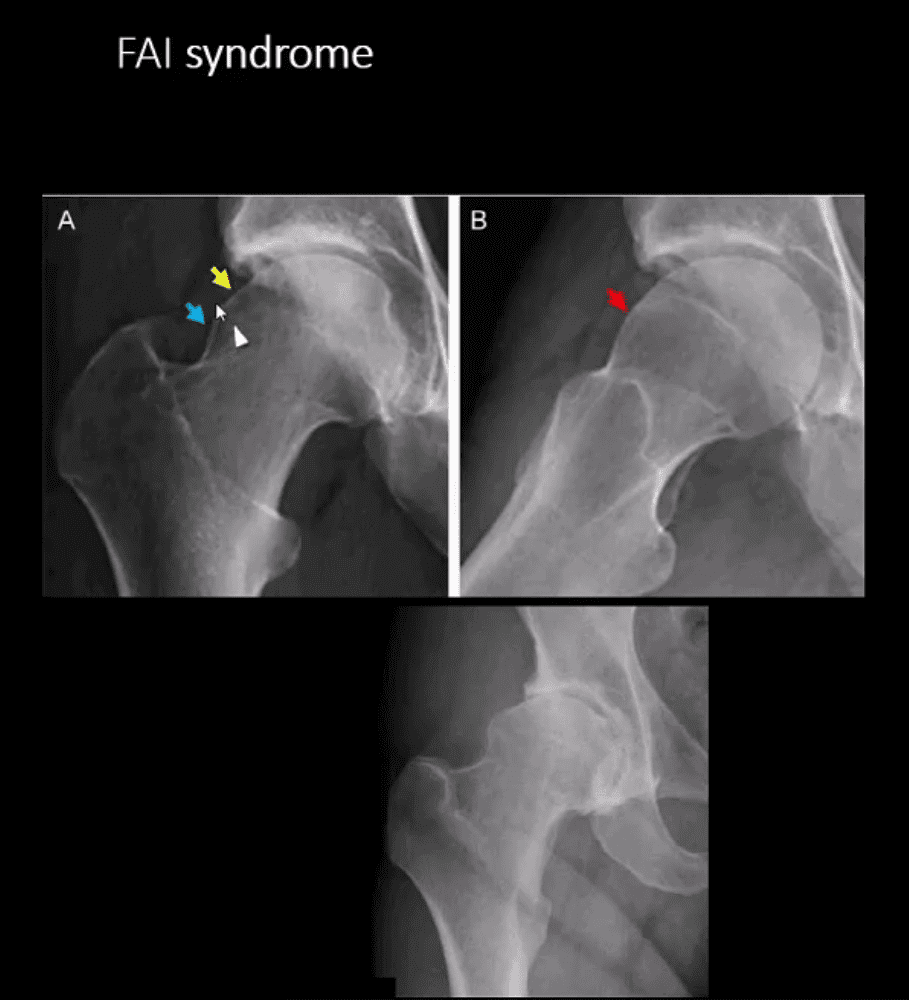
FAI Syndrome
CAM-type FAI syndrome
Radiography can be a reliable Dx tool
X-radiography findings:�osseous bump on the lateral aspect of femoral head-neck junction. Pistol-grip deformity. Loss of normal head sphericity. Associated features: os acetabule, synovial herniation pit (Pit’s pit). Evidence of DJD in advanced cases
MRI and MR arthrography (most accurate Dx of labral tear) can aid the diagnosis of labral tear and other changes of FAI
Referral to the Orthopedic surgeon is necessary to prevent DJD progression and repair labral abnormalities. Late Dx may lead to irreversible changes of DJD
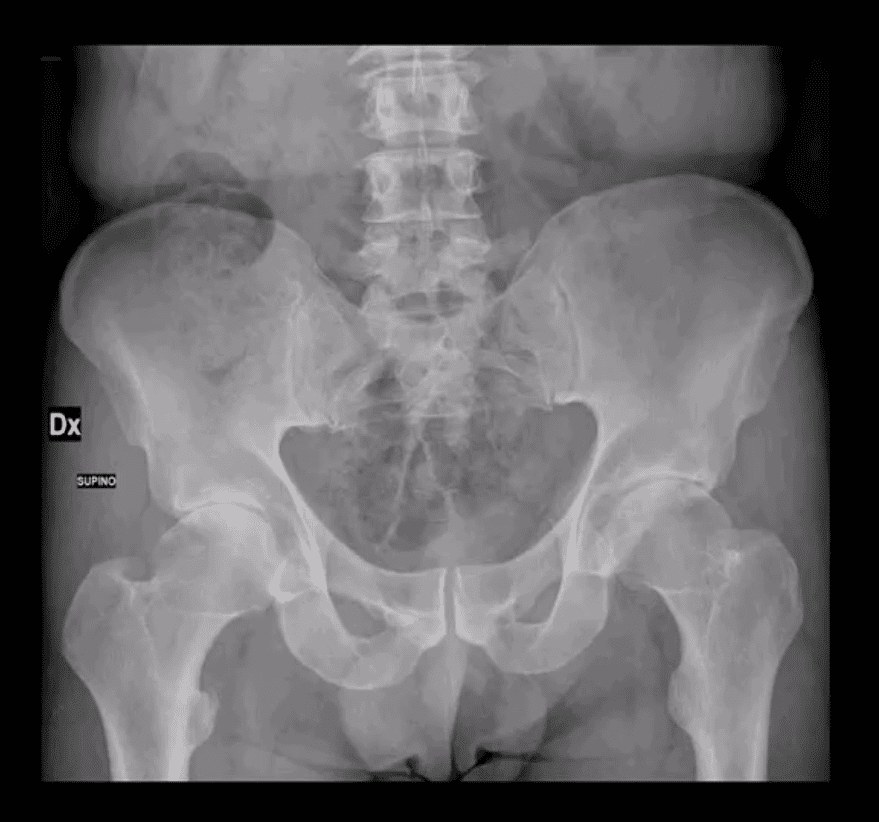
AP Pelvis: B/L CAM-type FAI syndrome
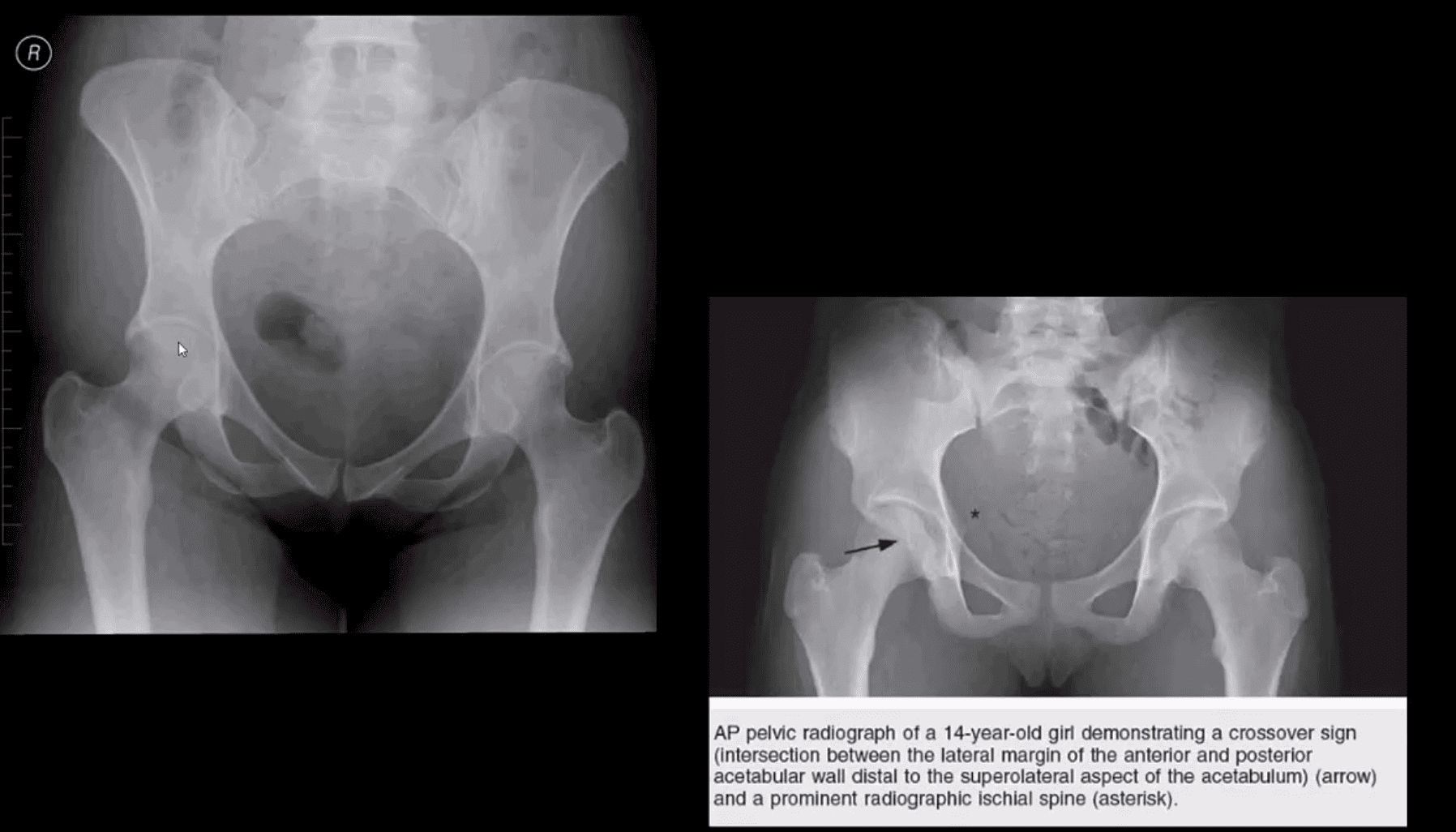
Pincer-Type FAI with Acetabula Over-Coverage
Key radiographic signs: “Cross-over sign” and abnormal center-edge and Alfa-angle evaluation methods
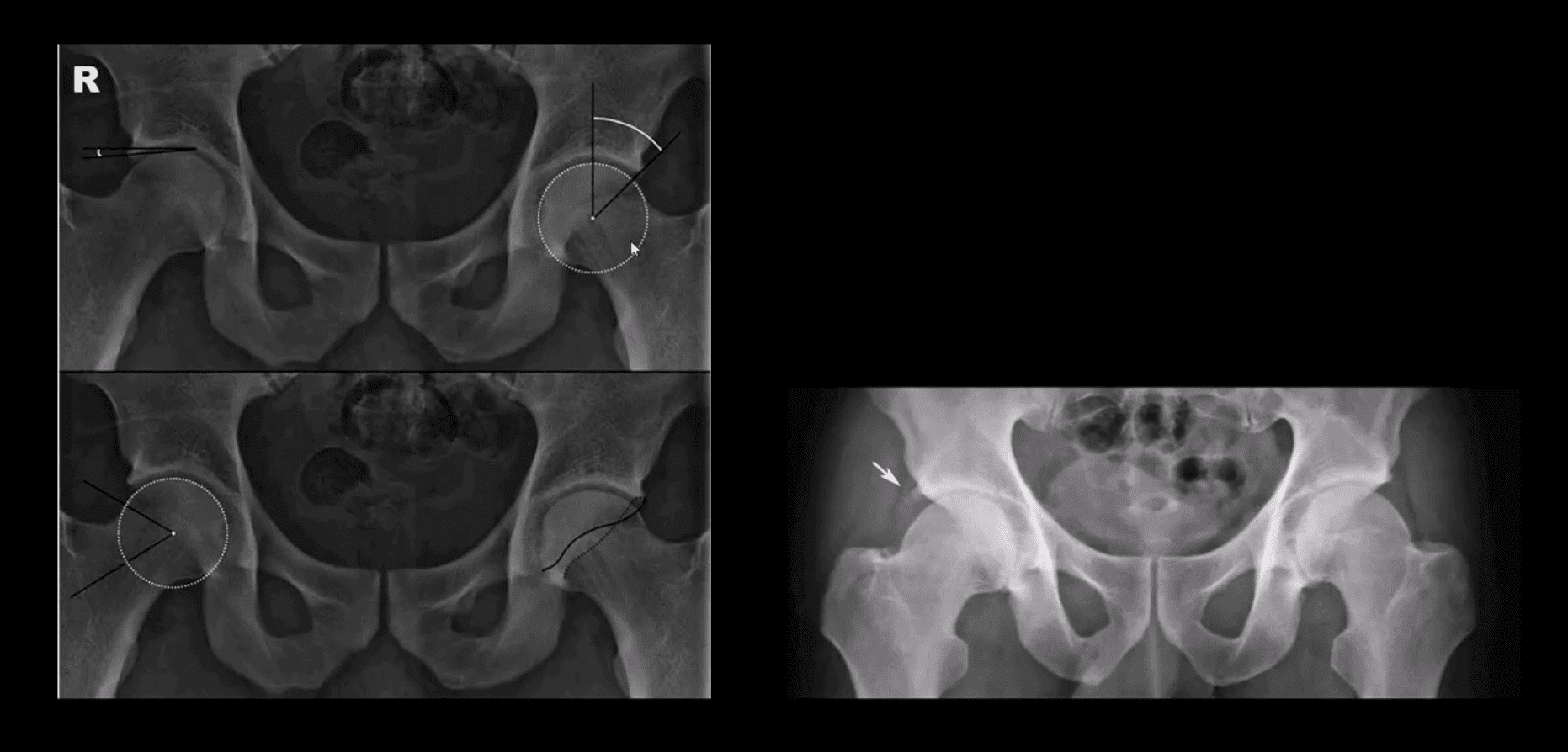
Dx of FAI
Center-edge angle (above the first image) and Alfa-angle (above the second image)
B/L CAM-type FAI with os acetabule�(above right image)
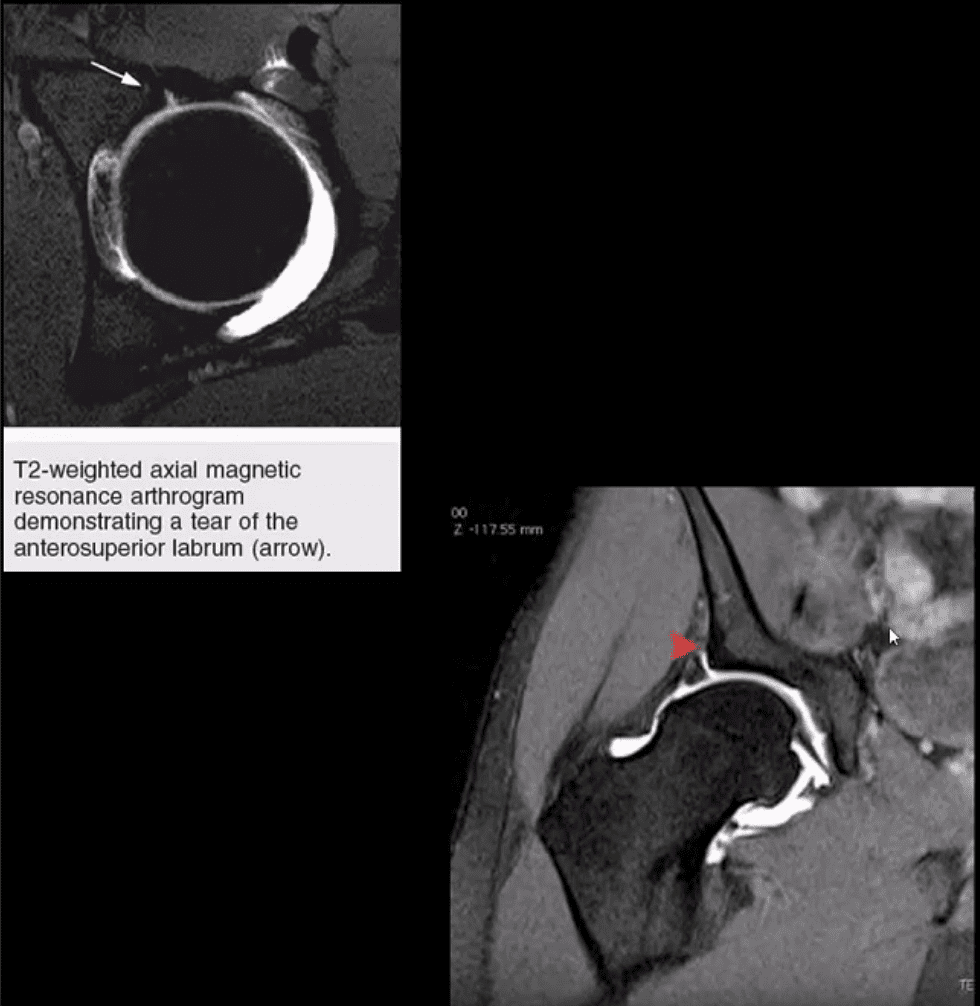
MR Arthrography
Labral tear and CAM-type FAI syndrome on axial (above left) and coronal T2 W (above right) MR arthrography
Note acetabula labral tear. Referral to an orthopedic surgeon is required. For more information:
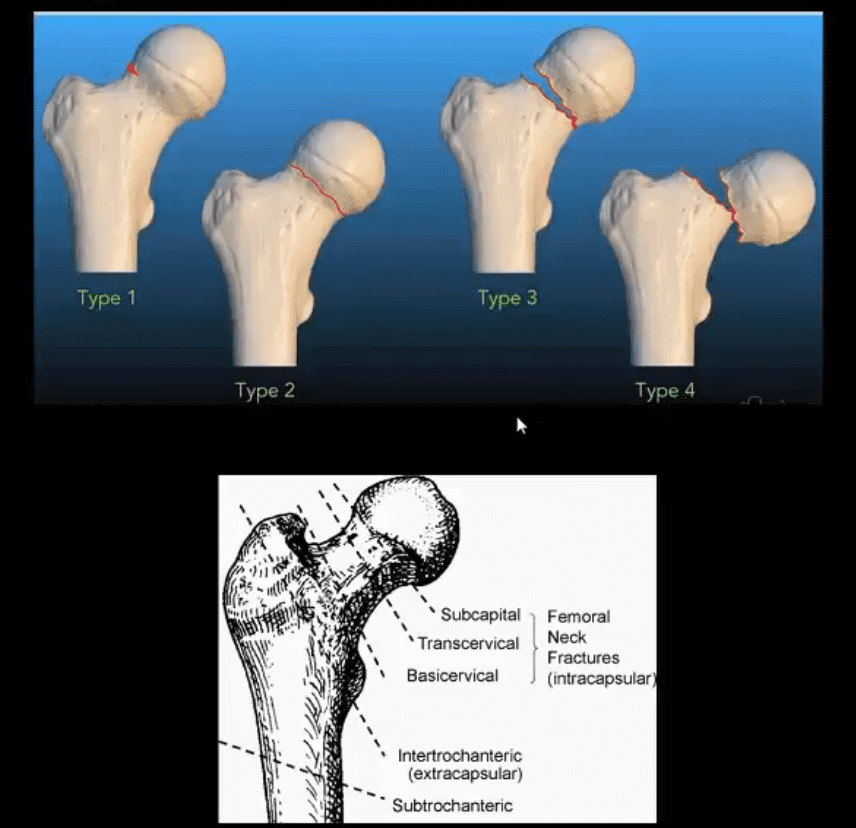
X-radiography pitfalls: some undisplaced Garden 1 & 2 Fxs may be missed d/t pre-existing DJD and osteophytes along the femoral head-neck junction that may overly the Fx line
Fx line is incomplete and too small/subtle especially if the study is read by non-radiologists
Incomplete Fxs if left untreated will not heal and likely to progress to complete Fxs
AP hip spot view: note valgus deformity of the head (above yellow arrow) with a small/subtle line of sclerosis in the sub-capital region representing Garden 1 Fx. MRI may help with Dx of subtle radiographic Fxs. If MRI contraindicated, Tc 99 radionuclide bone scan may help demonstrate high uptake of the radiopharmaceutical in Fx (below image)
Above – Tc99 Radionuclide Bone Scan Reveals Left Subcapital Femoral Neck Fx
Garden 2 complete undisplaced (above green arrows) Fx
AP hip: Garden 3 complete partially displaced Fx (above the first image)
AP pelvis: complete displaced Garden 4 Fx (above the second image)
Clinical pearls: in some cases of Garden 4 Fx, DDx may be difficult to differentiate from OSP vs. pathologic fx d/t to bone Mets of Multiple myeloma (MM)
Management: depends on patients age and activity level
Garden 3 & 4� require total hip arthroplasty in patients <85-y.o.
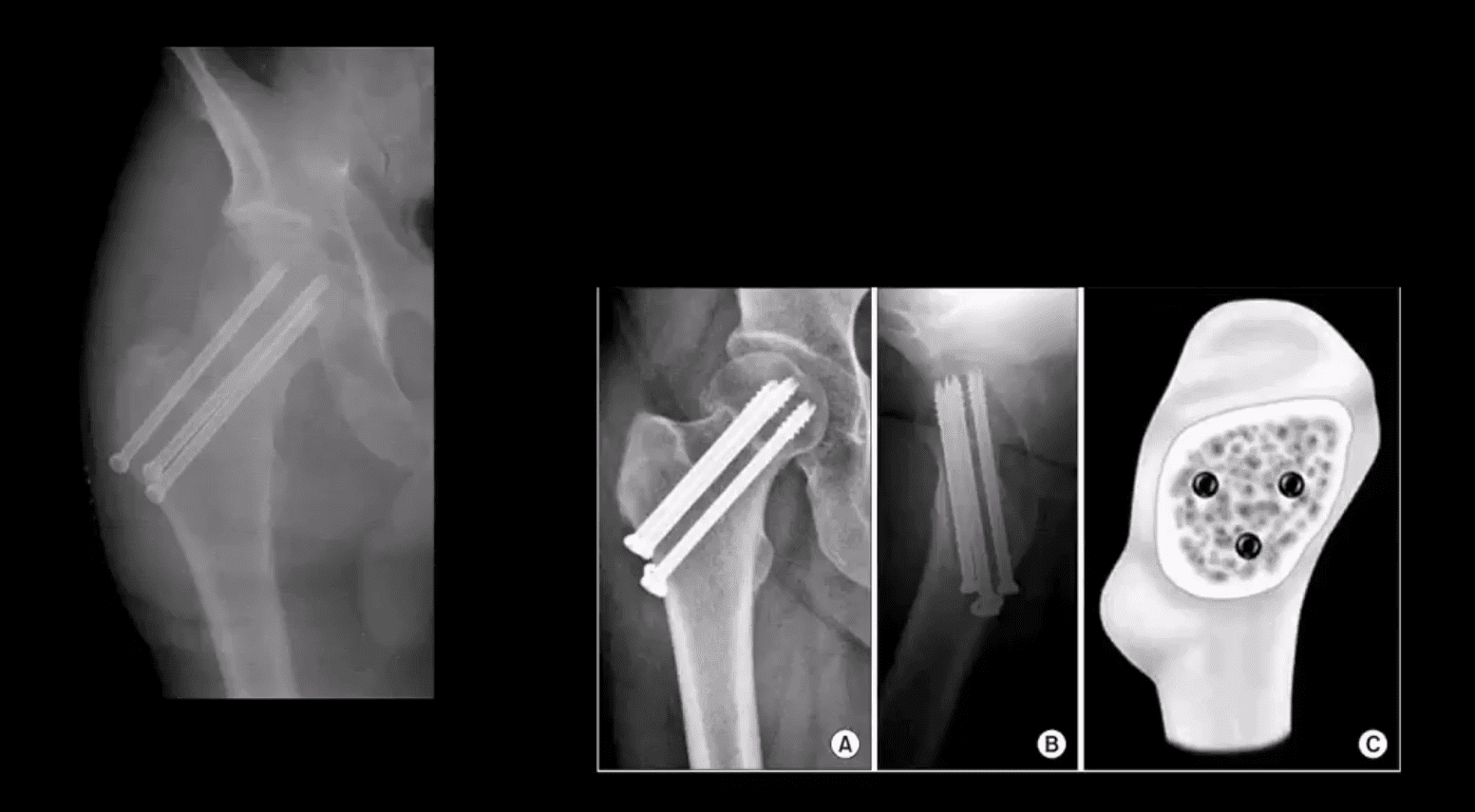
Garden 1 & 2 may be treated with closed reduction of fx and open capsule and 3-cannulated fixating screws
Pre-existing DJD may require total arthroplasty
Occasionally observation may be performed on patients who are not active and significant risks of surgery and depends on surgical centers
m/c Rx of Garden 1 & 2 undisplaced Fx with 3-screws. Screws proximity depends on the bone quality and Fx type
THA aka hip replacement: cemented THA with bone cement (above the first image) vs. non-cemented (biologic) that is used mostly in younger patients
2-types: metal on metal vs. metal on polyethylene
The femoral angle of the prosthesis should have slight valgus but never >140 degrees
The non-cemented component uses porous metal allowing the bone to integrate sometimes coating in bone cement from osteoconduction
THA has good outcome and prognosis
Occasionally cement failure, fractures, and infections may complicate this procedure
Unstable Fx: a result of high energy trauma with >50% d/t MVA
20% closed Fx and 50% of open Fx result in mortality
Mortality is associated with vascular and internal organs injuries
Vascular injury: 20% arterial 80% venous
Chronic morbidity/disability and prolonged pain
Unstable Fx are rarely seen in the outpatient setting and typically and present to the ED
Stable pelvic Fx are usually caused by muscles/tendons avulsions and more often seen in pediatric cases
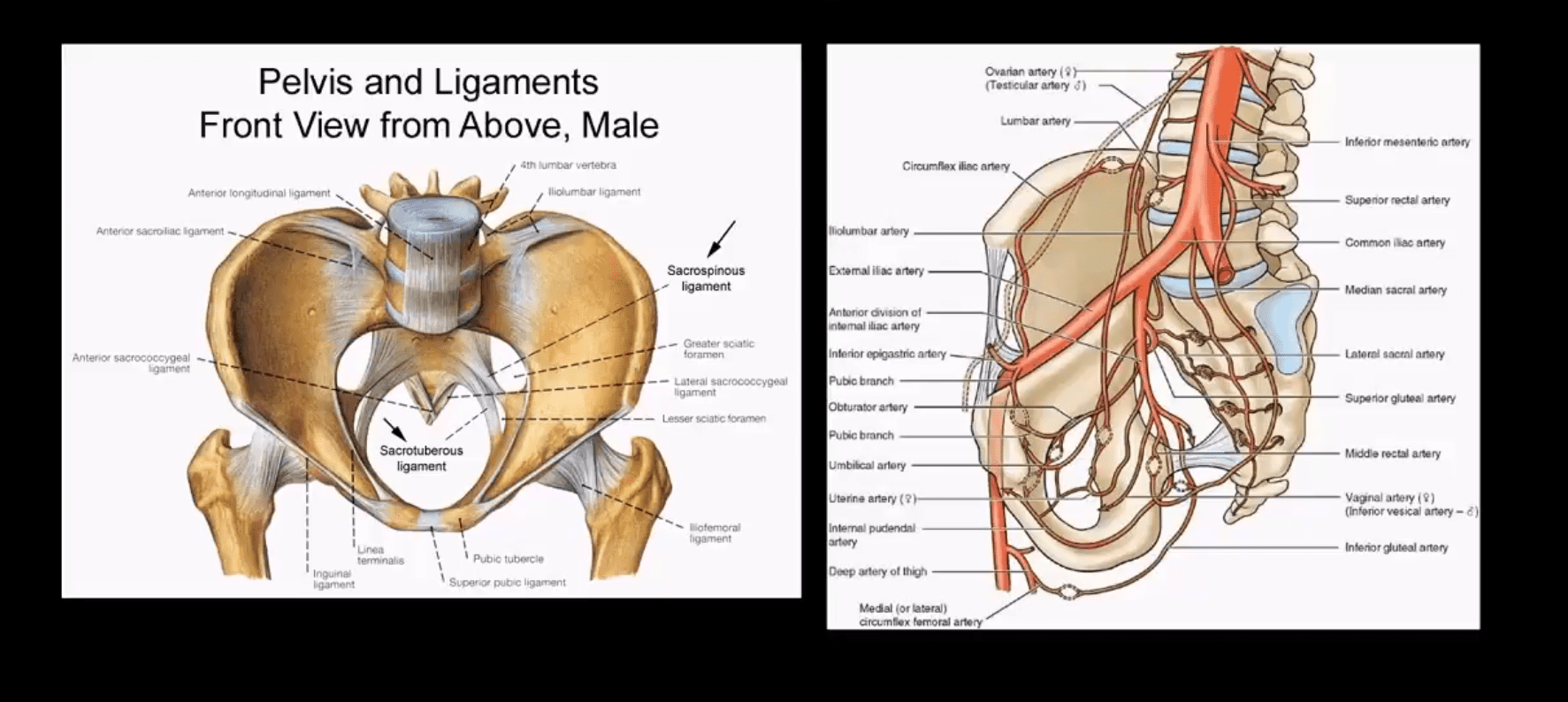
Understanding Pelvic Anatomy Is The Key To Successful Imaging Dx
The bony pelvis is a continuous ring of bone held by strong ligaments
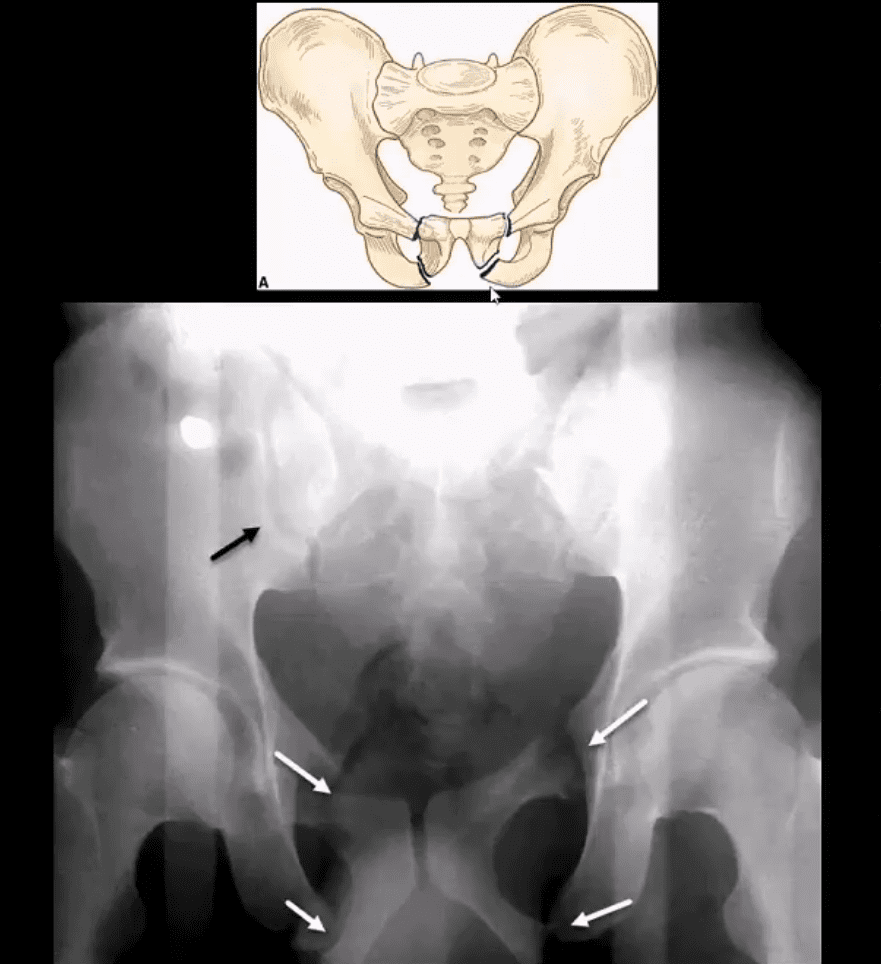
During significant impact, pelvic fractures may occur in more than one location because forces applied to one region of the ring will also correspond to injury on the other, usually the opposite side of the ring (above image)
Thus the majority of unstable pelvic Fx will typically demonstrate more than one break
Pelvic is seen as a ring of� bone connected by some of the strongest ligaments in the body
The pelvic ring comprises 2-semirings: anterior to the acetabulum and posterior to the acetabulum
The bony pelvis is in close proximity to major vessels carrying a greater chance of vascular injury
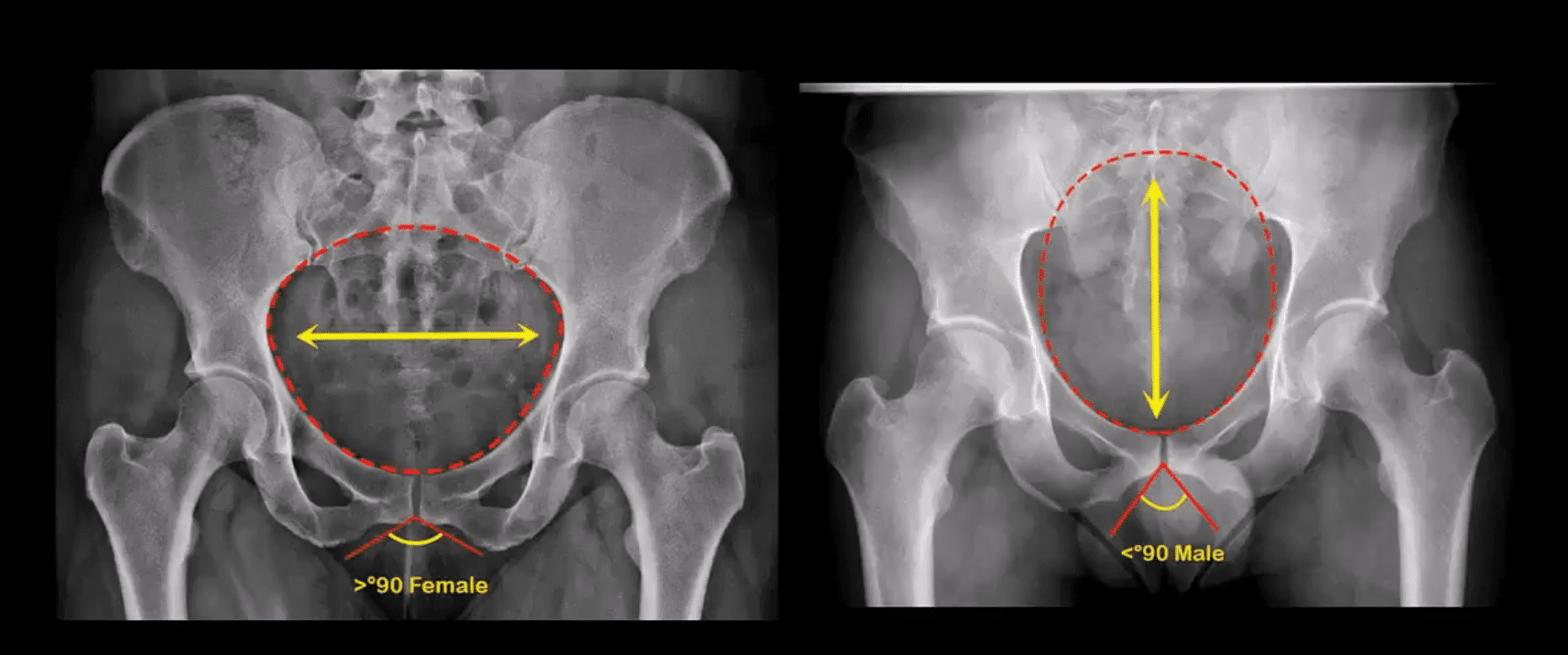
Anatomical Differences of The Female and Male Pelvis
Post-Traumatic Pelvic Views May Vary and Include:
Standard AP Pelvis (above images)
Judet views evaluating the acetabulo-pelvic region
Inlet/Outlet views helping with the symphysis and SIJ regions
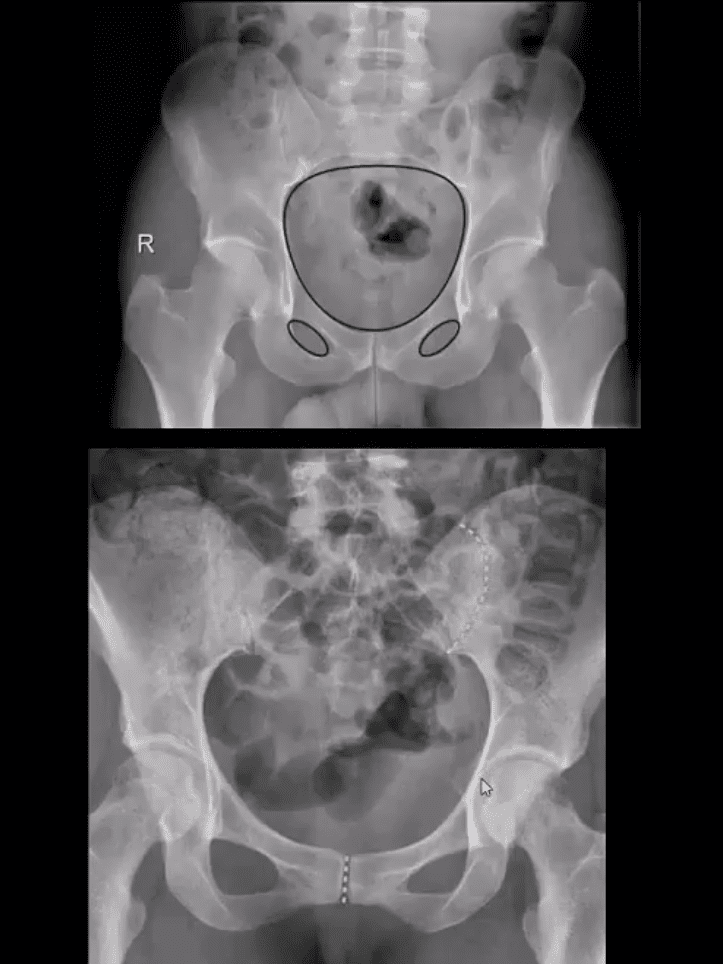
Rad survey of the pelvis should include evaluation of the continuity of pelvic rings:
Inlet/outlet, obturator rings (above the first image)
Symphysis pubis and SIJ for diastasis and post-trauma separation (above the second image)
Lumbosacral spine and hips should also be carefully examined
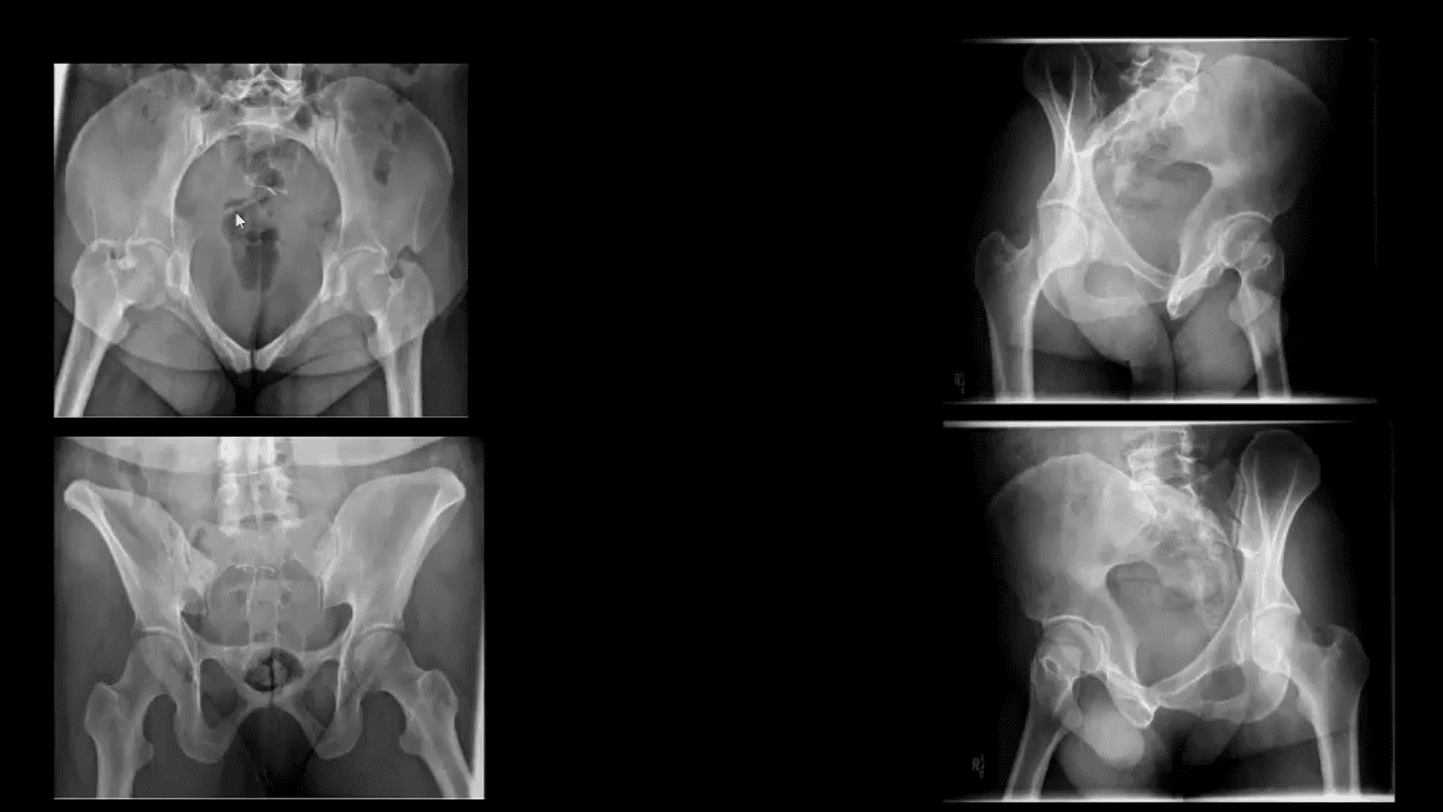
Pelvic inlet (above top left) and Outlet (above bottom left)
Judet views: left and right posterior oblique views
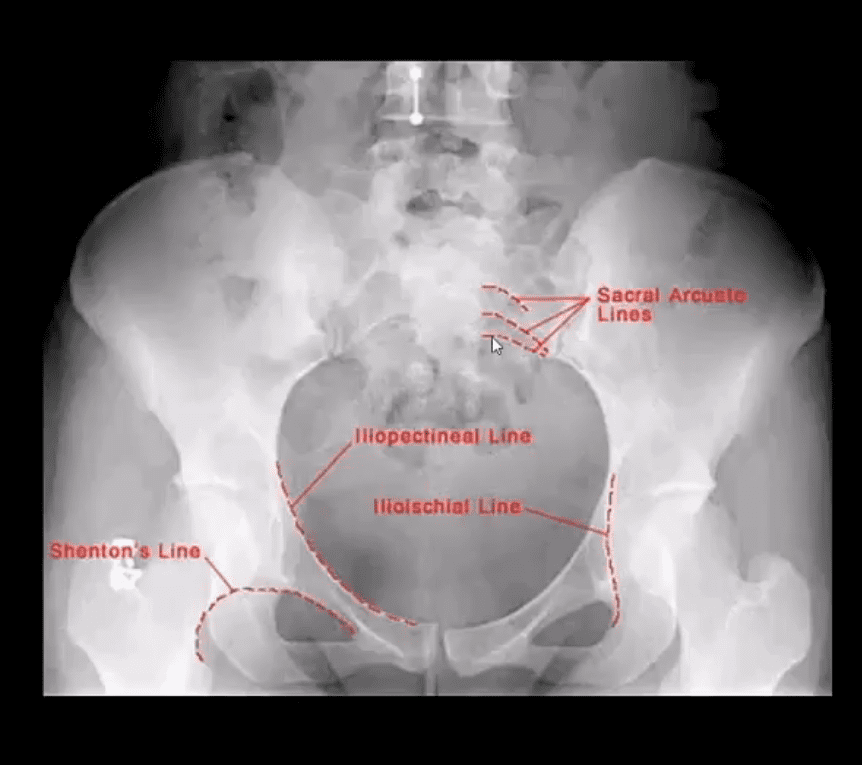
Additional Survey:
Iliopectineal, ilioischial, Shenton and Sacral arcuate lines will help detection of sacral, acetabular and hip fracture/dislocations
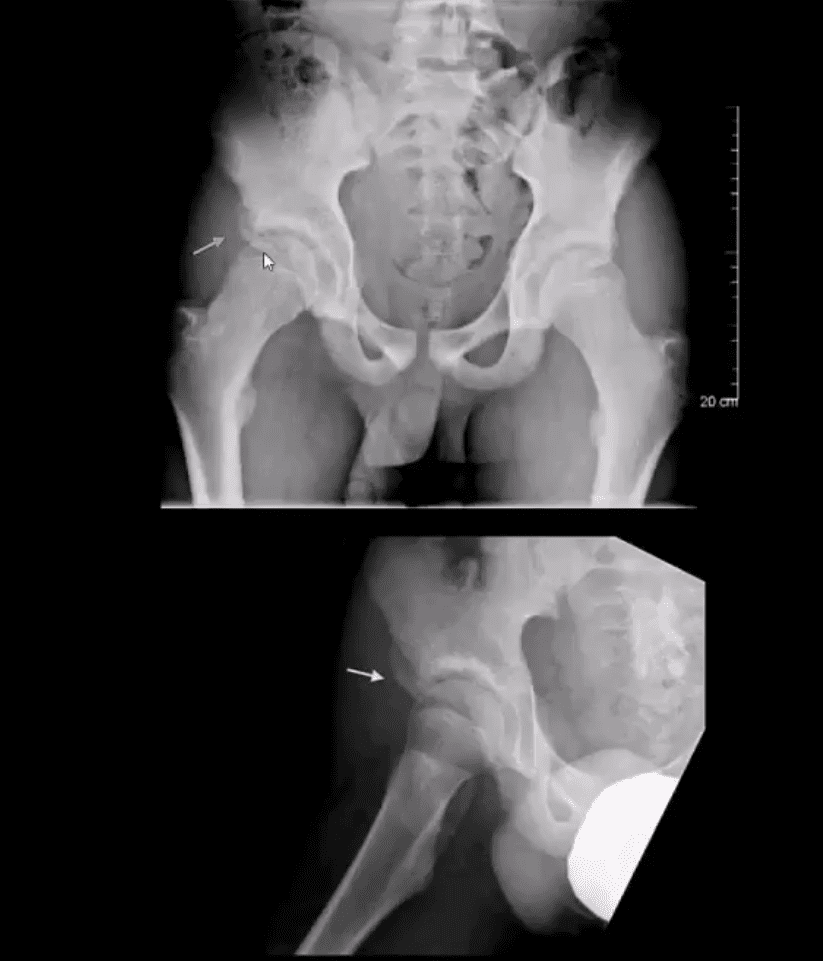
Stable Pelvic Fractures aka Avulsion Injury
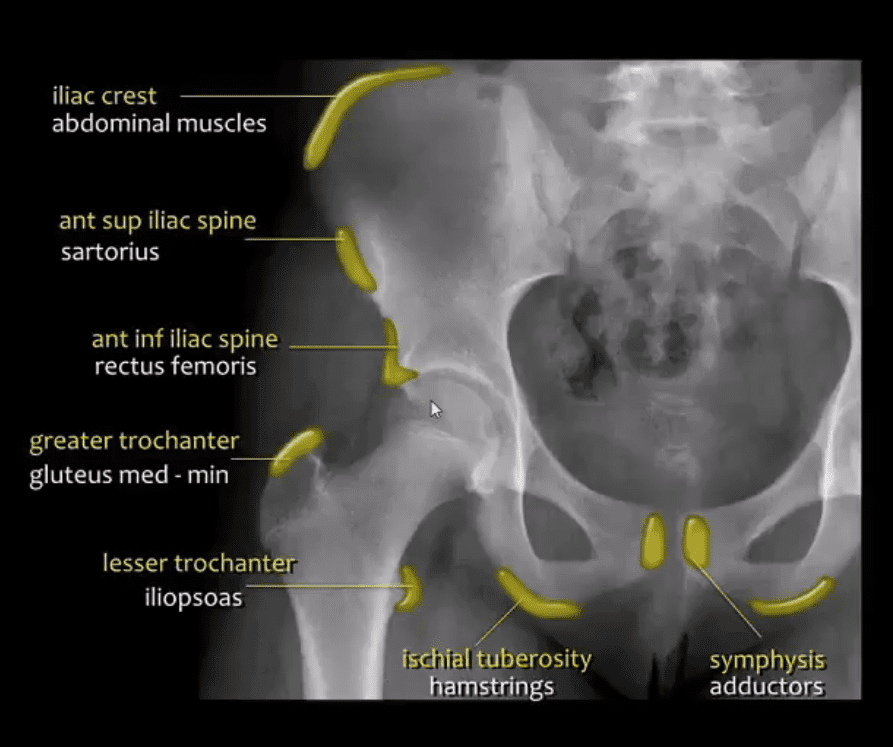
Appreciating anatomical sites of pelvic origin/insertion of different muscles will help Dx of pelvic avulsion Fx
Avulsion Fx of the AllS (origin of the direct head of Rectus femoris M)
Pelvic avulsions occur by sudden eccentric contraction especially during kicking or jumping
Imaging: x-radiography will suffice
Clinically: sudden snap or pop followed by local pain. Pt can weight bear
Care: non-operative with rest for 4-weeks. Non-union is rare. No major complications
DDx: key rad DDx feature is not to mistake an avulsion from an aggressive pediatric bone tumor-like osteosarcoma that may show some exuberant new bone formation d/t healing and bone callus
Commonly Encountered Unstable Pelvic Fractures
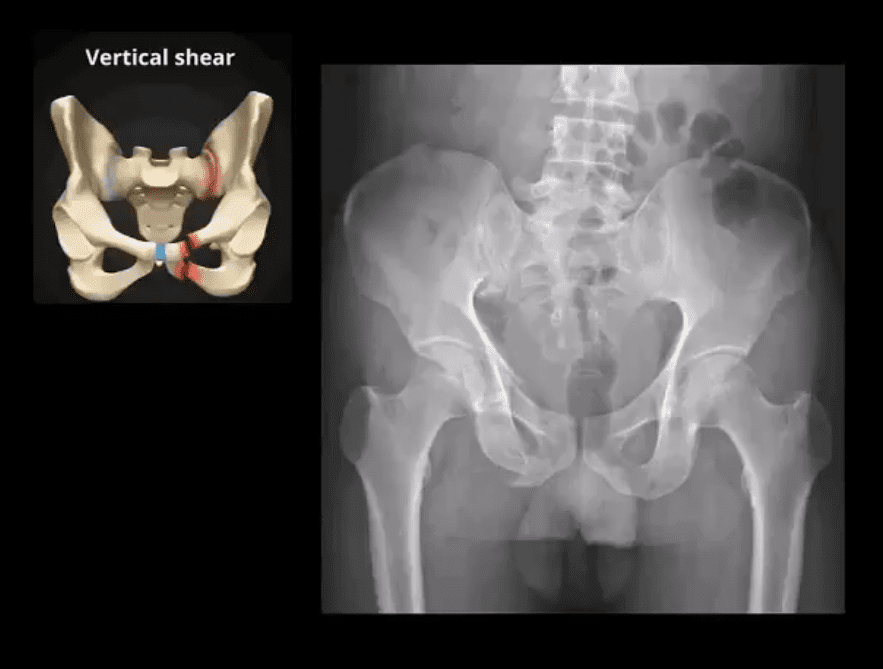
Malgaigne Fx: d/t vertical shear injury to the ipsilateral pelvis
Rad Dx: ipsilateral superior and inferior pubic rami Fx (anterior ring) with ipsilateral SIJ separation/Fx of the sacrum and adjacent ilium (posterior ring). Symphysis pubis diastasis can be seen. An additional clue is an avulsion of L4 and/or L5 TP that often signifies serious pelvic injury
Clinically: marked leg shortening, shock, inability to weight bear.
Damage to Superior Gluteal Artery can occur
Imaging: x-radiography followed by CT scanning w/o and with IV contrast esp. if visceral injury present
Care: surgical in most cases d/t significant instability. ORIF. Hemostasis, Pelvic stabilization
Prognosis: depends on the complexity, rate of visceral complications and stability. 10% Superior glut artery bleed requiring rapid hemostasis
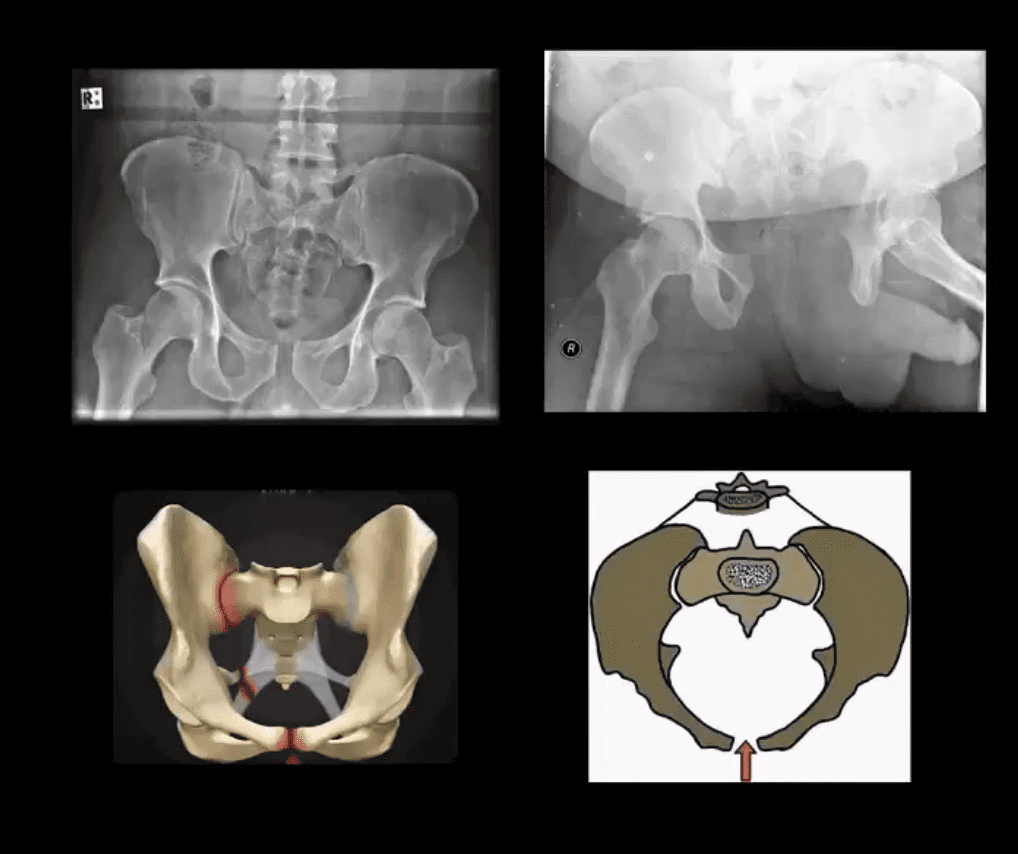
Open Book Pelvis (major instability)
Mechanism: AP compression of different force magnitude (picture depiction)
Rad Dx: diastasis of symphysis pubis with diastasis of SIJ with and w/o adjacent Fx of the ala
Imaging steps: x-radiographic, CT scanning with and w/o contrast for vascular injury, cystography for acute urinary bladder rupture
Immediate and delayed complications may occur: vascular injury, urethral/bladder injury
Straddle Injury: Unstable Fx
Mechanism: direct impact/collision
High risk of urinary bladder/urethral injury
Imaging: bilateral superior and inferior pubic rami Fx with or w/o diastasis and Fx of SIJ
CT with and w/o contrast for vascular injury
Cystourethrogram additionally evaluates a urogenital injury
2) Osteoporotic patients with low impact, trivial or no trauma (i.e., insufficiency Fx)
X-radiography is crucial to early Dx and prevention of complications which include:
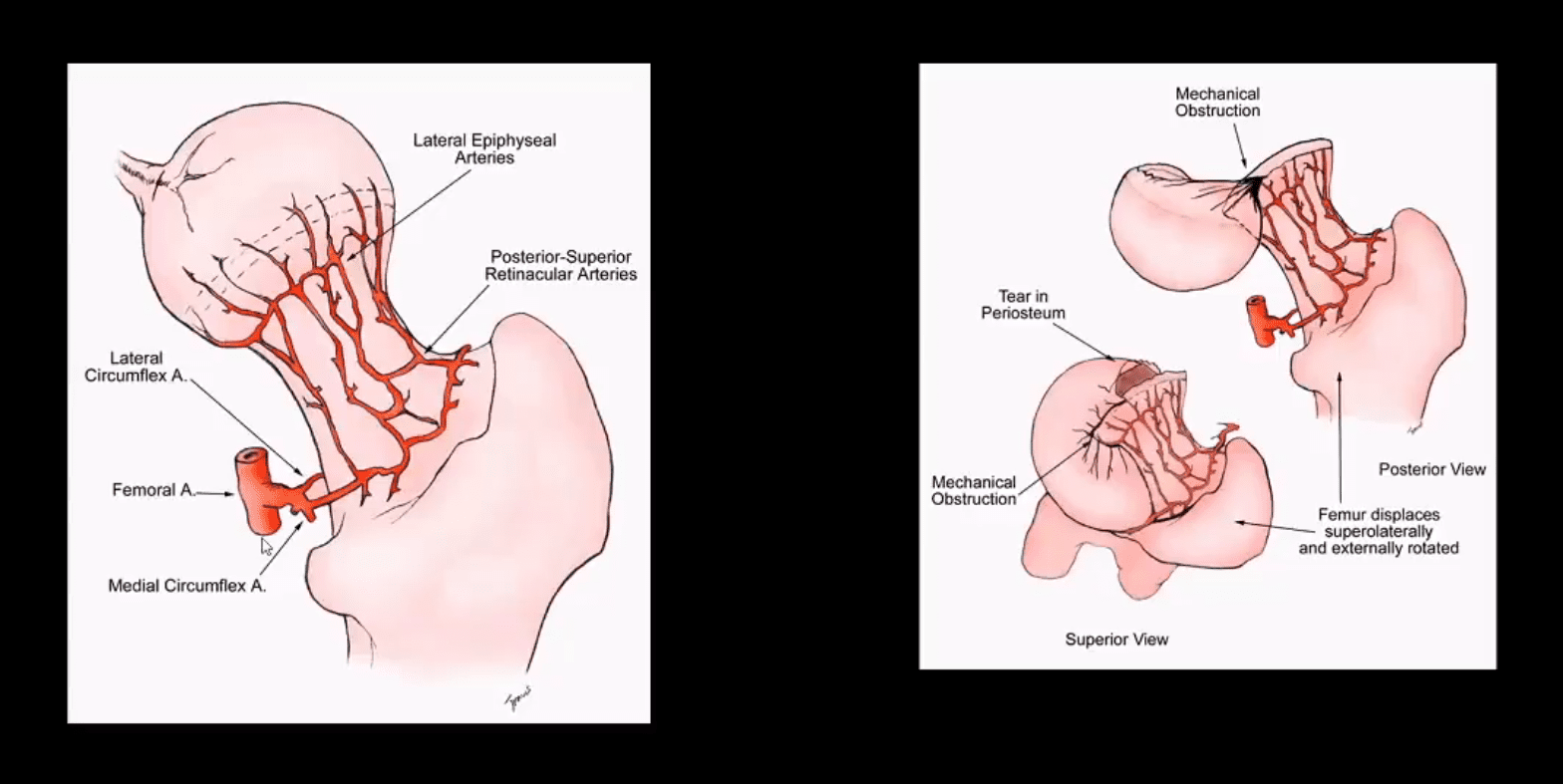
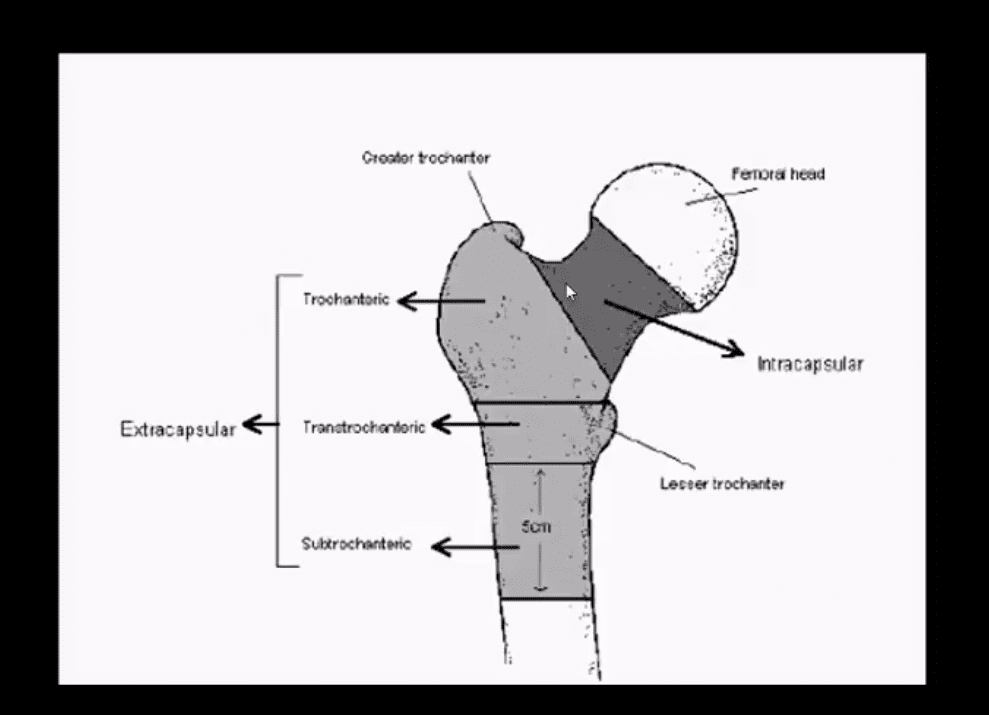
Dx: intra-capsular vs. extra-capsular Fx
Ischemic osteonecrosis aka avascular necrosis (AVN) of the femoral head and rapid disabling DJD
Epidemiology: USA has some of the highest rates of OSP hip Fx worldwide. Highest healthcare cost Fx to treat overall
Women>men, Caucasians>African-Americans
25-30% mortality within the 1st year. Mortality depends on co-morbidities and stat of activity prior Fx
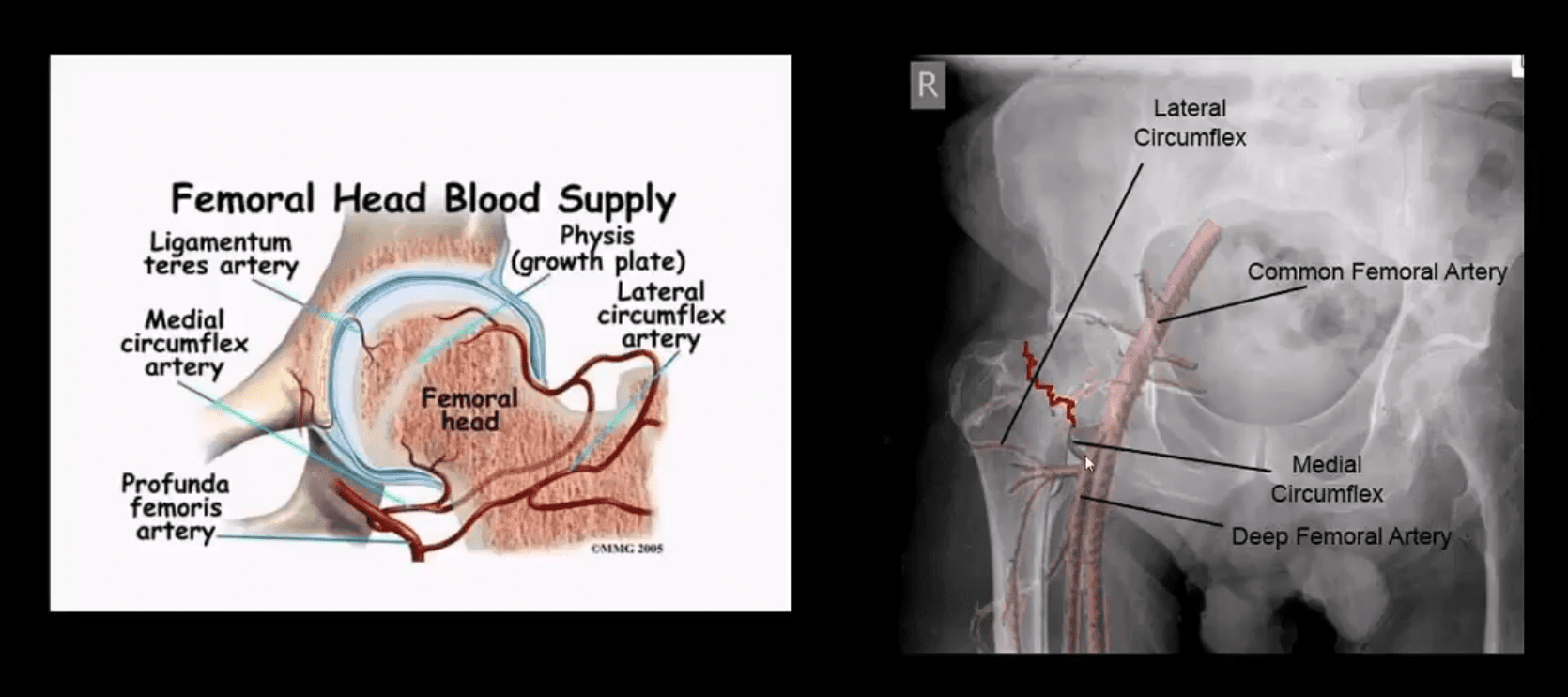
Pathophys: the femoral neck is intra-capsular and transmits arterial flow to the head. The neck is uncovered by the periosteum and unable to develop a good callus. The neck transmits maximum tensile forces through the proximal femur and prone to Fx and non-union
The vast majority of clinically suspected bone Mets are found in the axial skeleton and proximal femurs/humeri
Radiography is the most cost-effective and readily available initial imaging tool to investigate bone Mets but often fails early metastatic detection
Tc99 bone scintigraphy is the most sensitive and cost-effective imaging modality to demonstrate metastatic foci
MR imaging may help� regional identification of bone Mets especially if x-radiography is unrewarding
Significant limitations of MRI: inability to perform a whole-body MRI scan
Cost and other contraindications such as cardiac pacemakers and cochlear implants may be another limiting factor
Marrow Based Neoplasms
Malignancy originating from the marrow cells are often referred to as “round-cell tumors.”
Multiple Myeloma (MM)
Lymphoma
Ewing’s sarcoma
The last two are less frequent than MM
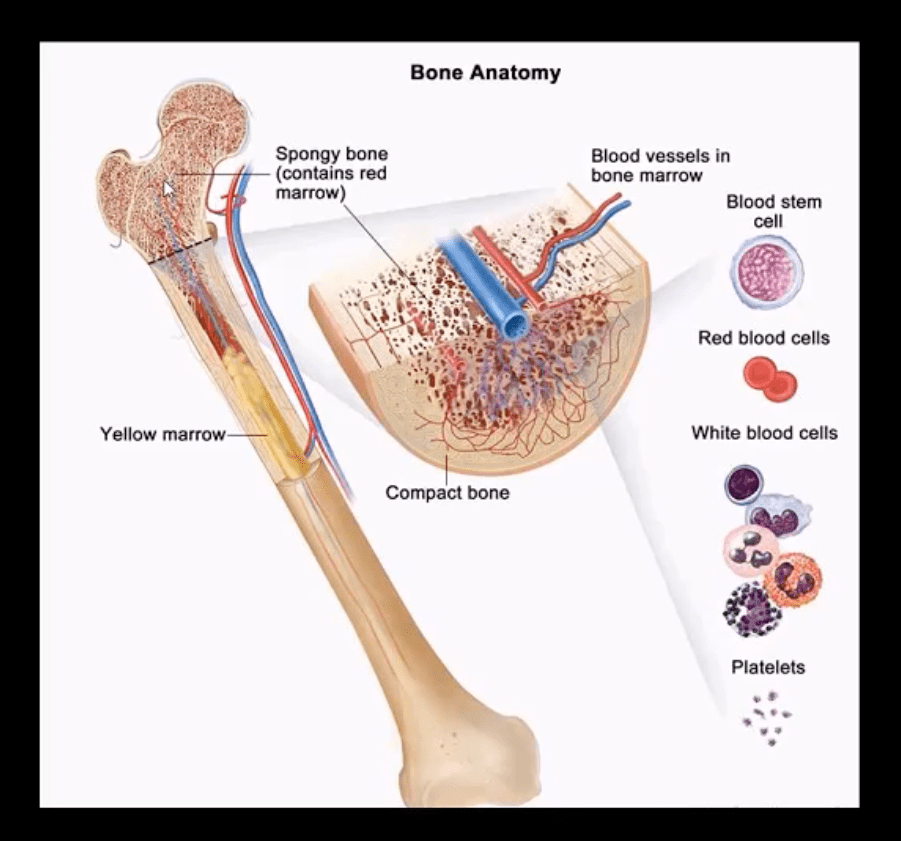
Red marrow in adults is in the axial skeleton and proximal femurs/humeri d/t gradual marrow “retraction” following the childhood
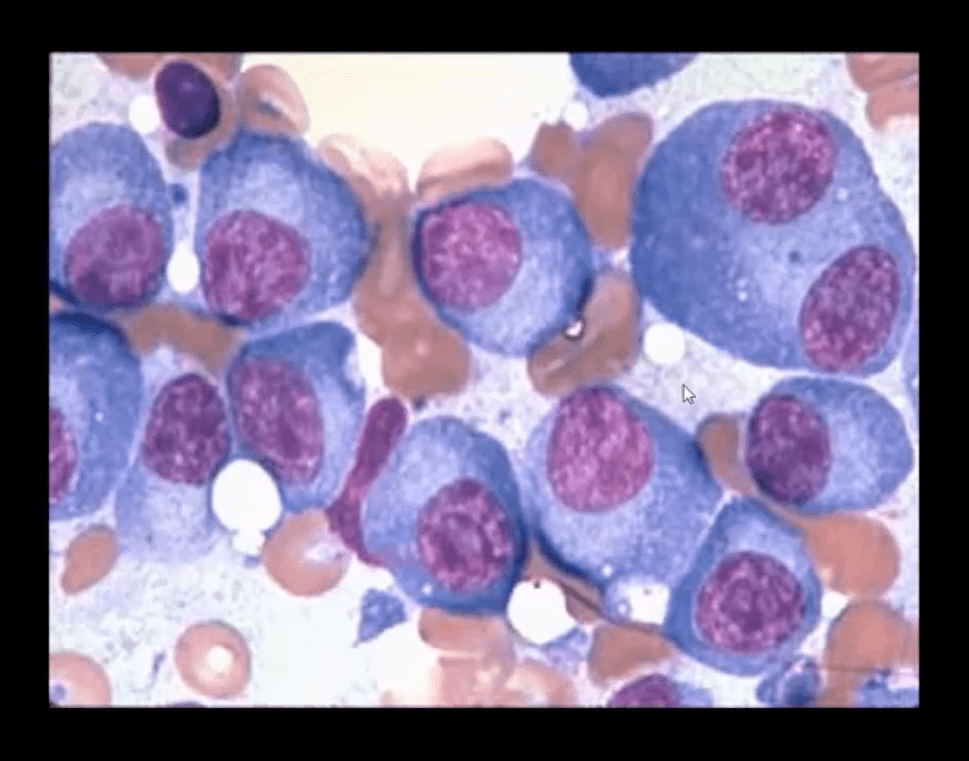
Note bone marrow biopsy histopathology specimen of MM with abnormal plasma cells replacing regular marrow residents (above image)
Multiple Myeloma (MM) is the most common primary bone neoplasm in adults>40s. Etiology is unknown, but many theories exist (e.g., genetic, environmental, radiation, chronic inflammation, MGUS)
MM: malignant proliferation of plasma cells >10% of red marrow, with subsequent replacement of normal marrow cells by myeloma cells and overproduction of monoclonal antibodies paraproteins (M protein) with heavy chains IgG (52%), IgA (21%), IgM (12%) and light chains kappa or lambda aka Bence-Jones proteins
Clinical Presentation of MM
MM is occasionally detected as unexplained anemia on routine blood studies for unrelated complaints
Common MSK symptoms: Bone pain/Pathologic fractures
Diagnostic imaging plays an essential role during the Dx of MM
Bone marrow aspiration biopsy, blood tests, and serum protein electrophoresis may be used
Imaging approach: bone pain is investigated with initial x-radiographs if radiographs are unrewarding MR imaging may help to reveal bone marrow abnormality. MRI is recommended as myeloma survey
Currently, MRI protocol known as “whole body myeloma scan” consisting of T1, T2-fat suppressed, and T1+C coronal sequences can detect MM in the skull, spine, pelvis, ribs and femurs/humeri. This technique is much more superior to radiographic “skeletal myeloma survey.”
Tc99 bone scintigraphy is not typically used for MM because over 30% of MM lesions are “cold” or photopenic on radionuclide bone scan d/t highly lytic nature of MM with osteoclasts outpacing osteoblasts.
A radiographic skeletal survey is considered more sensitive than bone scintigraphy in MM
PET-CT scanning of MM is gaining popularity due to the high level of detection of multiple sites of MM
Radiographic Dx of MM: consists of identification of characteristically localized focal osteolytic “punched out” or “moth-eaten” lesions of variable sizes following the distribution of adults red marrow
Note rad abnormality is known as “raindrop skull” is characteristic of MM
Radiographic appearance of MM may vary from “punched out” round radiolucencies to “moth-eaten” or permeating osteolytic lesion producing endosteal scalloping (yellow arrow)
Pelvis and femurs are commonly affected by MM and present radiographically as round lytic punched out or moth-eaten lesions
N.B. Occasionally MM may pose radiographic dilemma by presenting as generalized osteopenia in the spine that can be difficult to differentiate from age-related osteoporosis
MR imaging of MM reveals� marrow changes with low signal on T1, a high signal on fluid-sensitive sequences and bright contrast enhancement on T1+C gad d/t increased vasculature and high activity of� MM cells
Example of full-body MRI of “whole body myeloma scan” with T2-fat suppressed (A), T1 (B) and T1+C (C) pulse sequences produced in coronal slices
Note multiple foci of bone marrow changes in the spine pelvis and femurs
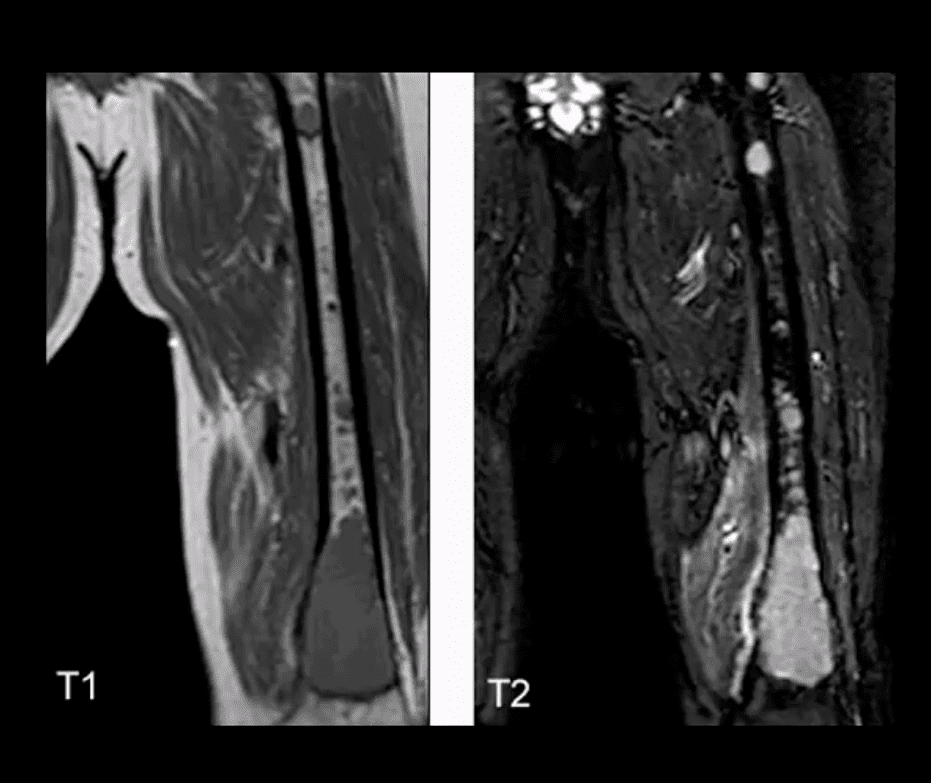
Miscellaneous Neoplasms of the Spinal Column
Chordoma: is relatively uncommon but considered the m/c primary malignant neoplasm that only affects the spine. D/t slow growth is often misdiagnosed for a considerable length of time as LBP
Pathology: derives from malignant transformation of notochordal cells presented as mucoid, gelatinous mass containing physaliphorous cells
Demo:�M: F 3:1 (30-70S). 50%-sacrococcygeal, 35% spheno-occipital 15%-spine
Clinically: asymptomatic for a long time until non-specific LBP, changes in bladder & bowel, neurological signs are less common d/t midline “outward” growth & inferior to S1. Local invasion worsens prognosis. 60%-survive 5-years, 40%-10-years, Mets are delayed, poor prognosis d/t local invasion. >50% can be id. on DRE.
Imaging:�x-rays often tricky d/t overlying gas/feces. CT is >sensitive to id the bone mass and internal calcifications. MRI: T2 bight signal, T1 heterogeneously low and high d/t mucus/blood decomposition, MRI best detects local invasion and essential for care planning. Rx:� complete excision is often impossible d/t local vascular invasion.
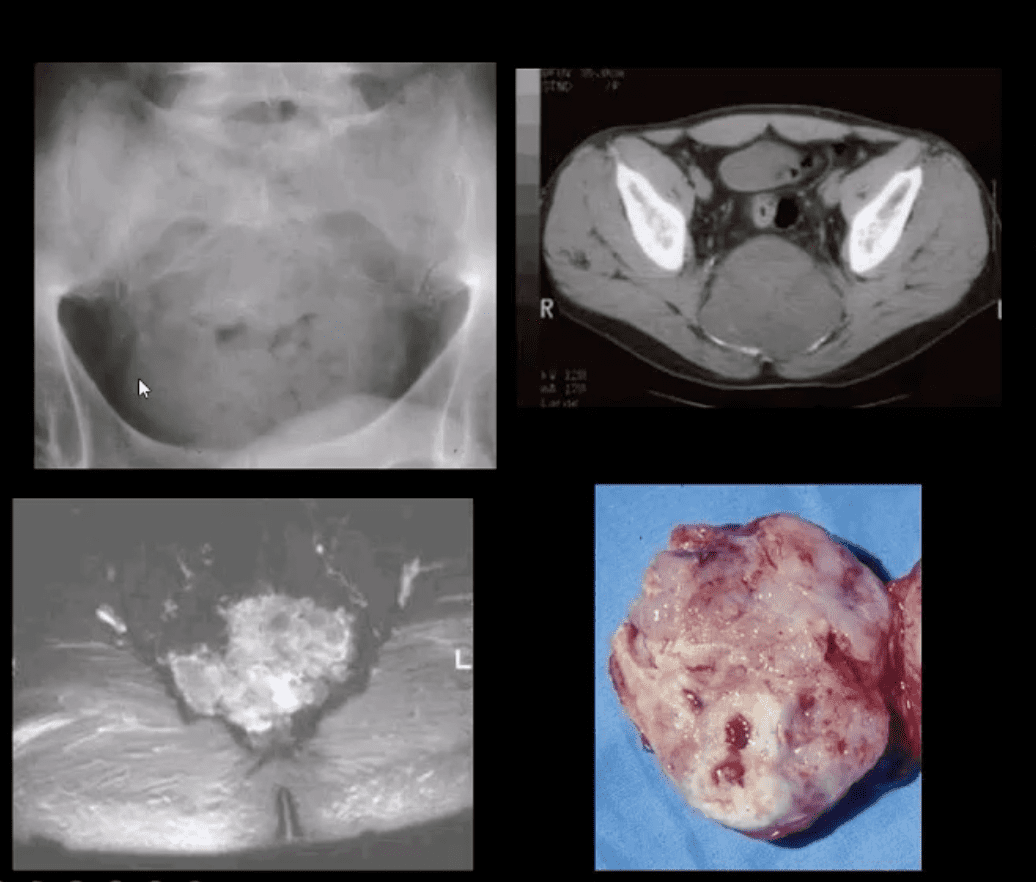
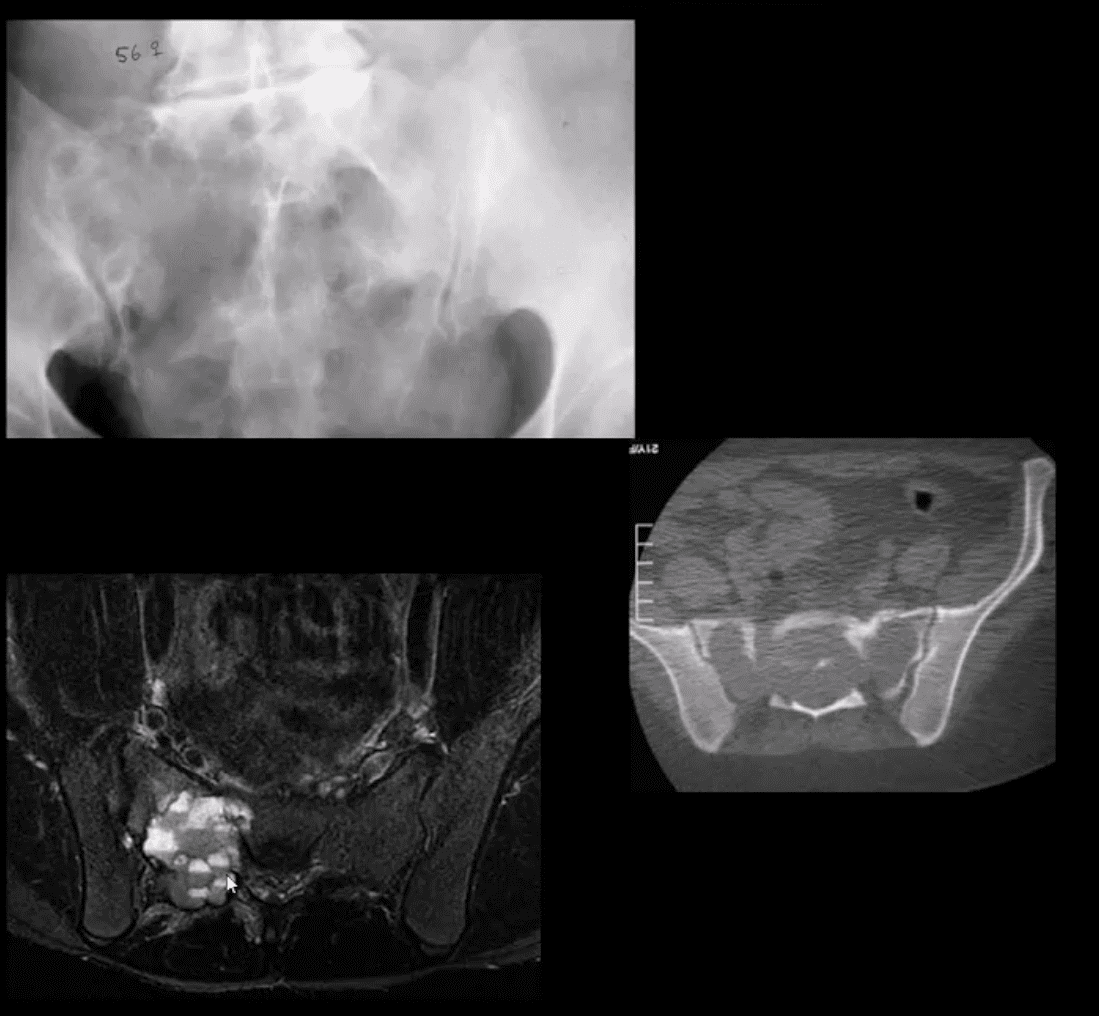
Giant cell tumor (GCT):�2nd most common primary sacral tumor. It is a histolgically benign neoplasm containing multinucleated Giant cells of Monocyte-Osteoclast origin
Imaging Dx:�x-radiography is the 1st step usually in response to complaints of LBP. Often challenging to id on x-rays d/t bowel gas/feces
Key rad feature: osteolytic expansile lesion noted by destruction of sacral arcuate lines. CT may id the lesion better. MRI is the modality of choice following x-rays. MRI: T1 low to intermediate signal. Heterogeneously high d/t edema with areas of low signal on T2 d/t blood degradation and fibrosis. Characteristic fluid-fluid levels may be noted especially if ABC develops within a GCT. Rx: operative. Prognosis is less favorable than GCT in long bones d/t lung Mets (deposits) in 13.7%
Aneurysmal Bone Cysts (ABC) are benign expansile tumor-like bone lesions (not a true neoplasm) composed and filled with numerous blood-filled channels. Thus the term “blood sponge.” ABC is m/c id in children and adolescents
Unknown etiology: trauma and pre-existing bone neoplasm (e.g., GCT) often reported. Clinically: pain that may be progressive d/t rapid nature of ABC expansion. In the spine, ABC m/c affects posterior elements and presented as expansile, soap-bubbly or lytic lesion.
DDx: can be broad, but Osteoblastoma and GCT are the top DDxs.
Imaging: x-rays demo expansile mass in posterior elements, CT is more sensitive than x-rays, MRI will demo characteristic fluid-fluid levels and mixed high and low signal d/t edema and blood decomposition/aging with some septations.
N.B. MRI fluid-fluid levels are not exclusive to ABC, and DDx includes GCT, osteoblastoma, telangiectatic osteosarcoma.
Rx: operative curettage and bone grafting, fibrosing agents. Recurrence 10-30%.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine