Defeat Chronic Pain: If you are one of the estimated 50 to 100 million Americans who struggles with Chronic Pain, you are aware of just how miserable and life-altering it can be. There is not a single area of you life that remains unaffected. You no longer sleep well. Your SEX LIFE is non-existent. Everyday activities have become your own personal �Mount Everest �. You cannot concentrate because the pain IS ALWAYS ON YOUR MIND. It is wearing you out, physically, mentally, and emotionally. It’s sapping your ability to think clearly or make decisions. In short we’re here to defeat chronic pain.
People can see the pain on your face and in your eyes. Chronic Pain and the inability to do the things you love, is making you feel DEPRESSED (not the other way around like your doctor may have suggested). Recent studies have even shown that brains of people suffering with Chronic Pain, show patterns of atrophy that are virtually indistinguishable from what is seen in patients with dementia or ALZHEIMER’S. In fact, a recent study from a prominent Canadian University showed that Chronic Pain causes the brain to degenerate at almost 10 times the rate of someone without pain!
Although Chronic Pain may seem hopeless, there are some things that you can do to help yourself � even though your doctor undoubtedly failed to educate you in this regard. Some of the most basic of these include eating only healthy foods (I recommend a PALEO DIET), taking only WHOLE FOOD SUPPLEMENTS, drinking more WATER, giving up the CIGARETTES, and EXERCISING to the degree that you can (difficult when suffering with Chronic Pain or FIBROMYALGIA).
Although DOING THESE SIMPLE THINGS will certainly help a large percentage who suffer and be able to defeat chronic pain; there is a significant percentage of you whose pain is not greatly diminished by these measures. It is for you that I created this website. But before we move on to treatment of Chronic Pain, you must first understand what Chronic Pain is and how it really works.
Defeat Chronic Pain: It Works Like This
For years, neuro-scientists have known that Chronic Pain can cause brain atrophy (shrinkage) that is indistinguishable from Alzheimer�s or Dementia. More recently, the prestigious Journal of Neuroscience reported research from McGill University showing that, “The longer the individual has had Fibromyalgia, the greater the gray matter loss, with each year of Fibromyalgia being equivalent to 9.5 times the loss in normal aging”. Think about this statement for a moment. Every single year you live with some sort of CHRONIC PAIN SYNDROME (or syndromes as the case may be) is the equivalent of nearly 10 times the brain loss seen in the normal aging process. Re-read this paragraph until the urgency of your situation sinks in!
Although there are several types of pain (the study of Chronic Pain can get extremely complex), we are going to try and keep this as simple as possible. For our purposes, there are two types of Chronic Pain. It has to do with where the pain comes from. Chronic Pain originates in one of the two following areas.
The Central Nervous System
The Body
As we will discuss shortly, Chronic Pain that arises in the CNS is frequently ‘learned’ pain. Let me explain. In order to learn how to SHOOT FREE THROWS, use chop sticks, PLAY THE PIANO, speak Swahili, you have to practice. Everyone remembers the old adage; Practice makes Perfect. If you stimulate pain pathways in the Brain & Nervous System long enough, or are exposed to enough stressors in your life (CHEMICAL, AUTOIMMUNE, EMOTIONAL, DIETARY, FOOD SENSITIVITIES, PHYSICAL, BACTERIAL, VIRAL, PARASITIC, FUNGAL, MOLD, ELECTROMAGNETIC, etc), you can alter the way your Brain and Central Nervous System function.
Hopefully your pain, even though severe, is still Type II (THE THREE TYPES OF PAIN). As people start losing control of numerous areas of physiology (DIGESTION, HORMONAL, IMMUNITY, BLOOD SUGAR REGULATION, HYPERSENSITIVITY, DYSBIOSIS, etc), the problems ramp up. Over time this pain can (will) become locked into the brain. Although pathological Pain Syndromes arising from a malfunctioning CNS are not the most common causes of Chronic Pain, if this is where you are at, you are going to have to find a way to deal with these underlying issues (FUNCTIONAL NEUROLOGY can be a fantastic starting point). Although I provide information that helps many people help themselves with the severe metabolic and neurological problems, this website is chiefly devoted to defeat chronic Pain that is not locked into the Brain, but is instead originating from the body (Type II Pain).
Defeat Chronic Pain: Nociception
“Simple Nociception” is the most basic type of pain. If someone steps on your toe, it hurts. This is normal, and means that your nervous system is functioning properly. Get the person off your toe, and the pain goes away — almost immediately. Simple. There are several different types of Nociceptive Pain, but the one that we are most concerned about on this website is the one that has to do with ‘deep’ musculoskeletal pain, otherwise known as Deep Somatic Pain (Greek �Soma� = body). Deep Somatic Pain is pain that originates in tissues that are considered to be ‘deep’ in the body. Although we do not always think of many of these tissue types as being deep, this category includes things like LIGAMENTS, TENDONS, MUSCLES, FASCIA, blood vessels, and bones. There are two main types of Nociceptors, chemical and mechanical.
I. Chemical Nociception
The Chemical Nociceptors are stimulated by noxious chemicals. The chief of these are the chemicals we collectively refer to as INFLAMMATION (bear in mind that once Inflammation is involved, we begin moving away from Type I pain and into Type II pain — Nociception is still involved, but so is the Inflammatory Cascade). Inflammation is actually made up of a large group of chemicals manufactured within your body as part of the normal Immune System response. They have names like prostaglandins, leukotrienes, histamines, cytokines, kinins, etc, etc, etc. When these chemicals are out of increased beyond what’s needed for normal tissue repair, the result will be a whole host of health problems —- and Chronic Pain.
Although “SYSTEMIC INFLAMMATION” is at the root of the vast majority of America’s health problems (DIABETES, CANCER, FIBROMYALGIA, THYROID PROBLEMS, ARTHRITIS, HEART DISEASE, and numerous others), you will soon see that even though Inflammation is always involved with the tissues of the “Deep Soma,” it sometimes gets more credit than it deserves. However, you also have to be aware that exposing MICROSCOPIC SCAR TISSUE to chronic inflammation can potentially hyper-sensitize nerves. This hypersensitization makes the nerves within Scar Tissue as much as 1,000 times more pain sensitive than normal (the work of the famous neurologist, DR. CHAN GUNN).
INCREASED TISSUE ACIDITY (usually caused by hypoxia — diminished tissue oxygen levels) is another common form of Chemical Nociception. This frequently occurs as the result of a JUNKY DIET, but is also caused by relentless Mechanical / Neurological / Immune System Dysfunction. It is a big reason that my Decompression Protocols utilize OXYGEN THERAPY extensively.
II. Mechanical Nociception
As you can imagine, Mechanical Dysfunction stimulates the Mechanical Nociceptors. This group of nociceptors (pain receptors) is stimulated by constant mechanical stress in the tissues of the Deep Soma — particularly ligaments, tendons, and fascia. Mechanical tension, mechanical deformation, mechanical pressure, etc are the things that cause Mechanical Nociception, which can in turn, cause pain — chronic, unrelenting, pain. Remove the offending mechanical stressor, and you can oftentimes remove the pain. Sounds simple, doesn�t it? Unfortunately, nothing is ever quite as simple as it initially appears.
Be aware that Nociceptive Pain can actually become Brain-Based over time. This is called ‘Supersensitivity’ and is caused by alterations in the Brain and Central Nervous System that perpetuate the pain cycle (many in the medical community are calling it CENTRALIZATION OR CENTRAL SENSITIZATION. In Mechanical Nociception, even though the injured tissue has, according to all of the medical tests, HEALED, it has healed improperly; i.e. microscopic scar tissue and tissue adhesion — particularly in the FASCIA. I probably do not need to tell you that this can be really really bad news — particularly because it is a significant feature of what I call “CHRONIC PAIN’S PERFECT STORM“.
As nerve function and PROPRIOCEPTION become increasingly fouled up, degenerative arthritis and joint deterioration begin to set in (HERE). Because of involvement in the Brain or Central Nervous System, this kind of pain is often referred to as Neuropathic Pain or Neruogenic Pain. Sometimes people end up with HYPERALGIA (Extreme sensitivity to pain. Stimulus that should cause a little pain, causes extraordinary amounts of pain). Or they end up with ALLODYNIA (Stimulus which do not normally elicit any pain at all, now causes pain). Sometimes these two overlap. Stay with me and you will begin to understand why.
Defeat Chronic Pain: Hypersensitized Nerves Relationship To Injured Or Damaged Fascia
Think of nerve endings as the twigs at the very end of a tree limb. Nerves (just like a tree) begin with a large trunk, which splits / divides into smaller and smaller branches until eventually you arrive at the end � the tiny twig (or nerve ending) at the end of the very smallest branches.
If you have ever seen a �topped� tree, you can understand what happens to nerve endings that are found in microscopic scar tissue. Professional Tree Trimmers cut (or �top�) the largest branches just above where the trunk splits into two or three limbs. What happens to these stubs? Instead of having limbs that continue to branch out and divide into ever-smaller limbs in a normal fashion, you get a stub or stump, that in a short matter of time, swells up and has hundreds of tiny twig-like limbs growing from it. �Topping� stimulates the growth of twigs from the stump. The injured nerves found in microscopic scar tissue act in much the same way.
As the larger nerves that are found in soft tissues are injured, you end up with an inordinate number of immature nerve endings (twigs) growing out of an inflamed nerve �stump�. As you might imagine, extra pain receptors are never a good thing! And because there in Inflammation present, this often leads to Microscopic Scar Tissue, which, even though it is up to 1,000 times more pain-sensitive than normal tissue, cannot be seen with even the most technologically advance imaging techniques such as CT / MRI (HERE). This is a commonly seen phenomenon in Facial Adhesions, and is why even though the people living this nightmare believe that because their pain is so severe that it should make their MRI “Glow Red”, it shows nothing. This tends to lead to deer-in-the-headlight looks when you ask your doctor what might be causing your pain, not to mention accusations of malingering, drug seeking, or attempting to get on Disability.
Defeat Chronic Pain: Nerves Are Like Tree Branches
Uninjured Nerves
Photo by Stephen McCulloch
Injured Nerves
Photo by Linda Bailey
Defeat Chronic Pain: Fascial Adhesions
Microscopic Scar Tissue & Chronic Pain
One of the biggest revelations for many people suffering with Chronic Pain is the absurd numbers of CHRONIC PAINSYNDROMES brought on by microscopic scarring of the FASCIA. It gets even worse once you realize that this Fascia is the most pain-sensitive tissue in the body —- yet it does not show up on even the most technologically advanced imaging techniques, including MRI. Simply read our “Fascia” page to see why microscopic scarring of this specific “Connective Tissue” is at the root of all sorts of Chronic Pain Cases — not to mention ILL HEALTH.
Have you ever experienced low back pain? If you haven’t already, there’s a high probability you will present at least one case of back pain sometime during your lifetime. Back pain is one of the most prevalent spine health issues reported among the population of the United States, affecting up to 80 percent of Americans at some point in their lives. Back pain is not a specific disease, rather it is a symptom which may develop as a result of a variety of injuries and/or conditions.�Although most cases typically resolve on their own, the effective treatment of acute low back pain is essential towards preventing chronic low back pain.
Chiropractors and physical therapists frequently utilize a similar series of treatment methods, such as spinal adjustments and manual manipulations as well as massage and physical therapy, to help treat symptoms of back and low back pain. Many healthcare professionals, however, have started using the McKenzie method to manage acute back pain. The purpose of the following article is to educate patients on the effectiveness of the McKenzie method for acute non-specific low back pain.
The McKenzie Method for the Management of Acute Non-Specific Low Back Pain: Design of a Randomised Controlled Trial
Abstract
Background
Low back pain (LBP) is a major health problem. Effective treatment of acute LBP is important because it prevents patients from developing chronic LBP, the stage of LBP that requires costly and more complex treatment.
Physiotherapists commonly use a system of diagnosis and exercise prescription called the McKenzie Method to manage patients with LBP. However, there is insufficient evidence to support the use of the McKenzie Method for these patients. We have designed a randomised controlled trial to evaluate whether the addition of the McKenzie Method to general practitioner care results in better outcomes than general practitioner care alone for patients with acute LBP.
Methods/Design
This paper describes the protocol for a trial examining the effects of the McKenzie Method in the treatment of acute non-specific LBP. One hundred and forty eight participants who present to general medical practitioners with a new episode of acute non-specific LBP will be randomised to receive general practitioner care or general practitioner care plus a program of care based on the McKenzie Method. The primary outcomes are average pain during week 1, pain at week 1 and 3 and global perceived effect at week 3.
Discussion
This trial will provide the first rigorous test of the effectiveness of the McKenzie Method for acute non-specific LBP.
Background
In Australia, low back pain (LBP) is the most frequently seen musculoskeletal condition in general practice and the seventh most frequent reason for consulting a physician[1,2]. According to the Australian National Health Survey, 21% of Australians reported back pain in 2001; additionally, the Australian Bureau of Statistic’s 1998 Survey of Disability, Ageing and Carers estimated that over one million Australians suffer from some form of disability associated with back problems[1].
LBP poses an enormous economic burden to society in countries such as the USA, UK and The Netherlands[3]. In the largest state in Australia, New South Wales, back injuries account for 30% of the cost of workplace injuries, with a gross incurred cost of $229 million in 2002/03[4]. It is expected that most people with an acute episode of LBP will improve rapidly, but a proportion of patients will develop persistent lower levels of pain and disability[5,6]. Those patients with chronic complaints are responsible for most of the costs[6]. Effective treatment of acute LBP is important because it prevents patients from developing chronic LBP, the stage of LBP that requires costly and more complex treatment.
There is a growing concern about effectiveness of treatments for LBP, as reflected in the large number of systematic reviews published in the last 5 years addressing this issue. [7-12]. Despite the large amount of evidence regarding LBP management, a definitive conclusion on which is the most appropriate intervention is not yet available. A comparison of 11 international clinical practice guidelines for the management of LBP showed that the provision of advice and information, together with analgesics and NSAIDs, is the approach consistently recommended for patients with an acute episode[13]. Most guidelines do not recommend specific exercises for acute LBP because trials to date have concluded that it is not more effective than other active treatments, or than inactive or placebo treatments[8]. However, some authors have suggested that the negative results observed in trials of exercises are a consequence of applying the same exercise therapy to heterogeneous groups of patients. [14-16]. This hypothesis has some support from a recent high-quality randomised trial in which treatment based on a diagnostic classification system led to larger reductions in disability and promoted faster return to work in patients with acute LBP than the therapy recommended by the clinical guidelines[17].
In 1981, McKenzie proposed a classification system and a classification-based treatment for LBP labelled Mechanical Diagnosis and Treatment (MDT), or simply McKenzie Method[18]. Of the large number of classification schemes developed in the last 20 years [19-26], the McKenzie Method has the greatest empirical support (e.g. validity, reliability and generalisability) among the systems based on clinical features[27] and therefore seems to be the most promising classification system for implementation in clinical practice.
Physiotherapists commonly adopt the McKenzie Method for treating patients with LBP[28,29]. A survey of 293 physiotherapists in 1994 found that 85% of them perceived the McKenzie Method as moderately to very effective[28]. Nevertheless, a recent systematic review concluded that there is insufficient evidence to evaluate the effectiveness of the McKenzie Method for patients with LBP [30]. A critical concern is that most trials to date have not implemented the McKenzie Method appropriately. The most common flaw is that all trial participants are given the same intervention regardless of classification, an approach contradictory to the principles of McKenzie therapy.
The primary aim of this trial is to evaluate whether the addition of the McKenzie Method to general practitioner (GP) care results in better outcomes than GP care alone for patients with acute non-specific LBP when effect is measured in terms pain, disability, global perceived effect, and persistent symptoms.
Methods
The University of Sydney Human Research Ethics Committee granted approval for this study.
Study Sample
One hundred and forty eight participants with a new episode of acute non-specific LBP who present to GPs will be recruited for the study. A new episode of LBP will be defined as an episode of pain lasting longer than 24 hours, preceded by a period of at least one month without LBP and in which the patient did not consult a health care practitioner[31]. Participants will be screened for eligibility at their first appointment with the GP according to the inclusion and exclusion criteria.
Inclusion Criteria
To be eligible for inclusion, participants must have pain extending in an area between the twelfth rib and buttock crease (this may or may not be accompanied by leg pain); pain of at least 24 hours duration; pain of less than 6 weeks duration; and they need to be eligible for referral to private physiotherapy practice within 48 hours.
Exclusion Criteria
Participants will be excluded if they have one of the following conditions: nerve root compromise (defined as 2 positive tests out of sensation, power and reflexes for the same spinal nerve root); known or suspected serious spinal pathology; spinal surgery within the preceding 6 months; pregnancy; severe cardiovascular or metabolic disease; or inability to read and understand English.
Recruiting GPs will record the number of patients who are invited to participate, the number who decline to participate, and the number of screened patients who are ineligible and their reasons for declining participation or ineligibility. Written consent will be obtained for each participant.
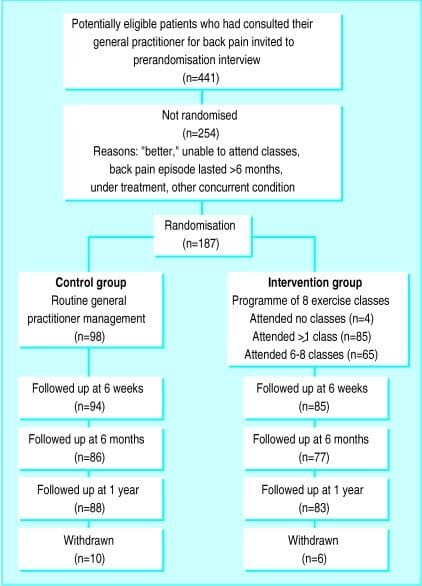
Subjects who volunteer to participate and satisfy the eligibility criteria will receive baseline treatment and then be randomly allocated to one of the study groups. To ensure equal-sized treatment groups, random permuted blocks of 4�8 participants will be used[32]. Randomisation will be stratified by Workcover compensation status. The stratified random allocation schedule will be generated by a person not otherwise involved in recruitment, assessment or treatment of subjects and the randomisation sequence will be placed in sequentially numbered, sealed envelopes. The flow of participants through the study is detailed in Figure ?1.
Figure 1: Flow of participants through the study. Legend: GP � General practitioner; NRS � Numeric pain rating scale; PSFS � Patient-specific functional scale; RMQ � Roland-Morris questionnaire; GPE � Global perceived effect; LBP � Low back pain.
Dr. Alex Jimenez’s Insight
In the management of low back pain, the attitudes, beliefs and treatment preferences of chiropractors, as well as that of physical therapists, can determine the most effective outcome measures in the care of patients with different types of spinal health issues. According to the following evidence-based research studies, the McKenzie method has been deemed to be one of the most useful treatment approaches for managing symptoms in patients with back and low back pain. Exercise and physical activity is also one of the most common treatment preferences for improving an individual’s strength, mobility and flexibility. Every healthcare professional varies in respect to their specific treatment preferences. These variations emphasize the need to identify the most effective treatment approach to guarantee proper treatment of LBP.
Outcome Measures
The McKenzie protocol is thought to promote rapid symptom improvement in patients with LBP[33,34] and this is one of the reasons that therapists choose this therapy. Therefore it is important to focus assessment on short-term outcomes. The primary outcomes will be:
Usual pain intensity over last 24 hours recorded each morning in a pain diary over the first week. Pain will be measured on a 0�10 numerical rating scale (NRS). The unit of analysis will be the mean of the 7 measures[35];
Usual pain intensity over last 24 hours (0�10 NRS) recorded at 1 and 3 weeks[35];
Global perceived effect (0�10 GPE) recorded at 3 weeks.
The secondary outcomes will be:
Global perceived effect (0�10 GPE) recorded at 1 week;
Patient-generated measure of disability (Patient-Specific Functional Scale; PSFS) recorded at 1 and 3 weeks[36];
Condition-specific measure of disability (Roland Morris Questionnaire; RMQ) recorded at 1 and 3 weeks[37];
Number of patients reporting persistent back pain at 3 months.
Following the screening consultation in which the inclusion and exclusion criteria are assessed, the GP will supervise the baseline measurement of pain. All patients will then receive an assessment booklet and a pre-paid envelope in which all other self-assessed outcome measures are to be recorded and sealed. One member of the research team will contact patients by telephone within 24 hours of the consultation with the GP in order to give explanations regarding the appropriate form of filling in the assessment booklet. At this time, other baseline outcomes will be recorded and then the patient will be randomised to study groups. The patient will be advised to keep the booklet at home, to seal it into the pre-paid envelope after the final assessment and mail the sealed envelope to the research team. To ensure the proper use of the assessment booklet and to avoid loss of data due to non-returned booklets, a blinded assessor will contact all patients by telephone 9 and 22 days after the consultation with the GP to collect patient’s answers from the 1st week and 3rd week assessments, respectively.
The procedure for obtaining outcome data will be followed for all participants, regardless of compliance with trial protocols. At 3 months, data regarding the presence of persistent (chronic) symptoms will be collected by telephone. Participants will be asked to answer the following yes-no question: “During the past 3 months have you ever been completely free of low back pain? By this I mean no low back pain at all and would this pain-free period have lasted for a whole month”. Those answering no will be considered to have persistent LBP. Information on additional treatment and the direct costs with low back pain management will also be collected at 3 months.
A secondary analysis will be performed on predictors of response to McKenzie treatment and prediction of chronicity. This will involve the measurement of participants’ expectation about the helpfulness of both treatments under investigation as well as information on the occurrence of the centralisation phenomenon. Expectation will be recorded prior to randomisation according to the procedures described by Kalauokalani et al[38].
Treatments
All participants will receive GP care as advocated by the NHMRC guideline for the management of acute musculoskeletal pain[2]. Guideline-based GP care consists of providing information on a favourable prognosis of acute LBP and advising patients to stay active, together with the prescription of paracetamol. Patients randomised to the experimental group will be referred to physiotherapy to receive the McKenzie Method. A research assistant not involved in the assessment or treatment of subjects will be responsible for the randomisation process and will contact therapists and patients to arrange the first physiotherapy session. The McKenzie treatment will be delivered by credentialed physiotherapists who will follow the treatment principles described in McKenzie’s text book[18]. All therapists will have completed the four basic courses taught by the McKenzie Institute International. To ensure the appropriate implementation of the McKenzie’s classification algorithm, a training session with a member of McKenzie’s educational program will be conducted prior to the commencement of the study. The treatment frequency will be at the discretion of the therapist with a maximum of 7 sessions over 3 weeks. We chose to restrict the McKenzie treatment to a maximum of 7 sessions based on the study of Werneke and colleagues[39], which concluded that further reductions in pain and function are not expected if favourable changes in pain location are not present until the seventh treatment visit. Treatment procedures from the McKenzie Method are summarised in the Appendix.
Participants randomised to the control group will continue their GP care as usual. All participants regardless of intervention group will be advised not to seek other treatments for their low back pain during the treatment period. Physiotherapists will be asked to withhold co-interventions during the course of the trial.
Several mechanisms will be used to ensure that the trial protocol is applied consistently. Protocol manuals will be developed and all involved researchers (GPs, physiotherapists, assessor, and statistician) will be trained to ensure that screening, assessment, random allocation and treatment procedures are conducted according to the protocol. A random sample of treatment sessions will be audited to check that treatment is being administered according to the protocol.
Data Analysis
Power was calculated based on the primary outcome measures (pain intensity and global perceived effect). A sample size of 148 participants will provide 80% power to detect a difference of 1 unit (15%) on a 0�10 pain scale (SD = 2.0) between the experimental and control groups, assuming alpha of 0.05. This allows for loss to follow-up of 15%. This sample size also allows the detection of a difference of 1.2 units (12%) on a 0�10 global perceived effect scale (SD = 2.4).
Data will be analysed by a research member blinded to group status. The primary analysis will be by intention-to-treat. In order to estimate treatment effects, between-group mean differences (95%CI) will be calculated for all outcome measures. In the primary analysis these will be calculated using linear models that include baseline values of outcome variables as covariates to maximise precision.
Discussion
We have presented the rationale and design of an RCT evaluating the effects of the McKenzie Method in the treatment of acute non-specific LBP. The results of this trial will be presented as soon as they are available.
Competing Interests
The author(s) declare that they have no competing interests.
Authors’ Contributions
LACM, CGM and RDH were responsible for the design of the study. HC was responsible for recruiting McKenzie therapists and she will also participate as a clinician in the trial. LACM and JMc will act as trial coordinators. All authors have read and approved the final manuscript.
Appendix
Clinical picture and treatment principles according to the McKenzie Method
This table summarises the procedures involved in the McKenzie Method (Table 1). For detailed description of all procedures and progressions, refer to McKenzie’s text book. This is particularly important for Derangement syndrome since the treatment is extremely variable and complex and the full description of procedures would not be appropriate for the purposes of this paper.
The authors thank the physiotherapists credentialed in the McKenzie Method for their participation in this project.
Managing Low Back Pain: Attitudes & Treatment Preferences of Physical Therapists & Chiropractors
Abstract
Background and Purpose:�Researchers surveyed physical therapists about their attitudes, beliefs, and treatment preferences in caring for patients with different types of low back pain problems.
Subjects and Methods: Questionnaires were mailed to all 71 therapists employed by a large health maintenance organization in western Washington and to a random sample of 331 other therapists licensed in the state of Washington.
Results: Responses were received from 293 (74%) of the therapists surveyed, and 186 of these claimed to be practicing in settings in which they treat patients who have back pain. Back pain was estimated to account for 45% of patient visits. The McKenzie method was deemed the most useful approach for managing patients with back pain, and education in body mechanics, stretching, strengthening exercises, and aerobic exercises were among the most common treatment preferences. There were significant variations among therapists in private practice, hospital-operated, and health maintenance organization settings with respect to treatment preferences, willingness to take advantage of the placebo effect, and mean number of visits for patients with back pain.
Conclusions and Discussion: These variations emphasize the need for more outcomes research to identify the most effective treatment approaches and to guide clinical practice.
In conclusion,�the effective treatment of acute low back pain is essential because it can potentially help prevent the development of chronic low back pain. A growing number of chiropractors and physical therapists, including other healthcare professionals, have utilized the McKenzie method to help manage acute non-specific low back pain in patients. According to the research study, further evidence is required to support the use of the McKenzie method for LBP, however, the outcome measures of the research study regarding the effectiveness of the McKenzie method for low back pain are promising. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is referred to as a collection of symptoms rather than a single type of injury or condition. The symptoms are characterized as radiating pain, numbness and tingling sensations from the sciatic nerve in the lower back, down the buttocks and thighs and through one or both legs and into the feet. Sciatica is commonly the result of irritation, inflammation or compression of the largest nerve in the human body, generally due to a herniated disc or bone spur.
Australian Institute of Health and Welfare . Australia’s health 2004. 1st. Camberra , AIHW; 2004.
Australian Acute Musculoskeletal Pain Guidelines Group Evidence-based management of acute musculoskeletal pain. . 2003. http://www.nhmrc.gov.au
Maetzel A, Li L. The economic burden of low back pain: a review of studies published between 1996 and 2001. Best Pract Res Clin Rheumatol. 2002;16:23�30. doi: 10.1053/berh.2001.0204. [PubMed][Cross Ref]
WorkCover Authority NSW . Statistical Bulletin. NSW Workers Compensation 2002/03. Sydney , The WorkCover Authority NSW ; 2003.
Pengel LH, Herbert RD, Maher CG, Kathryn RM. Acute low back pain: Systematic review of its prognosis. BMJ. 2003;327:1�5. [PMC free article][PubMed]
Thomas E, Silman AJ, Croft PR, Papageorgiou AC, Jayson M, Macfarlane GJ. Predicting who develops chronic low back pain in primary care: a prospective study. BMJ. 1999;318:1662�1667. [PMC free article][PubMed]
Guzm�n J, Esmail R, Karjalainen K, Malmivaara A, Irvin E, Bombardier C. Multidisciplinary rehabilitation for chronic low back pain: systematic review. BMJ. 2001;322:1511�1516. doi: 10.1136/bmj.322.7301.1511. [PMC free article][PubMed][Cross Ref]
van Tulder M, Malmivaara A, Esmail R, Koes B. Exercise therapy for low back pain. A systematic review within the framework of the Cochrane Collaboration Back Review Group. Spine. 2000;25:2784�2796. doi: 10.1097/00007632-200011010-00011. [PubMed][Cross Ref]
van Tulder M, Ostelo R, Vlaeyen JWS, Linton SJ, Morley SJ, Assendelft WJJ. Behavioral treatment for chronic low back pain. A systematic review within the framework of the Cochrane Back Review Group. Spine. 2000;25:2688�2699. doi: 10.1097/00007632-200010150-00024. [PubMed][Cross Ref]
Jellema P, van Tulder MW, van Poppel MN, Nachemson AL, Bouter LM. Lumbar supports for prevention and treatment of low back pain. A systematic review within the framework of the Cochrane Back Review Group. Spine. 2001;26:377�386. doi: 10.1097/00007632-200102150-00014. [PubMed][Cross Ref]
Ferreira ML, Ferreira PH, Latimer J, Herbert RD, Maher CG. Does spinal manipulative therapy help people with chronic low back pain? Aust J Physiother. 2002;48:277�284. [PubMed]
Pengel HM, Maher CG, Refshauge KM. Systematic review of conservative interventions for subacute low back pain. Clin Rehabil. 2002;16:811�820. doi: 10.1191/0269215502cr562oa. [PubMed][Cross Ref]
Koes BW, van Tulder MW, Ostelo R, Burton K, Waddell G. Clinical guidelines for the management of low back pain in primary care: an international comparison. Spine. 2001;26:2504�2514. doi: 10.1097/00007632-200111150-00022. [PubMed][Cross Ref]
Borkan J, Koes B, Reis S, Cherkin DC. A report from the Second International Forum for Primary Care Research on low back pain: reexamining priorities. Spine. 1998;23:1992�1996. doi: 10.1097/00007632-199809150-00016. [PubMed][Cross Ref]
Bouter LM, van Tulder MW, Koes BW. Methodologic issues in low back pain research in primary care. Spine. 1998;23:2014�2020. doi: 10.1097/00007632-199809150-00019. [PubMed][Cross Ref]
Leboeuf-Yde C, Lauritsen JM, Lauritzen T. Why has the search for causes of low back pain largely been nonconclusive? Spine. 1997;22:877�881. doi: 10.1097/00007632-199704150-00010. [PubMed][Cross Ref]
Fritz JM, Delitto A, Erhard RE. Comparison of classification-based physical therapy with therapy based on clinical practice guidelines for patients with acute low back pain. Spine. 2003;28:1363�1372. doi: 10.1097/00007632-200307010-00003. [PubMed][Cross Ref]
McKenzie R, May S. The lumbar spine. Mechanical diagnosis & therapy. 2nd. Vol. 1. Waikanae , Spinal Publications New Zealand Ltd; 2003. p. 374.
van Dillen LR, Sahrmann SA, Norton BJ, Caldwell CA, McDonnell MK, Bloom NJ. Movement system impairment-based categories for low back pain: stage 1 validation. J Orthop Sports Phys Ther. 2003;33:126�142. [PubMed]
BenDebba M, Torgerson WS, Long DM. A validated, practical classification procedure for many persistent low back pain patients. Pain. 2000;87:89�97. doi: 10.1016/S0304-3959(00)00278-5. [PubMed][Cross Ref]
Delitto A, Erhard RE, Bowling RW, DeRosa CP, Greathouse DG. A treatment-based classification approach to low back syndrome: identifying and staging patients for conservative treatment. Phys Ther. 1995;75:470�485. [PubMed]
Klapow JC, Slater MA, Patterson TL, Doctor JN, Atkinson JH, Garfin SR. An empirical evaluation of multidimensional clinical outcome in chronic low back pain patients. Pain. 1993;55:107�118. doi: 10.1016/0304-3959(93)90190-Z. [PubMed][Cross Ref]
Laslett M, van Wijmen P. Low back and referred pain: diagnosis and proposed new system of classification. N Z J Physiother. 1999;27:5�14.
Maluf KS, Sahrmann SA, van Dillen LR. Use of a classification system to guide nonsurgical management of a patient with chronic low back pain. Phys Ther. 2000;80:1097�1111. [PubMed]
Petersen T, Laslett M, Thorsen H, Manniche C, Ekdahl C, Jacobsen S. Diagnostic classification of non-specific low back pain. A new system integrating patho-anatomic and clinical categories. Physiother Theory Pract. 2003;19:213�237.
Stiefel F, deJonge P, Huyse F, al INTERMED – An assessment and classification system for case complexity: Results in patients with low back pain. Spine. 1999;24:378�384. doi: 10.1097/00007632-199902150-00017. [PubMed][Cross Ref]
McCarthy CJ, Arnall FA, Strimpakos N, Freemont A, Oldham JA. The biopsychosocial classification of non-specific low back pain: a systematic review. Phys Ther Rev. 2004;9:17�30. doi: 10.1179/108331904225003955. [Cross Ref]
Batti� MC, Cherkin DC, Dunn R, Ciol MA, Wheeler KJ. Managing low back pain: attitudes and treatment preferences of physical therapists. Phys Ther. 1994;74:219�226. [PubMed]
Li LC, Bombardier C. Physical therapy management of low back pain: An exploratory survey of therapist approaches. Phys Ther. 2001;81:1018�1028. [PubMed]
Machado LAC, de Souza MS, Ferreira PH, Ferreira ML. The McKenzie protocol for low back pain: a systematic review of the literature with a meta-analysis approach. Spine (in press) 2005. [PubMed]
de Vet HCWPD, Heymans MWMS, Dunn KMMP, Pope DPPD, van der Beek AJPD, Macfarlane GJPD, Bouter LMPD, Croft PRPD. Episodes of Low Back Pain: A Proposal for Uniform Definitions to Be Used in Research. Spine. 2002;27:2409�2416. doi: 10.1097/00007632-200211010-00016. [PubMed][Cross Ref]
Pocock SJ. Clinical trials. A practical approach. 1st. Chichester , John Wiley & Sons; 1984.
Delitto A, Cibulka MT, Erhard RE, Bowling RW, Tenhula JA. Evidence for use of an extension-mobilization category in acute low back syndrome: A prescriptive validation pilot study. Phys Ther. 1993;73:216�228. [PubMed]
Schenk RJ, Jozefczyk C, Kopf A. A randomized trial comparing interventions in patients with lumbar posterior derangement. J Manual Manip Ther. 2003;11:95�102.
Farrar J, Young J, LaMoreaux L, al Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain. 2001;94:149�158. doi: 10.1016/S0304-3959(01)00349-9. [PubMed][Cross Ref]
Stratford P, Gill C, Westaway M, Binkley J. Assessing disability and change on individual patients: a report of a patient specific measure. Physiother Can. 1995;47:258�263.
Roland M, Morris R. A study of the natural history of back pain. Part I: development of a reliable and sensitive measure of disability in low-back pain. Spine. 1983;8:141�144. [PubMed]
Kalauokalani D, Cherkin D, Sherman K, Koepsell T, R D. Lessons from a trial of acupuncture and massage for low back pain. Spine. 2001;26:1418�1424. doi: 10.1097/00007632-200107010-00005. [PubMed][Cross Ref]
Werneke M, Hart DL, Cook D. A descriptive study of the centralization phenomenon. A prospective analysis. Spine. 1999;24:676�683. doi: 10.1097/00007632-199904010-00012. [PubMed][Cross Ref]
Shin Splint: Whether you are an avid exerciser, an exuberant shopper, or a small child chaser, you have probably felt tightening and burning in your shin at one point in your life. Sometimes, the pain stops when the activity ceases, but other times the pain remains. If shin pain continues bothering you, it may be time to face the fact you have shin splints.
The shin is a bone located in the front part of your lower leg. Shin splints commonly occur in athletes who have intensified or changed their training routines. They also show up in regular people who have changed or added activity to their routine.
The shin has a lot of responsibility during exercise, as it absorbs the shock of the steps, raises the toes, and support the arch of the foot.
A few main culprits play a part in shin splints:
failing to stretch properly before exercising
walking or running on hard surfaces, like pavement
wearing the wrong type of shoes during activity
over-exerting the body with strenuous activity
skipping periods of rest between exercise
Individuals who perform any type of exercise should take appropriate measures to alleviate the above risk factors of shin splints. If you notice pain and soreness in the front part of your lower leg, know how to treat this injury properly.
If rest and ice aren�t doing the job and you’re still suffering pain, it’s time to see a doctor. A thorough exam and possibly an x-ray will diagnose the problem.
Chiropractic care is a powerful choice for treating shin splints and reducing their recurrence.
Chiropractic Treatment Benefits Those Suffering From Shin Splint/s:
Reduction In Pain
Chiropractic is proven to relieve the pain associated with bodily injuries and medical conditions, including shin splints. Sometimes one visit is enough to relieve the pain, other times the pain decreases over a series of appointments. Being able to diminish a high degree of pain down to a manageable level is possible for shin splint patients through chiropractic.
Full Body Alignment
The premise behind chiropractic is that it treats the body as a whole, and, in doing so, promotes healing and health to the injured or diseased areas. A chiropractor may work on your neck to help your calf. With shin splints, he or she may align your spine and joints to lessen the impact of activity on your shins. Again, the entire body is treated in order to create the best environment for health restoration.
Healing Through Adjustments
Treating shin splints is a common procedure for chiropractors. Common practice is to adjust the calf, ankle, and foot to stretch and increase blood flow to the area.
Drug Free Treatment Option
A primary benefit of chiropractic care is it requires no over-the-counter or prescription drugs. Individuals who suffer from stomach issues, or simply prefer to avoid drugs, find chiropractic visits a productive alternative to manage pain and promote healing.
It’s routine for chiropractic treatment of shin splints to include a series of stretching and strengthening exercises the individual performs at home between visits. These exercises further expand on the positive effects of the chiropractic therapy.
If you are one of the many people dealing with shin splints, don’t despair! Consider chiropractic care as your main treatment option or in conjunction with other modes of treatment. Within a few visits, you will experience pain reduction, and enjoy a decreased risk of ever dealing with painful shin splints again.
Based on statistical findings, approximately more than three million people in the United States are injured in an automobile accident every year. In fact, auto accidents are considered to be one of the most common causes for trauma or injury. Neck injuries, such as whiplash, frequently occur due to the sudden back-and-forth movement of the head and neck from the force of the impact. The same mechanism of injury can also cause soft tissue injuries in other parts of the body, including the lower back as well as the lower extremities. Neck, hip, thigh and knee injuries are common types of injuries resulting from auto accidents.
Abstract
Objective: The purpose of this systematic review was to determine the effectiveness of exercise for the management of soft tissue injuries of the hip, thigh, and knee.
Methods: We conducted a systematic review and searched MEDLINE, EMBASE, PsycINFO, the Cochrane Central Register of Controlled Trials, and CINAHL Plus with Full Text from January 1, 1990, to April 8, 2015, for randomized controlled trials (RCTs), cohort studies, and case-control studies evaluating the effect of exercise on pain intensity, self-rated recovery, functional recovery, health-related quality of life, psychological outcomes, and adverse events. Random pairs of independent reviewers screened titles and abstracts and assessed risk of bias using the Scottish Intercollegiate Guidelines Network criteria. Best evidence synthesis methodology was used.
Results: We screened 9494 citations. Eight RCTs were critically appraised, and 3 had low risk of bias and were included in our synthesis. One RCT found statistically significant improvements in pain and function favoring clinicbased progressive combined exercises over a �wait and see� approach for patellofemoral pain syndrome. A second RCT suggests that supervised closed kinetic chain exercises may lead to greater symptom improvement than open chain exercises for patellofemoral pain syndrome. One RCT suggests that clinic-based group exercises may be more effective than multimodal physiotherapy in male athletes with persistent groin pain.
Conclusion: We found limited high-quality evidence to support the use of exercise for the management of soft tissue injuries of the lower extremity. The evidence suggests that clinic-based exercise programs may benefit patients with patellofemoral pain syndrome and persistent groin pain. Further high-quality research is needed. (J Manipulative Physiol Ther 2016;39:110-120.e1)
Soft tissue injuries of the lower limb are common. In the United States, 36% of all injuries presenting to emergency departments are sprains and/or strains of the lower extremity. Among Ontario workers, approximately 19% of all approved lost time compensation claims are related to lower extremity injuries. Moreover, 27.5% of Saskatchewan adults injured in a traffic collision report pain in the lower extremity. Soft tissue injuries of the hip, thigh, and knee are costly and place a significant economic and disability burden on workplaces and compensation systems. According to the US Department of Labor Bureau of Statistics, the median time off work for lower extremity injuries was 12 days in 2013. Knee injuries were associated with the longest work absenteeism (median, 16 days).
Most soft tissue injuries of the lower limb are managed conservatively, and exercise is commonly used to treat these injuries. Exercise aims to promote good physical health and restore normal function of the joints and surrounding soft tissues through concepts which include range of motion, stretching, strengthening, endurance, agility, and proprioceptive exercises. However, the evidence about the effectiveness of exercise for managing soft tissue injuries of the lower limb is unclear.
Previous systematic reviews have investigated the effectiveness of exercise for the management of soft tissue injuries of the lower extremity. Reviews suggest that exercise is effective for the management of patellofemoral pain syndrome and groin injuries but not for patellar tendinopathy. To our knowledge, the only review reporting on the effectiveness of exercise for acute hamstring injuries found little evidence to support stretching, agility, and trunk stability exercises.
The purpose of our systematic review was to investigate the effectiveness of exercise compared to other interventions, placebo/sham interventions, or no intervention in improving self-rated recovery, functional recovery (eg, return to activities, work, or school), or clinical outcomes (eg, pain, health-related quality of life, depression) of patients with soft tissue injuries of the hip, thigh, and knee.
Methods
Registration
This systematic review protocol was registered with the International Prospective Register of Systematic Reviews on March 28, 2014 (CRD42014009140).
Eligibility Criteria
Population. Our review targeted studies of adults (?18 years) and/or children with soft tissue injuries of the hip, thigh, or knee. Soft tissue injuries include but are not limited to grade I to II sprains/strains; tendonitis; tendinopathy; tendinosis; patellofemoral pain (syndrome); iliotibial band syndrome; nonspecific hip, thigh, or knee pain (excluding major pathology); and other soft tissue injuries as informed by available evidence. We defined the grades of sprains and strains according to the classification proposed by the American Academy of Orthopaedic Surgeons (Tables 1 and 2). Affected soft tissues in the hip include the supporting ligaments and muscles crossing the hip joint into the thigh (including the hamstrings, quadriceps, and adductor muscle groups). Soft tissues of the knee include the supporting intra-articular and extra-articular ligaments and muscles crossing the knee joint from the thigh including the patellar tendon. We excluded studies of grade III sprains or strains, acetabular labral tears, meniscal tears, osteoarthritis, fractures, dislocations, and systemic diseases (eg, infection, neoplasm, inflammatory disorders).
Interventions. We restricted our review to studies that tested the isolated effect of exercise (ie, not part of a multimodal program of care). We defined exercise as any series of movements aimed at training or developing the body by routine practice or as physical training to promote good physical health.
Comparison Groups. We included studies that compared 1 or more exercise interventions to one another or one exercise intervention to other interventions, wait list, placebo/sham interventions, or no intervention.
Outcomes. To be eligible, studies had to include one of the following outcomes: (1) self-rated recovery; (2) functional recovery (eg, disability, return to activities, work, school, or sport); (3) pain intensity; (4) health-related quality of life; (5) psychological outcomes such as depression or fear; and (6) adverse events.
Study Characteristics. Eligible studies met the following criteria: (1) English language; (2) studies published between January 1, 1990, and April 8, 2015; (3) randomized controlled trials (RCTs), cohort studies, or case-control studies which are designed to assess the effectiveness and safety of interventions; and (4) included an inception cohort of a minimum of 30 participants per treatment arm with the specified condition for RCTs or 100 participants per group with the specified condition in cohort studies or case-control studies. Studies including other grades of sprains or strains in the hip, thigh, or knee had to provide separate results for participants with grades I or II sprains/strains to be included.
We excluded studies with the following characteristics: (1) letters, editorials, commentaries, unpublished manuscripts, dissertations, government reports, books and book chapters, conference proceedings, meeting abstracts, lectures and addresses, consensus development statements, or guideline statements; (2) study designs including pilot studies, cross-sectional studies, case reports, case series, qualitative studies, narrative reviews, systematic reviews (with or without meta-analyses), clinical practice guidelines, biomechanical studies, laboratory studies, and studies not reporting on methodology; (3) cadaveric or animal studies; and (4) studies on patients with severe injuries (eg, grade III sprains/strains, fractures, dislocations, full ruptures, infections, malignancy, osteoarthritis, and systemic disease).
Information Sources
We developed our search strategy with a health sciences librarian (Appendix 1). The Peer Review of Electronic Search Strategies (PRESS) Checklist was used by a second librarian to review the search strategy for completeness and accuracy. We searched MEDLINE and EMBASE, considered to be the major biomedical databases, and PsycINFO, for psychological literature through Ovid Technologies, Inc; CINAHL Plus with Full Text for nursing and allied health literature through EBSCOhost; and the Cochrane Central Register of Controlled Trials through Ovid Technologies, Inc, for any studies not captured by the other databases. The search strategy was first developed in MEDLINE and subsequently adapted to the other bibliographic databases. Our search strategies combined controlled vocabulary relevant to each database (eg, MeSH for MEDLINE) and text words relevant to exercise and soft tissue injuries of the hip, thigh, or knee including grade I to II sprain or strain injuries (Appendix 1). We also hand searched the reference lists of previous systematic reviews for any additional relevant studies.
Study Selection
A 2-phase screening process was used to select eligible studies. Random pairs of independent reviewers screened citation titles and abstracts to determine the eligibility of studies in phase 1. Screening resulted in studies being classified as relevant, possibly relevant, or irrelevant. In phase 2, the same pairs of reviewers independently screened the possibly relevant studies to determine eligibility. Reviewers met to reach consensus on the eligibility of studies and resolve disagreements. A third reviewer was used if consensus could not be reached.
Assessment of Risk of Bias
Independent reviewers were randomly paired to critically appraise the internal validity of eligible studies using the Scottish Intercollegiate Guidelines Network (SIGN) criteria. The impact of selection bias, information bias, and confounding on the results of a study was qualitatively evaluated using the SIGN criteria. These criteria were used to guide reviewers in making an informed overall judgment on the internal validity of studies. This methodology has been previously described. A quantitative score or a cutoff point to determine the internal validity of studies was not used for this review.
The SIGN criteria for RCTs were used to critically appraise the following methodological aspects: (1) clarity of the research question, (2) randomization method, (3) concealment of treatment allocation, (4) blinding of treatment and outcomes, (5) similarity of baseline�characteristics between/among treatment arms, (6) cointervention contamination, (7) validity and reliability of outcome measures, (8) follow-up rates, (9) analysis according to intention-to-treat principles, and (10) comparability of results across study sites (where applicable). Consensus was reached through reviewer discussion. Disagreements were resolved by an independent third reviewer when consensus could not be reached. The risk of bias of each appraised study was also reviewed by a senior epidemiologist (PC). Authors were contacted when additional information was needed to complete the critical appraisal. Only studies with low risk of bias were included in our evidence synthesis.
Data Extraction and Synthesis of Results
Data were extracted from studies (DS) with low risk of bias to create evidence tables. A second reviewer independently checked the extracted data. We stratified results based on the duration of the condition (recent onset [0-3 months], persistent [N3 months], or variable duration [recent onset and persistent combined]).
We used standardized measures to determine the clinical importance of changes reported in each trial for common outcome measures. These include a between-group difference of 2/10 points on the Numeric Rating Scale (NRS), 2/10 cm difference on the Visual Analog Scale (VAS), and 10/100 point difference on the Kujala Patellofemoral scale, otherwise known as the Anterior Knee Pain Scale.
Statistical Analyses
Agreement between reviewers for the screening of articles was computed and reported using the ? statistic and 95% confidence interval (CI). Where available, we used data provided in the studies with a low risk of bias to measure the association between the tested interventions and the outcomes by computing the relative risk (RR) and its 95% CI. Similarly, we computed differences in mean changes between groups and 95% CI to quantify the effectiveness of interventions. The calculation of 95% CIs was based on the assumption that baseline and follow-up outcomes were highly correlated (r = 0.80).
Reporting
This systematic review was organized and reported based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement.
Dr. Alex Jimenez’s Insight
As a doctor of chiropractic, automobile accident injuries are one of the most common reasons people seek chiropractic care. From neck injuries, such as whiplash, to headaches and back pain, chiropractic can be utilized to safely and effectively restore the integrity of the spine after a car crash. A chiropractor like myself will often use a combination of spinal adjustments and manual manipulations, as well as a variety of other non-invasive treatment methods,�to gently correct any spinal misalignments resulting from an auto accident injury. Whiplash and other types of neck injuries occur when the complex structures along the cervical spine are stretched beyond their natural range of movement due to the sudden back-and-forth movement of the head and neck from the force of the impact. Back injury, particularly in the lower spine, are also common as a result of an automobile accident. When the complex structures along the lumbar spine are damaged or injured, symptoms of sciatica may radiate down the lower back, into the buttocks, hips, thighs, legs and down into the feet. Knee injuries may also occur upon impact during an auto accident. Exercise is frequently used with chiropractic care to help promote recovery as well as improve strength, flexibility and mobility. Rehabilitation exercises are offered to patients to further restore the integrity of their body. The following research studies demonstrate that exercise, compared to non-invasive treatment options, is a safe and effective treatment method for individuals suffering with neck and lower extremity injury from a car crash.
Results
Study Selection
We screened 9494 citations based on the title and abstract (Figure 1). Of these, 60 full-text publications were screened, and 9 articles were critically appraised. The primary reasons for ineligibility during full text screening were (1) ineligible study design, (2) small sample size (n b 30 per treatment arm), (3) multimodal interventions not allowing isolation of the effectiveness of exercise, (4) ineligible study population, and (5) interventions not meeting our definition of exercise (Figure 1). Of those critically appraised, 3 studies (reported in 4 articles) had low risk of bias and were included in our synthesis. The interrater agreement for the screening of the articles was ? = 0.82 (95% CI, 0.69-0.95). The percentage agreement for the critical appraisal of studies was 75% (6/8 studies). Disagreement was resolved through discussion for 2 studies. We contacted authors from 5 studies during critical appraisal to request additional information and 3 responded.
Study Characteristics
The studies with low risk of bias were RCTs. One study, conducted in the Netherlands, examined the effectiveness of a standardized exercise program compared to a �wait and see� approach in participants with patellofemoral pain syndrome of variable duration. A second study, with outcomes reported in 2 articles, compared the benefit of closed vs open kinetic chain exercises in individuals with�variable duration patellofemoral pain syndrome in Belgium. The final study, conducted in Denmark, investigated active training compared to a multimodal physiotherapy intervention for the management of persistent adductor-related groin pain.
Two RCTs used exercise programs that combined strengthening exercises with balance or agility training for the lower extremity. Specifically, the strengthening exercises consisted of both isometric and concentric contractions of the quadriceps, hip adductor, and gluteal muscles for the management of patellofemoral pain46 and hip adductors and muscles of the trunk and pelvis for adductor-related groin pain. The exercise programs ranged from 646 to 1243 weeks in duration and were supervised and clinic based with additional daily home exercises. The exercise programs were compared to a �wait and see� approach or to multimodal physiotherapy. The third RCT compared 2 different 5-week protocols which combined either closed or open kinetic chain strengthening and stretching exercises for the lower extremity musculature.
Meta-analysis was not performed due to heterogeneity of accepted studies with respect to patient populations, interventions, comparators, and outcomes. Principles of best evidence synthesis were used to develop evidence statements and perform a qualitative synthesis of findings from studies with low risk of bias.
Risk of Bias Within Studies
The studies with low risk of bias had a clearly defined research question, used appropriate blinding methods where possible, reported adequate similarity of baseline characteristics between treatment arms, and performed an intention-to-treat analyses where applicable (Table 3). The RCTs had follow-up rates greater than 85%. However, these studies also had methodological limitations: insufficient detail describing methods for allocation concealment (1/3), insufficient detail describing methods of randomization (1/3), the use of outcome measures that have not been demonstrated to be valid or reliable (ie, muscle length and successful treatment) (2/3), and clinically important differences in baseline characteristics (1/3).
Of 9 relevant articles, 5 were deemed to have high risk of bias. These studies had the following limitations: (1) poor or unknown randomization methods (3/5); (2) poor or unknown allocation concealment methods (5/ 5); (3) outcome assessor not blinded (4/ 5); (4) clinically important differences in baseline characteristics (3/5); (5) dropouts not reported, insufficient information regarding dropouts per group or large differences in dropout rates between treatment arms (N15%) (3/5); and (6) a lack of information about or no intention-to-treat analysis (5/5).
Summary of Evidence
Patellofemoral Pain Syndrome of Variable Duration. Evidence from 1 RCT suggests that a clinic-based progressive exercise program may provide short- and long-term benefit over usual care for the management of patellofemoral pain syndrome of variable duration. van Linschoten et al randomized participants with a clinical diagnosis of patellofemoral pain syndrome of 2 months to 2 years duration to (1) a clinic-based exercise program (9 visits over 6 weeks) consisting of progressive, static, and dynamic strengthening exercises for the quadriceps, adductor, and gluteal muscles and balance and flexibility exercises, or (2) a usual care �wait and see� approach. Both groups received standardized information, advice, and home-based isometric exercises for the quadriceps based on recommendations from Dutch General Practitioner guidelines (Table 4). There�were statistically significant differences favoring the exercise group for (1) pain (NRS) at rest at 3 months (mean change difference 1.1/10 [95% CI, 0.2-1.9]) and 6 months (mean change difference 1.3/10 [95% CI, 0.4-2.2]); (2) pain (NRS) with activity at 3 months (mean change difference 1.0/10 [95% CI, 0.1-1.9]) and 6 months (mean change difference 1.2/10 [95% CI, 0.2-2.2]); and (3) function (Kujala Patellofemoral Scale [KPS]) at 3 months (mean change difference 4.9/100 [95% CI, 0.1-9.7]). However, none of these differences were clinically important. Furthermore, there were no significant differences in the proportion of participants reporting recovery (fully recovered, strongly recovered), but the exercise group was more likely to report improvement at 3-month follow-up (odds ratio [OR], 4.1 [95% CI, 1.9-8.9]).
Evidence from a second RCT suggests that physiotherapist- supervised closed kinetic chain leg exercises (where the foot remains in constant contact with a surface) may provide short-term benefit compared to supervised open kinetic chain exercises (where the limb moves freely) for some patellofemoral pain syndrome symptoms (Table 4). All participants trained for 30 to 45 minutes, 3 times per week for 5 weeks. Both groups were instructed to perform static lower limb stretching after each training session. Those randomized to closed chain exercises performed supervised (1) leg presses, (2) knee bends, (3) stationary biking, (4) rowing, (5) step-up and step-down exercises, and (6) progressive jumping exercises. Open chain exercise participants performed (1) maximal quad muscle contraction, (2) straight-leg raises, (3) short arc movements from 10� to full knee extension, and (4) leg adduction. Effect sizes were not reported, but the authors reported statistically significant differences favoring closed kinetic chain exercise at 3 months for (1) frequency of locking (P = .03), (2) clicking sensation (P = .04), (3) pain with isokinetic testing (P = .03), and (4) pain during night (P = .02). The clinical significance of these results is unknown. There were no statistically significant differences between groups for any other pain or functional measures at any follow-up period.
Persistent Adductor-Related Groin Pain
Evidence from 1 RCT suggests that a clinic-based group exercise program is more effective than a multimodal program of care for persistent adductor-related groin pain. H�lmich et al studied a group of male athletes with a clinical diagnosis of adductor-related groin pain of greater than 2 months duration (median duration, 38-41 weeks; range, 14-572 weeks) with or without osteitis pubis. Participants were randomized to (1) a clinic-based group exercise program (3 sessions per week for 8-12 weeks) consisting of isometric and concentric resistance strengthening exercises for the adductors, trunk, and pelvis; balance and agility exercises for the lower extremity; and stretching for the abdominals, back, and lower extremity (with the exception of the adductor muscles) or (2) a multimodal physiotherapy program (2 visits per week for 8-12 weeks) consisting of laser; transverse friction massage; transcutaneous electrical nerve stimulation (TENS); and stretching for the adductors, hamstrings, and hip flexors (Table 4). Four months after the intervention, the exercise group was more likely to report that their condition was �much better� (RR, 1.7 [95% CI, 1.0-2.8]).
Adverse Events
None of the included studies commented on the frequency or nature of adverse events.
Discussion
Summary of Evidence
Our systematic review examined the effectiveness of exercise for the management of soft tissue injuries of the hip, thigh, or knee. Evidence from 1 RCT suggests that a clinic-based progressive combined exercise program may offer additional short- or long-term benefit compared to providing information and advice for the management of patellofemoral pain syndrome of variable duration. There is also evidence that supervised closed kinetic chain exercises may be beneficial for some patellofemoral pain syndrome symptoms compared to open kinetic chain exercises. For persistent adductor-related groin pain, evidence from 1 RCT suggests that a clinic-based group exercise program is more effective than a multimodal program of care. Despite the common and frequent use of exercise prescription, there is limited high-quality evidence to inform the use of exercise for the management of soft tissue injuries of the lower extremity. Specifically, we did not find high-quality studies on exercise for the management of some of the more commonly diagnosed conditions including patellar tendinopathy, hamstring sprain and strain injuries, hamstring tendinopathy, trochanteric bursitis, or capsular injuries of the hip.
Previous Systematic Reviews
Our results are consistent with findings from previous systematic reviews, concluding that exercise is effective for the management of patellofemoral pain syndrome and groin pain. However, the results from previous systematic reviews examining the use of exercise for the management of patellar tendinopathy and acute hamstring injuries are inconclusive. One review noted strong evidence for use of eccentric training, whereas others reported uncertainty of whether isolated eccentric exercises were beneficial for tendinopathy compared to other forms of exercise. Furthermore, there is limited evidence of a positive effect from stretching, agility and trunk stability exercises, or slump stretching for the management of acute�hamstring injuries. Differing conclusions between systematic reviews and the limited number of studies deemed admissible in our work may be attributed to differences in methodology. We screened reference lists of previous systematic reviews, and most studies included in the reviews did not meet our inclusion criteria. Many studies accepted in other reviews had small sample sizes (b30 per treatment arm). This increases the risk of residual confounding while also reducing the effect size precision. Furthermore, a number of systematic reviews included case series and case studies. These types of studies are not designed to assess the effectiveness of interventions. Finally, previous reviews included studies where exercise was part of a multimodal intervention, and as a consequence, the isolated effect of exercise could not be ascertained. Of the studies that satisfied our selection criteria, all were critically appraised in our review, and only 3 had low risk of bias and were included in our synthesis.
Strengths
Our review has many strengths. First, we developed a rigorous search strategy that was independently reviewed by a second librarian. Second, we defined clear inclusion and exclusion criteria for the selection of possibly relevant studies and only considered studies with adequate sample sizes. Third, pairs of trained reviewers screened and critically appraised eligible studies. Fourth, we used a valid set of criteria (SIGN) to critically appraise studies. Finally, we restricted our synthesis to studies with low risk of bias.
Limitations and Recommendations for Future Research
Our review also has limitations. First, our search was limited to studies published in the English language. However, previous reviews have found that the restriction of systematic reviews to English language studies has not led to a bias in reported results. Second, despite our broad definition of soft tissue injuries of the hip, thigh, or knee, our search strategy may not have captured all potentially relevant studies. Third, our review may have missed potentially relevant studies published before 1990. We aimed to minimize this by hand searching the reference lists of previous systematic reviews. Finally, critical appraisal requires scientific judgment that may differ between reviewers. We minimized this potential bias by training reviewers in the use of the SIGN tool and using a consensus process to determine study admissibility. Overall, our systematic review highlights a deficit of strong research in this area.
High-quality studies on the effectiveness of exercise for the management of soft tissue injuries of the lower extremity are needed. Most studies included in our review (63%) had a high risk of bias and could not be included in our synthesis. Our review identified important gaps in the literature. Specifically, studies are needed to inform the specific effects of exercises, their long-term effects, and the optimal doses of intervention. Furthermore, studies are needed to determine the relative effectiveness of different types of exercise programs and if the effectiveness varies for soft tissue injuries of the hip, thigh, and knee.
Conclusion
There is limited high-quality evidence to inform the use of exercise for the management of soft tissue injuries of the hip, thigh, and knee. The current evidence suggests that a clinic-based progressive combined exercise program may lead to improved recovery when added to information and advice on resting and avoiding pain provoking activities for the management of patellofemoral pain syndrome. For persistent adductor-related groin pain, a supervised clinic- based group exercise program is more effective than multimodal care in promoting recovery.
Funding Sources and Potential Conflicts of Interest
This study was funded by the Ontario Ministry of Finance and the Financial Services Commission of Ontario (RFP no. OSS_00267175). The funding agency was not involved in the collection of data, data analysis, interpretation of data, or drafting of the manuscript. The research was undertaken, in part, thanks to funding from the Canada Research Chairs program. Pierre C�t� has previously received funding from a Grant from the Ontario Ministry of Finance; consulting for the Canadian Chiropractic Protective Association; speaking and/or teaching arrangements for the National Judicial Institute and Soci�t� des M�decins Experts du Quebec; trips/travel, European Spine Society; board of directors, European Spine Society; grants: Aviva Canada; fellowship support, Canada Research Chair Program�Canadian Institutes of Health Research. No other conflicts of interest were reported for this study.
Contributorship Information
Concept development (provided idea for the research): D.S., C.B., P.C., J.W., H.Y., S.V.
Design (planned the methods to generate the results): D.S., C.B., P.C., H.S., J.W., H.Y., S.V.
Supervision (provided oversight, responsible for organization and implementation, writing of the manuscript): D.S., P.C.
Data collection/processing (responsible for experiments, patient management, organization, or reporting data): D.S., C.B., H.S., J.W., D.e.S., R.G., H.Y., K.R., J.C., K.D., P.C., P.S., R.M., S.D., S.V.
Analysis/interpretation (responsible for statistical analysis, evaluation, and presentation of the results): D.S., C.B., P.C., H.S., M.S., K.R., L.C.
Literature search (performed the literature search): A.T.V.
Writing (responsible for writing a substantive part of the manuscript): D.S., C.B., P.C., H.S.
Critical review (revised manuscript for intellectual content, this does not relate to spelling and grammar checking): D.S., P.C., H.S., J.W., D.e.S., R.G., M.S., A.T.V., H.Y., K.R., J.C., K.D., L.C., P.S., S.D., R.M., S.V.
Practical Applications
There is evidence to suggest that clinic-based exercises may benefit patients with patellofemoral pain syndrome or adductor-related groin pain.
Supervised progressive exercises may be beneficial for patellofemoral pain syndrome of variable duration compared to information/advice.
Supervised closed kinetic chain exercises may provide more benefit compared to open kinetic chain exercises for some patellofemoral pain syndrome symptoms.
Self-rated improvement in persistent groin pain is higher after a clinic-based group exercise program compared to multimodal physiotherapy.
Are Non-Invasive Interventions Effective for the Management of Headaches Associated with Neck Pain?
Furthermore,�other non-invasive interventions, as well as non-pharmacological interventions, are also commonly utilized to help treat symptoms of neck pain and headaches associated with neck injuries, such as whiplash, caused by automobile accidents. As mentioned before, whiplash is one of the most common types of neck injuries resulting from auto accidents. Chiropractic care, physical therapy and exercise, can be used to improve the symptoms of neck pain, according to the following research studies.
Abstract
Purpose
To update findings of the 2000�2010 Bone and Joint Decade Task Force on Neck Pain and its Associated Disorders and evaluate the effectiveness of non-invasive and non-pharmacological interventions for the management of patients with headaches associated with neck pain (i.e., tension-type, cervicogenic, or whiplash-related headaches).
Methods
We searched five databases from 1990 to 2015 for randomized controlled trials (RCTs), cohort studies, and case�control studies comparing non-invasive interventions with other interventions, placebo/sham, or no interventions. Random pairs of independent reviewers critically appraised eligible studies using the Scottish Intercollegiate Guidelines Network criteria to determine scientific admissibility. Studies with a low risk of bias were synthesized following best evidence synthesis principles.
Results
We screened 17,236 citations, 15 studies were relevant, and 10 had a low risk of bias. The evidence suggests that episodic tension-type headaches should be managed with low load endurance craniocervical and cervicoscapular exercises. Patients with chronic tension-type headaches may also benefit from low load endurance craniocervical and cervicoscapular exercises; relaxation training with stress coping therapy; or multimodal care that includes spinal mobilization, craniocervical exercises, and postural correction. For cervicogenic headaches, low load endurance craniocervical and cervicoscapular exercises; or manual therapy (manipulation with or without mobilization) to the cervical and thoracic spine may also be helpful.
Conclusions
The management of headaches associated with neck pain should include exercise. Patients who suffer from chronic tension-type headaches may also benefit from relaxation training with stress coping therapy or multimodal care. Patients with cervicogenic headache may also benefit from a course of manual therapy.
We would like to acknowledge and thank all of the individuals who have made important contributions to this review: Robert Brison, Poonam Cardoso, J. David Cassidy, Laura Chang, Douglas Gross, Murray Krahn, Michel Lacerte, Gail Lindsay, Patrick Loisel, Mike Paulden, Roger Salhany, John Stapleton, Angela Verven, and Leslie Verville. We would also like to thank Trish Johns-Wilson at the University of Ontario Institute of Technology for her review of the search strategy.
Compliance with Ethical Standards
Conflict of Interest
Dr. Pierre C�t� has received a grant from the Ontario government, Ministry of Finance, funding from the Canada Research Chairs program, personal fees from National Judicial Institute for lecturing, and personal fees from European Spine Society for teaching. Drs. Silvano Mior and Margareta Nordin have received reimbursement for travel expenses to attend meetings for the study. The remaining authors report no declarations of interest.
Funding
This work was supported by the Ontario Ministry of Finance and the Financial Services Commission of Ontario [RFP# OSS_00267175]. The funding agency had no involvement in the study design, collection, analysis, interpretation of data, writing of the manuscript or decision to submit the manuscript for publication. The research was undertaken, in part, thanks to funding from the Canada Research Chairs program to Dr. Pierre C�t�, Canada Research Chair in Disability Prevention and Rehabilitation at the University of Ontario Institute of Technology.
In conclusion,�exercise included in chiropractic care and other non-invasive interventions should be utilized as an essential part of treatment to further help improve the symptoms of neck injury as well as that of hip, thigh and knee injury. According to the above research studies, exercise, or physical activity, is beneficial towards speeding up recovery time for patients with automobile accident injuries and for restoring strength, flexibility and mobility to the affected structures of the spine. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is referred to as a collection of symptoms rather than a single type of injury or condition. The symptoms are characterized as radiating pain, numbness and tingling sensations from the sciatic nerve in the lower back, down the buttocks and thighs and through one or both legs and into the feet. Sciatica is commonly the result of irritation, inflammation or compression of the largest nerve in the human body, generally due to a herniated disc or bone spur.
1. Lambers K, Ootes D, Ring D. Incidence of patients with lower
extremity injuries presenting to US emergency departments by
anatomic region, disease category, and age. Clin Orthop Relat
Res 2012;470(1):284-90.
2. Workplace Safety and Insurance Board. By the numbers: 2014
WSIB statistical report. Injury profile�schedule 1; historical
and supplementary data on leading part of body injuries.
[cited June 22, 2015]; Available from: http://www.
wsibstatistics.ca/en/s1injury/s1part-of-body/ 2014.
3. Hincapie CA, Cassidy JD, C�t� P, Carroll LJ, Guzman J.
Whiplash injury is more than neck pain: a population-based
study of pain localization after traffic injury. J Occup Environ
Med 2010;52(4):434-40.
4. Bureau of Labor Statistics US Department of Labor. Nonfatal
occupational injuries and illnesses requiring days away from
work. Table 5. Washington, DC 2014 [June 22, 2015];
Available from: http://www.bls.gov/news.release/archives/
osh2_12162014.pdf 2013.
5. New ZealandGuidelinesDevelopmentGroup. The diagnosis and
management of soft tissue knee injuries: internal derangements.
Best practice evidence-based guideline. Wellington: Accident
Compensation Corporation; 2003 [[June 22, 2015]; Available
from: http://www.acc.co.nz/PRD_EXT_CSMP/groups/
external_communications/documents/guide/wcmz002488.pdf].
6. Bizzini M, Childs JD, Piva SR, Delitto A. Systematic review of
the quality of randomized controlled trials for patellofemoral pain
syndrome. J Orthop Sports Phys Ther 2003;33(1):4-20.
7. Crossley K, Bennell K, Green S, McConnell J. A systematic
review of physical interventions for patellofemoral pain
syndrome. Clin J Sport Med 2001;11(2):103-10.
8. Harvie D, O�Leary T, Kumar S. A systematic review of
randomized controlled trials on exercise parameters in the
treatment of patellofemoral pain: what works? J Multidiscip
Healthc 2011;4:383-92.
9. Lepley AS, Gribble PA, Pietrosimone BG. Effects of electromyographic
biofeedback on quadriceps strength: a systematic
review. J Strength Cond Res 2012;26(3):873-82.
10. Peters JS, Tyson NL. Proximal exercises are effective in treating
patellofemoral pain syndrome: a systematic review. Int J Sports
Phys Ther 2013;8(5):689-700.
11. Wasielewski NJ, Parker TM, Kotsko KM. Evaluation of
electromyographic biofeedback for the quadriceps femoris: a
systematic review. J Athl Train 2011;46(5):543-54.
12. Kristensen J, Franklyn-Miller A. Resistance training in musculoskeletal
rehabilitation: a systematic review. Br J Sports Med
2012;46(10):719-26.
13. Larsson ME, Kall I, Nilsson-Helander K. Treatment of patellar
tendinopathy�a systematic review of randomized controlled
trials. Knee Surg Sports Traumatol Arthrosc 2012;20(8):1632-46.
14. Malliaras P, Barton CJ, Reeves ND, Langberg H. Achilles and
patellar tendinopathy loading programmes: a systematic review
comparing clinical outcomes and identifying potential mechanisms
for effectiveness. Sports Med 2013;43(4):267-86.
15. Wasielewski NJ, KotskoKM. Does eccentric exercise reduce pain
and improve strength in physically active adults with symptomatic
lower extremity tendinosis? A systematic review. J Athl Train
2007;42(3):409-21.
16. Reurink G, Goudswaard GJ, Tol JL, Verhaar JA, Weir A, Moen
MH. Therapeutic interventions for acute hamstring injuries: a
systematic review. Br J Sports Med 2012;46(2):103-9.
17. American Academy of Orthopaedic Surgeons. Sprains, strains,
and other soft-tissue injuries. [updated July 2007 March 11,
2013]; Available from: http://orthoinfo.aaos.org/topic.cfm?topic=
A00304 2007.
18. Abenhaim L, Rossignol M, Valat JP, et al. The role of activity in
the therapeutic management of back pain. Report of
the International Paris Task Force on Back Pain. Spine 2000;
25(4 Suppl):1S-33S.
19. McGowan J, Sampson M, Lefebvre C. An evidence
based checklist for the Peer Review of Electronic Search Strategies
(PRESS EBC). Evid Based Library Inf Pract 2010;5(1):149-54.
20. Sampson M, McGowan J, Cogo E, Grimshaw J, Moher D,
Lefebvre C. An evidence-based practice guideline for the peer
review of electronic search strategies. J Clin Epidemiol 2009;
62(9):944-52.
21. Almeida MO, Silva BN, Andriolo RB, Atallah AN, Peccin MS.
Conservative interventions for treating exercise-related musculotendinous,
ligamentous and osseous groin pain. Cochrane
Database Syst Rev 2013;6:CD009565.
22. Ellis R, Hing W, Reid D. Iliotibial band friction syndrome�a
systematic review. Man Ther 2007;12(3):200-8.
23. Machotka Z, Kumar S, Perraton LG. A systematic review of the
literature on the effectiveness of exercise therapy for groin pain in
athletes. SportsMed Arthrosc Rehabil Ther Technol 2009;1(1):5.
24. Moksnes H, Engebretsen L, Risberg MA. The current evidence
for treatment of ACL injuries in children is low: a systematic
review. J Bone Joint Surg Am 2012;94(12):1112-9.
25. Harbour R, Miller J. A new system for grading recommendations
in evidence based guidelines. BMJ 2001;323(7308):
334-6.
26. Carroll LJ, Cassidy JD, Peloso PM, Garritty C, Giles-Smith L.
Systematic search and review procedures: results of the WHO
Collaborating Centre Task Force on Mild Traumatic Brain
Injury. J Rehabil Med 2004(43 Suppl):11-4.
27. Carroll LJ, Cassidy JD, Peloso PM, et al. Methods for the best
evidence synthesis on neck pain and its associated disorders: the
Bone and Joint Decade 2000-2010 Task Force on Neck Pain
and Its Associated Disorders. JManipulative Physiol Ther 2009;
32(2 Suppl):S39-45.
28. C�t� P, Cassidy JD, Carroll L, Frank JW, Bombardier C. A
systematic review of the prognosis of acute whiplash and a new
conceptual framework to synthesize the literature. Spine (Phila
Pa 1976) 2001;26(19):E445-58.
29. Hayden JA, Cote P, Bombardier C. Evaluation of the quality of
prognosis studies in systematic reviews. Ann Intern Med 2006;
144(6):427-37.
30. Hayden JA, van der Windt DA, Cartwright JL, Cote P,
Bombardier C. Assessing bias in studies of prognostic factors.
Ann Intern Med 2013;158(4):280-6.
31. Spitzer WO, Skovron ML, Salmi LR, et al. Scientific
monograph of the Quebec Task Force on Whiplash-Associated
Disorders: redefining �whiplash� and its management. Spine
1995;20(8 Suppl):1S-73S.
32. van der Velde G, van Tulder M, Cote P, et al. The sensitivity of
review results to methods used to appraise and incorporate trial
quality into data synthesis. Spine (Phila Pa 1976) 2007;32(7):
796-806.
33. Slavin RE. Best evidence synthesis: an intelligent alternative to
meta-analysis. J Clin Epidemiol 1995;48(1):9-18.
34. Hinman RS, McCrory P, Pirotta M, et al. Efficacy of
acupuncture for chronic knee pain: protocol for a randomised
controlled trial using a Zelen design. BMCComplement Altern
Med 2012;12:161.
35. Crossley KM, Bennell KL, Cowan SM, Green S. Analysis of
outcome measures for persons with patellofemoral pain: which
are reliable and valid? Arch Phys Med Rehabil 2004;85(5):
815-22.
36. Cohen J. A coefficient of agreement for nominal scales. Educ
Psychol Meas 1960;20(1):37-46.
37. Abrams KR, Gillies CL, Lambert PC. Meta-analysis of
heterogeneously reported trials assessing change from baseline.
Stat Med 2005;24(24):3823-44.
38. Follmann D, Elliott P, Suh I, Cutler J. Variance imputation for
overviews of clinical trials with continuous response. J Clin
Epidemiol 1992;45(7):769-73.
39. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred
reporting items for systematic reviews and meta-analyses: the
PRISMA statement. BMJ 2009;339:b2535.
40. Askling CM, Tengvar M, Thorstensson A. Acute hamstring
injuries in Swedish elite football: a prospective randomised
controlled clinical trial comparing two rehabilitation protocols.
Br J Sports Med 2013;47(15):953-9.
41. Dursun N, Dursun E, Kilic Z. Electromyographic biofeedbackcontrolled
exercise versus conservative care for patellofemoral
pain syndrome. Arch Phys Med Rehabil 2001;82(12):1692-5.
42. Harrison EL, Sheppard MS, McQuarry AM. A randomized
controlled trial of physical therapy treatment programs in
patellofemoral pain syndrome. Physiother Can 1999;1999:93-100.
43. Holmich P, Uhrskou P, Ulnits L, et al. Effectiveness of active
physical training as treatment for long-standing adductor-related
groin pain in athletes: randomised trial. Lancet 1999;353(9151):
439-43.
44. Lun VM, Wiley JP, Meeuwisse WH, Yanagawa TL. Effectiveness
of patellar bracing for treatment of patellofemoral pain
syndrome. Clin J Sport Med 2005;15(4):235-40.
45. Malliaropoulos N, Papalexandris S, Papalada A, Papacostas E.
The role of stretching in rehabilitation of hamstring injuries: 80
athletes follow-up. Med Sci Sports Exerc 2004;36(5):756-9.
46. van Linschoten R, van Middelkoop M, Berger MY, et al.
Supervised exercise therapy versus usual care for patellofemoral
pain syndrome: an open label randomised controlled trial. BMJ
2009;339:b4074.
47. Witvrouw E, Cambier D, Danneels L, et al. The effect of exercise
regimens on reflex response time of the vasti muscles in patients
with anterior knee pain: a prospective randomized intervention
study. Scand J Med Sci Sports 2003;13(4):251-8.
48. Witvrouw E, Lysens R, Bellemans J, Peers K, Vanderstraeten G.
Open versus closed kinetic chain exercises for patellofemoral
pain. A prospective, randomized study. Am J Sports Med 2000;
28(5):687-94.
49. Johnson AP, Sikich NJ, Evans G, et al. Health technology
assessment: a comprehensive framework for evidence-based
recommendations in Ontario. Int J Technol Assess Health Care
2009;25(2):141-50.
Chiropractic Care: Our neck is a busy body part. It holds up and turns our head, allowing us to see, hear, and speak in the direction we choose.
Although the neck is a real “team player” it’s a bit of a diva, meaning it’s fairly delicate. There are many ways everyday motion injures the neck, ending up causing pain, decreased mobility, and varying degrees of short and long-term misery.
Whiplash is a common neck injury caused by a sudden movement that jerks the neck forth and then back in a whipping motion. Automobile accidents frequently result in whiplash, as the vehicle is moving and then stopping rapidly.
This affects the neck’s ligaments and joints in various degrees, depending on the speed of the vehicle and the site of the impact. In severe cases, the discs and the nerves may also be damaged.
Symptoms of whiplash include varying degrees of pain, stiffness in the neck, headaches, and sometimes dizziness, blurred vision, and nausea. Some people only suffer with whiplash a few days, while others experience ongoing issues.
If you have been injured in an automobile crash, it’s in your best interest to immediately schedule an appointment with a chiropractor. There are a myriad of ways chiropractic care assists in managing the pain and minimizing the symptoms of whiplash.
Here Are The 5 Best Reasons For Chiropractic Care:
#1: Reduces Inflammation To Promote Healing
The first order of business for whiplash sufferers is to get the neck’s inflammation reduced, as this hinders proper healing. Your chiropractor will utilize chiropractic adjustments, along with other forms of treatment based on your specific injury. It�s essential to undergo this type of treatment as soon after the injury occurs as possible in order to reach optimum results.
#2: Minimizes Pain For Greater Comfort
Whiplash can be extremely painful, as so many of the neck’s components may be involved, and the neck is such a mobile body part. Every neck movement hurting is no way to live! Chiropractic care soothes the pain of whiplash through therapeutic techniques that promote healing of the damaged area.
#3: Returns Proper Body Alignment
When the inflammation and the pain of whiplash are reduced, the next step is to promote healing and alignment within the body. A chiropractor will perform a series of chiropractic adjustments that includes the neck and spine, but may also incorporate other parts of the body. Whiplash does a number on the body’s natural alignment, and it’s the chiropractor’s job to put it all back together in workable order.
#4: Offers Exercises To Increase Mobility
Contrary to old movies where the whiplash sufferer wears a cumbersome neck brace, it’s vital to the rehabilitation process to keep moving. During chiropractic visits, patients receive a regimen of exercises to perform regularly at home. These, combined with chiropractic care, lessen the time it takes to recover.
#5: Provides An Alternative To Surgery
The good news is that a whiplash injury rarely requires surgery. However, it’s best to not tempt fate and visit a chiropractor to make certain your injuries are treated and begin healing. A chiropractor monitors improvements and keeps you apprised of your progress, empowering you to get better and back to normal activity faster than simply suffering through the symptoms, hoping they go away.
If you are involved in a motor vehicle crash and end up with whiplash, don’t despair. A chiropractor will map out a treatment regimen that will decrease inflammation and pain, increase mobility, and promote healing. Remember, the sooner you see your chiropractor, the faster the treatment begins, and the sooner you see results. Don’t suffer needlessly!
Chiropractic Care & Headaches
This article is copyrighted by Blogging Chiros LLC for its Doctor of Chiropractic members and may not be copied or duplicated in any manner including printed or electronic media, regardless of whether for a fee or gratis without the prior written permission of Blogging Chiros, LLC.
Back pain is one of the most common causes people visit their healthcare professional every year. A primary care physician is often the first doctor who can provide treatment for a variety of injuries and/or conditions, however, among those individuals seeking complementary and alternative treatment options for back pain, most people choose chiropractic care. Chiropractic care focuses on the diagnosis, treatment and prevention of trauma and disease of the musculoskeletal and nervous systems, by correcting misalignments of the spine through the use of spinal adjustments and manual manipulations.
Approximately 35% of individuals seek chiropractic treatment for back pain caused by automobile accidents, sports injuries, and a variety of muscle strains. When people suffer an trauma or injury as a result of an accident, however, they may first receive treatment for their symptoms of back pain in a hospital. Hospital outpatient care describes treatment which does not require an overnight stay at a medical facility. A research study conducted an analysis comparing the effects of chiropractic care and hospital outpatient management for back pain. The results are described in detail below.
Abstract
Objective: To compare the effectiveness over three years of chiropractic and hospital outpatient management for low back pain.
Design: Randomised allocation of patients to chiropractic or hospital outpatient management.
Setting: Chiropractic clinics and hospital outpatient departments within reasonable travelling distance of each other in I I centres.
Subjects: 741 men and women aged 18-64 years with low back pain in whom manipulation was not contraindicated.
Outcome measures: Change in total 0swestry questionnaire score and in score for pain and patient satisfaction with allocated treatment.
Results: According to total 0swestry scores improvement in all patients at three years was about 291/6 more in those treated by chiropractors than in those treated by the hospitals. The beneficial effect of chiropractic on pain was particularly clear. Those treated by chiropractors had more further treatments for back pain after the completion of trial treatment. Among both those initially referred from chiropractors and from hospitals more rated chiropractic helpful at three years than hospital management.
Conclusions: At three years the results confirm the findings of an earlier report that when chiropractic or hospital therapists treat patients with low back pain as they would in day to day practice those treated by chiropractic derive more benefit and long term satisfaction than those treated by hospitals.
Introduction
In 1990 we reported greater improvement in patients with low back pain treated by chiropractic compared with those receiving hospital outpatient management. The trial was “pragmatic” in allowing the therapists to treat patients as they would in day to day practice. At the time of our first report not all patients had been in the trial for more than six months. This paper presents the full results up to three years for all patients for whom follow up information from Oswestry questionnaires and for other outcomes was available for analysis. We also present data on pain from the questionnaire, which is by definition the main complaint prompting referral or self referral.
Methods
Methods were fully described in our first report. Patients initially referred or presenting either to a chiropractic clinic or in hospital were randomly allocated to be treated either by chiropractic or in hospital. A total of 741 patients started treatment. Progress was measured with the Oswestry questionnaire on back pain, which gives scores for I 0 sections for example, intensity of pain and difficulty with lifting, walking, and travelling. The result is expressed on a scale ranging from 0 (no pain or difficulties) to 100 (highest score for pain and greatest difficulty on all items). For an individual item, such as pain, scores range from 0 to 10. The main outcome measures are the changes in Oswestry score from before treatment to each follow up. At one, two, and three years patients were also asked about further treatment since the completion of their trial treatment or since the previous annual questionnaire. At the three year follow up patients were asked whether they thought their allocated trial treatment had helped their back pain.
In the random allocation of treatment minimisation was used within each centre to establish groups for the analysis of results according to initial referral clinic, length of current episode (more or less than ‘a month), presence or absence of a history of back pain, and an Oswestry score at entry of > 40 or <=40%.
Results were analysed on an intention to treat basis (subject to the availability of data at follow up as well as at entry for individual patients). Differences between mean changes were tested by unpaired t tests, and X2 tests were used to test for differences in proportions between the two treatment groups.
Dr. Alex Jimenez’s Insight
Chiropractic is a natural form of health care which purpose is to restore and maintain the function of the musculoskeletal and nervous systems, promoting spinal health and allowing the body to heal itself naturally. Our philosophy emphasizes on the treatment of the human body as a whole, rather than on the treatment of a single injury and/or condition. As an experienced chiropractor, my goal is to properly assess patients in order to determine which type of treatment will most effectively heal their individual type of health issue. From spinal adjustments and manual manipulations to physical activity, chiropractic care can help correct spinal misalignments that cause back pain.
Results
Follow up Oswestry questionnaires were returned by a consistently higher proportion of patients allocated to chiropractic than to hospital treatment. At six weeks, for example, they were returned by 95% and 89% of chiropractic and hospital patients, respectively and at three years by 77% and 70%.
Mean (SD) scores before treatment were 29-8 (14-2) and 28-5 (14-1) in the chiropractic and hospital treatment groups, respectively. Table I shows the differences between the mean changes in total Oswestry scores according to randomly allocated treatment group. The difference at each follow up is the mean change for the chiropractic group minus the mean change for the hospital group.
Positive differences therefore reflect more improvement (due to a greater change in score) in those treated by chiropractic than in hospital (negative differences the reverse). The 3-18 percentage point difference at three years in table I represents a 29% greater improvement in patients treated with chiropractic compared with hospital treatment, the absolute improvement in the two groups at this time being 14-1 and 10-9 percentage points, respectively. As in the first report those with short current episodes, a history of back pain, and initially high Oswestry scores tended to derive most benefit from chiropractic. Those referred by chiropractors consistently derived more benefit from chiropractic than those referred by hospitals.
Table II shows changes between the scores on pain intensity before treatment and the corresponding scores at the various follow up intervals. All these changes were positive that is, indicated improvement but were all significantly greater in those treated by chiropractic, including the changes early on that is, at six weeks and six months, when the proportions returning questionnaires were high. As with the results based on the full Oswestry score the improvement due to chiropractic was greatest in those initially referred by chiropractors, although there was also a non-significant improvement (ranging from 9% at six months to 34% at three years) due to chiropractic at each follow up interval in those referred by hospitals.
Other scores for individual items on the Oswestry index to show significant improvement attributable to chiropractic were ability to sit for more than a short time and sleeping (P=0’004 and 0 03, respectively, at three years), though the differences were not as consistent as for pain. Other scores (personal care, lifting, walking, standing, sex life, social life, and travelling) also nearly all improved more in the patients treated with chiropractic, though most of the differences were small compared with the differences for pain.
Higher proportions of patients allocated to chiropractic sought further treatment (of any kind) for back pain after completion of trial treatment than those managed in hospital. For example, between one and two years after trial entry 122/292 (42%) patients treated with chiropractic compared with 80/258 (3 1%) of hospital treated patients did so (Xl=6 8, P=0 0 1).
Table III shows the proportions of patients at three years who thought their allocated trial treatment had helped their back pain. Among those initially referred by hospitals as well as among those initially referred by chiropractors higher proportions treated by chiropractic considered that treatment had helped compared with those treated in hospital.
Key Messages
Back pain often remits spontaneously
Effective treatments for non-remitting episodes need to be more clearly identified
Chiropractic seems to be more effective than hospital management, possibly because more treatments are spread over longer time periods
A growing number of NHS purchasers are making complementary treatments, including chiropractic, available
Further trials to identify the effective components of chiropractic are needed
Discussion
The results at six weeks and six months shown in table I are identical with those in our first report, as all patients had then been followed up for six months. The findings at one year are similar as many patients had also been followed up then. The considerably larger numbers of patients with data now available at two and three years show smaller benefits at these intervals than previously, though these still significantly favour chiropractic. The substantial benefit of chiropractic on intensity of pain is evident early on and then persists. The consistently larger proportions lost to follow up throughout the trial in those treated in hospital than in those treated by chiropractic suggests greater satisfaction with chiropractic. This conclusion is supported (table III) by the higher proportions in each referral group considering chiropractic helpful by comparison with hospital treatment.
The main criticism of the trial after our first report centred on its “pragmatic” nature, particularly the larger number of chiropractic than hospital treatments and the longer period over which the chiropractic treatments were spread and which were deliberately allowed. These considerations and any consequences of the higher proportions of patients allocated to chiropractic who received further treatment in the later stages of follow up, however, do not apply to the results at six weeks and only apply to a limited extent at six months, when the proportions followed up were high and extra treatment had either not occurred at all or was not yet extensive. Benefits atributable to chiropractic were already evident (especially on pain, table II) at these shorter intervals.
We believe there is now more support for the need for “fastidious” trials focusing on specific components of management and on their feasibility. Meanwhile, the results of our trial show that chiropractic has a valuable part to play in the management of low back pain.
We thank Dr Iain Chalmers for commenting on an earlier draft of the paper. We thank the nurse coordinators, medical staff, physiotherapists, and chiropractors in the 11 centres for their work, and Dr Alan Breen of the British Chiropractic Association for his help. The centres were in Harrow Taunton, Plymouth, Bournemouth and Poole, Oswestry, Chertsey, Liverpool, Chelmsford, Birmingham, Exeter, and Leeds. Without the assistance of many staff members in each the trial could not have been completed.
Funding: Medical Research Council, the National Back Pain Association, the European Chiropractors Union, and the King Edward’s Hospital Fund for London.
Conflict of interest: None.
In conclusion,�after three years, the results of the research study comparing chiropractic care and hospital outpatient management for low back pain determined that people treated by chiropractic experienced more benefits as well as long-term satisfaction than those treated by hospitals. Because back pain is one of the most common�causes people visit their healthcare professional every year, its essential to seek the most effective type of health care. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
References
Meade TW, Dyer S, Browne W, Townsend J, Frank AO. Low back pain of mechanical origin: randomised comparison of chiropractic and hospital outpatient treatment.�BMJ.�1990 Jun 2;300(6737):1431�1437.�[PMC free article]�[PubMed]
Fairbank JC, Couper J, Davies JB, O’Brien JP. The Oswestry low back pain disability questionnaire.�Physiotherapy.�1980 Aug;66(8):271�273.�[PubMed]
Pocock SJ, Simon R. Sequential treatment assignment with balancing for prognostic factors in the controlled clinical trial.�Biometrics.�1975 Mar;31(1):103�115.�[PubMed]
Additional Topics: Sciatica
Sciatica is referred to as a collection of symptoms rather than a single type of injury or condition. The symptoms are characterized as radiating pain, numbness and tingling sensations from the sciatic nerve in the lower back, down the buttocks and thighs and through one or both legs and into the feet. Sciatica is commonly the result of irritation, inflammation or compression of the largest nerve in the human body, generally due to a herniated disc or bone spur.
In association with professional experience in fitness and chiropractic care,�symptoms of back pain have been determined to improve in people who participate in physical activity and exercise, as directed by a physiotherapist, or physical therapist, or any other healthcare professional, such as a chiropractor. Various complementary and alternative treatment options for back pain also involve the use of functional fitness therapy, however, additional evidence-based research studies on the effectiveness of physical activity and exercise are still needed.
On a personal note, chiropractic care utilizes spinal adjustments and manual manipulations to carefully correct misalignments on the spine, or spinal subluxations. Along with chiropractic treatment, a doctor of chiropractor may also recommend a series of stretches and exercises to help increase flexibility, strength and mobility, improving the overall function of the spine. Physical activity for low back pain has been evaluated in the randomized controlled trial below.
Abstract
Objective
To evaluate effectiveness of an exercise programme in a community setting for patients with low back pain to encourage a return to normal activities.
Design
Randomised controlled trial of progressive exercise programme compared with usual primary care management. Patients� preferences for type of management were elicited independently of randomisation.
Participants
187 patients aged 18-60 years with mechanical low back pain of 4 weeks to 6 months� duration.
Interventions
Exercise classes led by a physiotherapist that included strengthening exercises for all main muscle groups, stretching exercises, relaxation session, and brief education on back care. A cognitive-behavioural approach was used.
Main Outcome Measures
Assessments of debilitating effects of back pain before and after intervention and at 6 months and 1 year later. Measures included Roland disability questionnaire, Aberdeen back pain scale, pain diaries, and use of healthcare services.
Results
At 6 weeks after randomisation, the intervention group improved marginally more than the control group on the disability questionnaire and reported less distressing pain. At 6 months and 1 year, the intervention group showed significantly greater improvement in the disability questionnaire score (mean difference in changes 1.35, 95% confidence interval 0.13 to 2.57). At 1 year, the intervention group also showed significantly greater improvement in the Aberdeen back pain scale (4.44, 1.01 to 7.87) and reported only 378 days off work compared with 607 in the control group. The intervention group used fewer healthcare resources. Outcome was not influenced by patients� preferences.
Conclusions
The exercise class was more clinically effective than traditional general practitioner management, regardless of patient preference, and was cost effective.
Key Messages
Patients with back pain need to return to normal activities as soon as possible but are often afraid that movement or activity may be harmful
An exercise programme led by a physiotherapist in the community and based on cognitive-behavioural principles helped patients to cope better with their pain and function better even one year later
Patients� preferences for type of management did not affect outcome
Patients in the intervention group tended to use fewer healthcare resources and took fewer days off work
This type of exercise programme should be more widely available
Introduction
Low back pain is common and, although it may settle quickly, recurrence rates are about 50% in the following 12 months. Recent management guidelines recommend that an early return to physical activities should be encouraged, but patients are often afraid of movement after an acute onset of back pain. Trials of specific exercise programmes for acute back pain have not shown them to be effective, but a specific exercise programme may have to be tailored to suit the individual patient and so is less likely to be effective for a heterogeneous group of patients.
However, there is some evidence that a general exercise programme, which aims to increase individuals� confidence in the use of their spine and overcome the fear of physical activity, can be effective for patients with chronic back pain (of more than six months� duration). A recent randomised trial of a supervised exercise programme in a hospital setting reported significantly better outcomes at six months and two years for the exercise group compared with the control group. Whether this approach would be effective and cost effective for patients with low back pain of less than six months� duration in a primary care setting is unknown.
An important methodological problem occurs when it is not possible to blind subjects to the treatment they receive, since outcome is probably directly influenced by their preconceived ideas regarding the effectiveness of intervention. Thus, in trials where a double blind procedure is not feasible, participants who are not randomised to their treatment of choice may be disappointed and suffer from resentful demoralisation, whereas those randomised to their preferred treatment may have a better outcome irrespective of the physiological efficacy of the intervention. However, this problem may be partly ameliorated if patients� treatment preferences are elicited before randomisation, so that they can be used to inform the analysis of costs and outcomes.
In this paper, we report a fully randomised trial for the treatment of subacute low back pain in which the analysis was informed by patient preference.
Subjects and Methods
Recruitment of Subjects
Eighty seven general practitioners agreed to participate in the study, and the principal investigator (JKM) visited each practice to discuss participation. Selection of general practitioners was based in the York area and restricted by the need to provide easy access for patients to the classes. Only one invited practice declined to participate. Single handed practices were not invited. The general practitioners referred patients directly to the research team or sent a monthly list of patients who had consulted with back pain. Inclusion criteria were patients with mechanical low back pain of at least four weeks� duration but less than six months, aged between 18 and 60, declared medically fit by their general practitioner to undertake the exercise, and who had consulted one of the general practitioners participating in the study. Patients with any potentially serious pathology were excluded, as were any who would have been unable to attend or participate in the classes. The exclusion criteria were the same as described by Frost et al except that concurrent physiotherapy rather than previous physiotherapy was an exclusion criterion in this trial.
Evaluation
Patients who seemed eligible were contacted by telephone and if they were interested in participating in the study were invited to an initial interview, at which the study and its implications for participants were explained. Patients who met all the eligibility criteria and consented to participate attended a first assessment a week later.
This included a physical examination (to exclude possible serious spinal pathology) and collection of baseline data by means of validated measures of health status. The main outcome measures were the Roland back pain disability questionnaire, which measures functional limitations due to back pain, and the Aberdeen back pain scale, which is more a measure of clinical status. The Roland disability questionnaire consists of a 24 point scale: a patient scoring three points on the scale means that he or she reports, for example, �Because of my back I am not doing any of the jobs that I usually do around the house, I use a handrail to get upstairs, and I lie down to rest more often.� We also administered the EuroQoL health index (EQ-5D) and the fear and avoidance beliefs questionnaire (FABQ).
The second assessment was carried out at the patients� general practice six weeks after randomisation to treatment. The brief physical examination was repeated, and the patients were asked to complete the same outcome questionnaires.
In addition, patients were asked to complete pain diaries in the week before their first assessment and in the week before their second assessment. The diaries were used to assess subjective pain reports and asked �How strong is the pain?� and �How distressing is the pain?�
We also evaluated patients at six and 12 months� follow up by sending them outcome questionnaires to complete and return.
Randomisation and Treatments
A pre-prepared randomisation list was generated from a random numbers table and participants were stratified by practice in blocks of six. The trial coordinator ensured concealment of allocation from the clinical researchers by providing the research physiotherapist with a sealed envelope for a named patient before baseline assessment. A note inside the envelope invited the participant either to attend exercise classes or to continue with the current advice or treatment offered by his or her general practitioner. (One of the referring general practitioners used manipulation as usual treatment on most of his patients so that up to 37 patients in each arm of the study could also have received manipulation.) Each patient had an equal chance of being allocated to the intervention or the control group. Before patients were given their envelope they were asked whether they had any preference for the treatment assignment. The participants opened the envelope after leaving the surgery.
Intervention group�The exercise programme consisted of eight sessions, each lasting an hour, spread out over four weeks, with up to 10 participants in each class. The programme was similar to the Oxford fitness programme and included stretching exercises, low impact aerobic exercises, and strengthening exercises aimed at all the main muscle groups. The overall aim was to encourage normal movement of the spine. No special equipment was needed. Participants were discouraged from viewing themselves as invalids and from following the precept of �Let pain be your guide.� They were encouraged to improve their individual record and were selectively rewarded with attention and praise. Although partly based on a traditional physiotherapy approach, the programme used cognitive-behavioural principles. One simple educational message encouraging self reliance was delivered at each class. Participants were told that they should regard the classes as a stepping stone to increasing their own levels of activity.
Controls�Patients allocated to the control group continued under the care of their doctor and in some cases were referred to physiotherapy as usual. No attempt was made to regulate the treatment they received, but it was recorded.
Economic Analysis
We recorded patients� use of healthcare services using a combination of retrospective questionnaires and prospective diary cards, which they returned at 6 and 12 months� follow up. From this information we estimated the cost of each patient�s treatment. We compared the mean costs of treatment for the two groups by using Student�s t tests and standard confidence intervals. However, as cost data were highly positively skewed, these results were checked with a non-parametric �bootstrap.� The economic evaluation addressed both costs to the NHS and the costs to society. Participants were not charged for the classes, in line with any treatment currently available on the NHS.
Statistical Analysis
Our original intention was to recruit 300 patients, which, given a standard deviation of 4, would have provided 90% power at the 5% significance level to detect a 1.5 point difference between the two groups in the mean change on the Roland disability questionnaire. However, recruitment of patients to the study proved much slower than expected, and, because of the limitations of study resources, recruiting was stopped after 187 patients had been included into the study. This smaller sample reduced the power to detect such a difference to 72%, but there was still 90% power to detect a 2 point difference in outcome.
Our analysis was based on intention to treat. We estimated the effects of treatment on the outcome measures by means of analysis of covariance, with the change in scores as the dependent variable and adjustment being made for baseline score and patient preference. We used Student�s t tests to analyse the data from the pain diaries as the baseline scores were quite similar.
Dr. Alex Jimenez’s Insight
In consideration with the research study regarding a randomized controlled trial coordinated to determine the effectiveness of functional fitness towards the improvement of low back pain, we supplement our philosophies of overall health and wellness to our patients and we make sure to take their recovery and rehabilitation to the next level. Our fitness and chiropractic care treatment goes beyond many other medically advanced methods. The proprietary treatment methods offered at our clinic promote true well-being and fitness practices with a primary goal on the calibration of the human body. The outcome measures of the randomized controlled trial on exercise for low back pain involved two groups of participants, an intervention group and a control group. The results are recorded below.
Results
Study Population
Of the 187 patients included in the trial, 89 were randomised to the intervention and 98 to the control group. The figure shows their progress through the trial. In both groups those with the most severe back pain at randomisation were less likely to return follow up questionnaires: the mean Roland disability questionnaire score for responders at one year follow up was 5.80 (SD 3.48) compared with a mean score of 9.06 (4.58) for non responders respectively (P=0.002).
Baseline Characteristics
The clinical and demographic characteristics of the patients in the two groups were fairly well balanced at randomisation (Table 1), although those allocated to the intervention group tended to report more disability on the Roland disability questionnaire than did the control group. Most patients (118, 63%), when asked, would have preferred to be allocated to the exercise programme. Attendance of the classes was considered quite good, with 73% of the intervention group attending between six and eight of the classes. Four people failed to attend any classes and were included in the intention to treat analysis. No patients allocated to the control group took part in the exercise programme.
Table 1: Baseline characteristics of patients with mechanical low back pain included in study. Values are means (standard deviations) unless stated otherwise.
Clinical Outcomes
Table ?2 shows the mean changes in outcome measures over time, from randomisation to final follow up at one year. After adjustment for baseline scores, the intervention group showed greater decreases in all measures of back pain and disability compared with the controls. At six weeks after randomisation, patients in the intervention group reported less distressing pain than the control group (P=0.03) and a marginally significant difference on the Roland disability questionnaire scores. Other variables were not significantly different, but the differences in change were all in favour of the intervention group. At six months the difference of the mean change scores of the Roland disability questionnaire was significant, and at one year the differences in changes of both the Roland disability questionnaire and the Aberdeen back pain scale were significant (Table ?2). Most of the intervention group improved by at least three points on the Roland disability questionnaire: 53% (95% confidence interval 42% to 64%) had done so at six weeks, 60% (49% to 71%) at six months, and 64% (54% to 74%) at one year. A smaller proportion of the control group achieved this clinically important improvement: 31% (22% to 40%) at six weeks, 40% (29% to 50%) at six months, and 35% (25% to 45%) at one year.
Table 2: Changes in back pain scores from baseline values in intervention and control groups at 6 weeks, 6 months, and 1 year follow up.
Patients� Preference
We examined the effect of patients� baseline preference for treatment on outcome after adjusting for baseline scores and main effects. Preference did not significantly affect response to treatment. The intervention had similar effects on both costs and outcomes regardless of baseline preference. For example, the change in the Roland disability questionnaire score at 12 months in the control group was ?1.93 for patients who preferred intervention and ?1.18 for those who were indifferent (95% confidence interval of difference ?1.05 to 2.55), and in the intervention group the change in score was ?3.10 for those who preferred intervention and ?3.15 for those who were indifferent ((95% confidence interval of difference ?1.47 to 3.08). As the interaction term (preference by random allocation) was non-significant, the results shown in Table ?2 exclude the preference term.
Economic Evaluation
Patients in the intervention group tended to use fewer healthcare and other resources compared with those in the control group (Table ?3). However, the mean difference, totalling �148 per patient, was not significant: the 95% confidence interval suggests there could have been a saving of as much as �442 per patient in the intervention group or an additional cost of up to �146. Patients in the control group took a total of 607 days off work during the 12 months after randomisation compared with 378 days taken off by the intervention group.
Table 3: Use of services and their costs associated with back pain in the two study groups at 12 months follow up.
Discussion
Our results support the hypothesis that a simple exercise class can lead to long term improvements for back pain sufferers. Studies have shown that a similar programme for patients with chronic back pain can be effective in the hospital setting. In this study we show the clinical effectiveness for patients with subacute or recurrent low back pain who were referred by their general practitioner to a community programme.
Current management guidelines for low back pain recommend a return to physical activity and taking exercise. In particular, they recommend that patients who are not improving at six weeks after onset of back pain, which may be a higher proportion than previously realised, should be referred to a reactivation programme. The programme we evaluated fits that requirement well. It shows participants how they can safely start moving again and increase their levels of physical activity. It is simple and less costly than individual treatment.
It seemed to have beneficial effects even one year later, as measured by functional disability (Roland disability questionnaire) and clinical status (Aberdeen back pain scale). The mean changes in scores on these instruments were small, with many patients reporting mild symptoms on the day of entry to the trial. However, a substantially larger proportion of participants in the exercise classes gained increases of over three points on the Roland disability questionnaire at six weeks, six months, and one year, which might be clinically important. At six weeks, participants in the exercise classes reported significantly less distressing pain compared with the control group, although the intensity of pain was not significantly different. This is consistent with findings from a study of chronic back pain patients in Oxford, in which changes in distressing pain were much greater than were the changes in intensity of pain.
People with back pain who use coping strategies that do not avoid movement and pain have less disability. In our study the participants in the exercise classes were able to function better according to Roland disability questionnaire scores than the control group at six months and one year after randomisation to treatment, and at one year they also showed a significantly greater improvement in clinical status as measured by the Aberdeen back pain scale. This increase in differences in effect between the intervention and control groups over time is consistent with the results from long term follow up in comparable back pain trials.
Study Design
The design of this study was a conventional randomised controlled trial in that all eligible patients were randomised. However, the participants were asked to state their preferred treatment before they knew of their allocation. A study of antenatal services showed that preferences can be an important determinant of outcome, but we did not find any strong effect of preference on the outcome, although a much larger sample size would be needed to confidently exclude any modest interaction between preference and outcome. This information may be useful to clinicians in that it suggests that exercise classes are effective even in patients who are not highly motivated. Our trial design, of asking patients for their preferences at the outset, has substantial advantages over the usual patient preference design, in which costs and outcomes cannot be reliably controlled for confounding by preference.
Conclusions
Our exercise programme did not seem to influence the intensity of pain but did affect the participants� ability to cope with the pain in the short term and even more so in the longer term. It used a cognitive-behavioural model, shifting the emphasis away from a disease model to a model of normal human behaviour, and with minimal extra training a physiotherapist can run it. Patients� preferences did not seem to influence the outcome.
Figure 1: Flow chart describing patients’ progress through the trial.
Footnotes
Funding: This research was funded by the Arthritis Research Campaign, the Northern and Yorkshire Regional Health Authority, and the National Back Pain Association.
Competing interests: None declared.
In conclusion,�the participation of patients in functional fitness and/or exercise as recommended by a physiotherapist, or physical therapist, or any other healthcare professional, such as a chiropractor, is essential towards the improvement of their symptoms of low back pain. The exercise programme helped patients better cope with their symptoms of back pain where the intervention group showed that they used fewer healthcare resources and took fewer day off work, according to the outcome measures of the research study. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is referred to as a collection of symptoms rather than a single type of injury or condition. The symptoms are characterized as radiating pain, numbness and tingling sensations from the sciatic nerve in the lower back, down the buttocks and thighs and through one or both legs and into the feet. Sciatica is commonly the result of irritation, inflammation or compression of the largest nerve in the human body, generally due to a herniated disc or bone spur.
3.�Waddell G, Feder G, McIntosh A, Lewis M, Hutchinson A.�Low back pain evidence review.�London: Royal College of General Practitioners; 1996.
4.�Malmivaara A, Hakkinen U, Aro T, Heinrichs M, Koskenniemi L, Kuosma E, et al. The treatment of acute low back pain�bed rest, exercises or ordinary activity?�N Engl J Med.�1995;332:351�355.[PubMed]
5.�Faas A, Chavannes A, van Eijk JTM, Gubbels J. A randomized, placebo-controlled trial of exercise therapy in patients with acute low back pain.�Spine.�1993;18:1388�1395.�[PubMed]
6.�Frost H, Klaber Moffett J, Moser J, Fairbank J. Evaluation of a fitness programme for patients with chronic low back pain.�BMJ.�1995;310:151�154.�[PMC free article]�[PubMed]
7.�Frost H, Lamb S, Klaber Moffett J, Fairbank J, Moser J. A fitness programme for patients with chronic low back pain: 2 year follow-up of a randomised controlled trial.�Pain.�1998;75:273�279.�[PubMed]
8.�McPherson K, Britton A, Wennberg J. Are randomised controlled trials controlled? Patient preferences and unblind trials.�J R Soc Med.�1997;90:652�656.�[PMC free article]�[PubMed]
9.�Bradley C. Designing medical and educational studies.�Diabetes Care.�1993;16:509�518.�[PubMed]
10.�Clement S, Sikorski J, Wilson J, Candy B. Merits of alternative strategies for incorporating patient preferences into clinical trials must be considered carefully [letter]�BMJ.�1998;317:78.�[PubMed]
11.�Torgerson D, Klaber Moffett J, Russell I. Patient preferences in randomised trials: threat or opportunity?�J Health Serv Res Policy.�1996;1(4):194�197.�[PubMed]
12.�Roland M, Morris R. A study of the natural causes of back pain. Part 1: Development of a reliable and sensitive measure of disability in low-back pain.�Spine.�1983;8:141�144.�[PubMed]
13.�Ruta D, Garratt A, Wardlaw D, Russell I. Developing a valid and reliable measure of health outcome for patients with low back pain.�Spine.�1994;19:1887�1896.�[PubMed]
14.�Brooks R.with EuroQoL Group.�EuroQoL: the current state of play�Health Policy�19963753�72.[PubMed]
15.�Waddell G, Newton M, Henderson I, Somerville D, Main C. A fear-avoidance beliefs questionnaire (FABQ) and the role of fear-avoidance beliefs in chronic low back pain and disability.�Pain.�1993;52:157�168.�[PubMed]
16.�Jensen M, McFarland C. Increasing the reliability and validity of pain intensity measurement in chronic pain patients.�Pain.�1993;55:195�203.�[PubMed]
17.�Efron B, Tibshirani R.�An introduction to bootstrap.�New York: Chapman and Hall; 1993.
18.�Williams D, Keefe F. Pain beliefs and use of cognitive-behavioral coping strategies.�Pain.�1991;46:185�190.�[PubMed]
19.�Estlander A, Harkapaa K. Relationships between coping strategies, disability and pain levels in patients with chronic low back pain.�Scand J Behav Ther.�1989;18:56�69.
20.�Holmes J, Stevenson C. Differential effects of avoidant and attentional coping strategies on adaption to chronic and recent-onset pain.�Health Psychology.�1990;9:577�584.�[PubMed]
21.�Rosenstiel A, Keefe F. The use of coping strategies in chronic low back pain patients: relationship to patient characteristics and current adjustments.�Pain.�1983;17:33�44.�[PubMed]
22.�Slade P, Troup J, Lethem J, Bentley G. The fear avoidance model of exaggerated pain perception II Preliminary studies of coping strategies for pain.�Behav Res Ther.�1983;21:409�416.�[PubMed]
23.�Meade T, Dyer S, Browne W, Frank A. Randomised comparison of chiropractic and hospital outpatient management for low back pain: results from extended follow up.�BMJ.�1995;311:349�351.[PMC free article]�[PubMed]
24.�Cherkin D, Deyo R, Battie M, Street J, Barlow W. A comparison of physical therapy, chiropractic manipulation, and provision of an educational booklet for the treatment of patients with low back pain.�N Engl J Med.�1998;339:1021�1029.�[PubMed]
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine




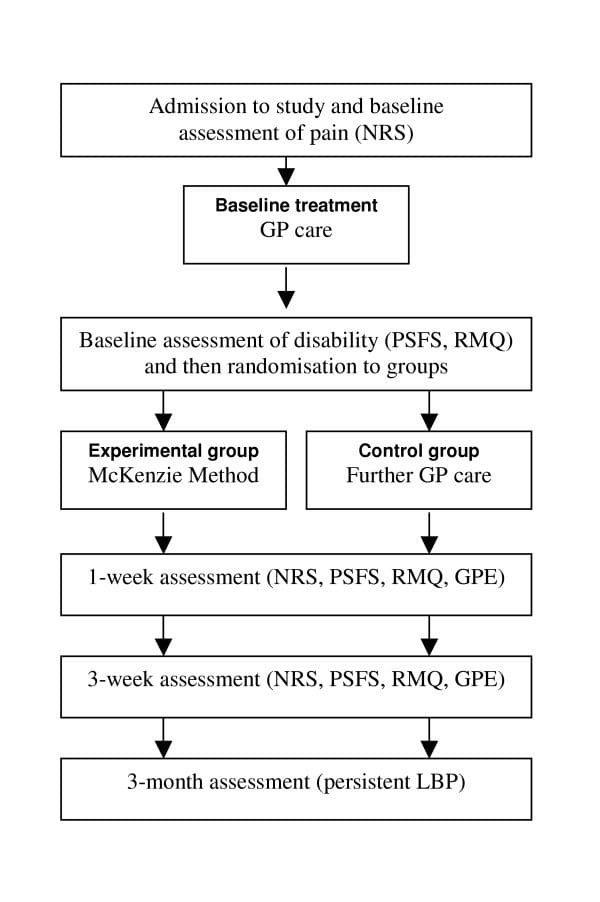


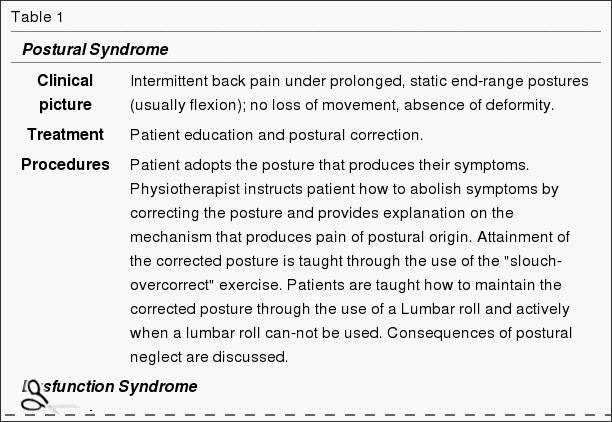






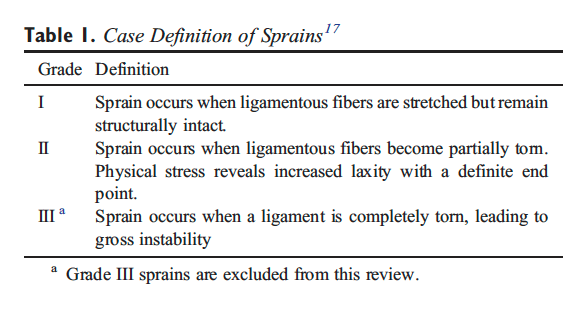
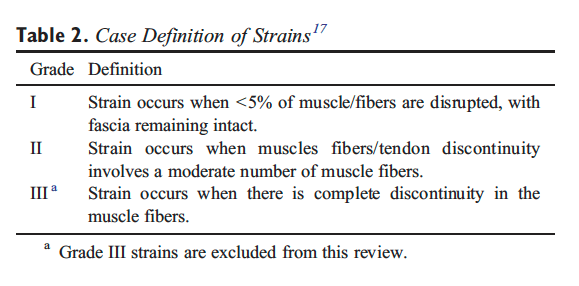

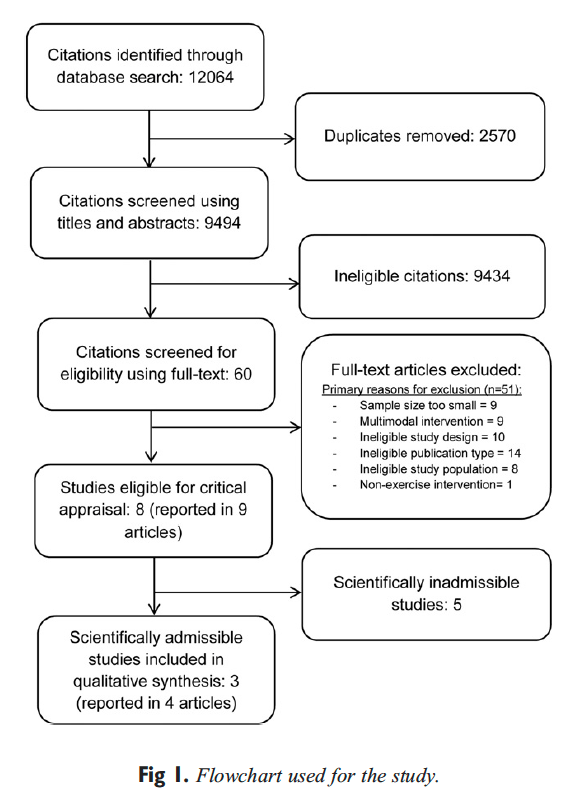
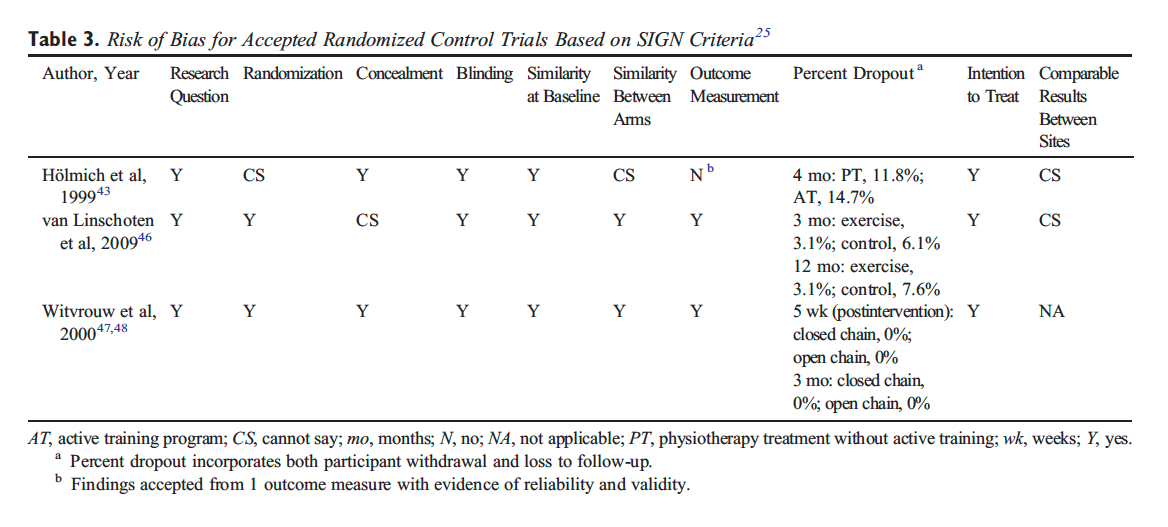

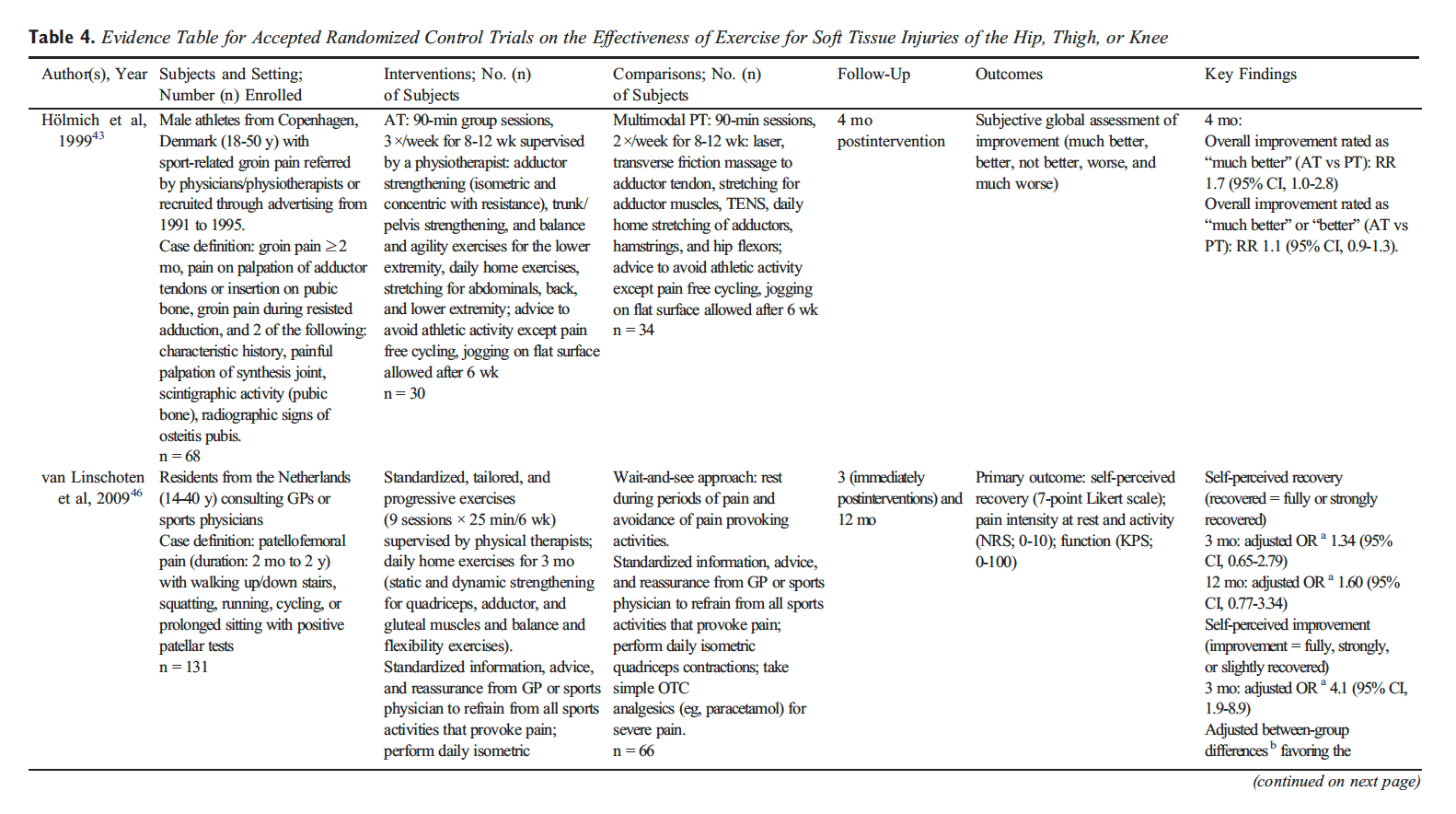
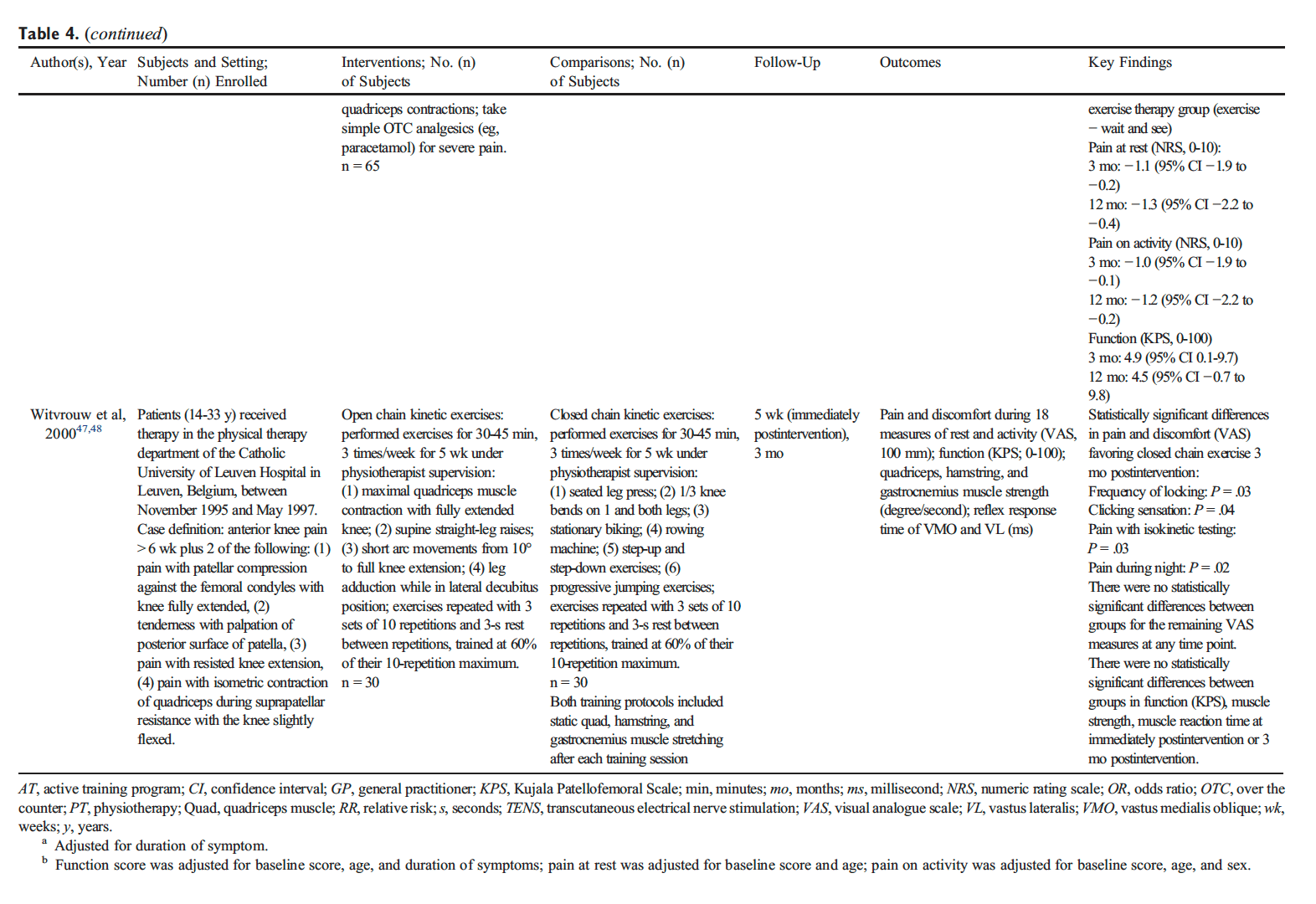



 #1: Reduces Inflammation To Promote Healing
#1: Reduces Inflammation To Promote Healing