Opioids and Prescription drug abuse and addiction is a significant problem in the United States. In fact, the U.S. Department of Health and Human Services (HHS) has declared it an epidemic.
Researchers estimate that as many as 36 million people worldwide abuse opioids. Estimates in the U.S. alone reached 2.1 million people in 2012. In 2014, six out of ten drug overdose deaths involved an opioid � including prescription opioids for pain relief.
Every day, 78 Americans die from an opioid overdose. As the Opioid drug problem continues to spiral further out of control, claiming more lives, people are looking for safer, drug free ways to relieve their pain. Chiropractic offers such an option.
What Are Opioids?
Opioids are prescription medications that are intended for pain relief. They work by diminishing the intensity level of pain signals as they reach the brain. They also affect the areas of the brain that control emotion thereby weakening the perception of the pain as well. There are several very popular medications that are classified as opioids:
Hydrocodone (Vicodin)
Oxycodone (Percocet, OxyContin)
Morphine (Avinza, Kadian)
Codeine
The most commonly prescribed opioids are hydrocodone products. They are used to treat pain from injuries, dental work, and typically moderate pain. Milder pain is often treated with codeine but it is also used to treat coughing as well as severe diarrhea. Overall, opioids are used to treat everything from cancer pain to post-op pain to osteoarthritis.
What Are The Dangers Of Opioids?
Opioids have a serious risk of abuse, addiction, and overdose. Even then they are taken as prescribed, opioids can have the following side effects:
Excessive sleepiness
Nausea
Dry mouth
Vomiting
Confusion
Dizziness
Depression
Constipation
Low energy
Sweating
Low testosterone levels that result in a diminished sex drive
Itching
Decreased strength
Increased pain sensitivity
Over time, the body can build up a tolerance to the drug which means that in order to achieve the same relief from pain they must take more of it. Physical dependence is also a concern, usually going hand in hand with tolerance. Once that point is reached the patient will experience symptoms of withdrawal if they stop taking the medication.
If Doctors Are Prescribing Opioids, How Are People becoming Addicted?
In 2013, doctors wrote almost a quarter of a billion prescriptions for opioids. To put that into perspective, that is enough for every adult in the U.S. to have their own bottle of the drug. Doctors prescribe opioids to their patients in an effort to treat pain, but most of the time it is just a band aid. Instead of seeking out the root of the problem and educating their patients on whole body wellness, they prescribe pills that numb the senses, cause unpleasant or even dangerous side effects, and create addictions.
As the patient develops a tolerance for the drug, the doctor increases the prescription. This cycle continues as the patient become more and more dependent upon the drug. They may even experience more pain as the drug increases their pain sensitivity. As patients become addicted, the number of prescription opioid overdose deaths is steadily increasing. The most common drugs involved in these overdose deaths include:
Hydrocodone (Vicodin)
Oxycodone (OxyContin)
Methadone
States are putting measures in place to monitor and regulate how doctors prescribe opiates, but when desperate, addicted patients will go to great lengths to obtain the drugs they are addicted to. They will go to different doctors to get additional prescriptions or even find ways to obtain the drug illegally. It is a heartbreaking problem that is completely preventable.
How Is Chiropractic A Safer Alternative To Opioids?
Chiropractic is a proven method for managing pain relief that is not only effective but safe and drug free. Numerous chiropractic studies confirm what chiropractic patients have been saying for decades: chiropractic care is an excellent pain management method. The spinal adjustments bring the body into balance but that is only the beginning of the benefits. Chiropractic focuses on whole body wellness so patients learn how to take proactive steps to treat their condition.
It also seeks to find the root of the problem and begin healing by treating the cause. Through exercise, diet, and lifestyle recommendations in addition to the chiropractic adjustments, patients can get relief from pain caused by injury, surgery, arthritis, and many other conditions. Chiropractic is so much more than a back pain treatment; it is a whole body, whole patient treatment.
Muscle Relaxants? Nearly everyone, more than 80 percent of the world�s population, will experience back pain at some point in their lifetime. Just ask the 31 million Americans suffering from low back pain at any given time.
In fact, globally it is the leading cause of disability. It is the most common reason that people miss work and the second more common reason for doctor�s office visits. In the United States alone more than $50 billion is spent each year trying to relieve back pain, but even that figure is not complete, but only based on trackable, identifiable costs.
There have been studies published over the years that unequivocally show chiropractic as a viable and extremely effective treatment for back pain. Several of these studies plainly show that chiropractic is better than muscle relaxants.
Muscle Relaxants & Chiropractic Study
One study that is one of the most notable was conducted at Life University in Georgia. It has been cited in several journals and used as a catalyst for proving the efficacy of chiropractic treatment for back pain and its superiority to muscle relaxants.
Study Parameters
The study involved 192 subjects who had been experiencing lower back pain for a period of time ranging from two to six weeks. The subjects were separated into three groups:
Group One – Chiropractic adjustments combined with placebo medication
Group Two � Muscle relaxants combined with sham chiropractic adjustments
Group Three � Control Group � received both placebo medication and sham chiropractic adjustments
All groups were given the same length of care, four weeks, with an evaluation of progress at the two-week mark and the four-week mark. The pain was assessed using the Zung Self-Rating for Depression scale, the Oswestry Low Back Pain Disability Questionnaire, and the Visual Analog Scale (VAS). Upon admission into the study during the initial visit as well as at the two-week evaluation, Shober�s Test for Lumbar Flexibility was also administered.
The subjects in all three groups were also allowed to take acetaminophen for pain. This was an additional evaluative measure to assess the need for additional self-medication.
During the course of the study there was a two-week treatment period where the subjects in the chiropractic adjustment group received a total of seven adjustments. These adjustments were tailored to each patient�s specific needs and included pelvic adjustments, sacral (lower back), or lumbar and upper cervical (neck and back).
The sham treatments mimicked all aspects of an actual chiropractic adjustment including dialog, normal visit length, and procedures. However, no actual adjustments were performed.
Study Results
At the conclusion of the study, the subjects who received chiropractic treatment reported a significant decrease in pain and an increase in flexibility. Of the groups that did not receive chiropractic treatment there were no significant differences noted. There was a decrease in disability and depression across all three groups, indicating that muscle relaxants are effective in treating back pain, but overall chiropractic care is the more effective option for treating back pain and disability.
What Does This Mean For Patients With Back Pain?
Patients suffering from back pain can receive greater relief without the undesirable side effects of muscle relaxants by seeking chiropractic care. Patients who are using muscle relaxants to treat their back pain should talk to their chiropractor and doctor about incorporating chiropractic treatment into their patient care regimen. Patients experiencing back pain should pursue chiropractic care before resorting to more aggressive methods including muscle relaxants.
Chiropractic care is a safe, non-invasive treatment for back pain. It also facilitates healing, increases flexibility, and improves mobility. Patients who are looking for a healthy treatment option that focuses on overall wellness, Chiropractic could be the answer.
Chiropractic Care: Tracy Ludech, club director and coach of the El Paso Diggers, expresses how much of a difference the fitness program at PUSH has done for her athletes. Working cohesively and diligently together with the staff and trainers at PUSH, Tracy Ludech has witnessed tremendous improvements in her athlete’s strength, mobility and flexibility. Tracy Ludech encourages others to experience the benefits that a fitness program can have on young athletes.
Chiropractic Care Power & Rehabilitation
Physical wellness is a condition of health and well-being and, more especially, the ability to do aspects of sport, jobs and daily activities. Physical fitness is generally accomplished through proper nourishment, moderate-vigorous physical exercise, and sufficient rest. An extensive fitness program tailored to someone normally concentrates on one or more specific skills, and on medical needs like bone health. Many sources also cite psychological, social and emotional wellbeing as an significant part overall wellbeing. Physical fitness may also prevent or treat several chronic health conditions brought on by unhealthy lifestyle or aging.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
Concussions are traumatic brain injuries that affect brain function. Effects from these injuries are often temporary but can include headaches, problems with concentration, memory, balance and coordination. Concussions are usually caused by a blow to the head or violent shaking of the head and upper body. Some concussions cause loss of consciousness, but most do not. And it is possible to have a concussion and not realize it. Concussions are common in contact sports, such as football. However, most people gain a full recovery after a concussion.
Can also happen due to excessive shaking of the head or acceleration/deceleration
Mild injuries (mTBI/concussions) are the most common type of brain injury
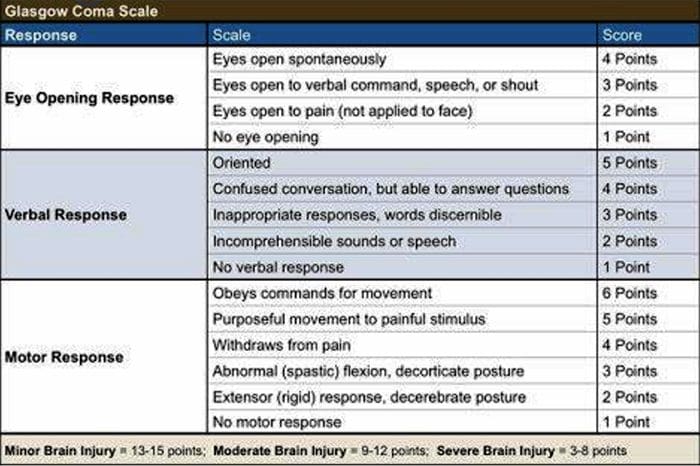
Glasgow Coma Scale
Common Causes Of Concussion
Motor vehicle collisions
Falls
Sports injuries
Assault
Accidental or intentional discharge of weapons
Impact with objects
Prevention
Prevention of concussive injuries can be paramount
Encourage Patients To Wear Helmets
Competitive sports, especially boxing, hokey, football and baseball
Horseback riding
Riding bicycles, motorcycles, ATVs, etc.
High elevation activates such as rock climbing, zip lining
Skiing, snowboarding
Encourage Patients To Wear Seatbelts
Discuss the importance of wearing seatbelts at all times in vehicles with all of your patients
Also encourage use of appropriate booster or car seats for children to ensure adequate fit and function of seat belts.
Driving Safely
Patients should never drive while under the influence of drugs, including certain medications or alcohol
Never text and drive
Make Spaces Safer For Children
Install baby gates and window latches in the home
May in areas with shock-absorbing material, such as hardwood mulch or sand
Supervise children carefully, especially when they�re near water
Prevent Falls
Clearing tripping hazards such as loose rugs, uneven flooring or walkway clutter
Using nonslip mats in the bathtub and on shower floors, and installing grab bars next to the toilet, tub and shower
Ensure appropriate footwear
Installing handrails on both sides of stairways
Improving lighting throughout the home
Balance training exercises
Balance Training
Single leg balance
Bosu ball training
Core strengthening
Brain balancing exercises
Concussion Verbiage
Concussion vs. mTBI (mild traumatic brain injury)
mTBI is the term being used more commonly in medical settings, but concussion is a more largely recognized term in the community by sports coaches, etc.
The two terms describe the same basic thing, mTBI is a better term to use in your charting
Evaluating Concussion
Remember that there does not always have to be loss of consciousness for there to be a concussion
Post-Concussion Syndrome can occur without LOC as well
Symptoms of concussion may not be immediate and could take days to develop
Monitor for 48 post head injury watching for red flags
Blurred eyesight or other vision problems, such as dilated or uneven pupils
Confusion
Dizziness
Ringing in the ears
Nausea or vomiting
Slurred speech
Delayed response to questions
Memory loss
Fatigue
Trouble concentrating
Continued or persistent memory loss
Irritability and other personality changes
Sensitivity to light and noise
Sleep problems
Mood swings, stress, anxiety or depression
Disorders of taste and smell
Mental/Behavioral Changes
Verbal outbursts
Physical outbursts
Poor judgment
Impulsive behavior
Negativity
Intolerance
Apathy
Egocentricity
Rigidity and inflexibility
Risky behavior
Lack of empathy
Lack of motivation or initiative
Depression or anxiety
Symptoms In Children
Concussions can present differently in children
Excessive crying
Loss of appetite
Loss of interest in favorite toys or activities
Sleep issues
Vomiting
Irritability
Unsteadiness while standing
Amnesia
Memory loss and failure to form new memories
Retrograde Amnesia
Inability to remember things that happened before the injury
Due to failure in recall
Anterograde Amnesia
Inability to remember things that happened after the injury
Due to failure to formulate new memories
Even short memory losses can be predictive of outcome
Amnesia may be up to 4-10 times more predictive of symptoms and cognitive deficits following concussion than is LOC (less than 1 minute)
Return To Play Progression
Baseline: No Symptoms
As the baseline step of the Return to Play Progression, the athlete needs to have completed physical and cognitive rest and not be experiencing concussion symptoms for a minimum of 48 hours. Keep in mind, the younger the athlete, the more conservative the treatment.
Step 1: Light Aerobic Activity
The Goal: Only to increase an athlete�s heart rate.
The Time: 5 to 10 minutes.
The Activities: Exercise bike, walking, or light jogging.
Absolutely no weight lifting, jumping or hard running.
Step 2: Moderate activity
The Goal: Limited body and head movement.
The Time: Reduced from typical routine.
The Activities: Moderate jogging, brief running, moderate-intensity stationary biking, and moderate-intensity weightlifting
Step 3: Heavy, non-contact activity
The Goal: More intense but non-contact
The Time: Close to typical routine
The Activities: Running, high-intensity stationary biking, the player�s regular weightlifting routine, and non- contact sport-specific drills. This stage may add some cognitive component to practice in addition to the aerobic and movement components introduced in Steps 1 and 2.
Step 4: Practice & full contact
The Goal: Reintegrate in full contact practice.
Step 5: Competition
The Goal: Return to competition.
Microglial Priming
After head trauma microglial cells are primed and can become over active
To combat this, you must mediate the inflammation cascade
Prevent repeated head trauma
Due to priming of the foam cells, response to follow-up trauma may be far more severe and damaging
What Is Post-Concussion Syndrome (PCS)?
Symptoms following head trauma or mild traumatic brain injury, that can last weeks, months or years after injury
Symptoms persist longer than expected after initial concussion
More common in women and persons of advanced age who suffer head trauma
Severity of PCS often does not correlate to severity of head injury
PCS Symptoms
Headaches
Dizziness
Fatigue
Irritability
Anxiety
Insomnia
Loss of concentration and memory
Ringing in the ears
Blurry vision
Noise and light sensitivity
Rarely, decreases in taste and smell
Concussion Associated Risk Factors
Early symptoms of headache after injury
Mental changes such as amnesia or fogginess
Fatigue
Prior history of headaches
Evaluation Of PCS
PCS is a diagnosis of exclusion
If patient presents with symptoms after head injury, and other possible causes have been ruled out => PCS
Use appropriate testing and imaging studies to rule out other causes of symptoms
Headaches In PCS
Often �tension� type headache
Treat as you would for tension headache
Reduce stress
Improve stress coping skills
MSK treatment of the cervical and thoracic regions
Constitutional hydrotherapy
Adrenal supportive/adaptogenic herbs
Can be migraine, especially in people who had pre-existing migraine conditions prior to injury
Reduce inflammatory load
Consider management with supplements and or medications
Reduce light and sound exposure if there is sensitivity
Dizziness In PCS
After head trauma, always assess for BPPV, as this is the most common type of vertigo after trauma
Dix-Hallpike maneuver to diagnose
Epley�s maneuver for treatment
Light & Sound Sensitivity
Hypersensitivity to light and sound is common in PCS and typically exacerbates other symptoms such as headache and anxiety
Management of excess mesencephalon stimulation is crucial in such cases
Sunglasses
Other light blocking glasses
Earplugs
Cotton in ears
Treatment Of PCS
Manage each symptom individually as you otherwise would
Manage CNS inflammation
Curcumin
Boswelia
Fish oil/Omega-3s � (***after r/o bleed)
Cognitive behavioral therapy
Mindfulness & relaxation training
Acupuncture
Brain balancing physical therapy exercises
Refer for psychological evaluation/treatment
Refer to mTBI specialist
mTBI Specialists
mTBI is difficult to treat and is an entire specialty both in the allopathic and complementary medicine
Primary objective is to recognize and refer for appropriate care
Pursue training in mTBI or plan to refer to TBI specialists
Sources
�A Head for the Future.� DVBIC, 4 Apr. 2017, dvbic.dcoe.mil/aheadforthefuture.
Alexander G. Reeves, A. & Swenson, R. Disorders of the Nervous System. Dartmouth, 2004.
�Heads Up to Health Care Providers.� Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 16 Feb. 2015, www.cdc.gov/headsup/providers/.
�Post-Concussion Syndrome.� Mayo Clinic, Mayo Foundation for Medical Education and Research, 28 July 2017, www.mayoclinic.org/diseases-conditions/post- concussion-syndrome/symptoms-causes/syc-20353352.
Functional short leg is a fairly common condition that typically occurs due to inflexibility or muscle weakness at the pelvis, ankle, and foot complex. Runners sometimes experience the condition when running over certain surfaces that are unstable or not level. It can also occur due to inappropriate footwear.
This condition can cause pain in the lower spine, hips, buttock, and leg. If left untreated, it can lead to balance issues, neck and shoulder problems, and incorrect weight distribution. Chiropractic care has been proven to effectively treat functional leg syndrome.
What Is Functional Short Leg?
Patients with a functional short leg have an apparent short leg although structurally both legs are the same length when measured. The most common method for measuring leg length is from the medial malleolus (inside ankle bone) to the ASIS (front of the pelvis). When the legs are measured in the case of a functional short leg, they are equal in length.
Mothers who always carry a child on one hip or individuals who always sleep on the same side can experience functional short leg syndrome. In fact, any movement, posture, or activity that causes increased stresses on the joints, nerves, and muscles involved can create an imbalance.
Functional Short Leg vs Anatomical Short Leg
Where with functional short leg syndrome one leg is apparently shorter than the other but not structurally so, an anatomical short leg is structurally shorter. This can happen due to growth problems, structural issues, and curvature of the spine.
The differences between the two conditions are significant, particularly when it comes to treatment. Both conditions can be treated by chiropractic for pain. Functional short leg syndrome can greatly benefit from chiropractic care as it helps to realign the body.
Symptoms Of Functional Short Leg
Functional short leg syndrome symptoms can remain confined to the leg, lower back, and hip region, or it can affect the entire body. When walking it can affect the way your feet hit the ground, causing pain in the foot and ankle.
However, it can even affect how you chew your food and how your teeth come together. When a person has short leg syndrome, they will often adjust their body in order to compensate, but that is when the real problems start. Symptoms of functional short leg syndrome include:
Pain in the lower back
Pain in the knee of both the long and short legs
Pain in the leg and lower back due to inflammation or sciatica
The human body is a marvelous, mysterious machine. When part of the machine is not working properly, the body will naturally attempt to fix it. If it cannot fix the problem, it finds a work around to compensate for the problem. This can lead to misalignment of the spine and imbalance in the body.
Chiropractic Treatment For Functional Short Leg
When you go to a chiropractor for functional short leg, he or she will do a thorough exam on you including diagnostic tests like MRI and x-ray. Once a diagnosis has been confirmed, the chiropractor will begin what is usually a multi-faceted approach that incorporates spinal alignment, a heel lift, lifestyle change recommendations, and exercises that you can do at home.
The chiropractic adjustments will return the spine to its natural position and bring the body back into balance. Patients will usually experience a dramatic decrease in pain or the pain will go away completely. They will also enjoy increased mobility and flexibility as well and an overall sense of wellness.
Injury Medical Clinic: Athletic Recovery & Rehabilitation
Tension headaches are the most prevalent types of headaches, occurring more often in women than in men. Research shows that 48 percent of women and 38 percent of men suffer from tension headaches.
Each year, patients spend more than $2 billion on over the counter headache medications. In fact, people spend a lot of money and effort seeking remedies for headaches. From prescription medication to over the counter drugs to alternative headache treatments like meditation, acupuncture, and chiropractic.
In fact, chiropractic is a proven treatment for these types headaches, but there is more to it than just adjustments. Chiropractic offers a whole body approach to treatment that can not only relieve the pain of these headaches, but help prevent them as well.
What Are Tension Headaches?
The most common type of headache is the tension headache which is described as pain ranging from mild to moderate that feels like a tight band is wrapped around the head. While stress can be a factor in the cause of these headaches, it still isn�t well understood how these headaches originate. Symptoms of a tension headache include:
Aching, dull pain in the head
Sensation of pressure or tightness on the back and sides of the head or across the forehead
Tenderness in the shoulder muscles, neck, and scalp
There are two categories of tension headaches: chronic and episodic. There are two primary factors that identify each type. The length of the headache and the frequency can help you determine which type of tension headache you have.
Chronic Tension Headaches
Length of Headache � hours and can be continuous
Frequency of Headache � occur 15 days or more a month for three or more months
Episodic Tension Headaches
Length of Headache – half hour to a week
Frequency of Headache � occur less than 15 days a month for three or more months
There are two primary risk factors for tension headaches:
Women � Research shows that nearly 90 percent of women will experience tension headaches throughout the course of their life. Only 70 percent of men will experience tension headaches in their lifetime.
Middle Age � Tension headaches increase as people approach 40 and peak at middle age, or when a person is in their 40s. However, anyone can get a tension headache, regardless of age.
Lifestyle Changes To Treat Tension Headaches
A chiropractor can treat tension headaches through traditional spinal manipulation and adjustments, but they also provide advice on lifestyle and nutrition. Several things that your chiropractor may suggest include applying heat or ice to the area around your neck, shoulders, or head. A warm bath or shower may also help.
Stress management is another way that you can learn to manage and prevent tension headaches. This is typically a combination of minimizing stress in your life and learning relaxation techniques. Your chiropractor may also help you improve your posture. Poor posture is a very common contributing factor for many types of headaches.
Chiropractic for Tension Headaches
Your Doctor of Chiropractic will sit down with you to discuss your history, including your headaches. He or she will conduct diagnostic tests including x-rays, MRIs and other to determine if there are underlying causes for your headaches. They will recommend various lifestyle changes including dietary changes and exercises that you can do.
Your doctor may also perform chiropractic adjustments, or spinal manipulation which will help return the body to proper balance, improving spinal function and alleviating stress on the body and system. This helps to relieve pain as an immediate treatment, but when performed consistently, chiropractic can also help prevent tension headaches, allowing you to live pain free.
Injury Medical Clinic: Migraine Treatment & Recovery
Injured: In 2014, there were 2.8 million occupational injuries. This crossed all industries, but 75 percent were in those that provided a service.
These injuries can lead to time lost at work, decrease in production, depression, and temporary (or permanent) disability. These injuries can be caused by slip and fall, vehicle collisions, electrocution, struck by hazards, and caught in or between accidents. However, work related injury can also be caused by sitting at a desk or hunched over a computer for extended periods of time. Chiropractic has been shown to help workers who have been injured on the job, so they can return to work faster.
Injured
Common Occupational Injuries
Occupational injuries are vast and varied with a host of causes and many different symptoms. They can range from minor annoyances to significant damage that can lead to temporary or permanent disability. Some may require surgery while others require extended physical therapy, braces, and intensive medical treatments.
Thoracic outlet syndrome � This injury is caused by flexing the shoulder, carrying loads on your shoulders, and extending your arms above shoulder height for a prolonged period of time. It is marked by swelling, pain, dull ache, weakness, or a burning sensation in the affected area.
Elbow tendonitis (Epicondylitis) � This injury is caused by forceful or repeated forearm rotation while simultaneously bending the wrist. It is marked by swelling, dull ache, pain, burning, and weakness in the affected area.
Carpal tunnel syndrome � This injury can be caused by several things including vibratory tools, repetitive motion, and secondary factors. It is marked by numbness, pain, tingling, wasting of muscles at the thumb base, and burning.
DeQuervain�s disease � This injury is caused by forceful gripping and repetitive hand twisting. It is marked by pain at the thumb base.
Tendonitis/tenosynovitis � This injury is caused by sustained hyperextension of the knee, repetitive motion, and prolonged load overuse. It is marked by numbness, pain, and swelling in the hands.
Back and neck pain � This injury can have a wide variety of causes from repetitive motion to accident to improper equipment. It is the most common work related injury.
Preventing Workplace Injuries
While a few work related injuries are unavoidable, many can be prevented with a little extra attention and care. The American Chiropractic Association recommends the following practices to reduce the risk of a workplace injury.
Get regular exercise. This helps prevent back injuries by keeping your body strong, fit, and flexible.
If you do desk work, get a chair that fits you. This means that there should be two inches between the backs of your knees and the front edge of the seat. Your knees should be level with your hips or slightly below, never higher.
When doing computer work, use a foot rest for support and keep your knees between a 90 degree and 120-degree angle.
If your job requires you to sit for extended periods of time, take breaks at least every two hours to walk and stretch.
When you lift something heavy or awkward, don�t bend over to do it. Bend at your knees and hips, squatting as you pick up the object and let your legs do the work and keeping the object close to your body while your back remains straight. Do not let your body twist while you are trying to lift.
Of course, you should also follow all recommended and required safety guidelines for your workstation and place of employment.
Chiropractic For Workplace Injuries
Chiropractic care can help speed your recovery, improve your posture, and restore your mobility and strength. Through various chiropractic techniques, many of the occupational injuries listed here can be effectively treated. Chiropractic is a proven method for managing pain for the back and neck, but it has also been proven to be very beneficial for conditions like carpal tunnel, elbow tendonitis, and knee injuries.
Chiropractic�s whole body approach helps injured workers not only manage their pain and help heal their injury through adjustments, it can also help with soft tissue rehabilitation and other noninvasive therapies that improve range of motion. In short, chiropractic can help workers get back to work faster so less time is lost from work and the financial impact is greatly decreased.
Injury Medical Clinic: Accident Treatment & Recovery
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine