Dr. Alex Jimenez, chiropractor in El Paso, TX, discusses BIA, BMI and basal metabolic rate with staff. Dr. Alex Jimenez, health coach Kenna Vaughn, Astrid Ornelas, Truide Torres, and biochemist Alexander Isaiah Jimenez all take part in a round table podcast discussion of the importance of measuring BMI, BIA, and basal metabolic rate. BMI or body mass index is frequently utilized to determine an individual’s relative weight according to their height. Healthcare professionals commonly utilize BMI, however, BMI may not be accurate for athletes because their body mass according to their height may demonstrate that they have excess weight or obesity utilizing BMI. BIA is the preferred analysis tool used to determine an athlete’s relative weight according to their height. Excess weight and obesity is a well-known risk factor that can ultimately increase the risk of metabolic syndrome, among other health issues, including diabetes, stroke, and heart disease. Dr. Alex Jimenez, health coach Kenna Vaughn, Astrid Ornelas, Truide Torres, and biochemist Alexander Isaiah Jimenez ultimately discuss in further detail how determining an individual’s BIA, BMI, and basal metabolic rate can help promote overall health and wellness as well as support weight loss for the general population and athletes alike. – Podcast Insight
If you have enjoyed this video and/or we have helped you in any way
please feel free to subscribe and share with us.
Thank You & God Bless.
Dr. Alex Jimenez RN, DC, MSACP, CCST
Dr. Alex Jimenez, a chiropractor in El Paso, TX, and Dr. Mario Ruja, a chiropractor in El Paso, TX, discuss how chiropractic care can help with personal injuries, especially automobile accidents. Personal injuries can also include work injuries and slip-and-fall injuries. Auto accidents can cause a variety of injuries and underlying conditions, including neck pain, whiplash, back pain, low back pain, and sciatica. Sports injuries can also cause a variety of health issues. Chiropractic care is a safe and effective alternative treatment option that focuses on the diagnosis, treatment, and prevention of health issues associated with the musculoskeletal and nervous system. Dr. Alex Jimenez and Dr. Mario Ruja discuss how spinal adjustments and manual manipulations are commonly utilized to treat neck pain and back pain associated with personal injuries. Whiplash-associated-disorders are the most common types of health issues resulting after an automobile accident. Chiropractic care can carefully restore the original alignment of the spine, treating neck pain and whiplash caused by personal injuries, especially an auto accident. Dr. Alex Jimenez, a chiropractor in El Paso, TX, and Dr. Mario Ruja, a chiropractor in El Paso, TX further discuss how it’s fundamental for people who’ve been involved in a car crash to seek chiropractic care to treat soft tissue injuries that can cause neck pain and back pain. – Podcast Insight
If you have enjoyed this video and/or we have helped you in any way
please feel free to subscribe and share us.
Thank You & God Bless.
Dr. Alex Jimenez RN, DC, MSACP, CCST
In the following podcast video article, Dr. Alex Jimenez, a chiropractor in El Paso, TX, and Daniel (Danny) Alvarado, owner of PUSH Fitness Center in El Paso, TX, discuss the three points of weight loss. Excess weight and obesity are associated with metabolic syndrome and a variety of other health issues. Metabolic syndrome is a cluster of risk factors that can ultimately increase the risk of developing diabetes, stroke, and diabetes, among other complications. Dr. Alex Jimenez and Daniel Alvarado discuss how weight loss can be a safe and effective way to improve metabolic syndrome as well as overall health and wellness. Decreasing or eliminating sugar and carbohydrate consumption, increasing the consumption of proteins, �good� fats, and vegetables, as well as engaging and participating in exercise and physical activity can ultimately help promote weight loss to improve metabolic syndrome and a variety of other health issues. Furthermore, Dr. Alex Jimenez and Daniel Alvarado discuss how they can help people with excess weight and obesity achieve their weight loss goals by encouraging and motivating them through every step of the way. Weight loss is essential for people with metabolic syndrome to achieve overall health and wellness. � Podcast Insight
If you have enjoyed this video and/or we have helped you in any way
please feel free to subscribe and share us.
Thank You & God Bless.
Daniel Alvarado & Dr. Alex Jimenez
Subscribe: http://bit.ly/drjyt
Facebook Fitness Center Page: https://www.facebook.com/PUSHftinessathletictraining/
Yelp: El Paso Rehabilitation Center: http://goo.gl/pwY2n2
Yelp: El Paso Clinical Center: Treatment: https://goo.gl/r2QPuZ
Metabolic syndrome is a cluster of risk factors that can ultimately increase the risk of developing a variety of health issues, including heart disease, stroke, and diabetes, among other problems. Central obesity, high blood pressure, high blood sugar, high triglycerides, and low HDL or good cholesterol levels are the 5 risk factors associated with metabolic syndrome. Having at least three of the five risk factors may suggest the presence of metabolic syndrome. Dr. Alex Jimenez, Alexander Jimenez, Truide Torres, Kenna Vaughn, and Astrid Ornelas explain the 5 risk factors associated with metabolic syndrome, in further detail, as they recommend diet and lifestyle modification advice and guidelines, such as the ketogenic diet or the keto diet, as well as demonstrate the biochemical and chemical pathways that the body goes through during ketosis to help people with metabolic syndrome improve their overall health and wellness. From eating good fats and staying hydrated to exercise and better sleep, Dr. Alex Jimenez, Alexander Jimenez, Truide Torres, Kenna Vaughn, and Astrid Ornelas discuss how diet and lifestyle modifications, such as the ketogenic diet or keto diet, can help improve the 5 risk factors associated with metabolic syndrome to prevent the risk of developing a variety of other health issues, including heart disease, stroke, and diabetes. � Podcast Insight
If you have enjoyed this video and/or we have helped you in any way
please feel free to subscribe and share us.
Thank You & God Bless.
Dr. Alex Jimenez RN, DC, MSACP, CCST
Everybody has a backstory. It is not easy. We got to PUSH Hard. It is not EASY…Dr. Alex Jimenez, a chiropractor in El Paso, TX, talks to Daniel (Danny) Alvarado, owner of the PUSH Fitness Center, about the importance of nutrition, diet, and fitness. Stress is the body’s natural response to any physical, mental, and emotional response. Although too much stress can be harmful, getting the right amount of stress is essential for survival. Dr. Alex Jimenez and Daniel Alvarado discuss how stress is the fundamental basis for inspiration and motivation. The PUSH Fitness Center was first created by Danny to help people achieve their optimal health and wellness goals. Hard-work and pushing towards your goal are essential for every individual. Danny discusses how he chooses to inspire and believe in his athletes in order to help them become the best person they can be. Nutrition, diet, and fitness can help prevent a variety of health issues, including metabolic syndrome, diabetes, stroke, and heart disease. Dr. Alex Jimenez, a chiropractor in El Paso, TX, and Daniel (Danny) Alvarado demonstrate how stress, inspiration, and motivation in people can support the hard work and the extra “push” they need to improve themselves, achieve their goals, and improve overall health and wellness. – Podcast Insight
If you have enjoyed this video and/or we have helped you in any way
please feel free to subscribe and share with us.
Thank You & God Bless.
Daniel Alvarado
Dr. Alex Jimenez
Facebook Fitness Center Page: https://www.facebook.com/PUSHftinessathletictraining/
Knee pain chiropractic: Around 40 percent of running injuries are knee injuries. They fall under a general term of runner�s knee. This includes chondromalacia patellae also referred to as patellofemoral pain syndrome (PFMS). Other knee injuries include iliotibial band syndrome and plica syndrome.
Rest and ice are common therapies, but when that doesn�t work or when pain and mobility issues comeback, chiropractic is a tried and true treatment option. Structural issues that affect the knees are often very responsive to chiropractic treatment.
In the case of chondromalacia patellae and other knee problems, it has proven to reduce pain and help improve the condition significantly, providing increased mobility and flexibility.
Anatomy
The knee is constructed to take the impact of the body�s weight when bending and moving. Under the knee is a layer of cartilage that is a natural shock absorber. Injury/s, overuse, aging, and other conditions can cause damage to the cartilage. The condition causes pain and impaired mobility, especially when walking up or downstairs. The pain can be reduced with rest and ice, but sometimes it’s not enough.
Common treatments include:
Chiropractic
Physical therapy
Medications
Surgery
Symptoms
Common symptoms include pain at the front of the knee. It can be described as a dull ache deep in the knee.
This pain can be made worse when:
Sitting with the knee bent for a long time
Squatting
Kneeling
Walking up and downstairs
The more the knee is in use the worse it is. Rest and ice work fairly quickly to help relieve the pain. But if the pain persists even with rest and ice, more aggressive treatment is the next step. Traditional doctors prescribe medication and surgery. But now more individuals are gravitating to a drug-free, less invasive treatment, like chiropractic.
Causes
The exact cause of chondromalacia patellae is still unknown. The condition has been linked to several factors.
Overuse and repetitive stress placed on the joint. This is seen in sports and physical activities that involve jumping and running.
Poor muscle control when the muscles that surround the knee and hip don�t operate properly making the tracking of the kneecap off balance.
Trauma such as a fracture or dislocation.
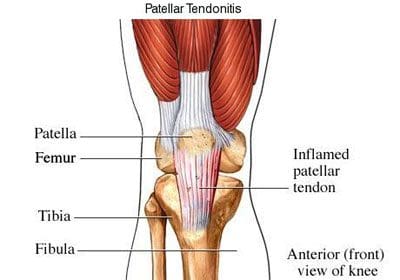
Figure 106. Patellar tendonitis (jumper�s knee).
Risks
A person�s risk of developing chondromalacia patellae can increase based on certain criteria.
Young adults and adolescents can acquire the injury as they’re still growing.
Older individuals with knee pain and possible arthritis are more susceptible to injury.
Gender is a risk factor, as women are twice as likely to develop the condition compared to men. Doctors theorize this is due to the skeletal structure of a woman as the pelvis is wider increasing the angle where the bones of the knee joint meet.
Those that participate in sports that involve a lot of jumping and running have a higher risk. Particularly if the individual increases their level of training.
Chiropractic
Chiropractic treatment for chondromalacia patellae includes nutritional intervention as well as adjustments, stretches and exercises. The treatment is focused on stretching shortened hamstrings and adjusting the sacroiliac joint.
The aim is to improve the tracking of the kneecap and increase motor control. Soft tissue work can help individuals with knee pain. The whole-body approach that chiropractic provides goes beyond relief from knee pain but curing or reducing the condition completely.
The Cost-effectiveness
Why see a chiropractor?
There are plenty of reasons why. From:
General health
Aches
Pains
Injury
Increased movement
Strength
Optimal health
Millions are now turning to chiropractic for natural healing, relief, and whole-body wellness. Some may think the price could hinder their decision to seek chiropractic. Lack of insurance and the number of treatments are two of the common reasons patients think it’s too expensive.
However, individuals need to understand the cost of other treatment options like medications and surgery that end up costing more than dollars with all the negative side-effects. Here are three reasons to visit a chiropractor, and the savings that come with it.
Prevention
Chiropractic promotes optimal health through prevention that is increasingly attracting those striving to remain younger, longer. It promotes whole-body healing through spinal adjustments/joint manipulations to increase mobility and optimize the body’s performance. It decreases blood pressure and reduces the chance of headaches.
Avoiding these health issues saves tens of thousands of dollars in medical bills. Seeing a professional chiropractor enables a person to stay healthy and enjoy a more active lifestyle because their back, bones, and joints are in optimal condition.
Re-Injured
Millions of bodies are injured from a variety of mishaps and accidents.
Sports injuries
Car accidents
Work injuries
Slips
Falls
Our backs, knees, ankles, hips, and feet take a beating. Chiropractic for injury/s is a wise choice as it promotes healing, decreases dependence on medications, and minimizes the chance of a recurrence. It also strengthens the other parts of the surrounding area of the body and not just the injured area. Treating injuries through chiropractic decreases money spent on expensive medicine and reduces time off work.
Chronic
Many types of medical conditions are ongoing, with no cure in sight. Daily pain, loss of strength and mobility are conditions that individuals power through and learn to live with when they don’t want to continually take medication and feel horrible. This is where chiropractic medicine can shine, as it’s all-natural. The aim is to get the body to react the way it is supposed to and heal itself.
An experienced chiropractor can treat these medical conditions by building a customized treatment plan to manage the symptoms with drug-free pain management. Adjustments to the afflicted area, proper anti-inflammation diet, and at-home exercises reduce pain symptoms and increases mobility. Chiropractic is a productive treatment for various injuries and medical conditions, combined with preventative therapy to maintain and prolong wellness.
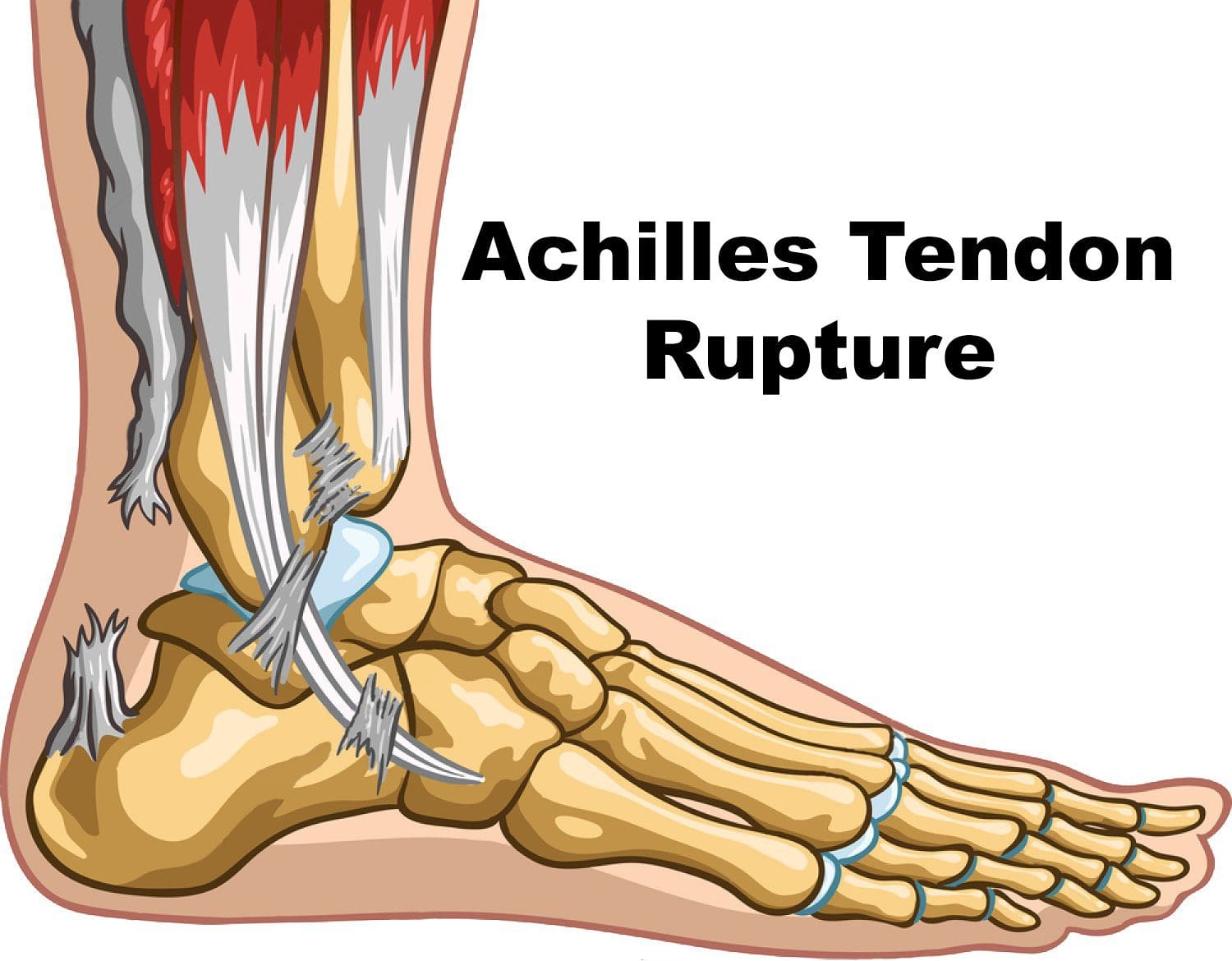
�Achilles injury, which turns out to be a ruptured Achilles tendon.
This is a devasting injury for anyone, especially world-class athletes. Take NBA player Kevin Durant and his injury that could keep him out for some time. To be fair Durant was dealing with a calf injury on the same leg, for some weeks before this injury.
But it was his first game back in action and it led to a crushing injury!
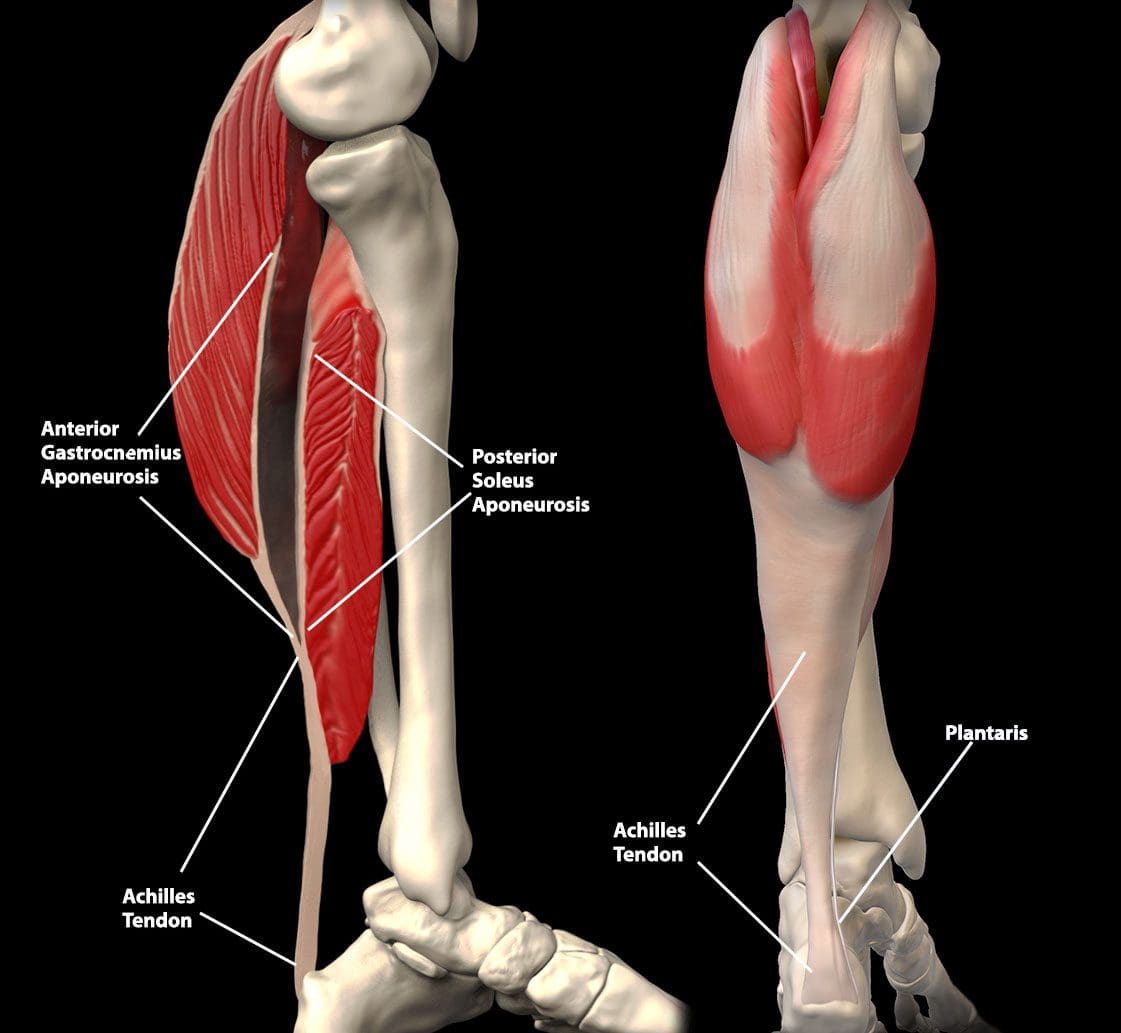
Calf & Achilles Tendon Relationship
The calf and Achilles tendon are so interrelated that when one has an issue so does the other.
The fascia of these muscles segue ways to form the Achilles tendon.
If the calf is tight, then the Achilles is going to be tight.
The relationship between calf injury and an Achilles injury.
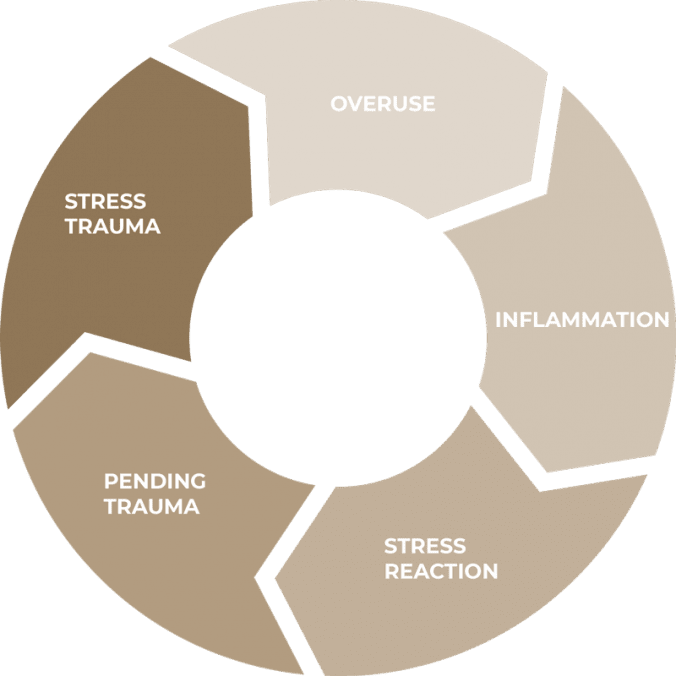
Cycle of Injury
Going through any area of the cycles can lead to a devastating injury.
Symptoms
Pain and stiffness around the lower leg, right above the back of the heel
Begins as a mild ache and worsens throughout the day
Jumping,� running, stair climbing, and sprinting can spark intense pain
Tenderness or stiffness especially in the morning, but improves with movement/activity
The key is to intervene to stop the cycle.
A few ways:
Rest
Massage
Physical Therapy
Chiropractic
Custom orthotics
Active Release Therapy (ART)
ART is extremely�effective�for breaking up scar tissue and improving issues with soft tissues. Treatment can do a lot to improve the health of your tendon and the surrounding tissues to avoid further complications. It will also do a lot to help relieve the pain you are experiencing.
Chiropractic Adjustments/Manual Manipulations
Many times, the issues with your Achilles tendon are the result of misalignment in other parts of your body. When your joints are misaligned it tends to put extra stress on your feet and Achilles tendons. To minimize the stress on your joints, your chiropractor will adjust your spine and other joints to ensure proper alignment.
Get Help for Your Achilles Injury & Call Us Today!
If you are experiencing heel pain, please get in touch with our chiropractic team. We can help to alleviate your pain and help you avoid experiencing further problems with your Achilles tendon.
Difference Foot Orthotics Make to *REDUCE FOOT PAIN* & Correct Posture | El Paso, TX (2019)
Custom made foot orthotics can help control foot motion and posture. Healthcare professionals prescribe custom foot orthotics to help patients focus on their foot posture and mobility control. Research studies have ascertained that using custom foot orthotics for posture and mobility control can help fix excessive foot pronation and supination to prevent a variety of foot health problems. The subsequent video describes how custom foot orthotics will help control foot posture and mobility to improve health and wellness.
What’s Afoot
If you have low back pain�or have had it, you are not alone. Experts estimate that around�80% of people�will experience some type of back problem at some point in their lives.�The Global Burden of Disease 2010�lists low back pain as the number one cause of disability worldwide. The good news is the majority of back pain is mechanical in origin or is not organic. This means that infection, cancer, fracture, inflammatory arthritis, and other serious conditions are not the cause. In fact, you may benefit by looking to your feet, knees,�and hips as the culprits.
NCBI Resources:
The large, thick tendon that travels up from the base of the heel and into the calf muscle is the Achilles tendon. It connects the calf muscle and heel. It allows you to walk, run and jump. The Achilles tendon is strong and durable, but it is possible to overwork it and cause enough overuse injury.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine