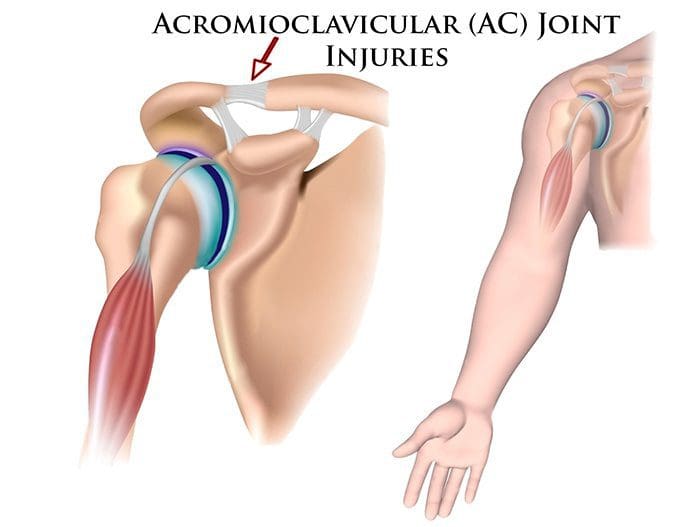
Shoulder pain along with the kinds of shoulder problems like sprains and strains that chiropractors regularly treat often involves a form of rotator dysfunction. The shoulder has the greatest mobility of any joint in the body. However, there is little stability when in certain positions the soft tissues in the shoulder area can get injured through sports injury/s, recreational activities, at work or in a fall.�
This usually begins with dysfunction of the rotator cuff muscles and progresses to:
In cases like this, there is no direct, acute injury.
Every sprain and strain injury to the shoulder must be treated and rehabilitated�properly�to avoid future injuries and pain. There is a higher probability of shoulder instability that becomes chronic after an injury. This is because the surrounding muscles and connective tissues are what create shoulder joint stability.
Shoulder Pain
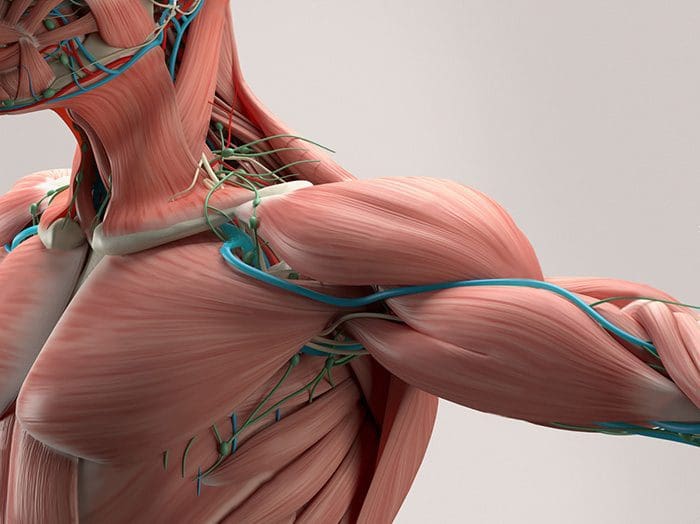
The shoulder goes through a great deal that we do not realize. It is made up of an intricate network of ligaments and muscles, with the rotator cuff taking most of the load/weight during movement and exertion. As aforementioned, the shoulder is the most flexible joint in the human body, but it is one of the most unstable. For athletes, shoulder injuries are pretty common, as the shoulder sustains more injuries than almost any other part of the body.
The shoulder is unstable because of its unique construction. Other joints like the ankle or elbow are limited in their range of motion. The shoulder, on the other hand, can move pretty widely, which leaves it open to stress, injury, and pain. The soft tissues in the shoulder, muscles, tendons, and ligaments can get injured from overuse, excessive strain, falls, and improper motion.
Treating shoulder pain can be a challenge because it is used so much daily. A Chiropractor can bring relief to shoulder pain and speed up the healing process.
Injury and pain causes
Shoulder pain can be caused by a variety of conditions. Injury is one of the most common causes and is seen in athletes, like swimmers, gymnasts, golfers, baseball players, bowlers, and tennis players, etc, who use their arms and shoulders regularly, place added stress on the joint.
Jobs that involve repetitive shoulder movements can also cause injury. People whose job requires repetitive motions or strenuous upper bodywork are at higher risk. Truck drivers, construction workers, warehouse and grocery store employees commonly experience shoulder injury and pain.
Prevention
Preventing shoulder pain and injury can be a simple process. Workers and athletes whose jobs require repetitive arm work or rotation should warm-up, and take stretching and shake out the hand/s and arm/s breaks. Pain should be addressed, as soon as it presents with ice/heat and a possible chiropractic appointment. Ignoring the pain could lead to a more serious/chronic condition.
Shoulder rest is always a must. The joint needs time off to heal and regular chores should not be resumed until the doctor or chiropractor clears the patient. Chiropractors usually recommend exercises and stretches geared toward the type of injury/s or condition/s.
Chiropractor
Chiropractic is highly beneficial for shoulder injury/s and shoulder pain.
It will:
Reduce pain
Relieve pain
Improve range of motion
Increase flexibility
Restore function to the joint
Different techniques are used depending on the type of injury or condition. The patient will be assessed by the chiropractor and will determine a treatment plan. Compression techniques have been found to be very effective for shoulder pain. It is favored because it is not strenuous for the doctor, is very safe, and is handled well by the patient. Chiropractic is the treatment of choice for shoulder pain because it is minimally invasive and it works.
Chiropractic addresses the entire body with its aim to relieve pain without drugs or surgery and keep the individual healthy and functioning at an optimal level. Are you, a family member, or friend suffering from shoulder stiffness/pain? If so, give us a call. Dr. Jimenez and his outstanding physical therapy team are here to help!
In the following podcast video article, Dr. Alex Jimenez, a chiropractor in El Paso, TX, and Daniel (Danny) Alvarado, owner of PUSH Fitness Center in El Paso, TX, discuss the three points of weight loss. Excess weight and obesity are associated with metabolic syndrome and a variety of other health issues. Metabolic syndrome is a cluster of risk factors that can ultimately increase the risk of developing diabetes, stroke, and diabetes, among other complications. Dr. Alex Jimenez and Daniel Alvarado discuss how weight loss can be a safe and effective way to improve metabolic syndrome as well as overall health and wellness. Decreasing or eliminating sugar and carbohydrate consumption, increasing the consumption of proteins, �good� fats, and vegetables, as well as engaging and participating in exercise and physical activity can ultimately help promote weight loss to improve metabolic syndrome and a variety of other health issues. Furthermore, Dr. Alex Jimenez and Daniel Alvarado discuss how they can help people with excess weight and obesity achieve their weight loss goals by encouraging and motivating them through every step of the way. Weight loss is essential for people with metabolic syndrome to achieve overall health and wellness. � Podcast Insight
If you have enjoyed this video and/or we have helped you in any way
please feel free to subscribe and share us.
Thank You & God Bless.
Daniel Alvarado & Dr. Alex Jimenez
Subscribe: http://bit.ly/drjyt
Facebook Fitness Center Page: https://www.facebook.com/PUSHftinessathletictraining/
Yelp: El Paso Rehabilitation Center: http://goo.gl/pwY2n2
Yelp: El Paso Clinical Center: Treatment: https://goo.gl/r2QPuZ
Metabolic syndrome is a cluster of risk factors that can ultimately increase the risk of developing a variety of health issues, including heart disease, stroke, and diabetes, among other problems. Central obesity, high blood pressure, high blood sugar, high triglycerides, and low HDL or good cholesterol levels are the 5 risk factors associated with metabolic syndrome. Having at least three of the five risk factors may suggest the presence of metabolic syndrome. Dr. Alex Jimenez, Alexander Jimenez, Truide Torres, Kenna Vaughn, and Astrid Ornelas explain the 5 risk factors associated with metabolic syndrome, in further detail, as they recommend diet and lifestyle modification advice and guidelines, such as the ketogenic diet or the keto diet, as well as demonstrate the biochemical and chemical pathways that the body goes through during ketosis to help people with metabolic syndrome improve their overall health and wellness. From eating good fats and staying hydrated to exercise and better sleep, Dr. Alex Jimenez, Alexander Jimenez, Truide Torres, Kenna Vaughn, and Astrid Ornelas discuss how diet and lifestyle modifications, such as the ketogenic diet or keto diet, can help improve the 5 risk factors associated with metabolic syndrome to prevent the risk of developing a variety of other health issues, including heart disease, stroke, and diabetes. � Podcast Insight
If you have enjoyed this video and/or we have helped you in any way
please feel free to subscribe and share us.
Thank You & God Bless.
Dr. Alex Jimenez RN, DC, MSACP, CCST
Everybody has a backstory. It is not easy. We got to PUSH Hard. It is not EASY…Dr. Alex Jimenez, a chiropractor in El Paso, TX, talks to Daniel (Danny) Alvarado, owner of the PUSH Fitness Center, about the importance of nutrition, diet, and fitness. Stress is the body’s natural response to any physical, mental, and emotional response. Although too much stress can be harmful, getting the right amount of stress is essential for survival. Dr. Alex Jimenez and Daniel Alvarado discuss how stress is the fundamental basis for inspiration and motivation. The PUSH Fitness Center was first created by Danny to help people achieve their optimal health and wellness goals. Hard-work and pushing towards your goal are essential for every individual. Danny discusses how he chooses to inspire and believe in his athletes in order to help them become the best person they can be. Nutrition, diet, and fitness can help prevent a variety of health issues, including metabolic syndrome, diabetes, stroke, and heart disease. Dr. Alex Jimenez, a chiropractor in El Paso, TX, and Daniel (Danny) Alvarado demonstrate how stress, inspiration, and motivation in people can support the hard work and the extra “push” they need to improve themselves, achieve their goals, and improve overall health and wellness. – Podcast Insight
If you have enjoyed this video and/or we have helped you in any way
please feel free to subscribe and share with us.
Thank You & God Bless.
Daniel Alvarado
Dr. Alex Jimenez
Facebook Fitness Center Page: https://www.facebook.com/PUSHftinessathletictraining/
Metabolic syndrome is a collection of risk factors that can ultimately increase the risk of developing a variety of health issues, including heart disease, stroke, and diabetes, among other problems. Central obesity, high blood pressure, high blood sugar, high triglycerides, and low HDL are the 5 risk factors associated with metabolic syndrome. Having at least three of the five risk factors may suggest the presence of metabolic syndrome. Dr. Alex Jimenez and Dr. Mario Ruja explain the 5 risk factors associated with metabolic syndrome, in further detail, as they recommend diet and lifestyle modification advice and guidelines to help people with metabolic syndrome improve their overall health and wellness. From eating fiber and staying hydrated to exercise and better sleep, Dr. Alex Jimenez and Dr. Mario Ruja discuss how diet and lifestyle modifications can help improve the 5 risk factors associated with metabolic syndrome to ultimately prevent the risk of developing a variety of other health issues, including heart disease, stroke, and diabetes. � Podcast Insight
If you have enjoyed this video and/or we have helped you in any way
please feel free to subscribe and share us.
Thank You & God Bless.
Dr. Alex Jimenez RN, DC, MSACP, CCST
In the following podcast video article, Dr. Alex Jimenez, a chiropractor in El Paso, TX, and Dr. Mario Ruja, another chiropractor in El Paso, TX, discuss chiropractic care and why it works. Chiropractic care is a safe and effective, alternative treatment option that focuses on the diagnosis, treatment, and prevention, of injuries and underlying conditions associated with the musculoskeletal and nervous system. Chiropractic care is a healthcare profession that has existed for many years throughout many civilizations and it focuses on the use of spinal adjustments and manual manipulations to carefully restore the original alignment of the spine and the human body as a whole. Dr. Alex Jimenez and Dr. Mario Ruja describe how they were first interested in becoming chiropractors, or doctors of chiropractic, as they also describe how they feel when they are able to provide pain relief to their patients. Dr. Jimenez and Dr. Ruja will focus on discussing why chiropractic care works and how it is different from other healthcare professions in the way it helps treat a variety of health issues associated with the spine, from neck pain to low back pain and sciatica. Chiropractic care can help promote overall health and wellness. � Podcast Insight
If you have enjoyed this video and/or we have helped you in any way
please feel free to subscribe and share us.
Thank You & God Bless.
Dr. Alex Jimenez RN, DC, MSACP, CCST
Dr. Alex Jimenez and Dr. Mario Ruja discuss basal metabolic rate, BMI, and BIA. Body mass and body fat can be measured in a variety of ways, however, several measurement tools may ultimately be inaccurate for many athletes. According to Dr. Alex Jimenez and Dr. Mario Ruja, calculating an individual�s body mass and body fat utilizing various tools is essential to determine overall health and wellness. BMI uses a person�s height divided by twice their weight. The results may be inaccurate for athletes because their body mass and body fat is different, in terms of weight, compared to the average person. Dr. Alex Jimenez and Dr. Mario Ruja demonstrate that BIA, or bioelectrical impedance analysis, and various other tools, such as the DEXA test, the Tanita scale, and the InBody, among others, can help more accurately determine an athlete�s body mass and body fat. Basal metabolic rate, BMI, and BIA is essential for parents that have young athletes as well as for the general population. Healthcare professionals that have these tools available can ultimately help provide individuals with the results they may need to maintain overall health and wellness. – Podcast Insight
If you have enjoyed this video and/or we have helped you in any way
please feel free to subscribe and share us.
Thank You & God Bless.
Dr. Alex Jimenez RN, DC, MSACP, CCST
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine