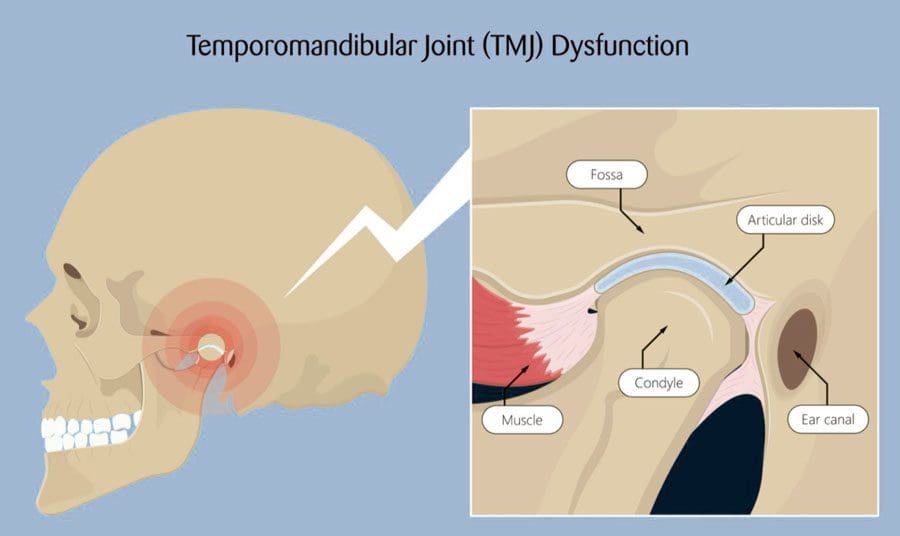
The temporomandibular (tem-puh-roe-man-dib-u-lur) joint TMJ acts as a sliding hinge that connects the jawbone to the skull. There is one joint on each side of the jaw. TMJ jaw disorders are also known as temporomandibular disorders – TMD. These disorders affect the connecting point between the jaw and the skull that causes swelling and pain in the joint and the muscles that control movement. The disorder can be caused by a combination of factors, like stress, genetics, arthritis, or injury. The symptoms, pain, and discomfort are often temporary and can be relieved with self-care and nonsurgical treatment like chiropractic.
Jaw Disorders
If the jaw is not moving correctly or becomes imbalanced, it can stress the temporomandibular joint. If this happens, the jaw muscles and the neck and shoulder muscles can tense up and over time become fatigued as they overwork to compensate and keep the jaw balanced. The bones that interact in the joint are covered with cartilage and are separated by a small shock-absorbing disc to maintain smooth movement. Jaw disorders can happen if:
The disc erodes or moves out of alignment.
The joint’s cartilage is damaged by arthritis.
The joint is damaged by impact trauma like hitting the head from a fall or sports accident.
Individuals that have been in an automobile accident.
Other factors include:
Tension or stress can cause individuals to grind or clench their teeth, known as bruxism.
Symptoms of TMJ vary from case to case. These symptoms might include:
Problems with opening or closing the mouth
Difficulty or pain while chewing
Pain or tenderness of the jaw
Pain in one or both of the temporomandibular joints
Aching facial pain
Neck and shoulder pain
Headaches
Aching pain in and around the ear
Dizziness
Locking of the joint
Clicking sound
Grating sensation
Chiropractic Relief
Chiropractors can help with TMJ by alleviating tension and dysfunction in the shoulder, neck, and jaw. Once the dysfunction is relieved, it reduces the pressure on various nerves. Treatment includes:
Manipulation of the jaw joint so it can move easily
Not all carbs are equal, with some having a more significant effect on insulin levels than others. For individuals with diabetes or insulin resistance, this is important. A food’s Glycemic Index – ranging from 0 to 100 – indicates how a particular carbohydrate will affect blood sugar and insulin levels.
Foods that digest quickly are high on the index.
Foods that digest slowly are lower on the index.
Foods high on the GI scale, include potatoes and white bread, are quickly broken down. This is what happens when going through a sugar rush that comes crashing down minutes later. Foods low on the GI scale, include sweet potatoes and whole oats, are digested gradually. This results in a steady rise in blood sugar levels. The following factors may influence the GI scale:
Food processing
The more processed the food, the higher the GI.
Fat and acid content
Foods high in fat, acid, or carbs eaten with fat or acid tend to have a lower GI.
Fiber content
Fiber slows down the rate of digestion, leading to a gradual, healthy rise in blood sugar levels.
Ripeness
Ripened fruits tend to have a higher GI than unripened fruit.
References
Alcantara, Joel et al. “Chiropractic care of a patient with temporomandibular disorder and atlas subluxation.” Journal of manipulative and physiological therapeutics vol. 25,1 (2002): 63-70. doi:10.1067/mmt.2002.120415
DeVocht, James W et al. “A pilot study of a chiropractic intervention for management of chronic myofascial temporomandibular disorder.” Journal of the American Dental Association (1939) vol. 144,10 (2013): 1154-63. doi:10.14219/jada.archive.2013.0034
Pavia, Steven et al. “Chiropractic Treatment of Temporomandibular Dysfunction: A Retrospective Case Series.” Journal of chiropractic medicine vol. 14,4 (2015): 279-84. doi:10.1016/j.jcm.2015.08.005
Rubis, Lisa M et al. “A collaborative approach between chiropractic and dentistry to address temporomandibular dysfunction: a case report.” Journal of chiropractic medicine vol. 13,1 (2014): 55-61. doi:10.1016/j.jcm.2013.10.003
The thoracic spine, also known as the upper or middle back, is designed for stability to anchor the rib cage and protect the organs in the chest. It is highly resistant to injury and pain. However, when thoracic back pain does present, it is usually from long-term posture problems or an injury. Thoracic back pain is less common than lower back and neck pain, but it does affect up to 20% of the population, particularly women. Treatment options include chiropractic for quick and long-term pain relief.
Thoracic Back Pain and Soreness
The thoracic area is vital for various functions related to:
Upper back pain usually feels like a sharp, burning pain localized to one spot or a general achiness that can flare up and spread out to the shoulder, neck, and arms.
Types of Upper Back Pain
These include:
Myofascial pain
Spine degeneration
Joint dysfunction
Nerve dysfunction
General spinal misalignments
Depending on what specific tissues are affected, pain can occur with breathing or arm use. It is recommended to have a healthcare professional perform an examination and get an accurate diagnosis. A chiropractor understands the delicate balance and functions that the thoracic spine provides and can develop a proper treatment plan.
Chiropractic
Treatment options will depend on the symptoms, underlying dysfunctions, and individual preferences. Recommendations for treatment often include:
Spine adjustments to improve alignment and nerve integrity.
Posture training to maintain spinal alignment.
Therapeutic massage.
Exercise training to restore muscular balance.
Non-invasive pain-relieving techniques.
Health coaching.
Body Composition
Plant-Based Diets for Weight Loss
Individuals who follow vegan, vegetarian, and semivegetarian diets have reported and shown they are less likely to be overweight or obese. This can indicate that reducing intake of meat and animal products is beneficial for weight loss. Studies have found that individuals who follow a vegan diet may lose more weight than individuals on a more conventional weight loss diet, even with similar calories consumed, and often have significant improvements in blood sugar and inflammation markers.
Plant-Based Protein and Muscle Gain
Some plant-based proteins are just as effective as animal protein at promoting muscle gain. A study found that supplementing rice protein following resistance training had similar benefits to whey protein supplementation. Both groups had:
Briggs AM, Smith AJ, Straker LM, Bragge P. Thoracic spine pain in the general population: prevalence, incidence and associated factors in children, adolescents and adults. A systematic review. BMC Musculoskelet Disord. 2009;10:77.
Cichoń, Dorota et al. “Efficacy of Physiotherapy in Reducing Back Pain and Improve Joint Mobility in Older Women.” Ortopedia, traumatologia, rehabilitacja vol. 21,1 (2019): 45-55. doi:10.5604/01.3001.0013.1115
Fouquet N, Bodin J, Descatha A, et al. Prevalence of thoracic spine pain in a surveillance network. Occup Med (Lond). 2015;65(2):122-5.
Jäger, Ralf et al. “Comparison of rice and whey protein isolate digestion rate and amino acid absorption.” Journal of the International Society of Sports Nutrition vol. 10,Suppl 1 P12. 6 Dec. 2013, doi:10.1186/1550-2783-10-S1-P12
Joy, Jordan M et al. “The effects of 8 weeks of whey or rice protein supplementation on body composition and exercise performance.” Nutrition journal vol. 12 86. 20 Jun. 2013, doi:10.1186/1475-2891-12-86
Medawar, Evelyn et al. “The effects of plant-based diets on the body and the brain: a systematic review.” Translational psychiatry vol. 9,1 226. 12 Sep. 2019, doi:10.1038/s41398-019-0552-0
Newby, PK et al. “Risk of overweight and obesity among semivegetarian, lactovegetarian, and vegan women.” The American journal of clinical nutrition vol. 81,6 (2005): 1267-74. doi:10.1093/ajcn/81.6.1267
Pope, Malcolm H et al. “Spine ergonomics.” Annual review of biomedical engineering vol. 4 (2002): 49-68. doi:10.1146/annurev.bioeng.4.092101.122107
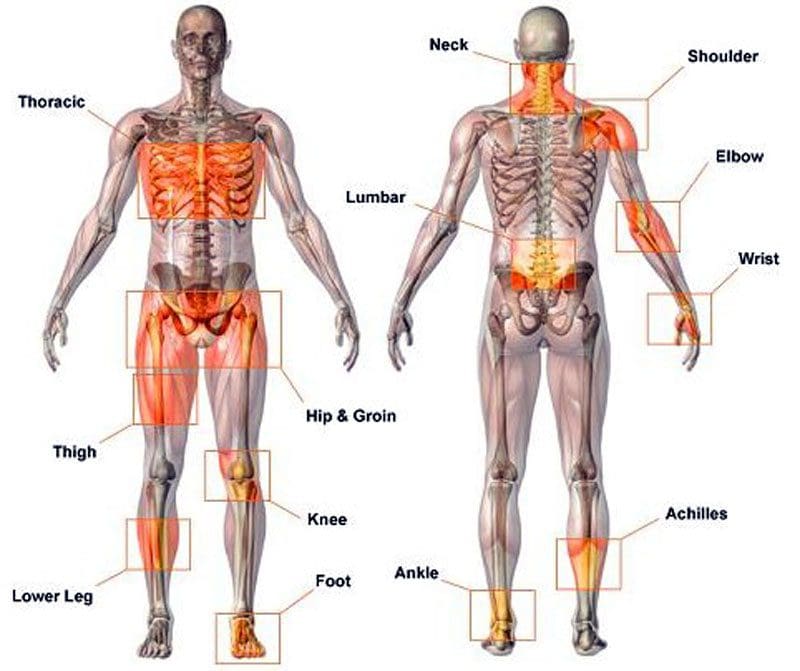
Musculoskeletal Disorders, or MSDs, are injuries, conditions, and disorders that affect the body’s musculoskeletal system. It includes the muscles, tendons, ligaments, nerves, discs, blood vessels, bones, and joints. MSDs are common, and the risk of developing them increases with age. The severity of an MSD can vary. They cause discomfort, recurrent pain, stiffness, swelling, and aching that interfere with everyday activities. Early diagnosis and treatment can alleviate symptoms and improve long-term health. Common disorders include:
The term musculoskeletal disorder is used as it accurately describes the injury or condition. Other terms used are repetitive motion injury, repetitive stress injury, and overuse injury. When individuals are exposed to MSD risk factors, they begin to fatigue. This can start a musculoskeletal imbalance. With time, fatigue completely overtakes recovery/healing, and the musculoskeletal imbalance continues, a musculoskeletal disorder develops. The risk factors are broken into two categories: work-related/ergonomic risk factors and individual-related risk factors.
Ergonomic Factors:
Force
Repetition
Posture
High Task Repetition
Many work tasks and cycles are repetitive and are typically controlled by hourly or daily production targets and work processes.
High task repetition combined with other risks factors like high force and/or awkward postures can contribute to the formation of MSD.
A job is considered highly repetitive if the cycle time is 30 seconds or less.
Forceful Exertions
Many job tasks require high force loads on the body.
Muscle effort increases in response to high force requirements. This increases associated fatigue.
Repetitive or Sustained Awkward Postures
Awkward postures place excessive force on joints, overload the muscles and tendons around affected joints.
The joints of the body are most efficient when they operate close to the mid-range motion of the joint.
The risk of MSD is increased when the joints are worked outside of this mid-range repetitively for sustained periods without a proper amount of recovery time.
Individual Factors
Unhealthy work practices
Lack of physical activity/fitness
Unhealthy habits
Poor diet
Unhealthy Work Practices
Individuals that engage in poor work practices, body mechanics, and lifting techniques are introducing unnecessary risk factors.
These poor practices create unnecessary stress on the body that increases fatigue and decreases the body’s ability to recover properly.
Poor Health Habits
Individuals who smoke, drink excessively, are obese, or exhibit numerous other poor health habits put themselves at risk for musculoskeletal disorders and other chronic diseases.
Insufficient Rest and Recovery
Individuals that do not get adequate rest and recovery put themselves at higher risk.
MSDs develop when fatigue outruns the individual’s recovery system, causing a musculoskeletal imbalance.
Poor Diet, Fitness, and Hydration
Individuals who eat unhealthily are dehydrated, at a poor level of physical fitness, and do not take care of their bodies are putting themselves at a higher risk of developing musculoskeletal and chronic health problems.
Causes
The causes of musculoskeletal disorders are varied. Muscle tissue can be damaged with the wear and tear of daily work, school, and physical activities. Trauma to the body can come from:
Postural strain
Repetitive movements
Overuse
Prolonged immobilization
Jerking movements
Sprains
Dislocations
Falling injuries
Auto accident injuries
Fractures
Direct trauma to the muscle/s
Poor body mechanics can cause spinal alignment problems and muscle shortening, causing other muscles to be strained, causing problems and pain.
Treatment Rehabilitation
A doctor will recommend a treatment plan based on the diagnosis and severity of the symptoms. They may recommend moderate exercise and over-the-counter medications like ibuprofen or acetaminophen to address occasional discomfort or pain. They often recommend chiropractic and physical therapy rehabilitation to learn how to manage pain and discomfort, maintain strength, range of motion, and adjust everyday activities. Different types of manual therapy, or mobilization, can treat body alignment problems. A doctor may prescribe medications like nonsteroidal anti-inflammatories NSAIDs to reduce inflammation and pain for more severe symptoms. For individuals with musculoskeletal disorders like fibromyalgia, medications to increase the body’s level of serotonin and norepinephrine may be prescribed in low doses to modulate sleep, pain, and immune system function.
Body Composition
Types of Pain
Pain can be grouped into three categories:
Early Warning Pain
This is most recognizable after having just touched a pan, and the hand jerks away before realizing how hot the pan is, also known as the withdrawal reflex.
This is a protective mechanism that helps avoid danger and is vital for survival.
Inflammatory Pain
This type of pain happens after an injury or surgery while the body is healing and recovering.
Inflammation prevents the body from performing movements to prevent and avoid re-injury.
Pathological Pain
This type of pain can happen after the body has healed, but the nervous system has been damaged.
This is often the case with individuals who sustain an injury and inform doctors that the injured area is never the same.
If the rehabilitation does not correctly heal the nervous system, protective pain measures can generate a false alarm causing pain signals to fire off.
References
Asada, Fuminari, and Kenichiro Takano. Nihon eiseigaku zasshi. Japanese journal of hygiene vol. 71,2 (2016): 111-8. doi:10.1265/jjh.71.111
da Costa, Bruno R, and Edgar Ramos Vieira. “Risk factors for work-related musculoskeletal disorders: A systematic review of recent longitudinal studies.” American journal of industrial medicine vol. 53,3 (2010): 285-323. doi:10.1002/ajim.20750
Malińska, Marzena. “Dolegliwości układu mięśniowo-szkieletowego u operatorów komputerowych” [Musculoskeletal disorders among computer operators]. Medycyna pracy vol. 70,4 (2019): 511-521. doi:10.13075/mp.5893.00810
Musculoskeletal system diseases. (n.d.). dmu.edu/medterms/musculoskeletal-system/musculoskeletal-system-diseases/
Roquelaure, Yves et al. “Troubles musculo-squelettiques liés au travail” [Work-related musculoskeletal disorders]. La Revue du praticien vol. 68,1 (2018): 84-90.
Villa-Forte A. (n.d.). Diagnosis of musculoskeletal disorders. merckmanuals.com/home/bone,-joint,-and-muscle-disorders/diagnosis-of-musculoskeletal-disorders/introduction
Muscle spasms also referred to as muscle cramps, are painful contractions and tightening of the muscles. They are common, involuntary, and unpredictable. Temperature drops and cold weather can cause the muscles and joints to contract and tighten, leading to spasms and pain. Chiropractic, physical therapy massage, exercises, stretching, and an anti-inflammatory diet can bring relief and help strengthen the muscles to prevent future episodes.
Muscle Spasms
Spasms are common and can affect any of the muscles. They can involve part of a muscle, all of a muscle, or several muscles in a group. Spasms occur when the muscle/s involuntary and forcibly contract uncontrollably and are unable to relax. The most common sites for muscle spasms include:
As the weather gets colder, this causes the muscles in the body to lose heat, causing them to contract. As a result, the muscles and joints become tighter, stiffer, and decrease mobility and range of motion. This forces the muscles to work harder than usual to compensate. This can increase the fatigue of the muscles, leading to more prolonged bouts of pain and discomfort after physical activity, movement, exercise, etc.
Symptoms and Causes
A cramp can last a few seconds or last up to 15 minutes. During a muscle spasm, the following may be experienced:
Twitching in the muscle.
Pain in the muscle.
Throbbing.
Hardness and/or stiffness.
The muscles appear physically distorted.
Because the muscles have to work harder, the cold weather can increase muscle spasms. One of the most common causes of muscle spasms is overuse and fatigue. However, exact causes vary from person to person. Some experts believe that one or more of the following contribute to the spasms/cramps, and they include:
Dehydration.
Stress.
Not stretching the body regularly.
Muscle fatigue.
Restricted blood circulation.
Involuntary nerve discharge/s.
Over-exercising.
Exercising in the heat.
Exhaustion of salts and minerals:
Potassium
Magnesium
Calcium
Possible causes for leg cramps at night or nocturnal leg cramps specifically include:
Sitting for too long without moving around to keep circulation healthy.
Sitting with unhealthy posture.
Overusing the muscles.
Standing or working on hard floors.
Dealing With The Cold
One way to deal with the cold is to warm up before any physical activity. Taking a few minutes to get the heart rate up can increase the blood flow and flexibility of the muscles. This will ensure the muscles are functioning correctly and avoid the need to work harder to stop spasms. When a cramp strikes, there are a few steps to try to alleviate the spasm:
Stretching the affected area.
Massaging the affected area manually with a massage roller, percussive massager.
Stand up.
Move around.
Apply heat or ice.
A warm bath, shower with massage setting if possible.
American Academy of Orthopaedic Surgeons. Muscle Cramp. (http://orthoinfo.aaos.org/topic.cfm?topic=A00200) Accessed 3/1/2021.
American Association of Osteopathy. Muscle Cramp—A Common Pain. (http://www.osteopathic.org/osteopathic-health/about-your-health/health-conditions-library/general-health/Pages/muscle-cramp.aspx) Accessed 3/1/2021.
Herzberg J. Stevermer J. Treatments for Nocturnal Leg Cramps. (https://www.aafp.org/afp/2017/1001/od3.pdf) Am Fam Physician 2017;96(7):468-469. Accessed 3/1/2021.
Young G. Leg Cramps. (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4429847/) BMJ Clin Evid 2015; May 13;1113. Accessed 3/1/2021.
A common symptom of sciatica is radiating/spreading pain running down the leg. However, the leg pain could be something to do with the blood vessels. If the pain travels from the low back to the hip, through the buttocks, down the leg, and into the foot, then more than likely it is sciatica. However, sciatica is just one condition that causes leg pain; other causes of leg pain include:
Bone spurs
Herniated disc
Arthritis
All can irritate the sciatic nerve causing sciatica.
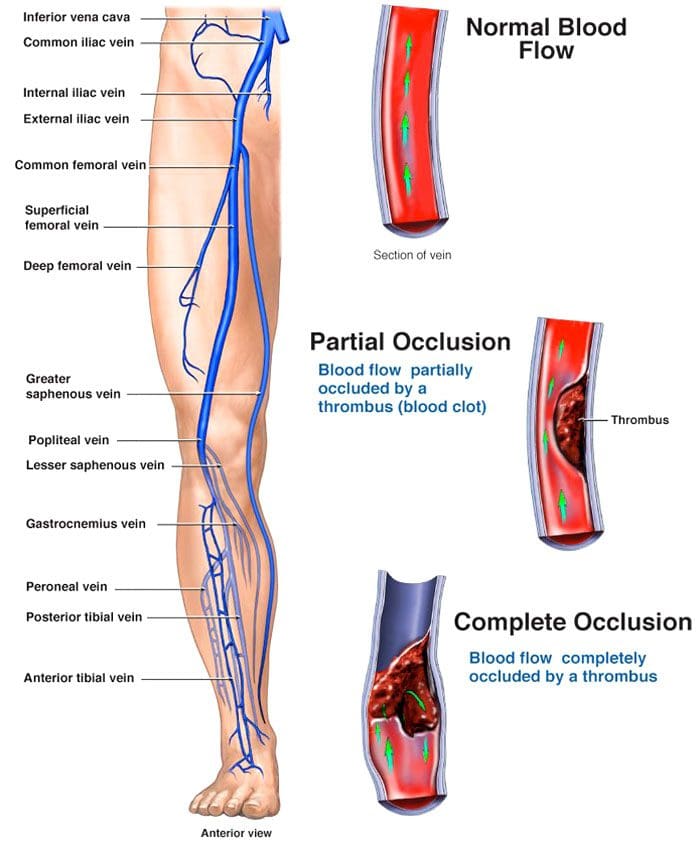
The vascular system, also called the circulatory system, comprises the vessels that circulate blood and lymph throughout the body. Problems with the vascular system are a less common cause of leg pain but can be severe. Therefore, it is vital to learn to tell the difference.
Deep Vein Thrombosis
Deep vein thrombosis – DVT happens when a blood clot forms in a deep vein in the body and not the superficial veins just under the skin. The legs’ deep veins are susceptible to clotting. The formation of a clot can happen:
After surgery
From an accident
When recovering, bed resting and not moving.
When the body is in the same position for a long time with little to no movement, like a long plane ride.
On long plane rides, try to get up and walk around every hour. If unable to walk, do three sets of 20 reps of heel-to-toe exercises every hour.
Deep vein thrombosis can cause leg pain or swelling but can also present without causing any symptoms. Other risk factors include:
Blunt or penetrating injury to the blood vessel and/or its walls.
Pain running down the leg from a blood clot feels like:
Tightness
Cramping soreness
Throbbing
Possible warmth
Swelling.
Blood clots and sciatica are reported to feel relatively different. The pain from a blood clot does not spread out and does not extend from or to the back. Sciatica does not cause swelling, redness, and warmth. If a doctor suspects a blood clot is causing the pain, they will order an ultrasound to confirm the diagnosis. If it is deep vein thrombosis, blood thinners could be recommended for three to six months.
A doctor may recommend aspirin, which can help in the prevention of blood clots.
In some cases, the clot may have to be surgically removed.
Vascular Conditions and Pain Running Down The Leg
Other blood vessel conditions that can cause individuals to believe they have sciatica include:
Peripheral artery disease – PAD
This often presents in individuals with diabetes or who smoke. It causes pain in the calf area but does not radiate throughout the leg. The pain usually presents with physical effort movement. If the pain occurs when at rest, this could be a serious medical emergency. Peripheral artery disease is a chronic condition that can worsen if lifestyle changes are not made to reduce risk factors.
Acute limb ischemia
This condition can cause leg pain, but not the same as sciatica. What happens is the leg is not receiving blood, causing:
Intense pain in the extremity
Change in the color of the skin
Numbness
Weakness
Loss of a pulse
This vascular condition is a medical emergency and requires immediate treatment.
Acute compartment syndrome
This can happen after some kind of trauma to the leg.
The pain is acute, with the leg swelling up and a building up of tight pressure.
It usually affects the lower part of the leg.
This condition can also cause:
Numbness
Tingling
Visible swelling
Bruising
It is considered a medical emergency and needs to be treated quickly to avoid complications.
Varicose veins
Varicose veins can cause some pain running down the leg and/or aching, but the discomfort is not as intense. Treatment has come a long way, is less invasive, and includes:
Compression stockings, including prescription socks/stockings
Laser treatments
Minimally invasive procedures
Not staying on the feet too much
Elevating the legs
Maintaining an ideal weight can help
Vascular Disorder Prevention
Healthy lifestyle habits are recommended to keep the vascular system operating correctly. This includes:
If it is sciatica, fortunately, most cases go away on their own, but if treatment is needed, it is recommended to start with conservative treatments such as:
Chiropractic
Physical therapy
Anti-inflammatory medication
Muscle relaxants
Corticosteroid injections
In severe cases, surgery like a microdiscectomy or laminectomy will be performed to relieve pressure on the sciatic nerve.
Body Composition
Why might blood pressure be different when measuring on each arm?
The heart sits just to the left of the midline in the chest cavity. The aorta is the largest blood vessel in the body. It leaves through the left side of the heart and transports blood to a network of blood vessels that branch out, supplying the body with oxygen and nutrients. The arteries that branch off the aorta and go to the left and right sides of the body are different.
On the right, the brachiocephalic trunk comes off the aorta and splits into the right common carotid artery and right subclavian artery. The left common carotid and left subclavian arteries branch directly off the aorta. The differences mean that the risk for arterial thrombosis is not the same for the right and left subclavian arteries. Arterial thrombosis causes the blood vessels to become stiff, causing obstruction over time and is more likely to happen in the left subclavian than in the right. The difference in arterial branching affects blood pressure measurements on the left and right arms. The blood vessels are surrounded by:
Muscle
Fat
Connective tissue
When muscles place pressure on the blood vessels around the heart, it can cause short-term turbulence changes that can affect blood pressure.
References
American Heart Association. Atherosclerosis and cholesterol. https://www.heart.org/en/health-topics/cholesterol/about-cholesterol/atherosclerosis
American Heart Association. What is excessive blood clotting (Hypercoagulation?) https://www.heart.org/en/health-topics/venous-thromboembolism/what-is-excessive-blood-clotting-hypercoagulation
Centers for Disease Control and Prevention. What is venous thromboembolism? https://www.cdc.gov/ncbddd/dvt/facts.html
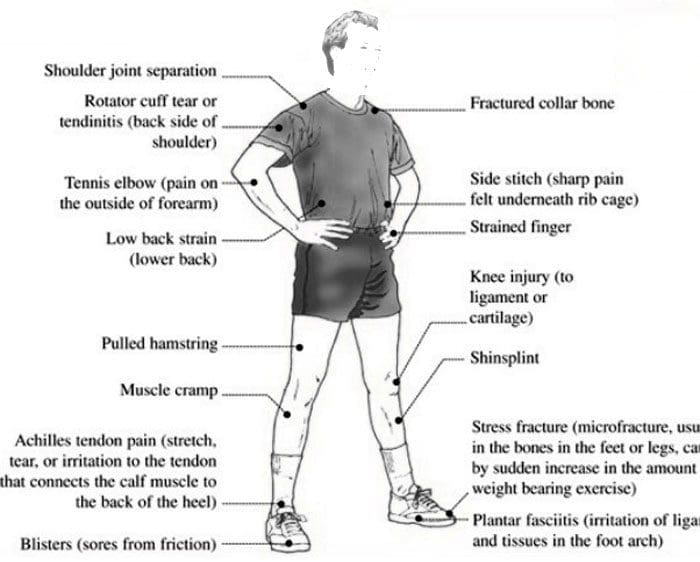
Acute and chronic sports injuries. Individuals who participate in sports or physical activities have an increased risk of experiencing an injury. These types of damages range from minor to severe and could require medical attention. Acute sports injuries happen suddenly and are usually the result of trauma to the area. A specific, identifiable incident is what causes an acute injury. Chronic sports injuries, also known as repetitive/overuse injuries, happen with time and are not caused by a single incident.
Acute and Chronic Sports Injuries Identification
Acute injuries can be identified by their cause. This could be a falling down during a run, sharp pain that presents in the shoulder after a throw, or a sprained ankle. The ability to focus on one cause usually means it’s acute. Acute injuries are characterized by:
Sudden pain in an area where there was none.
Swelling
Redness
Tenderness
Limited range of motion.
The inability of the injured area to support its weight.
A broken bone.
Dizziness
Headache
Nausea
Vomiting
Chronic injuries are different but are usually easy to identify. The pain begins gradually, usually over weeks or months. Repetitive activities like running, throwing, and swinging can exacerbate the pain. However, it is difficult to point to a specific issue that first caused the discomfort or pain. Chronic sports injuries are characterized by:
Pain and tenderness in the area, especially during and immediately after activity.
Minor swelling and limited range of motion.
Dull pain when resting.
These two types of injuries have different causes – trauma for acute and wear-and-tear for chronic – but they can both result in similar issues. For example, shoulder rotator cuff injuries are common, especially those that repeatedly use their shoulder to swing, throw, swim, etc. The individual needs to undergo a rotator cuff injury test to diagnose the injury correctly, whether the damage is acute or chronic. Chronic injuries can cause acute injuries, and acute injuries can lead to chronic injuries if left untreated.
Examples of Acute and Chronic Sports Injuries
Chronic and acute injuries are common in every type of sport. There’s an opportunity for both types of injuries. The most common include:
Other injuries from trauma, overuse, or both include:
Nonspecific Back Pain
Herniated Disc/s
Spondylolysis
Treatment
Minor acute injuries can be treated with rest, ice, compression, and elevation, aka R.I.C.E. Overuse injuries, are different as the injury has been gradually increasing in its severity, possibly causing scar tissue and ganglion cysts to develop. To prevent the injury from worsening, it’s recommended to see a sports injury chiropractor or physical therapist. These professionals can help heal the body and educate the individual on self-care and prevention.
Chiropractic
The musculoskeletal system takes a beating. Chronic injuries usually affect the bones, joints, muscles, or a combination. Chiropractic helps keep the musculoskeletal system limber and in proper alignment. Adjustments include:
Neck adjustments
Arm and hand adjustments
Shoulder adjustments
Knee adjustments
Hip adjustments
Foot adjustments
Physical Therapy
Physical therapy for a chronic injury can help prevent future injuries. A physical therapist helps:
Improve range of motion
Reduces pain and swelling
Increases strength
Whether an athlete or is just staying active and having some fun with sports, acute and chronic injuries can sneak up and worsen if they are not treated properly. Healing with the help of a professional can quicken recovery time and prevent future injuries.
Body Composition
Maintain Muscle Mass While Losing Fat
Individuals who want to lose weight should focus on losing excess fat tissue, not muscle mass. Studies have shown that diet and exercise are crucial to preserving Skeletal Muscle Mass while losing weight. Losing weight healthily includes:
A healthy balance of cardio and resistance training to burn calories and build muscle.
Wörtler, K, and C Schäffeler. “Akute Sportverletzungen und chronische Überlastungsschäden an Vor- und Mittelfuß” [Acute sports injuries and chronic overuse stress damage to the forefoot and midfoot]. Der Radiologe vol. 55,5 (2015): 417-32. doi:10.1007/s00117-015-2855-3
Yang, Jingzhen et al. “Epidemiology of overuse and acute injuries among competitive collegiate athletes.” Journal of athletic training vol. 47,2 (2012): 198-204. doi:10.4085/1062-6050-47.2.198
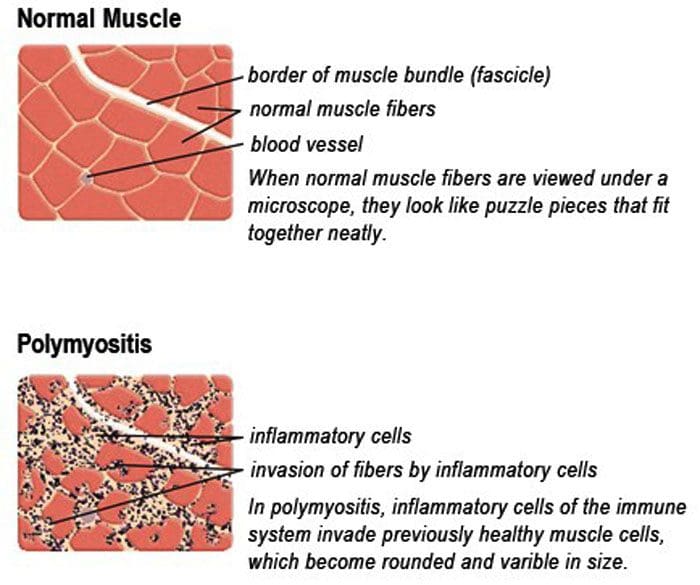
Polymyositis is a disease that causes the body’s muscles to become irritated and inflamed. It can affect the muscles all over the body. The muscles gradually begin to break down and weaken, making everyday movements difficult. This disease falls into a category known as inflammatory myopathies.
Polymyositis Unknown Causation
The causes of polymyositis are currently unknown. However, experts believe it could be associated with or triggered by a virus or an autoimmune reaction. An autoimmune response is when the body attacks itself along with the body’s tissues. It’s seen in individuals ages 31 to 60 and is rarely seen in individuals younger than 18. In some instances, medication can lead to an allergic reaction/response that causes muscle irritation and damage. But in most cases, healthcare experts are not able to find the exact cause.
Symptoms
The condition can affect the muscles all over the body. Physical activities like walking, getting up from a chair, or lifting objects can become difficult to perform. It can also affect the muscles that allow for eating and breathing. The muscles at the center of the body tend to be affected the most. Common symptoms include:
Muscle pain.
Muscle stiffness.
Muscle weakness, specifically in the abdomen, shoulders, upper arms, and hips.
Joint pain and stiffness.
Breathing problems.
Problems swallowing.
Abnormal weight loss can become an issue if there are problems with swallowing.
Irregular heart rhythms if the heart muscle/myocardium becomes inflamed.
Individuals may notice they have trouble climbing stairs or lifting their arms.
The inflammation can worsen, causing pain and weakness that affects the wrists, lower arms, and ankles.
Diagnosis
Diagnosis begins with the individual’s medical history, family medical history if necessary, and a physical examination. The examination includes seeing and feeling the strength of the muscles. Tests will be required that include:
Blood Tests
Blood tests allow the doctor to see if there are signs of muscle inflammation.
They also show if there are abnormal proteins that form in autoimmune diseases.
Electromyogram EMG
This test can be used to find abnormal electrical activity in the affected muscles.
MRI
Magnets and computer graphic imagery are used to help the doctor inspect for inflammation in the body.
Muscle Biopsy
A small piece of muscle tissue is removed to be analyzed with a microscope.
Treatment
Treatment depends on how severe the condition is,individual symptoms, age, and overall health. Currently, there is no cure for polymyositis, but symptoms can be managed. Individuals are recommended to utilize more than one type of treatment because the treatment plan may also need to be changed as treatment progresses. Treatments include:
Anti-inflammatory Medication
Steroid medication can help manage the disease and reduce symptoms, and corticosteroids can help ease inflammation in the body. The symptoms improve within 4 to 6 weeks, and a healthcare provider can lower the dosage after the symptoms decrease to reduce and ease any side effects.
Immunosuppressive Medication
These medications block or slow down the body’s immune system responses.
Talk with a doctor about the risks, benefits, and side effects of all medications.
Chiropractic and Physical therapy
Chiropractic treatment and physical therapy can help:
Aligning the spine to provide optimal nerve energy and blood circulation.
Therapeutic massage to stimulate and keep the muscles loose.
Specific exercises to help stretch and strengthen the muscles.
These can help keep the muscles from shrinking.
Heat therapy and Rest
Heat therapy and allowing the body to rest thoroughly can help decrease pain symptoms.
Special Braces
Body, hip, and leg braces can help support the muscles and help with mobility.
Complications
Polymyositis left untreated can lead to severe complications. The muscles become weaker, increasing the risk of falling and limiting daily activities.
If the chest muscles are affected, there could be problems with breathing that can lead to respiratory failure.
If the digestive tract is affected, malnutrition and unintentional weight loss can result.
Polymyositis poorly managed well can cause severe disability.
Body Composition
Nutrition and Muscle Growth
Protein
Protein is the foundation for gaining muscle.
This essential component is for all of the body’s daily functions.
It is essential to balance protein increase with overall diet.
Carbs should be a daily element of nutritional intake because they are the primary component.
Acquiring energy
Preventing muscle weakness and degradation
Consuming Carbs
Understanding how accurate results only happen when both sides work together.
Healthy consumption of protein and carbohydrates can help muscle growth and sustain optimal health for all body types.
References
Corrado, Bruno et al. “Supervised Physical Therapy and Polymyositis/Dermatomyositis-A Systematic Review of the Literature.” Neurology international vol. 12,3 77-88. 24 Nov. 2020, doi:10.3390/neurolint12030015
Findlay, Andrew R et al. “An overview of polymyositis and dermatomyositis.” Muscle & nerve vol. 51,5 (2015): 638-56. doi:10.1002/mus.24566
Sasaki, Hirokazu, and Hitoshi Kohsaka. “Current diagnosis and treatment of polymyositis and dermatomyositis.” Modern rheumatology vol. 28,6 (2018): 913-921. doi:10.1080/14397595.2018.1467257
Van Thillo, Anna et al. “Physical therapy in adult inflammatory myopathy patients: a systematic review.” Clinical rheumatology vol. 38,8 (2019): 2039-2051. doi:10.1007/s10067-019-04571-9
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine