Most of us know what sciatica means and that is low back pain that radiates/spreads into the buttock down into the leg and sometimes into the foot. The pain can be mild to excruciating, but fortunately, if it is mild�sciatica can usually be alleviated in 3 months.�These are a few non-invasive conservative treatment therapies that can be done at the house.
Here are a few at the house sciatica remedies for people who started experiencing sciatic nerve pain or whose pain is not severe. But you should get a doctor�s approval before trying any of these at the house therapies.
If sciatica has been present for a few weeks or the low back and leg pain has become debilitating you should see a doctor.
House Tip 1. Exercise is OK & Beneficial
It might seem strange to exercise when you�re in pain, but research has shown that too much rest can aggravate back and leg symptoms.
Remember this is not a hardcore burning massive calories exercise, but a gentle exercise routine that you can work into your day.
These Exercises should not be painful or strenuous.
A walk around the house is a great form of physical activity that keeps your spine strong without worsening the injury.
Make your spine stronger with core exercises, but make sure they will not exacerbate your sciatica symptoms. And remember that exercise triggers the release of endorphins to reduce the pain.
House Tip 2. Start Stretching
Start doing gentle stretches regularly. Stretching will improve your spinal flexibility and motion range and also builds core strength. Most stretches can be done while watching your favorite show/movie.
House Tip 3. Ice Packs and Heating Pads Help
Alternating heat and ice therapy can bring relief from nerve pain. Ice helps reduce inflammation, and heat generates blood flow to the areas of pain that speeds up healing. Both help reduce muscle spasms that usually come with sciatica.
Apply the ice pack for 15 minutes once every hour, and then bring the heat for 15 minutes every 2 or 3 hours. Remember to protect your skin when using these pads, and never sleep with the heat or ice pads.
House Tip 4. Change Your Posture
If you are working at your desk or just relaxing, don’t stay in the same position too long, as it can make the pain spike.
Therefore move around and change your posture every 20 minutes. Using the correct posture for various activities will help take the pressure off your spine and reduce symptoms.
House Tip 5. If You Need To Use Medication Properly
Over-the-counter non-steroidal anti-inflammatory medications can help ease symptoms when they present. These medications can relieve inflammation and pain, whereas acetaminophen (Tylenol) only reduces pain.
However, there are health risks, so make sure to discuss their safety with your doctor.
Examples include:
Ibuprofen (Advil, Motrin)
Aspirin (Ecotrin)
Naproxen (Aleve)
The Remedies Are Not Working
Recognize when at the house remedies are not reducing your symptoms. When the treatments aren’t helping, it could be time to see a doctor, chiropractor or spine specialist.
People including myself want to avoid the doctor. It could be knowing how to use your health insurance or if you don�t have any. Whatever the reason do not opt for the ignorance is bliss and hope it will all go away.
If you need help figuring out how to use your insurance here at Injury Medical our staff are trained to help guide you through the process. And if you don’t have insurance we can still help and work out different types of plans.
Now there are sciatica symptoms that warrant immediate medical attention. In these rare cases, holding off medical care could cause permanent nerve damage.
If any of the following occur, please see your doctor as soon as you can:
There is severe throbbing/stinging pain in your low back and legs
Nerve associated symptoms like:
Weakness
Numbness
Tingling
Electric shock-like pain
The pain is not improving after 2 weeks
The pain gets worse, even with house therapies
Loss of bowel or bladder control
At the end of the day reducing sciatica symptoms doesn�t always mean having to use an extreme treatment approach. Relieving sciatica symptoms at the house with light exercise, ice/heat therapy, correct posture, and medication can help speed up recovery. The most important thing you can do is to take it seriously and call your doctor or chiropractor if relief is not happening.
Please contact our chiropractic team today to schedule an appointment if you are experiencing symptoms of sciatica. We are ready to help you feel better and get back on your feet again!
*Effective Treatment* for Sciatic Nerve Pain| El Paso, Tx
NCBI Resources
A study cited by the health magazine�Prevention�found that sixty percent of sciatica sufferers who failed to get relief from other treatments found their symptoms improved after chiropractic care. In fact, they got the same level of relief as those who went through surgery � without any of the serious side effects that so often come with surgical procedures.
Being pregnant is one of life’s many joys, however, with the added weight comes normal back pain that can lead to severe back pain that can lead to sciatica.
Expecting mothers have much to look forward to but when back pain and sciatica take hold, it can be exhausting, frustrating, and extremely painful. Women experiencing pregnancyback pain varies from woman to woman. To help prevent and alleviate back pain/sciatica, here are some answers as to how and why symptoms develop and what to do to make the pregnancy a joyful occasion.
Pregnancy Back Pain and Sciatica
Changes to the body throughout pregnancy affect more than its physical appearance.
The most common change is weight gain. Increased body weight, especially when bending puts pressure on the spinal discs. The most pressure is placed on the low back. Back, leg pain, and sciatica are common complaints.
Weight gain can cause piriformis syndrome and sciatica. The piriformis muscles help with thigh movement. Piriformis syndrome can develop if the muscle compresses the sciatic nerve, which causes a pinching or electrical shock feeling in the buttocks and back of the leg.
What some might not know is that as the uterus grows, the body’s center of gravity gets thrown off. What happens is the uterus expands inside the pelvis, and the spinal nerves in the low back that flow into the sciatic nerve gets compressed and irritated.
Hormones like relaxin, which is a hormone that relaxes the pelvic ligaments and helps prepare the mother’s body for birth. Relaxin loosens the ligaments in the other areas of the body, but primarily the joints in the pelvis, low back, and knees. When exercising or lifting objects it is easy to strain these relaxed areas. Therefore, move slowly, and avoid any sudden movements.
What Steps To Take
Work with a:
Doctor
Chiropractor
Midwife
Health care provider to keep body weight in check
Take note of posture:
Stand up straight
Shoulders back
Avoid leaning backward
Try a pillow:
A standard-sized pillow
Body pillow to help make sleeping comfortable
A pillow can be positioned between the knees and under the abdomen for support.
Prenatal yoga helps:
Stretch and tone muscles
Maintain flexibility
Improve balance and circulation
Relieves tension
Deep breathing plays a major role in yoga and is an added benefit as it can help expecting mothers relax during labor.
Simple cardiovascular exercises like walking or swimming can help keep weight under control and the body in shape. Ask a doctor or chiropractor if these types of exercises are right for you.
Prenatal massage is another option to help relieve pain and tension.
This type of massage eases:
Anxiety by stabilizing hormone levels
Back pain
Pelvic pain
Hip pain
Improves circulation and digestion
Helps reduce fatigue
A warm shower or bath can helps ease back pain.
Expectant mothers should avoid aromatic oils or aromatherapy candles like:
Basil
Juniper
Peppermint
Rosemary
Star anise
Some of these oils can cause contractions.
Acupuncture is another form of alternative therapy that can treat back pain and sciatica. Sterile, millimeter thin disposable needles are inserted into points on the body that are known as energy channels. The needles help to restore the balance of energy in the body. However, expectant mothers need to be past six months to receive this type of treatment as the energy flow can cause contractions.
Ergonomics At Work & Home
Expectant mothers should avoid:
Awkward postures
Over-exercising
Heavy lifting
Repetitive work
Especially during the third trimester.
The low back and leg muscles have to work harder to keep the body balanced. Just basic standing or walking can be a challenge. Swelling is common. Make sure to take constant breaks and full-body rest combined with elevating the feet can be very helpful.
Adding an ergonomic and adjustable chair with a lumbar support backrest and footrest is worth the investment. A chair like this can helps take the pressure off of the spine and working at a desk much more comfortable. It benefits to frequently stand and sit continually changing the body’s posture and working the various muscles, joints, and ligaments to keep the body loose. And it can be a form of exercise.
Light walking also helps to reduce any swelling through increased circulation.
Hopefully, you will not have to go through any kind of back pain or sciatica. But if pregnancy back pain and sciatica start to creep in, talk to your doctor, chiropractor, midwife, or health care professional first.
When your body is truly healthy, you will arrive at your optimal fitness level proper physiological fitness state. We want to help you live a new and improved lifestyle. Over the last two decades, while researching and testing methods with thousands of patients, we have learned what works effectively at decreasing pain while increasing human vitality.
We focus on what works for you. We also strive to create fitness and better the body through researched methods and total wellness programs. These programs are natural and use the body’s own ability to achieve goals of improvement.
Back Pain During Pregnancy Treatment El Paso, TX Chiropractor
NCBI Resources
Keeping the body, including the spine, in proper alignment is vital to mobility, flexibility, and overall wellness of the body even when it is not pregnant. However, pregnancy puts specific stress on the body, creating certain needs that chiropractic care can meet. It is safe, it is effective, it is fast, and it works.
Do you have lower back pain or pain literally in the rear that runs down into one thigh or below the knee into the leg and even the foot? A doctor may diagnose these symptoms as sciatica, which describes compression of the sciatic nerve.
Sensations include:
Numbness
Tingling
Pins and needles
Electric like shock running through the leg
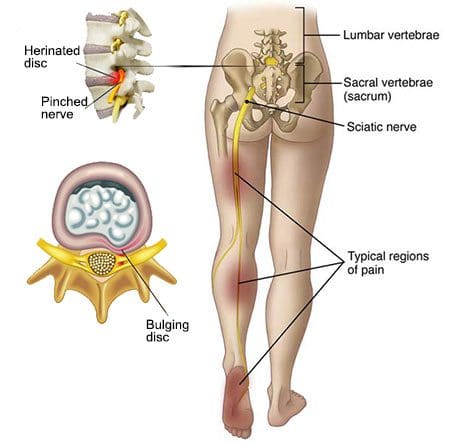
Depending on the nerve that is affected pain could radiate only into the buttock or all the way down to the foot. A common cause is a lumbar disc herniation or bone spur that presses down on the spinal nerve. Sciatic pain radiates along the nerve, usually from the low back, down the buttocks, into the thigh and leg, below the knee and sometimes into the foot and big toe.
Sciatica usually affects one side of the body.
Radicular Pain
A doctor may use the terms radicular pain or radiculopathy when talking about sciatica. Radiculopathy is pain/adverse sensation that travels along a nerve. When a spinal nerve root is compressed, pinched or injured, it becomes inflamed. Low back conditions that can contribute to this type of problem are spinal stenosis, foraminal stenosis or herniated disc.
Proper Diagnosis & Proper Treatment
The doctor will ask about your symptoms:
When did the pain begin?
Where is the pain most intense?
What activities worsen the pain?
What activities reduce pain?
Does the pain go all the way down the leg or stops at the knee?
Do you feel weakness or tingling in your legs or feet?
A doctor might perform a straight-leg test to see if there is an inflamed nerve. This is a simple exam where you lie on your back and the doctor lifts each leg. If this causes or produces pain and sensations, it can indicate there is a bulging/slipped or ruptured disc.
The compression of the nerve can also cause muscle weakness in the foot. Another exam may be to walk like you normally do, then on your heels and finally on your toes. This checks your balance and lower-body strength.
A doctor will:
Check your posture
Range of motion
Movements that cause pain
Check the curvature and alignment of your spine
Check for muscle spasms
Note your sensations
Test your reflexes and muscle strength
A doctor may order x-rays, CT scan or MRI.
The CT scan or MRI provides doctors with various images of your spine which can help in diagnosing whatever is causing your symptoms. These tests are then compared to what the doctor took note of during your medical history interview and the physical and neurological examinations. An accurate diagnosis is the first step in figuring out the best treatment plan.
Could something else be causing the nerve pain?
Only a doctor can tell if your symptoms are sciatica. There are other structures in the spine that can cause similar types of pain.
The sacroiliac joint between the pelvis and sacrum is the lowest part of the spine can cause sciatic pain.
The facet joint which connects the joints in the back of the spine gets sprained, it can also cause sciatica-like pain.
A tear in a spinal disc can cause pain down into the leg.
The hip joint can also cause pain in the thigh, that can radiate outward.
Sciatica Nerve Treatment
Sciatica can be treated non-surgically with:
Chiropractic care
Physical therapy
24 to 48 hours of bed rest
Over the counter pain relievers like ibuprofen or acetaminophen
Patients with sciatica feel better with time, usually a few weeks. If pain continues, other treatment modalities can be discussed. Muscle spasms can accompany sciatica symptoms and can be treated with heat or ice therapy. A doctor may advise light exercise like short walks and once recovery is established they may give you exercises to strengthen your back and core.
Severe *Sciatica”* Pain Relief | El Paso, Tx (2020)
NCBI Resources
A study cited by the health magazine�Prevention�found that sixty percent of sciatica sufferers who failed to get relief from other treatments found their symptoms improved after chiropractic care. In fact, they got the same level of relief as those who went through surgery � without any of the serious side effects that so often come with surgical procedures.
Chiropractic is effective for treating sciatica because it gets to the source of the problem � relieving pressure on the sciatic nerve.
Ergonomics involves the study and engineering of improving work tools/products to help employees and improve the physical demands of their jobs.
How does sciatica fit into this?
People that have to sit or stand for long periods in their jobs can develop back/hip conditions that can lead to:
Back
Buttock
Leg
Foot pain
And this can make working painfully difficult if not impossible contributing to lost workdays.
Check out these tips and apply ergonomic principles to everyday activities like:
Using a sit-to-stand up desk
Adjust sitting posture
Adjusting standing posture
Proper movement
These tips can help get you through the workday and the workweek with less pain.
Have a Seat
Sitting for long periods is not good for the spine or sciatic pain.
Try to stand up every 20 minutes and walk around the workspace.
Choose a well-designed ergonomic chair.
Add low back support with a lumbar pillow or even a rolled-up towel at the base of the chair.
Added tips to reduce sciatica while sitting:
Do not cross your legs
Keep feet flat on the floor
Keep hips and knees bent at a 45-degree angle
If the chair has wheels, roll around and make it an exercise, instead of twisting/turning the body in an awkward position that can exacerbate the pain.� Use the chair to move as a single unit.
Stand Up
Changing up posture is a wise way to exercise the spine on the job.
Mix it up when it comes to sitting and standing.
Sitting all day is connected to a variety of health problems that go beyond back pain. These include:
Obesity
Type 2 diabetes
There are great benefits when you can sit and stand at work. This can help the work routine immensely.
Standing lowers the risk of type 2 diabetes: Studies have shown people that sit for long periods at work had higher levels of fasting blood sugar.
Standing lowers the risk of cardiovascular problems: Research has linked people who spend even just two hours a day sitting have an increased risk for cardiovascular health problems by one-hundred percent.
Standing helps burn extra calories: A study found regular use of sit-stand desks at work can help burn calories and prevent weight gain when combined with proper diet and exercise.
An easy way is to use a sit-stand desk or sit-to-stand desk.
A sit-stand desk allows adjusting desk height to work seamlessly from sitting to standing.
Before purchasing this type of equipment, research the different styles and types to find the right model for you.
Although standing is important, don’t stand in one place or position for an extended time. Move around and stretch out.
If the job requires standing, rest one foot on a box or stool. and alternate every 10 to 15 minutes.
When standing with sciatica:
Take care when getting up from sitting to a standing position.
When getting up try not to bend at the waist, as this can stretch and aggravate the nerve.
Slide to the front of the seat and stand up by straightening the legs.
Keep Work Within Arms Reach
Keep your work close to avoid bending forward, as this also aggravates the nerve.
Keep your shoulders relaxed, and rest the elbows and arms on the desk or chair arms.
Computer Ergonomics
Create a sciatica-friendly workstation.
Position the monitor at eye level
Keep the keyboard and mouse close
Avoid reaching too far
Choose a proper ergonomic chair
Avoid leaning or slumping forward
Muscle Smarts
Don’t move or lift objects that require great muscular force, like pushing a sofa or picking up a table.
Carrying a:
Purse
Briefcase
Groceries
Luggage
It can be challenging, so carry an equal amount of weight to keep the body balanced.
Anything you don’t need, leave at home. You don’t need the extra weight.
Sleeping On The Proper Mattress Matters
After a long day, get off your feet and rest.
However, if the mattress you sleep on does not support your spine, then sciatica can become a permanent condition.
A soft and lumpy mattress does not properly support the spine, which leads to muscle fatigue and restless sleep.
If these measures:
Time
Ice
Heat
Over-the-counter medications
Don’t help reduce the back and leg pain, definitely call a doctor or chiropractor.
They can determine what is causing sciatica and will create a customtreatment plan to get you working at your best in the shortest amount of time possible.
El Paso, TX Best Sciatica Chiropractor Treatment
Sandra Rubio discusses how Dr. Alex Jimenez and his staff can help relieve your sciatica symptoms. Chiropractic care can improve pain and discomfort as well as reduce irritation and inflammation caused by sciatica. In addition, a chiropractor like Dr. Jimenez can also provide nutritional and fitness advice for sciatic nerve pain. Other treatment methods, like deep-tissue massage, can help relieve sciatica symptoms. Dr. Jimenez is the homeopathic, non-surgical choice for sciatic nerve pain and its associated symptoms.
NCBI Resources
You may be suffering from sciatica if you have ever experienced a shooting, nerve-like pain down one of your legs. The sciatic nerve can be impacted by a number of different things, including injury and degenerative diseases, that can lead to sciatica. Fortunately, chiropractic can be extremely effective for the treatment of sciatica.
A car accident can easily damage the spine and soft tissues. An auto accident may cause a misalignment of the spine, a herniated disc, or other injuries that cause symptoms of sciatica.
Many sufferers of sciatica do not realize that their workplace activities � including repetitive motions and sitting in one position for long periods of time � can lead to sciatica.
When the weather begins to change and that cold feeling starts to creep into the bones, especially down the back. That’s when sciatica symptoms can flare-up in the worst way.
Cold weather really make sciatica worse
Of the many patients that I’ve treated, those with sciatica firmly state that cold weather makes it worse.
There are bonafide reasons why sciatica acts up when the temperature goes down.
Sciatica
It is a type of radiculopathy, caused by pressure on one or more of the five nerve roots in the lower back;
This is known as the lumbar region of the spine.
The nerves run from the lower spine under buttocks and down each hip into the legs.
Several conditions can compress these nerves at one or more spots along the way:
Numbness
Weakness in the
Lower back
Buttock
Legs on one or both sides
Research Study
Cold weather affects sciatica because it affects different types of pain.
Researchers found that the men who worked in low temperatures reported higher cases of neck and low back pain.
This was compared with those working in warmer temperatures.
Cold Weather & the Spine
Pain and discomfort can increase because the muscles stiffen up in cold weather.
The spine’s muscles also become tight and tense.
Tension and stress, can make the pain worse and increase the risk of muscle strains/sprains.
Barometric Pressure
Air pressure drops before a storm or when the temperature changes.
These changes seep into the sensitive nerves of the lower back and cause swelling/inflammation and pain.
Physical Stress
Any type of movement can wreak havoc on a healthy spine.
This is due to the cold weather causing individuals not to:
Use correct posture
Use correct movement when performing tasks/chores
Hurrying tasks/chores
There is also the chance of a slip and fall accident or twisting your back.
All of this is the perfect set-up for spine and sciatic injury/s.
So How to reduce sciatic pain?
Keep Warm
Wear warm clothing and in layers.
A few thin layers can keep the body warmer than a single thick layer.
Keep the lower back warm
Tuck your shirt into your pants to make sure that your back doesn’t get a cold draft when you reach for something and then put a sweater on over that.
A couple of blankets or an electric blanket on your bed can help keep your muscles from tightening.
Keep home as warm as possible.
Run the car a few minutes to preheat it before heading out.
Wear Proper Shoes or Boots
Proper footwear should have enough tread to prevent slips and falls.
Proper shoes for walking in cold weather. Don’t do the flip-flop thing, that’s just asking for foot/back problems.
Orthotics can help with posture, pronation, and gait.
Warm-Up Before Starting Outdoor Activity
Stretch and loosen the muscles and joints before you go out to:
Trim the lawn/bushes
Take a walk
Play with the kids
Take a few minutes to stretch and warm up inside before going outside.
Do It Right
As previously mentioned use correct form, meaning, lift with your legs, not the back.
Move smaller amounts if landscaping etc., Do it in small increments instead of one or two heavy loads.
Don’t twist your back while lifting.
Face the direction you are going in.
Ask for Help
If sciatica is affecting the task at hand, do not be too proud or afraid to ask for help. Stubbornness can lead to severe injury/s that could have been avoided.
Stay Active
When cold weather starts to make itself known, most of us want to get on the couch, binge watch our favorite movies, sleep, get snuggly, etc.
Exercising and staying in shape is a top remedy for sciatica symptoms.
Consult with a chiropractor, physical therapist/trainer that can offer exercises that won’t present/exacerbate symptoms
Watch your weight when the cold weather kicks in and keep up with your exercise.
El Paso, TX Chiropractor Sciatica Symptoms
Sandra Rubio discusses sciatica, its causes, and its symptoms. Sciatica is the collection of symptoms caused by the compression of the sciatic nerve, the longest nerve in the human body which extends from the lower back to the feet. Sandra Rubio describes how she’s witnessed many patients come into Dr. Alex Jimenez’s office feeling painful and often severe symptoms of sciatica caused by a variety of spinal health issues. Fortunately, Dr. Jimenez is the non-surgical choice for the safe and effective treatment of sciatica symptoms.
Based upon how it’s defined, approximately 2 percent to 40 percent of individuals will experience sciatica symptoms at some point in their lifetime. It is most frequent during people’s ’40s and ’50s, and men are more frequently affected than women. About 90 percent of the time, sciatica symptoms are because of a disc herniation. Other issues that may bring about sciatica comprise of spondylolisthesis, spinal stenosis, piriformis syndrome, pelvic tumors, and compression by a baby’s head during pregnancy, among other spinal health issues.
NCBI Resources
Chiropractic care is a popular, alternative treatment option commonly utilized to help treat symptoms of sciatica. Sciatica is characterized as a collection of symptoms, rather than a single injury or condition. A chiropractor can help diagnose the source of a patient�s sciatic nerve pain, or sciatica, in order to properly determine the best treatment for their specific health issue.
Spinal adjustments and manual manipulations can be utilized to help carefully correct the alignment of the spine, restoring the natural integrity of the spine and allowing the body to heal itself, without the need for drugs and medications or surgery. In certain individuals, sciatica may fix itself, possibly happening just once or a few times throughout their lifetime. But, it�s important to remember that if an injury and/or aggravated condition is not treated effectively, symptoms may worsen.
Sciatica doesn�t have to prevent you from being able to travel.
Sometimes a journey can create a series of challenges for people with sciatic nerve pain in the low back and leg.
A common issue among individuals is to prevent sciatica from flaring up when on the road or in the air.
A solution for this is to find ways to keep moving. However, easier said than done, but it can be done!
Flying and driving often mean long periods of sitting and sitting in a position typically not friendly with sciatic pain.
“When we drive or fly for an extended trip, it means long sitting times, and sitting in a position that can cause sciatica to flare up at any time,” says Dr. Alexander Jimenez, D.C. in El Paso, Texas, and member of the American Chiropractic Association (ACA).
Dr. Jimenez shares some basic tips for keeping mobility up, all the while pain-free, when flying and driving with sciatica.
He also offers additional advice to keep radiating pain from starting, upon arrival.
Flying with Sciatica
Sciatica pain radiates through the lower body meaning:
The low back
Hips
Buttocks
Legs
So when a flight anchors you to a seat, this can aggravate the area and cause pain.
The first thing to consider is the seat choice.
An aisle seat allows you the easiest access out of the seat, allowing you to move more during the flight.
Also when flying with sciatica, tell the flight crew about your condition.
When the seatbelt off light comes on, get up, stretch your legs and move around anywhere you can find room.
With a good portion of the population suffering from sciatica, most crews have seen people with this condition, and will usually let you do some stretching if they’re not busy.
A good sciatica stretch is to put your hands on something stable and do some deep knee bends.
This will use the upper body weight to stretch the lumbar spine comfortably.
Do a few and make sure you feel and return to your seat stretched and refreshed.
When taking a long flight, do this every hour to feel better when landing.
Sciatica Road Trip
Road trips, on the other hand, are easier to stop and move around. However, it can also create over-concentration on the drive and forgetting how much you are hurting until the pain is unbearable.
Dr. Jimenez advises frequentstops, if possible every hour is best to prevent pain.
On the stops walk two or three laps around the car/Suv/truck.
Rear bumper stretching prop
Place one foot on the bumper, and the other a few feet behind, lean into the bumper and square the hips with the lead foot.
This is like a hurdle stretch.
Stretch both legs on each break.
Regular stretching helps relieve the pressure on the low back so you can drive comfortably.
Arrival
Packing light is a healthy tip because hauling heavy luggage will aggravate sciatic nerve pain.
There are a few things that Dr. Jimenez recommends packing or getting upon arrival.
Gel ice pack you can keep in the refrigerator or freezer in a hotel.
Apply the cold pack to the low back for 20-minute increments will go a long way toward relieving pain.
Topical agent/cream/gel that has menthol or camphor, that you can apply to any area of tenderness or pain before the ice gel pack.
This increases the ice pack’s power by helping relax muscles and decreasing pain.
Supportive shoes or custom foot orthotics
People with sciatica should choose footwear or orthotics that support all three arches of the foot.
Leg length is usually not equal on each side, and proper arch supports can be custom made for you by your chiropractor to compensate for the difference.
Even a 5mm difference can cause chronic back pain.
And if possible, ask your chiropractor or primary physician if they can recommend a chiropractor, physical/massage therapist,� or acupuncturist that you can see in case you need emergency treatment.
This can give you some peace of mind.
Keep Your Exercise/Stretching Routine When Traveling
When we travel especially on vacations it can be easy to let healthy lifestyle habits you practice at home slide.
All are sciatica�s natural enemies make sure to bring these healthy practices with you to your destination.
Use the same good sense when you travel just like at home getting:
Get plenty of rest
Drink plenty of water
Don’t overeat
You will need more rest when you travel and don’t forget when you travel to:
Walk
Stretch
Stay mobile
Difference Foot Orthotics Make to *REDUCE FOOT PAIN* & Correct Posture | El Paso, TX (2019)
Custom made foot orthotics can help control foot motion and posture. Healthcare professionals prescribe custom foot orthotics to help patients focus on their foot posture and mobility control. Research studies have ascertained that using custom foot orthotics for posture and mobility control can help fix excessive foot pronation and supination to prevent a variety of foot health problems. The subsequent video describes how custom foot orthotics will help control foot posture and mobility to improve health and wellness.
NCBI Resources
Sciatica is generally caused by the compression of lumbar or sacral nerves or by compression of the sciatic nerve. When sciatica is caused by compression of a dorsal nerve root, it’s known as lumbar radiculopathy. This can occur because of a spinal disk bulge or spinal disk herniation (a herniated intervertebral disc), or by roughening, enlarging, or misalignment (spondylolisthesis) of the fascia, or as a consequence of degenerated discs which can reduce the diameter of the lateral foramen by which nerve roots exit the spine.
What exercise/stretches help reduce sciatic nerve pain?
Here are 4 exercise/stretches that your chiropractor/physical therapist may recommend to help you reduce sciatic nerve pain:
Pelvic tilt
Knee to chest
Lower trunk rotations
Arm and leg extensions
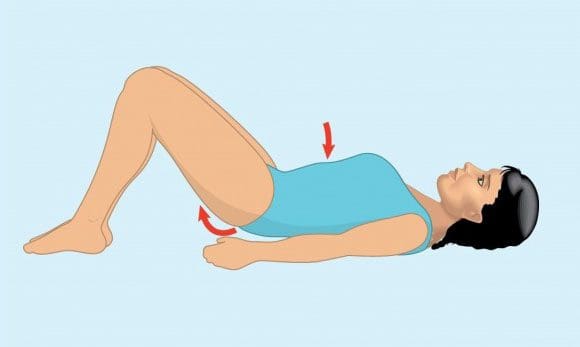
Pelvic Tilt
Its purpose is to strengthen the lower abdominal muscles and stretch the lower back.
How to do it:
Lie on back
Exhale and tighten abdominal muscles while pushing the belly button toward the floor and flatten the lower back
Hold the position for 5 seconds
Repeat 10 times holding the position for 5 seconds each
Am I doing it right?
Place the pinky finger on the hip bone and thumb on the lowest rib (same side).
When tightening the abdominal muscles, the amount of space between the pinky finger and thumb should get smaller.
Pelvic tilts help strengthen the lower abdominal muscles and stretch the low back.
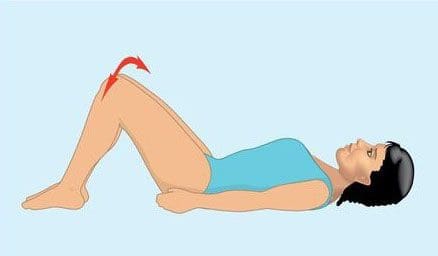
Knee to Chest
Its purpose is to help reduce nerve compression in the low back, that can help alleviate lower back pain.
Lie on back
Start with either� left or right knee and use hands to gently pull the bent knee toward chest
Hold for 10 seconds
Repeat movement on opposite knee
Perform 3 to 5 times holding position for 10 seconds each
Use hands to gently pull both knees toward chest
Hold for 10 seconds
Repeat movement with both knees 3 to 5 times holding position for 10 seconds each
Knee to chest exercise/stretches can help reduce nerve compression on the lumbar spine alleviating lower back pain.
Lower Trunk Rotation
Its purpose is to increase the spine�s mobility and flexibility.
Lie on back with both knees bent upright and both feet flat on the floor (aka the hook lying position).
Hold both knees together, rotate knees to one side
Hold for 3 to 5 seconds
There will be a gentle stretching sensation on the opposite side of lower back and hip area
Contract abdominal muscles and rotate both knees to opposite side
Hold for 3 to 5 seconds
Repeat 10 times on each side
Lower body rotations can help you strengthen your lower abdominal muscles and stretch your low back.�
All Fours Opposite Arm and Leg Extensions
Its purpose is to strengthen the abdominal muscles, low back and stabilize the areas.
Get in crawling position on all fours.
Contract abdominal muscles to keep back flat and straight
Raise one leg upward behind you and straighten outward
Hold for 3 to 5 seconds
Repeat the movement on the opposite side
Once this�exercise/stretch can be performed 10 times with functional pain, add arm movement with each leg extension:
Extend the arm (opposite side of leg) upward and outward in front of body
Hold for 3 to 5 seconds
Repeat on the opposite side
Perform 10 times
How do these exercise/stretches reduce sciatic pain
Abdominal and spinal muscles are essential components of the spine�s system.
These exercises/stretches can help:
Strengthen the spine
Increase flexibility
Increase range of motion
These exercises can help keep the spine�s structural components strong and healthy along with reducing pain and speeding up healing.
Regular exercise causes the body to release endorphins or hormones that interact with the pain receptors in the brain that reduce the perception of pain.
Will exercising with sciatica cause/exacerbate injury
Do not to perform any of these exercises without consulting your doctor,� spine specialist or chiropractor.
Whatever level of fitness, remember even trained professional athletes exercise with a doctor, physical therapist, or other healthcare expert’s approval and clearance.
Obtaining an accurate diagnosis for the exact cause of the sciatic pain
Is essential before considering any exercise program
Be gentle with your spine, don�t push too hard while doing exercises. This is to avoid exacerbating sciatic pain or creating a new injury.
If exercise increases pain or causes nerve-related symptoms like:
Weakness
Tingling sensation
Numbness
Stop and contact your doctor or chiropractor immediately!
El Paso, TX Best Sciatica Chiropractor Treatment
Sandra Rubio discusses Dr. Alex Jimenez and his team will help relieve your sciatica symptoms. Chiropractic care can improve pain and discomfort as well as reduce irritation and inflammation brought on by sciatica. Additionally, a chiropractor such as Dr. Jimenez can also offer nutritional and fitness tips for sciatic nerve pain. Other treatment procedures, such as deep-tissue massage, can help alleviate sciatica symptoms. Dr. Alex Jimenez is the homeopathic, noninvasive option for sciatic nerve disease and its related symptoms.
Sciatica is generally caused by the compression of lumbar or thoracic nerves or by compression of the sciatic nerve. When sciatica is caused by compression of a lower back nerve root, it’s called lumbar radiculopathy. This can happen due to a spinal disc bulge or spinal disk herniation (a herniated intervertebral disc), or by roughening, extending, or misalignment (spondylolisthesis) of the fascia, or as a result of degenerated discs that could reduce the diameter of the lateral foramen by which nerve roots exit the spine.
NCBI Resources
Sciatica is characterized by a shooting pain that originates in the lower back and travels down through the hip, buttock, and back of the leg. The pain can be so severe that it inhibits mobility and can prevent people from working, taking care of their home, or just enjoying their life. Doctors have treated the condition with medications and some invasive therapies, but chiropractic treatments have been found to be extremely effective in alleviating the pain and curing the condition.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine