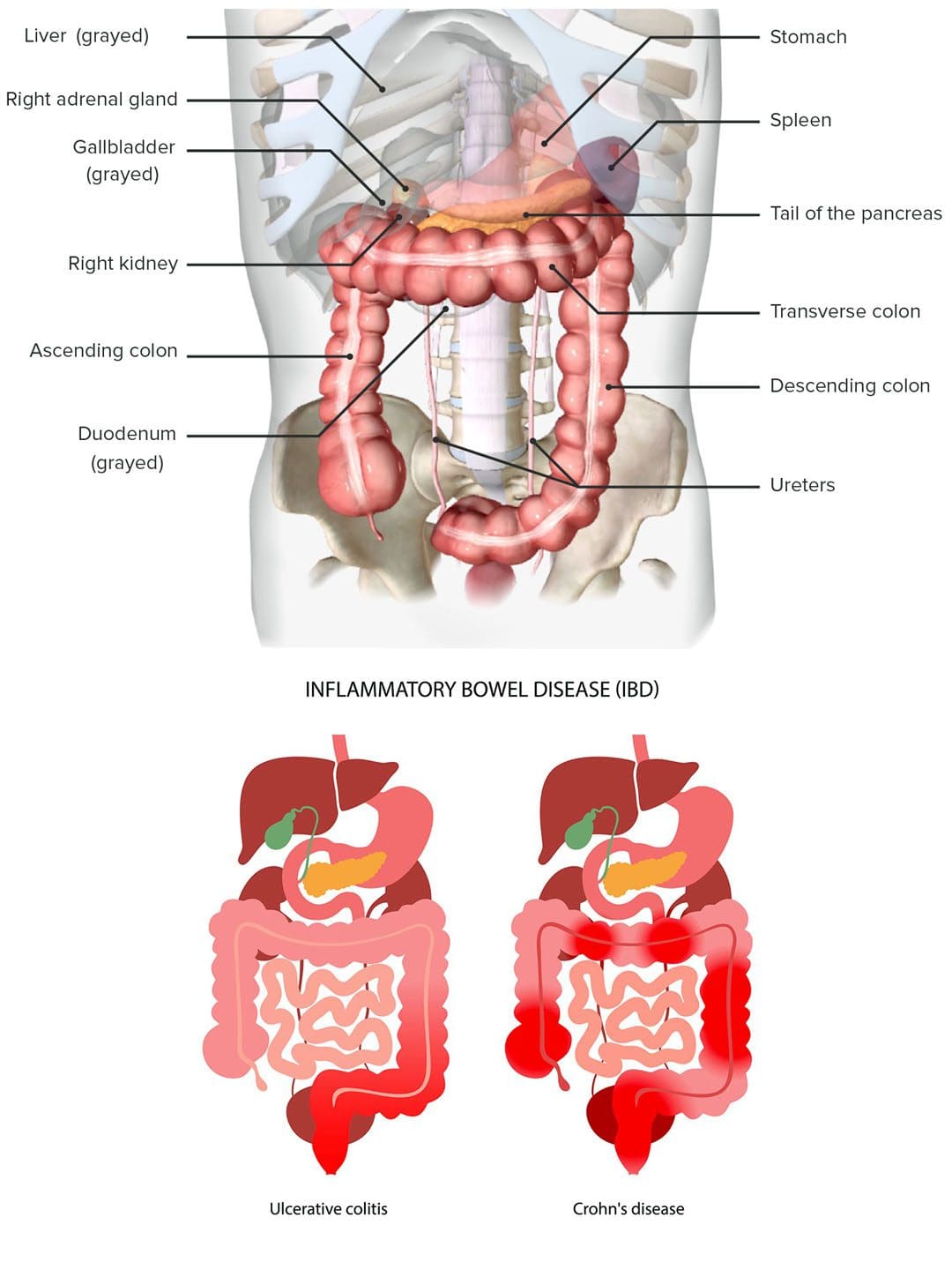
Inflammatory bowel disease, or IBD, causes inflammation of the digestive tract lining, which often involves the deeper layers. Gastrointestinal or GI problems of the stomach and intestines often include diarrhea, weight loss, rectal bleeding, fatigue, and back pain. The inflammation can reach the spine’s joints, causing stiffness, discomfort, and pain symptoms. Injury Medical Chiropractic and Functional Medicine Clinic can help manage symptoms and guide individuals on treatment options.
IBD Back Pain
IBD is a set of conditions associated with chronic or intermittent inflammation of the gastrointestinal tract. It includes Crohn’s disease – CD and ulcerative colitis – UC. Although there are genetic components that predispose individuals to IBD, environmental factors appear to contribute the most. Research shows that IBD is likely related to disturbances in the gut’s flora, which include:
Other environmental factors associated with IBD include the long-term use of birth control pills and nonsteroidal anti-inflammatory drugs/NSAIDs. Research theorizes that as the gut becomes inflamed, its normal integrity and structure become compromised and begin to leak out, causing an immune system overreaction response. This can cause non-gastrointestinal symptoms that include:
IBD can cause low back pain as the IBD can inflame the spine’s joints, especially the sacrum, as well as cause abdominal cramps and rectal sensations that radiate to the low back area. However, irritation, inflammation, or infection of any central, abdominal, or pelvic organs can cause low back pain.
Diagnosis
Diagnosis requires a physical examination of the colon – a sigmoidoscopy or a colonoscopy is used.
Both procedures take a biopsy of the intestinal tissues, which is studied to determine the extent and degree of inflammation.
Depending on the circumstances, an X-ray could be used to show the depth or extent of the condition.
Chiropractic Management
A chiropractor can help individuals decrease or completely alleviate musculoskeletal symptoms by realigning the spine and pelvis and massaging, releasing, and relaxing the muscles, which increases circulation and soothes inflammation. The reason why chiropractic care can effectively treat IBD is its ability to stabilize the internal systems. When the central nervous system and immune system communicate and function properly, this prevents the immune system from attacking the body’s tissue cells, preventing inflammation. The chiropractic whole-body approach can also help with recommendations regarding lifestyle changes and nutritional anti-inflammatory modifications.
Ulcerative Colitis
References
Centers for Disease Control and Prevention. “What Is Inflammatory Bowel Disease (IBD)?” 2022, https://www.cdc.gov/ibd/what-is-IBD.htm
Danese S, Fiocchi C. Etiopathogenesis of inflammatory bowel diseases. World J Gastroenterol. 2006;12(30):4807-4812. doi:10.3748/wjg.v12.i30.4807
Limsrivilai, Julajak et al. “Systemic Inflammatory Responses in Ulcerative Colitis Patients and Clostridium difficile Infection.” Digestive diseases and sciences vol. 63,7 (2018): 1801-1810. doi:10.1007/s10620-018-5044-1
van Erp, S J et al. “classifying Back Pain and Peripheral Joint Complaints in Inflammatory Bowel Disease Patients: A Prospective Longitudinal Follow-up Study.” Journal of Crohn’s & colitis vol. 10,2 (2016): 166-75. doi:10.1093/ecco-jcc/jjv195
Zeitz, Jonas, et al. “Pain in IBD Patients: Very Frequent and Frequently Insufficiently Taken into Account.” PloS one vol. 11,6 e0156666. 22 Jun. 2016, doi:10.1371/journal.pone.0156666
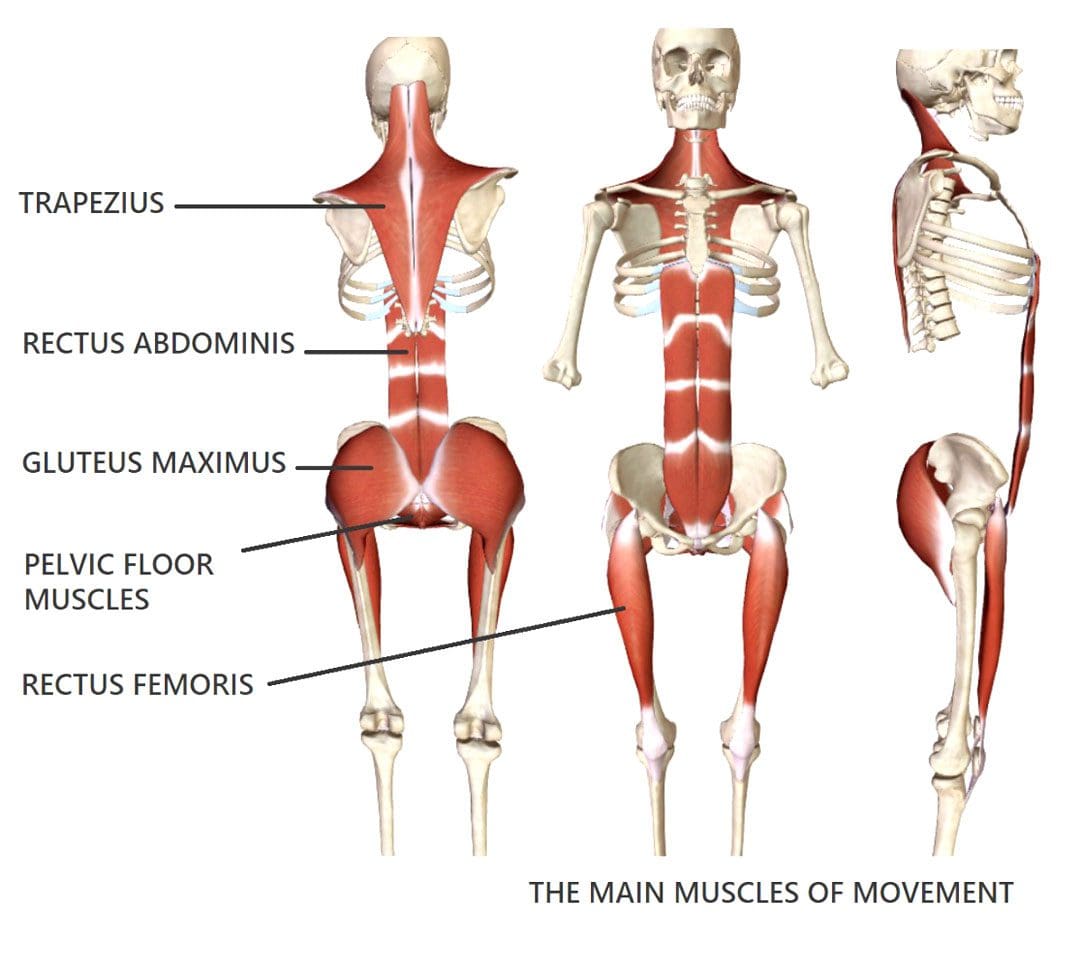
Making healthy posture adjustments is a process, especially for individuals that have been practicing unhealthy postures for years. Not only does the body have to relearn how to position itself correctly, but the muscles, especially those that haven’t been working, also have to adjust. This takes time and is usually at the beginning of postural training that individuals want to give up. This is because of the discomfort and soreness that goes with reactivating the core muscles. This is why it is recommended to go through the process with chiropractic care. A chiropractic therapy team can relieve sore muscles, strengthen the body, and help individuals gradually develop and maintain a healthy posture.
Posture Adjustments
Unhealthy postures shift the body out of balance, straining and stressing the muscles, especially those that have to work overtime every day. This causes the muscles to stiffen and tighten up to the point that they begin to pull the skeletal system in different directions, causing various symptoms that can lead to chronic conditions. Muscles can stay tight for years, with individuals getting used to the feeling. Individuals stretch out, thinking the muscles are loose but don’t realize that they return to their tight position because of the unhealthy muscle memory that developed.
Muscle Imbalance
Muscle imbalances usually progress over time and are typically caused by daily habitual physical routines.
This causes premature and advanced wear and tear on the body.
Postural Dysfunction
Individuals all have positions they spend a lot of time in.
Postural dysfunction begins with unhealthy positioning that shifts the spine and other joints out of balance and alignment.
The muscles become compromised, which leads to various neuromusculoskeletal symptoms.
Muscle fatigue and weakness occur from being overworked.
Headaches can present throughout the day.
Chiropractic Realignment
The muscles have become like tough meat, and the underlying imbalances are straining the neuromusculoskeletal system. The muscle tissues need to be broken up/tenderized and loosened up. Then they can be thoroughly stretched and strengthened to optimal health. Chiropractic care will identify and correct the underlying imbalance, and massage therapy will break up and release the compacted muscle tissue. A personalized treatment plan will consist of the following:
Mobilizing the joints and stretching/releasing shortened tight muscles and soft tissues.
Strengthening the elongated, weaker muscles to correct the body’s alignment and movement control.
Health coaching to identify and recommend lifestyle and nutritional adjustments.
This will restore the bio-mechanical systems, ensuring that equal muscle length and strength on both sides of the system joint or motion segment are maintained.
Posture Adjustments and Foot Orthotics
References
Aino, Masaki, et al. “Comparison of spinal column alignment and autonomic nervous activity using the intersegmental tenderness test in the segment above.” Journal of physical therapy science vol. 33,8 (2021): 570-575. doi:10.1589/jpts.33.570
Creze, Maud, et al. “Posture-related stiffness mapping of paraspinal muscles.” Journal of anatomy vol. 234,6 (2019): 787-799. doi:10.1111/joa.12978
Joshi, Reema, and Nishita Poojary. “The Effect of Muscle Energy Technique and Posture Correction Exercises on Pain and Function in Patients with Non-specific Chronic Neck Pain Having Forward Head Posture-a Randomized Controlled Trail.” International journal of therapeutic massage & bodywork vol. 15,2 14-21. 1 Jun. 2022, doi:10.3822/ijtmb.v15i2.673
Langford, M L. “Poor posture subjects a worker’s body to muscle imbalance, nerve compression.” Occupational health & safety (Waco, Tex.) vol. 63,9 (1994): 38-40, 42.
McLean, Linda. “The effect of postural correction on muscle activation amplitudes recorded from the cervicobrachial region.” Journal of electromyography and kinesiology: official journal of the International Society of Electrophysiological Kinesiology vol. 15,6 (2005): 527-35. doi:10.1016/j.jelekin.2005.06.003
Szczygieł, Elżbieta et al. “The Impact of Deep Muscle Training on the Quality of Posture and Breathing.” Journal of motor behavior vol. 50,2 (2018): 219-227. doi:10.1080/00222895.2017.1327413
The body is a complex machine with various muscles, tendons, ligaments, and vital organs that each play a specific role in maintaining functionality and stability to the host. The body allows movement and mobility from the neck down to the feet. When the body suffers from pain or has been affected by various issues that correlate with pain, two things can occur, one, where acute pain can affect the body and cause the individual to be sore for a few days or two, where the body suffers from chronic pain that leads to the development of myofascial pain syndrome that can lead to referred pain in different muscle groups and cause the body to dysfunction. Today’s article examines how to diagnose myofascial pain syndrome, how the body reacts to this condition, and how various treatments can reduce myofascial pain syndrome in the body. We refer patients to certified providers incorporating techniques and therapies for individuals dealing with myofascial pain syndrome affecting different body areas and causing functionality. By locating where the trigger points are coming from, many pain specialists utilize a treatment plan to reduce the effects that trigger points are causing on the body while coming up with a diagnosis to minimize the referred pain impacting the body. We encourage and appreciate each patient by referring them to associated medical providers based on their diagnosis when it is appropriate. We understand that education is a terrific way when asking our providers intricated questions at the patient’s request and understanding. Dr. Jimenez, D.C., only utilizes this information as an educational service. Disclaimer
How To Diagnose Myofascial Pain Syndrome
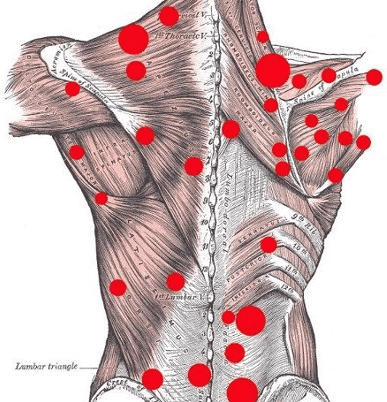
Have you been experiencing pain in different locations in your body? Do you have any areas of complaint that affect your daily lifestyle? Or do you have issues of stability and mobility when you are out and about? More often than not, approximately 25% of Americans are in some pain that can impact their lives and, if not treated right away, can cause the body to be dysfunctional. When there is constant pain in the body, it can cause overlapping risk profiles, known as myofascial pain syndrome. Myofascial pain syndrome is often defined as pain that originates along the musculoskeletal muscle groups and causes hyperirritable spots within the muscle fibers’ taut band, causing trigger points to develop. This means repetitive motions cause muscle strain and tightness along the muscle fibers when the body goes through repetitive movements daily.
When many people are dealing with myofascial pain syndrome, they would go to their primary doctor and explain that they are dealing with pain in different areas of their bodies, including their head, neck, shoulders, back, hips, etc. Afterward, their doctors conduct an examination to see where the issue is occurring. Many doctors often ask numerous questions to their patients about their daily activities before coming up with a diagnosis that myofascial pain syndrome is affecting their bodies. Studies reveal that the etiology of myofascial pain syndrome is not fully understood. Still, when the muscles, ligaments, and tissues are inflamed or undergo repetitive trauma, it can be accompanied by correlating conditions and disorders. To that point, doctors will work with their associated medical providers to develop a personalized treatment plan to diagnose and reduce myofascial pain syndrome associated with chronic conditions affecting the body.
How Does The Body React To Myofascial Pain Syndrome
Now when the body is dealing with myofascial pain syndrome, studies reveal that it can be a major health problem when it is not treated right away; it can cause the following:
Impaired mobility
Pain
Muscle hypersensitivity
Sleep issues
Neurological issues
According to “Myofascial Pain and Dysfunction: The Trigger Point Manual,” by Dr. Janet G. Travell, M.D., the book mentioned that when myofascial pain syndrome becomes aberrant, it can lead to a disorder known as myofascial pain modulation disorder. This means that when a person is dealing with trigger points in their bodies, it can distort their referred pain patterns when being diagnosed. Active trigger points normally project pain in different body locations, known as referred pain. However, with myofascial pain modulation disorder, the pain is not localized but aberrant, which causes distortion to the central nervous system and sends pain signals to cause structural damage to the affected muscles in the body.
An Overview Of Referred Pain- Video
Have you been experiencing pain in different locations in your body? Do you have mobility issues when turning your neck or hips? Do you feel like you are losing your quality of life? If you have been dealing with pain-like problems in your body, it could be due to myofascial pain syndrome causing these issues. Myofascial pain syndrome is when the body goes through repetitive motions or trauma that causes symptoms of muscle strain and stiffness that are correlated with referred pain. The video above explains what referred pain does to the body and how it can affect the muscles and the corresponding organs. This is known as somato-visceral dysfunction, where the muscles and the related vital organs are affected, causing pain. An example would be chest pain associated with cardiovascular issues that mimic a heart attack. Various treatments can now treat myofascial pain syndrome associated with trigger points that can reduce the localized pain affecting the body.
Various Treatments To Reduce Myofascial Pain Syndrome
Several available treatments can help the body and bring back a person’s quality of life when it comes to reducing pain-like symptoms associated with myofascial pain syndrome. As stated earlier, when a person is diagnosed with myofascial pain syndrome by their primary doctors, their doctors will work with other pain specialists, like physical therapists, massage therapists, and chiropractors, that can locate where the referred pain is in the body and alleviate the symptoms. This allows the treatment plan to be personalized and catered to the individual. When myofascial pain syndrome causes the muscles to become tight and stiff due to repetitive factors, the pain specialists work with the body to restore functionality and help loosen the muscles. Not only that, but many individuals would take up meditative practices to allow their bodies to relax and reduce future trigger points from developing. This will enable them to have a clear mind and be pain-free.
Conclusion
Myofascial pain syndrome is when the body has pain-like symptoms affecting different muscle groups. It can cause numerous symptoms associated with pain that can cause mobility and dysfunction in the individual. Since the body is a complex machine that incorporates various muscles, tendons, ligaments, and vital organs to maintain functionality, myofascial pain can cause referred pain to a different location of the body and can be a major health problem. However, available treatments can reduce the pain-like symptoms caused by myofascial pain syndrome. When doctors work with associated medical providers specializing in myofascial pain syndrome, they can develop a personalized treatment plan to reduce future pain-like symptoms associated with myofascial pain syndrome from causing more issues to the body and even reduce correlating conditions that overlap that trigger myofascial pain.
References
Cao, Qi-Wang, et al. “Expert Consensus on the Diagnosis and Treatment of Myofascial Pain Syndrome.” World Journal of Clinical Cases, U.S. National Library of Medicine, 26 Mar. 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8017503/.
Desai, Mehul J, et al. “Myofascial Pain Syndrome: A Treatment Review.” Pain and Therapy, U.S. National Library of Medicine, June 2013, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4107879/.
Jafri, M Saleet. “Mechanisms of Myofascial Pain.” International Scholarly Research Notices, U.S. National Library of Medicine, 2014, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4285362/.
Niddam, D M, et al. “Brain Structural Changes in Patients with Chronic Myofascial Pain.” European Journal of Pain (London, England), U.S. National Library of Medicine, Jan. 2017, https://pubmed.ncbi.nlm.nih.gov/27352085/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 2:the Lower Extremities. Williams & Wilkins, 1999.
When exercising, it is very important to warm each muscle group to prevent injuries from occurring when working out. Stretching the arms, legs, and back can loosen up stiff muscles and increase blood flow to allow each muscle fiber to warm up and allow maximum power when each set is performed. One of the best ways to reduce muscle fatigue or stiffness before working out is to foam roll each muscle group for at least 1-2 minutes max to provide optimal functionality. Foam rolling allows the muscles to warm up before an extensive workout session. Still, it can also offer many benefits when combined with other therapies to reduce pain-like symptoms like trigger point pain from causing further injuries from reoccurring in the body. Today’s article focuses on the benefits of foam rolling, how it reduces trigger point pain, and how it is combined with chiropractic care to achieve optimal health and wellness. We refer patients to certified providers incorporating techniques and therapies for individuals dealing with trigger point pain affecting different body areas. By locating where the trigger points are coming from, many pain specialists utilize a treatment plan to reduce the effects that trigger points are causing on the body while suggesting different tools, like using a foam roller to reduce pain in the other muscle groups. We encourage and appreciate each patient by referring them to associated medical providers based on their diagnosis when it is appropriate. We understand that education is a terrific way when asking our providers intricated questions at the patient’s request and understanding. Dr. Jimenez, D.C., only utilizes this information as an educational service. Disclaimer
The Benefits Of Foam Rolling
Have you been dealing with pain-like symptoms in different parts of your body? Do you feel stiffness in your muscles? Or have you been feeling exhausted throughout the entire day? Many people often feel stressed, overworked, and exhausted after a long day and need to find different ways to relieve stress. Whether going to the gym to work out or yoga class, many people should warm up for about 5-10 minutes to work out each muscle group to reduce muscle fatigue and stiffness. One of the tools that people should utilize is using a foam roller. Studies reveal that foam rolling before working out can improve muscle performance and flexibility and, at the same time, alleviate muscle fatigue and soreness.
Incorporating foam rolling as part of your warm-up can prevent issues like trigger point pain from causing more problems in the affected muscle group and causing more harm. Foam rolling has been known as a self-myofascial release (SMR) tool for many athletic people to relieve delay-onset muscle soreness (DOMS) and can help the recovery process for muscular performance. Studies show that when athletes have DOMS, their muscles are tender and stiff that which causes restricted movement. By foam rolling, each sore muscle group can get rolled out on a dense foam roll from the person’s body weight to apply pressure on the soft tissue. When performed correctly, the body’s range of motion will increase, and soft tissue restriction is prevented.
Foam Rolling To Reduce Trigger Point Pain
When the body has been overworked, the muscle fibers will start to overstretch and cause various issues in different body parts. When this happens, tiny, hard nodules form over time and cause referred pain to other body locations in each muscle group. This is known as myofascial pain syndrome or trigger points. Studies reveal that trigger point pain is when the affected muscles are either acute or chronic and cause pain in the surrounding connective tissues. Dr. Travell, M.D.’s book, “Myofascial Pain and Dysfunction,” mentioned that myofascial pain could cause somato-visceral dysfunction in the body as the affected muscles and nerves are correlated with the corresponding vital organs. This means that if someone is dealing with back pain, it could be an issue with their gut system. Now how does foam rolling help prevent trigger point pain? As mentioned earlier, foam rolling each muscle group can alleviate muscle soreness and improve blood circulation. Studies reveal that foam rolling on the muscle group affected by trigger point pain can increase blood flow to the affected muscle and reduce fascial inflammation in the body.
What Foam Rolling Does To The Body- Video
Have you been dealing with muscle soreness? Do you feel like you are constantly bending over or shuffling your feet? Or have you been experiencing constant aches and pains when stretching? If you have been dealing with these musculoskeletal issues, why not incorporate foam rolling as part of your routine? Many individuals have some pain that is affecting their muscles that is causing them pain. Regarding reducing pain, incorporating foam rolling on the affected muscles can increase blood flow to the muscle and reduce any symptoms associated with chronic conditions. Studies reveal that the combination of foam rolling and stretching before working out can provide these amazing benefits, which include the following:
Ease muscle pain
Increase range of motion
Reduce cellulite
Relieve back pain
Relive trigger points in muscles
The video above gives an excellent explanation of what foam rolling does to the body and why it provides relief to those different muscle groups. When people merge foam rolling with other treatments, it can benefit their health and wellness.
Foam Rolling & Chiropractic Care
As stated earlier, other various treatments can combine foam rolling to promote a healthy body. One of the treatments is chiropractic care. Chiropractic care incorporates mechanical and manual manipulation of the spine, especially in subluxation or spinal misalignment. When the spine is misaligned, it can cause muscle strain and mobility issues that can affect the body over time. So how does foam rolling play a part in chiropractic care? Well, a chiropractor or doctor of chiropractic can develop a plan to help manage the pain while treating the condition affecting the body. Since foam rolling is utilized in a warm-up session in association with physical therapy, many individuals who work with a personal trainer can incorporate foam rolling as part of their warm-up to loosen up stiff muscles and go to regular chiropractic treatments to improve muscle strength, mobility, and flexibility.
Conclusion
There are many beneficial properties that foam rolling can provide to the body. Foam rolling can allow blood circulation to the muscles while reducing muscle fatigue and soreness. Incorporating foam rolling as part of a daily warm-up can also prevent trigger points from forming in the muscle groups and can work out the tight knots that the muscle has occurred. At the same time, treatments like chiropractic care and physical therapy can combine foam rolling to promote health and wellness in the body and prevent muscle pain.
References
Konrad A, Nakamura M, Bernsteiner D, Tilp M. The Accumulated Effects of Foam Rolling Combined with Stretching on Range of Motion and Physical Performance: A Systematic Review and Meta-Analysis. J Sports Sci Med. 2021 Jul 1;20(3):535-545. doi: 10.52082/jssm.2021.535. PMID: 34267594; PMCID: PMC8256518.
Pagaduan, Jeffrey Cayaban, et al. “Chronic Effects of Foam Rolling on Flexibility and Performance: A Systematic Review of Randomized Controlled Trials.” International Journal of Environmental Research and Public Health, U.S. National Library of Medicine, 4 Apr. 2022, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8998857/.
Pearcey, Gregory E P, et al. “Foam Rolling for Delayed-Onset Muscle Soreness and Recovery of Dynamic Performance Measures.” Journal of Athletic Training, U.S. National Library of Medicine, Jan. 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4299735/.
Shah, Jay P, et al. “Myofascial Trigger Points Then and Now: A Historical and Scientific Perspective.” PM & R : the Journal of Injury, Function, and Rehabilitation, U.S. National Library of Medicine, July 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4508225/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 2:the Lower Extremities. Williams & Wilkins, 1999.
Wiewelhove, Thimo, et al. “A Meta-Analysis of the Effects of Foam Rolling on Performance and Recovery.” Frontiers in Physiology, U.S. National Library of Medicine, 9 Apr. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6465761/.
Everyone worldwide knows that feet are important. The feet allow many individuals to run, walk, or jog for long periods without feeling pain for a moderate amount of time. To that point, the various muscles and tendons surrounding the foot provide full body flexion, extension, and stability. Even though it is very easy to get in the recommended amount of steps into being healthy, around 75% of individuals will have foot pain that can impact their ability to walk. One of the most common foot pains is plantar fasciitis, which can become a painful foot condition if it is not treated as soon as possible. Today’s article looks at plantar fasciitis, its symptoms, how trigger points correlate, and treatments for it. We refer patients to certified providers incorporating techniques and therapies for individuals dealing with plantar fasciitis. By locating where the trigger points are coming from, many pain specialists can develop a treatment plan to reduce the effects that plantar fasciitis is causing on the feet. We encourage and appreciate each patient by referring them to associated medical providers based on their diagnosis when it is appropriate. We understand that education is a terrific way when asking our providers intricated questions at the patient’s request and understanding. Dr. Jimenez, D.C., only utilizes this information as an educational service. Disclaimer
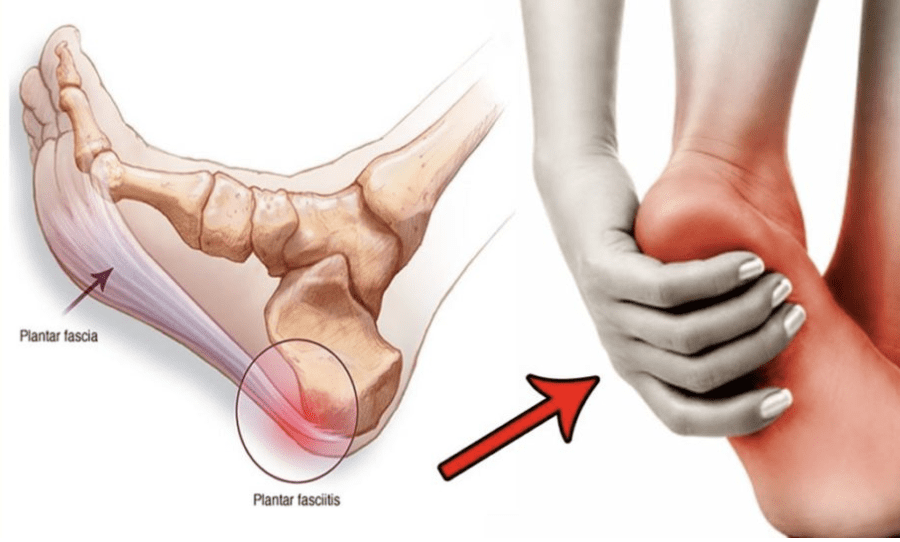
What Is Plantar Fasciitis?
Have you been dealing with constant heel pain? Do you feel pain shooting up your leg when you step or walk? Or do you feel a stabbing ache in your heel? Many of these pain issue people are dealing with correlate with plantar fasciitis. Studies reveal that plantar fasciitis results from degenerative irritation on the plantar fascia and its ligaments. This causes the muscle ligaments to become inflamed, swollen, and weak, which then causes the bottom of the foot or heel to hurt when a person is walking or standing. To that point, when there is a repetitive strain on the feet, it causes microtears in the plantar fascia. The plantar fascia in the foot plays an important role as it comprises three segments that support the medial arch and shock absorption when stepping down. As one of the most common causes of heel pain, the residual pain from plantar fasciitis tends to be a sharp, stabbing sensation. Plantar fasciitis is more prominent in middle-aged people. Still, anyone at any age can develop plantar fasciitis, especially if they have labor jobs requiring them to be constantly on their feet.
Symptoms Of Plantar Fasciitis
Since around 2 million Americans could potentially develop plantar fasciitis, it is important to know that when a person has been on their feet constantly, there will be inflammation along the tissues in the feet. Many individuals with a busy lifestyle that requires them to be on their feet frequently would often ignore the pain or discomfort. Some of the symptoms that plantar fasciitis causes include the following:
Pain on the bottom of the heel
Pain in the arch
Pain that is usually worse when waking up
Pain that increases over months
Swelling on the bottom of the heel
However, when the pain becomes overbearing, many people would often think they have sore feet or low back pain from being overly tired from work, under constant stress, or over-exerting their bodies. When this happens, many would think the pain would go away in a few days after resting for a short period.
Trigger Points Associated With Plantar Fasciitis
Now many individuals would often think that plantar fasciitis just only affects the heels, however, it can affect any part of the structure of the foot since all the surrounding muscle tissues are at risk of inflammation. When people start to ignore the pain and discomfort that plantar fasciitis is causing on the feet, it can overlap and develop trigger points in other areas of the body:
Ankles
Knees
Hips
Lower back
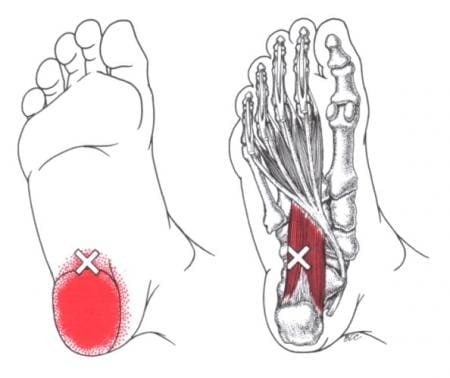
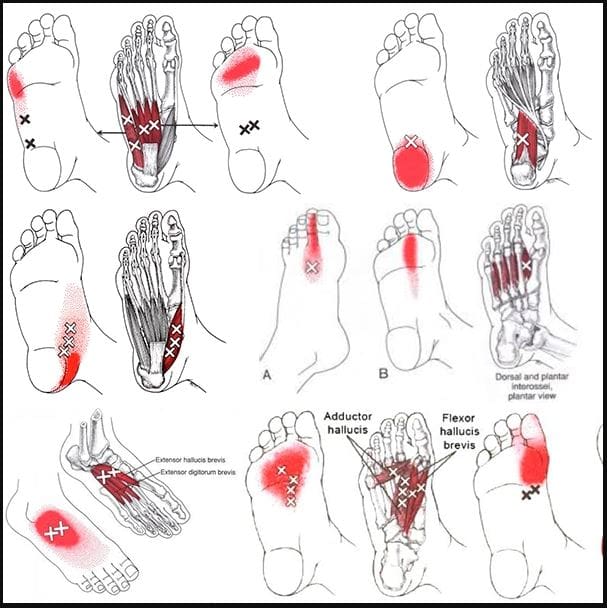
Studies reveal that trigger points or myofascial pain syndrome are hard, discrete, small nodules that are along the taut musculoskeletal band that causes numerous issues like inflammation, hypersensitivity, and pain to the affected muscle groups in the body. According to “Myofascial Pain and Dysfunction” written by Dr. Travell, M.D., it mentions that when the deep intrinsic muscles that work with the plantar fascia are affected by trigger points, would cause symptoms of numbness and the feeling of swelling in the foot. This causes many people to have limited mobility and have intense pain when walking, which can negatively impact their lifestyle.
An Overview Of Plantar Fasciitis- Video
Have you been dealing with aching feet? Do you feel a sharp, radiating pain in your feet? Or do you have difficulty walking? Many often think they are dealing with sore feet or other issues causing them pain. Around 75% of Americans often have foot pain affecting their ability to walk, and one of them is plantar fasciitis. The video above explains plantar fasciitis and how it can affect the feet. When the plantar fascia tendons become overused, it causes micro-tears in the muscle ligaments. When added compressive force starts to push against the heel boner, it can lead to a pathological state whereby the plantar fascia degenerates and creates dysfunction and pain. When this happens, it can lead to other conditions like trigger point pain along the muscle fibers in the foot. The pain and tenderness caused by trigger points in the plantar muscles may mask as plantar fasciitis. To that point, when plantar fasciitis becomes an issue and causes the individual to be in immense pain, it can become problematic. As luck would have it, treatments are available to reduce the pain from plantar fasciitis.
Treatments For Plantar Fasciitis
When treating plantar fasciitis, many available treatments can reduce the inflammatory effects in the heel and prevent trigger points from coming back. One of the available treatments is chiropractic care. Chiropractic care is an alternative treatment option to prevent, diagnose, and treat numerous injuries and conditions associated with the spine, primarily subluxations or spinal misalignments. Chiropractic focuses on restoring and maintaining the overall health and wellness of the musculoskeletal and nervous systems through spinal manipulation and adjustments. A chiropractor can carefully re-align the spine, improving a patient’s strength, mobility, and flexibility. Regarding plantar fasciitis, chiropractic care can work with other treatments, including physical therapy, massage, and even injections, to manage the pain and treat the condition. Even though plantar fasciitis takes several months to heal, chiropractic care can involve a precise technique that involves adjustments to the feet, ankles, and spinal alignment. This provides several benefits, which include the following:
Reduces Stress in the Plantar Fascia
Promotes Healing
Provides Effective Pain Management
Reduces the Risk of Further Injury
Conclusion
As many individuals worldwide are on their feet constantly, foot pain can hinder one’s ability to move. One of the most common foot pain is plantar fasciitis which can correlate with trigger points along the various muscles of the foot. Plantar fasciitis results from degenerative irritation on the plantar fascia and its ligaments, which causes sharp, stabbing pain on the heel. When this happens, it can cause the heel to be inflamed, swollen, and weak. To that point, it causes instability and pain when walking. However, plantar fasciitis can be treated when it is caught early through various treatments like chiropractic care. Chiropractic care can reduce the stress in the plantar fascia and help reduce the risk of further injuries. Combined with other therapies, many people can function normally and regain their walking ability without pain.
References
Buchanan, Benjamin K, and Donald Kushner. “Plantar Fasciitis – StatPearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 30 May 2022, https://www.ncbi.nlm.nih.gov/books/NBK431073/.
Petrofsky, Jerrold, et al. “Local Heating of Trigger Points Reduces Neck and Plantar Fascia Pain.” Journal of Back and Musculoskeletal Rehabilitation, U.S. National Library of Medicine, 2020, https://pubmed.ncbi.nlm.nih.gov/31594202/.
Shah, Jay P, et al. “Myofascial Trigger Points Then and Now: A Historical and Scientific Perspective.” PM & R : the Journal of Injury, Function, and Rehabilitation, U.S. National Library of Medicine, July 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4508225/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 2:the Lower Extremities. Williams & Wilkins, 1999.
The various muscles and tendons surrounding the foot play an important role as they provide stability to the lower parts of the body and allow the individual to move and flex their feet. These various muscles and tendons help support the ankles and allow leg movement. Many people will be on their feet constantly as the world moves and sometimes have to deal with various issues affecting their walking ability. As the body naturally ages, many people will shuffle their feet around, which causes strain on the foot muscles and can affect the calves and legs over time. To that point, it can lead to foot pain and other conditions that can affect the individual. Other issues that can affect the feet and their muscles could be incorrect footwear, how they are standing, or how they walk. When this happens, conditions like plantar fasciitis and trigger point pain can affect the feet differently. Today’s article focuses on the superficial intrinsic foot muscles, how trigger points and plantar fasciitis correlate with foot pain, and how to strengthen the foot muscles. We refer patients to certified providers incorporating techniques and therapies in the lower body extremities of trigger points affecting the feet. This helps many people with trigger point pain symptoms associated with plantar fasciitis along the intrinsic foot muscles. We encourage and appreciate each patient by referring them to associated medical providers based on their diagnosis when it is appropriate. We understand that education is a terrific way to ask our providers intricated questions at the patient’s request and understanding. Dr. Alex Jimenez, D.C., only utilizes this information as an educational service. Disclaimer
The Superficial Intrinsic Foot Muscles
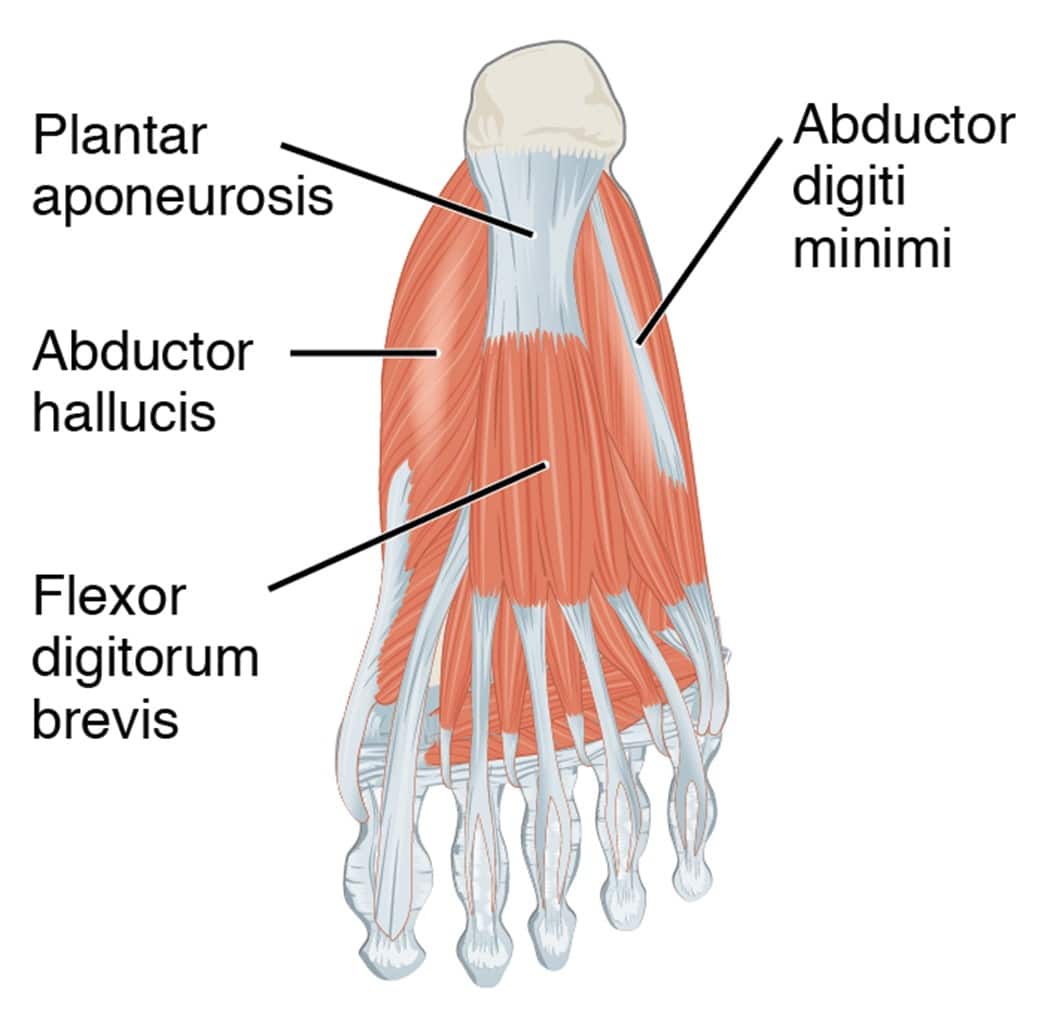
As stated earlier, the foot has various muscles and tendons that allow stability to the ankles and allow movement when a person is walking. The foot has two muscle groups: the extrinsic and intrinsic muscles. Today, we will look at the intrinsic foot muscles and their importance to the foot. Studies reveal that the intrinsic foot muscles are highly important as they are contained to the foot and contribute to supporting the medial longitudinal arch. The intrinsic foot muscles are superficial and help keep the toes straight while providing flexion and extension when in motion. The foot has about 29 muscles, including 10 surrounding the foot and ankle, while the other 19 are intrinsic and provide the roles for gait and posture. The 19 intrinsic muscles have the following:
Abductor Hallucis
Quadratus Plantae
Flexor Hallucis Brevis
Flexor Digitorum Brevis
Abductor Digiti Minimi
Flexor Digiti Minimi
The Interossei Muscles
The Lumbricals
These muscles allow individuals to walk, run, or jog without pain. However, when the intrinsic muscles become impaired, studies reveal that intrinsic foot muscle function could be linked to various foot conditions that affect a person’s walking ability.
How Does Foot Pain Correlate With Plantar Fasciitis & Trigger Points?
Studies reveal that foot pain can cause an unpleasant sensory and emotional experience. Many factors can affect how a person walks, leading to various issues affecting the mobility of the lower extremities. When multiple problems affect a person’s walking, the intrinsic muscle and other muscles surrounding the ankle and foot could become strained and overlap with other foot conditions. Coexisting muscle impairments could affect the alignment, motion, load distribution, and muscle performance that involves the legs when foot pain affects the intrinsic foot muscles. When these impairments cause foot pain, it can correlate with trigger points and conditions like plantar fasciitis, affecting a person’s walking ability. But how does foot pain connect with plantar fasciitis and trigger points?
According to Dr. Travell, M.D.’s book “Myofascial Pain and Dysfunction,” when tension starts to overload the foot, the intrinsic muscles develop tiny nodules in the muscle fibers and reduce the muscle strength of the medial arch. To that point, it can collapse and cause the foot to create inflammation associated with repetitive actions that cause plantar fasciitis in the feet. When this happens, it can affect a person’s ability to walk, run, and stand and affect the lower extremities’ mobility. If not treated right away, it can cause muscle and joint pain in the hips, legs, knees, and lower back.
An Overview Of The Intrinsic Foot Muscles-Video
Have you been dealing with issues on your feet? Do you find it difficult to step down or walk? Or have you been rubbing your feet constantly to reduce the soreness in your feet? Many of these issues correlate with trigger points affecting the intrinsic foot muscles that could cause foot issues like plantar fasciitis. The foot has various muscles, like the intrinsic muscles, that allow gait and stability to the body. Multiple factors affecting the intrinsic foot muscles can lead to instability, muscle strain, tendon stress, and muscle and joint pain. This can affect how a person moves throughout the day and their quality of life. The video above explains where each muscle is, which ones are extrinsic and intrinsic, and how each muscle helps with foot function. When various issues begin to affect the foot and cause mobility issues, multiple techniques are available to help strengthen the foot muscles and prevent future problems from affecting the feet.
Strengthening The Foot Muscles
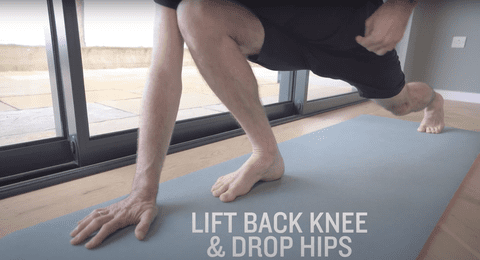
Regarding trigger point pain affecting the intrinsic foot muscles, various techniques can reduce the pain-like symptoms of trigger points and prevent foot issues like plantar fasciitis from re-occurring. Studies reveal that light, non-weight-bearing exercises like cycling and swimming can minimize muscle overload on the foot. Other ways to strengthen the intrinsic foot muscles are by stretching the toe flexors to help improve stability and prevent hypermobility in the foot. Different techniques to reduce trigger points in the foot’s muscle fibers include using a cylindrical or spherical object and rolling under the arches to massage and loosen stiff muscles. Many of these techniques could help restore foot functionality and stability while reducing future issues like plantar fasciitis in the feet. To that point, people should be allowed to walk pain-free again.
Conclusion
The foot has 29 muscles, including ten extrinsic muscles surrounding the foot and ankle and 29 intrinsic muscles on the foot. The intrinsic muscles are highly important for foot functionality as they are superficial and contribute to supporting the medial longitudinal arch. The intrinsic foot muscles also help keep the toes straight and allow flexion and extension when in motion. These muscles also help a person walk and stabilize the ankle. When various factors affect a person’s walking ability, it can lead to muscle strain and tendon stress to the foot, developing trigger points in the intrinsic muscle fibers and causing pain. This could cause foot conditions like plantar fasciitis and other co-existing muscle impairments that can affect the lower extremities’ mobility while causing muscle and joint pain in the hips, legs, knees, and lower back. Luckily, available techniques can help massage, stretch, and strengthen the intrinsic foot muscles while reducing trigger points and preventing their associated symptoms from recurring. To that point, these techniques can allow many individuals to walk without feeling pain.
References
Card, Ryan K, and Bruno Bordoni. “Anatomy, Bony Pelvis and Lower Limb, Foot Muscles.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 27 Feb. 2022, https://www.ncbi.nlm.nih.gov/books/NBK539705/.
Gooding, Thomas M, et al. “Intrinsic Foot Muscle Activation during Specific Exercises: A T2 Time Magnetic Resonance Imaging Study.” Journal of Athletic Training, U.S. National Library of Medicine, Aug. 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5094843/.
Hawke, Fiona, and Joshua Burns. “Understanding the Nature and Mechanism of Foot Pain.” Journal of Foot and Ankle Research, U.S. National Library of Medicine, 14 Jan. 2009, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2631512/.
Hayter, Matt. “Why Do We Need the Intrinsic Muscles of the Foot? [Guide 2022].” Dynamic Podiatry, 2022, https://foothealthguy.com/hammer-toes-causes-and-treatment/
Lim, Ang Tee, et al. “Management of Plantar Fasciitis in the Outpatient Setting.” Singapore Medical Journal, U.S. National Library of Medicine, Apr. 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4853481/.
Soysa, Achini, et al. “Importance and Challenges of Measuring Intrinsic Foot Muscle Strength.” Journal of Foot and Ankle Research, U.S. National Library of Medicine, 26 Nov. 2012, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3544647/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 2:the Lower Extremities. Williams & Wilkins, 1999.
There is a multitude of reasons why back muscles tighten and stiffen up. Muscles pull the bones and joints. Overuse and/or injuries can pull the bones, joints, and tendons out of place, thus causing the muscles to stay in a flexed or stretched position, the inability for the muscles to relax and return to their normal position, resulting in symptoms of discomfort, stiffness, and pain. Individuals can have reoccurring bouts of tight muscles, eventually becoming chronic. Chronic muscle tension can pull the spine out of alignment even if there is no specific injury. The Injury Medical Chiropractic and Functional Wellness Team can relieve tight back muscle tension and restore positioning, mobility, and function.
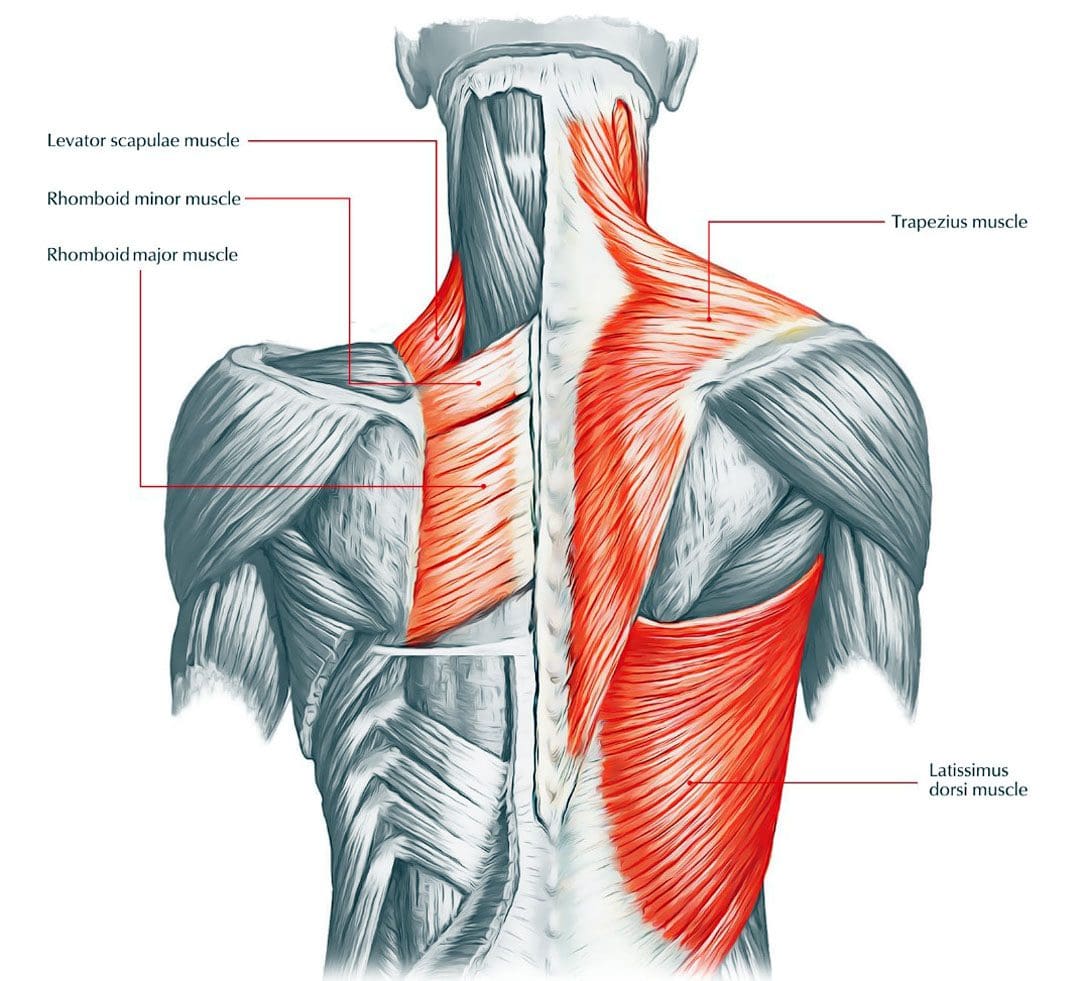
Muscles are the Key
Muscles make the body move and greatly impact the skeletal and nervous systems. When a muscle is overstretched or pulled, there is not just injury to the muscles but the potential for injury to the bones and tendons in the area. This, in turn, can pinch nerves and cause problems with the nervous system, especially in pain signal transmissions.
Symptoms
Symptoms will depend on the cause and severity. The most common include:
Constant or chronic muscle achiness, soreness, stiffness, and tightness.
Even after stretching or flexing, there is a dull aching or pain.
More serious symptoms may include:
Electrical or burning sensations
Sharp or stabbing pain.
Weakness in the legs or arms
Tingling or numbness in the legs, arms, or chest.
Chest discomfort symptoms.
Causes
Aging
The older a person is, the more likely they will experience back discomfort symptoms. Back issues most likely occur in 30- to 50-year-olds.
The aging process naturally wears the body.
Thinning bones
Muscle mass reduction
Fluid loss between joints in the spine.
All these can cause back issues and problems.
Unhealthy posture
Constant pressure on the spine can lead to general back discomfort symptoms. Practicing unhealthy posture can generate this pressure. The muscles and ligaments must work harder to keep the body balanced because the muscles are out of position, and the other muscles can’t perform their job properly. Overworking and overuse lead to tight back muscles, aches, and pain.
Muscle sprain or strain
Sprains are the tearing or stretching of ligaments. Strains are the tearing or stretching of muscles and tendons. Lifting heavy objects without proper form can easily cause a back sprain or strain. Sprains and strains can also occur after an awkward, sudden, or jerking movement.
Herniated disc
A herniated, slipped, or ruptured disc puts pressure on a nerve/s. This can stress the surrounding muscles causing tension to build up.
Fall or other injuries
Tight back muscles can result from the following:
A fall
Vehicle accident
Force Trauma
Sports accident
Weight gain
Added weight stresses and pulls the body down. This causes unhealthy posture and muscle tension.
Chiropractic Functional Wellness
Usually, tight muscles can be relieved with a hot bath or cold therapy. Reoccurring bouts of, or chronically tense back muscles, are signals that something is wrong and should not be ignored. Chiropractic care can release and relax tight back muscles and get them back into a natural state by re-aligning the spine through tissue manipulation, decompression, massage, and adjustments. The various treatment methods will relieve the discomfort, pain, tension, and realign the spinal column, and strengthen the body. When spinal components are put back into their proper place, the surrounding muscles no longer need to provide a counter-balance to the misalignment and begin to relax. Chiropractors can also recommend ways to improve posture and strengthen muscles to incur less wear and tear.
Chiropractic Back Therapy
References
Furlan, Andrea D et al. “Complementary and alternative therapies for back pain II.” Evidence report/technology assessment,194 (2010): 1-764.
Geneen, Louise J et al. “Physical activity and exercise for chronic pain in adults: an overview of Cochrane Reviews.” The Cochrane database of systematic reviews vol. 4,4 CD011279. 24 Apr. 2017, doi:10.1002/14651858.CD011279.pub3
Mayo Clinic Staff. (2017). Back pain: Symptoms. mayoclinic.org/diseases-conditions/back-pain/basics/symptoms/con-20020797
Miake-Lye, Isomi M et al. “Massage for Pain: An Evidence Map.” Journal of alternative and complementary medicine (New York, N.Y.) vol. 25,5 (2019): 475-502. doi:10.1089/acm.2018.0282
Nahian, Ahmed, et al. “Osteopathic Manipulative Treatment: Facial Muscle Energy, Direct MFR, and BLT Procedure – for TMJ Dysfunction.” StatPearls, StatPearls Publishing, 12 September 2022.
Rahman Shiri, Jaro Karppinen, Päivi Leino-Arjas, Svetlana Solovieva, Eira Viikari-Juntura, The Association Between Obesity and Low Back Pain: A Meta-Analysis, American Journal of Epidemiology, Volume 171, Issue 2, 15 January 2010, Pages 135–154, https://doi.org/10.1093/aje/kwp356
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine

 IBD Back Pain
IBD Back Pain
 Posture Adjustments
Posture Adjustments







 Muscles are the Key
Muscles are the Key





