In cold weather, it’s normal to experience cold hands and fingers. But if there is a coldness in only one finger while the rest of the hand is normal, changes to skin color, numbness, tingling, or pain symptoms could be a sign of poor circulation or an underlying medical condition. Cold fingers could indicate various problems, including overuse injuries, vitamin deficiencies, Raynaud’s syndrome, hypothyroidism, anemia, arterial disease, or an autoimmune condition. Chiropractic care and massage therapy can increase circulation, release compressed nerves, relax the muscles, and restore mobility and function.
Cold Fingers
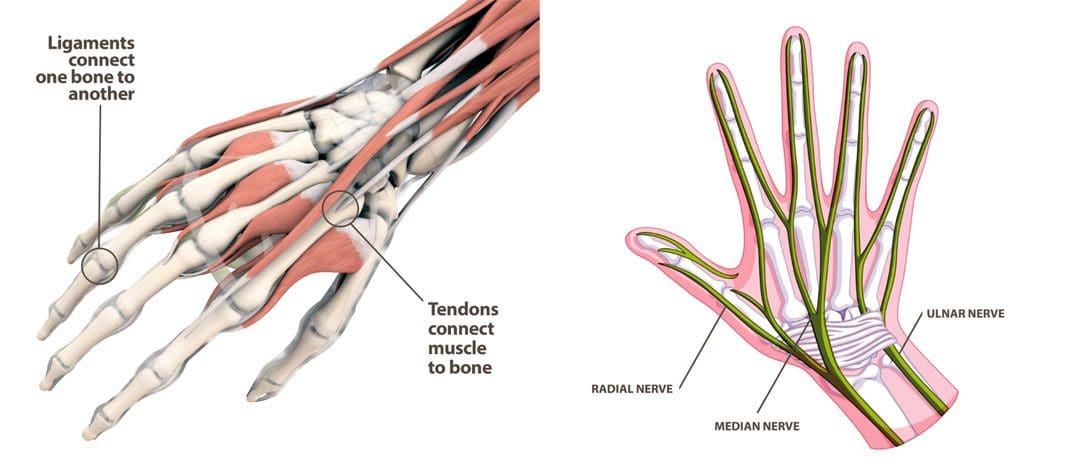
Blood circulates throughout, nourishing and maintaining body warmth. When compression, obstructions, or narrowing paths inhibit blood flow, the body cannot achieve proper circulation. Unhealthy circulation can cause several symptoms, including:
Pins and needles sensations along the shoulder, arm, hand, and fingers.
Weakened arm and hand muscles.
Numbness.
Cold finger/s.
Muscles aches, soreness, and tightness.
Swelling.
Pale or bluish skin color.
Overuse Injury
Repeating one movement or motion constantly over time can lead to overuse syndrome/repetitive motion disorder in the hands and arms. Certain jobs and activities can cause overuse syndrome, including:
Cashiers.
Food service work.
Graphic sign work.
Computer work.
Sewing work.
Landscaping.
All of these jobs and activities can put a lot of repeated stress on the hands and arms.
Vitamin B-12 Deficiency
Vitamin B-12 is required for proper red blood cell formation and neurological function. It is found in many foods, including eggs, fish, meat, poultry, and dairy products. A vitamin B-12 deficiency can cause neurological symptoms like numbness, tingling, and coldness in the hands and feet. Other symptoms include:
Anemia
Fatigue
Weakness
Difficulty maintaining balance
Depression
Soreness of the mouth
A doctor requires a blood sample to test for the deficiency. A common treatment is a high dose of an oral supplement or injections for individuals that have difficulties absorbing B-12 through the digestive tract.
Raynaud’s Syndrome
Raynaud’s syndrome is a condition that causes some areas of the body, usually the fingers, to feel cold and numb when exposed to cold temperatures or high-stress levels. This happens because the small arteries that supply blood to the skin are experiencing spasms. During an episode, the arteries narrow, which prevents blood from circulating correctly. The fingers can change color, going from white to blue to red. When the flare-up ends, and the blood flow returns to normal, there may be tingling, throbbing, or swelling. The condition isn’t usually debilitating, and treatment options often include medications that expand the blood vessels to improve circulation. These include calcium channel blockers,alpha-blockers, and vasodilators.
Hypothyroidism
Hypothyroidism is when the thyroid doesn’t produce enough hormones. Hypothyroidism comes on gradually and rarely generates symptoms in the early stages. Hypothyroidism doesn’t cause cold fingers but increases the body’s sensitivity to cold. Other symptoms include:
Fatigue
Muscle weakness, tenderness, and achiness.
Joint swelling, stiffness, and pain.
Puffiness.
Dry skin.
Hoarseness.
Weight gain.
High or elevated cholesterol levels.
Thinning hair and hair loss.
Depression.
Over time, the condition can cause complications such as obesity, joint pain, heart disease, and infertility. A doctor can detect hypothyroidism with a simple blood test. Treatment involves taking a daily dose of synthetic thyroid hormone.
Anemia
Anemia is when the blood has a lower-than-normal amount of red blood cells. It also occurs when the red blood cells lack a crucial iron-rich protein called hemoglobin. Hemoglobin assists red blood cells in delivering oxygen from the lungs to the rest of the body. A low supply of hemoglobin to carry oxygen to the hands can result in cold fingers. There may also be fatigue and weakness. Iron deficiency is what typically causes most cases. A doctor may suggest nutritional adjustments if blood work indicates low iron levels. An iron-rich nutritional plan and taking iron supplements can help relieve symptoms.
Arterial Diseases
Diseases that affect the arteries can reduce blood flow to the hands, causing cold fingers. This can be from plaque buildup or inflammation in the blood vessels. Any blockage in the blood vessels can prevent blood from circulating normally. Another arterial problem is primary pulmonary hypertension, which affects the lungs’ arteries and can lead to Raynaud’s syndrome.
Chiropractic Care
Chiropractic adjustments can remove misalignments, restore proper nerve communication, increase blood flow, and correct an overactive sympathetic nervous system. Massaging the shoulders, arms, and hands relaxes the nerves, and muscles, breaks up compressed tissues, and increase blood flow. The circulation of lymphatic fluid around the body is also promoted, which carries toxins away from the muscles and tissues. To improve circulation, the following may be utilized:
Deep tissue pressure is effective at relieving congestion and tension.
Percussive massage to break up scar tissue.
Non-surgical Decompression to stretch the spine and body out.
Lymphatic drainage is designed to improve the circulation of the fluid.
Bilić, R et al. “Sindromi prenaprezanja u saci, podlaktici i laktu” [Overuse injury syndromes of the hand, forearm and elbow]. Arhiv za higijenu rada i toksikologiju vol. 52,4 (2001): 403-14.
Ernst, E. “Manual therapies for pain control: chiropractic and massage.” The Clinical journal of pain vol. 20,1 (2004): 8-12. doi:10.1097/00002508-200401000-00003
InformedHealth.org [Internet]. Cologne, Germany: Institute for Quality and Efficiency in Health Care (IQWiG); 2006-. How does the blood circulatory system work? 2010 Mar 12 [Updated 2019 Jan 31]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK279250/
Pal, B et al. “Raynaud’s phenomenon in idiopathic carpal tunnel syndrome.” Scandinavian journal of rheumatology vol. 25,3 (1996): 143-5. doi:10.3109/03009749609080004
Waller, D G, and J R Dathan. “Raynaud’s syndrome and carpal tunnel syndrome.” Postgraduate medical journal vol. 61,712 (1985): 161-2. doi:10.1136/pgmj.61.712.161
Dr. Alex Jimenez, D.C., presents how chronic stress can impact the body and how it is correlated with inflammation in this 2-part series. Part 1 examined how stress correlates with various symptoms affecting the body’s gene levels. Part 2 looks at how inflammation and chronic stress correlate with the various factors that can lead to physical development. We refer our patients to certified medical providers who provide available treatments for many individuals suffering from chronic stress associated with the cardiovascular, endocrine, and immune systems affecting the body and developing inflammation. We encourage each of our patients by mentioning them to associated medical providers based on their analysis appropriately. We understand that education is a delightful way when asking our providers questions at the patient’s request and understanding. Dr. Jimenez, D.C., only uses this information as an educational service. Disclaimer
How Stress Can Impact Us?
Dr. Alex Jimenez, D.C., presents: Stress can create many emotions that can hugely impact many of us. Whether it is anger, frustration, or sadness, stress can make anyone reach a breaking point and cause underlying conditions that can develop into cardiovascular issues. So those people with the highest level of anger, when you look at the cardiovascular literature, have the least probability of survival. Anger is a bad player. Anger causes arrhythmia. This study looked at, now that we have people with ICDs and defibrillators, we can monitor these things. And we see that anger can trigger ventricular arrhythmias in patients. And it’s easy now to follow, with some of our technology.
Anger has been linked to episodes of atrial fibrillation. When you think about it, it’s adrenaline outpouring into the body and causing coronary constriction. It’s increasing the heart rate. All of these things can lead to arrhythmia. And it doesn’t have to be AFib. It can be APCs and VPCs. Now, some very interesting research has come out about telomerase and telomeres. Telomeres are little caps on the chromosomes, and telomerase is the enzyme linked to telomere formation. And now, we can understand through the language of science, and we’re starting to use technology and use science in a way that we could never do before to understand the impact of stress on telomeres and telomerase enzymes.
The Factors That Lead Up To Chronic Stress
Dr. Alex Jimenez, D.C., presents: So one of the key people to study this is the Nobel Prize-winning, Dr. Elizabeth Blackburn. And what she said is that this is a conclusion, and we’ll come back to some of her other studies. She tells us that the telomeres of babies from women in utero had a lot of stress or were even shorter in young adulthood compared to mothers who did not have the same stressful situations. Maternal psychological stress during pregnancy may exert a programming effect on the developing telomere biology system that is already apparent at birth as reflected by the setting of newborn leukocyte telemetry length. So children can come in imprinted, and even if they do, this can be transformed.
What about racial discrimination these boxes here show high racial discrimination leading to low telomere length, which most of us have ever thought about. So, shorter telomere length leads to an increased risk of cancer and overall mortality. Cancer incidence rates are 22.5 per 1000 person-years in the shortest telomere group, verse 14.2 in the middle group, and 5.1 in the longest telomere group. Shorter telomeres can lead to instability of the chromosome and result in cancer formation. So, now we understand, through the language of science, the impact of stress on the telomerase enzyme and the telomere length. According to Dr. Elizabeth Blackburn, 58 premenopausal women were caregivers of their chronically ill children verse women who had healthy children. The women were asked how they perceive stress in their lives and whether it impacts their health by affecting their cellular aging.
That was the question of the study as they looked at telomere length and telomerase enzyme, and this is what they found. Now, the keyword here is perceived. We are not to judge each other’s stress. Stress is personal, and some of our responses may be genetic. For example, someone who has homozygous comps with a sluggish gene may have much more anxiety than someone who doesn’t have this genetic polymorphism. Someone who has an MAOA in an MAOB may have more anxiety than someone who doesn’t have that genetic polymorphism. So there is a genetic component to our response, but what she found was perceived psychological stress. And the number of years caring for chronically ill children was associated with shorter telomere length and less telomerase activity, providing the first indication that stress can impact telomere maintenance and longevity.
How To Transform Our Stress Response?
Dr. Alex Jimenez, D.C., presents: That’s powerful, and many healthcare providers are under some form of stress. And the question is, what can we do to transform our response? Framingham also looked at depression and identified clinical depression as a bigger risk for cardiovascular events and poor outcomes than smoking, diabetes, high LDL, and low HDL, which is crazy because we spend all of our time on these things. Yet, we don’t spend much time dealing with the emotional aspects of vascular disease. This is affected depression, inventory, a simple screening test for depression, looking at people with high levels of depression versus low levels of depression. And you can see that as you go from the low to the highest level, as you work your way through, the chance of survival becomes less.
And many of us have our theories as to why this occurs. And is it because if we are depressed, we don’t say, “Oh, I’m going to eat some brussels sprouts, and I’m going to take those B vitamins, and I’m going to go out and exercise, and I’m going to do some meditation.” So post-MI independent risk factor for an event is depression. Our mindset regarding depression makes us incapable of functioning normally and can make our bodies develop issues that affect our vital organs, muscles, and joints. So, depression is a big player, as 75% of post-MI deaths are related to depression, right? So looking at patients, now, you have to ask the question: Is it the depression causing the problem, or is it the cytokine sickness that’s already led to the heart disease causing the depression? We have to factor all of this in.
And yet another study looked at over 4,000 people with no coronary disease at baseline. For every increase of five points on the depression scale, that increased risk by 15%. And those with the highest depression scores had a 40% higher coronary artery disease rate and a 60% higher death rate. So mostly everyone thinks it’s a cytokine sickness that leads to MI, vascular disease, and depression. And then, of course, when you have an event, and you come out with a whole host of issues around it, we know that people who are depressed have a twofold increase in mortality, a fivefold increase in death after a heart attack, and poor outcomes with surgery. It’s like this, what came first, the chicken or the egg?
How Depression Is Linked With Chronic Stress?
Dr. Alex Jimenez, D.C., presents: Every surgeon knows this. They don’t want to do surgery on depressed people. They know the outcome is not good, and of course, they are less likely to follow through on all of our great functional medicine recommendations. So what are some of the mechanisms of autonomic dysfunction have been evaluated heart rate variability and low levels of omega-3s, which have a profound effect on the brain, and low levels of vitamin D. There are those inflammatory cytokines we talked about not getting restorative sleep, and many of our heart patients do have apnea. And remember, don’t just think it’s the heavyset heart patients with thick short necks; it can be quite deceiving. And it’s really important to look at the structure of the face and, of course, social connection, which is the secret sauce. So is autonomic dysfunction a mechanism? One study looked at heart rate variability in people with a recent MI, and they looked at over 300 people with depression and those without depression. They found that four heart rate variability indices will lower in people with depression.
Gut Inflammation & Chronic Stress
Dr. Alex Jimenez, D.C., presents: So here are two groups of people having a heart attack and heart rate variability, rising to the top as a possible etiology. One of the many things that can also affect chronic stress in the body is how the gut microbiome plays its part in oxidative stress. The gut is everything, and many heart patients laugh because they would ask their cardiologists, “Why do you care about my gut microbiome? Why would this affect my heart?” Well, all that gut inflammation is causing cytokine sickness. And what a lot of us have forgotten since medical school is that many of our neurotransmitters come from the gut. So chronic inflammation and exposure to inflammatory cytokines appear to lead to alterations in dopamine function and the basal ganglia, reflected by depression, fatigue, and psychomotor slowing. So we can’t emphasize the role of inflammation and depression enough if we take a look at acute coronary syndrome and depression, which was associated with higher markers for inflammation, more elevated CRP, lower HS, lower heart rate variability, and something that never gets checked in the hospital, which is nutrition deficiencies.
And in this case, they looked at omega-3s and vitamin D levels, so at a minimum, an omega-3 check and a vitamin D level are warranted in all of our patients. And certainly, if you can get a full diagnosis for stress-induced inflammation. Another condition you must look at when it comes to stress-induced inflammation is osteoporosis in the joints. Many people with osteoporosis will have muscle loss, immune dysfunction, fat around the midline, and high blood sugar are associated with aging, and it can come from elevated cortisol levels in the body.
High cortisol heart disease risks are two times higher in people taking high doses of steroids. Small amounts of steroids don’t have the same risk, so it is not as big a deal. Of course, we try to get our patients off of steroids. But the point here is that cortisol is a stress hormone and is a stress hormone that raises blood pressure and puts weight on the midline, makes us diabetic, causes insulin resistance, and the list is endless. So, cortisol’s a big player, and when it comes to functional medicine, we have to look at the various tests that pertain to elevated levels of cortisol like food sensitivity, a 3-day stool valve, a nutra-valve, and an adrenal stress index test to look at what is going on with the patients. When there is a heightened sympathetic nervous system and high cortisol, we discussed everything from coagulopathy to decreased heart rate variability, central obesity, diabetes, and hypertension.
Parental Relationships & Chronic Stress
Dr. Alex Jimenez, D.C., presents: And turning on the renin-angiotensin system it’s all linked to stress. Let’s look at this study that looked at 126 Harvard Medical students, and they were followed for 35 years, a long research. And they said, what’s the incidence of significant illness, heart disease, cancer, hypertension? And they asked these students very simple questions, what was your relationship with your mom and your dad? Was it very close? Was it warm and friendly? Was it tolerant? Was it strained and cold? This is what they found. They found that if the students identified their relationship with their parents as strained 100% incidence of significant health risk. Thirty-five years later, if they said it was warm and close, the results cut that percentage in half. And it would help if you thought about what it is and what can explain this, and you’ll see how adverse childhood experiences make us sick in a few minutes and how we learn our coping skills from our parents.
Conclusion
Dr. Alex Jimenez, D.C., presents: Our spiritual tradition comes from our parents often. Our parents are the ones who frequently teach us how to get angry or how to resolve conflict. So our parents have had a profound effect on us. And when you think about that, our connection is also not very surprising. This is a 35-year follow-up study.
Chronic stress can lead to multiple issues that can correlate to illness and dysfunction in the muscles and joints. It can affect the gut system and lead to inflammation if it is not taken care of immediately. So when it comes to the impact of stress affecting our daily lives, it can be numerous factors, from chronic conditions to family history. Eating nutritious foods high in antioxidants, exercising, practicing mindfulness, and going to daily treatments can lower the effects of chronic stress and reduce the associated symptoms that overlap and cause pain to the body. We can continue with our health and wellness journey pain-free by utilizing various ways to lower chronic stress in our bodies.
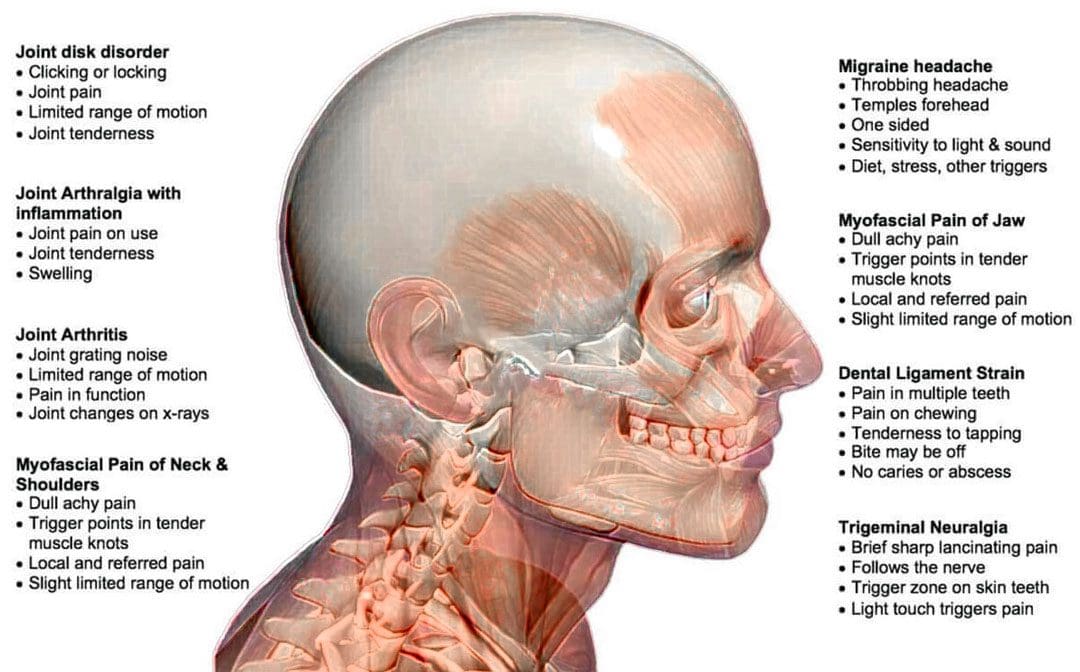
Bruxism is an abnormal jaw clenching or grinding of the teeth, either while awake or during sleep. This can cause neck and shoulder tension caused by excess pressure on the neck and jaw muscles. Individuals may not realize they have bruxism until a dentist notices excess wear and tear or a chiropractor examines their symptoms. Bruxism can play a role in temporomandibular disorders. Doctors and dentists agree that factors like stress increase the likelihood of jaw clenching. Dentists usually recommend a mouth guard to prevent grinding. Chiropractic care, massage, and decompression therapy can relieve symptoms, release and relax the muscles, realign the spine, and restore function.
Bruxism
There is awake bruxism and sleep bruxism. A tight jaw generates tension extending to the neck, shoulder, and upper back muscles. Over time, that excess strain irritates the joints, causing inflammation. Jaw clenching and teeth grinding can lead to health issues like damaged teeth, neck, shoulder, and upper back pain symptoms, and tension headaches.
Symptoms
Signs and symptoms can include:
Face, jaw, neck, and upper back aches, tightness, and soreness.
Tired or tight jaw muscles.
Headaches that start in the temples.
What feels like earache pain symptoms.
Damage from clenching on the inside of the cheek.
Increased tooth sensitivity.
Teeth that are loose, flattened, chipped, or fractured.
Sleep problems.
Risk Factors
Emotional tension – Stress, anxiety, frustration, and anger.
An unhealthy lifestyle – smoking, excess drinking, caffeine, etc., disrupts brain and cardiovascular functions.
Medications
Chiropractic Care for Jaw Clenching
If there is a jaw clenching or grinding issue, it is recommended to see a dentist for a professional diagnosis. Then a chiropractor can develop a personalized treatment plan that utilizes massage and decompression therapy to re-position the jaw, stretch, release and relax the muscles. They will recommend exercises to strengthen and maintain the relaxed jaw muscles and awareness exercises to help identify triggers and prevent clenching.
Jaw Exercises
References
Capellini, Verena Kise, et al. “Massage therapy in managing myogenic TMD: a pilot study.” Journal of applied oral science: Revista FOB vol. 14,1 (2006): 21-6. doi:10.1590/s1678-77572006000100005
Kuhn, Monika, and Jens Christoph Türp. “Risk factors for bruxism.” Swiss dental journal vol. 128,2 (2018): 118-124.
Nishida, Norihiro et al. “Stress analysis of the cervical spinal cord: Impact of the morphology of spinal cord segments on stress.” The journal of spinal cord medicine vol. 39,3 (2016): 327-34. doi:10.1179/2045772315Y.0000000012
Ohayon, M M et al. “Risk factors for sleep bruxism in the general population.” Chest vol. 119,1 (2001): 53-61. doi:10.1378/chest.119.1.53
Santos Miotto Amorim, Cinthia, et al. “Effectiveness of two physical therapy interventions, relative to dental treatment in individuals with bruxism: study protocol of a randomized clinical trial.” Trials vol. 15 8. 7 Jan. 2014, doi:10.1186/1745-6215-15-8
Dr. Alex Jimenez, D.C., presents how stress can impact many individuals and correlate with many conditions in the body in this 2-part series. We refer our patients to certified medical providers who provide multiple available treatments for many people suffering from hypertension associated with the cardiovascular, endocrine, and immune systems affecting the body. We encourage each of our patients by mentioning them to associated medical providers based on their analysis appropriately. We understand that education is a delightful way when asking our providers questions at the patient’s request and understanding. Dr. Jimenez, D.C., only uses this information as an educational service. Disclaimer
How Stress Impacts the Body
Dr. Alex Jimenez, D.C., presents: Now everyone responds to changes in the environment differently. When it comes to many individuals doing everyday activities from working at their job, opening on the weekends, traffic jams, taking exams, or preparing for a big speech, the body goes through a constant state of hyperreactive to a stage of emotional, mental exhaustion that leaves the individual to be exhausted and stressed out. And the key is to recognize this before it happens, as we see this impact of stress on our patients and ourselves. And the first thing to realize is what the initiating event is causing this impact.
Whatever the initiating event, the most important part is our perception of the event. What does it mean to us? Is it our perception? When the body goes through this initiating event, it can cause the perception to lead to the response and the effect on our body. So perception is everything as we talk about stress and the stress response. Now, we have over 1400 chemical reactions that occur in the body. So for this talk’s purpose, we’ll discuss the three key ones: adrenaline and neuro-adrenaline, aldosterone, and of course, cortisol.
And why are these important? Because every one of these has a huge impact on cardiovascular disease. Now, in the 1990s, many doctors were starting to understand the effect of stress on the physical body. And what happens to people when their HPA-axis signals that they are under threat and start flooding their bodies with stress hormones? Well, we see enhanced coagulation. We see a shift in the renin and angiotensin system. It revs up. We see weight gain in people and insulin resistance. What a lot of people don’t realize is that lipids become abnormal with stress. Almost every one of our patients knows that tachycardia and arrhythmia occur when our adrenaline is flowing, and our blood pressure increases. Now, think about this through the language of medicine.
Around the 1990s, doctors were giving aspirin and Plavix at the time for coagulation. We continue to provide ACEs and ARBs to our patients. The impact of cortisol causes weight gain and insulin resistance. We give statins; we give metformin. We provide beta blockers for that, tachycardia, and calcium blockers for that high blood pressure. So every single hormone that gets turned on with stress, we have a drug that we’re using to balance that. And quite frankly, for years, we talked about how good beta blockers were for the heart. Well, when you think about that, beta blockers do block adrenaline. So when doctors look at this, they begin to think, “Well, maybe we need to medicate and meditate, right? We’re using all these drugs, but we may need to look at other ways to transform the stress response.”
What is Vasoconstriction?
Dr. Alex Jimenez, D.C., presents: We won’t read every one of these symptoms because there are so many, but it all comes down to the same thing. Stress. We have to think of someone who’s in an auto accident, for example, and that person is bleeding. So the body is beautiful in that it puts together a way to stop the individual from bleeding or vasoconstriction. Vasoconstriction is constructing these blood vessels and making the platelets sticky so they form a clot, and the blood can stop. This increases the cardiac output by raising the heart rate and increases aldosterone, which causes salt and water retention to raise the blood pressure. So for someone in a medical emergency, like an accident, bleeding, or losing volume, this is the beauty of the human body. But unfortunately, we see people living this way, literally 24/7. So we know the vasoconstriction and the platelet stickiness, and we see increases in markers for inflammation, homocysteine, CRP, and fibrinogen, all of which increase cardiovascular risk.
We see the impact of cortisol, not only raising blood pressure, not only causing diabetes and insulin resistance, but also depositing abdominal fat around the midline. And then, as you’ll see in a few minutes, there are links between stressful events and arrhythmias like atrial fibrillation and even ventricular fibrillation. For the first time in medicine, in cardiology, we have a syndrome called takosubo cardiomyopathy, which is affectionately called broken heart syndrome. And this is a syndrome in which the myocardium becomes acutely stunned to the point of causing severe left ventricular function or dysfunction. And usually, this is triggered by bad news and an emotionally stressful event. It looks like someone needs a heart transplant. So when we think about the old Framingham risk factors, we say, which of these are impacted by stress?
Symptoms of Stress
Dr. Alex Jimenez, D.C., presents: People have all sorts of maladaptive behaviors to stress, whether 20 friends in this pack of cigarettes, eating this Cinnabon because it makes me feel good right now, or all the cortisol will make me fat and diabetic. Lipids go up under stress; blood pressure goes up under stress. So every one of these risk factors is impacted by stress hormones. And, of course, we know that with the turning on of the RAS system or the renin-angiotensin system, we always see a worsening in heart failure. And this is very much described in the literature. And, for those of you who may work in the emergency room, ask your patients what they were doing before coming in with their episode of congestive heart failure or chest pain. And you’re going to hear stories like, I was watching a bad movie, or I was watching a war movie, or I got upset over the football game, or something like that.
We’ll talk about heart rate variability, which gets impacted by stress. And, of course, stress affects our ability to resist infections. And we know that people are under stress when they’re vaccinated. For example, Cleco lasers work but don’t produce antibodies to the vaccine when they’re under stress. And, of course, as you’ll see in a minute, severe stress can cause sudden cardiac death, MI, and so on. So it is a bad player that’s overlooked. And for many of our patients, stress drives the train. So when we’re talking about eating brussels sprouts and cauliflower and, you know, lots of green leafy vegetables, and someone is under so much stress that they’re trying to figure out, “How am I going to get through the day?” They’re not hearing any of the other things that we’re recommending.
So, chronic stress and affective disorders, whether depression, anxiety, or panic, put our foot on the accelerator and rev up the sympathetic nervous system. We know that the same things we see with aging, as you’ll see in a minute, are linked to increased levels of stress hormones, especially cortisol. So whether it’s osteoporosis, decreased bone density, endothelial dysfunction, platelet activation, hypertension, central obesity, or insulin resistance, this comes from a stress response. And we have to have a plan for our patients on how to handle this. American Institute of Stress says that 75 to 90% of all healthcare provider visits result from stress-related disorders. And that’s way too high, but by looking at the patients and where they were coming in with, they tell their stories to their doctors. The results are the same; it doesn’t matter whether it was headaches, muscle tension, angina, arrhythmia, or irritable bowel; it almost always had some stress trigger.
Acute & Chronic Stress
Dr. Alex Jimenez, D.C., presents: There’s a difference between acute and chronic stress with our perception and social connection. Even though we gain some strength from a higher power, stress can impact anyone, and most of us might not be able to handle it well. So a great study was done many years ago by Dr. Ray and Holmes that stated, 50 years ago, put together a method for quantifying life-changing events. So let’s look at some areas, such as life-changing events. How do life-changing events and how do they rank? Which are the big ones, and which are the little ones?
And how does that ranking lead to major medical problems like cancer, heart attack, and sudden death in the future? So they looked at 43 life-changing events, ranked them originally, and re-ranked them in the 1990s. And some of them remained the same. They gave an adjustment score to the event, and then they looked at numbers that would be linked to major illness. So, for example, a life-changing event. Number one, 100 life-changing units, is a death of a spouse. Anyone could relate to that. Divorce was number two, separation number three, and the end of a close family member. But also noticed that some things got ranked that are, you might not equate with, being a major life-changing event that can impact a stress response like marriage or retirement.
Conclusion
Dr. Alex Jimenez, D.C., presents: So it wasn’t the actual single event that made the difference. It was the adding up of events. And what they found after looking at 67 physicians was if you had a life-changing unit score of somewhere between zero and one 50, not a big deal, no real major illness, but once you hit that 300 mark, there was a 50% chance of major illness. So this timeline of events in the patient’s life. We want to know what was going on in their life when their symptoms started and then bring it back earlier to understand the environment in which this individual was living. The impact of stress can make many individuals develop chronic conditions and mask other symptoms that can lead to muscle and joint pain. In part 2, we will dive in more about how the impact of stress affects a person’s body and health.
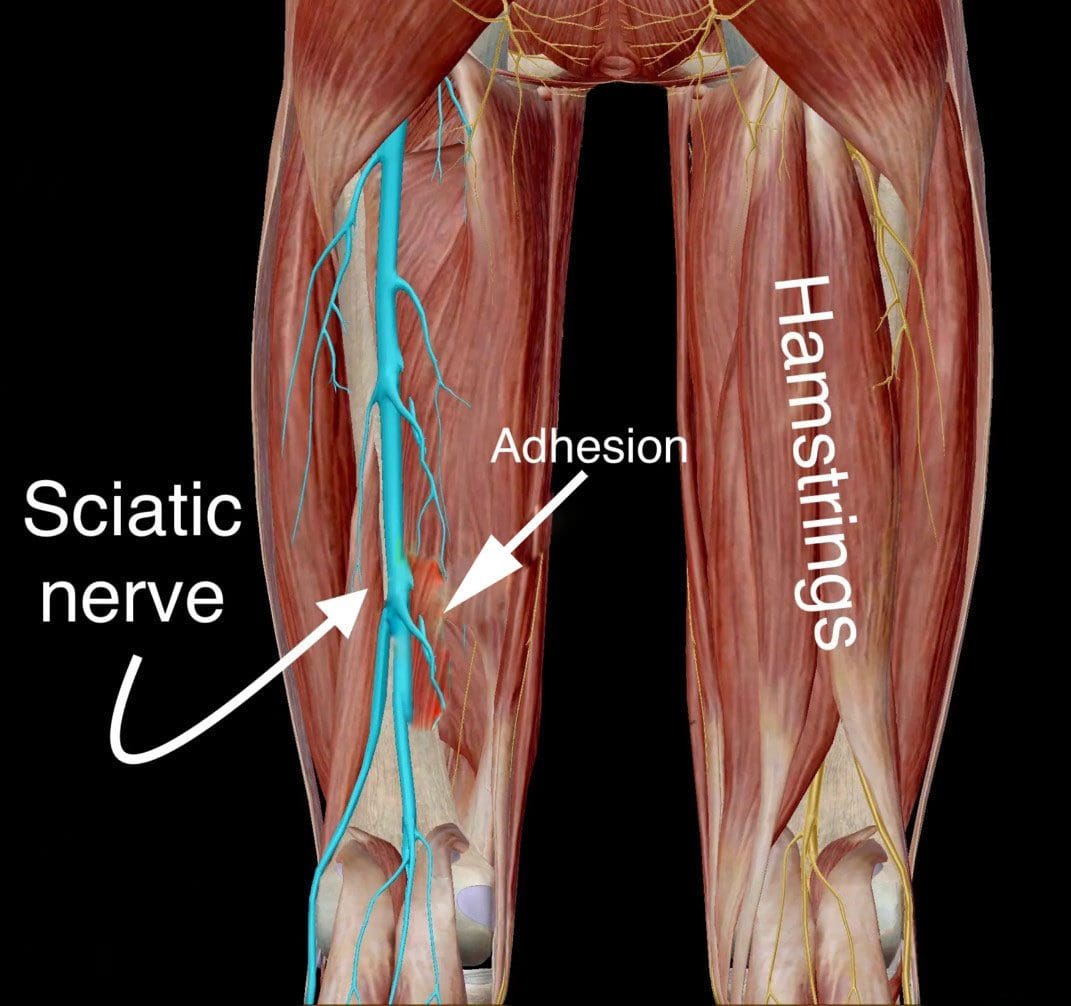
Hamstring syndrome is a condition where the sciatic nerve gets pinched between the hamstring muscles and the pelvic bone or by the tissue bands that connect the hamstring muscles causing compression on and around the nerve. It is seen in individuals that play sports that involve running, kicking, or jumping, in middle-aged individuals engaged in daily activities that have suffered falls, and in individuals that sit for many hours. Chiropractic care, massage, and decompression therapy can relieve the symptoms, release the trapped nerve, relax and stretch the muscles, and restore function.
Hamstring Muscles Trapped Sciatic Nerve
Three muscles make up the hamstrings in the back of the thigh. The sciatic nerve runs from the low back down the leg into the foot. A trapped sciatic nerve can cause various symptoms and sensations in the back of the leg, hip, buttock, and foot. It may hurt to sit down or stretch the legs out, and there is usually tightness in and/or around the buttock and back of the leg. The symptoms typically recede when lying on your back.
Cause
Regular wear and tear on the back muscles and hamstrings can contribute to the condition.
Often the sciatic nerve and/or the sheath surrounding the sciatic nerve gets trapped and irritated as it travels around the ischial tuberosity. The ischial tuberosities are known as the sit bones.
The area where the sciatic nerve runs down the back of the leg can become narrowed, leading to nerve irritation and stinging, numbing, and tingling sensations.
The injury often happens during sudden, quick, forceful movements that overstretch the tendons and/or muscles but can also happen during slow movements.
Movement agitates the pulling and rubbing of the nerve on the muscles.
A non-painful pull or pop of the hamstrings can cause the muscles to spasm and wrap around the nerve.
Symptoms
Symptoms usually include the following:
Leg pain that worsens when sitting.
Intense electrical shooting pain that makes it hard to stand or move.
Difficulties moving the leg or foot.
Numbness and weakness in and around the leg.
Tingling or burning sensations running down the leg.
Persistent pain on one side of the lower back.
Chiropractic Care
Chiropractic treatment can relieve the symptoms and release the trapped nerve. Treatment includes:
Accurate Diagnosis – A chiropractor will examine and review physical activity, work, and medical history.
Ice and Heat therapies will stop the swelling and increase blood flow.
Massage therapy relaxes the muscles and increases circulation.
Decompression therapy incrementally and gently stretches the body.
Chiropractic adjustments realign and reset the body.
Targeted stretches and exercises will keep the muscles loose and increase strength.
Nutritional recommendations will help reduce inflammation and prevent flare-ups.
Hamstrings and Sciatic Nerve Relationship
References
Lohrer, Heinz, et al. “Nerve entrapment after a hamstring injury.” Clinical journal of sports medicine: official journal of the Canadian Academy of Sports Medicine vol. 22,5 (2012): 443-5. doi:10.1097/JSM.0b013e318257d76c
Mattiussi, Gabriele, and Carlos Moreno. “Treatment of proximal hamstring tendinopathy-related sciatic nerve entrapment: presentation of an ultrasound-guided “Intratissue Percutaneous Electrolysis” application.” Muscles, ligaments and tendons journal vol. 6,2 248-252. 17 Sep. 2016, doi:10.11138/mltj/2016.6.2.248
McGregor, Catriona, et al. “Traumatic and overuse injuries of the ischial origin of the hamstrings.” Disability and rehabilitation vol. 30,20-22 (2008): 1597-601. doi:10.1080/09638280701786138
Saikku, Kari, et al. “Entrapment of the proximal sciatic nerve by the hamstring tendons.” Acta orthopaedica Belgica vol. 76,3 (2010): 321-4.
Dr. Alex Jimenez, D.C., presents how hypertension affects the human body and how to find ways to manage the symptoms associated with hypertension affecting many individuals in this 2-part series. Part 1 looked into the various factors that correlate with hypertension, and part 2 looked at the different genes and body levels affected by hypertension. We refer our patients to certified medical providers who provide multiple available treatments for many people suffering from hypertension associated with the cardiovascular, endocrine, and immune systems affecting the body. We encourage each of our patients by mentioning them to associated medical providers based on their analysis appropriately. We understand that education is a delightful way when asking our providers questions at the patient’s request and understanding. Dr. Jimenez, D.C., only makes use of this information as an educational service. Disclaimer
What Are ADMA Levels In Hypertension
Dr. Alex Jimenez, D.C., presents: Okay, so what affects ADMA levels? Upregulation of NRF-2 can decrease ADMA levels. So that’s great. So looking at things high in EGCG, think of green tea, sulforaphane, resveratrol, and exercises that reduce ADMA levels in the body. Improving blood sugar control improves ADMA levels, addressing the homocysteine pathway and looking at acidencial homocysteine. So this asks the question, what is the most common over-the-counter medication in the United States for gastroesophageal reflux or hyperacidity of the stomach that increases ADMA levels? And that is proton pump inhibitors, a poor diet, or elevated homocysteine. These are a couple of touch points on the ADMA that you can consider.
Let’s shift a little bit. Remember we talked about increased oxidative stress? There’s a whole enzyme system orchestra that addresses oxidative stress. And chronic oxidative stress can lead to hypertension. It also leads to fibrosis or gradual fibrosis of end organs. And so when you have elevated, reactive oxygen species, cell proliferation, migration changes, apoptosis changes, there’s increased inflammation. Reactive oxygen species make your tissue at the basal membrane level stiffer; your tissue becomes stiffer when you have increased oxidative stress. You start shifting with increased oxidative stress, extracellular matrix enzymes, and structure, and then you start getting endothelial dysfunction.
Many enzymes are influenced by nutrition and our genetic makeup that shift our balance of oxidative stress. Some of those enzymes are glutathione and glutathione peroxidase. The fifth enzyme down is GPX, which is the enzyme that helps us react to inflammation and toxins by altering the glutathione balance. We mentioned glutathione multiple times. We’ll talk about glutathione as a biomarker that you can check to assess oxidative stress in your patient. So is your oxidative stress because of mitochondrial dysfunction, or is your increased oxidative stress due to inflammation? We’ve seen this as a side effect in many patients, as increased inflammation leads to increased oxidative stress associated with increased mitochondrial dysfunction. This triangle is a matrix of interaction between the energy node, mitochondrial dysfunction, reactive oxygen species, and the defense and repair node inflammatory markers. We have seen this multiple in multiple different conditions.
How Oxidative Stress Is Associated With ADMA Levels?
Dr. Alex Jimenez, D.C., presents: When we see oxidative stress findings in many different organ systems in many other conditions in our medical practices, in many patients, we often see all these chronic conditions associated with oxidative stress as part of their symptoms. When this happens, we have to consider how to modulate them by asking them a few simple questions. We would ask them what kind of spices and herbs they use when they cook. Or what is their diet plan? These questions are important to analyze and assist the patient because culinary spices can affect many aspects of our body’s metabolism that could influence blood pressure.
By looking at the list of various spices, it is important to add them to food preparations or to alter the taste of food to add flavor and improve your health. Another thing to look for when it comes to lowering blood pressure is by adding these various spices into your food as part of your daily routine and being referred to a health coach or a nutritionist, whose main job is to add more spices to a patient’s diet and coming up with numerous recipes that have these spices. Remember, it doesn’t take a lot; a teaspoon to a tablespoon of mixed herbs in your food throughout the day could help normalize your blood pressure.
How To Come Up With A Plan To Lower Hypertension
Dr. Alex Jimenez, D.C., presents: Okay, how will you address oxidative stress, and what biomarkers might you look at? Well, oxidative stress affects many different levels of our cellular and subcellular levels. Oxidative stress can cause damaged DNA and change the fats in the membranes of the mitochondrial cell. It can induce increased lactation and disrupt protein structure in our bodies. So we start looking at total antioxidant capacity. Total antioxidant capacity is influenced by the nutritional adequacy of essential fats of too many simple carbohydrates of enough minerals, vitamins, and phytonutrients. So you can check glutathione levels in the serum, cysteine levels, enzymes, glutathione peroxidase, superoxide dismutase, and lipid peroxide on this list to see what is elevated in the body. You can check these different markers and get a clue of what portion of the cells or organ system is influenced by oxidative stress.
When we see these results, we need to develop a plan to increase the fat-soluble antioxidants, which can be fat and water-soluble, like alpha-lipoic acid. Or, say, for example, somebody has elevated eight-hydroxy-deoxy guanosine. What are the things that help you repair their DNA sequence? Well, it’s the components in one cellular, one-carbon metabolism. It’s your B vitamins. It’s methyl groups from essential fats. But then you have to ask, why is this elevated? Is it elevated because of micronutrient deficiency, mitochondrial toxicity, chronic inflammation, or hyperglycemia? So it’s common for your cardiometabolic patients to frequently see increased DNA oxidation marker eight-hydroxy-deoxy-guanosine.
Okay, those are biomarkers you can check in the urine or the blood. What’s another biomarker that you can check by looking at the nitric oxide angiotensin balance? What are ways that you can check endothelial function? What are ways that you can improve endothelial function even without checking? Well, there are different things that you can do to enhance nitric oxide. We’ve mentioned them before, like improving the bacterial balance, eating more flavonoids, increasing foods rich in nitrates, or even adding yoga to your regimen. There are ways that you can improve endothelial function without medications like sildenafil, as noted, that could potentially correlate with sleep apnea. It may address whether they have sleep apnea, need a mandibular split, and address some of the conditions they carry with them. Or, at the very bottom, it may manage their high-fat meals.
Okay, if you have somebody on a ketogenic diet, you must recognize potential oxidative stress and address it with your patients. So what are some early ways to detect vascular or endothelial dysfunction? One of the outpatient tools you can use is the vascular reactivity index. This detects vascular disease and looks at the pliability of the flexibility of the small capillaries and how well you profuse tissue downstream of an obstruction. So instead of looking at coronary arteries or carotids, it’s looking down at the level of the arterial, and we look at what’s called reactive hyperemia. So, it gives you some prognostic inflammation.
Measuring Blood Pressure
Dr. Alex Jimenez, D.C., presents: And there have been studies that follow people with reactive hyperemia to look at endothelial dysfunction and how that interacts with the Framingham risk score. And we know that when somebody has an abnormal index that predicts cardiovascular events, combining it with the end path lowers the lower endothelial function readings, which is associated with long-term cardiovascular disease. So how does it happen? You put a blood pressure cuff on your arm with a monitor on your finger. You blow the blood pressure cuff up to obstruct blood flow. You then, after five minutes, release it, and your vascular response to that surge of blood after having the blood flow occluded predicts hypertension and coronary heart disease. On the left, you see the normal endothelial function; the blue line on the top graph on the left is the obstruction of blood flow.
And then, after five minutes, you release the cuff, and you see this almost bell-shaped flow of blood down to the capillaries. You know the response, the endothelial function. That is a normal curve on the right. It is poor endothelial function. You can see there are no signs of arterial capillary flexibility. And so this is predictive up to seven years later. So then you ask yourself, is there anything that can improve endothelial function when I expect endothelial function dysfunction, or do I have an abnormal vascular reactivity index? And yes, let’s choose one as an example. Eating blueberries twice a day or taking them in powder form is rich in anthocyanins. To that point, you can add them to a smoothie that you have incorporated into your diet and have antioxidants in your system. The anthocyanins and their metabolites can help improve vascular function while increasing the mediated flow dilation and lowering 24-hour systolic blood pressure.
We use a lot of carotid in medial thickness because if I have somebody with hyperlipidemia, hyperglycemia, or hypertension, I want to use it as a leverage point to see if they have inflammation, their carotid bull or their internal carotid on each side to track to see if we’re getting systemic improvement in inflammation or can we get reversal with plaque. And so we’ve successfully done that through testing our clinic, advanced lipids, and education through group medical visits along with lifestyle interventions with nutraceuticals. And we have had a reduction in plaque and mark modulation and improvement in inflammation. If you don’t do anything helpful, the average increase in carotid intimal medial thickness per year is between 10 and 20% of the abnormal level. You can use this as a tool, as an outpatient, very easily to monitor the reduction in systemic vascular inflammation in plaque.
Looking At The Emerging Markers
Dr. Alex Jimenez, D.C., presents: Some other emerging markers, like HSCRP, uric acid, heavy metals, nutritional deficiencies, and TMAO, correlate with hypertension. And by improving those markers, you get improvement in blood pressure. Here’s the thing to remember. When you look at an HSCRP and see that it’s above one, here’s the connection. Now HSCRP inhibits endothelial nitric oxide synthase. So when you see an elevated HSCRP, you make a connection to lower nitric oxide. If you see an elevated HSCRP that downregulates the angiotensin-two receptors, it can increase blood pressure and is associated with increased cardiovascular risk.
How often do you check uric acid? It’s important to prevent uric acid in hypertensive patients. If it’s above six, you need to address it. How do you manage elevated uric acid levels? Well, by removing purine-rich foods or improving the metabolism of urine through your one carb metabolism, b12, fully b6, limiting their alcohol or avoiding a lot of extra high fructose sugar or improving their body weight, or addressing insulin resistance. All these mediate uric acid. If you have somebody who’s hyperemic, remember these five areas of modifiable physiologic imbalance. So I hope you’ve seen that hypertension is a syndrome. It’s not one thing; it’s not stiffness; it’s a syndrome in that you have three areas that you have to consider inflammation, oxidative stress, and immune response. You can look at a lot of the different imbalances around this dial.
Conclusion
Dr. Alex Jimenez, D.C., presents: You can look at your patient; you can look at what ways you can further evaluate them. And so, when you see a patient with hypertension, consider the treatments outlined in your clinical decision tree. And then, you can apply the modifiable lifestyle factors and the things to lower their blood pressure. Incorporating these lifestyle applications can improve the root cause and help you find the root cause of hypertension through the functional medicine lens.
Dr. Alex Jimenez, D.C., presents how hypertension affects the human body and some causes that can increase hypertension in many individuals in this 2-part series. We refer our patients to certified medical providers who provide multiple available treatments for many individuals suffering from hypertension associated with the cardiovascular and immune systems affecting the body. We encourage each of our patients by mentioning them to associated medical providers based on their analysis appropriately. We understand that education is a delightful way when asking our providers questions at the patient’s request and understanding. Dr. Jimenez, D.C., only makes use of this information as an educational service. Disclaimer
How To Look For Hypertension
Dr. Alex Jimenez, D.C., presents: Let’s go back to the decision tree so you can begin to think about how you will apply the go-to-it model in functional medicine to hypertension and how you will start better assessing somebody with hypertension rather than telling them that their blood pressure is elevated. Is the body influenced by inflammation, oxidative stress, or immune response? Is it affecting endothelial function or vascular smooth muscle from those three categories of reactions, inflammation, oxidative stress, or immune response? Do we choose a diuretic calcium channel blocker or an ACE inhibitor? And so to do that, it’s really important in our gather section. Taking the medical history and the timeline of their hypertension, you get a clue about the organ damage to the questionnaires. You’re looking at their anthropometrics.
This includes the following questions:
What are the inflammatory markers?
What are the biomarkers and clinical indicators?
Those are outlined through the clinical decision tree. And already just doing that, you’re going to expand and fine-tune your lens on what you might see in your hypertensive patient. Let’s add to the timeline when does hypertension begin? The timeframe of hypertension begins actually in prenatally. It’s important to ask your patient if they were early or large educational age. Was their mother stressed? Were they born early or premature? Was there nutritional stress in their pregnancy? If they know that, you can have two people with the same kidney size, but the person who didn’t have enough protein during pregnancy can have up to 40% less glomeruli. Knowing that will change how you adjust the medication decades later if you know they possibly have 40% less glomeruli.
The Timeline For Blood Pressure
Dr. Alex Jimenez, D.C., presents: So it’s important to take the timeline of their blood pressure. Then it’s also important to recognize what is happening when we begin to organize and collect data through the biomarkers; the basic biomarkers will give you clues about whether they have issues with insulin lipids, whether they have problems with vascular reactivity, autonomic nervous system balance, imbalance, coagulation, or immune toxin effects. So this is a reasonable thing to print off because, in your hypertensive patient, this is through just the biomarkers you can begin to get a clue as to what areas of dysfunction affect inflammation, oxidative stress, and immune response and how these biomarkers reflect that information for you. This is very reasonable to have in front of you to help change your thoughts about hypertension and also enables you to refine some of the characteristics of the person on the other side of your stethoscope in a more personalized, precise way.
But let’s start at the very beginning. Does your patient have high blood pressure? We know that depending on the end organ effects of their comorbidities, you may run someone a slightly higher blood pressure if you have a profusion issue in the brain and the kidneys or the heart, but some guidelines are there. Our 2017 American Heart Association guidelines for blood pressure categories are listed here. They’ve waxed and waned back and forth over the last couple of decades, but this is very clear. Having elevated blood pressure, anything above 120, really shifted how many people we start seeing or considering addressing the root causes of their blood pressure. So we will come back to this, especially in the case to help us look at how we categorize people with blood pressure issues.
The Criteria To Mesure Blood Pressure
Dr. Alex Jimenez, D.C., presents: What is the first step? It’s how do you have the blood pressure taken in your patient? Do they monitor it at home? Do they bring those numbers to you? How do you monitor blood pressure in your clinic? How do you get accurate readings in your clinic? Here are the criteria to accurately measure blood pressure and the questions to consider whether you’re doing all these.
Do you ask your patient whether they’ve had caffeine in the last hour?
Whether they’ve smoked in the previous hour?
Were they exposed to smoke in the last hour?
Is the place where you’re taking blood pressure warm and quiet?
Are they sitting with their back supported in a chair with their feet on the ground?
Do you use the roll-around side table to rest your arm at the heart level?
Are they sitting at the exam table with their feet dangling, and a nurse aide elevates their arm and puts in their axillary fold to hold their arm there?
Are their feet on the ground?
Have they sat there for five minutes?
Have they exercised in the previous 30 minutes?
You may have systolic blood pressure if everything is in the criteria. Here’s the challenge. There are 10 to 15 millimeters of mercury higher when it comes to sitting and taking blood pressure. What about the cuff size? We know last century; most adults had an upper arm circumference of fewer than 33 centimeters. Over 61% of people now have an upper arm circumference greater than 33 centimeters. So the size of the cuff is different for around 60% of your adult patients, depending on your population. So you have to use a large cuff. So take a look at how blood pressure is collected in your office. Let’s say the blood pressure is elevated in your patients; then we have to ask, is it normal? Great.
The Different Types Of Hypertension
Dr. Alex Jimenez, D.C., presents: Is it elevated because of white-coat hypertension? Do they have normal blood pressure, elevated outside the clinic, or masked hypertension? Or do they just have sustained hypertension which is a challenge? We’ll talk about that. So when you interpret, it is also important to consider ambulatory blood pressure monitoring. So if you have somebody who’s hypertensive and don’t know whether the blood pressure goes down and you’re trying to figure out whether they have sustained hypertension, you can use 24-hour blood pressure monitoring. The mean daytime blood pressure above 130 over 80 is hypertensive the mean nighttime blood pressure above 110 over 65 is hypertensive. So why is this important? The average blood pressure dips to around 15% at night because of the issue with blood pressure dipping. Failure to have blood pressure drop while you sleep at night could develop problems that can affect a person throughout the day.
If your patient sleeps at night, it should drop about 15% when they sleep. If they have non-dipping blood pressure, it is associated with comorbidities. What are some of those comorbidities in non-dipping blood pressure? Some of the conditions correlated with non-dipping blood pressure include:
Congestive Heart Disease
Cardiovascular Disease
Cerebrovascular Disease
Congestive Heart Failure
Chronic Renal Failure
Silent Cerebral Infractions
Co-morbidities Associated With Non-Blood Pressure
Dr. Alex Jimenez, D.C., presents: These are the comorbidities associated with non-blood pressure. All of us agree that elevated blood pressure is not necessarily good in all those conditions. So when you look at different people groups or other comorbidities, non-dipping blood pressure is most commonly associated with sodium-sensitive folks, people who have renal insufficiency, people who have diabetes, people who have left ventricular hypertrophy, people who have refractory hypertension or autonomic nervous system dysfunction and finally, sleep apnea. So, non-dipping blood pressure increases your association with subclinical cardiac damage. Okay, Reverse dipping means you are more hypertensive at night and is more ascent associated than during the day is more related to hemorrhagic stroke. And if you have somebody with nocturnal hypertension, you have to start thinking about things like the carotid arteries and increased carotid, internal medial thickness. You start thinking about left ventricular hypertrophy and may see it on EKG. Here’s what we know about nocturnal hypertension. Nocturnal hypertension is a nighttime blood pressure greater than 120 over 70. It is associated with greater predictability of cardiovascular morbidity and mortality.
If you have nocturnal hypertension, it increases your risk of mortality from cardiovascular disease by 29 to 38%. We must know what’s happening at night when we sleep, right? Well, what’s another refinement? Another refinement is recognizing that resting blood pressure is controlled by your renin-angiotensin system. Waking blood pressure is controlled by your sympathetic nervous system. So let’s talk about how their renal angiotensin system drives their nighttime hypertension, and you think about what medication they’re taking. You might change the medication dosing to nighttime. Well, studies have shown that if you have nighttime hypertension and are a non-dipper, it’s best to take your ACE inhibitors, ARBs, calcium channel blockers, and certain beta blockers at night before bed. But it makes sense that you wouldn’t move your diuretics to nighttime, or you will have a disruptive sleep.
Addressing Daytime & Nighttime Blood Pressure
Dr. Alex Jimenez, D.C., presents: So if we don’t address daytime and nighttime blood pressure, we have to consider the effect of blood pressure load. What is your average daytime blood pressure and your moderate sleeping blood pressure is. We know that blood pressure load in young adults is hypertensive only about 9% of the time. So meaning the systolic load is about 9% versus in the elderly, about 80% of the blood pressure load is systolic. And so when you have a higher systolic load, you have more complications and end-organ damage. So what we’re talking about is helping identify your patient with hypertension; what is their timeline? What is their phenotype? Are they only hypertensive during the day, or they’re hypertensive at night also? We have to look at what helps balance that.
Here’s the other point, only about 3.5% of people with hypertension do it have a genetic cause. Only 3.5% of people their genes cause hypertension. The power is at the bottom of the matrix and recognizing these patterns, right? So you look at exercise, sleep, diet, stress, and relationships. So we know that these four autonomic balances help determine blood pressure. We will examine the renal angiotensin system, plasma volume where they hold onto too much fluid, secondary salt load, and endothelial dysfunction. Abnormalities in any of these can lead to hypertension. We’ve been talking about another one that can lead to hypertension: the link between insulin resistance and hypertension.
This diagrammatically gives you an idea of the physiologic interactions between insulin resistance and hypertension. It affects increasing sympathetic tone and increasing renal-angiotensin system balance. So let’s spend a few minutes on the renin-angiotensin system pathway angiotensinogen down to angiotensin two. We take advantage of these enzymes by giving inhibitors to angiotensin-converting enzymes in our hypertensives patients. Elevated angiotensin two leads to cardiovascular hypertrophy, leads to sympathetic phase constriction, increased blood volume, sodium fluid, retention, and aldosterone release. Can you inquire about your patient biomarkers? Can you ask whether they have elevated renin levels?
Look For The Signs
Dr. Alex Jimenez, D.C., presents: Well, you can. You can check plasma renin activity and aldosterone levels. It’s important to do this if your patient is hypertensive and has never been on medication because this is where nitrous oxide is so important. This is where your endothelial nitric oxide synthase is present. This is where you have sheer and hemodynamic stress. This is where dietary intake of arginine or the environment that affects nitric oxide plays such a role in the health of this layer of endothelia. If you lay it all together somehow, miraculously, or at least in your mind’s eye, it’ll cover six tennis courts in the average adult. It’s a huge surface area. And the things that cause endothelial dysfunction are not new news to people in functional medicine. Increased oxidative stress and inflammation are two things we mentioned that play an effect.
And then, look at some of these other components, your ADMA being elevated and correlated with insulin resistance. It all begins to form together in a matrix that interacts. So you look at one comorbidity in cardiometabolic syndrome, and it affects another comorbidity. You suddenly see the interrelation between them or hyperhomocysteinemia, which is a one-carbon metabolism marker, meaning you’re looking at the adequacy of folate, b12, b6, riboflavin, and that activity of your one-carbon metabolism. So let’s look at some of these emerging risk markers to improve and track in patients with hypertension. Let’s reanalyze ADMA again. ADMA stands for asymmetric dimethyl arginine. Asymmetric, dimethyl arginine is a biomarker of endothelial dysfunction. That molecule inhibits nitric oxide synthase while impairing endothelial function, and in all of the comorbidities associated with cardiometabolic syndrome, ADMA can be elevated.
Conclusion
So, as a quick review, L-arginine is converted to nitric oxide via nitric oxide synthase, and nitric oxide adequacy leads to vasodilation. ADMA blocks this conversion. And if your ADMA levels are elevated and your nitric oxide levels are low, then you have decreased nitric oxide platelet aggregation increases in LDL oxidation. So many things reduce nitric oxide or are associated with lower nitric oxide levels, sleep apnea, low dietary arginine, protein, zinc insufficiency, and smoking.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine