As we get older, we become more prone to injuries, since our bodies are not as elastic as they once were. This is especially true for the inner material of your spine’s discs. Every year you become a little more at risk of experiencing herniated discs, a condition where a stressed disc ruptures, because the elasticity and water content of your intervertebral discs reduces overall.
But herniated discs aren’t only a problem for elderly people. A disc herniation can be experienced by anyone as a result of twisting or lifting the wrong way. And in the event that you currently have a bulging disc, a disc that is hurt but still intact, chances are higher that stress on the affected disc could cause it to rupture or become “herniated”.
A herniated disc can cause pain throughout the entire body, not just back pain. And as you might think of surgery being the sole remedy for a herniated disc, there are lots of complementary and alternative treatment option for herniated discs. Chiropractic specializes in supplying non-invasive spinal decompression treatment and therapy methods.
A visit to your chiropractor will help you confirm whether you have a herniated disc, a bulging disc, or even some other spinal problem altogether. If you do have an injured disc, a doctor of chiropractic can create an individual treatment plan to assist you avoid surgery and return to enjoying your life, pain-free.
What are Herniated Discs?
The 24 vertebrae of your spine are separated from one another by pads of cartilage known as intervertebral discs. These discs have an outer coating with a soft interior to cushion against stresses and strains as well as the shocks experienced in your spine. The discs are subject to injury, disease, and degeneration with use over time. Certain activities and types of work increase the risk of discs being damaged or deteriorating.
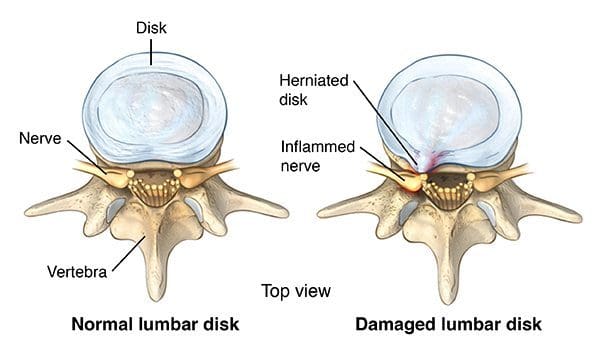
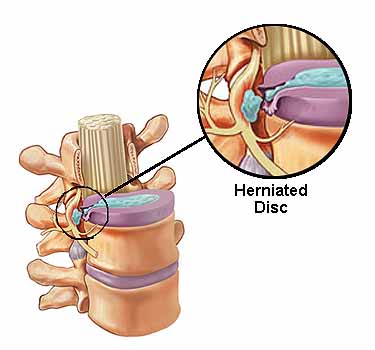
Once the soft inside material of a disc pushes or is bulged out through a tear or weakening in the outside covering, the disc is reported to be herniated. Slipped, ruptured and �prolapsed discs are also known as protruding, bulging, or degenerated discs. There are distinctions between these terms, but they really refer to a disc that is no longer in its normal condition and/or position and may require chiropractic care to treat them. Herniated discs trigger pain by impinging on (intruding upon, irritating, and pinching) as well as depriving nerves in the spine.
Chiropractic for Herniated Discs
A healthcare professional can help address back pain along with other herniated disc symptoms. In your first appointment, your chiropractor will go through your medical history, do a physical exam, and carry out orthopedic and neurological tests. The chiropractor will also look over your posture, and may order an X-ray or MRI, if necessary, to aid with the diagnostic procedure and determine the presence of a disc herniation.
Chiropractors assess the whole spine. Your chiropractor will examine your neck, too, even when you simply have back pain. She or he wants to see how well your backbone is functioning and recall: What happens in one area of your spine can affect other parts of your spine and/or body.
After reviewing this information, your physician can ascertain whether you have an intervertebral disc injury. The type of disc injury you have will determine what treatments your chiropractor will use to address your symptoms. Your chiropractor can provide treatment options to you to address your pain and other symptoms.
To treat a herniated disk, your physician will develop a treatment program that might include spinal manipulation–also called adjustments–and other chiropractic techniques to help alleviate your herniated disc symptoms. It might consist of therapy and exercises, although this will be an individualized treatment plan.
The particulars of what are on your treatment strategy are particular to your own pain, level of activity, general health, and what your chiropractor thinks is best. As with any treatment option, do not be afraid to ask questions regarding what chiropractic treatments are being recommended and why. You want to be sure you know how it can help relieve your pain and what will be performed. Therapy is safe and effective for most patients.
Chiropractic provides the distinctive training, techniques, and experience needed to safely and effectively adjust your spine so the stress on the discs is minimized, the pain alleviated, the damaged or displaced structures given a opportunity to heal, and your capacity to return to normal functioning restored.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Sciatica
Lower back pain is one of the most commonly reported symptoms among the general population. Sciatica, is well-known group of symptoms, including lower back pain, numbness and tingling sensations, which often describe the source of an individual’s lumbar spine issues. Sciatica can be due to a variety of injuries and/or conditions, such as spinal misalignment, or subluxation, disc herniation and even spinal degeneration.
Physical therapy plays a part in herniated disc recovery. Its methods not only offer you immediate pain relief, but they also teach you how you can condition your body to prevent further injury.
The discs are pads that serve as “cushions” between the vertebral bodies that serve to minimize the impact of movement on the spinal column. Each disc is designed like a jelly donut with a central softer component (nucleus pulposus).
As the disc degenerates from age or injury, the softer central portion can rupture (herniate) through the surrounding outer ring (annulus fibrosus). This abnormal rupture of the central portion of the disc is referred to as a disc herniation. The most common location for a herniated disc to occur is in the disc at the level between the fourth and fifth lumber vertebrae in the low back.
You will find a variety of physical therapy techniques, such as passive treatments, which help relax your body and include deep tissue massage, hot and cold therapy, electric stimulation (eg, TENS), and hydrotherapy, among others.
Your physical treatment program will usually begin with passive remedies. But once your body heals, you will start active treatments that strengthen your body and protect against additional pain. Your therapist will work with you to develop a strategy which best suits you.
Passive Physical Treatments for Herniated Discs
Deep Tissue Massage: There are more than 100 kinds of massage, but deep tissue massage is an ideal option when you’ve got a herniated disc because it uses a lot of pressure to ease deep muscle tension and spasms, which develop to stop muscle movement at the affected place.
Hot and Cold Therapy: Both hot and cold therapies offer their own set of advantages, and your physical therapist may alternate between them to get the best outcomes.
Your physical therapist may use heat to increase blood flow to the target region. Blood helps by delivering nutrients and additional oxygen cure the area. Blood also removes waste byproducts.
Conversely, cold therapy (also called cryotherapy) slows circulation. This decreases inflammation, muscle spasms and pain. Your physical therapist may put an ice pack give you an ice massage, or use a spray known to cool tissues.
Hydrotherapy: As the name implies, hydrotherapy involves water. As a passive therapy, hydrotherapy may involve sitting in warm shower or a bath. Hydrotherapy gently relieves pain and relaxes muscles.
Transcutaneous electric nerve stimulation (TENS): A TENS machine utilizes an electrical current to stimulate your muscles. It isn’t painful, although it seems extreme. A electric current is sent by electrodes to key points on the neural pathway. TENS reduces muscle spasms and is generally believed to activate the release.
Traction: The goal of traction is to decrease the effects of gravity to the spine. The aim is to cut back the disk herniation, by pulling the bones apart. The analogy is similar to a flat tire “disappearing” when you place a jack under the car and take strain off the tire. It can be carried out in the lumbar or cervical spine.
Active Physical Treatments for Herniated Discs
Active remedies help address flexibility, posture, strength, core stability, and joint motion. An exercise program may also be prescribed to achieve results. This will not just suppress recurrent pain but may also benefit your health. Your therapist may work with you to develop a schedule based on your diagnosis and health history.
Core equilibrium: Many people don’t realize how important a strong heart is to their spinal health. Your core (abdominal) muscles help your back muscles support your spine. It puts pressure when your heart muscles are weak. Your physical therapist may teach core to you.
Flexibility: Learning appropriate stretching and endurance techniques will prepare one for aerobic and strength exercises. Flexibility helps your body move simpler by warding off stiffness.
Hydrotherapy: Compared to just sitting in a hot bath or bath like its counterpart that is passive, active hydrotherapy can demand water to help condition your body without unnecessary strain.
Muscle strengthening: Strong muscles are a great support system for your backbone and better handle pain.
Your physician will teach you ways to condition and strengthen your back to help prevent future pain. So that you realize how to best treat your symptoms, you may learn fundamentals. The aim is that you develop the knowledge to maintain a way of life.
It is essential that you understand how to exercise and condition your back following the formal physical therapy ends. You won’t appreciate its results, if you don’t implement the lessons you learned during physical therapy. You might prevent additional disc pain, by taking care of your back on your own.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Sciatica
Lower back pain is one of the most commonly reported symptoms among the general population. Sciatica, is well-known group of symptoms, including lower back pain, numbness and tingling sensations, which often describe the source of an individual’s lumbar spine issues. Sciatica can be due to a variety of injuries and/or conditions, such as spinal misalignment, or subluxation, disc herniation and even spinal degeneration.
Complementary and alternative treatments like massage, acupressure, and acupuncture can relieve pain related to a bulging or herniated disc.
If you’re considering these remedies, you need to consult a complementary and alternative medicine (CAM) professional. This title can be confusing, although complementary medicine and other medicine follow the very same techniques, they’re distinct in that forms are used in place of traditional medicine, whereas complementary treatments are used with conventional medication.
A herniated disk refers to a problem with one of the rubbery cushions (disks) between the individual bones (vertebrae) that stack up to make your spine. A spinal disk is a little like a jelly donut, with a softer center encased within a tougher exterior. Sometimes called a slipped disk or a ruptured disk, a herniated disk occurs when some of the softer “jelly” pushes out through a tear in the tougher exterior.
A herniated disk can irritate nearby nerves and result in pain, numbness or weakness in an arm or leg. On the other hand, many people experience no symptoms from a herniated disk. Most people who have a herniated disk don’t need surgery to correct the problem, as a matter of fact, they can explore alternative treatment approaches.
Other Treatments for Herniated Discs
Exploring alternative approaches may not only help you feel relaxed and hassle free but these can also keep you away from the operating room. For a ruptured or herniated disc, you might want to try:
Acupuncture: This ancient Chinese practice is rooted in the belief that everyone has an energy force called the Chi (sometimes spelled Qi, but the two are pronounced “chee”). When the Chi is blocked or unbalanced, your body may react with sickness, pain and discomfort. Traditional acupuncturists aim to free up Chi channels, called meridians, by inserting extremely thin needles into certain points in your own body’s meridians.
Based on your particular diagnosis, the practitioner will probably insert multiple needles which are left in for approximately 20-40 minutes.
It’s also been suggested that acupuncture triggers the release of endorphins into the blood flow. In other words, endorphins are the body’s natural pain relievers. As such, their discharge decreases your perception of pain. Similarly, the Gate Control Theory can play a part in acupuncture’s efficacy in reducing pain. This theory maintains that pain signals traveling slowly from the area of injury to the spinal cord into the brain because the nerves may only deal with a limited number of signals at the same time. Acupuncture is supposed to create signals to audience the pain signs that were slow-moving, blocking out the pain.
Acupressure: Not surprisingly, acupressure is very much like acupuncture. Both are techniques that restore a healthy flow of energy throughout the entire body by stimulating specific meridian points. But acupressure relies on hands palms, and elbows, not needles, to manage pressure. Acupressure is for people of all ages but not for pregnant women (several acupressure points may lead to miscarriage) and those with high blood pressure.
Massage: When received frequently, massage can provide chronic low back pain relief. A massage involves the stroking, kneading, and manipulation of your tissues. Blood flow, which provides oxygen and nutrients to the muscles is increased by these movements. Extra blood also carries waste byproducts that may accumulate away.
Whilst massage is not a proven treatment for herniated discs, it is usually safe and free of side effects. However, massage might not be perfect for you in the event that you suffer from deep vein thrombosis, osteoporosis, skin infections, open wounds, or arthritis in or close to the area to be massaged.
You’ll find over 100 types of massage techniques. A Swedish massage, for example, uses long strokes to impact the superficial layers of the muscles. In contrast, a deep tissue massage uses slow strokes and direct pressure to soothe your layers of muscle and relieve chronic strain. Your massage therapist will work with you to determine what special massage will most likely reduce your pain.
When you start any new medical plan, let your practitioner know if you have any health conditions apart from pain from your herniated disc. Additionally, it is important to be aware that these treatments are best when used as complementary treatments (that can be combined with conventional medicine).
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Sciatica
Lower back pain is one of the most commonly reported symptoms among the general population. Sciatica, is well-known group of symptoms, including lower back pain, numbness and tingling sensations, which often describe the source of an individual’s lumbar spine issues. Sciatica can be due to a variety of injuries and/or conditions, such as spinal misalignment, or subluxation, disc herniation and even spinal degeneration.
Herniation of the nucleus pulposus, abbreviated as HNP, occurs when the nucleus pulposus, frequently described to have a gel-like substance, breaks through the anulus fibrosus, the tire-like structure of the intervertebral disc which acts as a spinal shock absorber.
A herniated disc occurs most frequently in the lumbar region of the backbone or spine, particularly at the L4-L5 and L5-S1 levels (L = Lumbar and S = Sacral). This is primarily because the lumbar spine generally carries the majority of the body’s weight. Since the elasticity and water content of the nucleus decreases with age through the natural process of degeneration, individuals between the ages of 30 and 50 often seem to be �more vulnerable to disc herniation.
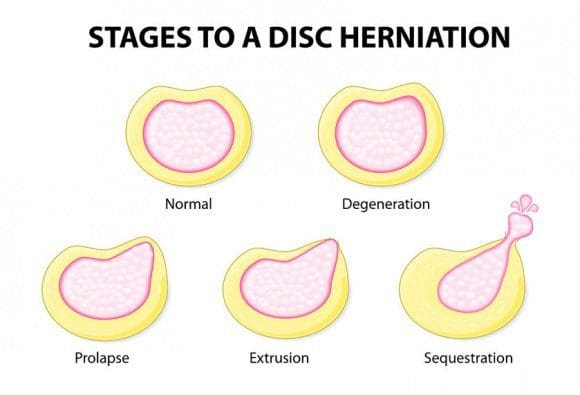
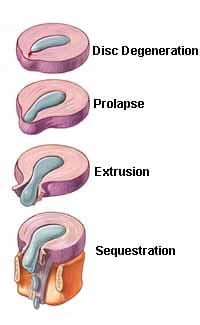
The progression of a herniation of the nucleus pulposus, best known as a herniated disc, can vary and typically occurs gradually over time. There are four stages: (1) disc protrusion (2) prolapsed disk (3) disc extrusion (4) sequestered disc. Stages 1 and 2 are known as incomplete disc herniations, or as a disc bulge, where 3 and 4 are known as complete disc herniations, ruptured discs or herniated discs. Pain may be combined with some radiculopathy, which means deficit. The deficit might include sensory alterations, such as tingling sensations and/or numbness, or motor changes, such as weakness and/or �weight loss. Nerve compression resulting from added pressure, compression or impingement of the spinal nerves due to the substance from the herniated disc is often what causes these changes.
Progression of Herniated Disc
The extremities affected by herniated discs are dependent upon the vertebral level at which they occur in. Consider the following examples:
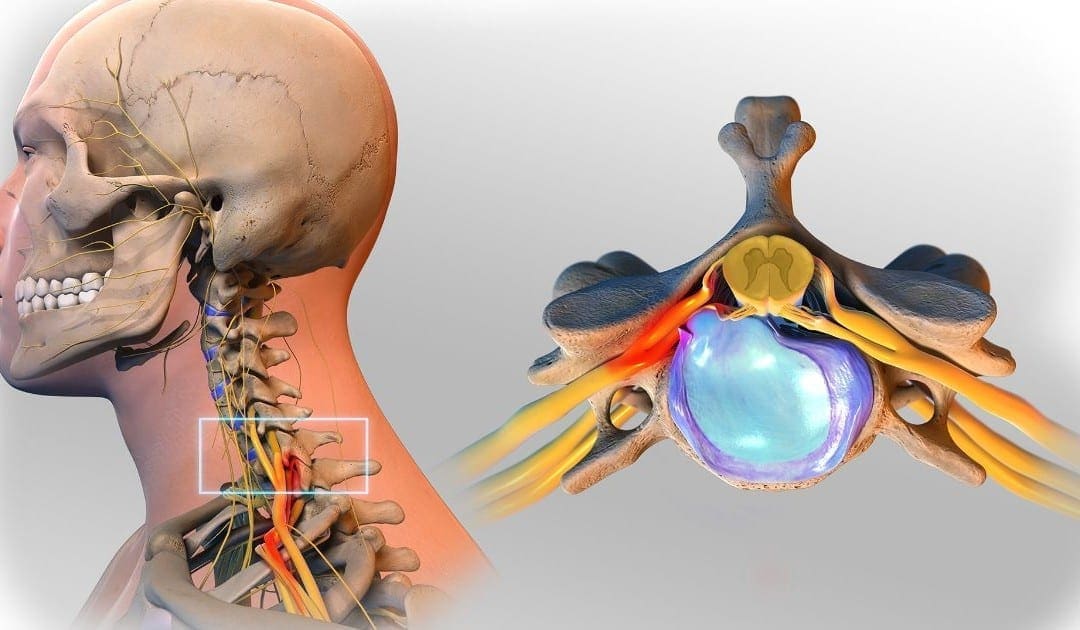
Cervical – Pain, discomfort and other symptoms in the throat, shoulders, and arms.
Thoracic – Symptoms radiate into the chest.
Lumbar – Symptoms extend into the buttocks, thighs, legs and feet. Sciatica is common.
Cauda Equina Syndrome is serious disorder requiring immediate surgical intervention which occurs from from a disc herniation. The symptoms include bilateral leg pain, reduction of perianal sensation (rectum), paralysis of the bladder, and weakness of the anal sphincter.
Analysis of Herniated Discs
The backbone is analyzed with the patient standing and laying down. Because of muscle spasm, a loss of normal spinal curvature may be noted. Radicular pain, described as inflammation of a spinal nerve, may increase if pressure is placed on the affected spinal segment.
A Lasegue test, also known as Straight-leg Raising Test, is often performed to determine the extent of the herniated disc and its manifested symptoms. To perform this test, the patient lies down, the knee is extended, and the hip is flexed. If pain is aggravated or produced, it is an indication the lower lumbosacral nerve roots may be inflamed.
Other neurological tests are performed to ascertain loss of sensation and/or engine function. Reflexes are noted as these changes may indicate the location of the herniation.
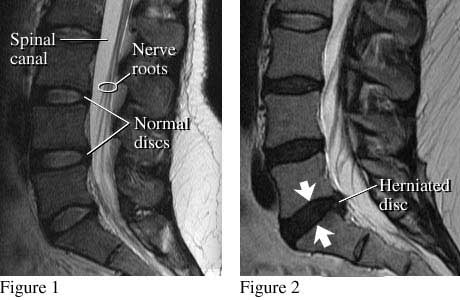
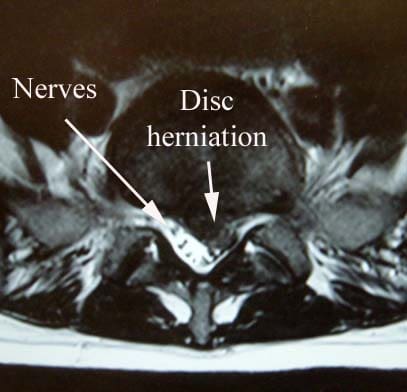
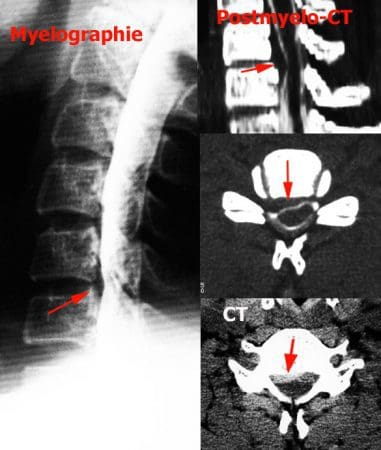
Radiographs can be helpful to determine the presence of a herniated disc, but Computed Axial Tomography (CAT) or Magnetic Resonance Imaging (MRI) provides more detail. The MRI is the best method allowing the physician to find the soft spinal tissues that are unseen in other imaging procedures.
Evidence of HNP
The findings in the examination and evaluations, such as the one below, are compared to earn a diagnosis. This includes ascertaining the precise location of the herniation so treatment options can be reviewed with the patient.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Sciatica
Lower back pain is one of the most commonly reported symptoms among the general population. Sciatica, is well-known group of symptoms, including lower back pain, numbness and tingling sensations, which often describe the source of an individual’s lumbar spine issues. Sciatica can be due to a variety of injuries and/or conditions, such as spinal misalignment, or subluxation, disc herniation and even spinal degeneration.
The previous rehab masterclass on Lisfrancs injuries highlighted the pathogenesis of injuries, the midfoot joint’s relevant factors, and typical injury mechanisms were presented along with diagnostic findings. In this masterclass scientific specialist Dr. Alexander Jimenez discusses the management of Lisfranc injuries…
Management
After the initial injury, it may not be clear exactly what harm the foot has been done to by the athlete. Both athlete and sports medicine staff may confuse. The athlete with subtle stage 1-type injuries will try to ‘run off’ the pain. As they continue and fail to reevaluate they will stop training/competition.
When an injury into the Lisfranc is suspected, the first MTP joint ought to be assessed to exclude a ‘toe’ injury and the ankle checked to exclude an ankle injury. They crutches till they could be properly analyzed and remain non-weightbearing ideally with an Aircast boot and need to ice the foot aggressively.
Non-operative�Treatment of Lisfranc Injuries
A stage 1 accident that’s functionally secure could be handled with a non-weight posture boot or cast for a first two weeks. They can be analyzed for tenderness on palpation over the TMT joint at this time and follow-up x-rays will be required to exclude any latent diastasis of the second and first metatarsal space. If pain-free on palpation and x ray is normal, they could have the weight bearing status assessed using complete weight bearing foot flat and position is raised by a toe. If that is normal they can stay out of the boot using a custom made orthotic and rehabilitation and return to conditioning may begin.
Then the boot is reapplied, if the foot stays painful to palpate or if they neglect raise test and they stay non weight bearing to partial weight bearing for a further four weeks.
For pain along with weightbearing status they’re reassessed in the stage. If these are uneventful then the rehabilitation and reconditioning stream is moved to by the athlete. If problematic they need to be assessed for postponed stabilisation.
The time period to get a injury that is secure could be a month recovery until return to play.
Operative Treatment Lisfranc Injuries
Stage 2 and stage 3 accidents need to have the midfoot surgically stabilized since they’re generally unstable injuries. Interestingly, Hummell et al (2010) recently clarified a successful result in a point 3 football player with non-operative treatment. The objective of surgery is to acquire a fantastic reduction to optimize functional results. Virtually all expert opinions relating to Lisfranc injuries emphasize the importance of gaining as to avoid long- term morbidity from the midfoot.
Myerson et al (1986) identified some things that result in poor outcome for example residual angulation between the metatarsals, diastasis greater than 2mm between the first and second metatarsals. Correcting these defects is essential to avoid long-term complications like chronic functional disability , post-injury arthritis and instability with walking.
To obtain reduction of the TMT joints reduction is usually necessary to remove any tissue for example little bone fragments or ligaments. Reduction is supported with fluoroscopy. Nevertheless, in instances percutaneous fixation can be accomplished if the dislocation can be reduced by the surgeon under fluoroscopy and stabilize the joints together with wires and screws. However, most will require an open reduction to properly visualize and access of the joints that are tarsometarsal.
The choice of hardware for surgery is debatable surgeons the choices are:
1. Cannulated screws;
2. Solid, Non-cannulated screws;
3. K wires;
4. Bridge plates for tarsometatarsal joints.
At a thorough literature review, Stavlas et al (2010) found that injuries to the first few metatarsals (lateral and middle column) react well with screw fixation, whereas harms to the fourth and fifth metatarsals (lateral column) may respond well with K wire fixation.
Post-Operative Rehabilitation
This will often involve a non-weight- bearing cast or boot to get the first 3 weeks with a CAM/Aircast boot used for the subsequent three to five weeks so that the athlete is complete weight. Weight is slowly built around the eight to twelve months post-operative interval so that in a custom-made orthotic the athlete can weight bear by 3 months that.
The hardware is often removed at 12-16 weeks post-op in lighter athletes and in heavier athletes (>200 lbs) it’s been suggested to take out the hardware in 24 weeks (Nunley and Verullo 2002).
Post-surgery the results are generally favourable. Nunley and Vertullo (2002) discovered that in stable stage 1 harms, great outcome was found with conservative treatment with athletes back to game at 11-18 weeks post-injury. Athletes with stage 2 injuries had good outcomes with ORIF and returned to play 12-20 weeks. Period 3 accidents were not described.
Physiotherapy
The athlete will see that the physiotherapist athletic coach weekly to regain mobility. Interventions will be necessary in addition to direct mobilizations to restore the accessory movements.
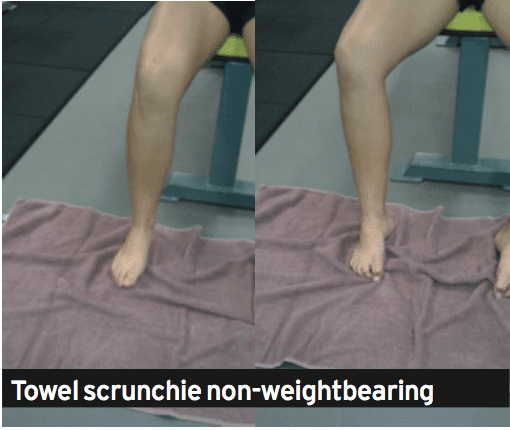
The therapist can also start intrinsic foot muscle exercises at approximately 8-10 weeks post-operative using the weight bearing exercises being postponed until week 12 post-operative. These exercises are designed to retrain the arch to be controlled by the foot muscles. Exercises that will satisfy this are towel scrunchies, cup drop, matt equilibrium and lunge exercises (see below).
The movement can be measured by the therapist regularly with knee.
1. Towel scrunchies. These have been used by therapists to strengthen the muscles that support the foot’s arch.
A. Place a towel onto a tiled or wooden floor (carpet will not work.
B. set the foot relaxed on the towel with all the foot in line with the knee and hip. The feet should be pointing directly ahead.
C. Initiate the movement by attempting to firstly raise the arch. Think about drawing the ball of the foot to the heel. You will see that the arch is going to lift.
D. Next use all the feet to loosen the towel under the foot.
E. Relax the foot and start again.
F. This exercise doesn’t cause any soreness the next day; the muscles should start to fatigue.
G. The development is seated, to standing on one leg and standing on two legs.
2. The cup drop. This can be an interesting and innovative way to integrate inherent arch muscle function and anti- pronator muscle function that is extrinsic using hip muscles that are hip, in particular the gluteus maximus and medius. During weight bearing, the hip is prevented by the gluteus medius muscle from rotating and adducting, and this action works well with the arch muscles preventing excess pronation.
A. Place a few small objects like marbles about one foot in front of your body.
B. Reach forward with the foot and also pick up the masonry with the feet. Of clawing at the masonry this activity will trigger the muscles.
C. Whilst holding the marble in the feet, circle the hip outwards into both sides of the body then behind the body and set the marble at a cup placed at 45 degrees to the cool.
D. It is necessary that the foot stays turned outwards as this retains the gluteus active.
3. The mat balance. This exercise incorporates these together with the arch muscles and adds contraction of the calf muscles both the gastrocnemius and soleus. The drill is done on a gentle matt, to create the exercise challenging. The mat surface generates an unstable situation, and there is mounting evidence that indicates that by incorporating a component of balance control to a rehab exercise may be necessary since the perturbations in movement excite all of the position feedback nerve endings which control proprioception. The nerve endings feedback to the muscle control system and also this potentiates the stimulation of their control muscles.
A.Place a soft mat in addition to a 6mm piece of timber or hard rubber mat. The thicker the mat that the harder the exercise.
B. Stand on the mat but just with the third, fourth and fifth feet connected with the matt. The first and second feet should be hanging unsupported from the mat.
C. This position of the foot makes a scenario whereby the foot wishes to turn in under gravity’s effect. The long pronation muscles in the shin and the muscles need to control the interior of the foot to keep it up and of the floor.
D. Attempting to keep equilibrium (and this will be hard when the matt is too soft), marginally boost the heel to participate the calf muscles.
E. Hold this position for 1-2 seconds and then slowly lower down to the beginning position.
F. Perform 3 sets of 10 repetitions.
4. Lunge with towel scrunchie. This workout is a high-level integration workout which combines gluteals and arch muscles whilst performing a exercise such as the lunge. This sort of exercise is done in late phase rehab prior to running as the muscle activation patterns more resemble what should happen in conducting concerning limb assistance — that is, the arch muscles control pronation, the quads control the knee and patella and the gluteus medius affirms the hip throughout foot strike.
A. Stand on a towel, very similar to Exercise 1 above.
B. Put some theratubing around a post and also wrapped round the upper tibia. The ring has to be guided to pull the tibia inwards, not outwards. This pulling in of the tibia can cause the top leg to follow along with this is imitating hip adduction and internal rotation. The goal of the exercise is to prevent it by maintaining the kneecap aligned with the next toes. The gluteals finally have to work to permit this to occur. Inwards and way would fall from the third toe, if they did not.
C. Gradually lower down into a lunge whilst keeping the monitoring of the kneecap over the next toe and also keeping the towel scrunched up under the foot.
D. Lift up to full knee extension. Rest. Start again.
Strength
The athlete will initially load throughout the foot with the foot impartial. Exercises such as split squat, high- foot leg press and posterior string movements such as deadlifts and stand pulls may start in the weight bearing phase. Exercises requiring more ankle dorsiflexion and so midfoot pronation will be delayed for a couple of weeks until strength and confidence improve (traditional one-leg squats, deadlifts and leg press).
Rehabilitation
The graded progressions for your athlete have been well summarized by Lorenz and Beauchamp (2013). The progression is a staged progression to gradually regain strength and confidence from landing and push-off positions. If the stage is pain free, the progressions could be made, the athlete could do selection and without compensations to the movement.
1. Bilateral heel raises
2. Heel raise,�single-leg eccentric lower
3. Single leg-heel raise from standing
4. Bilateral leaning heel raises
5.�Bilateral leaning heel raises, single leg�eccentric lower
6. Single-leg leaning heel raises
7. Single-leg triple extension heel raises
8. Mini-tramp low Impact exercises
A. Bilateral jumps in position
B. turns in place (two legs).
C. turns in place (two legs).
D. Jog in place
E. Three hops uninvolved, one hop involved
F. Two hops uninvolved, two hops involved
G. One hop uninvolved three hops involved
9. Agility ladder
A. Different frontal transverse plane designs
B. Hopscotch to involved negative (two to one)
10. Single-leg A/P jumps in place
11. Single leg M/L jumps in place
12. Single leg transverse jumps in position
13. Single leg hops in agility ladder
Return To Running
The choice as to when to remove the hardware will influences the choice. As a general rule, when the screws and wires are eliminated, the athlete will be permitted to attend and walk gym sessions to the elimination but running will probably be delayed.
The athlete is encouraged to walk a treadmill using a incline to promote the push. This can start at 12 weeks . The athlete may quickly advance into backward and forward running on grass and it’s expected they are doing so by week 14 depending on when the hardware was taken away. As they progress through running they could slowly begin to construct speed they reach sprint speed.
Gentle off-line running drills such as weaving, easy bypassing, stepping and caricoca drills would normally be started in around 16 weeks post-op and progressed into tougher single-leg and hard-cutting plyometrics as pain allowed. It would be expected that by 20 weeks post-op, the foot has sufficient strength, range of movement and confidence to start team- based ability function. Prior to this, the athlete can experience some frequent field hop tests like tests and single-leg triple jump to assess differences in abilities.
Functional Tests
A evaluation that is practical sports-specific is a test or field test that aims to mimic the movements. The use of practical tests aims to recognize imbalances and will boost confidence in both patient and the clinician the injured patient can return to play. It is effectively a way of reducing the hazard. The evaluation ought to be an objective, measurable and quantifiable test that includes a component of:
Strength
Agility
Power
Balance Neuromuscular status.
The aspects can be incorporated into practical tests such as agility and jumps/ movement evaluations.
The hop tests comprise:
1. Single jump
2. Triple hops
3. Crossover jump
4. 6m timed jump.
Single limb evaluations are necessary as study proves that dual limb and modified double limb tests don’t demonstrate any differences between groups since the uninvolved limb can mask deficits of the thoracic (Myer et al 2011). Single-leg hopping evaluations are sensitive enough to discover asymmetry, and specifically the crossover hop test at six months post-op is the most sensitive of these tests at predicting future function of the knee along with the 6m timed test is the most vulnerable and sensitive of under normal function at six months . (Logerstedt et al 2012).
Therefore isolated single-limb performance tests may provide a critical element to field-based operational performance testing to identify deficits in reduced limb performance, including deficits in force attenuation functional power and postural stability. The capability to maintain isolated single limb electricity is significant in sports that require significant control in stepping edge and cutting manoeuvres. This may require and ability to regenerate and divert and then to absorb force on one limb the motion.
Conclusion
Injuries are uncommon in athletes on account of the severe consequences they could have on athletic role, the sports medicine specialist has to be well versed in evaluation and initial management. They can be challenging injuries manage and to diagnose for the clinician.
Stable Lisfranc injuries with no instability can be handled conservatively stage 2 and 3 accidents involving diastasis of their second and first metatarsals requires consideration. This can be done usually using the open reduction and fixation with screws, K cables and/or plates
Rehabilitation after surgery will take no less than 12-16 weeks it’s typical for the return to sport to take in contact sport athletes. Successful return to competition time frames extend to the 20-24 week stage post-surgery and rehab will involve reduction of the entire limb kinetic chain but also not only the foot muscles.
References
1. Castro et al (2010) Lisfranc joint ligamentous complex: MRI with anatomic correlation in cadavers. AJR. 195; W447-455.
2. Chiodo CP and Myerson MS (2001) Developments and advances in the diagnosis and treatment of injuries to the
tarsometatarsal joint. Orthop Clin North America. 32(11); 11-20.
3. Garrick JG and Requa RK (1988) The epidemiology of foot and ankle injuries in sports. Clinical Sports Medicine. 7: 29-36.
4. Hummell et al (2010) Management of a stage 3 Lisfranc ligament injury in a collegiate football player. Athletic Training and Sports Health Care. 10(10); 1-5.
5. Logerstedt et al (2012) Single-legged hop tests as predictors of self reported knee function after ACL reconstruction. The Delaware-Oslo ACL cohort study. American Journal of Sports Med. 40(10); 2348-2356.
6. Lorenz and Beauchamp (2013) Case report. The functional progression and return to sport criteria for a high school football player following surgery for a Lisfranc injury. The International Journal of Sports Physical Therapy. 8(2); 162-171.
7. Myer GD, Schmitt LC, Brent JL, Ford KR, Barber KD, Scherer BJ, Heidt RS, Divine JG and Hewett TE (2011) Utilization of modified NFL combine testing to identify functional deficits in athletes following ACL reconstruction.
Journal of Sports Physical Therapy. 41(6); 377- 387.
8. Myers et al (1994) Midfoot sprains in collegiate football. American Journal of Sports Medicine. 21; 392-401.
9. Myerson et al (1986) Fracture dislocations of the tarsometatarsal joints: end results correlated with pathology and treatment. Foot and Ankle. 6(5); 225-242.
10. Nunley JA and Vertullo CJ (2002) Classification, investigation and management of midfoot sprains: Lisfranc injuries in the athlete. American Journal of Sports Medicine. 30(6); 871-878.
11. Ouzounian TJ and Sheriff MJ (1989) In vitro determination of midfoot motion. Foot and Ankle. 10; 140-146.
12. Rankine et al (2012) The diagnostic accuracy of radiographs in Lisfranc injury and the potential value of a craniocaudal projection. AJR. 198; W365-369.
13. Shapiro et al (1994) Rupture of the LisFranc�s ligament in athletes. American Journal of Sports Medicine. 22(5); 687-691.
14. Stavlas et al (2010) The role of reduction and internal fixation of Lisfranc fracturedislocation: a systematic review. International Orthopaedics. 34; 1083-1091.
Herniated lumbar discs, although considered common, can be very debilitating and disabling. While it may be impossible to prevent disc herniations, understanding the mechanism of injury and implementing that knowledge can cut the odds of developing this unpleasant injury. A range of factors may promote lumbar disc damage or injury. The mechanism of injury for herniated discs often involves flexion, compression and twisting of the lumbar spine.
Mechanism of Injury: Herniated Discs
The lumbar spine’s discs are specialized connective tissue structures which function as shock absorbers between the spinal bones or vertebrae of the spine. Intervertebral discs are springy in nature due to a moist, jelly-like center portion known as the nucleus pulposus. The nucleus pulposus is contained and surrounded by a more layered, fibrous tissue that makes up what is known as the annulus fibrosis. Herniated discs or ruptured discs occur when harm to the annulus fibrosis causes the nucleus pulposus material to escape its boundaries and protrude outward in the disc.
Flexion
Where lumbar disc herniations occur regularly in a normal setting, these aren’t easily reproduced in a research setting. It is notable that in scientific research studies, where disc herniations were created in animal or human lumbar spine specimens, most demanded a small amount of spine flexion. Because of this, Stuart McGill, Ph.D., author of the book “Low Back Disorders,” concludes that repeated or prolonged spine flexion will be the primary mechanism leading to lumbar disc herniation. In a lab setting, McGill and other scientific doctors found that the way they could produce herniated disc injuries was to place weight, or a weight, onto the spine while bending into flexion. These circumstances are consistent with what could happen with repetitive lifting activities where the spine is flexed forward.
Compression
A research presented in 2001 in the journal “Clinical Biomechanics” demonstrated a link between compression of the spinal joints, technically known as vertical loading, and disc herniation. Even though the analysis used spinal sections taken from the necks of pigs, the researchers tried to replicate loading patterns common to the lumbar spines of humans. In the scientific study, severe and more frequent cases of herniated discs resulted when compression forces on the spinal bones had been increased. However, compression forces were essential to cause damage or injury such as disc herniations, that were subjected to repetitions of forward and backward bending. The authors reasoned that flexion and extension moves likely play a larger part than compression alone in inducing disc herniations. To put it differently, the spine can resist compression forces, such as lifting, when in a vertical position. Including a load whilst bending forward and backward though, may quickly spell difficulty for the individual.
Twisting
Another study published in 2010 in “Cinical Biomechanics” analyzed the role of axial torque, or twisting, in disc herniation. Using an animal model, the researchers discovered that disc herniation was not caused by twisting that was isolated. However, twisting did damage the annulus fibrosis. With damage to the annulus, the discs were more vulnerable to rupture or herniation when subjected to flexion movements. This implies that if the mechanism of injury of a disc herniation is flexion, these may be contributed to by damage brought on by twisting weakened discs.
Occupational Factors
A study published in 1987 in the “Journal of Chronic Diseases” examined the risk of lumbar herniated discs associated with occupation. The researchers noted that the risk for this condition is greater among men in blue-collar jobs in contrast to those in white collar jobs. This relates to increased lifting and bending activities among blue-collar workers when compared with white-collar employees. The writers noted less variation by occupational groups among women. The risk of lumbar disc herniations, however, was greater among women who described their work as strenuous. An additional finding that may relate to the spinal flexion mechanism of injury is that the risk of lumbar disc herniations is high among individuals whose work entails driving an automobile. Sitting while driving places the lumbar spine in a sustained posture of slight flexion.
Diagnosis for Herniated Discs
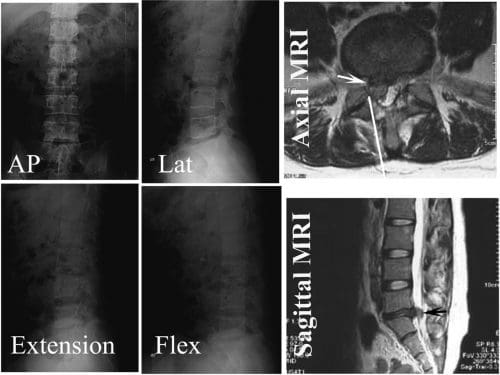
Lower back pain and symptoms associated with sciatica, are common manifestations resulting from lumbar spine disc herniation. Healthcare professionals, including chiropractors who specialize in sciatica, can help diagnose herniated discs as well as help determine the source of the individual’s symptoms. A spine specialist may provide the patient with or direct them to a clinic to have x-rays, MRI’s or CT scans to properly determine the presence of a herniated disc. Seeking immediate medical attention is essential towards the patient’s recovery.
MRI of a Lumbar Herniated Disc
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Sciatica
Lower back pain is one of the most commonly reported symptoms among the general population. Sciatica, is well-known group of symptoms, including lower back pain, numbness and tingling sensations, which often describe the source of an individual’s lumbar spine issues. Sciatica can be due to a variety of injuries and/or conditions, such as spinal misalignment, or subluxation, disc herniation and even spinal degeneration.
Sometimes called a ruptured or slipped disc, your lower back pain often occurs due to a herniated disc in the lumbar spine. In fact, it’s one of the most common causes of low back pain, in addition to sciatica.
Between 60 and 80 percent of people will experience back pain at least once throughout their lifetime. A high proportion of these individuals will have low back and leg pain brought on by a herniated disc.
Most people feel better with just a few weeks or months of non-surgical treatment though a disc can sometimes be very debilitating. Surgical therapy can also help alleviate discomfort and disc pain if symptoms are not resolved.
Nonsurgical Treatment of Herniated Discs
After the first injury, the doctor may recommend cold treatment and drugs.
During the first 24 to 48 hours, cold treatment helps to reduce pain by decreasing blood flow, muscle soreness, and swelling. Never use ice or cold directly to skin; instead wrap item or the ice pack in a towel and then apply for more than 15 minutes.
Medications may include an anti-inflammatory to lessen swelling, a muscle relaxant to calm anxiety, and a pain-killer to relieve intense but alleviate pain (severe pain).
Mild to moderate pain may be treated with anti inflammatory anti inflammatory drugs (NSAIDs). These work by relieving pain and swelling.
Please discuss use with your physician.
Usually heat treatment can be applied. Blood circulation increases to heat and relax soft tissues. Higher blood flow will help to flush out toxins that may accumulate in tissues as a consequence of muscle spasm and intervertebral disc injury. Never use heat directly to skin ( just like chilly); rather, wrap the heat source in a thick towel for no longer than 20 minutes.
Spinal Injection
Leg weakness is developing, or if leg pain is intense, the doctor may prescribe an anabolic steroid injection. Anti-inflammatory medication is put by an epidural steroid injection into the space near the nerves on your lumbar spine. Before beginning this therapy you need to discuss this option with your doctor and ask.
Physical Therapy
The doctor may recommend physical therapy. The doctor’s orders are transmitted to the physical therapist by prescription. Physical treatment includes a mixture of treatments to reduce pain and improve flexibility. Heat and ice therapy stretching, and grip are a few examples, but your therapist may work together to develop the best treatment plan for the pain and symptoms.
Surgical Treatment of a Lumbar Herniated Disc
If symptoms does not relieve spine surgery is known as. Persistent pain, leg fatigue, or lack of function requires additional evaluation. Rarely, does a lumbar herniated disc cause bowel/bladder incontinence or groin/genital numbness, which demands immediate medical attention.
In case surgery is recommended, constantly ask what outcomes you can expect and the goal of the surgery. You have to understand all details of what’s being advocated, and do not hesitate to get a second opinion. Surgery is a big decision, so you odn’t wish to rush in to it.
To alleviate nerve pressure and leg pain, surgery generally involves a discectomy (elimination of all or part of the intervertebral disc).
In addition, by removing some of the bone covering the nerve the surgeon may need to access the herniated disc. This procedure is called a laminotomy.
These processes can be done using minimally invasive methods. Minimally invasive spine surgery doesn’t require large incisions, but instead uses apparatus like endoscope and a microscope during the surgery and tiny specialized instruments and cuts.
Can You Prevent a Lumbar Herniated Disc?
Earlier we advised you that a cause of a lumbar disc is aging, and that can’t be avoided by us. Does that mean that you can not do anything to prevent a lumbar herniated disc?
Of course not. There are numerous factors which are also to take care of your spine, and within your hands, observe your posture, do not smoke, make healthy food choices, exercise, and use body mechanics, especially whenever you’re lifting something.
They’re usually healthy actions you can take to try and prevent lower back pain, although doing all of those things won’t ensure that you never get a lumbar herniated disc.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Sciatica
Lower back pain is one of the most commonly reported symptoms among the general population. Sciatica, is well-known group of symptoms, including lower back pain, numbness and tingling sensations, which often describe the source of an individual’s lumbar spine issues. Sciatica can be due to a variety of injuries and/or conditions, such as spinal misalignment, or subluxation, disc herniation and even spinal degeneration.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine