Emmanuel Korir, Michael Saruni and Mickael Hanany qualified to the IAAF (International Association of Athletics Federation) World Championships over the weekend.
Running in Nairobi, Kenya, Korir qualified to the 800m final with a time of 1:45.50 in the first heat, Saruni followed with a time of 1:46.10 in the second. In the men�s final, Korir (1:43.86) notched the crown and Saruni took third with a personal best of 1:44.61.
The All-Americans garnered a spot on the Kenya national team which heads to London, England to compete at the World Championships on August 5-8.
Also making his way to London will be former UTEP track and field star Mickael Hanany (France). Hanany took gold at the 2017 Euro Superleague with a leap over 2.26m (7-5) in the high jump. The seven time All-American will compete in his fourth IAAF World Championship.
The Nigerian trails will take place on July 7-8.
For more information on UTEP track and field, follow the Miners on Twitter (@UTEPTrack) and on Instagram (uteptrack).
Check Also
New UTEP Tennis Head Coach Ivan Fernandez announced his first two signees on Friday. Erandi �
A good read to understanding alteration of motion segment integrity (AOMSI) is the article �Biomechanical Analysis of clinical instability in the cervical spine� White, et al., Clin Ortho Relat Res, 1975;(109):85-96.
AOMSI is a biomechanical analysis. It�s all about numbers that have clinical meaning and significance. Threshold values have been determined that quantify without a doubt the patient has serious injury. It is a test of structural integrity of the ligaments interconnecting the motion segments. In this case, structural integrity has to do with the material properties of ligament tissue. Those properties include strength and flexibility. When a material is both strong and flexible, it�s called a semi-rigid material. Strength is related to the composition of the material. Strength might be thought of as load carrying capacity before failure.
Mechanism of Injury: Ligaments
Ligament tissue has previously been bench tested to describe its physical characteristics of stress/strain. That is, given so much load (stress) how much elongation will occur (strain). During normal physiologic loads the ligament remains intact and recoils to its original length when the load is removed. If the load becomes too large the materials (ligaments) begin to yield. They go past their elastic limit. When this happens the (strained) ligament fibers will not return to their original shape. The ligament loses its restraining capacity to hold the joint in normal stabilization and hypermobility occurs.
The ligaments, if sufficiently strained or avulsed results in AOMSI. The following paragraphs illustrates that if AOMSI is found there must be gross destruction or yielding of multiple ligaments. We need to build a BIG motion segment with Velcro ligaments. When you tear them off, they make a really nice ripping noise. That drives home the point.
In the White et al work, they found that the motion segment stayed intact i.e., less than 11 degrees� rotation (angualr mtion) and less than 3.5 mm translation, until they transected over 50% of the ligaments from an anterior or posterior approach. And when they transected from either approach the loss of stability was not linear but suddenly catastrophic. And they meant that suddenly the two vertebra totally separated in rotation or translation.
Suddenly Separated: pulled apart, head off of body, all neural components compromised, paralysis. Keeping that in mind, what are the injuries of someone just under the threshold? Severe to very severe. They stand the possibility of a serious event with much less force.
Prevalence of Ligament Injury: AOMSI
If AOMSI is detected, think about more than 50% of ligaments transected. That will start to explain the seriousness of the finding. In a patient/child that demonstrates hypermobility everywhere, then you take a statistical average of all segments, and look at the aberrant statistical finding if it exists. There are clues to injury everywhere when you understand what the numbers mean in reference to stability and function.
To diagnose ligament laxity, it is imperative that imaging be performed and a basic flexion-extension x-ray is all that is required. In today�s medical economy, advanced imaging of MRI or CT Scan, although accurate becomes an unnecessary expenditure and an x-ray renders very accurate demonstrative images to conclude a definitive diagnosis. In determining if there is an impairment, it is necessary to follow the AMA Guides to the Evaluation of Permanent Impairment as the 4th, 5th and 6th editions all render an impairment for AOMSI as sequella to ligament laxity, which is damage to the ligament from trauma.
This document is intended to serve as a simple explanation as to the severity of ligament damage and how to demonstrably diagnose the injury. It is also critical to remember that ligament do �wound repair.� In normal physiology, ligaments grow during puberty from cells within the ligaments called fibroblasts. They produce both collagen (white) and elastin (yellow) tissue, which gives the ligaments both tensile and elastic strength. Upon puberty the cells stop producing tissue and remains dormant. Upon injury, the fibroblast reactivates, but can only produce collage leaving the joint wound repaired in an aberrant juxtaposition (place) with poor movement abilities due to the lack of the requisite elastin. In turn, according to Hauser et. Al (2013) this leads to permanent loss of function of the ligament and arthritis of the joint. This is not a speculative statement; it is based upon Wolff�s that dates back to the late 1800�s and has been a guiding principle in healthcare for more than a century.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
References:
White, et al., Clin Ortho Relat Res, 1975;(109):85-96
Hauser, Dolan,Phillips, Newlin, Moore Woldin, B.A.(2013) Ligament injury and healing: A review of current clinical diagnostics and therapeutics.The Open Rehabilitation Journal, 6,1-20.
Additional Topics: Weakened Ligaments After Whiplash
Whiplash is a commonly reported injury after an individual has been involved in an automobile accident. During an auto accident, the sheer force of the impact often causes the head and neck of the victim to jerk abruptly, back-and-forth, causing damage to the complex structures surrounding the cervical spine. Chiropractic care is a safe and effective, alternative treatment option utilized to help decrease the symptoms of whiplash.
When the aberrant sequela to victims in car crashes has been investigated, providers often overlook and concurrently underestimate the tissue pathology and resultant biomechanical failures of spinal ligamentous damages commonly known as �strain � sprain.� In addition, the courts have been �blinded� by rhetoric in allowing this pathology to be deemed transient. There is an ever growing body of scientific literature that verifies strain – sprain as permanent pathology, which is the standard being taught in today�s medical and chiropractic academia.
In addition, strain � sprain as sequela to whiplash, renders a 25% whole person impairment based upon the American Medical Association�s Guide to the Evaluation of Permanent Impairment fifth and sixth editions.
Whiplash Associated Disorder Sequela Injuries
Juamard, Welch and Winkelstein (2011) reported:
��Rear end accelerations have been used to study the response of a variety of soft tissues in the cervical spine, including the facet capsular ligament. For simulations of whiplash exposures, the strains in the capsular ligament were found to be two � five times greater than those sustained during physiological motions of the cervical spine. In a similar but separate study, the facet joints of the cervical spine�s that were previously exposed to a whiplash injury ridden exercise under low � level tension and found to undergo elongations nearly 3 times greater than on exposed ligaments for the same tensile loads. Those capsular ligaments were also found to exhibit greater laxity after the purported injury. Since increased laxity may be linked to a reduction in the joints ability to stabilize the motion segment during sagittal motion, this finding suggests that whiplash exposure may alter the structure of the individual�s tissues of the facet, such as the capsular ligament, and/or the mechanotransduction processes that could maintain and repair the ligamentous structure. Accordingly, such an injury exposure could initiate a variety of signaling cascades that prevent a full recovery of the mechanical properties of the tissues of the facet joint.� (Pg 15)
Simply put, if we focus on the last sentence above, this �prevents a full recovery of the mechanical properties of the tissues of the facet joint,� which is referencing the ligaments of the spine that make up the tissues of the facet joint. In lay terms; it means that once injured, a joint is permanently damaged and it is demonstrable on x-rays with an extension and flexion view that does not have to show a full dislocation. Therein lies the core of the issue. Most radiologists are not trained in the latest literature on biomechanical tissue failures and therefore underreport the pathology.
Last month I attended a presentation by Michael Modic MD, Neuroradiology, a nationally renowned educator in neuroradiology who focuses on spondylolisthesis (vertebral segmental abnormal movements) and I asked a simple question �why don�t radiologist report more on abnormal positioning due to biomechanical failure as a result of ligament pathology� and his answer was �because their training focuses more on disease pathology.� Although I agree that is critical, so are biomechanical failures that lead to chronic degeneration, which is epidemic in our society. Simply look at the posture of our elderly for verification and much of that started with a simple �fender bender� years ago where the strain-sprain was either undiagnosed or deemed transient and not treated.
Ligament Pathology Diagnosis and Prognosis
The above scenario is why the American Medical Association values ligament pathology at 25% whole body impairment. There is also a growing body of doctors who are trained and credentialed in Spinal Biomechanical Engineering that understand how to create a diagnosis and prognosis, along with treatment plans around ligament pathology and fully understand the long-term effects of damaged facet joint tissues. These doctors are currently educating, based upon the current scientific literature their respective radiology communities to be able to diagnose and document the full extent of the injuries sustained.
We must also recognize that there is a significant amount of evidence in the scientific literature that verifies ligamentous damage as permanent and refutes the rhetorical claim of �transient.� In the end, it must be the facts of human physiology verified by science that sets the standards of healthcare and not deceptive rhetoric at any level.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
References:
Cocchiarella L., Anderson G., (2001) Guides to the Evaluation of Permanent Impairment, 5th Edition, Chicago IL, AMA Press
Juamard N., Welch W., Winkelstein B. (July 2011) Spinal Facet Joint Biomechanics and Mechanotransduction in Normal, Injury and Degenerative Conditions, Journal of Biomechanical Engineering, 133, 1-31
Additional Topics: Weakened Ligaments After Whiplash
Whiplash is a commonly reported injury after an individual has been involved in an automobile accident. During an auto accident, the sheer force of the impact often causes the head and neck of the victim to jerk abruptly, back-and-forth, causing damage to the complex structures surrounding the cervical spine. Chiropractic care is a safe and effective, alternative treatment option utilized to help decrease the symptoms of whiplash.
According to the American Academy of Orthopedic Surgery �The most common soft tissues injured are muscles, tendons, and ligaments.
Acute injuries are caused by a sudden trauma, such as a fall, twist, or blow to the body. Examples of an acute injury include sprains, strains, and contusions.�� (http://orthoinfo.aaos.org/topic.cfm?topic=A00111) We must also not forget that there are other soft tissues that can get injured and the true definition of soft tissue, which is anything not bone is soft tissue.
This includes the brain, lungs, heart and any other organ in the body. However, in medicine soft tissue injuries are commonly known to be limited to the muscles, ligaments and tendons.
Soft Tissue Injury Classification
When we look at the type of structures that muscles, tendons and ligament are composed of, we will realize that they are connective tissue. According to the National Institute of Health �Connective tissue is the material inside your body that supports many of its parts. It is the “cellular glue” that gives your tissues their shape and helps keep them strong. It also helps some of your tissues do their work (http://www.nlm.nih.gov/medlineplus/connectivetissuedisorders.html). Unlike fracture repair where the bone is replaced and usually heals properly if aligned and rested, connective tissue disorders undergo a different type of wound repair that has aberrant tissue replacement as sequella to bodily injury and has subsequent abnormal permanent function.
If we focus on sprains or ligamentous injuries, according to the American Academy of Orthopedic Surgery there are three types of sprains:
Sprains are classified by severity:1
Grade 1 sprain (mild):�Slight stretching and some damage to the fibers (fibrils) of the ligament.
Grade 2 sprain (moderate):�Partial tearing of the ligament. There is abnormal looseness (laxity) in the joint when it is moved in certain ways.
Grade 3 sprain (severe):�Complete tear of the ligament. This causes significant instability and makes the joint nonfunctional.
Regardless of the severity of the sprain, there is tissue damage or bodily injury and the next step is to determine if there is healing or wound repair. According to Woo, Hildebrand, Watanabe, Fenwick, Papageorgiou and Wang (1999) ��as a result the combination of cell therapy with growth factor therapy may offer new avenues to improve the healing of ligament and tendon. Of course, specific recommendations regarding growth factor selection, and timing and method of application cannot be made at this time.
Previous attempts at determining optimal doses of growth factors have provided contradictory results. Although growth factor treatment has been shown to improve the properties of healing ligaments and tendons, these properties do not reach the level of the uninjured tissue.� (p. s320)
�No treatment currently exists to restore an injured tendon or ligament to its normal condition.�, stated Dozer and Dupree (2005). (pg. 231).
Soft Tissue Recovery Process
According to Hauser, Dolan, Phillips, Newlin, Moore and Woldin (2013) �injured ligament structure is replaced with tissue that is grossly, histologically, biochemically and biomechanically similar to scar tissue. Fully remodeled scar tissue remains grossly, microscopically and functionally different from normal tissues� (p. 6) �the persisting abnormalities present in the remodeled ligament matrix can have profound implications on joint biomechanics, depending on the functional demands placed on the tissue.
Since remodel ligament tissue is morphologically and mechanically inferior to normal ligament tissue, ligament laxity results, causing functional disability of the affected joints and predisposing other soft tissues in and around the joints further damage.� (p.7) �studies of healing ligaments have consistently shown that certain ligaments do not heal independently following rupture, and those that didn�t feel, do so characteristically inferior compositional properties compared with normal tissue. It is not uncommon for more than one ligament undergo injury during a single traumatic event.� (p.8) �osteoarthritis for joint degeneration is one of the most common consequences of ligament laxity.
Traditionally, the pathophysiology of osteoarthritis was thought to be due of aging and wear and tear on the joint, but more recent studies have shown that ligaments play a critical role in the development of osteoarthritis. Osteoarthritis begins when one or more of ligaments become unstable or lax, and the bones began to track improperly and put pressure on different areas, resulting in the rubbing the bone on cartilage. This causes breakdown of cartilage and ultimately leads to deterioration, whereby the joint is reduced to bone on bone, a mechanical problem of the joint that leads to abnormality of the joints mechanics. Hypomobility and ligament laxity have become clear risk factors for the prevalence of osteoarthritis.� (p.9)
Looking globally at the research over the last 16 years, in 1999 it was concluded that the most current treatments to repair or heal the injured ligament do not reach the level of the uninjured tissue. In in 2005 it was concluded that no treatment currently exists to restore an injured tendons or ligaments to its normal condition. In addition the current standard of ligament research in 2013 concluded that that ligaments do not feel independently, but damage ligaments are a direct cause of osteoarthritis and biomechanical dysfunction (abnormality of joint mechanics). The latest research has also concluded that ligament damage or sprains is the key element in osteoarthritis and not simply aging or wear and tear on the joint.
As a result it is now clear based upon the scientific evidence that a soft tissue injury is a connective tissue disorder that has permanent negative sequela and is the cause of future arthritis. This is no longer a debatable issue and those in the medical legal forum who are still arguing �transient soft tissue injuries� are simply rendering rhetoric out of ignorance and a possible ulterior motive because the facts clearly delineate the negative sequella based upon decades of multiple scientific conclusions.
The caveat to this argument is that although there is irrefutable bodily injury with clear permanent sequella, does it also cause permanent functional loss in every scenario? Those are two separate issues and as a result of the function of ligaments, which is to connect bones to bones the arbiter for normal vs. abnormal function is ranges of motion of the joint. That can be accomplished by either a two-piece inclinometer for the spine, which according to the American Medical Association Guides to the Evaluation of Permanent Impairment, 5th Edition (p. 400) is the standard (and is still the medical standard as the 6th Edition refers to the 5th for Ranges of motion).
The other diagnostic demonstrable evidence to conclude aberrant function is to conclude laxity of ligaments through x-ray digitizing. Both diagnostic tools confirm demonstrably loss of function of the spinal joints. ��
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
Woo S, Hildebrand K., Watanabe N., Fenwick J., Papageorgiou C., Wang J. (1999) Tissue Engineering of Ligament and Tendon Healing, Clinical Orthopedics and Related Research 367S pgs. S312-S323
Tozer S., Duprez D. (2005) Tendon and Ligament: Development, Repair and Disease, Birth Defects Research (part C) 75:226-236
Hauser R., Dolan E., Phillips H., Newlin A., Moore R. and B. Woldin (2013) �Ligament Injury and Healing: A Review of Current Clinical Diagnostics and Therapeutics, The Open Rehabilitation Journal (6) 1-20
Cocchiarella L., Anderson G., (2001) Guides to the Evaluation of Permanent Impairment, 5th Edition, Chicago IL, AMA Press
Additional Topics: Preventing Spinal Degeneration
Spinal degeneration can occur naturally over time as a result of age and the constant wear-and-tear of the vertebrae and other complex structures of the spine, generally developing in people over the ages of 40. On occasion, spinal degeneration can also occur due to spinal damage or injury, which may result in further complications if left untreated. Chiropractic care can help strengthen the structures of the spine, helping to prevent spinal degeneration.
As you may have noticed settlement values have been on a steady downward trend for many years.�� Some of the decrease in claim value has been the result of insurers bad faith efforts to make their customers premiums an income stream for their corporate shareholders.�� Some of the decrease is related to the lack of documentation provided to attorneys by the health care industry. The high overhead of the medical practitioner ($100K+ malpractice premiums for a surgeon), coupled with ever decreasing reimbursements, necessitates a high-volume practice and too many critical details in in the doctor�s documentation is left out.
According to James Mathis, a former claims senior supervisor and management specialist for State Farm and Allstate who instituted these claims processing/reducing algorithms, there are 4 case value drivers:
Injuries
Impairment rating
Duties Under Duress: activities which you can do, but it hurts
Functional Loss:� activities that you can no longer do
A critical component is the impairment rating.�� This is due to the fact that the impairment rating unlocks the value in the �Duties Under Duress� and the �Functional Loss� categories.� According to Attorney Michael Schafer in his class titled �Demand Packages and Colossus� the impairment rating can unlock up to 75% of claim value.1
Computerized Radiographic Mensuration Analysis
The key test that unlocks an impairment rating in soft tissue (ligamentous damage) cases is called Computerized Radiographic Mensuration Analysis (CRMA).�� This test is the best way to document ligament laxity.�� It is my experience that up to 70% of your female and 50% of your male clients have this injury and that it is not being documented.
Dr. Bill Gallagher writes in the Attorney at Law Magazine, Greater Phoenix Edition:
�Ligament damage, the main underlying cause of soft tissue injuries can be measured with the proper x-rays and CRMA. When done so, a 25-28% impairment rating can be established.�2
The technical name for ligament laxity and damage is Alteration of Motion Segment Integrity (A.O.M.S.I.).�� The AMA Guides to the Evaluation of Permanent Impairment 5th edition, page 378 describes A.O.M.S.I. as:
�A.O.M.S.I. can be either loss of motion segment integrity (increased translation or angular motion) or decreased motion resulting mainly from developmental changes, fusion, fracture healing, healed infection or surgical arthrodesis (surgical fusion).�3
On page 379 the AMA Guides describes the definitions and how to determine its presence:
�Motion of the individual spinal segments cannot be determined by a physical examination, but is evaluated with flexion and extension roentgenograms.� Loss of motion segment integrity is defined as an anteroposterior motion of one vertebra over another that is:
greater than 3.5 mm in the cervical spine
greater than 2.5 mm in the thoracic spine
greater than 4.5 mm in the lumbar spine
Loss of motion segment is also defined as difference in angular motion of two adjacent motion segments greater than:
15 degrees at L1-2, L2-3 and L3-4
20 degrees at L4-5
25 degrees at L5-S1
More than 11 degrees greater than at either adjacent level in the cervical spine�4
Practitioners as myself, who are trained and specialize in biomechanical failure as a routine course of examination take motion x-rays immediately when the patient first arrives and again in 60 days.�� The initial x-rays may have muscle spasm and muscle guarding reducing the motion of the spine.� After 60 days, the muscle spasm should be reduced to a reasonable level and demonstrably reveal persistent pathology both biomechanically and of the connective tissue.
Insurance Companies and Diagnosis Results
According to Attorney Schaffer in his video conference on minor impact soft tissue injuries, insurance companies reserve $60,000 when they see a diagnosis of ligament laxity.5
A caveat is that you need to have a �Colossus ready� demand package to create a �fair and equitable� claim value.� One attorney, when I sent him this info, put together a two page demand with very little description of the injuries suffered by the client.�� Combined with the untrained adjustor and the computerized cost containment program, lead to his �low ball settlement offer.� This is common with too many lawyers and is a process that can be reversed to realize fair and equitable settlements.
Attorney Schaffer�s� courses from the MATA webinar archives (he provides a sample demand package for you in both) helps train you on this matter. Should you want more information, my office will help guide you through the steps to learn more about the technology used by the carriers to value your claims.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
References:
Michael Schafer, Esq.� Demand Brochures and Colossus, Seminar Web, December 1, 2016 www.seminarweb.com
Cocchiarella, Linda, and Gunnar B.J. Andersson.�Guides to the Evaluation of Permanent Impairment. 5th ed. AMA, Print. Page 378
Cocchiarella, Linda, and Gunnar B.J. Andersson.�Guides to the Evaluation of Permanent Impairment. 5th ed. AMA, Print. Page 379
Michael Schafer, Esq.� Maximizing the Value of M.I.S.T. Cases, Seminar Web, July 28, 2016 www.seminarweb.com
Additional Topics: Preventing Spinal Degeneration
Spinal degeneration can occur naturally over time as a result of age and the constant wear-and-tear of the vertebrae and other complex structures of the spine, generally developing in people over the ages of 40. On occasion, spinal degeneration can also occur due to spinal damage or injury, which may result in further complications if left untreated. Chiropractic care can help strengthen the structures of the spine, helping to prevent spinal degeneration.
According to the National Institute of Health�s, National Institute of Arthritis and Musculoskeletal and Skin Disorders:
A sprain is an injury to a ligament (tissue that connects two or more bones at a joint). In a sprain, one or more ligaments is stretched or torn. A strain is an injury to a muscle or a tendon (tissue that connects muscle to bone). In a strain, a muscle or tendon is stretched or torn.
Historically, doctors of all disciplines in the clinical setting and lawyers in the medical-legal arena have erroneously attempted to separate them into 2 distinct injuries allowing a false conclusion to be derived in either prognosis or legal arguments when considering connective tissue pathology as sequella to trauma.
Anatomy of Sprains and Strains
Solomonow (2009) wrote:
There are several ligaments in every joint in the human skeleton and they are considered as the primary restraints of the bones constituting the joint. Ligaments are also sensory organs and have significant input to sensation and reflexive/synergistic activation of muscles. The muscles associated with any given joint, therefore, also have a significant role as restraints. In some joints, such as the intervertebral joints of the spine, the role of the muscles as restraints is amplified. The role of ligaments as joint restraints is rather complex when considering the multitude of physical activities performed by individuals in routine daily functions, work and sports, the complexity of the anatomy of the different joints and the wide range of magnitude and velocity of the external loads. As joints go through their range of motion, with or without external load, the ligaments ensure that the bones associated with the joint travel in their prescribed anatomical tracks, keep full and even contact pressure of the articular surfaces, prevent separation of the bones from each other by increasing their tension, as may be necessary, and ensuring stable motion. Joint stability, therefore, is the general role of ligaments without which the joint may subluxate, cause damage to the capsule, cartilage, tendons, nearby nerves and blood vessels, discs (if considering spinal joints) and to the ligaments themselves. Such injury may debilitate the individual by preventing or limiting his/her use of the joint and the loss of function. Pgs. 136-137
While ligaments are primarily known as mechanical or supportive structures responsible for joint stability, they have equally important neurological functions. Anatomical studies have shown that ligaments in the extremities and the spine are endowed with nerves called mechanoreceptors. The presence of such that sense and send neurological information to the spine and brain in the ligaments confirms that they contribute to proprioception (feeling and analyzes one�s physical positon in space and time) and kinesthesia (similar to proprioception but can maintain feeling in these nerves even with aberrant neurological imput elsewhere) and also has a distinct role in reflex activation or inhibition of muscular activities.
Simply put, the nerves in ligaments attempts to alter muscle activity to prevent further biomechanical failure and pathology (bodily injury), which effects one�s ability to move in a balanced homeostatic manner leading to further functional loss in a short amount of time. The presence of such nerves in the ligaments confirms that they contribute to proprioception and kinesthesia and have a distinct role in reflex activation or inhibition of muscular activities. Therefore, the muscles and tendons (which are inherent in muscular activity), are responsive and dependent upon ligament activity in function with both normal and pathological (inclusive of trauma) activities.
Solomonow (2009) also reported that as far back as the turn of the last century, that a reflex may exist from sensory receptors in the ligaments to muscles that may directly or indirectly modify the load imposed on the ligament. A clear demonstration of a reflex activation of muscles finally provided in 1987 and reconfirmed several times since then. It was further shown that such a ligamento-muscular reflex exists in most extremity joints and in the spine.
Mechanism of Injury
A Single trauma according to Panjabi (2006) can cause either a tear in the ligament called laxity or a subfailure injury of the spinal ligaments and injury to the mechanoreceptors embedded in the ligaments and the following cascade of events occur: pgs. 669-670
NOTE: The subfailure injury of the spinal ligament is defined as an injury caused by stretching of the tissue beyond its physiological limit, but less than its failure point.
When the injured spine performs a task or it is challenged by an external load, the transducer signals generated by the mechanoreceptors are corrupted.
Neuromuscular control unit has difficulty in interpreting the corrupted transducer signals because there is spatial and temporal mismatch between the normally expected and the corrupted signals received.
The muscle response pattern generated by the neuromuscular control unit is corrupted, affecting the spatial and temporal coordination and activation of each spinal muscle.
The corrupted muscle response pattern leads to corrupted feedback to the control unit via tendon organs of muscles and injured mechanoreceptors, further corrupting the muscle response pattern.
The corrupted muscle response pattern produces high stresses and strains in spinal components leading to further subfailure injury of the spinal ligaments, mechanoreceptors and muscles, and overload of facet joints.
The abnormal stresses and strains produce inflammation of spinal tissues, which have abundant supply of nociceptive sensors and neural structures.
Consequently, over time, chronic biomechanical failure develops leading to premature degeneration and long-term pain.
Simply explained, when there is a ligament injury or sprain, the nerves in the ligament fire signals that go to the central nervous system and causes the muscles to react as compensation to bodily injury to stabilize the structure. That in turn sets up another cascade of problems if not compensated for or repaired as the muscle spasticity cannot maintain itself for long periods of time and goes into a posture of tetanus, or perpetual spasm until the lactic acid builds. This is followed by the muscle failing and putting the entire structure in a chronic biomechanically unstable position and causing the bone to remodel or become arthritic.
According to Hauser ET. Al (2013) ligament instability in either subfailures or laxity are a clear cause of osteoarthritis. This is not speculative as the inured will develop arthritis in 100% of the time and is consistent with Wolff�s Law that has been, and continues to be accepted since the late 18th century.
Therefore, as per the above scenario, strain-sprain is an intertwined syndrome that cannot either mechanically or neurologically be separated and will cause arthritis in 100% of the post-trauma instance. How much arthritis and how quickly it will develop is dependent upon how much ligamentous damage there is.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
Solomonow, M. (2009). Ligaments: a source of musculoskeletal disorders.Journal of Bodywork and Movement Therapies,13(2), 136-154.
Panjabi, M. M. (2006). A hypothesis of chronic back pain: ligament subfailure injuries lead to muscle control dysfunction.European Spine Journal,15(5), 668-676.
Hauser R., Dolan E., Phillips H., Newlin A., Moore R., Woldin B., Ligament & Healing Injuries: A Review of Current Clinical Diagnostics and Therapeutics, The Open Rehabilitation Journal, 2013, 6, 1-20
Additional Topics: Preventing Spinal Degeneration
Spinal degeneration can occur naturally over time as a result of age and the constant wear-and-tear of the vertebrae and other complex structures of the spine, generally developing in people over the ages of 40. On occasion, spinal degeneration can also occur due to spinal damage or injury, which may result in further complications if left untreated. Chiropractic care can help strengthen the structures of the spine, helping to prevent spinal degeneration.
Thomas M Kosloff1*�, David Elton1�, Jiang Tao2� and Wade M Bannister2�
CHIROPRACTIC & MANUAL THERAPIES
Abstract
Background: There is controversy surrounding the risk of manipulation, which is often used by chiropractors, with respect to its association with vertebrobasilar artery system (VBA) stroke. The objective of this study was to compare the associations between chiropractic care and VBA stroke with recent primary care physician (PCP) care and VBA stroke.
Methods: The study design was a case�control study of commercially insured and Medicare Advantage (MA) health plan members in the U.S. population between January 1, 2011 and December 31, 2013. Administrative data were used to identify exposures to chiropractic and PCP care. Separate analyses using conditional logistic regression were conducted for the commercially insured and the MA populations. The analysis of the commercial population was further stratified by age (<45 years; ?45 years). Odds ratios were calculated to measure associations for different hazard periods. A secondary descriptive analysis was conducted to determine the relevance of using chiropractic visits as a proxy for exposure to manipulative treatment.
Results: There were a total of 1,829 VBA stroke cases (1,159 � commercial; 670 � MA). The findings showed no significant association between chiropractic visits and VBA stroke for either population or for samples stratified by age. In both commercial and MA populations, there was a significant association between PCP visits and VBA stroke incidence regardless of length of hazard period. The results were similar for age-stratified samples. The findings of the secondary analysis showed that chiropractic visits did not report the inclusion of manipulation in almost one third of stroke cases in the commercial population and in only 1 of 2 cases of the MA cohort.
Conclusions: We found no significant association between exposure to chiropractic care and the risk of VBA stroke. We conclude that manipulation is an unlikely cause of VBA stroke. The positive association between PCP visits and VBA stroke is most likely due to patient decisions to seek care for the symptoms (headache and neck pain) of arterial dissection. We further conclude that using chiropractic visits as a measure of exposure to manipulation may result in unreliable estimates of the strength of association with the occurrence of VBA stroke.
Keywords: Chiropractic, Primary care, Cervical manipulation, Vertebrobasilar stroke, Adverse events
Background
The burden of neck pain and headache or migraine among adults in the United States is significant. Survey data indicate 13% of adults reported neck pain in the past 3 months [1]. In any given year, neck pain affects 30% to 50% of adults in the general population [2]. Prevalence rates were reportedly greater in more eco- nomically advantaged countries, such as the USA, with a higher incidence of neck pain noted in office and com- puter workers [3]. Similar to neck pain, the prevalence of headache is substantial. During any 3-month time- frame, severe headaches or migraines reportedly affect one in eight adults [1].
Neck pain is a very common reason for seeking health care services. �In 2004, 16.4 million patient visits or 1.5% of all health care visits to hospitals and physician offices, were for neck pain� [4]. Eighty percent (80%) of visits occurred as outpatient care in a physician�s office [4]. The utilization of health care resources for the treatment of headache is also significant. �In 2006, adults made nearly 11 million physician visits with a headache diagno- sis, over 1 million outpatient hospital visits, 3.3 million emergency department visits, and 445 thousand inpatient hospitalizations� [1].
In the United States, chiropractic care is frequently utilized by individuals with neck and/or headache com- plaints. A national survey of chiropractors in 2003 re- ported that neck conditions and headache/facial pain accounted respectively for 18.7% and 12% of the patient chief complaints [5]. Chiropractors routinely employ spinal manipulative treatment (SMT) in the management of patients presenting with neck and/or headache [6], either alone or combined with other treatment approaches [7-10].
While evidence syntheses suggest the benefits of SMT for neck pain [7-9,11-13] and various types of headaches [10,12,14-16], the potential for rare but serious adverse events (AE) following cervical SMT is a concern for researchers [17,18], practitioners [19,20], professional organizations [21-23], policymakers [24,25] and the public [26,27]. In particular, the occurrence of stroke affecting the vertebrobasilar artery system (VBA stroke) has been associated with cervical manipulation. A recent publication [28] assessing the safety of chiropractic care reported, �…the frequency of serious adverse events varied between 5 strokes/ 100,000 manipulations to 1.46 serious adverse events/ 10,000,000 manipulations and 2.68 deaths/10,000,000 manipulations�. These estimates were, however, derived from retrospective anecdotal reports and liability claims data, and do not permit confident conclusions about the actual frequency of neurological complications following spinal manipulation.
Several systematic reviews investigating the association between stroke and chiropractic cervical manipulation�have reported the data are insufficient to produce definitive conclusions about its safety [28-31]. Two case�control studies [32,33] used visits to a chiropractor as a proxy for SMT in their analyses of standardized health system databases for the population of Ontario (Canada). The more recent of these studies [32] also included a case-crossover methodology, which reduced the risk of bias from confounding variables. Both case�control studies reported an increased risk of VBA stroke in association with chiropractic visits for the population under age 45 years old. Cassidy, et al. [32] found, how- ever, the association was similar to visits to a primary care physician (PCP). Consequently, the results of this study suggested the association between chiropractic care and stroke was non-causal. In contrast to these studies, which found a significant association between chiropractic visits and VBA stroke in younger patients (<45 yrs.), the analysis of a population-based case-series suggested that VBA stroke patients who consulted a chiropractor the year before their stroke were older (mean age 57.6 yrs.) than previously documented [34].
The work by Cassidy, et al. [32] has been qualitatively appraised as one of the most robustly designed investigations of the association between chiropractic manipulative treatment and VBA stroke [31]. To the best of our knowledge, this work has not been reproduced in the U.S. population. Thus, the main purpose of this study is to replicate the case�control epidemiological design published by Cassidy, et al. [32] to investigate the association between chiropractic care and VBA stroke; and compare it to the association between recent PCP care and VBA stroke in samples of the U.S. commercial and Medicare Advantage (MA) populations. A secondary aim of this study is to assess the utility of employing chiropractic visits as a proxy measure for exposure to spinal manipulation.
Methods
Study design and population
We developed a case�control study based on the experience of commercially insured and MA health plan members between January 1, 2011 and December 31, 2013. General criteria for membership in a commercial or MA health plan included either residing or working in a region where health care coverage was offered by the in- surer. Individuals must have Medicare Part A and Part B to join a MA plan. The data set included health plan members located in 49 of 50 states. North Dakota was the only State not represented.
Both case and control data were extracted from the same source population, which encompassed national health plan data for 35,726,224 unique commercial and 3,188,825 unique MA members. Since members might be enrolled for more than one year, the average�annual commercial membership was 14.7 million members and the average annual MA membership was 1.4 million members over the three year study period, which is comparable to ~5% of the total US population based on the data available from US Census Bureau [35]. Administrative claims data were used to identify cases, as well as patient characteristics and health service utilization.
The stroke cases included all patients admitted to an acute care hospital with vertebrobasilar (VBA) occlusion and stenosis strokes as defined by ICD-9 codes of 433.0, 433.01, 433.20, and 433.21 during the study period. Pa- tients with more than one admission for a VBA stroke were excluded from the study. For each stroke case, four age and gender matched controls were randomly se- lected from sampled qualified members. Both cases and controls were randomly sorted prior to the matching using a greedy matching algorithm [36].
Exposures
The index date was defined as the date of admission for the VBA stroke. Any encounters with a chiropractor or a primary care physician (PCP) prior to the index date were considered as exposures. To evaluate the impact of chiropractic and PCP treatment, the designated hazard period in this study was zero to 30 days prior to the index date. For the PCP analysis, the index date was excluded from the hazard period since patients might consult PCPs after having a stroke. The standard health plan coverage included a limit of 20 chiropractic visits. In rare circumstances a small employer may have selected a 12-visit limit. An internal analysis (data not shown) revealed that 5% of the combined (commercial and MA) populations reached their chiropractic visit limits. Instances of an employer not covering chiropractic care were estimated to be so rare that it would have had no measurable impact on the analysis. There were no limits on the number of reimbursed PCP visits per year.
Analyses
Two sets of similar analyses were performed, one for the commercially insured population and one for the MA population. In each set of analyses, conditional logistic regression models were used to examine the association between the exposures and VBA strokes. To measure the association, we estimated the odds ratio of having the VBA stroke and the effect of total number of chiropractic visits and PCP visits within the hazard period. The analyses were applied to different hazard periods, including one day, three days, seven days, 14 days and 30 days for both chiropractic and PCP visits. The results of the chiropractic and PCP visit analyses were then compared to find evidence of excess risk of having stroke for patients with chiropractic visits during the
hazard period. Previous research has indicated that most patients who experience a vertebral artery dissection are under the age of 45. Therefore, in order to investigate the impact of exposure on the population at different ages, separate analyses were performed on patients stratified by age (under 45 years and 45 years and up) for the study of the commercial population. The number of visits within the hazard period was entered as a con- tinuous variable in the logistic model. The chi square test was used to analyze the proportion of co-morbidities in cases as compared to controls.
A secondary analysis was performed to evaluate the relevance of using chiropractic visits as a proxy for spinal manipulation. The commercial and MA databases were queried to identify the proportions of cases of VBA stroke and matched controls for which at least one chiropractic spinal manipulative treatment procedural code (CPT 98940 � 98942) was or was not recorded. The analysis also calculated the use of another manual therapy code (CPT 97140), which may be employed by chiropractors as an alternative means of reporting spinal manipulation.
Ethics
The New England Institutional Review Board (NEIRB) determined that this study was exempt from ethics review.
Results
The commercial study sample included 1,159 VBA stroke cases over the three year period and 4,633 age and gender matched controls. The average age of the patients was 65.1 years and 64.8% of the patients were male (Table 1). The prevalence rate of VBA stroke in the commercial population was 0.0032%.
There were a total of 670 stroke cases and 2,680 matched controls included in the MA study. The aver- age patient age was 76.1 years and 58.6% of the patients were male (Table 2). For the MA population, the prevalence rate of VBA stroke was 0.021%.
Claims during a one year period prior to the index date were extracted to identify comorbid disorders. Both the commercial and MA cases had a high percentage of comorbidities, with 71.5% of cases in the commercial study and 88.5% of the cases in the MA study reporting at least one of the comorbid conditions (Table 3). Six comorbid conditions of particular interest were identified, including hypertensive disease (ICD-9 401�404), ischemic�heart disease (ICD-9 410�414), disease of pulmonary circulation (ICD-9 415�417), other forms of heart disease (ICD-9 420�429), pure hypercholesterolemia (ICD-9 272.0) and diseases of other endocrine glands (ICD-9 249�250). There were statistically significant differences (p = <0.05) between groups for most comorbidities. Greater proportions of comorbid disorders (p = <0.0001) were reported in the commercial and MA cases for hyper- tensive disease, heart disease and endocrine disorders (Table 3). The commercial cases also showed a larger proportion of diseases of pulmonary circulation, which was statistically significant (p = 0.0008). There were no significance differences in pure hypercholesterolemia for either the commercial or MA populations. Overall, cases in both the commercial and MA populations were more likely (p = <0.0001) to have at least one co- morbid condition.
Among the commercially insured, 1.6% of stroke cases had visited chiropractors within 30 days of being admit- ted to the hospital, as compared to 1.3% of controls visit- ing chiropractors within 30 days prior to their index date. Of the stroke cases, 18.9% had visited a PCP within 30 days prior to their index date, while only 6.8% of controls had visited a PCP (Table 4). The proportion of exposures for chiropractic visits was lower in the MA sample within the 30-day hazard period (cases = 0.3%; controls = 0.9%). However, the proportion of exposures for PCP visits was higher, with 21.3% of cases having PCP visits as compared to12.9% for controls (Table 5).
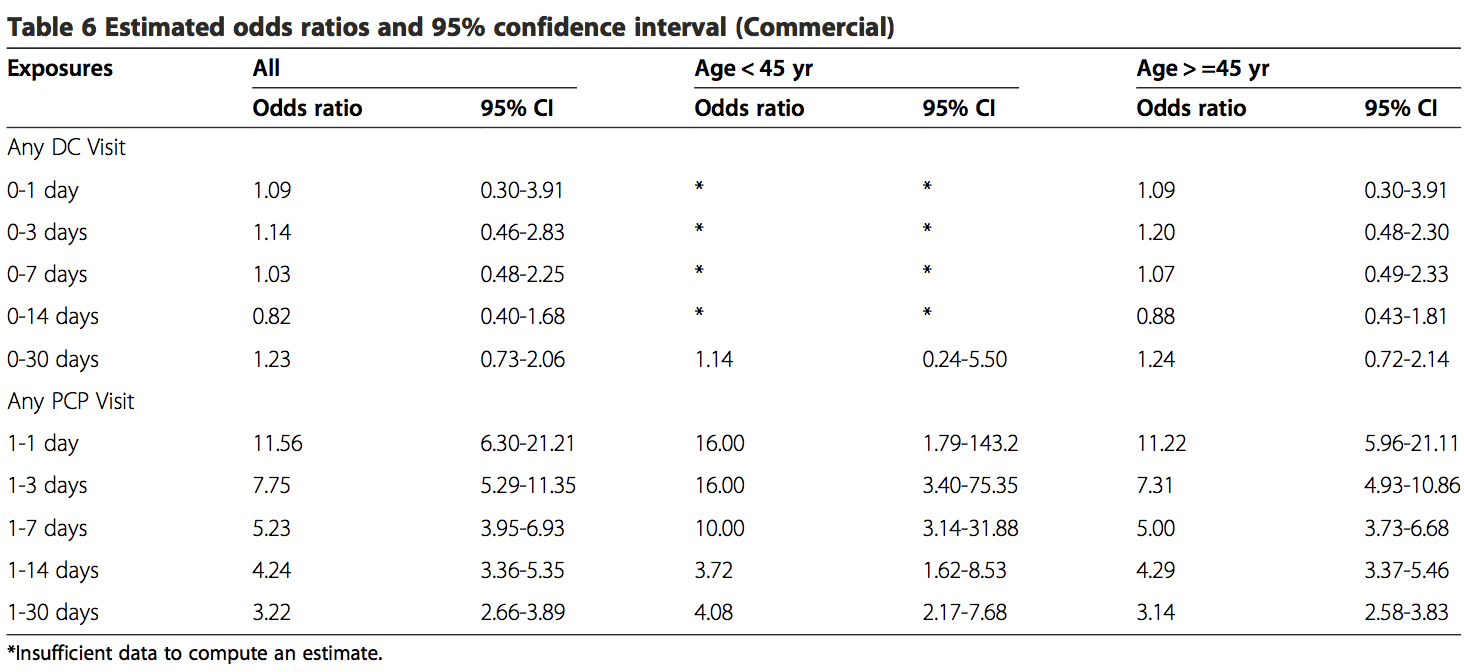
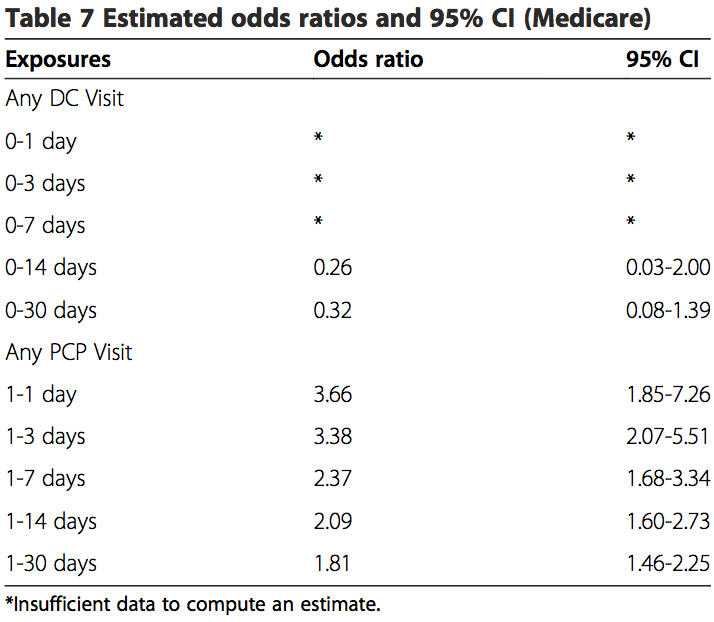
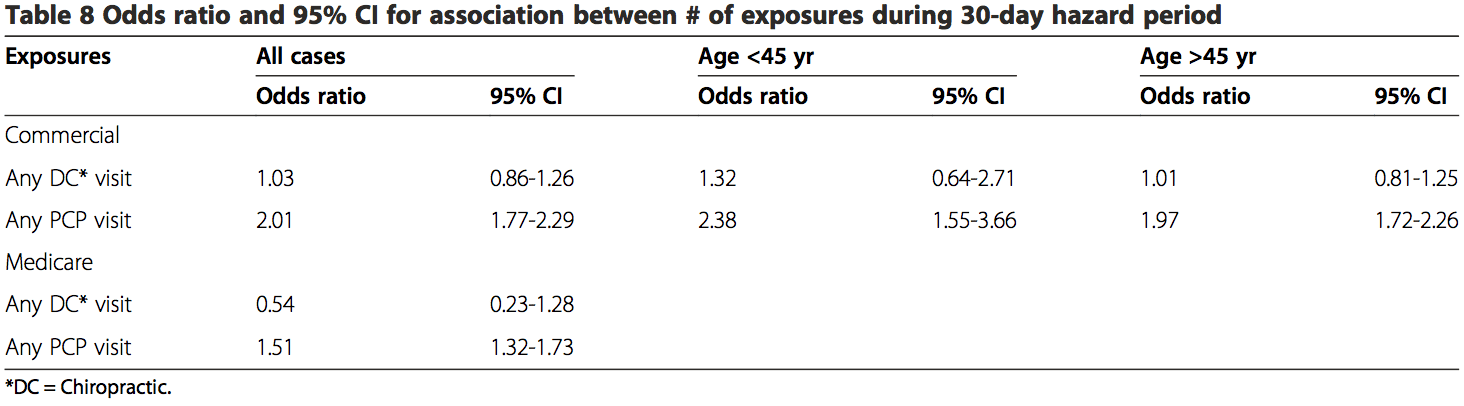
The results from the analyses of both the commercial population and the MA population were similar (Tables 6, 7 and 8). There was no association between chiropractic visits and VBA stroke found for the�overall sample, or for samples stratified by age. No estimated odds ratio was significant at the 95% confidence level. MA data were insufficient to calculate statistical measures of association for hazard periods less than 0�14 days for chiropractic visits. When stratified by age, the data were too sparse to calculate measures of association for hazard periods less than 0�30 days in the commercial population. The data were too few to analyze associative risk by headache and/or neck pain diagnoses (data not shown).
These results showed there is an association existing between PCP visits and VBA stroke incidence regardless of age or length of hazard period. A strong association was found for those visits close to the index date (OR 11.56; 95% CI 6.32-21.21) for all patients with a PCP visit within 0�1 day hazard period in the commercial sample. There was an increased risk of VBA stroke associated with each PCP visit within 30-days prior to the index date for MA patients (OR 1.51; 95% CI 1.32-1.73) and commercial patients (OR 2.01; 95% CI 1.77-2.29).
The findings of the secondary analysis showed � that of 1159 stroke cases from commercial population � there were a total of 19 stroke cases associated with chiropractic visits for which 13 (68%) had claims documentation indicating chiropractic SMT was performed. For the control group of the commercial cohort, 62 of 4633 controls had claims of any kind of chiropractic visits and 47 of 4633 controls had claims of SMT. In the commercial control group, 47 of 62 DC visits (76%) included SMT in the claims data. Only 1 of 2 stroke cases in the MA population included SMT in the claims data. For the MA cohort, 21 of 24 control chiropractic visits (88%) included SMT in the claims data (Table 9).
None of the stroke cases in either population included CPT 97140 as a substitute for the more conventionally re- ported chiropractic manipulative treatment procedural codes (98940 � 98942). For the control groups, there were three instances where CPT 97140 was reported without CPT 98940 � 98942 in the commercial population. The CPT code 97140 was not reported in MA control cohort.
Discussion
The primary aim of the present study was to investigate the association between chiropractic manipulative treatment and VBA stroke in a sample of the U.S. population. This study was modeled after a case�control design previously conducted for a Canadian population [32]. Administrative data for enrollees in a large national health care insurer were analyzed to explore the occurrence of VBA stroke across different time periods of exposure to chiropractic care in comparison with PCP care.
Unlike Cassidy et al. [32] and most other case�control studies [33,37,38], our results showed there was no significant association between VBA stroke and chiropractic visits. This was the case for both the commercial and MA populations. In contrast to two earlier case�control studies [32,33], this lack of association was found to be irrespective of age. Although, our results (Table 8) did lend credence to previous reports that VBA stroke occurs more frequently in patients under the age of 45 years. Additionally, the results from the present study did not identify a relevant temporal impact. There was no significant association, when the data were sufficient to calculate estimates, between chiropractic visits and stroke regardless of the hazard period (timing of most recent visit to a chiropractor and the occurrence of stroke).
There are several possible reasons for the variation in results with previous similar case�control studies. The younger (<45 yrs.) commercial cohort that received chiropractic care in our study had noticeably fewer cases. The 0�30 days hazard period included only 2 VBA stroke cases. There were no stroke cases for other hazard periods in this population. In contrast, earlier studies reported sufficient cases to calculate risk estimates for most hazard periods [32,33].
Another factor that potentially influenced the difference in results concerns the accuracy of hospital claims data in the U.S. vs. Ontario, Canada. The source population in the Province of Ontario was identified, in part, from the Discharge Abstract Database (DAD). The DAD includes hospital discharge and emergency visit diagnoses that have undergone a standardized assessment by a medical records coder [39]. To the best of our know- ledge, similar quality management practices were not routinely applied to hospital claims data used in sourcing the population for our study.
An additional reason for the disparity in results may be due to differences in the proportions of chiropractic visits where SMT was reportedly performed. Our study showed that SMT was not reported by chiropractors in more than 30% of commercial cases. It is plausible that a number of the cases in earlier studies also did not�include SMT as an intervention. Differences between studies in the proportion of cases reporting SMT may have affected the calculation of risk estimates.
Also, there were an insufficient number of cases having cervical and/or headache diagnoses in our study. Therefore, our sample population may have included proportionally less cases where cervical manipulation was performed.
Our results were consistent with previous findings [32,33] in showing a significant association between PCP visits and VBA stroke. The odds ratios for any PCP visit increase dramatically from 1�30 days to 1�1 day (Tables 6 and 7). This finding is consistent with the hypothesis that patients are more likely to see a PCP for symptoms related to vertebral artery dissection closer to the index date of their actual stroke. Since it is unlikely that the services provided by PCPs cause VBA strokes, the association�between recent PCP visits and VBA stroke is more likely attributable to the background risk related to the natural history of the condition [32].
A secondary goal of our study was to assess the utility of employing chiropractic visits as a surrogate for SMT. Our findings indicate there is a high risk of bias associated with using this approach, which likely overestimated the strength of association. Less than 70% of stroke cases (commercial and MA) associated with chiropractic care included SMT. A somewhat higher proportion of chiropractic visits included SMT for the control groups (commercial = 76%; MA = 88%).
There are plausible reasons that support these findings. Internal analyses of claims data (not shown) consistently demonstrate that one visit is the most common number associated with a chiropractic episode of care. The single visit may consist of an evaluation without treatment such as SMT. Further; SMT may have been viewed as contraindicated due to signs and symptoms of vertebral artery dissection (VAD) and/or stroke. This might explain the greater proportion of SMT provided to control groups in both the commercial and MA populations.
Overall, our results increase confidence in the findings of a previous study [32], which concluded there was no excess risk of VBA stroke associated chiropractic care compared to primary care. Further, our results indicate there is no significant risk of VBA stroke associated with chiropractic care. Additionally, our findings highlight the potential flaws in using a surrogate variable (chiropractic visits) to estimate the risk of VBA stroke in association with a specific intervention (manipulation).
Our study had a number of strengths and limitations. Both case and control data were extracted from the same source population, which encompassed national health plan data for approximately 36 million�commercial and 3 million MA members. A total of 1,829 cases were identified, making this the largest case� control study to investigate the association between chiropractic manipulation and VBA stroke. Due to the nationwide setting and large sample size, our study likely reduced the risk of bias related to geographic factors. However, there was a risk of selection bias � owing to the data set being from a single health insurer � including income status, workforce participation, and links to health care providers and hospitals.
Our study closely followed a methodological approach that had previously been described [32], thus allowing for more confident comparisons.
The current investigation analyzed data for a number of comorbid conditions that have been identified as potentially modifiable risk factors for a first ischemic stroke [40]. The differences between groups were statistically significant for most comorbidities. Information was not obtainable about behavioral comorbid factors e.g., smoking and body mass. With the exception of hypertensive disease, there are reasons to question the clinical significance of these conditions in the occurrence of ischemic stroke due to vertebral artery dissection. A large multinational case-referent study investigated the association between vascular risk factors (history of vascular disease, hypertension, smoking, hypercholesterolemia, diabetes mellitus, and obesity/overweight) for ischemic stroke and the occurrence of cervical artery dissection [41]. Only hypertension had a positive association (odds ratio 1.67; 95% confidence interval, 1.32 to 2.1; P <0.0001) with cervical artery dissection.
While the effect of other unmeasured confounders cannot be discounted, there is reason to suspect the absence of these data was not deleterious to the results. Cassidy, et al. found no significant differences in the results their case-crossover design, which affords better control of unknown confounding variables, and the findings of their case�control study [32].
Our results highlight just how unusual VBA stroke is in the MA cohort (prevalence = 0.021%) and � even more so � for the commercial population (prevalence = 0.0032%). As a result, some limitations of this study re- lated to the rarity of reporting VBA stroke events. Despite the larger number of cases, data were insufficient to calculate estimates and confidence intervals for seven measures of exposure (4 commercial and 3 MA) for chiropractic visits. Additionally, we were not able to compute estimates specifically for headache and neck pain diagnoses due to small numbers. Confidence intervals associated with estimates tended to be wide making the results imprecise [42].
There were limitations related to the use of administrative claims data. �Disadvantages of using secondary data for research purposes include: variations in coding from hospital to hospital or from department to department, errors in coding and incomplete coding, for example in the presence of comorbidities. Random errors in coding and registration of discharge diagnoses may dilute and attenuate estimates of statistical association� [43]. The recordings of unvalidated hospital discharge diagnostic codes for stroke have been shown to be less precise when compared to chart review [44,45] and validated patient registries�[43,46]. Cassidy, et al. [32] conducted a sensitivity analysis to determine the effect of diagnostic misclassification bias. Their conclusions did not change when the effects of misclassification were assumed to be similarly distributed between chiropractic and PCP cases.
A particular limitation in using administrative claims data is the paucity of contextual information surround- ing the clinical encounters between chiropractors/PCPs and their patients. Historical elements describing the occurrence/absence of recent trauma or activities reported in case studies [47-51] as potential risk factors for VBA stroke were not available in claims data. Confidence was low concerning the ability of claims data to provide accurate and complete reporting of other health disorders, which have been described in case�control designs as being associated with the occurrence of VBA stroke e.g., migraine [52] or recent infection [53]. Symptoms and physical examination findings that would have permitted further stratification of cases were not reported in the claims data.
The reporting of clinical procedures using current pro- cedural terminology (CPT) codes presented additional shortcomings concerning the accuracy and interpretation of administrative data. One inherent constraint was the lack of anatomic specificity associated with the use of standardized procedural codes in claims data. Chiropractic manipulative treatment codes (CPT 98940 � 98942) have been formatted to describe the number of spinal regions receiving manipulation. They do not identify the particular spinal regions manipulated.
Also, treatment information describing the type(s) of manipulation was not available. When SMT was re- ported, claims data could not discriminate among the range of techniques including thrust or rotational manipulation, various non-thrust interventions e.g., mechanical instruments, soft tissue mobilizations, muscle energy techniques, manual cervical traction, etc. Many of these techniques do not incorporate the same bio- mechanical stressors associated with the type of manipulation (high velocity low amplitude) that has been investigated as a putative risk factor for VBA stroke [54-56]. It seems plausible that the utility of future VBA stroke research would benefit from explicit descriptions of the particular type of manipulation performed.
Moreover, patient responses to care � including any adverse events suggestive of vertebral artery dissection or stroke-like symptoms � were not obtainable in the data set used for the current study.
In the absence of performing comprehensive clinical chart audits, it is not possible to know from claims data what actually transpired in the clinical encounter. Further, chart notes may themselves be incomplete or otherwise fail to precisely describe the nature of interventions [57]. Therefore, manipulation codes represent surrogate
measures, albeit more direct surrogate measures, than simply using the exposure to chiropractic visits.
Our study was also limited to replication of the case� control design described by Cassidy, et al. [32]. For pragmatic reasons, we did not attempt to conduct a case-crossover design. While the addition of a case- crossover design would have provided better control of confounding variables, Cassidy, et al. [32] showed the results were similar for both the case control and case crossover studies.
The findings of this case�control study and previous retrospective research underscore the need to rethink how to better conduct future investigations. Researchers should seek to avoid the use of surrogate measures or use the least indirect measures available. Instead, the focus should be on capturing data about the types of services and not the type of health care provider.
In alignment with this approach, it is also important for investigators to access contextual data (e.g., from electronic health records), which can be enabled by qualitative data analysis computer programs [58]. The acquisition of the elements of clinical encounters � including history, diagnosis, intervention, and adverse events � can provide the infrastructure for more action- able research. Because of the rarity of VBA stroke, large data sets (e.g., registries) containing these elements will be necessary to achieve adequate statistical power for making confident conclusions.
Until research efforts produce more definitive results, health care policy and clinical practice judgments are best informed by the evidence about the effectiveness of manipulation, plausible treatment options (including non-thrust manual techniques) and individual patient values [20].
Conclusions
Our findings should be viewed in the context of the body of knowledge concerning the risk of VBA stroke. In contrast to several other case�control studies, we found no significant association between exposure to chiropractic care and the risk of VBA stroke. Our secondary analysis clearly showed that manipulation may or may not have been reported at every chiropractic visit. Therefore, the use of chiropractic visits as a proxy for manipulation may not be reliable. Our results add weight to the view that chiropractic care is an unlikely cause of VBA strokes. However, the current study does not exclude cervical manipulation as a possible cause or contributory factor in the occurrence of VBA stroke.
Authors’ Contributions
DE conceived of the study, and participated in its design and coordination. JT participated in the design of the study, performed the statistical analysis and helped to draft the manuscript. TMK participated in the design and coordination of the study, and wrote the initial draft and revisions of the manuscript. WMB participated in the coordination of the study and the statistical analysis, and helped to draft the manuscript. All authors contributed to the interpretation of the data. All authors read and approved the final manuscript.
Author Details
1Optum Health � Clinical Programs at United Health Group, 11000 Optum Circle, Eden Prairie MN 55344, USA. 2Optum Health � Clinical Analytics at United Health Group, 11000 Optum Circle, Eden Prairie MN 55344, USA.
Received: 14 October 2014 Accepted: 28 April 2015
Published Online: 16 June 2015
References
1. Paulose R, Hertz R. The burden of pain among adults in the United States. In Pfizer Facts. Edited by Pfizer Inc. 2008. [http://www.pfizer.com/files/products/PF_Pain.pdf] Accessed May 14, 2014.
2. Carroll L, Hogg-Johnson S, van der Velde G, Haldeman S, Holm L, Carragee E, et al. Bone and Joint Decade 2000�2010 Task Force on Neck Pain and Its Associated Disorders: Course and prognostic factors for neck pain in the
general population: results of the Bone and Joint Decade 2000�2010 Task Force on Neck Pain and Its Associated Disorders. Spine (Phila Pa 1976).2008;33(4 Suppl):S75�82.
3. Hoy D, Protani M, De R, Buchbinder R. The epidemiology of neck pain. Best Pract Res Clin Rheumatol. 2010;24(6):783�92.
4. Jacobs J, Andersson G, Bell J, Weinstein S, Dormans J, Gnatz S, et al. Spine: low back and neck pain. In The Burden of Musculoskeletal Diseases in the United States. Chapter 2. Edited by Bone and Joint Decade USA
2002�2011. Rosemont, IL: The American Academy of Orthopaedic Surgeons; 2008:21�56.
5. Christensen M, Kollasch M, Hyland J, Rosner A. Chapter 8 � Patient Conditions. In Practice Analysis of Chiropractic: A Project Report, Survey Analysis, and Summary of the Practice of Chiropractic Within the United States. Greeley, CO: The National Board of Chiropractic Examiners. 2010:95�120.
6. Christensen M, Kollasch M, Hyland J, Rosner A. Chapter 9 � Professional functions and treatment procedures. In Practice Analysis of Chiropractic: A Project Report, Survey Analysis, and Summary of the Practice of
Chiropractic Within the United States. Greeley, CO: The National Board of Chiropractic Examiners. 2010:121�136.
7. D�Sylva J, Miller J, Gross A, Burnie S, Goldsmith G, Graham N, et al. Manual therapy with or without physical medicine modalities for neck pain: a systematic review. Man Ther. 2010;15(4):415�33.
8. Gross A, Miller J, D�Sylva J, Burnie S, Goldsmith G, Graham N, et al. Manipulation or mobilisation for neck pain: A Cochrane review. Man Ther. 2010;15(4):315�33.
9. Bryans R, Decina P, Descarreaux M, Duranleau M, Marcoux H, Potter B, et al. Evidence-based guidelines for the chiropractic treatment of adults with neck pain. J Manipulative Physiol Ther. 2014;37(1):42�63.
10. Bryans R, Descarreaux M, Duranleau M, Marcoux H, Potter B, Ruegg R, et al. Evidence-based guidelines for the chiropractic treatment of adults withheadache. J Manipulative Physiol Ther. 2011;34(5):274�89.
11. Childs J, Cleland J, Elliott J, Teyhen D, Wainner R, Whitman J, et al. Neck pain: clinical practice guidelines linked to the International Classification of Functioning, Disability, and Health from the Orthopaedic
Section of the American Physical Therapy Association. J Orthop Sports Phys Ther. 2008;38(9):A1�A34.
12. Clar C, Tsertsvadze A, Court R, Hundt G, Clarke A, Sutcliffe P. Clinical effectiveness of manual therapy for the management of musculoskeletal and non-musculoskeletal conditions: systematic review and update of UK
evidence report. Chiropr Man Therap. 2014;22(1):12.
13. Vincent K, Maigne J, Fischhoff C, Lanlo O, Dagenais S. Systematic review of manual therapies for nonspecific neck pain. Joint Bone Spine. 2013;80(5):508�15.
14. Bronfort G, Assendelft W, Evans R, Haas M, Bouter L. Efficacy of spinal manipulation for chronic headache: a systematic review. J Manipulative Physiol Ther. 2001;24(7):457�66.
15. Chaibi A, Tuchin P, Russell M. Manual therapies for migraine: a systematic review. J Headache Pain. 2011;12(2):127�33.
16. Racicki S, Gerwin S, Diclaudio S, Reinmann S, Donaldson M. Conservative physical therapy management for the treatment of cervicogenic headache: a systematic review. J Man Manip Ther. 2013;21(2):113�24.
17. Cassidy J, Bronfort G, Hartvigsen J. Should we abandon cervical spine manipulation for mechanical neck pain? No BMJ. 2012;344, e3680.
18. Wand B, Heine P, O�Connell N. Should we abandon cervical spine manipulation for mechanical neck pain? Yes BMJ. 2012;344, e3679.
19. Moloo J. What’s the Best Approach for Managing Neck Pain? NEJM Journal Watch 2012. [http://www.jwatch.org/jw201202090000004/2012/02/09/whats-best-approach-managing-neck-pain] Accessed May 14, 2014.
20. Schneider M, Weinstein S, Chimes G. Cervical manipulation for neck pain. PM&R. 2012;4(8):606�12.
21. Biller J, Sacco R, Albuquerque F, Demaerschalk B, Fayad P, Long P, et al. Cervical arterial dissections and association with cervical manipulative therapy:a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2014, Epub ahead of print.
22. American Chiropractic Association: ACA Response to AHA Statement on Neck Manipulation. 2014 (Aug 7). [http://www.acatoday.org/press_css.cfm? CID=5534] Accessed August 15, 2014.
23. American Physical Therapy Association: APTA responds to American Heart Association cervical manipulation paper. 2014 (Aug 7). [http://www.apta.org/Media/Releases/Consumer/2014/8/7/] Accessed August 15, 2014.
24. Kardys JA. Declaratory ruling regarding informed consent. Connecticut State Board of Chiropractic Examiners � State of Connecticut Department of Public Health. 2010. [http://www.ctchiro.com/upload/news/44_0.pdf]
Accessed May 14, 2014.
25. Wangler M, Fujikawa R, Hestb�k L, Michielsen T, Raven T, Thiel H, et al. Creating European guidelines for Chiropractic Incident Reportingand Learning Systems (CIRLS): relevance and structure. Chiropr Man
Therap. 2011;19:9.
26. Berger S: How safe are the vigorous neck manipulations done by chiropractors? Washington Post 2014 (Jan. 6). [http://www.washingtonpost.com/national/health-science/how-safe-are-the-vigorous-neck-manipulationsdone-by-chiropractors/2014/01/06/26870726-5cf7-11e3-bc56-c6ca94801fac_story.html] Accessed January 10, 2014.
27. Group wants provincial ban on some neck manipulation by chiropractors. Winnipeg Free Press 2012 (Oct 4). [http://www.winnipegfreepress.com/local/Group-wants-provincial-ban-on-some-neck-manipulation-bychiropractors-172692471.htm] Accessed May 14, 2014.
28. Gouveia L, Castanho P, Ferreira J. Safety of chiropractic interventions: a systematic review. Spine (Phila Pa 1976). 2009;34(11):E405�13.
29. Carlesso L, Gross A, Santaguida P, Burnie S, Voth S, Sadi J. Adverse events associated with the use of cervical manipulation and mobilization for the treatment of neckpain in adults: a systematic review. Man Ther. 2010;15(5):434 44.
30. Chung C, C�t� P, Stern P, L’Esp�rance G. The association between cervical spine manipulation and carotid artery dissection: a systematic review of the literature. J Manipulative Physiol Ther 2014, [Epub ahead of print].
31. Haynes M, Vincent K, Fischhoff C, Bremner A, Lanlo O, Hankey G. Assessing the risk of stroke from neck manipulation: a systematic review. Int J Clin Pract. 2012;66(10):940�7.
32. Cassidy J, Boyle E, Cote P, He Y, Hogg-Johnson S, Silver F, et al. Risk of vertebrobasilar stroke and chiropractic care: results of a population-based case�control and case-crossover study. Spine (Phila Pa 1976).
2008;33 Suppl 4:S176�83.
33. Rothwell D, Bondy S, Williams J. Chiropractic manipulation and stroke: a population-based case�control study. Stroke. 2001;32(5):1054�60.
34. Choi S, Boyle E, C�t� P, Cassidy JD. A population-based case-series of Ontario patients who develop a vertebrobasilar artery stroke after seeing a chiropractor. J Manipulative Physiol Ther. 2011;34(1):15�22.
35. U.S. Census Bureau: State and County QuickFacts. Data derived from Population Estimates, American Community Survey, Census of Population and Housing, State and County Housing Unit Estimates, County Business
Patterns, Nonemployer Statistics, Economic Census, Survey of Business Owners, Building Permits. 2014 (rev July 8). [http://quickfacts.census.gov/qfd/states/00000.html] Accessed August 19, 2014.
36. Kosanke J, Bergstralh E. GMatch Macro (SAS program): Mayo Clinic College of Medicine. 2004. [http://www.mayo.edu/research/departments-divisions/department-health-sciences-research/division-biomedical-statisticsinformatics/software/locally-written-sas-macros]Accessed June 6, 2014.
37. Smith W, Johnston S, Skalabrin E, Weaver M, Azari P, Albers G, et al. Spinal manipulative therapy is an independent risk factor for vertebral artery dissection. Neurology. 2003;60(9):1424�8.
38. Engelter S, Grond-Ginsbach C, Metso T, Metso A, Kloss M, Debette S, et al. Cervical Artery Dissection and Ischemic Stroke Patients Study Group: Cervical artery dissection: trauma and other potential mechanical trigger
events. Neurology. 2013;80(21):1950�7.
39. Ardal S, Baigent L, Bains N, Hay C, Lee P, Loomer S: The health analyst�s toolkit. Ministry of Health and Long-Term Care Health Results Team – Information Management. Ontario (CA) 2006 (January) [http://www.health.gov.on.ca/transformation/providers/information/resources/analyst_toolkit.pdf]
Accessed January 12, 2015.
40. Sacco RL, Benjamin EJ, Broderick JP, Dyken M, Easton JD, Feinberg WM, et al. American Heart Association Prevention Conference. IV. Prevention and rehabilitation of stroke. Risk factors. Stroke. 1997;28(7):1507�17.
41. Debette S, Metso T, Pezzini A, Abboud S, Metso A, Leys D, et al. Cervical Artery Dissection and Ischemic Stroke Patients (CADISP) Group: Association of vascular risk factors with cervical artery dissection and ischemic stroke in
young adults. Circulation. 2011;123(14):1537�44.
42. Guyatt G, Oxman A, Kunz R, Brozek J, Alonso-Coello P, Rind D, et al. GRADE guidelines 6. Rating the quality of evidence � imprecision. J Clin Epidemiol. 2011;64(12):1283�93.
43. Krarup L, Boysen G, Janjua H, Prescott E, Truelsen T. Validity of stroke diagnoses in a National Register of Patients. Neuroepidemiology. 2007;28(3):150�4.
44. Goldstein L. Accuracy of ICD-9-CM coding for the identification of patients with acute ischemic stroke: effect of modifier codes. Stroke. 1998;29(8):1602�4.
45. Liu L, Reeder B, Shuaib A, Mazagri R. Validity of stroke diagnosis on hospital discharge records in Saskatchewan, Canada: implications for stroke surveillance. Cerebrovasc Dis. 1999;9(4):224�30.
46. Ellekjaer H, Holmen J, Kr�ger O, Terent A. Identification of incident stroke in Norway: hospital discharge data compared with a population-based stroke register. Stroke. 1999;30(1):56�60.
47. Braksiak R, Roberts D. Amusement park injuries and deaths. An Emerg Med. 2002;39(1):65�72.
48. Dittrich R, Rohsbach D, Heidbreder A, Heuschmann P, Nassenstein I, Bachmann R, et al. Mild mechanical traumas are possible risk factors for cervical artery dissection. Cerebrovasc Dis. 2007;23(4):275�81.
49. Mas J, Bousser M, Hasboun D, Laplane D. Extracranial vertebral artery dissection: a review of 13 cases. Stroke. 1987;18(6):1037�47.
50. Slankamenac P, Jesic A, Avramov P, Zivanovic Z, Covic S, Till V. Multiple cervical artery dissection in a volleyball player. Arch Neuro. 2010;67(8):1024�5.
51. Weintraub M. Beauty parlor stroke syndrome: report of five cases. JAMA. 1993;269(16):2085�6.
52. Tzourio C, Benslamia L, Guilllon B, A�di S, Bertrand M, Berthet K, et al. Migraine and the risk of cervical artery dissection: a case control study. Neurology. 2002;59(3):435�7.
53. Guillon B, Berthet K, Benslamia L, Bertrand M, Bousser M, Tzourio C. Infection and the risk of cervical artery dissection: a case�control study. Stroke. 2003;34(7):e79�81.
54. Symons B, Leonard TR, Herzog W. Internal forces sustained by the vertebral artery during spinal manipulative therapy. J Manip Physiol Ther.2002;25(8):504�10.
55. Wuest S, Symons B, Leonard T, Herzog W. Preliminary report: biomechanics of vertebral artery segments C1-C6 during cervical spinal manipulation. J Manip Physiol Ther. 2010;33(4):273�8.
56. Herzog W, Leonard TR, Symons B, Tang C, Wuest S. Vertebral artery strains during high-speed, low amplitude cervical spinal manipulation. J Electromyogr Kinesiol. 2012;22(5):747�51.
57. Centers for Medicare & Medicaid: Comprehensive error rate testing (CERT). 2015 (Jan. 15). [http://www.cms.gov/Research-Statistics-Data-and-Systems/Monitoring-Programs/Medicare-FFS-Compliance-Programs/CERT/index.html?redirect=/cert] Accessed February 4, 2015.
58. Welsh E: Dealing with data: using NVivo in the qualitative data analysis process. Forum: Qualitative Social Research 2002, 3(2): Art. 26 [http://nbnresolving.de/urn:nbn:de:0114-fqs0202260] Accessed February 4, 2015.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine










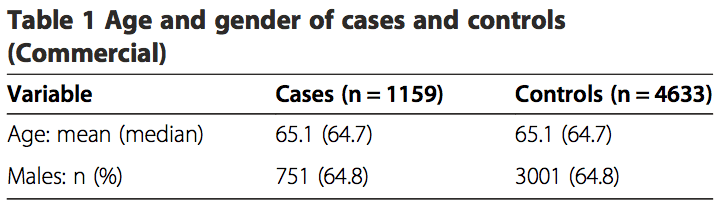
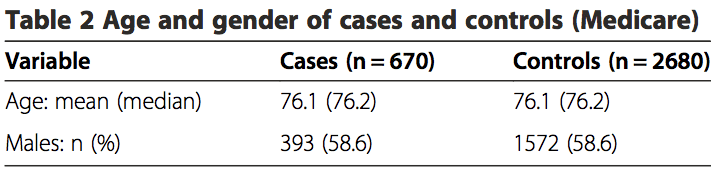
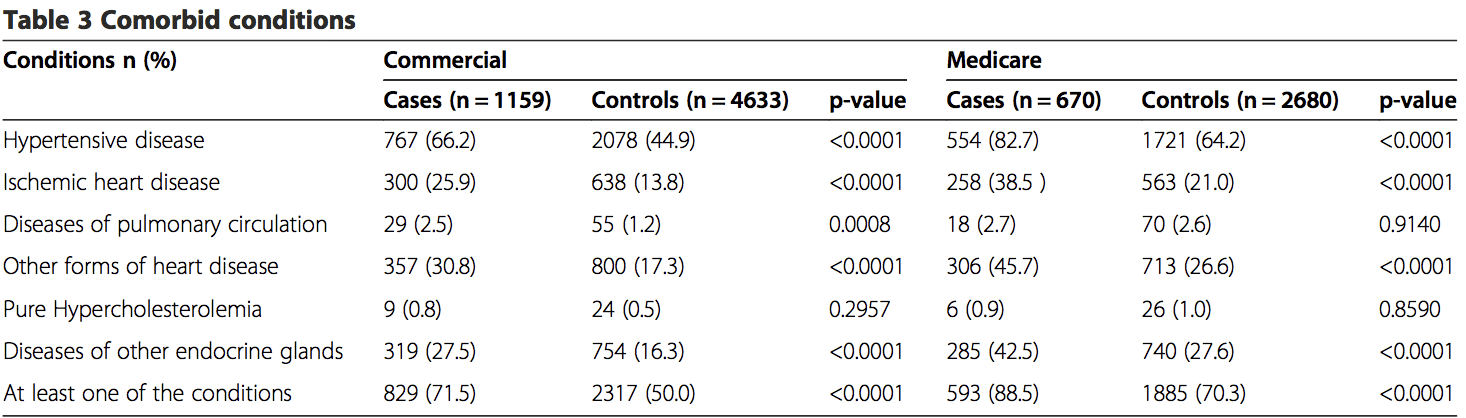 Among the commercially insured, 1.6% of stroke cases had visited chiropractors within 30 days of being admit- ted to the hospital, as compared to 1.3% of controls visit- ing chiropractors within 30 days prior to their index date. Of the stroke cases, 18.9% had visited a PCP within 30 days prior to their index date, while only 6.8% of controls had visited a PCP (Table 4). The proportion of exposures for chiropractic visits was lower in the MA sample within the 30-day hazard period (cases = 0.3%; controls = 0.9%). However, the proportion of exposures for PCP visits was higher, with 21.3% of cases having PCP visits as compared to12.9% for controls (Table 5).
Among the commercially insured, 1.6% of stroke cases had visited chiropractors within 30 days of being admit- ted to the hospital, as compared to 1.3% of controls visit- ing chiropractors within 30 days prior to their index date. Of the stroke cases, 18.9% had visited a PCP within 30 days prior to their index date, while only 6.8% of controls had visited a PCP (Table 4). The proportion of exposures for chiropractic visits was lower in the MA sample within the 30-day hazard period (cases = 0.3%; controls = 0.9%). However, the proportion of exposures for PCP visits was higher, with 21.3% of cases having PCP visits as compared to12.9% for controls (Table 5).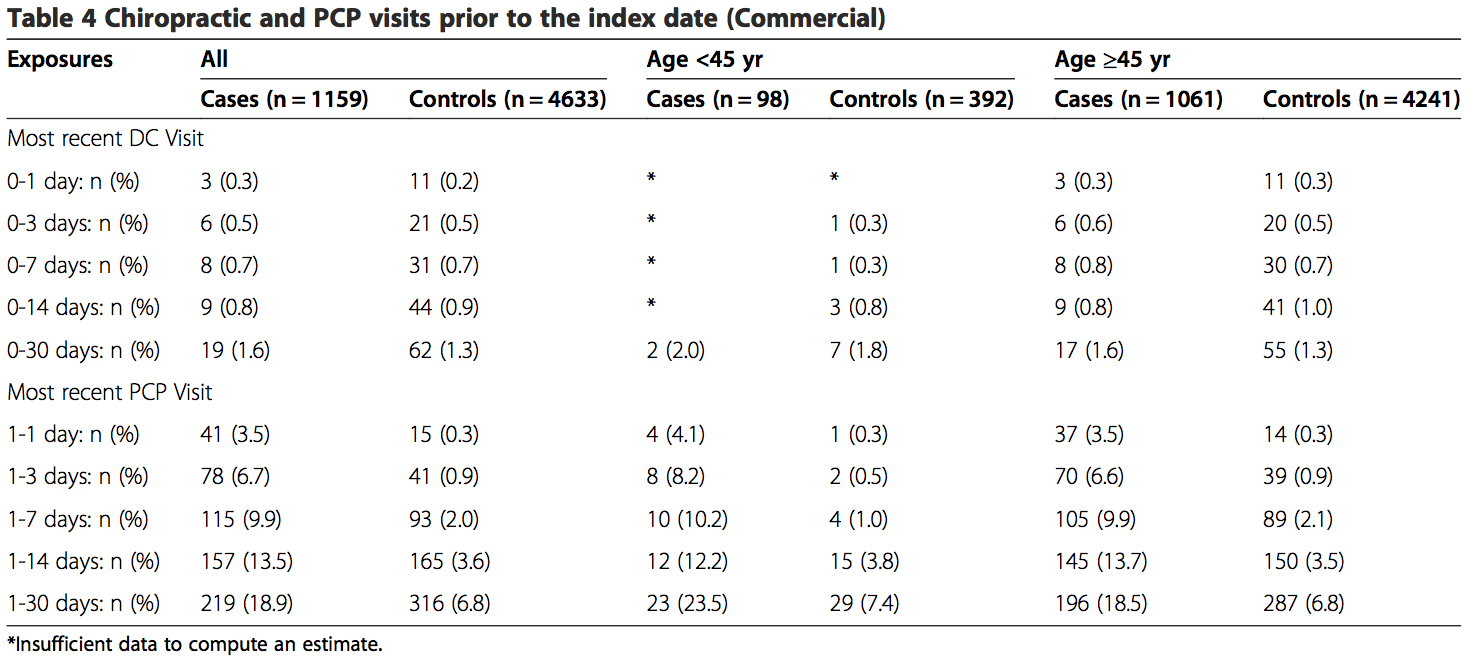
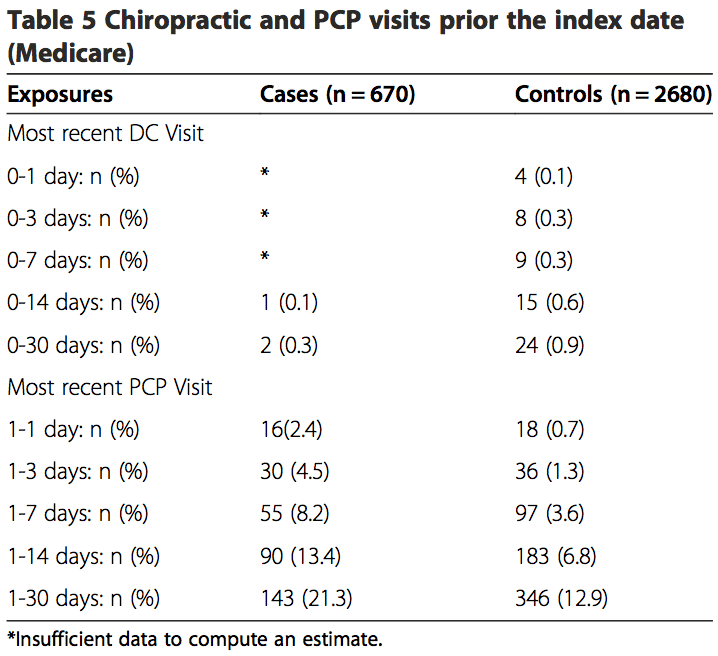 The results from the analyses of both the commercial population and the MA population were similar (Tables 6, 7 and 8). There was no association between chiropractic visits and VBA stroke found for the�
The results from the analyses of both the commercial population and the MA population were similar (Tables 6, 7 and 8). There was no association between chiropractic visits and VBA stroke found for the�