When the weather warms, melting the snow and ice as it ushers in the newness of spring, people are drawn outdoors, and increased activity soon follows. Runners top the list, training for upcoming marathons and races, or to get faster and increase endurance.
While some runners won�t let anything stop them, be it rain, sleet, or snow, most will not venture outside or engage in more rigorous training until the environment is more pleasant. This increased activity, though, can increase a person�s risk of injury, especially if they have been mostly inactive during the winter months. The most prevalent injury is runner�s knee, an umbrella term used to describe a variety of knee injuries including patellofemoral tracking syndrome.
What is Patellar Tracking Disorder?
When the patella, or kneecap, does not remain in place as the leg straightens or bends, it is called patellofemoral tracking syndrome. Many people believe that the kneecap only moves up and down, but that is not accurate. The kneecap is very mobile, rotating and tilting so that there are a variety of contact points between the femur and patella. The most common way that this disorder presents is the kneecap extends too far to the outside of the leg. Less frequent is when the kneecap shifts to the inside. The result is pain (sometimes severe) and limited mobility.
Understanding the syndrome means understanding the mechanics of the knee joint. The thighbone (femur) and lower leg (tibia and fibula) are joined by the knee, a large, complex hinge. A groove runs along the front of the joint, where the thighbone ends. The patella sits in the groove and is held in place by a network on the sides by ligaments and at the top and bottom by tendons. The underside of the kneecap is a layer of cartilage that allows it to move easily, or glide, along with the groove. When there is a problem with any of the parts that make up the knee it can lead to patellofemoral tracking syndrome.
Causes of Patellofemoral Tracking Syndrome
While overuse of the knee is the blanket term that describes the cause of patellofemoral tracking syndrome, it is the result of a combination of several problems. These can include:
Leg ligaments, tendons, or muscles that are too loose or too tight
Structural problems with the knee bones
Weak thigh muscles
The continuous stress put on the knee, such as activities that use a twisting motion to the knee
Repetitive, high-stress activities like running
Repeated movements like squatting, knee bending, or jumping
Improper alignment of the knee bones
Trauma to the knee that forces the kneecap off track, usually to the outside area of the leg
People who are most likely to develop the syndrome are those who experience any of these problems in addition to playing sports or running. Obesity or being overweight, when combined with the above problems can also put a person at risk for the syndrome.
Chiropractic for Patellofemoral Tracking Syndrome
Many people have experienced relief from the pain of patellofemoral tracking syndrome by using chiropractic care. Chiropractic for patellofemoral tracking syndrome is a medication free, non-invasive treatment that quickly and effectively treats the pain and helps to restore mobility. This is usually done by bringing the body back into alignment and performing specific manipulations depending on the unique needs of the patient. Treatment may involve the foot, ankle, spine, and hip in addition to the knee.
The patient may also be advised to make specific dietary adjustments, take special, targeted supplements, and do specific exercises in addition to the chiropractic treatments. Stretching is often recommended, and Kinesio taping is also a standard therapy to aid healing. Chiropractic will not only return the body to its natural balance and alignment, but it will get it to a state where it can begin healing itself.
Truide Torres started having back pain throughout the progression of her pregnancy. After she began to experiencing many limitations with her daily physical activities, Truide Torres visited Dr. Alex Jimenez, chiropractor, to receive chiropractic care for her back pain. Because of her pregnancy, Truide Torres had some doubts, and she felt unsure about receiving chiropractic care. However, Dr. Alex Jimenez and his staff reassured her and gave her the confidence to follow through with her treatment. Truide Torres recommends Dr. Alex Jimenez to anyone.
Chiropractic Help in Pregnancy
Chiropractic care provides maintenance to the spinal column, discs, bones, and nerves without drugs/medications or surgery. It helps correct any spinal misalignments, or subluxations, which reduces spinal nerve strain and promotes health and wellness throughout the body. There are no known contraindications to chiropractic care during pregnancy. All chiropractors are trained to work with women who are pregnant. Providing chiropractic care for pregnant women is routine care for the majority of chiropractors.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend�us.
Sagittal Fluid Sensitive MR slice showing large synovial popliteal (Baker’s) cyst (above top image) and sizeable synovial effusion (above bottom image)
Note multiple patchy dark signal areas on both images, representing fibrinoid inflammatory deposits aka “rice bodies” a characteristic MRI feature of RA
Management Rheumatological Referral & DRM
Conservative management followed by operative care in complicated cases of tendon ruptures and joints dislocations
Supplemental reading:
Diagnosis and Management of Rheumatoid Arthritis – AAFP
Septic arthritis – d/t bacterial or fungal contamination of the joint. SA may cause rapid joint destruction and requires prompt Dx and antibiotic administration
Joints affected: large joints with rich blood supply (knee 50%>hips>shoulders).
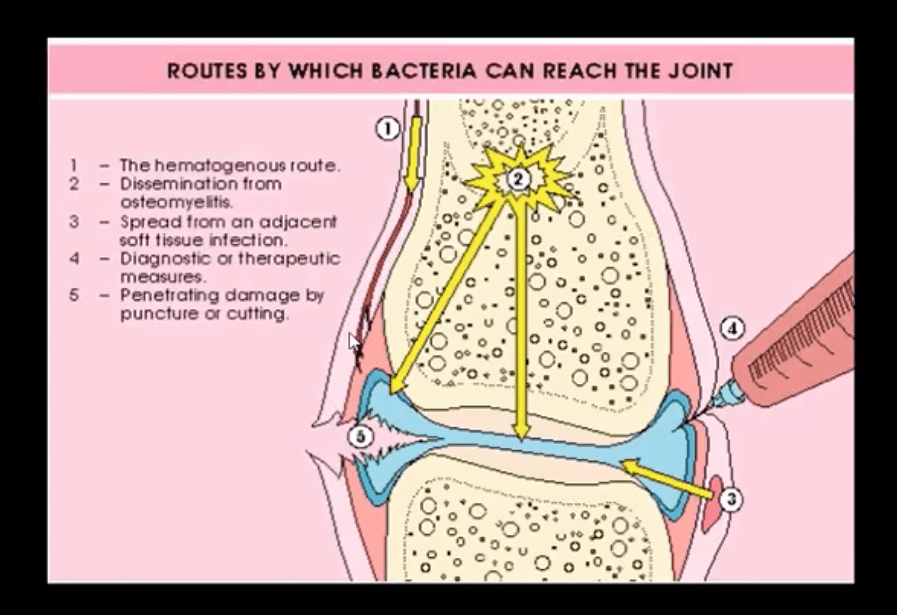
Routs of Infection:
1) Hematogenous is m/c
2) Spread from an adjacent site
3) Direct implantation (e.g., trauma, iatrogenically)
Patients at risk: children, diabetics, immunocompromised, pre-existing joint damage/inflammation, e.g., RA, etc.
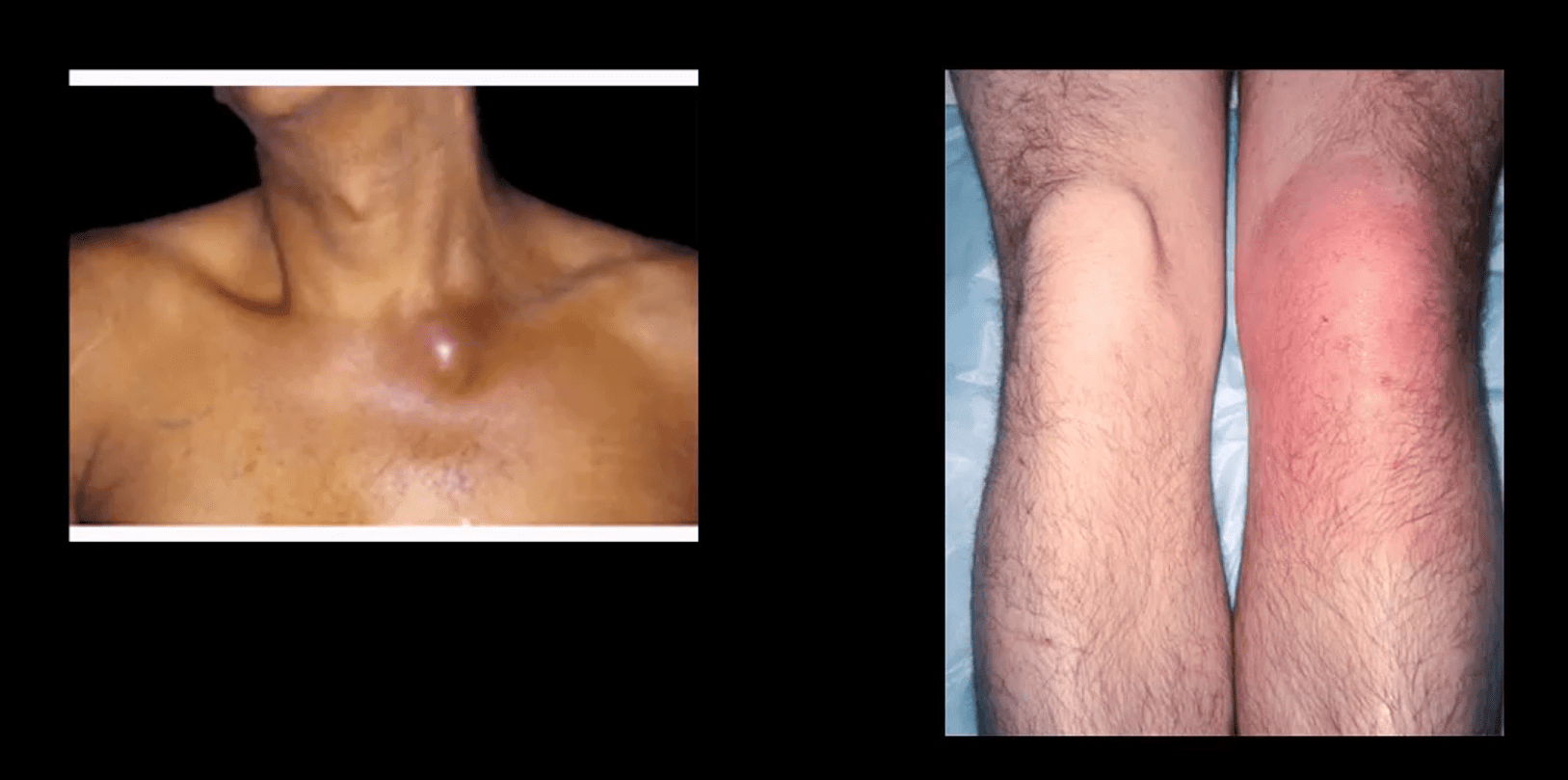
I.V. drug users are particularly at risk and also may contaminate atypical joints “the S joints” SIJ, SCJ, Symphysis pubis, ACJ, etc.
Clinically: may vary and depends on host immune response and bacterial virulence. May present with rapid onset or exacerbation of pre-existing joint pain, swelling, limitation of ROM. General signs of malaise, fever, fatigue and elevated ESR, CRP, Leucocytosis may be present.
N.B. Diabetics and immunocompromised may present with fewer manifestations and lack of fever d/t declining immune response
Dx: clinical, radiological and laboratory. Arthrocentesis may be necessary for culture, cell count and purulent synovial examination
Management: I.V. antibiotics
Imaging Dx: begins with radiography but in the early stage most likely will be unremarkable. MRI can be sensitive and help with early identification of joint effusion, bone edema, etc. US may be helpful in the superficial joints and children. US helps with needle guidance. Bone scintigraphy may be used occaisonally if MRI is contraindicated
Routes of Joint Contamination
1. Hematogenous (M/C)
2. Spread from the adjacent site
3. Direct inoculation
M/C organism-Staph aureus
N.B Gonococcal infection may be a top differential in some cases
IV drug users: Pseudomonas, candida
Sickle cell: Salmonella
Animal (cats/dogs) bites: Pasteurella
Occasionally fungal contamination may occur
Radiography
Initially non-specific ST/joint effusion, obscuration/distortion of fat planes. Because it takes 30% of compact and 50-75% trabecular bone to be destroyed before seen on x-rays, radiography is insensitive to some of the early changes. MR imaging is the preferred modality
If MRI is not available or contraindicated. Bone scintigraphy with Tc-99 MDT can help
In children, US preferred to avoid ionizing radiation. In children, US can be more sensitive than in adults due to lack of bone maturation
Radiographic Dx
Early findings are unrewarding. Early features may include joint widening d/t effusion. Soft tissue swelling and obscuration/displacement of fat planes
1-2 weeks: periarticular and adjacent osseous changes are manifesting as patchy demineralization, moth-eaten, permeating bone destruction, loss, and indistinctness of the epiphyseal “white cortical line” with an increase in soft tissue swelling. MRI may be helpful with early Dx.
Late features: complete joint destruction and ankyloses
N.B. Septic arthritis may progress rapidly within days and requires early I.V. antibiotic to prevent major joint destruction
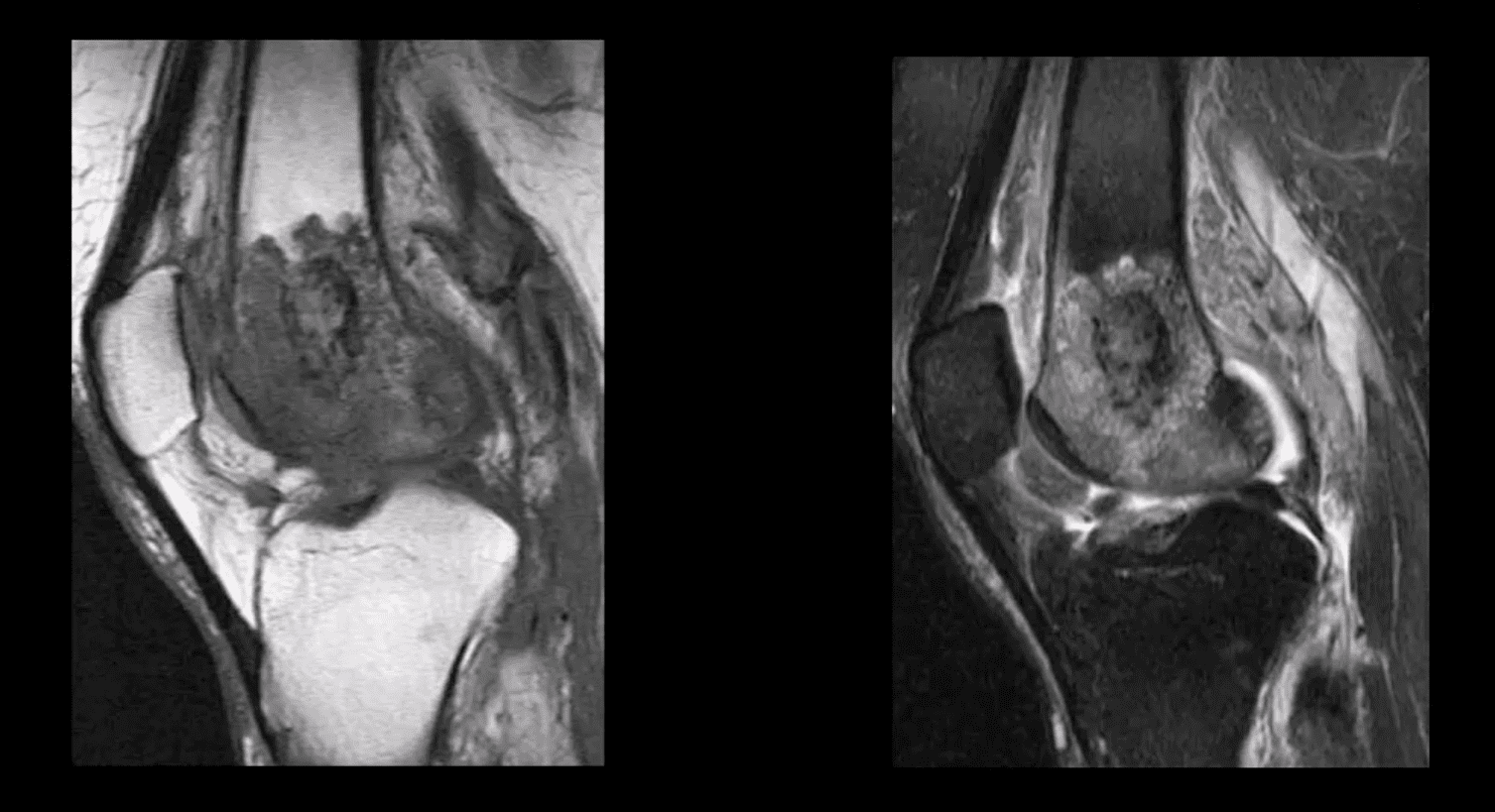
T1 & T2 Knee MRI
T1 (above left) and T2 fat-sat sagittal knee MRI slices reveal loss of normal marrow signal on T1 and increase on T2 due to septic edema. Bone sequestrum d/t osteomyelitis progressing into septic arthritis is noted. Marked joint effusion with adjacent soft tissue edema is seen. Dx: OSM and septic arthritis
Imaging may help the Dx of the septic joint. However, the final Dx is based on Hx, physical examination, blood tests and most importantly synovial aspiration (arthrocentesis)
Synovial fluid should be sent for Gram staining, culture, glucose testing, leukocyte count, and differential determination
ESR/CRP may be elevated
Synovial fluid: WBC can be 50,000-60,000/ul, with 80% neutrophils with depleted glucose levels Gram stain: in 75% gram-positive cocci. Gram staining is less sensitive in gonococcal infection with only 25% of cultures +
In 9% of cases, blood cultures are the only source of pathogen identification and should be obtained before antibiotic treatment
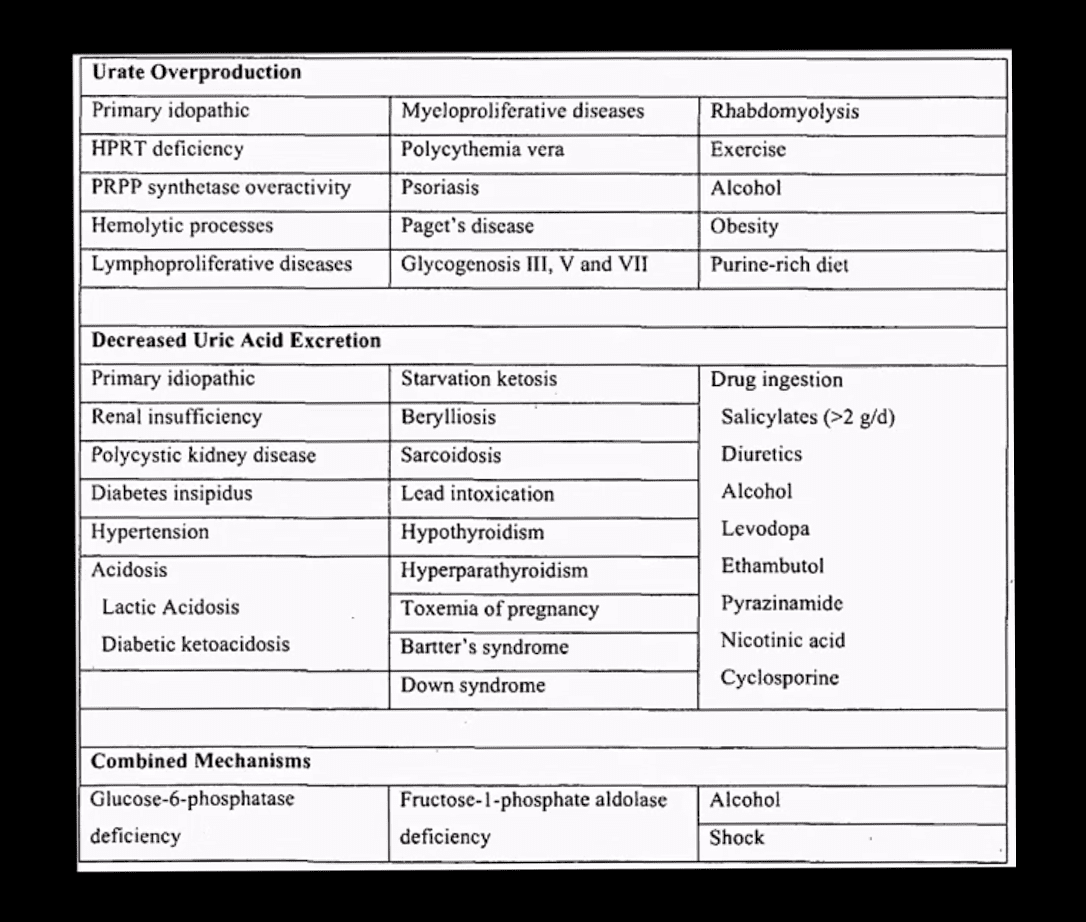
Gout: MSU deposition in and around joints and soft tissues. Elevated levels of serum uric acid (UA) (>7mg/dL) caused by overproduction or under-excretion of uric acid
Once UA reached/exceeded 7mg/dL, it will deposit in the peripheral tissues. Primary gout: disturbed metabolism of nucleic acids and purines break down. Secondary gout: increased cell turnover: Psoriasis, leukemia, multiple myeloma, hemolysis, chemotherapy, etc.
Gout presents with 5-characteristic stages:
1)asymptomatic hyperuricemia (years/decades)
acute attacks of gouty arthritis (waxes and wanes and lasts for several years)
Interval phase between attacks
Chronic tophaceous gout
Gouty nephropathy
Clinical Presentation
Depends� on stages
Acute attacks: acute joint pain “first and the worst” even painful to light touch
DDx: septic joint (both may co-exist) bursitis etc.
Gouty arthritis typically presents as monoarthropathy
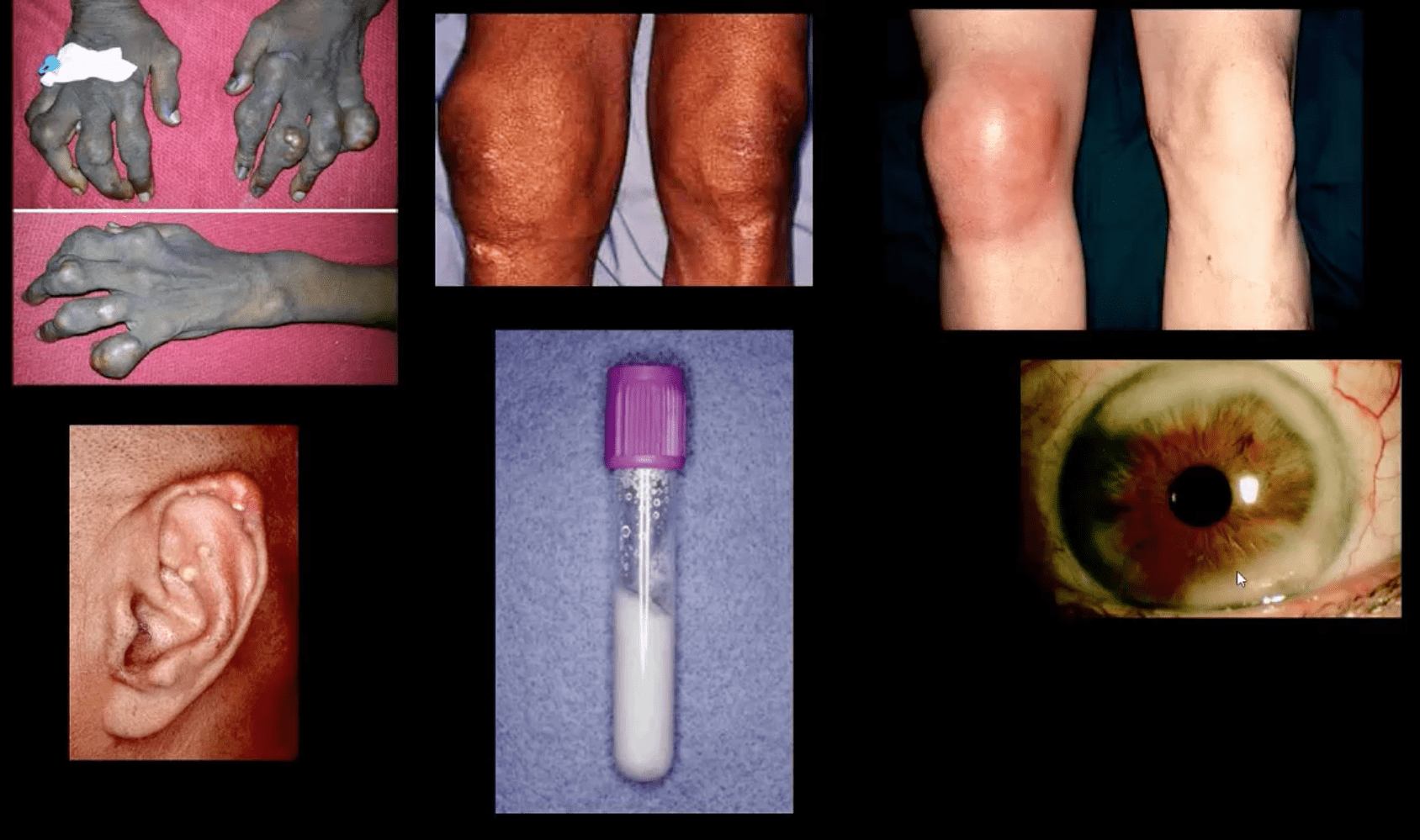
Chronic tophaceous stage: deposits in joints, ear pinna, ocular structures, and other regions. Nephrolithiasis etc. Men>women. Obesity, diet, and age >50-60.
Radiography: early attacks are unremarkable and may present as non-specific joint effusion
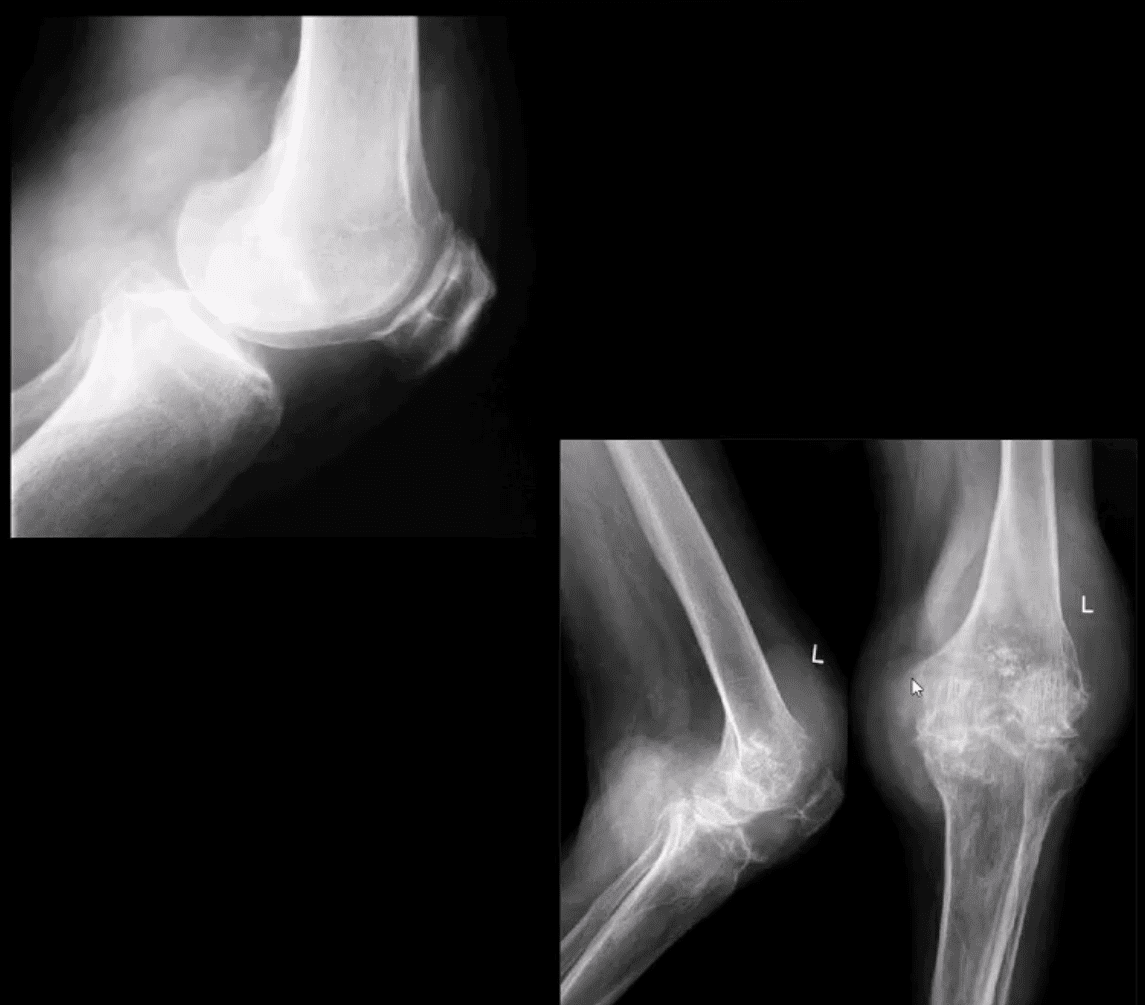
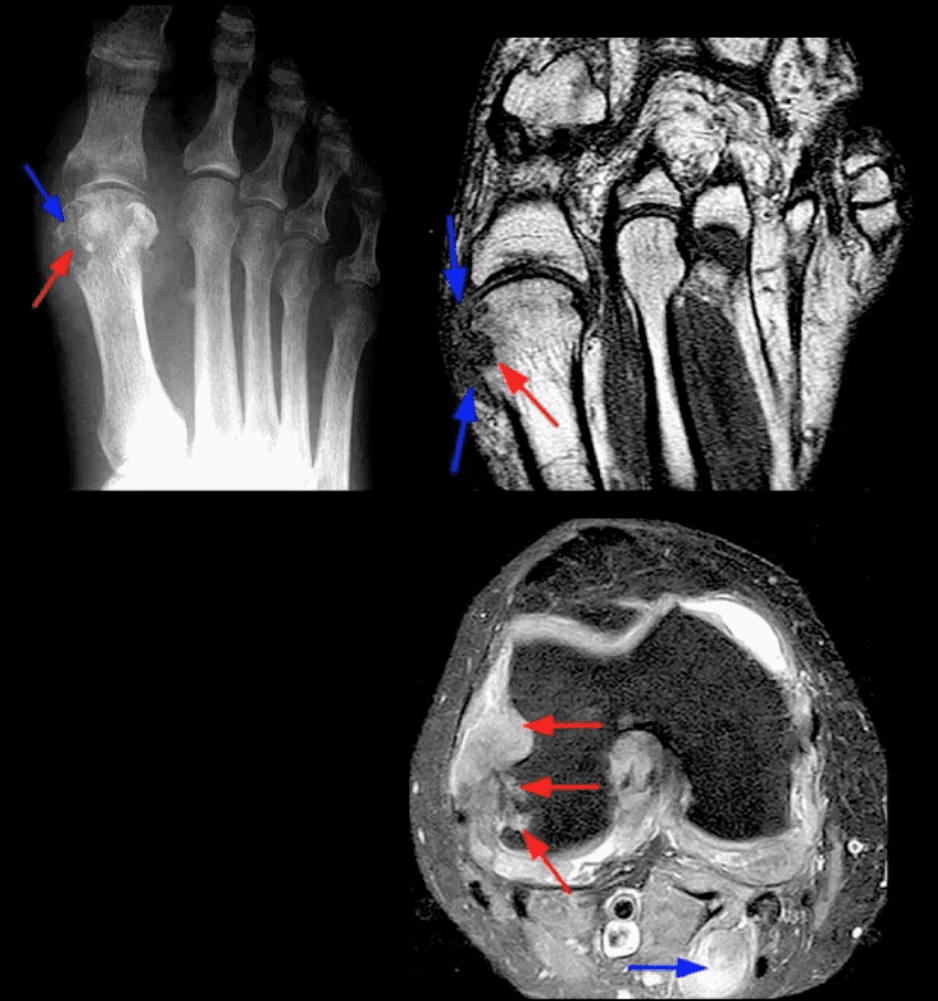
Chronic tophaceous gout radiography: punched out peri-articular, para-articular and intraosseous erosions with overhanging edges. A characteristic rim of sclerosis and internal calcification, soft tissue tophi. Target sites: lower extremity m/c
Rx: allopurinol, colchicine (esp. preventing acute episodes and maintenance)
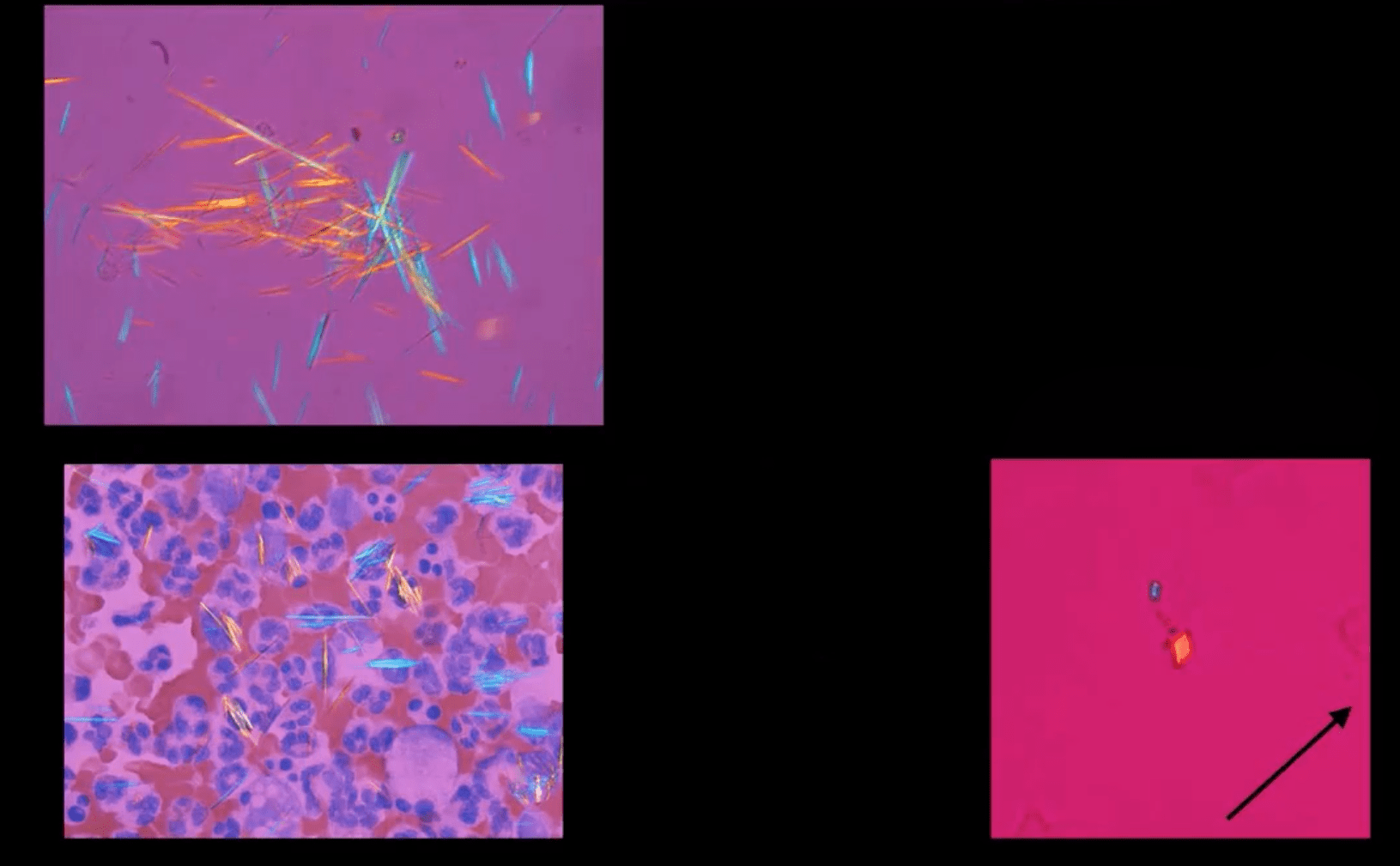
Synovial Aspiration
Synovial aspiration with polarized microscopy reveal negatively birefringent needle-shaped MSU crystals with large inflammatory PMN presence. DDx: positively birefringent rhomboid-shaped CPPD crystals (above bottom right) seen in Pseudogout and CPPD
Large S.T.
Density and joint effusion punched out osseous erosion with overhanging margins, overall preservation of bone density, internal calcifications Dx: chronic tophaceous gout
MRI Gout Features
Erosions with overhanging margins, a low signal on T1 and high on T2 and fat-suppressed images. Peripheral contrast enhancement of tophaceous deposits d/t granulation tissue
Dx: final Dx; synovial aspiration and polarized microscopy
The knee is the largest joint in the human body, where the complex structures of the lower and upper legs come together. Consisting of three bones, the femur, the tibia, and the patella which are surrounded by a variety of soft tissues, including cartilage, tendons and ligaments, the knee functions as a hinge, allowing you to walk, jump, squat or sit. As a result, however, the knee is considered to be one of the joints that are most prone to suffer injury. A knee injury is the prevalent cause of knee pain.
A knee injury can occur as a result of a direct impact from a slip-and-fall accident or automobile accident, overuse injury from sports injuries, or even due to underlying conditions, such as arthritis. Knee pain is a common symptom which affects people of all ages. It may also start suddenly or develop gradually over time, beginning as a mild or moderate discomfort then slowly worsening as time progresses. Moreover, being overweight can increase the risk of knee problems. The purpose of the following article is to discuss the evaluation of patients presenting with knee pain and demonstrate their differential diagnosis.
Abstract
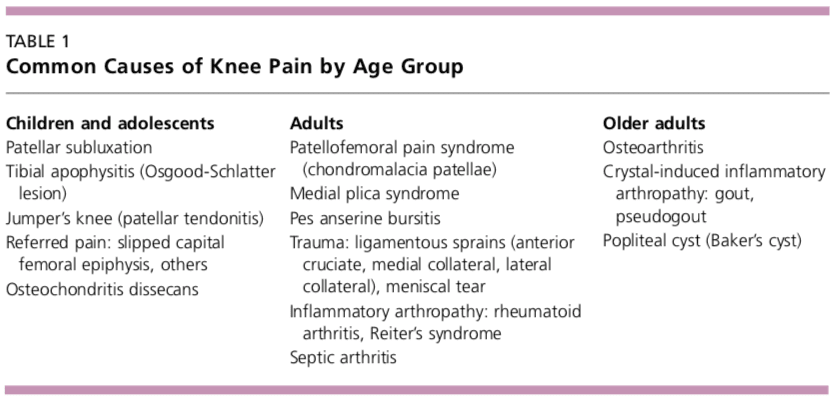
Knee pain is a common presenting complaint with many possible causes. An awareness of certain patterns can help the family physician identify the underlying cause more efficiently. Teenage girls and young women are more likely to have patellar tracking problems such as patellar subluxation and patellofemoral pain syndrome, whereas teenage boys and young men are more likely to have knee extensor mechanism problems such as tibial apophysitis (Osgood-Schlatter lesion) and patellar tendonitis. Referred pain resulting from hip joint pathology, such as slipped capital femoral epiphysis, also may cause knee pain. Active patients are more likely to have acute ligamentous sprains and overuse injuries such as pes anserine bursitis and medial plica syndrome. Trauma may result in acute ligamentous rupture or fracture, leading to acute knee joint swelling and hemarthrosis. Septic arthritis may develop in patients of any age, but crystal-induced inflammatory arthropathy is more likely in adults. Osteoarthritis of the knee joint is common in older adults. (Am Fam Physician 2003;68:917-22. Copyright� 2003 American Academy of Family Physicians.)
Introduction
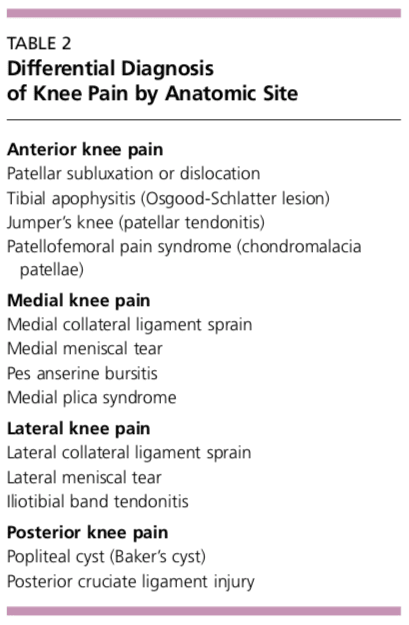
Determining the underlying cause of knee pain can be difficult, in part because of the extensive differential diagnosis. As discussed in part I of this two-part article,1 the family physician should be familiar with knee anatomy and common mechanisms of injury, and a detailed history and focused physical examination can narrow possible causes. The patient�s age and the anatomic site of the pain are two factors that can be important in achieving an accurate diagnosis (Tables 1 and 2). �
�
�
Children and Adolescents
Children and adolescents who present with knee pain are likely to have one of three common conditions: patellar subluxation, tibial apophysitis, or patellar tendonitis. Additional diagnoses to consider in children include slipped capital femoral epiphysis and septic arthritis.
Patellar Subluxation
Patellar subluxation is the most likely diagnosis in a teenage girl who presents with giving-way episodes of the knee.2 This injury occurs more often in girls and young women because of an increased quadriceps angle (Q angle), usually greater than 15 degrees.
Patellar apprehension is elicited by subluxing the patella laterally, and a mild effusion is usually present. Moderate to severe knee swelling may indicate hemarthrosis, which suggests patellar dislocation with osteochondral fracture and bleeding.
Tibial Apophysitis
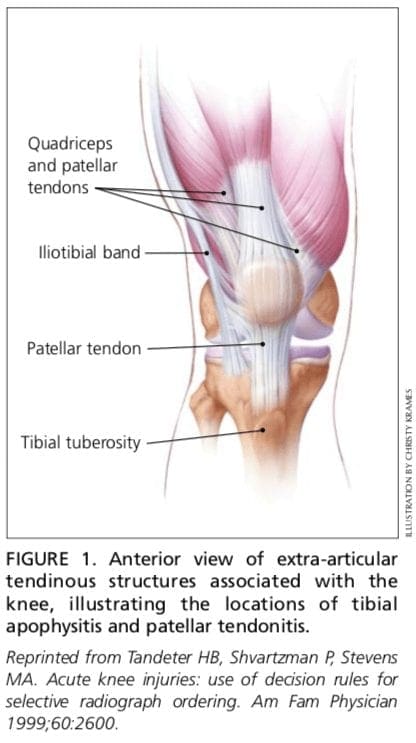
A teenage boy who presents with anterior knee pain localized to the tibial tuberosity is likely to have tibial apophysitis or Osgood- Schlatter lesion3,4 (Figure 1).5 The typical patient is a 13- or 14-year-old boy (or a 10- or 11-year-old girl) who has recently gone through a growth spurt.
The patient with tibial apophysitis generally reports waxing and waning of knee pain for a period of months. The pain worsens with�squatting, walking up or down stairs, or forceful contractions of the quadriceps muscle. This overuse apophysitis is exacerbated by jumping and hurdling because repetitive hard landings place excessive stress on the insertion of the patellar tendon.
On physical examination, the tibial tuberosity is tender and swollen and may feel warm. The knee pain is reproduced with the resisted active extension or passive hyperflexion of the knee. No effusion is present. Radiographs are usually negative; rarely, they show avulsion of the apophysis at the tibial tuberosity. However, the physician must not mistake the normal appearance of the tibial apophysis for an avulsion fracture. �
�
�
�
Patellar Tendonitis
Jumper�s knee (irritation and inflammation of the patellar tendon) most commonly occurs in teenage boys, particularly during a growth spurt2 (Figure 1).5 The patient reports vague anterior knee pain that has persisted for months and worsens after activities such as walking down stairs or running.
On physical examination, the patellar tendon is tender, and the pain is reproduced by resisted knee extension. There is usually no effusion. Radiographs are not indicated.
Slipped Capital Femoral Epiphysis
A number of pathologic conditions result in referral of pain to the knee. For example, the possibility of slipped capital femoral epiphysis must be considered in children and teenagers who present with knee pain.6 The patient with this condition usually reports poorly localized knee pain and no history of knee trauma.
The typical patient with slipped capital femoral epiphysis is overweight and sits on the examination table with the affected hip slightly flexed and externally rotated. The knee examination is normal, but hip pain is elicited with passive internal rotation or extension of the affected hip.
Radiographs typically show displacement of the epiphysis of the femoral head. However, negative radiographs do not rule out the diagnosis in patients with typical clinical findings. Computed tomographic (CT) scanning is indicated in these patients.
Osteochondritis Dissecans
Osteochondritis dissecans is an intra-articular osteochondrosis of unknown etiology that is characterized by degeneration and recalcification of articular cartilage and underlying bone. In the knee, the medial femoral condyle is most commonly affected.7
The patient reports vague, poorly localized knee pain, as well as morning stiffness or recurrent effusion. If a loose body is present, mechanical symptoms of locking or catching of the knee joint also may be reported. On physical examination, the patient may demonstrate quadriceps atrophy or tenderness along the involved chondral surface. A mild joint effusion may be present.7
Plain-film radiographs may demonstrate the osteochondral lesion or a loose body in the knee joint. If osteochondritis dissecans is suspected, recommended radiographs include anteroposterior, posteroanterior tunnel, lateral, and Merchant�s views. Osteochondral lesions at the lateral aspect of the medial femoral condyle may be visible only on the posteroanterior tunnel view. Magnetic resonance imaging (MRI) is highly sensitive in detecting these abnormalities and is indicated in patients with a suspected osteochondral lesion.7 �
�
A knee injury caused by sports injuries, automobile accidents, or an underlying condition, among other causes, can affect the cartilage, tendons and ligaments which form the knee joint itself. The location of the knee pain can differ according to the structure involved, also, the symptoms can vary. The entire knee may become painful and swollen as a result of inflammation or infection, whereas a torn meniscus or fracture may cause symptoms in the affected region. Dr. Alex Jimenez D.C., C.C.S.T. Insight
Adults
Overuse Syndromes
Anterior Knee Pain. Patients with patellofemoral pain syndrome (chondromalacia patellae) typically present with a vague history of mild to moderate anterior knee pain that usually occurs after prolonged periods of sitting (the so-called �theater sign�).8 Patellofemoral pain syndrome is a common cause of anterior knee pain in women.
On physical examination, a slight effusion may be present, along with patellar crepitus on the range of motion. The patient�s pain may be reproduced by applying direct pressure to the anterior aspect of the patella. Patellar tenderness may be elicited by subluxing the patella medially or laterally and palpating the superior and inferior facets of the patella. Radiographs usually are not indicated.
Medial Knee Pain. One frequently overlooked diagnosis is medial plica syndrome. The plica, a redundancy of the joint synovium medially, can become inflamed with repetitive overuse.4,9 The patient presents with acute onset of medial knee pain after a marked increase in usual activities. On physical examination, a tender, mobile nodularity is present at the medial aspect of the knee, just anterior to the joint line. There is no joint effusion, and the remainder of the knee examination is normal. Radiographs are not indicated.
Pes anserine bursitis is another possible cause of medial knee pain. The tendinous insertion of the sartorius, gracilis, and semitendinosus muscles at the anteromedial aspect of the proximal tibia forms the pes anserine bursa.9 The bursa can become inflamed as a result of overuse or a direct contusion. Pes�anserine bursitis can be confused easily with a medial collateral ligament sprain or, less commonly, osteoarthritis of the medial compartment of the knee. �
�
�
The patient with pes anserine bursitis reports pain at the medial aspect of the knee. This pain may be worsened by repetitive flexion and extension. On physical examination, tenderness is present at the medial aspect of the knee, just posterior and distal to the medial joint line. No knee joint effusion is present, but there may be slight swelling at the insertion of the medial hamstring muscles. Valgus stress testing in the supine position or resisted knee flexion in the prone position may reproduce the pain. Radiographs are usually not indicated.
Lateral Knee Pain. Excessive friction between the iliotibial band and the lateral femoral condyle can lead to iliotibial band tendonitis.9 This overuse syndrome commonly occurs in runners and cyclists, although it may develop in any person subsequent to activity involving repetitive knee flexion. The tightness of the iliotibial band, excessive foot pronation, genu varum, and tibial torsion are predisposing factors.
The patient with iliotibial band tendonitis reports pain at the lateral aspect of the knee joint. The pain is aggravated by activity, particularly running downhill and climbing stairs. On physical examination, tenderness is present at the lateral epicondyle of the femur, approximately 3 cm proximal to the joint line. Soft tissue swelling and crepitus also may be present, but there is no joint effusion. Radiographs are not indicated.
Noble�s test is used to reproduce the pain in iliotibial band tendonitis. With the patient in a supine position, the physician places a thumb over the lateral femoral epicondyle as the�patient repeatedly flexes and extends the knee. Pain symptoms are usually most prominent with the knee at 30 degrees of flexion.
Popliteus tendonitis is another possible cause of lateral knee pain. However, this condition is fairly rare.10
Trauma
Anterior Cruciate Ligament Sprain. Injury to the anterior cruciate ligament usually occurs because of noncontact deceleration forces, as when a runner plants one foot and sharply turns in the opposite direction. Resultant valgus stress on the knee leads to anterior displacement of the tibia and sprain or rupture of the ligament.11 The patient usually reports hearing or feeling a �pop� at the time of the injury and must cease activity or competition immediately. Swelling of the knee within two hours after the injury indicates rupture of the ligament and consequent hemarthrosis.
On physical examination, the patient has a moderate to severe joint effusion that limits the range of motion. The anterior drawer test may be positive, but can be negative because of hemarthrosis and guarding by the hamstring muscles. The Lachman test should be positive and is more reliable than the anterior drawer test (see text and Figure 3 in part I of the article1).
Radiographs are indicated to detect possible tibial spine avulsion fracture. MRI of the knee is indicated as part of a presurgical evaluation.
Medial Collateral Ligament Sprain. Injury to the medial collateral ligament is fairly common and is usually the result of acute trauma. The patient reports a misstep or collision that places valgus stress on the knee, followed by the immediate onset of pain and swelling at the medial aspect of the knee.11
On physical examination, the patient with medial collateral ligament injury has point tenderness at the medial joint line. Valgus stress testing of the knee flexed to 30 degrees reproduces the pain (see text and Figure 4 in part I of this article1). A clearly defined endpoint on valgus stress testing indicates a grade 1�or grade 2 sprain, whereas complete medial instability indicates full rupture of the ligament (grade 3 sprain).
Lateral Collateral Ligament Sprain. Injury of the lateral collateral ligament is much less common than the injury of the medial collateral ligament. Lateral collateral ligament sprain usually results from varus stress to the knee, as occurs when a runner plants one foot and then turns toward the ipsilateral knee.2 The patient reports acute onset of lateral knee pain that requires prompt cessation of activity.
On physical examination, point tenderness is present at the lateral joint line. Instability or pain occurs with varus stress testing of the knee flexed to 30 degrees (see text and Figure 4 in part I of this article1). Radiographs are not usually indicated.
Meniscal Tear. The meniscus can be torn acutely with a sudden twisting injury of the knee, such as may occur when a runner suddenly changes direction.11,12 Meniscal tear also may occur in association with a prolonged degenerative process, particularly in a patient with an anterior cruciate ligament-deficient knee. The patient usually reports recurrent knee pain and episodes of catching or locking of the knee joint, especially with squatting or twisting of the knee.
On physical examination, a mild effusion is usually present, and there is tenderness at the medial or lateral joint line. Atrophy of the vastus medialis obliquus portion of the quadriceps muscle also may be noticeable. The McMurray test may be positive (see Figure 5 in part I of this article1), but a negative test does not eliminate the possibility of a meniscal tear.
Plain-film radiographs usually are negative and seldom are indicated. MRI is the radiologic test of choice because it demonstrates most significant meniscal tears.
Infection
Infection of the knee joint may occur in patients of any age but is more common in those whose immune system has been weakened by cancer, diabetes mellitus, alcoholism,�acquired immunodeficiency syndrome, or corticosteroid therapy. The patient with septic arthritis reports abrupt onset of pain and swelling of the knee with no antecedent trauma.13
On physical examination, the knee is warm, swollen, and exquisitely tender. Even slight motion of the knee joint causes intense pain.
Arthrocentesis reveals turbid synovial fluid. Analysis of the fluid yields a white blood cell count (WBC) higher than 50,000 per mm3 (50 ? 109 per L), with more than 75 percent (0.75) polymorphonuclear cells, an elevated protein content (greater than 3 g per dL [30 g per L]), and a low glucose concentration (more than 50 percent lower than the serum glucose concentration).14 Gram stain of the fluid may demonstrate the causative organism. Common pathogens include Staphylococcus aureus, Streptococcus species, Haemophilus influenza, and Neisseria gonorrhoeae.
Hematologic studies show an elevated WBC, an increased number of immature polymorphonuclear cells (i.e., a left shift), and an elevated erythrocyte sedimentation rate (usually greater than 50 mm per hour).
Older Adults
Osteoarthritis
Osteoarthritis of the knee joint is a common problem after 60 years of age. The patient presents with knee pain that is aggravated by weight-bearing activities and relieved by rest.15 The patient has no systemic symptoms but usually awakens with morning stiffness that dissipates somewhat with activity. In addition to chronic joint stiffness and pain, the patient may report episodes of acute synovitis.
Findings on physical examination include decreased range of motion, crepitus, a mild joint effusion, and palpable osteophytic changes at the knee joint.
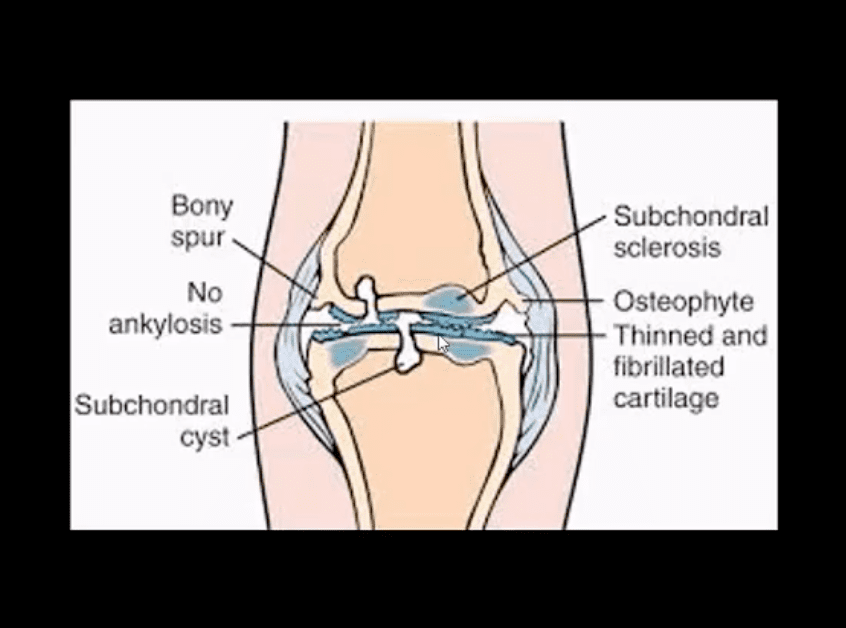
When osteoarthritis is suspected, recommended radiographs include weight-bearing anteroposterior and posteroanterior tunnel views, as well as non-weight-bearing Merchants and lateral views. Radiographs show�joint-space narrowing, subchondral bony sclerosis, cystic changes, and hypertrophic osteophyte formation.
Crystal-Induced Inflammatory Arthropathy
Acute inflammation, pain, and swelling in the absence of trauma suggest the possibility of a crystal-induced inflammatory arthropathy such as gout or pseudogout.16,17 Gout commonly affects the knee. In this arthropathy, sodium urate crystals precipitate in the knee joint and cause an intense inflammatory response. In pseudogout, calcium pyrophosphate crystals are the causative agents.
On physical examination, the knee joint is erythematous, warm, tender, and swollen. Even minimal range of motion is exquisitely painful.
Arthrocentesis reveals clear or slightly cloudy synovial fluid. Analysis of the fluid yields a WBC count of 2,000 to 75,000 per mm3 (2 to 75 ? 109 per L), a high protein content (greater than 32 g per dL [320 g per L]), and a glucose concentration that is approximately 75 percent of the serum glucose con- centration.14 Polarized-light microscopy of the synovial fluid displays negatively birefringent rods in the patient with gout and positively birefringent rhomboids in the patient with pseudogout.
Popliteal Cyst
The popliteal cyst (Baker�s cyst) is the most common synovial cyst of the knee. It originates from the posteromedial aspect of the knee joint at the level of the gastrocnemio-semimembranous bursa. The patient reports insidious onset of mild to moderate pain in the popliteal area of the knee.
On physical examination, palpable fullness is present at the medial aspect of the popliteal area, at or near the origin of the medial head of the gastrocnemius muscle. The McMurray test may be positive if the medial meniscus is injured. Definitive diagnosis of a popliteal cyst may be made with arthrography, ultrasonography, CT scanning, or, less commonly, MRI.
The authors indicate that they do not have any conflicts of interest. Sources of funding: none reported.
In conclusion, although the knee is the largest joint in the human body where the structures of the lower extremities meet, including the femur, the tibia, the patella, and many other soft tissues, the knee can easily suffer damage or injury and result in knee pain. Knee pain is one of the most common complaints among the general population, however, it commonly occurs in athletes. Sports injuries, slip-and-fall accidents, and automobile accidents, among other causes, can lead to knee pain.
As described in the article above, diagnosis is essential towards determining the best treatment approach for each type of knee injury, according to their underlying cause. While the location and the severity of the knee injury may vary depending on the cause of the health issue, knee pain is the most common symptom. Treatment options, such as chiropractic care and physical therapy, can help treat knee pain. The scope of our information is limited to chiropractic and spinal health issues. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez �
�
�
Additional Topic Discussion: Relieving Knee Pain without Surgery
�
Knee pain is a well-known symptom which can occur due to a variety of knee injuries and/or conditions, including�sports injuries. The knee is one of the most complex joints in the human body as it is made-up of the intersection of four bones, four ligaments, various tendons, two menisci, and cartilage. According to the American Academy of Family Physicians, the most common causes of knee pain include patellar subluxation, patellar tendinitis or jumper’s knee, and Osgood-Schlatter disease. Although knee pain is most likely to occur in people over 60 years old, knee pain can also occur in children and adolescents. Knee pain can be treated at home following the RICE methods, however, severe knee injuries may require immediate medical attention, including chiropractic care.
1. Calmbach WL, Hutchens M. Evaluation of patients presenting with knee pain: part I. History, physical examination, radiographs, and laboratory tests. Am Fam Physician 2003;68:907-12.
2. Walsh WM. Knee injuries. In: Mellion MB, Walsh WM, Shelton GL, eds. The team physician�s hand- book. 2d ed. St. Louis: Mosby, 1990:554-78.
3. Dunn JF. Osgood-Schlatter disease. Am Fam Physi- cian 1990;41:173-6.
4. Stanitski CL. Anterior knee pain syndromes in the adolescent. Instr Course Lect 1994;43:211-20.
5. Tandeter HB, Shvartzman P, Stevens MA. Acute knee injuries: use of decision rules for selective radiograph ordering. Am Fam Physician 1999;60: 2599-608.
6. Waters PM, Millis MB. Hip and pelvic injuries in the young athlete. In: DeLee J, Drez D, Stanitski CL, eds. Orthopaedic sports medicine: principles and practice. Vol. III. Pediatric and adolescent sports medicine. Philadelphia: Saunders, 1994:279-93.
7. Schenck RC Jr, Goodnight JM. Osteochondritis dis- secans. J Bone Joint Surg [Am] 1996;78:439-56.
8. Ruffin MT 5th, Kiningham RB. Anterior knee pain: the challenge of patellofemoral syndrome. Am Fam Physician 1993;47:185-94.
Cancer puts a tremendous amount of stress on the body. Cancer treatments add to that stress, affecting the organs as well as the musculoskeletal system. Pain is a common complaint among cancer patients. They experience a variety of aches and pains including headaches, neck pain, muscle tension, and back pain as well as painful peripheral neuropathy. They may also have mobility problems and difficulty walking.
Many cancer patients have found chiropractic care to be a very effective treatment for pain management and to improve flexibility, mobility, and muscle strength. They find it helps to reduce stress and helps the body function more efficiently.
It provides these benefits without the use of medication or invasive treatments. For patients undergoing chemotherapy, it is very beneficial because chiropractic�s whole body approach to wellness helps to combat the debilitating effects of the treatment.
Benefits of Chiropractic Care for Cancer Patients
There are many different reasons that cancer patients may seek chiropractic treatment. Cancer is, in itself, very hard on the body. The disease can cause headaches, muscle stiffness, neck pain, and back pain. However, the treatments can also cause problems.
Patients undergoing radiation treatment must lie on a table for extended periods of time which can be very uncomfortable. Surgery can cause pain in the joints and connective tissues. Chemotherapy drugs can cause unpleasant side effects including nausea, neuropathy, and headaches.
Often cancer patients have also reported improvements beyond the typical musculoskeletal complaints that chiropractic treats. Reduced effects of peripheral neuropathy, improved digestion, and even easier respiratory function are just some of the added benefits.
Chiropractic Treatment Approaches
Chiropractors use a drug-free, hands-on approach to treatment for a wide range of issues. It restores nerve function, corrects musculoskeletal problems, and helps to bring the body back into proper alignment. It is non-invasive and offers patients a safe, natural alternative to medications and other treatments that can have unwanted side effects.
One barrier that may prevent a patient from seeking chiropractic care is the common misconception that it is aggressive and forceful, even painful. The truth is, most chiropractic techniques are very gentle, applying very low force and some no force at all.
Most are also not painful at all and work quickly to enhance the range of motion and increase energy as well as reduce pain. It can help relieve a patient�s symptoms while helping them stay strong while they undergo treatment.
Some of the chiropractic treatment options that are used for cancer patients include:
Spinal manipulation
Ice
Heat
Hands-on adjustments
Non-force techniques
Electrical muscle stimulation
Massage
Special instrument applications
Traction
The Whole-Body Wellness Advantage
Whole body wellness is an integral part of chiropractic care. It can involve diet modification, lifestyle changes, exercise, and stress reduction practices.
When a chiropractor treats a cancer patient � or any patient � he or she will look beyond the obvious issues or symptoms to find the root of the problem and ways to help the body heal itself. Sometimes this may involve supplements, vitamins, or minerals that will aid in correcting the condition. Other times it may simply be a matter of getting the body to a healthy state where it is strong enough to combat the condition or heal from injury.
The treatment is individualized and tailored specifically to the patient�s needs and lifestyle. For instance, many conditions benefit from weight loss or exercise, and many pain issues respond well to adjustments in diet and stress reduction. Chiropractic looks at the whole body and works to provide it with what it needs to get strong and get healthy.
Pathology: da disease of the articular cartilage. Continuing mechanical stimulation follows by an initial increase in water and cartilage thickness. Gradual loss of proteoglycans and ground substance. Fissuring/splitting. Chondrocytes are damaged and release enzymes into the joint. Cystic progression and further cartilage loss. Subchondral bone is denuded and exposed to mechanical stresses. It becomes hypervascular forming osteophytes. Subchondral cysts and bone thickening/sclerosis develop.
Imaging plays a crucial role in Dx/grading and management
Clinically: pain on walking/rest, crepitus, swelling d/t synovitis, locking/catching d/t osseocartilaginous fragments and gradual functional loss. Knee OA typically presents as mono and oligoarthritis. DDx: morning pain/stiffness is >30-min DDx from inflammatory arthritis
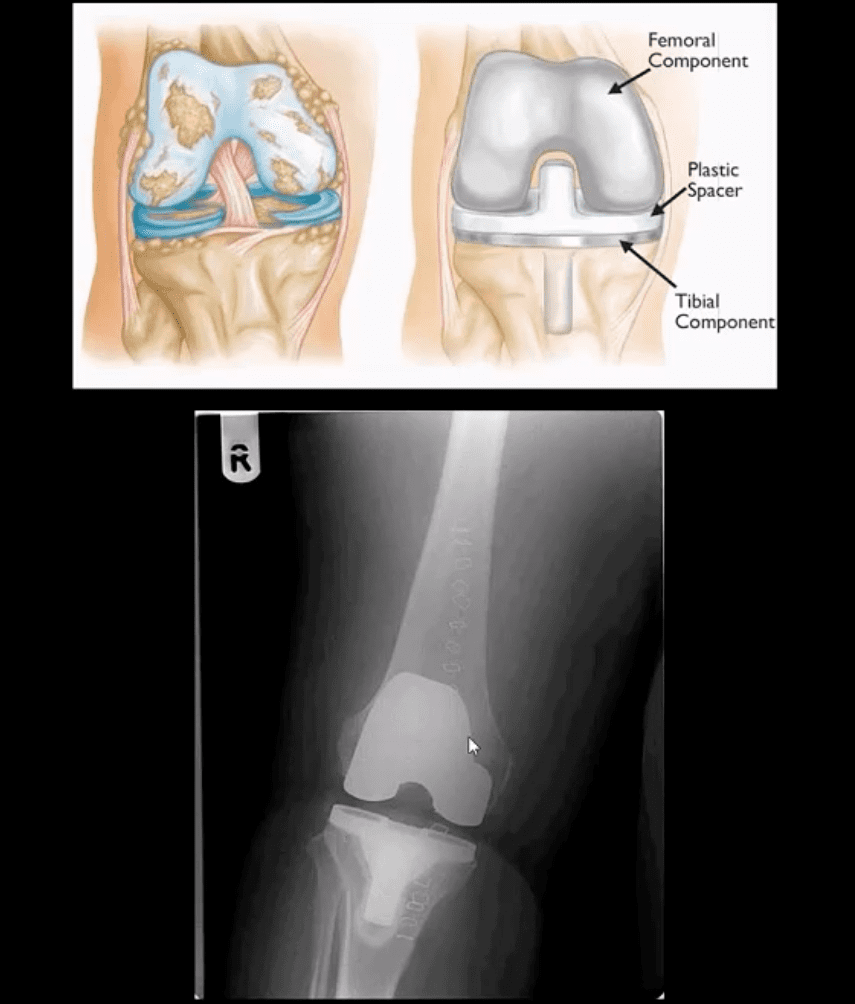
Treatment: in mild to moderate cases-conservative care. Severe OA-total knee arthroplasty
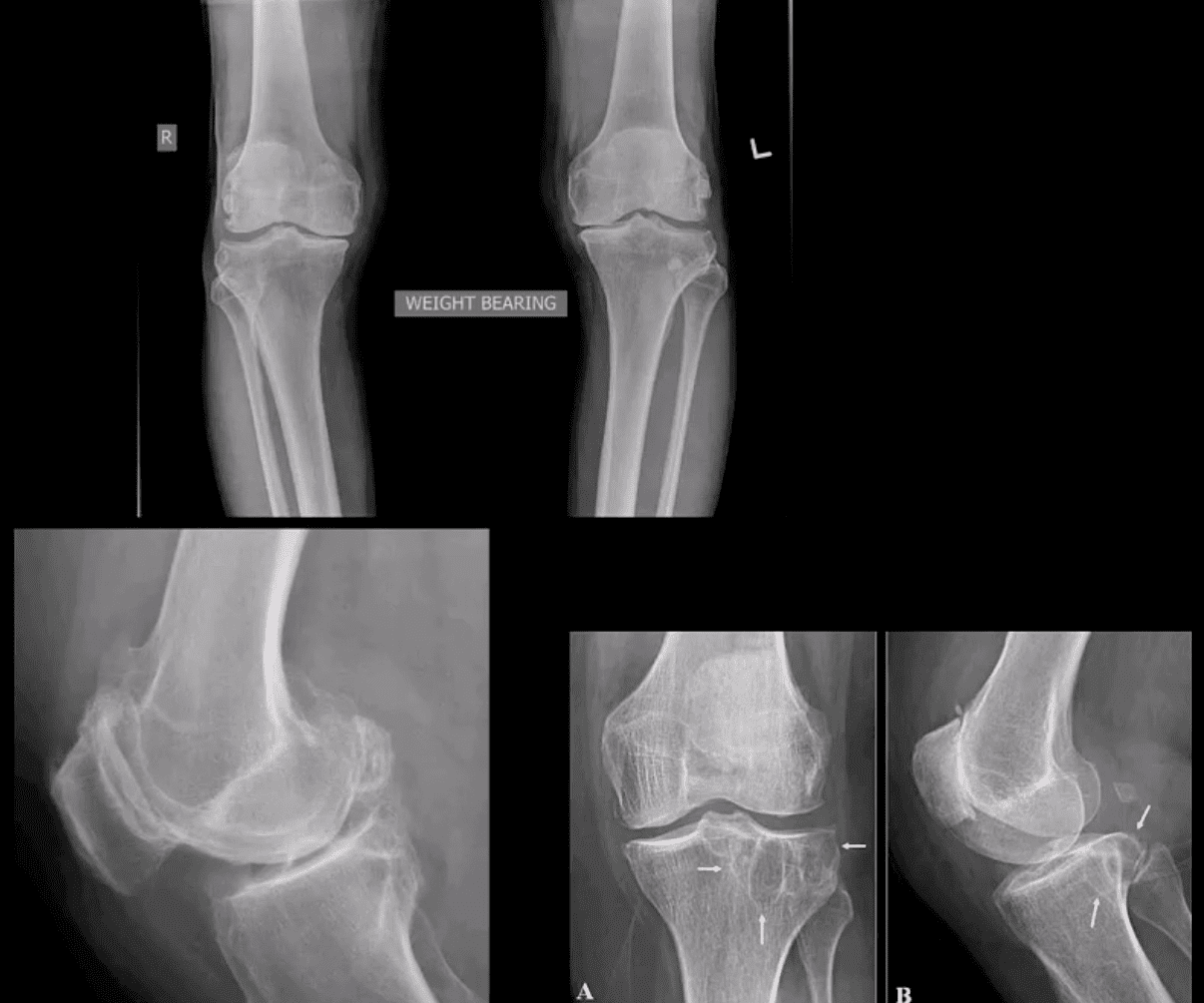
Grade 4: severe JSN, large osteophytes, marked subchondral sclerosis and definite bony deformity
Typical report language will state:
Minor, mild, moderate or severe aka advanced arthrosis
Technique
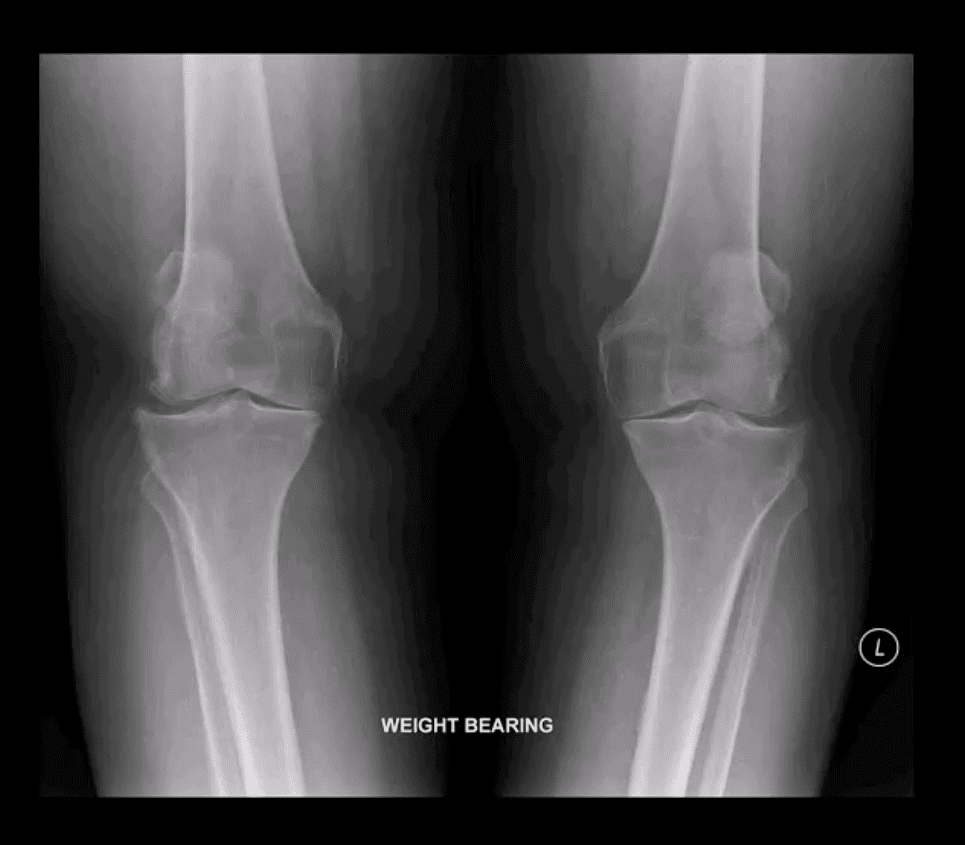
Radiography: AP weight-bearing knees: note severe JSN of the medial compartment more severely with lateral knee compartment. Osteophytes and marked genu varum deformity and bone deformation
Typically medial femorotibial compartment is affected early and more severely
The patellofemoral compartment is also affected and best visualized on the lateral and Sunrise views
Impressions: severe tri-compartmental knee arthrosis
Recommendations: referral to the orthopedic surgeon
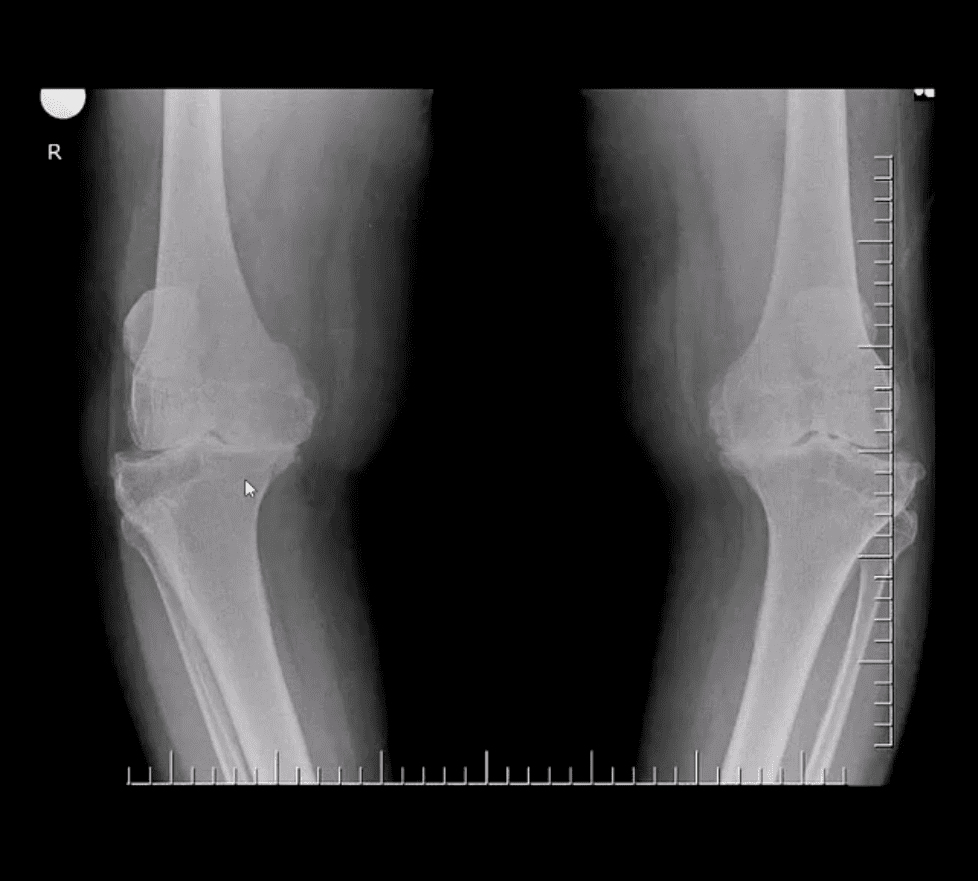
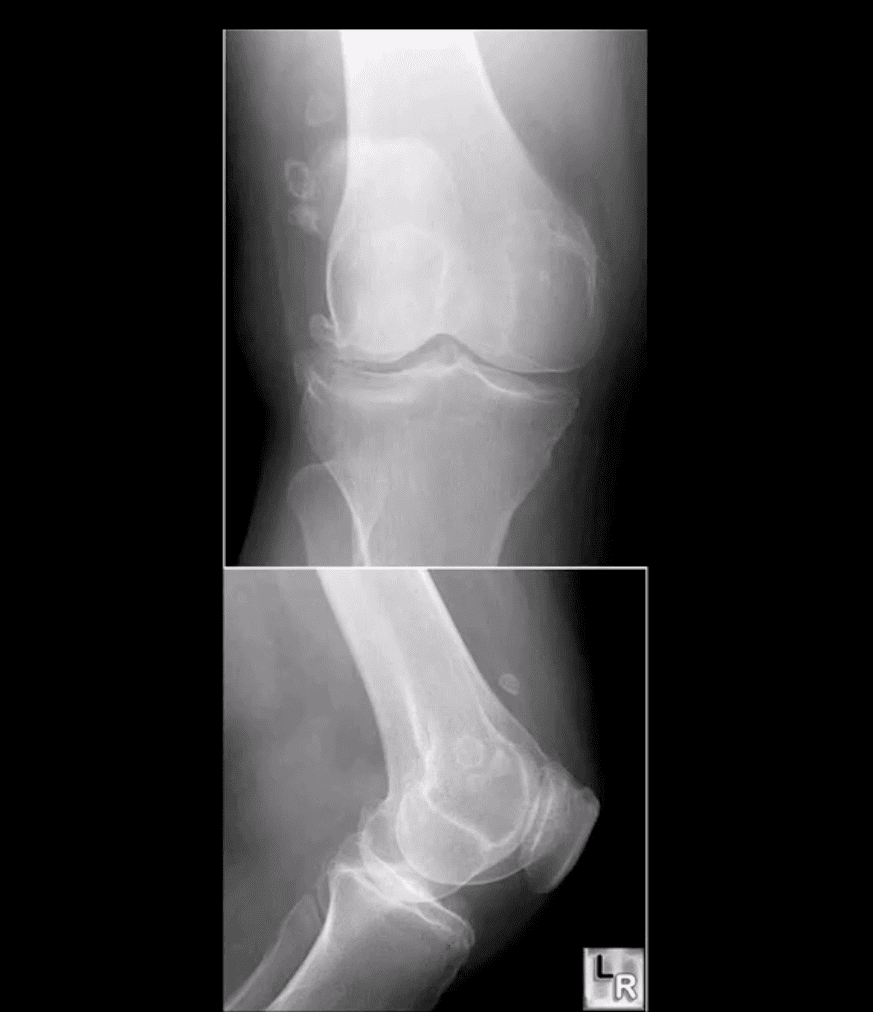
Moderate JSN
B/L AP weight-bearing view (above top image): Moderate JSN primarily of the medial femorotibial compartment. Osteophytosis, subchondral sclerosis and mild bone deformation (genu varum)
May present as asymptomatic chondrocalcinosis, CPPD arthropathy resembling DJD with pan predominance of large subchondral cysts. Often found as isolated PFJ DJD
Pseudogout with an acute attack of knee pain resembling gouty arthritis
Radiography is the 1st step and often reveals the Dx
Arthrocentesis with polarized microscopy may be helpful to DDx between CPPD and Gouty arthritis
Rheumatoid Arthritis
RA: an autoimmune systemic inflammatory disease that targets soft tissues of joints synovium, tendons/ligaments, bursae and extra-articular sites (e.g., eyes, lungs, cardiovascular system)
RA is the m/c inflammatory arthritis, 3% of women and 1% of men. Age: 30-50 F>M 3:1, but may develop at any age. True RA is uncommon in children and should not be confused with Juvenile Idiopathic Arthritis
RA most often affects small joints of the hands and feet as symmetrical arthritis (2nd 3rd MCP, 3rd PIPs, wrists & MTPs, sparing DIPs of fingers and toes)
Radiographically: RA presents with joint effusion leading to hyperemia and marginal erosions and periarticular osteoporosis. In the knee, the lateral compartment is affected more frequently leading to valgus deformity. Uniform aka concentric/symmetrical JSN affects all compartments and remains a key Dx clue
An absence of subchondral sclerosis and osteophytes. Popliteal cyst�(Baker’s cyst) may represent synovial pannus and inflammatory synovitis extending into the popliteal region that may rapture and extend into posterior leg compartment
N.B. Following initial RA joint destruction, it is not unusual to note superimposed 2nd OA
Radiography is the 1st step but early joint involvement may be undetectable by x-rays and can be helped by US and/or MRI.
Final Dx is based on Hx, clinical exam, labs, and radiology
Clinical pearls: patients with RA may present with a single knee being affected
Most patients are likely to have bilateral symmetrical hands/feet RA.
Cervical spine, particularly C1-2 is affected in 75-90% of cases throughout the course of the disease
N.B. Sudden exacerbation of joint pain in RA should not underestimate septic arthritis because patients with pre-existing RA are at higher risk of infectious arthritis. Joint aspiration may help with Dx.
Radiographic DDx
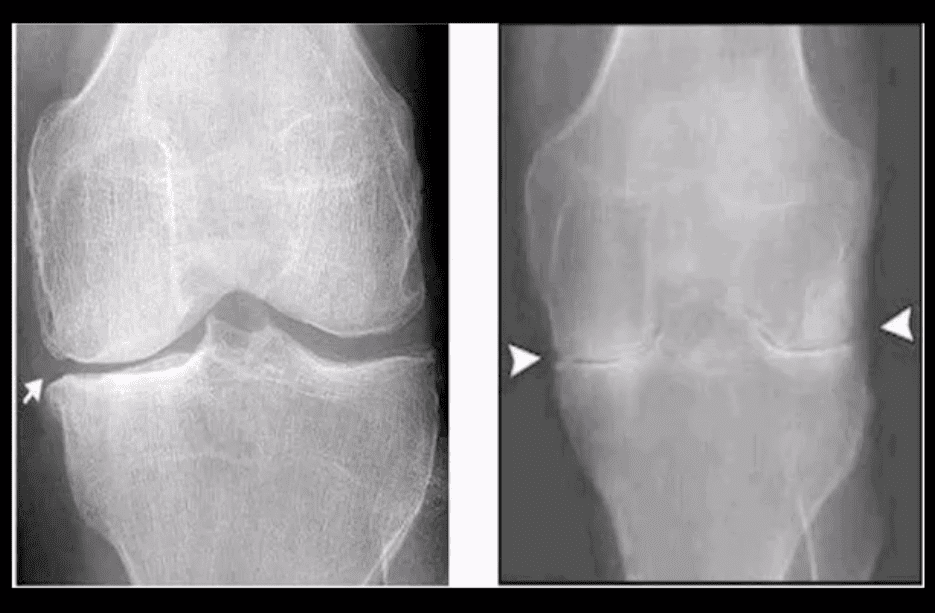
RA (above left) vs. OA (above right)
RA: concentric (uniform) joint space loss, lack of osteophytes and juxta-articular osteopenia.
Clinical Pearls: patients with RA may present radiographically with subchondral sclerosis d/t superimposed DJD. The latter feature should not be interpreted as OA but instead considered as secondary OA
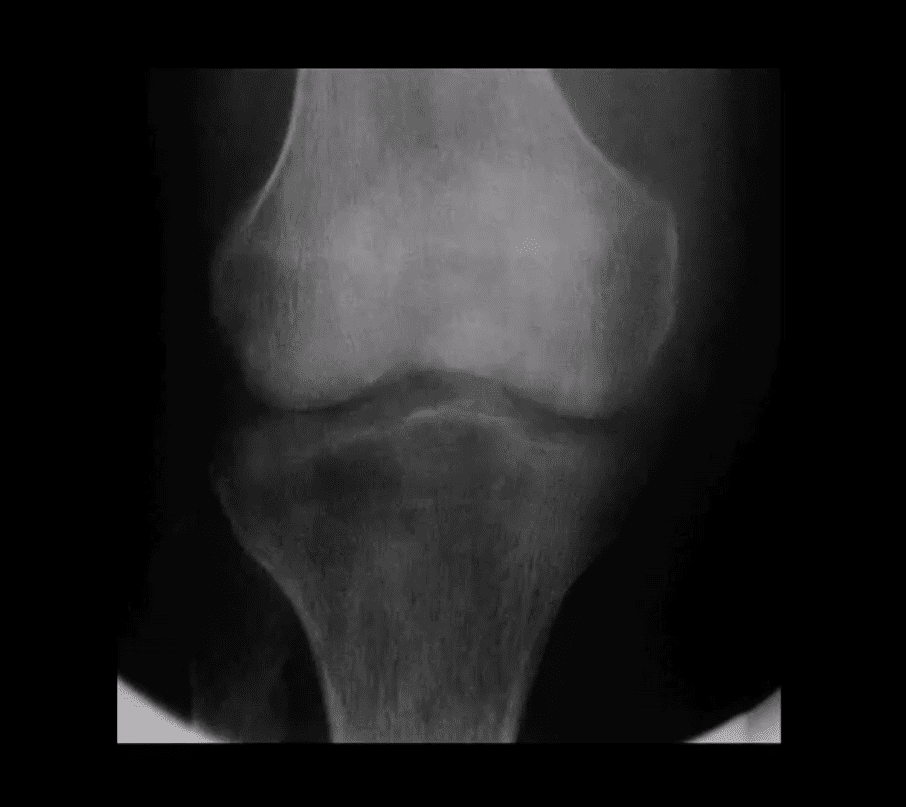
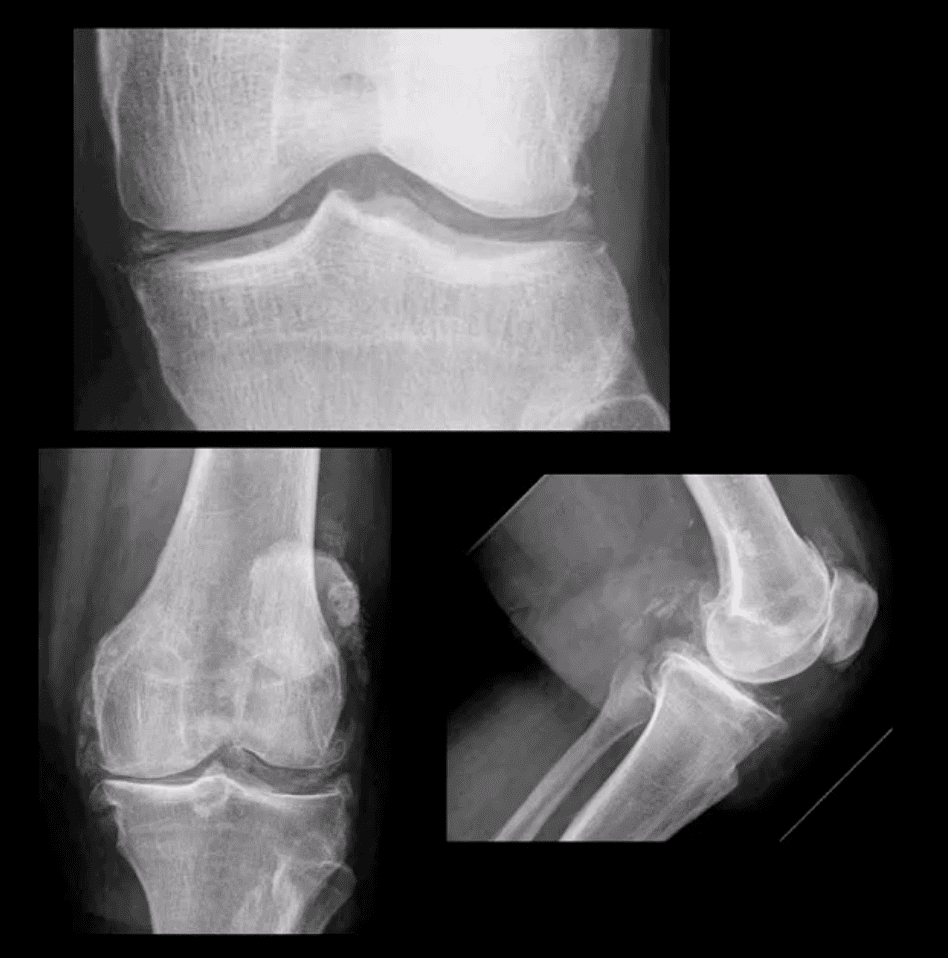
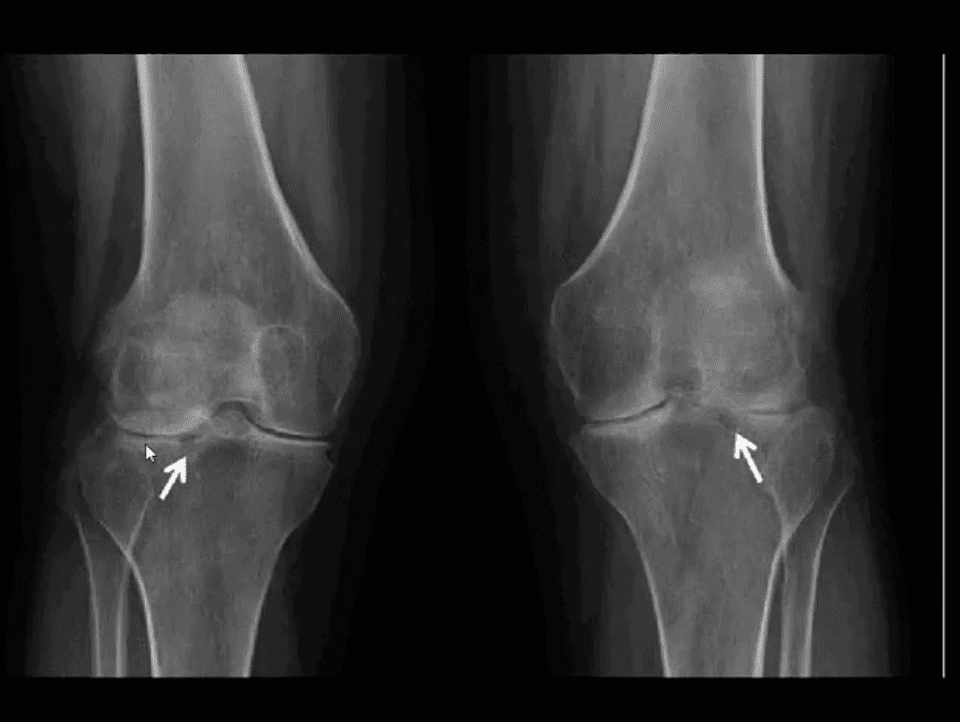
AP Knee Radiograph
Note marked uniform JSN, juxta-articular osteopenia and subchondral cystic changes
Clinical Pearls: subcortical cysts in RA will characteristically lack sclerotic rim noted in OA-associated subcortical cysts.
MRI Sensitivity
MRI is very sensitive and may aid during early Dx of RA.
T2 fat-sat or STIR and T1 + C gad contrast fat-suppressed sequences may be included
MRI Dx of RA: synovial inflammation/effusion, synovial hyperplasia, and pannus formation decreased cartilage thickness, subchondral cysts, and bone erosions
MRI is very sensitive to reveal juxt-articular bone marrow edema, a precursor to erosions
Intra-articular fibrinoid fragments known as “Rice bodies” are characteristic MR sign of RA
Note: T2 fat-sat sagittal MRI revealing large inflammatory joint effusion and pannus synovial proliferation (above arrowheads). No evidence of radiographic or MRI bone erosions present. Dx: RA
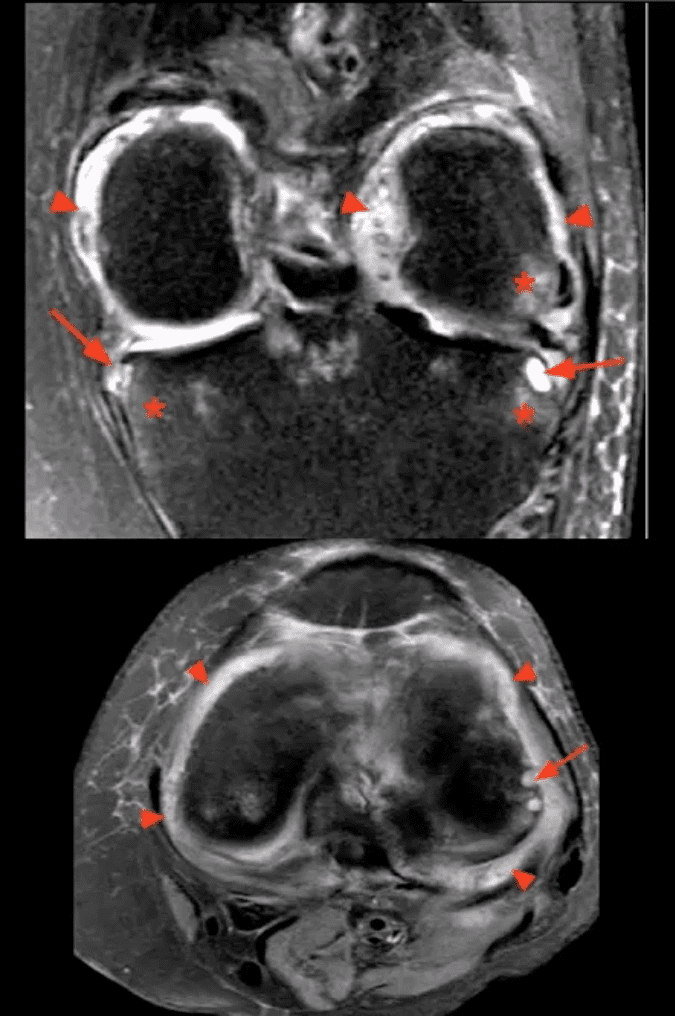
STIR MR Slices
Note: STIR MR slices in the axial (above bottom image) and coronal planes (above top image) demonstrate extensive synovitis/effusion (above arrowheads) and multiple erosions in the medial and lateral tibial plateau (above arrows)
Additionally, scattered patchy areas of bone marrow edema are noted (above asterisks) such marrow edema changes are indicative and predictive of future osseous erosions.
Additional features: note thinning and destruction of joint cartilage
Knee pain is a common health issue among athletes and the general population alike. Although symptoms of knee pain can be debilitating and frustrating, knee pain is often a very treatable health issue. The knee is a complex structure made up of three bones: the lower section of the thighbone, the upper region of the shinbone, and the kneecap.
Powerful soft tissues, such as the tendons and ligaments of the knee as well as the cartilage beneath the kneecap and between the bones, hold these structures together in order to stabilize and support the knee. However, a variety of injuries and/or conditions can ultimately lead to knee pain. The purpose of the article below is to evaluate patients with knee pain.
Abstract
Family physicians frequently encounter patients with knee pain. Accurate diagnosis requires a knowledge of knee anatomy, common pain patterns in knee injuries, and features of frequently encountered causes of knee pain, as well as specific physical examination skills. The history should include characteristics of the patient�s pain, mechanical symptoms (locking, popping, giving way), joint effusion (timing, amount, recurrence), and mechanism of injury. The physical examination should include careful inspection of the knee, palpation for point tenderness, assessment of joint effusion, range-of-motion testing, evaluation of ligaments for injury or laxity, and assessment of the menisci. Radiographs should be obtained in patients with isolated patellar tenderness or tenderness at the head of the fibula, inability to bear weight or flex the knee to 90 degrees, or age greater than 55 years. (Am Fam Physician 2003; 68:907-12. Copyright� 2003 American Academy of Family Physicians.)
Introduction
Knee pain accounts for approximately one-third of musculoskeletal problems seen in primary care settings. This complaint is most prevalent in�physically active patients, with as many as 54 percent of athletes having some degree of knee pain each year.1 Knee pain can be a source of significant disability, restricting the ability to work or perform activities of daily living.
The knee is a complex structure (Figure 1),2 and its evaluation can present a challenge to the family physician. The differential diagnosis of knee pain is extensive but can be narrowed with a detailed history, a focused physical examination and, when indicated, the selective use of appropriate imaging and laboratory studies. Part I of this two-part article provides a systematic approach to evaluating the knee, and part II3 discusses the differential diagnosis of knee pain.
History
Pain Characteristics
The patient�s description of knee pain is helpful in focusing the differential diagnosis.4 It is important to clarify the characteristics of the pain, including its onset (rapid or insidious), location (anterior, medial, lateral, or posterior knee), duration, severity, and quality (e.g., dull, sharp, achy). Aggravating and alleviating factors also need to be identified. If knee pain is caused by an acute injury, the physician needs to know whether the patient was able to continue activity or bear weight after the injury or was forced to cease activities immediately.
Mechanical Symptoms
The patient should be asked about mechan- ical symptoms, such as locking, popping, or giving way of the knee. A history of locking episodes suggests a meniscal tear. A sensation of popping at the time of injury suggests liga- mentous injury, probably complete rupture of a ligament (third-degree tear). Episodes of giving way are consistent with some degree of knee instability and may indicate patellar sub- luxation or ligamentous rupture.
Effusion
The timing and amount of joint effusion are important clues to the diagnosis. Rapid onset (within two hours) of a large, tense effusion suggests rupture of the anterior cru- ciate ligament or fracture of the tibial plateau with resultant hemarthrosis, whereas slower onset (24 to 36 hours) of a mild to moderate effusion is consistent with meniscal injury or ligamentous sprain. Recurrent knee effusion after activity is consistent with meniscal injury.
Mechanism of Injury
The patient should be questioned about specific details of the injury. It is important to know if the patient sustained a direct blow to the knee, if the foot was planted at the time of injury, if the patient was decelerating or stopping suddenly, if the patient was landing from a jump, if there was a twisting component to the injury, and if hyperextension occurred.
A direct blow to the knee can cause serious injury. The anterior force applied to the proximal tibia with the knee in flexion (e.g., when the knee hits the dashboard in an automobile accident) can cause injury to the posterior cruciate ligament. The medial collateral ligament is most commonly injured as a result of direct lateral force to the knee (e.g., clipping in football); this force creates a val- gus load on the knee joint and can result in rupture of the medial collateral ligament. Conversely, a medial blow that creates a varus load can injure the lateral collateral ligament.
Noncontact forces also are an important cause of knee injury. Quick stops and sharp cuts or turns create significant deceleration forces that can sprain or rupture the anterior cruciate ligament. Hyperextension can result in injury to the anterior cruciate ligament or posterior cruciate ligament. Sudden twisting or pivoting motions create shear forces that can injure the meniscus. A combination of forces can occur simultaneously, causing injury to multiple structures.
Medical History
A history of knee injury or surgery is important. The patient should be asked about previous attempts to treat knee pain, including the use of medications, supporting devices, and physical therapy. The physician also should ask if the patient has a history of�gout, pseudogout, rheumatoid arthritis, or other degenerative joint diseases.
Knee pain is a common health issue which can be caused by sports injuries, automobile accident injuries, or by an underlying health issue, such as arthritis. The most common symptoms of knee injury include pain and discomfort, swelling, inflammation and stiffness. Because treatment for knee pain varies according to the cause, it’s essential for the individual to receive proper diagnosis for their symptoms. Chiropractic care is a safe and effective, alternative treatment approach which can help treat knee pain, among other health issues.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
Physical Examination
Inspection and Palpation
The physician begins by comparing the painful knee with the asymptomatic knee and inspecting the injured knee for erythema, swelling, bruising, and discoloration. The mus- culature should be symmetric bilaterally. In particular, the vastus medialis obliquus of the quadriceps should be evaluated to determine if it appears normal or shows signs of atrophy.
The knee is then palpated and checked for pain, warmth, and effusion. Point tenderness should be sought, particularly at the patella, tibial tubercle, patellar tendon, quadriceps tendon, anterolateral and anteromedial joint line, medial joint line, and lateral joint line. Moving the patient�s knee through a short arc of motion helps identify the joint lines. Range of motion should be assessed by extending and flexing the knee as far as possible (normal range of motion: extension, zero degrees; flex- ion, 135 degrees).5
Patellofemoral Assessment
An evaluation for effusion should be conducted with the patient supine and the injured knee in extension. The suprapatellar pouch should be milked to determine whether an effusion is present.
Patellofemoral tracking is assessed by observing the patella for smooth motion while the patient contracts the quadriceps muscle. The presence of crepitus should be noted during palpation of the patella.
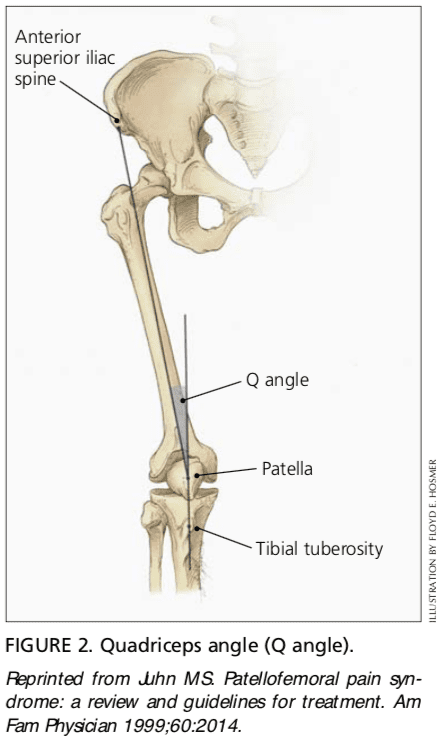
The quadriceps angle (Q angle) is determined by drawing one line from the anterior superior iliac spine through the center of the patella and a second line from the center of the patella through the tibial tuberosity (Figure 2).6 A Q angle greater than 15 degrees is a predisposing factor for patellar subluxation (i.e., if the Q angle is increased, forceful contraction of the quadriceps muscle can cause the patella to sublux laterally).
A patellar apprehension test is then performed. With fingers placed at the medial aspect of the patella, the physician attempts to sublux the patella laterally. If this maneuver reproduces the patient�s pain or a giving-way sensation, patellar subluxation is the likely cause of the patient�s symptoms.7 Both the superior and inferior patellar facets should be palpated, with the patella subluxed first medially and then laterally.
Cruciate Ligaments
Anterior Cruciate Ligament. For the anterior drawer test, the patient assumes a supine position with the injured knee flexed to 90 degrees. The physician fixes the patient�s foot in slight external rotation (by sitting on the foot) and then places thumbs at the tibial tubercle and fingers at the posterior calf. With the patient�s hamstring muscles relaxed, the physician pulls anteriorly and assesses anterior displacement of the tibia (anterior drawer sign).
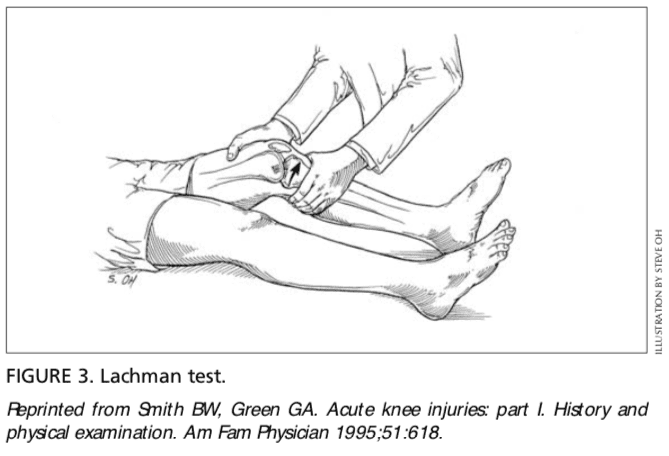
The Lachman test is another means of assessing the integrity of the anterior cruciate ligament (Figure 3).7 The test is performed with the patient in a supine position and the injured knee flexed to 30 degrees. The physician stabilizes the distal femur with one hand, grasps the proximal tibia in the other hand, and then attempts to sublux the tibia anteriorly. Lack of a clear end point indicates a positive Lachman test.
Posterior Cruciate Ligament. For the posterior drawer test, the patient assumes a supine position with knees flexed to 90 degrees. While standing at the side of the examination table, the physician looks for posterior displacement of the tibia (posterior sag sign).7,8 Next, the physician fixes the patient�s foot in neutral rotation (by sitting on the foot), positions thumbs at the tibial tubercle, and places fingers at the posterior calf. The physician then pushes posteriorly and assesses for posterior displacement of the tibia.
Collateral Ligaments
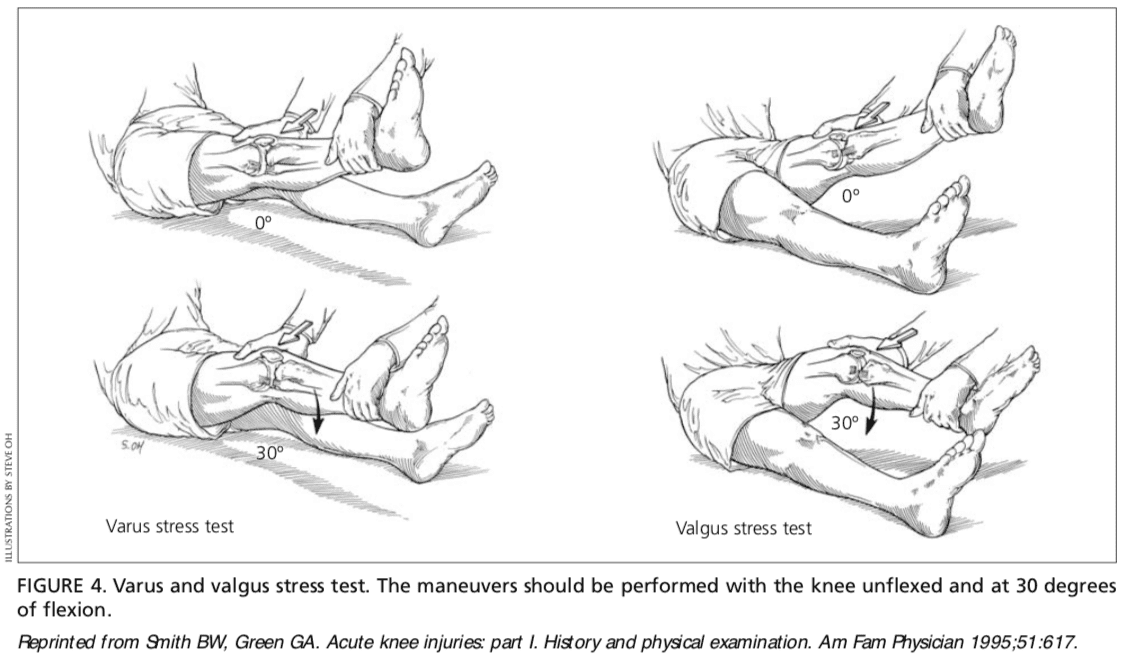
Medial Collateral Ligament. The valgus stress test is performed with the patient�s leg slightly abducted. The physician places one hand at the lateral aspect of the knee joint and the other hand at the medial aspect of the distal tibia. Next, valgus stress is applied to the knee at both zero degrees (full extension) and 30 degrees of flexion (Figure 4)7. With the knee at zero degrees (i.e., in full extension), the posterior cruciate ligament and the articulation of the femoral condyles with the tibial plateau should stabilize the knee; with the knee at 30 degrees of flexion, application of valgus stress assesses the laxity or integrity of the medial collateral ligament.
Lateral Collateral Ligament. To perform the varus stress test, the physician places one hand at the medial aspect of the patient�s knee and the other hand at the lateral aspect of the distal fibula. Next, varus stress is applied to the knee, first at full extension (i.e., zero degrees), then with the knee flexed to 30 degrees (Figure 4).7 A firm end point indicates that the collateral ligament is intact, whereas a soft or absent end point indicates complete rupture (third-degree tear) of the ligament.
Menisci
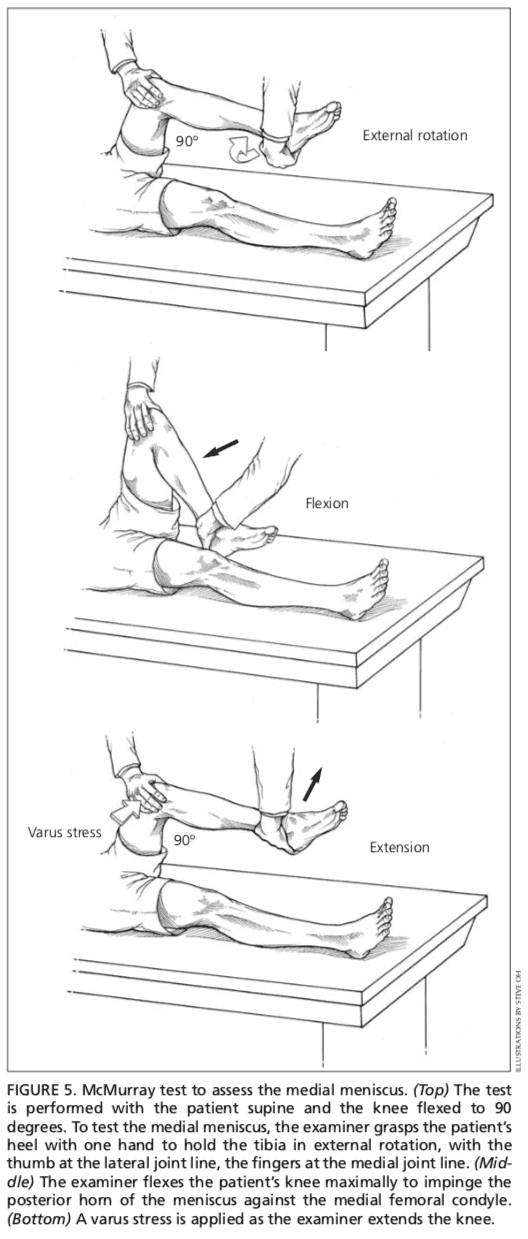
Patients with injury to the menisci usually demonstrate tenderness at the joint line. The McMurray test is performed with the patient lying supine9 (Figure 5). The test has been described variously in the literature, but the author suggests the following technique.
The physician grasps the patient�s heel with one hand and the knee with the other hand. The physician�s thumb is at the lateral joint line, and fingers are at the medial joint line. The physician then flexes the patient�s knee maximally. To test the lateral meniscus, the tibia is rotated internally, and the knee is extended from maximal flexion to about 90 degrees; added compression to the lateral meniscus can be produced by applying valgus stress across the knee joint while the knee is�being extended. To test the medial meniscus, the tibia is rotated externally, and the knee is extended from maximal flexion to about 90 degrees; added compression to the medial meniscus can be produced by placing varus stress across the knee joint while the knee is degrees of flexion. A positive test produces a thud or a click, or causes pain in a reproducible portion of the range of motion.
Because most patients with knee pain have soft tissue injuries, plain-film radiographs generally are not indicated. The Ottawa knee rules are a useful guide for ordering radiographs of the knee10,11.
If radiographs are required, three views are usually sufficient: anteroposterior view, lateral view, and Merchant�s view (for the patellofemoral joint).7,12 Teenage patients who report chronic knee pain and recurrent knee effusion require a notch or tunnel view (posteroanterior view with the knee flexed to 40 to 50 degrees). This view is necessary to detect radiolucencies of the femoral condyles (most�commonly the medial femoral condyle), which indicate the presence of osteochondritis dissecans.13
Radiographs should be closely inspected for signs of fracture, particularly involving the patella, tibial plateau, tibial spines, proximal fibula, and femoral condyles. If osteoarthritis is suspected, standing weight-bearing radiographs should be obtained.
Laboratory Studies
The presence of warmth, exquisite tenderness, painful effusion, and marked pain with even slight range of motion of the knee joint is consistent with septic arthritis or acute inflammatory arthropathy. In addition to obtaining a complete blood count with differential and an erythrocyte sedimentation rate (ESR), arthro- centesis should be performed. The joint fluid should be sent to a laboratory for a cell count with differential, glucose and protein measure- ments, bacterial culture and sensitivity, and polarized light microscopy for crystals.
Because a tense, painful, swollen knee may present an unclear clinical picture, arthrocentesis may be required to differentiate simple effusion from hemarthrosis or occult osteochondral fracture.4 A simple joint effusion produces clear, straw-colored transudative fluid, as in a knee sprain or chronic meniscal injury. Hemarthrosis is caused by a tear of the anterior cruciate ligament, a fracture or, less commonly, an acute tear of the outer portion of the meniscus. An osteochondral fracture causes hemarthrosis, with fat globules noted in the aspirate.
Rheumatoid arthritis may involve the knee joint. Hence, serum ESR and rheumatoid factor testing are indicated in selected patients.
The authors indicate that they do not have any conflicts of interest. Sources of funding: none reported.
In conclusion, knee pain is a common health issue which occurs due to a variety of injuries and/or conditions, such as sports injuries, automobile accidents, and arthritis, among other problems. Treatment of knee pain depends largely on the source of the symptoms. Therefore, it is essential for the individual to seek immediate medical attention to receive a diagnosis.
Chiropractic care is an alternative treatment option which focuses on the treatment of a variety of injuries and/or conditions associated with the musculoskeletal and nervous system. The scope of our information is limited to chiropractic and spinal health issues. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Relieving Knee Pain without Surgery
Knee pain is a well-known symptom which can occur due to a variety of knee injuries and/or conditions, including�sports injuries. The knee is one of the most complex joints in the human body as it is made-up of the intersection of four bones, four ligaments, various tendons, two menisci, and cartilage. According to the American Academy of Family Physicians, the most common causes of knee pain include patellar subluxation, patellar tendinitis or jumper’s knee, and Osgood-Schlatter disease. Although knee pain is most likely to occur in people over 60 years old, knee pain can also occur in children and adolescents. Knee pain can be treated at home following the RICE methods, however, severe knee injuries may require immediate medical attention, including chiropractic care.
1. Rosenblatt RA, Cherkin DC, Schneeweiss R, Hart LG. The content of ambulatory medical care in the United States. An interspecialty comparison. N Engl J Med 1983;309:892-7.
2. Tandeter HB, Shvartzman P, Stevens MA. Acute knee injuries: use of decision rules for selective radiograph ordering. Am Fam Physician 1999;60: 2599-608.
3. Calmbach WL, Hutchens M. Evaluation of patients presenting with knee pain: part II. Differential diag- nosis. Am Fam Physician 2003;68:917-22
4. Bergfeld J, Ireland ML, Wojtys EM, Glaser V. Pin- pointing the cause of acute knee pain. Patient Care 1997;31(18):100-7.
6. Juhn MS. Patellofemoral pain syndrome: a review and guidelines for treatment. Am Fam Physician 1999;60:2012-22.
7. Smith BW, Green GA. Acute knee injuries: part I. History and physical examination. Am Fam Physi- cian 1995;51:615-21.
8. Walsh WM. Knee injuries. In: Mellion MB, Walsh WM, Shelton GL, eds. The team physician�s hand- book. 2d ed. St. Louis: Mosby, 1997:554-78.
9. McMurray TP. The semilunar cartilage. Br J Surg 1942;29:407-14.
10. Stiell IG, Wells GA, Hoag RH, Sivilotti ML, Cacciotti TF, Verbeek PR, et al. Implementation of the Ottawa knee rule for the use of radiography in acute knee injuries. JAMA 1997;278:2075-9.
11. Stiell IG, Greenberg GH, Wells GA, McKnight RD, Cwinn AA, Caciotti T, et al. Derivation of a decision rule for the use of radiography in acute knee injuries. Ann Emerg Med 1995;26:405-13.
12. Sartoris DJ, Resnick D. Plain film radiography: rou- tine and specialized techniques and projections. In: Resnick D, ed. Diagnosis of bone and joint disor- ders. 3d ed. Philadelphia: Saunders:1-40.
13. Schenck RC Jr, Goodnight JM. Osteochondritis dis- secans. J Bone Joint Surg [Am] 1996;78:439-56.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine