Mitochondria are the “energy factory” of the human body. Several thousand mitochondria can be found in nearly every cell. Mitochondria also play several fundamental roles in the body, such as converting chemicals from the foods we eat into energy as well as to process oxygen. Mitochondria produce 90 percent of the energy the human body requires to function accordingly. The purpose of the following article is to describe an overview of mitochondrial disease and well-being. �
What are Mitochondrial Diseases?
Mitochondrial diseases are characterized as chronic, genetic, and often inherited health issues which ultimately occur when mitochondria fail to produce enough energy for the human body to function properly. Mitochondrial diseases may develop from birth however they can frequently develop at any age. Mitochondrial disease can affect any region of the human body, including the cells of the brain, muscles, heart, liver, kidneys, pancreas, eyes, ears, and nerves, among other structures. �
When the mitochondria don’t function as well as they should because of another health issue, mitochondrial dysfunction occurs. Furthermore, many health issues can cause secondary dysfunction and result in other neurological diseases, such as Alzheimer’s disease, Lou Gehrig’s disease, and muscular dystrophy. People with secondary dysfunction don’t have genetic mitochondrial disease and do not need to be concerned about the ongoing development or worsening of symptoms. �
What are the Symptoms of Mitochondrial Disease?
Symptoms of mitochondrial disease depend on which cells of the human body are affected. Symptoms can develop at any age, involve one or more organs, and may range from mild to severe. Even patients within the same household, having the exact same mitochondrial disease can have gaps in symptoms, severity, and age of onset or beginning of symptoms. �
Symptoms of mitochondrial diseases can include: �
Poor growth
Muscle pain, muscle weakness, exercise intolerance, low muscle tone
Vision and/or hearing problems
Learning disabilities, delays in development, mental retardation
In many people, primary mitochondrial disease is a genetic health issue which can be inherited in several ways. To understand inheritance types, it is helpful to find out more about genes and DNA. Genes are substances which provide us our traits, like brown eyes or blue eyes. Genes contain DNA, which is the “blueprint” which gives each person their distinctive make-up. �
In normal circumstances, a child inherits one gene from the father and one gene from the mother. A child with a mitochondrial disease doesn’t receive the pair of genes from the parents. The gene has mutated or has become defective. Learning how the mitochondrial disease is inherited helps predict the prospect of passing the disease(s) to children. �
Inheritance types of mitochondrial disease are: �
Autosomal recessive inheritance: The child receives one mutated copy of a gene from each parent. There is a 25 percent chance that each child in the family will inherit a mitochondrial disease.
Autosomal dominant inheritance: The child receives one mutated copy of a gene from either parent. There is a 50 percent chance that each child in the family will inherit a mitochondrial disease.
Mitochondrial inheritance: In this unique type of inheritance, the mitochondria contain their own DNA. Only mitochondrial disorders caused by mutations in the mitochondrial DNA are exclusively inherited from mothers. There is a 100 percent chance that each child in the family will inherit a mitochondrial disease.
Random mutations: Occasionally, genes develop a mutation of their own which is not inherited from a parent.
How are Mitochondrial Diseases Diagnosed?
Mitochondrial diseases can be difficult to diagnose by a healthcare professional because mitochondrial diseases can ultimately affect a variety of organs and tissues in the human body and patients can also have a variety of symptoms. There is currently no single lab test or diagnostic test which can confirm the identification of mitochondrial disease. That is why a referral to a medical facility with healthcare professionals who focus on these diseases is essential to making the diagnosis. �
Diagnosis begins with a series of evaluations and tests which may include: �
A review of a patient�s family history
A complete physical evaluation
A neurological evaluation
A metabolic evaluation which includes blood and urine tests, and, if needed, a cerebral spinal fluid test
Other evaluations, determined by the regions of the human body and the patient’s symptoms which may include: �
Magnetic resonance imaging (MRI) or spectroscopy (MRS) for neurological symptoms
Retinal exam or electroretinogram (ERG) for vision symptoms
Electrocardiogram (EKG) or echocardiogram for symptoms of heart disease
Audiogram or auditory-brainstem evoked responses (ABER) for hearing symptoms
Blood test to detect thyroid dysfunction if the patient has thyroid problems
Blood test to perform genetic DNA testing
Testing may include biochemical testing. Biopsies of skin and muscle tissue may also be utilized for diagnosis. �
How are Mitochondrial Diseases Treated?
Unfortunately, there is no cure for mitochondrial disease, however, treatment can help reduce symptoms or slow the decline of overall well-being. Treatment varies from patient to patient and depends on the severity and the mitochondrial disease characterized. There is absolutely no way to predict a patient’s reaction or forecast how that person will be affected in the long-term. No two people respond the same way to the same treatment even if they have the same mitochondrial disease. �
Treatments for mitochondrial disease may include: �
Vitamins and supplements, including Coenzyme Q10; B complex vitamins, such as thiamine (B1) and riboflavin (B2), Alpha lipoic acid, L-carnitine (Carnitor), Creatine, and L-Arginine.
Exercise and physical activity, including endurance exercises and resistance/strength training to increase muscle strength. Endurance exercises include walking, running, swimming, dancing, cycling and others. Resistance/strength training includes exercises such as sit-ups, arm curls, knee extensions, weight lifting and others.
Conserving energy. Don�t try to do too much in a short period of time. Pace yourself.
Other treatments including speech therapy, respiratory therapy, physical therapy, and chiropractic care, among others.
Avoid situations which can make the health issue worse. This includes exposure to cold and/or warmth, starvation, lack of sleep, stressful situations, and usage of alcohol, smokes and monosodium glutamate or MSG, a flavor enhancer commonly added to Chinese foods, canned vegetables, soups, as well as processed meats, among other processed foods. �
Mitochondrial diseases are long-term, genetic, and frequently inherited health issues which occur when the mitochondria fail to produce enough energy for the human body to function accordingly. According to research studies, approximately one in 5,000 people has a genetic mitochondrial disease. Chiropractic care is an alternative treatment option which can help relieve symptoms associated with a variety of health issues, including mitochondrial diseases. Many chiropractors are qualified and experienced in the treatment of neurological diseases. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
The purpose of the article above is to describe mitochondrial disease and its effect on overall health and wellness. Neurological diseases are associated with the brain, the spine, and the nerves. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
Cerebrovascular disease is characterized as a group of diseases, conditions, and disorders which ultimately affects the blood vessels and the blood supply to the human brain. Brain damage can occur when a blockage, malformation, or hemorrhage prevents the brain cells from receiving enough oxygen. Cerebrovascular disorders can include stroke, transient ischemic attack or TIA, aneurysm, and vascular malformation. �
Cerebrovascular disease can develop due to a variety of health issues, such as atherosclerosis, where the arteries become narrow; thrombosis or embolic arterial blood clot, which is a blood clot in an artery of the brain; or cerebral venous thrombosis, which is a blood clot in a vein of the brain. �
In the United States, cerebrovascular disease is one of the most common causes of death. In 2017, it caused about 44.9 deaths per 100,000 individuals or 146,383 deaths in total. Fortunately, people can decrease their risk of developing cerebrovascular disease. In the following article, we will describe the types, the symptoms, the diagnosis, and the treatment for cerebrovascular disease and how to prevent them. �
Cerebrovascular Disease Symptoms
The symptoms of cerebrovascular disease are commonly based on the region of the health issue and its effect on the brain. � Different types of cerebrovascular disease may have different symptoms, however, common symptoms can include: �
a severe and sudden headache
hemiplegia or paralysis on one side of the human body
weakness on one side, also known as hemiparesis
confusion
difficulty communicating, including slurred speech
losing vision on one side
loss of balance
becoming unconscious
Emergency Response
The American Stroke Association promotes the public knowledge of the F.A.S.T. acronym as a way to help people recognize the warning signs of a stroke or any other type of cerebrovascular disease to take action immediately, including: �
face drooping
arm weakness
speech difficulty
time to call 911
Immediate medical attention is fundamental if anyone demonstrates symptoms of a cerebrovascular disease attack because these may ultimately have long-term effects if not treated immediately, such as cognitive impairment and paralysis. �
Types of Cerebrovascular Disease
Stroke, TIA, and subarachnoid hemorrhage are several types of cerebrovascular disease. Aneurysms and hemorrhages may cause acute health issues. Blood clots can affect the brain directly or indirectly from other regions of the human body.
Ischemic Stroke
Ischemic strokes occur when a blood clot or atherosclerotic plaque blocks a blood vessel which supplies blood to the brain. A clot or thrombus may develop in a narrow artery. A stroke occurs when a blood supply deficiency causes brain cell death.
Embolism
An embolic stroke is the most common type of ischemic stroke. An embolism occurs when a clot breaks off from another region in the human body and travels to the brain and blocks a smaller artery. People who have arrhythmias, which are health issues associated with irregular heart rhythm, are more vulnerable to developing an embolism as well as other health issues. �
A tear in the lining of the carotid artery, which is found in the neck, can ultimately cause an ischemic stroke. The tear allows blood circulation to flow between the layers of the artery, reducing blood flow to the brain, and causing it to become narrow. �
Hemorrhagic Stroke
Hemorrhagic strokes occur when a blood vessel in part of the brain weakens and pops open, causing blood to flow into the brain. The leaking blood puts pressure on the brain tissue, causing edema, which can ultimately damage brain tissue. The hemorrhage may cause parts of the brain to lose their supply of oxygen-rich blood, causing a variety of other health issues. �
Cerebral Aneurysm or Subarachnoid Hemorrhage
A cerebral aneurysm or subarachnoid hemorrhage can occur due to structural health issues associated with the blood vessels of the brain. An aneurysm is a bulge which in the arterial wall which may rupture and bleed. A subarachnoid hemorrhage occurs when a blood vessel ruptures and bleeds between two membranes in the brain, damaging brain cells. �
Cerebrovascular Disease Causes
Cerebrovascular disease develops due to a variety of factors. If damage occurs to a blood vessel in the brain, it won’t be able to deliver enough or any blood to the necessary region of the brain. The deficiency of blood can affect the delivery of oxygen and brain cells can begin to die. Brain damage is irreversible. �
Immediate medical attention is fundamental to decrease a person’s risk of long-term brain damage and increase their chances of survival. Atherosclerosis is a key cause of cerebrovascular disease. This occurs when cholesterol levels, as well as inflammation in the brain’s arteries, cause cholesterol to build-up. This plaque may restrict or completely obstruct blood circulation into the brain, causing a cerebrovascular disease attack, including a stroke or TIA. �
Risk Factors
Stroke is the most common type of cerebrovascular disease. The risk of stroke increases with age, especially if a person or their close relatives have previously had a cerebrovascular disease attack. The risk doubles every 10 years, between 55 and 85 years of age. However, a stroke can occur at any age, even during infancy. � Factors which increase the risk of stroke and other types of cerebrovascular disease include: �
hypertension, which the American College of Cardiology defines as blood pressure of 130/80 mm Hg or higher
smoking
obesity
poor diet and lack of exercise
diabetes
blood cholesterol levels of 240 milligrams per deciliter (mg/dl) or higher
The same factors can increase a person’s risk of developing a cerebral aneurysm. However, people with a congenital anomaly or previous head trauma may also be at risk of developing a cerebral aneurysm. Pregnancy can also increase the risk of developing cerebral venous thrombosis which is a blood clot affecting a vein in the human brain. � Other risk factors of cerebrovascular disease include: �
Moyamoya disease, a progressive condition which causes a blockage of the cerebral arteries and their major branches
venous angiomas, which affect around 2 percent of the U.S. population and rarely bleed or cause symptoms
a vein of Galen malformation, an arterial disorder which develops in a fetus during pregnancy
Certain drugs and/or medication, as well as other health issues, can make the blood more likely to clot and also increase the risk of ischemic stroke. Hormone replacement therapy or HRT may also increase the risk of a cerebrovascular disease attack in people who currently have atherosclerosis or carotid artery disease, among other health issues. �
Cerebrovascular Disease Diagnosis
Any cerebrovascular disease can be considered a medical emergency and anybody who recognizes the symptoms must contact 911 for support and evaluation. Early diagnosis is fundamental to reduce brain damage. In the clinic, a doctor will ask about the person’s medical history and search for specific neurological, motor, and sensory health issues, including: �
changes in vision or visual fields
reduced or altered reflexes
abnormal eye movements
muscle weakness
decreased sensation
A doctor may also utilize a cerebral angiography, vertebral angiogram, or carotid angiogram to identify a vascular abnormality, such as a blood clot or a blood vessel health issue. These include injecting dye to demonstrate any clots as well as their size and form on MRI or CT imaging. �
A CAT scan will also help a doctor diagnose hemorrhagic strokes as it can distinguish between blood, bone, and brain tissue. However, it does not reveal damage from an ischemic stroke in the first phases. An MRI scan may detect early-stage strokes. An electrocardiogram (EKG or ECG) may diagnose cardiac arrhythmia which is a risk factor for embolic strokes. �
Cerebrovascular Disease Treatment
A cerebrovascular disease requires emergency treatment. Rapid diagnosis and treatment are crucial because a person must receive stroke drugs and/or medications from the beginning of their symptoms. In the case of an acute stroke, the emergency group may administer a medicine known as tissue plasminogen activator (tPA) which breaks up the blood clot. �
A neurosurgeon must evaluate a person who has had a brain hemorrhage. They may perform surgery to decrease the pressure which bleeding causes in the brain. A carotid endarterectomy involves making an incision in the carotid artery and removing the plaque. This allows blood to flow again. The surgeon then repairs the artery with sutures or a graft. �
Several patients may need carotid angioplasty and stenting which involves a doctor inserting a balloon-tipped catheter into the artery so that the artery reopens when they inflate the balloon. Then, the doctor matches a slim, metal mesh tube, or stent, within the carotid artery to improve blood flow in the formerly blocked artery. The stent helps to prevent the artery from closing-up or collapsing following the procedure.
Cerebrovascular Disease Rehabilitation
Because a cerebrovascular disease attack can cause irreversible brain damage, people can experience temporary or permanent disability. For this reason, they may require a variety of supportive and rehabilitative treatments so that they can keep as much function as possible. These may ultimately include: �
Physical therapy: The goal is to restore mobility, flexibility, and upper and/or lower extremity function.
Speech therapy: This helps improve communication and regain speech after a stroke or cerebrovascular disease attack.
Occupational therapy: This can help access facilities which support a return to work and daily life.
Psychological therapy: Physical disability can create unexpected emotional demands and often requires intensive readjustment. A person may benefit from visiting a psychiatrist, psychologist, or counselor after experiencing a cerebrovascular disease attack if they feel overwhelmed.
Cerebrovascular Disease Prevention
Techniques and methods which can ultimately help reduce the risk of cerebrovascular disease include: �
no smoking
getting at least 150 minutes of moderate to intense exercise and/or physical activity every week
eating a balanced diet which supports vascular health, such as the DASH diet
maintaining a healthy body weight
managing blood cholesterol and blood pressure with diet as well as drugs and/or medications, if necessary
People with heart arrhythmia should seek immediate medical attention from a healthcare professional and discuss whether they should be taking a blood thinner to prevent strokes. �
Stroke and other cerebrovascular diseases may lead to death but with immediate medical attention, a partial or full recovery is possible. Patients with cerebrovascular disease should follow their healthcare professional’s instructions and lifestyle modifications to ultimately help decrease the prospect of a cardiovascular disease attack. �
Decreasing the Risk of Stroke
Taking blood platelet inhibitors, including, Dipyridamole, Ticlopidine, and clopidogrel, can decrease the chance of stroke before it occurs. These can help prevent stroke in people who have a medical history or higher prospect of experiencing a cerebrovascular disease attack. �
Doctors recommended people to take a daily dose of aspirin to decrease the chance of a heart attack or stroke. However, current guidelines recommend people to take aspirin only if they’re at risk of experiencing cardiovascular disease because aspirin increases the risk of bleeding. � Doctors prescribe statins to manage high cholesterol levels and reduce the risk of ischemic stroke and heart attack. �
As previously mentioned above, cerebrovascular disease is identified as a group of diseases, conditions, and disorders which affects the blood vessels and the blood flow supply to the human brain. There are several types of cerebrovascular diseases and their diagnosis and treatment depends on the type and severity. Prompt treatment and lifestyle modifications can improve the outlook of a patient with cerebrovascular disease. Chiropractors are qualified and experienced to help patients with cerebrovascular disease recover from their symptoms. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
The purpose of the article above is to describe cerebrovascular disease and its effect on overall health and wellness. Neurological diseases are associated with the brain, the spine, and the nerves. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
Cerebral perfusion pressure, or CPP, is the net pressure gradient which carries oxygen to brain tissue. It is measured by the difference between the mean arterial pressure, or MAP, and the Intracranial Pressure, or ICP,� which is measured in millimeters of mercury (mm Hg). Regulating CPP is fundamental in the treatment of patients with intracranial pathology, including shock, hemodynamic distress, and traumatic brain injury. �
Although the average CPP is generally between 60 and 80 mm Hg, these values may change to the left or to the right depending on individual physiology. MAP and ICP has to be measured together because CPP is a calculated measure. Regulating CPP at hemodynamically unstable conditions with abnormal ICP or in cases of intracranial pathology will reduce the chance of ischemic brain injury. �
CPP = MAP – ICP
Cerebral Perfusion Pressure Physiology
CPP and ICP
At its own average range of 60 to 80 mm Hg, the CPP is determined by the ICP and the mean arterial pressure. Under regular standards, the ICP is between 5 and 10 mm Hg which has a reduced effect on the CPP than the MAP in clinical circumstances not associated with intracranial pathology. ICP is generally measured through intracranial pressure transduction.
Physiologically, the ICP is a function of intracranial compliance. Intracranial compliance is the relationship between the ICP and the volume of the intracranial cavity including cerebrospinal fluid, or CSF, brain tissue as well as arterial and venous blood volume. Because the skull is a fixed and rigid anatomic space, the ICP can increase if the intracranial volume increases while intracranial compliance decreases. As the ICP increases or intracranial compliance decreases, CPP also decreases. �
Several processes determine that ICP continues to stay within the average range for the longest extended period of time possible, especially throughout periods of affected intracranial volume and compliance. As volume adds to the intracranial space, CSF can shift into the spinal subarachnoid space, causing the ICP to continue significantly unchanged. As volume increases due to a growing space-occupying lesion, brain tissue edema or blood, this process ultimately becomes overwhelming, and ICP begins to increase substantially. �
Cerebral blood flow, or CBF, is also a fundamental factor in ICP homeostasis. Cerebral auto-regulation makes sure that steady blood flow is maintained in the brain over a wide range of physiologic alterations. When blood pressure decreases, auto-regulation causes cerebral vasodilation and an increase in CBF and cerebral blood volume, maintaining ICP and CPP. However, when blood pressure increases, auto-regulation causes cerebral vasoconstriction and a decrease in CBF with a decrease in cerebral blood volume, also regulating ICP and CPP. Too many changes outside of average CBF ranges can cause brain ischemia and injury. �
CPP and MAP
Because ICP in its average ranges is a considerably small number, the CPP generally depends on the mean arterial pressure. MAP is the normal blood pressure during one cardiac cycle which can be measured through invasive hemodynamic monitoring or calculated by the systolic blood pressure, plus two times the diastolic blood pressure, divided by three. The average range of MAP is 70 to 100 mm Hg. �
The average arterial pressure can be affected due to everyday activities, such as rest, stress, and exercise or physical activities. However, if the ICP continues to stay the same, the average arterial pressure can change across its significantly wide range without tremendously decreasing or increasing the CPP. As a matter of fact, CPP and CBF will continue to stay considerably unchanged across a wider range of MAP (50 � 150 mm Hg) than normal due to cerebral auto-regulation and vasoconstriction or vasodilation of cerebral vasculature. �
For patients with hypertension, the auto-regulation setpoint changes, decreasing the average arterial pressure associated with the patient�s normal arterial pressure, which causes vasodilation to increase CBF. Patients with lower than normal average arterial pressure at baseline will have auto-regulatory vasoconstriction as a reaction to an increase in their significant average MAP, to return CBF to baseline. When looking at CBF and CPP in the context of the patient�s average MAP, it is clinically significant based on the regulation of intracranial pathology and hemodynamic derangements. �
Cerebral Perfusion Pressure Complications
Diagnosing and treating cerebral perfusion pressure complications necessitates measuring both the ICP and the MAP. The MAP may be quantified through the utilization of invasive hemodynamic processes, most frequently cannulation of a peripheral artery such as the radial or femoral artery. The MAP may also be measured with a non-invasive blood pressure cuff by applying the formula mentioned above utilizing the systolic and diastolic blood pressures. � Intracranial pressure is generally measured through an intracranial pressure transduction device. The most common and most accurate method or technique is utilizing an intraventricular monitor. The intraventricular dimension of ICP is the normal standard. An intraventricular catheter is inserted into a hole drilled in the skull and into the lateral ventricle to gauge the pressure of the CSF. The benefit of an intraventricular catheter is that CSF could be eliminated, if needed, to decrease ICP. Considerable complications for the ICP include a possibility of bleeding, infection, and difficulty with proper placement. Options include sub-dural and intra-parenchymal monitors. �
The ICP can be measured non-invasively through several methods and techniques, including transcranial Doppler ultrasonography or TCD. TCD utilizes a temporal window to evaluate the speed of blood flow through the middle cerebral artery. Systolic and diastolic average flow velocity is utilized to determine a pulsatility index. The pulsatility index was determined to be closely associated with ICP in several research studies as well as be associated with ICP in other research studies. Therefore, it is not suggested to use TCD as a substitute for direct ICP dimension. Invasive diagnosis and treatment of the MAP through an arterial cannula and the ICP through an intraventricular catheter will give a continuous and accurate calculation of CPP. �
Cerebral Perfusion Pressure Clinical Significance
Two general types of pathologic health issues can ultimately occur where the regulation of the CPP is fundamental, such as intracranial pathology, where ICP regulation is essential and hemodynamic instability/shock where MAP regulation is the most essential. Intracranial pathology involves space-occupying lesions, such as tumors, epidural and subdural hematoma or severe intraparenchymal hemorrhage and cerebral edema as seen after ischemic injury, traumatic brain injury or acute hepatic encephalopathy. In these circumstances, average CPP depends on decreasing the ICP into a normal range as soon as possible while regulating the MAP. When CPP is normal, it’s fundamental to keep in mind that every individual’s brain tissue has a CPP that is “normal” in the context of that individual patient’s physiology, which may be affected by other health issues, such as hypertension or cardiovascular disease. Moving towards a more dynamic direction of the average CPP utilizing the patient’s personal auto-regulatory capacity. These diagnosis and treatment approaches involve more frequent and sophisticated monitoring and might not be readily available for widespread utilization. �
In the instance of considerable traumatic brain injury, significant cerebral edema can decrease intracranial compliance and CSF, developing an increased ICP or intracranial hypertension. Auto-regulatory mechanisms and techniques may or may not function normally and when ICP continues to be elevated, CPP will decrease causing further injury through an ischemic process. In circumstances such as these, together with starting the measures for decreasing the ICP, it is essential to prevent hypotension (MAP – ICP = CPP) and in some instances, allowing hypertension to reasonably occur. �
In circumstances of instability, the ICP is considerably stable as cerebral auto-regulation is undamaged. In the instance of hypotension, the MAP decreases due to blood loss, or hemorrhagic shock, intravascular leak, or distributive shock, and decreased cardiac output, or cardiogenic shock, and the CPP also decreases. It’s the association between MAP and CPP which carries resuscitation guidelines to recommend regulating a MAP greater than or equal to 65 mm Hg. With a normal ICP, this threshold must make sure that a CPP of 55 to 60, the minimum necessary to stop cerebral ischemic injury, is ultimately maintained. As in the circumstance of ICP and cerebral auto-regulation, the goal of MAP is to be within the context of an individual patient’s evaluation hemodynamic function. Patients with untreated hypertension must have increased MAP goals to maintain proper CBF and CPP. �
As previously mentioned in the following article, cerebral perfusion pressure, or CPP, is the net pressure gradient which affects cerebral blood flow to the brain, also known as brain perfusion. According to healthcare professionals, the CPP, or cerebral perfusion pressure, must be constantly regulated within a specific limit because too little pressure or too much pressure could potentially cause a variety of brain health issues. Cerebral perfusion pressure may be associated with a variety of neurological diseases. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
The purpose of the article is to discuss cerebral perfusion pressure and its association with neurodegenerative diseases. Neurological diseases are associated with the brain, the spine, and the nerves. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
You have probably heard about the “gray matter” of the brain which is made up of cells known as neurons, however, a lesser-known type of brain cell is ultimately what makes up the “white matter” of the brain.� These are known as glial cells. �
Glial cells, also known as glia or neuroglia, were only considered to simply offer structural support. The term “glia” literally translates to “neural adhesive.” However, relatively recent research studies have demonstrated that they play a variety of roles in the brain and the nerves which run throughout the entire human body. However, there is more left to find out. �
Types of Glial Cells
Glial cells commonly offer support to the neurons. Without them, several of the most fundamental roles would never be achieved although they may not perform these roles themselves. Glial cells come in numerous forms, each of which performs certain functions to keep the brain functioning properly or not, in case of a neurological disease which affects the glial cells. �
The central nervous system, or CNS, is made up of the brain, the spinal cord, and the nerves. Five types of glial cells include: �
Astrocytes
Oligodendrocytes
Microglia
Ependymal cells
Radial glia
Moreover, there are also glial cells on the peripheral nervous system, or PNS, which is made up of the nerves in the upper and lower extremities, away from the spine. The two types of glial cells found in the peripheral nervous system include: �
Schwann cells
Satellite cells
� �
Astrocytes
The most common type of glial cell in the central nervous system is the astrocyte, also known as astroglia. The “astro” part of the name refers to how they look like stars with projections coming out all over the glial cell. Protoplasmic astrocytes have thick projections with lots of branches. Fibrous astrocytes have long, slender arms. The fibrous ones are found in the white matter while others are found among neurons in the gray matter.� Astrocytes play several major roles, including: �
Developing the blood-brain barrier or BBB. The BBB is similar to a strict security system which only allows substances which are supposed to be in the brain. This filtering system is essential for maintaining brain health.
Regulating the substances around neurons. Neurons communicate utilizing chemical messengers known as neurotransmitters. Once a chemical has transmitted a message to a cell, it essentially stays there cluttering things up until an astrocyte recycles it through a process known as reuptake. The reuptake process is generally the main target of numerous medications, including anti-depressants. Astrocytes also clean up what’s left behind when a neuron dies, as well as excess potassium ions, which are chemicals that play a fundamental role in nerve function.
Regulating blood flow to the brain. For the brain to process information accordingly, it needs a certain amount of blood to flow throughout all of its different regions. An active region receives more blood flow than an inactive one.
Synchronizing the activity of axons. Axons are characterized as long, thread-like elements of the neurons and the nerve cells which ultimately conduct electricity to help transmit messages from one cell to another.
Astrocyte dysfunction has been potentially connected to a wide variety of neurological diseases, including: �
Amyotrophic lateral sclerosis (ALS or Lou Gehrig’s disease)
Huntington’s chorea
Parkinson’s disease
Animal models of astrocyte-related disorders are helping researchers learn more about these neurological diseases. �
Oligodendrocytes
Oligodendrocytes develop from stem cells. The term is made up of Greek words which, all together, mean “cells with several branches.” Their main role is to help information move faster. Oligodendrocytes appear like white spikey balls. Their purpose is to make a protective layer, similar to the plastic insulation on electric wires. This layer is known as the myelin sheath. �
The myelin sheath is not constant. There is a gap between each membrane which is known as the”node of Ranvier,” and it is the node which helps electrical signals move effectively along neural cells. The signal is transmitted from one node to the next, which increases the velocity of the nerve conduction whilst also reducing how much energy it takes to transmit it. �
Messages along myelinated nerves may travel as fast as 200 miles per second. At birth, you only have a few myelinated axons, and the quantity of these keeps growing until you’re about 25 to 30 years old. Myelination is thought to play an important role in intelligence. Oligodendrocytes also supply stability and transmit energy from blood cells into the axons. �
The expression “myelin sheath” may be familiar to you because of its association with multiple sclerosis. In multiple sclerosis, it is believed that the human body’s immune system attacks the myelin sheaths, which leads to the breakdown of these neurons and ultimately causes impaired brain functioning. Spinal cord injuries may also cause damage to these structures. � Other neurological diseases believed to be associated with oligodendrocyte dysfunction include: �
Leukodystrophies
Tumors known as oligodendrogliomas
Schizophrenia
Bipolar disorder
Several research studies suggest that oligodendrocytes may become affected by the neurotransmitter glutamate, which, among other functions, stimulates regions of the brain so that you’re able to focus and learn new information. Nonetheless, in high levels, glutamate can be considered an “excitotoxin,” which means that it may overstimulate cells until they die. �
Microglia
Microglia are tiny glial cells. They act as the brain’s dedicated immune system, which is necessary since the BBB isolates the brain from the rest of the human body. Microglia are attentive to indications of disease and injury. If they find a problem, they are in charge of taking care of it, even if it ultimately means clearing away dead cells or getting rid of a toxin or pathogen. �
If they respond to an injury, microglia cause inflammation as part of the recovery process. In some cases, such as in Alzheimer’s disease, they might become hyper-activated and cause too much inflammation. That is thought to cause amyloid plaques and other health issues connected with the neurological disease, among a variety of other brain health issues. � Along with Alzheimer’s disease, other neurological diseases which may be associated with microglial malfunction include: �
Fibromyalgia
Chronic neuropathic pain
Autism spectrum disorders
Schizophrenia
Microglia have been thought to play many fundamental roles beyond that, including learning-associated plasticity and guiding the development of the brain. The brain produces many connections between neurons which allow them to pass information back and forth. The brain produces a lot more of these than we need, which is not always efficient. �
Microglia detect unnecessary synapses and they clean them out. Microglial research has really taken off in recent decades, leading to an ever-increasing comprehension of their roles in both health and disease in the central nervous system. �
Ependymal Cells
Ependymal cells are primarily known for creating a membrane known as the ependyma, and it can be described as a thin membrane lining the central canal of the spinal cord and the ventricles or passageways of the brain. They also create cerebrospinal fluid. Ependymal cells are extremely small and they lineup closely together to make the membrane. �
Inside the ventricles, are the cilia, which look like small hairs which move back and forth to help circulate the cerebrospinal fluid. Cerebrospinal fluid provides nutrients and removes waste products in the brain. Additionally, it serves as a cushion and shock absorber between the skull and the brain. It’s also essential for homeostasis in the brain, regulating its temperature along with other attributes which keep its potential and functioning. Ependymal cells are also included in the BBB. �
Radial Glia
Radial glia are believed to be a type of stem cell, which means that they create other types of cells. In the developing brain, they’re the”parents” of neurons, astrocytes, and oligodendrocytes. They also supply scaffolding for developing neurons, thanks to long fibers which direct young brain cells into position as the brain forms in a human embryo. Their role as stem cells, especially as founders of neurons, is ultimately what makes them the focus of research studies regarding how to repair brain damage from injury or illness. Later in life, the radial glia perform important roles in neuroplasticity as well. �
Schwann Cells
Schwann cells are known after the physiologist Theodor Schwann, who discovered them. They function a lot like oligodendrocytes in which they supply myelin sheaths for axons, but they develop in the peripheral nervous system, or PNS, rather than in the central nervous system or CNS. However, Schwann cells form spirals directly across the axon. �
Ranvier’s nodes are found between the membranes of oligodendrocytes and these help in neural transmission in precisely the same exact way. Schwann cells can also be part of the PNS’s immune system. They ultimately have the ability to consume the axons of the nerve and give a protected path for a brand new axon to develop when another nerve cell is damaged. Neurological diseases involving abnormal Schwann cells include: �
Guillain-Barre’ syndrome
Charcot-Marie-Tooth disorder
Schwannomatosis
Chronic inflammatory demyelinating polyneuropathy
Leprosy
Several research studies on bronchial Schwann cells for spinal cord injury and other types of peripheral nerve damage have been promising. Schwann cells are implicated in certain types of chronic pain. Their activation following nerve damage may contribute to dysfunction in a type of nerve fiber known as nociceptors, which feel external factors like heat and cold. �
Satellite Cells
Satellite cells get their name due to the way they surround certain neurons, with several satellites forming a sheath around the cellular surface. Researchers have only just started to learn about these cells but they’re believed to be similar to astrocytes. The main role of satellite cells is believed to be the regulation of the surroundings around the nerves. �
The nerves which have satellite cells make up something known as ganglia, which are clusters of nerve cells in the autonomic nervous system and sensory apparatus. The autonomic nervous system regulates internal organs, even while the sensory system is what enables people to see, hear, taste, touch, and smell. Satellite cells provide nourishment to the neuron and absorb heavy metal toxins, such as lead and mercury, to stop them from damaging the nerves and other structures. �
They are also believed to assist transport several neurotransmitters and other substances, including: �
Glutamate
GABA
Norepinephrine
Adenosine triphosphate
Substance P
Capsaicin
Acetylcholine
Much like microglia, satellite cells detect and respond to injury and inflammation. However, their role in repairing cell damage isn’t yet fully well understood. Satellite cells have been connected to chronic pain between peripheral tissue injury, nerve damage, and a systemic heightening of pain, or hyperalgesia, which can ultimately result from chemotherapy. �
Glial cells, also known as glia or neuroglia, are characterized as non-neuronal cells which are ultimately found in the central nervous system, or CNS, and the peripheral nervous system, or PNS. There are various types of glial cells, including astrocytes, oligodendrocytes, microglia, ependymal cells, and radial glia in the CNS and Schwann cells and satellite cells in the PNS. The glial cells play many fundamental roles in the human nervous system. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
The purpose of the article is to discuss the types of glial cells associated with the brain and neurodegenerative diseases. Neurological diseases are associated with the brain, the spine, and the nerves. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
� For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
Neural cell death can occur both during the development and throughout the pathophysiology of the nervous system. Two different types of cell death, known as necrosis and apoptosis, are involved in pathological neuronal loss, however, apoptosis is the process of programmed cell death during development. All types of cells will go through apoptosis. This mechanism controls neuronal growth where an excess of neurons is produced and only those which form connections with the target structures will receive enough survival factors. The remaining neurons will then ultimately go through death and removal. �
Apoptosis continues throughout life and it is the main process involved in the elimination of surplus, unwanted, damaged or aged cells. Dysregulation of apoptosis is demonstrated after damage or injury as well as in neurodegeneration and in tumorigenesis. Treatment approaches which influence the apoptotic pathway offer valuable therapeutic options in a wide variety of pathological states. The purpose of the article is to describe the significance of apoptosis in neurological diseases. �
What is Apoptosis?
Apoptosis is the well-conserved and highly controlled process of cell death involved in the removal of unnecessary, surplus, aged or damaged cells. Dysregulation of apoptosis can ultimately develop mutated cells which can result in malformations, autoimmune diseases, and even cancer. Abnormal apoptosis can also result in the elimination of healthy cells which can occur in health issues such as infection, hypoxic-ischaemic injury, neurodegenerative or neuromuscular diseases, and AIDS. �
Apoptosis is different from necrotic cell death. In necrosis, cell death is caused by an external factor and involves the early loss of tissue, damage to organs, and the leakage of cytoplasmic contents, leading to the recruitment of phagocytes which can cause an acute inflammatory reaction. In contrast, apoptosis is often considered cell suicide. According to research studies, cells which die due to apoptosis retain membrane and organelle structure and function until late in the process while still developing plasma membrane blebbing, reduced cytoplasmic volume, chromatin condensation, and nuclear fragmentation. �
In the final phases, cell fragments wrapped in plasma membrane pull away as apoptotic bodies which are then phagocytosed by healthy cells. The removal of cell debris also occurs in the absence of an inflammatory response, and this silent, quick, and efficient elimination of apoptotic cells mean that apoptosis can be difficult to find in cells. However, as many as 50 percent of the cells in developing adulthood may go through apoptosis where less than 1 percent of cells are apoptotic at any one time. �
Apoptosis in the Nervous System
Programmed cell death by apoptosis occurs in several developmental processes, such as body sculpting and removal of self-reacting resistant cells as well as sexual organ growth and gamete formation. The general principle of growth in multicellular organisms involves the development of excess numbers of cells, where the excess or unwanted cells are then removed by apoptosis through the development of functional organs. In the developing nervous system, apoptosis has been demonstrated to occur in neural tube formation and continues throughout terminal differentiation of the neural system. �
A growing number of neurotrophic factors, such as nerve growth factor family, including both the neurokines and development factors like insulin-like growth variables (IGF-I and IGF-II), encourage the survival of several types of neurons. Targeted disruption of genes encoding these factors or their receptors demonstrate that neurotrophic factors are significant for the development of specific neuronal populations. Neurotrophic factors function by binding to specific receptors in the cell membrane. Moreover, the effects of NGF offer a good illustration of the subtle command the system permits. �
The nerve growth factor receptor has high and low affinity components. It will function as a survival factor if it binds to the high-affinity trkA receptor but it will also cause apoptosis of retinal neurons or oligodendrocytes once it binds to the low-affinity receptor p75 in the absence of trkA. Nerve growth factor in the extracellular environment is consequently able to control neural development by both boosting the growth of several types of cells as well as the removal of other cells. �
In some cases, however, concentrated genetic disruption of neurotrophic factors or their receptors may leave the central nervous system seemingly unaffected, demonstrating that these variables can ultimately become biased. According to research studies, it has now become evident that the control of neuronal survival does not only depend on the supply of trophic molecules by the targets but also on activity, humoral factors, and trophic support from glia or glial cells. �
Furthermore, neurons don’t simply undergo programmed cell death during differentiation. Apoptosis appears to regulate cell numbers in systems as diverse as the disappearance of the germinal layer during the third trimester of pregnancy, the sexual differentiation of the medial preoptic nucleus where apoptosis is controlled by testosterone, lineages throughout the olfactory epithelium, oligodendrocyte development in the optic nerve, and the development of Schwann cells in the peripheral nervous system. Programmed cell death occurs in a variety of other processes in the developing nervous system. �
Apoptosis in Nervous System Injuries & Diseases
Although apoptosis is a fundamental process involved in the developing nervous system, apoptosis can ultimately be involved in a variety of nervous system injuries and diseases. In most cases, the connection between a specific mutation or trauma as well as the activation of apoptotic cascades remains evasive. An overview of a developing list of neurological diseases in which apoptosis has been implicated as a significant pathological mechanism is provided below. �
Neuronal Injury
Cerebral hypoxic-ischaemic injury is a cause of neurological injury and death. Magnetic resonance spectroscopy studies have demonstrated that transient hypoxia-ischemia contributes to a biphasic disturbance of cerebral energy metabolism. Related to the biphasic energy collapse, two waves of cell death appear to follow hypoxic-ischaemic injury in the developing brain. Immediate neuronal death is most likely due to necrosis resulting from the accumulation of calcium ions. �
Delayed cell death caused by hypoxic-ischemic injury appears to involve further mechanisms with increasing data which demonstrates that in the delayed phase, cell death occurs by apoptosis. The amount of apoptosis is directly associated with the magnitude of ATP depletion during hypoxia-ischemia. Apoptosis can occur in the brains of newborn babies following birth asphyxia and sudden intrauterine death. Apoptosis can also be notable in white matter injury in newborn babies. �
Apoptosis may continue for months after an hypoxic-ischaemic injury due to constant changes in cerebral energy metabolism in infants during the months after birth asphyxia. Following focal neural injury, apoptosis has been discovered in remote regions from the initial damage. After severe spinal cord injury in reptiles, apoptosis of oligodendrocytes occurs in distant degenerating fiber tracts and after forebrain injury in rats, apoptosis was demonstrated in the cerebellum. �
The apoptotic loss of oligodendrocytes could consequently be a potential source of secondary demyelination in paraplegia and in the chronic degeneration related to multiple sclerosis. Further research studies must be performed in order to provide further evidence on the role of apoptosis in this type of injury which begins from the report of which Bcl-2 expression boosts the growth and regeneration of retinal axons. Apoptosis in neuronal injury can be demonstrated in a variety of ways. �
Neural Cancers
A connection between apoptosis and the cell cycle is demonstrated in carcinogenesis where proto-oncogenes, such as c-fos, c-jun, and c-myc, can activate apoptosis and promote cell division while inactivation of the pro-apoptotic p53 tumor suppressor gene is a frequent mark of human neoplasia. By way of instance, in a number of gliomas, the reduction of wild p53 activity was connected to tumor progression, possibly leading to resistance to chemotherapy and radiotherapy. �
Although there have been reports of Bcl-2 overexpression in glioma cell lines, the correlation between the anti-apoptotic effect of this gene and malignancy is not yet clear. However, a homolog of Bcl-2, the brain associated apoptosis gene (BRAG-1), is found predominantly in the brain, and it is upregulated in human gliomas as a rearranged transcript. As demonstrated above, the process of apoptosis can also be significant in the development of neural cancers, according to research studies. �
Infectious Disease
Apoptosis may play a role in HIV encephalopathy. In the brain, the virus reproduces primarily in microglia which it enters through the CD4 receptor. Although the activation of microglia is believed to be the main reason for adrenal loss and demyelination, neurons die by apoptosis in HIV encephalopathies because of HIV mediated alterations in astrocyte function and aberrant stimulation of NMDA receptors or due to nitric oxide from the activation of inducible nitric oxide synthase. �
In subacute sclerosing panencephalitis, widespread apoptotic death was demonstrated to develop in the brain, although no correlation was observed between viral load, lymphocyte infiltration, and the number of apoptotic cells. DNA fragmentation indicative of apoptosis was detected in scrapie-infected sheep and mice brains, suggesting a function associated with cell death in spongiform encephalopathies. Apoptosis may also ultimately be involved in another infectious disease. �
Neurodegeneration
Spinal muscular atrophy is associated with mutations in the survival of motor neuron and neuronal apoptosis inhibitory protein (NAIP) enzymes. NAIP is closely related to the baculovirus inhibitor of apoptosis protein and inhibits apoptosis in many cell types. This implies that mutations in NAIP could deregulate apoptosis in spinal motor nerves, causing their death. Recent studies emphasize the importance of anti-apoptotic genes in cerebral protection which can rescue neurons. �
Apoptosis has also been implicated in retinal dystrophies such as retinitis pigmentosa. In this case, apoptosis results from mutations in the three photoreceptor genes, rhodopsin, peripherin, and the ?-subunit of cyclic guanosine monophosphate di esterase, resulting in photoreceptor degeneration. The absence of c-fos prevents apoptosis in those cells is unknown. Moreover, defined neurotrophins and growth factors injected intraocularly in animal models of retinal degeneration improve photoreceptor survival, suggesting that the apoptotic cascade can be obstructed by supplying exogenous survival signs. �
The mutation underlying Huntington’s disease is an expanded trinucleotide which is fundamental for normal development and can be regarded as a cell survival gene. Transgenic models demonstrated increased apoptosis in the neurons of an embryonic neuroectoderm. During apoptosis, caspase-3 (apopain) is improved by a gain of function associated with the triplet expansion. This is supported by the overexpression of specific trinucleotide repeats in transgenic mice. �
Most cerebellar ataxias are associated with neuronal loss. Ataxia-telangiectasia, caused by mutations in the ATM gene, is considered to have an apoptotic component. ATM shares extensive and significant homology with the DNA dependent protein kinases involved in DNA damage responses at different cell cycle checkpoints and is downregulated in most patients with ataxia-telangiectasia. The simple fact that inappropriate p53 mediated apoptosis is the major cause of death in ataxia-telangiectasia cells suggests that the mutation causes improper triggering of apoptosis by otherwise non-lethal DNA injury. �
From the familial form of amyotrophic lateral sclerosis gain of function, mutations in the gene encoding copper-zinc superoxide dismutase (sod-1) develop a dominant pro-apoptotic sign. Although cell harm by the accumulation of free radicals can trigger apoptosis, these mutants can induce apoptosis both in nerve cells in culture and in transgenic mice. Mental retardation in Down’s syndrome has also been associated with abnormal apoptosis. Although cortical neurons from fetal Down’s syndrome brains are different, they then degenerate and undergo apoptosis, according to research studies. �
Degeneration is blocked by treatment with free radical scavengers, suggesting that a defect in the metabolism of reactive oxygen species is the trigger for apoptosis. In Parkinson’s disease, the death of dopaminergic neurons in the substantia nigra was demonstrated to occur through apoptosis and may be obstructed by delivery of glial-derived neurotrophic factor. Alzheimer’s disease is associated with the progressive accumulation of ?-amyloid protein which is the fundamental component of neural plaques. The ?-amyloid peptide can cause neurons to undergo apoptosis in vitro research studies. �
Inherited Metabolic Disease
Furthermore, few data suggest that the acute encephalopathy associated with maple syrup urine disease is because of the induction of apoptosis by an accumulating metabolite of leucine, ?-keto isocaproic acid. This compound is a potent inducer of apoptosis in central nervous system glial cells and the result is significantly enhanced in the presence of leucine. Phenylalanine and leucine do not induce apoptosis in this system, suggesting that this result is ultimately unique. �
There are two ways in which a cell can die, necrosis and apoptosis. While necrosis occurs due to an external factor which harms the cell, apoptosis follows a controlled, predictable routine. Apoptosis is generally known as programmed cell death. Apoptosis, or programmed cell death, has many fundamental functions in the developing structures of the human body, however, research studies have demonstrated that abnormal apoptosis can be associated with the development of a variety of neurological diseases. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
The purpose of the article above is to discuss the process of apoptosis, or cell death, in neurodegenerative diseases. Neurological diseases are associated with the brain, the spine, and the nerves. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
The human brain is the human body’s control center. It is a fundamental structure in the nervous system, which also includes the spinal cord and a system of nerves and neurons. The nervous system controls every structure and function in the human body. When the brain is damaged, it can ultimately affect the function of the nervous system, including memory, sensation, and even personality. Brain disorders include any health issues which affect the brain. This includes health issues due to: �
genetics
illness
trauma or injury
What are the Different Types of Brain Disorders?
There is a wide array of different brain disorders which can vary tremendously in symptoms and grade of severity. Below, we will demonstrate the different types of brain disorders and discuss several of the most common types of brain disorders. �
Brain Injuries
Brain injuries are generally caused by blunt trauma or injury. Trauma or injury can damage brain tissue, neurons, and nerves. This damage affects the brain’s capacity to communicate with the rest of the human body. Several brain injuries include: �
hematomas
blood clots
contusions or bruising of brain tissue
cerebral edema or swelling inside the skull
concussions
strokes
Common symptoms of brain injuries include: �
vomiting
nausea
speech difficulty
bleeding from the ear
numbness
paralysis
memory loss
problems with concentration
Furthermore, other common symptoms you may develop include: �
high blood pressure
low heart rate
pupil dilation
irregular breathing
Depending on the type of brain injury, treatment may include medication, rehabilitation, or brain surgery. Approximately half of the people with acute brain injuries require surgery to remove or repair damaged tissue and to relieve stress. Individuals with mild brain injuries may not require any treatment past medication. Many people with brain injuries may also require: �
physical therapy
speech and language therapy
psychiatry
Brain Tumors
Occasionally, brain tumors can develop and they can become quite dangerous. These are known as primary brain tumors. In other instances, cancer from other regions of the body can spread into the brain. These are known as secondary or metastatic brain tumors. Brain tumors may be categorized as either malignant (cancerous) or benign (noncancerous). Healthcare professionals also categorize brain tumors as grades 1, 2, 3, or 4. Higher numbers indicate more severe cancers. �
The main cause of the majority of brain tumors is largely unknown. They can occur in people of all age. Symptoms of brain cancers generally depend on the size and location of the tumor. The most common symptoms of brain tumors include: �
headaches
seizures
tingling sensations or numbness in the arms or legs
nausea
vomiting
changes in personality
difficulty with movement or balance
changes in hearing, speech, or vision
The type of treatment you’ll receive for the brain tumors depends on a variety of different factors, such as the size of the brain tumor, your age, and your overall health and wellness. The main types of treatment for brain tumors include: �
chemotherapy
radiation therapy
surgery
Neurodegenerative Diseases
Neurodegenerative disorders cause the brain and the nerves to gradually deteriorate as people age. They can affect an individual’s personality and cause confusion. They are also able to destroy the brain’s tissue and nerves. Brain disorders like Alzheimer’s disease may develop over time with age. It can slowly impair memory and thought processes. Other diseases, such as Tay-Sachs disease are genetic and can develop at any age. Common neurodegenerative diseases include: �
Huntington’s disease
ALS (amyotrophic lateral sclerosis), or Lou Gehrig’s disease
Parkinson’s disease
all types of dementia
Several of the most common symptoms of neurodegenerative diseases include: �
Memory loss
forgetfulness
apathy
anxiety
agitation
a loss of inhibition
mood changes
Neurodegenerative diseases can ultimately cause irreversible damage and symptoms generally have a tendency of becoming worse as the disease progresses. New symptoms can also continue to develop over time. Unfortunately, there’s no treatment for neurodegenerative diseases, however, treatment can help improve symptoms. The treatment goal for these health issues is to reduce symptoms and maintain quality of life. Treatment often involves the use of medications to control symptoms. �
Mental Disorders
Mental disorders, or mental illnesses, are a wide variety of health issues which affect behavior patterns. Much like the brain disorders previously mentioned, symptoms can also vary. Several of the most commonly diagnosed mental disorders are: �
depression
anxiety
bipolar disorder
post-traumatic stress disorder (PTSD)
schizophrenia
The symptoms of mental disorders can vary based on the health issue. Different people can experience exactly the same mental disorders differently. Make sure to speak with a healthcare professional if you notice any changes in your behavior, thought patterns, or mood. The two major types of treatments for mental disorders are medication and psychotherapy. Different treatments work better for different health issues. Many individuals find that a combination of both is best. �
If you believe that you may have a mental disorder, it’s important to speak to a healthcare professional for diagnosis in order to determine which treatment program is suitable for you. There are many resources available to treat mental disorders. �
What are the Risk Factors for Brain Disorders?
Brain disorders can affect anyone, however, the risk factors can ultimately vary for different types of brain disorders. Traumatic brain injury is most common in children under 4 years old, young adults between 15 and 25 years old, and adults 65 and older. Brain tumors may affect any individual at any given age. An individual’s risk for developing brain disorders generally depends on the individual’s genetics and their vulnerability to environmental risk factors, such as radiation. �
Older age and family history are the most important risk factors for neurodegenerative diseases. Mental disorders are extremely common. About 1 in 5 American adults have experienced a mental health issue. Your risk may be greater if you: �
have a family history of mental illness
have or have had traumatic or stressful life experiences
have a history of misusing drugs or alcohol
have or have experienced a traumatic brain injury
There are a variety of treatment approaches which can help improve brain disorders. The outlook for people with brain disorders depends on the type and severity of the brain disorder. Several of these health issues can be easily treated with the utilization of medication and other therapy methods and techniques. Other brain disorders, such as neurodegenerative diseases and several types of traumatic brain injuries have no cure, however, treatment approaches can help improve symptoms. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
The purpose of the article above is to discuss the different types of brain disorders, including neurodegenerative diseases. Neurological diseases are associated with the brain, the spine, and the nerves. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
Subluxation describes what happens when the spinal joints get shifted out of alignment. This can be caused by:
Stress
Trauma
Chemical imbalance
The nervous system, which consists of the (spine/nerves/brain) is the central headquarters of the body. Subluxation removal helps the body function at its optimum level.
Chiropractic adjustments reduce pressure on the nerves and ease the flow of communication and signals going back and forth.
These adjustments trigger the release of endorphins, which cause instant pain relief.
Our hips are made durable, but with age and normal wear and tear, this cartilage wears down, which can lead to injury.
This also includes the:
Muscles
Tendons
Bones in and around the hip
And can be caused by a number of conditions, including:
Arthritis
Avascular necrosis (osteonecrosis)
Cancers
Bursitis
Hip fractures
Hip labral tear
Muscle/tendon strain
Tendinitis
If adjustments seem to be only temporary, this could be an indicator of problems beyond the spine.
Pain or other symptoms in the body start with the body�s foundation: the feet.
When we walk there are incremental-segmental movements of the spine that are small motions but are very important in proper function.
If there are foot problems:
Spinal subluxations
Pain
Degeneration throughout the body can happen.
Research has found that poor foot mechanics can create severe problems that affect the normal functions of the:
Ankle
Knee
Hip
Back
Symptoms of Vertebral Subluxation
Neck and back pain
Headaches
Dizziness
Balance issues
Spine muscle spasms
Tightness
Weakness
Spinal mobility
Pain
Numbness
Tingling
Joint pain
Tenderness
Stiffness
Treatment
If you are experiencing any of these symptoms, subluxation could be the cause.
Chiropractic treatment and custom orthotics are the best way to correct the subluxation.
Chiropractors are experienced in finding and correcting these problems. And the custom orthotics can help keep you and your spine in perfect alignment.
Get Rid of *LOW BACK PAIN* with Custom Foot Orthotics | El Paso, TX (2019)
Approximately 80 percent of the population will experience some type of back pain sometime throughout their lifetime. Low back pain and sciatica are several of the most common complaints frequently reported in a doctor office setting. But, did you know that low back pain and sciatica can be caused due to foot problems? Custom-made functional foot orthotics can help support and promote the natural alignment of the spine. Poor posture associated with foot problems and other health issues can be corrected through the utilization of custom-made functional foot orthotics. Because every individual has unique foot anatomy, custom-made foot orthotics can be beneficial for a variety of people with foot problems and other health issues. Dr. Alex Jimenez is the non-surgical choice for foot problems.
What’s Afoot
Although many people try to treat their low back pain on their own first, one of the fastest and best ways to treat it is through custom orthotics, which actually optimize the performance of your entire body, not just your feet and lower back. Over-the-counter orthotics do not provide proper support and can even cause more damage to the body. Chronic lower back pain is not a normal thing that has to do with age or lifestyle.
If you are experiencing lower back pain, call a chiropractor and ask about how custom orthotics can help you.
NCBI Resources
Chiropractors use specific methods to return the vertebrae in their proper locations or muster them to allow them to go freely when subluxations happen. These techniques are called spinal manipulations or adjustments. During an adjustment, the vertebra is freed in the misaligned location and returned to the right place in the spinal column. The adjustment permits the entire body to cure and preserve homeostasis once performed.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine


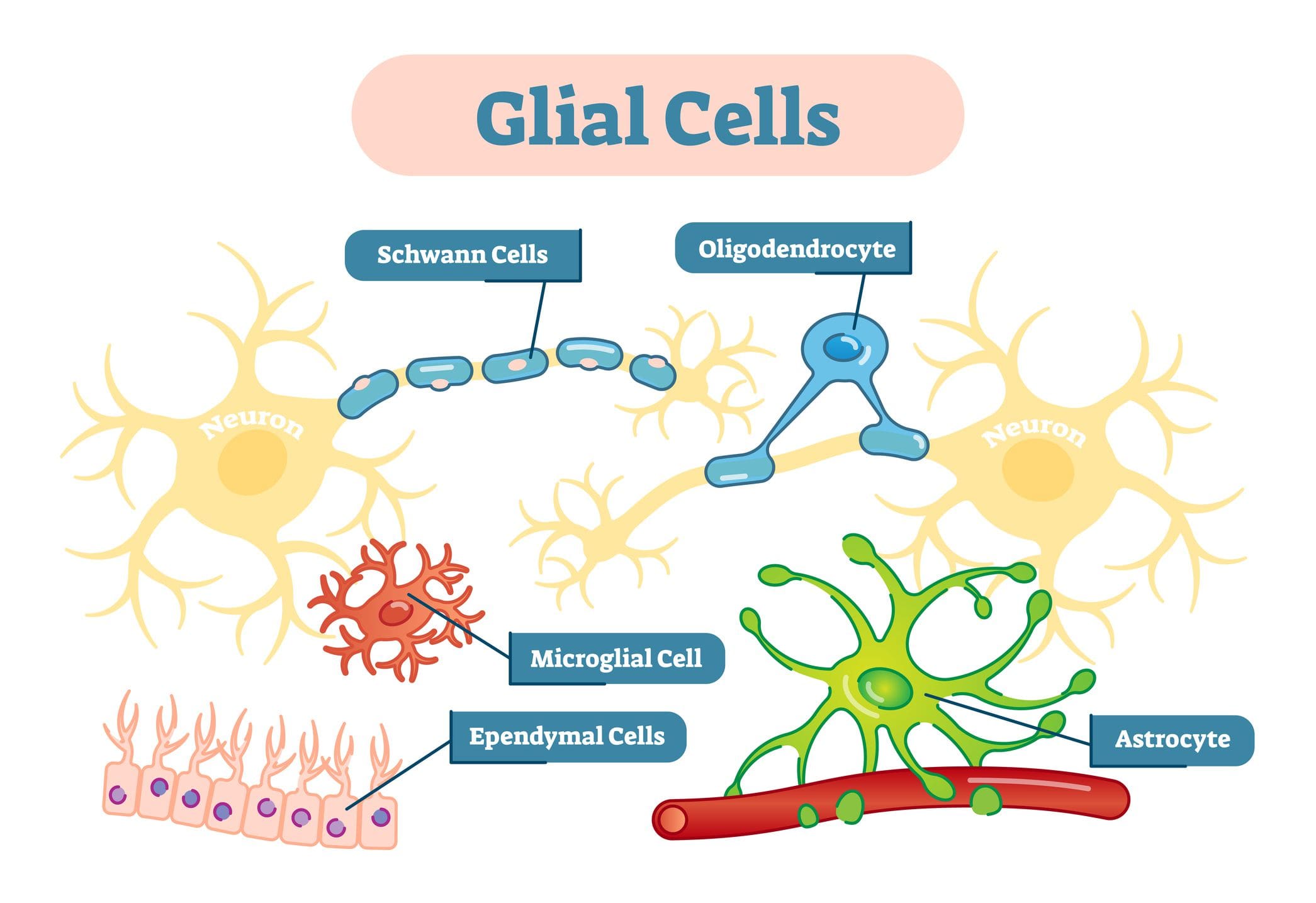 �
�