Lower back pain is a condition that pretty much affects most of us at some point in our lives. Some find:
Sitting
Standing
Walking
can be painfully difficult or helpful, depending on the position or the activity they’re involved in.
Low back pain varies from person to person, yet there remains no consensus on the optimal way to diagnose and treat patients.
Lower back pain can be caused by a multitude of factors and can be difficult to diagnose the exact cause. However, there is an advanced method of diagnosing and treating individuals with musculoskeletal conditions/injuries.
TENS, Transcutaneous Electrical Nerve Stimulation in Physical Therapy. Therapist Positioning Electrodes onto Patient’s Lower Back
Successful treatment
Dividing patients with lower back pain into more similar groups based on the same factors that aggravate and alleviate the pain means that a more custom based treatment plan can be created.
The one size fits all method just doesn’t cut it. A more focused approach for every individual leads to better results.
Patients find that placing their bodies in certain positions and certain physical activities can:
Activate
Aggravate
Deactivate their back pain.
Patients also find the pain being either better or worse.
Understanding why sitting, standing, and walking can change the severity of low back pain can be helpful in diagnosis.
These are important cues that help to diagnose and treat low back pain.
People sit, stand, and walk all day. This is why so much research has been conducted on how these specific positions and activities contribute to low back pain.
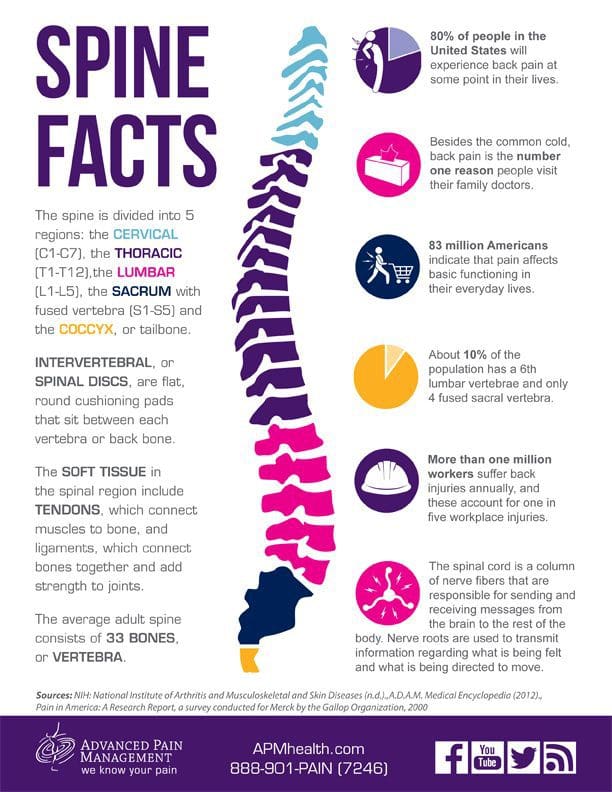
Spine Anatomy
The alignment of the spinal column, from the skull to the pelvis, is S-shaped.
The cervical and lumbar spinal segments curve towards the front of the body, and so are lordotic,�while the thoracic spine curves towards the back of the body and is kyphotic.
The amount of curvature does not stay in one place and changes based on body position.
Compared to standing, sitting decreases lumbar lordosis by about 50%.
Changes in lumbar lordosis can relieve pain from certain forms of back pain but can aggravate others.
Picture The Spine Bending
Imagine you are holding a garden hose. Holding it vertically in front of you. The hollow part of the tube represents the spinal canal, the part of the hose facing you is the posterior spinal column, and the part of the hose facing away from you is the anterior spinal column.
Bend the hose in half. The hose on the outward-facing side of the curve will stretch out, while the hose on the inward-facing side of the tube will be compressed.
This exercise helps visualize that an object being bent will experience two forces, either:
Compression
Tension
Increasing lumbar curvature will compress the posterior column�and stretch out the anterior column vertebrae and discs.
Decreasing lumbar curvature will�stretch out�the posterior column and�compress�the anterior column. This is the basis of why certain body positions can relieve back pain symptoms for some people and make it worse for others.
Prolonged sitting, and especially if poor posture is involved, can cause overstretching of spinal muscles.
Arthritis can affect the joints.
The facet joints are posterior based structures and can become compressed with increased curvature. When the facet joints are the primary cause of back pain, patients usually find that sitting improves the pain, while standing and walking make it worse.
When the discs are the pain generator, sitting seems to aggravate the pain as there is more compression in the tissue.
With certain types of disc herniations, sitting can compress the disc to the point that the herniated tissue starts to press against a nerve root causing radicular pain or pain that radiates out to another area of the body like the legs. In this case, walking seems to alleviate the pain.
Spinal Conditions
Various spinal conditions definitely contribute to back pain and have the same presentations and alleviations.
Spinal Stenosis which means the narrowing of the spinal canal. Patients with this type of spine pain improve with leaning forward sitting. This is because the posture increases/opens the size of the canal�and decreases the nerve root compression.
Spondylolisthesis is when one vertebra slips forward over the vertebra right underneath. This is more commonly known as a slipped disc. There are various forms of this condition. But the pain occurs immediately when sitting, bending or walking and is usually relieved when standing still or in a neutral position for short periods.
Sacroiliac Joint Dysfunction comes from the sacroiliac joint becoming inflamed. Pain is usually aggravated when sitting or about to sit. especially when there is added weight on the affected side. This can be difficult to diagnose because of trying to figure out if it’s the hip or low back causing the pain.
Locating the Pain Generator
Sitting, standing, walking low back pain causes are different for everyone. But finding the root cause helps to prescribe the best treatment possible. A chiropractor uses many different techniques to relieve pain. These include:
Applied pressure
Massage
Hands-on manipulation (adjustments)
X-rays
MRI’s
Lab work
Health coaching
Chiropractors don�t prescribe medications, but they do recommend therapeutic, rehabilitative exercises and nutritional lifestyle counseling to help the body heal itself.
Low Back Pain Treatment El Paso, Texas
NCBI Resources
A chiropractor sets up treatment approaches based on the individual. This begins with the natural, non-invasive treatments before moving on to more aggressive techniques. And as an added bonus patient�s who have received chiropractic treatment have experienced improvements to their digestive health and have reported better and deeper sleep after a chiropractic visit.
Do you often feel that your energy levels drop in the afternoons? Do you often feel brain fog or have unclear thoughts and poor concentration? Do you often experience brain fatigue with chronic pain and inflammation? Diet and supplements are essential for overall well-being. However, fish oil omega-3s are a common supplement with a variety of health benefits. �
Fish oil is a well-known supplement that comes from fatty fish, such as sardines, anchovies, mackerel, and salmon. Fish oil has two types of omega-3 fatty acids, known as eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), both of which are commonly used to support skin and heart health. Fish oil supplements can also promote brain health, especially when it comes to improving memory and mood problems like depression, as well as a variety of other health issues. The purpose of the following article is to discuss how the omega-3 fatty acids in fish oil may support and promote brain health. �
What Are Fish Oil Omega-3s?
Omega-3 fatty acids, best known as omega-3s, are polyunsaturated fats that offer most of the brain health benefits of fish oil. Fish oil has two main types of omega-3 fatty acids, EPA and DHA. These two omega-3s are found in cell membranes and these also have anti-inflammatory effects in the human body. They are also well-known for their fundamental roles in human development and heart health. EPA and DHA are found in fatty fish and fish oil. Because the majority of people do not eat the recommended amounts of fish, many people probably aren’t getting enough EPA and DHA in their regular diets. �
The human body can make EPA and DHA from another type of omega-3 fatty acid, known as alpha-linolenic acid (ALA). ALA is commonly found in a variety of foods, including walnuts, flaxseeds, chia seeds, canola oil, soybeans, and soybean oil. However, the human body can’t properly turn ALA into EPA and DHA, where healthcare professionals and researchers estimate that approximately less than 10 percent of the amount of ALA you eat is properly turned into EPA or DHA. Fish oil is a good option for people who don�t eat a lot of fish but are still looking to gain the health benefits of omega-3 fatty acids. �
How Do Omega-3s Improve Brain Health?
The omega-3 fatty acids EPA and DHA are essential for normal brain function during all stages of life. EPA and DHA play a fundamental role in the development of a baby�s brain. Several research studies have associated pregnant women�s fish intake or fish oil use with higher scores for their children on brain function and intelligence tests in early childhood. �
These omega-3s are also essential for the regulation of normal brain function throughout life. They are commonly found in the cell membranes of brain cells, preserving cell membrane health and facilitating communication between brain cells. �
When animals are fed diets without omega-3 fatty acids, the amount of DHA in their brains decreases, and they often demonstrate deficits in learning and memory. In older adults, decreased levels of DHA in the blood have ultimately been associated with smaller brain size, a prevalent symptom of accelerated brain aging. Clearly, it is essential to make sure that you get enough omega-3 fatty acids in order to avoid these detrimental effects on brain function and development. �
Fish Oil for Memory
The omega-3s found in fish oil play important roles in brain function and development. There are also claims that fish oil can improve brain function in people with memory problems, such as dementia and Alzheimer�s disease. Alzheimer�s disease affects brain function and quality of life in millions of elderly adults. That’s why finding a supplement or natural remedy that can help improve brain function in this population of individuals would be a major, if not a life-changing discovery. �
Unfortunately, a review of the research study found no compelling evidence that omega-3 supplements like fish oil can improve brain function in people with dementia and Alzheimer�s disease. However, several research studies suggest that fish oil supplements may improve brain function in people with more mild types of brain health issues, including mild cognitive impairment (MCI) or age-related cognitive decline. Although these types of brain conditions aren�t as severe as dementia and Alzheimer�s disease, they can still result in memory loss and sometimes other types of impaired brain function. �
One research study gave 485 older adults with age-related cognitive decline either 900 mg of DHA or a placebo every day. After 24 weeks, those taking DHA performed better on memory and learning tests. Similarly, another research study investigated the effects of taking 1.8 grams of omega-3 fatty acids from fish oil supplements daily for 24 weeks. The researchers found improvements in brain function in people with MCI but there were no benefits for those with dementia and Alzheimer�s disease. According to the research study, fish oil supplements may be most beneficial when people start taking them in the early stages of brain function decline. If you wait too long, fish oil may be of little benefit to brain health. �
Fish Oil for Depression
Finding treatments for depression and other mental health issues is still a public health priority. A recent review of several research studies concluded that taking fish oil supplements improved symptoms in people with depression. However, the greatest improvements in depressive symptoms seemed to occur in people who were also taking antidepressants. In addition, people seemed to experience greater effects when the fish oil supplement also had higher doses of EPA. �
It is still unclear how EPA and omega-3s help improve depressive symptoms. Researchers suggest that it may be associated with their effects on serotonin and serotonin receptors in the brain. Others have proposed that omega-3s from fish oil can improve depressive symptoms through their anti-inflammatory effects. Additional evidence suggests that fish oil may also help improve other mental health issues like borderline personality disorder and bipolar disorder. However, more high-quality research studies are required before the medical community can make definitive recommendations. �
Should You Take Fish Oil for Your Brain Health?
According to the evidence gathered from a variety of research studies, you may want to consider taking fish oil omega-3 fatty acids if you are experiencing mild memory loss, depression, or if you want to improve your overall brain health.�There are no official recommendations regarding how much omega-3s from fish oil you need to take to see benefits in brain function and mental health. The amounts of fish oil omega-3 fatty acids used in the research studies varied from each clinical trial. �
The US Food and Drug Administration has set a safe and effective limit for the intake of omega-3 fatty acid supplements to be at 3,000 mg per day. The European Food Safety Authority has set their recommendation a little higher, at no more than 5,000 mg per day. Taking 1,000 to 2,000 mg of omega-3 fatty acids from fish oil daily is likely a good starting point, which is under the recommended limit. People with depression should choose fish oil supplements with higher amounts of EPA. �
It is essential to read labels carefully when evaluating fish oil supplements. A 1,000-mg capsule of fish oil may have less than 500 mg of actual omega-3 fatty acids but this can vary for each brand. In general, fish oil supplements are considered to be safe and effective at dosages under those that were previously mentioned. Make sure you talk with a healthcare professional before taking fish oil omega-3 fatty acid supplements. Because research studies have reviewed their potential effects on blood clotting, this is especially important if you are taking blood-thinning medications or have an upcoming surgery. �
EPA and DHA are omega-3 fatty acids in fish oil that are fundamental for normal brain function and development. People with mild decline in memory or brain function and mood changes like depression may consider taking omega-3s from fish oil because these can improve symptoms and overall brain health. Although fish oil is typically praised for its benefits for heart health, it also has incredible effects on brain and mental health that are worth mentioning.�- Dr. Alex Jimenez D.C., C.C.S.T. Insight
Neurotransmitter Assessment Form
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. Symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
Do you often feel that your energy levels drop in the afternoons? Do you often feel brain fog or have unclear thoughts and poor concentration? Do you often experience brain fatigue with chronic pain and inflammation? Diet and supplements are essential for overall well-being. However, fish oil omega-3s are a common supplement with a variety of health benefits. �
Fish oil is a well-known supplement that comes from fatty fish, such as sardines, anchovies, mackerel, and salmon. Fish oil has two types of omega-3 fatty acids, known as eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), both of which are commonly used to support skin and heart health. Fish oil supplements can also promote brain health, especially when it comes to improving memory, mood problems like depression, as well as neurological diseases and other health issues. The purpose of the article above was to discuss how the omega-3 fatty acids in fish oil support and promote brain health. �
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.�
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Food Sensitivity for the IgG & IgA Immune Response
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with food sensitivities. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
To get the best treatment for upper or mid-back back pain, you should understand what may be causing it.
A doctor or chiropractor can help you figure out what is contributing to your back pain, then determine the root cause, and set up a treatment outline. Here are some of the more common causes.
Improper posture
Poor posture is one of the leading causes of upper back pain because so many people spend their workdays sitting at some station for most if not the entire day. Sitting with a:
Rounded back
Shoulders hunched forward
Just these two positional behaviors can put massive stress on the back muscles.
Getting into bad habits and not sitting properly, and sitting for so many hours a day is a sure way to bring out some form of body pain.
Not lifting objects properly
When picking something up, you should use proper lifting body mechanics to protect the spine.
Not using proper lifting form can definitely cause injury/s.
Overloaded backpack/purse
Anyone who uses backpacks and big purses is at risk for upper back injury and consistent pain.
Over-loading backpacks and purses can be dangerous to the spine and shoulders.
Also not wearing the backpack correctly, for example just using one strap causes imbalance, which leads to soreness, and that leads to injury.
Trauma Accident
Auto accidents, slips, and falls can cause all kinds of injuries including upper back pain.
Fracturing a vertebra or a spinal bone is possible.� When this happens part of the vertebrae presses on a spinal nerve and can cause pain.
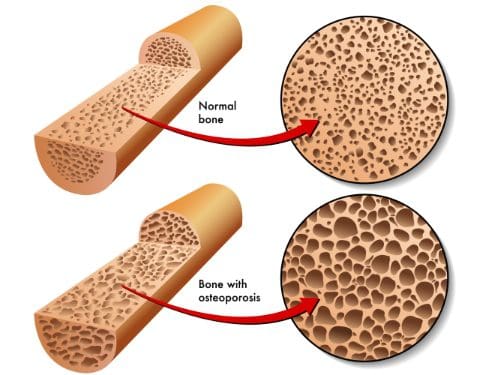
Osteoporosis
This condition affects the bones, and an individual might not know they have osteoporosis until some type of fracture like a vertebral compression fracture.
It weakens the bones, which can affect how the body supports its weight. This opens the door for fractures.
Weakened vertebrae won’t support the body’s weight correctly, so the muscles, ligaments, and tendons have to work harder.
That leads to:
Sprains
Strains
Muscle fatigue
Various injuries
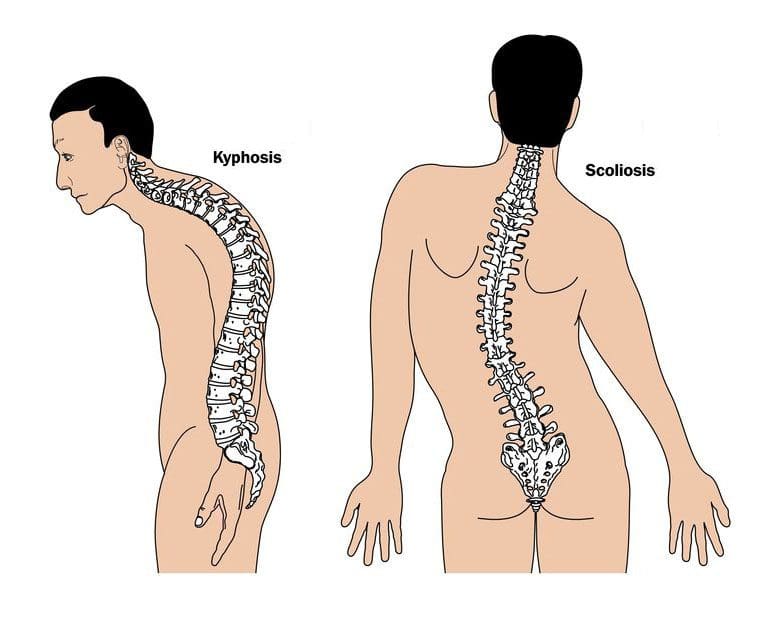
Kyphosis
The spine is supposed to curve outwards in the upper back; the curve is called kyphosis or a kyphotic curve.
With problematic kyphosis, the spine begins to curve outward in an exaggerated fashion that can lead to back pain.
Scoliosis
Scoliosis causes an unusual curve or curves in the spine. It makes the spine look like the letter “S” or “C” when seen from the back.
Non-Spine Conditions
Upper back pain can develop from other medical conditions that are not related to the spine. For example:
These conditions can cause individuals to move or contort into awkward positions, and swelling of muscle tissues that radiate into the upper mid-back.
Upper Back Structure
The upper back is the more stable area of the spine compared to the neck and lower back. It does not move as much because part of its main job is to protect the organs in the chest. This works in conjunction with the ribs, that is attached to the mid-back.
Because it doesn’t move as much, joint and disc problems are not as common. But that does not mean that you can’t get a herniated disc. It’s also less common to have degenerative problems in the upper mid-back.
We want you to live a life that is fulfilled with more energy, a positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life. I have made a life of taking care of every one of my patients.
I assure you, I will only accept the best for you.
Lower Back Pain Specialist El Paso, TX Chiropractor
Mike Melgoza is a very active person who is always engaging in physical activity, as a result, he occasionally suffers from debilitating back pain symptoms. Mr. Melgoza was struggling to sleep properly due to his symptoms of back pain before receiving chiropractic care with Dr. Jimenez.
Back pain is one of the most common reasons people visit the doctor or miss work and it is also a leading cause of disability globally. The majority of people have back pain at least once throughout their lifetimes. Luckily, you can take steps to prevent or relieve back pain.
NCBI Resources
Pain in the upper and/or mid-back is not as common as lower back or neck pain. Movement in the upper back is limited because of the attachments to the rib cage.
Upper back pain is generally caused by soft tissue injuries, like sprains or strains, muscle tension, bad posture, or looking downward for extended periods like texting, over phone use.
Neurological diseases, including well-known neurodegenerative disorders like Alzheimer’s disease (AD) and Parkinson’s disease (PD) as well as other rare health issues, such as Huntington’s disease (HD) and amyotrophic lateral sclerosis (ALS), affect millions of people worldwide. Unfortunately, these are estimated to increase due to the aging population. Currently, there is no treatment available for any neurodegenerative disorder. Treatments for symptoms are available for several neurological diseases, such as PD and HD, but the therapeutic benefits are limited. Although the causes and symptoms for these health issues are different for each neurodegenerative disorders, their molecular pathogeneses share common underlying factors and characteristics, including excessive levels of reactive oxygen species (ROS), mainly due to mitochondrial impairment, neuroinflammation, and disturbances in protein homeostasis (proteostasis). This increases the possibility of developing a universal treatment that will focus on targeting the common triggers of neurological diseases. �
Nrf2 Activation Pathways and the Human Brain
The transcription factor, Nrf2, regulates the main endogenous defense mechanism against oxidative and xenobiotic stress and inflammation. Nrf2 also plays a fundamental role in the management of mitochondrial function and cellular proteostasis, which suggests the possible benefits of Nrf2 to control neurodegenerative disorders. When under stress, Nrf2 activates the transcriptional upregulation of a large network of cytoprotective genes that allow adaptation and survival. The levels and activity of Nrf2 are controlled through ubiquitination and proteasomal degradation mediated by several ubiquitin ligase systems, including Keap1-Cul3/Rbx1, ?-TrCP-Cul1, and Hrd1. Keap1 is the most well understood key regulator of Nrf2. �
Keap1 functions as a primary sensor for electrophiles and oxidants, which chemically change certain cysteines in Keap1, leading to conformational changes that protect Nrf2 from Keap1-associated degradation. Subsequently, Nrf2 will accumulate and then translocate to the nucleus where it binds as a heterodimer with a small Maf transcription factor to antioxidant response elements in the promoter of its target genes to activate the expression of a large network of detoxification, antioxidant, and anti-inflammatory genes as well as other genes involved in the clearance of damaged proteins. Of particular interest is also the upregulation of genes responsible in the biosynthesis and the regeneration of glutathione (GSH), a major intracellular antioxidant. Moreover, Nrf2 also suppresses proinflammatory responses through transcriptional repression and it is involved in the regulation of mitochondrial function. Keap1 and p62/SQSTM1 are Nrf2-associated proteins and main regulators of negative and positive feedback loop mechanisms. In addition, p62 targets Keap1 for selective degradation through autophagy, therefore contributing to the sustained Nrf2 activation response. �
Aging has been associated with the increase in ROS and chronic inflammation, which suggests a loss of adaptability and/or impairment of Nrf2 signaling, which are particularly pronounced in age-dependent neurodegenerative disorders. Surprisingly, rare mutations in SQSTM1 can cause susceptibility to the human neurodegenerative disorder, ALS as well as frontotemporal lobar degeneration, and are associated with muted Nrf2 activation responses in clinical trials. Research studies suggest a reciprocal correlation and show negative effects of mutant disease-related proteins on Nrf2 signaling, thus suggesting the inhibition of the Nrf2 pathway as a possible mechanism underlying neurodegeneration and health issues. �
Nrf2 Activation for Neurodegenerative Disorders
ALS, an adult-onset neurodegenerative disorder caused by the selective death of motor neurons in the brain and spinal cord, is commonly characterized by progressive muscle weakness and atrophy which is generally considered to be fatal, typically within 5 years of diagnosis. ALS has a predominant sporadic ALS form with no apparent genetic component, however, approximately 5 to 10 percent of cases show an autosomal dominant inheritance pattern or familial form of the disease, known as fALS, with is known to cause gene mutations. The symptoms of sporadic ALS and familial ALS are similar, which suggests the involvement of common pathogenic mechanisms, including oxidative stress and neuroinflammation. �
Research studies show that oxidative stress and neuroinflammation should be the key therapeutic targets of Nrf2 signaling in ALS. Genetic research studies in ALS mouse models have shown a considerable therapeutic effect of increased Nrf2 levels in astrocytes, the main GSH producers for neurons. Furthermore, Nrf2 signaling is fundamental for controlling neuroinflammation in ALS through the management of the effects of activated microglial cells on overall neuronal survival. Consistent with the therapeutic potential of Nrf2 signaling, treatment with small molecule activators, including the extremely potent cyanoenone triterpenoids, has ultimately shown efficacy in research study mouse ALS models. �
The neuroprotective potential of Nrf2 activation has been evaluated in experiments utilizing genetic mouse HD models. HD is an autosomal dominant and highly penetrant neurodegenerative disorder, which results from the pathological expansion of a trinucleotide CAG repeats encoding polyglutamines in HTT protein. Brains from patients with HD usually show marked striatal and cortical atrophy at the time of diagnosis. Once motor or other symptoms become apparent, generally throughout midlife, the affected individuals become increasingly disabled over the course of 15 to 25 years before eventually succumbing to the effects of severe physical and mental deterioration, according to evidence from research studies. �
Complex pathogenic mechanisms have been shown in HD, however, excessive oxidative stress has been recognized as a fundamental driver of pathology. The harmful role of oxidative stress has been described in both HD patients and in experimental clinical trial models and it is potentially due to the neuronal sensitivity of an excess in ROS. The levels of several Nrf2-dependent antioxidant proteins, including glutathione peroxidases, catalase, and superoxide dismutase 1, are increased in human HD brains as compared with non-disease controls, suggesting a partial activation of Nrf2 defense signaling yet insufficient enough to block progressive neurodegeneration. Pharmacological activation of Nrf2 results in the broad antioxidant effects of HD in mouse brains and ameliorates the neurological phenotype. Increased expression of several key inflammatory mediators has been shown in the blood, the striatum, the cortex, and the cerebellum from postmortem patient HD tissues, however, neuroinflammation in HD patients seems to be less pronounced than in ALS or PD patients. �
Neurological Disease Treatment with Nrf2 Activation
Finally, the neurological phenotype of the most common neurological disease and neurodegenerative disorder, PD, can be challenged by Nrf2 activation. PD is characterized by the progressive loss of dopaminergic neurons in the substantia nigra and the profound reduction of dopamine in the striatum. Currently available dopaminergic treatments offer relief from several symptoms but these only address the motor manifestations. Multiple genetic and environmental factors have been suggested in the etiology of PD, however, like ALS, the majority of the clinical cases are sporadic. The discovery that the environmental neurotoxin 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP) causes Parkinson’s disease in humans, led to the development of the MPTP mouse model of disease, which to date, remains one of the most highly utilized animal models of sporadic PD, including the evaluation of drug efficiency. Nrf2 activators showed neuroprotective effects in MPTP mice, which are associated with a reduction of oxidative damage and neuroinflammation. The identification of causative mutations in SNCA, the gene encoding ?-synuclein (aSyn), developed genetic mouse PD models, in which daily oral delivery of the Nrf2 activator dimethyl fumarate (DMF) protected nigral dopaminergic neurons against aSyn toxicity. �
Although oxidative stress and neuroinflammation are pathological hallmarks of AD, a therapeutic role of Nrf2 signaling has developed more slowly, perhaps due to the complexity of disease pathogenesis and readouts of efficiency. Nonetheless, there is a number of recent research studies that demonstrate the efficiency of Nrf2 activators in AD mouse models. � DMF, a U.S. FDA-approved drug (Tecfidera, Biogen-Idec) for the treatment of relapsing multiple sclerosis, activates Nrf2 through the regulation of the Keap1 sensor. DMF is of seemingly low potency and specificity, which prevents neurodegeneration. Drug-like molecules with a similar mechanism of action or with the ability of direct interference with the Keap1/Nrf2 interaction are emerging. The data demonstrate the feasibility to develop Nrf2 activators for treatment. �
In summary, although the causes and symptoms of neurological diseases are different, neurodegenerative disorders share similar molecular mechanisms, which could be regulated and managed with Nrf2 activators. Moreover, targeting Nrf2 signaling may offer a safe and effective treatment approach for a variety of these health issues. Because pharmacological Nrf2 activation targets the broad mechanisms of these health issues, all neurodegenerative conditions would be eligible for treatment. Furthermore, the main goal is to develop noninvasive oral treatment(s) for patients under the supervision of healthcare professionals, which targets both sporadic and familial patients. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Neurotransmitter Assessment Form
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. Symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
Neurological diseases, including well-known neurodegenerative disorders like Alzheimer’s disease (AD) and Parkinson’s disease (PD) as well as other rare health issues, such as Huntington’s disease (HD) and amyotrophic lateral sclerosis (ALS), affect millions of people worldwide. Unfortunately, these are estimated to increase due to the aging population. Currently, there is no treatment available for any neurodegenerative disorder. Treatments for symptoms are available for several neurological diseases, such as PD and HD, but the therapeutic benefits are limited. Although the causes and symptoms for these health issues are different for each neurodegenerative disorders, their molecular pathogeneses share common underlying factors and characteristics, including excessive levels of reactive oxygen species (ROS), mainly due to mitochondrial impairment, neuroinflammation, and disturbances in protein homeostasis (proteostasis). This increases the possibility of developing a universal treatment that will focus on targeting the common triggers of neurological diseases. �
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
References: �
Dinkova-Kostova, Albena T, et al. �Activation of Nrf2 Signaling as a Common Treatment of Neurodegenerative Diseases.� Activation of Nrf2 Signaling as a Common Treatment of Neurodegenerative Diseases | Neurodegenerative Disease Management, 23 May 2017, www.futuremedicine.com/doi/full/10.2217/nmt-2017-0011#.
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
�
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Food Sensitivity for the IgG & IgA Immune Response
�
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with food sensitivities. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
How often do you feel unclear thoughts or concentration and brain fog? How often do you experience pain, discomfort, and/or inflammation? How often do you feel mental and physical fatigue after eating meals? Inflammation is an essential immune response, however, chronic inflammation, especially in the brain and the joints, can cause a variety of health issues. Fortunately, there are many natural remedies that can help reduce inflammation, including turmeric or curcumin. �
Turmeric, sometimes known as Indian saffron or the golden spice, is a tall plant that grows in Central America and Asia. The turmeric that we commonly see on shelves and in spice cabinets is made of the ground roots of the plant. Moreover, the bright yellow color of processed turmeric has inspired many cultures to use it as a dye. Ground turmeric is also the main ingredient in curry powder. Capsules, powders, teas, and extracts are several ways that turmeric is available commercially. �
Curcumin is the active ingredient found in turmeric and it has many powerful biological properties. Ayurvedic medicine, a traditional Indian system of treatment, recommends utilizing turmeric for a variety of health issues, including chronic pain and inflammation. Western medicine has started to evaluate the use of turmeric as a pain reliever. �In the following article, we will discuss the health benefits and risks of turmeric as well as how these can affect overall health and wellness. �
Health Benefits of Turmeric
According to the Arthritis Foundation, research studies in which turmeric has been utilized helped reduce chronic inflammation in the clinical trial participants. The anti-inflammatory properties of turmeric, or curcumin, may help reduce arthritis joint pain and discomfort. Together with other supplements, such as an Nrf2 activator, research studies have shown that these can reduce inflammatory cytokines by dampening NF-?B activity and down-regulating COX, LOX, iNOS, matrix metalloproteiases, INF-a, and interleukines-1, 2, 6, 8, 12 as well as chemokines. The Arthritis Foundation suggests taking capsules of 400 to 600 milligrams (mg) of turmeric or curcumin up to three times per day for chronic pain and inflammation. �
Many researchers and healthcare professionals believe that turmeric may not only be efficient at reducing inflammation but it may also be safe and effective as a chronic pain reliever. As previously mentioned, the spice is reputed to help relieve arthritis as well as fibromyalgia symptoms. Research tudies seem to support the utilization of turmeric for pain relief, with one source noting that it seemed to work as well as ibuprofen (Advil) in people with arthritis. Although dosing recommendations seem to vary, those who participated in the research study took 800 mg of turmeric in capsules, each day. �
Turmeric has also recently been getting a lot of attention because of its antioxidant abilities. The antioxidant effects of turmeric appear to be so powerful that it may even help stop or prevent your liver from being damaged by toxins. This could be good news for people who take strong medicines for diabetes or any other health issues that may damage their liver through long-term utilization. Curcumin has also shown great promise as a type of cancer treatment. Research studies suggest that curcumin can have protective effects against pancreatic cancer, prostate cancer, and multiple myeloma. �
Turmeric is utilized in curry powder is because it helps add a delicious element to foods. However, turmeric can also play a fundamental role in the digestive process of that food. Because of its antioxidant and anti-inflammatory properties, turmeric can help promote healthy digestion. It’s utilized in ayurvedic medicine as a digestive system healing agent. Today, Western medicine has started to evaluate how turmeric, or curcumin, can help with gut inflammation as well as gut permeability, two measures of your digestive efficiency. Turmeric is even being explored as a possible treatment approach for irritable bowel syndrome (IBS). Turmeric can have many health benefits but curcumin supplements may also have several health risks. �
Health Risks of Turmeric
The same healing agents in turmeric that support healthy digestion can unfortunately also cause irritation when consumed in large amounts. Several research study participants looking at the utilization of turmeric as a type of cancer treatment had to drop out of the clinical trial because their digestive system was so negatively affected by the spice. Turmeric stimulates the stomach to produce more gastric acid. Although this can help with digestion, it can negatively affect digestion for others. �
Turmeric’s purifying properties may also make you bleed more easily. It’s not completely understood why this happens. However, people who take blood-thinning medicines, such as warfarin (Coumadin) should avoid consuming large doses of turmeric or curcumin.�
Researchers and healthcare professionals hypothesize that turmeric’s other benefits, including its capability to lower blood pressure and cholesterol, may have something to do with how turmeric affects your blood. Furthermore, researchers and healthcare professionals believe that the way curcumin is extracted from turmeric can be the cause of this health issue. Approximately 95 percent of curcumin in the U.S. is extracted by carcinogenic solvents. �
You may have also heard that eating foods seasoned with curry can stimulate labor. Although there’s little evidence to back up this claim, research studies suggest that turmeric can help ease symptoms of PMS. But perhaps, there may be some truth behind the old wives’ tale. Because of its blood-thinning effects alone, however, pregnant women are recommended to avoid taking turmeric supplements. Adding small amounts of turmeric as a spice to food or meals shouldn’t be a problem. �
The Takeaway of Turmeric
It appears that there are many health benefits to including turmeric as a part of your regular diet. The golden spice supports a healthy immune system, helps relieve chronic pain, and can even help promote healthy digestion, among other health benefits. However, because of some of its health risks and side effects, turmeric or curcumin may not be worth taking for several people. It’s essential to utilize caution when deciding whether turmeric is something you may want to try. As with any alternative treatment option, talk with your doctor before you utilize turmeric to treat any health issue. If you want to buy a turmeric or curcumin supplement, then there is an excellent selection online with thousands of great customer reviews. �
Turmeric, or curcumin, is a powerful, natural remedy which has been demonstrated to have many health benefits, especially for chronic pain and inflammation, among others. However, too much of the powerful, golden spice can also have several health risks and side effects. It’s fundamental to talk to a healthcare professional to discuss if turmeric or curcumin is a good treatment option. Turmeric, or curcumin, can be utilized for a variety of health issues, including arthritis and fibromyalgia. Make sure to talk to a doctor before using turmeric or curcumin supplements. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Neurotransmitter Assessment Form
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. Symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
How often do you feel unclear thoughts or concentration and brain fog? How often do you experience pain, discomfort, and/or inflammation? How often do you feel mental and physical fatigue after eating meals? Inflammation is an essential immune response, however, chronic inflammation, especially in the brain and the joints, can cause a variety of health issues. Fortunately, there are many natural remedies that can help reduce inflammation, including turmeric or curcumin. �
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Food Sensitivity for the IgG & IgA Immune Response
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with food sensitivities. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
If you are experiencing any of these situations, then you might be experiencing fibromyalgia.
Fibromyalgia is a common and chronic syndrome that causes pain and mental distress in the body. It causes widespread musculoskeletal pain, and it is accompanied by fatigue, sleep memory, and mood issues to the body.�The symptoms may be similar to arthritis; however, fibromyalgia is a rheumatic condition and causes soft tissue pain or myofascial pain.
There are three symptoms that fibromyalgia causes a person to have discomfort in their daily lives. They are:
Widespread pain: This pain is associated with fibromyalgia, and it is described as a constant dull ache that can last for at least three months. For it to be considered as widespread pain, it must occur both sides of the body, as well as above and below the waist.
Fatigue:Individuals with fibromyalgia often awaken tired, even though they have been sleeping for long periods. The pain that fibromyalgia causes can disrupt the person’s sleep patterns, causing them to have sleep disorders such as restless legs syndrome and sleep apnea.
Cognitive difficulties: This symptom is commonly known as �fibro fog.� It impairs the person�s ability to focus, pay attention, and concentrate on mental tasks.
Other symptoms can include:
IBS (irritable bowel syndrome)
Stiff joints and muscles in the morning
Headaches
Problems with vision
Nausea
Pelvic and urinary problems
Depression and anxiety
In the past, studies have shown that patients diagnosed with fibromyalgia had 11 out of 18 specific trigger points all around their bodies. Healthcare providers would check their patients and document how many of these points were painful to their patients by firmly, but gently, pressing their bodies to get a diagnosis.
The typical trigger points include:
The back of the head
The tops of the shoulders
The upper chest
The hips
The knees
The outer elbows
Nowadays, in a 2016 revised diagnostic criteria, healthcare providers can diagnose patients with fibromyalgia if the patient has pain in 4 out of 5 areas of the body that is causing them pain. The protocol when diagnosing patients is referred to as �multisite pain.�
Fibromyalgia Affecting the Endocrine System
When it comes to fibromyalgia, the symptoms are associated with the endocrine system. Research shows that fibromyalgia-like symptoms such as muscle pain and tenderness, exhaustion, reduced exercise capacity, and cold intolerance can resemble symptoms that are associated with the endocrine dysfunction like hypothyroidism and adrenal or growth hormone insufficiency.
More research has stated that fibromyalgia causes a person to develop chronic fatigue syndrome. Chronic fatigue syndrome causes the body to have a deficiency of serotonergic activity and the hypofunction of sympathetic nervous system function that could contribute to the abnormalities of the central components of the HPA axis. It can distort the body’s hormonal pattern that is being attributed to the hyperactivity of the CRH neurons. The hyperactivity caused by the CRH neurons can be driven and sustained by stress being exerted by chronic pain that has originated in the musculoskeletal system or the alternation of the central nervous system mechanism of nociception.
Researchers believe that repeated nerve stimulation causes the brains of patients with fibromyalgia to change. The change causes an abnormal increase level of certain chemicals (neurotransmitters) in the brain that signals pain. In addition, the brain�s pain receptors will develop a sort of memory of the pain that is causing problems to the patient�s body and causing them to be more sensitive since the signals are overreacting.
Treating Fibromyalgia
Even though fibromyalgia pain can be uncomfortable and consistent enough to interfere with a person�s daily routine. There are ways to relieve the pain and inflammation that fibromyalgia causes the body. Pain medication can bring down the inflammation and help a person sleep a little better. Other safe treatments that can help manage fibromyalgia pain are:
Acupuncture: Acupuncture is a Chinese medical system that uses needles to cause changes in the blood flow and the levels of neurotransmitters in the brain and spinal cord.
Therapy: A variety of different therapies can help a person reduce the effects that fibromyalgia has caused.
Yoga and tai chi: These practices combine meditation, slow movements, deep breathing, and relaxation � both help control fibromyalgia symptoms.
Reducing stress: Developing a plan to avoid or limit overexertion and emotional stress is useful when dealing with fibromyalgia. Learning to meditate and trying stress management techniques can help a person feel calm and recharged for the rest of the day.
Getting enough sleep: Since fatigue is one of the main characteristics of fibromyalgia, getting enough sleep is essential. Practicing good sleep habits and going to bed and getting up at the same time each day can lessen the effects of fatigue.
Exercising regularly: At first, exercising may increase the pain, but doing it gradually and regularly over time can decrease the symptoms. This can be walking, swimming, biking, and water aerobics can be beneficial to the body.
Pacing yourself: Keeping track of activities is beneficial for people with fibromyalgia. Moderation of daily activities on the good days can help a person overcome the symptoms when they flare-up.
Maintaining a healthy lifestyle: Eating healthy food that has anti-inflammatory properties can be useful for the body, and finding enjoyable hobbies can be beneficial as well.
Conclusion
Fibromyalgia is a chronic illness that causes pain and inflammation that affects the soft tissue in the body. The symptoms can resemble joint inflammation and causes people to have fatigue and discomfort all over their body. When these symptoms flare up, it can cause body damage. Treatments can help a person reduce the effects of fibromyalgia and be beneficial. Some products are formulated to counter the effects of temporary stress and offer support in the gastrointestinal system and the body�s metabolism.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at�915-850-0900�.
References:
Felman, Adam. �Fibromyalgia: Symptoms, Causes, and Treatment.� Medical News Today, MediLexicon International, 5 Jan. 2018, www.medicalnewstoday.com/articles/147083.php.
Geenen, Rinie, et al. �Evaluation and Management of Endocrine Dysfunction in Fibromyalgia.� Rheumatic Diseases Clinics of North America, U.S. National Library of Medicine, May 2002, www.ncbi.nlm.nih.gov/pubmed/12122926.
Neeck, G, and L J Crofford. �Neuroendocrine Perturbations in Fibromyalgia and Chronic Fatigue Syndrome.� Rheumatic Diseases Clinics of North America, U.S. National Library of Medicine, Nov. 2000, www.ncbi.nlm.nih.gov/pubmed/11084955.
Staff, Mayo Clinic. �Fibromyalgia.� Mayo Clinic, Mayo Foundation for Medical Education and Research, 11 Aug. 2017, www.mayoclinic.org/diseases-conditions/fibromyalgia/symptoms-causes/syc-20354780.
Staff, Mayo Clinic. �Fibromyalgia.� Mayo Clinic, Mayo Foundation for Medical Education and Research, 11 Aug. 2017, www.mayoclinic.org/diseases-conditions/fibromyalgia/diagnosis-treatment/drc-20354785.
Unknown, Unknown. �Fibromyalgia.� National Institute of Arthritis and Musculoskeletal and Skin Diseases, U.S. Department of Health and Human Services, 30 Sept. 2019, www.niams.nih.gov/health-topics/fibromyalgia.
Wolfe, Frederick, et al. �2016 Revisions to the 2010/2011 Fibromyalgia Diagnostic Criteria.� Seminars in Arthritis and Rheumatism, W.B. Saunders, 30 Aug. 2016, www.sciencedirect.com/science/article/abs/pii/S0049017216302086?via%3Dihub.
Health Coaching is a recent position that is being utilized by doctor offices around the country. Many doctors have realized that their patients are needing more one on one guidance but they are unable to provide this due to their hectic schedule. This is where they have created and utilized health coaches.
Health coaching is extremely beneficial for patients and can help them achieve their health goals. For more information about health coaches and a general overview of the essential role they play in the healthcare field, please see last week’s article linked here.
Health coaches use many different techniques depending on the patient they are working with, but the core values of their methods remain the same. These core values can be broken down into 6 different steps, with each individual step having smaller more detailed steps of their own. These steps can be identified as:
Identifying values and vision
Determining goals
Building a plan for action
Tracking progress
Visualizing one’s best self
Creating a plan for resiliency
Step 1: Identify Values
With this step being the first, it is one of the most crucial. When a patient comes to a physician or a health coach, it is usually because they have been recently diagnosed or are unhappy with their current health status. However, this does not mean that the patient is fully ready to accept their condition or understands it fully.
The patient will be asked to write down inventory in the categories of physical, emotional, spiritual, social, recreational, intellectual, and environmental. The purpose of this is so the patient is able to search and reflect on where they’re currently at and where they would like to be.
From here, there are different techniques and models that a coach may use. One being the transtheoretical model, in which the patient will use stages to move through a behavior change.
At this point, the conversation is less about treatment and more about obtaining an awareness of their health risks, experience with a current illness or any symptoms they�re experiencing. The patient is welcome and encouraged to express their emotions openly. The health coach will move through these next 6 steps to help outline the patient’s treatment and see what stage they are at.
1. Precontemplation: the patient does not intend to take action in the foreseeable future
2. Contemplation: intending to start introducing healthy behaviors within the next 6 months
3. Preparation: patients are ready to take action in the next 30 days
4. Action: the patient has recently changed their behavior and intends to keep moving forward
5. Maintenance: the patient has sustained their behavior change for 6 months and intends to maintain the behavior change for more than six months
6. Termination: the patient has grown and is now self-aware of their behaviors and has no desire to return to their previously unhealthy behaviors
As we all know, values are formed starting in early childhood. These values are then later consciously re-evaluated and may change. It is important for the patient to work with the health coach so they properly understand their personal values. This allows the patient to get clarity and build self-awareness to make intelligent decisions and keep a balance in life.
Actually sitting down identifying values might be difficult, as many individuals do not think about them often. If this is the case, the health coach might help by asking questions like:
What is more important in your life: Beyond basic human needs, what must you have in your life to experience fulfillment?
Take this time and consider a meaningful moment: What was happening to you and what values were you honoring?
Consider a time when you were angry or upset: What were you feeling and, if you flip those feelings around, what value is being suppressed?
These questions aid in triggering times that the patient might not have been connecting to values. After the patient has identifies values, the health coach will work with the patient to select between 5-10 of their core values and then rank them in order of importance. From here, the patient is able to evaluate their values and proceed to determining goals.
Step 2: Determine Goals
Once a patient has identified their values, the health coach will shift their focus and have them brainstorm what they would like to focus on in their healing plan. This step is important because it will determine what they specifically want to change or improve. Some patients may feel unsure or are apprehensive, but allowing the patient time to journal or write out everything they want to accomplish, big or small, as well as the known steps or tasks, will help the patient get there.
When determining goals, the health coach will encourage the patient to create goals for multiple areas in their life. Some of these areas may include, health, family, relationships, and recreation. The health coach will encourage the patient’s goals by having them consider the following questions:
What do I want to achieve?
How will I achieve this goal?
Why do I want to reach this goal?
Who will I need to work with to achieve this goal?
What are the conditions and limitations to achieving this goal?
Based on the core areas and goals, the health coach will work with the patient to determine SMART goals. A SMART goal is a goal-setting technique that brings structure and trackability to goals. SMART goals stand for Specific, Measurable, Attainable, Relevant, and Timely. These create a verifiable trajectory towards a specific objective with clear milestones. By determining SMART goals, it clarifies how and when the goal will be achieved, rather than just stating a desire.
A health coach will help patients turn “I want to lose weight” into ” I want to lose 20 pounds to have more energy to play with my grandchildren. I will do so by exercising four times a week and eating less processed foods, and more fruits and vegetables. I will lose an average of two pounds every week for 10 weeks.”
By doing this, the health coach is working on a goal that immediately interests the patient and puts it into a way that is more attainable. The health coach can help the patient stay encouraged and motivated as they work together to achieve small successes, eventually leading to the patient being more willing to take on bigger challenges.
Using health coaching can be more beneficial than one might originally think. As one can see, they really go deep into one’s life and can help them in ways they might not have planned on originally. In the next article, the steps of building a plan for action and tracking progress and results will be discussed in great detail.
Changing your lifestyle can be difficult and does not happen overnight. Those who work with a coach to reach their goals are more successful and less likely to give up when things get difficult. Coaches are amazing for accountability, advice, health help, goal setting, and organizing expectations in a realistic timeline. Look at it this way: People use a wedding coordinator to help them oragnize food, timelines, expectations, etc. and that is for an event that lasts 1 day. So why are you not using a health coach to help you organize all of these same things for something that will last a lifetime? In addition you’re getting to help decide your future and gain a deeper undestanding of what lies ahead. Investing in yourself is one of the best things you can do for yourself. – Kenna Vaughn, Senior Health Coach
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
The information from this article was found in an article written by Integrative Practioner. The sources can be found listed below.
Resources:
American Psychological Association (2019). The Road to Resilience. Retrieved from: https://www.apa.org/helpcenter/road-resilience
Jonas, W. (2019). Empowering patients with chronic diseases to live healthier through health coaching: Integrative primary care case study. Samueli Integrative Health Programs.Retrieved from: https://www.health.harvard.edu/staying-healthy/give-yourself-a-health-self-assessment
Miller, W. and Rose, G. (1991). Motivational Interviewing: Preparing People to Change Addictive Behavior. Guilford Publications.
Pecoraro, Wendy. �A Six-Step Approach To Health And Wellness Coaching: A Toolkit for Practice Implementation.� Integrative Practitioner.Com, 2019.
Trzeciak, S. and Mazzarelli, A. (2019). Compassionomics. Studer Group. Virginia Polytechnic Institute and State University. The Stages of Change.�Retrieved from: http://www.cpe.vt.edu/gttc/presentations/8eStagesofChange.pdf
Your Coach (2009). SMART goals. Retrieved from: https://www.yourcoach.be/en/coaching-tools/
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine