Inversion tables and inversion treatment/therapy could help with low back/leg pain and sciatica. It�s non-surgical and an option your doctor, or chiropractor could recommend to you before looking into more invasive options. Individuals with low back pain, sciatica or both found inversion therapy with an inversion table provided relief from symptoms, and continued use has kept them and their spines healthy.
With an inversion table, you don�t have to use gravity boots or completely hanging upside down. There are inversion boots and hanging racks that also offer inversion therapy, this type is not for beginners. With experience, you can move on to this type but for now, leave it to individuals in top health and athletic condition. This type of inversion table therapy is an alternative that doesn’t require being completely upside down.
An Ancient Therapy Brought Back
Inversion therapy is nothing new. Hippocrates, the father of medicine, saw what inversion therapy could do and the benefits around 400 BC. The goal is to use gravity to release compression in the spine. The downward force pulls everything toward the earth’s center.
How It Works
Inversion therapy works in a way like spinal traction.
For example, when we stand and sit gravity pulls the spine downward and this is what compresses the discs, vertebral bodies, nerves, and other spinal structures. The physical dynamics along with gravity helps relieve spinal compression. As the spine is stretched out the pressure on your back is reduced.
The theory behind inversion therapy sounds like a fantastic non-surgical option to back pain. However, the research going into inversion therapy is a bit more mixed. One study found that almost 77% of patients that were candidates for surgery no longer needed the surgery after using inversion therapy. For patients that didn�t use inversion therapy, only 23% avoided surgery.
But like all back pain/sciatica treatment plans, it’s what works for you. Ask your doctor/chiropractor about the pros and cons of this type of treatment as it relates to your condition to make an informed decision.
Other Benefits
Many patients report that inversion therapy is a great way to:
Stretch the muscles and ligaments
Reduce muscle spasms
Improve circulation
Stretching stimulates the lymph glands which increases the flow of lymphatic fluids, that are part of the body’s waste disposal. Cellular health depends on healthy blood circulation to be delivered, to nourish and remove waste.
The therapy also helped to relieve motion sickness and stress. This is because the body is more aware of its spatial orientation along with balance as the inner ear gets stimulated while inverted. As stated earlier it is not necessary to be positioned completely upside down to benefit from this therapy. Inversion tables are adjustable and offer the flexibility to find the best angle.
Discuss Inversion Therapy with A Doctor
Before you start using an inversion table�talk to your doctor. Certain medications and health conditions could make using an inversion table unsafe.
It could be recommended against inversion table therapy if you have:
There could be other medical conditions that are not listed but could interfere with inversion therapy, so make sure your doctor knows all your medical history/conditions and current health state before beginning.
Starting Inversion Therapy
How to start an inversion therapy program? Take it very slow, easy, taking your time and have someone there to help and assist until you are comfortable doing it on your own.�The tables can be set at different angles and it is recommended you start at the first and work your way to the last. At the 15-degree angle, your body will feel a stretch along with the benefits of increased blood circulation.
Most people don’t have to go beyond 60-degrees, as the spine decompresses at this angle. But you might want to completely invert yourself as you work through the different degrees and go for the full inversion. But don’t overdo it and listen to what your body tells you.
The tables come in a variety of styles, so be sure to research the different brands. Some tables can include a sliding backrest and foot lock that lets you work in gentle stretching exercises during inversion. This could include head movements from side-to-side, stretching the arms overhead, and doing abdominal sit-ups or crunches.
But first, find out from your doctor how often you should invert and the kinds of movements that will help with your condition and enhance your inversion program. Inversion therapy is another option for a back, sciatic pain treatment plan. For the different forms of spine pain, a doctor will try several non-surgical treatment options before discussing surgery. Inversion therapy could be part of a conservative treatment plan and could help prevent the need for spine surgery.
*Effective Treatment* for Sciatic Nerve Pain| El Paso, Tx
NCBI Resources
The spine is the primary support for the body. When it breaks down, the body suffers. Regular chiropractic treatment ensures that the spinal column remains in proper alignment which, in turn, keeps the body in proper alignment. It helps with joint health as well as the health of the related muscles and ligaments.
Your chiropractor can also recommend stretching and strength-building exercises to help keep your spine healthy and supple. Chiropractic helps to keep the back flexible which aids in preventing injury. A healthy spine is also less likely to become misaligned or experience pain. It can significantly improve your quality of life as you are more flexible and mobile.
Dopamine and serotonin are known as the “happy chemicals” because they play a fundamental role in regulating our mood. These two neurotransmitters or chemical messengers control a variety of functions in the brain and body, including digestion and sleep. Although dopamine and serotonin are in charge of many of the same things, these happy chemicals do so in slightly different ways. Dopamine and serotonin deficiencies can also cause a variety of health issues, including mood changes and depression. In the following article, we will ultimately discuss the differences between dopamine and serotonin. �
What is a Neurotransmitter?
As previously mentioned, a neurotransmitter is a chemical messenger in the brain that sends signals to other areas of the body. Dopamine and serotonin are two of the many different types of neurotransmitters in the brain and body. Below is a list of some of the most well-known neurotransmitters, including: �
Dopamine
Serotonin
Norepinephrine
Acetylcholine
Glycine
Glutamate
GABA
Understanding Neurotransmitters
Our brain is one of the most complex organs in the human body. The nervous system contains more than 100 billion nerves which are continuously sending signals from the brain to the rest of the body, ultimately regulating our mental and physical health. However, various factors can cause many problems. Dopamine and serotonin deficiencies, by way of instance, can cause a variety of mental and physical health issues, such as depression. While these two neurotransmitters are both commonly referred to as “happy chemicals”, it’s important to understand that dopamine and serotonin also play different roles. �
What is Dopamine?
Dopamine is a well-known neurotransmitter released in the brain to send signals between nerve cells. Our brain and body use dopamine to produce other compounds known as norepinephrine and epinephrine. Dopamine plays a fundamental role in the “pleasure and reward center” in the brain, or a collection of functions in the brain that control mood, motivation, and movement. Healthy dopamine levels can also affect a variety of other functions, including: �
alertness
learning
mood
motivation
movement
blood circulation
urine output
sleep
What is Serotonin?
Serotonin is another neurotransmitter used to send signals between nerve cells. However, about 90 percent of the human body’s serotonin can be found in the gut, where it helps control a variety of functions in the digestive system. Healthy serotonin levels can also affect a variety of other functions, including: �
focus and concentration
mood, emotions, and feelings
appetite and digestion
hormonal activity
circadian rhythm or sleep-wake cycle
blood clotting
body temperature
Dopamine, Serotonin, and Depression
Depression is one of the most common and well-known mental health issues which is ultimately caused by a variety of factors, such as dopamine and serotonin deficiencies. Both of these neurotransmitters or chemical messengers can also play a fundamental role in depression, however, many healthcare professionals are still trying to understand the true cause of depression. Research studies have demonstrated that dopamine and serotonin deficiencies caused by other underlying health issues may be associated with depression. Several common symptoms of depression can ultimately include: �
decreased or reduced motivation
feelings of helplessness
loss of interest in things that used to interest you
Dopamine, Serotonin, and Other Health Issues
Because dopamine and serotonin play a fundamental role in a variety of functions in the brain and body, it is no surprise that these “happy chemicals” are also essential in our mental and physical health. When both of these neurotransmitters are functioning accordingly, they can ultimately help us feel happy and more emotionally balanced. As previously mentioned, however, dopamine and serotonin deficiencies can also cause various other health issues. � Doing anything that we find enjoyable, from eating a good meal to having sex, can trigger the release of dopamine in the brain and body. That release is what makes several things addicting like drugs and gambling. Scientists have determined that it doesn’t take long for the brain to associate several of these things with a release of dopamine. Research studies have also found that dopamine deficiencies may be associated with other health issues, such as: �
Parkinson’s disease
attention deficit hyperactivity disorder (ADHD)
schizophrenia
bipolar disorder
Furthermore, according to several research studies in 2014, serotonin deficiencies were also associated with a variety of other health issues, including: �
anxiety disorders
obsessive-compulsive disorder (OCD)
autism
bipolar disorder
What are the Differences Between Dopamine and Serotonin?
Dopamine and serotonin are both neurotransmitters or chemical messengers that send signals between the brain and body. However, the primary functions of these well-known “happy chemicals” are very different. Dopamine is associated with the pleasure and reward center in the brain while serotonin is associated with our mood and it is more of a stabilizer than a booster. Also, dopamine controls movement while serotonin controls digestion and sleep. �
Dopamine and serotonin are two well-known neurotransmitters, or chemical messengers, that play a fundamental role in our mood and a variety of other functions in the brain and body. Dopamine helps control mood, motivation, and movement while serotonin helps control positive feelings and social behavior, learning and memory, appetite as well as our circadian rhythm or sleep-wake cycle. Dopamine and serotonin deficiencies can cause a variety of mental and physical health issues, including anxiety, depression, Parkinson’s disease, schizophrenia, obsessive-compulsive disorder (OCD), and bipolar disorder. In this article, we will discuss the differences between the release of dopamine and serotonin in the brain and body.�- Dr. Alex Jimenez D.C., C.C.S.T. Insight
Dopamine and serotonin are known as the “happy chemicals” because they play a fundamental role in regulating our mood. These two neurotransmitters or chemical messengers control a variety of functions in the brain and body, including digestion and sleep. Although dopamine and serotonin are in charge of many of the same things, these happy chemicals do so in slightly different ways. Dopamine and serotonin deficiencies can also cause a variety of health issues, including mood changes and depression. In the article above, we ultimately discussed the differences between dopamine and serotonin. �
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.�
Curated by Dr. Alex Jimenez �
References:
Eske, Jamie. �Dopamine vs. Serotonin: Similarities, Differences, and Relationship.� Medical News Today, MediLexicon International, 19 Aug. 2019, www.medicalnewstoday.com/articles/326090.php.
Vandergriendt, Carly. �What’s the Difference Between Dopamine and Serotonin?� Healthline, Healthline Media, 5 Dec. 2018, www.healthline.com/health/dopamine-vs-serotonin.
Puskar, Michael. �What Is The Difference Between Serotonin And Dopamine?� Betterhelp, BetterHelp, 6 May 2018, www.betterhelp.com/advice/medication/what-is-the-difference-between-serotonin-and-dopamine/.
Neurotransmitter Assessment Form
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. The following symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance. �
Neural Zoomer Plus for Neurological Disease
�
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Food Sensitivity for the IgG & IgA Immune Response
�
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with a variety of food sensitivities and intolerances. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs. �
Gut Zoomer for Small Intestinal Bacterial Overgrowth (SIBO)
�
Dr. Alex Jimenez utilizes a series of tests to help evaluate gut health associated with small intestinal bacterial overgrowth (SIBO). The Vibrant Gut ZoomerTM offers a report that includes dietary recommendations and other natural supplementation like prebiotics, probiotics, and polyphenols. The gut microbiome is mainly found in the large intestine and it has more than 1000 species of bacteria that play a fundamental role in the human body, from shaping the immune system and affecting the metabolism of nutrients to strengthening the intestinal mucosal barrier (gut-barrier). It is essential to understand how the number of bacteria that symbiotically live in the human gastrointestinal (GI) tract influences gut health because imbalances in the gut microbiome may ultimately lead to gastrointestinal (GI) tract symptoms, skin conditions, autoimmune disorders, immune system imbalances, and multiple inflammatory disorders. �
Formulas for Methylation Support
� XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
� �
Modern Integrated Medicine
The National University of Health Sciences is an institution that offers a variety of rewarding professions to attendees. Students can practice their passion for helping other people achieve overall health and wellness through the institution’s mission. The National University of Health Sciences prepares students to become leaders in the forefront of modern integrated medicine, including chiropractic care. Students have an opportunity to gain unparalleled experience at the National University of Health Sciences to help restore the natural integrity of the patient and define the future of modern integrated medicine. �
Serotonin is a neurotransmitter that plays a fundamental role in a variety of brain and bodily functions. This chemical messenger helps regulate mood and social behavior as well as support our circadian rhythm or sleep-wake cycle. Research studies demonstrated that “healthy” serotonin levels are associated with positive feelings and longevity. We can naturally increase our serotonin levels by eating tryptophan-rich foods or taking tryptophan supplements. This essential amino acid is used to synthesize serotonin. In the following article, we will discuss foods that can help naturally increase serotonin. �
Pineapple
According to several research studies, eating pineapple may boost bromelain, a well-known protein that can help suppress coughs as well as reduce the side-effects of chemotherapy in the brain and body. Combine pineapple with other tryptophan-rich foods to also naturally increase your serotonin levels. �
Nuts and Seeds
All nuts and seeds are excellent sources of tryptophan. Research studies demonstrate that eating a handful of nuts and/or seeds every day can ultimately help lower your risk for respiratory health issues, heart disease, and cancer. Nuts and seeds are also excellent sources of vitamins, antioxidants, and fiber. �
Salmon
Salmon is a well-known tryptophan-rich food that also has a variety of other nutritional benefits, including being another tremendous source of omega-3 fatty acids as well as helping to lower blood pressure and regulate cholesterol. Combine salmon with other tryptophan-rich foods to boost serotonin. �
Turkey
There’s a good reason why many people take a relaxing nap on the couch after their Thanksgiving day meal. Turkey is basically filled with a lot of tryptophan. �
Eggs
According to research studies, the amount of protein that is found in eggs can considerably help naturally increase tryptophan levels in your blood plasma, leading to the production of serotonin. And always make sure to never leave out the egg yolks. Egg yolks contain omega-3 fatty acids, biotin, choline, tyrosine, tryptophan, and a variety of other nutrients, many of which can provide you with many health benefits. Eggs also have antioxidant properties. �
Cheese
Cheese is yet another tryptophan-rich food that you can eat to help naturally increase serotonin. Although you can eat many different types of cheese in a variety of ways, a popular meal you could make is mac and cheese which combines cheddar cheese with eggs and milk, other tryptophan-rich foods. �
Tofu
Eating plenty of soy products like tofu can also help naturally increase serotonin because these are also full of tryptophan. Substitute tofu for any protein source as an excellent source of tryptophan for vegetarians and vegans. Tofu or soy products are also calcium-set and can provide us with calcium. �
Nutrition and Serotonin
Because serotonin isn’t found in food, eating foods that have tryptophan, the amino acid used to synthesize serotonin, is fundamental to help naturally increase this neurotransmitter or chemical messenger in the brain and body. Eating foods that are also excellent sources of protein, iron, riboflavin, and vitamin B-6 generally have great amounts of this essential amino acid. However, eating tryptophan-rich foods alone won’t boost serotonin levels. Eating carbohydrates triggers the release of insulin which can promote the absorption of other amino acids while leaving more tryptophan in the bloodstream. �
Combining tryptophan-rich foods with carbs can help naturally increase serotonin in the brain and body. Tryptophan has to compete with many other amino acids in order to penetrate the BBB and enter the brain from the bloodstream which is why the tryptophan in the foods we eat may ultimately have a minor effect on serotonin levels. However, this effect is different from tryptophan supplements that have pure tryptophan which can considerably boost serotonin. Always make sure to talk to your healthcare professional before taking any supplements. Eating tryptophan-rich foods can safely help increase serotonin. �
Other Ways to Naturally Increase Serotonin
Eating tryptophan-rich foods and taking tryptophan supplements aren�t the only ways to naturally increase serotonin in the brain and body. �
Take probiotics. Eating fiber can support gut bacteria that play a fundamental role in serotonin levels through the gut-brain connection.
Do Exercise. Research studies have shown that doing regular exercise and physical activity can help balance your mood.
Get Sunlight. Getting plenty of sunlight is a common remedy for seasonal depression. Research studies have shown a connection between being exposed to sunlight and serotonin levels in the brain and body. To boost your mood, try getting enough (but not too much) sunlight.
Be Positive. Research studies have also shown that simply being more positive can naturally help increase serotonin levels.
Serotonin is a well-known neurotransmitter, or chemical messenger, that is associated with mood and a variety of other important functions in the human brain and body. Serotonin helps promote positive feelings and social behavior, control appetite, support learning and memory as well as regulate our circadian rhythm or sleep-wake cycle. Serotonin deficiencies can cause a variety of brain and mental health issues, including anxiety, depression, sleep problems, fatigue, abnormal appetite and cravings as well as nausea and digestive problems. Fortunately, eating tryptophan-rich foods can help naturally increase serotonin levels in the human brain and body. In the following article, we will discuss how eating certain well-known tryptophan-rich foods can help naturally increase serotonin as well as promote overall health and wellness.�- Dr. Alex Jimenez D.C., C.C.S.T. Insight
Serotonin is a neurotransmitter that plays a fundamental role in a variety of brain and bodily functions. This chemical messenger helps regulate mood and social behavior as well as support our circadian rhythm or sleep-wake cycle. Research studies demonstrated that “healthy” serotonin levels are associated with positive feelings and longevity. We can naturally increase our serotonin levels by eating tryptophan-rich foods or taking tryptophan supplements. This essential amino acid is ultimately used to synthesize serotonin. In the article, we discussed foods that can ultimately help naturally increase serotonin. �
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.�
Curated by Dr. Alex Jimenez �
References:
Healthline Editorial Team. �7 Foods That Could Boost Your Serotonin: The Serotonin Diet.� Healthline, Healthline Media, 29 Aug. 2018, www.healthline.com/health/healthy-sleep/foods-that-could-boost-your-serotonin.
Raypole, Crystal. �6 Ways to Boost Serotonin Without Medication.� Healthline, Healthline Media, 22 Apr. 2019, www.healthline.com/health/how-to-increase-serotonin.
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. The following symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance. �
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Food Sensitivity for the IgG & IgA Immune Response
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with a variety of food sensitivities and intolerances. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs. �
Gut Zoomer for Small Intestinal Bacterial Overgrowth (SIBO)
Dr. Alex Jimenez utilizes a series of tests to help evaluate gut health associated with small intestinal bacterial overgrowth (SIBO). The Vibrant Gut ZoomerTM offers a report that includes dietary recommendations and other natural supplementation like prebiotics, probiotics, and polyphenols. The gut microbiome is mainly found in the large intestine and it has more than 1000 species of bacteria that play a fundamental role in the human body, from shaping the immune system and affecting the metabolism of nutrients to strengthening the intestinal mucosal barrier (gut-barrier). It is essential to understand how the number of bacteria that symbiotically live in the human gastrointestinal (GI) tract influences gut health because imbalances in the gut microbiome may ultimately lead to gastrointestinal (GI) tract symptoms, skin conditions, autoimmune disorders, immune system imbalances, and multiple inflammatory disorders. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
� �
Modern Integrated Medicine
The National University of Health Sciences is an institution that offers a variety of rewarding professions to attendees. Students can practice their passion for helping other people achieve overall health and wellness through the institution’s mission. The National University of Health Sciences prepares students to become leaders in the forefront of modern integrated medicine, including chiropractic care. Students have an opportunity to gain unparalleled experience at the National University of Health Sciences to help restore the natural integrity of the patient and define the future of modern integrated medicine.
Everyone needs to take care of their back/spine because it is what holds us up as long as we keep it straight and strong. Strengthening the core can help prevent a weak and misaligned spine from getting worse and helps to eliminate pain.�
Back safety should be priority one, as it affects all aspects of your life. Not only are you protecting your back, but are preventing future injury. From the time you wake until bedtime, here are some tips for changes in sleeping position, and getting in and out of a car.
We all need to pay attention to proper body positioning and body mechanics, as it will pay off in the long run.
Getting In and Out of Bed
This is usually the time when the pain starts and can make the rest of the day miserable. Here are a few tips that can help.
Lean forward from your hips, not from your back.
Try not to arch your back.
Push your upper body off the bed with your elbows and hands and swing both legs to the floor.
Keep your back straight.
Try not to bend at the waist.
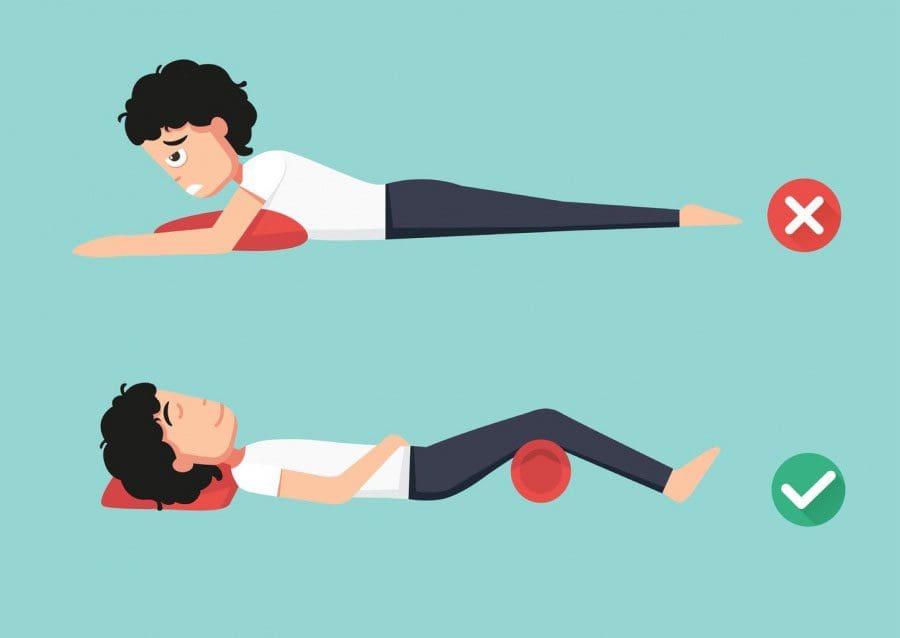
Position for Sleeping
Sleep is very important. Finding a comfortable position while sleeping can be tough, especially with back pain. Using quality pillows in the right way can help provide comfort, support for your neck and back and keep you asleep.
Sleeping on your back is optimal but you should bend your legs and place a pillow under your knees allowing for optimal blood circulation.
Do not sleep on your stomach, as this places pressure on the pelvis and the lower back because there is no support underneath. If you must sleep like this try to keep it for a short while before changing position and place a pillow or two underneath for support.
A firm mattress can help keep your spine in line. But talk to a doctor or chiropractor to find out what style of mattress would benefit your back.
Rotate your mattress every three months and flip it over twice a year.
Take Care When Entering/Exiting an Automobile
Getting in and out of a car can be a tough challenge when dealing with back pain. Here are a few tips to help.
When getting in or out move the seat back as far as it goes, hold onto the side of the car, back of the seat, or the dashboard for support when lifting yourself out or when easing into the seat.
Bend at the knees, not the back and avoid twisting and turning to reach for objects, etc.
The use of proper body mechanics keeps the muscles working properly.
Use both arms and legs when raising and lowering yourself in and out of the seat.
Keep your body aligned and only turn your body as much as needed.
The key is to be aware of your posture and safety awareness.
Daily living including sports and household chores should be done with overall and spinal safety in mind.
Whatever positions work for you and your regular activities bending, retrieving, lifting, and carrying objects, using correct techniques combined with proper posture will take care of your neck and back.
Back Pain Chiropractic Care | El Paso, Tx
NCBI Resources
Chiropractic can take care of your spine which means it is good for your overall health. While many people think that its only purpose is to treat back pain, chiropractic focuses on total body wellness. All too often problems within the body are interrelated. For instance, back pain could be the result of an altered gait due to an ankle injury.� A misaligned neck could cause a headache due to awkward sleep positions (or even the wrong pillow).
Serotonin is a well-known neurotransmitter that plays an essential role in various functions of the brain and body, including mood and digestion. This chemical messenger helps promote positive feelings and social behavior, control appetite, support learning and memory as well as regulate our circadian rhythm or sleep-wake cycle. However, serotonin deficiencies can also cause several health issues, including anxiety, depression, sleep problems, fatigue, abnormal appetite and cravings as well as nausea and digestive problems. In the following article, we will discuss natural ways to increase serotonin.
Eat Tryptophan-rich Foods
Although serotonin isn’t directly found in food, you can eat tryptophan-rich foods. Tryptophan is an essential amino acid that the brain and body use to turn it into serotonin. Tryptophan is found in high-protein foods, such as turkey and salmon. However, simply eating plenty of tryptophan-rich foods isn’t enough to help naturally increase serotonin levels. Tryptophan-rich foods are generally even higher in other essential amino acids and these other substances are more likely than tryptophan to cross the blood-brain barrier (BBB) or the protective shield that controls what compounds enter the brain from the bloodstream. Healthcare professionals believe that eating carbohydrates with tryptophan-rich foods can help more of this essential amino acid enter the brain.
Take Probiotics
Healthcare professionals recommend adding more probiotics into your diet as another natural way to increase serotonin. Taking probiotic supplements or eating probiotic-rich foods, such as yogurt and fermented foods like kimchi or sauerkraut, can trigger the release of tryptophan into the bloodstream.
Get Enough Sunlight
Several research studies have demonstrated that serotonin can typically be lower during winter and higher during summer. Scientists have also found that, because serotonin can affect our mood, changes in serotonin levels during different seasons may actually be associated with seasonal affective disorders as well as other brain and mental health issues also associated with the seasons. Scientists suggest that the skin may be able to synthesize serotonin.
Do Exercise and Physical Activity
Exercise and physical activity can also trigger the release of tryptophan into the bloodstream from the brain. It can also reduce the number of other essential amino acids. This can ultimately help create an excellent scenario for more tryptophan to penetrate the BBB and enter the brain from the bloodstream.
Take Supplements
According to healthcare professionals, taking dietary supplements can help trigger the release of serotonin by increasing tryptophan. However, make sure to talk to your healthcare professional before taking any new supplements to prevent further health issues. Also, make sure to tell them if you are taking any over-the-counter or prescription drugs/medications, vitamins, and minerals, as well as any herbal remedies. Choose supplements made by a well-known manufacturer that can be researched for reports on the quality of their products. Supplements can naturally help increase serotonin levels, including: �
Pure Tryptophan
Tryptophan supplements have more tryptophan than food which can make it more possible to penetrate the BBB and enter the brain from the bloodstream. A 2006 research study suggests that tryptophan supplements can also have an antidepressant effect in women but further evidence is still required.
SAMe (S-adenosyl-L-methionine)
Taking SAMe supplements also seems to help increase serotonin levels which can help improve symptoms, such as depression. However, it’s not recommended to take it with any other supplements or drugs/medications that increase serotonin, including certain antidepressants and antipsychotics.
5-HTP
The substance 5-HTP can penetrate the BBB and enter the brain from the bloodstream to trigger the release of serotonin. A 2013 research study demonstrated that 5-HTP supplements were as effective as antidepressants in people with early symptoms like depression. Other research studies on taking 5-HTP supplements to help naturally increase serotonin and reduce symptoms of depression have ultimately demonstrated mixed results.
Get a Massage
Massage therapy can also help naturally increase serotonin as well as dopamine neurotransmitter or chemical messenger that controls mood and various other functions in the brain and body. Getting a massage can also help decrease cortisol, a hormone that is released by the brain with stress. Although you can visit a licensed massage therapist, this may not always be necessary. A 2004 research study evaluated 84 pregnant women with depression. The women who received massage therapy twice a week reported feeling decreased symptoms of depression and had increased serotonin levels.
Serotonin is a neurotransmitter, or chemical messenger, associated with mood and a variety of other functions in the human brain and body. Serotonin helps promote positive feelings and social behavior, control appetite, support learning and memory as well as regulate our circadian rhythm or sleep-wake cycle. Serotonin deficiencies can cause a variety of brain and mental health issues, including anxiety, depression, sleep problems, fatigue, abnormal appetite and cravings as well as nausea and digestive problems. In the following article, we will discuss natural ways to increase serotonin, including eating tryptophan-rich foods, taking probiotics, doing exercise/physical activities, and taking supplements, among several others.�- Dr. Alex Jimenez D.C., C.C.S.T. Insight
Serotonin is a well-known neurotransmitter that plays an essential role in various functions of the brain and body, including mood and digestion. This chemical messenger helps promote positive feelings and social behavior, control appetite, support learning and memory as well as regulate our circadian rhythm or sleep-wake cycle. However, serotonin deficiencies can also cause several health issues, including anxiety, depression, sleep problems, fatigue, abnormal appetite and cravings as well as nausea and digestive problems. In the article above, we discussed natural ways to increase serotonin.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.�
Curated by Dr. Alex Jimenez
References:
Raypole, Crystal. �6 Ways to Boost Serotonin Without Medication.� Healthline, Healthline Media, 22 Apr. 2019, www.healthline.com/health/how-to-increase-serotonin.
[wp-embedder-pack width=”100%” height=”1050px” download=”all” download-text=”” attachment_id=”52657″ /]
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. The following symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue.
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention.
Food Sensitivity for the IgG & IgA Immune Response
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with a variety of food sensitivities and intolerances. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs.
Gut Zoomer for Small Intestinal Bacterial Overgrowth (SIBO)
Dr. Alex Jimenez utilizes a series of tests to help evaluate gut health associated with small intestinal bacterial overgrowth (SIBO). The Vibrant Gut ZoomerTM offers a report that includes dietary recommendations and other natural supplementation like prebiotics, probiotics, and polyphenols. The gut microbiome is mainly found in the large intestine and it has more than 1000 species of bacteria that play a fundamental role in the human body, from shaping the immune system and affecting the metabolism of nutrients to strengthening the intestinal mucosal barrier (gut-barrier). It is essential to understand how the number of bacteria that symbiotically live in the human gastrointestinal (GI) tract influences gut health because imbalances in the gut microbiome may ultimately lead to gastrointestinal (GI) tract symptoms, skin conditions, autoimmune disorders, immune system imbalances, and multiple inflammatory disorders.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download* All of the above XYMOGEN policies remain strictly in force.
Modern Integrated Medicine
The National University of Health Sciences is an institution that offers a variety of rewarding professions to attendees. Students can practice their passion for helping other people achieve overall health and wellness through the institution’s mission. The National University of Health Sciences prepares students to become leaders in the forefront of modern integrated medicine, including chiropractic care. Students have an opportunity to gain unparalleled experience at the National University of Health Sciences to help restore the natural integrity of the patient and define the future of modern integrated medicine.
Sitting is wonderful, however, sitting for too long is considered worse than smoking. Sitting for too long could be considered a disease. Today’s society is about technology. However, this technology involves a great deal of inactivity and sitting for a long time. This behavior has been linked to chronic disease and on a variety of health issues not to mention the havoc, it inflicts on your spine.
Unfortunately, many work environments encourage their employees to sit for hours and hours without any kind of movement except for using the bathroom. Something has to change because as someone said, “if you don’t take the time to focus on yourself and your health, you will be forced to take the time to focus on your illness.”
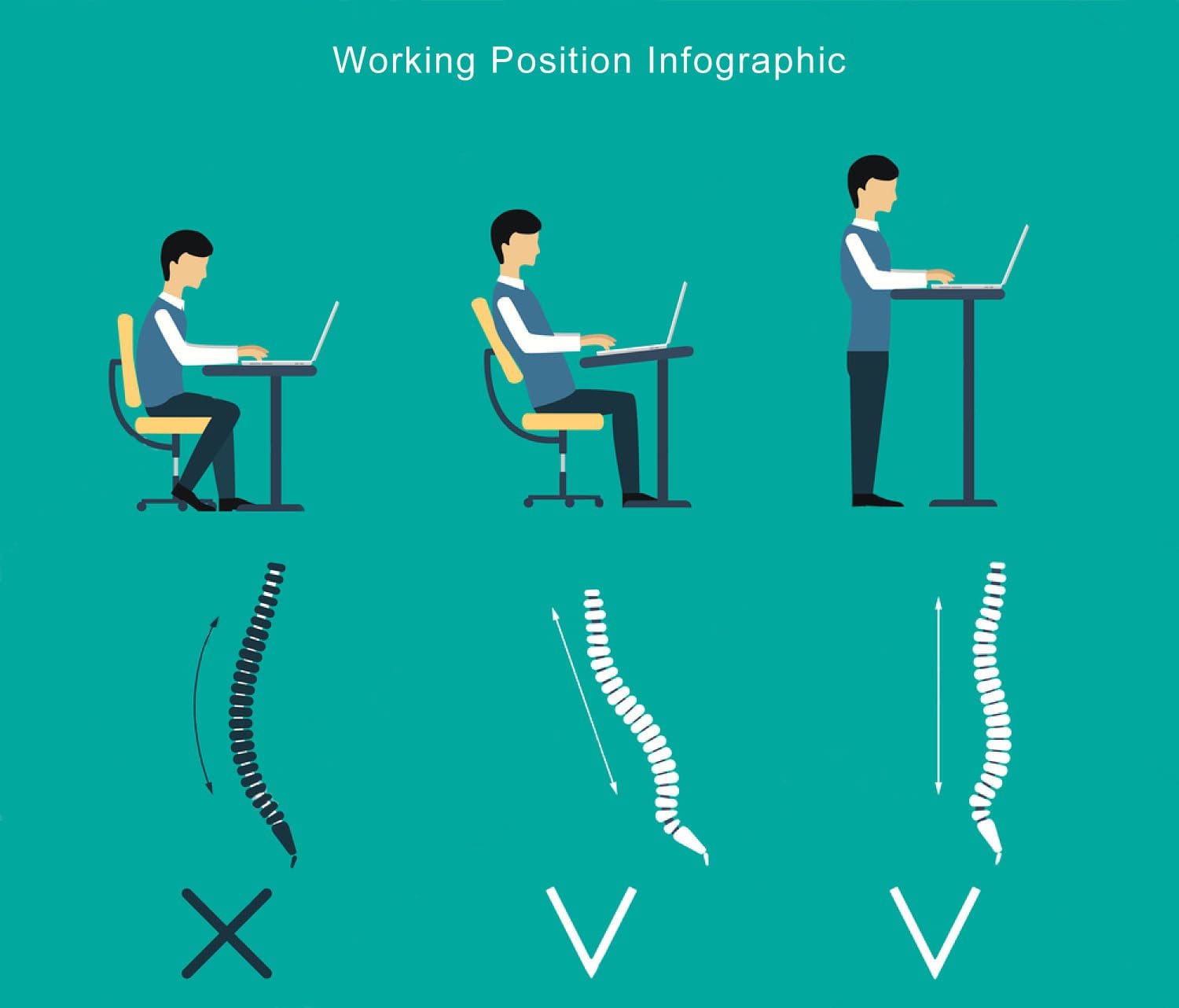
The Sedentary Work Lifestyle
Being in front of a computer all day may be part of the job, however, the goal is to bring in more activity into the day. This can be accomplished by maintaining proper posture through exercise, stretching and if need be to invest in a sit-stand desk.
Understanding why you should avoid long bouts of time sitting, means you need to know the research about what the medical community is dubbing the sitting disease.
Health Hazards of Sitting Too Long
Up to 80% of people sit for six or more hours every day, according to a study from the National Health and Nutrition Examination Surveys. Whether at work, plopped down in front of the TV,� or the daily commute doesn’t matter, the point is that people are spending long hours sitting down and the impact of inactivity is not good.
Individuals that sit for prolonged periods have a greater risk of dying from all causes. This is because a sedentary lifestyle has been shown to increase the risk for:
Cardiovascular disease
Cancers (breast, colon, colorectal, endometrial, and epithelial ovarian)
Type 2 diabetes in adults
These results came from 47 studies that focused on the health effects of being sedentary. These included the types of activity people engage in, from leisure activities to strong physical activity. Those who did not exercise had the greatest risk of health problems with being sedentary. Adding only two minutes of light exercise for every hour spent sitting lowers the risk of presenting health issues/conditions by one-third, according to the Clinical Journal of the American Society of Nephrology study.
The Way Sitting Hurts the Back and Neck
Spending the majority of the day every day in a seated position will eventually take its toll leaving your spine sore, stiff, and in pain. Too much sitting puts stress on the muscles and discs of the back and neck.
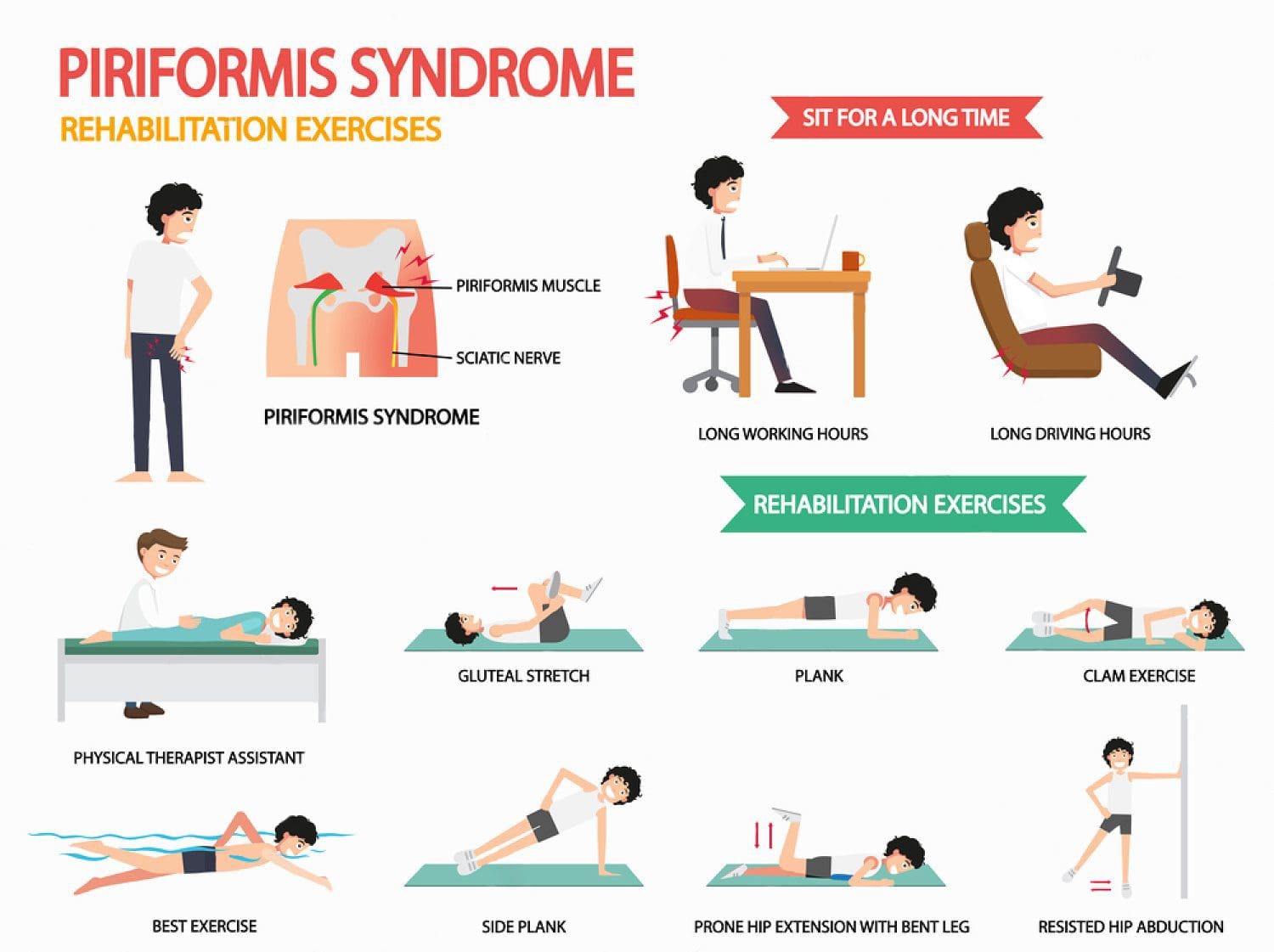
What happens from all the sitting is tightness in the hip flexors like the iliopsoas muscle forms, along with pressure and restricted blood flow in the muscles of the gluteus maximus. This muscle supports a good amount of the weight placed on the spine.
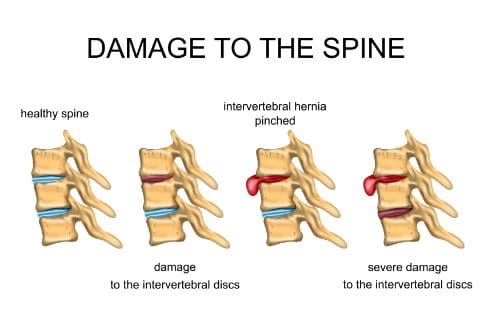
The longer individuals continue to repeat unhealthy sitting behavior, the higher the risk their posture begins to fall into slouching, into incorrect posture and possibly into spinal conditions and diseases. Slouching over time causes the ligaments to stretch beyond their healthy limit, combined with poor posture strains the spinal discs that can lead to herniation, bulging and complete loss of the intervertebral discs.
This results in added strain to the outer annulus of the disc and increases disc bulging and disc pressure.
When sitting, it’s usually at a computer/working on tasks at a desk that results in the head being in a constant forward position, with rounded shoulders that results in what is known as poor posture syndrome. Staying in the office chair or any chair too long leads to an isolated episode of back or neck pain/soreness. What’s happening is that the normal wear and tear of the spinal discs is sped up from the unhealthy weight and pressure being placed on the spine. This results in back pain that becomes a regular daily thing instead of an occasional problem.
Ergonomic chairs, sit-stand desks, fitness/stability balls and utilizing proper posture/exercises are tools to help mitigate the damage of sitting all day.
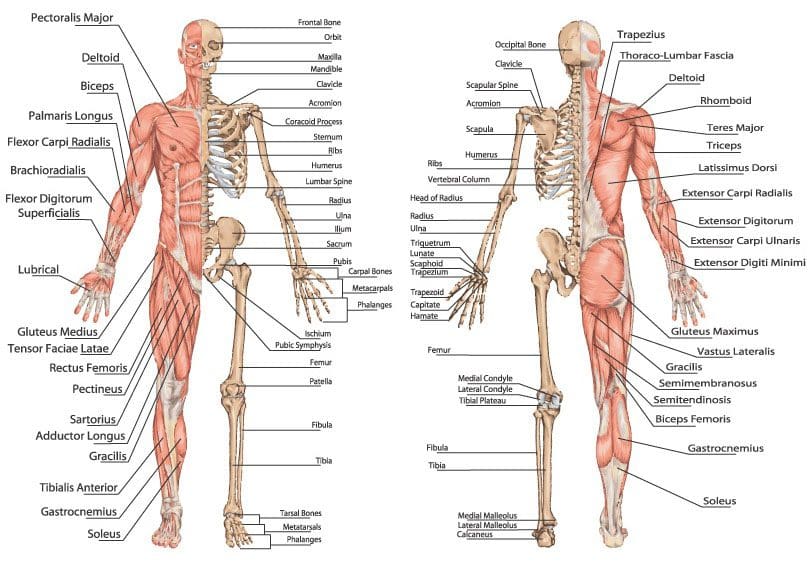
This includes stretching the muscles like the:
Pectorals
Scalene muscles in the neck
Hip flexors
Strengthening the muscles that are not used is very important. Muscles like the abdominals, glutes, back extensors and scapular muscles will bring back the spine�s normal balance, improving posture and getting relief from pain. Varying posture is another great way to exercise different muscles and ligaments by occasionally standing and moving around for a few minutes every half-hour. This keeps joints, muscles, tendons, and ligaments loose and pain-free.
Work Health
We�ve all been there working, typing feeling the positive flow and then you see two hours have passed and you haven�t gotten up from your chair at all.
Experts recommend activity every 20-30 minutes, with 20 minutes of standing per hour. Desk technology has arrived and wants to keep employees healthy. Sit-stand desks are proving to be highly beneficial to companies throughout the country. These desks allow you to transition from sitting to standing while your desk stays the same.
Standing at work has shown to boost productivity all the while allowing you to readjust posture, lose weight by burning 30% more calories and keeps your spine healthy.
Stand Up
Even without a sit-stand desk, there are still ways of combating sitting disease and protecting your spine. Consider:
Doing some work standing up at a high table or counter.
Walk laps during discussions so you and your co-workers get some movement.
Take stand-and-stretch breaks every 30 minutes, set a timer if you have to.
Walk to a coworkers office to tell them in person instead of emailing/texting.
Park your car a little bit further from the office to work your steps.
After lunch walk around or do some stand-up work as this will help with digestion.
This will reduce your sitting throughout the day. Remember that changing posture is good for your back and neck, but don�t take it to the other extreme and stop sitting. It’s all about mixing it up. Sitting, standing, and moving around throughout the day is the best way to keep your spine/body-safe, and in optimal health at work and home.
Low Back Pain Relief! | El Paso, Tx
NCBI Resources
This may sound melodramatic, but it�s true. As we talked about above, sitting for prolonged periods of time puts you at greater risk of diseases that may end up killing you.�A study�published in the Archives of Internal Medicine, �found people who sat for over 11 hours a day had a 40% greater risk of dying within three years from any cause than people who sat less than 4 hours a day.�
Detailed lab testing is becoming more and more essential as integrative medicine is on the rise. Detailed lab testing goes more in-depth than the traditional blood levels usually taken. This allows physicians to understand more of the underlying issues that are causing the patients headaches, inflammation, pain, or overall discomfort.
There are multiple lab companies that utilize top of the line technology in order to obtain the best results for the patient. By running a detailed test, it allows more data to be collected and the physician to get a deeper look at what the patient might be lacking.
SpectraCell
One test that is extremely detailed and allows an abundance of information is the Micronutrient test from SpectraCell. Micronutrients are essential for the body to function properly. The body requires macronutrients and micronutrients. Macronutrients are those obtained through the diet, such as protein, carbohydrates, and fat. Micronutrients are vitamins and minerals that the body needs to achieve proper nutrition.
The Micronutrient test came from Dr. William Shive who was a biochemist that realized many serum (blood tests) do not adequately show the number of vitamins and minerals in an individual. In turn, the labs are not a true number of the patients health.
The Micronutrient test from Spectracell is unique because it is the only test on the market that obtains a history of 4-6 months from inside the cells. Thus, allowing practitioners and patients to see if their cells are truly healthy and what they are lacking in.
Who Should Be Tested?
Micronutrients are needed to perform almost all metabolic processes in the body. When these essential vitamins and minerals are lacking, the body is more prone to degenerative processes like arthritis.
Getting tested can provide an inside look at what is actually happening in your body. This can shine some light and possibly even explain some health symptoms you’ve been struggling with. Due to the fact that micronutrients are needed in the body and not having them does affect your health, getting tested could help prevent a compromised immune system.
Applications
As mentioned earlier, this test measures micronutrients, which are essential vitamins and minerals in the body. But, what else can this test really tell an individual besides the fact that they’re lacking in vitamin D?� This test can help provide measures for:
Diabetes
Alzheimer’s
Mood Disorders
Osteoporosis
Fatigue
Sports Performance Optimization
SpectraCell is all about giving their patients high-end results that lead to real solutions. By creating a test that captures the functional level and the actual capability of the nutrients present in the white blood cells, it allows physicians to see a patient’s metabolism from a different standpoint. Getting tested could be the first step towards a healthier future.
SpectraCell is an amazing company, which is why we use them! This test is very detailed and provides us with a great deal of information. The science behind this test not only allows our patients to feel better by getting on the correct vitamin regimen for their body but also by allowing us to treat patients on an individualized level without the guesswork. – Kenna Vaughn, Senior Health Coach
*All information for this article was found onSpectraCell.com and is properly cited below
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request.�
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine